

Abstract
COVID-19 symptoms can cause substantial disability, yet no therapy can currently reduce their frequency or duration. We conducted a double-blind placebo-controlled trial of hesperidin 1000 mg once daily for 14 days in 216 symptomatic nonvaccinated COVID-19 subjects. Thirteen symptoms were recorded after 3, 7, 10, and 14 days. The primary endpoint was the proportion of subjects with any of four cardinal (group A) symptoms: fever, cough, shortness of breath, or anosmia. At the baseline, symptoms in decreasing frequency were as follows: cough (53.2%), weakness (44.9%), headache (42.6%), pain (35.2%), sore throat (28.7%), runny nose (26.9%), chills (22.7%), shortness of breath (22.2%), anosmia (18.5%), fever (16.2%), diarrhea (6.9%), nausea/vomiting (6.5%), and irritability/confusion (3.2%). Group A symptoms in the placebo vs. hesperidin group were 88.8% vs. 88.5% (day 1) and reduced to 58.5 vs. 49.4% at day 14 (OR 0.69, 95% CI 0.38–1.27, p = 0.23). At day 14, 15 subjects in the placebo group and 28 in the hesperidin group failed to report their symptoms. In an attrition bias analysis imputing “no symptoms” to missing values, the hesperidin group showed reduction of 14.5% of group A symptoms from 50.9% to 36.4% (OR: 0.55, 0.32–0.96, p = 0.03). Anosmia, the most frequent persisting symptom (29.3%), was lowered by 7.3% to 25.3% in the hesperidin group vs. 32.6% in the placebo group (p = 0.29). The mean number of symptoms in the placebo and hesperidin groups was 5.10 (SD 2.26) vs. 5.48 (SD 2.35) (day 1) and 1.40 (SD 1.65) vs. 1.38 (SD 1.76) (day 14) (p = 0.92). In conclusion, most nonvaccinated COVID-19 infected subjects remain symptomatic after 14 days with anosmia being the most frequently persisting symptom. Hesperidin 1 g daily may help reduce group A symptoms. Earlier treatment of longer duration and/or higher dosage should be tested.
1. Introduction
Since the end of December 2019, the COVID-19 pandemic has led to important worldwide morbidity and mortality. Despite the success of vaccination, a substantial proportion of the world population are still awaiting immunization and therefore at risk of getting infected with the inherent risk of viral mutations that could lead to vaccine resistant strains of the virus. Most infected subjects report symptoms of varying severity that can become debilitating and persist for prolonged periods in a substantial proportion. Currently, no therapy has been shown to reduce the burden and length of COVID-19 symptoms in nonhospitalized subjects.
COVID-19 occurs due to an infection by a novel beta-coronavirus, identified as 2019-nCoV [1], now known as severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2), whose entry into cells has been shown to be dependent on angiotensin-converting enzyme 2 (ACE2) [2]. In a meta-analysis of 212 studies, Lie et al. [3] reported that the most common symptoms of COVID-19 were fever (78.8%), cough (53.9%), and malaise (37.9%). Other reported symptoms were fatigue (32.3%), expectoration (24.2%), myalgia (21.3%), shortness of breath (18.99%), chills (15.7%), diarrhea (9.5%), chest pain (9%), rhinorrhea (7.5%), vomiting (4.7%), and abdominal pain (4.5%). Furthermore, patients with a severe form of the disease were more subject to shortness of breath, abdominal pain, chills, and dizziness than patients with a nonsevere form. Studies also reported taste and smell dysfunction, such as anosmia, as a common symptom in people infected with COVID-19 [4, 5]. Some subjects at higher risk may show marked inflammation in response to the infection, referred to as the cytokine storm, leading to greater disease severity with acute respiratory distress and risk of hospital admission and death [6, 7]. The evolution of COVID-19 symptoms in nonhospitalized and nonvaccinated subjects during the third wave of the pandemic has not been reported. Compared to the first and second waves, large-scale PCR testing became available during the third wave and was largely publicised and encouraged in all possibly infected subjects. The true proportion and evolution of symptoms may therefore differ from what was reported in previously more selected populations.
Hesperidin, a flavonoid naturally present in the peel of citrus fruits, inhibits 3-chymotrypsin-like protease 3 (3CLpro) involved in SARS-CoV2 replication [8]. As well, hesperidin was reported to target the binding interface between the spike protein of SARS-CoV-2 and the ACE2 receptor, potentially preventing the interaction of ACE 2 with the spike regional binding domain (RBD) [9].
In vivo experimentation in rats infected with the H1N1 virus revealed that hesperidin effectively reduced lung impairment and suppressed pulmonary inflammation by reducing proinflammatory cytokines and recruitment of proinflammatory cells [10]. These anti-inflammatory and pulmonary protective effects were also reported in rats and mice with ventilator-induced and lipopolysaccharide-induced acute lung injury, respectively [11, 12]. Furthermore, evidence of cardioprotective and neuroprotective effects of flavanones, through their antioxidant and anti-inflammatory actions, was reviewed within the last decade and suggested the therapeutic potential of these compounds in conditions associated with inflammation and oxidative stress [13–15].
Considering its possible effects on SARS-CoV-2 entry into cells and replication, as well as its anti-inflammatory action and its effectiveness in animal models of acute respiratory distress, hesperidin may be of interest in the treatment of COVID-19-related symptoms and complications. This study was designed to determine the effects of 14 days hesperidin treatment on the burden of COVID-19 symptoms in nonhospitalized subjects.
2. Methods
2.1. Participants
This was a phase 2, randomized, double-blind, placebo-controlled study conducted at the Montreal Heart Institute (MHI) and compared the effects of hesperidin (1000 mg once daily) and placebo (ratio 1 : 1) on COVID-19 symptoms during 14 days in participants infected with COVID-19 (the detailed protocol is presented in S1 Protocol). Health Canada gave its authorization to conduct the study, which was also reviewed and approved by the Montreal Heart Institute Research and Ethics Committees (2021–2841). The study of hesperidin on COVID-19 symptoms (HESPERIDIN) was registered at clinicaltrials.gov (NCT04715932). A total of 216 subjects were recruited between February 18 and May 20, 2021, in the province of Quebec, Canada. All subjects were recruited by the Montreal Heart Institute research center, and the study was coordinated by the Montreal Health Innovations Coordinating Center (MHICC).
Nonhospitalized male and female subjects of at least 18 years of age with a positive diagnosis of COVID-19 confirmed by polymerase chain reaction (PCR) testing within the last 48 hours and with at least one COVID-19 symptom were included. Female participants had to be without childbearing potential (postmenopausal for at least one year or surgically sterile) or with childbearing potential and practicing at least one method of contraception. Subjects were excluded if they were currently hospitalized or under immediate consideration for hospitalization, currently in shock or with hemodynamic instability, or undergoing chemotherapy for cancer. Other exclusion criteria for participants were as follows: unable to take their oral temperature daily, having received at least one dose of the COVID-19 vaccine, pregnant (or considering becoming pregnant during the study) or breastfeeding women, taking anticoagulant or antiplatelet medications, bleeding disorders, and within 2 weeks of received or planned surgery. People with regular consumption of natural products containing more than 150 mg of hesperidin or regular consumption of more than one glass of orange juice per day were also excluded, as were subjects with known allergy to any of the medicinal and nonmedicinal ingredients of the study drug.
This was a no-contact study with screening, randomization, and follow-ups at day 3, 7, 10, and 14 performed exclusively by phone. All randomized subjects signed an electronic informed consent form using the DocuSign online service. The study medication and material were delivered to the patients' home and included an oral electronic thermometer (Physio logic© Acuflex Pro) and a daily symptom log. Allocation was performed through a randomization list generated by the MHICC (block sequence was fixed with a block size of 4) and provided to the MHI pharmacists who dispensed medication (hesperidin or placebo) according to the list after randomization of the participants by study coordinators, keeping participants, investigators, and staff blinded to drug assignment for the whole study duration. The symptoms log listed 13 COVID-19 symptoms including the temperature readings in degree Celsius. Participants were asked to take two capsules (500 mg each) of study medication once daily at bedtime on an empty stomach. They were requested to record their symptoms and temperature daily in the symptom log and return it to the study team at the end of their participation. At each follow-up call, the information recorded in the symptom log was captured in an electronic case report form (InForm V 6.0, Oracle Health Sciences) by the study team. The trial ended according to the protocol, namely, after last patient last visit. Hesperidin capsules and matching placebo were kindly provided by Valeo Pharma (Kirkland, Quebec, Canada).
2.2. Outcomes
The primary endpoint was the proportion of subjects with any of the following cardinal COVID-19 symptoms: fever, cough, shortness of breath, or anosmia at day 3, 7, 10, and 14. These symptoms are referred to as group A symptoms in the province of Quebec, Canada. The secondary endpoints were as follows: (1) the mean number of all COVID-19 symptoms (range 0–13) at day 3, 7, 10, and 14; (2) duration of COVID-19 symptoms, defined as the number of days between the first symptom and complete disappearance of any symptom; and (3) for each 13 COVID-19 symptoms listed in the symptom log (recent cough of aggravation of chronic cough, fever, chills, sore throat, runny nose, shortness of breath, nausea/vomiting, headache, general weakness, pain, irritability/confusion, diarrhea, and anosmia defined as sudden loss of smell), the proportion of subjects with the symptom at day 3, 7, 10, and 14. Fever was defined as a temperature of >38.0°C by oral temperature using the supplied electronic thermometer.
The study also included two exploratory endpoints: (1) for each COVID-19 listed in the symptom log, the proportion of subjects with the symptom on a daily basis and (2) composite of COVID-19-related hospitalization, mechanical ventilation, or death in 14 days following randomization.
The safety data were reviewed by a fully independent 3-member Data and Safety Monitoring Board (DSMB) after randomization of 50 subjects. Serious adverse events were reported to the DSMB on a weekly basis after their first meeting.
2.3. Statistical Analyses
Sample size was based on the proportion of subjects with any of the following group A COVID-19 symptoms: fever, cough, shortness of breath, or anosmia at day 7. We assumed that 50% of placebo subjects would be symptomatic at this time point. These symptoms, referred to as group A symptoms in Quebec, are among the most frequent COVID-19 symptoms and are more objectively assessable. These symptoms were used as a diagnostic criterion in the epidemiological definition of COVID-19 prior to the widespread use and availability of PCR testing. Using a two-sided 0.05 significance level, considering achieving 80% power to detect an absolute difference of 20% between both groups in the proportion of symptomatic participants, and factoring in a 15% drop out rate, we determined that 216 participants (108 per group) were required to complete the study.
Efficacy analyses were based on an intent-to-treat (ITT) principle. All participants who received medication were included in the ITT population. The primary analysis compared the proportion of subjects between both treatment groups using a generalized linear mixed model (GLMM), more precisely, a repeated binary logistic regression model with terms for the treatment group (placebo and hesperidin), time (3, 7, 10, and 14 days), and treatment group × time interaction. Contrasts under this model allowed for the comparisons of the proportions at each time point. Then, for secondary analyses, the number of COVID-19 symptoms was compared between treatment groups using another GLMM, namely, a repeated Poisson regression model with similar terms for the group, time, and interaction. Rate ratios are presented with 95% confidence intervals and p values. Duration of COVID-19 symptoms was compared using a log rank test with Kaplan–Meier curves. Subjects who still had at least one symptom at their last assessment were censored on the day of the last assessment. The statistical approach used for the primary endpoint was also used to compare individual COVID-19 symptoms over time. Composite of COVID-19-related hospitalization, mechanical ventilation, or death was compared between both groups using a chi-square test. Statistical analyses were described in a statistical analysis plan that was approved prior to database lock and unblinding.
Safety of hesperidin was evaluated with descriptive statistics on adverse events, and serious adverse events were broken down by groups and presented on the safety population of all subjects who took at least one dose of the study medication.
To account for a possible attrition bias and evaluate its impact, two post-hoc sensitivity analyses on the primary endpoint were conducted. Both imputed data in subjects who stopped reporting symptoms prior to day 14. The first analysis used the last observation which was carried forward as a worst-case scenario to impute missing symptoms, while the second imputed “no symptom” when symptoms were missing as a best-case scenario. All statistical tests were two-sided and conducted at the 0.05 significance level. Statistical analyses were performed using SAS version 9.4.
3. Results
The study flowchart is shown in Figure 1. A total of 217 subjects were enrolled, and there was one screen fail due to administration of the COVID-19 vaccine prior to randomization. A total of 216 subjects were randomized into the study group, with 109 were assigned to placebo and 107 were assigned to hesperidin. All participants who received placebo completed the study, but there was one who lost to follow-up in the hesperidin group.
Figure 1.
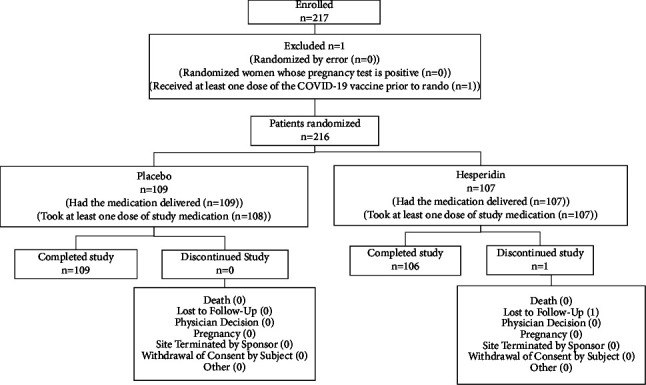
Study flowchart.
3.1. Baseline Characteristics (Table 1)
Table 1.
Patients' baseline characteristics, intent-to-treat population.
| Placebo N = 109 | Hesperidin N = 107 | All N = 216 | |
|---|---|---|---|
| Age (years) | 40.67 (SD 11.26) | 41.31 (SD 13.02) | 40.98 (SD 12.14) |
| Male | 49 (45.0%) | 48 (44.9%) | 97 (44.9%) |
| BMI (kg/m2) | 28.21 (SD 6.82) | 28.12 (SD 6.38) | 28.16 (SD 6.59) |
| Delay from symptoms to randomization (days) | 3.78 (SD 1.81) | 3.88 (SD 1.89) | 3.83 (SD 1.84) |
| Delay from diagnosis to randomization (days) | 1.10 (SD 0.43) | 1.10 (SD 0.39) | 1.10 (SD 0.41) |
| COVID-19 symptoms | |||
| Cough | 55 (50.5%) | 60 (56.1%) | 115 (53.2%) |
| General weakness | 49 (45.0%) | 48 (44.9%) | 97 (44.9%) |
| Headache | 45 (41.3%) | 47 (43.9%) | 92 (42.6%) |
| Pain | 39 (35.8%) | 37 (34.6%) | 76 (35.2%) |
| Sore throat | 28 (25.7%) | 34 (31.8%) | 62 (28.7%) |
| Runny nose | 24 (22.0%) | 34 (31.8%) | 58 (26.9%) |
| Chills | 21 (19.3%) | 28 (26.2%) | 49 (22.7%) |
| Shortness of breath | 20 (18.3%) | 28 (26.2%) | 48 (22.2%) |
| Anosmia | 20 (18.3%) | 20 (18.7%) | 40 (18.5%) |
| Fever | 17 (15.6%) | 18 (16.8%) | 35 (16.2%) |
| Diarrhea | 6 (5.5%) | 9 (8.4%) | 15 (6.9%) |
| Nausea/vomiting | 8 (7.3%) | 6 (5.6%) | 14 (6.5%) |
| Irritability/confusion | 5 (4.6%) | 2 (1.9%) | 7 (3.2%) |
| Risk factors | |||
| Diabetes | 1 (0.9%) | 6 (5.6%) | 7 (3.2%) |
| Hypertension | 9 (8.3%) | 14 (13.1%) | 23 (10.6%) |
| Heart diseases | 0 (0%) | 0 (0%) | 0 (0%) |
| Stroke | 0 (0%) | 0 (0%) | 0 (0%) |
| Respiratory diseases | 18 (16.5%) | 15 (14.0%) | 33 (15.3%) |
| Asthma | 17 | 14 | 31 |
| COPD | 1 | 0 | 1 |
| Pulmonary fibrosis | 0 | 1 | 1 |
Demographics as well as the clinical profile at randomization are shown in Table 1. For the whole study population, the mean age was 40.98 (SD 12.14) years with a proportion of males of 44.9%. The delay between the beginning of symptoms and randomization in the placebo group and the hesperidin group was similar at 3.78 (SD 1.81) and 3.88 (SD 1.89) days, respectively. The mean delay between COVID-19 diagnosis and randomization was 1.10 (SD 0.43) days in the placebo group and 1.10 (SD 0.39) days in the hesperidin group. The most common COVID-19 symptoms in decreasing frequency were as follows: cough (53.2%), general weakness (44.9%), headache (42.6%), pain (35.2%), sore throat (28.7%), runny nose (26.9%), chills (22.7%), shortness of breath (22.2%), anosmia (18.5%), fever (16.2%), diarrhea (6.9%), nausea/vomiting (6.5%), and irritability/confusion (3.2%). This was a low-risk population evidenced by the low prevalence of diabetes, hypertension, heart diseases, and respiratory diseases.
3.2. Primary Endpoint: Proportion of Participants with Group A Symptoms at Day 3, 7, 10, and 14 (Table 2)
Table 2.
Proportion of patients with group A COVID-19 symptoms, intent-to-treat population.
| Placebo | Hesperidin | All | OR (95% CI)a | p valuea | |
|---|---|---|---|---|---|
| Day 1 | N = 107 | N = 104 | N = 211 | ||
| No | 12 (11.2%) | 12 (11.5%) | 24 (11.4%) | ||
| Yesb | 95 (88.8%) | 92 (88.5%) | 187 (88.6%) | 0.97 (0.41; 2.28) | 0.9413 |
|
| |||||
| Day 3 | N = 103 | N = 102 | N = 205 | ||
| No | 13 (12.6%) | 9 (8.8%) | 22 (10.7%) | ||
| Yesb | 90 (87.4%) | 93 (91.2%) | 183 (89.3%) | 1.49 (0.60; 3.69) | 0.3849 |
|
| |||||
| Day 7 | N = 101 | N = 91 | N = 192 | ||
| No | 25 (24.8%) | 17 (18.7%) | 42 (21.9%) | ||
| Yesb | 76 (75.2%) | 74 (81.3%) | 150 (78.1%) | 1.43 (0.71; 2.88) | 0.3139 |
|
| |||||
| Day 10 | N = 99 | N = 90 | N = 189 | ||
| No | 39 (39.4%) | 32 (35.6%) | 71 (37.6%) | ||
| Yesb | 60 (60.6%) | 58 (64.4%) | 118 (62.4%) | 1.18 (0.65; 2.14) | 0.5886 |
|
| |||||
| Day 14 | N = 94 | N = 79 | N = 173 | ||
| No | 39 (41.5%) | 40 (50.6%) | 79 (45.7%) | ||
| Yesb | 55 (58.5%) | 39 (49.4%) | 94 (54.3%) | 0.69 (0.38; 1.27) | 0.2328 |
aComparison between the placebo group and hesperidin group. Significant when p < 0.05. bSubject has at least one of the group A COVID-19 symptoms: fever, cough, shortness of breath, or anosmia. N represents the number of subjects who completed the daily symptom diary.
The proportion of subjects presenting with any of the four selected group A symptoms (fever, cough, shortness of breath, and anosmia) in the hesperidin group compared to the placebo group was, respectively, 88.5% vs. 88.8% (day 1), 91.2% vs. 87.4% (day 3), 81.3% vs. 75.2% (day 7), 64.4% vs. 60.6% (day 10), and 49.4% vs. 58.5% (day 14). At 14 days, there was a 9.1% absolute reduction in group A symptoms in the hesperidin group (OR: 0.69, p=0.2328). There was progressive attrition in the number of participants that reported their symptoms between day 1 and day 14, with 15 missing in the placebo group and 28 in the hesperidin group. In the first post-hoc sensitivity analysis using the last observation carried forward imputation, there was also no statistically significant difference in the primary endpoint at each time point (S2 table). In this worst-case analysis, we still observed a reduction at day 14 in the hesperidin subjects from 59.3% to 52.3%, a 7.0% difference (OR 0.75, p=0.3098). In the second post-hoc sensitivity analysis imputing “no symptom” to any missing value (S2 table), the hesperidin group showed a statistically significant absolute reduction of 14.5% in group A symptoms from 50.9% to 36.4% (OR: 0.55, p=0.0343).
3.3. Effect of Hesperidin Treatment on the Number of COVID-19 Symptoms at Day 3, 7, 10, and 14
Figure 2 presents the effect of hesperidin on the number of COVID-19 symptoms at day 1, 3, 7, 10, and 14. Hesperidin did not improve the mean number of COVID-19 symptoms for the whole treatment duration: day 1 : 5.10 (SD 2.26) vs. 5.48 (SD 2.35), day 3 : 4.16 (SD 2.39) vs. 4.74 (SD 2.52), day 7 : 2.96 (SD 2.46) vs. 3.13 (SD 2.49), day 10 : 1.95 (SD 2.12) vs. (2.01 SD) 2.19, and day 14 : 1.40 (SD 1.65) vs. 1.38 (SD 1.76) in placebo vs. hesperidin group, respectively.
Figure 2.
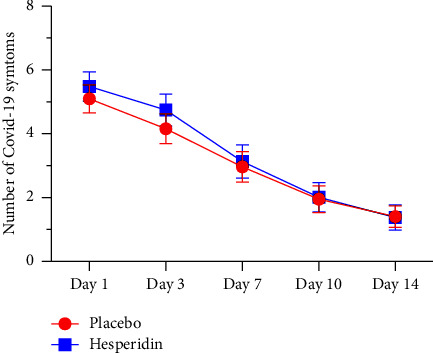
Mean number of COVID-19 symptoms at day 1, 3, 7, 10, and 14 in the placebo and the hesperidin groups. Values are presented as a mean with a 95% confidence interval.
3.4. Effect of Hesperidin Treatment on the Duration of COVID-19 Symptoms
The Kaplan–Meier curve showing the proportion of symptom-free subjects over 14 days is shown in Figure 3. Fourteen days after randomization, only 31.1% patients in the placebo group and 27.4% in the hesperidin group were symptom-free, indicating that the health of about 70% of our participants was still impacted by COVID-19 infection 14 days after study randomization and about 18 days after the beginning of symptoms. There was no difference in time to complete disappearance of symptoms between the two groups (p=0.8834). In subjects with complete disappearance of symptoms, the duration of all COVID-19 symptoms in the placebo group vs. the hesperidin group, defined as the number of days between randomization and complete disappearance of any symptom, was similar in both groups at 9.88 (SD 2.71) days with placebo vs. 10.34 (SD 3.15) days with hesperidin.
Figure 3.
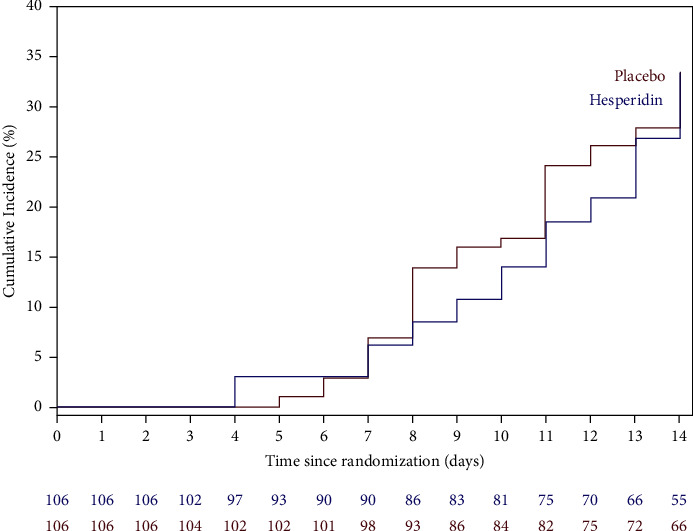
Kaplan–Meier curve. Proportion of symptom-free subjects over 14 days in the ITT population in the placebo and the hesperidin groups.
3.5. Effect of Hesperidin Therapy on the Proportion of Subjects with Each COVID-19 Symptom and on the Composite of Hospital Admission, Mechanical Ventilation, and Death
Figure 4 presents the proportion of subjects with each of the thirteen selected COVID-19 symptoms at day 1, 3, 7, 10, and 14. Detailed data and statistics for each symptom at each time point are presented in S3 tables. The four graphs in the top row of Figure 4 represent group A symptoms. The results showed that, except for fever which was absent at day 14 in the hesperidin group, each COVID-19 symptom was present at each time point in a certain proportion of patients that greatly vary depending on the symptom. For the whole duration of the study, the most prominent symptoms for their frequency and duration were cough and anosmia, two group A symptoms which affected 60.8% and 43.9% of participants at day 1 and persisted in 28.7% and 29.3% of them, respectively, at day 14. Some other symptoms such as runny nose, shortness of breath/difficulty breathing, headache, and general weakness were still present in more than 10% of the whole population at the end of the study. All other symptoms were markedly reduced with time and only affected a small proportion of patients at day 14. For each time point, hesperidin had no statistically significant impacts on the proportion of patients with each of these thirteen COVID-19 symptoms compared to the placebo group. Anosmia, the most frequently persisting symptom, was the only symptom to increase during the time course of the study as 54.1% of the whole study group was affected at day 3. At day 14, persisting anosmia was reduced by 7.3% in the hesperidin group (25.3%) compared to the placebo group (32.6%, OR 0.70 (0.36–1.37), p=0.2952).
Figure 4.
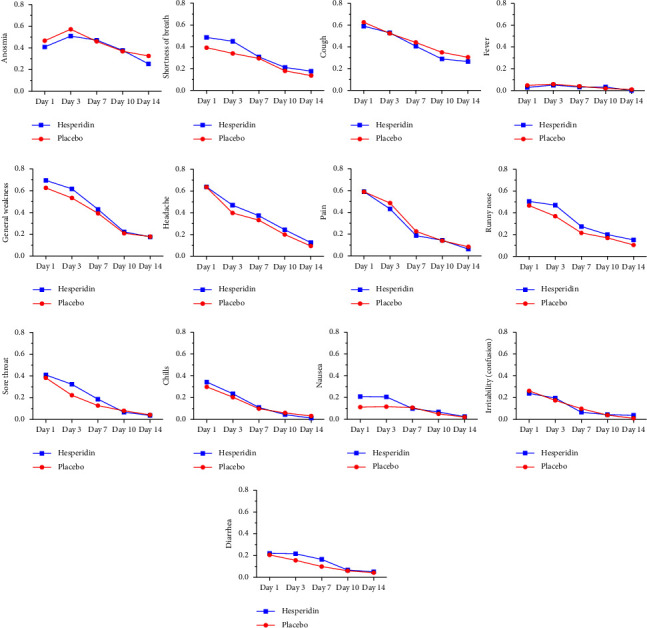
Proportion of subjects with each of thirteen COVID-19 symptoms at day 1, 3, 7, 10, and 14 in the placebo and the hesperidin groups.
The composite of COVID-19-related hospitalization, mechanical ventilation, or death in 14 days following randomization occurred in 1 subject in the placebo group and in 3 subjects in the hesperidin group (p=0.3669). One placebo subject was hospitalized for COVID-19 pneumonia that required intubation and ventilation. In the hesperidin group, two participants were hospitalized with pneumonia not requiring mechanical ventilation and one subject was hospitalized for pneumonia and dehydration. There was no death.
3.6. Safety Profile of Hesperidin
Treatment emergent adverse events (AEs) and treatment emergent serious adverse events (TESAEs) are presented in S4 Table. There were 16 adverse events in the placebo group and 23 in the hesperidin group. Two subjects experienced at least one severe AE in the placebo group and three subjects in the hesperidin group. AE possibly related to study treatment occurred in four placebo participants and in three hesperidin participants. The majority of AEs were related to COVID-19 infection. AE led to study drug withdrawal in five placebo subjects and eight hesperidin subjects. There was one TESAE in the placebo group and four in the hesperidin group, and none were related to study treatment.
4. Discussion
Commonly reported COVID-19 symptoms are cough, fever, malaise, and anosmia [3, 4]. More severe cases present an exaggerated inflammatory response, which is depicted as a cytokine storm that can lead to respiratory distress [6, 7]. Because SARS-CoV-2 is an evolutive virus with possible emergence of new variants that may not respond to current vaccines, it remains imperative to find treatments to reduce disease severity. Symptoms associated with COVID-19 in nonhospitalized subjects can be responsible for substantial disability, absenteeism, and loss of productivity [16]. During the first and second waves of the pandemic, availability of COVID-19 PCR diagnosis was limited and restricted to more symptomatic subjects, therefore introducing a selection bias in studies evaluating symptoms. During the recent third wave of the pandemic, PCR testing for COVID-19 has become widely available and testing has been strongly encouraged for all symptomatic subjects and contacts. There has been no prospective evaluation of COVID-19 symptoms in nonhospitalized and nonvaccinated subjects during the third wave. Here, we prospectively evaluated COVID-19 symptoms and the effects of 14-days hesperidin therapy, a flavonoid naturally present in citrus fruits, on 216 nonhospitalized and nonvaccinated symptomatic subjects who tested positive for COVID-19.
4.1. Frequency and Evolution of COVID-19 Symptoms during the Third Wave
Subjects in this trial were randomized a mean of 3.83 (SD 1.84) days after the beginning of symptoms and a mean of 1.10 (SD 0.41) days after PCR diagnosis and followed for 14 days. Therefore, at the end of the study, the participants were at about 18 days since the beginning of symptoms. At randomization, the most frequent symptoms, present in more than 1/3 of subjects, were cough, general weakness, headache, and pain. In 20%–30% of participants, the most common symptoms were sore throat, runny nose, chills, and shortness of breath. Anosmia was present in 18.5%, whereas fever was present in only 16.2%. Other symptoms, including diarrhea, nausea/vomiting, and irritability/confusion, were present in only a minority of patients in a proportion of less than 7% each. With the notable exception of anosmia, all symptoms steadily decreased in frequency with time as the mean number of symptoms went from 5.3 to 1.4 from day 1 to day 14. Still, most subjects, about 70%, remained symptomatic at day 14. The proportion of subjects with anosmia tripled from randomization to day 3 when it reached a proportion of 54.1%. At day 14, anosmia was the most frequent persisting symptom (29.3%). Considering the previous reports on the importance of persisting anosmia after COVID-19 and its impact on quality of life, our study confirms that anosmia occurs in about 50% of infected subjects and persists more than 14 days in 30%. Clearly, because of its clinical importance, new sudden onset anosmia represents the best objective symptomatic target for COVID-19 therapeutic studies.
The incidence of fever found in this study is much lower that what was previously reported early in the pandemic [17], but confirms later reports in non-hospitalized COVID-19 subjects that found comparable incidence [18]. Indeed, in 4066 outpatient adults with COVID-19 diagnosis and a mean age of 43, 10.3% patients reported fever [18]. This rate is similar to 16.2% found at randomization in our study as self-reported by participants. Our study further emphasizes on the discrepancy in self-reported fever and mandatory measured temperature since we provided subjects with a thermometer and required daily temperature measurements. Baseline temperature at randomization was inquired by the phone, while day 1 temperature was measured with the provided electronic thermometer and entered in the symptom log. Fever measured at day 1 in our study (defined as greater than 38.0 by an oral thermometer) was present in only 3.9% of subjects, yet 32% reported chills at day 1 in the symptom log. Our study therefore shows that objective fever is rare in most nonhospitalized COVID-19 subjects about 4 days after the beginning of symptoms.
4.2. Effects of Hesperidin Therapy on COVID-19 Symptoms
The primary endpoint of this trial was the proportion of subjects with any of 4 cardinal COVID-19 symptoms: fever, cough, shortness of breath, and new onset anosmia. In the province of Quebec, Canada, they were referred to as group A symptoms, being more frequent and considered more specific for COVID-19 diagnosis. These symptoms were used for epidemiological diagnosis of COVID-19 contacts when large-scale PCR testing was not available. Group A symptoms were present in 88.6% of patients at day 1 (88.8% placebo and 88.5% hesperidin) and persisted in 54.3% of patients at day 14. At day 14, hesperidin reduced group A symptoms by 8.9% from 58.5% in the placebo group to 49.4%, without reaching statistical significance (OR 0.69, p=0.23).
Despite repeated recalls by phones and emails, there was progressive attrition in the number of participants reporting symptoms, greater in the hesperidin group (28/107) than in the placebo group (15/109). To account and explore the extremes of a possible attrition bias, we performed a worst-case and best-case imputation analysis of missing values. In the worst-case analysis, we imputed the “last observation carried forward” approach, and symptomatic subjects were therefore considered symptomatic for all subsequent missing days. In the best-case analysis, we imputed the absence of symptoms to all missing values. In the worst-case analysis, we found no statistically significant difference in group A symptoms at all-time points but still observed a reduction at day 14 in the hesperidin group from 59.3% to 52.3%, a 7.0% difference (OR 0.75, p = 0.3098). In the best-case analysis, the difference at day 14 became significant with a reduction of 14.5% from 50.9% in the placebo group to 36.4% in the hesperidin group (OR 0.55, p = 0.0343). Although speculative, the reason for the greater attrition rate in the reporting of symptoms in the hesperidin group may be due to symptomatic improvement and decreased willingness to cooperate for the participants that felt better. The attrition rate increased with the study duration, a recognized factor of poorer compliance. Our study, powered to detect a 20% absolute difference in symptoms at day 7, did not find statistically significant differences between treatments. A smaller absolute reduction, especially for anosmia, could however be highly clinically significant. Based on the attrition bias analysis and a best-case scenario where noncompliant subjects have no symptom, we cannot exclude that hesperidin could have beneficial effects, and thus, further studies are encouraged. Because of its clinical importance, persistence, and more subjective evaluation, new onset anosmia should be a primary therapeutic target in COVID-19 therapeutic studies.
The rationale and interest for using hesperidin in the treatment and even in the prevention of COVID-19 have been highlighted by others, both for its antioxidant and anti-inflammatory properties, and for its ability to block the entry and replication of SARS-CoV-2 [19, 20]. The current phase 2 study does not close the chapter on hesperidin therapy for COVID-19 with a signal of possible benefits on selected symptoms driven by a reduction of anosmia. Furthermore, since we did not grade the severity of each symptom in the design of this trial, we cannot exclude a potential benefit of treatment on this important component. Besides the attrition bias discussed above, there are several limitations that need to be considered in the planning of future phase 3 studies: delay of treatment, dosing, duration of treatment, and follow-up. The mean delay of 3.83 SD 1.84 days before enrollment into the trial may certainly mitigate the benefits of therapy as it has been largely reported that viral load peaks at symptom onset and for a few days, which is concordant with the infectiousness profile of COVID-19 [21]. The optimal therapeutic dosage of hesperidin has not previously been reported in human subjects. Participants were asked to take 2 capsules of 500 mg each once daily, the maximal allowable daily dose by the Non-Prescription and Natural Health Products Directorate (NNHPD) of Canada. Higher dosage more than once a day may be necessary to obtain optimal therapeutic effects. Finally, the duration of therapy and follow-up may need to be longer to provide maximal benefits and better detect improvement of persisting symptoms, especially anosmia.
Our study showed good safety of hesperidin with no evidence for greater drug-related AE compared to placebo and no drug-related SAE. This concords with previous preclinical observations in Sprague-Dawley rats, with low observed adverse effects at a dosage of 1000 mg/kg in a subchronic oral toxicity study [22]. As well, human studies showed a safe profile of hesperidin at a dosage ranging from 500 mg daily for 3 weeks [23] to 800 mg daily for up to 4 weeks [24] in both men and women. Although we excluded pregnant women from the current study, the use of veinotonics containing hesperidin to treat hemorrhoids and varices in pregnant women appears safe with no increase in reported adverse outcomes [25]. Finally, the US Food and Drug Administration issued a Generally Recognized as Safe Notice (GRAS No. 796) in 2018 [26] for the use of orange extract with 85% hesperidin content as well as GRAS No. 901 [27] for glucosyl hesperidin to be used as additives in food and beverages. Collectively, these data support the use of higher dosage of hesperidin in future trials.
5. Conclusion
During the third wave of the COVID-19 pandemic, only 30% of initially symptomatic nonhospitalized and nonvaccinated subjects were asymptomatic about 18 days after symptom onset. Anosmia affected 50% of subjects and was the most frequently persisting symptom in 30%. Hesperidin therapy is safe and may help reduce a composite of selected COVID-19 symptoms including fever, cough, shortness of breath, and anosmia. Further trials with this agent are encouraged. This research has previously been published as a preprint [28].
Acknowledgments
The study was funded by the Montreal Heart Institute (https://www.fondationicm.org) through dedicated donations by the Ariane Riou and Réal Plourde Foundation, the Sandra and Alain Bouchard Foundation (https://www.fsab.ca), the Lise and Richard Fortin Foundation, and Jacques D'Amours and Ingenew Pharma Inc. (https://www.ingenewpharma.com). Valeo Pharma Inc. (https://www.valeopharma.com) also supported the study by providing the study drug and placebo free of charge. Ingenew Pharma Inc. played a vital role in the study design, decision to publish, and preparation of the manuscript.
Data Availability
All data are fully available without restriction upon request.
Disclosure
The other funders did not play any role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Supplementary Materials
S1 Protocol. Version 2.0 of the Hesperidin study protocol approved by the Montreal Heart Institute Research and Ethics Committees. S2 table. Proportion of patients with group A COVID-19 symptoms,attrition bias analysis. S3 table. Summary and statistical analysis for the presence of each 13 COVID-19 symptoms. S4 table. Overall summary of treatment emergent adverse events (TEAEs) and serious adverse events (TESAEs).
References
- 1.Zhu N., Zhang D., Wang W., et al. A novel coronavirus from patients with pneumonia in China, 2019. New England Journal of Medicine . 2020;382(8):727–733. doi: 10.1056/NEJMoa2001017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hoffmann M., Kleine-Weber H., Schroeder S., et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell . 2020;181(2):271–280. doi: 10.1016/j.cell.2020.02.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Li J., Huang D. Q., Zou B., et al. Epidemiology of COVID-19: a systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. Journal of Medical Virology . 2021;93(3):1449–1458. doi: 10.1002/jmv.26424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Beltran-Corbellini A., Chico-Garcia J. L., Martinez-Poles J., et al. Acute-onset smell and taste disorders in the context of COVID-19: a pilot multicentre polymerase chain reaction based case-control study. European Journal of Neurology . 2020;27(9):1738–1741. doi: 10.1111/ene.14273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Moein S. T., Hashemian S. M., Mansourafshar B., Khorram-Tousi A., Tabarsi P., Doty R. L. Smell dysfunction: a biomarker for COVID-19. International Forum of Allergy & Rhinology . 2020;10(8):944–950. doi: 10.1002/alr.22587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Huang C., Wang Y., Li X., et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet . 2020;395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liu F., Li L., Xu M., et al. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. Journal of Clinical Virology . 2020;127 doi: 10.1016/j.jcv.2020.104370.104370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lin C. W., Tsai F. J., Tsai C. H., et al. Anti-SARS coronavirus 3C-like protease effects of Isatis indigotica root and plant-derived phenolic compounds. Antiviral Research . 2005;68(1):36–42. doi: 10.1016/j.antiviral.2005.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wu C., Liu Y., Yang Y., et al. Analysis of therapeutic targets for SARS-CoV-2 and discovery of potential drugs by computational methods. Acta Pharmaceutica Sinica B . 2020;10(5):766–788. doi: 10.1016/j.apsb.2020.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ding Z., Sun G., Zhu Z. Hesperidin attenuates influenza A virus (H1N1) induced lung injury in rats through its anti-inflammatory effect. Antiviral Therapy . 2018;23(7):611–615. doi: 10.3851/IMP3235. [DOI] [PubMed] [Google Scholar]
- 11.Ma H., Feng X., Ding S. Hesperetin attenuates ventilator-induced acute lung injury through inhibition of NF-κB-mediated inflammation. European Journal of Pharmacology . 2015;769:333–341. doi: 10.1016/j.ejphar.2015.11.038. [DOI] [PubMed] [Google Scholar]
- 12.Ye J., Guan M., Lu Y., et al. Protective effects of hesperetin on lipopolysaccharide-induced acute lung injury by targeting MD2. European Journal of Pharmacology . 2019;852:151–158. doi: 10.1016/j.ejphar.2019.02.042. [DOI] [PubMed] [Google Scholar]
- 13.Hajialyani M., Hosein Farzaei M., Echeverria J., Nabavi S. M., Uriarte E., Sobarzo-Sanchez E. Hesperidin as a neuroprotective agent: a review of animal and clinical evidence. Molecules . 2019;24(3):p. 648. doi: 10.3390/molecules24030648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chanet A., Milenkovic D., Manach C., Mazur A., Morand C. Citrus flavanones: what is their role in cardiovascular protection? Journal of Agricultural and Food Chemistry . 2012;60(36):8809–8822. doi: 10.1021/jf300669s. [DOI] [PubMed] [Google Scholar]
- 15.Testai L., Calderone V. Nutraceutical value of citrus flavanones and their implications in cardiovascular disease. Nutrients . 2017;9(5):p. 502. doi: 10.3390/nu9050502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tenforde M. W., Kim S. S., Lindsell C. J., et al. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate health care systems network—United States, March–June 2020. Morbidity and Mortality Weekly Report . 2020;69(30):993–998. doi: 10.15585/mmwr.mm6930e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fu L., Wang B., Yuan T., et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: a systematic review and meta-analysis. Journal of Infection . 2020;80(6):656–665. doi: 10.1016/j.jinf.2020.03.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mizrahi B., Shilo S., Rossman H., et al. Longitudinal symptom dynamics of COVID-19 infection. Nature Communications . 2020;11(1):p. 6208. doi: 10.1038/s41467-020-20053-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bellavite P., Donzelli A. Hesperidin and SARS-CoV-2: new light on the healthy function of citrus fruits. Antioxidants . 2020;9(8):p. 742. doi: 10.3390/antiox9080742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Haggag Y. A., El-Ashmawy N. E., Okasha K. M. Is hesperidin essential for prophylaxis and treatment of COVID-19 infection? Medical Hypotheses . 2020;144 doi: 10.1016/j.mehy.2020.109957.109957 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.He X., Lau E. H. Y., Wu P., et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nature Medicine . 2020;26(5):672–675. doi: 10.1038/s41591-020-0869-5. [DOI] [PubMed] [Google Scholar]
- 22.Li Y., Kandhare A. D., Mukherjee A. A., Bodhankar S. L. Acute and sub-chronic oral toxicity studies of hesperidin isolated from orange peel extract in Sprague Dawley rats. Regulatory Toxicology and Pharmacology . 2019;105:77–85. doi: 10.1016/j.yrtph.2019.04.001. [DOI] [PubMed] [Google Scholar]
- 23.Rizza S., Muniyappa R., Iantorno M., et al. Citrus polyphenol hesperidin stimulates production of nitric oxide in endothelial cells while improving endothelial function and reducing inflammatory markers in patients with metabolic syndrome. Journal of Clinical Endocrinology and Metabolism . 2011;96(5):E782–E792. doi: 10.1210/jc.2010-2879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Demonty I., Lin Y., Zebregs Y. E. M. P., et al. The citrus flavonoids hesperidin and naringin do not affect serum cholesterol in moderately hypercholesterolemic men and women. Journal of Nutrition . 2010;140(9):1615–1620. doi: 10.3945/jn.110.124735. [DOI] [PubMed] [Google Scholar]
- 25.Lacroix I., Beau A. B., Hurault-Delarue C., et al. First epidemiological data for venotonics in pregnancy from the EFEMERIS database. Phlebology . 2016;31(5):344–348. doi: 10.1177/0268355515589679. [DOI] [PubMed] [Google Scholar]
- 26.Susan C. GRAS notice (GRN) no. 796 [internet] 2018. https://www.fda.gov/food/generally-recognized-safe-gras/gras-notice-inventory .
- 27.Dennis M. K. GRAS notice (GRN) no. 901 [internet] 2019. https://www.fda.gov/food/generally-recognized-safe-gras/gras-notice-inventory .
- 28.Dupuis J., Laurin P., Tardif J.-C., et al. Fourteen-days evolution of COVID-19 symptoms during the third wave in non-vaccinated subjects and effects of hesperidin therapy: a randomized, double-blinded, placebo-controlled study. medRxiv . 2021 doi: 10.1155/2022/3125662. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
S1 Protocol. Version 2.0 of the Hesperidin study protocol approved by the Montreal Heart Institute Research and Ethics Committees. S2 table. Proportion of patients with group A COVID-19 symptoms,attrition bias analysis. S3 table. Summary and statistical analysis for the presence of each 13 COVID-19 symptoms. S4 table. Overall summary of treatment emergent adverse events (TEAEs) and serious adverse events (TESAEs).
Data Availability Statement
All data are fully available without restriction upon request.