

Abstract
Nasal septal mucoceles are a rare occurance, and reports in the current literature are limited. We describe the case of a 73-year-old woman who developed a nasal septal mucocele several days after an episode of angioedema. The lesion was treated with 2 rounds of needle aspiration with antibiotics and the application of silastic splints. There was no recurrence after 1 month, though the patient developed a saddle nose deformity. She ultimately underwent reconstruction with a diced-cartilage dorsal augmentation graft with fibrin glue. We review the learning points of this case and summarize existing literature on this disease.
Keywords: nasal septum, mucocele, saddle nose, diced cartilage, dorsal augmentation, fibrin glue, rhinoplasty
Introduction
Mucoceles are benign, expansile, mucus-filled, epithelial-lined, cystic masses.1 Although common in the paranasal sinuses, mucoceles of the nasal septum are rare, with only 15 cases reported in the literature, and there are no previous descriptions of saddle nose deformity resulting from these lesions. We describe a nasal septal mucocele causing saddle nose deformity and discuss subsequent reconstruction with a diced-cartilage dorsal augmentation graft with fibrin glue. Written patient consent was obtained for photographs and publication. For a full timeline of the case, see Table 1 and Figure 1.
Table 1:
Relevant medical history and interventions
| 73-Year-Old Woman with Past Medical History of Hypertension, Raynaud’s Disease, and Hashimoto’s Thyroiditis, and No History of Nasal Surgery, Trauma, or Other Problems. | |||
| Date | Summaries from initial and follow-up visits | Diagnostic testing, including dates | Interventions |
| 8/13/19 | Presented with 1 wk of nasal swelling, paroxysmal nocturnal dyspnea, and nasal obstruction following angioedema episode. Examination notable for midvault distension and bilateral swelling of the anterior nasal septum. | Magnetic resonance imaging revealed nasal septal mucocele (8/23/19); fine needle aspiration biopsy demonstrated acute inflammation, no malignancy (8/13/19); culture of fluid grew Eikenella corrodens and Staphylococcus aureus (8/13/19). | Fine needle aspiration of 9.5 cc turbid yellow fluid. Full course of amoxicillin-clavulanate. |
| 9/04/19 | Followed up for recurrence of mass and symptoms. | N/A | Fine needle aspiration of 6 cc. Silastic splints placed bilaterally along septum. Full course of amoxicillin-clavulanate. |
| 9/21/19 | No recurrence of mucocele. | N/A | Silastic splints removed. |
| 2/27/20 | Patient noticed saddle nose deformity, elects to pursue nasal septal reconstruction. | N/A | Dorsal augmentation with bilateral auricular conchae cartilage graft and fibrin glue (8/24/20). |
| 9/03/20 | Excellent aesthetic outcome. No recurrence of mucocele. | N/A | N/A |
| 10/09/20 | Excellent auesthetic outcome. No recurrence of mucocele. | N/A | N/A |
| 3/08/21 | 1 mm depression appreciated at mid-dorsum. | N/A | N/A |
Figure 1:

Case timeline from presentation to clinical follow up.
Case Narrative
A 73-year-old woman presented with a week of nasal swelling, postnasal discharge, and nasal obstruction starting several days after an episode of angioedema. She was a nonsmoker, and her medical history was significant for hypertension, Raynaud’s disease, and Hashimoto’s thyroiditis. The patient had no history of nasal trauma or surgery of the nose. She was found to have bilateral swelling of the anterior nasal septum and distension of the midvault. Magnetic resonance imaging was consistent with a nasal septal mucocele (Figure 2). Turbid yellow fluid (9.5 mL) was aspirated from the lesion. Bacterial cultures yielded Eikenella corrodens and Staphylococcus aureus, for which she was treated with oral amoxicillin-clavulanate. Fine needle aspiration demonstrated acute inflammation and was negative for malignancy.
Figure 2:
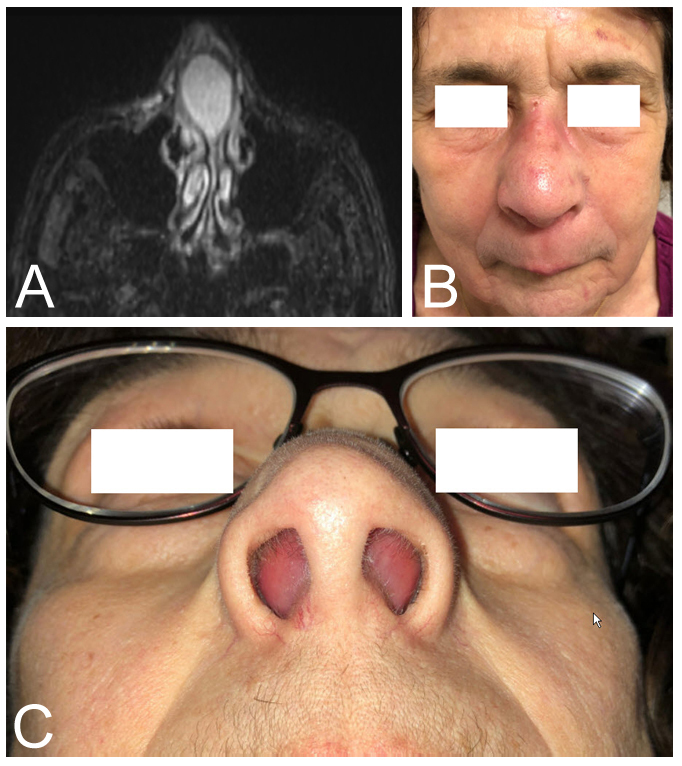
(A) Magnetic resonance imaging demonstrating a cystic mass of the anterior nasal septum. (B) Widening of the nasal midvault and tip. (C) Distension of the septal mucosa into the nasal vestibules bilaterally.
The patient then presented to the senior author (MT) a month later with recurrence of the mass. Fluid was again aspirated (6 mL), and silastic splints were placed along the septum bilaterally. She was given a course of amoxicillin-clavulanate, and the splints were removed 2 weeks later. No recurrence of the mucocele was noted after 1 month. However, at this point she was noted to have developed collapse of the nasal midvault. A year later, the decision was made to pursue dorsal augmentation to improve her saddle nose deformity.
In the operating room, an open rhinoplasty approach was performed without elevation of the septal mucoperichondrial flaps, in an effort to maintain separation between the area of prior mucocele and the soft-tissue envelope. The septum was noted to be destabilized and inferiorly displaced with intact attachments to the upper lateral cartilages. There was no evidence of septal perforation. Cartilage was harvested from bilateral auricular conchae, diced, and fashioned into a dorsal augmentation graft with fibrin glue. A cap graft of the same material was positioned over the nasal tip.
At follow-up 10 days and 1 month after surgery, the patient had an excellent aesthetic outcome and no evidence of recurrence of the mucocele. At 6-month follow-up, a 1 mm depression at the mid-dorsum could be appreciated (Figure 3). On palpation, the dorsal augmentation graft was otherwise intact and midline. The septum remained intact without evidence of perforation. The patient’s nasal obstruction symptom evaluation score was 10, indicating minimal symptoms.
Figure 3:

(A) Preoperative and postoperative lateral views at (B) 10 days and (C) 6 months, demonstrating reconstruction of saddle nose deformity. Slight depression of the mid-dorsum was appreciated at 6 months.
Discussion
Nasal septal mucoceles are rare, with only 15 cases described in the existing literature (Table 2). Only 2 of these prior patients were women, and all had resolution of symptoms. Most of these cases arose in the setting of prior nasal surgery or trauma, and only 3 idiopathic adult cases exist in the literature.2-4 Interestingly, our patient had no relevant nasal history, though she did present after an episode of angioedema. Though angioedema is known to affect the skin, oral cavity, and pharyngeal mucosa,5 nasal involvement would be an unusual manifestation. She also had a history of autoimmune disease but none that classically affect the nasal cavity, such as granulomatosis with polyangiitis or sarcoidosis.
Table 2:
Summary of existing literature on nasal septal mucoceles
| Reference | Age | Sex | History of trauma or surgery | Presentation | Treatment | Reconstruction | Resolution (follow-up) |
|---|---|---|---|---|---|---|---|
| Arrué et al 19986 | 36 | M | Facial trauma, 10 y ago | Nasal swelling | Endoscopic marsupialization | - | Yes |
| Gall et al 20027 | 62 | M | Septoplasty, 20 y ago | Nasal obstruction, pain, anosmia, headache | Endoscopic marsupialization | - | Yes |
| Hermann et al 20028 | 54 | F | Sinus surgeries, 9 and 15 y ago | Facial pain | Marsupialization | - | Yes |
| Lei et al 20042 | 37 | M | No | Nasal mass and pain | Endoscopic marsupialization | - | Yes (10 mo) |
| Yilmaz et al 20119 | 13 | M | No | Nasal obstruction | Endoscopic excision | - | Yes (6 mo) |
| Taskin et al 20123 | 45 | M | No | Nasal mass and pain | Endoscopic excision | - | Yes |
| Aynali et al 201310 | 34 | M | Rhinoplasty | Nasal obstruction, rhinorrhea | Endoscopic excision | - | Yes (6 mo) |
| Friedmann et al 201311 | 32 | M | Nasal fracture, 10 y ago | Nasal obstruction | Open excision via rhinoplasty approach and endoscopic marsupialization | - | Not stated |
| Liu et al 201412 | 37 | M | Nasal bone and Lefort, 2 fracture 9 y ago | External nasal swelling, nasal congestion, hyposmia | Open excision (gull wing) | Bony septum overlay | Yes |
| Lo Casto et al 201413 | 49 | M | Ogston-Luc procedure, 23 y ago | Nasal obstruction | Endoscopic marsupialization | - | Yes |
| Lee et al 20154 | 52 | F | No | Incidental on magnetic resonance imaging, asymptomatic | Marsupialization with microdebrider, no splints | - | Yes (16 mo) |
| Halawani et al 201614 | 20 | M | Inferior turbinectomy, 3 mo ago | Nasal obstruction, rhinorrhea, pain, headache | Endoscopic excision | - | Yes (6 mo) |
| Rawl et al 20191 | 57 | M | 3 septorhinoplasties, incision and drainage of septal hematoma, 35 y ago | Nasal obstruction | Endoscopic excision, splints for 3 wk | - | Yes (3 wk) |
| Ghorbani et al 201915 | 27 | M | Septoplasty and turbinoplasty, 5 y ago | Nasal obstruction, headache | Endoscopic marsupialization | - | Yes (2 y) |
| Fontes Lima et al 202016 | 49 | M | Maxillofacial trauma, 24 y ago | Nasal obstruction | Endoscopic marsupialization | - | Yes |
HA, headache.
Although saddle nose deformity in the setting of nasal septal mucocele has not previously been described, its occurrence is perhaps not surprising given destabilization of the nasal dorsum with this locally destructive process. Compared to other causes of saddle nose deformity such as syphilis, cocaine abuse, granulomatosis with polyangiitis, and relapsing chondritis, which are typically progressive, it is unclear if the natural history of saddle nose from a septal mucocele would follow a similar course. Given the stability of our patient’s examination for a year after development of the nasal deformity, our suspicion is that the area of inflammation at the anterior septum was likely replaced by mature fibrosis at that point. Numerous dorsal augmentation techniques involving both alloplastic materials and autologous tissues have been described to improve the contour of saddle or short noses.17-20 Diced cartilage grafts with fibrin glue are thought to provide lasting favorable outcomes in these cases.21 One challenge in our case was the development of a 1 mm depression at the mid-dorsum at 6 months which was not present immediately after surgery. This could be due to dorsal augmentation graft resorption, further destabilization of the septum at the midvault over time, or insufficient volume of the graft over the inferiorly displaced septum and upper lateral cartilages during surgery.
Conclusion
Nasal septal mucoceles can be successfully treated with needle aspiration and application of silastic splints. In cases that develop saddle nose deformity and require reconstruction, dorsal augmentation with diced cartilage and fibrin glue is an effective method for reconstruction, though caution should be taken with a destabilized septum.
Footnotes
Funding: None declared
Conflicts of Interest: None declared
Author Contributions: David W Chou, MD, provided substantial contributions to the study conception and design as well as acquisition, analysis, and interpretation of data, and drafted the article. Jacob E Hoerter, MD, provided substantial contributions to the acquisition, analysis, and interpretation of data for this work, and revised the article. Charles Shih, MD, provided substantial contributions to the study conception and design, and revised the work. Matthew Tamplen, MD, provided substantial contributions to the study conception and design, and revised the article. All co-authors agree to be accountable for all aspects of the work in ensuring its accuracy and integrity, and approve of this version to be published.
Presented at: This research was presented as a poster at the American Academy of Facial Plastic and Reconstructive Surgery Spring Meeting at Combined Otolaryngology Spring Meetings, April 9 and 10, 2021.
Consent: Informed consent was received from the case patient.
References
- 1.Rawl JW, Rossi NA, Chaaban MR, Brindley P. Intraseptal mucocele as A long-term complication of revision septorhinoplasty: A case report and review of A rare entity. Allergy Rhinol (Providence). 2019;10. 10.1177/2152656719845325 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lei L, Wang R, Han D. Pneumatization of perpendicular plate of the ethmoid bone and nasal septal mucocele. Acta Otolaryngol. 2004;124(2):221–222. 10.1080/00016480310015849 [DOI] [PubMed] [Google Scholar]
- 3.Taskin U, Korkut YA, Aydin S, Oktay FM. Atypical presentation of primary giant nasal septal mucopyocele. J Craniofac Surg. 2012;23(1):e5–7. 10.1097/SCS.0b013e3182420711 [DOI] [PubMed] [Google Scholar]
- 4.Lee DH, Lee JJW, Cho WS, Lim SC. Mucocele of the nasal septum: Case report and review of the literature. J Rhinol. 2015;22(2):112. 10.18787/jr.2015.22.2.112 [DOI] [Google Scholar]
- 5.Pfaue A, Schuler PJ, Mayer B, Hoffmann TK, Greve J, Hahn J. Clinical features of angioedema induced by renin-angiotensin-aldosterone system inhibition: A retrospective analysis of 84 patients. J Community Hosp Intern Med Perspect. 2019;9(6):453–459. 10.1080/20009666.2019.1698259 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Arrué P, Kany MT, Serrano E, et al. Mucoceles of the paranasal sinuses: Uncommon location. J Laryngol Otol. 1998;112(9):840–844. 10.1017/s0022215100141854 [DOI] [PubMed] [Google Scholar]
- 7.Gall R, Witterick I. Mucocele of the nasal septum. J Otolaryngol. 2002;31(4):246–247. 10.2310/7070.2002.21184 [DOI] [PubMed] [Google Scholar]
- 8.Hermann P, Jahnke K. Space-occupying lesion of the nasal septum in a patient with left-sided facial pain. Mucocele of the septum. HNO. 2002;50(6):570–571. 10.1007/s00106-001-0572-x [DOI] [PubMed] [Google Scholar]
- 9.Sinan Yilmaz M, Guven M, Dicle M. Nasal septal mucocele in A child: A rare presentation. Int J Pediatr Otorhinolaryngol Extra. 2011;6(4):414–415. 10.1016/j.pedex.2011.06.004 [DOI] [Google Scholar]
- 10.Aynali G, Sevrice M, Unal F, Dogan M, Unlu E, Yariktas M. A giant mucocele of nasal septum: Case report and literature review. Ann Clin Anal Med. 2013;4(Supplement 1):1–3. 10.4328/JCAM.1885 [DOI] [Google Scholar]
- 11.Friedmann DR, Roman B, Lebowitz RA, Bloom JD. Radiology quiz case 2. Diagnosis: Intraseptal mucocele. JAMA Otolaryngol Head Neck Surg. 2013;139(6):647–648. 10.1001/jamaoto.2013.3179a [DOI] [PubMed] [Google Scholar]
- 12.Liu Y-C, Chhabra N, Houser S, Jarchow A. A nasal mucocele originating from complex facial fractures. Am J Otolaryngol. 2014;35(2):233–235. 10.1016/j.amjoto.2013.05.005 [DOI] [PubMed] [Google Scholar]
- 13.Lo Casto A, Lorusso F, Lombardo F, Speciale R. Secondary septal mucocele diagnosed by MRI and CBCT and treated surgically. B-ENT. 2014;10(3):221–225. [PubMed] [Google Scholar]
- 14.Halawani RT, Banjar A. Mucocele of the nasal septum post inferior turbunectomy. Int J Otorhinolaryngol Head Neck Surg. 2016;2(2):102. 10.18203/issn.2454-5929.ijohns20160965 [DOI] [Google Scholar]
- 15.Ghorbani J, Doraghi K. Nasal septal mucocele, presenting as nasal midline mass. Ann Clin Case Rep. 2019;4:1610. [Google Scholar]
- 16.Fontes Lima A, Carvalho Moreira F, Azevedo C, Vilarinho S. Nasal septum mucocele in a patient with two other mucoceles of the paranasal sinuses: Late complications of maxillofacial trauma. RHINOL. 2020;3(3):152–156. 10.4193/RHINOL/20.055 [DOI] [Google Scholar]
- 17.Huang J, Liu Y. A modified technique of septal extension using a septal cartilage graft for short-nose rhinoplasty in Asians. Aesthetic Plast Surg. 2012;36(5):1028–1038. 10.1007/s00266-012-9945-7 [DOI] [PubMed] [Google Scholar]
- 18.Ezzat WH, Compton RA, Basa KC, Levi J. Reconstructive techniques for the saddle nose deformity in granulomatosis with polyangiitis: A systematic review. JAMA Otolaryngol Head Neck Surg. 2017;143(5):507–512. 10.1001/jamaoto.2016.3484 [DOI] [PubMed] [Google Scholar]
- 19.Emsen IM, Benlier E. Autogenous calvarial bone graft versus reconstruction with alloplastic material in treatment of saddle nose deformities: A two-center comparative study. J Craniofac Surg. 2008;19(2):466–475. 10.1097/SCS.0b013e3180690085 [DOI] [PubMed] [Google Scholar]
- 20.Min P, Wang Z, Zhang Z, Zhang Y, Pu Z. Septal reconstruction with folded porous polythylene implants: An alternative technique for the correction of severe saddle nose deformities in Asian populations. J Craniofac Surg. 2021;32(4):1325–1330. 10.1097/SCS.0000000000007260 [DOI] [PubMed] [Google Scholar]
- 21.Tasman A-J, Diener P-A, Litschel R. The diced cartilage glue graft for nasal augmentation. Morphometric evidence of longevity. JAMA Facial Plast Surg. 2013;15(2):86–94. 10.1001/2013.jamafacial.120 [DOI] [PubMed] [Google Scholar]