

Abstract
Background
Rebleeding is an important cause of death and disability in people with aneurysmal subarachnoid haemorrhage. Rebleeding is probably related to the dissolution of the blood clot at the site of the aneurysm rupture by natural fibrinolytic activity. This review is an update of previously published Cochrane Reviews.
Objectives
To assess the effects of antifibrinolytic treatment in people with aneurysmal subarachnoid haemorrhage.
Search methods
We searched the Cochrane Stroke Group Trials Register (May 2022), CENTRAL (in the Cochrane Library 2021, Issue 1), MEDLINE (December 2012 to May 2022), and Embase (December 2012 to May 2022). In an effort to identify further published, unpublished, and ongoing studies, we searched reference lists and trial registers, performed forward tracking of relevant references, and contacted drug companies (the latter in previous versions of this review).
Selection criteria
Randomised trials comparing oral or intravenous antifibrinolytic drugs (tranexamic acid, epsilon amino‐caproic acid, or an equivalent) with control in people with subarachnoid haemorrhage of suspected or proven aneurysmal cause.
Data collection and analysis
Two review authors (MRG & WJD) independently selected trials for inclusion, and extracted the data for the current update. In total, three review authors (MIB & MRG in the previous update; MRG & WJD in the current update) assessed risk of bias. For the primary outcome, we dichotomised the outcome scales into good and poor outcome, with poor outcome defined as death, vegetative state, or (moderate) severe disability, assessed with either the Glasgow Outcome Scale or the Modified Rankin Scale. We assessed death from any cause, rates of rebleeding, delayed cerebral ischaemia, and hydrocephalus per treatment group. We expressed effects as risk ratios (RR) with 95% confidence intervals (CI). We used random‐effects models for all analyses. We assessed the quality of the evidence with GRADE.
Main results
We included one new trial in this update, for a total of 11 included trials involving 2717 participants. The risk of bias was low in six studies. Five studies were open label, and we rated them at high risk of performance bias. We also rated one of these studies at high risk for attrition and reporting bias.
Five trials reported on poor outcome (death, vegetative state, or (moderate) severe disability), with a pooled risk ratio (RR) of 1.03 (95% confidence interval (CI) 0.94 to 1.13; P = 0.53; 5 trials, 2359 participants; high‐quality evidence), which showed no difference between groups. All trials reported on death from all causes, which showed no difference between groups, with a pooled RR of 1.02 (95% CI 0.90 to 1.16; P = 0.77; 11 trials, 2717 participants; high‐quality evidence). In trials that combined short‐term antifibrinolytic treatment (< 72 hours) with preventative measures for delayed cerebral ischaemia, the RR for poor outcome was 0.98 (95% CI 0.81 to 1.18; P = 0.83; 2 trials, 1318 participants; high‐quality evidence).
Antifibrinolytic treatment reduced the risk of rebleeding, reported at the end of follow‐up (RR 0.65, 95% CI 0.47 to 0.91; P = 0.01; 11 trials, 2717 participants; absolute risk reduction 7%, 95% CI 3 to 12%; moderate‐quality evidence), but there was heterogeneity (I² = 59%) between the trials. The pooled RR for delayed cerebral ischaemia was 1.27 (95% CI 1.00 to 1.62; P = 0.05; 7 trials, 2484 participants; moderate‐quality evidence). However, this effect was less extreme after the implementation of ischaemia preventative measures and < 72 hours of treatment (RR 1.10, 95% CI 0.83 to 1.46; P = 0.49; 2 trials, 1318 participants; high‐quality evidence). Antifibrinolytic treatment showed no effect on the reported rate of hydrocephalus (RR 1.09, 95% CI 0.99 to 1.20; P = 0.09; 6 trials, 1992 participants; high‐quality evidence).
Authors' conclusions
The current evidence does not support the routine use of antifibrinolytic drugs in the treatment of people with aneurysmal subarachnoid haemorrhage. More specifically, early administration with concomitant treatment strategies to prevent delayed cerebral ischaemia does not improve clinical outcome. There is sufficient evidence from multiple randomised controlled trials to incorporate this conclusion in treatment guidelines.
Keywords: Humans, Antifibrinolytic Agents, Antifibrinolytic Agents/therapeutic use, Brain Ischemia, Hydrocephalus, Persistent Vegetative State, Persistent Vegetative State/drug therapy, Subarachnoid Hemorrhage, Subarachnoid Hemorrhage/drug therapy
Plain language summary
Drugs for preventing blood clot dissolution (antifibrinolytic therapy) to improve recovery after subarachnoid haemorrhage from a ruptured aneurysm (aneurysmal)
Research question
What are the effects of antifibrinolytic treatment in people with aneurysmal subarachnoid haemorrhage?
Background
A subarachnoid haemorrhage is bleeding into the small space between the brain and the skull that contains blood vessels that supply the brain (the subarachnoid space). The cause of this type of bleeding is most often a rupture of a weak spot (aneurysm) in one of the brain vessels. A subarachnoid haemorrhage is a relatively uncommon type of stroke, but often occurs at a young age (half the people are younger than 50 years), and therefore, has a significant socioeconomic impact. The outcome following a subarachnoid haemorrhage is often poor; one‐third of people die after the haemorrhage, and of those who survive, one‐fifth will require help for everyday activities. An important cause of poor recovery after a subarachnoid haemorrhage is repeated (recurrent) bleeding from the aneurysm (rebleeding). This is thought to be caused from natural blood clot dissolving (fibrinolytic) activity. Drugs that reduce the speed of the blood clot dissolving, called antifibrinolytic drugs, were introduced as a treatment to reduce the risk of recurrent bleeding and improve recovery after a subarachnoid haemorrhage.
Study characteristics
The evidence is current to May 2022. This review included 11 trials, with a total of 2717 participants, which investigated the effect of antifibrinolytic drugs in people with a subarachnoid haemorrhage caused by a ruptured aneurysm.
Key results
Antifibrinolytic treatment reduces the risk of rebleeding, but does not improve overall survival, or the chance of being independent in everyday activities. We conclude that there is no evidence to support routinely giving antifibrinolytic treatment to people with a subarachnoid haemorrhage caused by a ruptured aneurysm.
Quality of evidence
We assessed the evidence for the outcomes as moderate‐ to high‐quality, which means we are very, or moderately confident in the results.
Summary of findings
Summary of findings 1. Antifibrinolytic therapy for aneurysmal subarachnoid haemorrhage.
| Antifibrinolytic therapy compared with standard care for aneurysmal subarachnoid haemorrhage | ||||
| Patient or population | adults with aneurysmal subarachnoid haemorrhage (SAH) | |||
| Setting | hospital | |||
| Intervention | antifibrinolytic (AF) therapy | |||
| Comparison | standard care | |||
| Outcomes | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments |
| Poor outcome | RR 1.03 (0.94 to 1.13) | 2359 (5) | ++++ (high) | At a range of three to six months; low heterogeneity (I² = 0%) between studies and and subgroups |
| All cause mortality | RR 1.02 (0.90 to 1.16) | 2717 (11) | ++++ (high) | At a range of three weeks to six months; low heterogeneity (I² = 4%) between studies and and subgroups |
| Rebleeding | RR 0.65 (0.47 to 0.91) | 2717 (11) | +++ (moderate)a | Heterogeneity (I² = 59%) between studies and and subgroups |
| Delayed cerebral ischemia | RR 1.27 (1.00 to 1.62) | 2484 (7) | +++ (moderate)b | Heterogeneity (I² = 52%) between studies is largely based on early studies that did not implement ischemia preventive therapy. This resulted in a relatively high OR. Recent studies have implemented ischemia prevention as standard SAH care. It is likely that future research will result in a lower OR for DCI |
| Hydrocephalus | RR 1.09 (0.99 to 1.20) | 1992 (6) | ++++ (high) | Low heterogeneity (I² = 0%) between studies and and subgroups |
CI: confidence interval; DCI: delayed cerebral ischemia; OR: odds ratio; RR: risk ratio
aQuality reduced due to inconsistencies in results bQuality reduced due to inconsistency and indirectness
GRADE Working Group grades of evidence
High quality: further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: we are uncertain about the estimate.
Background
Description of the condition
In people with aneurysmal subarachnoid haemorrhage (SAH), rebleeding is a leading cause of death and disability (Roos 2000b; Stienen 2018). Without aneurysm treatment, approximately 30% of people with SAH experienced a rebleed within one month of the initial haemorrhage (Locksley 1966). The rebleeding rate has now been reduced to about 15%, because in most people, the aneurysm is occluded early after admission (Germans 2014; Roos 2000b). The risk of rebleeding is highest in the first 24 hours after aneurysmal SAH, with more than half of those rebleeds occurring in the first four hours (Germans 2014; Guo 2011). The prognosis after rebleeding is poor; approximately 60% of people who rebleed die, and another 30% remain dependent for activities of daily living (Naidech 2005; Stienen 2018).
Description of the intervention
Antifibrinolytic drugs have been used to reduce the occurrence of rebleeding for decades, and were first mentioned in 1967 (Gibbs 1967; Mullan 1967). These drugs are administered orally or intravenously, and block endogenous fibrinolytic activity in the hope of preventing rebleeding.
How the intervention might work
Dissolution of the blood clot at the site of the ruptured aneurysm is thought to be an important factor in the development of rebleeding. This dissolution probably results from endogenous fibrinolytic activity after SAH. Since antifibrinolytic agents reduce fibrinolytic activity, they may reduce the occurrence of rebleeding, and thereby, improve clinical outcome after SAH. However, concerns have been raised that antifibrinolytic therapy may cause an increase of other complications, such as delayed cerebral ischaemia or early brain injury, impeding the recovery from the initial haemorrhage. Delayed cerebral ischaemia is a complication of SAH that occurs in about 30% to 35% of people between 4 and 10 days after SAH. In older trials, the beneficial effect of antifibrinolytic treatment (reducing rebleeding) was offset by an increase in delayed cerebral ischaemia, resulting in a neutral effect on outcome (Baharoglu 2013). To reduce this complication, recent literature has been directed more towards short‐term antifibrinolytic therapy with concomitant preventative measures for the development of delayed cerebral ischaemia, which may prevent the negative effects, but still provide a protective effect for rebleeding.
Why it is important to do this review
In 1967, Gibbs and O'Gorman published the first report on antifibrinolytic treatment in people with SAH (Gibbs 1967). Since then, over 100 studies of antifibrinolytic therapy in aneurysmal SAH have been published. Unfortunately, most of these studies are uncontrolled, and only a minority of the controlled studies are randomised. Moreover, the results of some of the individual randomised studies contradict each other. Furthermore, as mentioned above, concerns have been raised that antifibrinolytic therapy might increase the occurrence of delayed cerebral ischaemia or early brain injury. In a previous version of this review, we found that short‐term antifibrinolytic treatment in people concomitantly treated with measures to prevent or reverse cerebral ischaemia, may be more effective than the administration regimen in older studies (Baharoglu 2013). This led to the hypothesis that when people with aneurysmal SAH are treated according to current guidelines, and with short‐term antifibrinolytic agents, the beneficial effect of reducing rebleeds is not impeded by complications from the treatment itself. In this update of the 2013 Cochrane Review, we searched for new trials, and gave particular attention to evaluate the effectiveness of short‐term antifibrinolytic treatment in people concomitantly treated with measures to prevent or reverse delayed cerebral ischaemia (Baharoglu 2013).
Objectives
To assess the effects of antifibrinolytic treatment in people with aneurysmal subarachnoid haemorrhage.
Methods
Criteria for considering studies for this review
Types of studies
All randomised trials in which, after concealed allocation, antifibrinolytic drugs were compared with control treatment (open studies) or placebo (blind studies) in an intention‐to‐treat analysis.
We excluded all trials in which allocation to treatment or control group was not concealed (e.g. trials in which people were allocated by means of an open random number list, alternation, or based on date of birth, days of the week, or hospital number), since foreknowledge of treatment allocation might lead to biased treatment allocation (i.e. selective enrolment). We also excluded trials in which an intention‐to‐treat analysis was not performed, and could not be reconstructed on the basis of published data without a loss of 20% or more of all randomised participants.
Types of participants
Trials in which participants were included with clinical symptoms and signs of subarachnoid haemorrhage (SAH), presumably caused by a ruptured aneurysm, and with confirmation of the diagnosis by the presence of subarachnoid blood on computed tomography (CT) scan, or on cerebrospinal fluid (CSF) examination.
Types of interventions
Antifibrinolytic drugs (e.g. tranexamic acid, epsilon amino‐caproic acid, or equivalent drugs), oral or intravenous, versus control treatment (open studies) or placebo treatment (blind studies). Since the risk of rebleeding is highest during the first two weeks after the initial bleeding, treatment had to start within two weeks after onset of the SAH. Distinction was made between a combination of early start and short‐term duration(< 72 hours of onset of symptoms, i.e. before usual timing of onset of cerebral ischaemia) versus long‐term (> 72 hours) treatment duration and concomitant measures to prevent delayed cerebral ischaemia or not.
Types of outcome measures
Primary outcomes
The primary outcome measure was poor outcome (death, vegetative state, or (moderate) severe disability), assessed with either the Glasgow Outcome Scale or the Modified Rankin Scale, at the end of at least three months of follow‐up after SAH.
Death from all causes, at a minimum follow‐up of at least three weeks, was our second primary outcome, since most studies only reported on case fatality.
Secondary outcomes
Secondary outcome measures were the effects of antifibrinolytic treatment on both the rates of reported and CT scan, or autopsy confirmed (sensitivity analyses) episodes of rebleeding, delayed cerebral ischaemia, and hydrocephalus.
Search methods for identification of studies
We searched for trials in all languages, and arranged translations of relevant reports when required.
Electronic searches
We searched the Cochrane Stroke Group Trials Register (last searched 31 May 2022), the Cochrane Central Register of Controlled Trials (CENTRAL; 2021, issue 3) in the Cochrane Library (searched 31 May 2022; Appendix 1), MEDLINE Ovid (1946 to 31 May 2022; Appendix 2), and EMBASE Ovid (1980 to 31 May 2022; Appendix 3).
We developed comprehensive search strategies with the help of the Cochrane Stroke Group Information Specialist, and adapted the MEDLINE strategy for CENTRAL and Embase. Where appropriate, we combined them with subject strategy adaptations of the highly sensitive search strategies, designed by Cochrane to identify RCTs and controlled clinical trials (described in the Technical Supplement to Chapter 4 in the Cochrane Handbook for Systematic Reviews of Interventions (Lefebvre 2021)).
All search strategies were revised and updated to account for newly identified, relevant index headings, and keywords. Both versions of the search strategies are included in Appendix 4 and Appendix 5.
We also searched the following trial registers for ongoing clinical trials.
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; searched 31 May 2022; Appendix 6)
World Health Organization (WHO) International Clinical Trials Registry Platform (www.trialsearch.who.int; searched 31 May 2022; Appendix 7)
The following resources were searched for the previous iteration of this review. The EU Clinical Trials Register and ISRCTN data sets are now accessible in the WHO International Clinical Trials Registry Platform; the Stroke Trials Registry site is no longer operational.
EU Clinical Trials Register (https://www.clinicaltrialsregister.eu; last searched 1 December 2012)
Stroke Trials Registry (www.strokecenter.org/trials/; last searched 1 December 2012)
ISRCTN registry (formerly known as Current Controlled Trials; www.isrctn.com; last searched 1 December 2012)
Searching other resources
In an effort to identify further published, unpublished, and ongoing studies:
we searched the list of references quoted in all included studies and reviews on antifibrinolytic therapy (Adams 1982; Adams 1987; Biller 1988; Carley 2005; Chawjol 2008; Connolly 2012; Fodstad 1982; Lindsay 1987; Maira 2006; Mayberg 1994; Post 2021; Ramirez 1981; Ren 2021; Rinkel 2008; Van Gijn 2001; Van Gijn 2007; Vermeulen 1980; Vermeulen 1996; Weaver 1994; Weir 1987);
we used Science Citation Index Cited Reference Search for forward tracking of important articles; and
for the first version of this review (Roos 1998), we contacted the pharmaceutical company Pharmacia and Upjohn, formerly Kabi, manufacturer and license holder of the antifibrinolytic drug tranexamic acid. We identified no additional (unpublished) studies.
Data collection and analysis
Selection of studies
Two review authors (MRG and WJD) independently screened the titles and abstracts of the records obtained from the electronic searches and excluded obviously irrelevant records. We obtained the full‐text articles for the remaining studies, and the same two review authors independently selected the trials that met the predefined inclusion criteria. The review authors resolved disagreements by discussion, and when necessary, in consultation with a third review author (YBWEMR).
Data extraction and management
Two review authors (MRG and WJD) independently reviewed the additional eligible studies, and extracted details on the number of participants in the treated and the placebo or control groups, the randomisation method, blinding method, the definitions for diagnosis and complications, and also ascertained whether an intention‐to‐treat analyses was done or could be reconstructed from the published data. When consensus could not be reached, the review authors consulted a third review author (YBWEMR).
Assessment of risk of bias in included studies
Two review authors (MRG and WD) independently assessed the risk of bias of each additional study using RoB 1, which comprises the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 8 (Higgins 2011). Any disagreements were resolved by discussion. We assessed the risk of bias according to the following domains.
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias): all outcomes
Blinding of outcome assessment (detection bias): all outcomes
Incomplete outcome data (attrition bias): all outcomes
Selective outcome reporting (reporting bias)
Other bias
We graded each potential source of bias as high risk, low risk, or unclear risk of bias, and provided information from each study in the risk of bias tables.
Measures of treatment effect
We processed data in accordance with the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 6 (Higgins 2022). For the primary outcome, we dichotomised the outcome scales between good and poor outcome for the analysis. Poor outcome was defined as death, vegetative state, or (moderate) severe disability, as assessed with either the Glasgow Outcome Scale or the modified Rankin Scale. We scored death from any cause, rates of rebleeding, delayed cerebral ischaemia, and hydrocephalus per treatment group. We expressed effects as risk ratios (RR) with 95% confidence intervals (CI).
Unit of analysis issues
The unit of analysis was the individual participant, since we only included individually randomised trials with a parallel design.
Dealing with missing data
In trials without intention‐to‐treat analysis, we tried to reconstruct one, based only on the published data. When the proportion of missing values for outcome was less than 20%, we included the study in our analysis. For two trials, we tried to contact the principal investigator to retrieve data on the number of participants in whom rebleeding or cerebral ischaemia were proven on CT scan or at autopsy (Hillman 2002; Tsementzis 1990). We received a reply from one of the study authors. We made no effort to obtain additional information for studies published 15 or more years ago.
Assessment of heterogeneity
For each outcome, we assessed statistical heterogeneity using the I²statistic, according to the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 10 (Higgins 2022). We considered an I² statistic less than 50% as low heterogeneity.
Assessment of reporting biases
To investigate possible publication bias, we planned to create funnel plots for poor outcome, death from all causes, and the rebleeding rate, if they were measured by at least 10 studies, according to the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 13 (Higgins 2022).
Data synthesis
Because we expected heterogeneity between studies, we used the Mantel‐Haenszel random‐effects model for pooled analyses, in Review Manager software (Review Manager Web 2020).
Subgroup analysis and investigation of heterogeneity
To assess whether masked studies showed different results from unmasked studies, we divided all analyses into two groups: trials with control treatment (open studies) and trials with placebo treatment (blind studies). We added an additional subgroup analysis to evaluate the effect of antifibrinolytic therapy on all outcomes in trials with and without additional measures to prevent or reverse delayed cerebral ischaemia, and to evaluate the effect of antifibrinolytic therapy according to treatment duration. We divided the included trials into one of three groups: (1) trials without ischaemia prevention and treatment duration > 72 hours, (2) trials with ischaemia prevention and treatment duration > 72 hours, and (3) trials with ischaemia prevention and treatment duration < 72 hours. Because we defined that a minimum of one study should be included in a subgroup, we did not include a fourth group (trials without ischaemia prevention and treatment duration < 72 hours), as there were no trials that met these criteria.
In addition, we checked whether data were available on aneurysm treatment (i.e. clipping or coiling) according to antifibrinolytic treatment, to evaluate whether a subgroup analysis on clipping versus coiling was possible.
Sensitivity analysis
Because our secondary outcome measures were more prone to bias, we carried out sensitivity analyses on confirmed (rather than reported) rebleeding, delayed cerebral ischaemia, and hydrocephalus rates.
Summary of findings and assessment of the quality of the evidence
We reported the summary of findings according to the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 14 (Higgins 2022). We assessed the quality of the evidence by investigating imprecision by 95% confidence intervals, inconsistency by heterogeneity, indirectness, and study and publication bias by reporting them in risk of bias tables, according to GRADE. Outcomes included poor outcome (death, vegetative state, or (moderate) severe disability), all‐cause mortality, rebleeding, delayed cerebral ischaemia, and hydrocephalus.
Summary of findings and assessment of the certainty of the evidence
We reported the summary of findings according to the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 14 (Higgins 2022). We assessed the quality of the evidence by investigating imprecision by 95% confidence intervals, inconsistency by heterogeneity, indirectness, and study and publication bias by reporting them in risk of bias tables according to GRADE. Outcomes included poor outcome (death, vegetative state, or (moderate) severe disability), all‐cause mortality, rebleeding, delayed cerebral ischemia, and hydrocephalus.
Results
Description of studies
Results of the search
The updated 2022 search of the bibliographic databases yielded a total of 1024 records, from which we removed 146 duplicates, leaving a total of 878 records. After screening titles and abstracts, we excluded 872 records, leaving six records for which we obtained the full‐text articles. Three studies were included in the list of excluded studies in the previous version. Further assessment resulted in one potentially relevant trial (Post 2021). Eleven trials met the inclusion criteria for the review; we excluded eight trials. For an overview of the search results, see Figure 1.
1.
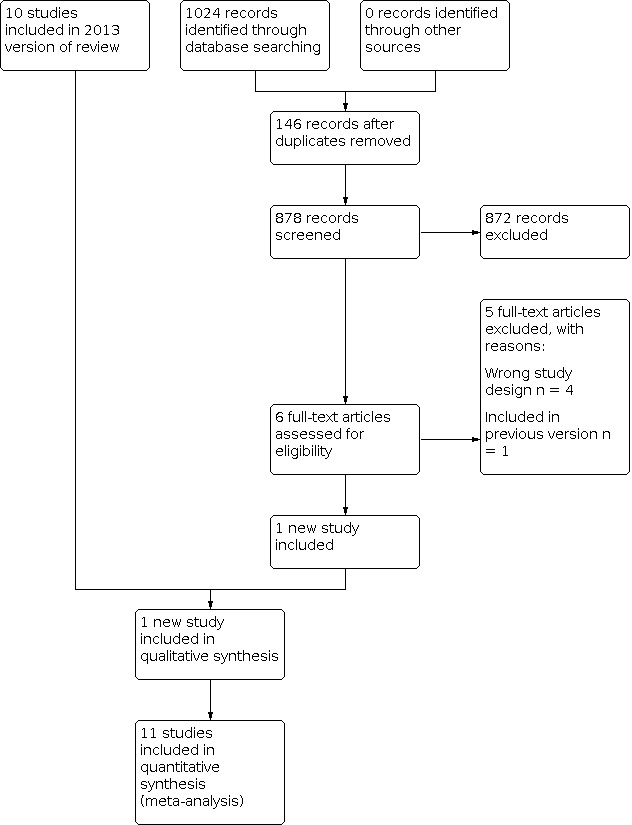
PRISMA overview of updated search (December 2012 to May 2022)
Included studies
Since the previously published review of Baharoglu 2013, one new trial met the inclusion criteria (Post 2021). Therefore, we included 11 studies, which are described in detail in the Characteristics of included studies table (Chandra 1978; Fodstad 1981; Girvin 1973; Hillman 2002; Kaste 1979; Maurice 1978; Post 2021; Roos 2000a; Tsementzis 1990; Van Rossum 1977; Vermeulen 1984). These 11 studies included 2717 participants, 1368 of whom were randomised to receive antifibrinolytic drugs, 597 to receive placebo treatment, and 752 to receive control treatment. The Girvin 1973 study used epsilon‐amino‐caproic acid (39 participants); tranexamic acid was used in all other studies. The Post 2021 study is the largest trial, including 955 participants; however, the study also included participants with non‐aneurysmal SAH (14%). The data for the current review were extracted from Tsementzis 1990, which only presented the results of the aneurysmal SAH (Post 2021). In three studies, participants were concomitantly treated with measures to prevent or reverse cerebral ischaemia (Hillman 2002; Post 2021; Roos 2000a). The duration of antifibrinolytic treatment differed considerably between studies, and ranged from less than 72 hours to six weeks. Short‐term treatment was used in two studies (Hillman 2002; Post 2021). In these studies, participants were treated up to 72 hours after SAH (Hillman 2002), or up to 24 hours after the start of tranexamic acid treatment (Post 2021). All other studies treated participants for at least 10 days (or until occlusion of the aneurysm) after SAH.
Five studies reported clinical outcome, and we were able to reconstruct the number of participants with poor outcomes (Hillman 2002; Post 2021; Roos 2000a; Tsementzis 1990; Vermeulen 1984). Death from all causes and rebleeding rates were reported in all 11 studies. In six studies, episodes of rebleeding were defined primarily by clinical symptoms.
Three trials reported computed tomography (CT) scan‐ or autopsy‐confirmed episodes of rebleeding (Fodstad 1981; Hillman 2002; Post 2021). Three trials defined and reported rebleeding in two ways: as 'probable' if the diagnosis was suspected solely on clinical grounds, and as 'definite' when proven by CT (after comparison with an earlier CT), or at autopsy; the Dutch‐British trial (Vermeulen 1984), STAR study (Roos 2000a), and the ULTRA trial (Post 2021).
Delayed cerebral ischaemia was reported in seven studies, but defined in only four: in two studies, cerebral ischaemia was defined and reported in the same manner as episodes of rebleeding; as 'probable' and as 'definite' (CT scan‐ or autopsy‐confirmed) cerebral ischaemia (Roos 2000a; Vermeulen 1984). Again, as for rebleeding, Fodstad 1981 reported on CT scan‐ or autopsy‐confirmed cerebral ischaemia. Post 2021 defined delayed cerebral ischaemia according to the definition used by a multidisciplinary research group (Vergouwen 2010). Hillman 2002 reported the percentage of transient and permanent delayed ischaemic neurological deficits. No clear definition was given, and CT scans were not routinely used to confirm delayed cerebral ischaemia. Because other studies did not make a distinction between permanent or transient delayed cerebral ischaemia, we decided to combine these outcomes. Hillman 2002 reported visible infarction on CT scan; however, after contact with the study author, we decided not to use this as a measure for delayed cerebral ischaemia, since this was not always correlated to clinical signs of delayed cerebral ischaemia. The other two studies made no distinction between participants with episodes clinically suggestive of delayed cerebral ischaemia, or participants with confirmed delayed cerebral ischaemia, and reported only an all‐inclusive number of participants (Girvin 1973; Tsementzis 1990). One study reported on 'delayed cerebral ischaemia' and 'postoperative ischaemia' (Roos 2000a). Since the other studies did not make this distinction, and reported an overall number of participants with delayed cerebral ischaemia, we grouped these subgroups of ischaemia for the analysis on cerebral ischaemia.
Six trials reported on hydrocephalus. Hydrocephalus was defined in two studies by means other than clinical grounds, and therefore, could be included in the sensitivity analysis for confirmed hydrocephalus (Post 2021; Roos 2000a). No trials reported on aneurysm treatment modality (i.e. coiling versus clipping) according to antifibrinolytic or control treatment, and thus, we were unable to undertake a subgroup analysis based on aneurysmal occlusion modality.
Excluded studies
We excluded eight studies (see Characteristics of excluded studies table): some were comparative trials between two or more antifibrinolytic agents, others used unconcealed allocation, and some were not randomised but used historical controls. We excluded Fodstad 1978, as 23% of the participants in the trial were later excluded, and we were unable to reconstruct an intention‐to‐treat analysis on the basis of the published data.
Risk of bias in included studies
For a summary of the risk of bias see Figure 2 and Figure 3. Six of the 11 included trials used an intention‐to‐treat analysis; in one of the remaining trials, we were unable to reconstruct this analysis using the available follow‐up data (Maurice 1978).
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study
3.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
Allocation
Girvin 1973 used 'flip‐of‐a‐coin' randomisation as the method of allocation, which is more susceptible to bias compared with, for instance, the sealed envelope method. Nevertheless, we decided to include this study, since this is an accepted form of randomisation with allocation sequence generation and concealment according to Cochrane guidelines. All other studies used a method of concealed allocation that was considered appropriate at the time the trial was conducted, although it was not always mentioned whether or not the sealed envelopes that were used were opaque, resulting in an unclear risk of bias assessment (Fodstad 1981; Hillman 2002).
Blinding
Six studies used a double‐blind method (placebo controlled), and five used a control group with standard treatment without placebo. The control group studies were open label, and we rated them at high risk of performance bias (all five studies), and detection bias (one study: Hillman 2002).
Incomplete outcome data
In five trials, there was no follow‐up information available for participants who were excluded after randomisation (Fodstad 1981; Hillman 2002; Post 2021; Tsementzis 1990; Van Rossum 1977). In four studies, a very small number of participants were excluded from the final analysis (Fodstad 1981 (n = 1); Post 2021 (n = 10); Tsementzis 1990 (n = 4); Van Rossum 1977 (n = 3); therefore, we still included these studies.
In one study, 91 (15%) of the 596 participants were excluded after randomisation (Hillman 2002). Because this was less than the prespecified proportion of 20%, we included this study in our analysis. We rated this study at high risk of bias for incomplete outcome data (attrition bias).
Selective reporting
In one study, no previously published protocol was mentioned, and clinical outcome was reported, although not described, in the introduction or methods (Hillman 2002). For the Post 2021 study, a protocol was published (Germans 2013). The primary outcome and most secondary outcomes were reported, including all secondary outcomes relevant to this review. In two other studies, the selective reporting could not be assessed, and we reported them as unclear risk of bias (Chandra 1978; Tsementzis 1990).
Other potential sources of bias
No studies showed a high risk of other source of bias, however, in four studies, we could not assess this, and therefore, we reported them as unclear risk of bias (Chandra 1978; Kaste 1979; Maurice 1978; Tsementzis 1990). The funnel plots for death and rebleeding are shown in Figure 4 and Figure 5. The plot on 'poor outcome' (Figure 5), shows no asymmetry and heterogeneity was low between studies, indicating no publication bias.
4.

Funnel plot of included trials assessing case fatality
5.

Funnel plot of included trials assessing rebleeding
Effects of interventions
See: Table 1
Antifibrinolytic treatment versus control treatment with or without placebo
Poor outcome
The results were inconclusive for poor outcome (risk ratio (RR) 1.03, 95% confidence interval (CI) 0.94 to 1.13; P = 0.53; 5 trials, 2359 participants; high‐quality evidence; Analysis 1.1). The results remained inconclusive when analysed by duration of treatment (P = 0.83; Analysis 1.2).
1.1. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 1: Poor outcome (death, vegetative, or (moderate) severe disability) at end of follow‐up: open versus blind studies
1.2. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 2: Poor outcome (death, vegetative, or (moderate) severe disability) at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration
All‐cause mortality
The pooled RR for our second primary outcome measure, all‐cause mortality, was 1.02 (95% CI 0.90 to 1.16; P = 0.77; 11 trials, 2717 participants; high‐quality evidence; Analysis 1.3). Duration of treatment showed no effect on all‐cause mortality (P = 0.77; Analysis 1.4).
1.3. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 3: Death from all causes at end of follow‐up: open versus blind studies
1.4. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 4: Death from all causes at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration
Confirmed rebleeding
In the analysis on rebleeding rates, antifibrinolytic therapy reduced the risk of rebleeding (RR 0.65, 95% CI 0.47 to 0.91; P = 0.01; 11 trials, 2717 participants; moderate‐quality evidence; absolute risk reduction 7%, 95% CI 3 to 12%; Analysis 1.5). Heterogeneity was detected for this comparison (I² = 59%; P = 0.007; Analysis 1.5). Similar estimates were found in the subgroup analysis of the six double‐blind and placebo‐controlled studies (RR 0.64; P = 0.03; Analysis 1.5); the sensitivity analysis including five studies with CT scan‐ or autopsy‐confirmed rebleeding (RR 0.50; P < 0.001; Analysis 1.6); and in the subgroup analysis of two studies with ischaemia prevention and < 72 hours of treatment (RR 0.42; P = 0.14; Analysis 1.7).
1.5. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 5: Rebleeding reported at end of follow‐up: open versus blind studies
1.6. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 6: Confirmed rebleeding at end of follow‐up (sensitivity analysis): open versus blind studies
1.7. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 7: Rebleeding reported at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration
Delayed cerebral ischaemia
Seven trials that reported delayed cerebral ischaemia rates showed moderate‐quality evidence that antifibrinolytic treatment increased the risk of delayed cerebral ischaemia (RR 1.27, 95% CI 1.00 to 1.62; P = 0.05; 7 trials, 2484 participants; moderate‐quality evidence; absolute increase of 36 per 1000 people; Analysis 1.8). Similar effects were seen in the subgroup analysis of the three placebo‐controlled trials (RR 1.38; P = 0.17; Analysis 1.8). This effect was reduced, and showed no association after the implementation of ischaemia preventative measures and < 72 hours of treatment (RR 1.10; P = 0.49; Analysis 1.10). Heterogeneity of intervention effect was detected in all seven studies combined (I² = 52%; P = 0.05; Analysis 1.10). This effect was reduced in the two trials with ischaemia prevention and treatment < 72 hours, with low heterogeneity (I² = 35%; P = 0.49; Analysis 1.10).
1.8. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 8: Delayed cerebral ischaemia reported at end of follow‐up: open versus blind studies
1.10. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 10: Delayed cerebral ischaemia reported at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration
Hydrocephalus
Hydrocephalus was reported in six trials. Overall, antifibrinolytic treatment had no effect on the reported rates of hydrocephalus (RR 1.09, 95% CI 0.99 to 1.20; P = 0.09; 6 trials, 1992 participants; high‐quality evidence; Analysis 1.11). In the subgroup analysis on placebo versus open studies, antifibrinolytic treatment in the placebo controlled studies showed a more pronounced effect for hydrocephalus (RR 1.19; P = 0.13; Analysis 1.11), whereas in the open label trials, it was more protective for hydrocephalus (RR 0.94; P = 0.73; Analysis 1.11). The sensitivity analysis on two trials with CT scan‐ or autopsy‐confirmed hydrocephalus, including 93% of all hydrocephalus patients, showed no association between antifibrinolytic treatment and hydrocephalus (RR 1.09, 95% CI 0.99 to 1.21; P = 0.09; 2 trials, 1275 participants; Analysis 1.12). Ischaemia prevention did not seem to have any effect on hydrocephalus in the subgroup analyses (P = 0.85; Analysis 1.13).
1.11. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 11: Hydrocephalus reported at end of follow‐up: open versus blind studies
1.12. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 12: Confirmed hydrocephalus at end of follow‐up (sensitivity analysis): open versus blind studies
1.13. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 13: Hydrocephalus reported at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration
Discussion
Summary of main results
Although this systematic review and meta‐analysis show that antifibrinolytic treatment reduces the rate of rebleeding by approximately 35%, there is no evidence of benefit from antifibrinolytic treatment on poor outcome or death from all causes. We added the recent and largest ULTRA trial, which administered antifibrinolytic treatment ultra‐early and short‐term, to the review, but there was no change in the overall conclusion compared to previous versions (Post 2021). A sensitivity analysis on trials with ischaemia prevention and short‐term (< 72 hours) antifibrinolytic treatment did not show a difference in the effect on either poor outcome, or death from all causes. Furthermore, the risk for delayed cerebral ischaemia was not increased by antifibrinolytic treatment when ischaemia preventative measures were applied. The current, high‐quality evidence does not support the routine use of antifibrinolytic treatment in people with aneurysmal subarachnoid haemorrhage.
Overall completeness and applicability of evidence
Trials in which people were included with symptoms and signs of subarachnoid haemorrhage (SAH) of suspected or proven aneurysmal cause, with confirmation of the diagnosis by the presence of subarachnoid blood on computed tomography (CT) or on cerebrospinal fluid (CSF) examination were eligible for this review. We chose this pragmatic approach, and did not restrict our review to people with angiographically‐proven aneurysms, because antifibrinolytic treatment may also be started after CT angiography (CTA)‐confirmed presence of an intracranial aneurysm. However, we chose not to limit our analysis to radiologically‐proven aneurysmal SAH, because CTA was not regularly applied when most of the trials were conducted. In the past decades, the outcome of aneurysmal SAH has constantly improved, which is attributable to improved intensive care management, aneurysm treatment techniques, and reduced interval to aneurysm treatment. Especially, earlier aneurysm treatment may have had influence on a reduced incidence of rebleeds, diminishing the potential effect of reducing rebleeds by antifibrinolytic treatment. Nevertheless, the evidence undisputedly shows that despite a significant reduction in rebleeds, the overall outcome is not improved with antifibrinolytic therapy. However, the current evidence is unclear about the effect of antifibrinolytic treatment in a subgroup of people at a very high risk for rebleeding, such as those who are diagnosed very early, or in those for whom there is anticipated delay in aneurysm treatment.
The included trials were performed in a timespan of 48 years, during which overall clinical outcome has improved. Treating people with aneurysmal SAH with preventative measures for delayed cerebral ischaemia has eliminated the increased risk of this complication of antifibrinolytic treatment. Even then, antifibrinolytic treatment does not improve poor outcome or death from all causes. The consistency of results in several studies with low risks of bias, and persistency over years even with optimisation of the treatment of complications, makes this conclusion generalisable. It is very unlikely that future trials will change the conclusion that routine antifibrinolytic treatment has no evidence of benefit in people with aneurysmal subarachnoid haemorrhage.
Quality of the evidence
We only included true randomised controlled trials, and performed a subgroup analysis on placebo‐controlled versus open studies in an attempt to minimise allocation and performance bias. Many of the included studies were older (published between 1973 and 1990), and most did not report on many sources of potential bias, such as how the randomisation sequence was generated, and whether participant outcome was assessed by individuals who were blinded to the given intervention. Therefore, we scored many potential sources as unclear risk of bias, as can be seen in Figure 2 and Figure 3. Luckily, the studies assessed with several sources of unclear risk were small, and in total, comprised about 10% of all included participants. The majority of the included participants originated from four studies (Hillman 2002; Post 2021; Roos 2000a; Vermeulen 1984). Three of these studies, comprising 65% of all data, were rated as low risk of bias for all sources, except for performance bias in Post 2021 (Post 2021; Roos 2000a; Vermeulen 1984). In Hillman 2002, many potential sources of bias could not be scored and were unclear, such as sequence generation, allocation concealment, and blinded outcome assessment. Moreover, 15% of included participants were later excluded from the analysis, and the baseline characteristics and outcomes of these participants were not reported. We included this study in the subgroup analysis with ischaemia prevention and treatment duration < 72 hours, in which the much larger and methodologically sound study of Post 2021 was also included. Because the latter study showed no large changes in effect on primary outcomes compared to Hillman 2002, and because heterogeneity between studies was probably not important for poor outcome (I² 33%; Analysis 1.1); and death from all causes (I² 0%; Analysis 1.3), we assume that the results of this subgroup are trustworthy.
Visual inspection of the funnel plots for death from all causes at end of follow‐up (Figure 4), and rebleeding reported at end of follow‐up (Figure 5), revealed a potential publication bias, with a lack of small studies showing a harmful effect (RR > 1) of antifibrinolytic treatment. We did not do a statistical analysis on these plots, due to the relatively small number of studies. Because several large randomised studies have been performed, the influence of small studies with negative results that were not published would not have changed the overall estimate of death or rebleeding after treatment with antifibrinolytic therapy.
Potential biases in the review process
We searched all major medical electronic databases and other sources, using sensitive and validated search strategies. However, it is possible that we did not find all relevant publications. Furthermore, we only included studies that were published in medical literature and did not search the grey literature, such as government reports and unpublished information. Although all included trials met the predefined inclusion criteria, the studies differed considerably in participant selection, disease severity at baseline, start and duration of treatment, dosage and type of trial medication, classification of events, outcome assessment, and duration of follow‐up. This clinical heterogeneity may, in part, account for the statistical heterogeneity found in the analyses on rebleeding and delayed cerebral ischaemia. The process of selecting eligible studies and assessing sources of bias in the latest version of this review were not performed by the same assessors as in previous versions. However, one of the assessors in the current version was also an assessor in the previous version (MRG), which should have reduced interobserver variability, and therefore, reduced observer bias.
Agreements and disagreements with other studies or reviews
Our results are similar to the results from the most recent meta‐analysis (Ren 2021). Ren 2021 included all randomised controlled trials included in the present update, except Girvin 1973. Our results are also comparable with Gaberel 2012, in which all studies compared antifibrinolytic treatment with control treatment, including retrospective analyses, and studies with historical control groups. Retrospective analyses are known to be much more susceptible to selection and reporting bias, since the decision to treat a person is made subjectively. Gaberel 2012 did not compare placebo‐controlled versus open studies, which is another potential source of bias, since all outcomes, except for death, are made on subjective clinical grounds, and can be easily biased when the outcome assessor is not blinded to the treatment given.
We only included randomised clinical trials in our review, and performed several sensitivity analyses, which should yield less biased results. Since most studies did not describe whether outcomes were assessed by a blinded outcome assessor, sensitivity analyses were essential. Despite the fact that all study authors reported that confirmation of rebleeding was investigated, in many cases, the diagnosis of rebleed was confirmed by examination of the CSF. Because CSF examination is an unreliable test to confirm rebleeding, we were not always able to prove the diagnosis of rebleeding (Vermeulen 1983). Therefore, we decided to perform sensitivity analyses on reported versus confirmed (with confirmatory evidence on CT scan or at autopsy) rebleeding, cerebral ischaemia, and hydrocephalus. These different analyses showed similar results, so lack of confirmatory evidence of these complications appears to be of minor importance in our analyses. The analyses we performed on trials with a control treatment compared with those given placebo treatment showed similar reducing effects of antifibrinolytic treatment on rebleeding, and similar increasing effects on delayed cerebral ischaemia, whereas, hydrocephalus trials with a control treatment showed a tendency towards a beneficial effect compared with trials with placebo treatment, demonstrating a tendency towards increased hydrocephalus rates.
Authors' conclusions
Implications for practice.
Antifibrinolytic treatment does not improve clinical outcome in people after aneurysmal subarachnoid haemorrhage, although it does reduce the risk of rebleeding. Based on the currently available data, there is no evidence to support routine treatment with antifibrinolytic drugs for people with subarachnoid haemorrhage from a presumed or proven aneurysmal origin.
Implications for research.
Over decades, the interval between initial haemorrhage and aneurysm treatment has reduced. This is not only attributable to the improved in‐hospital logistics and resources, but also to the earlier diagnosis and shorter transfer time of people to a centre that specialises in aneurysm treatment. The earlier assessment of people with an aneurysmal subarachnoid haemorrhage inherently increases the rebleed rate, because the majority of rebleeds occur in the first hours after the initial haemorrhage. More detailed analysis of the time intervals between initial haemorrhage, start of antifibrinolytic treatment, and aneurysm treatment in relation to rebleeds may reveal a subgroup who could benefit from a reduction in rebleed rate by antifibrinolytic treatment.
What's new
| Date | Event | Description |
|---|---|---|
| 31 May 2022 | New citation required but conclusions have not changed | Conclusions not changed |
| 31 May 2022 | New search has been performed | We included one more major study with 813 participants (Post 2021), resulting in a total of 11 included studies involving 2717 participants. We updated the searches, and included a summary of findings table. |
History
Protocol first published: Issue 3, 1998 Review first published: Issue 3, 1998
| Date | Event | Description |
|---|---|---|
| 5 September 2013 | Feedback has been incorporated | Minor layout changes |
| 4 February 2013 | New citation required and conclusions have changed | A new subgroup analysis was added and the conclusions changed. |
| 4 February 2013 | New search has been performed | Updated searches completed and a new study added. We included one new study with 505 participants (Hillman 2002).This study is different in treatment timing and duration of therapy, and contributes 26.5% of all participants. The review now includes 10 trials and 1904 participants in total. |
| 21 July 2008 | Amended | Converted to new review format. |
| 7 February 2003 | New search has been performed | We added the results of the recently published STAR‐study, the second largest placebo‐controlled randomised trial of antifibrinolytic treatment in subarachnoid haemorrhage to the review. This study contributes 33% of all included participants in this review, and 39% of the participants included in the comparison of antifibrinolytic treatment versus placebo. We also added a plain language summary. |
Acknowledgements
Previous versions of this review were supported by research grants from the Netherlands Heart Foundation (Nederlandse Hart Stichting). We thank Brenda Thomas and Joshua Cheyne for their help in developing and performing the new electronic database searches. We thank Hazel Fraser for her editorial advice.
Appendices
Appendix 1. CENTRAL search strategy, 2022 update
ID Search Hits #1 MeSH descriptor: [Subarachnoid Hemorrhage] this term only 592 #2 MeSH descriptor: [Intracranial Hemorrhages] this term only 280 #3 MeSH descriptor: [Cerebral Hemorrhage] this term only 975 #4 MeSH descriptor: [Intracranial Aneurysm] this term only 443 #5 MeSH descriptor: [Rupture, Spontaneous] this term only 110 #6 #4 and #5 28 #7 MeSH descriptor: [Aneurysm, Ruptured] this term only 130 #8 MeSH descriptor: [Brain] explode all trees 11710 #9 MeSH descriptor: [Meninges] explode all trees 295 #10 #8 or #9 11983 #11 #7 and #10 10 #12 ((subarachnoid or arachnoid) near/6 (haemorrhage* or hemorrhage* or bleed* or blood*)):ti,ab,kw 2058 #13 MeSH descriptor: [Vasospasm, Intracranial] this term only 151 #14 ((cerebral or intracranial or cerebrovascular) near/6 (vasospasm or spasm)):ti,ab,kw 530 #15 (sah):ti,ab,kw 903 #16 #1 or #2 or #3 or #6 or #11 or #12 or #13 or #14 or #15 3535 #17 MeSH descriptor: [Antifibrinolytic Agents] explode all trees 781 #18 (anti‐fibrinolytic* or antifibrinolytic* or antifibrinolysin* or anti‐fibrinolysin* or antiplasmin* or anti‐plasmin* or (plasmin near/3 inhibitor*)):ti,ab,kw 1675 #19 (fibrinolysis near/3 (prevent* or inhib* or antag*)):ti,ab,kw 292 #20 MeSH descriptor: [Tranexamic Acid] this term only 1107 #21 ("4 amino methylcyclohexane carboxylate" or "4 aminomethylcyclohexanecarbonic acid" or "4 aminomethylcyclohexanecarboxylic acid" or amca or AMCHA):ti,ab,kw 33 #22 (amchafibrin or amikapron or "aminomethyl cyclohexane carboxylic acid" or "aminomethyl cyclohexanecarboxylic acid" or "aminomethylcyclohexane carbonic acid" or "aminomethylcyclohexane carboxylic acid"):ti,ab,kw 17 #23 ("aminomethylcyclohexanecarbonic acid" or "aminomethylcyclohexanecarboxylic acid" or "aminomethylcyclohexanocarboxylic acid" or "aminomethylcyclohexanoic acid" or amstat or anexan or antivoff or anvitoff orcaprilon or "cis 4 aminomethylcyclohexanecarboxylic acid" or "cis aminomethyl cyclohexanecarboxylic acid"):ti,ab,kw 4 #24 ("cl 65336" or cl65336 or cyclocapron or cyclokapron or cyklocapron or cyklokapron or exacyl or fibrinon or frenolyse or hemostan or hexacapron or hexakapron or "kabi 2161" or kalnex or micranex or para "aminomethylcyclohexane carboxylic acid"):ti,ab,kw 70 #25 (rikaparin or ronex or spotof or theranex or tramic or tranex or tranexam or "tranexamic acid" or "tranexanic acid" or tranexic or "trans 1 aminomethylcyclohexane 4 carboxylic acid" or "trans 4 aminomethylcyclohexane 1 carboxylic acid" or "trans 4 aminomethylcyclohexane carboxylic acid"):ti,ab,kw 2963 #26 ("trans 4 aminomethylcyclohexanecarboxylic acid" or "trans achma" or "trans amcha" or "trans aminomethyl cyclohexane carboxylic acid" or "trans aminomethylcyclohexane carboxylic acid"):ti,ab,kw 3 #27 ("trans aminomethylcyclohexanecarboxylic acid" or transamin or "transaminomethylcyclohexane carboxylic acid" or "transexamic acid" or traxamic or trenaxin or ugurol):ti,ab,kw 31 #28 MeSH descriptor: [Aminocaproates] explode all trees 205 #29 (acikaprin or afibrin or amicar or "amino caproic acid" or "aminocaproic acid" or "aminohexanoic acid" or capracid or capramol or caproamin or caprocid or caprogel or caprolest or caprolisin or caprolisine or "caprolysin orcapromol"):ti,ab,kw 282 #30 ("cl 10304" or cl10304 or "cy 116" or cy116 or "e aminocaproic acid" or EACA or ecapron or ekaprol or epsamon or epsicaprom or epsicapron or epsikapron or epsilcapramin or "epsilon amino caproate" or "epsilon amino caproic acid"):ti,ab,kw 114 #31 ("depsilon aminocaproate" or "epsilon aminocaproic acid" or "epsilonaminocaproic acid" or epsilonaminocapronsav or "etha aminocaproic acid" or "ethaaminocaproic acid" or "gamma aminocaproic acid" or "gamma aminohexanoic acid"):ti,ab,kw 165 #32 (hemocaprol or hepin or hexalense or ipsilon or "jd 177" or jd177 or neocaprol or "nsc 26154" or nsc26154 or resplamin or tachostyptan):ti,ab,kw 2 #33 MeSH descriptor: [Aprotinin] this term only 522 #34 ("9921 rp" or antagosan or antilysin or antilysine or apronitin or apronitine or apronitrine or aprotimbin or "aprotinin bovine" or aprotinine or aprotonin or "bayer a 128" or "bayer a128" or "bovine pancreatic secretory trypsin inhibitor" or contrical or contrycal or contrykal or "frey inhibitor" or gordox or haemoprot):ti,ab,kw 44 #35 (iniprol or "kallikrein trypsin inhibitor" or "kazal type trypsin inhibitor" or kontrikal or kontrycal or "Kunitz inhibitor" or "Kunitz trypsin inhibitor" or midran or "pancreas antitrypsin" or "pancreas secretory trypsin inhibitor" or "pancreas trypsin inhibitor"):ti,ab,kw 3 #36 ("pancreatic antitrypsin" or "pancreatic secretory trypsin inhibitor" or "pancreatic trypsin inhibitor" or "protinin orriker 52g" or rivilina or "rp 9921" or rp9921 or tracylol or trascolan or trasilol or traskolan or trasylol or trazylol or "tumor associated trypsin inhibitor" or zymofren):ti,ab,kw 107 #37 ("4 aminomethylbenzoic acid" or "4 amino methylbenzoic acid" or "alpha amino para toluic acid" or "amino methylbenzoic acid" or "aminomethyl benzoic acid" or "aminomethylbenzoic acid" or PAMBA or "para aminomethylbenzoic acid" or "para amino methylbenzoic acid" or styptopur or styptosolut):ti,ab,kw 19 #38 MeSH descriptor: [Fibrinolysis] this term only and with qualifier(s): [antagonists & inhibitors ‐ AI, drug effects ‐ DE] 626 #39 #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31 or #32 or #33 or #34 or #35 or #36 or #37 or #38 4899 #40 #16 and #39 123
Appendix 2. MEDLINE search strategy, 2022 update
1. intracranial hemorrhages/ or cerebral hemorrhage/ or subarachnoid hemorrhage/ or hemorrhagic stroke/ 2. Intracranial Aneurysm/ 3. Rupture, Spontaneous/ 4. 2 and 3 5. Aneurysm, Ruptured/ 6. exp brain/ or exp meninges/ 7. 5 and 6 8. ((subarachnoid or arachnoid) adj6 (haemorrhage$ or hemorrhage$ or bleed$ or blood$)).tw. 9. Vasospasm, Intracranial/ 10. ((cerebral or intracranial or cerebrovascular) adj6 (vasospasm or spasm)).tw. 11. SAH.tw. 12. 1 or 4 or 7 or 8 or 9 or 10 or 11 13. exp Antifibrinolytic Agents/ 14. (anti‐fibrinolytic$ or antifibrinolytic$ or antifibrinolysin$ or anti‐fibrinolysin$ or antiplasmin$ or anti‐plasmin$ or (plasmin adj3 inhibitor$)).tw. 15. (fibrinolysis adj3 (prevent$ or inhib$ or antag$)).tw. 16. Tranexamic Acid/ 17. (4 amino methylcyclohexane carboxylate or 4 aminomethylcyclohexanecarbonic acid or 4 aminomethylcyclohexanecarboxylic acid or amca or AMCHA or amchafibrin or amikapron or aminomethyl cyclohexane carboxylic acid or aminomethyl cyclohexanecarboxylic acid or aminomethylcyclohexane carbonic acid or aminomethylcyclohexane carboxylic acid or aminomethylcyclohexanecarbonic acid or aminomethylcyclohexanecarboxylic acid or aminomethylcyclohexanocarboxylic acid or aminomethylcyclohexanoic acid or amstat or anexan or antivoff or anvitoff orcaprilon or cis 4 aminomethylcyclohexanecarboxylic acid or cis aminomethyl cyclohexanecarboxylic acid or cl 65336 or cl65336 or cyclocapron or cyclokapron or cyklocapron or cyklokapron or exacyl or fibrinon or frenolyse or hemostan or hexacapron or hexakapron or kabi 2161 or kalnex or micranex or para aminomethylcyclohexane carboxylic acid or rikaparin or ronex or spotof or theranex or tramic or tranex or tranexam or tranexamic acid or tranexanic acid or tranexic or trans 1 aminomethylcyclohexane 4 carboxylic acid or trans 4 aminomethylcyclohexane 1 carboxylic acid or trans 4 aminomethylcyclohexane carboxylic acid or trans 4 aminomethylcyclohexanecarboxylic acid or trans achma or trans amcha or trans aminomethyl cyclohexane carboxylic acid or trans aminomethylcyclohexane carboxylic acid or trans aminomethylcyclohexanecarboxylic acid or transamin or transaminomethylcyclohexane carboxylic acid or transexamic acid or traxamic or trenaxin or ugurol).tw,nm. 18. exp Aminocaproic Acids/ 19. (acikaprin or afibrin or amicar or amino caproic acid or aminocaproic or aminohexanoic acid or beta aminocaproic acid or capracid or capramol or caproamin or caprocid or caprogel or caprolest or caprolisin or caprolisine or caprolysin orcapromol or cl 10304 or cl10304 or cy 116 or cy116 or e aminocaproic acid or EACA or ecapron or ekaprol or epsamon or epsicaprom or epsicapron or epsikapron or epsilcapramin or epsilon amino caproate or epsilon amino caproic aci or depsilon aminocaproate or epsilon aminocaproic acid or epsilonaminocaproic acid or epsilonaminocapronsav or etha aminocaproic acid or ethaaminocaproic acid or gamma aminocaproic acidor gamma aminohexanoic acidor hemocaprol or hepin or hexalense or ipsilon or jd 177 or jd177 or neocaprol or nsc 26154 or nsc26154 or resplamin or tachostyptan).tw,nm. 20. Aprotinin/ 21. (9921 rp or antagosan or antilysin or antilysine or apronitin or apronitine or apronitrine or aprotimbin or aprotinin bovine or aprotinine or aprotonin or bayer a 128 or bayer a128 or bovine pancreatic secretory trypsin inhibitor or contrical or contrycal or contrykal or frey inhibitor or gordox or haemoprot or iniprol or kallikrein trypsin inhibitor or kazal type trypsin inhibitor or kontrikal or kontrycal or Kunitz inhibitor or Kunitz trypsin inhibitor or midran or pancreas antitrypsin or pancreas secretory trypsin inhibitor or pancreas trypsin inhibitor or pancreatic antitrypsin or pancreatic secretory trypsin inhibitor or pancreatic trypsin inhibitor or protinin orriker 52g or rivilina or rp 9921 or rp9921 or tracylol or trascolan or trasilol or traskolan or trasylol or trazylol or tumor associated trypsin inhibitor or zymofren).tw,nm. 22. (4 aminomethylbenzoic acid or 4 amino methylbenzoic acid or alpha amino para toluic acid or amino methylbenzoic acid or aminomethyl benzoic acid or aminomethylbenzoic acid or PAMBA or para aminomethylbenzoic acid or para amino methylbenzoic acid or styptopur or styptosolut).tw,nm. 23. Fibrinolysis/ai, de [Antagonists & Inhibitors, Drug Effects] 24. or/13‐23 25. randomized controlled trial.pt. 26. controlled clinical trial.pt. 27. randomized.ab. 28. placebo.ab. 29. drug therapy.fs. 30. randomly.ab. 31. trial.ti. 32. groups.ab. 33. or/25‐32 34. exp animals/ not humans.sh. 35. 33 not 34 36. 12 and 24 and 35
Appendix 3. Embase search strategy, 2022 update
1. subarachnoid hemorrhage/ 2. brain hemorrhage/ or brain artery aneurysm rupture/ 3. brain vasospasm/ 4. exp Intracranial Aneurysm/ 5. exp rupture/ 6. 4 and 5 7. Aneurysm Rupture/ 8. exp brain/ or exp meninx/ 9. 7 and 8 10. ((subarachnoid or arachnoid) adj6 (haemorrhage$ or hemorrhage$ or bleed$ or blood$)).tw. 11. ((cerebral or intracranial or cerebrovascular) adj6 (vasospasm or spasm)).tw. 12. SAH.tw. 13. 1 or 2 or 3 or 6 or 9 or 10 or 11 or 12 14. exp antifibrinolytic agent/ 15. (anti‐fibrinolytic$ or antifibrinolytic$ or antifibrinolysin$ or anti‐fibrinolysin$ or antiplasmin$ or anti‐plasmin$ or (plasmin adj3 inhibitor$)).tw. 16. (fibrinolysis adj3 (prevent$ or inhib$ or antag$)).tw. 17. tranexamic acid/ 18. (4 amino methylcyclohexane carboxylate or 4 aminomethylcyclohexanecarbonic acid or 4 aminomethylcyclohexanecarboxylic acid or amca or AMCHA or amchafibrin or amikapron or aminomethyl cyclohexane carboxylic acid or aminomethyl cyclohexanecarboxylic acid or aminomethylcyclohexane carbonic acid or aminomethylcyclohexane carboxylic acid or aminomethylcyclohexanecarbonic acid or aminomethylcyclohexanecarboxylic acid or aminomethylcyclohexanocarboxylic acid or aminomethylcyclohexanoic acid or amstat or anexan or antivoff or anvitoff orcaprilon or cis 4 aminomethylcyclohexanecarboxylic acid or cis aminomethyl cyclohexanecarboxylic acid or cl 65336 or cl65336 or cyclocapron or cyclokapron or cyklocapron or cyklokapron or exacyl or fibrinon or frenolyse or hemostan or hexacapron or hexakapron or kabi 2161 or kalnex or micranex or para aminomethylcyclohexane carboxylic acid or rikaparin or ronex or spotof or theranex or tramic or tranex or tranexam or tranexamic acid or tranexanic acid or tranexic or trans 1 aminomethylcyclohexane 4 carboxylic acid or trans 4 aminomethylcyclohexane 1 carboxylic acid or trans 4 aminomethylcyclohexane carboxylic acid or trans 4 aminomethylcyclohexanecarboxylic acid or trans achma or trans amcha or trans aminomethyl cyclohexane carboxylic acid or trans aminomethylcyclohexane carboxylic acid or trans aminomethylcyclohexanecarboxylic acid or transamin or transaminomethylcyclohexane carboxylic acid or transexamic acid or traxamic or trenaxin or ugurol).tw. 19. aminocaproic acid/ 20. (acikaprin or afibrin or amicar or amino caproic acid or aminocaproic acid or aminohexanoic acid or capracid or capramol or caproamin or caprocid or caprogel or caprolest or caprolisin or caprolisine or caprolysin orcapromol or cl 10304 or cl10304 or cy 116 or cy116 or e aminocaproic acid or EACA or ecapron or ekaprol or epsamon or epsicaprom or epsicapron or epsikapron or epsilcapramin or epsilon amino caproate or epsilon amino caproic aci or depsilon aminocaproate or epsilon aminocaproic acid or epsilonaminocaproic acid or epsilonaminocapronsav or etha aminocaproic acid or ethaaminocaproic acid or gamma aminocaproic acidor gamma aminohexanoic acidor hemocaprol or hepin or hexalense or ipsilon or jd 177 or jd177 or neocaprol or nsc 26154 or nsc26154 or resplamin or tachostyptan).tw. 21. aprotinin/ 22. (9921 rp or antagosan or antilysin or antilysine or apronitin or apronitine or apronitrine or aprotimbin or aprotinin bovine or aprotinine or aprotonin or bayer a 128 or bayer a128 or bovine pancreatic secretory trypsin inhibitor or contrical or contrycal or contrykal or frey inhibitor or gordox or haemoprot or iniprol or kallikrein trypsin inhibitor or kazal type trypsin inhibitor or kontrikal or kontrycal or Kunitz inhibitor or Kunitz trypsin inhibitor or midran or pancreas antitrypsin or pancreas secretory trypsin inhibitor or pancreas trypsin inhibitor or pancreatic antitrypsin or pancreatic secretory trypsin inhibitor or pancreatic trypsin inhibitor or protinin orriker 52g or rivilina or rp 9921 or rp9921 or tracylol or trascolan or trasilol or traskolan or trasylol or trazylol or tumor associated trypsin inhibitor or zymofren).tw. 23. 4 aminomethylbenzoic acid/ 24. (4 aminomethylbenzoic acid or 4 amino methylbenzoic acid or alpha amino para toluic acid or amino methylbenzoic acid or aminomethyl benzoic acid or aminomethylbenzoic acid or PAMBA or para aminomethylbenzoic acid or para amino methylbenzoic acid or styptopur or styptosolut).tw. 25. or/14‐24 26. Randomized Controlled Trial/ or "randomized controlled trial (topic)"/ 27. Randomization/ 28. Controlled clinical trial/ or "controlled clinical trial (topic)"/ 29. control group/ or controlled study/ 30. clinical trial/ or "clinical trial (topic)"/ or phase 1 clinical trial/ or phase 2 clinical trial/ or phase 3 clinical trial/ or phase 4 clinical trial/ 31. crossover procedure/ 32. single blind procedure/ or double blind procedure/ or triple blind procedure/ 33. placebo/ or placebo effect/ 34. (random$ or RCT or RCTs).tw. 35. (controlled adj5 (trial$ or stud$)).tw. 36. (clinical$ adj5 trial$).tw. 37. clinical trial registration.ab. 38. ((control or treatment or experiment$ or intervention) adj5 (group$ or subject$ or patient$)).tw. 39. (quasi‐random$ or quasi random$ or pseudo‐random$ or pseudo random$).tw. 40. ((control or experiment$ or conservative) adj5 (treatment or therapy or procedure or manage$)).tw. 41. ((singl$ or doubl$ or tripl$ or trebl$) adj5 (blind$ or mask$)).tw. 42. (cross‐over or cross over or crossover).tw. 43. (placebo$ or sham).tw. 44. trial.ti. 45. (assign$ or allocat$).tw. 46. controls.tw. 47. or/26‐46 48. 13 and 25 and 47
Appendix 4. MEDLINE search strategy, 2013 publication
1. Subarachnoid Hemorrhage/ 2. intracranial hemorrhages/ or cerebral hemorrhage/ 3. Intracranial Aneurysm/ 4. Rupture, Spontaneous/ 5. 3 and 4 6. Aneurysm, Ruptured/ 7. exp brain/ or exp meninges/ 8. 6 and 7 9. ((subarachnoid or arachnoid) adj6 (haemorrhage$ or hemorrhage$ or bleed$ or blood$)).tw. 10. Vasospasm, Intracranial/ 11. ((cerebral or intracranial or cerebrovascular) adj6 (vasospasm or spasm)).tw. 12. sah.tw. 13. 1 or 2 or 5 or 8 or 9 or 10 or 11 or 12 14. exp Antifibrinolytic Agents/ 15. (anti‐fibrinolytic$ or antifibrinolytic$ or antifibrinolysin$ or anti‐fibrinolysin$ or antiplasmin$ or anti‐plasmin$ or (plasmin adj3 inhibitor$)).tw. 16. (fibrinolysis adj3 (prevent$ or inhib$ or antag$)).tw. 17. tranexamic acid/ 18. (4 amino methylcyclohexane carboxylate or 4 aminomethylcyclohexanecarbonic acid or 4 aminomethylcyclohexanecarboxylic acid or amca or AMCHA or amchafibrin or amikapron or aminomethyl cyclohexane carboxylic acid or aminomethyl cyclohexanecarboxylic acid or aminomethylcyclohexane carbonic acid or aminomethylcyclohexane carboxylic acid or aminomethylcyclohexanecarbonic acid or aminomethylcyclohexanecarboxylic acid or aminomethylcyclohexanocarboxylic acid or aminomethylcyclohexanoic acid or amstat or anexan or antivoff or anvitoff orcaprilon or cis 4 aminomethylcyclohexanecarboxylic acid or cis aminomethyl cyclohexanecarboxylic acid or cl 65336 or cl65336 or cyclocapron or cyclokapron or cyklocapron or cyklokapron or exacyl or fibrinon or frenolyse or hemostan or hexacapron or hexakapron or kabi 2161 or kalnex or micranex or para aminomethylcyclohexane carboxylic acid or rikaparin or ronex or spotof or theranex or tramic or tranex or tranexam or tranexamic acid or tranexanic acid or tranexic or trans 1 aminomethylcyclohexane 4 carboxylic acid or trans 4 aminomethylcyclohexane 1 carboxylic acid or trans 4 aminomethylcyclohexane carboxylic acid or trans 4 aminomethylcyclohexanecarboxylic acid or trans achma or trans amcha or trans aminomethyl cyclohexane carboxylic acid or trans aminomethylcyclohexane carboxylic acid or trans aminomethylcyclohexanecarboxylic acid or transamin or transaminomethylcyclohexane carboxylic acid or transexamic acid or traxamic or trenaxin or ugurol).tw,nm. 19. exp Aminocaproic Acids/ 20. (acikaprin or afibrin or amicar or amino caproic acid or aminocaproic acid or aminohexanoic acid or capracid or capramol or caproamin or caprocid or caprogel or caprolest or caprolisin or caprolisine or caprolysin orcapromol or cl 10304 or cl10304 or cy 116 or cy116 or e aminocaproic acid or EACA or ecapron or ekaprol or epsamon or epsicaprom or epsicapron or epsikapron or epsilcapramin or epsilon amino caproate or epsilon amino caproic aci or depsilon aminocaproate or epsilon aminocaproic acid or epsilonaminocaproic acid or epsilonaminocapronsav or etha aminocaproic acid or ethaaminocaproic acid or gamma aminocaproic acidor gamma aminohexanoic acidor hemocaprol or hepin or hexalense or ipsilon or jd 177 or jd177 or neocaprol or nsc 26154 or nsc26154 or resplamin or tachostyptan).tw,nm. 21. Aprotinin/ 22. (9921 rp or antagosan or antilysin or antilysine or apronitin or apronitine or apronitrine or aprotimbin or aprotinin bovine or aprotinine or aprotonin or bayer a 128 or bayer a128 or bovine pancreatic secretory trypsin inhibitor or contrical or contrycal or contrykal or frey inhibitor or gordox or haemoprot or iniprol or kallikrein trypsin inhibitor or kazal type trypsin inhibitor or kontrikal or kontrycal or Kunitz inhibitor or Kunitz trypsin inhibitor or midran or pancreas antitrypsin or pancreas secretory trypsin inhibitor or pancreas trypsin inhibitor or pancreatic antitrypsin or pancreatic secretory trypsin inhibitor or pancreatic trypsin inhibitor or protinin orriker 52g or rivilina or rp 9921 or rp9921 or tracylol or trascolan or trasilol or traskolan or trasylol or trazylol or tumor associated trypsin inhibitor or zymofren).tw,nm. 23.( 4 aminomethylbenzoic acid or 4 amino methylbenzoic acid or alpha amino para toluic acid or amino methylbenzoic acid or aminomethyl benzoic acidor aminomethylbenzoic acid or PAMBA or para aminomethylbenzoic acid or para amino methylbenzoic acid or styptopur or styptosolut).tw,nm 24. Fibrinolysis/ai, de [Antagonists & Inhibitors, Drug Effects] 25. or/14‐24 26. 13 and 25 27. exp animals/ not humans.sh. 28. 26 not 27
Appendix 5. Embase search stragety, 2013 publication
1. Subarachnoid Hemorrhage/ 2. brain hemorrhage/ or brain artery aneurysm rupture/ 3. Brain Vasospasm/ 4. exp Intracranial Aneurysm/ 5. exp rupture/ 6. 4 and 5 7. Aneurysm Rupture/ 8. exp brain/ or exp meninx/ 9. 7 and 8 10. ((subarachnoid or arachnoid) adj6 (haemorrhage$ or hemorrhage$ or bleed$ or blood$)).tw. 11. ((cerebral or intracranial or cerebrovascular) adj6 (vasospasm or spasm)).tw. 12. sah.tw. 13. 1 or 2 or 3 or 6 or 9 or 10 or 11 or 12 14. exp antifibrinolytic agent/ 15. (anti‐fibrinolytic$ or antifibrinolytic$ or antifibrinolysin$ or anti‐fibrinolysin$ or antiplasmin$ or anti‐plasmin$ or (plasmin adj3 inhibitor$)).tw. 16. (fibrinolysis adj3 (prevent$ or inhib$ or antag$)).tw. 17. tranexamic acid/ 18. (4 amino methylcyclohexane carboxylate or 4 aminomethylcyclohexanecarbonic acid or 4 aminomethylcyclohexanecarboxylic acid or amca or AMCHA or amchafibrin or amikapron or aminomethyl cyclohexane carboxylic acid or aminomethyl cyclohexanecarboxylic acid or aminomethylcyclohexane carbonic acid or aminomethylcyclohexane carboxylic acid or aminomethylcyclohexanecarbonic acid or aminomethylcyclohexanecarboxylic acid or aminomethylcyclohexanocarboxylic acid or aminomethylcyclohexanoic acid or amstat or anexan or antivoff or anvitoff orcaprilon or cis 4 aminomethylcyclohexanecarboxylic acid or cis aminomethyl cyclohexanecarboxylic acid or cl 65336 or cl65336 or cyclocapron or cyclokapron or cyklocapron or cyklokapron or exacyl or fibrinon or frenolyse or hemostan or hexacapron or hexakapron or kabi 2161 or kalnex or micranex or para aminomethylcyclohexane carboxylic acid or rikaparin or ronex or spotof or theranex or tramic or tranex or tranexam or tranexamic acid or tranexanic acid or tranexic or trans 1 aminomethylcyclohexane 4 carboxylic acid or trans 4 aminomethylcyclohexane 1 carboxylic acid or trans 4 aminomethylcyclohexane carboxylic acid or trans 4 aminomethylcyclohexanecarboxylic acid or trans achma or trans amcha or trans aminomethyl cyclohexane carboxylic acid or trans aminomethylcyclohexane carboxylic acid or trans aminomethylcyclohexanecarboxylic acid or transamin or transaminomethylcyclohexane carboxylic acid or transexamic acid or traxamic or trenaxin or ugurol).tw. 19. aminocaproic acid/ 20. (acikaprin or afibrin or amicar or amino caproic acid or aminocaproic acid or aminohexanoic acid or capracid or capramol or caproamin or caprocid or caprogel or caprolest or caprolisin or caprolisine or caprolysin orcapromol or cl 10304 or cl10304 or cy 116 or cy116 or e aminocaproic acid or EACA or ecapron or ekaprol or epsamon or epsicaprom or epsicapron or epsikapron or epsilcapramin or epsilon amino caproate or epsilon amino caproic aci or depsilon aminocaproate or epsilon aminocaproic acid or epsilonaminocaproic acid or epsilonaminocapronsav or etha aminocaproic acid or ethaaminocaproic acid or gamma aminocaproic acidor gamma aminohexanoic acidor hemocaprol or hepin or hexalense or ipsilon or jd 177 or jd177 or neocaprol or nsc 26154 or nsc26154 or resplamin or tachostyptan).tw. 21. aprotinin/ 22. (9921 rp or antagosan or antilysin or antilysine or apronitin or apronitine or apronitrine or aprotimbin or aprotinin bovine or aprotinine or aprotonin or bayer a 128 or bayer a128 or bovine pancreatic secretory trypsin inhibitor or contrical or contrycal or contrykal or frey inhibitor or gordox or haemoprot or iniprol or kallikrein trypsin inhibitor or kazal type trypsin inhibitor or kontrikal or kontrycal or Kunitz inhibitor or Kunitz trypsin inhibitor or midran or pancreas antitrypsin or pancreas secretory trypsin inhibitor or pancreas trypsin inhibitor or pancreatic antitrypsin or pancreatic secretory trypsin inhibitor or pancreatic trypsin inhibitor or protinin orriker 52g or rivilina or rp 9921 or rp9921 or tracylol or trascolan or trasilol or traskolan or trasylol or trazylol or tumor associated trypsin inhibitor or zymofren).tw. 23. 4 aminomethylbenzoic acid/ 24. (4 aminomethylbenzoic acid or 4 amino methylbenzoic acid or alpha amino para toluic acid or amino methylbenzoic acid or aminomethyl benzoic acid or aminomethylbenzoic acid or PAMBA or para aminomethylbenzoic acid or para amino methylbenzoic acid or styptopur or styptosolut).tw. 25. fibrinolysis/pc [Prevention] 26. or/14‐25 27. 13 and 26 28. limit 27 to human
Appendix 6. ClinicalTrials search strategy, 2022 update
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov)
( antifibrinolytics OR fibrinolysis OR antiplasmin OR tranexamic acid OR aminocaproic acids OR aprotinin ) AND AREA[StudyType] EXPAND[Term] COVER[FullMatch] "Interventional" AND AREA[ConditionSearch] ( subarachnoid hemorrhage OR intracranial hemorrhages OR cerebral hemorrhage OR brain aneurysm OR intracranial vasospasm ) AND AREA[StdAge] EXPAND[Term] COVER[FullMatch] ( "Adult" OR "Older Adult" ) AND AREA[StudyFirstPostDate] EXPAND[Term] RANGE[12/01/2012, 04/19/2021]
Appendix 7. WHO ICTRP search strategy, 2022 update
World Health Organization International Clinical Trials Registry Platform (apps.who.int/trialsearch)
subarachnoid hemorrhage OR subarachnoid haemorrhage
Data and analyses
Comparison 1. Antifibrinolytic treatment versus control treatment with or without placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Poor outcome (death, vegetative, or (moderate) severe disability) at end of follow‐up: open versus blind studies | 5 | 2359 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.94, 1.13] |
| 1.1.1 Trials with control treatment (open studies) | 2 | 1318 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.81, 1.18] |
| 1.1.2 Trials with placebo treatment (blind studies) | 3 | 1041 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.93, 1.21] |
| 1.2 Poor outcome (death, vegetative, or (moderate) severe disability) at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration | 5 | 2359 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.94, 1.13] |
| 1.2.1 Trials without ischaemia prevention, treatment duration > 72 hours | 2 | 579 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.86, 1.22] |
| 1.2.2 Trials with ischaemia prevention, treatment duration > 72 hours | 1 | 462 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.91, 1.34] |
| 1.2.3 Trials with ischaemia prevention, treatment duration < 72 hours | 2 | 1318 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.81, 1.18] |
| 1.3 Death from all causes at end of follow‐up: open versus blind studies | 11 | 2717 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.90, 1.16] |
| 1.3.1 Trials with control treatment (open studies) | 5 | 1522 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.74, 1.30] |
| 1.3.2 Trials with placebo treatment (blind studies) | 6 | 1195 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.87, 1.19] |
| 1.4 Death from all causes at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration | 11 | 2717 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.90, 1.16] |
| 1.4.1 Trials without ischaemia prevention, treatment duration > 72 hours | 8 | 937 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.78, 1.35] |
| 1.4.2 Trials with ischaemia prevention, treatment duration > 72 hours | 1 | 462 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.79, 1.34] |
| 1.4.3 Trials with ischaemia prevention, treatment duration < 72 hours | 2 | 1318 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.84, 1.26] |
| 1.5 Rebleeding reported at end of follow‐up: open versus blind studies | 11 | 2717 | Risk Ratio (M‐H, Random, 95% CI) | 0.65 [0.47, 0.91] |
| 1.5.1 Trials with control treatment (open studies) | 5 | 1522 | Risk Ratio (M‐H, Random, 95% CI) | 0.66 [0.35, 1.24] |
| 1.5.2 Trials with placebo treatment (blind studies) | 6 | 1195 | Risk Ratio (M‐H, Random, 95% CI) | 0.64 [0.43, 0.97] |
| 1.6 Confirmed rebleeding at end of follow‐up (sensitivity analysis): open versus blind studies | 5 | 2318 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.34, 0.74] |
| 1.6.1 Trials with control treatment (open studies) | 3 | 1377 | Risk Ratio (M‐H, Random, 95% CI) | 0.52 [0.25, 1.08] |
| 1.6.2 Trials with placebo treatment (blind studies) | 2 | 941 | Risk Ratio (M‐H, Random, 95% CI) | 0.46 [0.25, 0.86] |
| 1.7 Rebleeding reported at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration | 11 | 2717 | Risk Ratio (M‐H, Random, 95% CI) | 0.65 [0.47, 0.91] |
| 1.7.1 Trials without ischaemia prevention, treatment duration > 72 hours | 8 | 937 | Risk Ratio (M‐H, Random, 95% CI) | 0.79 [0.47, 1.31] |
| 1.7.2 Trials with ischaemia prevention, treatment duration > 72 hours | 1 | 462 | Risk Ratio (M‐H, Random, 95% CI) | 0.58 [0.42, 0.80] |
| 1.7.3 Trials with ischaemia prevention, treatment duration < 72 hours | 2 | 1318 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.13, 1.31] |
| 1.8 Delayed cerebral ischaemia reported at end of follow‐up: open versus blind studies | 7 | 2484 | Risk Ratio (M‐H, Random, 95% CI) | 1.27 [1.00, 1.62] |
| 1.8.1 Trials with control treatment (open studies) | 4 | 1443 | Risk Ratio (M‐H, Random, 95% CI) | 1.17 [0.88, 1.55] |
| 1.8.2 Trials with placebo treatment (blind studies) | 3 | 1041 | Risk Ratio (M‐H, Random, 95% CI) | 1.38 [0.87, 2.19] |
| 1.9 Confirmed cerebral ischaemia at end of follow‐up (sensitivity analysis): open versus blind studies | 4 | 1813 | Risk Ratio (M‐H, Random, 95% CI) | 1.17 [0.90, 1.51] |
| 1.9.1 Trials with control treatment (open studies) | 2 | 872 | Risk Ratio (M‐H, Random, 95% CI) | 1.32 [0.56, 3.07] |
| 1.9.2 Trials with placebo treatment (blind studies) | 2 | 941 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [0.82, 1.89] |
| 1.10 Delayed cerebral ischaemia reported at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration | 7 | 2484 | Risk Ratio (M‐H, Random, 95% CI) | 1.27 [1.00, 1.62] |
| 1.10.1 Trials without ischaemia prevention, treatment duration > 72 hours | 4 | 704 | Risk Ratio (M‐H, Random, 95% CI) | 1.77 [1.30, 2.40] |
| 1.10.2 Trials with ischaemia prevention, treatment duration > 72 hours | 1 | 462 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.75, 1.23] |
| 1.10.3 Trials with ischaemia prevention, treatment duration < 72 hours | 2 | 1318 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.83, 1.46] |
| 1.11 Hydrocephalus reported at end of follow‐up: open versus blind studies | 6 | 1992 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [0.99, 1.20] |
| 1.11.1 Trials with control treatment (open studies) | 3 | 951 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.66, 1.34] |
| 1.11.2 Trials with placebo treatment (blind studies) | 3 | 1041 | Risk Ratio (M‐H, Random, 95% CI) | 1.19 [0.95, 1.48] |
| 1.12 Confirmed hydrocephalus at end of follow‐up (sensitivity analysis): open versus blind studies | 2 | 1275 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [0.99, 1.21] |
| 1.12.1 Trials with control treatment (open studies) | 1 | 813 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.97, 1.21] |
| 1.12.2 Trials with placebo treatment (blind studies) | 1 | 462 | Risk Ratio (M‐H, Random, 95% CI) | 1.17 [0.87, 1.55] |
| 1.13 Hydrocephalus reported at end of follow‐up: trials with and without ischaemia prevention, according to treatment duration | 6 | 1992 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [0.99, 1.20] |
| 1.13.1 Trials without ischaemia prevention, treatment duration > 72 hours | 4 | 717 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.74, 1.43] |
| 1.13.2 Trials with ischaemia prevention, treatment duration > 72 hours | 1 | 462 | Risk Ratio (M‐H, Random, 95% CI) | 1.17 [0.87, 1.55] |
| 1.13.3 Trials with ischaemia prevention, treatment duration < 72 hours | 1 | 813 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.97, 1.21] |
1.9. Analysis.

Comparison 1: Antifibrinolytic treatment versus control treatment with or without placebo, Outcome 9: Confirmed cerebral ischaemia at end of follow‐up (sensitivity analysis): open versus blind studies
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Chandra 1978.
| Study characteristics | ||
| Methods | Single centre study Random allocation (method of randomisation not described) Double‐blind treatment ITT analysis | |
| Participants | Clinical diagnosis of aneurysmal SAH confirmed in CSF and on angiography Male:female: treatment group 11:9; placebo group 10:9 Mean age 51 years (range 20 to 65) Excluded: SAH > 7 days, relevant associated illness | |
| Interventions | Tranexamic acid (6 g per day iv in 6 doses) versus identical‐appearing placebo treatment for a treatment duration of 3 weeks No report on surgical interventions | |
| Outcomes | Outcome: deaths from all causes at 3‐week follow‐up Events: rebleeding: reported, not defined; cerebral ischaemia: not reported; hydrocephalus: not reported | |
| Notes | No report on how many cases of rebleeding were established on CT scan or at necropsy | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | In the text, participants were reported to be randomly allocated, but how this was achieved is not reported |
| Allocation concealment (selection bias) | Low risk | Identical medication; however, unclear how medication was coded |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Neither the investigators nor the patients knew which subjects received which substance" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described in text |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Unclear risk | Unclear |
| Other bias | Unclear risk | More male than female participants included, which could point to some form of bias, since people with SAH are more often female |
Fodstad 1981.
| Study characteristics | ||
| Methods | Single‐centre study Random allocation (identical sequentially numbered, sealed envelope) No blind treatment Not strictly ITT: 1 of the 30 control participants was excluded after randomisation because he had received tranexamic acid before admission | |
| Participants | Clinical diagnosis of aneurysmal SAH verified with CSF, CT scan, and angiography Male:female: treatment group 13:17; control group 12:17 Mean age: treatment group 50 years (range 19 to 72); control group 53 years (range 27 to 70) Excluded: SAH > 3 days and known thrombotic disease | |
| Interventions | Tranexamic acid (6 g per day iv in 6 doses during the first week, 4 g in 4 doses iv in week 2, and 6 g orally in 4 doses in weeks 3 to 6) for a maximum duration of 6 weeks versus control group. Treatment continued until rebleeding, operation, discharge, or death | |
| Outcomes | Outcome: deaths from all causes at 6‐week follow‐up Events: rebleeding: reported, confirmed by CSF examination/spectrophotometry, CT scan or at necropsy; cerebral ischaemia: reported, not defined; hydrocephalus: reported, not defined | |
| Notes | Of the participants with rebleeding, 5 of 6 in the treatment group and 5 of 7 in the control group died. All had necropsy. In the remaining participants, rebleeding was confirmed by CT. 6 of 8 participants with cerebral ischaemia in the treatment group, and 2 of 3 in the control group died. All had necropsy, in the remaining participants, cerebral ischaemia was established on CT | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described in the text |
| Allocation concealment (selection bias) | Unclear risk | "Patients were assigned randomly" and "the sealed envelope technique was used" It was not mentioned whether these envelopes were opaque or not |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and personnel were not blinded (open study) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Part of recurrent haemorrhages were confirmed by lumbar puncture |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 participant was excluded from final analysis |
| Selective reporting (reporting bias) | Low risk | Protocol was previously published |
| Other bias | Low risk | None suspected, based on study design and outcome |
Girvin 1973.
| Study characteristics | ||
| Methods | Single‐centre study Random allocation (flip‐of‐a‐coin) No blind treatment ITT | |
| Participants | Clinical diagnosis of aneurysmal SAH probably confirmed on angiography Male:female ratio not described ("in control group were a relatively greater number of female patients") Age distribution not described Excluded: SAH > 7 days | |
| Interventions | Epsilon amino‐caproic acid, dosage probably 24 g per day (6 times 4 g) orally versus control group, duration on average in treatment group 7.7 days versus 5.5 in control group Treatment continued until operation or death | |
| Outcomes | Outcome: deaths from all causes (at unknown week) Events: rebleeding: reported, not defined; ischaemia: reported, not defined; hydrocephalus: not reported | |
| Notes | Poor description of study methods, definitions and results | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The cases were randomised on admission, by the flip of a coin" |
| Allocation concealment (selection bias) | Low risk | "The cases were randomised on admission, by the flip of a coin" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and personnel were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described in the text |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Low risk | Primary outcome described as "raison d'etre" of the study |
| Other bias | Low risk | None suspected, based on study design and outcome |
Hillman 2002.
| Study characteristics | ||
| Methods | Multi‐centre study Random allocation (sequence generation not specified) with sealed envelopes (not specified if opaque or not) No blind treatment Not strictly ITT: 91 participants excluded after randomisation because no aneurysm was found | |
| Participants | People suffering from CT‐verified SAH within 48 hours prior to hospital admission Male:female ratio: 1.89 in both groups Age distribution similar in both groups Excluded: SAH > 48 hours, age < 15 years, pregnancy, and history of thromboembolic disease. People in whom no aneurysm was demonstrated on angiographic studies were excluded after randomisation | |
| Interventions | Tranexamic acid (1 g iv immediately before transport, 1 g iv after 2 hours, and then 1 g every 6th hour until aneurysm occlusion, up to 72 hours after SAH) versus control treatment | |
| Outcomes | Outcome: Glasgow Outcome Scale at 6 months Events: rebleeding confirmed on CT or during operation, until 72 hours after admission; clinically established delayed ischaemic neurological deficit at 6 months, not confirmed by imaging | |
| Notes | Poor description of delayed ischaemic neurological deficit and how this was scored No mention of follow‐up for rebleeding after 72 hours | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation was not described in the text |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelopes were used that contained a randomisation document; however, it was not reported how these were ordered and if they were opaque or not |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and personnel were not blinded (open study) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described in the text |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 15% of included participants not evaluated in final analysis, which might have resulted in an overestimation of the effect estimate |
| Selective reporting (reporting bias) | High risk | Previously published protocol was not mentioned, clinical outcome reported, although not described in introduction or methods |
| Other bias | Low risk | None suspected, based on study design and outcome |
Kaste 1979.
| Study characteristics | ||
| Methods | Single‐centre study Random allocation (identical sequentially numbered treatment boxes) Double‐blind treatment Code broken after final evaluation ITT | |
| Participants | Clinical diagnosis of aneurysmal SAH verified in the CSF Male:female: active treatment group 16:16; placebo group 14:18 Age distribution similar in both groups Excluded: SAH > 72 hours, myocardial infarction within 6 months, unconsciousness, coagulation disorders or thrombotic disease, renal failure, and pregnancy | |
| Interventions | Tranexamic acid (6 g per day iv in 6 doses) versus identical‐appearing placebo treatment for a maximum treatment duration of 3 weeks Treatment discontinued at operation | |
| Outcomes | Outcome: deaths from all causes at 3 months Events: rebleeding: suspected when 2 of: sudden deterioration of consciousness, increase of neck rigidity, headache, or focal signs ‐ rebleeding verified in CSF or at necropsy; ischaemia: reported, not defined; hydrocephalus: reported, not defined | |
| Notes | No definition of cerebral ischaemia or hydrocephalus: 'vasospasm and ventricular dilatation were seen on angiography' | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation was not described in the text |
| Allocation concealment (selection bias) | Low risk | Tranexamic acid and placebo were prepared in identical vials and were coded; the code was only broken after final evaluation of the trial |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Tranexamic acid and placebo were prepared in identical vials and were coded; the code was only broken after final evaluation of the trial |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "The code identifying each substance was broken only after the final evaluation of all 64 patients" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Low risk | Protocol was previously published |
| Other bias | Unclear risk | Unconscious people not included, causing the results to be less generalisable |
Maurice 1978.
| Study characteristics | ||
| Methods | Single‐centre study Random allocation (identical sequentially numbered, sealed envelop) No double‐blind treatment Not published as ITT, but ITT analysis could be reconstructed | |
| Participants | Clinical diagnosis of aneurysmal SAH probably verified in the CSF No description of age or sex ratios ('treatment group matched in age and sex control group') Excluded: SAH > 4 days, person > 65 years, unconsciousness | |
| Interventions | Tranexamic acid (6 g per day iv in 6 doses during the first week, 6 g orally in 4 doses in week 2 until week 6) for a maximum duration of 6 weeks versus control group; treatment continued until operation or death | |
| Outcomes | Outcome: deaths from all causes at 3 months Events: rebleeding: reported and defined; 'confirmed in CSF or at necropsy'; ischaemia: reported, not defined; hydrocephalus: reported, not defined | |
| Notes | Rebleeding confirmed by CSF examination are not useable (see text), not reported how many rebleedings were established on CT scan or at necropsy | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequentially numbered, sealed envelopes were used, but no description was made of how these numbers were created |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered, sealed envelopes were used |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and personnel were not blinded (open study) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described in the text |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data, ITT analysis could be reconstructed |
| Selective reporting (reporting bias) | Low risk | Protocol was previously published |
| Other bias | Unclear risk | People "under 65" and "relatively little disturbed by the first bleed" not included in study, causing the results to be less generalisable |
Post 2021.
| Study characteristics | ||
| Methods | Multi‐centre study Random allocation No blind treatment ITT | |
| Participants | Patients suffering from CT‐verified SAH with symptoms for less than 24 hours
Male:female ratio treatment group 1:2,2 and control group 1:1,9.
Age distribution similar in both groups Excluded: SAH > 24 hours, age < 18 years, perimesencephalic haemorrhage without loss of consciousness with WFNS grade 1 or 2, bleeding pattern on CT compatible with a traumatic SAH, treatment for deep vein thrombosis, history of blood coagulation disorder, pregnancy, severe renal or liver failure, imminent death within 24 hours |
|
| Interventions | Tranexamic acid (bolus of 1 g iv as soon as possible after randomisation, followed by 1 g continuous iv every 8 hours). Treatment was continued until the start of endovascular, or surgical treatment of the aneurysm, or until a maximum of 24 hours, or a maximum of 4 g tranexamic acid The control group received standard, usual care | |
| Outcomes | mRS at six months after randomisation Events: rebleeding, hydrocephalus, DCI, thromboembolic events | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Sequence was generated by a web‐based allocation program. Allocation by stratifying according to permuted blocks with block sizes with a maximum of 12 Allocation by treatment centre |
| Allocation concealment (selection bias) | Low risk | Sequence was generated by a web‐based allocation program |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and personnel were not blinded (open label) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessement of outcome was performed by a dedicated research nurse who was blind to randomisation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | < 1% of data was missing |
| Selective reporting (reporting bias) | Low risk | Previously published study protocol and statistical analysis protocol |
| Other bias | Low risk | ‐ |
Roos 2000a.
| Study characteristics | ||
| Methods | Multicentre study Random allocation with secured web‐based system that stratified according to permuted blocks (random block sizes; maximum of 12) by treatment centre Prospective, randomised, open label trial with blinded outcome assessment ITT | |
| Participants | Adult patients (18 years or older) if they were admitted to one of the eight participating referring hospitals or treatment centres, with signs and symptoms for less than 24 hours indicating SAH, and a non‐contrast CT confirming SAH Excluded: perimesencephalic bleeding pattern on CT in combination with a Glasgow Coma Scale score of 13 to 15, and without loss of consciousness, directly after ictus or focal neurological deficit on admission; traumatic subarachnoid haemorrhage pattern on CT; ongoing treatment for deep vein thrombosis or pulmonary embolism; a history of a hypercoagulability disorder; pregnancy; severe renal failure (serum creatinine > 150 µmol/l), or imminent death within 24 hours Male:female: treatment group 89:140; placebo group 73:160 Mean age: treatment group 56 years; placebo group 55 years |
|
| Interventions | Immediatley after randomisation, administration of one bolus of 1 g tranexamic acid iv, directly followed by 1 g continuous intravenous infusion every eight hours. Treatment was continued until the start of endovascular, or surgical treatment of the aneurysm, or until a maximum of 24 hours, whichever came first All participants received treatment according to current guidelines with standard anti‐ischaemic treatment with nimodipine | |
| Outcomes | Primary outcome: mRS by a standardised and validated telephone interview at 6 months
Secondary outcomes: excellent clinical outcome (mRS 0 to 2), and ordinal shift analysis of the mRS score at 6 months (sensitivity analyses), and all‐cause mortality at 30 days and after 6 months Events: rebleeding after randomisation and before treatment of the aneurysm(s), hydrocephalus, DCI, complications of treatment of the aneurysm(s) (per‐procedural thrombo‐embolic, per‐procedural rupture, cerebral infarction related to clipping); other complications (extracranial thrombosis, deep venous thrombosis, pulmonary embolism, intra‐ and extracranial haemorrhagic complications, severe hyponatremia, pneumonia, infectious meningitis, urinary tract infection, seizures, delirium, and Terson’s syndrome); suspected unexpected serious adverse drug reactions, or other serious adverse events, or both during hospital admission |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Sequence was generated by use of random number tables |
| Allocation concealment (selection bias) | Low risk | Identical, sequentially numbered treatment boxes, blocked per centre were used and boxes were consecutively numbered and administered in the same order to each following participant |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Identical and sequentially numbered treatment boxes were used |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Only after recording of all events and outcomes, the trial code was broken" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Low risk | Previously published protocol |
| Other bias | Low risk | None suspected, based on study design and outcome |
Tsementzis 1990.
| Study characteristics | ||
| Methods | Single‐centre study Random allocation (identical sequentially numbered medication boxes) Double‐blind treatment Not strictly ITT: 4 participants who missed a few doses of medication were excluded after randomisation | |
| Participants | Clinical diagnosis of aneurysmal SAH verified on CT or in the CSF Male:female: treatment group 20:30; placebo group 26:24 Age distribution similar in both groups Excluded: SAH > 72 hours, antihypertensives or medication known to affect the fibrinolytic or coagulation systems, acute myocardial infarction, coagulation disorders or thrombotic disease, renal failure, pregnancy, previous tranexamic acid‐treatment, or people in whom death seemed imminent | |
| Interventions | Tranexamic acid (9 g per day iv in 6 doses in week 1, orally in 4 doses in week 2, 3, and 4) versus identical‐appearing placebo treatment for a maximum treatment duration of 4 weeks Treatment was discontinued if an operation for the aneurysm began, or if deep vein thrombosis or pulmonary infarction developed | |
| Outcomes | Outcome: Glasgow Outcome Scale at discharge, 1, 3, and 6 months Events: rebleeding: reported and defined ‐ 'clinical signs confirmed on CT, in the CSF, or at necropsy'; ischaemia: reported and defined ‐ 'clinical signs combined with the absence of evidence of rebleeding on CT or CSF'; hydrocephalus: reported, not defined | |
| Notes | No report of how many participants' rebleedings or cerebral ischaemia were established on CT scan or at necropsy No definition of hydrocephalus other then 'ventricular dilatation was seen on angiography' | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation was not described |
| Allocation concealment (selection bias) | Low risk | Placebo controlled trial with sequentially numbered boxes with trial medication was used |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Boxes with either tranexamic acid or placebo were used that were numbered consecutively by the pharmacist |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not reported in the text, but because of control with placebo, not thought to have influenced results |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 4 participants were excluded; no mention is made on their outcome |
| Selective reporting (reporting bias) | Unclear risk | Not reported in the text |
| Other bias | Unclear risk | 20 participants with protocol violations were excluded from the analysis after randomisation |
Van Rossum 1977.
| Study characteristics | ||
| Methods | Multicentre study Random allocation ("drug or placebo randomly administered in a sequence prescribed by and only known to the statistician") Double‐blind treatment Not strictly ITT: 3 participants excluded, because of other diagnosis, after randomisation | |
| Participants | Clinical diagnosis of aneurysmal SAH verified in the CSF Male:female ratio or age distribution not described Excluded: SAH > 14 days (in 94% of the participants, treatment started within 1 week) | |
| Interventions | Tranexamic acid (4 g per day iv in 4 doses) versus identically appearing placebo treatment for a maximum treatment duration of 10 days Treatment was discontinued after the aneurysm operation | |
| Outcomes | Outcome: all‐cause mortality at 3 months Events: rebleeding: reported and defined ‐ 'clinical signs confirmed in the CSF or at necropsy'; ischaemia: not reported; hydrocephalus: not reported | |
| Notes | Rebleeds confirmed by CSF examination are not useable (see text), not reported how many rebleedings were established on CT scan or at necropsy | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Sequence was generated by an independent statistician |
| Allocation concealment (selection bias) | Low risk | Sequence was only known to the statistician and "it was impossible for medical staff or patients to distinguish between drug‐ and placebo‐containing ampoules" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "It was impossible for medical staff or patients to distinguish between drug‐ and placebo‐containing ampoules" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not reported in the text, but because of control with placebo not thought to have influenced results |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 3 participants were excluded, and not mentioned further |
| Selective reporting (reporting bias) | Low risk | Protocol was previously published |
| Other bias | Low risk | None suspected, based on study design and outcome |
Vermeulen 1984.
| Study characteristics | ||
| Methods | Multicentre study Random allocation (identical sequentially numbered treatment boxes), blocked per centre Double‐blind treatment Code broken after all events and outcomes had been recorded ITT | |
| Participants | Clinical diagnosis of aneurysmal SAH verified on CT or in the CSF: if negative CT, angiography had to confirm an aneurysm before randomisation Male:female: treatment group 95:146; placebo group 94:144 Mean age in both groups 50 years Excluded: SAH > 72 hours, coagulation disorders or thrombotic disease, renal failure, pregnancy, previous tranexamic acid‐treatment, or people in whom death appeared imminent | |
| Interventions | Tranexamic acid (6 g per day iv in 6 doses in week 1 and 2, 4 g iv or 6 g orally per day in 4 doses in week 3 and 4) versus identical‐appearing placebo treatment for a maximum treatment duration of 4 weeks Treatment was discontinued when an aneurysm operation began, if the angiography was negative, if venous thrombosis or pulmonary infarction developed, or a diagnosis other than aneurysm was established | |
| Outcomes | Outcome: Glasgow Outcome Scale at 3 months Events: rebleeding‐definite: confirmed by CT scan or at necropsy; rebleeding‐possible: sudden deterioration and death; infarction‐definite: confirmed by CT scan or at necropsy; infarction‐probable: gradual development of focal neurologic signs with or without deterioration in the level of consciousness; hydrocephalus: reported, not defined | |
| Notes | No definition of hydrocephalus other than 'requiring shunting' | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number tables were used |
| Allocation concealment (selection bias) | Low risk | Consecutively‐numbered boxes were used and were administered in that order to included participants |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Placebo was used as control and the trial code was unbroken until the trial was finished |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "The trial code was broken in May 1983, after all events and outcomes had been recorded" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No incomplete data |
| Selective reporting (reporting bias) | Low risk | Protocol was previously published |
| Other bias | Low risk | Not suspected, based on study design and outcome |
CSF: cerebrospinal fluid CT: computed tomography DCI: delayed cerebral ischaemia ITT: intention‐to‐treat iv: intravenous mRS: modified Rankin Scale SAH: subarachnoid haemorrhage WFNS: World Federation of Neurosurgical Societies
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Adams 1981 | Comparative trial between antifibrinolytic agents and blood pressure reduction or fluid restriction |
| Brzecki 1974 | All participants received epsikapron, while being randomised between trasylol or placebo; also historical control group |
| Chowdhary 1979 | Not strictly randomised; allocation to treatment or placebo according to days of the week |
| Chowdhary 1981 | Comparative trial between tranexamic acid and EACA |
| Chowdhary 1986 | No report on clinical outcome or death, only data on rebleeding and cerebral ischaemia |
| Eastin 2014 | Wrong study design |
| Fodstad 1978 | No ITT analysis possible; too many participants (14 of a of total 60 randomised) excluded from final analysis after randomisation |
| Gelmers 1980 | Not strictly randomised; allocation to treatment or placebo according to days of the week |
EACA: epsilon amino‐caproic acid ITT: intention‐to‐treat
Differences between protocol and review
In the update of 2013, we added an additional subgroup analysis to evaluate the effect of antifibrinolytic therapy on all outcomes in trials with and without additional measures to prevent or reverse delayed cerebral ischaemia, and to evaluate the effect of antifibrinolytic therapy according to treatment duration.
Contributions of authors
Menno Germans: coordinated the updated review; collected data; undertook all aspects of the searches; was responsible for data management and analysis; reviewed all data and wrote the 2022 update
Wouter Dronkers: undertook all aspects of the searches; reviewed all data; participated in data analyses; and participated in writing the present update.
Irem Baharoglu: co‐ordinated and wrote the previous version of this review; and critically reviewed the 2022 update
René Post: co‐ordinated the newly included study in this update; and critically reviewed the 2022 update
Dagmar Verbaan: supervised the newly included study in this update; and critically reviewed the 2022 update
Gabriel Rinkel: participated in writing and reviewing the 2022 and previous versions of the review; and secured funding for previous versions
Yvo Roos: co‐ordinated and wrote previous versions of this review; oversaw the data collection and critically reviewed the 2022 update
Sources of support
Internal sources
-
none to declare, Other
none
External sources
-
Nederlandse Hartstichting (Netherlands Heart Foundation), Netherlands
research grant
Declarations of interest
Menno Germans: co‐investigator in Post 2021 Wouter Dronkers: none known Merih Baharoglu: none known René Post: investigator in Post 2021 Dagmar Verbaan: principal investigator in Post 2021 Gabriel Rinkel: co‐investigator in Roos 2000a Yvo Roos: principal investigator in Roos 2000a None of the review authors have any financial or other commercial conflict of interest to disclose.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Chandra 1978 {published data only}
- Chandra B. Treatment of subarachnoid hemorrhage from ruptured intracranial aneurysm with tranexamic acid: a double-blind clinical trial. Annals of Neurology 1978;3:502-4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Fodstad 1981 {published data only}
- Fodstad H, Forssell A, Liliequist B, Schannong M. Antifibrinolysis with tranexamic acid in aneurysmal subarachnoid hemorrhage: a consecutive controlled clinical trial. Neurosurgery 1981;8:158-65. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Girvin 1973 {published and unpublished data}
- Girvin JP. The use of antifibrinolytic agents in the preoperative treatment of ruptured intracranial aneurysms. Transactions of the American Neurological Association 1973;98:150-2. [MEDLINE: ] [PubMed] [Google Scholar]
Hillman 2002 {published data only}
- Hillman J, Fridriksson S, Nillson O, Yu Z, Saveland H, Jakobsson KE. Immediate administration of tranexamic acid and reduced incidence of early rebleeding after aneurysmal subarachnoid hemorrhage: a prospective randomized study. Journal of Neurosurgery 2002;97:771-8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Kaste 1979 {published data only}
- Kaste M, Ramsay M. Tranexamic acid in subarachnoid hemorrhage. A double-blind study. Stroke 1979;10:519-22. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Maurice 1978 {published data only}
- Maurice-Williams RS. Prolonged antifibrinolysis: an effective non-surgical treatment for ruptured intracranial aneurysms? British Medical Journal 1978;1:945-7. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Post 2021 {published and unpublished data}
- Germans MR, Post R, Coert BA, Rinkel GJE, Vandertop WP, Verbaan D. Ultra-early tranexamic acid after subarachnoid hemorrhage (ULTRA): study protocol for a randomized controlled trial. Trials 2013;14(143):1-6. [DOI: 10.1186/1745-6215-14-143] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Post R, Germans MR, Vandertop WP, Verbaan D, on behalf of the ULTRA Investigators. Ultra-early tranexamic acid after subarachnoid haemorrhage: a randomised controlled clinical trial. Lancet 2021;397(10269):112-8. [DOI] [PubMed] [Google Scholar]
- Tjerkstra MA, Post R, Germans MR, Vergouwen MD, Jellema K, Koot RW, et al. Tranexamic acid after aneurysmal subarachnoid hemorrhage: post-hoc analysis of the ULTRA trial. Neurology 2022 October 20 [Epub ahead of print]. [DOI: 10.1212/WNL.0000000000201160] [DOI] [PubMed]
Roos 2000a {published and unpublished data}
- Roos Y, for the STAR-study group. Antifibrinolytic treatment in aneurysmal subarachnoid haemorrhage: a randomized placebo-controlled trial. Neurology 2000;54:77-82. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Tsementzis 1990 {published data only}
- Tsementzis SA, Hitchcock ER, Meyer CH. Benefits and risks of antifibrinolytic therapy in the management of ruptured intracranial aneurysms. A double-blind placebo-controlled study. Acta Neurochirurgica 1990;102:1-10. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Tsementzis SA, Honan WP, Nightingale S, Hitchcock ER, Meyer CH. Fibrinolytic activity after subarachnoid haemorrhage and the effect of tranexamic acid. Acta Neurochirurgica 1990;103:116-21. [DOI] [PubMed] [Google Scholar]
Van Rossum 1977 {published data only}
- Van Rossum J, Wintzen AR, Endtz LJ, Schoen JH, Jonge H. Effect of tranexamic acid on rebleeding after subarachnoid hemorrhage: a double-blind controlled clinical trial. Annals of Neurology 1977;2:238-42. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Vermeulen 1984 {published data only}
- Vermeulen M, Lindsay KW, Murray GD, Cheah F, Hijdra A, Muizelaar JP, et al. Antifibrinolytic treatment in subarachnoid hemorrhage. New England Journal of Medicine 1984;311:432-7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Adams 1981 {published data only}
- Adams HP Jr, Nibbelink DW, Torner JC, Sahs AL. Antifibrinolytic therapy in patients with aneurysmal subarachnoid hemorrhage. A report of the cooperative aneurysm study. Archives of Neurology 1981;38:25-9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Brzecki 1974 {published data only}
- Brzecki A, Misztal S. Results of Trasylol treatment of subarachnoid hemorrhage [Wyniki leczenia Trasylolem krwotoku podpajeczynowkowego]. Polski Tygodnik Lekarski 1974;29(2):53-5. [MEDLINE: ] [PubMed] [Google Scholar]
Chowdhary 1979 {published data only}
- Chowdhary UM, Carey PC, Hussein MM. Prevention of early recurrence of spontaneous subarachnoid haemorrhage by epsilon-aminocaproic acid. Lancet 1979;1:741-3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Chowdhary 1981 {published data only}
- Chowdhary UM, Sayed K. Comparative clinical trial of epsilon amino-caproic acid and tranexamic acid in the prevention of early recurrence of subarachnoid haemorrhage. Journal of Neurology, Neurosurgery and Psychiatry 1981;44:810-3. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chowdhary 1986 {published data only}
- Chowdhary UM, Sayed K. Prevention of early recurrence of aneurysmal subarachnoid haemorrhage by tranexamic acid: a controlled clinical trial. Vascular Surgery 1986;1:8-13. [EMBASE: 1986195828] [Google Scholar]
Eastin 2014 {published data only}
- Eastin TR, Snipes CD, Seupaul RA. Are antifibrinolytic agents effective in the treatment of aneurysmal subarachnoid hemorrhage? Annals of Emergency Medicine 2014;64(6):658-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Fodstad 1978 {published data only}
- Fodstad H, Liliequist B, Schannong M, Thulin CA. Tranexamic acid in the preoperative management of ruptured intracranial aneurysms. Surgical Neurology 1978;10:9-15. [MEDLINE: ] [PubMed] [Google Scholar]
Gelmers 1980 {published data only}
- Gelmers HJ. Prevention of recurrence of spontaneous subarachnoid haemorrhage by tranexamic acid. Acta Neurochirurgica 1980;52:45-50. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Additional references
Adams 1982
- Adams HP. Current status of antifibrinolytic therapy for treatment of patients with aneurysmal subarachnoid hemorrhage. Stroke 1982;13:256-9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Adams 1987
- Adams HP. Antifibrinolytics in aneurysmal subarachnoid hemorrhage. Do they have a role? Maybe. Archives of Neurology 1987;44:114-5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Biller 1988
- Biller J, Godersky JC, Adams HP. Management of aneurysmal subarachnoid hemorrhage. Stroke 1988;19:1300-5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Carley 2005
- Carley S, Sen A. Best evidence topic report. Antifibrinolytics for the initial management of sub arachnoid haemorrhage. Emergency Medicine Journal 2005;22:274-5. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chawjol 2008
- Chawjol M, Starke RM, Kim GH, Majer SA, Connolly ES. Antifibrinolytic therapy to prevent early rebleeding after subarachnoid hemorrhage. Neurocritical Care 2008;8:418-26. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Connolly 2012
- Connolly ES, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2012;43:1711-37. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Fodstad 1982
- Fodstad H. Antifibrinolytic treatment in subarachnoid haemorrhage: present state. Acta Neurochirurgica 1982;63:233-44. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Gaberel 2012
- Gaberel T, Magheru C, Emery E, Derlon JM. Antifibrinolytic therapy in the management of aneurismal subarachnoid hemorrhage revisited. A meta-analysis. Acta Neurochirurgica 2012;154(1):1-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Germans 2013
- Germans MR, Post R, Coert BA, Rinkel GJE, Vandertop WP, Verbaan D. Ultra-early tranexamic acid after subarachnoid hemorrhage (ULTRA): study protocol for a randomized controlled trial. Trials 2013;14(143):1-6. [DOI: 10.1186/1745-6215-14-143] [DOI] [PMC free article] [PubMed] [Google Scholar]
Germans 2014
- Germans MR, Coert BA, Vandertop WP, Verbaan D. Time intervals from subarachnoid hemorrhage to rebleed. Jornal of Neurology 2014;261(7):1425-31. [DOI: 10.1007/s00415-014-7365-0] [DOI] [PubMed] [Google Scholar]
Gibbs 1967
- Gibbs JR, O'Gorman P. Fibrinolysis in subarachnoid haemorrhage. Postgraduate Medical Journal 1967;43(506):779-84. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Guo 2011
- Guo L, Zhou H, Xu J, Wang Y, Qiu Y, Jiang J. Risk factors related to aneurysmal rebleeding. World Neurosurgery 2011;76:292-8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/. [URL: www.handbook.cochrane.org]
Higgins 2022
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook. [URL: www.training.cochrane.org/handbook]
Lefebvre 2021
- Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf M-I, et al. Technical Supplement to Chapter 4: Searching for and selecting studies. In: Higgins JPT, Thomas J, Chandler J, Cumpston MS, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021 . Available from training.cochrane.org/handbook/archive/v6.2. [www.training.cochrane.org/handbook.]
Lindsay 1987
- Lindsay KW. Antifibrinolytic agents in subarachnoid haemorrhage. Journal of Neurology 1987;234:1-8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Locksley 1966
- Locksley HB. Natural history of subarachnoid hemorrhage, intracranial aneurysms and arteriovenous malformations. Journal of Neurosurgery 1966;25:321-68. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Maira 2006
- Maira G, Albanese A, Pentimalli L, Tirpakova B. Treatment of intracranial aneurysms. Clinical and Experimental Hypertension 2006;28:371-6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Mayberg 1994
- Mayberg MR, Batjer HH, Dacey R, Diringer M, Haley EC, Heros RC, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Circulation 1994;90:2592-605. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Mullan 1967
- Mullan S, Dawley J. Antifibrinolytic therapy for intracranial aneurysms. Journal of Neurosurgery 1967;28(1):21-3. [DOI: 10.3171/jns.1968.28.1.0021] [DOI] [PubMed] [Google Scholar]
Naidech 2005
- Naidech AM, Janjua N, Kreiter KT, Ostapkovich ND, Fitzsimmons BF, Parra A, et al. Predictors and impact of aneurysm rebleeding after subarachnoid hemorrhage. Archives of Neurology 2005;62:410-6. [DOI] [PubMed] [Google Scholar]
Ramirez 1981
- Ramirez-Lassepas M. Antifibrinolytic therapy in subarachnoid hemorrhage caused by ruptured intracranial aneurysm. Neurology 1981;31:316-22. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ren 2021
- Ren J, Qian D, Wu J, Ni L, Qian W, Zhao G, et al. Safety and efficacy of tranexamic acid in aneurysmal subarachnoid hemorrhage: a meta-analysis of randomized controlled trials. Forntiers in Neurology 2021;12:1-10. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Review Manager Web 2020 [Computer program]
- Review Manager Web 5 (RevMan Web 5). Version 5.4.1. The Cochrane Collaboration, 2020. Available at revman.cochrane.org.
Rinkel 2008
- Rinkel GJ. Medical management of patients with aneurysmal subarachnoid haemorrhage. International Journal of Stroke 2008;3:193-204. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Roos 2000b
- Roos YB, Haan RJ, Beenen LF, Groen RJ, Albrecht KW, Vermeulen M. Complications and outcome in patients with aneurysmal subarachnoid haemorrhage: a prospective hospital based cohort study in the Netherlands. Journal of Neurology, Neurosurgery and Psychiatry 2000;68:337-41. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stienen 2018
- Stienen MN, Germans MR, Burkhardt JK, Neidert MC, Fung C, Bervini D, et al. Predictors of in-hospital death after aneurysmal subarachnoid hemorrhage: analysis of a nationwide database (Swiss SOS [Swiss Study on Aneurysmal Subarachnoid Hemorrhage]). Stroke 2018;49(2):333-40. [DOI: 10.1161/STROKEAHA.117.019328] [DOI] [PubMed] [Google Scholar]
Van Gijn 2001
- Van Gijn J, Rinkel GJ. Subarachnoid haemorrhage: diagnosis, causes and management. Brain 2001;124:249-78. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Van Gijn 2007
- Van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet 2007;369:306-18. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Vergouwen 2010
- Vergouwen MD, Vermeulen M, Gijn J, Rinkel GJ, Wijdicks EF, Muizelaar JP, et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke 2010;41(10):2391-5. [DOI: 10.1161/STROKEAHA.110.589275] [DOI] [PubMed] [Google Scholar]
Vermeulen 1980
- Vermeulen M, Muizelaar JP. Do antifibrinolytic agents prevent rebleeding after rupture of a cerebral aneurysm? A review. Clinical Neurology and Neurosurgery 1980;82:25-30. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Vermeulen 1983
- Vermeulen M, Gijn J, Blijenberg BG. Spectrophotometric analysis of CSF after subarachnoid hemorrhage: limitations in the diagnosis of rebleeding. Neurology 1983;33:112-4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Vermeulen 1996
- Vermeulen M. Subarachnoid haemorrhage: diagnosis and treatment. Journal of Neurology 1996;243:496-501. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Weaver 1994
- Weaver JP, Fisher M. Subarachnoid hemorrhage: an update of pathogenesis, diagnosis and management. Journal of the Neurological Sciences 1994;125:119-31. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Weir 1987
- Weir B. Antifibrinolytics in subarachnoid hemorrhage. Do they have a role? No. Archives of Neurology 1987;44:116-8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Baharoglu 2013
- Baharoglu MI, Germans MR, Rinkel GJE, Algra A, Vermeulen M, Van Gijn J, et al. Antifibrinolytic therapy for aneurysmal subarachnoid haemorrhage . Cochrane Database of Systematic Reviews 2013, Issue 8. Art. No: CD001245. [DOI: 10.1002/14651858.CD001245.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Roos 1998
- Roos YB, Vermeulen M, Rinkel GJ, Algra A, Van Gijn J, Algra A. Systematic review of antifibrinolytic treatment in aneurysmal subarachnoid haemorrhage. Journal of Neurology, Neurosurgery and Psychiatry 1998;65:942-3. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Roos 2003
- Roos YB, Rinkel GJE, Vermeulen M, Algra A, Gijn J. Antifibrinolytic therapy for aneurysmal subarachnoid haemorrhage. Cochrane Database of Systematic Reviews 2003, Issue 2. Art. No: CD001245. [DOI: 10.1002/14651858.CD001245] [DOI] [PubMed] [Google Scholar]