

Abstract
Objectives Congress and Medicare have required real-time benefit tools (RTBT) to provide patient-specific medication price information during prescribing to decrease the cost of medications. We sought physicians' perspectives on how these tools might most effectively improve their selection of low-cost medication.
Methods We conducted 15 semi-structured interviews of physicians (6 oncologists, 1 endocrinologist, 4 rheumatologists, and 4 from internal medicine) and identified key themes across interviews during coding and analysis.
Results Although physicians saw value in real-time medication price information, they were wary of the complexity of obtaining specific information and the potential for inaccuracies. Physicians described how medication price information would be used in various prescribing scenarios including from simple substitutions (different drug formulations) to more complex decisions (different drug classes). In more complex situations, physicians were concerned that price information might only be available after discussing options with the patient, which would be too late to inform decisions. Concern about adding more information to the electronic health record was common.
Conclusion While most physicians saw value in implementation of RTBTs, they also expressed concerns related to the accuracy of information, the availability of information at the right time in the clinical workflow, and the most effective format for information. Many concerns raised paralleled the “Five Rights of Clinical Decision Support” framework and indicate the need for additional design work to achieve benefit from RTBTs. Beyond the public policy that has supported the availability of RTBTs, substantial development will be required to ensure that information is used to improve prescribing decisions.
Keywords: costs, clinical decision support, qualitative, providers
Background and Significance
High out-of-pocket prices for prescription drugs place a substantial financial burden on patients and are associated with low adherence to prescribed medications. 1 2 3 Because the out-of-pocket price of a given medication can depend on the specific coverage decisions made by an insured patient's pharmacy benefit plan, real-time, patient-specific information on out-of-pocket prices could inform a prescriber's choice of medication. 4 5 6 Towards that end, Congress has mandated that Medicare Part D drug sponsors provide real-time benefits information to electronic health records (EHRs) and that EHRs include real-time benefit tools (RTBTs) to provide patient-specific information on out-of-pocket prices for medications prescribed to Medicare beneficiaries. 7 A key focus of these efforts is on clinician-facing RTBTs that leverage interoperable exchange between pharmacy benefit managers' information systems and prescribers' EHRs. 8 9 10
Despite policymakers' and some clinicians' enthusiasm for sharing price information at the point of prescribing, 11 past evidence on the effect of displaying prices to clinicians has not demonstrated consistent benefit. 12 However, previous evaluations tested tools that presented clinicians with a medication's average price across payers (which may vary substantially from an individual patient's out-of-pocket price) or the medication's list price (which includes amounts paid by payers and patients and may also vary substantially from the patient's true out-of-pocket price). Efforts to estimate patient-specific out-of-pocket prices with greater precision may be more impactful than prior interventions. Yet, providing patient-specific information addresses only one barrier to effectively considering price in the prescribing process.
RTBTs can be considered a form of clinical decision support aimed at prescriber decision making. Achieving substantial benefit from clinical decision support tools has been challenging. Physicians report high levels of fatigue with clinical decision support tools and are often frustrated by systems they perceive are not effective. 13 14 15 Like all clinical decision support, effective implementation of RTBTs will depend on design decisions that match end users' needs, such as those described by the “Five Rights of Clinical Decision Support” framework. 16
Achieving value from RTBT is further complicated because patient-specific price information may also involve cost conversations and shared decision making between prescribers and patients to weigh the costs and benefits of different medications. Prior evidence indicates that these conversations often do not occur or are not effective. 17 18 Taken together, RTBTs face substantial obstacles to effectiveness: they must leverage accurate and usable interoperable information exchange between payers and providers, delivered to prescribers through effective clinical decision support, in the context of shared decision making. Preliminary evaluations of the impact of RTBTs on prescribing have shown that of 368,632 medication orders placed, only 512 medications were changed following use of the RTBT. 19
Objectives
Given the anticipated challenges to implementing RTBTs into practice, we conducted a series of semi-structured interviews with physicians to identify their views on implementation elements that might alter the impact of RTBTs.
Methods
Physician Interviews
We interviewed physicians from four select specialties guided by discussion with a study advisory committee. Those specialties were oncology, endocrinology, rheumatology, and internal medicine. We selected these first three specialties because they frequently prescribe high-cost medications and the latter because they are the most frequent prescriber of medications for patients, but the availability of relevant alternatives varies across specialties and therefore lends itself to identifying varied information needs. Physicians were identified and referred by members of a multidisciplinary advisory board convened for the parent study and were recruited by email and direct conversation. We contacted 59 physicians to request their participation in the study (7 from endocrinology, 18 from internal medicine, 21 from oncology, and 13 from rheumatology). We sent up to two reminder emails with outreach occurring between September and November 2020. Interviews were conducted by a trained moderator over Zoom, a videoconferencing platform, between October 24 and December 5, 2020, and lasted for approximately 60 minutes. The study was reviewed by the Vanderbilt University Medical Center Institutional Review Board.
Interviews followed an interview guide created following review of the prior literature on cost conversations and price display tools and input from the study advisory committee. Key themes and topic areas were developed from prior instruments, 18 20 21 22 23 refined for our specific setting, and extended when no prior instrument had addressed an important issue. Open-ended scripted questions were related to (1) importance of cost discussion; (2) discussion preparedness; (3) barriers and facilitators to cost conversation; (4) roles and responsibilities related to conversation; (5) influence on treatment decisions; and (6) perceived value of the proposed RTBT transparency tool. Follow-up questions were asked for clarity and to facilitate detailed discussion. Upon completion of the interviews, participants were compensated with a $100 Visa gift card. Physician interviews were audio-recorded, transcribed, and de-identified for analysis. Interviewers and study team members met to discuss themes and the content of interviews. The team determined that saturation had been reached based on redundancy in the content of new interviews. 24
Qualitative Analysis
Qualitative data coding was managed by the Vanderbilt University Qualitative Research Core, led by a PhD-level psychologist. Data coding and analysis adhered to the Consolidated Criteria for Reporting Qualitative Studies (COREQ) guidelines, 25 an evidence-based qualitative methodology. A hierarchical coding system was developed and refined using the moderator's guide and a preliminary review of the transcripts. Major categories included: cost communication; experience with cost conversations; barriers to conversation; current resources used for conversation; decision making; strategies and solutions for conversation; proposed RTBTs; workflow presentation; change over time; emotions; clarifying question; actual cost at pharmacy; and worth 15-minute appointment time. Major categories were further divided from one to nine subcategories, with subcategories having additional levels of hierarchical divisions. Definitions and rules were written for the use of coding categories.
Our interviews and coding focused primarily on patient out-of-pocket price (rather than total drug price, paid by both the patient and their insurer) since that was the primary focus of RTBTs and was of most concern to respondents. We did probe respondents on the difference between patient-specific and average out-of-pocket prices, since the average price would be a simpler alternative to estimate and has been previously evaluated. Physicians used a variety of related terms to refer to patient out-of-pocket prices (including coinsurance, deductibles, and co-pays). These were coded as referring to out-of-pocket prices generally and considered separately from infrequent reference to other types of price (such as those to society more broadly).
To establish reliability, three experienced qualitative coders independently coded two of the transcripts. Coding of each transcript was compared, and any discrepancies reconciled to create a single coded transcript. Each statement was treated as a separate quote and could be assigned up to 10 different codes. Transcripts were combined and sorted by code. Management of transcripts, quotations, and codes were done using Microsoft Excel 2016 and SPSS version 27.0.
Finally, coders and study team members reviewed the codes and coded transcripts to identify higher order themes and identified parallels between these themes and the Five Rights of Clinical Decision Support framework. 26 27 Specifically, we sought to characterize perspectives on the value of patient-specific prices relative to average prices; the additional information that would make price data most impactful; views on who should review price information; when in the clinical workflow price information should appear; and in what format and through which channels the information should be presented.
Results
In total, we conducted 15 individual interviews with physicians. Of these, 6 were oncologists, 1 endocrinologist, 4 rheumatologists, and 4 specialized in internal medicine.
Right Information (Themes 1–3)
The first “Right” included is “Right Information” described as information that is “evidence-based, suitable to guide action, and pertinent to the circumstance.” 16 We identified three themes that corresponded to the notion of providing the “Right Information.”
Theme 1: Physicians clearly preferred patient-specific out-of-pocket price information to average prices but were wary of incorrect price information.
Most interviewed physicians had a clear preference for patient-specific out-of-pocket price information over average out-of-pocket price. In particular, physicians were concerned that average prices may not be useful to distinguish between multiple expensive medications whose patient-specific cost may vary depending on the specifics of insurance coverage ( Table 1 ). However, physicians were also concerned about the complexity of obtaining accurate patient-specific price information and expected errors given variation in prices depending on the pharmacy where the patient filled the prescription, any changes to their coverage between the visit and filling their prescription (e.g. moving into the “donut hole”), and other variables (for example, see Table 1 —Theme 1). Some physicians suggested including a potential margin of error related to the patient-specific price, and indicated that a tool that was correct within 10 to 20% of the patient-specific price might be acceptable.
Table 1. Key themes and illustrative quotations from interviews.
| Theme 1: Physicians clearly preferred patient-specific price information to average prices but were wary of incorrect price information. |
| “You got to figure out how much the patient's already spent that year, and then what pharmacy prices are going to be for different pharmacies, mail order versus their local, and what the preferred drug is from the insurance company and why they won't let you use the drug, what it would take to get to the drug you want to use, what they have to say and what they have to have as a co-morbidity to generate that. So, if somebody can put all that together in a real sophisticated AI, sure. That's great. But anything else is just a waste of time.” (Participant 13, Rheumatology) |
| Theme 2: Physicians identified several different scenarios in which patient-specific prices might be used. |
| There's a big presumption here that all of these drugs are equally effective for the condition. I think that that is sometimes true, and I think when you're picking antibiotics is often true. [But] I think there are just not a ton of scenarios where this is true, that you truly feel like you can say any of these are options that I feel comfortable are all effective and I would recommend them all for therapy for this particular condition. (Participant 9, Oncology) |
| Theme 3: Physician engagement with the RTBT will be maximized if it provides actionable information. |
| “If you could actually have an alert… that was concise and practical and gave you the alternative…Well, that's pretty useful. I can click on that. It's when something pops up and says non-specifically, ‘Hey, this might be pretty expensive for this patient,’ and then you're saying, ‘Well, maybe it is. Now do I need to go do a lot more work?’ That's much less pragmatic in terms of getting me to be ready to take action. I'm not sure I articulated that well but...” (Participant 6, Internal Medicine) |
| Theme 4: Physicians identified multiple time points—most prominently during conversation with patient and during prescribing—when information should be displayed. |
| “The two places that you could embed this would be either just a resource that I know about that I can go to and say, “I'm just going to go to this website and type in apixaban it's going to tell me what the range might be.” And that I can do whenever I want. The other time would be to do it at the time that I'm ordering the medication to give me a warning.” (Participant 9, Oncology) |
| Theme 5: Physicians felt they were the right person to discuss price information, but sought team-based solutions to improve communication and reduce the burden. |
| “I think primarily I think it should be the physician. I think if there is support within the group of, sometimes group have a pharmacist, the AIDS patients I think a pharmacist could have a role, but we don't have that position at the VA.” (Participant 5, Rheumatology) |
| Theme 6: Physicians had conflicting opinions about the best format to display price information. |
| I first put in dabigatran, something pops up right away that says, “For this patient's insurance, this patient has a high-deductible, crummy copayment insurance plan, so they're going to charge him $400 for this...” In the ideal world, you would even say, “Here's a low-cost substitute. Would you like that instead?” (Participant 6, Internal Medicine) I think it's got to be easily accessible at the point of care. So, ideally linked within the electronic health record. Whether that be literally when you go to write a prescription or some type of resource that you can get to while you're in the medical record without trying to go elsewhere. (Participant 7, Internal Medicine) |
| Theme 7: Physicians viewed the EHR as the appropriate channel with some interest in an external “resource.” |
| It's like a busy screen. There's so much on there. I think probably when you go and prescribe a medicine, there's a link. In our system, when you go prescribe a medicine, there's a little link at the top of the prescription that has a knowledge link. And if you hover over it, you can pull up the dosing information, and the side effects, and when to modify doses for organ dysfunction. If there was a way to pull up cost information as you're prescribing, I think that would be really helpful. I don't think it's helpful to just have like every medicine a person is on and what the costs are somewhere. I think that's just overwhelming. (Participant 11, Oncology) |
Abbreviations: AIDS, acquired immune deficiency syndrome; EHR, electronic health record; RTBT, real-time benefit tool; VA, Veterans Affairs.
When asked specifically about the potential value of a tool that provided the average out-of-pocket price, a minority of interviewed clinicians indicated that they would prefer an average price over an exact price because they would not trust the patient-specific price provided. A consistent theme was that physicians generally expressed that the average out-of-pocket prices could help guide some discussions but were concerned that the price for patients might vary widely from the average.
Theme 2: Physicians identified several different scenarios in which patient-specific prices might be used.
Physicians were generally supportive of the need to consider medication prices when making prescribing decisions. However, they noted that the value of price information varied across clinical scenarios from largely determining choice to “nice to have.” This variation appeared to primarily be based on the availability of identical or similar alternative medications ( Table 1 —Theme 2 and Table 2 ). Four scenarios emerged in interviews: (1) simple substitutions where nearly identical medications were available but varied in price (e.g., tablet vs. capsule formulation of the same medication), such that price might determine choice; (2) somewhat more complex situations where multiple brand name medications were available with relatively similar effectiveness and side-effect profiles but prices varied based on patient-specific pharmacy benefit, where prices might be highly influential in prescribing choice; (3) more complex cases in which the only viable substitutes varied substantially in price and side-effect profile, so that price was one important consideration among others; and (4) situations in which there was no obvious alternative regardless of price but price information “would be nice to be able to anchor the discussion with the patient, to some extent, at least” (Participant 1, Oncology).
Table 2. Varied use cases of real-time benefit tool described by physicians.
| Illustrative quotation | |
|---|---|
| Similar brand-named medications | I will always advocate for my patients and go for the one that I think that is the most efficacious and safe. But if my estimation is that we have the same probability of having a good kind of success, I think that's when price plays an important role as I start the conversation. (Participant 5, Rheumatology) |
| Price differences by format | I told you about doxycycline. I had no idea that the capsule[s] were cheaper than the tablets. It would have never even occurred to me. If a pop up occurred in an electronic health record, of course I would be like there's absolutely no reason for me to give you a tablet. No value add from that. (Participant 7, Quality improvement) |
| Important considerations beyond price | And then there's the times when you have to actually think about a different class or change. Like if you were thinking about Coumadin instead of Adalat, that's obviously a totally different management plan. It's a different set of downsides. It's a level of inconvenience for the patient, and so that would be a bigger decision. So yeah, I think it would change. It would just give me greater transparency and probably make us more connected to the patient's experience. (Participant 14, Oncology) |
| No real alternative | The number of cases where there's multiple similar drugs that I can prescribe that seem equally effective is relatively small, like for cancer treatments. But even then, in other words, if I'm going to prescribe this drug called Tagrisso, at least having access to this information about Tagrisso would be nice to be able to anchor the discussion with the patient, to some extent, at least. (Participant 1, Oncology) |
Theme 3: Physician engagement with the RTBT will be maximized if it provides actionable information.
Participants repeatedly expressed the need for actionable information to allow quick changes to medications rather than requiring further research (see, for example, Table 1 —Theme 3). Most commonly, physicians indicated wanting an easy option to select alternative medications, with one physician noting that “These medicines all work the same, I'm going to choose the one that's $150 instead of $300, instead of just giving me the price, they could give me the alternative in the same category and their prices, that would be super helpful. (Participant 8, Internal Medicine).” Many physicians also expressed a preference for other medication information, such as common side effects, to be available near or alongside price information.
Right Time (Theme 4)
The second “Right” is “Right Time” described as information that is provided “at the right time in workflow.”
Theme 4: Physicians identified multiple time points—most prominently during conversation with patient and during prescribing—when information should be displayed.
Physicians identified multiple potential times during a patient encounter when medication price information may be most helpful, ranging from medication reconciliation to after the visit when a patient identifies a high price for a medication that was prescribed ( Fig. 1 ). Still, physicians focused on two primary times when price information would be most useful: during order entry, when it might be most immediately actionable; or just before or during discussion of medications, so that information could be incorporated into their discussion with the patient (see Table 1 —Theme 4). For example, one clinician described an ideal as “a comprehensive tool [that] answers all the questions immediately after you pick out the drug” during order entry (Participant 13, Rheumatology). Generally, clinicians favoring display during order entry highlighted the immediacy of the action and the potential ease of “operationalizing” such an out-of-pocket price check within the EHR. However, some physicians felt that a tool that presented prices during order entry would provide the information too late to inform discussion with the patient:
Fig. 1.
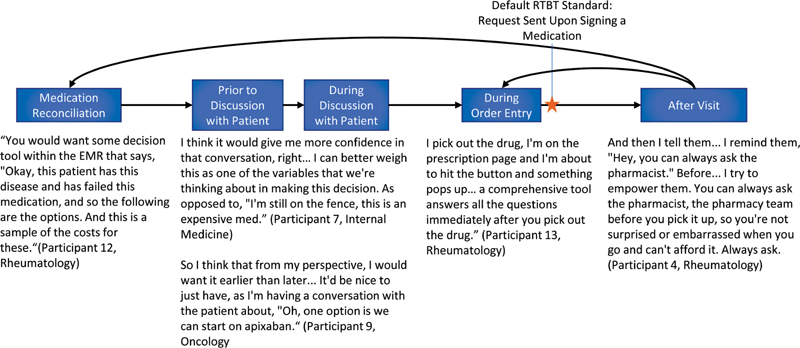
Physicians' views on when during a patient encounter medication price information may be most helpful.
If I have had all of those conversations and then I go to write the prescription for the medication, and then this pops up, it throws you off at that point, right? Because you've already gone through the whole conversation to now you're prescribing the medication. And now you're getting this pop up and you're going to now backtrack and say, “Okay, wait. I have a whole other piece of information for you. The medication that we just spent 20 minutes talking about, that you decided on, is five times the cost of the other one that we were just talking about.” (Participant 12, Rheumatology)
Right Person (Theme 5)
The third “Right” is “Right Person,” which considers information needs of “all members of the care team, including clinicians, patients, and their caregivers.”
Theme 5: Physicians felt they were the right person to discuss price information, but sought team-based solutions to improve communication and reduce burden.
Overall, physicians indicated that the primary responsibility for initiating and discussing costs was with the prescriber, with one respondent stating, “when we prescribe something, it's not just about effectiveness it's about, are they actually putting the pills in their mouths? You're not going to bankrupt them, right?” (Participant 7, Internal Medicine; see also Table 1 —Theme 5). Similarly, participants indicated that the physician or prescriber would be central to selecting alternative medications when changes were necessary due to price.
Nevertheless, physicians were also open to a team-based approach, noting important roles for medical assistants, nurses, clinical social workers, and, most prominently, pharmacists. Physicians noted that these roles might each be in a position to screen for or otherwise hear about price-related challenges and might therefore gather important information not raised during an office visit.
Physicians were also wary of the additional burden on them of discussing price. They described the potential value of specific individuals—such as pharmacists working within larger clinics—being assigned the responsibility to monitor patient-specific prices, but some indicated that no one played that role. For instance, one respondent stated “If we had unlimited resources, and I had a social worker in my clinic with me? Sure, that'd be great if the social worker would meet with the patient and find out what's going on with their lives. … but we don't have any of that stuff.” (Participant 13, Internal Medicine)
Right Format (Theme 6)
The fourth “Right” is “Right Format” described as information such as an “alert, order set, or reference information to answer a clinical question.”
Theme 6: Physicians had conflicting opinions about the best format to display price information.
Physicians described alternative strategies for displaying information within the EHR with no consensus on an optimal format to display price information (see Table 1 —Theme 6, for examples). Varied participants discussed the potential display of information directly in the EHR, use of pop-up alerts, buttons/links to information outside the EHR, icons within the EHR, and flags. Yet for each option, physicians were quick to point out downsides to each format, referencing “alert fatigue,” “flag fatigue,” the “busy” display of information within the EHR and the multitude of available tools each requiring “just two more clicks,” which in aggregate led to excessive interaction with the EHR.
Right Channel (Theme 7)
The fifth “Right” is “Right Channel” described as information such as an “electronic medical record, personal health record, or a more general channel such as the internet or a mobile device.”
Theme 7: Physicians viewed the EHR as the appropriate channel with some interest in external “educational resources.”
Participants were asked to provide input on the usefulness of a hypothetical RTBT within the context of an EHR system, and most clinicians focused on the use of an EHR-based tool within the context of an office visit. Some physicians expressed concerns about adding more information (or clutter) to the EHR (see Table 1 —Theme 7, for examples). A few respondents mentioned other potential channels. In a few cases, physicians referenced preferring an “educational resource”—likely a website—over a display within the EHR. They noted the ability to visit that resource as needed, and in some cases by launching it through the EHR. Two participants specifically referenced the value of a reference resource (UpToDate) used in other context. One respondent described patients potentially looking up price information independently and sharing that information via a “chat bot” or secure message.
Discussion
Interviews with physicians on the potential value and use of a RTBT highlighted both the high need for a tool that provides accurate patient-specific medication cost information to inform shared decision making and the prescribing process, and the challenges to maximizing the value of these tools. Our findings point toward the need for further research and development to identify ideal solutions and implementation strategies to ensure these tools meet the needs of patients and clinicians, especially as policymaking has mandated increasing support for such tools starting in 2021.
A clear consensus emerged about information needs related to medication prices: physicians revealed an interest in tools that provided patient-specific and accurate out-of-pocket price information. Physicians also desired tools that made follow-up action, such as selection of alternatives, simple. However, physicians were concerned about the accuracy of such a tool, the complexity in gathering relevant data, and the potential that a tool would provide information but not solutions.
Beyond the need for accurate, patient-specific price information, themes from interviews revealed a high degree of variation in how RTBTs should be designed and would be used rather than a single consensus. Physicians identified four different scenarios in which price information would be useful, ranging from simple differences in price by formulation with few other considerations to situations requiring complex trade-offs and shared decision-making. Physicians similarly described substantial variation related to when prices and price differences should be displayed: early in the visit, at the time of order entry, or following medication nonadherence. It is likely that the optimal time and format of RTBT depends on the specific trade-offs involved and the practice style of clinicians such that a one-sized-fits-all approach may not be effective.
The need to display price information prior to order entry creates a potentially complex technical challenge. Leading commercial RTBT suppliers, and the National Council for Prescription Drug Programs' standard, retrieve price information after sending orders to plans, during order entry. There is a good reason to do so as obtaining accurate prices requires information such as dose, formulation, days of supply, and specific information regarding the pharmacy where the patient will obtain their medication. Without this information, it would be challenging to compare the final prices to an individual patient. A crucial open question from our interviews is how to best design the tool to provide price information when it is most needed to inform shared decision-making. While this remains a challenge, interviews also provided some reason for hope: it is clear that the current workflow, in which prescribers often learn of high prices only when patients arrive at the pharmacy to fill their medication (if at all), is extremely inefficient, such that even nonoptimal implementation of an RTBT might be a major improvement.
Interview data revealed another important challenge to implementation of an RTBT. Although the EHR remains an enticing platform through which to drive change in the health care delivery system, physicians' frustrations with EHR-based solutions form a crucial barrier to adoption and use. Across interviews physicians repeatedly expressed concerns about “another” inaccurate or unhelpful tool and the time burden associated with its use. In consequence, the margin of error in design and implementation of new tools is narrow, with physician patience for additional popups, clicks, or even “busier” screens exhausted. This suggests the potential use of alternative forms of clinical decisions support. For instance, in the simplest discussed scenarios where price varied across formulation, intelligent defaults might be effective.
These challenges should be interpreted in the context of ongoing limitations related to engaging in cost conversations. A recent review highlighted that cost conversations about medications occur less often than patients desire, that limited knowledge of prices and limited time during encounters are two prime reasons physicians choose not to engage in cost conversations, and that cost conversations are less common for some patients (older patients and those of non-White race). 28 Taken together, the social context that these tools will be used in indicates a high bar for their design: efficiently presented, highly accurate price information that is available and actionable during cost conversations, especially in less resourced settings, is what is needed to effectively improve how medication prices are considered during prescribing.
Our study is subject to a number of limitations. First, our study leveraged qualitative methods to probe physicians' views on specific information resources and, while this approach allows for identification of themes through engagement with experienced respondents, it does not easily facilitate generalizable inference. However, because we received input from a range of physicians in a range of specialties, transferability to a broad set of physicians is likely. Relatedly, our interviews included a relatively small number of physicians from four specific specialties; we concluded recruitment as interviews resulted in redundant concepts indicating saturation. Nevertheless, because our study focused on a limited set of specialties, and intentionally focused on some specialties known to frequently prescribe high-priced medications, their responses may not reflect other specialties' perspectives or experience. Participants had varied experiences using information technology tools to review medication prices and in some cases were generally reporting on their perception of how they would use a hypothetical tool rather than speaking from experience using existing tools. This approach allowed for broader recruitment of participants and was likely necessary given the low adoption of RTBT and engagement with the tools when present.
Conclusion
Although physicians agreed on the potential benefit of patient-specific medication price information through an RTBT, they also identified crucial challenges related to the design and implementation of these tools and the varied circumstances in which they would be used. Turning policy that supports the development of RTBTs and provision of information into real patient benefit will require substantial innovation and a flexible approach to provide information at multiple points during care delivery and reflecting the underlying complexity of decision making under varied scenarios.
Clinical Relevance Statement
While the availability of RTBTs is increasing rapidly, how to most effectively use these tools is not clear. Clinicians and administrators should carefully consider the design and implementation of RTBTs to ensure that their implementation reflects the varied contexts of their use and that information is available when it is most valuable. Clinicians should consider how, when, and how to most effectively gather price information with these tools given their present practices.
Multiple Choice Questions
-
Which scenario did clinicians identify as the simplest to use real-time benefit information?
When prices varied by formulation
When prices varied by class
When no clear alternative existed
When available options had substantially different side-effect profiles
Correct Answer: The correct answer is option a. When prices varied by formulation. In this case, price was viewed as the only differentiating factor and picking the lowest price was a “no brainer.” When prices varied by class, decisions were often more complicated and involved more factors, similar to option d. When no clear alternatives existed, information was viewed as “nice to have” but difficult to make it useful.
-
At what time did physicians indicate information was needed to inform cost conversations when necessary?
At order entry
During the patient visit and before order entry
Before the patient visit
After the visit
Correct Answer: The correct answer is option b. Physicians indicated that when the selection of medication was not necessarily straightforward even with accurate price information, order entry would be too late to inform a useful cost conversation. The preference was to have that information available just as it was needed to inform a conversation leading to decision making.
Acknowledgement
The authors thank Sarah Henderson and Audrey Cheng for their research support. The authors thank Kemberlee R. Bonnet and the Qualitative Research Core at the Vanderbilt Institute for Clinical and Translational Research (VICTR) for facilitating focus groups and qualitative data coding. VICTR is sponsored by the National Center for Advancing Translational Sciences' Clinical Translational Science Award Program (5UL1TR002243-03).
Funding Statement
Funding This study was supported by Robert Wood Johnson Foundation.
Conflict of Interest T.J.M. reports grant support from the U.S. Food and Drug Administration, National Institute on Minority Health and Health Disparities, and PhRMA Foundation, and consulting fees from the Arnold Foundation and PhRMA unrelated to this work. S.D. reports grant support from Arnold Ventures, the Leukemia and Lymphoma Society, Commonwealth Fund, and National Cancer Institute, and receives honoraria from West Health and the Institute for Clinical and Economic Review. J.E. is currently an employee of the Office of the National Coordinator for Health Information Technology (ONC). This research was completed in his personal capacity. The opinions expressed in this article are the author's own and do not reflect the views of ONC, the Department of Health and Human Services, or the United States Government. S.D. serves on the Medicare Payment Advisory Commission. The views presented are those of the authors and do not reflect those of the commission.
Protection of Human and Animal Subjects
The study was performed in compliance with the World Medical Association Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects, and was reviewed by the Vanderbilt University Medical Center Institutional Review Board.
References
- 1.Zolnierek K BH, Dimatteo M R. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47(08):826–834. doi: 10.1097/MLR.0b013e31819a5acc. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Simpson S H, Eurich D T, Majumdar S R.A meta-analysis of the association between adherence to drug therapy and mortality BMJ 2006333(7557):15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Harrold L R, Briesacher B A, Peterson D. Cost-related medication nonadherence in older patients with rheumatoid arthritis. J Rheumatol. 2013;40(02):137–143. doi: 10.3899/jrheum.120441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sloan C E, Millo L, Gutterman S, Ubel P A. Accuracy of physician estimates of out-of-pocket costs for medication filling. JAMA Netw Open. 2021;4(11):e2133188–e2133188. doi: 10.1001/jamanetworkopen.2021.33188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sinaiko A D, Mehrotra A, Sood N. Cost-sharing obligations, high-deductible health plan growth, and shopping for health care: enrollees with skin in the game. JAMA Intern Med. 2016;176(03):395–397. doi: 10.1001/jamainternmed.2015.7554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Abaluck J, Gruber J. Evolving choice inconsistencies in choice of prescription drug insurance. Am Econ Rev. 2016;106(08):2145–2184. doi: 10.1257/aer.20130778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.42 USC §1395w-104(o) - Beneficiary protections for qualified prescription drug coverage
- 8.CMS. Medicare Advantage and Part D Drug Pricing Final Rule (CMS-4180-F). Accessed December 6, 2021 at:https://www.cms.gov/newsroom/fact-sheets/medicare-advantage-and-part-d-drug-pricing-final-rule-cms-4180-f
- 9.Federal Register. Medicare Program; Contract Year 2021 Policy and Technical Changes to the Medicare Advantage Program, Medicare Prescription Drug Benefit Program, and Medicare Cost Plan Program. Published June 2, 2020. Accessed December 6, 2021 at:https://www.federalregister.gov/documents/2020/06/02/2020-11342/medicare-program-contract-year-2021-policy-and-technical-changes-to-the-medicare-advantage-program
- 10.42 U.S. Code § 300jj - Definitions
- 11.Bhat S, Derington C G, Trinkley K E. Clinicians' values and preferences for medication adherence and cost clinical decision support in primary care: a qualitative study. Appl Clin Inform. 2020;11(03):405–414. doi: 10.1055/s-0040-1712467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mummadi S R, Mishra R. Effectiveness of provider price display in computerized physician order entry (CPOE) on healthcare quality: a systematic review. J Am Med Inform Assoc. 2018;25(09):1228–1239. doi: 10.1093/jamia/ocy076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.with the HITEC Investigators . Ancker J S, Edwards A, Nosal S, Hauser D, Mauer E, Kaushal R. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inform Decis Mak. 2017;17(01):36. doi: 10.1186/s12911-017-0430-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Page N, Baysari M T, Westbrook J I. A systematic review of the effectiveness of interruptive medication prescribing alerts in hospital CPOE systems to change prescriber behavior and improve patient safety. Int J Med Inform. 2017;105:22–30. doi: 10.1016/j.ijmedinf.2017.05.011. [DOI] [PubMed] [Google Scholar]
- 15.Menachemi N, Rahurkar S, Harle C A, Vest J R. The benefits of health information exchange: an updated systematic review. J Am Med Inform Assoc. 2018;25(09):1259–1265. doi: 10.1093/jamia/ocy035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sirajuddin A M, Osheroff J A, Sittig D F, Chuo J, Velasco F, Collins D A. Implementation pearls from a new guidebook on improving medication use and outcomes with clinical decision support. Effective CDS is essential for addressing healthcare performance improvement imperatives. J Healthc Inf Manag. 2009;23(04):38–45. [PMC free article] [PubMed] [Google Scholar]
- 17.Hunter W G, Hesson A, Davis J K. Patient-physician discussions about costs: definitions and impact on cost conversation incidence estimates. BMC Health Serv Res. 2016;16(01):108. doi: 10.1186/s12913-016-1353-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Alexander G C, Casalino L P, Meltzer D O. Patient-physician communication about out-of-pocket costs. JAMA. 2003;290(07):953–958. doi: 10.1001/jama.290.7.953. [DOI] [PubMed] [Google Scholar]
- 19.Davison A, Merrey J.NCPDP Foundation RTPB Grant: Final ReportAccessed September 30, 2022 at:http://ncpdpfoundation.org/pdf/NCPDPFoundationRTPBGrant_FinalReport.pdf
- 20.Patel M R, Wheeler J R. Physician-patient communication on cost and affordability in asthma care. Who wants to talk about it and who is actually doing it. Ann Am Thorac Soc. 2014;11(10):1538–1544. doi: 10.1513/AnnalsATS.201408-363OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Perez S L, Weissman A, Read S.US internists' perspectives on discussing cost of care with patients: structured interviews and a survey Ann Intern Med 2019170(9_Suppl):S39–S45. [DOI] [PubMed] [Google Scholar]
- 22.Tarn D M, Paterniti D A, Heritage J, Hays R D, Kravitz R L, Wenger N S. Physician communication about the cost and acquisition of newly prescribed medications. Am J Manag Care. 2006;12(11):657–664. [PubMed] [Google Scholar]
- 23.Carroll J K, Farah S, Fortuna R J.Addressing medication costs during primary care visits: a before–after study of team-based training Ann Intern Med 2019170(9_Suppl):S46–S53. [DOI] [PubMed] [Google Scholar]
- 24.Saunders B, Sim J, Kingstone T. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(04):1893–1907. doi: 10.1007/s11135-017-0574-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(06):349–357. doi: 10.1093/intqhc/mzm042. [DOI] [PubMed] [Google Scholar]
- 26.Campbell R.The five “rights” of clinical decision support J AHIMA 2013841042–47., quiz 48 [PubMed] [Google Scholar]
- 27.Digital Healthcare Research. Section 2 - Overview of CDS Five Rights. Accessed December 6, 2021 at:https://digital.ahrq.gov/ahrq-funded-projects/current-health-it-priorities/clinical-decision-support-cds/chapter-1-approaching-clinical-decision/section-2-overview-cds-five-rights
- 28.Everson J, Henderson S C, Cheng A, Senft N, Whitmore C, Dusetzina S B. Demand for and occurrence of medication cost conversations: a narrative review. Med Care Res Rev. 2022 doi: 10.1177/10775587221108042. [DOI] [PubMed] [Google Scholar]