

Abstract
Interscalene block, the gold standard for shoulder surgeries is inevitably associated with phrenic nerve palsy, even at low volumes. The major innervation of the shoulder joint is by suprascapular nerve and axillary nerve. Suprascapular nerve block has been used commonly for postoperative analgesia in shoulder surgeries done under GA. Combining axillary block with suprascapular nerve block was found to provide superior analgesia when compared to suprascapular block alone. Selective Suprascapular and Axillary nerve (SSAX) block provides effective analgesia in shoulder surgeries without causing diaphragm palsy, but has limited published literature. We performed ultrasound guided suprascapular block in the supraspinous fossa (posterior approach) using 10 ml of 0.25% Ropivacaine and axillary block in the quadrangular space using 6ml of 0.25% Ropivacaine before administration of general anaesthesia (GA) in 4 cases. Among four cases, 2 were closed shoulder manipulation with intra-articular steroid injection for periarthritis, 1 was closed reduction and K-wire fixation for chronic shoulder subluxation and the 4th was Latarjet procedure for recurrent shoulder dislocation. All patients received paracetamol 1g at the end of the procedure and every 6 h postoperatively. No patient experienced pain during recovery and the analgesia lasted for a mean duration of 347.5 minutes. Tramadol was required for rescue analgesia in only one patient (Latarjet surgery). We found that SSAX block provided effective analgesia in all patients, but needs randomized controlled trials with larger sample size comparing with interscalene block.
Keywords: SSAX block, diaphragm sparing, shoulder surgeries
Introduction
Shoulder surgeries are commonly associated with severe postoperative pain. Combining regional anesthetic techniques with general anesthesia reduces operating time, maintains hemodynamics, decreases opioid consumption, allows earlier hospital discharge, and improves patient satisfaction. Interscalene block (ISB), the gold standard for shoulder surgeries is inevitably associated with phrenic nerve palsy, even at low volumes of 5 mL.[1] Selective Suprascapular and Axillary nerve (SSAX) block, both being branches of brachial plexus innervating the majority of the shoulder joint, provides effective analgesia in shoulder surgeries without causing diaphragm palsy but has limited published literature[2,3] and it got popularized as shoulder block nowadays.[4] We performed SSAX block in four shoulder orthopedic procedures done under general anesthesia and observed effective analgesia.
Case Report
Among the four cases, two were closed-shoulder manipulation with intra-articular steroid injection for periarthritis causing frozen shoulder, one was closed reduction and K-wire fixation for chronic shoulder subluxation, and the fourth case was Latarjet procedure for recurrent shoulder dislocation (as described in Table 1). Latarjet surgery was the only open surgical procedure in this series.
Table 1.
Clinical characteristics of the cases
| Patient characteristics | Surgical procedure | Anesthesia technique | Duration of Analgesia (min) | Number of rescue tramadol doses | Patient satisfaction score |
|---|---|---|---|---|---|
| 56 years, female | Shoulder mobilization + steroid injection | GA- BMV | 450 | 0 | 4/5 |
| 50 years, male | Shoulder mobilization + steroid injection | GA- BMV | 420 | 0 | 5/5 |
| 54 years, female | Shoulder reduction + K-wire fixation | GA- LMA | 390 | 0 | 4/5 |
| 40 years, male | Latarjet- Bairstow procedure | GA- ETT | 130 | 2 | 3/5 |
GA: General anesthesia, BMV: Bag and mask ventilation, LMA: Laryngeal mask airway, ETT: EndoTracheal tube
The blocks were given 30 min before administration of general anesthesia (GA) in all four cases. Suprascapular nerve and axillary nerve were blocked individually using ultrasound with linear, high-frequency probe (6–13 MHz) in lateral position. Suprascapular nerve block was performed by posterior approach in the supraspinous fossa around the pulsation of suprascapular artery using 10 mL of 0.25% ropivacaine by out-of-plane approach with 22-G, 10 cm Stimuplex needle [Figure 1]. Axillary nerve block was performed in the quadrangular space of the upper arm using 6 mL of 0.25% ropivacaine around the posterior circumflex humeral artery near the surgical neck of the humerus by an in-plane technique using 10 cm, 22-G Stimuplex needle [Figure 2].
Figure 1.
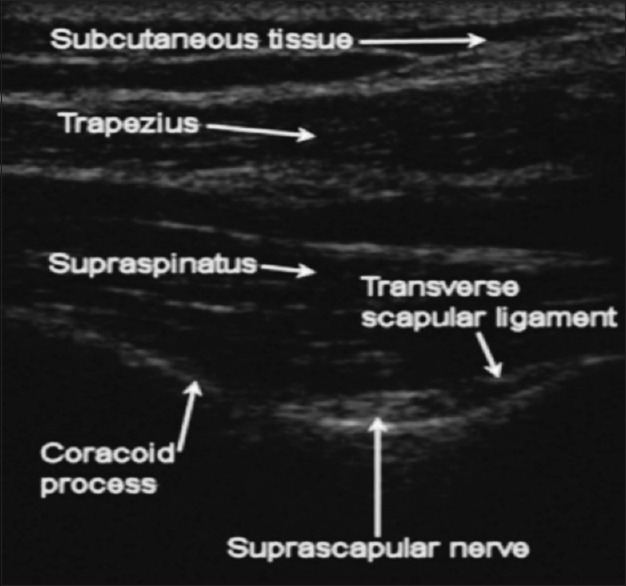
Ultrasound-guided suprascapular nerve block
Figure 2.
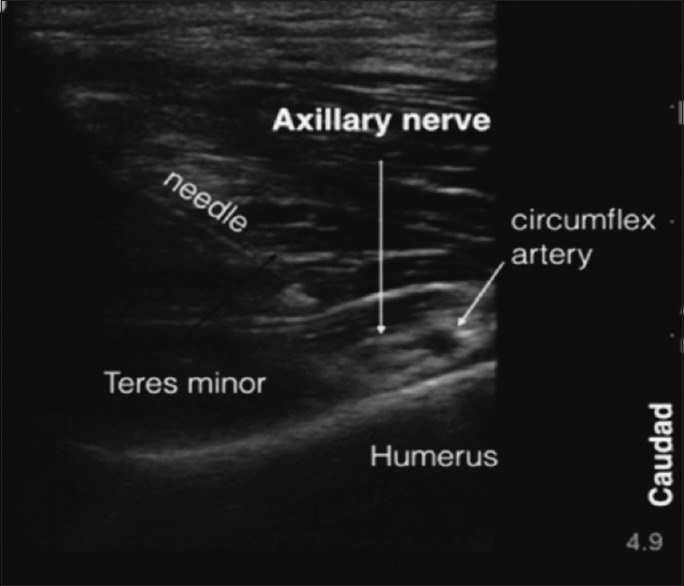
Ultrasound-guided axillary nerve block
Fentanyl 2 mcg/kg and propofol 2 mg/kg were used during induction of anesthesia and maintained with nitrous oxide-oxygen and sevoflurane. The duration of surgery lasted less than 30 min in the first three cases and for 2 h in case of Latarjet procedure. Intraoperative hemodynamic parameters were well maintained. All the patients received paracetamol 1 g at the end of the procedure and every 6 h postoperatively. The patients were monitored in the Post Anaesthesia Care Unit (PACU) for pain assessment and analgesic requirements.
None of the patient experienced pain during recovery and the analgesia lasted for a mean duration of 347.5 min. Visual analogue scale scores for pain remained better (<4/10) throughout the 24-h postoperative period. Tramadol was used for rescue analgesia and was required in only one patient (Latarjet surgery). Patient satisfaction scores were good (>3/5) in all the patients.
Discussion
The major innervation of the shoulder joint is by suprascapular nerve, arising from superior trunk of the brachial plexus (contributes to 70% of joint innervation) covering the posterior aspect of the joint and axillary nerve arising from the posterior cord (25% of nerve supply) along with subscapular (posterior cord) and lateral pectoral nerve (lateral cord) innervates the anterior aspect of the joint.[5]
Suprascapular nerve block, though first described in 1941, has recently been used commonly for postoperative analgesia in shoulder surgeries, which can be blocked by either anterior or posterior approach.[6] Continous suprascapular nerve blocks with indwelling catheters have also been described in shoulder surgeries.[7] However, the anterior aspect of the joint, which is supplied by axillary nerve will not be adequately blocked. Combining axillary nerve block (also known as circumflex nerve block) along with suprascapular nerve block was found to provide superior analgesia when compared with suprascapular block alone.[8] SSAX block can be used as an effective alternative for interscalene block in shoulder surgeries with the advantage of sparing the phrenic nerve, thereby avoiding hemidiaphragmatic palsy and consequent respiratory complications. Hence, this would be ideal for patients with respiratory disorders such as chronic obstructive pulmonary disease (COPD) and morbid obesity. Also, the other disadvantages of ISB like hoarseness of voice, Horner's syndrome, and neurological complications can be overcome with SSAX block.[3,5,9]
The analgesic efficacy of SSAX block was demonstrated in various studies[2,3] and was found to be comparable with interscalene block in terms of postoperative pain scores, duration of analgesia, and morphine consumption. Neuts et al.[10] observed that the SSAX block is inferior to ISB for immediate postoperative analgesia (<8 h) but comparable with ISB after that till 24 h and increased incidence of dyspnea and discomfort in the ISB group.
We found that SSAX block provided effective analgesia in all patients, but needs randomized controlled trials with a larger sample size compared with interscalene block.
Conclusion
Suprascapular and Axillary nerve (SSAX) block can be used as an effective and diaphragm-sparing alternative to interscalene block for shoulder surgeries.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Riazi S, Carmichael N, Awad I, Holtby RM, McCartney CJ. Effect of local anaesthetic volume (20 vs 5 ml) on the efficacy and respiratory consequences of ultrasound-guided interscalene brachial plexus block. Br J Anaesth. 2008;101:549–56. doi: 10.1093/bja/aen229. [DOI] [PubMed] [Google Scholar]
- 2.Dhir S, Sondekoppam RV, Sharma R, Ganapathy S, Athwal GS. A comparison of combined suprascapular and axillary nerve blocks to interscalene nerve block for analgesia in arthroscopic shoulder surgery: An equivalence study. Reg Anesth Pain Med. 2016;41:564–71. doi: 10.1097/AAP.0000000000000436. [DOI] [PubMed] [Google Scholar]
- 3.Waleed A. Postoperative analgesia for arthroscopic shoulder surgery: Comparison between ultrasound-guided interscalene block and combined suprascapular and axillary nerve blocks. Ain-Shams J Anaesthesiol. 2016;9:536–41. [Google Scholar]
- 4.Zanfaly HE, Aly AA. Shoulder block versus interscalene block for postoperative pain relief after shoulder arthroscopy. Ain-Shams J Anaesthesiol. 2016;9:296–303. [Google Scholar]
- 5.Tran DQ, Elgueta MF, Aliste J, Finlayson RJ. Diaphragm-sparing nerve blocks for shoulder surgery. Reg Anesth Pain Med. 2017;42:32–8. doi: 10.1097/AAP.0000000000000529. [DOI] [PubMed] [Google Scholar]
- 6.Wiegel M, Moriggl B, Schwarzkopf P, Petroff D, Reske AW. Anterior suprascapular nerve block versus interscalene brachial plexus block for shoulder surgery in the outpatient setting: A randomized controlled patient- and assessor-blinded trial. Reg Anesth Pain Med. 2017;42:310–8. doi: 10.1097/AAP.0000000000000573. [DOI] [PubMed] [Google Scholar]
- 7.Careskey M, Naidu R. Continuous suprascapular nerve block with a perineural catheter for reverse shoulder arthroplasty rescue analgesia in a patient with severe chronic obstructive pulmonary disease. A A Case Rep. 2016;7:37–40. doi: 10.1213/XAA.0000000000000338. [DOI] [PubMed] [Google Scholar]
- 8.Lee JJ, Kim DY, Hwang JT, Lee SS, Hwang SM, Kim GH, et al. Effect of ultrasonographically guided axillary nerve block combined with suprascapular nerve block in arthroscopic rotator cuff repair: A randomized controlled trial. Arthroscopy. 2014;30:906–14. doi: 10.1016/j.arthro.2014.03.014. [DOI] [PubMed] [Google Scholar]
- 9.Pitombo PF, Meira Barros R, Matos MA, Pinheiro Módolo NS. Selective suprascapular and axillary nerve block provides adequate analgesia and minimal motor block. Comparison with interscalene block. Braz J Anesthesiol. 2013;63:45–51. doi: 10.1016/S0034-7094(13)70197-1. [DOI] [PubMed] [Google Scholar]
- 10.Neuts A, Stessel B, Wouters PF, Dierickx C, Cools W, Ory JP, et al. Selective suprascapular and axillary nerve block versus interscalene plexus block for pain control after arthroscopic shoulder surgery: A noninferiority randomized parallel-controlled clinical trial. Reg Anesth Pain Med. 2018;43:738–44. doi: 10.1097/AAP.0000000000000777. [DOI] [PubMed] [Google Scholar]