

 This work is licensed under a
This work is licensed under a Abstract
Purpose
The aim of this systematic review and meta-analysis was to compare re-rupture rates, complication rates, functional outcomes, as well as return to work (RTW)/sport (RTS) among different rehabilitation protocols following operative treatment of acute Achilles tendon ruptures.
Methods
Systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Five databases were searched for randomized controlled trials (RCTs) comparing at least two rehabilitation protocols following surgical repair of acute Achilles tendon ruptures. Rehabilitation protocols were classified as a variation of either non-weightbearing (NWB) or weightbearing (WB) and immobilization (IM) or mobilization (M). The data collection consisted of re-ruptures, complications, and RTW/RTS.
Results
Out of 2760 studies screened, 20 RCTs with 1007 patients were eligible. Fourteen studies included a group consisting of WB + M (Group 1), 11 of WB + IM (Group 2), 3 of NWB + M (Group 3), and 13 of NWB + IM (Group 4). Outcome parameters available for a meta-analysis were re-ruptures, complications, RTW, and RTS. Re-ruptures overall occurred in 2.7%, with prevalences ranging between 0.04 and 0.08. Major complications occurred in 2.6%, with prevalences ranging between 0.02 and 0.03. Minor complications occurred in 11.8% with prevalances ranging between 0.04 to 0.17. Comparing the odds-ratios between the four different groups revealed no significant differences with overall favourable results for group 1 (WB+M).
Conclusion
Early functional rehabilitation protocols with early ankle M and WB following surgical repair of acute Achilles tendon ruptures are safe and they apparently allow for a quicker RTW and RTS and seem to lead to favourable results.
Keywords: Achilles tendon rupture, rehabilitation, surgical treatment
Background
Achilles tendon ruptures are common injuries (1, 2, 3, 4) and occur most frequently in young and active males around 40 years old (1, 3, 4). Over the past few decades, treatment concepts (non-surgical/surgical and rehabilitation) have evolved considerably from non-surgical treatment to open reconstruction to minimally invasive techniques. The transition to surgical treatment was predominantly driven by lower re-rupture rates and better functional results but at the cost of higher rates of wound issues and surgical site infections (4, 5, 6). The implementation of minimally invasive techniques enabled surgeons to significantly decrease the risk of surgical site infections while maintaining the many advantages of surgery (7). Still, even surgically treated patients face a prolonged recovery, and all too often fail to reach pre-injury functional levels even if they do not suffer a re-rupture or complication first (8, 9, 10).
Postoperative rehabilitation protocols have evolved substantially from restrictive to more progressive. Postoperative rehabilitation protocols generally consist of two major components that exist on a binomial axis: non-weightbearing (NWB)/weightbearing (WB) and immobilization (IM)/mobilization (M) (10). Traditionally, patients were advised to maintain NWB for 6–8 weeks with IM in equinus position (11, 12). But these restrictive rehabilitation protocols have been shown to result in calf muscle atrophy and ankle joint stiffness. More progressive postoperative rehabilitation protocols have therefore been developed. It has been shown that progressive protocols have a pronounced influence on functional outcomes, including a faster return to work (RTW) and sports (RTW) (10, 13). Despite the considerable amount of literature on this topic, most physicians still facilitate restrictive postoperative rehabilitation protocols (10, 13).
In 2014, our study group conducted a systematic review on functional rehabilitation protocols. Based on 12 randomized controlled trials (RCTs) in which only open surgical procedures were used, immediate full WB and controlled ankle M starting by week 3 seemed to be recommendable (14). However, due to the growing body of evidence (15) on the subject and the persistent hesitance of applying more progressive rehabilitation protocols, we conducted another systematic review, but this time in conjunction with a meta-analysis. The aim was to compare re-rupture rates, complication rates, functional outcomes, as well as RTW/RTS among different rehabilitation protocols following operative treatment of acute Achilles tendon ruptures.
Materials and methods
The systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (16). The protocol was registered to Prospero (CRD42019136005).
Search strategy
MEDLINE (PubMed), CINAHL, Scopus, Central, and EMBASE were utilized as search engines from inception to May 28, 2019 (date of the database search). The search strategy is composed of three main concepts: Achilles tendon, rupture, and operative treatment. The different terms of each concept were combined with the OR operator and the three concepts were combined using the AND operator. The full search strategy for each database is provided in Supplementary Appendix 1 (see section on supplementary materials given at the end of this article). A grey literature search for conference proceedings in both Scopus and EMBASE was performed, and all references of the studies included were hand-searched to identify studies that might have been missed by the systematic search.
Inclusion/exclusion criteria
The inclusion/exclusion criteria were designed according to the PICOS criteria (17) (Table 1). Studies eligible were randomized controlled studies comparing at least two different postoperative rehabilitation protocols in surgically treated, acute, isolated ruptures of the Achilles tendon which reported objective outcomes. Acute was defined as surgery within 14 days after injury (18). The type of surgical treatment (open, minimal invasive, or percutaneous) was of no matter. Studies must be published in German or English. Studies including patients with ruptures treated more than 2 weeks postinjury, re-ruptures, or with a mixed population were excluded.
Table 1.
PICOS criteria (17).
| Participants | Patients with an acute, isolated Achilles tendon rupture |
| Intervention | Any operative repair of the Achilles tendon rupture |
| Comparison | At least two different postoperative treatment protocols |
| Outcomes | Patient satisfaction, patient reported outcome measures, functional assessment, time to return to work/sports, tendon elongation, re-rupture, complications |
| Study design | Randomized controlled trial |
Study selection and data extraction
Each database was searched separately, and the resulting datasets were exported to Endnote™ (version 20.1; Fa. Clarivate). Following removal of duplicates, the final dataset was exported to Covidence™ (Melbourne, Australia). Each step of study selection and data extraction was performed by two investigators independently. Disagreements were resolved by discussion with a third investigator.
Data extracted from each study was performed on predefined data extraction sheets including the following data points: study design, sample size, operative technique of tendon repair, description of rehabilitation protocol, time of follow-up, patient satisfaction, patient-rated outcome measures (PROMS), functional assessment, time to RTW and RTS, tendon elongation, re-rupture, and complications. Data extraction was again performed by two blinded investigators independently and disagreements were again resolved by discussion with a third investigator.
Quality assessment
Quality assessment was conducted independently by two reviewers and disagreements were resolved by discussion with a third reviewer. Assessment was performed utilizing a modified version of the original Coleman Methodology Score (CMS; Table 2) (19, 20) and, for the risk of bias, the Cochrane risk-of-bias tool for randomized trials (21).
Table 4.
Demographic details and prevalence of re-rupture, major-, and minor complication rates per the different rehabilitation groups.
| Age (years) | Sex (male) | Side (right) | Prevalence (95% CI) of | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Re-ruptures | Major complications | Minor complications | |||||||
| Values | Studies, n | Values | Studies, n | Values | Studies, n | ||||
| Group 1 | Ø 39 | 86% | 42% | 0.04 (0.02–0.06) | 12 | 0.02 (0.01–0.03) | 11 | 0.04 (0.02–0.07) | 11 |
| Group 2 | Ø 38 | 89% | 53% | 0.08 (0.04–0.13) | 8 | 0.03 (0.00–0.05) | 8 | 0.10 (0.03–0.17) | 8 |
| Group 3 | Ø 39 | 78% | 48% | 0.06 (0.00–0.41) | 3 | NA | 2 | NA | 2 |
| Group 4 | Ø 38 | 81% | 47% | 0.05 (0.03–0.06) | 12 | 0.03 (0.01–0.05) | 11 | 0.17 (0.08–0.25) | 11 |
Primary and secondary outcomes
Re-rupture rate was defined as the primary outcome measure. Secondary outcome measures included major and minor complications, time to RTW, time to RTS, and any PROMS or functional outcome measures. Complications were differentiated between minor and major complications. Minor complications included superficial wound infections, delayed wound healing, muscle stiffness, and mechanical irritations due to scarring or similar. Major complications included deep vein thrombosis, deep wound infections, loss of Achilles tendon, secondary flap coverage due to wound complications, or persisting sensory deficit/nerve damage.
Categorization of the different rehabilitation protocols
The rehabilitation protocols were grouped according to the M of the ankle and the permitted WB following the surgical treatment. ‘Weightbearing’ was defined as weightbearing on the operative leg within the first 4 weeks following the surgery. ‘Non-weightbearing’ was defined as no weightbearing within the first 4 weeks. ‘Mobilization’ was defined as any active or passive ankle movement within the first 4 weeks following the surgical treatment. ‘Immobilization’ was defined as rigid fixation of the ankle (equinus or neutral position). The resulting four groups of possible rehabilitation protocols are outlined in Table 3. The different protocols of each control and intervention group of each study are summarized in the Supplementary Appendix.
Table 3.
Grouping of the different rehabilitation protocols.
| Group 1 | Weightbearing and mobilization (WB + M) |
| Group 2 | Weightbearing and immobilization (WB + IM) |
| Group 3 | Non-weightbearing and mobilization (NWB + M) |
| Group 4 | Non-weightbearing and immobilization (NWB + IM) |
Statistical analysis
Outcomes that were reported in at least three publications were analysed. The prevalence with exact 95% CI from binomial distribution for binary outcomes was estimated for each study. Pooled prevalence with 95% CI across studies was calculated using inverse-variance method with random-effects model. The prevalence was calculated using RStudio (version 1.3, Boston, MA, USA).
A meta-analysis was conducted if three or more studies revealed sufficient comparability for the outcome parameters re-rupture rate and major and minor complications. The meta-analysis was conducted using Cochrane RevMan 5.4.1 (version 5.4. The Cochrane Collaboration). The chosen statistical method was the Mantel–Haenszel method, and the analysis model was a random-effects model. Odds ratios (ORs) were calculated between the different groups. I2 statistic was used to represent between studies heterogeneity which quantified the percentage of total variation across studies in study outcomes. Chi-square test was performed to test whether the true between-study variance is equal to zero (22).
Results
Study selection and overview
The study selection flowchart is presented in Fig. 1. Out of 2760 studies screened, 20 studies were eligible per the inclusion and exclusion criteria (8, 9, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40).
Figure 1.

PRISMA flow diagram for the systematic literature review.
Table 2 summarizes the eligible 20 RCTs per the different rehabilitation groups compared. Fourteen studies (8, 23, 26, 27, 28, 29, 30, 32, 33, 36, 37, 38, 39, 40) included a Group 1 (WB + M), 11 studies (9, 24, 25, 28, 29, 30, 31, 32, 34, 37, 39) a Group 2 (WB + IM), 3 studies (8, 35, 38) a Group 3 (NWB + M), and 13 studies (8, 9, 23, 24, 25, 26, 27, 31, 33, 34, 35, 36, 40) a Group 4 (NWB + IM) rehabilitation protocol. In these 20 RCTs, a total of 1007 patients were included with a mean age of 39 years (range: 19–73 years, not stated in 2 studies (33, 36)), 85% were male patients, and in 44%, the rupture occurred in the right leg (not stated in 9 studies (9, 26, 28, 29, 32, 35, 36, 37, 40)). The mean follow-up period was 23.5 months (range: 3–132 months, not stated in 3 studies (9, 28, 30)). The demographic data per treatment group are presented in Table 3.
An open reconstruction of the Achilles tendon was performed in 16 studies (8, 23, 24, 25, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39), a percutaneous (9, 26, 40) or minimal-invasive (27) technique in the remaining 4 studies. Most studies (n = 10; 50%) used Kessler or modified Kessler sutures (8, 28, 29, 30, 32, 33, 34, 35, 37, 38). In the remaining studies, other suture techniques such as Bunell (31, 38) (n = 2; 10%) or Krackow (36) (n = 1; 5%) were used or it was not stated (n = 7; 35%).
Re-ruptures, major/minor complications, RTW, and RTS were commonly assessed and therefore available for further analysis. Various outcome scores were assessed at various time points throughout the studies. The Achilles Tendon Rupture Score (ATRS) (41) was the only score assessed by three or more studies at 1 year follow-up. The ATRS contains 10 different items of patient-rated outcome with scores ranging from 0 to 10 points. These 10 items add up to a possible total score of 100 points, which represents the best functional result.
Study quality
The mean modified CMS (19, 20) was 73.3 ± 13.0 points (range: 48–87points) (Table 4). Based on the Cochrane risk-of-bias tool for randomized trials, 16 studies were overall rated as ‘some concerns’ and 4 as ‘high risk’ of bias, all due to an unclear allocation sequence during randomization of the patients (Fig. 2).
Figure 2.
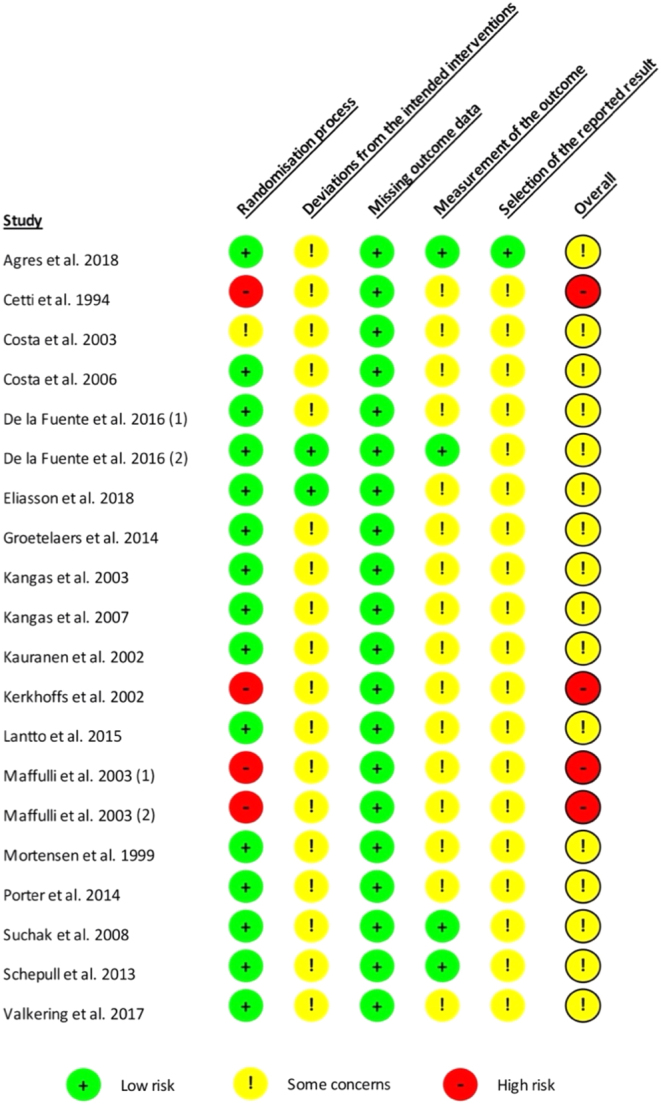
Risk of bias (based on Cochrane risk-of-bias tool for randomized trials) (40).
Primary outcome – re-ruptures
Seventeen studies (85%) reported an overall re-rupture rate of 2.7% (25 of 913). The group-specific prevalences are presented in Table 4. Overall, Group 1 had the lowest prevalence for re-rupture (0.04; 95% CI: 0.02–0.06). For all groups, a low heterogeneity (I2 = 0%; P = 0.38–0.96) was found.
Forest plots of the estimated OR for re-rupture rates (Fig. 3) were calculated for studies directly comparing similar rehabilitation groups (Table 4). Four studies compared Group 1 (WB + M) to Group 2 (WB + IM) with a non-significant OR of 0.63 (95% CI: 0.16–2.55; P = 0.520) in favour for Group 1. All studies used an open surgical repair. Seven studies compared Group 1 (WB + M) to Group 4 (NWB + IM), again, with a non-significant OR of 0.61 (95% CI: 0.15–2.47; P = 0.490) in favour of Group 1, based on 4 studies reporting events. An open repair was used in half of the studies, while the other half used a minimally invasive technique. Four studies compared Group 2 (WB + IM) to Group 4 (NWB + IM) with a non-significant OR of 2.13 (95% CI: 0.33–13.61; P = 0.420) in favour for Group 4, based on 3 studies reporting events. All studies used an open surgical repair. Again, a low heterogeneity was found for all three comparisons (I2 = 0%; P = 0.28–0.49).
Figure 3.

Forest plots of estimated odds ratio of developing a re-rupture.
Secondary outcome
Major complications
Seventeen studies (85%) reported a total of 2.6% (23 of 913) major complications. The group-specific prevalences are presented in Table 3, with Group 1 having the lowest prevalence for a major complication (0.02; 95% CI: 0.01–0.03). The overall risk of bias was low (I2 = 0%; P = 0.75–0.94).
Second, a meta-analysis on major complications was conducted for studies directly comparing similar rehabilitation groups (Fig. 4). Four studies compared Group 1 (WB + M) to Group 2 (WB + IM) with an OR of 0.97 (95% CI: 0.21–4.52; P = 0.960) based on three studies reporting events. Six studies compared Group 1 (WB + M) to Group 4 (NWB + IM), with two studies not reporting events, and a non-significant OR of 0.82 (95% CI: 0.24–2.83; P = 0.750) in favour of Group 1. Both comparisons revealed a low level of heterogeneity (I2 = 0; P = 0.620, P = 0.520). For the remaining groups, no cumulative analysis could be performed. A specific analysis in regard to open or minimally invasive surgical technique was not possible.
Figure 4.

Forest plot of estimated odds ratio of developing a major complication.
Minor complications
Seventeen studies reported minor complications in 11.8% (108 of 913) of patients. The group-specific prevalences are presented in Table 4, with Group 1 revealing the lowest prevalence for a minor complication (0.04; 95% CI: 0.02–0.07) at a moderate level of heterogeneity (I2 = 49% 84%; P = 0.0011–0.03).
A group comparing meta-analysis could only be conducted for Group 2 vs Group 4 (Fig. 5), reporting no relevant differences (OR: 0.96; 95% CI: 0.47–1.96; P = 0.910) between the 4 studies included at no heterogeneity (I2 = 0%; P = 0.750).
Figure 5.

Forest plots of estimated odds ratio of developing a minor complication.
Return to work and sports
Seven/six studies reported the time to RTW (23, 24, 26, 27, 33, 34, 35)/RTS (24, 25, 31, 33, 34, 35). The individual studies and significant differences are outlined in Table 5. Due to the varying data value presentation in the individual manuscripts, no pooled statistical analysis could be performed. Overall, Group 4 revealed the poorest results for RTW and RTS.
Table 5.
Return to work, return to sports and ATRS at 12 months per the different rehabilitation groups. Data are presented as mean ± s.d. or as median (IQR).
| Group 1 | Group 2 | Group 3 | Group 4 | P-value | |
|---|---|---|---|---|---|
| Return to work (days) | |||||
| Cetti et al. (23) | 20.2 (3–75) | 53.4 (1–182) | <0.001* | ||
| Maffulli et al. (33) | 64.4 ± 17.5 | 92.4 ± 21 | 0.05* | ||
| De la Fuente et al. (40) | 6.2 ± 3.6 | 11.1 ± 2.1 | <0.001* | ||
| Groetelaers et al. (27) | 28 (0–84) | 28 (7–280) | 0.78 | ||
| Costa et al. (24) | 56 (14–91) | 28 (7–91) | 0.59 | ||
| Maffuli et al. (34) | 14.7 ± 6.3 | 23.8 ± 9.1 | NA | ||
| Mortensen et al. (35) | 43 (1–103) | 68 (2–285) | <0.05* | ||
| Return to sports (months) | |||||
| Maffulli et al. (33) | 5.1 ± 2.8 | 6.0 ± 3.0 | 0.04* | ||
| Costa et al. (25) | 6.0 (2.0)** | 8.0 (8.0)** | NA | ||
| Costa et al. (24) | 9.0 (4.1–13.8) | 6.0 (9.2–20.7) | 0.341 | ||
| Kerkhoffs et al. (31) | 1.89 | 2.43 | NA | ||
| Maffuli et al. (34) | 5.2 ± 3.0 | 6.1 ± 2.8 | 0.05* | ||
| Mortensen et al. (35) | 4.0 (2–13) | 7.5 (3–22) | <0.001* | ||
| ATRS at 12 months (score value) | |||||
| Schepull et al. (37) | 92 (78–94) | 91 (80–92) | NA | ||
| Porter et al. (36) | 88 ± 1 | 87 ± 1 | NA | ||
| Eliasson et al. (8) | 74 ± 4 | 79 ± 4 | 77 ± 4 | 0.24 | |
*P-value significant; **value is median (SIQR).
ATRS, Achilles tendon rupture score; IQR, interquartile range; NA, not available; SIQR, semi-interquartile range.
Achilles Tendon Rupture Scores
The ATRS assessed at 12 months follow-up was reported in three studies (8, 36, 37). No study reported significant differences between the treatment groups (Table 5). Due to the limited number of studies within each group, no cumulative analysis could be conducted.
Discussion
This systematic review and meta-analysis was based on 20 RCTs; all eligible of which were grouped according to their postoperative rehabilitation protocols (WB/NWB and M/IM). Unfortunately, considerable interstudy heterogeneity was observed regarding the assessment of objective functional outcome parameters. Even if comparable scores/parameters were assessed, the time points of the assessment and/or the means of the assessment differed considerably. Therefore, a quantitative analysis did not seem appropriate for the functional outcome parameters, although it was possible for complications. The ORs for re-rupture rate and major and minor complications did not differ significantly among the different rehabilitation groups. However, early WB and M (Group 1) had the lowest prevalence and the most favourable outcomes for re-rupture rates, major complication, and minor complication.
A first meta-analysis on this topic by Suchak et al. in 2006 (42) found early functional rehabilitation protocols to improve patient satisfaction without increasing the re-rupture rate. However, the analysis was limited to six RCTs with a total of 315 patients. In 2015, McCormack and Bovard published a meta-analysis based on 10 RCTs comprising 570 patients comparing bracing to casting (43). No significant differences were found for major complications. Further outcome parameters assessed, all in favour of the bracing group, were RTW, RTS, patient satisfaction, and functional outcome. Still, the authors did not differentiate for the allowed WB and reported a high level of heterogeneity. In 2014, our study group published a systematic literature review to propose an evidence-based rehabilitation protocol for surgically treated Achilles tendon ruptures (14). Based on 12 RCTs, we found higher satisfaction, earlier return to pre-injury activities, and superior functional outcomes for full WB and early ankle M. The current systematic review 5 years later has identified 20 eligible RCTs with a total of 1007 patients. To the authors’ best knowledge, the current systematic review includes the largest number of RCTs and patients specifically investigating the effect of the rehabilitation regime in surgically treated acute Achilles tendon ruptures. Still, the applied rehabilitation protocols varied considerably from NWB and IM for a period of over 6 weeks (23) to immediate WB and early ankle M (39). In order to allow for a principal comparison, the different rehabilitation protocols were grouped into four basic rehabilitation protocols (Table 3). Despite the considerable number of RCTs included and the broad categorization, no further cumulative statistical analysis could be conducted for patient satisfaction, patient-rated outcome, or functional outcome parameters due to the considerable variation in how and when these parameters were assessed in the individual RCTs.
Table 2.
Baseline characteristics and overview of all studies included in the systematic review and meta-analysis. Data are presented as mean ± s.d. or as median (IQR).
| Reference | FU (months) | Group | n | Suture | Re-ruptures | Major complications | Minor complications | RTS (months) | RTW (days) | ATRS at 1 year | CMS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1 vs group 2 | |||||||||||
| Kangas et al. (29) | 12 | 87 | |||||||||
| 1 | 25 | Open | 1 (4%) | 1 (4%) | 0 | ||||||
| 2 | 25 | Open | 2 (8%) | 0 | 0 | ||||||
| Kangas et al. (28) | NA | 59 | |||||||||
| 1 | 25 | Open | NA | NA | NA | ||||||
| 2 | 25 | Open | NA | NA | NA | ||||||
| Kauranen et al. (30) | NA | 67 | |||||||||
| 1 | 15 | Open | NA | NA | NA | ||||||
| 2 | 15 | Open | NA | NA | NA | ||||||
| Lantto et al. (32) | 132 | 69 | |||||||||
| 1 | 25 | Open | 1 (4%) | 0 | 1 (4%) | ||||||
| 2 | 25 | Open | 2 (8%) | 1 (4%) | 1 (4%) | ||||||
| Schepull et al. (37) | 12 | 86 | |||||||||
| 1 | 18 | Open | 1 (6%) | 2 (11%) | 0 | 92 (78–94) | |||||
| 2 | 17 | Open | 0 | 2 (12%) | 0 | 91 (80–92) | |||||
| Valkering et al. (39) | 12 | 49 | |||||||||
| 1 | 27 | Open | 0 | 0 | 0 | ||||||
| 2 | 29 | Open | 1 (3%) | 0 | 0 | ||||||
| Group 1 (WB + M) vs group 4 (NWB + IM) | |||||||||||
| Cetti et al. (23) | 12 | 77 | |||||||||
| 1 | 30 | Open | 1 (3%) | 0 | 6 (20%) | 20.2 (3–75) | |||||
| 4 | 30 | Open | 2 (7%) | 1 (3%) | 16 (53%) | 53.4 (1–182) | |||||
| Maffulli et al. 2003 (33) | 21 | 87 | |||||||||
| 1 | 26 | Open | 0 | 0 | 7 (27%) | 5.1 ± 2.8 | 64.4 ± 17.5 | ||||
| 4 | 27 | Open | 0 | 0 | 7 (26%) | 6.0 ± 3.0 | 92.4 ± 21 | ||||
| Porter & Shadbolt (36) | 12 | 69 | |||||||||
| 1 | 26 | Open | 0 | 0 | 0 | 88 ± 1 | |||||
| 4 | 28 | Open | 0 | 0 | 0 | 87 ± 1 | |||||
| De la Fuente et al. (40) | 3 | 72 | |||||||||
| 1 | 13 | MIS | 0 | 1 (8%) | 0 | ||||||
| 4 | 13 | MIS | 1 (8%) | 0 | 0 | ||||||
| De la Fuente et al. (40) | 3 | 77 | |||||||||
| 1 | 20 | MIS | 1 (5%) | 3 (15%) | 0 | 6.2 ± 3.6 | |||||
| 4 | 19 | MIS | 1 (5%) | 2 (11%) | 0 | 11.1 ± 2.1 | |||||
| Groetelaers et al. (27) | 12 | 84 | |||||||||
| 1 | 32 | MIS | 1 (3%) | 1 (3%) | 0 | 28 (0–84) | |||||
| 4 | 28 | MIS | 1 (4%) | 3 (11%) | 0 | 28 (7–280) | |||||
| Group 2 vs group 4 | |||||||||||
| Costa et al. (25) | 12 | 67 | |||||||||
| 2 | 14 | Open | 1 (7%) | 0 | 2 (14%) | 6.0 (2.0)* | |||||
| 4 | 14 | Open | 0 | 0 | 2 (14%) | 8.0 (8.0)* | |||||
| Costa et al. (24) | 12 | 77 | |||||||||
| 2 | 23 | Open | 2 (9%) | 1 (4%) | 6 (26%) | 9.0 (4.1–13.8) | 56 (14–91) | ||||
| 4 | 25 | Open | 0 | 2 (8%) | 5 (20%) | 6.0 (9.2–20.7) | 28 (7–91) | ||||
| Kerkhoffs et al. (31) | 80 | 52 | |||||||||
| 2 | 16 | Open | 0 | 0 | 7 (44%) | 1.89 | |||||
| 4 | 23 | Open | 1 (4%) | 0 | 9 (39%) | 2.43 | |||||
| Maffuli et al. 2003 (34) | 31 | 85 | |||||||||
| 2 | 28 | Open | 0 | 0 | 5 (18%) | 5.2 ± 3.0 | 14,7 ± 6.3 | ||||
| 4 | 28 | Open | 0 | 0 | 8 (29%) | 6.1 ± 2.8 | 23.8 ± 9.1 | ||||
| Agres et al. (9) | NA | 48 | |||||||||
| 2 | 6 | MIS | NA | NA | NA | ||||||
| 4 | 8 | MIS | NA | NA | NA | ||||||
| Group 1 vs group 3 | |||||||||||
| Suchak et al. (38) | 6 | 83 | |||||||||
| 1 | 55 | Open | 0 | 0 | 8 (15%) | ||||||
| 3 | 55 | Open | 0 | 2 (4%) | 9 (16%) | ||||||
| Group 1 vs Group 3 vs group 4 | |||||||||||
| Eliasson et al. (8) | 12 | overall 1 | overall 5 | 87 | |||||||
| 1 | 25 | Open | 0 | 74 ± 4 | |||||||
| 3 | 25 | Open | 2 (8%) | 79 ± 4 | |||||||
| 4 | 25 | Open | 0 | 77 ± 4 | |||||||
| Group 3 vs group 4 | |||||||||||
| Mortensen et al. (35) | 16 | 83 | |||||||||
| 3 | 36 | Open | 1 (3%) | 1 (3%) | 2 (6%) | 4.0 (2–13) | 43 (1–103) | ||||
| 4 | 35 | Open | 2 (6%) | 0 | 2 (6%) | 7.5 (3–22) | 68 (2–285) | ||||
*Value is presented as median (SIQR).
ATRS, Achilles tendon rupture score; CMS, Coleman methodology score; FU, follow-up; IM, immobilization; IQR, interquartile range; M, mobilization; MIS, minimal-invasive suture or percutaneous suture technique; n, number/tendons; NA, not available; NWB, non-weightbearing; Open, open suture technique; RTS, return to sports; RTW, return to work; SIQR, semi-interquartile range; WB, weightbearing.
Our meta-analysis found no significant differences in re-rupture rates, major complication, or minor complication between the four different rehabilitation protocol groups. The most progressive rehabilitation protocol (Group 1) appeared slightly superior to the other protocols with respect to the risk of complications and re-rupture. Accelerated rehabilitation protocols have now even been implemented for nonoperative management of acute Achilles tendon ruptures. Several recent meta-analyses compared accelerated rehabilitation to delayed rehabilitation protocols (44, 45, 46). Similar to our study, they found no differences between the different rehabilitation regimes for re-rupture rate or complications. Therefore, accelerated functional rehabilitation protocols following surgical treatment of Achilles tendon ruptures can be considered safe.
Whether accelerated functional rehabilitation protocols also have a functional advantage remains a matter of debate. In line with the meta-analysis by McCormack and Bovard (43), more aggressive rehabilitation appears to have a beneficial effect on RTW and RTS. The only patient-reported outcome score that allowed a limited analysis was the ATRS at 1 year follow-up, which was assessed by three studies (8, 36, 37). These could not find any significant differences between the different rehabilitation protocols.
Several limitations need to be considered. First, relevant papers might have been missed by our search strategy, exhaustive though it was. To reduce this selection bias, a clearly defined search strategy was applied to five databases, a grey literature search was included, and the abstract/paper screening was conducted by two independent reviewers. Next, the conclusions of this systematic review are limited somewhat by the heterogenous quality of the studies included. The modified CMS varied between 48 and 87 points (average 72.9 ± 12.8 points) and the Cochrane tool showed ‘some concerns’ in 16 and ‘high risk’ of bias in another 4 studies. But this was predominantly due to an unclear randomization process, which might also be a shortcoming in the composition of the papers. Furthermore, most of the meta-analysis conducted revealed a low level of heterogeneity, unlike in the two previous meta-analyses (42, 43).
This low heterogeneity reflects one of the major strengths of this paper. Due to the large number of RCTs identified, the categorizing of the rehabilitation protocols, and the rigorous methodology for the meta-analysis conducted, we were able to generate homogenous groups which could be analysed in the aggregate. The downside to this strict methodology was that only a few parameters could be analysed. It is an unfortunate limitation in orthopaedic research that there is a lack of standardization of study protocols. It would be advantageous if RCTs could be subject to clear guidelines with respect to outcome parameters, data analysis and presentation, and consistent with respect to the time points of post-operative evaluation. This standardization would significantly increase both the ability to conduct cumulative analysis and its relative utility, all with ultimate goal of increasing the level of evidence within orthopaedics.
Conclusion
This systematic review and meta-analysis proved early functional rehabilitation protocols with early ankle M and WB following surgical repair of acute Achilles tendon ruptures to be safe. It appears these protocols may allow for a quicker RTW and RTS. Whether they also result in superior functional outcomes remains a matter of debate. Consequently, the previously postulated best evidence rehabilitation protocol for surgically treated Achilles tendon ruptures (14) remains the standard at our clinic.
Supplementary Material
ICMJE Conflict of Interest Statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding Statement
This publication was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant Number UL1TR001873. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. https://www.irvinginstitute.columbia.edu/about-us/cite-grant.
Ethical approval
There is no ethical approval necessary as this study is a systematic review and meta-analysis.
Informed consent
There is no informed consent necessary as this study is a systematic review and meta-analysis.
Author contribution statement
F K Massen: Data curation, formal analysis, investigation, statiscial analyses, methodology, visualization, writing – original draft. S Shoap: Data curation, formal analysis, language editing. J T Vosseller: Supervision, writing – review and editing, language editing. W Fan: Statiscial analyses. John Usseglio: Search strategy, database search. W Boecker: Supervision, writing – review and editing. S F Baumbach: Conceptualization, methodology, statiscial analyses, project administration, supervision, validation, writing original draft. H P: Conceptualization, methodology, project administration, supervision, review and editing. S F Baumbach and H Polzer equally contributed to this work.
References
- 1.Ganestam A, Kallemose T, Troelsen A, Barfod KW. Increasing incidence of acute Achilles tendon rupture and a noticeable decline in surgical treatment from 1994 to 2013. A nationwide registry study of 33,160 patients. Knee Surgery, Sports Traumatology, Arthroscopy 2016243730–3737. ( 10.1007/s00167-015-3544-5) [DOI] [PubMed] [Google Scholar]
- 2.Huttunen TT, Kannus P, Rolf C, Fellander-Tsai L, Mattila VM. Acute Achilles tendon ruptures: incidence of injury and surgery in Sweden between 2001 and 2012. American Journal of Sports Medicine 2014422419–2423. ( 10.1177/0363546514540599) [DOI] [PubMed] [Google Scholar]
- 3.Lemme NJ, Li NY, DeFroda SF, Kleiner J, Owens BD. Epidemiology of Achilles tendon ruptures in the United States: athletic and nonathletic injuries from 2012 to 2016. Orthopaedic Journal of Sports Medicine 201862325967118808238. ( 10.1177/2325967118808238) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ochen Y, Beks RB, van Heijl M, Hietbrink F, Leenen LPH, van der Velde D, Heng M, van der Meijden O, Groenwold RHH, Houwert RM. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. BMJ 2019364 k5120. ( 10.1136/bmj.k5120) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lantto I, Heikkinen J, Flinkkila T, Ohtonen P, Siira P, Laine V, Leppilahti J. A prospective randomized trial comparing surgical and nonsurgical treatments of acute Achilles tendon ruptures. American Journal of Sports Medicine 2016442406–2414. ( 10.1177/0363546516651060) [DOI] [PubMed] [Google Scholar]
- 6.Wilkins R, Bisson LJ. Operative versus nonoperative management of acute Achilles tendon ruptures: a quantitative systematic review of randomized controlled trials. American Journal of Sports Medicine 2012402154–2160. ( 10.1177/0363546512453293) [DOI] [PubMed] [Google Scholar]
- 7.Meulenkamp B, Woolnough T, Cheng W, Shorr R, Stacey D, Richards M, Gupta A, Fergusson D, Graham ID. What is the best evidence to guide management of acute Achilles tendon ruptures? A systematic review and network meta-analysis of randomized controlled trials. Clinical Orthopaedics and Related Research 20214792119–2131. ( 10.1097/CORR.0000000000001861) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Eliasson P, Agergaard AS, Couppe C, Svensson R, Hoeffner R, Warming S, Warming N, Holm C, Jensen MH, Krogsgaard Met al. The ruptured Achilles tendon elongates for 6 months after surgical repair regardless of early or late weightbearing in combination with ankle mobilization: a randomized clinical trial. American Journal of Sports Medicine 2018462492–2502. ( 10.1177/0363546518781826) [DOI] [PubMed] [Google Scholar]
- 9.Agres AN, Gehlen TJ, Arampatzis A, Taylor WR, Duda GN, Manegold S. Short-term functional assessment of gait, plantarflexor strength, and tendon properties after Achilles tendon rupture. Gait and Posture 201862179–185. ( 10.1016/j.gaitpost.2018.03.007) [DOI] [PubMed] [Google Scholar]
- 10.Zellers JA, Christensen M, Kjaer IL, Rathleff MS, Silbernagel KG. Defining components of early functional rehabilitation for acute Achilles tendon rupture: a systematic review. Orthopaedic Journal of Sports Medicine 201972325967119884071. ( 10.1177/2325967119884071) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Inglis AE, Scott WN, Sculco TP, Patterson AH. Ruptures of the tendo achillis. An objective assessment of surgical and non-surgical treatment. Journal of Bone and Joint Surgery: American Volume 197658990–993. ( 10.2106/00004623-197658070-00015) [DOI] [PubMed] [Google Scholar]
- 12.Jacobs D, Martens M, Van Audekercke R, Mulier JC, Mulier F. Comparison of conservative and operative treatment of Achilles tendon rupture. American Journal of Sports Medicine 19786107–111. ( 10.1177/036354657800600302) [DOI] [PubMed] [Google Scholar]
- 13.Frankewycz B, Krutsch W, Weber J, Ernstberger A, Nerlich M, Pfeifer CG. Rehabilitation of Achilles tendon ruptures: is early functional rehabilitation daily routine? Archives of Orthopaedic and Trauma Surgery 2017137333–340. ( 10.1007/s00402-017-2627-9) [DOI] [PubMed] [Google Scholar]
- 14.Brumann M, Baumbach SF, Mutschler W, Polzer H. Accelerated rehabilitation following Achilles tendon repair after acute rupture – development of an evidence-based treatment protocol. Injury 2014451782–1790. ( 10.1016/j.injury.2014.06.022) [DOI] [PubMed] [Google Scholar]
- 15.Gould HP, Bano JM, Akman JL, Fillar AL. Postoperative rehabilitation following Achilles tendon repair: a systematic review. Sports Medicine and Arthroscopy Review 202129130–145. ( 10.1097/JSA.0000000000000309) [DOI] [PubMed] [Google Scholar]
- 16.Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. & PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews 20154 1. ( 10.1186/2046-4053-4-1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S. PICO, PICOS and Spider: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Services Research 201414 579. ( 10.1186/s12913-014-0579-0) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lansdaal JR, Goslings JC, Reichart M, Govaert GA, van Scherpenzeel KM, Haverlag R, Ponsen KJ. The results of 163 Achilles tendon ruptures treated by a minimally invasive surgical technique and functional aftertreatment. Injury 200738839–844. ( 10.1016/j.injury.2006.12.010) [DOI] [PubMed] [Google Scholar]
- 19.Braunstein M, Baumbach SF, Boecker W, Carmont MR, Polzer H. Development of an accelerated functional rehabilitation protocol following minimal invasive Achilles tendon repair. Knee Surgery, Sports Traumatology, Arthroscopy 201826846–853. ( 10.1007/s00167-015-3795-1) [DOI] [PubMed] [Google Scholar]
- 20.Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD. Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scandinavian Journal of Medicine and Science in Sports 2000102–11. ( 10.1034/j.1600-0838.2000.010001002.x) [DOI] [PubMed] [Google Scholar]
- 21.Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SMet al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019366 l4898. ( 10.1136/bmj.l4898) [DOI] [PubMed] [Google Scholar]
- 22.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Statistics in Medicine 2002211539–1558. ( 10.1002/sim.1186) [DOI] [PubMed] [Google Scholar]
- 23.Cetti R, Henriksen LO, Jacobsen KS. A new treatment of ruptured Achilles tendons. A prospective randomized study. Clinical Orthopaedics and Related Research 1994308155–165. [PubMed] [Google Scholar]
- 24.Costa ML, MacMillan K, Halliday D, Chester R, Shepstone L, Robinson AH, Donell ST. Randomised controlled trials of immediate weight-bearing mobilisation for rupture of the tendo achillis. Journal of Bone and Joint Surgery: British Volume 20068869–77. ( 10.1302/0301-620X.88B1.16549) [DOI] [PubMed] [Google Scholar]
- 25.Costa ML, Shepstone L, Darrah C, Marshall T, Donell ST. Immediate full-weight-bearing mobilisation for repaired Achilles tendon ruptures: a pilot study. Injury 200334874–876. ( 10.1016/s0020-1383(0200205-x) [DOI] [PubMed] [Google Scholar]
- 26.De la Fuente C, Peña y Lillo R, Carreño G, Marambio H. Prospective randomized clinical trial of aggressive rehabilitation after acute Achilles tendon ruptures repaired with Dresden technique. Foot 20162615–22. ( 10.1016/j.foot.2015.10.003) [DOI] [PubMed] [Google Scholar]
- 27.Groetelaers RP, Janssen L, van der Velden J, Wieland AW, Amendt AG, Geelen PH, Janzing HM. Functional treatment or cast immobilization after minimally invasive repair of an acute Achilles tendon rupture: prospective, randomized trial. Foot and Ankle International 201435771–778. ( 10.1177/1071100714536167) [DOI] [PubMed] [Google Scholar]
- 28.Kangas J, Pajala A, Ohtonen P, Leppilahti J. Achilles tendon elongation after rupture repair: a randomized comparison of 2 postoperative regimens. American Journal of Sports Medicine 20073559–64. ( 10.1177/0363546506293255) [DOI] [PubMed] [Google Scholar]
- 29.Kangas J, Pajala A, Siira P, Hamalainen M, Leppilahti J. Early functional treatment versus early immobilization in tension of the musculotendinous unit after Achilles rupture repair: a prospective, randomized, clinical study. Journal of Trauma 2003541171–1180; discussion 80–81. ( 10.1097/01.TA.0000047945.20863.A2) [DOI] [PubMed] [Google Scholar]
- 30.Kauranen K, Kangas J, Leppilahti J. Recovering motor performance of the foot after Achilles rupture repair: a randomized clinical study about early functional treatment vs. early immobilization of Achilles tendon in tension. Foot and Ankle International 200223600–605. ( 10.1177/107110070202300703) [DOI] [PubMed] [Google Scholar]
- 31.Kerkhoffs GM, Struijs PA, Raaymakers EL, Marti RK. Functional treatment after surgical repair of acute Achilles tendon rupture: wrap vs walking cast. Archives of Orthopaedic and Trauma Surgery 2002122102–105. ( 10.1007/s004020100312) [DOI] [PubMed] [Google Scholar]
- 32.Lantto I, Heikkinen J, Flinkkila T, Ohtonen P, Kangas J, Siira P, Leppilahti J. Early functional treatment versus cast immobilization in tension after achilles rupture repair: results of a prospective randomized trial with 10 or more years of follow-up. American Journal of Sports Medicine 2015432302–2309. ( 10.1177/0363546515591267) [DOI] [PubMed] [Google Scholar]
- 33.Maffulli N, Tallon C, Wong J, Lim KP, Bleakney R. Early weightbearing and ankle mobilization after open repair of acute midsubstance tears of the Achilles tendon. American Journal of Sports Medicine 200331692–700. ( 10.1177/03635465030310051001) [DOI] [PubMed] [Google Scholar]
- 34.Maffulli N, Tallon C, Wong J, Peng Lim K, Bleakney R. No adverse effect of early weight bearing following open repair of acute tears of the Achilles tendon. Journal of Sports Medicine and Physical Fitness 200343367–379. [PubMed] [Google Scholar]
- 35.Mortensen HM, Skov O, Jensen PE. Early motion of the ankle after operative treatment of a rupture of the Achilles tendon. A prospective, randomized clinical and radiographic study. Journal of Bone and Joint Surgery: American Volume 199981983–990. ( 10.2106/00004623-199907000-00011) [DOI] [PubMed] [Google Scholar]
- 36.Porter MD, Shadbolt B. Randomized controlled trial of accelerated rehabilitation versus standard protocol following surgical repair of ruptured Achilles tendon. ANZ Journal of Surgery 201585373–377. ( 10.1111/ans.12910) [DOI] [PubMed] [Google Scholar]
- 37.Schepull T, Aspenberg P. Early controlled tension improves the material properties of healing human achilles tendons after ruptures: a randomized trial. American Journal of Sports Medicine 2013412550–2557. ( 10.1177/0363546513501785) [DOI] [PubMed] [Google Scholar]
- 38.Suchak AA, Bostick GP, Beaupre LA, Durand DC, Jomha NM. The influence of early weight-bearing compared with non-weight-bearing after surgical repair of the Achilles tendon. Journal of Bone and Joint Surgery: American Volume 2008901876–1883. ( 10.2106/JBJS.G.01242) [DOI] [PubMed] [Google Scholar]
- 39.Valkering KP, Aufwerber S, Ranuccio F, Lunini E, Edman G, Ackermann PW. Functional weight-bearing mobilization after Achilles tendon rupture enhances early healing response: a single-blinded randomized controlled trial. Knee Surgery, Sports Traumatology, Arthroscopy 2017251807–1816. ( 10.1007/s00167-016-4270-3) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.De la Fuente CI, Lillo RP, Ramirez-Campillo R, Ortega-Auriol P, Delgado M, Alvarez-Ruf J, Carreño G. Medial gastrocnemius myotendinous junction displacement and plantar-flexion strength in patients treated with immediate rehabilitation after Achilles tendon repair. Journal of Athletic Training 2016511013–1021. ( 10.4085/1062-6050-51.12.23) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Nilsson-Helander K, Thomee R, Silbernagel KG, Thomee P, Faxen E, Eriksson BI, Karlsson J. The Achilles Tendon Total Rupture Score (ATRS): development and validation. American Journal of Sports Medicine 200735421–426. ( 10.1177/0363546506294856) [DOI] [PubMed] [Google Scholar]
- 42.Suchak AA, Spooner C, Reid DC, Jomha NM. Postoperative rehabilitation protocols for Achilles tendon ruptures: a meta-analysis. Clinical Orthopaedics and Related Research 2006445216–221. ( 10.1097/01.blo.0000203458.05135.74) [DOI] [PubMed] [Google Scholar]
- 43.McCormack R, Bovard J. Early functional rehabilitation or cast immobilisation for the postoperative management of acute Achilles tendon rupture? A systematic review and meta-analysis of randomised controlled trials. British Journal of Sports Medicine 2015491329–1335. ( 10.1136/bjsports-2015-094935) [DOI] [PubMed] [Google Scholar]
- 44.Zhang YJ, Long X, Du JY, Wang Q, Lin XJ. Is early controlled motion and weightbearing recommended for nonoperatively treated acute Achilles tendon rupture? A systematic review and meta-analysis. Orthopaedic Journal of Sports Medicine 2021923259671211024605. ( 10.1177/23259671211024605) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Coopmans L, Amaya Aliaga J, Metsemakers WJ, Sermon A, Misselyn D, Nijs Set al. Accelerated rehabilitation in nonoperative management of acute Achilles tendon ruptures – a systematic review and meta-analysis. Journal of Foot and Ankle Surgery 202261157–162. ( 10.1053/j.jfas.2021.07.007) [DOI] [PubMed] [Google Scholar]
- 46.Dai W, Leng X, Wang J, Hu X, Ao Y. Rehabilitation regimen for non-surgical treatment of Achilles tendon rupture: a systematic review and meta-analysis of randomised controlled trials. Journal of Science and Medicine in Sport 202124536–543. ( 10.1016/j.jsams.2020.12.005) [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.