

ABSTRACT
Introduction:
In March 2020, due to the pandemic caused by COVID-19, a pilot experience of pharmaceutical continuity of care received by hospital outpatients was launched in Cantabria, a Spanish autonomous community. Thanks to this experience, the medication was dispensed by the hospital pharmacy through the community pharmacy of the patient’s choice. Our objective was to estimate the costs avoided by this practice during the months of April and May 2020.
Methods:
The analysis of the economic impact was carried out in terms of saved costs, from the hospital and from the social perspective. Savings associated with the avoided home delivery of medication and avoided labor productivity losses were calculated, as well as the time associated with avoided trips in monetary terms.
Results:
A total of 2,249 hospital-dispensed drugs were delivered through the community pharmacy in the analyzed period, with an average of 57.7 daily deliveries. The experience, which involved one hospital and 262 pharmacies of Cantabria, saved patients 93,305 km in trips to the hospital, associated with an average time saving of 1,374 hours. In terms of costs, the hospital saved on shipments by courier, estimated at €30,205, since it was the community pharmacy and the distribution warehouses that delivered the drugs. From a social perspective, this initiative saved €23,309 due to the trips (€8,907) and productivity losses (€14,402) that were avoided.
Conclusions:
This exceptional situation may be a good opportunity to improve the coordination between hospital pharmacies and community pharmacies in Spain, not only during the pandemic but also in the post-COVID-19 era.
Keywords: Community pharmacy, Continuity of care, COVID-19, Hospital pharmacy, Spain, Telepharmacy
Introduction
In March 2020, the pandemic caused by the SARS-CoV-2 coronavirus (COVID-19) forced the Spanish authorities to confine the population, an unprecedented milestone in recent history. The rapid increase in infections and hospitalizations caused the Spanish National Health System to experience an unknown pressure on healthcare to date. The peak of the pandemic, reached in mid-April, caused the saturation of many hospital intensive care units.
This situation forced the rapid launch of organizational innovations that might otherwise have taken years to become a reality. Among them, the creation of parallel care circuits, the flexibilization of some healthcare processes, the significant increase in teleconsultations, and the quick purchases of healthcare materials stand out.
In Spain, a country with decentralized health competencies, some specialty drugs are dispensed by hospital pharmacies. During the COVID-19 pandemic, some regional health services incorporated new features in the dispensing of these drugs. In particular, the Spanish Society of Hospital Pharmacy designed a new protocol regarding the dispensing of medication to outpatients. This protocol included, among other measures, promoting the delivery of drugs by appointment, extending delivery schedules to space out appointments, limiting the presence and/or overlap of patients within the Pharmacy Service, and promoting home delivery for those patients in home isolation due to positive coronavirus diagnosis or to avoid possible contagion (1).
Cantabria is an autonomous community of about 5,300 km2 and 583,000 inhabitants in the north of Spain. This region is geographically divided into 42 basic health areas and, at the time of this study, had four public hospitals and 274 community pharmacies (2,3). During the central phase of the lockdown (April and May 2020), a joint action of continuity of care between community pharmacies and hospital pharmacies was designed and carried out in Cantabria, with the purpose of avoiding patient visits to the hospital and all their associated risks. In this pilot experience, some of the hospital drugs dispensed on an outpatient basis by three hospital pharmacies were temporarily picked up at the patient’s previously chosen community pharmacy, where an informed supply of the drugs was carried out. In all cases the patients were informed about the dosage regimen of the medication by the community pharmacist. Therefore, all supplies can be considered as informed deliveries.
The objective of this work was to estimate the costs avoided due to this pilot experience of pharmaceutical continuity of care in Cantabria during April and May 2020, from the perspective of the hospital and from the social perspective.
Methods
For the purpose of implementing this pilot experience, a joint protocol involving hospital pharmacies and community pharmacies was developed in order to ensure adequate pharmaceutical care, drug distribution, dispensing, informed delivery, and traceability. Patients who were likely to be involved in this experience were first identified, following the order of appointments made for hospital pharmaceutical care consultations, which became telematic during the lockdown (4). During the telephone consultations, patients were informed of the possibility of collecting their medication from their chosen community pharmacy. Verbal consent was requested. For technical and legal purposes, the hospital remained responsible for the dispensing of these drugs. The ease of a bidirectional communication between the hospital pharmacy and the community pharmacy was one of the items developed in the protocol.
The data analyzed were provided by the Official College of Pharmacists of Cantabria and correspond to the Marqués de Valdecilla University Hospital in Santander, the capital of Cantabria, which was the only hospital with sufficient information to carry out the analysis. The hospital’s database collected information on the individual drugs that were dispensed in community pharmacies under this experience during April and May 2020.
The analysis of the economic impact of this pilot experience was carried out in terms of saved costs, from the perspective of the hospital and from the social perspective (Tab. I).
TABLE I -.
Description of each avoided cost, any assumption made, method used for its monetization, and unit cost applied
| Type of avoided cost | Assumption | Monetization method | Unit cost applied |
|---|---|---|---|
| To the hospital: cost of avoided deliveries | All deliveries that were carried out | Cost estimation based on whether or not the drug required CCM, and considering the possibility of grouping same-day deliveries to the same CPh in one single package | External parcel delivery company fees for nonurgent deliveries <1 kg: €9.90 without CCM and €20.04 with CCM (5) |
| To society: cost of avoided trips to hospital | CPh located in a municipality outside of Santander | Cost estimation based on the distance from the hospital to the CPh (in kilometers) | Cantabria’s official tariff assigned to patient travel: €0.10 per kilometer (6,7) |
| To society: cost of avoided labor productivity losses | CPh located more than 1 km away from the hospital | Cost of avoided traveling time, calculated as the average disposable income adjusted by the population size of the municipality | Average disposable income per hour worked (assumed to be 37.5 h per week): between €8.40 and €12.9 per hour (8) |
CCM = cold chain maintenance; CPh = community pharmacy.
From the hospital’s perspective, the new informed delivery circuit, which was exceptional in nature, was completely altruistic for the public healthcare system, since the cost of delivering the drugs was borne by the distribution warehouses and the community pharmacies involved in the experience. Savings associated with the avoided home delivery of medication were calculated as the costs that the hospital would have incurred had medication been delivered through a private courier. The need for cold chain maintenance, if any, was taken into account (5). Medicines delivered on the same day by the same community pharmacy were considered a single shipment from the hospital.
From the social perspective, which includes both the public health service of Cantabria and society in general, only two avoided costs were taken into account: 1) those associated with the patients’ trips to the hospital and 2) labor productivity losses related to the time that would have been spent on these trips.
To perform the analysis, once the baseline data were properly cleaned, we extracted the exact address of each community pharmacy chosen by the patients in this experience (2). Using Google Maps, we obtained the exact distance between each pharmacy and the Marqués de Valdecilla University Hospital, and the average time associated with each corresponding trip (by car).
Based on this information, the cost associated with the trips avoided by patients was obtained by applying the official public rate of Cantabria (€0.10 per km) to round trips outside of Santander (6,7). Avoided labor productivity losses were estimated by calculating the time associated with avoided trips in monetary terms. This monetization was done by applying the average disposable income per hour and adjusted to the population size of the municipality where each community pharmacy was located (8).
Results
Descriptive analysis
The pilot experience led to the informed delivery of 2,249 medications from community pharmacies throughout the 2 months of the analysis, with an average of 57.7 (standard deviation [SD] 28.5) informed deliveries per day. The number of informed deliveries decreased over time, which was consistent with the improvement of the pandemic, with a 66% correlation rate between the number of daily informed deliveries and the evolution of hospitalizations due to COVID-19 at the Marqués de Valdecilla University Hospital (9) (Fig. 1).
Fig. 1 -.
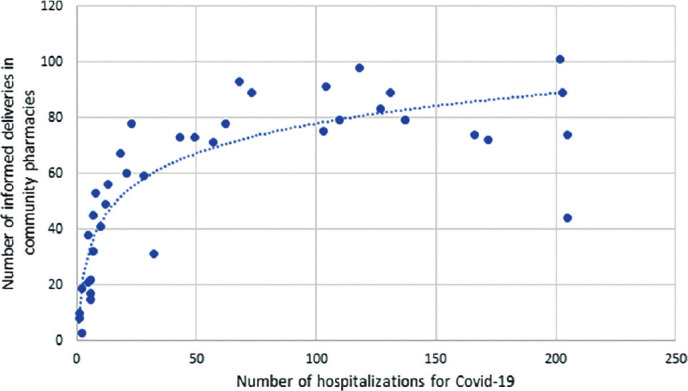
Relationship between the number of informed deliveries in community pharmacies and the number of patients hospitalized for COVID-19 at the Marqués de Valdecilla University Hospital, April-May 2020.
Overall, 262 community pharmacies, located in 86 of the 102 municipalities of Cantabria (84%), participated in this pilot experience. These pharmacies serve 99.0% of the population of this autonomous community. Most deliveries (34.9%) were carried out in Santander, the only municipality with over 100,000 inhabitants, by its 85 pharmacies (32%). Almost one-fifth of all informed deliveries were performed in the 65 pharmacies located in highly rural municipalities (less than 5,000 inhabitants), hence bearing the highest average informed delivery ratio per 1,000 inhabitants (Tab. II).
TABLE II -.
Descriptive analysis of informed deliveries, by municipality population size
| Municipality population size (inhabitants) | Municipalities | Community pharmacies | Informed deliveries | Mean informed deliveries per 1,000 inhabitants | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| 100,001-500,000 | 1 | 1.2 | 85 | 32.4 | 784 | 34.9 | 4.54 |
| 50,001-100,000 | 1 | 1.2 | 22 | 8.4 | 95 | 4.2 | 1.84 |
| 20,001-50,000 | 3 | 3.5 | 28 | 10.7 | 327 | 14.5 | 3.74 |
| 10,001-20,000 | 5 | 5.8 | 24 | 9.2 | 312 | 13.9 | 4.64 |
| 5,001-10,000 | 11 | 12.8 | 32 | 12.2 | 300 | 13.3 | 3.79 |
| 1,000-5,000 | 45 | 52.3 | 51 | 19.5 | 378 | 16.8 | 3.78 |
| <1,000 | 20 | 23.3 | 20 | 7.6 | 53 | 2.4 | 4.76 |
| TOTAL | 86 | 100.0 | 262 | 100.0 | 2,249 | 100.0 | 4.04 |
Overall, 53.05% of the drugs delivered required cold chain maintenance. With regard to route of administration, 42.02% of the informed deliveries were subcutaneous drugs and 41.35% were oral medications (Tab. III).
TABLE III -.
Distribution of delivered drugs, by route of administration and need of cold chain maintenance
| Route of administration | No cold needed (n = 1,056) | Cold needed (n = 1,193) | Total (2,249) |
|---|---|---|---|
| Subcutaneous | 5.11% | 74.69% | 42.02% |
| Oral | 84.85% | 2.85% | 41.35% |
| Intravenous and subcutaneous | 0.95% | 19.20% | 10.63% |
| Other combinations | 6.72% | 1.93% | 4.18% |
| Other routes* | 2.37% | 1.34% | 1.82% |
| TOTAL | 100% | 100% | 100% |
*Other routes of administration: cutaneous, inhalation, intestinal, and ophthalmic.
Two-thirds of the drugs delivered through this initiative were antineoplastic and immunomodulatory agents (Tab. IV). Overall, 59.7% of the drugs were classified as hospital diagnosis, while 32.5% were for hospital use, and the remaining 7,8% were drugs used in special situations. Most of the latter were aimed at pathologies related to the cardiovascular system.
TABLE IV -.
Distribution of delivered drugs by ATC1 code (organ or system in which the drug acts) and by type of prescription
| ATC1 Code | Hospital diagnosis (%) | Hospital use (%) | Drugs used in special situations (%) | Overall total (%) |
|---|---|---|---|---|
| L – Antineoplastic and immunomodulating agents | 89.3 | 27.9 | 16.9 | 63.7 |
| B – Blood and blood-forming organs | 0.7 | 27.4 | 0.6 | 9.3 |
| J – Anti-infectives for systemic use | 0.8 | 25.2 | 1.7 | 8.8 |
| C – Cardiovascular system | 1.8 | 6.6 | 57.1 | 7.7 |
| N – Nervous system | 1.4 | 7.1 | 3.4 | 3.4 |
| A – Alimentary tract and metabolism | 0.8 | 1.2 | 16.9 | 2.2 |
| H – Systemic hormonal preparations, excluding sex hormones and insulins | 1.3 | 3.0 | 1.7 | 1.9 |
| R – Respiratory system | 2.0 | 0.1 | 0.6 | 1.3 |
| S – Sensory organs | 1.4 | 0.0 | 0.0 | 0.8 |
| G – Genitourinary system and sex hormones | 0.0 | 1.4 | 0.0 | 0.4 |
| D – Dermatological | 0.4 | 0.0 | 0.6 | 0.3 |
| V – Miscellaneous | 0.1 | 0.0 | 0.6 | 0.1 |
| Overall total | 100 | 100 | 100 | 100 |
ATC = Anatomical, Therapeutic, Chemical classification system.
Cost estimate
This continuity of care pilot experience carried out at the Marqués de Valdecilla University Hospital saved patients a total of 93,305 km in two-way trips to the hospital. These avoided trips were associated with a total saved time of 1,374 hours. Trips avoided from outside the municipality of Santander amounted to a total of 89,073 km (Tab. VI, supplementary material).
This initiative involved a total of 1,939 shipments by the hospital to community pharmacies (53.33% of them requiring cold chain maintenance). From the hospital perspective, this experience prevented the hospital from making shipments by courier, estimated at €30,205 in total.
From a social perspective, the initiative saved €23,309 in total, including the costs of avoided trips (€8,907) and avoided productivity losses (€14,402) (Tab. V). If extrapolated to a year, this avoided social cost figure would amount to approximately €139,860 per year.
TABLE V -.
Estimate of hospital and social costs avoided by the initiative
| Perspective | Costs avoided | Amount |
|---|---|---|
| Hospital | Home delivery of medication avoided by the Health Service of Cantabria | €30,205 |
| Social | Patient trips avoided by the Health Service of Cantabria | €8,907 |
| Productivity losses avoided | €14,402 | |
| TOTAL | €23,309 |
According to a subgroup analysis, 58% of the €23,309 saved from a social perspective corresponded to drugs for hospital diagnosis, while 35% were drugs for hospital use. Almost two-thirds of the social costs avoided were associated with antineoplastic and immunomodulatory agents. Finally, by type of administration route, 39% of the avoided social cost corresponded to subcutaneous drugs (Tabs. VII, VIII, and IX, supplementary material).
Discussion
Catalonia, Andalusia, Aragon, La Rioja, and Cantabria are among the autonomous communities that implemented circuits of continuity care, organizing deliveries with community pharmacies (10-13). To our knowledge, our study presents the first detailed analysis of the economic impact of such experience on hospitals and on society that has been published in Spain to date. This temporary initiative for the delivery of medicines in the community pharmacy allowed the hospital to save private courier costs associated with medication home delivery, estimated at €30,205 in 2 months (this is equivalent to 0.04% of the hospital pharmaceutical expenditure of Cantabria in April and May (14)). The magnitude of the economic impact would have been even greater had the study been extended to 100% of the hospitals in Cantabria.
During the COVID-19 pandemic, hospital pharmacy departments in Spain have been forced to reorganize their procedures in order to face a conflicting scenario. On the one hand, the Royal Decree that supported the State of Alarm (an emergency procedure in Spain that limits the freedom of movement) allowed individuals, as an exception, to leave the house to pick up medication, either at the community pharmacy or at the hospital. On the other hand, the authorities strongly urged all citizens not to visit hospitals in order to prevent the spread of the virus (15).
The health crisis caused by the pandemic has been an ideal time to implement telepharmacy services along with the more traditional outpatient services provided by hospital pharmacies. In Spain, this transformation has been largely promoted within the Strategic Map for Outpatient Care (or MAPEX after its Spanish initials), although legal adjustments were required (16).
Before this health crisis, 83.2% (95% confidence interval [CI]: 77.1-88.3%) of the Spanish National Health Service hospitals carried out face-to-face pharmaceutical care activities only, including the delivery of medication (17). In contrast, during the first 6 weeks of confinement, remote pharmaceutical care and informed dispensing were used by over 80% of outpatients in the 41 hospitals included in the study by Tortajada et al. (17). The main procedure was home dispensing (87% of deliveries), whereas 5.6% of all deliveries were made in coordination with community pharmacies.
The initiative that we have analyzed in this article was carried out in Cantabria. It started in March 2020 with 110 pharmacies and focused on providing services to the most vulnerable patients (immunosuppressed patients, with respiratory or mobility problems). As the health situation worsened, the program was extended to all hospital pharmacy outpatients (18). In the end, practically all community pharmacies in Cantabria (262 out of 274) participated in this experience (19). The average number of medicines delivered through this initiative was approximately 58 per day. This is more than a third of the medicines usually dispensed on an outpatient basis by the pharmacy service of the Marqués de Valdecilla University Hospital, which treats about 163 patients daily (20). Our analysis showed that most of the drugs delivered were antineoplastic and immunomodulatory agents, indicating that the initiative largely helped the most vulnerable patients. Another aspect to highlight from our results is that almost 8% of the informed deliveries were drugs dispensed in special situations.
As we have shown, this pilot experience has spared patients from unnecessary trips to the hospital during the crisis caused by COVID-19. The initiative prevented not only the patients but also their caregivers from visiting the hospital, which entailed savings in terms of travel costs and time, especially when patients and caregivers inhabited the most remote areas outside the capital. In addition, we could also refer to other potential advantages of the initiative, which should be confirmed in future studies. Picking up the drug at the community pharmacy may have allowed the patient to establish a more humanized, personalized, and continuous contact than if the delivery had been done by a courier, thus benefiting from pharmaceutical advice. The latter may have led to greater safety, adherence, and therapeutic compliance, key aspects to reinforce during a crisis situation such as the one caused by COVID-19, which forced delays in continuous and direct contact with the system. Another potential advantage of this experience may be that it spared the patients the suffering and fear associated with having to visit the hospital in the middle of the pandemic, as well as the risk of possible contagion. Moreover, the flexibility of community pharmacies with regard to the schedule could have been another potential benefit to patients compared to hospital dispensing. Because of these benefits the initiative was supported by the Spanish Patient Forum (21).
Other studies support our claim that this initiative had many benefits other than cost savings. A recent internal survey carried out by the Pharmacist Chamber of Cantabria reveals the high degree of satisfaction shown by the patients who participated in this pilot experience. Over 70% of respondents (n = 61) described the accessibility, schedules, and waiting time in their community pharmacy as “adequate or very adequate” and rated their overall level of satisfaction with received care with an average score of 7.7 out of 10. Overall, 69.3% of those surveyed stated that they would like to continue picking up their hospital medication at their community pharmacy.
Finally, the experience may have also improved the coordination between the hospital pharmacy and community pharmacies during the most delicate moments of the pandemic. An improved coordination can avoid problems related to patient delivery data, as well as discrepancies between documentation and dispensed medication. Moreover, this may have facilitated the traceability of drug distribution and dispensing; keeping drugs within the pharmaceutical channel throughout the process; and avoiding breaking cold chain maintenance.
One of the weak points of this initiative is that it can only involve medication received by stable chronic patients. Furthermore, the fact that the shipment costs are entirely borne by community pharmacies and/or by distribution warehouses may not be sustainable over time. In order to be efficient, this type of service should not imply an extra cost over existing alternatives for the healthcare system. These alternatives are based on the development of an internal support service within the hospital or hiring a distribution warehouse that could deliver the drugs with proper preservation conditions. Another possible alternative could be to channel the drugs directly from the manufacturing laboratory to community pharmacies through pharmaceutical distributors.
Our study is not without limitations. First, the available data allowed us to analyze the experience carried out in only one of the three participating hospitals, and only during the months of April and May. It would be desirable to widen the scope of the analysis to other centers and time horizons, to test the consistency and representativeness of the results. Second, we lack information on the age or age group of the patients, which would have allowed us to make more specific and reality-adjusted assumptions, especially regarding actual avoided productivity losses. Third, we have considered mean costs, but the avoided transport costs may differ in some extent from region to region. Finally, it would also have been desirable to have collected information on whether the patient was accompanied by another person in order to compute the additional time avoided by the patient’s companion.
In conclusion, this exceptional situation may be a good opportunity to enhance the coordination between hospital pharmacies and community pharmacies in Spain not only during the pandemic but also in the post-COVID-19 era. In the current environment of greater healthcare humanization, it may be desirable to incorporate a mixed model of outpatient pharmaceutical care, which combines the advantages of both hospital and community pharmacy procedures, further adapting to patients’ individual and changing needs. Looking into the future, further analyses on the efficiency of alternative non-face-to-face pharmaceutical dispensing options are encouraged in order to base future decisions regarding drug dispensing flexibility on real evidence.
Disclosures
Financial support: This research received funding from the Spanish General Council of Official Colleges of Pharmacists.
Conflict of interest: NZ and AGD work at Weber, a consultancy firm that received funding from the Spanish General Council of Official Colleges of Pharmacists to develop this project. NC, RP, AH, AB and MT work for the Spanish General Council of Official Colleges of Pharmacists or for a regional Official College of Pharmacists.
Supplementary material: estimate of trips avoided, and distribution of associated savings.
Table VI.
Estimate of trips avoided and associated time due to the pilot experience
| Total avoided trips (km)* | 93,305 |
| Avoided trips from outside of Santander (km) | 89,073 |
| Time associated with total avoided trips (hours) | 1,374 |
* Note: informed deliveries in CPh located less than 1 km from the hospital were not taken into account
Table VII.
Distribution of savings associated with trips avoided, by prescription type
| Prescription type | Savings associated with trips avoided | Avoided labor productivity losses | ||
|---|---|---|---|---|
| € | % | € | % | |
| Hospital diagnosis | 5,132 | 57.6% | 8,385 | 58.2% |
| Hospital use | 3,207 | 36.0% | 4,986 | 34.6% |
| Medication used in special situations | 568 | 6.4% | 1,031 | 7.2% |
| Total | 8,907 | 100% | 14,402 | 100% |
Table VIII.
Distribution of savings associated with trips avoided, by ATC1 code
| ATC1 Code | Savings associated with trips avoided | Avoided labor productivitylosses | ||
|---|---|---|---|---|
| € | % | € | % | |
| A - Alimentary tract and metabolism | 230 | 2.6% | 343 | 2.4% |
| B - Blood and blood-forming organs | 996 | 11.2% | 1,527 | 10.6% |
| C - Cardiovascular system | 581 | 6.5% | 1,034 | 7.2% |
| D - Dermatological | 28 | 0.3% | 47 | 0.3% |
| G - Genitourinary system and sex hormones | 23 | 0.3% | 44 | 0.3% |
| H - Systemic hormonal preparations, excluding sex hormones and insulins | 220 | 2.5% | 324 | 2.3% |
| J - Anti-infectives for systemic use | 749 | 8.4% | 1,208 | 8.4% |
| L - Antineoplastic and immunomodulating agents | 5,596 | 62.8% | 9,081 | 63.1% |
| N - Nervous system | 283 | 3.2% | 470 | 3.3% |
| R - Respiratory system | 126 | 1.4% | 197 | 1.4% |
| S - Sensory organs | 67 | 0.8% | 117 | 0.8% |
| V - Miscellaneous | 7 | 0.1% | 10 | 0.1% |
| Total | 8,907 | 100% | 14,402 | 100% |
Table IX.
Distribution of savings associated with trips avoided, by route of administration
| Route of administration | Savings associated with trips avoided | Avoided labor productivity losses | ||
|---|---|---|---|---|
| € | % | € | % | |
| Oral | 3,941 | 44% | 6,255 | 43% |
| Intravenous/subcutaneous | 1,078 | 12% | 1,670 | 12% |
| Subcutaneous | 3,378 | 38% | 5,654 | 39% |
| Other forms | 159 | 2% | 263 | 2% |
| Other combinations | 355 | 4% | 590 | 4% |
| Total | 8,907 | 100% | 14,402 | 100% |
References
- 1.Sociedad Española de Farmacia Hospitalaria (SEFH). Procedimientos de Farmacia Hospitalaria para la gestión del tratamiento con antivirales en la enfermedad por el nuevo coronavirus SARS-Cov-2 (Covid-19). Online Accessed August 25, 2020. [Google Scholar]
- 2.Colegio Oficial de Farmacéuticos de Cantabria. Farmacias en Cantabria. Online Accessed August 25, 2020. [Google Scholar]
- 3.Instituto Cántabro de Estadística – ICANE. Online Accessed August 25, 2020. [Google Scholar]
- 4.Ministerio de la Presidencia, Relaciones con las Cortes y Memoria Democrática. BOE Núm. 163. Online Real Decreto ley 21/2020, de 9 de junio, de medidas urgentes de prevención, contención y coordinación para hacer frente a la crisis sanitaria ocasionada por el COVID-19. Accessed October 22, 2020. [Google Scholar]
- 5.SEUR. Online Transporte de Paquetería y Mensajería Nacional e Internacional. Accessed August 31, 2020. [Google Scholar]
- 6.Gobierno de Cantabria. BOC Número 98. Online Orden SAN/27/2007, de 8 de mayo, por la que se establece el régimen de ayudas para pacientes de la Comunidad Autónoma de Cantabria y, en su caso, acompañantes, por gastos de desplazamiento, manutención y alojamiento con fines asistenciales. Accessed August 28, 2020. [Google Scholar]
- 7.Gobierno de Cantabria. Online BOC Número 15. Orden SAN/2/2019, de 7 de enero, por la que se modifica parcialmente la Orden SAN/27/2007, de 8 de mayo, por la que se establece el régimen de ayudas para pacientes de la Comunidad Autónoma de Cantabria y, en su caso, acompañantes, por gastos de desplazamiento, manutención y alojamiento con fines asistenciales. Accessed August 28, 2020. [Google Scholar]
- 8.Agencia Tributaria. Estadística de los declarantes del IRPF por municipios: 2017. Online Renta bruta y renta disponible, por tamaño del municipio, en Cantabria. Accessed August 27, 2020. [Google Scholar]
- 9.Servicio Cántabro de Salud. Situación epidemiológica de la Covid-19 en Cantabria. Online Accessed August 27, 2020. [Google Scholar]
- 10.Margusino-Framiñán L, Cid-Silva P, Martínez-Roca C et al. Implementation of specialized pharmaceutical care hospital outpatient clinics in a hospital pharmacy department. Farm Hosp. 2017;41(6):660–666. doi: 10.7399/fh.10771. PubMed [DOI] [PubMed] [Google Scholar]
- 11.El Global. El RD de “nueva normalidad” prolonga el envío de fármacos a domicilio desde hospitales. Online Accessed September 2, 2020. [Google Scholar]
- 12.Servei Català de la Salut. Resolució per la qual, amb motiu de la situació de la crisi sanitària ocasionada per la COVID-19, s’estableixen mesures per a la dispensació de la medicació hospitalària de dispensació ambulatòria en la modalitat no presencia. Online Accessed September 1, 2020. [Google Scholar]
- 13.DiarioFarma. El CGCOF calcula que unos 7.000 pacientes recogen DH en farmacias. Online Accessed September 25, 2020. [Google Scholar]
- 14.Ministerio de Hacienda. Indicadores sobre Gasto Farmacéutico y Sanitario. Online Accessed September 4, 2020. [Google Scholar]
- 15.Ministerio de la Presidencia, Relaciones con las Cortes y Memoria Democrática. BOE-A-2020-3692. Real Decreto 463/2020, de 14 de marzo, por el que se declara el estado de alarma para la gestión de la situación de crisis sanitaria ocasionada por el COVID-19. 2020 Online Accessed July 20, 2020. [Google Scholar]
- 16.Sociedad Española de Farmacia Hospitalaria (SEFH). Proyecto MAPEX: marco estratégico en telefarmacia. Online Accessed September 1, 2020. [Google Scholar]
- 17.Tortajada-Goitia B, Morillo-Verdugo R, Margusino-Framiñán L, Marcos JA, Fernández-Llamazares CM. Survey on the situation of telepharmacy as applied to the outpatient care in hospital pharmacy departments in Spain during the COVID-19 pandemic. Farm Hosp. 2020;44(4):135–140. doi: 10.7399/fh.11527. PubMed [DOI] [PubMed] [Google Scholar]
- 18.Margusino-Framiñán L, Illarro-Uranga A, Lorenzo-Lorenzo K et al. Pharmaceutical care to hospital outpatients during the COVID-19 pandemic. Telepharmacy. Farm Hosp. 2020;44(7):61–65. doi: 10.7399/fh.11498. PubMed [DOI] [PubMed] [Google Scholar]
- 19.Colegio Oficial de Farmacéuticos de Cantabria. Farmacias y Botiquines. Online Accessed September 2, 2020. [Google Scholar]
- 20.Hospital Universitario Marqués de Valdecilla. Memoria 2015 del Servicio de Farmacia del Hospital Universitario Marqués de Valdecilla. Online Accessed August 28, 2020. [Google Scholar]
- 21.Sociedad Española de Farmacia Familiar y Comunitaria (SEFAC). La farmacia comunitaria puede evitar desplazamientos de riesgo de infección por COVID-19. Online [Google Scholar]