

Abstract
Background:
Exposome research aims to describe and understand the extent to which all the exposures in human environments may affect our health over the lifetime. However, the way in which humans interact with their environment is socially patterned. Failing to account for social factors in research exploring the exposome may underestimate the magnitude of the effect of exposures or mask inequalities in the distribution of both exposures and outcomes.
Objectives:
We aimed to describe the extent to which social factors appear in the exposome literature, the manner in which they are used in empirical analyses and statistical modeling, and the way in which they are considered in the overall scientific approach.
Methods:
We conducted a scoping review of the literature using three databases (PubMed, Embase, and Web of Science) up to January 2022. We grouped studies based on the way in which the social variables were used in the analyses and quantified the type and frequency of social variables mentioned in the articles. We also qualitatively described the scientific approach used by authors to integrate social variables.
Results:
We screened 1,001 records, and 73 studies were included in the analysis. Fifty-five () used social variables as exposures or confounders or both, and a wide array of social variables were represented in the articles. Individual-level social variables were more often found, especially education and race/ethnicity, as well as neighborhood-level deprivation indices. Half of the studies used a hypothesis-free approach and the other half, a hypothesis-driven approach. However, in the latter group, of 35 studies, only 8 reported and discussed at least one possible social mechanism underlying the relationship observed between the social variable and the outcome.
Discussion:
Social factors in exposome research should be considered in a more systematic way, considering their role in structuring both the specific external and the internal exposome. Doing so could help to understand the mechanisms of construction and, potentially, alleviate social inequalities in health and mitigate the emergence of new ones. https://doi.org/10.1289/EHP11015
Introduction
Exposome research aims to describe and understand the extent and nature of all the exposures in human environments over the lifetime which may affect our health.1 The exposome originally “encompasses life-course environmental exposures (including lifestyle factors), from the prenatal period onwards.”2 The exposome can be classified into a) the external exposome, which refers to exposures outside of the body that can be general (broader social, cultural, and ecological contexts) or specific (chemical pollutants or lifestyle factors), and b) the internal exposome, which refers to exposures inside the body that are unique to the individual (metabolic processes, circulating blood biomarkers, hormones).3 These two domains are complementary, interrelated, and intertwined.
Increasingly, exposome scientists are taking an interest in social determinants of health—nonmedical factors that influence health outcomes, well-being, and quality of life (e.g., gender, race, education, income, housing, food security)—and how these may be included in the exposome framework, namely as part of the external exposome.4 A wide literature on social determinants of health has developed over many decades, predating the exposome concept,5,6 and which has established the relationship between social inequalities and health inequalities, tracked trends in these inequalities over time and across contexts, and examined potential processes and mechanisms that may underlie the observed associations.7 Although behavioral and lifestyle factors are important determinants of mortality, several epidemiological studies have shown that social inequalities cannot fully be explained by traditional risk factors.8,9 One set of mechanisms linking social exposures to subsequent health is via differential activation of a wide range of physiological responses.10
The social-to-biological transition10,11 refers to how the social environment can lead to biological alterations and may be of particular interest to exposome science. Social environments may influence health through two main types of socially distributed initial exposures: a) exposures of exogenous origin, emerging from the specific external exposome (environmental exposures such as pollution, pesticides, work exposures; behaviors such as tobacco, alcohol, diet), and b) exposures of endogenous origin involving the subjective interpretation of conditions (challenges, interpersonal relationships, and so on) followed by the response of internal biological mechanisms, mainly linked to stress perception and stress response systems (especially psychosocial exposures) likely to modify the internal exposome.12,13 Therefore, the hypothesis of a biological embodiment of the social environment makes the link between social factors in the general external exposome and biological responses that make up the internal exposome and consequence on health while taking into account the specific external exposome.14
Indeed, well-defined socially structured exposures, such as occupation, education, or deprivation, have been examined in relation to biological measures,15 which, in turn, are related to morbidity or mortality.16–18 The way humans interact with their environment is socially patterned, meaning that external exposures that may elicit internal biological responses should be considered in their social context. This has led some epidemiologists to argue that social factors should be considered as “fundamental causes” of disease19 and some sociologists to propose the socio-exposome framework.6 The importance of including social factors in research exploring the exposome is evident if we are to understand health outcomes and health inequalities. Failing to account for social factors in environmental health research may lead to underestimating the magnitude of the effect of exposures and/or masking inequalities in the distribution of both exposures and outcomes. However, the way in which social variables are included deserves thoughtful consideration because their meaning, what they measure, and the mechanisms by which they can have an impact on health are different.11 From an analytical point of view, exposome researchers may, on the one hand, want to take an “agnostic” and exploratory approach, using exposure-wide analyses to explore clusters of social exposures. On the other hand, they may have explicit reasons to include specific social variables based on previous research, aiming to test relevant pathways or to account for confounding. The debate among epidemiologists about the legitimacy of taking an agnostic approach and the choice of one method above another is not new,20 and this could have had practical consequences for current knowledge on exposome and health inequities. Nevertheless, both approaches present challenges when using social variables that deserve to be specified.
We carried out a scoping review to describe a) the extent to which social factors appear in the exposome empirical literature, b) the manner in which social variables are used in empirical analyses and statistical modeling, and c) the way in which social factors are considered in hypotheses or the overall scientific approach. Our objective is to establish the role of social determinants in recent exposome science and to consider how research on the exposome may move forward in its aim to develop an understanding of how the social environment affects our health, building upon existing research on social determinants of health and health inequalities over the life course.
Methods
Search Strategy
Based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines,21 a structured search strategy was developed to include title–abstract–keywords in a search string. The search strategy focused on articles related to both the social environment and the concept of the exposome. The full set of search terms was as follows:
(soci* OR justice OR injustice OR equity OR inequity OR gender OR race OR ethnicity OR exclusion OR discrimination OR class OR oppression OR dominance OR geograph* OR housing OR “living conditions” OR urban OR “built environment” OR psychosoci* OR workplace OR education* OR income OR occupation* OR lifecourse OR “work conditions” OR rural) AND (exposom*).
The choice of keywords was based on the social epidemiology literature and is related to the socioeconomic determinants of health (material and psychosocial exposures), excluding behaviors. The search was limited to peer-reviewed articles from inception up until 3 January 2022 and was run using three databases: Pubmed, Embase, and Web of Science. All studies identified as suitable were extracted using Zotero (version 5.0.96.3; Zotero).
Eligibility Criteria
Eligible articles met the following inclusion criteria: a) peer-reviewed articles, b) empirical articles (controlled trials, cohort, or cross-sectional study designs), c) on human populations, d) dealing with the concept of exposome—we used a broad definition of the exposome as multiple exposures (at least two), and e) using at least one variable related to the social environment. We excluded a) animal studies and b) books, book reviews, book chapters, conference abstracts, conference papers, editorials or letters to the editor, commentaries, and literature reviews. After applying the inclusion and exclusion criteria, all articles were written in English; therefore, no language restrictions were needed.
Screening and Extraction of Data
After removing duplicates, we conducted a screening process to select the papers to be fully reviewed. First, titles and abstracts were examined by four authors. L.N. fully screened the whole extraction and, in parallel, M.K.I., R.C., and L.M. conducted a second blind screening (one-third each) so that each abstract was screened twice. Then, studies classified as irrelevant in both the parallel screenings were excluded from further review. All disagreements regarding classification were resolved by discussion between reviewers. Extracted data included a) article identification (first author name, publication year, journal, publication title, keywords, and country), b) definition of the exposome, c) nature of the social variables and their usage, and d) suggested social mechanisms underlying the association.
Synthesis of Results
Given the heterogeneity among the studies, we used a descriptive approach to review the available evidence regarding the use of social factors in an exposome context. We grouped studies according to the manner in which social variables were used in the analyses (exposure, confounder, effect-modifier, descriptive). We used the following definitions. A confounder is a variable that causes both the exposure and outcome of interest.22 An effect-modifier modulates the effect of an exposure on the outcome across levels of this variable,23 for example, the relationship between exposure to air pollution and respiratory health is different for children in low vs. high income and education groups.24 We further quantified the type and frequency of social variables mentioned in the articles. We then built a word cloud using the package ggwordcloud in R software (version 4.0.5; R Development Core Team) as a visualization tool. We also qualitatively described the approach used by authors to integrate social variables into the exposome definition (agnostic or a priori hypothesis-driven) and the presence of a social hypothesis in the introduction and a social mechanism in the discussion. We considered agnostic/hypothesis-free approaches when researchers aimed to explore their data with no predefined hypothesis of interest, and hypothesis-driven approaches when researchers aimed to test an explicit hypothesis about the relationship between exposure(s) and outcome(s). We considered a social mechanism to be present if any underlying process linking the social factor(s) to the outcome(s) was mentioned in the discussion.
Results
Selection of Articles
The search yielded a total of 1,001 articles: 309 records in PubMed, 365 in Embase, and 327 records in Web of Science. Once all the articles were retrieved, 536 duplicates were identified and 465 articles were retained. The first screening stage—titles and abstracts—led to the exclusion of 382 articles that did not meet the eligibility criteria. The second screening stage—full-text assessment—led to the exclusion of an additional 10 articles, 7 of which did not contain social variables in the text and 3 were methodological articles. A final sample of 73 articles was retained for the scoping review (Figure S1).
Description of the Selected Articles
Characteristics of the selected studies.
As shown in Table S1, there was a gradual increase in the use of social variables in exposome research over time: Among the 73 studies, 6 were published before 2017 compared with 16 published in 2020, 18 published in 2021, and already 2 published in the first month of 2022. Nearly half of the studies [33 (45%)] were conducted in Europe and 21 (29%) in the United States. Regarding the study population, 28 (38%) of the included articles focused on the period around childbirth [pregnant women, 6 (8%); new-borns, 9 (12%); and young children, 13 (18%)]; 25 (34%) on adults; and 10 (14%) on children and adolescents. Finally, 7 (10%) used geographical units and 2 (3%) focused on households. There was also 1 meta-analysis (1%). Most of the included papers defined the term “exposome” using the original definition by Wild referring to the totality of exposure experienced from conception until death and referred to his 2012 paper.3 Nevertheless, 26 papers did not give any formal definition of the term exposome.
Use of social variables.
As shown in Table S2, of the 73 articles included in the scoping review, 22 (30%) used social variables as exposures, 15 (21%) used social variables as confounders, and 18 (25%) used social variables as both exposures and confounders. In addition, 18 studies used social variables in mixed ways: 5 studies used social variables as descriptive parameters of the study population, 2 as an effect-modifier, 1 as both exposure and effect-modifier, 2 as both confounder and effect-modifier, and 8 as exposure, confounder, and descriptive parameters.
Nature and type of social variables.
In total, 285 different social variables were identified by reviewing the 73 articles (Figure 1). Detailed information regarding the social variables are provided in Table S3. The most frequently represented category was individual-level social characteristics, accounting for 105 variables (37%). Area-level social characteristics accounted for 80 variables (28%), parental social characteristics for 59 variables (21%), and family/household social characteristics for 41 variables (14%).
Figure 1.
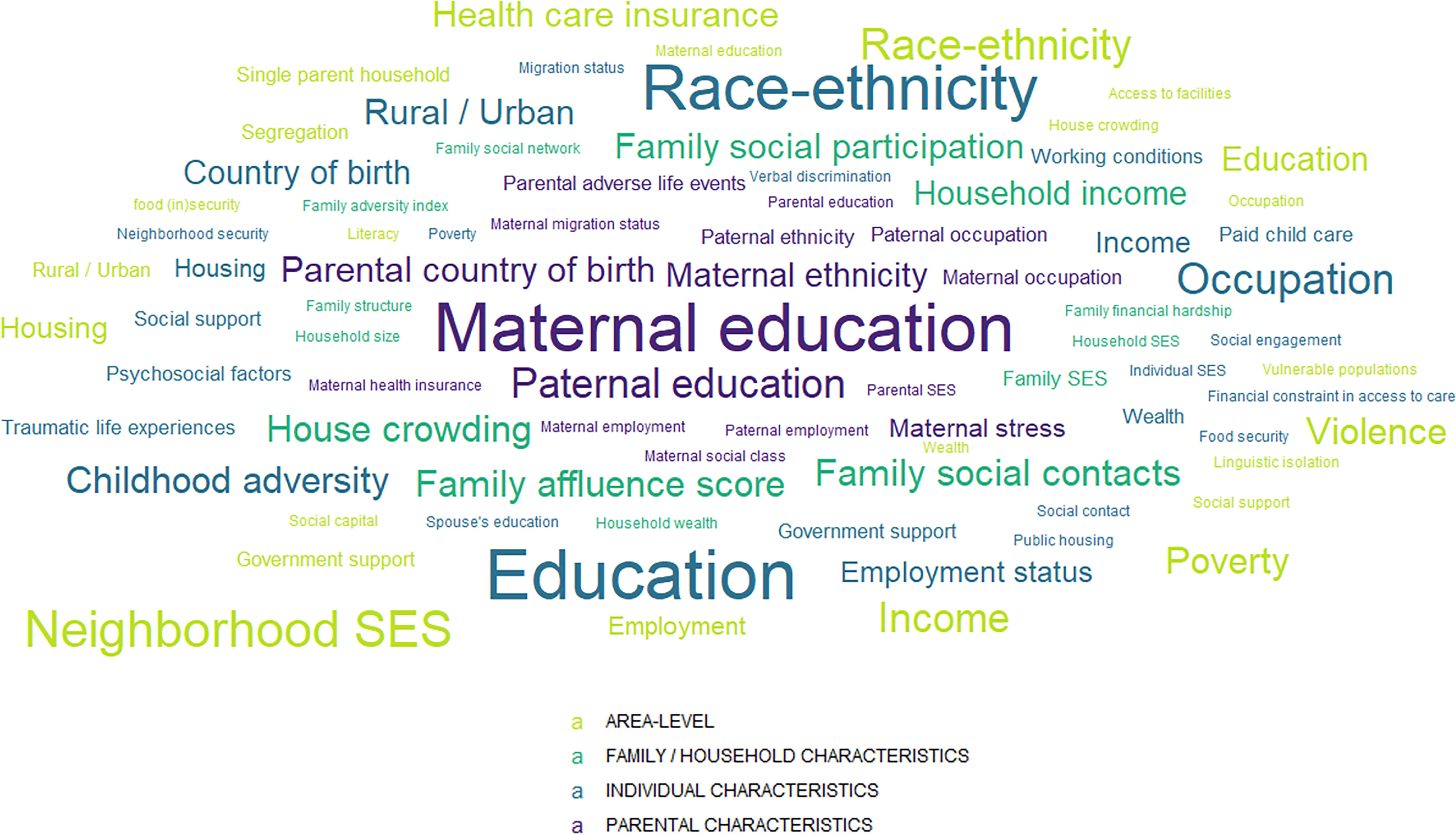
Word cloud of the social variables used in the selected articles. Detailed table is available in Table S3. Note: SES, socioeconomic status.
Among individual-level characteristics, education and race/ethnicity were the most frequently used social variables [ times (41%)]. Among parental characteristics, education was the most commonly used social indicator, with (53%). Maternal characteristics, and especially education, were more often used compared with paternal characteristics. Regarding household characteristics, material conditions (e.g., income), social network and living conditions (e.g., house crowding) were the most frequently used social variables. Among area-level characteristics, financial difficulties and especially poverty were more often used [ (20%)], followed by neighborhood deprivation [ (15%)].
By examining the usage of each type of social variable, most were introduced as exposures [ (58%)], and () were used as confounders. We observed that in articles where social variables were considered exposures, a considerable number of variables were included, whereas in those where social variables were considered confounders, fewer social variables were included. In particular, parental education and participant’s race/ethnicity were mostly used as confounders.
Agnostic, a priori hypothesis-driven approaches and underlying social mechanisms.
We described the approach used by authors regarding the inclusion of the social environment into the exposome in Figure 2. Among the 73 studies, 36 (49%) used a hypothesis-free (agnostic) approach, 35 (48%) used a hypothesis-driven approach, and 2 (3%) used a mixed approach (Table S4). Among articles using an agnostic approach, 16 mentioned social hypotheses or mechanisms.
Figure 2.

Social environment, a priori hypotheses and underlying mechanisms. Detailed table is available in Table S4. Note: Agnostic approach, data exploration with no predefined hypothesis of interest; hypothesis-driven approach, test of an explicit hypothesis about the relationship between exposure(s) and outcome(s).
Among articles using a hypothesis-driven approach, eight discussed one or more possible mechanisms underlying the relationship between social variables and the outcome,25–32 among which seven also mentioned social hypothesis in the introduction.25–31 The mechanisms referred to different health behaviors27,31,32 (nutrition), different occupational26,28 (physical and chemical) and domestic26,32 (pesticides) exposures, or different psychosocial exposures25,29–32 (stress, social network), depending on social position. Two of the studies also mentioned epigenetics and the social-to-biological processes29,30—or how social factors are associated with biological mechanisms. Of note, most of the studies using a hypothesis-driven approach did not mention any social hypothesis nor social-to-biological mechanism33–54 [ (63%)].
Discussion
The first objective of our study was to describe the extent to which social factors appear in the exposome literature. Our review identified 73 articles where social variables had been included: relatively few compared with the overall number of articles in the field of exposome research. Although the social environment partly determines the level of exposure for many factors19 (physicochemical exposures, behaviors), this dimension is still poorly considered in the exposome literature. It is important to emphasize that this scarce consideration of the social environment may point toward an underappreciation of potentially important underlying mechanisms in some exposome research, such as the impact of socially distributed psychosocial exposures that may modify biological functioning (via the stress response system in particular) and may interact with other exposures.
Among the 73 studies matching the inclusion criteria for our scoping review, most [ (75%)] used social variables as exposures and/or confounders and a wide array of social variables were used across the articles. Individual-level social variables were more often found, especially education and race/ethnicity. Deprivation indices at the neighborhood level were also widely used. Around half of the studies used a hypothesis-free approach and the other half a hypothesis-driven approach. However, in the latter group, only 8 studies reported and discussed one or more possible social mechanisms underlying the relationship observed between the social variable and the outcome.
The wide range of potential social factors available present conceptual and methodological challenges given that their meanings may change over time, space, and in relation to sociocultural contexts. When such variables were used as exposures, we observed two main approaches, each with their conceptual and methodological advantages and challenges. First, agnostic, or hypothesis-free approaches, are common place in exposome research and mimic methods used in genomics. Often the aim in these studies is to identify internal omic signals of external exposures to pollutants or toxins,4 and an agnostic approach means that new and relatively unknown biomarkers or signals can be found and then replicated or subsequently examined in more depth. This approach may help researchers to establish the biological plausibility of relationships between external exposures and internal biomarkers.55 The question arising is whether such exposure-wide approaches make sense when social variables are being considered. By agnostically treating exposure variables the same way in these types of analyses, any inherent structural or hierarchical relation between variables is ignored. Yet race/ethnicity or class are stratifying or “upstream” variables that affect the distribution of many other social factors, such as housing or psychosocial stressors.56 By deciding to treat variables agnostically, does a hypothesis that these variables are “equivalent” and unrelated to each other not inevitably slip in?
The second approach we observed, commonly used in epidemiology, is where one or several hypotheses are tested. In the context of exposome research, the hypothesis would be that a social variable is associated with biomarkers or with a health outcome, or both. At present, there is a vast literature on the relationships between social factors of different types and a variety of biological markers through multiple mechanisms15 and decades of research on health inequalities.57 In our review of the literature, we observed that relatively few of the hypothesis-driven papers, 12 of 35 (34%), put forward an explicit hypothesis about the relationship between the social variables and the outcome. When considering social-to-biological research, the underlying hypothesis and nature of the relationship is worth clarifying to facilitate the interpretation of findings and draw conclusions in terms of health inequalities.11 Researchers working with social and health data within the exposome framework may be interested in examining their hypotheses using one of the many existing causal inference methods, including the use of instrumental variables, such as mendelian randomization, mediation analysis, and many others.58
Of note, it is entirely plausible when using social variables in relation to health outcomes that reverse causation may occur.59 As well as social factors causing health outcomes, health conditions can impact conditions such as where people live, through access to care or socioeconomic factors, or lead people to change their employment status, among many other examples. This is a standard problem in any quantitative analysis and deserves attention from the researchers performing the analyses. When longitudinal data collected from childhood are used, as is the case for some exposome analysis, the temporal sequence of early life experiences helps to some extent to avert the problem of reverse causation.60
As well as using social variables as exposures in either hypothesis-free or hypothesis-driven approaches, many of the studies in our sample used them as confounding factors. This means that the authors wanted to adjust their statistical associations for a social variable, potentially associated with their exposure and outcome, to avoid spurious results. Controlling for social variables as potential confounders may be necessary; however, it is important to avoid interpreting the association between the confounding variable and outcome in multivariable analyses. Such interpretations may lead to table 2 fallacy, and lead to mistakes in the interpretation of these estimates.61 Moreover, such practice has been considered as inappropriate by some epidemiologists who argue that social variables should instead be systematically treated as “fundamental causes.”19,62
Beyond the question of integrating social variables in exposome studies, it is fundamental to recognize that the choice of an agnostic or hypothesis-driven approach brings with it a different theoretical framework that will influence how exposome researchers consider the question of the origins of social inequalities in health.63–65 Many pragmatic issues arise regarding the availability of social variables and their comparability or harmonization across data sets. As such, it was unsurprising to see that many of the papers we reviewed used education (individual or parental) as a social variable. Education is often used as a measure of socioeconomic position, a global concept that captures both resources and prestige.66 It is relatively straightforward to collect, often measuring the number of years of education or level of diploma, and therefore seemingly easy to harmonize across data sets. However, there are a number of considerations to bear in mind when using education as a social variable. Over time, the proportion of people attending school, achieving a high school-level diploma and attending further education has increased, thus the way in which educational attainment relates to other social factors and health outcomes has evolved.57 Therefore, we must consider a number of questions: Is the quality of education equivalent across context and time? In a specific country at a specific time, who was able to achieve a high level of education? What was the mandatory legal school age limit? Did this vary according to gender, race, class? What kind of benefits does a high level of education offer over time, between countries?67 When education is used in relation to health outcomes, it is important to consider the mechanisms that may underlie the association, such as behavioral, psychosocial, and material pathways,68 a point we will return to in our recommendations below.
The second most used variable was race/ethnicity. In our scoping review, we found that race/ethnicity variables were most often used as a confounder. Although this type of adjustment may reduce bias, it does not help to understand the role or the meaning of race/ethnicity. Race and ethnicity variables may be used at the individual and neighborhood levels as socially constructed categories reflecting societal and individual histories of discrimination and dispossession experienced by minoritized people69 and vary according to the socio-political history of each country. Providing that researchers understand the theorical bases upon which race/ethnicity affects health and disease along the life course, the exposome research framework can provide the opportunity to explore the relationships between minoritized groups within a population and their physical and social environments. Given the potential harms of discrimination to health that may operate through social-to-biological pathways,70 using a conceptually clear race/ethnicity variable in relation to biological and health measures may elucidate important connections between the social experience of minoritized people and the consequences of this upon their health in the aim of understanding and redressing inequalities.70
Deprivation indices are another type of very commonly used social variable. Deprivation, covering the various conditions, independent of income, experienced by people who are poor, is a multidimensional concept, closely related to poverty.71 Ecological indices of deprivation are mainly constructed from population census data and are often used as a way to deal with an absence of individual socioeconomic data collected alongside biological or health data.72,73 These indices measure relative deprivation at a given geographical level, as opposed to other measures of relative poverty and deprivation that require individual-level survey questions. Once the respective scores are constructed and divided into a suitable variable, such as quintiles, each ward or postal code is attributed a deprivation quintile. Inhabitants of that place may be attributed the corresponding deprivation quintile to represent the deprivation level of their place of residence and possibly as a proxy-variable for their social position, should individual-level data be unavailable. Both the Carstairs and Townsend indices,74 developed in the 1980s in the UK and on which many other deprivation indices are based, have shown that a higher level of deprivation is associated with an increased risk of mortality and morbidity.74 Even if the geographical scale being used is small, it is important to consider the potential for error when using ecological indices to approximate individual socioeconomic position, which may lead to an underestimation of the extent of social inequality that would be observed with individual-level indicators.73,75 We think that exposome studies using such social variables would benefit from outlining the respective strengths and limitations of specific variable, and the underlying hypothesis the variable is being used to test, in the case of hypothesis-driven work (see the “recommended questions” in Figure 3).
Figure 3.

Recommendations regarding the use of social variables in the exposome context.
Regarding parental characteristics, we found that maternal characteristics were more often considered than paternal characteristics. This lack of attention paid to paternal exposures has been discussed by Sharp et al.76 who underlined that empirical literature on paternal exposures is rare. Often the data regarding the father are lacking, and where they do exist, tend to be of lower quality. Moreover, the emphasis on maternal exposures and the lack of available data on paternal exposures reflect in part gender imbalances in power and health inequities that result from broader structural power imbalances.
Limitations
Some limitations of this review should be mentioned. By using the term “exposom*” in our literature review, we may have restricted our search to the most recent articles using this concept and left out older articles where multiple exposures were being considered before the term “exposome” was coined. We also acknowledge that other social variables may not have been captured by the search terms we used; therefore, we most likely selected a subset of the exposome studies using social variables. Finally, we restricted our scoping review to peer-reviewed articles published in English and did not consider the gray literature nor the bibliographies of studies included in our pool. This may have biased our selection of papers. However, this scoping review did not aim to be systematic but, rather, to provide an overall picture of the use of social variables in exposome research.
Recommendations
Based on our review, we developed a set of recommendations to guide exposome researchers when using social variables based on the health inequalities literature (Figure 3). The first decision researchers may need to make is about whether the social variables are being used as exposures or confounders, the two most common usages found in our review. When using them as exposures, there are two main approaches used in exposome research that deserve to be made explicit, each with their advantages and disadvantages: agnostic or hypothesis-driven approaches. The agnostic approach may be helpful for generating hypotheses to be subsequently tested using a hypothesis-driven approach. Based on the health inequalities and social-to-biological literature,10,11 we suggest that researchers using social variables as exposures in hypothesis-driven studies first make explicit their hypothesis about how a social variable relates to biological/health outcomes and after which develop a theoretical model for testing this hypothesis, with the use of resources such as Bartley (2015),57 including potential underlying mechanisms. Only then should they select which social variables are most appropriate to carry out their analyses.67 To help develop this theoretical model, it may be useful to consider three broad explanatory models, the behavioral, material, and psychosocial.57
The behavioral model suggests that the social variable in question is related to different health behaviors, such as smoking, drinking, food preferences, or exercise. The material model suggests that the social variable is related to physical and chemical exposures due to housing conditions, occupational exposures, or exposures in the place of residence, for example. When considering social-to-biological processes, these two models refer to mechanisms of exogenous origin, consisting of processes through which socially patterned conditions external to the body enter the body and elicit a physiological response from it and/or a physical effort. Finally, the psychosocial model pertains to social variables being related to stressors, such as adverse childhood experiences, discriminations, or job stress. This last model underlines a mechanism of endogenous origin that refers to internal biological processes that occur as a consequence of sensory and neurobiological signals triggered by perceptions and emotions. These mechanisms driving social-to-biological processes may operate simultaneously (e.g., poor material conditions and psychosocial adverse experiences) but also interact with each other (material conditions, as well as psychosocial experiences, are likely to influence behaviors). All three processes are likely to contribute to “how we literally incorporate, biologically, the world around us.”65
Conclusion
Our scoping review established the small but growing role of social variables in recent exposome science.77 Overall, we conclude that researchers in the exposome field are increasingly aiming to integrate social variables into their studies, which is important considering the social distribution of various dimensions of the exposome. However, the role of these social variables is not always made explicit, and their use is often not placed within the context of an appropriate body of literature on the social determinants of health. Based on our findings, we have made recommendations to guide researchers when using social variables in their exposome study, and suggest that, when appropriate, they make their hypothesis about the relation between the social variable and outcome clear. Moving toward a more interdisciplinary exposome framework, for example, by including social scientists in environmental health research, could accelerate the development of theoretical approaches to specifying social forces that should be included in exposome research.
Supplementary Material
Acknowledgments
L.N. is supported by the Healthy Choices project, funded by the Research Council of Norway grant 289440. S.K.S. is supported by the Australian Research Council Center of Excellence in Population Ageing Research (project no. CE170100005). M.K.I., C.D., and R.C. are members of the Expanse Consortium funded by the European Union’s Horizon 2020 research and innovation program under grant 874627. L.M. is supported by the Ligue contre le Cancer as part of the labeling process.
References
- 1.Vermeulen R, Schymanski EL, Barabási AL, Miller GW. 2020. The exposome and health: where chemistry meets biology. Science 367(6476):392–396, PMID: , 10.1126/science.aay3164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wild CP. 2005. Complementing the genome with an “exposome”: the outstanding challenge of environmental exposure measurement in molecular epidemiology. Cancer Epidemiol Biomarkers Prev 14(8):1847–1850, PMID: , 10.1158/1055-9965.EPI-05-0456. [DOI] [PubMed] [Google Scholar]
- 3.Wild CP. 2012. The exposome: from concept to utility. Int J Epidemiol 41(1):24–32, PMID: , 10.1093/ije/dyr236. [DOI] [PubMed] [Google Scholar]
- 4.Vineis P, Robinson O, Chadeau-Hyam M, Dehghan A, Mudway I, Dagnino S. 2020. What is new in the exposome? Environ Int 143:105887, PMID: , 10.1016/j.envint.2020.105887. [DOI] [PubMed] [Google Scholar]
- 5.Juarez PD, Matthews-Juarez P, Hood DB, Im W, Levine RS, Kilbourne BJ, et al. . 2014. The public health exposome: a population-based, exposure science approach to health disparities research. Int J Environ Res Public Health 11(12):12866–12895, PMID: , 10.3390/ijerph111212866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Senier L, Brown P, Shostak S, Hanna B. 2017. The socio-exposome: advancing exposure science and environmental justice in a postgenomic era. Environ Sociol 3(2):107–121, PMID: , 10.1080/23251042.2016.1220848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marmot M, Allen J, Bell R, Bloomer E, Goldblatt P, Consortium for the European Review of Social Determinants of Health and the Health Divide. 2012. WHO European review of social determinants of health and the health divide. Lancet 380(9846):1011–1029, PMID: , 10.1016/S0140-6736(12)61228-8. [DOI] [PubMed] [Google Scholar]
- 8.Gallo V, Mackenbach JP, Ezzati M, Menvielle G, Kunst AE, Rohrmann S, et al. . 2012. Social inequalities and mortality in Europe—results from a large multi-national cohort. PLoS One 7(7):e39013, PMID: , 10.1371/journal.pone.0039013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Stringhini S, Dugravot A, Shipley M, Goldberg M, Zins M, Kivimäki M, et al. . 2011. Health behaviours, socioeconomic status, and mortality: further analyses of the British Whitehall II and the French GAZEL prospective cohorts. PLoS Med 8(2):e1000419, PMID: , 10.1371/journal.pmed.1000419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Blane D, Kelly-Irving M, d’Errico A, Bartley M, Montgomery S. 2013. Social-biological transitions: how does the social become biological? Longit Life Course Stud 4(2):136–146, 10.14301/llcs.v4i2.236. [DOI] [Google Scholar]
- 11.Kelly-Irving M, Delpierre C. 2021. Framework for understanding health inequalities over the life course: the embodiment dynamic and biological mechanisms of exogenous and endogenous origin. J Epidemiol Community Health 75(12):1181–1186, PMID: , 10.1136/jech-2021-216430. [DOI] [PubMed] [Google Scholar]
- 12.McEwen BS. 2007. Physiology and neurobiology of stress and adaptation: central role of the brain. Physiol Rev 87(3):873–904, PMID: , 10.1152/physrev.00041.2006. [DOI] [PubMed] [Google Scholar]
- 13.Meloni M, Cromby J, Fitzgerald D, Lloyd S. 2018. The Palgrave Handbook of Biology and Society. London, UK: Palgrave Macmillan. [Google Scholar]
- 14.Juarez PD, Hood DB, Song MA, Ramesh A. 2020. Use of an exposome approach to understand the effects of exposures from the natural, built, and social environments on cardio-vascular disease onset, progression, and outcomes. Front Public Health 8:379, PMID: , 10.3389/fpubh.2020.00379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vineis P, Delpierre C, Castagné R, Fiorito G, McCrory C, Kivimaki M, et al. . 2020. Health inequalities: embodied evidence across biological layers. Soc Sci Med 246:112781, PMID: , 10.1016/j.socscimed.2019.112781. [DOI] [PubMed] [Google Scholar]
- 16.Stringhini S, Carmeli C, Jokela M, Avendaño M, Muennig P, Guida F, et al. . 2017. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1.7 million men and women. Lancet 389(10075):1229–1237, PMID: , 10.1016/S0140-6736(16)32380-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rocha V, Fraga S, Moreira C, Carmeli C, Lenoir A, Steptoe A, et al. . 2020. Life-course socioeconomic disadvantage and respiratory-related functioning lost in older adults: a multi-cohort study of 53 788 individuals. Eur Respir J 56(suppl 64):437, 10.1183/13993003.congress-2020.437. [DOI] [Google Scholar]
- 18.Kivimäki M, Vahtera J, Tabák AG, Halonen JI, Vineis P, Pentti J, et al. . 2018. Neighbourhood socioeconomic disadvantage, risk factors, and diabetes from childhood to middle age in the Young Finns Study: a cohort study. Lancet Public Health 3(8):e365–e373, PMID: , 10.1016/S2468-2667(18)30111-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Link BG, Phelan J. 1995. Social conditions as fundamental causes of disease. J Health Soc Behav Spec No: 80–94, PMID: , 10.2307/2626958. [DOI] [PubMed] [Google Scholar]
- 20.Shim JK, Thomson LK. 2010. The end of the epidemiology wars? Epidemiological ‘ethics’ and the challenge of translation. Biosocieties 5(2):159–179, 10.1057/biosoc.2010.6. [DOI] [Google Scholar]
- 21.Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. . 2018. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 169(7):467–473, PMID: , 10.7326/M18-0850. [DOI] [PubMed] [Google Scholar]
- 22.VanderWeele TJ. 2019. Principles of confounder selection. Eur J Epidemiol 34(3):211–219, PMID: , 10.1007/s10654-019-00494-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.VanderWeele TJ. 2009. On the distinction between interaction and effect modification. Epidemiology 20(6):863–871, PMID: , 10.1097/EDE.0b013e3181ba333c. [DOI] [PubMed] [Google Scholar]
- 24.Cakmak S, Hebbern C, Cakmak JD, Vanos J. 2016. The modifying effect of socioeconomic status on the relationship between traffic, air pollution and respiratory health in elementary schoolchildren. J Environ Manage 177:1–8, PMID: , 10.1016/j.jenvman.2016.03.051. [DOI] [PubMed] [Google Scholar]
- 25.Barzilay R, Moore TM, Calkins ME, Maliackel L, Jones JD, Boyd RC, et al. . 2021. Deconstructing the role of the exposome in youth suicidal ideation: trauma, neighborhood environment, developmental and gender effects. Neurobiol Stress 14:100314, PMID: , 10.1016/j.ynstr.2021.100314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bergmann AJ, North PE, Vasquez L, Bello H, Del Carmen Gastañaga Ruiz M, Anderson KA. 2017. Multi-class chemical exposure in rural Peru using silicone wristbands. J Expo Sci Environ Epidemiol 27(6):560–568, PMID: , 10.1038/jes.2017.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Buekers J, Colles A, Cornelis C, Morrens B, Govarts E, Schoeters G. 2018. Socio-economic status and health: evaluation of human biomonitored chemical exposure to per-and polyfluorinated substances across status. Int J Environ Res Public Health 15(12):2818, PMID: , 10.3390/ijerph15122818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Eyles E, Manley D, Jones K. 2019. Occupied with classification: which occupational classification scheme better predicts health outcomes? Soc Sci Med 227:56–62, PMID: , 10.1016/j.socscimed.2018.09.020. [DOI] [PubMed] [Google Scholar]
- 29.Martins J, Czamara D, Sauer S, Rex-Haffner M, Dittrich K, Dörr P, et al. . 2021. Childhood adversity correlates with stable changes in DNA methylation trajectories in children and converges with epigenetic signatures of prenatal stress. Neurobiol Stress 15:100336, PMID: , 10.1016/j.ynstr.2021.100336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Nwanaji-Enwerem JC, Van Der Laan L, Kogut K, Eskenazi B, Holland N, Deardorff J, et al. . 2021. Maternal adverse childhood experiences before pregnancy are associated with epigenetic aging changes in their children. Aging (Albany NY) 13(24):25653–25669, PMID: , 10.18632/aging.203776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sehgal H, Toscano WA. 2021. Neighborhood exposures and blood pressure outcomes: a cross-sectional environmental study among 19–53 years-old Parsis in Mumbai. Int J Environ Res Public Health 18(16):8594, PMID: , 10.3390/ijerph18168594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Yitshak-Sade M, Fabian MP, Lane KJ, Hart JE, Schwartz JD, Laden F, et al. . 2020. Estimating the combined effects of natural and built environmental exposures on birthweight among urban residents in Massachusetts. Int J Environ Res Public Health 17(23):8805, PMID: , 10.3390/ijerph17238805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bennett B, Workman T, Smith MN, Griffith WC, Thompson B, Faustman EM. 2020. Characterizing the neurodevelopmental pesticide exposome in a children’s agricultural cohort. Int J Environ Res Public Health 17(5):1479, PMID: , 10.3390/ijerph17051479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Chung MK, Kannan K, Louis GM, Patel CJ. 2018. Toward capturing the exposome: exposure biomarker variability and coexposure patterns in the shared environment. Environ Sci Technol 52(15):8801–8810, PMID: , 10.1021/acs.est.8b01467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Doherty BT, Pearce JL, Anderson KA, Karagas MR, Romano ME. 2020. Assessment of multipollutant exposures during pregnancy using silicone wristbands. Front Public Health 8:547239, PMID: , 10.3389/fpubh.2020.547239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Dreno B, Shourick J, Kerob D, Bouloc A, Taïeb C. 2020. The role of exposome in acne: results from an international patient survey. J Eur Acad Dermatol Venereol 34(5):1057–1064, PMID: , 10.1111/jdv.16119. [DOI] [PubMed] [Google Scholar]
- 37.Ferrreira APSDS, Pereira EC, Salles FJ, Silva FFD, Batista BL, Handakas E, et al. . 2019. Home-based and informal work exposes the families to high levels of potentially toxic elements. Chemosphere 218:319–327, PMID: , 10.1016/j.chemosphere.2018.11.083. [DOI] [PubMed] [Google Scholar]
- 38.Gagliardi A, Dugué PA, Nøst TH, Southey MC, Buchanan DD, Schmidt DF, et al. . 2020. Stochastic epigenetic mutations are associated with risk of breast cancer, lung cancer, and mature B-cell neoplasms. Cancer Epidemiol Biomarkers Prev 29(10):2026–2037, PMID: , 10.1158/1055-9965.EPI-20-0451. [DOI] [PubMed] [Google Scholar]
- 39.Lau CHE, Siskos AP, Maitre L, Robinson O, Athersuch TJ, Want EJ, et al. . 2018. Determinants of the urinary and serum metabolome in children from six European populations. BMC Med 16(1):202, PMID: , 10.1186/s12916-018-1190-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lee WC, Fisher M, Davis K, Arbuckle TE, Sinha SK. 2017. Identification of chemical mixtures to which Canadian pregnant women are exposed: the MIREC Study. Environ Int 99:321–330, PMID: , 10.1016/j.envint.2016.12.015. [DOI] [PubMed] [Google Scholar]
- 41.Levin-Schwartz Y, Gennings C, Schnaas L, Del Carmen Hernández Chávez M, Bellinger DC, Téllez-Rojo MM, et al. . 2019. Time-varying associations between prenatal metal mixtures and rapid visual processing in children. Environ Health 18(1):92, PMID: , 10.1186/s12940-019-0526-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Li N, Friedrich R, Maesano CN, Medda E, Brescianini S, Stazi MA, et al. . 2019. Lifelong exposure to multiple stressors through different environmental pathways for European populations. Environ Res 179(pt A):108744, PMID: , 10.1016/j.envres.2019.108744. [DOI] [PubMed] [Google Scholar]
- 43.Maitre L, Robinson O, Martinez D, Toledano MB, Ibarluzea J, Marina LS, et al. . 2018. Urine metabolic signatures of multiple environmental pollutants in pregnant women: an exposome approach. Environ Sci Technol 52(22):13469–13480, PMID: , 10.1021/acs.est.8b02215. [DOI] [PubMed] [Google Scholar]
- 44.Mueller W, Steinle S, Pärkkä J, Parmes E, Liedes H, Kuijpers E, et al. . 2020. Urban greenspace and the indoor environment: pathways to health via indoor particulate matter, noise, and road noise annoyance. Environ Res 180:108850, PMID: , 10.1016/j.envres.2019.108850. [DOI] [PubMed] [Google Scholar]
- 45.Nielsen CC, Amrhein CG, Shah PS, Stieb DM, Osornio-Vargas AR, Canadian Neonatal Network, et al. 2020. Space-time hot spots of critically ill small for gestational age newborns and industrial air pollutants in major metropolitan areas of Canada. Environ Res 186:109472, PMID: , 10.1016/j.envres.2020.109472. [DOI] [PubMed] [Google Scholar]
- 46.Nielsen CC, Amrhein CG, Serrano-Lomelin JA, Osornio-Vargas AR, DoMiNO Team. 2019. Geographic information assessment of maternal ambient health hazards and adverse birth outcomes in Canada. Sci Total Environ 696:134091, 10.1016/j.scitotenv.2019.134091. [DOI] [Google Scholar]
- 47.Ourshalimian S, Naser AM, Rahman M, Doza S, Stowell J, Narayan KMV, et al. . 2019. Arsenic and fasting blood glucose in the context of other drinking water chemicals: a cross-sectional study in Bangladesh. Environ Res 172:249–257, PMID: , 10.1016/j.envres.2018.12.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Salles FJ, Tavares DJB, Freire BM, Ferreira APSDS, Handakas E, Batista BL, et al. . 2021. Home-based informal jewelry production increases exposure of working families to cadmium. Sci Total Environ 785:147297, 10.1016/j.scitotenv.2021.147297. [DOI] [Google Scholar]
- 49.Shaw GM, Yang W, Roberts EM, Kegley SE, Stevenson DK, Carmichael SL, et al. . 2018. Residential agricultural pesticide exposures and risks of spontaneous preterm birth. Epidemiology 29(1):8–21, PMID: , 10.1097/EDE.0000000000000757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Stratakis N, Conti DV, Borras E, Sabido E, Roumeliotaki T, Papadopoulou E, et al. . 2020. Association of fish consumption and mercury exposure during pregnancy with metabolic health and inflammatory biomarkers in children. JAMA Netw Open 3(3):e201007, PMID: , 10.1001/jamanetworkopen.2020.1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Travis SC, Aga DS, Queirolo EI, Olson JR, Daleiro M, Kordas K. 2020. Catching flame retardants and pesticides in silicone wristbands: evidence of exposure to current and legacy pollutants in Uruguayan children. Sci Total Environ 740:140136, PMID: , 10.1016/j.scitotenv.2020.140136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Wan Y, North ML, Navaranjan G, Ellis AK, Siegel JA, Diamond ML. 2022. Indoor exposure to phthalates and polycyclic aromatic hydrocarbons (PAHs) to Canadian children: the Kingston allergy birth cohort. J Expo Sci Environ Epidemiol 32(1):69–81, PMID: , 10.1038/s41370-021-00310-y. [DOI] [PubMed] [Google Scholar]
- 53.Yan Q, Liew Z, Uppal K, Cui X, Ling C, Heck JE, et al. . 2019. Maternal serum metabolome and traffic-related air pollution exposure in pregnancy. Environ Int 130:104872, PMID: , 10.1016/j.envint.2019.05.066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Yang Q, Zhao Y, Qiu X, Zhang C, Li R, Qiao J. 2015. Association of serum levels of typical organic pollutants with polycystic ovary syndrome (PCOS): a case–control study. Hum Reprod 30(8):1964–1973, PMID: , 10.1093/humrep/dev123. [DOI] [PubMed] [Google Scholar]
- 55.Hill AB. 1965. The environment and disease: association of causation? Proc R Soc Med 58(5):295–300, PMID: , 10.1177/003591576505800503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Solar O, Irwin A. 2010. A Conceptual Framework for Action on the Social Determinants of Health. Social Determinants of Health: Social Determinants of Health Discussion Paper 2 (Policy and Practice). http://apps.who.int/iris/bitstream/10665/44489/1/9789241500852_eng.pdf [accessed 15 January 2022].
- 57.Bartley M. 2016. Health Inequality: An Introduction to Concepts, Theories and Methods. 2nd ed. Cambridge, UK: Polity Press. [Google Scholar]
- 58.Kelly-Irving M, Ball WP, Bambra C, Delpierre C, Dundas R, Lynch J, et al. . 2022. Falling down the rabbit hole? Methodological, conceptual and policy issues in current health inequalities research. Crit Public Health. Published online 7 February 2022, 10.1080/09581596.2022.2036701. [DOI] [Google Scholar]
- 59.Kröger H, Pakpahan E, Hoffmann R. 2015. What causes health inequality? A systematic review on the relative importance of social causation and health selection. Eur J Public Health 25(6):951–960, PMID: , 10.1093/eurpub/ckv111. [DOI] [PubMed] [Google Scholar]
- 60.Kuh D, Ben-Shlomo Y, Lynch J, Hallqvist J, Power C. 2003. Life course epidemiology. J Epidemiol Community Health 57(10):778–783, PMID: , 10.1136/jech.57.10.778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Westreich D, Greenland S. 2013. The table 2 fallacy: presenting and interpreting confounder and modifier coefficients. Am J Epidemiol 177(4):292–298, PMID: , 10.1093/aje/kws412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Clouston SAP, Link BG. 2021. A retrospective on fundamental cause theory: state of the literature, and goals for the future. Annu Rev Sociol 47(1):131–156, PMID: , 10.1146/annurev-soc-090320-094912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Galea S, Freudenberg N, Vlahov D. 2006. A Framework for the Study of Urban Health. In: Cities and the Health of the Public. Freudenberg N, Galea S, Vlahov D, eds. Nashville, TN: Vanderbilt University Press, 3–18. [Google Scholar]
- 64.Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT. 2017. Structural racism and health inequities in the USA: evidence and interventions. Lancet 389(10077):1453–1463, PMID: , 10.1016/S0140-6736(17)30569-X. [DOI] [PubMed] [Google Scholar]
- 65.Krieger N. 2001. Theories for social epidemiology in the 21st century: an ecosocial perspective. Int J Epidemiol 30(4):668–677, PMID: , 10.1093/ije/30.4.668. [DOI] [PubMed] [Google Scholar]
- 66.Krieger N, Williams DR, Moss NE. 1997. Measuring social class in US public health research: concepts, methodologies, and guidelines. Annu Rev Public Health 18(1):341–378, PMID: , 10.1146/annurev.publhealth.18.1.341. [DOI] [PubMed] [Google Scholar]
- 67.Khalatbari-Soltani S, Maccora J, Blyth FM, Joannès C, Kelly-Irving M. 2022. Measuring education in the context of health inequalities. Int J Epidemiol 51(3):701–708, PMID: , 10.1093/ije/dyac058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Chandola T, Clarke P, Morris JN, Blane D. 2006. Pathways between education and health: a causal modelling approach. J R Stat Soc Ser A Stat Soc 169(2):337–359, 10.1111/j.1467-985X.2006.00411.x. [DOI] [Google Scholar]
- 69.Krieger N. 2004. Data, “race,” and politics: a commentary on the epidemiological significance of California’s Proposition 54. J Epidemiol Community Health 58(8):632–633, PMID: , 10.1136/jech.2003.018549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Krieger N. 2014. Discrimination and health inequities. Int J Health Serv 44(4):643–710, PMID: , 10.2190/HS.44.4.b. [DOI] [PubMed] [Google Scholar]
- 71.Townsend P. 1987. Deprivation. J Soc Policy 16(2):125–146, 10.1017/S0047279400020341. [DOI] [Google Scholar]
- 72.Krieger N. 1992. Overcoming the absence of socioeconomic data in medical records: validation and application of a census-based methodology. Am J Public Health 82(5):703–710, PMID: , 10.2105/ajph.82.5.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Lamy S, Molinié F, Daubisse-Marliac L, Cowppli-Bony A, Ayrault-Piault S, Fournier E, et al. . 2019. Using ecological socioeconomic position (SEP) measures to deal with sample bias introduced by incomplete individual-level measures: inequalities in breast cancer stage at diagnosis as an example. BMC Public Health 19(1):857, PMID: , 10.1186/s12889-019-7220-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Morris R, Carstairs V. 1991. Which deprivation? A comparison of selected deprivation indexes. J Public Health Med 13(4):318–326, PMID: , 10.1093/oxfordjournals.pubmed.a042650. [DOI] [PubMed] [Google Scholar]
- 75.Bryere J, Pornet C, Copin N, Launay L, Gusto G, Grosclaude P, et al. . 2017. Assessment of the ecological bias of seven aggregate social deprivation indices. BMC Public Health 17(1):86, PMID: , 10.1186/s12889-016-4007-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Sharp GC, Lawlor DA, Richardson SS. 2018. It’s the mother!: how assumptions about the causal primacy of maternal effects influence research on the developmental origins of health and disease. Soc Sci Med 213:20–27, PMID: , 10.1016/j.socscimed.2018.07.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Giroux É, Fayet Y, Serviant-Fine T. 2021. L’exposome: tensions entre holisme et réductionnisme. Med Sci (Paris) 37(8–9):774–778, PMID: , 10.1051/medsci/2021092. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.