

Abstract
Objective:
Fatigue is a common, debilitating symptom experienced by individuals with chronic disease. Avoidance, or the act of evading unwanted experiences, is associated with fatigue across chronic disease samples. The current study sought to determine the strength of association between fatigue severity and avoidance in individuals with chronic disease.
Methods:
PubMed, PsycINFO, CINAHL, and ProQuest Dissertations and Theses databases were searched. Eligible studies measured fatigue and avoidance in chronic disease samples. Sixty-six studies were included. Data analyses were conducted in Rstudio. A random effects model was employed, and a weighted mean effect size was computed for fatigue severity and avoidance. Mixed-effects meta-regression analyses were conducted to examine moderating variables, including patient, clinical, and measurement characteristics. Publication bias was examined using funnel plot, trim-and-fill, and p-curve.
Results:
The meta-analysis comprised of 71 unique patient samples from 66 studies. The total number of included participants was 13,024. A small, positive association was found between fatigue severity and avoidance, r(71) = .22, p < .001, 95% CI [.18-.27], SE = .02. There was also significant heterogeneity, Q(70) = 349.96, p <.001. Moderator analyses examining age, sex, illness duration, avoidance type, and disease sample were all non-significant. Regarding publication bias, trim-and-fill resulted in a modified weighted mean effect size (r(83) = .18, p < .001) and a p-curve analysis supported the evidential value of the current analysis.
Conclusion:
Findings support that among individuals with chronic disease, fatigue severity and avoidance are positively associated, which has implications for behavioral interventions in this population.
Keywords: fatigue, avoidance, chronic disease, transdiagnostic processes, meta-analysis
Introduction
Fatigue, characterized as a feeling of exhaustion or lack of energy and reduced capacity in functioning [1–3], is a nonspecific symptom experienced by most at some point across the lifetime. Fatigue is common among healthy individuals and frequently reported by patients with chronic conditions. Fatigue is prominent in many cancers, and prevalence of fatigue has been reported in patients after stroke [4] and patients with rheumatic diseases [5, 6], inflammatory bowel disease [7], multiple sclerosis [8], and systemic lupus erythematosus [9, 10], to name a few of many. More recently, as individuals recover from COVID-19, many experience persistent fatigue post-recovery [11].
Fatigue is also associated with chronic disease treatment, including chemotherapy, radiotherapy, hemodialysis, and immunotherapy [12]. Although biological mechanisms of fatigue have been investigated [13], no confirmatory biomarker exists, which complicates diagnosis and treatment. Although fatigue among healthy individuals is relieved through rest, individuals with chronic disease experience fatigue that is severe, persistent, and debilitating.
Fatigue experienced by those with chronic disease is associated with significant impairment across life domains, including physical and mental functioning [14] and reduced quality of life in children, adolescents, and adults [15–18]. It is linked to adverse outcomes such as disability, work absenteeism, and productivity loss [15, 19–22]. Patients with chronic disease frequently identify fatigue as one of the most distressing symptoms [23], adversely affecting daily life [24, 25], and more disruptive than pain [26]. Given that fatigue management impacts patient outcomes (e.g., disability and depression), measuring and attending to fatigue may be important in promoting early intervention. `
Better understanding fatigue maintenance could provide insight into how fatigue-related disability and impairment develop and whether there is a temporal window during which intervention is most effective. Given that treatment regimens may induce fatigue, reducing the impact of existent fatigue may be more practical. Considering the prevalence across numerous chronic diseases, identifying transdiagnostic risk factors may be one way to better understand fatigue maintenance. Transdiagnostic risk factors, or risk factors that are related to various diseases, are associated with significant health problems among those with chronic diseases, including chronic pain and distress [27]. Since having a chronic disease is associated with fatigue, targeting risk or maintenance processes may be helpful at fatigue onset, especially among cases where etiology is undetermined. One such process that may be a risk or maintaining factor for fatigue in individuals with chronic disease is avoidance.
Avoidance
Avoidance is the universal tendency to evade unwanted experiences [28]. Individuals can engage in different types of avoidance, whether trying to prevent internal experiences such as thoughts or emotions [29], or reducing activity or movement [30]. Avoidance can be an adaptive response under many circumstances when applied in the short-term. For example, if an avid runner sprains an ankle, avoiding running temporarily until the injury is healed is likely recommended. Avoidance, however, can become maladaptive when rigidly applied over time. For instance, individuals who experience chronic pain that avoid physical activity for extended periods of time are at risk for increasing pain intensity, deconditioning, and depression [30].
As such, it is hypothesized that avoidance (broadly) by individuals with chronic disease experiencing fatigue can become problematic when used persistently. This is in line with previous avoidance models, which have theorized that the cost of engaging in persistent avoidance can impair one’s functioning [30]. Fatigued individuals with chronic disease in particular may be at a heightened risk of using avoidance long-term, which may be ineffective and lead to paradoxical results. As indicated earlier, the fatigue experienced by individuals with chronic disease is more severe and persistent than fatigue in healthy individuals, and it is typically not relieved by rest. In healthy individuals, choosing to avoid something (e.g., activity) in response to fatigue can be effective because once fatigue severity is reduced, engagement in daily activities can resume. Conversely, in an individual with chronic disease, the same form of avoidance (e.g., activity) will likely not lead to a reduction in fatigue severity. In fact, prolonged periods of rest may instead increase fatigue severity because fatigue is expected to be persistent in chronic disease samples. As such, persistent avoiding (e.g., experiential avoidance, avoidance of movement, avoidance of fatigue), by individuals with chronic disease may become maladaptive when strictly applied long-term.
Again, it is important to note that avoidance is a common behavior that is effective in some contexts, but pervasive, repeated avoidance is likely to interfere with pursuit of personal values. The association between fatigue and avoidance has been examined across chronic disease samples. For example, fatigue and avoidance have been significantly associated in patients with breast cancer [31], chronic fatigue syndrome, rheumatic diseases [32], and multiple sclerosis [33]. Studies examining the association between fatigue and avoidance in chronic disease samples use a range of different measures. For example, general avoidance of internal experiences (experiential avoidance) is measured with the Acceptance and Action Questionnaire-II [34] (sample item: “I worry about not being able to control my worries and feelings”). Chronic disease-specific avoidance is measured with the Brief Coping Orientation to Problems Experienced [35] questionnaire (sample item: “I’ve been giving up the attempt to cope”). Fatigue-specific avoidance is also measured, in modified scales, such as the modified Tampa Scale for Kinesiophobia [36] (sample item: “If I would try to overcome it, my fatigue would increase.”).
Objectives of the present study
Although there is ample research examining the relation between fatigue severity and avoidance, the strength of these associations across chronic disease samples has not yet been synthesized. Meta-analysis may inform interventions for individuals with chronic disease experiencing fatigue, including identification of avoidance as a key process. The current study assessed the strength of association between fatigue and avoidance in patients with chronic disease, and a small-to-moderate positive association was hypothesized. Moderating variables were examined to determine the role of patient, clinical, and measurement characteristics.
Method
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRIMSA) protocol was used [37] and is provided in supplementary material (Table S1). The study protocol was not registered.
Inclusion criteria
Studies meeting the following criteria were considered appropriate for inclusion: (1) publication in English; (2) human subjects; (3) diagnosis of a chronic physical disease (a disease that has lasted or is expected to last one-year or longer, or results in the need for continuing medical care or impairment to activities of daily living [38]); (4) studies including self-report questionnaires of fatigue severity and/or impact; (5) studies including self-report questionnaires of general, fatigue-, or disease-specific avoidance; (6) and the inclusion of Pearson correlations between fatigue severity and avoidance. Measures of fatigue severity and impact were both eligible for inclusion, as self-report questionnaires of fatigue impact are commonly used to identify greater levels of fatigue. Studies did not have to meet a clinically meaningful fatigue threshold of fatigue.
Unpublished studies, including dissertations and theses, were included to reduce publication bias [39]. Only empirical studies were examined. If an experimental, longitudinal, or intervention study met the above criteria, only baseline or pre-intervention data was utilized. If a study included appropriate fatigue and avoidance measures, but did not report Pearson correlations, the corresponding author was contacted to request data. Contacted authors were asked to provide other relevant data. Only the effect size of Pearson correlations between fatigue and avoidance were included due to recent research suggesting that prior conversions from beta-coefficient to correlations [40] can produce large biases [41].
Exclusion criteria
Studies were excluded if published in a language other than English, the sample were non-human subjects (i.e., animals), participants were nonchronically ill, or the study included experimentally-induced fatigue. Qualitative studies and case studies were excluded.
Chronic psychological conditions (e.g., depression) were excluded. Although depression and fatigue are theorized to have similar biological mechanisms [13, 42], and fatigue and loss of energy are included in the diagnostic criteria for depression [43], the onset of depression can also be in response to chronic disease. To avoid overlap in conceptualizing depression as an inciting event and as an adverse outcome, chronic psychological conditions were excluded.
Search Strategy
A Psychology and Education librarian assisted with the database search strategy. The final search was conducted on June 28, 2021, in the following databases: PubMed, PsycINFO, CINAHL (EBSCO), and ProQuest Dissertations and Theses. The PubMed search strategy, including key word searches and MeSH terms, can be found in the supplementary material (Table S2). Search strategies for other databases are available upon request. All results of the search were then uploaded to Rayyan [44], a free web-based tool for screening records for inclusion in systematic reviews. Duplicate citations were removed. Initial screening of title and abstracts was conducted by the first author (JLA). If the title and abstracts appeared to meet inclusion criteria, the full text was then examined for eligibility. See Figure 1 for the PRISMA flow diagram.
Figure 1.
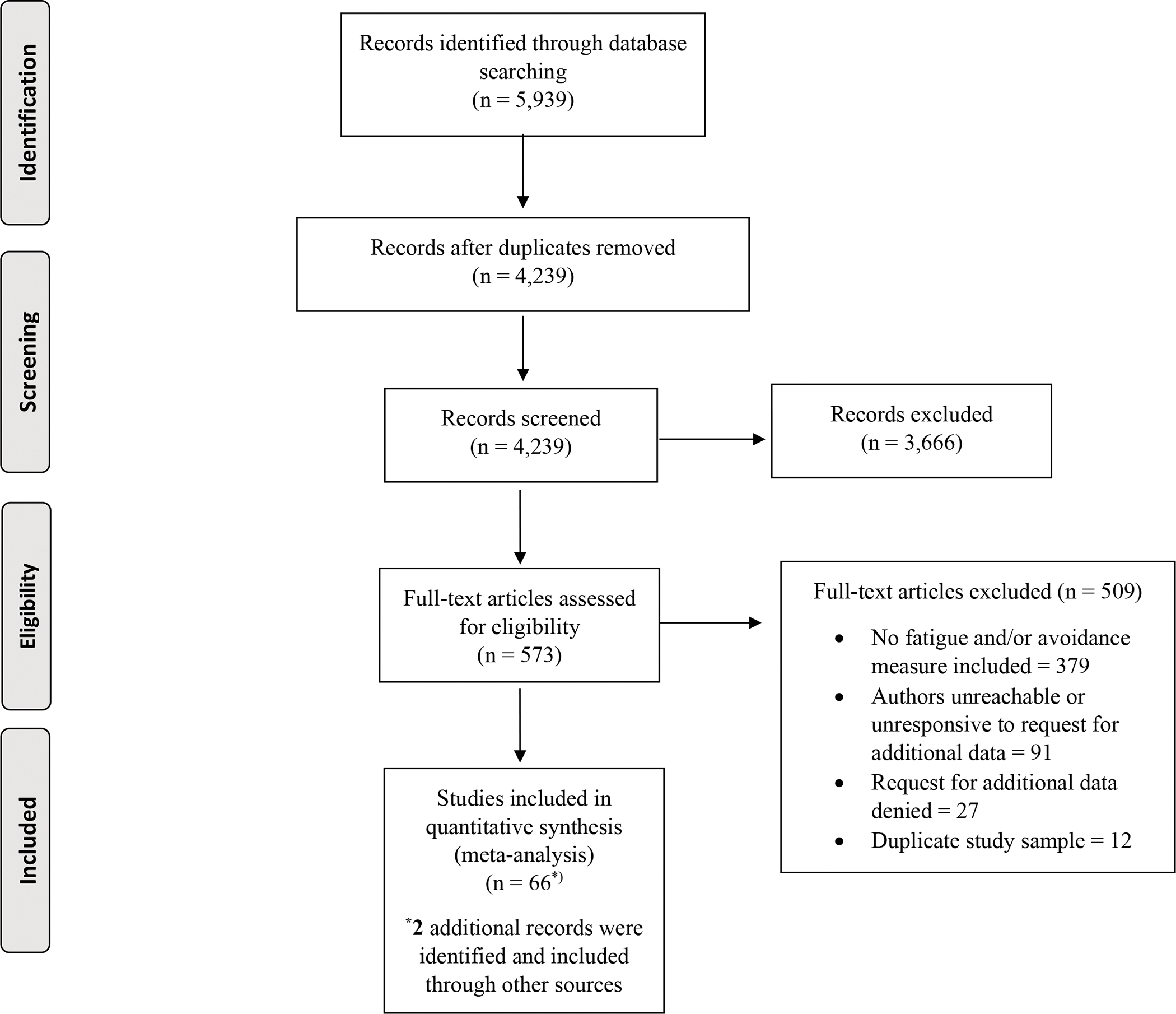
PRISMA flow diagram.
Selection of predictor variables
Measures of fatigue severity and impact were included. Most measures provided a total or global score of general fatigue. Some measures included subscales, such as physical or mental fatigue. In cases where both total and subscale scores were reported, total score was used. If multiple subscales of the same measure were reported, but not the total score, the average across subscales was computed. Studies reported visual analog scales (VAS) of fatigue, validated measures, or measures modified to be fatigue-specific. Table S3 summarizes all the fatigue scales reported in the current analysis.
General avoidance and fatigue-specific avoidance measures were included. Measures related to other specific symptom, such as pain, were excluded, whereas measures of avoidance broadly related to one’s chronic disease were included. Table S4 summarizes the avoidance scales reported in the current analysis.
Selection of moderator variables
Moderator variables for the current meta-analysis included patient, clinical, and measurement characteristics such as age, sex, illness duration, disease type, and type of avoidance measure. Data were extracted from all included studies or requested by authors if not reported. Mean age and percentage of females in the sample were examined. Both mean (preferred) or median illness duration were examined. Type of chronic disease sample was tested as a moderator; only chronic disease samples with three or more studies were examined. Finally, type of avoidance was examined (i.e., general, fatigue-, or disease-specific).
Data extraction
The first (JLA) and second authors (MVB) completed the data extraction of eligible studies. To assess for inter-rater reliability, both authors double-coded a random selection of 30% of the included studies. Inter-rater reliability fell within the strong range (K = .81) [45]. All disagreements were discussed until 100% agreement was achieved. The following variables were coded from each study if the data were available: (a) type of chronic disease sample; (b) sample size (N); (c) age of sample (mean or median); (d) sex (percent female); (e) illness duration of chronic disease in years (mean or median); (f) fatigue measure(s); (g) avoidance measure(s); and (h) Pearson correlation(s) between the fatigue severity and avoidance measure(s).
Analytic strategy
Data analysis was conducted using Rstudio software (Version 4.0.2), using the metafor package [46]. A random effects model was employed because differences in effect sizes were expected, given that studies include different patient types and different measures [47]. Evidence suggests that random effects models provide greater accuracy in measurement than fixed effects models [48]. All Pearson correlations were converted into Fisher’s z, and a single weighted mean effect size was computed for fatigue severity and avoidance. Publication bias was examined using both visual and objective measures, including a funnel plot [49, 50], Egger’s regression test [51], Begg and Mazumdar’s rank correlation test [52, 53], Duval and Tweedie’s trim-and-fill [54–56], and p-curve analysis [57]. Heterogeneity was examined with Cochrane’s Q and I2 [58]. Moderator analyses were conducted using mixed-effects meta-regression, which is appropriate for continuous and categorical outcomes [59].
Results
Study and patient characteristics
Details of the included studies can be found in Table S5. A total of 66 unique studies were included in this meta-analysis, with 64 published between 1990 and 2021. One of the included studies is currently in press [60] while another is from baseline data of an ongoing, unpublished trial [61]. Six of the included studies were doctoral dissertations/theses [62–67].
Several studies [68–73] utilized multiple fatigue severity and/or avoidance measures. Two [70, 71] included two measures of fatigue severity: a validated measure (the Checklist of Individual Strength) and a VAS; the correlation between avoidance and the validated measure was retained to be maximally conservative, as a stronger correlation was observed with the VAS. Two utilized multiple validated fatigue severity measures [69, 73] and two utilized multiple validated avoidance measures [68, 74]. Scale reliabilities were not reported and thus could not be compared, so weakest correlations were retained. More specifically, for the studies with multiple fatigue severity measures, a disease-specific fatigue measure (the Irritable Bowel Disease Fatigue Scale) was retained over the Multidimensional Fatigue Inventory [69], while the Fatigue Scale of Motor and Cognitive Functions was retained over the Chalder Fatigue Questionnaire [73]. For the studies with multiple avoidance measures, the Impact of Events Scale was retained over Cognitive and Behavioral Responses to Symptoms Questionnaire [68], while the Illness Management Questionnaire was retained over the COPE questionnaire [72]. Overall, a variety of avoidance and fatigue severity measures were reported (see Tables S3 and S4).
Several studies [65, 75–77] examined more than one chronic disease sample; when available, data for each sample were examined separately. Thus, the current meta-analysis is comprised of 71 unique patient samples from 66 studies. The total number of included participants is 13,024. Sample size ranged from 21 to 1,127 participants (M = 183.40, SD = 197.23). The average percentage of females in each sample was 72.58% (range: 0 to 100). The average age was 46.88 years old (SD = 11.93, range: 14.60 to 67.80); four studies (6.06%) did not include mean age. The average illness duration (mean and median) was 8.42 years (SD = 8.19, range: .05 to 55); 24 studies (36.36%) did not report illness duration.
Nineteen chronic disease samples were represented in the 66 studies. Most studies examined patients with cancer (n=23) [31, 62, 66, 68, 78–96], spanning breast, prostate, gynecologic, lung, gastrointestinal, colorectal, leukemia, lymphoma, and brain cancer. Fifteen studies examined individuals with multiple sclerosis [61, 65, 73, 97–108]. Fourteen studies examined individuals with chronic fatigue syndrome, myalgic encephalomyelitis and/or chronic fatigue immune dysfunction [32, 60, 63–65, 70–72, 76, 109–113], five with rheumatoid arthritis [65, 75, 114–116]; and two studies with fibromyalgia [65, 77], irritable bowel disease [69, 77], systemic lupus erythematosus [65, 67], and heart disease or heart failure [117, 118]. One study was included examining: end-stage kidney disease [119], vulvodynia [120], asthma [76], antineutrophil cytoplasmic antibody associated vasculitis [75], atrial fibrillation [121], stroke [122], non-specific chronic low back pain [123], and late-onset sequelae of poliomyelitis [124]. One study combined a group of autoimmune rheumatic diseases (e.g., connective tissue disease, spondyloarthropathy, and systemic sclerosis) [116], whereas another included two separate groups, one comprised of patients with autoimmune conditions, and the other with a functional somatic syndrome [65].
Preliminary Analyses
Preliminary analyses were conducted to investigate outliers and influential cases [125, 126]. Two studies were identified as potential outliers and influential [82, 115] and were rechecked for coding accuracy. These studies observed correlations between fatigue severity and avoidance that were moderately-sized and negative (−.30 and −.28, respectively) and authors retained both studies to avoid biasing results. It is possible that these studies were outliers because of the patient samples; one included a sample of patients with cancer who were adolescents, and the other included a sample of patients with rheumatoid arthritis in the early stages.
Effect size analyses and heterogeneity
For primary analyses, an effect size and variance for each study was computed; then, a single weighted mean effect size was calculated (Table 1). The weighted mean effect size of the association between fatigue severity and avoidance was significant, r(71) = .22, p <.001, 95% CI [.18-.27], SE = .02. This finding indicates that among individuals with chronic disease, those with greater levels of fatigue report more engagement in avoidance, and those who report more engagement in avoidance report greater fatigue severity. Figure 2 illustrates a forest plot with the computed weighted mean effect, study effect sizes, and confidence intervals. Cochran’s Q tests of heterogeneity revealed significant variation between study effects, Q(70) = 349.96, p <.001, indicating between- and within-study variability and justifying moderator analyses. Of the total heterogeneity, I2 indicated that 81.50% reflects true differences in effect size, or between-study differences. According to I2 thresholds [127], this percentage reflects high variance. These findings support the use of a random-effects model and justify moderator analyses.
Table 1.
Effect size r estimates for the association between fatigue and avoidance.
| r | 95% CI | z | k | Q | I2 | |
|---|---|---|---|---|---|---|
|
| ||||||
| Total | 0.22 | 0.18 to 0.27 | 10.12*** | 71 | 349.96*** | 81.50 |
| General avoidance | 0.19 | 0.08 to 0.31 | 3.22** | 15 | 81.79*** | 87.80 |
| Fatigue-specific avoidance | 0.28 | 0.21 to 0.35 | 7.50*** | 8 | 10.27 | 43.10 |
| Disease-specific avoidance | 0.23 | 0.18 to 0.28 | 8.77*** | 48 | 207.64*** | 79.74 |
p <.05
p < .01
p < .001
Figure 2.
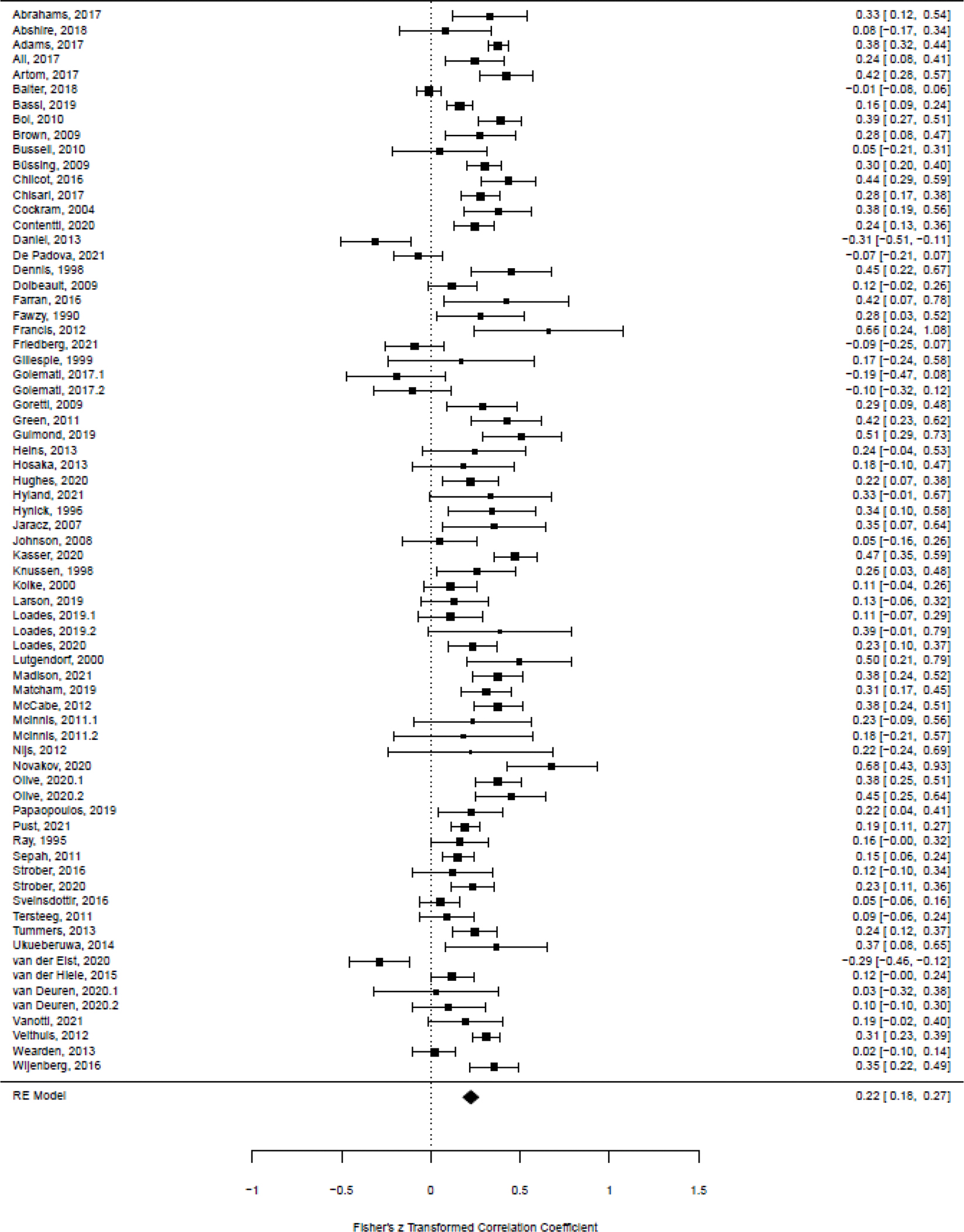
Fatigue and avoidance among individuals with chronic disease – forest plot.
Weighted mean effect sizes were computed to examine the associations between fatigue severity and general, fatigue-, and disease-specific avoidance. Regarding fatigue severity and general avoidance, the weighted mean effect size indicated a positive association (r(15) = .19, p < .01). The weighted mean effect size for fatigue severity and fatigue-specific avoidance (r(8)= .28, p < .001) and disease-specific avoidance (r(48) = .23, p <.001) demonstrated positive associations.
Moderator analyses
Moderator analyses were conducted to investigate variables that may explain between-study and within-study variance (see Table 2). Specifically, mixed-effects meta-regression was used to examine whether the association between fatigue severity and avoidance was moderated by age, sex, illness duration, disease type, and type of avoidance. Findings revealed that age, sex, and illness duration did not have a significant moderating effect. The association between fatigue severity and avoidance was not significantly affected by avoidance type. Regarding chronic disease type, samples examined included cancer, multiple sclerosis, chronic fatigue syndrome, autoimmune rheumatic diseases (i.e., rheumatoid arthritis, systematic lupus erythematosus, connective tissue disease, and spondyloarthropathy [5]) and cardiovascular diseases (i.e., heart disease, heart failure, atrial fibrillation, and stroke). The association between fatigue severity and avoidance was not significantly moderated by chronic disease type.
Table 2.
Tests of mixed-effects meta-regression for moderation of association between fatigue and avoidance.
| Moderator | Point estimate | 95% CI | z | t | k | F | df | Q |
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Age | 0.0028 | −0.0010 to 0.0066 | 1.43 | 67 | 2.03 | |||
| Percent Female | 0.0006 | −0.0014 to 0.0025 | 0.57 | 70 | 0.32 | |||
| Illness duration | −0.0032 | −0.0096 to 0.0031 | −1.00 | 47 | 0.99 | |||
| Type of avoidance measure | 71 | 0.66 | 2, 68 | |||||
| General avoidance | 0.1801 | 0.0822 to 0.2781 | 3.67*** | 14 | ||||
| Fatigue-specific avoidance | 0.0906 | −0.0748 to 0.2560 | 1.09 | 8 | ||||
| Disease-specific avoidance | 0.0487 | −0.0628 to 0.1602 | 0.87 | 48 | ||||
| Chronic disease sample | 59 | 1.68 | 4, 54 | |||||
| Cancer | 0.2278 | 0.1536 to 0.3019 | 6.16*** | 24 | ||||
| Multiple sclerosis | 0.0397 | −0.0799 to 0.1594 | 0.67 | 14 | ||||
| Chronic fatigue syndrome | −0.0798 | −0.2109 to 0.0512 | −1.22 | 12 | ||||
| Autoimmune rheumatic diseasesa | −0.1347 | −0.3111 to 0.0417 | −1.53 | 5 | ||||
| Cardiovascular diseasesb | 0.1106 | −0.1065 to 0.3277 | 1.02 | 4 | ||||
p <.05
p < .01
p < .001
Autoimmune rheumatic diseases include rheumatoid arthritis, systemic lupus erythematosus, connective tissue disease, spondyloarthropathy (seronegative spondylarthritis)
Cardiovascular diseases include heart failure, heart disease, atrial fibrillation, and stroke.
Publication bias
A funnel plot was examined visually, appearing asymmetrical. A trim-and-fill method imputed “missing” studies into the analyses to adjust for asymmetry in the funnel plot. Following the trim-and-fill, twelve studies were imputed to the left of the mean (Figure 3). Although the trim-and-fill analysis resulted in a modified weighted mean effect size, the association between fatigue severity and avoidance remained statistically significant, r(83) = .18, p <.001, 95% CI [.13-.22], SE = .02. Both Egger’s regression test (z = .82, p = .41) and rank correlation test (Kendall’s tau = .01, p = .89) were non-significant, suggesting insufficient evidence of publication bias.
Figure 3.
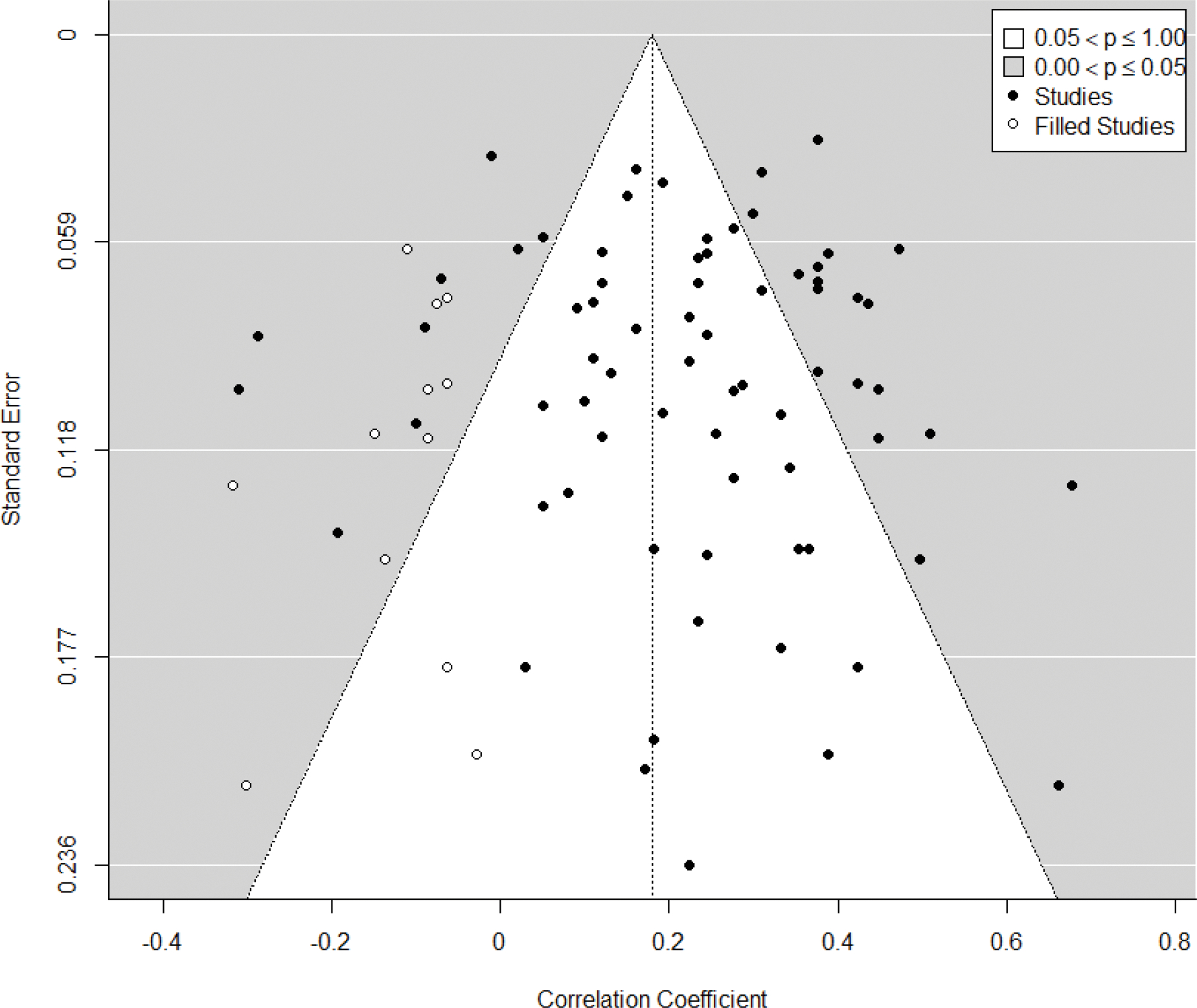
Funnel plot of standard error following trim-and-fill method.
A p-curve examined if significant studies contained evidential value. A right-skewed distribution indicates true effects with more p-values on the lower end (.01), rather than the higher end (.04 or .05), to provide an indication of the degree of p-hacking and selective reporting of significant effects [57]. Notably, the p-curve analysis only examines statistically significant findings. As shown in Figure 4, the p-curve of included statistically significant studies includes mostly (84%) those at the ≤.01 significance value suggesting evidential value, Z = −18.97, p <.001. Although some evidence of publication bias (i.e., funnel plot) was observed, several empirical tests supported the evidential value of the current analysis (i.e., regression test, rank correlation test, and p-curve). Even after adjusting for probable publication bias (i.e., trim-and-fill), the association between fatigue severity and avoidance remained significant.
Figure 4.
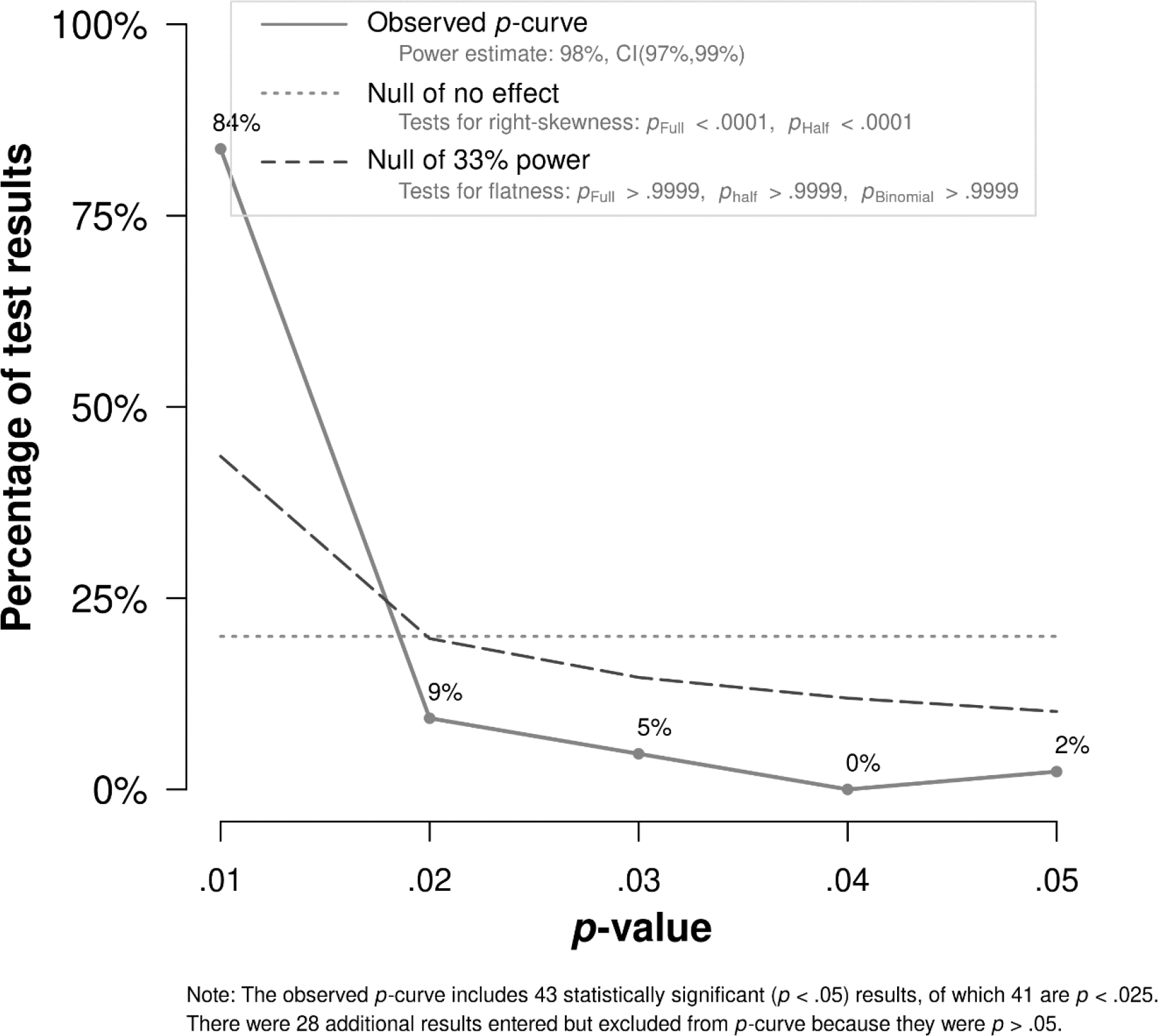
P-curve distribution for p-values of statistically significant effects, p < .05.
Discussion
The current meta-analysis examined the association between fatigue severity and avoidance among individuals with chronic disease. The findings show a modest, yet significant, positive association between fatigue severity and avoidance. Given the current meta-analysis draws from correlational data, causality and directionality of this relation cannot be inferred. Tests of heterogeneity in the current analysis indicated there was a significant amount of between-study and within-study variability; however, moderator analyses of age, sex, illness duration, and type of disease and avoidance were all non-significant.
Although the association with fatigue severity appeared strongest with fatigue-specific avoidance, type of avoidance did not moderate the association. Notably, fatigue-specific avoidance was the least commonly measured domain among the included studies. In the 8 studies that examined fatigue-specific avoidance, four total measures were used: two that were validated measures modified for fatigue severity (Coping Strategies Questionnaire [128] and Tampa Scale for Kinesiophobia [36]), and two multi-item scales created that were not tested beyond initial development (Avoidance of Activity [129] and Fatigue Coping Behavior Scale [114]). These findings suggest there may be a paucity of fatigue-specific avoidance measures. Without widely available and utilized measurement of this domain, both researchers and clinicians remain unaware of an important fatigue management strategy. Future research should examine the relation between fatigue severity and fatigue-specific avoidance, including the development and validation of fatigue-specific avoidance scales that can be used across a range of samples and include multiple domains of avoidance (i.e., physical activity or cognitive avoidance).
Relatedly, over twenty different fatigue severity and impact measures were used across studies. Moderation of the type of fatigue measure used (i.e., severity or impact) was not explored in the current study, as most measures of fatigue include items of both severity and impact. For example, the Brief Fatigue Inventory asks participants to rate the level of fatigue right now on a scale of 0 (no fatigue) to 10 (as bad as you can imagine) and to rate how much fatigue has interfered across several life domains on a scale of 0 (does not interfere) to 10 (completely interferes). It also appears that many measures of fatigue do not utilize subscale scores, but rather total global indexes. Regardless of type, the measurement of fatigue, in chronic disease is common. A future direction in fatigue measurement may be re-evaluation of the measures being used to ensure that fatigue severity and fatigue impact are not being conflated. This would allow for distinction between the experience of intense fatigue versus the impairment caused by fatigue. A critical review that examined fatigue severity measures for chronic disease [130] found six scales that demonstrated good psychometric properties; nearly all of the six were included in studies examined herein. Given the prevalence of fatigue across disease populations, future research may benefit from the development and validation of fatigue severity measures that are suitable across disease samples. One existing measure that may be most appropriate is the Patient-Reported Outcomes Measurement Information System (PROMIS) fatigue item bank [131]. The PROMIS fatigue measure has been evaluated across multiple chronic disease populations, is responsive to symptom change across conditions, and is deemed appropriate for between-group comparisons [2]. Surprisingly, none of the included studies used the PROMIS fatigue item bank for the measurement of fatigue.
Given tests of heterogeneity showed a significant amount of between-study and within-study variability, several moderator analyses tested the impact of several patient and clinical demographics on the association between fatigue severity and avoidance. All the variables examined, however, did not significantly impact the strength of association between fatigue severity and avoidance. It is possible that the inclusion criteria for the current study may have had an impact on these analyses. Per the definition of chronicity, it is possible that the length of illness was non-significant due to range restriction. The moderator analyses of age and gender were also non-significant. Though limited, these findings align with other work that examined the role of cognitive and behavioral avoidance on fatigue in patients with chronic fatigue syndrome [132]. Regarding the non-significant effect of age, range restriction among included studies may have impacted findings.
The current study also examined the impact of type of chronic disease. Moderator analyses found that the strength of the association between fatigue severity and avoidance was not impacted by chronic disease type. This finding suggests that different disease groups (cancer, multiple sclerosis, chronic fatigue syndrome, autoimmune rheumatic diseases, and cardiovascular diseases) may not differ from each other regarding the strength of the fatigue-avoidance relation. Other research has found that fatigue severity in chronic disease is largely explained by transdiagnostic factors, over and above chronic disease type [14]. As such, transdiagnostic approaches may broaden the reach of interventions that apply widely to chronic disease types. Future research should continue to examine how chronic disease type impacts the relation between fatigue severity and avoidance. The current study examined all cancers as one disease category. Future work may benefit from examining the relation between fatigue and avoidance among different categories of cancer.
Clinical Significance
Findings support a significant, albeit small, association between fatigue severity and avoidance. As both fatigue and avoidance impact multiple domains of functioning, psychological interventions targeting avoidance more broadly may improve fatigue, as well as other areas of functioning (e.g., symptoms of depression or anxiety). Some prior research has shown support for cognitive-behavioral therapy (CBT) and exercise-related interventions (e.g., graded exercise therapy) for treatment of fatigue. These interventions may be targeting avoidance. In CBT, patients often learn to identify avoidance and approach feared situations. In exercise-based interventions, patients are taught to approach, rather than avoid, physical activity. Relatedly, preliminary support exists for third-wave CBT approaches, such as acceptance and commitment therapy (ACT), for the treatment of fatigue [133–135]. ACT targets experiential avoidance, or the avoidance of private experiences (e.g., thoughts). The effectiveness of these CBT and graded exercise therapy in particular for managing fatigue severity is contentious in chronic fatigue syndrome [136]. More research on the treatment-related mechanisms of change could shed light on the effect avoidance has on fatigue outcomes, as well as other therapeutic processes. Finally, recent findings regarding the COVID-19 pandemic have found that 20% of individuals who recovered from the illness experienced elevated fatigue post-diagnosis [137]. Given the increased likelihood of individuals experiencing post-COVID-19 fatigue worldwide, identifying malleable key processes that could be targeted with early intervention is critical.
Limitations
Several limitations should be considered. The study protocol of this meta-analysis was not pre-registered. Although great attempts were made to include all possible studies meeting inclusion criteria, many articles identified for inclusion did not report the Pearson correlation between fatigue severity and avoidance directly, though data were requested. Though the search strategy for chronic disease inclusion was broad, not all categories were reflected in the included samples. Future research would benefit from the examination of fatigue severity and avoidance in more diverse chronic disease samples. Relatedly, the current study only examined chronic physical health conditions. As such, results cannot generalize to chronic psychological conditions or to non-chronically ill individuals. Future research should continue to examine the relationship between fatigue and avoidance in more populations, such as individuals with depressive disorders and healthy individuals. Inclusion criteria also included measures of both fatigue severity and impact. Measures of fatigue impact appear to use the impact on daily activities from fatigue (i.e., such as impairment in motivation and functioning) as a proxy for fatigue severity. Thus, it is possible that some of the measurements used may assess different aspects of fatigue. This limitation should be considered when interpreting the results of this meta-analysis and these measures more broadly. Relatedly, inclusion criteria did not specify a threshold for what is considered “elevated” or “clinically meaningful” to capture the full range of fatigue severity. Lastly, as the meta-analysis draws from correlational data; directionality of this relation cannot be inferred.
Conclusion
Fatigue is a common and impairing symptom experienced among individuals with chronic disease. It is related to adverse outcomes, such as reduced health-related quality of life, psychological distress, and impairment in functioning. Avoidant responses to fatigue may contribute to adverse outcomes. Avoidance is examined as a transdiagnostic process and a risk and/or maintenance factor for significant adverse physical health outcomes. The current study aimed to synthesize the strength of the association across chronic disease samples. A small positive association was found between fatigue severity and avoidance, such that those with greater fatigue severity reported more engagement in avoidance, and those with more engagement in avoidance reported greater fatigue severity. Future research should focus on the development and validation of fatigue-specific avoidance measures as well as fatigue severity measures that can be used across chronic disease samples.
Supplementary Material
Acknowledgements
Many thanks to Kelly Hangauer for help with the systematic review and to Dr. Susan Lutgendorf, Dr. Mark Vander Weg, Dr. Natalie Denburg, and Dr. Michelle Voss for the helpful feedback on this manuscript.
Funding Statement
This work was supported in part by the National Institute of Health (NIH) grants T32GM108540 (JLA & MVB) and F31DK124997 (MVB). Neither the NIH nor the University of Iowa had any role in the study design, collection, analysis, or interpretation of the data, writing of the manuscript, or the decision to submit the paper for publication.
Footnotes
Conflicts of Interest: The authors have no competing interest to report.
Research involving human participants and/or animals: For this type of study formal consent is not required. This article does not contain any studies with human participants or animals performed by any of the authors.
References
*indicates study included in the meta-analysis
- [1].Swain MG, Fatigue in chronic disease, Clin Sci. 99(1) (2000) 1–8. 10.1042/cs0990001. [DOI] [PubMed] [Google Scholar]
- [2].Cella D, Riley W, Stone A, Rothrock N, Reeve B, Yount S, Amtmann D, Bode R, Buysse D, Choi S, The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008, J Clin Epidemio. 63(11) (2010) 1179–1194. 10.1016/j.jclinepi.2010.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Herdman TH, Nursing Diagnoses 2012–14: Definitions and Classification, John Wiley & Sons, Ames, 2012. [Google Scholar]
- [4].Cumming TB, Packer M, Kramer SF, English C, The prevalence of fatigue after stroke: a systematic review and meta-analysis, Int J Stroke. 11(9) (2016) 968–977. 10.1177/1747493016669861. [DOI] [PubMed] [Google Scholar]
- [5].Seifert O, Baerwald C, Impact of fatigue on rheumatic diseases, Best Pract Res Clin Rheumatol. 33(3) (2019) 101435. 10.1016/j.berh.2019.101435. [DOI] [PubMed] [Google Scholar]
- [6].Basta F, Afeltra A, Margiotta DPE, Fatigue in systemic sclerosis: a systematic review, Clin Exp Rheumatol. 36(4) (2018) 150–160. [PubMed] [Google Scholar]
- [7].Villoria A, García V, Dosal A, Moreno L, Montserrat A, Figuerola A, Horta D, Calvet X, Ramírez-Lázaro MJ, Fatigue in out-patients with inflammatory bowel disease: prevalence and predictive factors, PLoS One. 12(7) (2017) e0181435. 10.1371/journal.pone.0181435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Weiland TJ, Jelinek GA, Marck CH, Hadgkiss EJ, van der Meer DM, Pereira NG, Taylor KL, Clinically significant fatigue: prevalence and associated factors in an international sample of adults with multiple sclerosis recruited via the internet, PLoS One. 10(2) (2015) e0115541. 10.1371/journal.pone.0115541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Tench C, McCurdie I, White P, d’Cruz D, The prevalence and associations of fatigue in systemic lupus erythematosus, Rheumatol. 39(11) (2000) 1249–1254. 10.1093/rheumatology/39.11.1249. [DOI] [PubMed] [Google Scholar]
- [10].Cleanthous S, Tyagi M, Isenberg D, Newman S, What do we know about self-reported fatigue in systemic lupus erythematosus?, Lupus. 21(5) (2012) 465–476. 10.1177/0961203312436863. [DOI] [PubMed] [Google Scholar]
- [11].Kamal M, Abo Omirah M, Hussein A, Saeed H, Assessment and characterisation of post-COVID-19 manifestations, Int J Clin Pract. 75(3) (2021) e13746. 10.1111/ijcp.13746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Tiesinga LJ, Dassen TWN, Halfens RJG, Fatigue: A Summary of the Definitions, Dimensions, and Indicators, Int J Nurs Terminol Classif. 7(2) (1996) 51–62. 10.1111/j.1744-68X.1996.tb00293.x. [DOI] [PubMed] [Google Scholar]
- [13].Matura LA, Malone S, Jaime-Lara R, Riegel B, A systematic review of biological mechanisms of fatigue in chronic illness, Biol Res Nurs. 20(4) (2018) 410–421. 10.1177/1099800418764326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Menting J, Tack CJ, Bleijenberg G, Donders R, Droogleever Fortuyn HA, Fransen J, Goedendorp MM, Kalkman JS, Strik-Albers R, van Alfen N, van der Werf SP, Voermans NC, van Engelen BG, Knoop H, Is fatigue a disease-specific or generic symptom in chronic medical conditions? Health Psychol. 37(6) (2018) 530–543. 10.1037/hea0000598. [DOI] [PubMed] [Google Scholar]
- [15].Ricci JA, Chee E, Lorandeau AL, Berger J, Fatigue in the US workforce: prevalence and implications for lost productive work time, J Occup Enviorn Med. 49(1) (2007) 1–10. 10.1097/01.jom.0000249782.60321.2a. [DOI] [PubMed] [Google Scholar]
- [16].Nunes MDR, Jacob E, Bomfim EO, Lopes-Junior LC, de Lima RAG, Floria-Santos M, Nascimento LC, Fatigue and health related quality of life in children and adolescents with cancer, Eur J Oncol Nurs. 29 (2017) 39–46. 10.1016/j.ejon.2017.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Antolín A, Martínez-Piñeiro L, Romero M, Ramos J, Bellido D, Toro J, García-Porrero A, Veiga F, Prevalence of fatigue and impact on quality of life in castration-resistant prostate cancer patients: The Vital study, BMC Urol 19 (2019). 10.1186/s12894-019-0527-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Pittion-Vouyovitch S, Debouverie M, Guillemin F, Vandenberghe N, Anxionnat R, Vespignani H, Fatigue in multiple sclerosis is related to disability, depression and quality of life, J Neurol Sci. 243(1–2) (2006) 39–45. 10.1016/j.jns.2005.11.025. [DOI] [PubMed] [Google Scholar]
- [19].Amato MP, Ponziani G, Rossi F, Liedl CL, Stefanile C, Rossi L, Quality of life in multiple sclerosis: the impact of depression, fatigue and disability, Mult Scler. 7(5) (2001) 340–4. 10.1177/135245850100700511. [DOI] [PubMed] [Google Scholar]
- [20].Varekamp I, Heutink A, Landman S, Koning CE, de Vries G, van Dijk FJ, Facilitating empowerment in employees with chronic disease: qualitative analysis of the process of change, J Occup Rehabil. 19(4) (2009) 398–408. 10.1007/s10926-009-9188-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Roelen CA, van Rhenen W, Groothoff JW, van der Klink JJ, Bültmann U, Prolonged fatigue is associated with sickness absence in men but not in women: prospective study with 1-year follow-up of white-collar employees, Int Arch Occup Enviorn Health. 87(3) (2014) 257–263. 10.1007/s00420-013-0856-y. [DOI] [PubMed] [Google Scholar]
- [22].Druce KL, Aikman L, Dilleen M, Burden A, Szczypa P, Basu N, Fatigue independently predicts different work disability dimensions in etanercept-treated rheumatoid arthritis and ankylosing spondylitis patients, Arthritis Res Ther. 20(1) (2018) 1–9. 10.1186/s13075-018-1598-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Hong F, Blonquist TM, Halpenny B, Berry DL, Patient-reported symptom distress, and most bothersome issues, before and during cancer treatment, Patient Relat Outcome Meas. 7 (2016) 127. 10.2147/PROM.S95593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Vogelzang NJ, Breitbart W, Cella D, Curt GA, Groopman JE, Horning SJ, Itri LM, Johnson DH, Scherr SL, Portenoy RK, Patient, caregiver, and oncologist perceptions of cancer-related fatigue: results of a tripart assessment survey. The Fatigue Coalition, Semin Hematol, 1997, pp. 4–12. [PubMed] [Google Scholar]
- [25].Curt GA, Breitbart W, Cella D, Groopman JE, Horning SJ, Itri LM, Johnson DH, Miaskowski C, Scherr SL, Portenoy RK, Impact of cancer-related fatigue on the lives of patients: new findings from the Fatigue Coalition, Oncologist. 5(5) (2000) 353–360. 10.1634/theoncologist.5-5-353. [DOI] [PubMed] [Google Scholar]
- [26].Ahlberg K, Ekman T, Gaston-Johansson F, Mock V, Assessment and management of cancer-related fatigue in adults, Lancet. 362(9384) (2003) 640–650. 10.1016/S0140-6736(03)14186-4. [DOI] [PubMed] [Google Scholar]
- [27].Dindo L, Brandt CP, Fiedorowicz JG, Cross-sectional relations between psychological inflexibility and symptoms of depression and anxiety among adults reporting migraines or risk factors for cardiovascular disease, J Contextual Behav Sci. 13 (2019) 1–6. 10.1016/j.jcbs.2019.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Levin ME, MacLane C, Daflos S, Seeley JR, Hayes SC, Biglan A, Pistorello J, Examining psychological inflexibility as a transdiagnostic process across psychological disorders, J Contextual Behav Sci. (3) (2014) 155–163. 10.1016/j.jcbs.2014.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Boulanger JL, Hayes SC, Pistorello J, Experiential avoidance as a functional contextual concept, in: Kring AM & Sloan DM (Eds.), Emotion regulation and psychopathology: A transdiagnostic approach to etiology and treatment. The Guilford Press, 2010, pp. 107–136. [Google Scholar]
- [30].Vlaeyen JW, Kole-Snijders AM, Boeren RG, Van Eek H, Fear of movement/(re) injury in chronic low back pain and its relation to behavioral performance, Pain. 62(3) (1995) 363–372. 10.1016/0304-3959(94)00279-N. [DOI] [PubMed] [Google Scholar]
- *[31].Hughes A, Suleman S, Rimes KA, Marsden J, Chalder T, Cancer-related fatigue and functional impairment–Towards an understanding of cognitive and behavioural factors, J Psychosom Res. 134 (2020) 110127. 10.1016/j.jpsychores.2020.110127. [DOI] [PubMed] [Google Scholar]
- *[32].Ali S, Matcham F, Irving K, Chalder T, Fatigue and psychosocial variables in autoimmune rheumatic disease and chronic fatigue syndrome: a cross-sectional comparison, J Psychosom Res. 92 (2017) 1–8. 10.1016/j.jpsychores.2016.11.002. [DOI] [PubMed] [Google Scholar]
- *[33].Skerrett TN, Moss-Morris R, Fatigue and social impairment in multiple sclerosis: the role of patients’ cognitive and behavioral responses to their symptoms, J Psychosom Res. 61(5) (2006) 587–593. 10.1016/j.jpsychores.2006.04.018. [DOI] [PubMed] [Google Scholar]
- [34].Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, Orcutt HK, Waltz T, Zettle RD, Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance, Behav Ther. 42(4) (2011) 676–88. 10.1016/j.beth.2011.03.007. [DOI] [PubMed] [Google Scholar]
- [35].Carver CS, You want to measure coping but your protocol’s too long: consider the brief COPE, Int J Behav Med. 4(1) (1997) 92–100. 10.1207/s15327558ijbm0401_6. [DOI] [PubMed] [Google Scholar]
- [36].Silver A, Haeney M, Vijayadurai P, Wilks D, Pattrick M, Main C, The role of fear of physical movement and activity in chronic fatigue syndrome, J Psychosom Res 52(6) (2002) 485–493. 10.1016/S0022-3999(01)00298-7. [DOI] [PubMed] [Google Scholar]
- [37].Moher D, Liberati A, Tetzlaff J, Altman DG, Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement, Int J Surg 8(5) (2010) 336–341. 10.1016/j.ijsu.2010.07.299. [DOI] [PubMed] [Google Scholar]
- [38].Hwang W, Weller W, Ireys H, Anderson G, Out-of-pocket medical spending for care of chronic conditions, Health Aff 20(6) (2001) 267–278. 10.1377/hlthaff.20.6.267. [DOI] [PubMed] [Google Scholar]
- [39].Rosenthal R, The file drawer problem and tolerance for null results, Psycholo Bull. 86(3) (1979) 638. 10.1037/0033-2909.86.3.638. [DOI] [Google Scholar]
- [40].Peterson RA, Brown SP, On the use of beta coefficients in meta-analysis, J Appl Psychol. 90(1) (2005) 175. 10.1037/0021-9010.90.1.175. [DOI] [PubMed] [Google Scholar]
- [41].Roth PL, Le H, Oh I-S, Van Iddekinge CH, Bobko P, Using beta coefficients to impute missing correlations in meta-analysis research: Reasons for caution, J Appl Psychol. 103(6) (2018) 644. 10.1037/apl0000293. [DOI] [PubMed] [Google Scholar]
- [42].Penninx BWJH, Milaneschi Y, Lamers F, Vogelzangs N, Understanding the somatic consequences of depression: biological mechanisms and the role of depression symptom profile, BMC Med. 11(1) (2013) 129. 10.1186/1741-7015-11-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].American Psychiatric Association, Diagnostic and statistical manual of mental disorders, Fifth Edition (DSM-5), American Psychiatric Association, Arlington, 2013. [Google Scholar]
- [44].Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A, Rayyan—a web and mobile app for systematic reviews, Syst Rev. 5(1) (2016) 1–10. 10.1186/s13643-016-0384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].McHugh ML, Interrater reliability: the kappa statistic, Biochemia Medica. 22(3) (2012) 276–282. 10.11613/BM.2012.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Viechtbauer W, Conducting meta-analyses in R with the metafor package, J Stat Softw. 36(3) (2010) 1–48. 10.18637/jss.v036.i03. [DOI] [Google Scholar]
- [47].Borenstein M, Hedges LV, Higgins JP, Rothstein HR, A basic introduction to fixed-effect and random-effects models for meta-analysis, Res Synth Methods. 1(2) (2010) 97–111. 10.1002/jrsm.12. [DOI] [PubMed] [Google Scholar]
- [48].Schmidt FL, Oh IS, Hayes TL, Fixed-versus random-effects models in meta-analysis: Model properties and an empirical comparison of differences in results, Br J Math Stat Psychol. 62(1) (2009) 97–128. 10.1348/000711007X255327. [DOI] [PubMed] [Google Scholar]
- [49].Light R, Singer JD, Willett JB, The visual presentation and interpretation of meta-analyses., in: Copper M HL(Ed.), The Handbook of Research Synthesis, Russell Sage Foundation New York, NY, 1994. [Google Scholar]
- [50].Light RJ, Pillemer DB, Summing up: the science of reviewing research, Harvard University Press, 1984. [Google Scholar]
- [51].Egger M, Smith GD, Schneider M, Minder C, Bias in meta-analysis detected by a simple, graphical test, BMJ. 315(7109) (1997) 629–634. 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Begg CB, Mazumdar M, Operating characteristics of a rank correlation test for publication bias, Biometrics. (1994) 1088–1101. 10.2307/2533446. [DOI] [PubMed] [Google Scholar]
- [53].Sterne JA, Gavaghan D, Egger M, Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature, J Clin Epidemiol. 53(11) (2000) 1119–1129. 10.1016/S0895-4356(00)00242-0. [DOI] [PubMed] [Google Scholar]
- [54].Duval S, The trim and fill method, in: Rothstein HR, Sutton AJ, & Borenstein M (Eds.), Publication bias in meta-analysis: Prevention, assessment and adjustments, John Wiley & Sons, Ltd, 2005, pp. 127–144. [Google Scholar]
- [55].Duval S, Tweedie R, A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis, JASA. 95(449) (2000) 89–98. 10.1080/01621459.2000.10473905. [DOI] [PubMed] [Google Scholar]
- [56].Duval S, Tweedie R, Trim and fill: a simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis, Biometrics. 56(2) (2000) 455–463. 10.1111/j.0006-341X.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- [57].Simonsohn U, Nelson LD, Simmons JP, P-curve: a key to the file-drawer, J Exp Psychol Gen. 143(2) (2014) 534. 10.1037/a0033242. [DOI] [PubMed] [Google Scholar]
- [58].Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, Botella J, Assessing heterogeneity in meta-analysis: Q statistic or I2 index?, Psychol Methods. 11(2) (2006) 193. 10.1037/1082-989X.11.2.193. [DOI] [PubMed] [Google Scholar]
- [59].Schwarzer G, Carpenter JR, Rücker G, Meta-analysis with R, Springer, 2015. [Google Scholar]
- *[60].Friedberg F, Adamowicz J, Bruckenthal P, Milazzo M, Ramjan S, Quintana D, Non-improvement in chronic fatigue syndrome: relation to activity patterns, uplifts and hassles, and autonomic dysfunction, Psychosom Med. 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[61].van der Hiele K, van Gorp DA, Heerings MA, van Lieshout I, Jongen PJ, Reneman MF, van der Klink JJ, Vosman F, Middelkoop HA, Visser LH, The MS@ Work study: a 3-year prospective observational study on factors involved with work participation in patients with relapsing-remitting Multiple Sclerosis, BMC Neurolo. 15(1) (2015) 1–8. 10.1186/s12883-015-0375-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[62].Cockram CA, Level of demoralization as a predictor of stage of change in patients with gastrointestinal and colorectal cancer, University of South Florida. (2004). Available from ProQuest Dissertation & Theses Global. (305122437). [Google Scholar]
- *[63].Gillespie JM, An examination of generalized hypervigilance, functional impairment, and coping in chronic fatigue syndrome, University of Western Ontario. Ottawa: National Library of Canada. (2000). [Google Scholar]
- *[64].Hynick TJ, An examination of factors associated with successful adaptation to chronic fatigue immune dysfunction syndrome in adolescence, Antioch England Graduate School (1998). Available from ProQuest Dissertation & Theses Global; (9718684). [Google Scholar]
- *[65].McInnis O, Factors influencing fatigue and fatigue-related illnesses, Carleton University, Ottawa: National Library of Canada. (2011). [Google Scholar]
- *[66].Sepah S, How positive emotions benefit patients: Effects on immunity, physical symptoms, and biopsychosocial pathways, University of California, Los Angeles: 2011. Available from ProQuest Dissertations & Theses Global. (937119314). [Google Scholar]
- *[67].Dennis JM, Coping, psychosocial adjustment, and health status in women with systemic lupus erythematosus, University of Kansas. (1998). Available from ProQuest Dissertations & Theses Global; (304421028). [Google Scholar]
- *[68].Abrahams H, Smits L, De Lugt M, de Roos W, Kamm Y, Heins M, Verhagen C, Gielissen M, Knoop H, Severe fatigue after treatment of ductal carcinoma in situ: A comparison with age-matched breast cancer survivors and healthy controls, The Breast. 31 (2017) 76–81. 10.1016/j.breast.2016.10.020. [DOI] [PubMed] [Google Scholar]
- *[69].Artom M, Czuber-Dochan W, Sturt J, Murrells T, Norton C, The contribution of clinical and psychosocial factors to fatigue in 182 patients with inflammatory bowel disease: a cross-sectional study, AP&T. 45(3) (2017) 403–416. 10.1111/apt.13870. [DOI] [PubMed] [Google Scholar]
- *[70].Heins M, Knoop H, Nijs J, Feskens R, Meeus M, Moorkens G, Bleijenberg G, Influence of symptom expectancies on stair-climbing performance in chronic fatigue syndrome: effect of study context, Int J Behav Med. 20(2) (2013) 213–218. 10.1007/s12529-012-9253-2. [DOI] [PubMed] [Google Scholar]
- *[71].Nijs J, Meeus M, Heins M, Knoop H, Moorkens G, Bleijenberg G, Kinesiophobia, catastrophizing and anticipated symptoms before stair climbing in chronic fatigue syndrome: an experimental study, Disabil Rehabil. 34(15) (2012) 1299–1305. 10.3109/09638288.2011.641661. [DOI] [PubMed] [Google Scholar]
- *[72].Ray C, Jefferies S, Weir WR, Coping with chronic fatigue syndrome: illness responses and their relationship with fatigue, functional impairment and emotional status, Psychol Med. 25(5) (1995) 937–945. 10.1017/S0033291700037429. [DOI] [PubMed] [Google Scholar]
- *[73].Pust GE, Randerath J, Goetzmann L, Weierstall R, Korzinski M, Gold SM, Dettmers C, Ruettner B, Schmidt R, Association of fatigue severity with maladaptive coping in multiple sclerosis: A data-driven psychodynamic perspective, Front Neurol. 12 (2021) 427. 10.3389/fneur.2021.652177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[74].Ray C, Jefferies S, Weir WR, Coping with chronic fatigue syndrome: illness responses and their relationship with fatigue, functional impairment and emotional status, Psychol Med. 25(5) (1995) 937–45. 10.1017/S0033291700037429. [DOI] [PubMed] [Google Scholar]
- *[75].Golemati CV, Mavragani CP, Lionaki S, Karaiskos D, Moutsopoulos HM, Stress and disease onset in antineutrophil cytoplasmic antibody-associated vasculitis, Front Psychiatry. 8 (2017) 286. 10.3389/fpsyt.2017.00286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[76].Loades ME, Rimes K, Lievesley K, Ali S, Chalder T, Cognitive and behavioural responses to symptoms in adolescents with chronic fatigue syndrome: A case-control study nested within a cohort, Clin Child Psychol Psychiatry. 24(3) (2019) 564–579. 10.1177/1359104519835583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[77].Olive LS, Emerson CA, Cooper E, Rosenbrock EM, Mikocka-Walus AA, Fatigue, Physical Activity, and Mental Health in People Living With Inflammatory Bowel Disease, Fibromyalgia, and in Healthy Controls: A Comparative Cross-Sectional Survey, Gastroenterol Nurs 43(2) (2020) 172–185. 10.1097/SGA.0000000000000415. [DOI] [PubMed] [Google Scholar]
- *[78].Adams RN, Mosher CE, Cohee AA, Stump TE, Monahan PO, Sledge GW Jr, Cella D, Champion VL, Avoidant coping and self-efficacy mediate relationships between perceived social constraints and symptoms among long-term breast cancer survivors, Psychooncology. 26(7) (2017) 982–990. 10.1002/pon.4119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[79].Baitar A, Buntinx F, De Burghgraeve T, Deckx L, Schrijvers D, Wildiers H, van den Akker M, The influence of coping strategies on subsequent well-being in older patients with cancer: A comparison with 2 control groups, Psychooncology. 27(3) (2018) 864–870. 10.1002/pon.4587. [DOI] [PubMed] [Google Scholar]
- *[80].Bussell VA, Naus MJ, A longitudinal investigation of coping and posttraumatic growth in breast cancer survivors, J Psychosoc Oncol. 28(1) (2010) 61–78. 10.1080/07347330903438958. [DOI] [PubMed] [Google Scholar]
- *[81].Büssing A, Fischer J, Interpretation of illness in cancer survivors is associated with health-related variables and adaptive coping styles, BMC Women’s Health 9(1) (2009) 1–11. 10.1186/1472-6874-9-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[82].Daniel LC, Brumley LD, Schwartz LA, Fatigue in adolescents with cancer compared to healthy adolescents, Pediatr Blood Cancer 60(11) (2013) 1902–1907. 10.1002/pbc.24706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[83].Dolbeault S, Cayrou S, Bredart A, Viala A, Desclaux B, Saltel P, Gauvain-Piquard A, Hardy P, Dickes P, The effectiveness of a psycho-educational group after early-stage breast cancer treatment: results of a randomized French study, Psychooncology. 18(6) (2009) 647–656. 10.1002/pon.1440. [DOI] [PubMed] [Google Scholar]
- *[84].Fawzy FI, Cousins N, Fawzy NW, Kemeny ME, Elashoff R, Morton D, A structured psychiatric intervention for cancer patients: I. Changes over time in methods of coping and affective disturbance, Arch Gen Psychiatry. 47(8) (1990) 720–725. 10.1001/archpsyc.1990.01810200028004. [DOI] [PubMed] [Google Scholar]
- *[85].Green HJ, Wells DJ, Laakso L, Coping in men with prostate cancer and their partners: a quantitative and qualitative study, Eur J Cancer Care 20(2) (2011) 237–247. 10.1111/j.1365-2354.2010.01225.x. [DOI] [PubMed] [Google Scholar]
- *[86].Guimond AJ, Ivers H, Savard J, Clusters of Psychological Symptoms in Breast Cancer: Is There a Common Psychological Mechanism?, Cancer Nurs. 43(5) (2020) 343–353. 10.1097/NCC.0000000000000705. [DOI] [PubMed] [Google Scholar]
- *[87].Hosaka T, Tokuda Y, Aoki T, Kojoh Y, Coping styles among Japanese women with breast cancer, Tokai J Exp Clin Med 20(2) (1995) 137–141. [PubMed] [Google Scholar]
- *[88].Larson AG, Morris KJ, Juckett MB, Coe CL, Broman AT, Costanzo ES, Mindfulness, experiential avoidance, and recovery from hematopoietic stem cell transplantation, Ann of Behav Med 53(10) (2019) 886–895. 10.1093/abm/kay097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[89].Lutgendorf SK, Anderson B, Rothrock N, Buller RE, Sood AK, Sorosky JI, Quality of life and mood in women receiving extensive chemotherapy for gynecologic cancer, Cancer. 89(6) (2000) 1402–1411. 10.1002/1097-0142(20000915)89:6<1402::AID-CNCR26>3.0.CO;2-H. [DOI] [PubMed] [Google Scholar]
- *[90].Papadopoulos D, Kiagia M, Charpidou A, Gkiozos I, Syrigos K, Psychological correlates of sleep quality in lung cancer patients under chemotherapy: A single-center cross-sectional study, Psychooncology. 28(9) (2019) 1879–1886. 10.1002/pon.5167. [DOI] [PubMed] [Google Scholar]
- *[91].van Deuren S, Van Dulmen-den Broeder E, Boonstra A, Gielissen M, Blijlevens N, Loonen J, Knoop H, Fatigue-Related Cognitive-Behavioral Factors in Survivors of Childhood Cancer: Comparison with Chronic Fatigue Syndrome and Survivors of Adult-Onset Cancer, J Adolesc Young Adult Oncol (2020). 10.1089/jayao.2020.0094. [DOI] [PubMed] [Google Scholar]
- *[92].Velthuis MJ, Van den Bussche E, May AM, Gijsen BC, Nijs S, Vlaeyen JW, Fear of movement in cancer survivors: validation of the Modified Tampa Scale of Kinesiophobia—Fatigue, Psychooncology. 21(7) (2012) 762–770. 10.1002/pon.1971. [DOI] [PubMed] [Google Scholar]
- *[93].Novakov I, Emotional state, fatigue, functional status and quality of life in breast cancer: exploring the moderating role of psychological inflexibility, Psychol Health Med. 26(7) (2021) 877–886. 10.1080/13548506.2020.1842896. [DOI] [PubMed] [Google Scholar]
- *[94].Madison AA, Peng J, Shrout MR, Renna ME, Alfano CM, Povoski SP, Lipari AM, Agnese DM, Carson WE, Malarkey WB, Distress Trajectories in Black and White Breast Cancer Survivors: From Diagnosis to Survivorship, Psychoneuroendocrinology (2021) 105288. 10.1016/j.psyneuen.2021.105288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[95].Hyland KA, Nelson AM, Eisel SL, Hoogland AI, Ibarz-Pinilla J, Sweet K, Jacobsen PB, Knoop H, Jim HS, Fatigue perpetuating factors as mediators of change in a cognitive behavioral intervention for targeted therapy-related fatigue in chronic myeloid leukemia: a pilot study, Ann Behav Med. (2021). 10.1093/abm/kaab035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[96].De Padova S, Grassi L, Vagheggini A, Belvederi Murri M, Folesani F, Rossi L, Farolfi A, Bertelli T, Passardi A, Berardi A, Post-traumatic stress symptoms in long-term disease-free cancer survivors and their family caregivers, Cancer Med. (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[97].Bassi M, Grobberio M, Negri L, Cilia S, Minacapelli E, Niccolai C, Pattini M, Pietrolongo E, Quartuccio ME, Viterbo RG, The contribution of illness beliefs, coping strategies, and social support to perceived physical health and fatigue in multiple sclerosis, J Clin Psychol Med Settings. (2019) 1–12. 10.1007/s10880-019-09692-6. [DOI] [PubMed] [Google Scholar]
- *[98].Bol Y, Duits AA, Lousberg R, Hupperts RM, Lacroix MH, Verhey FR, Vlaeyen JW, Fatigue and physical disability in patients with multiple sclerosis: a structural equation modeling approach, J Behav Med. 33(5) (2010) 355–363. 10.1007/s10865-010-9266-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[99].Brown RF, Valpiani EM, Tennant CC, Dunn SM, Sharrock M, Hodgkinson S, Pollard JD, Longitudinal assessment of anxiety, depression, and fatigue in people with multiple sclerosis, Psychol Psychother. 82(1) (2009) 41–56. 10.1348/147608308X345614. [DOI] [PubMed] [Google Scholar]
- *[100].Contentti EC, López PA, Pettinicchi JP, Alonso R, Tizio S, Tkachuk V, Caride A, Galea I, Do people with multiple sclerosis want to discuss their long-term prognosis? A nationwide study in Argentina, Multiple Scler Relat Disord. 37 (2020) 101445. 10.1016/j.msard.2019.101445. [DOI] [PubMed] [Google Scholar]
- *[101].Farran N, Ammar D, Darwish H, Quality of life and coping strategies in Lebanese Multiple Sclerosis patients: A pilot study, Multiple Scler Relat Disord. 6 (2016) 21–27. 10.1016/j.msard.2015.12.003. [DOI] [PubMed] [Google Scholar]
- *[102].Goretti B, Portaccio E, Zipoli V, Hakiki B, Siracusa G, Sorbi S, Amato MP, Coping strategies, psychological variables and their relationship with quality of life in multiple sclerosis, Neurol Sci 30(1) (2009) 15–20. 10.1007/s10072-008-0009-3. [DOI] [PubMed] [Google Scholar]
- *[103].Kasser SL, Zia A, Mediating role of resilience on quality of life in individuals with multiple sclerosis: a structural equation modeling approach, Arch Phys Med Rehabil 101(7) (2020) 1152–1161. 10.1016/j.apmr.2020.02.010. [DOI] [PubMed] [Google Scholar]
- *[104].Strober L, Arnett P, Unemployment among women with multiple sclerosis: the role of coping and perceived stress and support in the workplace, Psychol Health Med. 21(4) (2016) 496–504. 10.1080/13548506.2015.1093645. [DOI] [PubMed] [Google Scholar]
- *[105].Strober L, Determinants of unemployment in multiple sclerosis (MS): The role of disease, person-specific factors, and engagement in positive health-related behaviors, Multiple Scler Relat Disord. 46 (2020) 102487. 10.1016/j.msard.2020.102487. [DOI] [PubMed] [Google Scholar]
- *[106].Wijenberg ML, Stapert SZ, Köhler S, Bol Y, Explaining fatigue in multiple sclerosis: cross-validation of a biopsychosocial model, J Behav Med. 39(5) (2016) 815–822. 10.1007/s10865-016-9749-3. [DOI] [PubMed] [Google Scholar]
- *[107].Ukueberuwa DM, Arnett PA, Evaluating the role of coping style as a moderator of fatigue and risk for future cognitive impairment in multiple sclerosis, J Int Neuropsychol Soc 20(7) (2014) 751–5. 10.1017/S1355617714000587. [DOI] [PubMed] [Google Scholar]
- *[108].Vanotti S, Cabral N, Eizaguirre MB, Marinangeli A, Roman MS, Alonso R, Silva B, Garcea O, Coping strategies: Seeking personalized care in relapsing-remitting multiple sclerosis. A patient reported measure–coping responses inventory, Mult Scler J Exp Transl Clin 7(1) (2021). 10.1177/2055217320987588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[109].Johnson SK, Gil-Rivas V, Schmaling KB, Coping strategies in chronic fatigue syndrome: Outcomes over time, Stress Health. 24(4) (2008) 305–312. 10.1002/smi.1185. [DOI] [Google Scholar]
- *[110].Knussen C, Lee D, Chronic fatigue syndrome: Symptoms, appraisal and ways of coping, Br J Health Psychol 3(2) (1998) 111–121. 10.1111/j.2044-8287.1998.tb00560.x. [DOI] [Google Scholar]
- *[111].Loades ME, Stallard P, Morris R, Kessler D, Crawley E, Do adolescents with chronic fatigue syndrome (CFS/ME) and co-morbid anxiety and/or depressive symptoms think differently to those who do not have co-morbid psychopathology?, J Affect Disord. 274 (2020) 752–758. 10.1016/j.jad.2020.05.113. [DOI] [PubMed] [Google Scholar]
- *[112].Tummers M, Knoop H, van Dam A, Bleijenberg G, Moderators of the treatment response to guided self-instruction for chronic fatigue syndrome, J Psychosom Res. 74(5) (2013) 373–377. 10.1016/j.jpsychores.2013.01.007. [DOI] [PubMed] [Google Scholar]
- *[113].Wearden AJ, Emsley R, Mediators of the effects on fatigue of pragmatic rehabilitation for chronic fatigue syndrome, J Consult Clin Psychol. 81(5) (2013) 831–8. 10.1037/a003356110.1037/a0033561. [DOI] [PubMed] [Google Scholar]
- *[114].Koike T, Kazuma K, Kawamura S, The relationship between fatigue, coping behavior, and inflammation in patients with rheumatoid arthritis, Mod Rheumatol. 10(3) (2000) 141–149. 10.3109/s101650070021. [DOI] [PubMed] [Google Scholar]
- *[115].Van der Elst K, Verschueren P, De Cock D, De Groef A, Stouten V, Pazmino S, Vriezekolk J, Joly J, Moons P, Westhovens R, One in five patients with rapidly and persistently controlled early rheumatoid arthritis report poor well-being after 1 year of treatment, RMD Open 6(1) (2020) e001146. 10.1136/rmdopen-2019-001146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[116].Matcham F, Ali S, Irving K, Chalder T, Psychological Predictors of Fatigue, Work and Social Adjustment, and Psychological Distress in Rheumatology Outpatients, Eur J Health. Psychol (2019). 10.1016/j.jpsychores.2016.11.002. [DOI] [Google Scholar]
- *[117].Abshire M, Russell SD, Davidson PM, Budhathoki C, Han H-R, Grady KL, Desai S, Himmelfarb CD, Social support moderates the relationship between perceived stress and quality of life in patients with a left ventricular assist device, J Cardiovasc Nurs. 33(5) (2018) E1. 10.1097/JCN.0000000000000487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[118].Francis F, Burger I, Poll EM, Reineke A, Strasburger CJ, Dohmen G, Gilsbach JM, Kreitschmann-Andermahr I, Can cardiac surgery cause hypopituitarism? Pituitary. 15(1) (2012) 30–6. 10.1007/s11102-011-0322-3. [DOI] [PubMed] [Google Scholar]
- *[119].Chilcot J, Moss-Morris R, Artom M, Harden L, Picariello F, Hughes H, Bates S, Macdougall IC, Psychosocial and clinical correlates of fatigue in haemodialysis patients: the importance of patients’ illness cognitions and behaviours, Int J Behav Med. 23(3) (2016) 271–281. 10.1007/s12529-015-9525-8. [DOI] [PubMed] [Google Scholar]
- *[120].Chisari C, Chilcot J, The experience of pain severity and pain interference in vulvodynia patients: The role of cognitive-behavioural factors, psychological distress and fatigue, J Psychosom Res. 93 (2017) 83–89. 10.1016/j.jpsychores.2016.12.010. [DOI] [PubMed] [Google Scholar]
- *[121].McCabe PJ, Barnason SA, Illness perceptions, coping strategies, and symptoms contribute to psychological distress in patients with recurrent symptomatic atrial fibrillation, J Cardiovas Nurs. 27(5) (2012) 431–444. 10.1097/JCN.0b013e31821e7ab1. [DOI] [PubMed] [Google Scholar]
- *[122].Jaracz K, Mielcarek L, Kozubski W, Clinical and psychological correlates of poststroke fatigue. Preliminary results, Neurologia i neurochirurgia polska 41(1) (2007) 36–43. [PubMed] [Google Scholar]
- *[123].Sveinsdottir V, Eriksen HR, Ursin H, Hansen ÅM, Harris A, Cortisol, health, and coping in patients with nonspecific low back pain, Appl Psychophysio Biofeedback. 41(1) (2016) 9–16. 10.1007/s10484-015-9300-2. [DOI] [PubMed] [Google Scholar]
- *[124].Tersteeg IM, Koopman FS, Stolwijk-Swüste JM, Beelen A, Nollet F, Group CS, A 5-year longitudinal study of fatigue in patients with late-onset sequelae of poliomyelitis, Arch Phys Med Rehabil. 92(6) (2011) 899–904. 10.1016/j.apmr.2011.01.005. [DOI] [PubMed] [Google Scholar]
- [125].Viechtbauer W, Cheung MWL, Outlier and influence diagnostics for meta-analysis, Research synthesis methods. 1(2) (2010) 112–125. 10.1002/jrsm.11. [DOI] [PubMed] [Google Scholar]
- [126].Baujat B, Mahé C, Pignon JP, Hill C, A graphical method for exploring heterogeneity in meta-analyses: application to a meta-analysis of 65 trials, Stat Med. 21(18) (2002) 2641–2652. 10.1002/sim.1221. [DOI] [PubMed] [Google Scholar]
- [127].Higgins JP, Thompson SG, Deeks JJ, Altman DG, Measuring inconsistency in meta-analyses, BMJ. 327(7414) (2003) 557–560. 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [128].Rosenstiel AK, Keefe FJ, The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment, Pain. 17(1) (1983) 33–44. 10.1016/0304-3959(83)90125-2. [DOI] [PubMed] [Google Scholar]
- [129].Vercoulen JH, Swanink CM, Fennis JF, Galama JM, van der Meer JW, Bleijenberg G, Dimensional assessment of chronic fatigue syndrome, J Psychosom Res. 38(5) (1994) 383–392. 10.1016/0022-3999(94)90099-X. [DOI] [PubMed] [Google Scholar]
- [130].Whitehead LC, Unahi K, Burrell B, Crowe MT, The experience of fatigue across long-term conditions: a qualitative meta-synthesis, J Pain Symptom Manag. 52(1) (2016) 131–143. e1. 10.1016/j.jpainsymman.2016.02.013. [DOI] [PubMed] [Google Scholar]
- [131].Lai J-S, Cella D, Choi S, Junghaenel DU, Christodoulou C, Gershon R, Stone A, How item banks and their application can influence measurement practice in rehabilitation medicine: a PROMIS fatigue item bank example, Arch Phys Med Rehabil. 92(10) (2011) S20–S27. 10.1016/j.apmr.2010.08.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [132].Heijmans MJWM, Coping and adaptive outcome in chronic fatigue syndrome: Importance of illness cognitions, J Psychosom Res. 45(1) (1998) 39–51. 10.1016/S0022-3999(97)00265-1. [DOI] [PubMed] [Google Scholar]
- [133].Jacobsen HB, Kallestad H, Landrø NI, Borchgrevink PC, Stiles TC, Processes in acceptance and commitment therapy and the rehabilitation of chronic fatigue, Scand J Psychol. 58(3) (2017) 211–220. 10.1111/sjop.12363. [DOI] [PubMed] [Google Scholar]
- [134].Brugnera A, Nordstrand Jacobsen T, Woodhouse A, Compare A, Børsting Jacobsen H, Effectiveness of an ACT-based rehabilitation program for the treatment of chronic fatigue: Results from a 12-months longitudinal study, Scand J Psychol. (2020). 10.1111/sjop.12672. [DOI] [PubMed] [Google Scholar]
- *[135].Wearden AJ, Emsley R, Mediators of the effects on fatigue of pragmatic rehabilitation for chronic fatigue syndrome, J Consult Clin Psychol 81(5) (2013) 831. 10.1037/a003356110.1037/a0033561. [DOI] [PubMed] [Google Scholar]
- [136].Sharpe M, T Chalder P White, Evidence-based care for people with chronic fatigue syndrome and myalgic encephalomyelitis, J Gen Intern Med 37 (2022) 449–452. 10.1007/s11606-021-0788-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [137].Nehme M, Braillard O, Chappuis F, Courvoisier DS, Guessous I, Team CS, Prevalence of symptoms more than seven months after diagnosis of symptomatic COVID-19 in an outpatient setting, Ann Intern Med. 174(9) (2021) 1252–1260. 10.7326/M21-0878. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.