

Abstract
Genital ulcer disease (GUD) continues to be an important cause of morbidity and mortality worldwide. It is an important risk factor for the acquisition of HIV. GUD is mainly caused by five sexually transmitted infections. Three pathogens most frequently associated with GUD are herpes simplex virus 2 (HSV-2), Treponema pallidum, and Haemophilus ducreyi. Although their prevalence varies among different geographical regions, HSV-2 is the leading cause of this syndrome globally. In recent years, there has been an epidemiological transition of HSV-1 with a growing role of this virus as a causative agent of GUD. GUD may present with unique features depending on the etiological agent that can help clinicians identify the etiology and start treatment. However, owing to atypical presentations and co-infections, an accurate clinical diagnosis is often a challenge without confirmatory laboratory tests. Standard methods used to detect the causative pathogens of GUD have limitations. Molecular methods can provide a more sensitive and rapid microbiological diagnosis, with detection of the pathogen from the clinical sample directly. In situations where no laboratory support is available, the syndromic approach for management should be followed. The current scenario, clinical presentation (typical and atypical), laboratory diagnosis, and management of GUD will be discussed in this review. We searched PubMed literature and Google search engine using the terms “genital ulcer disease,” “epidemiology of genital ulcer disease,” and “clinical features of genital ulcer disease and atypical presentations” and relevant literature was selected to provide current perspectives of GUD.
Keywords: Genital ulcer disease, haemophilus ducreyi, herpes simplex virus, sexually transmitted infections, treponema pallidum
Introduction
Genital ulcer disease (GUD) is a common and important health problem in both developed and developing countries. It is an established risk factor for acquisition of HIV infection due to increased shedding of HIV through breached epithelium. Because of suboptimal laboratory facilities in developing countries including India, most cases are diagnosed clinically—an approach fraught with a high probability of misdiagnosis because of significant variability and overlap in morphologic presentation. As a result, most of the developing countries are currently managing GUDs syndromically—an approach based primarily on the clinical presentation of GUDs but one that needs to be validated periodically.
The etiology of GUD varies in different parts of the world. The three pathogens most frequently incriminated include herpes simplex virus 1 (HSV-1) and HSV-2, Treponema pallidum, and Haemophilus ducreyi.[1,2]
This review focuses on the current scenario, clinical features, laboratory diagnosis, and management of GUD. This serves as guidance to the family physicians and primary care physicians in terms of atypical presentations of genital ulcers, epidemiological transition, as well as the new at-risk populations and the appropriate diagnostic technologies to be used, for timely management of the GUDs or refer to specialist/higher centers, as they are the first point of contact. We searched PubMed literature and Google search engine using the terms “genital ulcer disease,” “epidemiology of genital ulcer disease,” and “clinical features of genital ulcer disease and atypical presentations” and relevant literature was selected to provide current perspectives of GUD.
Etiological agent and transmission
Genital herpes (GH): HSV-2 (mainly) and 1 are the causative agents of GH. The average incubation period for an initial herpes infection is 4 days (ranging from 2 to 12) after exposure.[3] After infection, HSV establishes a latent state followed by viral reactivation and recurrent local disease. Recurrences are less frequent with HSV-1 than HSV-2, but mother to child transmission is higher.[4] Although conventionally HSV-2 is considered the cause of GH, HSV-1 is now associated with an increasing proportion of patients, especially among young women and men who have sex with men (MSM).[5,6,7] Infection of the same anatomic site by both HSV-1 and HSV-2 has been documented.
Chances of infection are higher from a patient with active GH, but infection can also occur from an infected asymptomatic partner due to asymptomatic viral shedding.[8] HSV-1 commonly causes orolabial herpes (cold sores) and is primarily transmitted by oral-to-oral contact but genital infection by HSV-1 is trending due to increased frequency of orogenital contact.[9,10]
Syphilis: Treponema pallidum is highly infectious with attack rate within 30 days of sexual exposure to a patient with syphilis being 16% to 30%.[11] Incubation period is usually 2 to 3 weeks but can range from 9 to 90 days.[12]
It is transmitted mainly by sexual contact, viz. vaginal, anogenital, and orogenital, but can also be spread vertically and rarely via blood products and organ donation. Extragenital syphilitic lesions on the fingers and in the nose of healthcare providers, laboratory workers, and transmission via human bite in sexual as well as non-sexual circumstances has also been reported.[13]
Chancroid: Epidermal microabrasions during sexual intercourse may lead to establishment of H. ducreyi infection. The incubation period may range from 4 to 7 days after experiencing an encounter with minor trauma or microabrasions.[14]
The likelihood of transmission of H. ducreyi infection from an infected individual during a single sexual encounter is 0.3 to 0.35. Untreated infected patients are estimated to be infectious for up to 45 days.[15]
Lymphogranuloma venereum (LGV): Chlamydia trachomatis serotypes L1, L2, and L3 causes LGV.[16] Incubation period ranges between 3 and 30 days. The degree of infectiousness and the reservoir of disease have not been accurately defined, but transmission has been attributed mainly to asymptomatic female carriers and in the MSM population.[17] Subvariants such as L2b causing proctitis in MSM have been reported from United states and European countries.[18]
LGV can be transmitted through unprotected vaginal, anal, or oral sexual contact.[17] Developmental cycle of C. trachomatis alternates between two forms: the infectious elementary body (EB) and the noninfectious replicating form, the reticulate body. The attachment process of the elementary body to a host cell is the event most crucial to a successful transmission of infection.[17]
Donovanosis: Caused by Klebsiella granulomatis (formerly known as Calymmatobacterium granulomatis) is a rare cause of GUD. The rate of transmission is thought to be low in general. The incubation period is around 50 days.[19,20] It is a chronic, progressive, and indolent sexually transmitted bacterial disease that affects the skin and mucous membranes of the genital and perigenital regions in adults aged 20 to 40 years.[19]
Predisposing factors for GUD
Early age of coitarche, partners with untreated GUDs, multiple sexual partners, sexual contact with commercial sex workers, previous STIs, practice of condomless vaginal or anal sex (especially in MSM), and other sexual risk behaviors (use of drugs for sex, chemsex, and sex in group), uncircumcised men, trauma or microabrasion to the skin or mucosa during sexual act, visit to areas where a particular GUD is endemic, and lower education level are the predisposing factors for acquisition of GUD.[8,20,21,22,23,24,25]
Epidemiology
GH: It is the most common cause of GUD worldwide. In 2016, a global estimation of 187 million people (5.0% of the world’s population) aged 15 to 49 years had at least one episode of HSV-related GUD, of those 95% had HSV-2 related GUD and 5% with HSV-1. HSV-related GUD burden was highest in African region and almost double in women compared with men.[26]
Earlier HSV-2 was mainly reported to cause GH,[27,28,29] but recent studies from India by Brijwal et al.[30] using real-time PCR have indicated HSV-1 to cause 25% of GH. Also, in a meta-analytic study by Khadr L et al.,[31] which included published data from Asian countries, 19% of GH cases were due to HSV-1 (as opposed to HSV-2) and accounted for 6% of GUD cases.
Syphilis: Syphilis is the second most common cause of GUD in many parts of world including India.[32] The prevalence of syphilis has dropped sharply in the late 1990s in countries with endemic syphilis. This is possibly due to the introduction of syndromic management for STIs and effect of AIDS mortality disrupting the sexual networks and behavioral changes. But an increase in the rates of syphilis has been seen, especially among MSM’s after the introduction of antiretroviral therapy (ART), probably due to the reconstruction of sexual network and increased frequency of sexual contact.[11]
In general, the distribution of syphilis differs between low- and middle-income countries (LMICs) and high-income countries. LMICs generally have higher burdens of syphilis with endemic rates of syphilis among the general populations, with the highest prevalence reported from African region. In contrast, high-income countries have concentrated epidemics of syphilis in specific populations, like MSMs, transgender women, and sex workers.[11]
Chancroid: It was once the most common GUD seen in STD clinics across Africa, Asia, and Latin America.[33] Globally, the proportion of GUD caused by H. ducreyi before the year 2000 ranged from 0.0% (Thailand and China) to 69.0% (South Africa). A high proportion (>40%) of H. ducreyi infection was reported from African countries. Studies from India, United states (during a localized outbreak), Jamaica, Dominican Republic, and including 10 African countries reported H. ducreyi as the etiological agent of GUD in 20% to 40% cases.[34]
After the year 2000, a low proportion (<10%) of H. ducreyi causing GUD was reported from most countries.[34] This rapid decline in the incidence of chancroid was largely due to the widespread use of syndromic approach in the management of STDs.
LGV: LGV is endemic in many parts of Africa, Southeast Asia, Latin America, and the Caribbean.[35] Till 2003, only sporadic cases were reported in Europe and North America. However, in 2003, several cases of LGV proctitis were reported among MSMs, first in Rotterdam, followed by reports coming from other countries in Western Europe, North America, and Australia. LGV has now become increasingly common in North America and Europe among gay, bisexuals, and MSM communities. These epidemics were caused almost exclusively by the L2b serovar.[36,37]
Similar trends are now being reported from India as well.[38] Dhawan B et al.,[39] reported the first case of proctitis from India due to C. trachomatis in a bisexual male patient. Following this case, rectal chlamydial infection was found in 30% and 53.3% of MSM population in two different studies conducted from same center.[40,41] Due to the financial constraints, typing of the isolates could not be performed. Nonetheless, the data extrapolated indicates the recognition of pre-existing non-heterosexual orientation in the Indian population.
Donovanosis: The endemic areas for donovanosis have been in tropical and subtropical countries such as Papua New Guinea, South Africa, India, Indonesia, Australia, the Caribbean, Argentina, French Guiana, and Brazil. Over the past two decades, the prevalence of donovanosis has decreased significantly and fewer cases are reported nowadays even in countries where the prevalence was once high.[42,43]
In India, donovanosis was endemic along the east coast (Orissa, Andhra Pradesh, and Tamil Nadu). Recently, six cases have been reported in two years (2016–2017) from central India. High-risk sexual behavior among all cases including exposure to commercial sex workers and history of sexual exposure in endemic regions were probable causes in these cases.[44]
Clinical features
GH: Genital HSV presents as painful, localized clusters of erythematous papules and vesicles on the genital [Figure 1a and 1b] or perianal area, with the first episode occurring within 4 to 7 days of high-risk exposure. These vesicular lesions may coalesce or form erosions over few days. With the primary infection, some patients may develop regional lymphadenopathy, dysuria, and systemic symptoms. The lesions may recur during times of stress, illness, or menstruation.[45,46]
Figure 1.
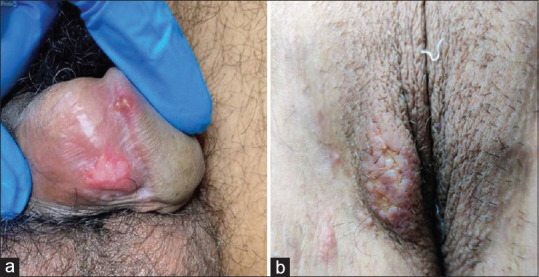
(a) Shows herpetic lesion on male external genitalia. (b) Shows herpetic lesions on labia majora
Atypical presentation of genital HSV includes fissures (vulvar, penile, or perianal), cystitis, urethritis, vaginal discharge without apparent genital lesions, localized recurrent erythema, recurrent radicular or lower back pain, and lesions at unusual sites like buttocks and thighs.[47] Complications like aseptic meningitis which may be recurrent (Mollaret’s meningitis), sacral autonomic nervous system dysfunction, and secondary bacterial or yeast infections have been seen.[46]
Syphilis: It is a systemic disease and can involve any organ. It typically presents with a genital ulcer but its manifestations are protean. Primary syphilis is characterized by a papule at the point of entry of the bacterium that breaks down into an ulcer (chancre). It classically presents with a solitary, firm, indurated, 0.5 to 2 cm in diameter, painless ulcer typically on the glans penis in men and vulva or cervix in women and associated with regional lymphadenopathy, that usually heals spontaneously over a period of 4 to 6 weeks.[48,49]
Location and presentation of these ulcers can be sometimes atypical, including mouth (30% of cases are transmitted through orogenital contact), rectum, or any site where the organism comes into contact with the skin or mucosa. It can present as multiple chancres, painful papules, or ulcers. Atypical presentations occur especially in the context of HIV-1 coinfection.[48,49] In a recent case report by Rawre J et al.,[50] a non-healing single, painful genital ulcer over labia majora in an HIV positive patient [Figure 2] has been reported. On investigation, the lesion was found to be positive for both Treponema pallidum and HSV-2 and on further investigations, the ulcer was also positive for co-infection with Cytomegalovirus. Moreover, the clinical manifestations of GUD in immunosuppressed patients like HIV positive patients or transplant recipients may follow an accelerated course with more florid development.
Figure 2.

Perigenital ulcer co-infected with HSV-2 and CMV
Chancroid: H. ducreyi infection initially presents as a tender papule surrounded by a zone of erythema. The papule becomes pustular and subsequently ruptures in 2 to 3 days to produce a shallow ulcer, which is painful and has well demarcated borders with ragged and undermined edges [Figure 3]. Purulent discharge and bleeding may be seen when the ulcers are scraped. In the absence of antibiotic therapy, these ulcers may persist for weeks to months with slow and incomplete resolution. Lesions are usually located on the prepuce and frenulum of men and vulva, cervix, and perianal region of women.[14] Its lesions are more readily apparent and therefore more commonly reported among men. Painful inguinal lymphadenitis is a characteristic feature seen in approximately 50% of patients with chancroid, mostly men. If untreated, the formation of buboes can be observed that may eventually rupture and discharge pus.[49]
Figure 3.

Multiple necrotic penile ulcers in chancroid
Atypical clinical presentation includes dwarf, follicular, transient varieties, and ulcers which are serpiginous, giant, and phagedenic form.[51] Extragenital chancroid are rare and may present with lesions on the inner thighs, breasts, and fingers.[14] Complications associated with chancroid include the development of fistulous tracts secondary to suppurative lymphadenitis and the destruction of the deep tissues of the genitalia by either secondary or superinfection by bacteria. Cicatrix formation and phimosis is a late complication requiring circumcision.[14,51]
LGV: Classically, LGV symptoms are divided into three stages. In primary stage, a small painless papule or pustule appears that may erode to form a small herpetiform ulcer. Usually, it heals within 1 week and often remains unnoticed, but it may present as a chancre also. Secondary stage begins 2 to 6 weeks after the primary lesion. It is characterized by painful inguino-femoral lymphadenopathy that is often unilateral, painful, firm, and known as buboes. Enlargement of the inguinal nodes above and the femoral nodes below the inguinal ligament leads to development of “groove sign” in some patients. Constitutional symptoms like fever, chills, malaise, etc., may accompany.[16,18]
Atypical presentations like anorectal syndrome resulting in inflammatory mass in the rectum and retroperitoneum, mimicking carcinoma and rare cases of oropharyngeal LGV affecting cervical lymph nodes have been reported in MSM. Other rare reactive and septic presentations are also described in studies, for example, reactive arthritis, cardiac involvement, and perihepatitis.[18,52,53] Chronic lymphangitis and subsequent lymphatic obstruction caused by LGV can lead to complications like regional lymphedema and genital elephantiasis.[16,18] Infertility, rectovaginal fistulas, and rectal strictures have also been reported as severe complications of tertiary LGV.[49]
Donovanosis: Four types of lesions are mainly described in donovanosis. The most common type is ulcerative granulomatous with beefy red ulcers that bleed to touch. Others include hypertrophic type with raised irregular edge, necrotic type with offensive smelling ulcer causing tissue destruction, and sclerotic or cicatricial type with fibrous/scar tissue.[19] Regions most affected in men are the coronal groove, the balanoprepucial area, and the anus. In women, the areas commonly affected include the labia minora, vaginal furcula, and, occasionally, the cervix and upper genital tract, where they can simulate carcinomas.[44] In 90% of cases, the genitals are affected but inguinal region may be involved in 10%.[19]
Extragenital presentation accounts for 6% of cases, causing leisons at atypical sites like lip, gums, cheek, palate, pharynx, neck, nose, larynx, and chest. Disseminated donovanosis is seen to involve bone and liver. As the ulcer bleeds readily, the risk of associated HIV infection is also increased.[19,43]
Laboratory diagnosis of GUD
The diagnosis of GUD is based on the presence of mucocutaneous ulcers involving the genitalia, perineum, or anus. Diagnosing the cause of genital ulcers is based on a combination of history, physical examination, and laboratory findings. Figure 4a and 4b shows the diagnostic algorithm of GUD.
Figure 4.

(a) Diagnostic algorithm of painful ulcer. (b) Diagnostic algorithm of painless ulcer
Treatment of GUD
For the treatment of GUD, syndromic approach is used in many developing countries including India. Seven pre-packed color-coded kits for Sexually Transmitted Infections including Reproductive Tract Infections kits are proposed under National AIDS Control Programme-IV and are procured by National AIDS control organization/State AIDS Control Society.
Treatment of individual etiological agents of GUD
GH: Systemic antiviral drugs (acyclovir, valacyclovir, and famciclovir) can partially alleviate symptoms and hasten recovery when used to treat first clinical and recurrent episodes or when used as daily suppressive therapy. But these drugs neither eradicate latent virus nor affect the risk, frequency, or severity of recurrences after the drug is discontinued.[54]
Syphilis: The treatment of choice for syphilis at all stages of disease is Penicillin G. For adults with primary, secondary, or early-latent stage of less than 1 year’s duration, the recommended regimen of benzathine penicillin G is 2.4 million units IM in a single dose. For adults in the late latent stage, the recommended regimen is 2.4 million units IM once per week for 3 successive weeks.[54]
Chancroid: The recommended regimen for chancroid by CDC is azithromycin 1 g orally in a single dose or ceftriaxone 250 mg im in a single dose or ciprofloxacin 500 mg orally twice a day for 3 days or erythromycin base 500 mg orally three times a day for 7 days. Azithromycin and ceftriaxone offer the advantage of single dose therapy.[54]
Donovanosis: Recommended regimen: azithromycin 1 g orally once per week or 500 mg daily for at least 3 weeks and until all lesions have completely healed. Alternative regimens: doxycycline 100 mg orally twice a day for at least 3 weeks and until all lesions have completely healed or ciprofloxacin/erythromycin base/trimethoprim-sulfamethoxazole can also be used.[54]
LGV: Recommended regimen: doxycycline 100 mg orally twice a day for 21 days. Erythromycin base 500 mg orally four times a day for 21 days is the alternative regimen. If the patient presents with buboes, aspiration, incision, and drainage may be required.[49,54]
Conclusion
HSV-2 is considered the leading cause of this GUD globally. HSV-1, though known to cause orolabial lesions mainly, has been increasingly seen to cause GUD as well. The prevalence of other agents varies among geographic regions. After the introduction of ART, an increase in the rates of syphilis has been seen in high-risk sexual behaviors, mainly the MSM community. Whereas, chancroid has become exceedingly uncommon in the developed countries and is only occasionally reported in developing countries probably due to syndromic management of STIs. Owing to frequently atypical presentation and mixed infections, an accurate clinical diagnosis of GUD is very difficult. Successful management of GUD depends on accurate diagnosis confirmed by performance of appropriate laboratory tests when possible. There is a need to use sensitive and reliable molecular methods to prevent the underdiagnosis of the etiological agents of GUD and help formulate guidelines for the management of GUD.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Carmine L. Genital ulcer disease-A review for primary care providers caring for adolescents. Curr Probl Pediatr Adolesc Health Care. 2020;50:100834. doi: 10.1016/j.cppeds.2020.100834. [DOI] [PubMed] [Google Scholar]
- 2.Looker KJ, Welton NJ, Sabin KM, Dalal S, Vickerman P, Turner KME, et al. Global and regional estimates of the contribution of herpes simplex virus type 2 infection to HIV incidence: A population attributable fraction analysis using published epidemiological data. Lancet Infect Dis. 2019;20:240–9. doi: 10.1016/S1473-3099(19)30470-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kimberlin DW, Rouse DJ. Clinical practice. Genital herpes. N Engl J Med. 2004;350:1970–7. doi: 10.1056/NEJMcp023065. [DOI] [PubMed] [Google Scholar]
- 4.James SH, Sheffield JS, Kimberlin DW. Mother-to-child transmission of herpes simplex virus. J Pediatric Infect Dis Soc. 2014;3:19–23. doi: 10.1093/jpids/piu050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zhu S, Viejo-Borbolla A. Pathogenesis and virulence of herpes simplex virus. Virulence. 2021;12:2670–702. doi: 10.1080/21505594.2021.1982373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Magdaleno-Tapial J, Hernandez-Bel P, Valenzuela-Onate C, Ortiz-Salvador JM, Garcia-Legaz-Martinez M, Martinez-Domenech A, et al. Genital infection with herpes simplex virus type 1 and type 2 in Valencia, Spain: A retrospective observational study. Actas Dermosifiliogr. 2020;111:53–8. doi: 10.1016/j.ad.2019.06.002. [DOI] [PubMed] [Google Scholar]
- 7.Ryder N, Jin F, McNulty AM, Grulich AE, Donovan B. Increasing role of herpes simplex virus type 1 in first-episode anogenital herpes in heterosexual women and younger men who have sex with men 1992-2006. Sex Transm Infect. 2009;85:416–9. doi: 10.1136/sti.2008.033902. [DOI] [PubMed] [Google Scholar]
- 8.Hammad WAB, Konje JC. Herpes simplex virus infection in pregnancy-An update. Eur J Obstet Gynecol Reprod Biol. 2021;259:38–45. doi: 10.1016/j.ejogrb.2021.01.055. [DOI] [PubMed] [Google Scholar]
- 9.Ayoub HH, Chemaitelly H, Abu-Raddad LJ. Characterizing the transitioning epidemiology of herpes simplex virus type 1 in the USA: Model-based predictions. BMC Med. 2019;17:57. doi: 10.1186/s12916-019-1285-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Benedetti J, Corey L, Ashley R. Recurrence rates in genital herpes after symptomatic first-episode infection. Ann Intern Med. 1994;121:847–54. doi: 10.7326/0003-4819-121-11-199412010-00004. [DOI] [PubMed] [Google Scholar]
- 11.Kojima N, Klausner JD. An Update on the Global Epidemiology of Syphilis. Curr Epidemiol Rep. 2018;5:24–38. doi: 10.1007/s40471-018-0138-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.French P. Syphilis. BMJ. 2007;334:143–7. doi: 10.1136/bmj.39085.518148.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Stoltey JE, Cohen SE. Syphilis transmission: A review of the current evidence. Sex Health. 2015;12:103–9. doi: 10.1071/SH14174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lewis DA. Chancroid: From clinical practice to basic science. AIDS Patient Care STDS. 2000;14:19–36. doi: 10.1089/108729100318109. [DOI] [PubMed] [Google Scholar]
- 15.Trees DL, Morse SA. Chancroid and Haemophilus ducreyi: An update. Clin Microbiol Rev. 1995;8:357–75. doi: 10.1128/cmr.8.3.357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.O’ Byrne P, MacPherson P, DeLaplante S, Metz G, Bourgault A. Approach to lymphogranuloma venereum. Can Fam Physician. 2016;62:554–8. [PMC free article] [PubMed] [Google Scholar]
- 17.Ceovic R, Gulin SJ. Lymphogranuloma venereum: Diagnostic and treatment challenges. Infect Drug Resist. 2015;8:39–47. doi: 10.2147/IDR.S57540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.de Vries HJC, de Barbeyrac B, de Vrieze NHN, Viset JD, White JA, Vall-Mayans M, et al. 2019 European guideline on the management of lymphogranuloma venereum. J Eur Acad Dermatol Venereol. 2019;33:1821–8. doi: 10.1111/jdv.15729. [DOI] [PubMed] [Google Scholar]
- 19.O’ Farrell N, Moi H. 2016 European guideline on donovanosis. Int J STD AIDS. 2016;27:605–7. doi: 10.1177/0956462416633626. [DOI] [PubMed] [Google Scholar]
- 20.Santiago-Wickey JN, Crosby B. StatPearls Treasure Island (FL): StatPearls Publishing; 2021. [Updated 2020 Aug 10]. Granuloma Inguinale. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513306 . [PubMed] [Google Scholar]
- 21.Uribe-Salas F, Hernandez-Avila M, Juarez-Figueroa L, Conde-Glez CJ, Uribe-Zuniga P. Risk factors for herpes simplex virus type 2 infection among female commercial sex workers in Mexico City. Int J STD AIDS. 1999;10:105–11. doi: 10.1258/0956462991913727. [DOI] [PubMed] [Google Scholar]
- 22.Tideman RL, Taylor J, Marks C, Seifert C, Berry G, Trudinger B, et al. Sexual and demographic risk factors for herpes simplex type 1 and 2 in women attending an antenatal clinic. Sex Transm Infect. 2001;77:413–5. doi: 10.1136/sti.77.6.413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Caldeira TD, Goncalves CV, Oliveira GR, Fonseca TV, Goncalves R, Amaral CT, et al. Prevalence of herpes simplex virus type 2 and risk factors associated with this infection in women in southern Brazil. Rev Inst Med Trop Sao Paulo. 2013;55:315–21. doi: 10.1590/S0036-46652013000500004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Arando M, Fernandez-Naval C, Mota-Foix M, Martinez D, Armengol P, Barbera MJ, et al. Early syphilis: Risk factors and clinical manifestations focusing on HIV-positive patients. BMC Infect Dis. 2019;19:727. doi: 10.1186/s12879-019-4269-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Todd J, Munguti K, Grosskurth H, Mngara J, Changalucha J, Mayaud P, et al. Risk factors for active syphilis and TPHA seroconversion in a rural African population. Sex Transm Infect. 2001;77:37–45. doi: 10.1136/sti.77.1.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.James C, Harfouche M, Welton NJ, Turner KM, Abu-Raddad LJ, Gottlieb SL, et al. Herpes simplex virus: Global infection prevalence and incidence estimates 2016. Bull World Health Organ. 2020;98:315–29. doi: 10.2471/BLT.19.237149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nahmias AJ, Lee FK, Beckman-Nahmias S. Sero-epidemiological and -sociological patterns of herpes simplex virus infection in the world. Scand J Infect Dis Suppl. 1990;69:19–36. [PubMed] [Google Scholar]
- 28.Smith JS, Robinson NJ. Age-specific prevalence of infection with herpes simplex virus types 2 and 1: A global review. J Infect Dis. 2002;186(Suppl 1):S3–28. doi: 10.1086/343739. [DOI] [PubMed] [Google Scholar]
- 29.Corey L, Wald A. Genital herpes. In: Holmes KK, Sparling FP, Mardh PA, Lemon SM, Piot P, et al., editors. Sexually Transmitted Diseases. 3rd ed. New York, NY: McGraw-Hill; 1999. pp. 285–312. [Google Scholar]
- 30.Brijwal M, Rawre J, Dhawan B, Khanna N, Choudhary A, Dar L. Herpes simplex virus type 1 genital ulcer disease at a tertiary care hospital in North India. Clin Infect Dis. 2019;68:1783–4. doi: 10.1093/cid/ciy943. [DOI] [PubMed] [Google Scholar]
- 31.Khadr L, Harfouche M, Omori R, Schwarzer G, Chemaitelly H, Abu-Raddad LJ. The epidemiology of herpes simplex virus type 1 in Asia: Systematic review, meta-analyses, and meta-regressions. Clin Infect Dis. 2019;68:757–72. doi: 10.1093/cid/ciy562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Muralidhar S, Talwar R, Anil Kumar D, Kumar J, Bala M, Khan N, et al. Genital ulcer disease: How worrisome is it today?A status report from New Delhi, India. J Sex Transm Dis. 2013;2013:203636. doi: 10.1155/2013/203636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Alfa M. The laboratory diagnosis of Haemophilus ducreyi. Can J Infect Dis Med Microbiol. 2005;16:31–4. doi: 10.1155/2005/851610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gonzalez-Beiras C, Marks M, Chen CY, Roberts S, Mitja O. Epidemiology of Haemophilus ducreyi Infections. Emerg Infect Dis. 2016;22:1–8. doi: 10.3201/eid2201.150425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Herring A, Richens J. Lymphogranuloma venereum. Sex Transm Infect. 2006;82(4):23–5. doi: 10.1136/sti.2006.023143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Spaargaren J, Fennema HS, Morré SA, de Vries HJ, Coutinho RA. New lymphogranuloma venereum Chlamydia trachomatis variant, Amsterdam. Emerg Infect Dis. 2005;11:1090–2. doi: 10.3201/eid1107.040883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Spaargaren J, Schachter J, Moncada J, de Vries HJ, Fennema HS, Pena AS, et al. Slow epidemic of lymphogranuloma venereum L2b strain. Emerg Infect Dis. 2005;11:1787–8. doi: 10.3201/eid1111.050821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Juyal D, Rawre J, Dhawan B. Under diagnosis of the lymphogranuloma venereum serovars in the Indian population. Indian J Med Microbiol. 2019;37:595–7. doi: 10.4103/ijmm.IJMM_19_475. [DOI] [PubMed] [Google Scholar]
- 39.Dhawan B, Makharia GK, Juyal D, Sebastian S, Bhatia R, Khanna N. Chlamydia trachomatis proctitis masquerading as carcinoma rectum: First case report from India. Indian J Pathol Microbiol. 2017;60:259–61. doi: 10.4103/IJPM.IJPM_114_16. [DOI] [PubMed] [Google Scholar]
- 40.Arif N, Juyal D, Sebastian S, Khanna N, Dhawan B. Analysis of laboratory testing results for Chlamydia trachomatis infection in an STI clinic in India: Need for extragenital screening. Int J Infect Dis. 2017;57:1–2. doi: 10.1016/j.ijid.2017.01.004. [DOI] [PubMed] [Google Scholar]
- 41.Dhawan B, Rawre J, Dhawan N, Bhatia R, Gupta V, Khanna N. High prevalence of Mycoplasma genitalium in men who have sex with men: A cross-sectional study. Indian J Dermatol Venereol Leprol. 2020;86:195–6. doi: 10.4103/ijdvl.IJDVL_494_18. [DOI] [PubMed] [Google Scholar]
- 42.Belda Junior W. Donovanosis. An Bras Dermatol. 2020;95:675–83. doi: 10.1016/j.abd.2020.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.O’ Farrell N. Donovanosis. Sex Transm Infect. 2002;78:452–7. doi: 10.1136/sti.78.6.452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hajare SA, Mukhi JI, Rambhia KD, Singh RP. Donovanosis in Central India: A series of six cases and review of literature. J Clin Diag Res. 2019;13:01–5. [Google Scholar]
- 45.Parra-Sanchez M. Genital ulcers caused by herpes simplex virus. Enferm Infect Microbiol Clin. 2019;37:260–4. doi: 10.1016/j.eimc.2018.10.020. [DOI] [PubMed] [Google Scholar]
- 46.Corey L, Adams HG, Brown ZA, Holmes KK. Genital herpes simplex virus infections: Clinical manifestations, course, and complications. Ann Intern Med. 1983;98:958–72. doi: 10.7326/0003-4819-98-6-958. [DOI] [PubMed] [Google Scholar]
- 47.Uuskula A, Raukas E. Atypical genital herpes: Report of five cases. Scand J Infect Dis. 2004;36:37–9. doi: 10.1080/00365540310017276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Nyatsanza F, Tipple C. Syphilis: Presentations in general medicine. Clin Med (Lond) 2016;16:184–8. doi: 10.7861/clinmedicine.16-2-184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Maliyar K, Mufti A, Syed M, Selk A, Dutil M, Bunce PE, et al. Genital ulcer disease: A review of pathogenesis and clinical features. J Cutan Med Surg. 2019;23:624–34. doi: 10.1177/1203475419858955. [DOI] [PubMed] [Google Scholar]
- 50.Rawre J, Rai M, Namdeo D, Das R, Khanna N, Dar L, et al. Herpes simplex virus type 2 and cytomegalovirus perigenital ulcer in an HIV infected woman. Indian J Med Microbiol. 2018;36:441–3. doi: 10.4103/ijmm.IJMM_18_203. [DOI] [PubMed] [Google Scholar]
- 51.Inamadar AC, Palit A. Chancroid: An update. Indian J Dermatol Venereol Leprol. 2002;68:5–9. [PubMed] [Google Scholar]
- 52.Mabey D, Peeling RW. Lymphogranuloma venereum. Sex Transm Infect. 2002;78:90–2. doi: 10.1136/sti.78.2.90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Galeano-Valle F, Perez-Latorre L, Diez-Romero C, Fanciulli C, Aldamiz-Echeverria-Lois T, Tejerina-Picado F. Cervical and oropharyngeal lymphogranuloma venereum: Case report and literature review. Sex Transm Dis. 2019;46:689–92. doi: 10.1097/OLQ.0000000000001036. [DOI] [PubMed] [Google Scholar]
- 54.Workowski KA, Bolan GA. Centers for disease control and prevention. Sexually transmitted diseases treatment guidelines. MMWR Recomm Rep. 2015;64:1–137. [PMC free article] [PubMed] [Google Scholar]