

INTRODUCTION:
The 13C-methacetin breath test (13C-MBT) is a dynamic method for assessing liver function. This proof-of-concept study aimed to investigate the association between 13C-MBT values and outcomes in patients with hepatocellular carcinoma (HCC) undergoing transarterial chemoembolization (TACE).
METHODS:
A total of 30 patients with HCC were prospectively recruited. Of these, 25 were included in baseline and 20 in longitudinal analysis. 13C-MBTs were performed before the first and second TACE session. Patients were followed for at least 1 year.
RESULTS:
At baseline, the median 13C-MBT value was 261 μg/kg/hr (interquartile range 159–387). 13C-MBT, albumin-bilirubin, Child-Pugh, and Model for End-Stage Liver Disease scores were associated with overall survival in extended univariable Cox regression (13C-MBT: standardized hazard ratio [sHR] 0.297, 95% confidence interval [CI] 0.111–0.796; albumin-bilirubin score: sHR 4.051, 95% CI 1.813–9.052; Child-Pugh score: sHR 2.616, 95% CI 1.450–4.719; Model for End-Stage Liver Disease score: sHR 2.781, 95% CI 1.356–5.703). Using a cutoff of 140 μg/kg/hr at baseline, 13C-MBT was associated with prognosis (median overall survival 28.5 months [95% CI 0.0–57.1] vs 3.5 months [95% CI 0.0–8.1], log-rank P < 0.001). Regarding prediction of 90-day mortality after second 13C-MBT, the relative change in 13C-MBT values yielded an area under the receiver-operating characteristic curve of 1.000 (P = 0.007).
DISCUSSION:
Baseline and longitudinal 13C-MBT values predict survival of patients with HCC undergoing TACE. The relative change in 13C-MBT values predicts short-term mortality and may assist in identifying patients who will not benefit from further TACE treatment.
INTRODUCTION
Hepatocellular carcinoma (HCC) is the most common primary liver cancer. In 2020, primary liver cancer incidence ranked sixth and mortality third among all malignant tumors worldwide (1). In light of the global increase in patients with nonalcoholic fatty liver disease, the incidence of HCC is expected to continue to rise (2). Transarterial chemoembolization (TACE) is the standard-of-care treatment for patients with intermediate-stage HCC (3). Although the TACE technique has been optimized to minimize harm for healthy liver tissue, the TACE procedure carries the potential risk of damaging liver function in patients with liver cirrhosis, who already have an impaired functional liver reserve (4). Immunotherapy with atezolizumab and bevacizumab has led to unprecedented overall survival (OS) rates in patients with advanced-stage disease (5,6). However, only patients with preserved liver function are candidates for systemic therapy (7). Thus, it is critical to (i) assess functional liver reserve before TACE as accurately as possible and (ii) closely monitor liver function during therapy to switch to systemic therapy before residual liver function is too poor, preventing further sequential therapy. A prospective trial of 245 patients with HCC undergoing locoregional therapy (LRT) indicated that only 13.5% of patients who progressed under LRT subsequently received systemic therapy or were included in clinical trials (8). Consequently, it is questionable whether currently used blood-based liver function parameters and derived scores are sensitive enough to detect early alterations in liver function during TACE therapy (9).
The 13C-methacetin breath test (13C-MBT) is a bedside test for the dynamic measurement of liver function. Intravenously injected 13C-methacetin is selectively metabolized by the hepatic cytochrome P450 1A2. Resulting carbon dioxide (13CO2) is measured in exhaled air as 13CO2/12CO2 ratio, thereby reflecting liver function (10). In recent years, 13C-MBT has been established for various applications (11–16), particularly in the context of preoperative assessment of liver function (10). This prospective proof-of-concept study aimed to (i) evaluate the prognostic value of baseline and longitudinal 13C-MBTs and (ii) assess whether it can detect changes in liver function more sensitively than established parameters during TACE therapy.
METHODS
Study design and patient cohort
This prospective, monocentric, proof-of-concept, observational cohort study recruited patients between December 2017 and May 2021 at the University Medical Center of the Johannes Gutenberg-University Mainz, Germany. Patients aged 18 years or older with a histologically or radiologically confirmed HCC, planned TACE, and a life expectancy of ≥ 3 months were screened for eligibility. All patients were followed for at least 12 months after first 13C-MBT. The primary end point of this study was OS. Patients who received liver transplantation were censored on the day of transplantation. Because this is a noninterventional proof-of-concept study, a sample size of 25 patients was considered sufficient to investigate the clinical practicality and utility of 13C-MBT. This article was written based on the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist (17).
13C-MBT and blood sampling
13C-MBT (LiMAx [Liver Maximum Capacity] test; Humedics, Berlin, Germany) is a real-time, noninvasive, bedside test, which determines maximum liver function capacity (10,18). Intravenously injected nonradioactive 13C-methacetin is metabolized in hepatocytes by the enzyme cytochrome P450 1A2 into paracetamol and 13CO2 (10). 13CO2 is exhaled and measured as 13CO2/12CO2 ratio (10). Patients were laid flat and quiet during the test procedure and were fasting for at least 3 hours beforehand. Shortly before and during the measurement, the patients did not receive any other medications or infusions. Detailed information is described elsewhere (10). A LiMAx FLIP 2.0 detection device and test kits were provided by Humedics. Baseline (e.g., pre-TACE) 13C-MBT was performed immediately before the first TACE session. Second 13C-MBT (e.g., post-TACE 1) was performed immediately before the second TACE session or, if not indicated, around 6 weeks post-TACE 1. On the day of 13C-MBT, blood was collected to determine blood-based liver function parameters and derived scores (Model for End-Stage Liver Disease [MELD], albumin-bilirubin [ALBI], and Child-Pugh scores). In the rare case that single laboratory values were not determined on the day of 13C-MBT, values determined up to 30 days before 13C-MBT were used.
TACE and conversion to systemic therapy
A multidisciplinary tumor board made the decision to initiate TACE therapy in the enrolled patients. TACE procedures were performed according to a standardized protocol in the Department of Diagnostic and Interventional Radiology at our tertiary care center. Details of the technical procedures are described elsewhere (19, 20). In general, TACE procedures were performed in a selective or superselective manner. Only in rare cases with a very high tumor load, lobar TACE was performed. In the case of tumor progression, the patient was represented to our multidisciplinary tumor board. If tumor progression was considered TACEable in our tumor board, re-TACE was initiated. Systemic therapy was initiated in the case of a newly diagnosed portal vein thrombosis or extrahepatic spread and if intrahepatic tumor progression was considered unTACEable.
Ethics
Written informed consent was obtained from all study patients. This study was conducted according to the ethical guidelines of the 1975 Declaration of Helsinki (Sixth revision, 2008) and was approved by the responsible ethics committee of the Medical Association of Rhineland Palatinate, Mainz, Germany (permit number 837.242.17 [11076]).
Statistical analysis
Metric data are reported as median with interquartile range (IQR) and categorical data as frequencies with percentages. The Spearman rank correlation coefficient (Spearman ρ) was used to test for correlations of baseline parameters (2-tailed). OS was calculated from the time of the first TACE session to death or last follow-up and progression-free survival (PFS) from the first TACE session to tumor progression, death, or last follow-up. Tumor progression was determined radiographically. Univariable Cox proportional hazards models were applied to determine the association of the respective covariates with OS. Results are reported as hazard ratio (HR) with its 95% confidence interval (CI). Kaplan-Meier curves were used to display OS of patients and log-rank tests to determine differences between curves. Regarding baseline 13C-MBT values, patients were divided into 2 groups using a cutoff of 140 μg/kg/hr, as previously suggested (18). Differences between 13C-MBT and liver function parameters pre-TACE and post-TACE were analyzed using a paired-samples t-test, a Wilcoxon signed-rank test, or a sign test, depending on whether test assumptions were met. In the case of missing values, patients were excluded from the corresponding test. The Shapiro-Wilk test was used to determine whether a certain variable is clearly not normally distributed. Extended univariable Cox models were used to investigate the association of longitudinal 13C-MBT values and established liver function scores with OS. For this purpose, only patients with at least 2 consecutive longitudinal 13C-MBTs were included (in total n = 20; n = 18 had 2, one had 4 and another had 5 13C-MBTs available).
In addition, continuous variables (13C-MBT, ALBI, Child-Pugh, and MELD scores) were standardized to make the strengths of the associations more comparable. To assess the discriminative accuracy of baseline and percent delta values regarding the prediction of 90-day mortality from the time of the first TACE session or second 13C-MBT, respectively, receiver-operating characteristic (ROC) curve analysis including the area under the curve (area under the receiver-operating characteristic curve [AUROC]) was performed. For this purpose, percent delta values were used {([baseline value − post-TACE value]/baseline value) × 100}. P values < 0.05 were considered statistically significant. IBM SPSS Statistics (version 27.0.1.0 and version 28.0.1.0; IBM Corp, Armonk, NY), R (version 4.13; R Foundation for Statistical Computing, Vienna, Austria, https://www.R-project.org/), RStudio (version 1.2.5033; Integrated Development for R. RStudio, PBC, Boston, MA, http://www.rstudio.com/), and GraphPad Prism (version 9.3.1; GraphPad Software, San Diego, CA) were used for statistical analysis.
RESULTS
Demographics and baseline characteristics of the study cohort
In total, 30 patients met the inclusion criteria and were enrolled. Of these, 5 patients were excluded from baseline analysis; another 5 patients were excluded from longitudinal analysis. Detailed inclusion/exclusion criteria and reasons for exclusion from analysis are demonstrated in Figure 1. Baseline characteristics of the study cohort are summarized in Table 1. The median age of patients was 71 years (IQR 68–75), 21 (84.0%) were male, and most had alcohol-related liver cirrhosis (n = 15, 60%). A total of 23 patients (92.0%) had Barcelona Clinic Liver Cancer stage B; 22 (88.0%) had ≥ 3 HCC nodules. Most patients had no prior HCC treatment (n = 19, 76.0%), followed by prior partial liver resection (n = 5, 20.0%).
Figure 1.

Inclusion and exclusion criteria and reasons for dropout. 13C-MBT, 13C-methacetin breath test; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HCC, hepatocellular carcinoma; NYHA, New York Heart Association; TACE, transarterial chemoembolization; TARE, transarterial radioembolization.
Table 1.
Baseline characteristics of study participants
| Variable | Study cohort (n = 25) |
| Age, yr, median (IQR) | 71 (68–75) |
| Male sex, n (%) | 21 (84.0) |
| BMI, kg/m2, median (IQR) | 26.20 (25.50–30.53) |
| ECOG, n (%) | |
| 0 | 8 (32.0) |
| 1 | 12 (48.0) |
| 2 | 5 (20.0) |
| Underlying etiology, n (%) | |
| Harmful alcohol use | 15 (60.0) |
| NAFLD | 2 (8.0) |
| HBV | 2 (8.0) |
| HCV | 1 (4.0) |
| AIH | 1 (4.0) |
| Other | 4 (16.0) |
| BCLC stage, n (%) | |
| A | 2 (8.0) |
| B | 23 (92.0) |
| Comorbidities, n (%) | |
| Diabetes mellitus | 13 (52.0) |
| Coronary artery disease | 4 (16.0) |
| No. of HCC nodules, n (%) | |
| 2 | 3 (12.0) |
| ≥ 3 | 22 (88.0) |
| Largest nodule, cm, median (IQR)a | 4.20 (2.60–5.80) |
| HCC treatment before TACE, n (%) | |
| No prior treatment | 19 (76.0) |
| Hemihepatectomy | 1 (4.0) |
| Partial liver resection | 5 (20.0) |
| Bilirubin, mg/dL, median (IQR) | 1.20 (0.75–2.07) |
| Albumin, g/L, median (IQR) | 35.00 (30.00–38.00) |
| INR, median (IQR) | 1.20 (1.10–1.30) |
| Creatinine, mg/dL, median (IQR) | 0.94 (0.78–1.33) |
| CRP, mg/L, median (IQR) | 8.60 (2.20–17.00) |
| AFP, ng/mL, median (IQR) | 33.00 (4.35–496.50) |
AFP, alpha-fetoprotein; AIH, autoimmune hepatitis; BCLC, Barcelona Clinic Liver Cancer; BMI, body mass index; CRP, C-reactive protein; ECOG, Eastern Cooperative Oncology Group; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; INR, international normalized ratio; IQR, interquartile range; NAFLD, nonalcoholic fatty liver disease; TACE, transarterial chemoembolization.
Values of 2 patients missing.
TACE procedures, systemic therapy, and follow-up
In total, 6 patients (24.0%) received conventional TACE, 8 patients (32.0%) drug-eluting bead TACE, and 11 patients (44.0%) both conventional TACE and drug-eluting bead TACE. Of the 25 patients included in the baseline analysis, 18 (72%) received more than 1 TACE. Of these, the median time between the first and second TACE sessions was 49 days (IQR 40.25–72.25).
A total of 14 patients (56.0%) received systemic therapy after tumor progression during TACE therapy. The details of systemic therapy are given in Supplementary Table 1 (Supplementary Digital Content 1, https://links.lww.com/CTG/A875). An overview of the reasons why the other 11 patients did not receive systemic therapy after TACE is provided in Supplementary Table 2 (Supplementary Digital Content 1, https://links.lww.com/CTG/A875). The median follow-up time was 365 days (IQR 220–644). By April 2022, 14 patients (56.0%) had died. Causes of death are listed in Supplementary Table 3 (Supplementary Digital Content 1, https://links.lww.com/CTG/A875).
13C-MBT
The median time from baseline 13C-MBT to the first TACE session was 1 day (IQR 0–2). Median duration of baseline 13C-MBT was 45.0 minutes (IQR 40.25–58.75). No adverse events were observed.
13C-MBT values and established liver function parameters at baseline
At baseline, the median 13C-MBT value was 261 μg/kg/hr (IQR 159–387, Table 2 and Supplementary Figure 1, Supplementary Digital Content 1, https://links.lww.com/CTG/A875). In total, 5 (20.0%), 17 (68.0%), and 3 (12.0%) patients had ALBI grade 1, 2, or 3, respectively. The median Child-Pugh score was 6 (IQR 5–7) with 18 patients (72.0%), 6 patients (24.0%), and 1 patient (4.0%) having Child-Pugh class A, B, or C, respectively. The median MELD score was 10 (IQR 8–13). 13C-MBT values correlated negatively with ALBI and Child-Pugh scores (Spearman rank correlation coefficients [Spearman ρ] = −0.693 [P < 0.001] and −0.555 [P = 0.004]). In the case of MELD score, there was a strong trend, but significance was missed (P = 0.056, Supplementary Figure 2, Supplementary Digital Content 1, https://links.lww.com/CTG/A875).
Table 2.
13C-MBT value and established liver function scores at baseline (n = 25)
| 13C-MBT, μg/kg/hr, median (IQR) | 261 (159–387) |
| ALBI score, median (IQR) | −2.13 (−2.51 to −1.55) |
| ALBI grade, n (%) | |
| 1 | 5 (20.0) |
| 2 | 17 (68.0) |
| 3 | 3 (12.0) |
| Child-Pugh score, median (IQR) | 6 (5–7) |
| Child-Pugh class, n (%) | |
| A | 18 (72.0) |
| B | 6 (24.0) |
| C | 1 (4.0) |
| MELD score, median (IQR) | 10 (8–13) |
13C-MBT, 13C-methacetin breath test; ALBI, albumin-bilirubin; IQR, interquartile range; MELD, Model for End-Stage Liver Disease.
Prognostic value of baseline 13C-MBT values and established liver function parameters
To estimate the prognostic value of 13C-MBT readouts, several univariable Cox proportional hazards models were applied. Here, sex, 13C-MBT, ALBI, and Child-Pugh were significantly associated with OS (Table 3). Next, 13C-MBT values were divided into 3 groups as suggested in previous studies (13C-MBT value > 315 μg/kg/hr: regular liver function [grade 1]; 13C-MBT value 140–315 μg/kg/hr: moderately impaired liver function [grade 2]; 13C-MBT value < 140 μg/kg/hr: severely impaired liver function [grade 3]) (18). Patients with severely impaired liver function had on average a significantly shorter survival than patients with regular or moderately impaired liver functions, respectively (HR 13.017, 95% CI 2.385–71.041, P = 0.003; HR 5.942, 95% CI 1.283–27.521, P = 0.023). However, there was no significant difference between patients with moderately impaired vs regular liver function (HR 1.183, 95% CI 0.311–4.506, P = 0.805). Similarly, patients with ALBI grade 3 showed on average a significantly shorter OS than those with ALBI grade 1 or 2, respectively, but not patients with ALBI grade 2 vs 1 (Table 3). No significant difference was found for Child-Pugh B vs A (Table 3). Given that only 1 patient had Child-Pugh C at baseline in this study, this category was intentionally not incorporated in the analysis. MELD score was not significantly associated with OS (HR 1.073, 95% CI 0.931–1.236, P = 0.334). A multivariable Cox regression was deliberately not used because of the insufficient number of events (n = 14 at final data cutoff).
Table 3.
Univariable Cox models using baseline parameters as the covariate (n = 25)
| Covariates | Univariable | ||
| HR | 95% CI | P value | |
| Age, yr | 1.003 | 0.933–1.077 | 0.944 |
| Sex (female vs male) | 4.964 | 1.357–18.155 | 0.015 |
| BMI, kg/m2 | 1.042 | 0.908–1.197 | 0.556 |
| ECOG (1/2 vs 0) | 2.975 | 0.820–10.790 | 0.097 |
| Etiology (other vs alcohol) | 1.133 | 0.390–3.294 | 0.818 |
| Pretreatment (surgery vs none) | 1.281 | 0.394–4.168 | 0.681 |
| BCLC stage (A vs B) | 0.778 | 0.100–6.069 | 0.811 |
| Number of nodules (≥3 vs 2) | 1.203 | 0.255–5.677 | 0.815 |
| Largest nodule, cma | 1.046 | 0.822–1.332 | 0.713 |
| 13C-MBT, μg/kg/hr | 0.993 | 0.988–0.998 | 0.010 |
| 13C-MBT grade | |||
| 140–315 μg/kg/hr (2) vs > 315 μg/kg/hr (1) | 1.183 | 0.311–4.506 | 0.805 |
| < 140 μg/kg/hr (3) vs > 315 μg/kg/hr (1) | 13.017 | 2.385–71.041 | 0.003 |
| < 140 μg/kg/hr (3) vs 140–315 μg/kg/hr (2) | 5.942 | 1.283–27.521 | 0.023 |
| ALBI score | 9.059 | 2.944–27.876 | <0.001 |
| ALBI grade | |||
| 2 vs 1 | 2.025 | 0.430–9.541 | 0.372 |
| 3 vs 1 | 16.501 | 2.200–123.777 | 0.006 |
| 3 vs 2 | 6.977 | 1.535–31.722 | 0.012 |
| Child-Pugh score | 1.686 | 1.181–2.407 | 0.004 |
| Child-Pugh stage | |||
| B vs A | 3.175 | 0.913–11.043 | 0.069 |
| MELD | 1.073 | 0.931–1.236 | 0.334 |
P values < 0.05 are marked in bold.
13C-MBT, 13C-methacetin breath test; ALBI, albumin-bilirubin; BCLC, Barcelona Clinic Liver Cancer; BMI, body mass index; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; MELD, Model for End-Stage Liver Disease.
Values of 2 patients missing.
Next, patients were dichotomized in 2 groups according to baseline 13C-MBT values using a cutoff of 140 μg/kg/hr (13C-MBT grade 3 vs grade 2 plus grade 1). Kaplan-Meier analysis showed a significant difference between both groups for OS (Figure 2a, log-rank P < 0.001). Median OS was 28.5 months (95% CI 0.0–57.1) for patients with baseline 13C-MBT values ≥ 140 μg/kg/hr and 3.5 months (95% CI 0.0–8.1) for patients with values < 140 μg/kg/hr. Kaplan-Meier curves of 13C-MBT divided into 3 groups—ALBI grade, Child-Pugh stage, and MELD score (dichotomized by its median)—are displayed in Figure 2b–e.
Figure 2.

Prognostic value of baseline 13C-MBT values and established scores using Kaplan-Meier curve analysis. (a) Baseline 13C-MBT values dichotomized by 140 μg/kg/hr. (b) Baseline 13C-MBT values divided into 3 groups as previously suggested (18). (c) Baseline ALBI grades. (d) Baseline Child-Pugh stages. (e) Baseline MELD scores dichotomized by median (10). Ticks on survival curves indicate censored cases. 13C-MBT, 13C-methacetin breath test; ALBI, albumin-bilirubin; FU, follow-up; MELD, Model for End-Stage Liver Disease; TACE, transarterial chemoembolization.
By contrast, PFS did not differ between patients when stratified into 3 groups according to their baseline 13C-MBT values (log-rank P = 0.165; see Supplementary Figure 3, Supplementary Digital Content 1, https://links.lww.com/CTG/A875). In addition, no association was found for baseline 13C-MBT values (as continuous variable) and PFS in a univariable Cox model (HR 0.998, 95% CI 0.994–1.002, P = 0.277).
Longitudinal analysis of baseline and post-TACE 13C-MBT values and established liver function parameters
The median time between baseline and second (e.g., post-TACE) 13C-MBT was 39 days (IQR 33–58). As previously described, 20 patients were included in the longitudinal analysis. The median post-TACE 13C-MBT value was 253 μg/kg/hr (IQR 124–386), showing no significant change compared with its baseline values (median 13C-MBT delta −0.50 μg/kg/hr [IQR -60.00–73.25], P = 0.952, Table 4). Similarly, Child-Pugh score did not change significantly (median Child-Pugh delta 0.00 [IQR −1.00 to 0.00], P = 0.289). By contrast, both ALBI and MELD scores showed significant alterations between both tests (median ALBI delta −0.19 [IQR −0.40 to 0.12], P = 0.027; median MELD delta −1.00 [IQR −2.00 to 0.00], P = 0.024). In addition, albumin and CRP values changed significantly (median albumin delta 2.00 [IQR −1.25 to 5.00], P = 0.037; median CRP delta −7.50 [IQR −18.85 to 0.25], P = 0.012).
Table 4.
Comparison of baseline and post-TACE 1 parameters (n = 20)
| Variable, median (IQR) | Baseline, n = 20 | Post-TACE 1, n = 20 | Delta | P value |
| 13C-MBT, μg/kg/hr | 275 (163 to 371) | 253 (124 to 386) | −0.50 (−60.00 to 73.25) | 0.952 |
| ALBI score | −2.12 (−2.52 to −1.55) | −2.09 (−2.51 to −1.41)a | −0.19 (−0.40 to 0.12)a | 0.027 |
| MELD score | 11 (7 to 13) | 11 (7 to 15) | −1.00 (−2.00 to 0.00) | 0.024 |
| Child-Pugh score | 6 (5 to 7) | 6 (5 to 8)a | 0.00 (−1.00 to 0.00)a | 0.289 |
| Bilirubin, mg/dL | 1.15 (0.80 to 2.14) | 0.95 (0.70 to 2.68) | −0.09 (−0.40 to 0.38) | 0.823 |
| Albumin, g/L | 35 (30 to 38) | 33 (30 to 38)a | 2.00 (−1.25 to 5.00)a | 0.037 |
| INR | 1.10 (1.10 to 1.30) | 1.20 (1.00 to 1.38) | −0.05 (−0.10 to 0.00) | 0.181 |
| Creatinine, mg/dL | 0.90 (0.73 to 1.34) | 0.95 (0.75 to 1.19) | −0.02 (−0.14 to 0.08) | 0.908 |
| CRP, mg/L | 8.85 (2.15 to 17.00) | 14.50 (10.00 to 25.00) | −7.50 (−18.85 to 0.25) | 0.012 |
| AFP, ng/mL | 31.00 (4.28 to 570.25) | 36.00 (3.80 to 85.00)b | 0.10 (−7.70 to 123.00)b | 0.646 |
P values < 0.05 are marked in bold.
13C-MBT, 13C-methacetin breath test; AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; CRP, C-reactive protein; INR, international normalized ratio; IQR, interquartile range; MELD, Model for End-Stage Liver Disease; TACE, transarterial chemoembolization.
Values of 2 patients missing.
Values of 1 patient missing.
Association between longitudinal changes in 13C-MBT values and established parameters and OS
Next, we fitted extended univariable Cox models to evaluate the association of longitudinal changes in 13C-MBT values and established liver function parameters with OS (Table 5). 13C-MBT, ALBI, Child-Pugh, and MELD scores were standardized for better comparability. All were significantly associated with OS, with ALBI score having the highest effect size (13C-MBT standardized: HR 0.297, 95% CI 0.111–0.796, P = 0.016; ALBI score standardized: HR 4.051, 95% CI 1.813–9.052, P = 0.001; Child-Pugh score standardized: HR 2.616, 95% CI 1.450–4.719, P = 0.001; MELD standardized: HR 2.781, 95% CI 1.356–5.703, P = 0.005). Regarding the categorized versions of the scores, 13C-MBT grade 2 vs 1, ALBI grade 2 vs 1, and Child-Pugh B vs A were not significantly associated with OS, respectively. By contrast, all of them showed significant associations when comparing 13C-MBT grade 3 vs 1 or 2 and ALBI grade 3 vs 1 or 2, respectively. Child-Pugh C vs A was significant, whereas C vs B was not (Table 5).
Table 5.
Extended Cox proportional hazards models (n = 20)
| Covariates | Univariable | ||
| HR | 95% CI | P value | |
| 13C-MBT, μg/kg/hr | 0.993 | 0.987–0.999 | 0.016 |
| 13C-MBT, μg/kg/hr (standardized) | 0.297 | 0.111–0.796 | 0.016 |
| 13C-MBT grade | |||
| 140–315 μg/kg/hr (2) vs > 315 μg/kg/hr (1) | 1.105 | 0.222–5.498 | 0.903 |
| < 140 μg/kg/hr (3) vs > 315 μg/kg/hr (1) | 8.629 | 1.783–41.769 | 0.007 |
| < 140 μg/kg/hr (3) vs 140–315 μg/kg/hr (2) | 7.807 | 1.646–37.033 | 0.010 |
| ALBI scorea | 6.421 | 2.205–18.696 | 0.001 |
| ALBI score (standardized)a | 4.051 | 1.813–9.052 | 0.001 |
| ALBI gradea | |||
| 2 vs 1 | 1.100 | 0.122–9.968 | 0.932 |
| 3 vs 1 | 18.362 | 1.482–227.505 | 0.023 |
| 3 vs 2 | 16.688 | 2.859–97.428 | 0.002 |
| Child-Pugh scorea | 1.641 | 1.211–2.223 | 0.001 |
| Child-Pugh (standardized)a | 2.616 | 1.450–4.719 | 0.001 |
| Child-Pugh stagea | |||
| B vs A | 11.317 | 0.732–174.987 | 0.082 |
| C vs A | 14.444 | 2.373–87.907 | 0.004 |
| C vs B | 1.276 | 0.103–15.827 | 0.849 |
| MELD | 1.282 | 1.077–1.526 | 0.005 |
| MELD (standardized) | 2.781 | 1.356–5.703 | 0.005 |
P values < 0.05 are marked in bold.
13C-MBT, 13C-methacetin breath test; ALBI, albumin-bilirubin; CI, confidence interval; HR, hazard ratio; MELD, Model for End-Stage Liver Disease.
Values of 2 patients missing.
Predictive performance of baseline and percent delta values for short-term mortality
Next, ROC curves were used to investigate the predictive capacity of baseline and percent delta values on short-term mortality. Short-term mortality was defined as 90-day mortality from the time of the first TACE session (baseline parameter, n = 25) or second 13C-MBT (percent delta values, n = 20) until death, respectively. AUROC for baseline 13C-MBT, ALBI, Child-Pugh, and MELD was 0.804, 0.880, 0.717, and 0.587, respectively. However, none of them provided significantly more discriminatory power than a random classification (Supplementary Figure 4, Supplementary Digital Content 1, https://links.lww.com/CTG/A875). Next, percent delta values were used for ROC analysis. One patient underwent liver transplantation at 80 days after second 13C-MBT and was, therefore, excluded from this analysis. Two patients lacked ALBI and Child-Pugh scores because albumin levels were not available. Percent delta values of 13C-MBT showed an AUROC of 1.000 (95% CI 1.000–1.000, P = 0.007). AUROCs of percent delta values of ALBI, Child-Pugh, and MELD scores were 0.952 (95% CI 0.843–1.000, P = 0.017), 0.976 (95% CI 0.907–1.000, P = 0.012), and 0.938 (95% CI 0.808–1.000, P = 0.019), respectively (Figure 3).
Figure 3.
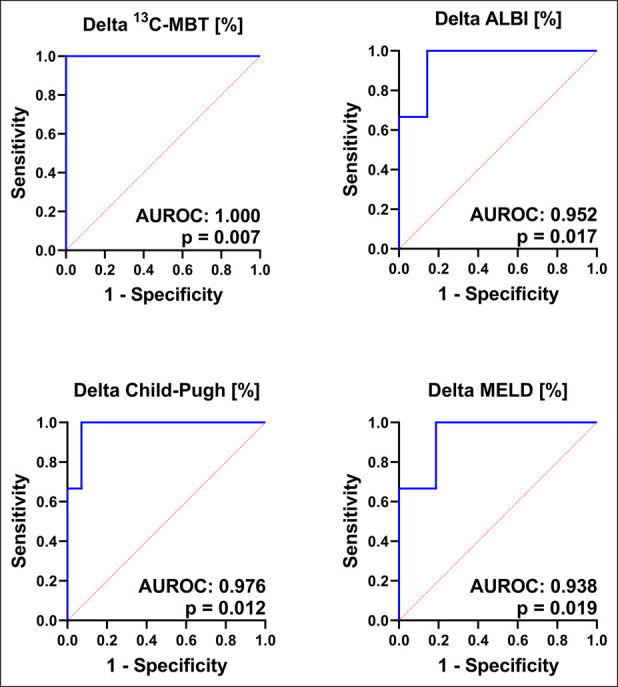
Predictive performance of percent delta values for predicting 90-day mortality after the second 13C-MBT. P values are displayed in the corresponding graph. One patient was excluded because of liver transplantation 80 days after the second 13C-MBT. n = 19 (13C-MBT and MELD), n = 17 (ALBI and Child-Pugh). 13C-MBT, 13C-methacetin breath test; ALBI, albumin-bilirubin; AUROC, area under the receiver-operating characteristic; MELD, Model of End-Stage Liver Disease.
DISCUSSION
In this prospective proof-of-concept study, we demonstrated that baseline 13C-MBT values (i) correlate with established liver function parameters and (ii) are associated with survival in TACE-treated patients with HCC. In addition, longitudinal changes in 13C-MBT values are strongly associated with OS, as shown in an extended Cox model. Importantly, the relative difference between baseline 13C-MBT values and 13C-MBT values determined after the first TACE treatment was found to predict 90-day mortality.
Three recent studies evaluated the value of 13C-MBT in TACE-treated patients with HCC (21–23). However, none of these studies investigated the association of baseline and longitudinal 13C-MBT values with prognosis and mortality prediction. Our study found that both baseline and longitudinal 13C-MBT values predict the outcome of patients with HCC undergoing TACE. We divided patients into 3 subgroups according to their 13C-MBT value as previously suggested (18). Although there was a significant difference between grade 3 vs 1 and 3 vs 2, no significant difference was found between patients with regular and moderately impaired liver function (grade 2 vs 1). The same was true for ALBI grade (no significant difference between ALBI grade 2 vs 1) and Child-Pugh stage (no significant difference between Child-Pugh B vs A). Thus, threshold values may need to be redefined in these patient cohorts to more accurately distinguish between patients with regular and moderately impaired hepatic function. Given the study design (proof-of-concept) and the small number of deaths (14 events), we intentionally did not perform multivariable analysis to directly compare 13C-MBT with ALBI, Child-Pugh, or MELD score. Given the positive results of this study, larger studies are needed to compare 13C-MBT head to head with these scores.
For hepato-oncologists, the evaluation of short-term mortality and decline in residual liver function during TACE therapy are highly relevant indicators for conversion to systemic therapy or termination of therapy. As a previous study showed, only few HCC patients with disease progression during LRT ultimately receive systemic therapy (8) and even treatment with a single TACE session can lead to a relevant decline in liver function (4). In this context, prediction of 90-day mortality by relative changes in 13C-MBT values after the first TACE session showed promising results in this study. Given the small sample size of this proof-of-concept study, no relevant differences were observed in this regard compared with Child-Pugh, ALBI, and MELD scores. However, the high dispersion range of 13C-MBT delta values may reflect sensitive detection of (altered) liver function, as reported in previous studies (21). Thus, further studies should focus on the value of longitudinal 13C-MBTs in predicting short-term mortality during TACE therapy by analyzing percent delta values. Of note, we found a higher rate of subsequent systemic therapy in our cohort (56%) compared with Memon et al. (8). The higher rate of systemic therapy in our cohort mirrors the standard of care at our center, which has evolved in the past decade because of newly available systemic treatment options. In recent years, several new therapies including lenvatinib and, in particular, immunotherapeutic agents have emerged. Therefore, changing a patient's treatment strategy from TACE to systemic therapy in the case of unTACEable progression is no longer the exception but the rule at our center.
As mentioned above, 3 recent pilot studies evaluated 13C-MBT in patients with liver cancer undergoing TACE. First, Barzakova et al. (21) included 40 patients with both primary and secondary liver cancers in a retrospective study. 13C-MBT values were determined at baseline, 1 day, and 30 days after TACE. Although mean 13C-MBT values decreased by 10% at day 1 post-TACE, no significant changes were observed after 30 days (21). Second, Reichert et al. measured 13C-MBT values at baseline and 1 day after each TACE in 11 prospectively recruited patients with HCC (22). Median baseline 13C-MBT values were 276 μg/kg/hr (±166) and, thus, comparable with our median baseline 13C-MBT values of 261 μg/kg/hr (IQR 159–387). In line with our data, baseline 13C-MBT values correlated with the baseline ALBI score. In agreement with our data, no significant alterations of sequentially determined 13C-MBT values were found in this study (22). Senk et al. performed 13C-MBT 1 day before and after TACE in 20 patients with HCC. Patients with an objective response or disease control according to modified response evaluation criteria in solid tumors (mRECIST) 6 weeks after TACE showed significantly higher baseline 13C-MBT values, respectively (23).
Our study has several limitations. First and foremost, the small sample size (n = 25) of this proof-of-concept study impairs the generalizability of our data, and all test results have to be interpreted with caution. In addition, given the low number of events (14 patients deceased at final data cutoff), a multivariable Cox model could not be applied to directly compare 13C-MBT with ALBI, Child-Pugh, and MELD scores. Because we aimed to generate new hypotheses in this proof-of-concept study, exploratory data analyses were performed, and no Bonferroni corrections for multiple comparisons were applied. Third, sequential 13C-MBTs were usually performed only after the first TACE session and not after additional sessions, a fact that may underestimate the value of 13C-MBT in the context of longitudinal liver function monitoring during TACE therapy. Importantly, the exclusion of patients from longitudinal analysis was random and not only because of missing second TACE sessions: 3 of the 5 excluded patients received ≥ 3 TACE sessions while 5 of 7 patients who received only 1 TACE underwent both 13C-MBTs and were, therefore, included in the longitudinal analysis. Thus, no selection bias must be considered in this respect. Finally, activity and/or expression of the cytochrome CYP1A2 might be increased in patients with chronic alcohol consumption (24,25). Thus, the 13C-MBT results in patients with alcohol-related liver disease might overestimate residual liver function.
In summary, both baseline and longitudinal 13C-MBT values are associated with OS in TACE-treated patients with HCC. In addition, the relative change in 13C-MBT values after the first TACE session predicts short-term mortality and may assist in identifying patients who will not benefit from further TACE treatment. Given the high clinical relevance of this parameter, larger clinical trials should focus on investigating the value of 13C-MBT in this context.
CONFLICTS OF INTEREST
Guarantor of the article: Friedrich Foerster, MD.
Specific author contributions: S.J.G., C.Z., J.U.M., J.M.S., C.L., R. Kloeckner, A.W., P.R.G., M.-A.W., and F.F: conceptualization. S.J.G., A.C., J.W., A.K., S.S., and F.F: data curation. S.J.G. and R. Kuchen: formal analysis. C.Z., J.U.M., J.M.S., A.W., P.R.G., M.-A.W., and F.F: funding acquisition. S.J.G., L.M., A.C., J.W., A.K., S.S., F.S., M.B.P., R. Kloeckner, and F.F: investigation. S.J.G., R. Kuchen, C.Z., J.U.M., J.M.S., C.L., A.W., P.R.G., M.-A.W., and F.F: methodology. S.J.G., C.Z., J.M., B.K.S., J.U.M., J.M.S., R. Kloeckner, A.W., P.R.G., M.-A.W., and F.F: project administration. J.U.M., J.M.S., R.K., A.W., P.R.G., M.-A.W., and F.F: resources. S.J.G. and R. Kuchen: software. C.Z., J.M., B.K.S., J.U.M., J.M.S., C.L., R.K., A.W., P.R.G., M.-A.W., and F.F: supervision. S.J.G., R. Kuchen, and F.F: validation. S.J.G: visualization. S.J.G., R. Kuchen, L.M., C.L., and F.F: writing—original draft. S.J.G., R. Kuchen, L.M., A.C., J.W., A.K., S.S., C.Z., F.S., M.B.P., J.M., B.K.S., J.U.M., J.M.S., C.L., R.K., A.W., P.R.G., M.-A.W., and F.F: writing—review and editing. All authors have approved the final manuscript submitted.
Financial support: This study was financially supported by Humedics (Berlin, Germany). The study was conducted independently.
Potential competing interests: S.J.G. reports receiving travel and accommodation costs from Ipsen and Gilead. R.K. has received consultancy fees from Boston Scientific, Bristol-Myers Squibb, Guerbet, Roche, and SIRTEX and lecture fees from BTG, EISAI, Guerbet, Ipsen, Roche, Siemens, SIRTEX, and MSD Sharp & Dohme, all of them unrelated to this project. P.R.G.: Medical Advisory Board Humedics. Honoraria (consulting, lectures) from Bayer, Boston Scientific, AstraZeneca, Adaptimmune, BMS, MSD, Sirtex, Lilly, Roche, Guerbet, and Ipsen. F.F. reports receiving consultancy and lecture fees from Roche and lecture fees from Lilly and Pfizer. All other authors disclose no potential financial or nonfinancial conflict of interests.
IRB approval statement: Written informed consent was obtained from all study patients. The study was conducted according to the ethical guidelines of the 1975 Declaration of Helsinki (6th revision, 2008) and was approved by the responsible ethics committee of the Medical Association of Rhineland Palatinate, Mainz, Germany (permit number 837.242.17 [11076]).
Study Highlights.
WHAT IS KNOWN
✓ Hepatocellular carcinoma (HCC) is associated with poor prognosis.
✓ Transarterial chemoembolization (TACE) is the standard therapy for patients with intermediate-stage HCC (Barcelona Clinic Liver Cancer stage B).
✓ TACE can reduce residual liver function in patients with liver cirrhosis and HCC, which may limit the number of patients eligible for subsequent systemic therapy.
✓ The 13C-methacetin breath test (13C-MBT) is an accurate method to assess hepatic function and is routinely used for assessing liver functional reserve before liver surgery.
WHAT IS NEW HERE
✓ Both baseline and longitudinal 13C-MBT values are associated with overall survival of patients with HCC undergoing TACE.
✓ The relative change in 13C-MBT values after the first TACE session predicts 90-day mortality.
✓ This may help identify patients in whom TACE should be discontinued because they will not derive clinical benefit from further TACE treatment.
Supplementary Material
ACKNOWLEDGEMENTS
This study contains parts of the medical thesis of Alper Cankaya, Jan Weerts, and Simon Sachse. S.J.G., L.M., and F.S. are supported by the Clinician Scientist Fellowship Else Kröner Research College: 2018_Kolleg.05. We thank Jasmin Mathes for her assistance with trial data management.
Footnotes
SUPPLEMENTARY MATERIAL accompanies this paper at https://links.lww.com/CTG/A875
Contributor Information
Robert Kuchen, Email: robert.kuchen@uni-mainz.de.
Lukas Müller, Email: Lukas.Mueller@unimedizin-mainz.de.
Alper Cankaya, Email: acankaya@students.uni-mainz.de.
Jan Weerts, Email: jweerts@students.uni-mainz.de.
Akin Kapucu, Email: akapucu@students.uni-mainz.de.
Simon Sachse, Email: ssachse@students.uni-mainz.de.
Carolin Zimpel, Email: carolin.zimpel@uni-luebeck.de.
Fabian Stoehr, Email: Fabian.Stoehr@unimedizin-mainz.de.
Michael B. Pitton, Email: Michael.Pitton@unimedizin-mainz.de.
Jens Mittler, Email: Jens.Mittler@unimedizin-mainz.de.
Beate Katharina Straub, Email: Beate.Straub@unimedizin-mainz.de.
Jens Uwe Marquardt, Email: Jens.Marquardt@uksh.de.
Jörn M. Schattenberg, Email: Joern.Schattenberg@unimedizin-mainz.de.
Christian Labenz, Email: Christian.labenz@unimedizin-mainz.de.
Roman Kloeckner, Email: Roman.Kloeckner@unimedizin-mainz.de.
Arndt Weinmann, Email: arndt.weinmann@unimedizin-mainz.de.
Peter Robert Galle, Email: Peter.Galle@unimedizin-mainz.de.
Marcus-Alexander Wörns, Email: Marcus-Alexander.Woerns@klinikumdo.de.
REFERENCES
- 1.Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71(3):209–49. [DOI] [PubMed] [Google Scholar]
- 2.Foerster F, Gairing SJ, Müller L, et al. NAFLD-driven HCC: Safety and efficacy of current and emerging treatment options. J Hepatol 2022;76(2):446–57. [DOI] [PubMed] [Google Scholar]
- 3.European Association for the Study of the Liver. EASL clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol 2018;69(1):182–236. [DOI] [PubMed] [Google Scholar]
- 4.Miksad RA, Ogasawara S, Xia F, et al. Liver function changes after transarterial chemoembolization in US hepatocellular carcinoma patients: The LiverT study. BMC Cancer 2019;19(1):795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Foerster F, Gairing SJ, Ilyas SI, et al. Emerging immunotherapy for hepatocellular carcinoma: A guide for hepatologists. Hepatology 2022;75(6):1604–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Finn RS, Qin S, Ikeda M, et al. IMbrave150: Updated overall survival (OS) data from a global, randomized, open-label phase III study of atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in patients (pts) with unresectable hepatocellular carcinoma (HCC). J Clin Oncol 2021;39(3 Suppl):267. [Google Scholar]
- 7.Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation Barcelona Clinic Liver Cancer (BCLC) staging system. The 2022 update. J Hepatol 2022;76(3):681–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Memon K, Kulik L, Lewandowski RJ, et al. Prospective evaluation of patients with early-/intermediate-stage hepatocellular carcinoma with disease progression following arterial locoregional therapy: Candidacy for systemic treatment or clinical trials. J Vasc Interv Radiol 2013;24(8):1189–97.e2. [DOI] [PubMed] [Google Scholar]
- 9.Müller L, Hahn F, Mähringer-Kunz A, et al. Immunonutritive scoring in patients with hepatocellular carcinoma undergoing transarterial chemoembolization: Prognostic nutritional index or controlling nutritional status score? Front Oncol 2021;11:696183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stockmann M, Lock JF, Riecke B, et al. Prediction of postoperative outcome after hepatectomy with a new bedside test for maximal liver function capacity. Ann Surg 2009;250(1):119–25. [DOI] [PubMed] [Google Scholar]
- 11.Kaffarnik M, Stoeger G, Liebich J, et al. Liver function, quantified by LiMAx test, after major abdominal surgery. Comparison between open and laparoscopic approach. World J Surg 2018;42(2):557–66. [DOI] [PubMed] [Google Scholar]
- 12.Rashidi-Alavijeh J, Kahraman A, Gerken G, et al. Enzymatic liver function measured by LiMAx is superior to current standard methods in predicting transplant-free survival after TIPS implantation. Sci Rep 2021;11(1):13834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fontana RJ, Stravitz RT, Durkalski V, et al. Prognostic value of the 13 C-methacetin breath test in adults with acute liver failure and non-acetaminophen acute liver injury. Hepatology 2021;74(2):961–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nee J, Schroeder T, Vornholt F, et al. Dynamic determination of functional liver capacity with the LiMAx test in post-cardiac arrest patients undergoing targeted temperature management—A prospective trial. Acta Anaesthesiol Scand 2020;64(4):501–7. [DOI] [PubMed] [Google Scholar]
- 15.Lock JF, Westphal T, Rubin T, et al. LiMAx test improves diagnosis of chemotherapy-associated liver injury before resection of colorectal liver metastases. Ann Surg Oncol 2017;24(9):2447–55. [DOI] [PubMed] [Google Scholar]
- 16.Kreimeyer H, Buechter M, Best J, et al. Performance of the LiMAx test, fibrinogen, and transient elastography in patients with acute liver injury. Dig Dis 2022. doi: 10.1159/000523696. [DOI] [PubMed] [Google Scholar]
- 17.von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007;370(9596):1453–7. [DOI] [PubMed] [Google Scholar]
- 18.Stockmann M, Lock JF, Malinowski M, et al. The LiMAx test: A new liver function test for predicting postoperative outcome in liver surgery. HPB (Oxford) 2010;12(2):139–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lencioni R, de Baere T, Burrel M, et al. Transcatheter treatment of hepatocellular carcinoma with doxorubicin-loaded DC Bead (DEBDOX): Technical recommendations. Cardiovasc Intervent Radiol 2012;35(5):980–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.de Baere T, Arai Y, Lencioni R, et al. Treatment of liver tumors with lipiodol TACE: Technical recommendations from experts opinion. Cardiovasc Intervent Radiol 2016;39(3):334–43. [DOI] [PubMed] [Google Scholar]
- 21.Barzakova ES, Schulze-Hagen M, Zimmermann M, et al. Monitoring liver function of patients undergoing transarterial chemoembolization (TACE) by a 13C breath test (LiMAx). Cardiovasc Intervent Radiol 2019;42(12):1702–8. [DOI] [PubMed] [Google Scholar]
- 22.Reichert MC, Massmann A, Schulz A, et al. Volume-function analysis (LiMAx test) in patients with HCC and cirrhosis undergoing TACE-A feasibility study. Dig Dis Sci 2021;66(7):2452–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Senk K, Wilcke J, Haimerl M, et al. Prediction of Transarterial Chemoembolization (TACE)—Outcome by pre- and postinterventional 13C-methacetin breath test. Clin Hemorheol Microcirc 2021;79:73–80. [DOI] [PubMed] [Google Scholar]
- 24.Le Daré B, Lagente V, Gicquel T. Ethanol and its metabolites: Update on toxicity, benefits, and focus on immunomodulatory effects. Drug Metab Rev 2019;51(4):545–61. [DOI] [PubMed] [Google Scholar]
- 25.Zhu Q, Huang C, Meng X, et al. CYP1A2 contributes to alcohol-induced abnormal lipid metabolism through the PTEN/AKT/SREBP-1c pathway. Biochem Biophys Res Commun 2019;513(2):509–14. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.