

Abstract
Background: SARS-CoV-2 transmission has been reported to be associated with close contact with infected individuals. However, the mechanistic pathway for transmission in close contact settings is unclear. Our objective was to identify, appraise and summarise the evidence from studies assessing the role of close contact in SARS-CoV-2 transmission.
Methods: This review is part of an Open Evidence Review on Transmission Dynamics of SARS-CoV-2. We conduct ongoing searches using WHO Covid-19 Database, LitCovid, medRxiv, PubMed and Google Scholar; assess study quality based on the QUADAS-2 criteria and report important findings on an ongoing basis.
Results: We included 181 studies: 171 primary studies and 10 systematic reviews. The settings for primary studies were predominantly in home/quarantine facilities (31.6%) and acute care hospitals (15.2%). The overall reporting quality of the studies was low to moderate. There was significant heterogeneity in design and methodology. The frequency of attack rates (PCR testing) was 3.5-75%; attack rates were highest in prison and wedding venues, and in households. The frequency of secondary attack rates was 0.3-100% with rates highest in home/quarantine settings. Three studies showed no transmission if index cases had recurrent infection. Viral culture was performed in three studies of which two found viable virus; culture results were negative where index cases had recurrent infections. Ten studies performed genomic sequencing with phylogenetic analysis – the completeness of genomic similarity ranged from 81-100%. Findings from systematic reviews showed that children were significantly less likely to transmit SARS-CoV-2 and household contact was associated with a significantly increased risk of infection.
Conclusions: The evidence from published studies demonstrates that SARS-CoV-2 can be transmitted via close contact settings. The risk of transmission is greater in household contacts. There was wide variation in methodology. Standardized guidelines for reporting transmission in close contact settings should be developed to improve the quality reporting.
Keywords: Close contact, transmission, COVID-19, systematic review
Introduction
The SARS-CoV-2 (COVID-19) pandemic is a major public health concern. Based on WHO data, there have been over 120 million confirmed cases and over two and a half million deaths globally as of 20th March 2021 1 . Many national governments have implemented prevention and control measures and vaccines are now being approved and administered; the overall global spread of the virus now appears to be slowing. Current evidence from epidemiologic and virologic studies suggest SARS-CoV-2 is primarily transmitted via respiratory droplets and direct and indirect contact 2, 3 . However, controversy still exists about how the virus is transmitted and the relative frequency of the modes of transmission and if these modes may be altered in specific settings 4, 5 .
Although close contact is thought to be associated with transmission of SARS-CoV-2, there is uncertainty about the thresholds of proximity for “close contact” and the factors that may influence the transmission in a “close contact”. Furthermore, there is lack of clarity about how research should be conducted in the setting of transmission with close contact which may include transmission via any one of or the combination of respiratory droplets, direct contact, or indirect contact.
Several studies investigating the role of close contact in SARS-CoV-2 transmission have been published but the pathways and thresholds for transmission are not well established. The objective of this review was to identify, appraise and summarize the evidence from primary studies and systematic reviews investigating the role of close contact in the transmission of SARS-CoV-2. Terminology for this article can be found in Box 1.
Box 1. Terminology.
Close contact: Someone who was within 6 feet of an infected person for a cumulative total of 15 minutes or more over a 24-hour period starting from 2 days before illness onset (or, for asymptomatic patients, 2 days prior to test specimen collection) until the time the patient is isolated 1 ; The World Health Organization (WHO) additionally includes direct physical contact with a probable or confirmed case, direct care for a patient with probable or confirmed COVID-19 disease without using proper PPE, and other situations as indicated by local risk assessments.
Attack rate: The proportion of those who become ill after a specified exposure 2 .
Secondary attack rate: The probability that infection occurs among susceptible persons within a reasonable incubation period following known contact with an infectious person or an infectious source 3 .
Cycle threshold: The number of cycles required for the fluorescent signal to cross the threshold. Ct levels are inversely proportional to the amount of target nucleic acid in the sample 4 .
2 https://www.who.int/foodsafety/publications/foodborne_disease/Annex_7.pdf
3Halloran ME. Secondary Attack Rate. In: Peter A, Theodore C, editors. Encyclopedia of Biostatistics. New York: John Wiley & Sons Ltd; 2005
Methods
We are undertaking an open evidence review examining the factors and circumstances that impact on the transmission of SARS-CoV-2, based on our published protocol last updated on the 1 December 2020 (Version 3: 1 December 2020, Extended data: Appendix 1 6 ). This review aims to identify, appraise, and summarize the evidence (from peer-reviewed studies or studies awaiting peer review) examining the role of close contact in the transmission of SARS-CoV-2 and the factors that influence transmissibility. We are conducting an ongoing search in WHO Covid-19 Database, LitCovid, medRxiv, and Google Scholar for SARS-CoV-2 for keywords and associated synonyms. For this review, we also conducted searches on PubMed. The searches for this update were conducted up to 20th December 2020 ( Extended data: Appendix 2 6 ). We did not impose any language restrictions.
We included studies of any design that investigated transmission associated with close contact but excluded predictive or modelling studies. We reviewed the results for relevance and for articles that appeared particularly relevant, we undertook forward citation matching to identify relevant results. We assessed the risk of bias of included primary studies using five domains from the QUADAS-2 criteria 7 ; we adapted this tool because the included studies were not primarily designed as diagnostic accuracy studies. We did not perform formal assessments of the quality of included systematic reviews but summarized their findings, including quality of their included studies as reported by the authors. We extracted the following information from included studies: study design characteristics including the definition used of “close contact”, population, main methods, and associated outcomes including the number of swab samples taken with frequency and timing of samples, and cycle thresholds and samples concentrations. We also extracted information on viral cultures including the methods used. One reviewer (IJO) assessed the risk of bias from primary studies, and these were independently verified by a second reviewer (EAS). One reviewer (IJO) extracted data from the included primary studies, and these were independently checked by a second reviewer (CJH). One reviewer (CJH) extracted data from the included systematic reviews, and these were independently checked by a second reviewer (IJO). Disagreements in the data extraction or bias assessments were resolved by consensus. We presented the results in tabular format, and bar charts used to present the frequency of positive tests. We reported results of specific subgroups of studies where relevant. Because of substantial heterogeneity across the included studies, we considered meta-analyses inappropriate.
Results
We identified 1202 non-duplicate citations of which 229 were considered eligible ( Figure 1). We excluded 48 full-text studies for various reasons (see Extended data: Appendix 3 6 for the list of excluded studies and reasons for exclusion). Finally, we included 181 studies: 171 primary studies and 10 systematic reviews (see Extended data: Appendix 4 for references to included studies). The main characteristics of the included primary studies and systematic reviews are shown in Table 1 and Table 2, respectively.
Figure 1. Flow diagram showing the process for inclusion of studies assessing close contact transmission in SARS-CoV-2.

Table 1. Close contact study characteristics.
| Study ID | Country | Study Design/Setting | Type of
transmission |
Population/environment | Test method | Timing of sample collection | Viral
culture |
Cycle threshold | Other information |
|---|---|---|---|---|---|---|---|---|---|
| Abdulrahman 2020 | Bahrain | Observational comparative
Country-wide 09/2020 |
Community | Before and after study of subjects
attending 2 religious events |
PCR | Not reported | No | >40 was considered
negative |
A 10-day period before the event was compared to a 10-day
period beginning 10 days after the event. All symptomatic individuals and close contacts to a confirmed case were tested. Positive and negative controls were included for quality control purposes. |
| Adamik 2020 | Poland | Observational Home | Household | 9756 index cases; 3553 secondary cases | Not reported | Not reported | No | No | Only cases for which clear epidemiological links were
registered as household transmission together with their source cases were included. Cases in social care units and households of minimum 15 inhabitants were removed from the analysis, as an initial analysis revealed that those were not representative for the overall population, due to over- represented comorbidities and severe cases. |
| Agergaard 2020 | Denmark | Home quarantine with 1
asymptomatic index case 11/03/2020 to 01/04/2020 |
Household | Family cluster of 5: Index case arranged
a self-imposed 2-week home quarantine along with family of four |
PCR
Serology |
Not reported for PCR | No | Not specified for PCR | Index case recently returned from skiing trip in Austria
iFlash SARS-CoV-2 N/S IgM/IgG cut-off: ≥12 AU/ml = positive. DiaSorin SARS-CoV-2 S1/S2 IgG cut-off: ≥15 AU/ml = positive |
| Angulo-Bazán 2020 | Peru | Observational retrospective
Household 23/04/2020 to 02/05/2020 |
Household | 52 households in Metropolitan Lima with
only one member with COVID-19 Contacts cohabited in same home with index case |
RT-PCR (index)
Serology |
Not reported | No | Not specified | Evaluation was conducted 13.6 ± 3.7 days after the diagnostic
test |
| Armann 2020 | Germany | Observational - cross-sectional
Schools, homes May to October 2020 |
Local
Household |
1538 students and 507 teachers were
initially enrolled, and 1334 students and 445 teachers completed both study visits. |
Serology | Week 0 and Week 16 | No | N/A | an index (S/C) of < 1.4 was considered negative whereas
one >/= 1.4 was considered positive) and an ELISA detecting IgG against the S1 domain of the SARS-CoV-2 spike protein (Euroimmun® Anti-SARS CoV-2 ELISA) (a ratio < 0.8 was considered negative, 0.8–1.1 equivocal, > 1.1 positive) |
| Arnedo-Pena 2020 | Spain | Retrospective cohort Homes
February-May 2020 |
Household | 347 index cases: 745 household contacts | RT-PCR | Not reported | No | Not specified | COVID-19 cases of community outbreaks and from institutions
as nursing homes were excluded. Secondary attack rate was defined as the proportion of secondary cases from the total of contacts that live in the household of index case. |
| Baker 2020 | USA | Observational
Acute-care hospital |
Nosocomial | 44 HCWs who provided care for a
hospitalized patient with COVID-19 without PPE due to delayed diagnosis of COVID-19 |
RT-PCR | Not reported | No | Not specified | Contact and droplet precautions (including eye protection)
were instituted |
| Baettig 2020 | Switzerland | Retrospective case series
Military canton March 2020 |
Local | 1 index case; 55 contacts | RT-PCR Serology | PCR: Within 24 hrs of index case
for symptomatic subjects Serology: 14 days post-exposure |
No | Not reported | Positive cases were defined with two positive PCR testing for
SARS-CoV-2 from nasopharyngeal swabs. |
| Bao 2020 | China | Observational Entertainment
venue January and February 2020 |
Community | Potentially exposed workers, customers
and their family members potentially exposed to COVID‐19 subject at a swimming pool |
RT-PCR | Not reported | No | Not specified | Men and women exhibited different usage behaviour in that
male bathers occupied the entire area, but mainly stayed at the lounge hall, while female bathers always went home after a bath. The temperature and humidity were significantly higher than what they would have been in an open air‐conditioning environment. |
| Basso 2020 | Norway | Observational study
Hospital |
Nosocomial | Quarantined HCWs exposed to COVID-19
patient |
PCR
Serology |
Approximately 2 weeks after viral
exposure; 3 weeks for serology |
No | N/A
S/CO ratio ≥1 is positive for antibody |
The HCWs were quarantined for 2 weeks due to participation
in aerosol-generating procedures (AGPs) with insufficient personal protective equipment (PPE), or close contact viral exposure (defined as ≤2 m for ≥15 min). |
| Bays 2020 | USA | Observational study
Community hospital and university medical centre February and March, 2020 |
Nosocomial | Two index patients and 421 exposed HCWs | RT-PCR | Not reported | No | Not specified | Exposed staff were identified by analyzing the EMR and
conducting active case finding in combination with structured interviews. They wore neither surgical masks nor eye protection, and were risk stratified based on examination of the medical record and subsequent phone interviews as follows: high risk: nose or mouth exposed during intubation or bronchoscopy; moderate: nose or mouth exposed and for over 2 minutes; and low: nose or mouth exposed under 2 minutes. Ct was 25 for 1 index case - day 15 |
| Bi 2020 | China | Retrospective cohort
Home or quarantine facility January-February 2020 |
Local
Household Community |
391 SARS-CoV-2 cases and 1286 close
contacts |
RT-PCR | RT-PCR | No | Not reporred | Close contacts were identified through contact tracing of
a confirmed case and were defined as those who lived in the same apartment, shared a meal, travelled, or socially interacted with an index case 2 days before symptom onset. Casual contacts (eg, other clinic patients) and some close contacts (eg, nurses) who wore a mask during exposure were not included in this group. |
| Blaisdell 2020 | USA | Observational study
4 overnight camps June–August 2020 |
Community | Multilayered prevention and mitigation
strategy 642 children and 380 staff members, aged 7–70 years |
RT-PCR | 4.1 to 9.1 days after camp arrival | No | Not specified | Hygiene measures: Precamp quarantine, pre- and postarrival
testing and symptom screening, cohorting, and physical distancing between cohorts. In addition, camps required use of face coverings, enhanced hygiene measures, enhanced cleaning and disinfecting, maximal outdoor programming, and early and rapid identification of infection and isolation. |
| Böhmer 2020 | Germany | Observational
Workplace, home January-February 2020 |
Local
Household |
1 index case; 241 contacts | RT-PCR WGS | 3–5 days post-exposure | No | Not reported | |
| Boscolo-Rizzo 2020 | Italy | Cross-sectional
Homes March to April 2020 |
Household | 179 primary cases; 296 household contacts | RT-PCR | Unclear | No | Not reported | |
| Brown 2020 | USA | Survey - cross-sectional
Classroom February to March, 2020 |
Local | Students exposed to an index case
(teacher) |
Serology | 2 weeks post-exposre to index
case |
No | Reciprocal titers of
>400 considered positive Reciprocal titers of >100 but <400 considered indeterminate |
|
| Burke 2020 | USA | Observational prospective
Homes February to March 2020 |
Household | 10 primary cases; 445 close contacts | Not reported | Within 2 weeks of exposure to
infected case |
No | Not reported | 19 (4%) of the 445 contacts were members of a patient’s
household, and five of these 19 contacts continued to have household exposure to the patient with confirmed COVID- 19 during the patient’s isolation period; 104 (23%) were community members who spent at least 10 minutes within 6 feet of a patient with confirmed disease; 100 (22%) were community members who were exposed** to a patient in a health care setting; and 222 (50%) were health care personnel |
| Canova 2020 | Switzerland | Observational case series
Primary care setting |
Nosocomial | 1 index case; 21 HCWs who interacted with
index case without PPE |
RT-PCR | 7 days after the initial exposure | No | Not reporred | |
| Cariani 2020 | Italy | Retrospective
Hospital March to April 2020 |
Nosocomial | HCWs in close contact with SARS-CoV-2-
positive cases (patients, co-workers, or relatives), or with symptoms of RTI |
RT-PCR | Not reported | No | <40 considered
positive |
|
| Charlotte 2020 | France | Retrospective
Indoor choir rehearsal March 2020 |
Community | Nonventilated room; sitting less close to
one another than usual, but at a distance of <1.82m |
RT-PCR | Not reported | No | Not reported | |
| Chaw 2020 | Brunei | Observational
Various March 2020 |
Local
Community |
Primary cases: Presumably infected at
religious event in Malaysia Secondary cases: Epidemiologic link to a primary case |
RT-PCR | Not reported | No | Not reported | Household, workplace, social, and a local religious gathering.
Initial cluster of SARS-CoV-2 cases arose from 19 persons who had attended the Tablighi Jama’at gathering in Malaysia, resulting in 52 locally transmitted cases. |
| Chen 2020 | China | Aircraft
24 January 2020 |
Aircraft | Close contact to 2 passengers presenting
with a fever and URTI symptoms |
RT-PCR | Not reported | No | Not reported | The aircraft was equipped with air handling systems. |
| Chen 2020a | China | Retrospective observational
Home or workplace January-March 2020 |
Local
Household |
69 recurrent-positive patients; 209 close
contacts |
RT-PCR | Every 3 days | No | Not specified | |
| Chen 2020b | China | Prospective cohort
Hospital January-February 2020 |
Nosocomial | 5 index patients; 105 HCWs | RT-PCR
Serology |
From 14 days post-exposure: 1st
& 14th day of quarantine |
No | <40 considered
positive |
|
| Chen 2020c | China | Observational
Various January to March 2020 |
Local
Household Community Nosocomial |
157 locally reported confirmed cases,
30 asymptomatic infections; 2147 close contacts |
Not reported | Unclear | No | Not reported | Family members, relatives, friends/pilgrims, colleagues/
classmates, medical staff, and general personnel judged by the investigator. |
| Cheng 2020 | Taiwan | Observational
Homes, hospital January to March 2020 |
Household
Nosocomial |
100 confirmed cases of confirmed; 2761
close contacts |
RT-PCR | Unclear | No | Not reported | |
| Chu 2020 | USA | Observational
Various January 2020 |
Community | Close contacts for an early confirmed case
of COVID-19 |
RT-PCR
Serology |
Unclear | No | Antibody titers
>400 considered seropositive. |
Office, Community, Urgent care clinic identified via contact
tracing |
| Chu 2020a | USA | Retrospective cohort study
Household |
Household | Household contacts of primary cases
defined as children and adolescents with lab-confirmed COVID-19 (n=224) |
Not reported | Not reported | No | Not reported | Did not distinguish between confirmed and probable cases
among household contacts. A “primary case” is camp attendee with the earliest onset date in the household and a “secondary case” as a household contact with confirmed or probable COVID-19. |
| Contejean 2020 | France | Observational Comparative
Tertiary-care university hospital Feb-Mar 2020 |
Nosocomial | HCW exposed to COVID-19 patients | RT-PCR | Not reported | No | Not reported:
result was +ve if 3/5 of gene targets amplified |
Hygiene measures: All employees were encouraged to wear
a face mask as often as possible in hospital (particularly in the presence of other persons), to wash/disinfect their hands regularly (and after every contact with other persons), to stay at least 2 meters away from others, to cover their mouth and nose with a tissue or sleeve when coughing or sneezing, to put used tissues in the bin immediately and wash hands afterwards, to avoid touching eyes, mouth. Educational messages were released on the internal website and on posters placed in all hospital premises. |
| COVID-19 National Emergency Response Center 2020 | S. Korea | Observational
Various January to March 2020 |
Local
Household Nosocomial |
30 cases; 2,370 contacts | RT-PCR | Not reported | No | Not reported | Homes, work, hospitals |
| Danis 2020 | France | Observational case series
Chalet, school January to February 2020 |
Local
Household |
I adult case with 15 contacts in chalet; 1
paediatric case with 172 school contacts |
RT-PCR | Within 5 days of diagnosis of
cases |
No | Not reported | The index case stayed 4 days in the chalet with 10 English
tourists and a family of 5 French residents. One pediatric case, with picornavirus and influenza A coinfection, visited 3 different schools while symptomatic. |
| Dattner 2020 | Israel | Observational
Home March to June 2020 |
Household | 637 households, average household size of
5.3 |
RT-PCR
Serology |
Serology: 4 weeks post PCR
testing |
No | Not reported | |
| de Brito 2020 | Brazil | Observational descriptive
Household April-May 2020 |
Household | Socially distanced household contacts of
index case |
RT-PCR
Serology |
Serology: 4 weeks post-exposure
PCR unclear |
No | Not reported | Index case: First member of the cluster who had symptoms
and who had a known risk of exposure outside the household during the family's stay in the same condominium; secondary case: Contacts with the index case. Asymptomatic patients: Those who had household contact and positive serology but no symptoms. Probable cases corresponded to confirmed case contacts who developed symptoms compatible with COVID despite negative serology and/or negative RT-PCR results. |
| Deng 2020 | China | Observational
Home January to February 2020 |
Household | 27 cases; 347 close contacts | Not reported | Not reported | No | Not reported | |
| Desmet 2020 | Belgium | Observational - cross-sectional
School November 2019 to March 2020 |
Local | 84 aged between 6 and 30 months
attending daycare |
RT-PCR | First weeks of the epidemic in
Belgium |
No | Not reported | |
| Dimcheff 2020 | USA | Survey: cross-sectional
Tertiary-care referral facility June 8 to July 8, 2020 |
Community
Nosocomial Household |
HCW exposed to COVID-19 patients either
in or outside hospital |
Serology | 8 weeks post-exposure | No | Not reported | Hygiene measures: Daily COVID-19 symptom screening
upon building entry, exclusion of visitors from the facility, and institution of telework in remote offices or at home, isolation of confirmed COVID-19 patients, conversion of COVID-19 wards to negative pressure environments, use of PAPRs) or N95 respirators along with PPE by staff. |
| Dong 2020 | China | Observational
Homes |
Household | 135 cases; 259 close contacts | Not reported | Not reported | No | Not reported | |
| Doung-ngern 2020 | Thailand | Retrospective case-control
Various March to April 2020 |
Local | 3 large clusters in nightclubs, boxing
stadiums, and a state enterprise office |
RT-PCR | Not reported | No | Not reported | Hygiene measures: Consistent wearing of masks,
handwashing, and social distancing in public. |
| Draper 2020 | Australia | Observational Various
March to April 2020 |
Local
Household Nosocomial |
28 cases; 445 close contacts | RT-PCR | Within 2 weeks of exposure to
infected case |
No | Not reported | Cruise ship, homes, aircraft, hospital |
| Dub 2020 | Finland | Retrospective cohort (2)
School and Household |
Local
Household |
School and household contacts of 2 index
cases who contracted COVID-19 at school |
RT-PCR
Serology |
Serology: >4 weeks post-exposure | No | MNT titre of ≥ 6
considered positive FMIA titre 3·4 U/ml considered positive |
|
| Expert Taskforce 2020 | Japan | Observational prospective
Cruise ship February 2020 |
Local | 3,711 persons in cruise ship | RT-PCR | Not reported | No | Not reported | Passengers were allowed a 60-minute period on an exterior
deck each day, during which they were instructed to wear masks, refrain from touching anything, and maintain a 1-meter distance from others. Monitors observed these periods. After each group came a 30-minute period in which the areas were disinfected. Room cleaning was suspended. Food and clean linens were delivered to cabin doors by crew, and dirty dishes and linens were picked up at cabin doors by crew. Only symptomatic close contacts were tested initially. |
| Fateh-Moghadam 2020 | Italy | Observational Various
March to April 2020 |
Community | 2,812 cases; 6,690 community contacts | Not reported | Not reported | No | Not reported | Institutional settings including nursing homes, hospitals, day
and residential centers for the disabled and similar structures, and convents |
| Firestone 2020 | USA | Observational retrospective
Motorcycle rally August-September 2020 |
Local | 51 primary event-associated cases, and 35
secondary or tertiary cases |
RT-PCR
WGS Phylogenetic analysis |
Unclear | No | Not reported |
Secondary cases: Laboratory-confirmed infections in persons
who did not attend the rally but who received SARS-CoV- 2–positive test results after having contact with a person who had a primary case during their infectious period. Tertiary cases were laboratory-confirmed cases in persons who had contact with a person who had a secondary case during their infectious period. SARS-CoV-2 RNA-positive clinical specimens were obtained from clinical laboratories, and |
| Fontanet 2020 | France | Retrospective cohort study
School March to April 2020 |
Local | 661 participants: pupils, their parents
and siblings, as well as teachers and non- teaching staff of a high-school |
Serology | 10 weeks | No | N/A | |
| Fontanet 2020a | France | Retrospective cohort study
Schools April 2020 |
Local | 510 participants: pupils, their parents
and siblings, as well as teachers and non- teaching staff of a high-school |
Serology | 10 weeks | No | N/A | 6 primary schools |
| Gan 2020 | China | Observational retrospective
survey Various January-February 2020 |
Local
Household Community |
1 052 cases in 366 epidemic clusters | Not reported | Not reported | No | Not reported | Family living together, gathering dinner, collective work, ride-
thy-car, other aggregation exposure, |
| Ghinai 2020 | USA | Observational
2 Social gatherings January-March 2020 |
Community | 16 cases (7 confirmed and 9 probable) (1
index case) |
RT-PCR | Not reported | No | Not reported | A birthday party, funeral, and church attendance. |
| Gong 2020 | China | Observational
Various January-February 2020 |
Household
Community |
3 clusters: 5 index cases; 9 close contacts | RT-PCR | Not reported | No | Not reported | Travelling and dining, or were living together |
| Gong 2020 | China | Observational
Karaoke room January 2020 |
Local | 14 people exposed to 2 index cases in a karaoke room | RT-PCR
Serology |
PCR: Within 72 hrs post-exposure
Serology: 6 weeks post-exposure |
No | Not reported | |
| Hamner 2020 | USA | Observational
Choir practice March 2020 |
Local | 1 index case; 60 close contacts | RT-PCR | Within 2 weeks of index case | No | Not reported | |
| Han 2020 | S. Korea | Observational
Spa facility Mar-April 2020 |
Community | Contacts for 10 index cases from Spa
facility |
RT-PCR | Not reported | No | Not reported | |
| Heavey 2020 | Ireland | Observational
School March 2020 |
Local | 6 index cases; 1155 contacts | Not reported | Not reported | No | No | Three paediatric cases and three adult cases of COVID-19 with
a history of school attendance were identified. Exposed at school in the classroom, during sports lessons, music lessons and during choir practice for a religious ceremony, which involved a number of schools mixing in a church environment. |
| Helsingen 2020 | Norway | RCT
Training facilities May-June 2020 |
Local | Members of the participating training
facilities age 18 years or older who were not at increased risk for severe Covid-19 |
RT-PCR
Serology |
Serology: 4 weeks after start
of study |
No | Not reported | Hygiene measures: Avoidance of body contact; 1 metre
distance between individuals at all times; 2 metre distance for high intensity activities; provision of disinfectants at all work stations; cleaning requirements of all equipment after use by participant; regular cleaning of facilities and access control by facility employees to ensure distance measures and avoid overcrowding. Changing rooms were open, but showers and saunas remained closed. All participants were mailed a home-test kit including two swabs and a tube with virus transport medium for SARS-CoV-2 RNA |
| Hendrix 2020 | USA | Observational
Hair salon May 2020 |
Local | Contacts for 2 stylists who tested positive
for COVID-19 |
PCR | Not reported | No | Not reported | Hygiene measures: During all interactions with clients at
salon A, stylist A wore a double-layered cotton face covering, and stylist B wore a double-layered cotton face covering or a surgical mask. |
| Hirschman 2020 | USA | Observational study
Home and social gatherings June 2020 |
Household
Community |
2 index cases; 58 primary and secondary
contacts |
RT-PCR | Unclear | No | Not reported | |
| Hobbs 2020 | USA | Case-control study
University Medical Centre September-November 2020 |
Local
Household Community |
397 children and adolescents: Cases 154;
controls 243 |
RT-PCR | Not reported | No | Not reported | |
| Hoehl 2020 | Germany | Observational
Daycare Centre 12 weeks (June-Sept 2020) |
Local
Community |
Attendees and staff from 50 daycare
centres |
RT-PCR | Not reported | No | Not reported | Hygiene measures: Barring children and staff with symptoms
of COVID-19, other than runny nose, from entering the facilities, as well as denying access to individuals with known exposure to SARS-CoV-2. Access to the facilities was also denied to children if a household member was symptomatic, or was in quarantine due to contact with SARS-CoV-2. Wearing of masks was not mandatory for children or nor staff. The access of caregivers to the facilities was limited. |
| Hong 2020 | China | Observational prospective
Home January-April 2020 |
Household | 9 patients with recurrent infection; 13
close contacts |
RT-PCR
Serology NGS |
After re-admission of index
patients. |
No | Not reported | |
| Hu 2020 | China | Observational retrospective
Various January to April 2020 |
Household
Community |
1178 cases; 15,648 contacts | Not reported | Not reported | No | Not reported | Homes, social events, travel, other settings |
| Hua 2020 | China | Observational retrospective
Home January to April 2020 |
Household | Children and adult contacts from the 314
families |
RT-PCR | Not reported | No | Not reported | |
| Huang 2020 | China | Prospective contact-tracing study
Restaurant, home January 2020 |
Household
Community |
1 indes case; 22 close contacts | RT-PCR | Within 3 days of index cases | No | Not reported | Close contacts quarantined at home or hospital |
| Huang 2020a | Taiwan | Retrospective case series
Various January-April 2020 |
Local
Household Community Nosocomial |
15 primary cases: 3795 close contacts | RT-PCR | Not reported | No | Not reported | Aircraft, home, classroom, workplace, hospital |
| Islam 2020 | Bangladesh | Observational
Various March to June 2020 |
Local
Household Community Nosocomial |
181 cases; 391 close contacts | Not reported | Not reported | No | Not reported | Household, health care facility, funeral ceremony, public
transportation, family members, and others |
| Jia 2020 | China | Observational
Home January to February 2020 |
Household | 11 clusters (n=583) | RT-PCR | Not reported | No | <37 considered
positive |
A
close contact was defined as a person who did not take
effective protection against a suspected or confirmed case 2 d before the onset of symptoms or an asymptomatic infected person 2 d before sampling. Ct-value of 40 or more was defined as negative. |
| Jiang 2020 | China | Observational
Home January to February 2020 |
Household
Community |
8 index cases, 300 contacts | rRT-PCR
WGS Phylogenetic analysis |
Every 24 hours for 2 weeks | No | <37 considered
positive |
Ct value ≥40 was considered negative. The maximum
likelihood phylogenetic tree of the complete genomes was conducted by using RAxML software with 1000 bootstrap replicates, employing the general time-reversible nucleotide substitution mode |
| Jing 2020 | China | Retrospective cohort study
Homes January-February 2020 |
Household | 195 unrelated close contact groups (215
primary cases, 134 secondary or tertiary cases, and 1964 uninfected close contacts) |
RT-PCR | Days 1 and 14 of quarantine | No | Not reported | |
| Jing 2020a | China | Observational study
Homes, public places February 2020 |
Household
Community |
68 clusters involving 217 cases | RT-PCR | Not reported | No | Not reported | |
| Jones 2020 | UK
France |
Observational
Super League Rugby August to October 2020 |
Local | 136: 8 index cases: 28 identified close
contacts and 100 other players |
RT-PCR | Within 14 days of match day | No | Not specified: Ct for index cases 17.8 to 27 |
Close contacts were defined by analysis of video footage
for player interactions and microtechnology (GPS) data for proximity analysis. All participants were within a ≤7-day RT-PCR screening cycle |
| Kang 2020 | S. Korea | Observational
Night clubs April-May 2020 |
Local | 96 primary cases and 150 secondary cases;
5,517 visitors |
Not reported | Not reported | No | Not reported | |
| Kant 2020 | India | Retrospective (contact tracing)
Regional Medical Research Centre May 2020 |
Local
Community Nosocomial |
1 index case diagnosed post-mortem;
number of exposures unclear |
RT-PCR | Unclear | No | Not reported | Contacts traced: People from the market where the index case
had his shop, his treating physicians, people who attended his funeral, family members and friends |
| Kawasuji 2020 | Japan | Case-control study
University Hospital April-May 2020 |
Nosocomial | 28 index cases: 105 close contacts | RT-PCR | Unclear | No | Not reported | Index patients and those with secondary transmission were
estimated based on serial intervals in the family clusters. |
| Khanh 2020 | Vietnam | Retrospective
Aircraft March 2020 |
Community | 1 index case: 217 close contacts | PCR | 4 days after positive test result of
index case |
No | Not reported | Successfully traced passengers and crew members were
interviewed by use of a standard questionnaire, tested for SARS-CoV-2 |
| Kim 2020 | S. Korea | Retrospective observational
Home setting January-April 2020 |
Household | 107 paediatric index cases: 248 household
members of which 207 were exposed |
RT-PCR | Within 2 days of COVID-19
diagnosis of the index case |
No | Ct value of ≤35 is
positive and >40 is negative |
Guardian wore a KF94 (N95 equivalent) mask, gloves, full body
suit (or waterproof long-sleeve gowns) and goggles. |
| Kim 2020a | S. Korea | Case series
Various January-February 2020 |
Household
Community |
1 index case; 4 close contacts | RT-PCR | 4 days post-exposure | No | N/A | 2 household contacts, 1 church contact, 1 restaurant |
| Kim 2020b | S. Korea | Retrospective observational
University hospital February 2020 |
Nosocomial | 4 confirmed cases: 290 contacts | RT-PCR | Within 8 days of index case
diagnosis |
No | Ct <35 was considered positive | Medical staff in the triage room used level-D PPE and everyone
in the hospital was encouraged to wear masks and follow hand hygiene practices. Contact with confirmed COVID-19 cases was frequent among inpatients and medical support personnel. |
| Kumar 2020 | India | Observational
Community March-May 2020 |
Community | 144 source cases: | RT-PCR | Unclear | No | Not reported | Persons with symptoms of ILI and SARI as well as known high-
risk contacts of a confirmed COVID-19 patient were included. |
| Kuwelker 2020 | Norway | Prospective case-ascertained
study Homes Feb-April 2020 |
Household | 112 index cases; 179 household members | Serology | 6–8 weeks after symptom onset
in the index case. |
No | N/A | Single-person households were excluded from the analysis.
Serum samples from index cases and household members were collected 6–8 weeks after symptom onset in the index case. |
| Kwok 2020 | Hong Kong | Retrospective observational
Quarantine or isolation February 2020 |
Local
Household |
53 cases; 206 close contacts | Not reported | Not reported | No | Not reported | A
secondary case referred to the first generation of infection
induced by an index case following contact with this case |
| Ladhani 2020 | UK | Prospective
Care homes April 2020 |
Nosocomial | 6 London care homes reporting a
suspected outbreak (2 or more cases); 254 staff members |
RT-PCR | Not reported | No | Not reported | 254 of 474 (54%) staff members provided a nasal self-swab; 12
were symptomatic at the time of swabbing |
| Ladhani 2020a | UK | Prospective
Care homes April 2020 |
Nosocomial | 6 London care homes reporting a
suspected outbreak (2 or more cases); 254 staff members; 264 residents |
RT-PCR | Not reported | Yes | Unclear: Ct values <35 were cultured | 254 of 474 (54%) staff members provided a nasal self-swab; 12
were symptomatic at the time of swabbing |
| Laws 2020 | USA | Prospective cohort
Home setting March-May 2020 |
Household | 1 pediatric index case: 188
household contacts |
RT-PCR | Study enrollment (day 0); study
close-out (day 14) |
No | Not reported | Index case: household member with earliest symptom onset
(and positive SARS-CoV-2 RT-PCR test result). Community prevalence in the 2 metropolitan areas was low during this time, and both were under stay-at-home orders. All enrolled index case patients and household contacts were followed prospectively for 14 days. Five households were selected for intensive swabbing requiring collection of respiratory specimens from all household members during four interim visits regardless of symptom presence. |
| Laxminarayan 2020 | India | Observational
Various April to August 2020 |
Local
Household Community |
3,084,885 known exposed contacts | Not reported | Not reported | No | Not reported | Individual-level epidemiological data on cases and contacts,
as well as laboratory test results, were available from 575,071 tested contacts of 84,965 confirmed cases. |
| Lee 2020 | S. Korea | Observational
Hospital February-June 2020 |
Household | 12 paediatric cases; 12 guardians as close
contact. All guardians used PPE |
Not reported | Not reported | No | Not reported | |
| Lee 2020a | S. Korea | Observational
Homes February to March 2020 |
Household | 23 close contacts | PCR | Unclear | No | Not reported | |
| Lewis 2020 | USA | Observational
Homes March to April 2020 |
Household | 58 households (Utah, n = 34; Wisconsin
n = 24), 58 primary patients and 188 household contacts |
RT-PCR
Serology |
Not reported | No | Not reported | |
| Li 2020 | China | Observational
Home setting Feb 2020 |
Household | Family cluster of 1 index case: 5 household
contacts |
RT-PCR | One day after index case tested
positive |
No | Not reported | Unknown when index case started shedding virus |
| Li 2020a | China | Observational case series
Home, hospital January-February 2020 |
Household
Nosocomial |
2-family cluster of 1 index case: 7 close
contacts |
Not reported | Not reported | No | Not reported | |
| Li 2020b | China | Retrospective observational
Home January-February 2020 |
Household | 3-family cluster of 3 index cases: 14 close
contacts |
RT-PCR | Every 2–3 days until hospital
discharge. |
No | <38 considered
positive |
|
| Li 2020c | China | Retrospective observational
Home January-March 2020 |
Household | 30 cases from 35 cluster-onset families
(COFs) and 41 cases from 16 solitary-onset families (SOFs) |
Not reported | Not reported | No | Not reported | |
| Li 2020d | China | Observational
Household February to March 2020 |
Household | 105 index patients; 392 household
contacts |
RT-PCR | Within 2 weeks of exposure to
infected case |
No | Not reported | |
| Liu 2020 | China | Retrospective observational
Home setting Feb 2020 |
Household | Family cluster of 1 index case: 7 household
contacts |
RT-PCR | Immediately after index case
tested positive |
No | If both the
nCovORF1ab and nCoV-NP showed positive results, COVID-19 infection was considered |
Unclear whether the index case was actually first case |
| Liu 2020a | China | Retrospective case series
Hospital January 2020 |
Nosocomial | 30 HCWs with direct contact with patients | RT-PCR | Not reported | No | <40 considered
positive |
30 cases have a history of direct contact with patients with
neo-coronary pneumonia (within 1 m), 1 to 28 contacts, an average of 12 (7,16) contact times, contact time of 0.5 to 3.5 h, the average cumulative contact time of 2 (1.5, 2.7)h. |
| Liu 2020b | China | Retrospective cohort study
Various January-March 2020 |
Household
Community Nosocomial |
1158 index cases: 11,580 contacts | RT-PCR | Every several days | No | Not reported | Homes, social venues, various types of transportations |
| Liu 2020c | China | Prospective observational | Unclear | 147 asymptomatic carriers: 1150 close
contacts |
RT-PCR | Not reported | No | Not reported | RT-PCR for asymptomatic carriers - testing method not
described for close contacts |
| López 2020 | USA | Retrospective contact tracing
School setting April-July 2020 |
Local
Household |
12 index pediatric cases: 101 facility
contacts; 184 overall contacts |
RT-PCR | Not reported | No | Not reported | Index case: first confirmed case identified in a person at the
child care facility Primary case: Earliest confirmed case linked to the outbreak. Overall attack rates include facility-associated cases, nonfacility contact cases iand all facility staff members and attendees and nonfacility contacts |
| Lopez Bernal 2020 | UK | Observational
Homes January to March 2020 |
Household
Community |
233 households with two or more people;
472 contacts. |
PCR | Unclear | No | Not reported | Healthcare workers, returning travellers and airplane
exposures were excluded. |
| Lucey 2020 | Ireland | Observational
Hospital March-May 2020 |
Nosocomial | 5 HCWs in cluster 1; 2 HCWs in cluster 3;
HCW in cluster 2 not specified; 52 patients infected with SARS-CoV-2; |
RT-PCR
WGS Phylogenetic analysis |
Not reported | No | Not reported | SARS-CoV-2 RNA was extracted from nasopharyngeal swabs
obtained from COVID-19 cases and their corresponding HCWs were sequenced to completion. HA COVID-19 was classified into two groups according to the length of admission: >7 days and >14 days. The majority of patients required assistance with mobility (65%) and selfcare (77%) |
| Luo 2020 | China | Observational retrospective
Public transport January 2020 |
Community | 1 index case; 243 close contacts | RT-PCR | Within 2 weeks of exposure to
index case |
No | Not reported | The tour coach was with 49 seats was fully occupied with all
windows closed and the ventilation system on during the 2.5-hour trip. |
| Luo 2020a | China | Prospective cohort study
Various January to March 2020 |
Household
Community Nosocomial |
391 index cases; 3410 close contacts | RT-PCR
Serology |
Every 24 hours. | No | Not reported | Homes, public transport; healthcare settings, entertainment
venues, workplace, multiple settings |
| Lyngse 2020 | Denmark | Retrospective
Homes February to July 2020 |
Household | 990 primary cases; 2226 household
contacts |
Not reported | Within 14 days of exposure to
primary case |
No | Not reported | Secondary cases: those who had a positive test within 14
days of the primary case being tested positive. 3 phases of epidemic examined. Assumed that the secondary household members were infected by the household primary case, although some of these secondary cases could represent co-primary cases. A longer cutoff time period could result in misclassification of cases among household members with somewhere else being the source of secondary infections. |
| Ma 2020 | China | Observational
Medical isolation |
Unclear | 1665 close contacts | RT-PCR | Not reported | No | Not reported | |
| Macartney 2020 | Australia | Prospective cohort study
Educational settings April to May 2020 |
Local | 27 primary cases; 633 contacts | RT-PCR, serology, or both | PCR: 5–10 days after last case
contact if not previously collected Serology: day 21 following last case contact. |
No | Not reported |
Index case: The first identified laboratory-confirmed case
who attended the facility while infectious. A school or ECEC setting primary case was defined as the initial infectious case or cases in that setting, and might or might not have been the index case. Primary case: Initial infectious case or cases in that setting, and might or might not have been the index case Secondary case: Close contact with SARS-CoV-2 infection (detected through nucleic acid testing or serological testing, or both), which was considered likely to have occurred via transmission in that educational setting. |
| Malheiro 2020 | Portugal | Retrospective cohort study
Homes March to April 2020 |
Household | Intervention group (n=98), Control (n=453) | Not reported | Not reported | No | Not reported | The intervention group comprised all COVID-19 confirmed
cases that were either identified as close contacts of an index caseor returned from affected areas and placed under mandatory quarantine, with daily follow-up until laboratory confirmation of SARS-CoV-2 infection. The control group included all COVID-19 confirmed cases that were not subject to contact tracing nor to quarantine measures preceding the diagnosis. |
| Maltezou 2020 | Greece | Retrospective observational
Home setting February to June 2020 |
Household | 203 SARS-CoV-2-infected children; number
of index cases and close contacts unclear |
RT-PCR | Not reported | No | Ct >38 considered
negative |
A
family cluster was defined as the detection of at least 2
cases of SARS-CoV-2 infection within a family. First case was defined as the first COVID-19 case in a family. High, moderate, or low viral load (Ct <25, 25–30 or >30, respectively) |
| Maltezou 2020a | Greece | Retrospective observational
Home setting February to May 2020 |
Household | 23 family clusters of COVID-19; 109
household members |
RT-PCR | Not reported | No | <25, 25–30 or >30 | A
family cluster was defined as the detection of at least 2
cases of SARS-CoV-2 infection within a family. Index case was defined as the first laboratory-diagnosed case in the family. |
| Mao 2020 | China | Cross-sectional study
Home, family gatherings January-March 2020 |
Household
Local |
67 clusters with 226 cases confirmed cases | RT-PCR | Not reported | No | Not reported | |
| Martinez-Fierro 2020 | Mexico | Cross-sectional
June-July 2020 |
Unclear | 19 asymptomatic index cases; 81 contacts | RT-PCR
Serology |
Not reported | No | Not reported | |
| Mponponsuo 2020 | Canada | Observational
Hospital March-April 2020 |
Nosocomial | 5 HCWs were index cases; 39 HCWs (16
underwent testing) and 33 patients were exposed (22 underwent testing) |
RT-PCR | Not reported | No | Not reported | All 5 HCWs had E gene cycle threshold (Ct) values between
10.9 and 30.2. Those exposed to the index HCWs were followed for 30 days |
| Ng 2020 | Singapore | Retrospective cohort study
Various January-April 2020 |
Household
Local Community |
1114 PCR-confirmed COVID-19 index cases
in the community in Singapore. 13 026 close contacts (1863 household, 2319 work, and 3588 social) |
RT-PCR
Serology |
If contacts reported symptoms | No | Not reported |
Lower risk contacts: Other contacts who were with the index
case for 10–30 min within 2 m Contacts who reported symptoms were admitted to the hospital for COVID-19 testing by PCR. |
| Ning 2020 | China | Observational study
Various January-February 2020 |
Household
Local Community |
Local cases: 3,435 close contacts
Imported cases: 3,666 close contacts |
Not reported | Not reported | No | Not reported | Imported cases, farmers' markets, malls and wildlife exposure |
| Njuguna 2020 | USA | Observational
Prison May 2020 |
Local | 98 incarcerated and detained persons | RT-PCR | Not reported | No | Not reported | Unclear how many index or close contacts |
| Ogawa 2020 | Japan | Observational
Hospital |
Nosocomial | 1 index patient; 15 HCWs were contact | RT-PCR
Serology |
RT-PCR: 10th day after exposure
Serology: Before isolation |
No | Not specified | Viral culture performed for only the index patient |
| Paireau 2020 | France | Retrospective observational
Various January to March 2020 |
Household
Local Nosocomial |
735 index cases; 6,082 contacts | RT-PCR | Not reported | No | Not reported | Family, home, work, hospital.
Index case: A case whose detection initiated an investigation of its contacts through contact tracing Only contacts who developed symptoms compatible with COVID-19 were tested for SARS-CoV-2 |
| Park 2020 | S. Korea | Retrospective observational
Various February 2020 |
Local
Household Community |
2 index cases; 328 contacts | RT-PCR | 24 hrs for 37 first contacts;
others within 2 weeks |
No | <40 considered
positive |
Aircraft, home, restaurant, clinic, pharmacy.
Contact tracing of COVID-19 cases was conducted from 1 day before symptom onset or 1 day before the case was sampled. |
| Park 2020a | S. Korea | Observational study
Homes January to March 2020 |
Household
Non-household |
5,706 COVID-19 index patients; 59,073
contacts |
Not reported | Not reported | No | Not reported | |
| Park 2020b | S. Korea | Observational study
Workplace, home March 2020 |
Local
Household |
216 employees, 225 household contacts | RT-PCR | Within 2 weeks of report of
infected case |
No | Not reported | Employees do not generally go between floors, and they do
not have an in-house restaurant for meals. Sent a total of 16,628 text messages to persons who stayed >5 minutes near the building X; we tracked these persons by using cell phone location data. |
| Passarelli 2020 | Brazil | Observational
Hospital August 2020 |
Nosocomial | 6 index cases; 6 close contacts | RT-PCR | Not reported | No | <40 considered
positive |
All index cases were asymptomatic hospital visitors |
| Patel 2020 | UK | Retrospective observational
Hospital, community March to April 2020 |
Household | 107 cases; 195 household contacts | RT-PCR | Not tested | No | Not reported | |
| Pavli 2020 | Greece | Observational contact tracing
Aircraft February to March 2020 |
Aircraft | 6 index cases; 891 contacts | RT-PCR | Not reported | No | Not reported | A COVID-19 case was defined at that time as a case with
signs and symptoms compatible with COVID-19 in a patient with laboratory-confirmed SARS-CoV-2 infection, recent travel history to a country with evidence of local transmission of SARS-CoV-2 or close contact with a laboratory-confirmed case |
| Phiriyasart 2020 | Thailand | Observational
Homes April 2020 |
Household | 471 household contacts | RT-PCR | Within 5 days of exposure | No | Not reported | |
| Poletti 2020 | Italy | Observational
February-April 2020 |
Unclear | 5,484 close contacts from clusters | RT-PCR
Serology |
Not reported | No | Not reported | Only contacts belonging to clusters (i.e. groups of contacts
identified by one positive index case) were included. 1,364 (25%) were tested with only RT-PCR, 3,493 (64%) with only serology at least a month after the reporting date of their index case and 627 (11%) were tested both by RT-PCR and serology. |
| Pung 2020 | Singapore | Observational
Various February 2020 |
Local
Community |
425 close contacts from 3 clusters; index
case unclear |
PCR
WGS Phylogenetic analysis |
Not reported | No | Not reported | Company conference, church, tour group.
Close contacts under quarantine for 14 days from last exposure to the individual with confirmed COVID-19, either at home or at designated government quarantine facilities. |
| Pung 2020a | Singapore | Observational
Homes Up till March 2020 |
Household | 277 were primary or co‐primary cases: 875
household contacts |
Not reported | Not reported | No | Not reported | Household contacts were tested if they showed symptoms of
SARS-CoV-2 infection, or if aged 12 years or below |
| Qian 2020 | Hong Kong | Observational retrospective
Various January to February 2020 |
Local
Household Community |
Unclear | Not reported | Not reported | No | Not reported | Homes, transport, restaurants, shopping and entertainment
venues. Four categories of infected individuals were considered based on their relationship: family members, family relatives, socially connected individuals, and socially non‐connected individuals |
| Ravindran 2020 | Indonesia | Retrospective cohort
Wedding March 2020 |
Local | 41 guests; no. of index cases unclear | RT-PCR | Not reported | No | Not reported |
Primary case: Any person who attended the wedding events
in Bali Indonesia during 15–21 March 2020 and who tested positive. Secondary case: any person who tested positive on SARS- CoV-2 after the 14 day period and who was a close contact of a COVID-19 case from the wedding events. |
| Razvi 2020 | UK | Observational study
Hospital May to June 2020 |
Nosocomial | 2,521 HCWs | Serology | Voluntary first-come, first-served
basis |
No | N/A | |
| Rosenberg 2020 | USA | Observational retrospective
Homes March 2020 |
Household | 229 cases; 498 household contacts | RT-PCR | Not reported | No | Not reported | |
| Roxby 2020 | USA | Observational - cross-sectional
Nursing home March 2020 |
Nosocomial | 80 residents and 62 staff members; no
index case |
RT-PCR | Day 1 and 7 days late | No | No | Residents isolated in their rooms; no communal meals or
activities, no visitors allowed in the facility, staff member screening and exclusion of symptomatic staff members implemented. Enhanced hygiene practices were put into effect, including cleaning and disinfection of frequently touched surfaces and additional hand hygiene stations in hallways for workers to use. All residents were tested again 7 days later. |
| Sang 2020 | China | Case series
Home February 2020 |
Household | 1 index case; 6 family members | Not reported | Within 24 hrs of index case | No | Not reported | Central air conditioner was always running at home |
| Schumacher 2020 | Qatar | Prospective cohort study
Football team June to September 2020 |
Local | 1337; no index cases | RT-PCR
Serology |
RT-PCR: Every 3–5 days
Serology: Every 4 weeks |
No | ≤30 positive | Strict hygiene measures and regular testing.
Two phases, the quarantine phase (entry until exit) and the training and match phase (after quarantine exit until the first test done during the week after the last match. Ct >30 but <40 reactive. 1337 subjects were tested at least once; however, some players and staff joined their team and were gradually included in (or left) the programme during the study period. |
| Schwierzeck 2020 | Germany | Observational
Hospital paediatric dialysis unit |
Nosocomial | 1 index case; 48 contacts | RT-PCR | 24 hrs after index case | No | Not specified |
Outbreak was defined as two or more COVID-19 infections
resulting from a common exposure |
| Shah 2020 | India | Observational
Homes March to July 2020 |
Household | 74 primary cases; 386 household contacts | RT-PCR | Not reported | No | Not reported | |
| Shen 2020 | USA | Observational
Social gathering January to February 2020 |
Household
Community |
1 index case: 539 social and family contacts | RT-PCR | If contact had symptoms | No | Not specified | |
| Sikkema 2020 | Netherlands | Cross-sectional
Hospital March 2020 |
Nosocomial | 1796 HCWs; index case not specified | RT-PCR
WGS Phylogenetic analysis |
N/A | No | <32 considered
positive |
HCWs across 3 hospitals. |
| Son 2020 | S. Korea | Observational study
Homes January to March 2020 |
Household | 108 primary cases; 3223 contacts | RT-PCR | Unclear | No | Not reported | |
| Song 2020 | China | Observational case series
Home January 2020 |
Household | 4 family clusters. 4 index cases: 18 close
contacts |
RT-PCR | 0 to 72 hrs after index case
tested positive |
No | Not reported | |
| Speake 2020 | Australia | Observational retrospective
Aircraft March 2020 |
Aircraft | 241 passengers some of whom had
disembarked from 1 of 3 cruise ships that had recently docked in Sydney Harbour. 6 primary cases initially |
RT-PCR
WGS Phylogenetic analysis |
Within 2 weeks of primary cases | Yes | Not specified |
Primary cases as passengers with SARS-CoV-2 who had been
on a cruise ship with a known outbreak in the 14 days before illness onset and whose specimen yielded a virus genomic sequence closely matching that of the ship’s outbreak strain Secondary cases: Passengers with PCR-confirmed SARS- CoV-2 infection who had not been on a cruise ship with a known SARS-CoV-2 outbreak within 14 days of illness onset and in whom symptoms developed >48 hours after and within 14 days of the flight; or international passengers who had not been on a cruise ship in the 14 days before illness and whose specimens yielded a WGS lineage not known to be in circulation at their place of origin but that closely matched the lineage of a primary case on the flight. |
| Stein-Zamir 2020 | Israel | Observational - cross-sectional
Schools May 2020 |
Local | 1,190 students aged 12–18 years (grades
7–12) and 162 staff members. |
PCR | Unclear | No | Not reported | |
| Sugano 2020 | Japan | Observational retrospective
Music concerts February 2020 |
Local | 1 index case; 72 exposures | RT-PCR | Not reported | No | Not specified | |
| Sun 2020 | China | Observational
Homes |
Household | Family clusters | Not reported | Not reported | No | Not reported | |
| Taylor 2020 | USA | Observational
Skilled nursing facilities April-June 2020 |
Nosocomial | 259 tested residents, and 341 tested HCP | RT-PCR
WGS Phylogenetic analysis |
Weekly serial testing (every
7–10 days) |
No | Not specified | |
| Teherani 2020 | USA | Observational
Homes March to June 2020 |
Household | 32 paediatric cases; 144 household
contacts |
PCR | Within 2 weeks of exposure to
infected case |
No | Not reported | Only children who presented with symptoms concerning for
COVID-19 infection were included. |
| Thangaraj 2020 | India | Observational
Tourist group February 2020 |
Community | 1 index case; 26 close contacts | RT-PCR | Within 24 hrs of index case | No | Not reported | |
| Torres 2020 | Chile | Cross-sectional
Community March-May 2020 |
Community | 1009 students and 235 staff | Serology | 8–10 weeks after school
outbreak |
No | N/A | The school was closed on March 13, and the entire community
was placed in quarantine |
| Tshokey 2020 | Bhutan | Observational
Tourists May 2020 |
Local
Community |
27 index cases; 75 high-risk contacts, 1095
primary contacts; 448 secondary contacts |
RT-PCR | High-risk contacts: minimum of
three times with RT-PCR |
No | ≤ 40 considered
positive |
|
| van der Hoek 2020 | Netherlands | Observational
Household March to April 2020 |
Household | 231 cases; 709 close contacts. 54 families
have 239 participants, 185 of whom are family members. |
RT-PCR
Serology |
Not reported | No | Not reported | |
| Wang 2020 | China | Observational
Home January-February 2020 |
Nosocomial
Household |
25 HCWs, 43 family members | RT-PCR
WGS Phylogenetic analysis |
Not reported | No | Not reported | |
| Wang 2020a | China | Retrospective observational
Home February 2020 |
Household | 85 primary cases: 155 household contacts
in 78 households |
RT-PCR | Not reported | No | <37 considered
positive |
|
| Wang 2020b | China | Retrospective cohort study
Homes February to March 2020 |
Household | 124 primary cases; 335 close
contacts |
RT-PCR | Within 2 weeks of symptom
onset of the primary case |
No | Not reported | |
| Wee 2020 | Singapore | Observational
Tertiary Hospital February to May 2020 |
Nosocomial | 28 index cases; 253 staff close-contacts
and 45 patient close-contacts |
RT-PCR | If patient close-contacts or
staff close-contacts developed symptoms |
No | Not specified | Infection control bundle was implemented comprising
infrastructural enhancements, improved PPE, and social distancing between patients. Patients were advised to wear surgical masks, to remain within their room or cohorted cubicle at all times, and to avoid mingling with each other. |
| Wendt 2020 | Germany | Observational
Hospital March 2020 |
Nosocomial | 1 index case physician; 187 contacts with
HCWs and 67 contacts with patients - 23 high-risk contacts in total |
RT-PCR
Serology |
5-days post exposure (5 & 10 days
post exposre for high-risk contacts |
No | <36 or <39 considered positive | All high-risk contacts and the index physician were examined
serologically on days 15 or 16 and days 22 or 23 after exposure. |
| Wolf 2020 | Germany | Observational case series
Hospital quarantine January-February 2020 |
Household | Family cluster: 1 index case, 4 close
contacts |
RT-PCR | 5-days after index case tested
positive |
No | Not reported | The parents were asked to wear masks; wearing masks was
not practical for the children. |
| Wong 2020 | Hong Kong | Observational
Hospital February 2020 |
Nosocomial | 1 index case in AIIR: 71 staff and 49 patients | RT-PCR | End of 28-day surveillance | No | Not specified | |
| Wood 2020 | UK | Retrospective cohort
HCW homes |
Household | 241,266 adults did not share a household
with young children; 41,198, 23,783 and 3,850 shared a household with 1, 2 and 3 or more young children |
PCR | Not reported | No | Not reported | Primary exposure was the number of children aged 0 to 11
years in each household. |
| Wu 2020 | China | Retrospective cohort study
Various January-February 2020 |
Household
Local Community |
144 cases, 2994 close contacts | Not reported | Not reported | No | Not reported | Shared transport, visit, medical care, household, brief contact. |
| Wu 2020a | China | Prospective observational
Homes February to March 2020 |
Household | 35 index cases; 148 household contacts | Not reported | Not reported | No | Not reported | All consecutive patients with probable or confirmed COVID-
19 admitted to the Fifth Affiliated Hospital of Sun Yat-sen University from 17 January to 29 February 2020 were enrolled. All included patients and their household members were interviewed |
| Xie 2020 | China | Cross-sectional
Home January-February 2020 |
Household | 2 family clusters with 61 residents (5 cases) | RT-PCR | 7 days after primary or index
cases diagnosed |
No | Not reported | |
| Xin 2020 | China | Prospective cohort study
Homes January to March 2020 |
Household | 31 primary cases; 106 household contacts | RT-PCR | Not reported | No | Not reported | |
| Yang 2020 | China | Observational cohort study
Home quarantine February-May 2020 |
Household
Local |
93 recurrent-positive patients; 96 close
contacts and 1,200 candidate contacts |
RT-PCR
Serology |
Within 14 days post-exposure | Yes | ≤ 40 considered
positive |
|
| Yau 2020 | Canada | Retrospective cohort study
Hospital dialysis unit April 2020 |
Nosocomial | 2 index cases; 330 contacts (237 patients
and 93 staff) |
RT-PCR | Not reported | No | Not reported | All symptomatic contacts were referred for testing but
asymptomatic household contacts were not routinely tested as per public health protocols at the time. |
| Ye 2020 | China | Observational
Religious gathering January-February 2020 |
Local
Community |
66 confirmed cases and 15 asymptomatic
infections: 1,293 close contacts |
RT-PCR | Not reported | No | Not reported | All close contacts were quarantined |
| Yoon 2020 | S. Korea | Observational
Childcare Centre February-March 2020 |
Local | 1 index case: 190 persons (154 children
and 36 adults) were identified as contacts; 44 were defined as close contacts (37 children and 7 adults) |
PCR | 8–9 days after the last exposure | No | <37 considered positive | Wearing masks, more frequent hand hygiene, and disinfection
of the environment were required before the child index case tested positive. |
| Yousaf 2020 | USA | Survey: cross-sectional
Tertiary-care referral facility June 8 to July 8, 2020 |
Household | 198 household contacts; index cases not
specified |
RT-PCR | Day 1 of study | No | Not reported | |
| Yu 2020 | China | Observational study
Homes January to February 2020 |
Household | 560 index cases; 1587 close contacts | Not reported | Within 2 weeks of exposure to
primary case |
No | Not reported | Exposure environments included workplace, medical centre,
etc. Contact methods included eating or living together, sleeping together, living in same house, etc |
| Yung 2020 | Singapore | Observational prospective
Homes March to April 2020 |
Household | 137 households, 213 paediatric contacts | Not reported | Unclear | No | Not reported | |
| Zhang 2020 | China | Retrospective Observational
Aircraft March-April 2020 |
Aircraft | 4462 passengers screened for COVID-19
based on close contact |
RT-PCR | Not reported | No | Not reported | All passengers were quarantined after arrival |
| Zhang 2020a | China | Retrospective observational
Various January-March 2020 |
Household
Local Community |
359 cases: 369 close contacts | Not reported | Not reported | No | Not reported | Households, social contact, workplace |
| Zhang 2020b | China | Observational study
Hospital April 2020 |
Household | 3 index cases; 10 close contacts | RT-PCR
Serology |
Not reported | No | <37 considered
positive |
Ct value of 40 or more was defined as a negative test. |
| Zhang 2020c | China | Observational
Quarantine January-February 2020 |
Local
Household |
Multi-family cluster of 22 cases: 93 close
contacts |
RT-PCR | Not specified | No | Not reported | All close contacts were quarantined in centralized facilities. |
| Zhang 2020d | China | Observational
Supermarket January-February 2020 |
Local | 1 index case: 8437 contacts | RT-PCR | Not reported | No | Not reported | |
| Zhuang 2020 | China | Observational study
Various January to February 2020 |
Household
Community |
Cluster outbreaks; 8363 close contacts | Not reported | Not reported | No | Not reported | Family and non-family cases |
Table 2. Main characteristics of systematic reviews.
| Study ID (n=9) | Fulfils
systematic review methods |
Research question (search date up to) | No. of included studies
(No. of participants) |
Main results | Key conclusions |
|---|---|---|---|---|---|
| Chen 2020 | Yes | To estimate seroprevalence by different types of
exposures, within each WHO region, we categorized all study participants into five groups: 1) close contacts, 2) high-risk healthcare workers, 3) low-risk healthcare workers, 4) general populations, and 5) poorly-defined populations (Search from Dec 1, 2019 to Sep 25, 2020). |
230 studies involving
1,445,028 participants were included in our meta-analysis after full-text scrutiny: Close contacts 16 studies 2901 positives out of 9,349 participants |
Estimated seroprevalence of all infections, 22.9% [95% CI,
11.1–34.7] compared to relatively low prevalence of SARS- CoV-2 specific antibodies among general populations, 6,5% (5.8–7.2%) see Appendix table 15 (page 152). The overall risk of bias was low. |
There were a very limited number of high-quality studies
of exposed populations, especially for healthcare workers and close contacts, and studies to address this knowledge gap are needed. Pooled estimates of SARS-CoV-2 seroprevalence based on currently available data demonstrate a higher infection risk among close contacts and healthcare workers lacking PPE, |
| Chu 2020 | Yes | To investigate the effects of physical distance, face
masks, and eye protection on virus transmission in health-care and non-health-care (eg, community) settings (We searched up to March 26, 2020) |
Identified 172 studies; 44
studies included in the meta-analysis which 7 were Covid-19 |
A strong association was found of proximity of the exposed
individual with the risk of infection (unadjusted n=10 736, RR 0·30, 95% CI 0·20 to 0·44; adjusted n=7782, aOR 0·18, 95% CI 0·09 to 0·38; absolute risk [AR] 12·8% with shorter distance vs 2·6% with further distance, risk difference. There were six studies on COVID-19, the association was seen irrespective of causative virus (p value for interaction=0·49). The risk of bias was generally low-to-moderate. |
Physical distancing of at least 1 m is strongly associated
with protection, but distances of up to 2 m might be more effective. |
| Fung 2020 | Yes | To review and analyze available studies of the
household SARs for SARS-CoV-2. Searched PubMed, bioRxiv, and medRxiv on 2 September 2020 for published and prepublished studies reporting empirical estimates of household SARs for SARS-CoV-2. Considered only English-language records posted on or after 1 January 2019. Inclusion criteria: Reported estimates of the household SAR or the data required to compute the household SAR; (2) comprised data from more than 1 household; and (3) they tested—at a minimum—all symptomatic household contacts by reverse transcription polymerase chain reaction (RT-PCR). |
22 papers met the eligibility
criteria: 6 papers reported results of prospective studies and 16 reported retrospective studies. The number of household contacts evaluated per study ranged from 11 to 10592. |
The 22 studies considered 20 291 household contacts, 3151
(15.5%) of whom tested positive for SARS-CoV-2. Household secondary attack rate estimates ranged from 3.9% in the Northern Territory, Australia to 36.4% in Shandong, China. The overall pooled random-effects estimate of SAR was 17.1% (95% confidence interval [CI], 13.7–21.2%), with significant heterogeneity (p<0.0001). The household secondary attack rates was highest for index cases aged 10–19 years (18.6%; 95% CI, 14.0–24.0%) and lowest for those younger than 9 (5.3%; 95% CI, 1.3–13.7%). 4 of the studies were judges as high quality; 14 as moderate quality; and 4 as low quality. Between-study variation could not be explained by differences in study quality. |
Secondary attack rates reported using a single follow-up
test may be underestimated, and testing household contacts of COVID-19 cases on multiple occasions may increase the yield for identifying secondary cases. There is a critical need for studies in Africa, South Asia and Latin America to investigate whether there are setting-specific differences that influence the household SAR. |
| Koh 2020 | Yes | The secondary attack rate (SAR) in household and
healthcare settings. Search between Jan 1 and July 25, 2020. |
118 studies, 57 were included
in the meta-analyses. |
Pooled household SAR 18.1% (95% CI: 15.7%, 20.6%)
significant heterogeneity (p <0.001). No significant difference in secondary attack rates in terms of the definition of household close contacts, whether based on living in the same household (18.2%; 95% CI: 15.3%, 21.2%) or on relationships such as family and close relatives (17.8%; 95% CI: 13.8%, 21.8%) In three studies, the household secondary attack rates of symptomatic index cases (20.0%; 95% CI: 11.4%, 28.6%) was higher than asymptomatic ones (4.7%; 95% CI: 1.1%, 8.3%) SAR from 14 studies showed close contacts adults were more likely to be infected compared to children (<18), relative risk 1.71 (95% CI: 1.35, 2.17). 43 high-quality studies were included for meta-analysis. |
There was variation in the definition of household
contacts; most included only those who resided with the index case, some studies expanded this to include others who spent at least a night in the same residence or a specified duration of at least 24 hours of living together, while others included family members or close relatives. |
| Li 2020 | No (quality
assesment not performed) |
~Carriage and transmission potential of SARS-
CoV-2 in children in school and community settings (Search performed on 21 June 2020 with entry date limits from late 2019) |
33 studies were included for
this review. Four new studies on SARS-CoV-2 transmission in school settings were identified. |
There is a lack of direct evidence on the dynamics of child
transmission, however the evidence to date suggests that children are unlikely to be major transmitters of SARS-CoV-2. |
The balance of evidence suggests that children play
only a limited role in overall transmission, but it is noted that the relative contribution of children to SARS-CoV-2 transmission may change with reopening of society and schools |
| Ludvigsson 2020 | No (quality
assesment not performed) |
Are children the main drivers of the COVID‐19
pandemic (Search to 11 May 2020) |
47 full texts studied in detail. | This review showed that children constituted a small fraction
of individuals with COVID‐19 |
Children are unlikely to be the main drivers of the
pandemic. Data on viral loads were scarce, but indicated that children may have lower levels than adults, |
| Madewell 2020 | Yes | What is the household secondary attack rate for
severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)? ( Searched through Oct 19, 2020) single database assessed |
54 studies with 77,758
participants |
Household secondary attack rates was 16.6%; restricted index
cases to children (<18 years), lower SAR of 0.5% Secondary attack rates for household and family contacts 3 times higher than for close contacts (4.8%; 95% CI, 3.4%- 6.5%; P < .001); Estimated mean household secondary attack rates from symptomatic index cases (18.0%; 95% CI, 14.2%-22.1%) higher than from asymptomatic or presymptomatic index cases (0.7%; 95% CI, 0%-4.9%; P < .001), there were few studies in the latter group. Infection risk was highest for spouses, followed by nonspouse family members and other relatives, all higher than other contacts. Estimated mean household secondary attack rates to spouses (37.8%; 95% CI, 25.8%-50.5%) higher than to other contacts (17.8%; 95% CI, 11.7%-24.8%). Significant heterogeneity was found among studies of spouses (I2 = 78.6%; P < .001) and other relationships (I2 = 83.5%; P < .001). Contact frequency with index case associated with higher odds of infection, At least 5 contacts during 2 days before the index case was confirmed; at least 4 contacts and 1 to 3 contacts, or frequent contact within 1 meter. Secondary attack rates for households with 1 contact (41.5%; 95% CI, 31.7%-51.7%) higher than households with at least 3 contacts (22.8%; 95% CI, 13.6%-33.5%; P < .001) but not different than households with 2 contacts (38.6%; 95% CI, 17.9%-61.6%). There was significant heterogeneity in secondary attack rates between studies with 1 contact (I2 = 52.9%; P = .049), 2 contacts (I2 = 93.6%; P < .001), or 3 or more contacts (I2 = 91.6%; P < .001). Information was not available on household crowding. A total of 16 of 54 studies (29.6%) were at high risk of bias, 27 (50.0%) were moderate, and 11 (20.4%) were low. |
Secondary attack rates were higher in households
from symptomatic index cases than asymptomatic index cases, to adult contacts than to child contacts, to spouses than to other family contacts, and in households with 1 contact than households with 3 or more contacts. Our study had several limitations. The most notable is the large amount of unexplained heterogeneity across studies. This is likely attributable to variability in study definitions of index cases and household contacts, frequency and type of testing, sociodemographic factors, household characteristics (eg, density, air ventilation), and local policies (eg, centralized isolation). The findings of this study suggest that households are and will continue to be important venues for transmission, even where community transmission is reduced. |
| Xu 2020 | Yes | Evidence for transmission of COVID-19 by
children in schools ( search in MEDLINE up to 14 September 2020. Further hand-searched reference lists of the retrieved eligible publications to identify additional relevant studies). Included children (defined as ≤18 years old) who were attending school, and their close contacts (family and household members, teachers, school support staff) during the COVID-19 pandemic |
11 studies were included: 5
cohort studies and 6 cross- sectional studies. |
Overall infection attack rate (IAR) in cohort studies: 0.08%,
95% CI 0.00%-0.86%. IARs for students and school staff were 0.15% (95% CI 0.00%-0.93%) and 0.70% (95% CI = 0.00%- 3.56%) respectively (p<0.01). Six cross-sectional studies reported 639 SARS-CoV-2 positive cases in 6682 study participants tested [overall SARS-CoV-2 positivity rate: 8.00% (95% CI = 2.17%-16.95%). SARS-CoV-2 positivity rate was estimated to be 8.74% (95% CI = 2.34%-18.53%) among students, compared to 13.68% (95% CI = 1.68%-33.89%) among school staff (p<0.01). Overall study quality was judged to be poor with risk of performance and attrition bias |
There is limited high-quality evidence to quantify the
extent of SARS-CoV-2 transmission in schools or to compare it to community transmission. Emerging evidence suggests lower IAR and SARS-CoV-2 positivity rate in students compared to school staff. |
| Yanes-Lane 2020 | Yes | Proportion of asymptomatic infection among
coronavirus disease 2019 (COVID-19) positive persons and their transmission potential. (Search up to up to 22 June 2020) |
28 moderate/high quality
studies included; 43 low quality studies excluded |
Asymptomatic COVID-19 infection at time of testing ranged
from 20% - 75%; among three studies in contacts it was 8.2% to 50%. Asymptomatic infection in obstetric patients pooled proprtion was 95% (95% CI, 45% to 100%) of which 59% (49% to 68%) remained asymptomatic through follow-up; Among nursing home residents, the proportion of asymtomoatic was 54% (42% to 65%) of which 28% (13% to 50%) remained asymptomatic through follow-up. |
The proportion of asymptomatic infection among
COVID-19 positive persons appears high and transmission potential seems substantial. |
| Zhu 2020 | Meta-analysis:
Quality assessment not performed |
Role of children in SARS-CoV-2 in household
transmission clusters ( Search between Dec, 2019 & Aug, 2020). |
57 articles with 213 clusters | 8 (3.8%) transmission clusters were identified as having
a paediatric index case. Asymptomatic index cases were associated with lower secondary attack rates in contacts than symptomatic index cases [RR] 0.17 (95% CI,0.09–0.29). SAR in paediatric household contacts was lower than in adult household contacts (RR, 0.62; 95% CI, 0.42–0.91). |
The data suggest that should children become infected
at school during this period, they are unlikely to spread SARS-CoV-2 to their co-habiting family members. |
Quality of included studies
None of the included primary studies reported a published protocol except one (Helsingen 2020). The risk of bias of the included primary studies is shown in Table 5. Only 61 studies (35.7%) adequately reported the methods used, and 97 (56.7%) adequately described the sources of sample collection. Only six studies (3.5%) adequately reported methods used to address biases. The overall quality of the studies was judged as low to moderate (see the risk of bias graph in Figure 2).
Figure 2. Risk of bias graph in primary studies of close contacts in SARS-CoV-2.
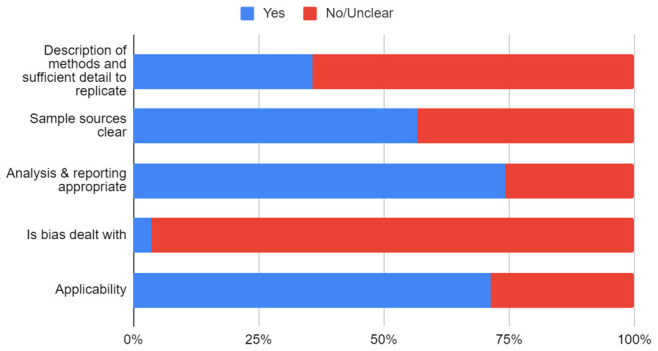
Reviews
We included 10 systematic reviews investigating the role of close contact in SARS-CoV-2 transmission ( Table 2). The studies included in the reviews were primarily observational. In one review (Chen 2020), there was a higher risk of infection in close contacts and healthcare workers without PPE compared to the general population. A second review (Chu 2020) found a significant association between proximity of exposure (distance <1m), absence of barriers (not using face covering or eye protection) and the risk of infection. The authors of three reviews (Li 2020, Ludvigsson 2020, Zhu 2020) concluded that children were unlikely to be the main conduit for transmission of SARS-CoV-2, and results of one review (Koh 2020) showed that adults with close contact exposure were significantly more likely to be infected compared with children (14 studies, RR: 1.71 (95% CI: 1.35, 2.17)). In one review (Xu 2020), the attack rates were significantly less in students compared with staff (p<0.01). One review (Fung 2020) reported household SARs ranging from 3.9% to 36.4%, but also highlighted the lack of SARS-CoV-2 research in Africa, South Asia, and Latin America. One review (Madewell 2020) found that SARs were higher in households from symptomatic index cases than asymptomatic index cases, and one review (Yanes-Lane 2020) concluded that the proportion of asymptomatic infection was high (20–75%). In two reviews (Koh 2020, Yanes-Lane 2020), studies judged to be of low quality were excluded from their meta-analyses. In one review (Chen 2020), the overall quality was reported as low, while 80% of included studies were reported as moderate or high quality in another two (Fung 2020, Madewell 2020). Another review (Chu 2020) reported the overall risk of bias as low-to-moderate, and one (Xu 2020) rated the overall quality as low. Three reviews did not assess study quality (see Table 2).
Primary studies
We found 171 primary studies ( Table 1). In general, the studies did not report any hypothesis but assessed epidemiological or mechanistic evidence for transmission associated with close contact settings. Ninety-three studies (54.4%) were conducted in Asia, 43 (25.1%) in Europe, 27 (15.8%) in North America, five (2.9%) in South America and three (1.8%) in Australasia. The study settings included home/quarantine facilities (n=54), hospital (n=26), social/religious gatherings (n=13), public transport (n=7) care homes (n=4), and educational settings (n=8). Thirteen studies used two settings (home plus one other setting). In 25 studies (15.2%), the settings were multiple (3 or more different settings). Two studies were conducted in professional sports settings: one Super League Rugby (Jones 2020) and one football team (Schumacher 2020)
All the included studies were observational in design except one RCT (Helsingen 2020): 24 studies were described as cohort, nine were case series and 12 cross-sectional. One study used a before and after study design. The number of close contact participants included ranged from 4 to 8437. Three studies (Chen 2020a, Hong 2020, Yang 2020) examined transmission dynamics in close contacts of index or primary cases with recurrent SARS-CoV-2 infections.
Eighty-two studies (46.8%) reported definitions of close contacts ( Table 3). There was a variation in the definitions across the studies. Seventeen studies (9.9%) defined close contact as exposure to the index or primary case within two metres for at least 15 minutes while four defined it as being within 2m for at least 10 minutes. In 24 studies, there was no specified distance reported - close contact definitions included unprotected exposure, living in the same household or bedroom, sharing a meal, or having repeated and prolonged contact. In five studies of airline passengers, close contact was defined as all passengers on the flight (Chen 2020), seated within two rows of the index case (Draper 2020, Pavli 2020, Speake 2020), or being within 2m for at least 15 minutes (Khanh 2020). Eighty-seven studies (50.9%) did not define close contact and the definition was unclear in four studies. Twenty-nine studies (17%) defined other types of contacts including primary contact, secondary contact, high-risk contact, household contact, social contact, and work contact (see Table 3).
Table 3. Definitions and descriptions of close contacts.
| Study ID | Definitions of close contacts | Definition of other contacts | Contact duration & proximity |
|---|---|---|---|
| Abdulrahman 2020 | Not defined | Not reported | Not reported |
| Adamik 2020 | Not defined | Other cases in each of the infected households were
regarded as secondary cases |
Not reported |
| Agergaard 2020 | Not defined | Not reported | 2 weeks |
| Angulo-Bazán 2020 | Not defined | Not reported | Not reported |
| Armann 2020 | Not defined | Not reported | Not reported |
| Arnedo-Pena 2020 |
Close contacts living in the same household of the index case and no other
sources of transmission apart from the index case could be found. |
Closed contacts from work, social events, relatives live
in other household were excluded and index cases live alone. |
Not reported |
| Baker 2020 | Not defined | Not reported | Median cumulative time spent with the patient 45 mins
(10–720 mins) |
| Baettig 2020 |
Close contact: Less than 2 m for more than 15 min in the last 48 hours before
onset symptom of the COVID-19 positive index patient. |
Not reported | <2m for >15 mins 48 hours before onset symptom of the
COVID-19 positive index patient |
| Bao 2020 | Not defined | Not reported | Average stay duration of 2.5 hr daily before the COVID‐19
outbreak. |
| Basso 2020 |
Close contact: ≥15 min at ≤2 m, or during AGPs, between HCWs and the non-
isolated COVID-19 patient |
Not reported | ≤2 m for ≥15 min or during AGP |
| Bays 2020 | Not defined | Not reported | Not specified |
| Bi 2020 |
Close contacts were identified as those who lived in the same apartment,
shared a meal, travelled, or socially interacted with an index case 2 days before symptom onset. |
Casual contacts (eg, other clinic patients) and some
close contacts (eg, nurses) who wore a mask during exposure were not included in this group. |
Not specified |
| Blaisdell 2020 | Not defined | Not reported | 1 week |
| Böhmer 2020 | High risk if they had cumulative face-to-face contact with a patient with
laboratory-confirmed SARS-CoV-2 infection for at least 15 min, had direct contact with secretions or body fluids of a patient with confirmed COVID-19, or, in the case of health-care workers, had worked within 2 m of a patient with confirmed COVID-19 without PPE |
All other contacts were classified as low-risk contacts. | Face-to-face for at least 15 minutes, direct contact without
PPE |
| Boscolo-Rizzo 2020 | Not defined | Not reported | Not reported |
| Brown 2020 | Not defined | Not reported | Mean in-class time = 50 minutes |
| Burke 2020 | Either at least 10 minutes spent within 6 feet of the patient with confirmed
COVID-19 (e.g., in a waiting room) or having spent time in the same airspace (e.g., the same examination room) for 0–2 hours after the confirmed COVID-19 patient. |
Not reported | Within 6 feet for at least 10 minutes |
| Canova 2020 | Not defined | Not reported | 5 HCWs: >30 minutes
5 HCWs: >15–30 mins 6 HCWs: 5–15 mins 5 HCWs: ≤5 mins |
| Cariani 2020 | Not defined | Not reported | Not reported |
| Charlotte 2020 | Not defined | Not reported | 2-hours |
| Chaw 2020 |
Close contact: Any person living in the same household as a confirmed case-
patient or someone who had been within 1 m of a confirmed case-patient in an enclosed space for >15 minutes |
Not reported | Within 1m for >15 mins |
| Chen 2020 | Close contact: All passengers were regarded as close contacts | Not reported | Flight duration 5 hours approx |
| Chen 2020a |
Close contacts are persons who have had close contact with re-positive patients
without effective protection with masks, such as living and working together |
Not reported | Not specified |
| Chen 2020b | Not defined | Not reported | Not specified |
| Chu 2020 |
Community contact: Any close contact (being within 6 feet of the case-patient)
for a prolonged time (>10 minutes); being an office co-worker of the case-patient with close contact of any duration; contact with infectious secretions from the case-patient; or sharing a healthcare waiting room or area during the same time and up to 2 hours after the case-patient was present. |
Healthcare contact: Face-to-face interaction between
healthcare personnel (HCP) and the case-patient without wearing the full PPE that was recommended at the time of the investigation or potential contact with the case-patient’s secretions by HCP without wearing full PPE. |
>10 mins to 2 hours |
| Chen 2020c | Not defined | Not reported | Not reported |
| Cheng 2020 | Close contact was a person who did not wear appropriate PPE while having
face-to-face contact with a confirmed case for more than 15 minutes during the investigation period. A contact was listed as a household contact if he or she lived in the same household with the index case. Those listed as family contacts were family members not living in the same household. For health care settings, medical staff, hospital workers, and other patients in the same setting were included; close contact was defined by contacting an index case within 2 m without appropriate PPE and without a minimal requirement of exposure time |
Those listed as family contacts were family members
not living in the same household. |
Within 2 m without PPE, face-to-face contact for >15
minutes |
| Chu 2020a | Not defined | Not reported | Stayed ≥1 night in the household during case’s infectious
period |
| Contejean 2020 | Close contact: Distance <2 meters for >10 minutes was defined as close contact | Not reported | <2 metres for >10 minutes |
| COVID-19 National Emergency Response Center 2020 | Close contact (or high risk exposure)” was being within 2 meters of a COVID-19
case |
Daily contact (or low risk exposure) was defined as
having proximity with a person who was a confirmed COVID-19 case, without having had close contact. |
Not reported |
| Danis 2020 | All children and teachers who were in the same class as the symptomatic pediatric
case were considered as high risk contacts and were isolated at home. Moderate/high risk: Person who had prolonged (> 15 min) direct face-to-face contact within 1 m with a confirmed case, shared the same hospital room, lived in the same household or shared any leisure or professional activity in close proximity with a confirmed case, or travelled together with a COVID-19 case in any kind of conveyance, without appropriate individual protection equipment. |
Low risk: Person who had a close (within 1 m) but
short (< 15 min) contact with a confirmed case, or a distant (> 1 m) but prolonged contact in public settings, or any contact in private settings that does not match with the moderate/high risk of exposure criteria. Negligible risk: Person who had short (< 15 min) contact with a confirmed case in public settings such as in public transportation, restaurants and shops; healthcare personnel who treated a confirmed case while wearing appropriate PPE without any breach identified. |
4 days in chalet |
| Dattner 2020 | Not defined | Not reported | Not reported |
| de Brito 2020 | Close contact: Close and prolonged contact in the same room | Not reported | Not specified |
| Deng 2020 | Not defined | Not reported | Not reported |
| Desmet 2020 | Not defined | Not reported | Not reported |
| Dimcheff 2020 |
Close contact: Within 2 m or 6 feet) with an individual with confirmed COVID-19
for >15 minutes with the example being exposed to a family member at home who has had a positive COVID-19 nasal swab |
Not reported | Within 2m for >15 mins |
| Dong 2020 | Not defined | Not reported | Not reported |
| Doung-ngern 2020 |
High-risk if they were family members or lived in the same household as a
COVID-19 patient, if they were within a 1-meter distance of a COVID-19 patient longer than 15 minutes; if they were exposed to coughs, sneezes, or secretions of a COVID-19 patient and were not wearing protective gear, such as a mask; or if they were in the same closed environment within a 1-meter distance of a COVID- 19 patient longer than 15 minutes and were not wearing protective gear |
Not reported | <15 min vs >15 min, <1m vs >1m |
| Draper 2020 | Close contact was defined as anyone who had face-to-face contact with a
confirmed COVID-19 case for more than 15 minutes cumulatively or continuously (e.g. household setting or healthcare setting without appropriate use of personal protective equipment) or who was in the same room with an infectious case for more than 2 hours (e.g. school room, workplace) while a case was symptomatic or during the 24 hours preceding symptom onset. Aircraft close contacts included passengers seated in the same row as, or in the two rows in front of or behind, an infectious case. If the case was a crew member, the passengers in the area in which the crew member worked were classified as close contacts. Passengers disembarking from cruise ships with high incidence of COVID-19 were also classified as close contacts for surveillance purposes. |
Not reported | Not reported |
| Dub 2020 |
Close household contact, i.e. an individual sharing the main residence of the
secondary case |
A regular household contact, i.e. an individual who
would regularly host or stay in the same residence of a secondary case (step-sibling, divorced parent and new partner). Extended contact, i.e. an individual who would have frequent contact with the secondary case around and after the exposure, for example, grandparents who were involved in caring of the secondary case, according to parents’ reports. |
<2 meters for >10 minutes |
| Expert Taskforce 2020 | Close contact: Cabinmates of confirmed case-patients | Not reported | Not specified |
| Fateh-Moghadam 2020 | Contact of a COVID-19 case has been considered any person who has had
contact with a COVID-19 case within a time frame ranging from 48 hours before the onset of symptoms of the case to 14 days after the onset of symptoms |
Not reported | Not reported |
| Firestone 2020 |
Close contact: Being within 6 feet of a patient with laboratory-confirmed COVID-
19 infection for ≥15 minutes |
Not reported | Within 2m for >15 mins |
| Fontanet 2020 | Not defined | Not reported | Not reported |
| Fontanet 2020a | Not defined | Not reported | Not reported |
| Gan 2020 | Not defined | Not reported | Not reported |
| Ghinai 2020 | Not defined | Not reported | Not reported |
| Gong 2020 |
Close contact: Anyone who was closely in contact with a suspected, confirmed
and asymptomatic case without effective personal protection (classified protection according to the contact situation, including gloves, medical protective masks, protective face screens, isolation clothing, etc.) since onset of symptoms in the suspected case and confirmed case or the day asymptomatic case’s specimens were collected. The close contact included: (i) living, working, or studying in one house or classroom, (ii) diagnosing, treating, or visiting cases in hospital ward, (iii) being within short distance in the same vehicle, (iv) other situations assessed by the field investigators. |
Not reported | Not reported |
| Gu 2020 | Not defined | Not reported | 5 hrs, no natural ventilation or face masks;
distance between each other <0.5 m |
| Hamner 2020 | Close contact: Within 6 feet of infected case | Not reported | 2.5 hrs within 2 m |
| Han 2020 |
Close contact: Travel was defined as someone who was in close contact with
a confirmed case for over three hours as they traveled to another region aside from Region A. Close contact: meal was defined as someone who was in close contact with a confirmed case for over 30 minutes after having a meal together. |
A casual contact was defined as someone who spent
several minutes with a confirmed case within the same space without any mask on (or a person was established as a contact by an Epidemic intelligence Officer). |
30 mins to 3 hours |
| Heavey 2020 |
Close contact: Any individual who has had greaterthan 15 minutes face-to-face
(<2 meters distance*) contact with a case, in any setting. |
Casual contact: Any individual who has shared a closed
space with a case for less than two hours. |
Up to 2 hours in duration |
| Helsingen 2020 | Not defined | Not reported | Not reported |
| Hendrix 2020 | Not defined | Not reported | Not reported |
| Hirschman 2020 |
Close contact: Within 6 feet of an infected person for at least 15 minutes
starting from 2 days before illness onset. |
Not reported | "Hours" |
| Hobbs 2020 |
Close contact: Within 6 feet for ≥15 minutes) with a person with known COVID-
19, school or child care attendance, and family or community exposures ≤14 days before the SARS-CoV-2 test |
Not reported | Within 2 m for ≥15 minutes |
| Hoehl 2020 | Not defined | Not reported | Not reported |
| Hong 2020 | Anyone who ever came within 2 m of a diagnosed patient without the use of
effective personal protective equipment |
Not reported | 258 person-days |
| Hu 2020 |
Close contacts were defined as individuals who had close-proximity interactions
(within 1 meter) with clinically suspected and laboratory-confirmed SARS-CoV-2 cases, for the period from 2 days before, to 14 days after, the potential infector’s symptom onset. For those exposed to asymptomatic subjects, the contact period was from 2 days before, to 14 days after, a respiratory sample was taken for real-time RT-PCR testing. Close contacts included, but were not limited to, household contacts (i.e., household members regularly living with the case), relatives (i.e., family members who had close contacts with the case but did not live with the case), social contacts (i.e., a work colleague or classmate), and other close contacts (i.e., caregivers and patients in the same ward, persons sharing a vehicle, and those providing a service in public places, such as restaurants or movie theatres) |
Not reported | Not reported |
| Hua 2020 | Not defined | Not reported | |
| Huang 2020 | Close contacts quarantined at home or hospital | Not reported | Not reported |
| Huang 2020a | Not defined | Not reported | Not reported |
| Islam 2020 | Close contact was defined as individuals who were closely linked by contact
tracing and were considered a close contact group provided that no PPE was worn having direct face to face contacts. |
Household contacts were defined as individuals who
lived and were sharing the same room and same apartment in the same household. Family contacts were those who are the members of the same family but not living in the same household. |
Face-to-face |
| Jia 2020 | A
close contact was defined as a person who did not take effective protection
against a suspected or confirmed case 2 d before the onset of symptoms or an asymptomatic infected person 2 d before sampling. |
Not reported | Not reported |
| Jiang 2020 |
Close contacts: Lived with the patients and individuals who had contact with
the patients within 1 meter without wearing proper personal protection. Ct value ≥40 was considered negative. The maximum likelihood phylogenetic tree of the complete genomes was conducted by using RAxML software with 1000 bootstrap replicates, employing the general time-reversible nucleotide substitution mode |
Not reported | 1 m |
| Jing 2020 | A
close contact was defined as an individual who had unprotected close
contact (within 1 m) with a confirmed case within 2 days before their symptom onset or sample collection. Individuals who were linked by contact tracing were considered a close contact group |
Not reported | Not reported |
| Jing 2020a | Not defined | Not reported | Not reported |
| Jones 2020 |
Close contacts were defined by analysis of video footage for player interactions
and microtechnology (GPS) data for proximity analysis. |
Not reported | Within 1 m, face-to-face for ≥3 secs |
| Kang 2020 | Not defined | Not reported | Not reported |
| Kant 2020 | Not defined | Not reported | Not reported |
| Kawasuji 2020 | Not defined | Not reported | Not reported |
| Khanh 2020 |
Close contact: <2 m distance for >15 minutes. Successfully traced passengers
and crew members were interviewed by use of a standard questionnaire, tested for SARS-CoV-2 |
Not reported | <2 m distance for >15 minutes. |
| Kim 2020 | Not defined | Household contact: Occurring at least 1 day after but
within 14 days from the last point of exposure. |
2 days during the presymptomatic period and 1 day during
the symptomatic period of the index case. |
| Kim 2020a | Not defined | Not reported | 2 hrs to 4 days |
| Kim 2020b |
Contact was defined as presence in the same room with COVID-19 confirmed
patients, or in the same outpatient clinic or examination room, 30 minutes before and after COVID-19 confirmed patients. Within 2 m of confirmed patients (via CCTV) |
Not reported | Within 2 m of confirmed patients for 30 mins |
| Kumar 2020 | Not defined | Not reported | Not reported |
| Kuwelker 2020 | Not defined | Household members were defined as individuals who
resided in the same household as the index case. |
Not reported |
| Kwok 2020 |
Close contacts referred to anyone who: (i) provided care to the case (including
a family member or healthcare worker) or had other close physical contact; or (ii) stayed at the same place (including household members or visitors) while the case was ill. |
Not reported | Not reported |
| Ladhani 2020 | Not defined | Not reported | Not reported |
| Ladhani 2020a | Not defined | Not reported | Not reported |
| Laws 2020 | Not defined | Not reported | Unclear |
| Laxminarayan 2020 | High-risk contacts had close social contact or direct physical contact with index
cases without protective measures High-risk travel exposures—defined as close proximity to an infected individual in a shared conveyance for ≥6 hours |
Low-risk contacts were in the proximity of index cases
but did not meet criteria for high-risk exposure |
Not reported |
| Lee 2020 | Not defined: Frequent close contact | Not reported | >1 m |
| Lee 2020a | Close contact (household contact) | Not reported | Mean contact period was calculated to be 7.7 days. |
| Lewis 2020 | Not defined | Household contacts were defined as all persons living
in the same household as the primary patient. |
Not reported |
| Li 2020 | Not defined | Not reported | Unclear |
| Li 2020a | Not defined | Not reported | Not reported |
| Li 2020b |
Close contact was defined as an act of sharing a meal, party, vehicle or living
room with a confirmed or latently infected patient within 14 days. |
Not reported | Not reported |
| Li 2020c |
Close contacts were mainly those who have not take effective protection from
close contact with the suspected and confirmed cases 2 days before symptoms appeared, or the asymptomatic infected persons 2 days before the specimen collection. |
Not reported | Not reported |
| Li 2020d | Not defined | Not reported | Not reported |
| Liu 2020 | Not defined | Not reported | Unclear |
| Liu 2020a | Direct contact with patients with neo-coronary pneumonia (within 1 m) | Not reported | Within 1m for 2.5 hrs |
| Liu 2020b |
Close contacts were defined by the China Prevention and Control Scheme of
COVID-19. |
Not reported | 7.8 (95%CI: 7.0–8.7) close contacts per index case. |
| Liu 2020c | Not defined | Not reported | Not reported |
| López 2020 |
Close contact: Anyone who was within 6 feet of a person with COVID-19 for at
least 15 minutes ≤2 days before the patient’s symptom onset. |
Not reported | ≤1.83m of a person with COVID-19 for at least 15 minutes
≤2 days before the patient’s symptom onset |
| Lopez Bernal 2020 | Household contacts were defined as those living or spending significant time in
the same household. Household contacts, others with direct face to face contact and healthcare workers who had not worn recommended PPE |
Not reported | Not reported |
| Lucey 2020 |
Close contact: HCW or patient who spent more than 15 minutes face-to-face
within 2 metres of a confirmed case or patients who shared a multi-bedded room with a confirmed case for more than 2 hours. |
Not reported | Not reported |
| Luo 2020 | Unclear: The tour coach was with 49 seats was fully occupied with all windows
closed and the ventilation system on during the 2.5-hour trip. |
Not reported | 1 to 4.5m; up to 2.5 hours on a bus |
| Luo 2020a |
Close contacts: Anyone who has had contact, without effective protection
regardless of duration of exposure, with 1 or more persons with suspected or confirmed COVID-19 any time starting 2 days before onset of symptoms in persons with a suspected or confirmed case, or 2 days before sampling for laboratory testing of asymptomatic infected persons. |
Not reported | Not reported |
| Lyngse 2020 | Not defined | Not reported | Not reported |
| Ma 2020 | Not defined | Not reported | Longest contact time: 8 days
Shortest contact time: 0 days |
| Macartney 2020 |
Close contacts: Children or staff with face-to-face contact for at least 15 min,
or who shared a closed indoor space for at least 40 min with a case during their infectious period. |
Not reported | Face-to-face contact for at least 15 min, or who shared a
closed indoor space for at least 40 min |
| Malheiro 2020 |
Close contacts (high risk)were defined as individuals who have spent 15 min or
more in closeproximity (2 m or less) to, or in a closed space with, a case. |
Not reported | Not reported |
| Maltezou 2020 |
Close contact was defined as a contact of >15 minutes within a distance of <2 m
with a COVID-19 case. |
Household members were defined as persons living in
the same residence. |
>15 minutes within <2 m |
| Maltezou 2020a |
Close contact was defined as a contact of >15 minutes within a distance of <2
meters with a COVID-19 case |
Household contacts were defined as persons either
living in the same residence or having close contacts with a family member for >4 hours daily in the family residence. |
Household: >4 hours daily
Close contact: >15 minutes within <2 m |
| Mao 2020 | Not defined | Not reported | Not reported |
| Martinez-Fierro 2020 | Individual who has had closer than <6 feet for ≥15 min with people with
a positive diagnosis for COVID-19, whether they were symptomatic or asymptomatic according to the CDC definition |
Not reported | ≥15 min at a distance of <1.83m |
| Mponponsuo 2020 | An interaction of >15 minutes at a distance of <1 m | Not reported | >15 minutes at a distance of <1 m |
| Ng 2020 |
Close contacts were individuals who had contact for at least 30 min within a 2 m
distance from the index case. |
Work contacts were defined as individuals who came
into close contact with the index case at work, from 2 days before the onset of symptoms to isolation of the case, to account for pre-symptomatic transmission. Social contacts were defined as individuals who came into close contact with the index case, from 2 days before onset of symptoms to isolation of the case, through social activities. Transport contacts were excluded Lower risk contacts: Other contacts who were with the index case for 10–30 min within 2 m |
At least 30 min within a 2 m |
| Ning 2020 | Not defined | Not reported | Unclear |
| Njuguna 2020 | Not defined | Not reported | Unclear |
| Ogawa 2020 | Not defined | Not reported | Not reported |
| Paireau 2020 | Not defined | Not reported | Not reported |
| Park 2020 | Not defined | Not reported | Not reported |
| Park 2020a | High-risk contact (household contacts of COVID-19 patients, healthcare
personnel) |
Household contact was a person who lived in the
household of a COVID-19 patient and a nonhousehold contact was a person who did not reside in the same household as a confirmed COVID-19 patient. |
Not reported |
| Park 2020b | Not defined | Not reported | Not reported |
| Passarelli 2020 | Not defined | Not reported | Not reported |
| Patel 2020 | Not defined | Not reported | Not reported |
| Pavli 2020 |
Close contacts were defined as persons sitting within a distance of <2 m for >15 min,
including passengers seated two seats around the index case and all crew members and persons who had close contact with the index case. |
Not reported | <2 m for >15 min |
| Phiriyasart 2020 | Close contact was defined as a person who had at least one of these following
criteria : (i) a person who came into close (within 1 meter) contact with, or had a conversation with any patient for >5 minutes, or was coughed or sneezed on by any patient when he/she did not wear appropriate personal protective equipment (PPE), e.g. a face mask, (ii) a person who was in an enclosed space without proper ventilation, e.g. in the same air-conditioned bus/air-conditioned room as any patient , and was within one meter of any patient for >15 minutes without wearing appropriate PPE. High-risk close contact was defined as a close contact who was likely to contract the virus from any patient through exposure to respiratory secretions of any patient while not wearing PPE according to standard precautions. |
A low-risk close contact was defined as a close contact
who was less likely to contract the virus from any patient. This includes close contacts who have not met the definition for high-risk close contacts. |
Not reported |
| Poletti 2020 | Not defined | Not reported | Not reported |
| Pung 2020 |
Close contacts: People who spend a prolonged time within 2 m of a confirmed
case |
Other contacts: People who had some interactions
with the case. |
Unclear |
| Pung 2020a | Unclear: Close household contacts | Not reported | Unclear |
| Qian 2020 | Four categories of infected individuals were considered based on their
relationship: family members, family relatives, socially connected individuals, and socially non‐connected individuals |
Not reported | Not reported |
| Ravindran 2020 |
Close contact: Face-to-face contact for greater than 15 minutes cumulative in
the period extending from 48 hours before onset of symptoms in a confirmed case; or sharing of closed space with a confirmed case for a prolonged period of time in the period extending from 48 hours before onset of symptoms in a confirmed case. |
Not reported | Face-to-face contact for at least 15 min, or who shared a
closed indoor space for prolonged period 48 hrs before onset of symptoms |
| Razvi 2020 | Not defined | Not reported | Not reported |
| Rosenberg 2020 | Not defined | Not reported | |
| Roxby 2020 | Not defined | Not reported | Not reported |
| Sang 2020 | Not defined | Not reported | Not reported |
| Schumacher 2020 | Close contact: Approximately 30–90 seconds in close proximity (<1.5 m) of other
players |
Close social contacts (including sharing a car) | 30–90 seconds in close proximity (<1.5 m) |
| Schwierzeck 2020 | Not defined | Not reported | Not reported |
| Shah 2020 | Household contact was defined as contact sharing same residential address. | Not reported | Not reported |
| Shen 2020 |
Close contacts defined as individuals who had close, prolonged, and repeated
interactions with the 2 source cases (Cases 2 and 3). |
All other contacts are defined as casual contacts. | Not reported |
| Sikkema 2020 | Not defined | Not reported | Not reported |
| Son 2020 | Not defined | A contact was defined as anyone who was in contact
with a confirmed case from a day before the symptoms occurred, in a manner that offered the potential for transmission through respiratory droplets |
Not reported |
| Song 2020 | Unclear: shared the same bedroom, had dinner together | Not reported | Not reported |
| Speake 2020 | 2 rows in front and behind infectious passenger on an airplane | Not reported | Unclear |
| Stein-Zamir 2020 | Not defined | Not reported | Not reported |
| Sugano 2020 | Not defined | Not reported | Unclear |
| Sun 2020 | Not defined | Not reported | Not reported |
| Taylor 2020 | Not defined | Not reported | Unclear |
| Teherani 2020 | Household contacts (HCs) were defined as an adult ( 18 years) or a child (<18
years) who resided in the home with the SIC at the time of diagnosis. |
Not reported | Not reported |
| Thangaraj 2020 | Not defined | Not reported | Unclear |
| Torres 2020 | Not defined | Not reported | Unclear |
| Tshokey 2020 | Unclear: Close friends, roommates, flight seat partner, spouse or partner, cousin,
physician, tour driver |
Primary contacts: Individuals coming in some form of
contact with the confirmed cases such as conveyance in the same cars/flights, encounter in clinics, serving meals, or providing housekeeping services in hotels. Secondary contacts: Individuals coming in contact with the primary contacts |
Unclear |
| van der Hoek 2020 | Not defined | Not reported | |
| Wang 2020 | Not defined | Not reported | Unclear |
| Wang 2020a | Not defined | Not reported | Unclear |
| Wang 2020b | Close contact was defined as being within 1 m or 3 feet of the primary case, such
as eating around a table or sitting together watching TV. |
Not reported | Unclear |
| Wee 2020 | Not defined | Not reported | Within 2 m of the index case for a cumulative time of ≥15
minutes, or who had performed AGPs without appropriate PPE. |
| Wendt 2020 |
High-risk contacts: >15 min face-to-face contact, sitting in a row behind
physician for 45 mins, transfer in an ambulance (45-min drive). |
Not reported | >15 min face-to-face contact |
| Wolf 2020 | Not defined | Not reported | Not specified |
| Wong 2020 |
Contact case was defined as a patient or staff who stayed or worked in the same ward as the
index patient. Patients who shared the same cubicle with the index case were considered as ‘patient close contact’. Staff close contact: Staff who had contact within 2 m of the index case for a cumulative time of >15 min, or had performed AGPs, without ‘appropriate’ PPE. |
Casual contacts: All staff and patients who did not fulfill
the pre-defined criteria for close contacts. Casual/low-rosk contact: HCW wearing a facemask or respirator only and have prolonged close contact with a patient who was wearing a facemask, or HCW using all recommended PPE or HCW (not using all recommended PPE) who have brief interactions with a patient regardless of whether patient was wearing a facemask. Patient close contacts were quarantined into an AIIR (or quarantine camp if the patient was deemed clinically stable to be discharged from hospital) for 14 days. |
Within 2 m of the index case for a cumulative time of >15
min |
| Wood 2020 | Not defined | Not reported | Not reported |
| Wu 2020 |
Close contact: Been within 1 metre of a confirmed case, without effective PPE,
within the period since 5 days before the symptom onset in the index case or since 5 days before sampling if the index case was asymptomatic. |
Not reported | Within 1 metre of a confirmed case, without effective PPE |
| Wu 2020a | Household contacts were defined as person who spent at least 1 night in the
house after the symptom onset of the index patient. A household was defined as ≥2 people living together in the same indoor living space. A household index was the first person to introduce SARS-CoV-2 into the household. |
Not reported | At least 1 night |
| Xie 2020 |
Close contact: An individual who has not taken effective protection when in
proximity of suspected or confirmed cases 2 days before the onset of symptoms or 2 days before the collection of asymptomatic specimens. |
Not reported | Unclear |
| Xin 2020 | Close contacts were defined as persons who had a short‐range contact history
for 2 days before the onset of symptoms in COVID‐19‐suspected and ‐confirmed cases, or 2 days before the collection of samples from asymptomatic cases without taking effective protective measures, such as family members in the same house, direct caregivers, and medical staff who provided direct medical care, colleagues in the same office or workshop, etc. |
The effective contact duration for the close contacts
was defined as the contact days with index patients with confirmed COVID‐19, which was calculated as the last contact date minus the start contact date, and all dates were corresponding to the definition of close contacts |
The median effective contact duration with patients
with COVID‐19 was 4 (IQR: 1–6) days, with 57 (53.8%) experiencing effective contact between 3 and 11 days, and 9 (8.5%) with effective contact duration > 11 days |
| Yang 2020 | Close contacts: Uunprotected exposure. | Candidate contacts: Teachers and classmates | Not reported |
| Yau 2020 | Close unprotected contact with someone who has tested positive for COVID-19
in the last 14 days |
Not reported | Unclear |
| Ye 2020 | Not defined | Not reported | Not reported |
| Yoon 2020 |
Close contact was defined as a person who had face-to-face contact for >15
minutes or who had direct physical contact with the index case-patient. Persons who used the same shuttle bus were also considered to be close contacts. |
Not reported | Face-to-face contact for >15 minutes or direct physical
contact |
| Yousaf 2020 | Not defined | Not reported | Not reported |
| Yu 2020 |
Close contacts were defined as those who lived in the same household, shared
meals, traveled or had social interactions with a confirmed case two days before the onset of COVID-19 symptoms |
Not reported | Not reported |
| Yung 2020 | Not defined | Not reported | Not reported |
| Zhang 2020 | Not defined | Not reported | Not reported |
| Zhang 2020a |
Close contact: Refers to a person who had contact with index case without
using proper protection during 2 days before the index case was tested. |
Not reported | Not reported |
| Zhang 2020b | Not defined | Not reported | Not reported |
| Zhang 2020c |
Close contacts were individuals who lived with a PCR-confirmed case or
interacted with a case within 1 metre from the case without any personal protections. |
Not reported | Within 1m of case |
| Zhang 2020d | Not defined | Not reported | Not reported |
| Zhuang 2020 | Not defined | Not reported | Not reported |
Eighteen studies (10.5%) reported data on the contact duration between close contacts and the index or primary cases ( Table 3). The average contact duration ranged from 30 minutes to 8 days across 16 studies that investigated transmission rates using RT-PCR. In two studies that examined transmission using serology (Agergaard 2020, Hong 2020), the durations of contact were two weeks and 258 person-days, respectively. The mean contact duration was either unclear or not reported in 148 studies (90.2%).
A total of 110 studies (64.3%) used RT-PCR as a test method for confirming SARS-CoV-2 positivity, while eight studies (4.8%) exclusively investigated transmission using serology. In 24 studies (14%), both PCR and serology were used to investigate close contact in SARS-CoV-2 transmission. Thirty-one studies (18.1%) did not report the test method used. For PCR, the timing of sample collection varied from within 24 hours to 14 days after exposure to the index or primary case; for serology, this ranged from 2–10 weeks post-exposure. In total, 71 studies (41.5%) reported the timing of sample collection. The timing of sample collection was either not reported or unclear in 100 studies (58.5%).
Twenty-two studies (12.9%) reported Ct values for determining PCR test positivity: ≤40 (eight studies), <37 (five studies), ≤35 (three studies), <38 (two studies), one each for <25, ≤30, <32 and <36 (or 39). Only eight studies reported the Ct values for close contacts in their results – these ranged from 16.03 to 38.
Thirty-two studies reported conducting serological tests to assess transmission of SARS-CoV-2 ( Table 4). There was variation in the description of the tests. Fifteen studies determined the antibody responses to SARS-CoV-2 spike proteins using Immunoglobulin G (IgG) and IgM while 11 used only IgG. In 17 studies, the threshold for serological positivity was not reported. Three studies (Kuwelker 2020, Ng 2020, Yang 2020) performed neutralisation assays to confirm positive serologic samples. In one study (Torres 2020), study participants self-administered the serological tests.
Table 4. Description of serological tests in close contact studies of SARS-CoV-2.
| Study ID | Serological test | Description of test | Thresholds for serological positivity |
|---|---|---|---|
| Agergaard 2020 | IgG and IgM | iFlash and DiaSorin | iFlash SARS-CoV-2 N/S IgM/IgG cut-off: ≥12 AU/ml = positive.
DiaSorin SARS-CoV-2 S1/S2 IgG cut-off: ≥15 AU/ml = positive, 12 < x < 15 AU/ml = equivocal, and ≤12 AU/ml = negative. |
| Angulo-Bazán 2020 | IgG and IgM | Coretests ® COVID-19 IgM / IgG Ab Test (Core Technology Co. Ltd), a lateral flow immunochromatographic test that qualitatively
detects the presence of antibodies against SARS-CoV-2, with a sensitivity and specificity reported by the manufacturer for IgM / IgG of 97.6% and 100%, respectively |
Not reported |
| Armann 2020 | IgG | Diasorin LIAISON® SARS-CoV-2 S1/S2 IgG Assay). All samples with a positive or equivocal LIAISON® test result, as well as all samples
from participants with a reported personal or household history of a SARS-CoV-2 infection, were re-tested with two additional serological tests: These were a chemiluminescent microparticle immunoassay (CMIA) intended for the qualitative detection of IgG antibodies to the nucleocapsid protein of SARS-CoV-2 (Abbott Diagnostics® ARCHITECT SARS-CoV-2 IgG ) (an index (S/C) of < 1.4 was considered negative whereas one >/= 1.4 was considered positive) and an ELISA detecting IgG against the S1 domain of the SARS- CoV-2 spike protein (Euroimmun® Anti-SARS-CoV-2 ELISA) (a ratio < 0.8 was considered negative, 0.8–1.1 equivocal, > 1.1 positive) Participants whose positive or equivocal LIAISON® test result could be confirmed by a positive test result in at least one additional serological test were considered having antibodies against SARS-CoV_x0002_2. |
Antibody levels > 15.0 AU/ml were considered positive and levels
between 12.0 and 15.0 AU/ml were considered equivocal. |
| Baettig 2020 | IgG and IgM | Used commercially available immunochromatography rapid test with SARS-CoV-2 protein-specific IgM and IgG. This test was
performed according to the manufacturers’ instructions with a reported sensitivity and specificity of 93% and 95%, respectively. |
Not reported |
| Basso 2020 | IgG and IgM | Sera were collected approximately 3 weeks following exposure for the detection of antibodies against SARS-CoV-2. EDI Novel
Coronavirus COVID-19 lgG and IgM ELISA (Epitope Diagnostics, Inc., San Diego, CA, USA) were used for initial testing, and supplemented with tests from DiaSorin (LIAISON SARS-CoV-2 S1/S2 IgG test), Abbott (Alinity i SARS-CoV-2 IgG), Roche (Elecsys Anti- SARS-CoV-2) and Wantai (WANTAI SARS-CoV-2 Ab ELISA). |
Not reported |
| Brown 2020 | IgG and IgM | ELISA (authors referenced another study) | Reciprocal titers of >400 to be positive and reciprocal titers of
>100 but <400 to be indeterminate. |
| Chen 2020b | IgG and IgM | In-house enzyme immunoassay (EIA). 96-well plates were coated with 500 ng/mL of recombinant RBD or NP protein overnight,
incubating with diluted serum samples at 1:20. Plates were incubated with either anti-human IgM or IgG conjugated with HRP. Optical density (OD) value (450nm-620nm) was measured. |
Preliminary cut-off values were calculated as the mean of the
negative serum OD values plus 3 standard deviation (SD) from 90 archived healthy individuals in 2019. A close contact was considered seropositive if OD of 1:20 diluted serum was above the cut-off values for either IgM or IgG against both RBD and NP protein |
| Chu 2020 | IgG and IgM | Serum samples were tested at CDC using a SARS-CoV-2 ELISA with a recombinant SARS-CoV-2 spike protein (courtesy of Dr. Barney
Graham, National Institutes of Health, Bethesda, MD, USA) as an antigen. Protein ELISA 96-well plates were coated with 0.15 μg/mL of recombinant SARS-CoV-2 spike protein and ELISA was carried out as previously described. An optimal cutoff optical density value of 0.4 was determined for >99% specificity and 96% sensitivity. Serum samples from the case-patient were used as a positive control and commercially available serum collected before January 2020 from an uninfected person as a negative control. |
Total SARS-CoV-2 antibody titers >400 were considered
seropositive. |
| Dattner 2020 | IgG | Abbott SARS-CoV-2 IgG, whose specificity was estimated as ∼100% and whose sensitivity at ≥ 21 days was estimated as ∼85% | Not reported |
| de Brito 2020 | IgG and IgM | Chemiluminescence 4 weeks after contact with the index case | Not reported |
| Dimcheff 2020 | IgG | Serum IgG to thD4:D12e nucleoprotein of SARS-CoV-2 was measured using a Federal Food and Drug Administration (FDA)
emergency-use–authorized chemiluminescent microparticle immunoassay performed on an automated high throughput chemistry immunoanalyzer (Architect i2000SR, Abbott Laboratories, Abbott Park, IL). The sensitivity of this assay is reported to be 100% with a specificity of 99% at >14 days after symptom onset in those infected with SARS-CoV-2.1 At 5% prevalence, the positive predictive value is 93.4% and the negative predictive value is 100% |
Results are reported in a relative light units (RLU) index; a value
≥1.4 RLU is considered a positive antibody response. |
| Dub 2020 | IgG | IgG antibodies to SARS-CoV-2 nucleoprotein (The Native Antigen Company, United Kingdom) were measured
with a fluorescent bead-based immunoassay (manuscript in preparation). Antigen was conjugated on MagPlex Microspheres and bound IgG antibodies were identified by a fluorescently labeled conjugated antibody (R_x0002_Phycoerythrin- conjugated Goat Anti-Human IgG, Jackson Immuno Research, USA). The plate was read on Luminex® MAGPIX® system. xPONENT software version 4.2 (Luminex®Corporation, Austin, TX) was used to acquire and analyze data. Median fluorescent intensity was converted to U/ml by interpolation from a 5- parameter logistic standard curve. The specificity and sensitivity of the assay was assessed using receiver operator curve (ROC) with 100% specificity and 97.9% sensitivity |
MNT titre of ≥ 6 considered positive
FMIA titre 3·4 U/ml considered positive |
| Fontanet 2020 | IgG | Antibody responses to SARS-CoV-2 using several assays developed by Institut Pasteur : an ELISA N assay, detecting antibodies
binding to the N protein; a S-Flow assay, which is a flow-cytometry based assay detecting anti-S IgG; and a LIPS assay, which is an immunoprecipitation-based assay detecting anti-N and anti-S1 IgG. |
Participants were considered seropositive for SARS-CoV-2 if any
test was positive, since all tests had a specificity higher than 99% with the cut-offs chosen for positivity |
| Fontanet 2020a | Not specified | Serological testing was conducted using the S-Flow assay, a flow_x0002_cytometry-based serological test developed by the Institut
Pasteur. The assay is based on the recognition of the SARS-CoV-2 Spike protein expressed at the surface of 293T cells. In previous studies, the sensitivity of the assay was estimated at 99.4% (95% CI = 96.6% - 100%) on a panel of 160 RT-PCR confirmed mild forms of COVID-1928, while its specificity was found to be 100% (one-sided 97.5% CI = 97.4% - 100%) on a panel of 140 pre-epidemic sera |
Not reported |
| Gu 2020 | IgG | Not described | Not reported |
| Helsingen 2020 | IgG | Measurement of IgG antibodies was performed with a multiplex flow cytometric assay known as microsphere affinity proteomics
(MAP) |
Not specified. Referenced |
| Hong 2020 | IgG and IgM | Qualitative colloidal gold assay (Innovita (Tangshan) Biological Technology, Co., Ltd, Tangshan, China), following manufacturers’
instructions. The sensitivity of the assay was 87.3% (95%CI 80.4–92.0%), and the specificity was 100% (95%CI 94.20–100%) according to the instructions of the assay. |
Not reported |
| Kuwelker 2020 | IgG | A two-step ELISA was used for detecting SARS-CoV-2-specific antibodies, initially by screening with receptor-binding domain (RBD)
and then confirming seropositivity by spike IgG. Endpoint titres were calculated as the reciprocal of the serum dilution giving an optical density (OD) value=3 standard deviations above the mean of historical pre-pandemic serum samples. Individuals with no antibodies were assigned a titre of 50 for calculation purposes. Neutralisation assays were used to quantify SARS-CoV-2-specific functional antibodies. VN titres were determined as the reciprocal of the highest serum dilution giving no CPE. Negative titres (<20) were assigned a value of 10 for calculation purpose. |
Not specified. |
| Lewis 2020 | Not specified | ELISA (authors referenced another study) | Not specified |
| Luo 2020a | IgG and IgM | Not described | Asymptomatic: Specific IgM detected in serum.
Symptomatic: Detectable SARS-CoV-2–specific IgM and IgG in serum, or at least a 4-fold increase in IgG between paired acute and convalescent sera. |
| Macartney 2020 | IgA, IgG, IgM | SARS-CoV-2-specific IgG, IgA, and IgM detection was done using an indirect immunofluorescence assay (IFA) that has a sensitivity
compared with nucleic acid testing of detecting any of SARS-CoV-2-specific IgG, IgA, or IgM when samples were collected at least 14 days after illness onset of 91·3% (95% CI 84·9–95·6) and specificity of 98·9% (95% CI 98·4–99·3%; MVNO, personal communication). |
Not specified |
| Martinez-Fierro 2020 | IgG and IgM | IgM and IgG against SARS-CoV-2 were determined using a total blood sample through a 2019 nCov IgG/IgM rapid test (Genrui
Biotech, Shenzen, China) |
Not specified |
| Ng 2020 | Not specified | human ACE-2 (hACE2) protein (Genscript Biotech, New Jersey, United States) was coated at 100 ng/well in 100 mM carbonate-
bicarbonate coating buffer (pH 9.6). 3ng of horseradish peroxidase (HRP)-conjugated recombinant receptor binding domain (RBD) from the spike protein of SARS-CoV-2 (GenScript Biotech) was pre-incubated with test serum at the final dilution of 1:20 for 1 hour at 37°C, followed by hACE2 incubation for 1 h at room temperature.Serum samples were tested with a surrogate viral neutralising assay for detection of neutralising antibodies to SARS-CoV-2. |
A positive serological test result was concluded if the surrogate
viral neutralising assay for a particular sample resulted in inhibition of 30% or greater (98·9% sensitivity and 100·0% specificity) |
| Ogawa 2020 | IgG | Abbott® (Abbott ARCHITECT SARS-CoV-2 IgG test, Illinois, USA) | Not specified |
| Poletti 2020 | IgG | Not described | Not specified |
| Razvi 2020 | IgG and IgM | Blood samples were analysed on the day of collection using the Roche Elecsys Anti-Sars-CoV-2 serology assay. This
electrochemiluminescent immunoassay is designed to detect both IgM and IgG antibodies to SARS-CoV-2 in human serum and plasma and has been shown to have a high sensitivity and specificity |
Not specified |
| Schumacher 2020 | IgG and IgM | SARS-CoV-2-specific antibodies were measured in serum samples using an
electrochemiluminescence immunoassay (Elecsys® Anti-SARS-CoV-2, Roche Diagnostics, Rotkreuz, Switzerland). |
Cut-off indices ≤1 reported as negative and indices >1 as positive. |
| Torres 2020 | IgG and IgM | Novel Coronavirus (2019-nCoV) IgG/IgM Test Kit (Colloidal gold) from Genrui Biotech Inc. The study nurse and/or technician viewed
the photo provided by the participant along with the participant’s self-report as to the visibility of the three bands, and determined whether the tests were IgG+, IgM+, IgG & IgM+, Negative, Invalid, or Indeterminate. Participants were asked to attach a photo of the test after 15 minutes had elapsed and self-report the appearance of the three lines, G (IgG), M (IgM), and C (test control) |
Colour-coded - self-administered test: self-reporting the
appearance of the three lines, G (IgG), M (IgM), and C (test control) |
| van der Hoek 2020 | IgG | Fluorescent bead-based multiplex-immunoassay. Referenced | A cut-off concentration for seropositivity (2.37 AU/mL; with
specificity of 99% and sensitivity of 84.4%) was determined by ROC-analysis of 400 pre-pandemic control samples |
| Wendt 2020 | IgA and IgG | ELISA (Euroimmun, Lübeck, Germany), following the manufacturer’s instructions. | Inconclusive (≥0.8 and <1.1) or Positive (≥1.1 |
| Yang 2020 | IgA, IgG, IgM | Serum immunoglobulin (Ig) antibody against the SARS-CoV-2 surface spike protein receptor-binding domain (RBD) was measured
using a chemiluminescence kit (IgM, IgG, and total antibody, Beijing Wantai Biotech, measured by cut-off index [COI]) or ELISA kit (IgA, Beijing Hotgen Biotech, measured by optical density at 450/630 nm [OD450/630]). The cut-off for seropositivity was set according to the manufacturer’s instruction, verified using positive (169 serum specimens from confirmed COVID-19 patients) and negative (128 serum specimens from healthy persons) controls, and both of sensitivity and specificity were 100%. Virus neutralization assays were performed using SARS-CoV-2 virus strain 20SF014/vero-E6/3 (GISAID accession number EPI_ISL_403934) in biosafety level 3 (BSL-3) laboratories. Neutralizing antibody (NAb) titer was the highest dilution with 50% inhibition of cytopathic effect, and a NAb titer of ≥1:4 was considered positive. |
Specimens with COI>1 (IgM, IgG, or total antibody),
OD450/630 > 0.3 (IgA) were considered positive. |
| Zhang 2020b | IgG and IgM | SARS-CoV-2-specific IgM and IgG were tested by paramagnetic particle chemiluminescent immunoassay using iFlash-SARS-CoV-2
IgM/IgG assay kit (Shenzhen YHLO Biotech Co., Ltd) and iFlash Immunoassay Analyzer (Shenzhen YHLO Biotech Co., Ltd). The specificity and sensitivity of SARS-CoV-2 IgM and IgG detection were also evaluated |
Not specified |
Table 5. Quality of included studies.
| Study | Description of methods
and sufficient detail to replicate |
Sample
sources clear |
Analysis &
reporting appropriate |
Is bias
dealt with |
Applicability | Notes |
|---|---|---|---|---|---|---|
| Abdulrahman 2020 | Unclear | Yes | Yes | No | Yes | |
| Adamik 2020 | Unclear | Unclear | Yes | No | Unclear | |
| Agergaard 2020 | No | Yes | Yes | No | Yes | |
| Angulo-Bazán 2020 | Yes | No | Yes | Unclear | Yes | |
| Armann 2020 | Unclear | Yes | Yes | No | Yes | |
| Arnedo-Pena 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Baker 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Baettig 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Bao 2020 | Unclear | Yes | Yes | No | Yes | |
| Basso 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Bays 2020 | Unclear | Yes | Yes | No | Yes | |
| Bi 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Blaisdell 2020 | Yes | No | Yes | Unclear | Yes | |
| Böhmer 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Boscolo-Rizzo 2020 | Unclear | Yes | Yes | No | Yes | |
| Brown 2020 | Yes | Yes | Yes | Unclear | Unclear | |
| Burke 2020 | Unclear | No | Yes | No | Yes | |
| Canova 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Cariani 2020 | Unclear | Yes | Unclear | Unclear | Yes | |
| Charlotte 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Chaw 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Chen 2020 | Unclear | Unclear | Yes | No | Unclear | |
| Chen 2020a | Unclear | Yes | Yes | Unclear | Yes | |
| Chen 2020b | Yes | Yes | Yes | Unclear | Yes | |
| Chen 2020c | Unclear | No | Yes | No | Yes | |
| Cheng 2020 | Yes | No | Yes | Unclear | Yes | |
| Chu 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Chu 2020a | Unclear | Unclear | Unclear | No | Yes | |
| Contejean 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| COVID-19 National Emergency Response Center 2020 | Unclear | No | Yes | No | Yes | |
| Danis 2020 | Yes | Yes | Yes | No | Yes | |
| Dattner 2020 | Yes | Yes | Yes | Unclear | Yes | |
| de Brito 2020 | Yes | Yes | Unclear | Unclear | Yes | |
| Deng 2020 | Unclear | No | Unclear | Unclear | Unclear | |
| Desmet 2020 | Yes | Yes | Yes | No | Unclear | |
| Dimcheff 2020 | Yes | Unclear | Yes | Unclear | Unclear | |
| Dong 2020 | Unclear | No | Unclear | No | Yes | |
| Doung-ngern 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Draper 2020 | Yes | Yes | Yes | No | Yes | |
| Dub 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Expert Taskforce 2020 | Unclear | Unclear | Yes | Unclear | Unclear | |
| Fateh-Moghadam 2020 | Unclear | No | Yes | No | Yes | |
| Firestone 2020 | Unclear | Unclear | Yes | Unclear | Yes | |
| Fontanet 2020 | Yes | Yes | Yes | No | Yes | |
| Fontanet 2020a | Yes | Yes | Yes | No | Yes | |
| Gan 2020 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Ghinai 2020 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Gong 2020 | Yes | Yes | Unclear | Unclear | Unclear | |
| Gu 2020 | Unclear | Unclear | Unclear | No | Unclear | |
| Hamner 2020 | Unclear | Unclear | Yes | No | Yes | |
| Han 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Heavey 2020 | Unclear | No | Yes | No | Yes | |
| Helsingen 2020 | Yes | Yes | Yes | Yes | Yes | |
| Hendrix 2020 | Yes | Yes | Yes | No | Yes | |
| Hirschman 2020 | Unclear | Unclear | Unclear | No | Yes | |
| Hobbs 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Hoehl 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Hong 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Hu 2020 | Unclear | No | Yes | No | Yes | |
| Hua 2020 | Yes | Unclear | Yes | Unclear | Yes | |
| Huang 2020 | Unclear | Unclear | Yes | No | Unclear | |
| Huang 2020a | Unclear | Unclear | Yes | Unclear | Unclear | |
| Islam 2020 | Yes | No | Yes | No | Yes | |
| Jia 2020 | Unclear | Unclear | Yes | No | Unclear | |
| Jiang 2020 | Yes | Yes | Unclear | No | Yes | |
| Jing 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Jing 2020a | Unclear | Yes | Unclear | Unclear | Unclear | |
| Jones 2020 | Unclear | Yes | Yes | Unclear | Unclear | |
| Kang 2020 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Kant 2020 | Unclear | Yes | Unclear | No | Unclear | |
| Kawasuji 2020 | Unclear | Yes | Unclear | Unclear | Unclear | |
| Khanh 2020 | Yes | Yes | Yes | No | Yes | |
| Kim 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Kim 2020a | Unclear | Yes | Yes | No | Unclear | |
| Kim 2020b | Yes | Yes | Yes | No | Yes | |
| Kumar 2020 | Unclear | Yes | Unclear | No | Unclear | |
| Kuwelker 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Kwok 2020 | Unclear | Unclear | Yes | Unclear | Unclear | |
| Ladhani 2020 | No | Unclear | Unclear | No | Yes | |
| Ladhani 2020a | Unclear | Unclear | Yes | Unclear | Yes | |
| Laws 2020 | Unclear | Unclear | Yes | Unclear | Yes | |
| Laxminarayan 2020 | Yes | No | Yes | No | Yes | |
| Lee 2020 | Unclear | Unclear | Yes | Unclear | Unclear | |
| Lee 2020a | Unclear | No | Yes | No | Yes | |
| Lewis 2020 | Yes | Yes | Yes | No | Yes | |
| Li 2020 | Unclear | Yes | Unclear | No | Unclear | |
| Li 2020a | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Li 2020b | Unclear | Yes | Unclear | Unclear | Unclear | |
| Li 2020c | Unclear | No | Unclear | Unclear | Unclear | |
| Li 2020d | Yes | Yes | Yes | No | Yes | |
| Liu 2020 | Unclear | Unclear | Unclear | No | Yes | |
| Liu 2020a | Yes | Yes | Yes | Unclear | Unclear | |
| Liu 2020b | Unclear | Yes | Yes | Unclear | Yes | |
| Liu 2020c | Unclear | Unclear | Unclear | No | Unclear | |
| López 2020 | Unclear | Unclear | Yes | Unclear | Yes | |
| Lopez Bernal 2020 | Yes | Unclear | Yes | No | Yes | |
| Lucey 2020 | Unclear | Yes | Yes | No | Yes | |
| Luo 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Luo 2020a | Unclear | Yes | Yes | Yes | Yes | They use multiple
imputation to minimise inferential bias, and they discuss recall bias, selection bias and regression to the mean. |
| Lyngse 2020 | Yes | Unclear | Yes | Yes | Yes | They investigate bias
within their data and discuss this fairly fully |
| Ma 2020 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Macartney 2020 | Yes | Unclear | Yes | Unclear | Yes | |
| Malheiro 2020 | Yes | Unclear | Yes | Unclear | Yes | |
| Maltezou 2020 | Unclear | Unclear | Unclear | Unclear | Yes | |
| Maltezou 2020a | Unclear | Unclear | Unclear | No | Yes | |
| Mao 2020 | Unclear | Unclear | Yes | No | Unclear | |
| Martinez-Fierro 2020 | Unclear | Yes | Yes | No | Yes | |
| Mponponsuo 2020 | Unclear | Yes | Yes | Yes | Yes | Recall bias was minimized
by examining multiple data sources for both index cases and exposed persons |
| Ng 2020 | Unclear | Yes | Yes | Yes | Yes | Authors looked at
differences that could have led to bias |
| Ning 2020 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Njuguna 2020 | Unclear | Unclear | Yes | Unclear | Yes | |
| Ogawa 2020 | Unclear | Unclear | Yes | No | Yes | |
| Paireau 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Park 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Park 2020a | Unclear | No | Yes | No | Yes | |
| Park 2020b | Unclear | Yes | Yes | No | Unclear | |
| Passarelli 2020 | Unclear | No | Unclear | Unclear | Yes | |
| Patel 2020 | Yes | Yes | Yes | Unclear | Unclear | |
| Pavli 2020 | Unclear | Yes | Yes | No | Yes | |
| Phiriyasart 2020 | Yes | Yes | Yes | No | Yes | |
| Poletti 2020 | Unclear | Yes | Yes | Yes | Unclear | |
| Pung 2020 | Yes | Unclear | Yes | Unclear | Yes | |
| Pung 2020a | Unclear | No | Unclear | Unclear | Unclear | |
| Qian 2020 | Unclear | Unclear | Unclear | No | Unclear | |
| Ravindran 2020 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Razvi 2020 | Unclear | Yes | Yes | No | Yes | |
| Rosenberg 2020 | Yes | Yes | Yes | No | Yes | |
| Roxby 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Sang 2020 | Unclear | Yes | Unclear | No | Unclear | |
| Schumacher 2020 | Unclear | Yes | Unclear | Unclear | Yes | |
| Schwierzeck 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Shah 2020 | Unclear | No | Unclear | No | Yes | |
| Shen 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Sikkema 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Son 2020 | Unclear | Unclear | Yes | No | Yes | |
| Song 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Speake 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Sugano 2020 | Unclear | Unclear | Yes | Unclear | Yes | |
| Stein-Zamir 2020 | Yes | Unclear | Yes | No | Yes | |
| Sun 2020 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Taylor 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Teherani 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Thangaraj 2020 | Unclear | Yes | Yes | Unclear | Unclear | |
| Torres 2020 | Yes | Unclear | Yes | Unclear | Yes | |
| Tshokey 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| van der Hoek 2020 | Unclear | Yes | Yes | No | Yes | |
| Wang 2020 | Unclear | Yes | Unclear | Unclear | Yes | |
| Wang 2020a | Yes | Unclear | Yes | Unclear | Yes | |
| Wang 2020b | Yes | Yes | Yes | No | Yes | |
| Wee 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Wendt 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Wolf 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Wong 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Wood 2020 | Unclear | No | Yes | Unclear | Yes | |
| Wu 2020 | Yes | Unclear | Yes | Unclear | Yes | |
| Wu 2020a | Yes | Unclear | Yes | Unclear | Yes | |
| Xie 2020 | Unclear | Yes | Yes | Unclear | Yes | |
| Xin 2020 | Yes | No | Yes | No | Yes | |
| Yang 2020 | Unclear | Yes | Unclear | Unclear | Yes | |
| Yau 2020 | Unclear | Yes | Unclear | Unclear | Unclear | |
| Ye 2020 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Yoon 2020 | Yes | Yes | Yes | Unclear | Yes | |
| Yousaf 2020 | Unclear | Yes | Unclear | Unclear | Unclear | |
| Yu 2020 | Yes | No | Yes | No | Yes | |
| Yung 2020 | Unclear | Yes | Yes | No | Yes | |
| Zhang 2020 | Unclear | Unclear | Unclear | No | Unclear | |
| Zhang 2020a | Yes | Unclear | Yes | Unclear | Unclear | |
| Zhang 2020b | Unclear | Yes | Unclear | Unclear | Yes | |
| Zhang 2020c | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Zhang 2020d | Unclear | Yes | Unclear | Unclear | Unclear | |
| Zhuang 2020 | Unclear | No | Yes | No | Unclear |
Three studies (Ladhani 2020a, Speake 2020, Yang 2020) performed viral culture, while 10 studies (Böhmer 2020, Firestone 2020, Jiang 2020, Ladhani 2020a, Lucey 2020, Pung 2020, Sikkema 2020, Speake 2020, Taylor 2020, Wang 2020) performed genome sequencing (GS) plus phylogenetic analysis.
Frequency of SARS-CoV-2 attack rates (ARs)
Twenty-three studies reported data on attack rates using RT-PCR ( Table 6). The settings included healthcare (n=3), household (n=8), public transport (n=2), educational settings (n=3). In one study of 84 children in daycare centres during the first few weeks of the pandemic (Desmet 2020), the AR was 0%; similar results were reported in another study of hospital healthcare workers (Basso 2020). The frequency of ARs in the remaining 21 studies ranged from 3.5 to 75% ( Figure 3a). The ARs were highest in weddings (69%), prison (69.5%) and households (75%). Attack rates appeared lower in healthcare settings; two healthcare settings with higher ARs (Ladhani 2020, Ladhani 2020a) included nursing home residents – the definition of SARS-CoV-2 infection in both studies did not include the full constellation of respiratory and non-respiratory symptoms. In sports settings, the AR during matches was between 4.2% and 4.7%.
Figure 3a. Primary attack rates of SARS-CoV-2 in close contacts (PCR).

Table 6. Main results of included studies.
| Study ID | Type of transmission | Total number of contacts | Cycle threshold | Attack rates and/or secondary attack rates (SAR) | Notes |
|---|---|---|---|---|---|
| Abdulrahman 2020 | Community |
Eid Alfitr
Pre-: 71,553; Post-: 76,384 Ashura Pre-: 97,560; Post-: 118,548 |
Not reported |
Eid Alfitr
Pre-: 2990 (4.2%); Post-: 4987 (6.7%); p <0.001 Ashura Pre-: 3571 (3.7%); Post-: 7803 (6.6%); p <0.001 |
The rates of positive tests was significantly
greater after religious events |
| Adamik 2020 | Household | Unclear | Not reported | Unclear: 3553 (AR 26.7%) | |
| Agergaard 2020 | Household | PCR: 5
Serology: 5 |
Not reported | Index case plus 1 family member tested positive-
PCR All 5 displayed a serological SARS-CoV-2 N/S IgG response |
|
| Angulo-Bazán 2020 | Household | 52 households (n=236 people)
4.5±2.5 members per household |
Not reported | Serology: Amongst cohabitants, SAR was 53.0%
(125 cases): 77.6% of cases were symptomatic |
Convenience sampling, no component of
temporality, selection bias |
| Armann 2020 | Local
Household |
2045 in Phase 1
1779 in Phase 2 |
N/A | Serology: 12/2045 (0.6%)
Serology: 12/1779 (0.7%) |
|
| Arnedo-Pena 2020 | Household | 745 | Not reported | 11.1% (95% CI 9.0–13.6) | |
| Baker 2020 | Nosocomial | 44 | Not reported | 3/44 (6.8%): 1 of these was also exposed to a
household member with COVID-19. |
Recall error and bias, report is limited to
a single exposure, change in mask policy partway through the exposure period |
| Baettig 2020 | Local | 55 | Not reported | Serologic attack rates: 2/55 (3.6%) | Serological testing was positive for the 2
contacts 14 days after index case |
| Bao 2020 | Community | 57 index cases
1895 exposed |
Not reported | SAR was 3.3% at the bathing pool, 20.5% in
the colleagues’ cluster and 11.8% in the family cluster. |
Delayed detection of the activity trajectory of
the primary case, reporting bias, overlap of close contacts |
| Basso 2020 | Nosocomial | 60 HCWs - ≥106 unique high-risk
contacts |
Not reported | Attack rate: 0/60 (0%)
Serology: 0/60 (0%) |
Delay in diagnosing index case, recall bias |
| Bays 2020 | Nosocomial | 421 HCWs | Not reported | 8/421 (1.9%) | In all 8 cases, the staff had close contact with
the index patients without sufficient PPE. Hospital staff developing ILI symptoms were tested for SARS-CoV-2, regardless of whether they had contact with an index patient |
| Bi 2020 | Local
Household Community |
1,296 | Not reported | 98/1286 (7.6%) | |
| Blaisdell 2020 | Community | 1,022 | Not reported | 1.8% of camp attendees (10 staff members and
8 campers) |
Travel was assumed to be from home state
but intermediate travel might have occurred |
| Böhmer 2020 | Local
Household |
241 | Not reported | 75·0% (95% CI 19·0–99·0; three of four people)
among members of a household cluster in common isolation, 10·0% (1·2–32·0; two of 20) among household contacts only together until isolation of the patient, and 5·1% (2·6–8·9; 11 of 217) among non-household, high-risk contacts. |
|
| Boscolo-Rizzo 2020 | Household | 296 | Not reported | 74/296 (25.0%, 95% CI 20.2–30.3%) | The prevalence of altered sense of smell or
taste was by far lower in subjects negative to SARS-CoV-2 compared to both positives (p < 0.001) and non-tested cases (p < 0.001). |
| Brown 2020 | Local | 21 | Not reported | Serologic attack rate: 2/21 (1%) | Social desirability bias likely |
| Burke 2020 | Household | 445 | Not reported | 0.45% (95% CI = 0.12%–1.6%) among all close
contacts, and a symptomatic secondary attack rate of 10.5% (95% CI = 2.9%–31.4%) among household members. |
2 persons who were household members
of patients with confirmed COVID-19 tested positive for SARS-CoV-2. |
| Canova 2020 | Nosocomial | 21 | Not reported | 0/21 (0%) | |
| Cariani 2020 | Nosocomial | Unclear | 33.6 to 38.03 | 182 out of 1683 (10.8%) tested positive; 27 of
whom had close contact with COVID-positive patients |
Unclear how many HCWs had close contact;
likelihood of recall bias |
| Charlotte 2020 | Community | 27 | Not reported | 19 of 27 (70%) tested positive | High risk of selection bias: The index case-
patients were not identified. A majority of patients were not tested for SARS-CoV-2 |
| Chaw 2020 | Local
Community |
1755 | Not reported | Close contact: 52/1755 (29.6%)
Nonprimary attack rate: 2.9% (95% CI 2.2%– 3.8%) |
Potential environmental factors were not
accounted for: relative household size, time spent at home with others, air ventilation, and transmission from fomites. |
| Chen 2020 | Aircraft | 335 | Not reported | 16/335 (4.8%) | Recall bias. Did not perform virus isolation
and genome sequencing of the virus, which could have provided evidence of whether viral transmission occurred during the flight. |
| Chen 2020a | Local
Household |
209 | Not reported | 0/209 (0%) | |
| Chen 2020b | Nosocomial | 105 | Not reported | Serology: 18/105 (17.1%) | |
| Chen 2020c | Local
Community Household Nosocomial |
2147 | Not reported | 110/2147 (5.12%) | |
| Cheng 2020 | Household
Nosocomial |
2761 | Not reported | 0.70% | |
| Chu 2020 | Community | 50 exposed | Not reported | None for antigen or antibody: 0/50 (0%) | Testing was biased toward contacts who knew
the case-patient personally (office co-workers) or provided direct care for the case-patient (HCP). |
| Chu 2020a | Household | 526 exposed | Not reported | 48 (9%) (CI 7-12%) | Very high risk of selection bias |
| Contejean 2020 | Nosocomial | 1344 exposed | Not reported | 373 (28%) | |
| COVID-19 National Emergency Response Center 2020 | Local
Household Nosocomial |
2370 | Not reported | 13/2370 (0.6%) | There were 13 individuals who contracted
COVID-19 resulting in a secondary attack rate of 0.55% (95% CI 0.31–0.96). There were 119 household contacts, of which 9 individuals developed COVID-19 resulting in a secondary attack rate of 7.56% (95% CI 3.7–14.26). |
| Danis 2020 | Local
Household |
Chalet: 16
School: 172 |
Not reported | Attack rate: 75% in chalet
Attack rate: 0% in school |
Only 73 of 172 school contacts were tested
- all tested negative |
| Dattner 2020 | Household | 3353 | Not reported | Attack rates: 25% in children and 44% adults (45% overall)
Serology: 9/714 (1.3%) |
|
| de Brito 2020 | Household | 24 exposed | Not reported | RT-PCR: 6/7 (86%); Seropositivity: 18/24 (75%) | |
| Deng 2020 | 347 | Not reported | 25/347 (7.2%) | ||
| Desmet 2020 | Local | 84 | 38.8 | Attack rate: 0/84 (0%) | Ct reported for only one test result |
| Dimcheff 2020 | Community
Nosocomial Household |
1476 | Not reported | Seroprevalence 72/1476: 4.9% (95% CI,
3.8%–6.1%) |
|
| Dong 2020 | Household | 259 | Not reported | 53/259 (20.5%) | |
| Doung-ngern 2020 | Local | 211 cases plus
839 non-matched controls |
Not reported | ||
| Draper 2020 | Local
Household Nosocomial |
445 | Not reported | 4/445 (0.9%) | None of the 326 aircraft passengers or
4 healthcare workers who were being monitored close contacts became cases. |
| Dub 2020 | Local
Household |
121 | Not reported | Child index case: No positive cases
Adult index case: 8/51 (16%) Serology: 6/101 (5.9%) |
|
| Expert Taskforce 2020 | Local | Unclear | Not reported | Attack rate 20.4% | Attack rates were highest in 4-person cabins
(30.0%; n = 18), followed by 3-person cabins (22.0%; n = 27), 2-person cabins (20.6%; n = 491), and 1-person cabins (8%; n = 6). |
| Fateh-Moghadam 2020 | Community | 6690 | Not reported | 890/6690 (13.3%) | |
| Firestone 2020 | Local | Unclear | Not reported | 41 (80%) interviewed patients with primary
event-associated COVID-19 reported having close contact with others during their infectious period, with an average of 2.5 close contacts per patient. 36 (75%) of 48 interviewed patients with primary event-associated cases reported having close contact with persons in their household while infectious, and 17 (35%) reported having other (social/workplace) close contacts while infectious. |
|
| Fontanet 2020 | Local | 661 | N/A | Serology: 171/661 (25.9%, 95%CI 22.6-29.4) | |
| Fontanet 2020a | Local | 510 | N/A | Serology: 45/510 (8.8%) | |
| Gan 2020 | Local
Household Community |
Unclear | Not reported | Not reported | Family clusters accounted for 86.9% (914/1
050) of cases, followed by party dinners (1.1%) |
| Ghinai 2020 | Community | Unclear | Not reported | Unclear | |
| Gong 2020 | Household
Community |
Unclear | Not reported | Unclear | |
| Gu 2020 | Local | 14 | Not reported | RT-PCR - 3/14 (21.4%)
Serology - 2/14 (14.3%) |
|
| Hamner 2020 | Local | 60 | Not reported | Confirmed: 32/60 (53.3%)
Probable: 20/60 (33.3%) |
|
| Han 2020 | Community | 192 | Not reported | 7/192 (3.7%) | |
| Heavey 2020 | Local | 1155 | Not reported | 0/1155 (0%) | |
| Helsingen 2020 | Local | Training arm: 1,896
Nontraining arm: 1,868 |
Not reported | 11/1896 (0.8%) vs 27/1868 (2.4%); P=0.001 | |
| Hendrix 2020 | Local | 139 exposed | Not reported | 0% | Six close contacts of stylists A and B outside
of salon A were identified: four of stylist A and two of stylist B. All four of stylist A’s contacts later developed symptoms and had positive PCR test results for SARS-CoV-2. These contacts were stylist A’s cohabitating husband and her daughter, son-in-law, and their roommate, all of whom lived together in another household. None of stylist B’s contacts became symptomatic. |
| Hirschman 2020 | Household
Community |
58 | Not reported | 27/58 (47%) | |
| Hobbs 2020 | Local
Household Community |
397 | Not reported | Not reported | |
| Hoehl 2020 | Local
Community |
825 children and 372 staff: 7,366 buccal
mucosa swabs and 5,907 anal swabs |
Not reported | 0% viral shedding in children; 2/372 (0.5%)
shedding for staff. No inapparent transmissions were observed |
Study was conducted in the summer of 2020,
when activity of other respiratory pathogens was also low |
| Hong 2020 | Household | 431 tests | Not reported | 0/13 (0%) | Index cases had lived with their family
members without personal protections for a total of 258 person-days. |
| Hu 2020 | Household
Community |
15648 | Not reported | 471/15648 (3%) | |
| Hua 2020 | Household | 835 | Not reported | 151/835 (18.1%) | |
| Huang 2020 | Household
Community |
22 | Not reported | 7/22 (31.8%) | |
| Huang 2020a | Local
Household Community Nosocomial |
3795 | Not reported | 32/3795 (0.84%) | |
| Islam 2020 | Household
Local Community Nosocomial |
391 | Not reported | The overall secondary clinical attack rate was
4.08 (95% CI 1.95–6.20) |
|
| Jia 2020 | Household | Unclear | Not reported | Attack rate 44/583 (7.6%) | |
| Jiang 2020 | Household
Community |
300 | Not reported | 6/300 (2%) | |
| Jing 2020 | Household | Unclear | Not reported | Household contacts 13·2%
Non-household contacts 2·4% |
The risk of household infection was
significantly higher in the older age group (≥60 years) |
| Jing 2020a | Household
Community |
Unclear | Not reported | Close contacts 17.1% to 19%
Family members 46.1% to 49.6% |
|
| Jones 2020 | Local | 128 | Not reported | 6/128 (4.7%) | |
| Kang 2020 | Local | 5517 | Not reported | 96/5517 (1.7%) | |
| Kant 2020 | Local
Community Nosocomial |
Not reported | Not reported | Not reported | No details on number of contacts for index case |
| Kawasuji 2020 | Nosocomial | 105 | Not reported | 14/105 (1.33%) | |
| Khanh 2020 | Community | 217 | Not reported | 16/217 (7.4%) | |
| Kim 2020 | Household | 207 | 17.7 to 30 | 1/207 (0.5%) | |
| Kim 2020a | Household
Community |
4 | 18.7 to 32.1 | N/A | |
| Kim 2020b | Nosocomial | 3,091 respiratory samples from 2,924
individuals |
Not reported | 3/290 (1%) | |
| Kumar 2020 | Community | 822 | Not reported | 144/822 17.5%) | Spread of infection within the state was
significantly higher from symptomatic cases, p=0.02 |
| Kuwelker 2020 | Household | 179 | N/A | 45% | The elderly (>60 years old) had a significantly
higher attack rate (72%) than adults< 60years old (46%, p=0·045) |
| Kwok 2020 | Local
Household |
206 | Not reported | 24/206 (11.7%) | |
| Ladhani 2020 | Nosocomial | 254 | Not reported | Unclear: 53/254 (21%) tested positive. | Staff working across different care homes
(14/27, 52%) had a 3.0-fold (95% CI, 1.9–4.8; P<0.001) higher risk of SARS-CoV-2 positivity than staff working in single care homes (39/227, 17%). |
| Ladhani 2020a | Nosocomial | Residents: 264
Staff members: 254 |
Not specified | Unclear: 105/264 (53%) residents tested positive | Infectious virus recovery in asymptomatic
staff and residents emphasises their likely importance as silent reservoirs and transmitters of infection and explains the failure of infection control measures which have been largely based on identification of symptomatic individuals. |
| Laws 2020 | Household | 188 | Not reported | 55/188 (29.3%) | |
| Laxminarayan 2020 | Local
Household Community |
575,071 | Not reported | 10.7% (10.5 to 10.9%) for high-risk contacts
4.7% (4.6 to 4.8%) for low-risk contacts 79.3% (52.9 to 97.0%) for high-risk travel exposure |
|
| Lee 2020 | Household | 12 | Not reported | 0/12 (0%) | |
| Lee 2020a | Household | 23 | Not reported | 1/23 (4.4%) | |
| Lewis 2020 | Household | 188 | Not reported | RT-PCR: 55/188 (29%)
Serology: 8/52 (15%) |
|
| Li 2020 | Household | 5 | 19.66 to 26.16 | 4/5 (80%) | |
| Li 2020a | Household
Nosocomial |
7 | Not reported | 7/7 (100%) | During January 14–22, the authors report that
index patient had close contact with 7 persons |
| Li 2020b | Household | 14 | Not reported | 14/14 (100%) | |
| Li 2020c | Household | Unclear | Not reported | Unclear | In COFs, the transmission rates of respiratory
droplets in secondary and non-infected patients were 11.9 % and 66.7 %, respectively, while the transmission rates of respiratory droplets with close contacts were 88.1 % and 33.3 %, respectively. In SOFs, the proportion of respiratory droplet and respiratory droplet transmission with close contacts was 40 % and 60 %, respectively |
| Li 2020d | Household | 392 | Not reported | 64/392 (16.3%) | |
| Liu 2020 | Household | 7 | Not reported | 4/7 (57.1%) | |
| Liu 2020a | Nosocomial | 30 | Not reported | N/A | |
| Liu 2020b | Household
Community Nosocomial |
11580 | Not reported | 515/11580 (4.4%) | |
| Liu 2020c | Unclear | 1150 | Not reported | 47/1150 (4.1%) | The 16 confirmed cases who had previously
been asymptomatic accounted for 236 close contacts, with a second attack rate of 9.7%, while the remaining 131 asymptomatic carriers accounted for 914 close contacts, with a second attack rate of 2.6% (p<0.001) |
| López 2020 | Local
Household |
285 | Not reported | Facility SAR: 22/101 (21.8%)
Overall SAR: 38/184 (20.7%) |
Variation in hygiene procedures across 3
facilities. Facility A required daily temperature and symptom screening for the 12 staff members and children and more frequent cleaning and disinfection; staff members were required to wear masks. Facility B: temperatures of the five staff members and children were checked daily, and more frequent cleaning was conducted; only staff members were required to wear masks. Facility C: 84 staff members and children check their temperature and monitor their symptoms daily; masks were not required for staff members or children. |
| Lopez Bernal 2020 | Household
Community |
472 | Not reported | 37% (95% CI 31–43%) | |
| Lucey 2020 | Nosocomial | Not specified | N/A | Not reported | |
| Luo 2020 | Community | 243 | Not reported | 12/243 (4.9%) | No viral genetic sequence data were available
from these cases to prove linkage; and some of the secondary and tertiary cases could have been exposed to unknown infections, especially asymptomatic ones, before or after the bus trips. |
| Luo 2020a | Household
Community Nosocomial |
3410 | Not reported | 127/3410 (3.7%) | |
| Lyngse 2020 | Household | 2226 | Not reported | 371/2226 (16.7%) | |
| Ma 2020 | Unclear | 1665 | Not reported | 10/1/1665 (0.6%) | Only close contacts who fell ill were tested
(n=10) |
| Macartney 2020 | Local | 633 | Not reported | 18/633 (1.2%)
Serologic attack rates: 8/171 (4.8%) |
|
| Malheiro 2020 | Household | 1627 | Not reported | Overall AR 154/1627 (9.5%) | |
| Maltezou 2020 | Household | Unclear | <25 (28.1%)
25–30 (26.8%) >30 (45.1%) |
Median attack rate 40% (range: 11.1%–100%)
per family. |
|
| Maltezou 2020a | Household | Unclear | Not reported | Median attack rate: 60% (range: 33.4%-100%) | Adults were more likely to develop a severe
clinical course compared to children (8.8% versus 0%, p-value=0.021) |
| Mao 2020 | Household
Local |
Unclear | Not reported | 6.10% | Average attack rate was 8.54% (1.02–100%) |
| Martinez-Fierro 2020 | Unclear | 81 | Not reported | 34/81 (42%)
Serologic attack rates: 13/87 (14.9%) |
16% of contact showed positive serology after
>2 weeks |
| Mponponsuo 2020 | Nosocomial | 38 | N/A | 0/38 (0%) | |
| Ng 2020 | Household
Local Community |
13026 | Not reported | 188/7770 (2.4%)
Household: 5·9% Work contacts: 1.3% Social contacts: 1.3% Serology: 44/1150 (3.8%) |
Serology results were positive for 29 (5·5%)
of 524 household contacts, six (2·9%) of 207 work contacts, and nine (2·1%) of 419 social contacts. |
| Ning 2020 | Household
Local Community |
Unclear | Not reported | Imported cases: 69/3435 (0.8%)
Local cases: 31/3666 (2.0%) |
|
| Njuguna 2020 | Local | 98 | Not reported | Attack rate 57% to 82% | |
| Ogawa 2020 | Nosocomial | 30 PCR/serology | 33.53 to 36.83 | 0/15 (0%) for both PCR and serology | |
| Paireau 2020 | Household
Local Nosocomial |
6028 | Not reported | 248/6028 (4.1%) | Family contacts, index case was 60–74, or
older than 75 years old were significantly associated with increased odds of transmission. The proportion of nosocomial transmission was significantly higher than in contact tracing (14% vs 3%, p<0.001) |
| Park 2020 | Local
Household Community |
328 | 17.7 to 35 | 22/328 (6.7%) | |
| Park 2020a | Household
Non-household |
59,073 | Not reported | Household contacts: 11.8% (95% CI 11.2%–
12.4%) Non-household contacts: 1.9% (95% CI 1.8%–2.0%) |
|
| Park 2020b | Local
Household |
441 | Not reported | Attack rate 43.5% (95% CI 36.9%–50.4%)
Secondary attack rate 16.2% (95% CI 11.6%– 22.0%) |
|
| Passarelli 2020 | Nosocomial | 6 | Not reported | 2/6 (33.3%) | |
| Patel 2020 | Household | 185 | Not reported | 79/185 (43%) | Contacts not reported as tested |
| Pavli 2020 | Aircraft | 891 | Not reported | 5/891 (0.6%) | |
| Phiriyasart 2020 | Household | 471 | Not reported | 27/471 (5.7%) | |
| Poletti 2020 | Unclear | 2484 | Not reported | 2824/5484 (51.5%) | |
| Pung 2020 | Local
Community |
425 | Not reported | 36/425 (8.5%) | |
| Pung 2020a | Household | Unclear | Not reported | 43/875 (4.9%) | |
| Qian 2020 | Local
Household Community |
Not reported | Not reported | Not reported | Home‐based outbreaks were the dominant
category (254 of 318 outbreaks; 79.9%), followed by transport‐based outbreaks (108; 34.0%) |
| Ravindran 2020 | Local | Not reported | Not reported | Attack rate 61% to 77% | All attendees participated in activities resulting
in potential exposure, such as shaking hands, kissing, dancing, sharing drinks and sharing shisha (smoking water pipes). |
| Razvi 2020 | Nosocomial | 2521 | Not reported | Serologic attack rate 19.4% | |
| Rosenberg 2020 | Household | 498 | Not reported | 286/498 (57%) | |
| Roxby 2020 | Nosocomial | 142 | Not reported | Attack rate in 1st round: 5/142 (3.5%) | One additional positive test result was
reported for an asymptomatic resident who had negative test results on the first round. |
| Sang 2020 | Household | 6 | Not reported | 4/6 (66.7%) | |
| Schumacher 2020 | Local | Quarantine phase: 757 tests
Match phase: 1167 tests |
Unclear | Quarantine phase AR: 3.6%
Match phase AR: 4.2% Serology: 1.1% |
|
| Schwierzeck 2020 | Nosocomial | 48 | 16.03 to 32.98 | 9/48 (18.8%) | Ct values of symptomatic cases were
significantly lower compared to asymptomatic cases 22.55 vs 29.94, p<0.007 (approximately 200-fold higher viral load) |
| Shah 2020 | Household | 386 | Not reported | 34/386 (8.8%) | |
| Shen 2020 | Household
Community |
480 | Not reported | Close contact: 2/7 (29%)
Casual contact: 3/473 (0.6%) |
|
| Sikkema 2020 | Nosocomial | 1796 | Not specified. WGS for Ct <32 | Attack rate 96/1796 (5%) | 46 (92%) of 50 sequences from health-care
workers in the study were grouped in three clusters. Ten (100%) of 10 sequences from patients in the study grouped into the same three clusters: |
| Son 2020 | Household | 3223 | Not reported | 8.2% (95% CI, 4.7 to 12.9) | |
| Song 2020 | Household | 20 | Not reported | 16/20 (80%) | |
| Speake 2020 | Aircraft | 111 | Not reported | 11/111 (9.9%) | |
| Stein-Zamir 2020 | Local | 1312 | Not reported | Attack rate 178/1312 (13.6%) | |
| Sugano 2020 | Local | 72 | Not reported | 23/72 (31.9%) | |
| Sun 2020 | Household | Unclear | Not reported | 34.43% | |
| Taylor 2020 | Nosocomial | 600 | Not reported | Resident attack rate: 137/259 (52.9%) 1st round
HCW Attack rate: 114/341 (33.4%) |
|
| Teherani 2020 | Household | 144 | Not reported | 67/144 (46.5%) | Of the total number of household contacts, at
least 29 (20%) had known SARS-CoV2 testing. Child-to-adult transmission was suspected in 7/67 cases (10.5%). |
| Thangaraj 2020 | Community | 26 | Not reported | 17/26 (65.4%) | |
| Torres 2020 | Community | 1244 | N/A | Overall serologic attack rate: 139/1244 (11.2%) | |
| Tshokey 2020 | Local
Community |
1618 | Not reported | 14/1618 (0.9%) | SAR: High-risk contacts was 9.0% (7/75),
and that among the primary contacts was 0.6% (7/1,095), and none (0/448) among the secondary contacts. |
| van der Hoek 2020 | Household | 174 | 25.1 to 35.1 | 47/174 (27%)
Serology on day 3 - family members: 43/148 (29.1%) |
|
| Wang 2020 | Nosocomial
Household |
43 | Not reported | 10/43 (23.3%) | |
| Wang 2020a | Household | 155 | Not reported | 47/155 (30%) | |
| Wang 2020b | Household | 335 | Not reported | 77/335 (23%) | |
| Wee 2020 | Nosocomial | 298 | Not reported | 1/298 (0.3%) | |
| Wendt 2020 | Nosocomial | 254 | Not reported | 0/254 (0%)
Serologic attack rates 0/23 (0%) |
|
| Wolf 2020 | Household | 4 | Not reported | 3/4 (75%) | 7-month old female who was breastfed, was
asymptomatic throughout the observation period and never developed fevers or any other symptoms, despite continuous exposure to her parents and siblings. She remained SARS-CoV-2 PCR-negative in repeat testing of pharyngeal swab and stool specimens over the entire observation period. |
| Wong 2020 | Nosocomial | 76 tests were performed on 52
contacts |
Not reported | 0/52 (0%) | Findings suggest that SARS-CoV-2 is not
spread by an airborne route. Ct value for throat and tracheal aspirate of index case were 22.8 and 26.1 respectively |
| Wood 2020 | Household | Not reporred | Not reported | Not reported | |
| Wu 2020 | Household
Local Community |
2994 | Not reported | 71/2994 (2.4%) | |
| Wu 2020a | Household | 148 | Not reported | 48/148 (32.4%) | |
| Xie 2020 | Household | 56 | Not reported | 0/56 (0%) | |
| Xin 2020 | Household | 187 | Not reported | 19/187 (17.9%) | |
| Yang 2020 | Household
Local |
1296 | Not reported | 0/1296 (0%)
Serologic attack rates: 0/20 (0%) |
Viral culture of 4 specimens with Ct <30 were
negative |
| Yau 2020 | Nosocomial | 330 | Not reported | 22/330 (6.7%) | |
| Ye 2020 | Local
Community |
1293 | Not reported | 39/1,293 (3.02%) | |
| Yoon 2020 | Local | 190 | N/A | 0/190 (0%) | |
| Yousaf 2020 | Household | 198 | Not reported | 47/198 (23.7%) | |
| Yu 2020 | Household | 1587 | Not reported | 150/1587 (9.5%) | |
| Yung 2020 | Household | 213 | Not reported | Attack rate 6.1% | |
| Zhang 2020 | Aircraft | 4492 | Not reported | Attack rate 161/4492 (3.6%) | The authors report attack rate of 0.14% based
on 94 flights (n=14 505); however, only 4492 people were screened |
| Zhang 2020a | Household
Local Community |
369 | Not reported | 12/369 (3.3%, 95% CI 1.9%–5.6%) | |
| Zhang 2020b | Household | 10 | Not reported | 0/10 (0%)
Serologic attack rates: 0/10 (0%) |
|
| Zhang 2020c | Local
Household |
93 | Not reported | 5/93 (5.4%) | |
| Zhang 2020d | Local | 8437 | Not reported | 25/8437 (0.3%) | |
| Zhuang 2020 | Household
Community |
8363 | Not reported | 239/8363 (2.9%) |
Twenty-nine studies reported data on ARs using serology ( Table 6). The settings included educational (n=4), households (n=4) and healthcare (n=3). In eight studies, the frequency of attack was 0%. The frequency of attacks in the remaining 21 studies ranged from 0.7% to 75% ( Figure 3b). The frequency of attacks was highest in households but lower in educational settings - especially daycare centres.
Figure 3b. Primary attack rates of SARS-CoV-2 in close contacts (serology).

Frequency of SARS-CoV-2 secondary ARs
Overall, 126 studies (73.7%) reported data on secondary ARs ( Table 6). The studies reported the rates based on RT-PCR tests, except for one study (Angulo-Bazán 2020) that used serology. In 16 of these studies, the SAR was 0%. The secondary ARs in the remaining 110 studies ranged from 0.3 to 100% (see Figure 4). The highest frequencies of secondary ARs (75–100%) occurred in household or quarantine settings; similar findings were observed when studies with higher reporting quality were examined (57–75%). In the three studies of index or primary cases with recurrent infections, there was no positive case amongst the 1518 close contacts across the studies.
Figure 4. Frequency of secondary attack rates of SARS-CoV-2 with Close Contacts.

Risk of infection
Forty-six studies (26.9%) reported results on the risk of infection ( Table 7). One study of airline passengers (Khanh 2020) showed that seating proximity was significantly associated with the risk of contracting SARS-CoV-2 (RR 7.3, 95% CI 1.2–46.2); a second study (Speake 2020) reported that not sitting by the window was associated with a significantly increased risk of infection (RR 5.2; 95% CI 1.6–16.4; p<0.007)). The results of five studies (Chen 2020b, Doung-ngern 2020, Hobbs 2020, Wang 2020b, Wu 2020) showed that use of face covering during close contact with infected cases was associated with significantly lower risks of infection compared with no face covering; findings from one of these studies (Doung-ngern 2020) showed that wearing masks all the time during contact was not significantly different from wearing masks sometimes. The result of one study (Rosenberg 2020) showed that the incidence of infection significantly increased with age (p<0.0001), while those from another study (Poletti 2020) showed that being 70 years or older was associated with a significantly increased risk of SARS-CoV-2-related death (p<0.001), while another study (Zhang 2020a) reported that elderly close contacts (≥60 years) had a higher SAR compared with younger age groups. Findings from five studies (Bi 2020, Hu 2020a, Islam 2020, Luo 2020a, Wu 2020, Zhang 2020a) showed that household contact settings had significantly higher risks of infection compared with other types of contact settings, e.g., social, healthcare, workplace and public transport. One study (Lewis 2020) showed that the risk of infection was significantly increased amongst household contacts who were immunocompromised (OR 15.9, 95% CI 2.4–106.9). Finally, three studies (Bi 2020a, Wu 2020, Zhang 2020a) showed that the more frequent contacts with an index case was significantly associated with an increased risk of infection.
Table 7. Risk of infection in close contacts.
| Study ID | Type of
transmission |
Risk of infection |
|---|---|---|
| Abdulrahman 2020 | Community | Eid Alfitr: Pre-: 2990 (4.2%); Post-: 4987 (6.7%); p <0.001; Ashura: Pre-: 3571 (3.7%); Post-: 7803 (6.6%); p <0.001 |
| Arnedo-Pena 2020 | Household | The health profession of index case was a significant protective factor (p<0.007). Older age of secondary cases, two household members, and
higher age of index case were significantly associated with elevated risk of infection: p<0.001 in each case |
| Bi 2020 | Local
Household Community |
Household contact (OR 6·3; 95% CI 1·5–26·3) and travelling together (OR 7·1; 1·4–34·9) were significantly associated with infection. Reporting
contact that occurred often was also associated with increased risk of infection compared with moderate-frequency contact (OR 8·8; 95% CI 2·6–30·1) |
| Chen 2020b | Nosocomial | In multivariate analysis, there existed higher risk of seroconversion for close contacts with patient 2 (OR, 6.605, 95% CI, 1.123, 38.830) and
doctors exposed to their patient (OR, 346.837, 95% CI 8.924, 13479.434), while the lower risk of seroconversion was closely related to direct contact with COVID-19 patients wearing face mask (OR, 0.127, 95% CI 0.017, 0.968). |
| Chen 2020c | Local
Community Household Nosocomial |
Infection rate is highest when living with the case (13.26%), followed by taking the same means of transportation (11.91%). After removing
the influence factors of the "super spreader" incident, the infection rate of vehicle contact dropped to 1.80%. The infection rate (7.18%) of entertainment activities such as gatherings, meeting guests, and playing cards was also relatively high, as was short-term face-to-face unprotected conversations or doing errands (6.02%). There was a statistically significant difference in the infection rate among the four categories of life contact, transportation contact, medical contact, and other contact (p<0.005). participation in Buddhist gatherings caused transmission. A total of 28 people were diagnosed as confirmed cases of new coronavirus pneumonia, 4 were asymptomatic infections, and the infection rate of close contacts reached 32.99% (32/97), which was much higher than the average infection rate (6.15). %), the difference is statistically significant (p<0.005). |
| Cheng 2020 | Household
Nosocomial |
The overall secondary clinical attack rate was 0.7% (95% CI, 0.4%-1.0%). The attack rate was higher among the 1818 contacts whose exposure
to index cases started within 5 days of symptom onset (1.0% [95% CI, 0.6%-1.6%]) compared with those who were exposed later (0 cases from 852 contacts; 95% CI, 0%-0.4%). The 299 contacts with exclusive presymptomatic exposures were also at risk (attack rate, 0.7% [95% CI, 0.2%-2.4%]). The attack rate was higher among household (4.6% [95% CI, 2.3%-9.3%]) and nonhousehold (5.3% [95% CI, 2.1%-12.8%]) family contacts than that in health care or other settings. The attack rates were higher among those aged 40 to 59 years (1.1% [95% CI, 0.6%-2.1%]) and those aged 60 years and older (0.9% [95% CI, 0.3%-2.6%]). |
| Chu 2020a | Household | Five (10%) of 48 secondary cases compared with 130 (33%) of 398 non-case household contacts reported potential community exposures:
unadjusted OR 0.24 (95%CI 0.09 to 0.62), p=0.003 |
| Dattner 2020 | Household | PCR: 44% of adults were infected compared to 25% of the children (n=3353: 1809 children and 1544 adults)
Serology: 34% of these children and 48% of the adults tested serologically positive (n=705: 417 children and 288 adults |
| Dimcheff 2020 | Community
Nosocomial Household |
HCWs exposed to a known COVID-19 case outside work had a significantly higher seroprevalence at 14.8% (23 of 155) compared to those who
did not 3.7% (48 of 1,296; OR, 4.53; 95% CI, 2.67–7.68; P < 0.0001) |
| Doung-ngern 2020 | Local | Wearing masks all the time during contact was independently associated with lower risk of COVID-19 infection compared to not wearing
masks (aOR 0.23, 95% CI 0.09–45 0.60), while wearing masks sometimes during contact was not (aOR 0.87, 95% CI 0.41–1.84). Maintaining at least 1m distance from a COVID patient (aOR 0.15, 95% CI 0.04–0.63) and duration of close contact ≤15 minutes versus longer (aOR 0.24, 95% CI 0.07–0.90) were significantly associated with lower risk of infection transmission |
| Fateh-Moghadam 2020 | Community | Workplace exposure was associated with higher risk of becoming a case than cohabi_x0019_ng with a case or having a non-cohabiting family
member or friend who was a case. The greatest risk of transmission to contacts was found for the 14 cases <15 years of age (22.4%); 8 of the 14, who ranged in age from <1 to 11 years) infected 11 of 49 contacts. |
| Fontanet 2020a | Local | No significant difference in attack rates across primary school pupils, teachers, non-teaching staff, parents, and relatives, respectively (p=0.29). |
| Helsingen 2020 | Local | 11 individuals in the training arm (0.8% of those tested) and 27 in the non-training arm (2.4% of those those tested) tested positive for SARS-
CoV-2 antibodies (p=0.001) |
| Hobbs 2020 | Local
Household Community |
Case-patients were significantly more likely to have had close contact with a person with known COVID-19 than control participants (aOR = 3.2,
95% CI = 2.0–5.0) Case-patients were significantly more likely to have attended gatherings with persons outside their household, including social functions (aOR = 2.4, 95% CI = 1.1–5.5), activities with children (aOR = 3.3, 95% CI = 1.3–8.4), or to have had visitors at home (aOR = 1.9, 95% CI = 1.2–2.9) during the 14 days before the SARS-CoV-2 test. Parents of 64% of case-patients and 76% of control participants reported that their child and all staff members wore masks inside the facility (aOR = 0.4, 95% CI = 0.2–0.8). |
| Hu 2020 | Household
Community |
Household contacts were associated with a significantly larger risk of SARS-CoV-2 infection than other types of contact (P<0.001).
The transmission risk in the first generation was significantly higher than the later generations (p<0.001), possibly due to improved case isolation and contacts quarantine that deplete the number of susceptible individuals in the cluster. |
| Hua 2020 | Household | Incidence of infection in child close contacts was significantly lower than that in adult contacts: 13.2% vs 21.2%, p=0.004 |
| Islam 2020 | Household
Local Community Nosocomial |
The secondary attack rate among household contacts was at the highest risk of attack (13.04%, 95% CI 9.67-16.41) followed by funeral
ceremonies (8.33%, 95% CI 3.99-12.66) and family contacts (6.52%, 95% CI 4.02-9.02). The attack rate was higher in age groups 50–59 (10.89%, 95% CI 7.05-14.66) and 60–69 (9.09%, 95% CI 5.08-13.09) |
| Kawasuji 2020 | Nosocomial | Among symptomatic patients (n =18), the estimated viral load at onset was higher in the index than in the non-index patients (median [95%
confidence interval]: 6.6 [5.2–8.2] vs. 3.1 [1.5–4.8]. In adult (symptomatic and asymptomatic) patients (n = 21), median viral load at the initial sample collection was significantly higher in the index than in the non-index patients (p = 0.02) |
| Khanh 2020 | Community | Seating proximity was strongly associated with increased infection risk (RR 7.3, 95% CI 1.2–46.2). |
| Laws 2020 | Household | There were no significant differences in secondary infection rates between adult and pediatric contacts among all households (OR: 1.11; 95%
CI: 0.56 to 2.21) or among households with children (OR: 0.99; 95% CI: 0.51 to 1.90). |
| Laxminarayan 2020 | Local
Household Community |
Secondary attack rate estimates ranged from 1.2% (0.0 to 5.1%) in health care settings to 2.6% (1.6 to 3.9%) in the community and 9.0% (7.5 to
10.5%) in the household. |
| Lewis 2020 | Household | Household contacts to COVID-19 patients with immunocompromised conditions and household contacts who themselves had diabetes
mellitus had increased odds of infection with ORs 15.9 (95% CI, 2.4–106.9) and 7.1 (95% CI: 1.2–42.5). Household contacts of a male primary patient were more likely to have secondary infection than those of a female primary patient (SIR, 36% vs 18%; OR, 2.4; 95% CI, 1.1–5.3). |
| Li 2020d | Household | The secondary attack rate to children (aged <18 years) was 4% compared with 20.5% for adult members (odds ratio [OR], .18; 95% confidence
interval [CI], .06–.54; P = .002). The secondary attack rate to the contacts in the household with index patients quarantined at home immediately since onset of symptoms was 0% compared with 18.3% for the contacts in the households without index patients quarantined during the period between initiation of symptoms and hospitalization (OR, 0; 95% CI, .00–.00; p=0.000). The secondary transmission rate for individuals who were spouses of index cases was 27.8% compared with 17.3% for other members in the households (OR, 2.27; 95% CI, 1.22–4.22; p=0.010). |
| Liu 2020b | Household
Community Nosocomial |
Compared to young adults aged 20–29 years, the infected risk was higher in children (RR: 2.59, 95%CI: 1.79–3.76), and old people aged 60–69
years (RR: 5.29, 95%CI: 3.76–7.46). People having close relationship with index cases encountered higher infected risk (RR for spouse: 20.68, 95%CI: 14.28–29.95; RR for non-spouse family members: 9.55, 95%CI: 6.73–13.55; RR for close relatives: 5.90, 95%CI: 4.06–8.59). Moreover, contacts exposed to index case in symptomatic period (RR: 2.15, 95%CI: 1.67–2.79), with critically severe symptoms (RR: 1.61, 95%CI: 1.00–2.57) |
| Lopez Bernal 2020 | Household
Community |
Secondary attack rates were highest where the primary case was aged <18 years with a significantly higher odds of secondary infection (OR
61, 95% CI 3.3-1133). Where the primary case was admitted to hospital there was a significantly lower odds of secondary infection in the household (OR 0.5, 95% CI 0.2-0.8). Secondary attack rates were lower in larger households. |
| Luo 2020a | Household
Community Nosocomial |
Household contacts had a significantly higher risk for secondary infection than did persons who were exposed in health care settings (OR,
0.09, 95%CI 0.04 to 0.20) or those who were exposed on public transportation (OR, 0.01, 95%CI, 0.00 to 0.08). |
| Macartney 2020 | Local | The rate of staff member to child transmission was lower (1·5%) than staff to staff transmission (4·4%). |
| Malheiro 2020 | Household | Among the intervention cohort,16 of 132 closecontacts tested positive during the follow-up period (attack rate:12.1%, 95% confidence interval
[CI]: 7.1-18.9). In the control cohort,138 of 1495 participants tested positive (attack rate: 9.2%, 95% CI:7.8-10.8) |
| Park 2020a | Household
Non-household |
With index patients 30–39 years of age as reference, detection of COVID-19 contacts was significantly higher for index patients >40 years of
age in nonhousehold settings. |
| Phiriyasart 2020 | Household | Locally religious and household contacts of confirmed cases had significantly higher risks of SARS-CoV-2 infection than other community
members. |
| Poletti 2020 | Unclear | Individuals younger than 70 years were at a significantly lower risk of death after infection than older patients (p<0.001). The risk of death was
62% lower (95% CI: 31–80%; p<0.001) during the second phase of the epidemic. |
| Razvi 2020 | Nosocomial | HCWs in patient facing roles had a significantly higher frequency of positive COVID-19 antibody tests (295/1302 [22.7%]) than those in non-
patient facing roles (88/669 [13.2%]), p<0.0001) |
| Rosenberg 2020 | Household | Prevalence significantly increased with age, ranging from 23% among those aged <5 years to 68% among those 65 years or older (p<0.0001) |
| Speake 2020 | Aircraft | The risk for secondary infections among passengers seated in the mid cabin was significantly greater than for those seated in the aft cabin
(p<0.005). The SAR among mid-cabin passengers in window seats was significantly greater than among those not in window seats (RR 5.2; 95% CI 1.6–16.4; p<0.007). |
| Sun 2020 | Household | The family recurrence rate of spouses who introduced cases from the family was 63.87%, which was higher than the recurrence rate of
children (30.53%), parents (28.37%) and other family members (20.93%), and the difference was statistically significant ( P <0.001) . |
| Torres 2020 | Community | Antibody positivity rates were 9.9% (95%CI: 8.2-11.8) for 1,009 students and 16.6% (95%CI: 12.1-21.9) for 235 staff. Among students, positivity
was significantly associated with history of contact with a confirmed case (p<0.0001). The greater the number of contacts, the greater the probability that a child was antibody positive (p=0.05). |
| van der Hoek 2020 | Household | In families of a confirmed COVID-19 patient, children between 1 and 11 years were less often positive in PCR and serology than older children
and adults. |
| Wang 2020b | Household | Face mask use by the primary case and family contacts before the primary case developed symptoms was 79% effective in reducing
transmission (OR=0.21, 95% CI 0.06 to 0.79). Daily use of chlorine or ethanol based disinfectant in households was 77% effective (OR=0.23, 95% CI 0.07 to 0.84). Wearing a mask after illness onset of the primary case was not significantly protective. The risk of household transmission was 18 times higher with frequent daily close contact with the primary case (OR=18.26, 95% CI 3.93 to 84.79), and four times higher if the primary case had diarrhoea (OR=4.10, 95% CI 1.08 to 15.60). Household crowding was not significant. |
| Wood 2020 | Household | Households without children had a significantly lower rate of COVID-19: HR per child 0.89; 95% CI 0.84–0.95. Households with childen had
higher rates of COVID-19 tests (9.2% vs 6.1%) Compared to those in households without children, the risk of COVID-19 requiring hospitalisation was lower in those with one child and lower still in those with two or more children: HR 0.72 per child (95% CI 0.60-0.85, p<0.001); adjusted for age - HR 0.83 per child (95% CI 0.70-0.99) |
| Wu 2020 | Household
Local Community |
Contacts living in the same household as the index case had significantly higher risk of infection vs those who had only had brief contact with
the index case: RR 41.7 (17.7–98.5), p<0.001). Contacts who had visited, or had contact with the index case in a medical institution had significantly higher risk of acquiring infection vs brief contact with the index case: RR 3.6 (1.42–8.98), p=0.004. Family members who had contact with an index case had significantly higher risk of infection vs healthcare providers or other patients who had been exposed to an index case: RR 31.6 (7.69–130.01), p<0.001. Those who had contact with the index case through work, through study, or in a place of entertainment had a significantly higher risk of infection vs those who had contact with the index case in a medical institution: RR 6.7 (1.34–33.25), p=0.01. Those who had contact with the index case in or near his/her home had a significantly higher risk of infection vs those who had contact with the index case in a medical institution: RR 17.3 (4.20–70.77), p<0.001. The incidence rate among those who wore face masks was significantly lower than that among those who did not use protective measures (0.3% vs. 4.7%, respectively, p<0.001). The incidence rate of contacts with data collected by field investigation was significantly higher than that of contacts with data collected by big data (5.35% versus 0.07%, p<0.001). |
| Wu 2020a | Household | Contacts with >72 hours of exposure (SIR, 41.7%; [95% CI: 26.8%–58.3%]) had a higher SIR compared with those without (SIR, 23.2%; [95% CI:
11.4%–41.5%]). One household-level factor was significantly associated with SIR: household members without protective measures after illness onset of the index patient (odds ratio [OR], 4.43; [95% CI: 1.37–14.34]). |
| Xin 2020 | Household | Increasing risk of infection among household contacts with female index patients (adjusted hazard ratio [aHR] = 3.84, 95% CI = 1.07–13.78),
critical disease index patients (aHR = 7.58, 95% CI = 1.66–34.66), effective contact duration with index patients > 2 days (aHR = 4.21, 95% CI = 1.29–13.73), and effective contact duration > 11 days (aHR = 17.88, 95% CI = 3.26–98.01) |
| Yu 2020 | Household | Family members, colleagues/classmates/travel companions, and doctors-patients accounted for 88.1% (1398), 10.7% (170), and 0.3% (5),
respectively. Following this order, the infection rate was 10.2%, 1.8% and 40.0%, respectively. |
| Yung 2020 | Household | Young children <5 years old were at lowest risk of infection (1.3%). Children were most likely to be infected if the household index case was the
mother. |
| Zhang 2020a | Household
Local Community |
SAR among household contacts was 16.1% vs 1.1% for social contacts, and 0% for workplace contacts.
Older close contacts had the highest SAR compared with other age groups; 8.0% in persons >60 years of age compared with 1.4%–5.6% in persons <60 years of age. Close contacts that lived with an index case-patient had 12 times the risk for infection and those who had frequent contact with an index case- patient, >5 contacts during 2 days before the index case was confirmed, had 29 times the risk for infection. |
| Zhuang 2020 | Household
Community |
The main sources of secondary infection were family exposure (74.5%, 178 cases), transportation exposure accounted for 8.4% (20 cases),
friend/colleague meal exposure accounted for 5.9% (14 cases). Shopping malls, markets, pharmacies and other public place exposure accounted for 5.0% (12 cases), workplace exposure accounted for 3.8% (9 cases), and community exposure accounted for 2.5% (6 cases). |
Viral culture
Three studies (Ladhani 2020a, Speake 2020, Yang 2020) performed viral culture ( Table 8). All studies utilised Vero E6 cells for viral culture. In Ladhani 2020a (a study of elderly nursing home residents), positive samples with a Ct of <35 were incubated on Vero E6 cells and confirmed by cytopathic effect (CPE) up to 14 days post-inoculation. Positive culture results were obtained for symptomatic, post-symptomatic, pre-symptomatic and asymptomatic cases (21 residents and 12 staff); higher Ct values was significantly associated with decreasing ability to recover the virus (p<0.001). Among residents the virus was isolated 12 days before symptom onset and up to 13 days after and in staff up to 6 days before and 7 days after symptom onset. In Speake 2020, specimens were inoculated in Vero-E6 cells and inspected for CPE daily for up to 10 days with identity confirmed using “in-house” PCRs. The primary cases had boarded the flight from a cruise ship and had SARS-CoV-2 with the strain A2-Ruby Princess (A2-RP). Nine of 17 (53%) of PCR-positive samples grew SARS-CoV-2 in culture. Eight secondary cases who were in the same flight cabin with the infected travellers from the cruise ship all had viruses of the A2-RP strain (3 by full and 1 by partial sequence) ( Table 8). In the third study of index patients with recurrent infection swab specimens were also inoculated on Vero cells, and monitored for CPE daily for 10 days (Yang 2020). All four viral cultures were negative (0%).
Table 8. Results of viral cultures.
| Study ID | Types of participants | Method used for viral culture | Results of viral culture |
|---|---|---|---|
| Ladhani 2020a | Staff and residents of 6 London
care homes |
All SARS-CoV-2 positive samples with a Ct value of
>35 were incubated on Vero E6 mammalian cells and virus detection was confirmed by cytopathic effect (CPE) up to 14 days post-inoculation |
87 samples with Ct values <35 were cultured and infectious virus
was recovered from all (21 residents and 12 staff). Live virus was isolated up to 13 days after and 12 days before symptom onset among residents and up to 6 days before and 7 days after symptom onset among staff. Higher Ct values was significantly associated with decreasing ability to recover infectious virus (p<0.001). There were no significant differences in virus recovery rates between symptomatic and asymptomatic residents (5/17 [29.4%] vs. 14/33 [42.4%]; P = 0.37) and staff (2/6 [33.3%] vs. 10/31 [32.3%]; P = 0.96) at the time of testing. |
| Speake 2020 | 241 airline passengers some
of whom had disembarked from 1 of 3 cruise ships that had recently docked in Sydney Harbour. 6 primary cases initially |
Virus culture was attempted for primary samples .
Clinical specimens were inoculated in triplicate wells with Vero-E6 cells at 80% confluency, incubated at 37°C in 5% CO2, and inspected for cytopathic effect daily for up to 10 days. Identity was confirmed by in-house PCRs as described for previous sequences. |
9/17 of PCR positive samples grew SARS-CoV-2 on viral culture.
Sufficient viral RNA was available to generate an adequate sequence for 25 of the 29 samples positive by PCR. 11 passengers had PCR-confirmed SARS-CoV-2 infection and symptom onset within 48 hours of the flight. All 11 passengers had been in the same cabin with symptomatic persons who had culture- positive A2-RP virus strain. |
| Yang 2020 | Home quarantine: 93 recurrent-
positive patients; 96 close contacts and 1,200 candidate contacts |
Vero-E6 cells were used for virus isolation in a BSL-
3 laboratory. |
Viral culture of 4 specimens with Ct <30 were negative |
Genome sequencing (GS) and phylogenetic analysis
Ten studies (Böhmer 2020, Firestone 2020, Jiang 2020, Ladhani 2020a, Lucey 2020, Pung 2020, Sikkema 2020, Speake 2020, Taylor 2020, Wang 2020) performed GS and phylogenetic analysis ( Table 9). The studies were primarily conducted in outbreak clusters and methods used for performing these investigations were essentially similar across the studies. The completeness of genomic similarity ranged from 81–100% across six studies (Firestone 2020, Jiang 2020, Lucey 2020, Sikkema 2020, Speake 2020, Wang 2020). Transmission from one case to a contact was demonstrated by nonsynonymous nucleotide polymorphism in SARS-CoV-2 from these two cases onwards, but not in any cases detected prior to this instance (Böhmer 2020). In one study of skilled nursing home facilities (Taylor 2020), samples from 75 residents and five healthcare staff shared genetically related strains. In another study of care homes (Ladhani 2020a), reported nine separate introductions of SARS-CoV-2 into care homes by healthcare staff. In one study which used multiple settings (Pung 2020), the viral genomic sequences for four cases in one cluster shared identical sequences over the full genome length and shared a common base difference relative to the earlier sequences (see Table 8).
Table 9. GS and phylogenetic analysis.
| Study ID | Study Setting | Method used for WGS | Phylogenetic analysis | Results |
|---|---|---|---|---|
| Böhmer 2020 | Home, workplace | Whole genome sequencing involved
Roche KAPA HyperPlus library preparation and sequencing on Illumina NextSeq and MiSeq instruments as well as RT-PCR product sequencing on Oxford Nanopore MinION using the primers described in Corman and colleagues. Patient 1 was sequenced on all three platforms; patients 2–7 were sequenced on Illumina NextSeq, both with and without RT-PCR product sequencing with primers as in Corman and colleagues; and patients 8–11, 14, and 16 were sequenced on Oxford Nanopore MinION. Sequencing of patient 15 was not successful. Sequence gaps were filled by Sanger sequencing. |
Not reported | Presymptomatic transmission from patient 4 to patient 5 was strongly
supported by virus sequence analysis: a nonsynonymous nucleotide polymorphism (a G6446A substitution) was found in the virus from patients 4 and 5 onwards but not in any cases detected before this point (patients 1–3). Later cases with available specimens, all containing this same substitution, were all traced back to patient 5. The possibility that patient 4 could have been infected by patient 5 was excluded by detailed sequence analysis: patient 4 had the novel G6446A virus detected in a throat swab and the original 6446G virus detected in her sputum, whereas patient 5 had a homogeneous virus population containing the novel G6446A substitution in the throat swab. |
| Firestone 2020 | Motorcycle rally | WGS was conducted at the MDH Public
Health Laboratory on 38 specimens using previously described methods. |
Phylogenetic relationships,
including distinct clustering of viral whole genome sequences, were inferred based on nucleotide differences via IQ-TREE using general time reversible substitution models as a part of the Nextstrain workflow. |
38 (73%) specimens (23 [61%] from primary and 15 [39%] from secondary
and tertiary cases) were successfully sequenced, covering at least 98% of the SARS-CoV-2 genome. Six genetically similar clusters with known epidemiologic links were identified (i.e., cases in patients who were close contacts or who had common exposures at the rally), five of which demonstrated secondary or secondary and tertiary transmission. |
| Jiang 2020 | Home | Positive samples were sequenced directly
from the original specimens as previously described. *Reference virus genomes were obtained from GenBank using Blastn with 2019- nCoV as a query. The open reading frames of the verified genome sequences were predicted using Geneious (version 11.1.5) and annotated using the Conserved Domain Database. Pairwise sequence identities were also calculated using Geneious. Potential genetic recombination was investigated using SimPlot software and phylogenetic analysis. |
The maximum likelihood
phylogenetic tree of the complete genomes was conducted by using RAxML software with 1000 bootstrap replicates, employing the general time-reversible nucleotide substitution model. |
The full genome of 8 patients were >99.9% identical across the whole
genome. Phylogenetic analysis showed that viruses from patients were clustered in the same clade and genetically similar to other SARS-CoV-2 sequences reported in other countries. |
| Ladhani 2020a | Care homes | Whole genome sequencing (WGS) was
performed on all RT-PCR positive samples. Viral amplicons were sequenced using Illumina library preparation kits (Nextera) and sequenced on Illumina short-read sequencing machines. Raw sequence data was trimmed and aligned against a SARS- CoV-2 reference genome (NC_045512.2). A consensus sequence representing each genome base was derived from the reference alignment. |
Consensus sequences were
assessed for quality, aligned using MAFFT (Multiple Alignment using Fast Fourier Transform, version 7.310), manually curated and maximum likelihood phylogenetic trees derived using IQtree (version 2.04). |
All 158 PCR positive samples underwent WGS analysis and 99 (68
residents, 31 staff) distributed across all the care homes yielded sequence sufficient for WGS analysis. Phylogenetic analysis identified informal clusters, with evidence for multiple introductions of the virus into care home settings. All care home clusters of SARS-CoV-2 genomes included at least one staff member, apart from care home B with no PCR positive staff and high rates of staff self-isolation. Care home A exhibited three distinct sequence clusters and six singletons, potentially representing up to nine separate introductions. Genomic analysis did not identify any differences between asymptomatic/symptomatic residents/staff. The 10 sequences from residents who died were distributed across the lineages identified and were closely matched to sequences derived from non-fatal cases in the same care homes. |
| Lucey 2020 | Hospital | Complementary DNA was obtained from
isolated RNA through reverse transcription and multiplex PCR according to the protocol provided by the Artic Network initiative. Libraries were prepared using the NEBNext Ultra II kit (New England Biolabs) and sequenced on an Illumina MiSeq using 300-cycle v2 reagent kits (Illumina). Bowtie 2 was used for aligning the sequencing reads to the reference genome for SARS-CoV-2 (GenBank number, MN908947.3) and SAMtools for manipulating the alignments. |
SNPs were used to define
clusters and a median-joining network was generated including these data from this study and an additional 1,000 strains collected from GISAID available on May 22nd. Clade annotation was included for the Pangolin, GISAID and NextStrain systems. |
WvGS identified six clusters of nosocomial SARS-CoV-2 transmission. The
average sequence quality per samples was > 99% for 46 samples, and between 92 and 94% for 4 samples. Phylogenetic analysis identified six independent groups of which clusters 1–3 were related to 39 patients. |
| Pung 2020 | Multiple:
Company conference, church, tour group. |
Strain names, GISAID EpiCoV accession
numbers used for genomic sequencing |
Phylogenetic tree utilised the
Neighbor-Joining method and confirmed using Maximum Likelihood approaches. Replicate trees with bootstrap used. All ambiguous positions were removed for each sequence pair (pairwise deletion option). Evolutionary analyses were conducted in MEGA X. Strain names, GISAID EpiCoV accession numbers and collection dates are shown, followed by the case number if available. |
Cluster A: Viral genomic sequences were available for four cases (AH1,
AH2, AH3, and AT1) and phylogenetic analysis confirmed their linkage, as suggested by the epidemiological data. |
| Sikkema 2020 | Hospital | Samples were selected based on a Ct
<32. A SARS-CoV-2-specific multiplex PCR for nanopore sequencing was done. The resulting raw sequence data were demultiplexed using qcat. Primers were trimmed using cutadapt,17 after which a reference-based alignment to the GISAID (Global Initiative on Sharing All Influenza Data) sequence EPI_ISL_412973 was done using minimap2. The consensus genome was extracted and positions with a coverage less than 30 reads were replaced with N using a custom script using biopython software (version 1.74) and the python module pysam (version 0.15.3). Mutations in the genome were confirmed by manually checking the alignment, and homopolymeric regions were manually checked and resolved, consulting the reference genome. Genomes were included when having greater than 90% genome coverage. All available full-length SARS-CoV-2 genomes were retrieved from GISAID20 on March 20, 2020 (appendix 1 pp 8–65), and aligned with the newly obtained SARS-CoV-2 sequences in this study using the multiple sequence alignment software MUSCLE (version 3.8.1551). Sequences with more than 10% of N position replacements were excluded. The alignment was manually checked for discrepancies, after which the phylogenomic software IQ-TREE (version 1.6.8) was used to do a maximum- likelihood phylogenetic analysis, with the generalised time reversible substitution model GTR+F+I+G4 as best predicted model. The ultrafast bootstrap option was used with 1000 replicates. Clusters were ascertained based on visual clustering and lineage designations. |
The code to generate
the minimum spanning phylogenetic tree was written in the R programming language. Ape24 and igraph software packages were used to write the code to generate the minimum spanning tree, and the visNetwork software package was used to generate the visualisation. Pairwise sequence distance (used to generate the network) was calculated by adding up the absolute nucleotide distance and indel- block distance. Unambiguous positions were dealt with in a pairwise manner. Sequences that were mistakenly identified as identical, because of transient connections with sequences containing missing data, were resolved. |
46 (92%) of 50 sequences from health-care workers in the study were
grouped in three clusters. Ten (100%) of 10 sequences from patients in the study grouped into the same three clusters: |
| Speake 2020 | Aircraft | Processed reads were mapped to the
SARS-CoV-2 reference genome (GenBank accession no. MN908947). Primer- clipped alignment files were imported into Geneious Prime version 2020.1.1 for coverage analysis before consensus calling, and consensus sequences were generated by using iVar version 1.2.2. |
Genome sequences of SARS-
CoV-2 from Western Australia were assigned to lineages by using the Phylogenetic Assignment of Named Global Outbreak LINeages (PANGOLIN) tool ( https://github.com/cov-lineages/pangolinExternal Link). On July 17, 2020, we retrieved SARS-CoV-2 complete genomes with corresponding metadata from the GISAID database. The final dataset contained 540 GISAID whole-genome sequences that were aligned with the sequences from Western Australia generated in this study by using MAFFT version 7.467. Phylogenetic trees were visualized in iTOL (Interactive Tree Of Life, https:// itol.embl.deExternal Link) and MEGA version 7.014. |
100% coverage was obtained for 21 and partial coverage (81%–99%) for 4
samples. The phylogenetic tree for the 21 complete genomes belonged to either the A.2 (n = 17) or B.1 (n = 4) sublineages of SARS-CoV-2 |
| Taylor 2020 | Skilled
nursing facilities |
WGS was conducted by MDH-PHL on
available specimens using previously described methods. |
Phylogenetic relationships,
including distinct clustering of viral whole genome sequences, were inferred based on nucleotide differences via IQ-TREE, using general time reversible substitution models |
Specimens from 18 (35%) residents and seven (18%) HCP at facility A
were sequenced - Strains from 17 residents and five HCP were genetically similar. At facility B, 75 (66%) resident specimens and five (7%) HCP specimens were sequenced, all of which were genetically similar. |
| Wang 2020 | Home | Full genomes were sequenced using the
BioelectronSeq 4000. WGS integrated information from 60 published genomic sequences of SARS-CoV-2. Full-length genomes were combined with published SARS-CoV-2 genomes and other coronaviruses and aligned using the FFT- NS-2 model by MAFFT. |
Maximum-likelihood
phylogenies were inferred under a generalised-time-reversal (GTR)+ gamma substitution model and bootstrapped 1000 times to assess confidence using RAxML. |
The phylogenetic tree of full-length genomes showed that SARS-CoV-2
strains form a monophyletic clade with a bootstrap support of 100%. Sequences from six HCWs in the Department of Neurosurgery and one family member were closely related in the phylogenetic tree. 33 family members of the HCWs were not secondarily infected, due to the strict self-quarantine strategies taken by the HCWs immediately after their onset of illness, including wearing a facial mask when they came home, living alone in a separated room, never eating together with their families. |
Discussion
Summary of main findings
We identified 171 primary studies assessing the role of close contact in transmission of SARS-CoV-2. The evidence from these observational studies suggest that the risk of transmission is significantly increased through close contact with an infected case - the greater the frequency of contact, the greater the risk. Household contact setting is significantly more likely to result in transmission of SARS-CoV-2 compared to other types of contact settings. This risk of transmission appears to decrease with use of face masks and in cases where the index or primary cases are in the paediatric age group. The risk of close contact transmission is significantly increased in the elderly. Enclosed environments and social gatherings appear to increase the likelihood of close contact transmission. Close contact with persons having recurrent infection with SARS-CoV-2 is unlikely to result in transmission of the virus. There is wide heterogeneity in study designs and methods and the overall quality of evidence from published primary studies is sub-optimal. The results of systematic reviews also suggest that household contact setting increases the risk of transmission and being elderly is also associated with increased risks of transmission and mortality.
The positive results of viral cultures observed in two studies support the results of PCR and serologic tests showing that close contact setting was associated with transmission of SARS-CoV-2. The failure to successfully isolate the virus in the third study supports the view that individuals who are re-infected are unlikely to transmit the virus in close contact settings. The positive findings from all 10 studies that performed GS and phylogenetic analysis with identical strains supports the hypothesis that close contact setting is associated with SARS-CoV-2 transmission through respiratory droplets or direct contact. The failure of the majority of studies to report Ct values casts doubts on the strengths of any reported associations because of the likelihood of false positives, as is the lack of (and variation in) reporting of the timelines for sample collections. The variations observed in the definitions of close contacts also cast further doubts on the validity of overall results.
Comparison with the existing literature
The results of our review are consistent with several guidelines suggesting that close contact with index cases can result in transmission of SARS-CoV-2 8– 10 . Our findings are also consistent with those of a systematic review which concluded that face masks are effective for preventing transmission of respiratory viruses 11 . The results of our review also support those of a previous review which showed that the elderly are at increased risk of infection and mortality with coronavirus 12 . However, our review contains a greater number of studies compared to each of the included individual reviews and shows evidence demonstrating positive culture of virus as well as genomic evidence of close contact transmission. This differs from the findings from our reviews of fomite, orofecal and airborne transmission that failed to show evidence of either positive culture or genomic sequences demonstrating SARS-CoV-2 transmission 13– 15 .
Strengths and limitations
To our knowledge, this is the most comprehensive review to date investigating the role of close contact in the transmission of SARS-CoV-2. We extensively searched the literature for eligible studies, accounted for the quality of included studies and have reported outcomes (viral culture and GS) that were previously unreported in previous reviews. However, we recognize some limitations. We may not have identified all relevant studies examining the role of close contact in transmission - this is especially true for unpublished studies. We included results from non-peer reviewed studies which may affect the reliability of the review results. However, such studies could potentially be of research benefit because of the ongoing pandemic; in addition, we performed forward citation search of relevant studies.
Implications for research
Future studies should endeavour to include Ct values (or preferably convert the Ct values to number of genome copies using standard curves) when reporting research results and should describe the timing and methods of sample collection. Details surrounding the proximity, timing, and activities within the context of close contact need to be described. In studies of elderly subjects, more detailed description of baseline demographics should be reported. Further studies showing virus isolation in close contact settings should be conducted to strengthen the current evidence base; this could include performing serial cultures. Similarly, more research examining genomic sequences and phylogenetic trees in suspected close contact transmissions should be conducted - this should also extend to research examining other modes of transmission. The variation in methods and thresholds of the serological tests add to the confusion about diagnostic accuracy of testing; indeed, some authors have questioned the value of serological tests for diagnosing SARS-CoV-2 16 . To overcome the challenge of interpreting antibody responses, guidelines for better reporting of serological tests and results should be developed; this has previously been emphasized by other authors. Internationally recognized research dictionary of terms defining and describing close contact settings should be developed. Standardized guidelines for reporting research results should be a priority. Local, national, and international health organisations should promote good hygiene measures including advising against close contact with SARS-CoV-2 infected individuals; use of medical masks should be encouraged in circumstances where close contact with infected cases is likely. Activities in enclosed settings should be discouraged and social distancing in close contact settings should be encouraged.
Conclusion
The evidence from published observational studies and systematic reviews indicate that SARS-CoV-2 can be transmitted via close contact settings. Household contact and increased frequency of contact with infected cases significantly increase the risk of transmission. The quality of evidence from published studies is low-to moderate. Variations in study designs and methodology restrict the comparability of findings across studies. Standardized guidelines for the reporting of future research should be developed.
Data availability
Underlying data
All data underlying the results are available as part of the article and no additional source data are required.
Extended data
Figshare: Extended data: SARS-CoV-2 and the Role of Close Contact in Transmission: A Systematic Review, https://doi.org/10.6084/m9.figshare.14312630.v1 6 .
This project contains the following extended data:
Updated Protocol
Search Strategy
List of Excluded Studies
References to Included Studies
Data are available under the terms of the Creative Commons Attribution 4.0 International license (CC-BY 4.0).
Acknowledgements
This work was commissioned and paid for by the World Health Organization (WHO). Copyright on the original work on which this article is based belongs to WHO. The authors have been given permission to publish this article. The author(s) alone is/are responsible for the views expressed in the publication. They do not necessarily represent views, decisions, or policies of the World Health Organization.
Funding Statement
The review was funded by the World Health Organization: Living rapid review on the modes of transmission of SARs-CoV-2 reference WHO registration No2020/1077093. CH and ES also receive funding support from the NIHR SPCR Evidence Synthesis Working Group project 390.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
[version 1; peer review: 1 approved with reservations
References
- 1. World Health Organization: WHO Coronavirus Disease (COVID-19) Dashboard. [Last Accessed 20/03/2021]. Reference Source [Google Scholar]
- 2. World Health Organization: Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations. [Accessed 16/01/2021]. Reference Source [Google Scholar]
- 3. World Health Organization: Coronavirus disease 2019 (COVID-19) Situation Report – 73. [Accessed 28 February 2021]. Reference Source [Google Scholar]
- 4. Tanne JH: Covid-19: CDC publishes then withdraws information on aerosol transmission. BMJ. 2020;370:m3739. 10.1136/bmj.m3739 [DOI] [PubMed] [Google Scholar]
- 5. Tang JW: SARS-CoV-2 and aerosols-Arguing over the evidence. J Virol Methods. 2021;289:114033. 10.1016/j.jviromet.2020.114033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Onakpoya I, Heneghan C, Spencer E, et al. : Extended data: SARS-CoV-2 and the Role of Close Contact in Transmission: A Systematic Review. figshare. Figure.2021. 10.6084/m9.figshare.14312630.v1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Whiting PF, Rutjes AWS, Westwood ME, et al. : QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–36. 10.7326/0003-4819-155-8-201110180-00009 [DOI] [PubMed] [Google Scholar]
- 8. World Health Organization: Q&A: How is COVID-19 transmitted?[Accessed 06/04/2021]. Reference Source [Google Scholar]
- 9. Center for Disease Control and Prevention: COVID-19 Overview and Infection Prevention and Control Priorities in non-US Healthcare Settings.Updated Feb. 26, 2021. Reference Source [Google Scholar]
- 10. Public Health England: Guidance 12. COVID-19 infection prevention and control guidance: glossary of terms.Updated 21 January 2021. Reference Source [Google Scholar]
- 11. Liang M, Gao L, Cheng C, et al. : Efficacy of face mask in preventing respiratory virus transmission: A systematic review and meta-analysis. Travel Med Infect Dis. 2020;36:101751. 10.1016/j.tmaid.2020.101751 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Park JE, Jung S, Kim A, et al. : MERS transmission and risk factors: a systematic review. BMC Public Health. 2018;18(1):574. 10.1186/s12889-018-5484-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Onakpoya IJ, Heneghan CJ, Spencer EA, et al. : SARS-CoV-2 and the role of fomite transmission: a systematic review [version 1; peer review: awaiting peer review]. F1000Res. 2021;10:233. 10.12688/f1000research.51590.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Heneghan CJ, Spencer EA, Brassey J, et al. : SARS-CoV-2 and the role of orofecal transmission: a systematic review [version 1; peer review: awaiting peer review]. F1000Res. 2021;10:231. 10.12688/f1000research.51592.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Heneghan C, Spencer EA, Brassey J, et al. : SARS-CoV-2 and the role of airborne transmission: a systematic review [version 1; peer review: awaiting peer review]. F1000Res. 2021;10:232. 10.12688/f1000research.52091.1 [DOI] [Google Scholar]
- 16. Bastos ML, Tavaziva G, Abidi SK, et al. : Diagnostic accuracy of serological tests for covid-19: systematic review and meta-analysis. BMJ. 2020;370:m2516. 10.1136/bmj.m2516 [DOI] [PMC free article] [PubMed] [Google Scholar]