

Abstract
Background
Inhaled antibiotics are commonly used to treat persistent airway infection with Pseudomonas aeruginosa that contributes to lung damage in people with cystic fibrosis. Current guidelines recommend inhaled tobramycin for individuals with cystic fibrosis and persistent Pseudomonas aeruginosa infection who are aged six years or older. The aim is to reduce bacterial load in the lungs so as to reduce inflammation and deterioration of lung function. This is an update of a previously published review.
Objectives
To evaluate the effects of long‐term inhaled antibiotic therapy in people with cystic fibrosis on clinical outcomes (lung function, frequency of exacerbations and nutrition), quality of life and adverse events (including drug‐sensitivity reactions and survival).
Search methods
We searched the Cochrane Cystic Fibrosis Trials Register, compiled from electronic database searches and handsearching of journals and conference abstract books. We also searched ongoing trials registries.
Date of last search: 28 June 2022.
Selection criteria
We selected trials where people with cystic fibrosis received inhaled anti‐pseudomonal antibiotic treatment for at least three months, treatment allocation was randomised or quasi‐randomised, and there was a control group (either placebo, no placebo or another inhaled antibiotic).
Data collection and analysis
Two authors independently selected trials, judged the risk of bias, extracted data from these trials and judged the certainty of the evidence using the GRADE system.
Main results
The searches identified 410 citations to 125 trials; 18 trials (3042 participants aged between five and 45 years) met the inclusion criteria. Limited data were available for meta‐analyses due to the variability of trial design and reporting of results. A total of 11 trials (1130 participants) compared an inhaled antibiotic to placebo or usual treatment for a duration between three and 33 months. Five trials (1255 participants) compared different antibiotics, two trials (585 participants) compared different regimens of tobramycin and one trial (90 participants) compared intermittent tobramycin with continuous tobramycin alternating with aztreonam. One trial (18 participants) compared an antibiotic to placebo and also to a different antibiotic and so fell into both groups. The most commonly studied antibiotic was tobramycin which was studied in 12 trials.
Inhaled antibiotics compared to placebo
We found that inhaled antibiotics may improve lung function measured in a variety of ways (4 trials, 814 participants). Compared to placebo, inhaled antibiotics may also reduce the frequency of exacerbations (risk ratio (RR) 0.66, 95% confidence interval (CI) 0.47 to 0.93; 3 trials, 946 participants; low‐certainty evidence). Inhaled antibiotics may lead to fewer days off school or work (quality of life measure) (mean difference (MD) ‐5.30 days, 95% CI ‐8.59 to ‐2.01; 1 trial, 245 participants; low‐certainty evidence). There were insufficient data for us to be able to report an effect on nutritional outcomes and there was no effect on survival. There was no effect on antibiotic resistance seen in the two trials that were included in meta‐analyses. We are uncertain of the effect of the intervention on adverse events (very low‐certainty evidence), but tinnitus and voice alteration were the only events occurring more often in the inhaled antibiotics group. The overall certainty of evidence was deemed to be low for most outcomes due to risk of bias within the trials and imprecision due to low event rates.
Different antibiotics or regimens compared
Of the eight trials comparing different inhaled antibiotics or different antibiotic regimens, there was only one trial for each unique comparison. We found no differences between groups for any outcomes except for the following. Aztreonam lysine for inhalation probably improved forced expiratory volume at one second (FEV1) % predicted compared to tobramycin (MD ‐3.40%, 95% CI ‐6.63 to ‐0.17; 1 trial, 273 participants; moderate‐certainty evidence). However, the method of defining the endpoint was different to the remaining trials and the participants were exposed to tobramycin for a long period making interpretation of the results problematic. We found no differences in any measure of lung function in the remaining comparisons. Trials measured pulmonary exacerbations in different ways and showed no differences between groups except for aztreonam lysine probably leading to fewer people needing treatment with additional antibiotics than with tobramycin (RR 0.66, 95% CI 0.51 to 0.86; 1 trial, 273 participants; moderate‐certainty evidence); and there were fewer hospitalisations due to respiratory exacerbations with levofloxacin compared to tobramycin (RR 0.62, 95% CI 0.40 to 0.98; 1 trial, 282 participants; high‐certainty evidence). Important treatment‐related adverse events were not very common across comparisons, but were reported less often in the tobramycin group compared to both aztreonam lysine and colistimethate. We found the certainty of evidence for these comparisons to be directly related to the risk of bias within the individual trials and varied from low to high.
Authors' conclusions
Long‐term treatment with inhaled anti‐pseudomonal antibiotics probably improves lung function and reduces exacerbation rates, but pooled estimates of the level of benefit were very limited. The best evidence available is for inhaled tobramycin. More evidence from trials measuring similar outcomes in the same way is needed to determine a better measure of benefit. Longer‐term trials are needed to look at the effect of inhaled antibiotics on quality of life, survival and nutritional outcomes.
Plain language summary
Inhaling antibiotics to treat lung infection in people with cystic fibrosis
Review question
Are inhaled antibiotics helpful against persistent infection with Pseudomonas aeruginosa in people with cystic fibrosis (CF)?
Key messages
As people with CF get older, they are more likely to become infected on a long‐term basis with Pseudomonas aeruginosa. This is the most common cause of chronic lung infection in people with CF.
We wanted to find out whether antibiotics targeting Pseudomonas aeruginosa would reduce the effects of infection when they are breathed into the lungs. We wanted to learn whether this treatment would improve lung function, quality of life and survival. We also looked for any harmful effects.
What is CF?
Cystic fibrosis is an inherited disease which results in abnormal mucus in several parts of the body and mainly affects the lungs, which are susceptible to infection by certain bacteria. Infection causes inflammation which results in progressive damage to the lungs.
What did we find?
The review includes 18 trials with 3042 people with CF aged between five and 45 years of age. The trials lasted from three to 33 months. In 11 trials investigators compared inhaled antibiotics with a placebo (an inhaled substance without the medication in it) and people were selected for one treatment or the other randomly. Eight trials compared one inhaled antibiotic with either a different inhaled antibiotic or a different schedule of the same inhaled antibiotic. One of the trials compared an antibiotic both to placebo and to a different antibiotic and so fell into both groups.
Main results
Results from four trials showed that when compared to placebo, inhaled antibiotics may improve lung function and reduce the number of times the people with CF had a worsening of symptoms (exacerbation). Inhaled antibiotics may also mean fewer days off school or work (a measure of quality of life). They did not seem to have an effect on survival. We are not sure of the side effects of inhaled antibiotics, but tinnitus and changes in voice were reported more often in people inhaling antibiotics rather than the placebo. We did not find enough evidence to be able to comment on how inhaled antibiotics affect height and weight.
Where the trials compared different inhaled antibiotics or schedules, there was only one trial in each of the eight different comparisons. The only differences we found in all these comparisons were for two outcomes. In one trial we found that aztreonam lysine probably improved lung function more than tobramycin, but no important differences were found in the other trials with regard to lung function. Aztreonam lysine also probably led to fewer people needing additional courses of antibiotics than tobramycin and there were fewer hospitalisations after levofloxacin compared to placebo. We noted that important side effects that were related to the treatment were not very common in the trials, but they were less common with tobramycin than with other antibiotics.
What are the limitations of the evidence?
The trials that we included in this review measured lung function in different ways and also how often people experienced a sudden worsening of symptoms. That made it difficult for us to combine the results of different trials to strengthen our evidence. We thought the overall certainty of evidence was low for most outcomes, mainly due to risks of bias within the trials and low event rates meaning results were not precise.
How up to date is this evidence?
The evidence is current to: 28 June 2022.
Summary of findings
Summary of findings 1. Summary of findings: anti‐pseudomonal antibiotics versus placebo.
| Anti‐pseudomonal antibiotics compared with placebo for long‐term therapy in CF | ||||||
|
Patient population: adults and children with CF and P aeruginosa Settings: outpatients Intervention: inhaled anti‐pseudomonal antibiotics Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Inhaled anti‐pseudomonal antibiotics | |||||
|
FEV1 (% predicted) Follow‐up: at 3 months and up to 36 months |
4 trials found a significant improvement in FEV1 with inhaled antibiotics compared to placebo, although no data were available for 3 of these. 1 trial reported that the rate of decline in FEV1 favoured antibiotics. The remaining 6 trials showed no significant difference between inhaled antibiotics and placebo. |
NA | 1130 (11) | ⊕⊕⊝⊝
lowa |
The included trials all measured FEV1 but in different ways and for different lengths of time. It was not possible to combine the trials in a meta‐analysis. | |
|
FVC (% predicted) Follow‐up: at 3 months and up to 36 months |
5 of the 10 trials found significant changes in FVC at the end of the trial period, favouring inhaled antibiotics when compared to placebo. 1 trial found no significant difference in absolute values of FVC % predicted between inhaled antibiotics and control but found that mean change in FVC % predicted was significantly different (favouring antibiotics). 1 trial found a combination of gentamycin and carbenicillin versus placebo to be significantly different and favouring antibiotics yet ceftazidime versus placebo was not significantly different. 3 trials found no significant difference between antibiotics and placebo with regard to FVC % predicted. |
NA | 1097 (10) | ⊕⊕⊝⊝
lowa |
FVC was measured differently across the trials. | |
|
Pulmonary exacerbations: frequency of one or more hospital admissions Follow‐up: over 3 months and up to 12 months |
397 per 1000 | 262 per 1000 (187 to 369 per 1000) | RR 0.66 (0.47 to 0.93) | 946 (3) | ⊕⊕⊝⊝
lowa |
|
|
Quality of life: lost school or working days Follow‐up: over 3 months and up to 12 months |
The mean number of lost school or working days in the control group was 10 days. | The mean number of lost school or working days in the inhaled antibiotic group was 5.3 days lower (8.59 lower to 2.01 lower). | NA | 245 (1) | ⊕⊕⊝⊝
lowb,c |
|
|
Survival: number of deaths Follow‐up: over 3 months and up to 12 months |
17 per 1000 | 3 per 1000 (1 to 19 per 1000) | RR 0.17 (0.03 to 1.09) | 767 (2) | ⊕⊕⊝⊝ lowb,c | |
|
Antibiotic resistance: frequency of tobramycin‐resistant P aeruginosa Follow‐up: at end of trial (12 months) |
105 per 1000 | 205 per 1000 (90 to 464 per 1000) | RR 1.95 (0.86 to 4.42) | 672 (2) | ⊕⊕⊕⊝
moderateb |
|
|
Adverse events Follow‐up: at the end of the trial (84 days to 33 months) |
There were no significant differences between inhaled antibiotics and placebo for auditory impairment, pneumothorax, haemoptysis. Tinnitus and voice alteration were significantly more common in the inhaled antibiotics groups. |
NA | 1014 (6) |
⊕⊝⊝⊝ very lowa,c | Rate of auditory impairment reported in 5 trials for 996 participants. Rate of pneumothorax reported in 3 trials for 558 participants. Rate of haemoptysis reported in 1 trial for 520 participants. Rate of tinnitus reported in 1 trial for 520 participants. Rate of voice alteration reported in 2 trials for 701 participants. |
|
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CF: cystic fibrosis; CI: confidence interval; FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; P aeruginosa: Pseudomonas aeruginosa; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded twice due to most trials included in the comparison being at unclear or high risk of bias. 3 trials were at high or unclear risk of bias across all domains. All the 11 trials were at high or unclear risk of bias for randomisation or allocation concealment (or both) and also blinding of participants or outcome assessors (or both). bDowngraded once because of unclear risk of bias across some domains (randomisation or allocation concealment (or both) and blinding of participants or outcome assessment (or both)) of the included trials. cDowngraded once due to imprecision due to low event rates.
Summary of findings 2. Summary of findings: colistimethate dry powder for inhalation (Colobreathe®) versus tobramycin for inhalation solution.
| Colistimethate dry powder (Colobreathe®) compared with TISfor long‐term therapy in CF | ||||||
|
Patient population: children and adults with CF and P aeruginosa infection Settings: outpatients Intervention: colistimethate dry powder for inhalation (1 1.6625 MU capsule twice daily for 24 weeks) Comparison: TIS (3 cycles of 28 days of TIS (300 mg/5 mL) twice daily followed by a 28‐day off period) | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| TIS | Colistimethate dry powder for inhalation (Colobreathe®) | |||||
|
FEV1 (% predicted): mean change from baseline Follow‐up: 24 weeks |
Adjusted mean difference between the groups (ITT population LOCF) for the change in FEV1 % predicted, MD ‐0.98% (95% CI‐2.74% to 0.86%). There was no significant difference between the 2 groups for this outcome. |
NA | 374
(1) |
⊕⊕⊝⊝
lowa,b |
The data were not normally distributed and were analysed using log‐transformation analysis. We have reported the results directly from the paper. | |
|
FVC (% predicted): mean change from baseline Follow‐up: 24 weeks |
There was no significant difference between groups for FVC % predicted in the ITT population (LOCF), MD 0.01 L (95% CI ‐0.09 to 0.10). |
NA | 374 (1) |
⊕⊕⊝⊝
lowa,b |
The data were not normally distributed and were analysed using log‐transformation analysis. We have reported the results directly from the paper. | |
|
Pulmonary exacerbations: number of pulmonary exacerbations Follow‐up: 24 weeks |
262 per 1000 | 312 per 1000 (225 to 430 per 1000) | RR 1.19 (0.86 to 1.64) | 374 (1) | ⊕⊕⊕⊝
moderatea |
|
|
Quality of life: adjusted mean change in CFQ‐R score at the end of treatment Follow‐up: 24 weeks |
The adjusted mean changes at the end of the trial favoured the Colobreathe® group in terms of treatment burden (P = 0.091). This difference was significant at Week 4 (P < 0.001). |
NA | 374 (1) | ⊕⊕⊝⊝
lowa,c |
The trial was not powered to detect differences in overall quality of life. Results reported directly from paper. |
|
|
Survival: number of deaths Follow‐up: over 3 months and up to 12 months |
10 per 1000 | 2 per 1000 (0 to 43 per 1000) | RR 0.21 (0.01 to 4.32) | 374 (1) | ⊕⊕⊝⊝
lowa,d |
|
|
Antibiotic resistance: change in mean MIC50 and MIC90 at the end of the trial Follow‐up: 24 weeks |
The mean MIC50 (breakpoint of ≥ 8 mg/L) changed in the TIS group by 0.5 compared to 0.0 in the Colobreathe® group. The mean MIC90 (breakpoint of ≥ 8 mg/L) changed in the both groups by 4.0. |
NA | 374 (1) |
⊕⊕⊝⊝ lowa,c | ||
|
Adverse events: number of treatment related adverse events Follow‐up: 24 weeks |
466 per 1000 | 820 per 1000 (699 to 969 per 1000) |
RR 1.76 (1.50 to 2.08) |
379 (1) | ⊕⊕⊝⊝ lowa,d | Treatment‐related adverse events were significantly lower in the TIS group than the Colobreathe® group P < 0.0001. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CF: cystic fibrosis; CI: confidence interval; FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; ITT: intention‐to‐treat; LOCF: last observation carried forward; MIC: minimum inhibitory concentration; P aeruginosa: Pseudomonas aeruginosa; RR: risk ratio; TIS: tobramycin for inhalation solution. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded once due to an unclear or high risk of bias across 4 out of the 7 domains, particularly randomisation, allocation concealment and participant blinding. bDowngraded once due to LOCF analysis increasing risk of bias. cDowngraded once for imprecision; the trial was underpowered to detect differences in overall quality of life. dDowngraded once for imprecision due to low event rates.
Summary of findings 3. Summary of findings: inhaled TOBI® (IV preparation) versus tobramycin for inhalation solution.
| Inhaled TOBI® (IV preparation) compared with TIS for long‐term therapy in CF | ||||||
|
Patient population: adults and children with CF and P aeruginosa Settings: outpatients Intervention: inhaled tobramycin (TOBI®) (IV preparation) continuous twice‐daily 80 mg Comparison: TIS intermittent (4‐weekly on‐off cycles) twice‐daily 300 mg/5 mL | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| TIS intermittent | Inhaled tobramycin (IV preparation) continuous | |||||
|
FEV1 (% predicted): change from baseline Follow‐up: the end of the first treatment phase (12 weeks) |
The change from baseline in FEV1 % predicted was on average 1.07% less in the TIS group than in the inhaled tobramycin (IV preparation) group, values ranged from 11.20% less to 9.06% higher. |
NA | 32 (1) | ⊕⊝⊝⊝
very lowa,b |
Trial investigators provided individual participant data for lung function and we have analysed the first‐period data ourselves using the generic inverse variance method in RevMan. | |
|
FVC (% predicted): change from baseline Follow‐up: the end of the first treatment phase (12 weeks) |
The change from baseline in FVC % predicted was on average 0.01% more in the TIS group than in the inhaled tobramycin (IV preparation) group, values ranged from 9.48% less to 9.50% higher. | NA | 32 (1) | ⊕⊝⊝⊝
very lowa,b |
Trial investigators provided individual participant data for lung function and we have analysed the first‐period data ourselves using the generic inverse variance method in RevMan. | |
|
Pulmonary exacerbations Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Quality of life Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Survival Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Antibiotic resistance Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Adverse events Follow‐up: NA |
Outcome not reported. | NA | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CF: cystic fibrosis; CI: confidence interval; FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; IV: intravenous; NA: not applicable; P aeruginosa: Pseudomonas aeruginosa;TIS: tobramycin for inhalation solution. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded twice due to risk of bias being unclear or high across all the domains. The trial was at risk due to lack of blinding of participants or outcome measurement. This was because of the interventions being significantly different making it impossible to blind. Some outcomes (sputum bacteriology and oxygen saturation) were listed in the methods but not reported in the results. bDowngraded once due to imprecision. The sample size was small as only the first arm of a cross‐over trial was used.
Summary of findings 4. Summary of findings: tobramycin for inhalation powder versus tobramycin for inhalation solution.
| TIP compared with TIS for long‐term therapy in CF | ||||||
|
Patient population: children and adults with CF and P aeruginosa Settings: outpatients Intervention: TIP twice‐daily 4 capsules (total of 112 mg) (3 cycles (28 days on‐drug, 28 days off‐drug)) Comparison: TIS twice‐daily 300 mg/5 mL | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| TIS | TIP | |||||
|
FEV1 (% predicted): relative change from baseline Follow‐up: 24 weeks |
The MD between the 2 groups was 1.10 (95% CI ‐2.33 to 4.53) favouring TIS, but not significantly. |
NA | 517 (1) | ⊕⊕⊕⊝
moderatea |
TIP was found to be non‐inferior to TIS. | |
|
FVC Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Pulmonary exacerbations: number of participants experiencing pulmonary exacerbation Follow‐up: 24 weeks |
301 per 1000 |
337 per 1000 (259 to 436 per 1000) |
RR 1.12 (0.86 to 1.45) | 517 (1) | ⊕⊕⊕⊝
moderatea |
|
|
Quality of life Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Survival: number of deaths Follow‐up: 24 weeks |
Not calculable as there were no deaths in the TIS group. There were 3 deaths in the TIP group. |
RR4.76 (0.25 to 91.62) | 517 (1) | ⊕⊕⊝⊝
lowa,b |
||
|
Antibiotic resistance: mean change from baseline in P aeruginosa sputum density Follow‐up: 24 weeks |
Mucoid and non‐mucoid P aeruginosa sputum densities showed a decrease from baseline in both groups at all time points. Mean change was ‐1.6 versus ‐0.92 log10 CFU/g for mucoid phenotype and ‐1.77 versus ‐0.73 log10 CFU/g for non‐mucoid phenotype. |
NA | 517 (1) |
⊕⊕⊕⊝ moderatea | ||
|
Adverse events: number of any adverse event reported Follow‐up: 24 weeks |
842 per 1000 | 901 per 1000 (842 to 968 per 1000) |
RR 1.07 (1.00 to 1.15) |
517 (1) | ⊕⊕⊕⊝
moderatea |
A range of adverse events were reported but the only adverse events which were significantly different between the 2 groups were favouring TIS
|
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CF: cystic fibrosis; CFU: colony forming units; CI: confidence interval; FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; MD: mean difference; NA: not applicable; P aeruginosa: Pseudomonas aeruginosa; RR: risk ratio; TIP: tobramycin inhalation powder TIS: tobramycin for inhalation solution. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded once due to risk of bias within the trial. This was an open‐label trial and so was at high risk of bias for blinding and had an unclear risk for randomisation and allocation concealment. bDowngraded once for imprecision due to low event rates.
Summary of findings 5. Summary of findings: aztreonam lysine for inhalation versus tobramycin for inhalation solution.
| AZLI compared with TIS for long‐term therapy in CF | ||||||
|
Patient population: children and adults with CF and P aeruginosa Settings: outpatients Intervention: AZLI 75 mg 3 times daily Comparison: TIS 300 mg twice‐daily | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| TIS | AZLI | |||||
|
FEV1 (% predicted): mean relative change from baseline averaged across 3 cycles Follow‐up: 24 weeks |
The MD between groups was ‐3.40 (95% CI ‐6.63 to ‐0.17), favouring AZLI. |
NA | 268 (1) | ⊕⊕⊕⊝
moderatea |
||
|
FVC Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Pulmonary exacerbations: need for additional antibiotics Follow‐up: 24 weeks |
576 per 1000 | 380 per 1000 (294 to 495 per 1000) |
RR 0.66 (0.51 to 0.86) |
268 (1) | ⊕⊕⊕⊝
moderatea |
|
|
Quality of life: mean change from baseline in CFQ‐R respiratory symptom scale averaged across 3 cycles Follow‐up: 24 weeks |
The mean (SD) change in CFQ‐R score was 2.2 (17.7) in the TIS group. | The mean change in CFQ‐R score in the AZLI group was 4.10 points higher (0.06 points lower to 8.26 points higher). | NA | 268 (1) | ⊕⊕⊕⊝
moderatea |
|
|
Survival Follow‐up: 24 weeks |
See comments. | 268 (1) | ⊕⊕⊝⊝ lowa,b | 2 participants died during the trial, but neither were related to treatment and the treatment group was not specified. | ||
|
Antibiotic resistance: change from baseline in P aeruginosa CFU/g of sputum at week 24 Follow‐up: 24 weeks |
The mean (SD) change in log10 CFU/g was ‐0.32 (1.87) in the TIS group. | The mean change in log10 CFU/g in the AZLI group was 0.23 lower (0.76 lower to 0.3 log10 CFU/g higher). | NA | 268 (1) | ⊕⊕⊕⊝
moderatea |
|
|
Adverse events: number of treatment‐related adverse events Follow‐up: 24 weeks |
129 per 1000 | 228 per 1000 (133 to 392 per 1000) | RR 1.77 (1.03 to 3.04) | 268 (1) | ⊕⊕⊕⊝
moderatea |
Whilst treatment‐related events were significantly more likely in the AZLI‐treated group P < 0.04), the difference in serious adverse events (also more likely in the AZLI group) did not quite reach significance. No significant difference was reported for any other reported adverse event. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). AZLI: aztreonam lysine for inhalation; CFQ‐R: cystic fibrosis questionnaire ‐ revised; CF: cystic fibrosis; CFU: colony forming units; CI: confidence interval; FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; MD: mean difference; NA: not applicable; P aeruginosa: Pseudomonas aeruginosa;RR: risk ratio; SD: standard deviation; TIS: tobramycin for inhalation solution. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded once due to risk of bias within the trial. The trial was open‐label with the treatments given at a different frequency and so obvious to participants. There was also an unclear risk attributed to blinding of outcome assessment. bDowngraded once due to imprecision from low event rates.
Summary of findings 6. Summary of findings: amikacin liposome inhalation suspension (ALIS) versus tobramycin for inhalation solution.
| ALIS compared with TIS for long‐term therapy in CF | ||||||
|
Patient or population: children and adults with CF and P aeruginosa Settings: outpatients Intervention: ALIS 590 mg once daily with eFlow® nebuliser Comparison: TIS 300 mg twice daily via PARI LC® PLUS nebuliser | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| TIS | ALIS | |||||
|
FEV1: LS mean FEV1 (L) Follow‐up: 168 days |
The difference in LS mean FEV1 (L) adjusted for treatment and randomisation strata, at the end of treatment was MD –1.31% (95% CI, –4.95 to 2.34; P = 0.48). | NA | 262 (1) | ⊕⊕⊕⊝
moderatea |
This analysis was carried out on the per‐protocol data. The lower CI was above ‐5% indicating non‐inferiority of ALIS to TIS. |
|
|
FVC Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Pulmonary exacerbations: frequency of pulmonary exacerbations Follow‐up: 168 days |
There were more participants in the ALIS group experiencing an exacerbation than in the TIS group (63.5% in the ALIS group compared to 51.4% in the TIS group, P = 0.02). |
NA | 294 (1) |
⊕⊕⊕⊝ moderatea | The study also reported on hospitalisations and found that there was no difference, RR 0.82 (95% CI 0.50 to 1.33). Time to first exacerbation was also shorter in the ALIS group, HR 1.51 (95% CI 1.07 to 2.13) P = 0.03. |
|
|
Quality of life: change in CFQ‐R domain scores (mean CFQ‐R score) Follow‐up: 168 days |
There was no difference in change in CFQ‐R scores between groups at the end of the study across any domain. |
NA | 294 (1) | ⊕⊕⊕⊝ moderatea | ||
|
Survival Follow‐up: NA |
Outcome not reported. | NA | No deaths were reported in either group for the duration of the study (Bilton 2020). | |||
|
Antibiotic resistance: change from baseline in P aeruginosa CFU/g of sputum density Follow‐up: 168 days |
LS mean difference was no different between groups at the end of the study P = 0.13 | NA | 259 (1) | ⊕⊕⊕⊝ moderatea | The authors also report that mean P aeruginosa sputum densities were below baseline level at day 168 in both the ALIS group and the TIS group (Bilton 2020). | |
|
Adverse events: number of participants experiencing any TEAE Follow‐up: 168 days |
788 per 1000 | 1000 per 1000 (638 to 1000 per 1000) | RR 1.47 (0.81 to 2.66) | 294 (1) | ⊕⊕⊕⊝ moderatea | There were no differences between groups by severity of TEAE. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). ALIS: amikacin liposome inhalation solution; CFU colony forming units; CF: cystic fibrosis; CFQ‐R: cystic fibrosis questionnaire ‐ revised; CI: confidence interval; FEV1: forced expiratory volume at 1 second; HR: hazard ratio; LS: least squares; MD: mean difference; NA: not applicable; P aeruginosa: Pseudomonas aeruginosa;RR: risk ratio; TEAE: treatment‐related adverse event; TIS: tobramycin for inhalation solution. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded once due to risk of bias within the trial being unclear or high across all domains, largely due to the trial being open label with unclear process for generation of sequence and allocation concealment.
Summary of findings 7. Summary of findings: levofloxacin for inhalation solution versus tobramycin for inhalation solution.
| LIS compared with TIS for long‐term therapy in CF | ||||||
|
Patient population: adults and children aged over 12 with CF and P aeruginosa Settings: outpatients Intervention: LIS (Aeroquin™, MP376, APT‐1026) 240 mg (2.4 mL of 100 mg per mL solution) twice daily Comparison: TIS 300 mg/5 mL twice daily | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| TIS | LIS | |||||
|
FEV1 (% predicted): relative mean change from baseline Follow‐up: 6 months |
The mean (SD) change in % predicted FEV1 was ‐1.5 (14.8) in the TIS group. | The mean change in % predicted FEV1 in the LIS group was 0.30 higher (3.02 lower to 3.62 higher). | NA | 282 (1) | ⊕⊕⊕⊕ high | |
|
FVC(% predicted): relative mean change from baseline Follow‐up: 6 months |
The mean (SD) change in FVC % predicted was ‐1.3 (12.8) in the TIS group. | The mean change in FVC % predicted in the LIS group was 0.60 higher (2.23 lower to 3.43 higher). | NA | 282 (1) | ⊕⊕⊕⊕ high | |
|
Pulmonary exacerbations: number of hospitalisations due to respiratory exacerbations Follow‐up: 6 months |
280 per 1000 | 173 per 1000 (112 to 274 per 1000) | RR 0.62 (0.40 to 0.98) | 282 (1) | ⊕⊕⊕⊕ high | |
|
Quality of life: change from baseline in CFQ‐R Follow‐up: 6 months |
The trial reported that scores in the respiratory domain of the CFQ‐R were similar in the 2 groups at baseline, increased in the LIS group and decreased in the TIS group at day 28 and were similar again by the end of the trial. | NA | 282 (1) | ⊕⊕⊝⊝ lowa,b | No data could be entered into analysis. | |
|
Survival Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Antibiotic resistance: mean change in P aeruginosa sputum density (log10 CFU/g) Follow‐up: 6 months |
The mean (SD) sputum density in the TIS group was ‐0.25 (1.76) log10 CFU/g. |
The mean sputum density in the LIS group was 0.12 higher (0.31 log10 CFU/g lower to 0.55 log10 CFU/g higher). |
NA | 282 (1) | ⊕⊕⊕⊕ high | |
|
Adverse events: number of treatment‐related adverse events Follow‐up: 6 months |
Significantly fewer participants in the LIS group reported epistaxis, RR 0.2 (95% CI 0.04 to 1.00), general malaise, RR 0.1 (95% CI 0.01 to 0.83) and increased blood glucose, RR 0.28 (95% CI 0.08 to 0.94). Significantly more participants in the LIS group reported dysgeusia, RR 46.25 (95% CI 2.88 to 742). No other differences were noted. |
NA | 282 (1) | ⊕⊕⊕⊕ high | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CF: cystic fibrosis; CFU: colony forming units; CI: confidence interval; FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; LIS: levofloxacin for inhalation solution; NA: not applicable; P aeruginosa: Pseudomonas aeruginosa;RR: risk ratio; TIS: tobramycin for inhalation solution. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded once due to indirectness. Quality of life was measured by the CFQ‐R score but no data were provided, just a summary. It is unclear which participants were included in this outcome. bDowngraded once due to publication bias as the results were not presented in full for this outcome.
Summary of findings 8. Summary of findings: continuous cycles alternating aztreonam lysine for inhalation with tobramycin for inhalation solution versus continuous cycles alternating placebo with tobramycin for inhalation solution.
| Continuous AZLI/TIScompared with continuous placebo/TIS (i.e. intermittent TIS) for long‐term therapy in CF | ||||||
|
Patient population: children and adults with CF and P aeruginosa Settings: outpatients Intervention: continuous alternating cycles of AZLI (75 mg (diluted in 0.17% NaCL) 3 times‐daily) and TIS (300 mg/5 mL twice‐daily) Comparison: alternating cycles of placebo (lactose monohydrate and sodium chloride reconstituted with the same diluent used for AZLI 3 times daily) and TIS (300 mg/5 mL twice‐daily) | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| TIS/placebo | AZLI/TIS | |||||
|
FEV1 (% predicted): mean change from baseline (average values across the end of the 3 treatment cycles) Follow‐up: 6 months (24 weeks) |
The change from baseline in FEV1 % predicted was on average 1.33% more in the AZLI/TIS group than in the in the TIS/placebo group, values ranged from 0.51% lower to 3.17% higher. |
NA | 90 (1) | ⊕⊕⊝⊝
lowa,b |
||
|
FVC Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Pulmonary exacerbations: rate of PDEs per participant year Follow‐up: 24 weeks |
489 per 1000 | 347 per 1000 (210 to 577 per 1000) | RR 0.71 (0.43 to 1.18) | 90 (1) | ⊕⊕⊝⊝
lowa,b |
The rate of PDEs was lower in the AZLI/TIS group (1.31 PDEs per participant year) than in the placebo/TIS group (1.76 PDEs per participant year). The difference between the groups was not reported to be significant (P = 0.25, RR 0.74 (95% CI 0.45 to 1.24)). |
|
Quality of life: CFQ‐R respiratory symptom scores averaged from weeks 4, 12 and 20 Follow‐up: 24 weeks |
Scores improved by a mean (SE) 1.00 (1.74) in the AZLI/tobramycin group, they worsened by a mean (SE) ‐2.06 (1.63) in the placebo/TIS group. The difference between the groups was not found to be significant, MD 3.06 (95% CI ‐1.61 to 7.73). | NA | 90 (1) | ⊕⊕⊝⊝
lowa,b |
||
|
Survival Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Antibiotic resistance: mean change from baseline in Paeruginosa sputum density (CFU/g) Follow‐up: 24 weeks |
Adjusted mean changes from baseline sputum Paeruginosa density after each course of AZLI/placebo or TIS during the comparative phase were small (0.36 to ‐0.55 log10 CFU/g) and differences between treatment groups were not statistically significant. | NA | 87 (1) |
⊕⊕⊝⊝
lowa,b |
Results reported narratively from the paper. | |
|
Adverse events: any adverse event in the comparative phase Follow‐up: 24 weeks |
978 per 1000 | 949 per 1000 (880 to 1000) | RR 0.97 (0.90 to 1.05) | 88 (1) | ⊕⊕⊝⊝
lowa,b |
A range of adverse events were reported but the only adverse events which were significantly different between the 2 groups were: favouring continuous treatment
favouring intermittent treatment
|
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). AZLI: inhaled aztreonam lysine; CF: cystic fibrosis;CFQ‐R: cystic fibrosis questionnaire ‐ revised; CFU: colony forming units; CI: confidence interval; FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; MD: mean difference; NA: not applicable; PDE: protocol‐defined exacerbation; P aeruginosa: Pseudomonas aeruginosa;RR: risk ratio; SE: standard error; TIS: tobramycin for inhalation solution. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded once due to risk of bias being unclear across 5 of the domains around randomisation, allocation concealment, blinding of participants and incomplete outcome data. bDowngraded once due to imprecision as trial enrolment was limited and the trial was underpowered.
Background
Description of the condition
Cystic fibrosis (CF) is a life‐limiting inherited disease caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene which results in abnormal ion transfer at the apical surface of epithelial cells (Rosenstein 1998). This leads to production of thick sticky mucus affecting many systems around the body. One major impact of this genetic abnormality is lung disease, which is characterised by abnormal airway secretions, persistent bacterial infection and inflammation.
Around 10,400 people in the UK and around 100,000 people worldwide are affected by CF (CF Foundation 2019; CF Trust 2021). Whilst it was once viewed as a disease of childhood, the median life expectancy has been improving with children born in the year 2000 having a median life expectancy greater than 50 years (Dodge 2007). More than half of the CF population is now aged 18 or over (CF Foundation 2019).
The pattern of bacterial infection changes with age. As people with CF approach adulthood, acquisition of Pseudomonas aeruginosa becomes more common with over 30% of UK adults with CF being chronically infected (CF Trust 2021). This is associated with an accelerated decline in lung function, increased frequency of exacerbations, increased burden of treatment, and ultimately hastened mortality (Emerson 2002; Zemanick 2015). This review will focus on inhaled anti‐pseudomonal antibiotic therapy.
Description of the intervention
Delivering anti‐pseudomonal antibiotics by the inhalation of an aerosol is used to achieve high concentrations of the antibiotic in airways to control infection without the disadvantages of oral or parenteral administration (Touw 1995). The clinical settings in which inhaled anti‐pseudomonal antibiotics have been used are:
eradication of infection in the early stages of infection;
prophylaxis;
treatment of acute exacerbations of lung infection; and
for longer‐term suppression of chronic infection.
The fourth of these indications is the subject of this review. There is a recommendation to use inhaled tobramycin for treating individuals with CF who are six years of age and older, who have moderate to severe lung disease and with persistent P aeruginosa infection (Flume 2007; Mogayzel 2013). Information from the CF Trust Registry in 2016 showed that at least one of the following inhaled antibiotics were used in people with chronic P aeruginosa infection:
tobramycin solution (20.9%);
other aminoglycoside (2.6%);
colistin (25.3%);
promixin (29.8%);
aztreonam (18.8%);
colistimethate (DPI) (16.7%);
tobramycin inhalation powder (TIP) (27.8%);
at least one of the above (87.6%).
The current consensus view is that 90% of people chronically infected with P aeruginosa in the UK should be treated with at least one of the above inhaled antibiotics (CF Trust 2021). Inhaled anti‐pseudomonal antibiotics were typically given in 28‐day cycles of one month on and one month off (CF Trust 2009). Current practise in the UK is to give continuous nebulised colistin as a first‐line treatment, although the antibiotic regimen may be changed to treat exacerbations (NICE 2017). In the USA, chronic suppression of P aeruginosa is with continuous inhaled tobramycin. Colistin is not recommended in USA guidelines for chronic suppression of P aeruginosa (Yankaskas 2004).
How the intervention might work
The aim of treatment is to reduce the bacterial load in the lung, which in turn should reduce inflammation in the lung, thereby reducing lung damage and so reduce the rate of deterioration of lung function and frequency of exacerbations of infection. These outcomes should be associated with improvement in quality of life (QoL) and in survival. Additional issues of relevance around the use of inhaled anti‐pseudomonal antibiotics in CF include financial cost, increased time of treatment, risks of adverse effects of the drugs and an increase in the likelihood of acquisition of infection with drug‐resistant organisms by long‐term exposure to antibiotics.
Why it is important to do this review
This review aims to identify the most effective inhaled anti‐pseudomonal antibiotic treatment regimens for long‐term maintenance therapy in people with CF.
We know that antibiotic treatment can clear P aeruginosa from respiratory secretions in children with CF, and that treating early P aeruginosa with nebulised antibiotics (or a combination of inhaled and oral antibiotics) is better than not treating (Langton Hewer 2017). There is also evidence from earlier versions of this review that inhaled antibiotic treatment of chronic infection is of some benefit in terms of improvement in lung function and reduction in exacerbations (Ryan 2011). However, we do not know what the best treatment is for suppressing chronic P aeruginosa infection (Ryan 2011). We consider it to be important to extend the minimum duration for included trials from one month and over, to three months and over at this update in order to study the longer‐term effects of treatment.
This is an updated version of the 2018 Cochrane Review (Smith 2018) previously titled 'Inhaled antibiotics for long‐term therapy cystic fibrosis' which was first published with the original title 'Nebulised anti‐pseudomonal antibiotics for cystic fibrosis' in 1999 (Ryan 1999; Ryan 2003; Ryan 2011).
Objectives
To evaluate the effects of long‐term inhaled antibiotic therapy in people with CF on clinical outcomes (lung function, frequency of exacerbations and nutrition), QoL and adverse events (including drug‐sensitivity reactions and survival).
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) or quasi‐RCTs. We included parallel‐designed trials and cross‐over trials where appropriate.
Types of participants
People with CF diagnosed by clinical features associated with an abnormal sweat electrolyte test or mutations of the CFTR gene or both. All ages and all levels of severity of respiratory disease were included.
Types of interventions
Any inhaled antibiotic (all doses and methods of inhalation) with activity against P aeruginosa given for at least three monthsa compared to an inhaled placebo or no placebo, i.e. usual treatment (where this did not include any oral or intravenous antibiotic therapy during the trial), or another inhaled anti‐pseudomonal antibiotic. Trials in which an antibiotic was tested at two or more doses are also eligible.
aIn a post hoc change the duration of the intervention was extended from that stated in the original review where the duration of intervention considered was one month or over.
Types of outcome measures
We planned to assess the following outcome measures.
Primary outcomes
-
Lung function (measured in litres (L) or per cent (%) predicted)
forced expiratory volume in one second (FEV1)
forced vital capacity (FVC)
-
Exacerbation of respiratory infection (defined as any deterioration in clinical condition resulting in treatment with oral or intravenous antibiotics, either at home or in hospital)
hospital admissions
days in hospital
courses of intravenous antibiotics
-
pulmonary exacerbations
frequency
time to first exacerbation
Secondary outcomes
-
Nutrition
height
weight
QoL
Survival
Antibiotic resistance in P aeruginosa or other organisms
-
Adverse events
renal impairment ‐ serum creatinine increase
auditory impairment ‐ impaired audiometry
sensitivity reactions ‐ bronchospasm
other (post hoc change)
Search methods for identification of studies
Trial searches were not restricted by date, language, or publication status.
Electronic searches
Relevant trials were identified from the Group's Cystic Fibrosis Trials Register using the terms: antibiotics AND (maintenance OR unknown) AND (inhaled or not stated), ALSO: macrolide AND inhaled.
The Cystic Fibrosis Trials Register is compiled from electronic searches of the Cochrane Central Register of Controlled Trials (CENTRAL) (updated each new issue of the Cochrane Library), weekly searches of MEDLINE, a search of Embase to 1995 and the prospective handsearching of two journals ‐ Pediatric Pulmonology and the Journal of Cystic Fibrosis. Unpublished work is identified by searching through the abstract books of three major cystic fibrosis conferences: the International Cystic Fibrosis Conference, the European Cystic Fibrosis Conference and the North American Cystic Fibrosis Conference. For full details of all searching activities for the register, please see the relevant sections of the Cystic Fibrosis and Genetic Disorders Group website.
Date of the most recent search of the Group's Cystic Fibrosis Trials Register: 28 June 2022.
Additional search strategies for online databases are detailed in the appendices (Appendix 1); date last searched was 7 June 2022.
Searching other resources
We have previously contacted manufacturers of inhaled antibiotics; however, due to the poor response from them, we have decided not to pursue this approach from 2018 onwards.
Data collection and analysis
Selection of studies
Two authors (for earlier versions of the review GR and MS, for later versions of the review two of the three authors SS, NR and KR) independently reviewed the full text of articles or abstracts identified from the search to select trials which fulfilled the inclusion criteria. They recorded reasons for excluding trials. The authors settled any disagreement on article selection by consensus. The authors did not re‐score full text articles from the previous versions of the review for this update.
Data extraction and management
The authors prepared a form to record details of trial design, participant numbers and characteristics, interventions, and outcomes. Two authors (for earlier versions of the review GR and MS, for later versions of the review SS, NR and KR) independently recorded the quality characteristics of each included trial and extracted the relevant outcome data. The authors settled any disagreement by consensus. At the 2018 update onwards, the new author team did not repeat this process for previously assessed and recorded trials.
The authors reported outcome measures at three months, over three and up to 12 months and annually thereafter to accommodate trials of different lengths. Where trials reported multiple time points for one category, the authors only used the longest time‐point data.
Assessment of risk of bias in included studies
The authors (initially GR and MS, 2010 update GR and KD, 2017 update SS and NR) assessed the risk of bias for each included trial using the criteria specified in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017). This involves a judgement of how the investigators generated the allocation sequence and how well they concealed the allocation schedule, how they blinded participants and investigators, whether they included all randomised participants in the analysis and reported all outcomes measured, and if they avoided other factors with a potential for biassed results. The authors recorded judgements as having a low, unclear or high risk of bias (which related to the original judgements of adequate, unclear or inadequate respectively). At the 2018 update, the new author team did not re‐assess the judgements for previously assessed trials.
Two authors (as above) planned to assess outcome reporting bias by either comparing outcomes stated in the trial protocols to their full publications when available, or by obtaining data from a clinical trial registry, or by comparing the methods section to the results section in a publication with our knowledge of the clinical area. If they had suspected outcome reporting bias, they planned to contact the trial investigators to find out if they had measured and analysed the outcome in question and to obtain the data. The review authors also planned to contact experts in the field to attempt to identify any unpublished trials.
Measures of treatment effect
For dichotomous outcome data (exacerbation of respiratory infection, survival, antibiotic resistance in P aeruginosa or other organisms, adverse events), the authors calculated a pooled estimate of the treatment effect for each outcome across trials using risk ratio (RR) and 95% confidence intervals (95% CIs) where appropriate.
For continuous outcome data (lung function, nutrition, QoL), they recorded either mean relative change from baseline for each group or mean post‐treatment or post‐intervention values and standard deviations (SDs). If standard errors (SEs) were reported (and if possible) they converted these to SDs. The authors calculated a pooled estimate of treatment effect by calculating the mean difference (MD) and 95% CIs where appropriate.
Unit of analysis issues
The protocol for this review did not exclude trials using a cross‐over design, although they are not the ideal trial design because of the progressive nature and deterioration of CF lung function. There are methods for meta‐analysis of results from cross‐over trials (Elbourne 2002), which rely on the data that are reported within the primary paper. In this review the authors have only used data from the first treatment period, ignoring the second period, i.e. regarding as a parallel trial. If results of the first period were not available, the authors describe the results of the trial in the text. The trial was only included if the first period was at least three months in duration.
Dealing with missing data
If the authors needed additional information on the trials considered for this review, they planned to contact the original investigators. They did request additional information from the authors of the Wiesemann trial, but have not yet received a reply (Wiesemann 1998). They have also contacted the lead investigators of three trials on two occasions (Chuchalin 2007; McCoy 2008; Nikolaizik 2008), and have received data from one trial (Nikolaizik 2008).
Assessment of heterogeneity
The authors planned to assess the degree of heterogeneity between trials using the I2 statistic which describes the percentage of total variation across trials which is due to heterogeneity rather than by chance. The values of I2 lie between 0% and 100%, and a simplified categorisation of heterogeneity that the authors planned to use is (Higgins 2021):
0% to 40%: might not be important;
30% to 60%: may represent moderate heterogeneity;
50% to 90%: may represent substantial heterogeneity; and
75% to 100%: considerable heterogeneity.
Assessment of reporting biases
The authors planned to assess publication bias by constructing a funnel plot if 10 or more trials had been available. If the funnel plot is not symmetrical, publication bias may be present. However, there are other reasons for funnel plot asymmetry (i.e. heterogeneity), so the plot should be interpreted with caution. To minimise publication bias, the authors searched trial registries and contacted experts in the field for any unpublished trials.
The authors checked outcomes reported against the protocol for the trial (if this was available) or against the methods section of the paper if not.
The authors aimed to check the different methods of reporting certain outcome measures (e.g. FEV1) to ensure they have not been selectively reported.
Data synthesis
The authors mainly analysed the data using a fixed‐effect model, but where they identified a moderate to high degree of heterogeneity (see above), they used a random‐effects model to analyse the data.
Subgroup analysis and investigation of heterogeneity
We considered the major potential sources of heterogeneity to be the intervention (drugs, dose, regimens, method of aerosol generation and inhalation) and severity of disease (baseline FEV1, clinical stability). The authors investigated these with informal subgroup analyses when they were able to combine data from at least two trials and where there was at least substantial heterogeneity (I2 greater than 50%) in the results (two instances). We considered the reasons for heterogeneity and described why it may have occurred in the text. If we are able to include and combine more trials in future updates, we will carry out the following formal subgroup analyses:
different drugs or doses;
different drug regimens;
drug delivery method; and
severity of disease.
Sensitivity analysis
Where we carried out meta‐analyses, we planned to perform sensitivity analyses based on the risk of bias in the trials to look at the effect of removing trials at high risk of bias; however, there were not a sufficient number of trials included and combined in the meta‐analyses to be able to do this. We also planned to look at the effect of removing quasi‐RCTs. In a post hoc change we also planned a sensitivity analysis with and without cross‐over trials where this was possible. Again, we were not able to include sufficient trials in the meta‐analyses to be able to do this.
Summary of findings and assessment of the certainty of the evidence
In a post hoc change, and in accordance with current Cochrane guidance, we have included a summary of findings table for each comparison in the review at the 2018 update. The main comparisons are as follows (the exception to this is where a particular antibiotic or combination of antibiotics is no longer included in current guidelines):
inhaled anti‐pseudomonal antibiotics versus placebo or usual treatment;
inhaled anti‐pseudomonal antibiotics compared to another inhaled anti‐pseudomonal antibiotic, including different dose or regimen (we have created a separate summary of findings table for each unique comparison, e.g. tobramycin versus aztreonam, tobramycin versus levofloxacin); and
continuous versus intermittent cycles of inhaled antibiotics.
We have selected the following seven outcomes, which we consider to be the most important, to include in the tables, but have also graded our other outcomes and described the certainty judgements in the text alone.
FEV1
FVC
Pulmonary exacerbations
QoL
Survival
Antibiotic resistance
Adverse events
We used the GRADE approach to assess the certainty of the evidence for each outcome based on the risk of bias within the trials, relevance to our population of interest (indirectness), unexplained heterogeneity or inconsistency, imprecision of the results or high risk of publication bias. We downgraded the certainty of the evidence once if the risk was serious and twice if the risk was deemed to be very serious.
Results
Description of studies
Please see the tables for the characteristics of the trials (Characteristics of included studies; Characteristics of excluded studies; Characteristics of studies awaiting classification).
Results of the search
The searches retrieved 410 citations to 125 trials (three trials were identified from the ongoing trials databases). In total, 18 trials (115 citations) with 3042 participants were included in the review and 102 trials (291 citations) were excluded. Four trials are listed under 'Studies awaiting classification' until more information becomes available (EUCTR2007‐004277‐26‐NL; Herrmann 2017; Nikonova 2010; NCT03341741). One trial that was previously listed in awaiting classification has now been excluded (Ramsey 2017). No trials are currently listed as ongoing. Results of the search are shown in a PRISMA diagram (Figure 1).
1.
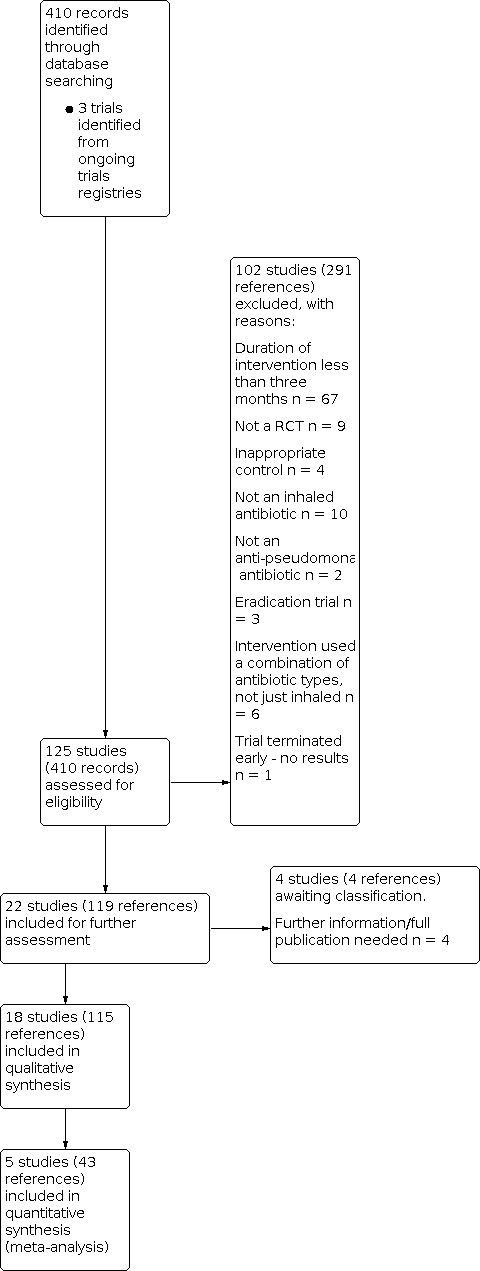
Study flow diagram.
Included studies
Inhaled anti‐pseudomonal antibiotic compared to placebo or usual treatment
An inhaled anti‐pseudomonal antibiotic was compared to placebo or usual treatment in 11 of the 18 included trials (1130 participants) (Chuchalin 2007; Day 1988; Hodson 1981; Jensen 1987; Kun 1984; MacLusky 1989; Murphy 2004; Nathanson 1985; Ramsey 1999; Stead 1987; Wiesemann 1998). Two trials were published only as abstracts in conference proceedings (Day 1988; Nathanson 1985). There was large variation between trials in terms of design, intervention and outcome measures. One trial compared an inhaled antibiotic to both placebo and another inhaled antibiotic and is therefore included in two comparisons in this review (Stead 1987).
Searches of the Group's CF Trials Register identified 32 citations that report data from a single trial which was first fully published in 1999 (Ramsey 1999). This trial is widely known as the 'TOBI' trial from the trade name of the preservative‐free formulation of tobramycin used in the trial (Ramsey 1999). Another report of this trial is published in full and provides information on the effect of tobramycin treatment on the isolation of drug‐resistant organisms (Burns 1999). A third report of this trial is on the effect of tobramycin on hospitalisation and home intravenous antibiotic use; it is only an abstract and results can not be analysed (Birnbaum 1998).
Trial design
Seven out of 11 trials were described as double‐blinded (Chuchalin 2007; Day 1988; Hodson 1981; Jensen 1987; Nathanson 1985; Ramsey 1999; Wiesemann 1998), three trials were described as single‐blinded (Kun 1984; MacLusky 1989; Stead 1987). One trial was not blinded (Murphy 2004).
A cross‐over design was used in five trials with 92 participants (8% of the total participants for this comparison) (Day 1988; Hodson 1981; Kun 1984; Nathanson 1985; Stead 1987). In one of these trials, the first period could be analysed as a parallel design trial for the first year (Kun 1984). None of the five cross‐over trials examined for carry‐over or period effects. The remaining six trials were of parallel design (Chuchalin 2007; Jensen 1987; MacLusky 1989; Murphy 2004; Ramsey 1999; Wiesemann 1998).
Duration of treatment ranged from a minimum of three months (Jensen 1987; Nathanson 1985) to the longest which had a mean treatment duration of 33 months (MacLusky 1989). Treatment lasted three months in two trials (Jensen 1987; Nathanson 1985), four months in one trial (Stead 1987), six months in four trials (Chuchalin 2007; Day 1988; Hodson 1981; Ramsey 1999), 12 months in two trials (Kun 1984; Wiesemann 1998), 56 weeks in one trial (Murphy 2004) and there was a mean treatment duration of 33 months in one trial (MacLusky 1989).
Four of the trials were multicentre, these were carried out in: Hungary, Poland and Russia (Chuchalin 2007); USA and Canada (Murphy 2004); USA (Ramsey 1999); and Germany (Wiesemann 1998). Two were single‐centre trials carried out in Australia (Kun 1984) and Canada (MacLusky 1989). The remaining five trials did not state whether they were single‐centre or multicentre or in which country they were carried out (Day 1988; Hodson 1981; Jensen 1987; Nathanson 1985; Stead 1987).
The sample size for each trial varied from seven randomised participants (Nathanson 1985) to 520 randomised participants (Ramsey 1999), with a total of 1130 participants enroled across all included trials.
Participants
Participants were both children and adults, with the youngest being five years of age (Day 1988) and the eldest being 45 years old (Chuchalin 2007), although an accurate age distribution is difficult to determine from the reports and is not available for the largest trial (Ramsey 1999). The numbers of males and females was equally distributed in seven of the trials where 50% to 55% of the participants were male (Chuchalin 2007; Day 1988; Hodson 1981; Jensen 1987; MacLusky 1989; Murphy 2004; Ramsey 1999). Two of the trials were weighted towards males with 67% male participants in the Stead trial (Stead 1987) and 60% male participants in the Wiesemann trial (Wiesemann 1998). The numbers of male and female participants was not stated in either the Kun trial or the Nathanson trial (Kun 1984; Nathanson 1985).
Six out of 11 trials stated criteria for the diagnosis of CF (Chuchalin 2007; Hodson 1981; MacLusky 1989; Murphy 2004; Ramsey 1999; Stead 1987); however since participants were recruited from CF centres we accepted all 11 trials. It is unlikely that an important number of participants without CF were included.
There is also a wide range of disease severity as measured by baseline FEV1, with some participants having an FEV1 lower than 30% predicted and some over 100% predicted. However, it is not possible to know the numbers in categories of 'no', 'mild', 'moderate' or 'severe' impairment of lung function. Evidence of P aeruginosa in sputum culture was an inclusion requirement in all trials except one, in which P aeruginosa was present in eight out of 33 participants (Kun 1984).
The pattern of respiratory disease in CF tends to be of progressive deterioration over years and with episodes of acute deterioration and some recovery. Due to these short‐term fluctuations in severity, the timing of entry of participants into a trial in relation to exacerbations may determine outcome. In two trials, participants were recruited immediately after a course of anti‐pseudomonal intravenous antibiotics (Day 1988; Jensen 1987). Three trials stated that participants were recruited at least two weeks after a course of intravenous antibiotics in an attempt to ensure a stable state (Hodson 1981; Ramsey 1999; Stead 1987). One trial excluded participants if they had had an exacerbation in the previous month (Chuchalin 2007). This aspect of participant selection was not stated in the remaining five trials (Kun 1984; MacLusky 1989; Murphy 2004; Stead 1987; Wiesemann 1998).
Interventions
A unique feature of two trials was the intermittent use of nebulised tobramycin, i.e. cycles of tobramycin 300 mg twice daily for four weeks, followed by four weeks off treatment for a trial duration of six months (Ramsey 1999) and 56 weeks (Murphy 2004).
The dose of drug delivered to the lung depends on a number of factors including the method of aerosol generation and delivery, the volume of solution in the nebuliser and the method of inhalation (Newman 1985). Four trials reported details of the nebuliser and pump system (Chuchalin 2007; Kun 1984; Murphy 2004; Ramsey 1999). Another four trials stated which nebuliser the participants used (Jensen 1987; MacLusky 1989; Stead 1987; Wiesemann 1998). Five of the eight trials which reported using jet nebulisers stated the volume of solution they used, which varied from 1 mL to 5 mL (Jensen 1987; MacLusky 1989; Ramsey 1999; Stead 1987; Wiesemann 1998). Three trials did not provide any details of aerosol delivery (Day 1988; Hodson 1981; Nathanson 1985).
In three of the seven double‐blinded trials, the placebo was normal saline, and it is possible that in these trials the taste of the antibiotic solution was not completely masked (Day 1988; Jensen 1987; Nathanson 1985). In the remaining four double‐blinded trials, investigators uses varying saline concentrations and the addition of other chemicals (lactose or quinine or preservatives) to match drug and placebo solutions (Chuchalin 2007; Hodson 1981; Ramsey 1999; Wiesemann 1998). Of the four trials which did not use a double‐blind design, Kun and Murphy used usual treatment as control (Kun 1984; Murphy 2004), MacLusky used normal saline (MacLusky 1989) and Stead used 3.5% sodium chloride solution (hypertonic saline) as a placebo (Stead 1987), but since then hypertonic saline has been shown to have a therapeutic effect in CF (Wark 2009).
The trials used the following individual antibiotics.
Colistin
Two trials with 54 participants compared colistin to placebo, using a dose of one million units twice daily for three months (Jensen 1987) and for six months (Day 1988).
Tobramycin
Five trials with 998 participants compared tobramycin to placebo or usual treatment for between six and 33 months (Chuchalin 2007; MacLusky 1989; Murphy 2004; Ramsey 1999; Wiesemann 1998); 52% of participants were in one high‐quality trial (Ramsey 1999). Tobramycin was used in varying doses; two trials used 80 mg (MacLusky 1989; Wiesemann 1998) and three trials used 300 mg (Chuchalin 2007; Murphy 2004; Ramsey 1999). The frequency of dosing also varied with four trials using twice‐daily nebulisation (Chuchalin 2007; Murphy 2004; Ramsey 1999; Wiesemann 1998) and one trial using three‐times daily nebulisation (MacLusky 1989).
Gentamicin
Two cross‐over trials (n = 40) compared gentamicin as a single agent; one trial used 20 mg twice daily for 12 months (Kun 1984) and the second used 80 mg three times daily for three months (Nathanson 1985).
Ceftazidime
Only one trial with 18 participants used ceftazidime in the third arm of a three‐way cross‐over trial without a washout period; the dose was 1.0 g twice daily (Stead 1987).
Gentamicin and carbenicillin
Two cross‐over trials with 38 participants tested a combination of gentamicin 80 mg with carbenicillin 1.0 g twice daily (Hodson 1981; Stead 1987).
Aztreonam lysine (AZLI)
No trial investigated the use of AZLI compared to placebo.
Outcomes
All 11 trials included lung function (FEV1 and FVC) as an outcome measure; however, the duration of the trials and the method of expression of results varied across the trials. The most common method (five trials) was the change in FEV1 and FVC from baseline to the end of treatment; this change was expressed as change as % predicted in four trials (Chuchalin 2007; Jensen 1987; Kun 1984; Ramsey 1999) and as change in L in one trial (Stead 1987). The Jensen trial reported on lung function over three months (see 'Effects of interventions') and also on improvement in clinical score and inflammatory parameters, neither of which are outcome measures for this review (Jensen 1987). Two trials compared absolute FEV1 and FVC at the end of treatment, one as % predicted (Day 1988) and one in L (Nathanson 1985). Lung function was reported as the mean of monthly measurements for six months in one trial (Hodson 1981) and the rate of decline of predicted FEV1 in two trials (MacLusky 1989; Murphy 2004). One trial only provided a narrative statement on difference between groups (Wiesemann 1998). Four of the trials did not include SDs or SEs for lung function (Day 1988; Hodson 1981; Kun 1984; Nathanson 1985).
Seven trials included some measurement of frequency of exacerbations of lung infection; four measured number of hospital admissions (Chuchalin 2007; Day 1988; Ramsey 1999; Stead 1987), one reported days in hospital during the trial (Kun 1984) and two trials reported both hospital admissions and number of days (MacLusky 1989; Murphy 2004). Seven trials measured the number of courses of antibiotics during the trial (Chuchalin 2007; Day 1988; Hodson 1981; Kun 1984; Murphy 2004; Ramsey 1999; Stead 1987).
Six trials reported some score of disease severity, which included symptoms, but were not consistent in their methodology (Day 1988; Jensen 1987; Kun 1984; MacLusky 1989; Nathanson 1985; Ramsey 1999).
Sputum bacteriology for antibiotic sensitivity was reported in seven trials (Chuchalin 2007; Hodson 1981; Jensen 1987; Kun 1984; MacLusky 1989; Ramsey 1999; Stead 1987).
Four trials measured renal function (Chuchalin 2007; MacLusky 1989; Murphy 2004; Ramsey 1999) and five trials measured hearing as a marker of toxicity (Chuchalin 2007; Hodson 1981; MacLusky 1989; Murphy 2004; Ramsey 1999).
Other outcome measures used infrequently were death, chest X‐ray score, blood antibiotic levels, quantitative bacterial count in sputum, blood levels of inflammatory parameters, weight, treatment satisfaction and number of lost school or working days.
Inhaled anti‐pseudomonal antibiotics compared
Seven trials reported on this comparison with 1840 participants (Assael 2013; Bilton 2020; Elborn 2015; Schuster 2013; Konstan 2010b; Nikolaizik 2008; Stead 1987). One trial (18 participants) compared to both placebo and another inhaled antibiotic and is therefore included in two comparisons in this review (Stead 1987).
Trial design
Two of the trials (n = 50) were cross‐over in design (Nikolaizik 2008; Stead 1987). One trial employed two arms with each arm lasting three months and no washout period described (Nikolaizik 2008). The second cross‐over trial had three treatment arms with each one lasting four months (Stead 1987). The remaining five trials (n = 1790) employed a parallel design (Assael 2013; Bilton 2020; Elborn 2015; Konstan 2010b; Schuster 2013).
The duration of the trials varied; five trials lasted six months (Assael 2013: Bilton 2020; Elborn 2015; Konstan 2010b; Schuster 2013). The Nikolaizik trial ran over three months (Nikolaizik 2008) and Stead over four months (Stead 1987).
Sample size ranged from 18 participants (Stead 1987) to 553 participants (Konstan 2010b).
Two of the seven trials did not state whether they were multicentre or single‐centre or in which country they were carried out (Nikolaizik 2008; Stead 1987). The remaining five trials were multicentre: one being set in Europe and USA (Assael 2013); one in Europe and Canada (Bilton 2020); one in Europe, USA and Israel (Elborn 2015); and one across Europe, Russia and Ukraine (Schuster 2013). The Konstan trial was conducted in 127 centres in 15 countries, though the individual countries were not stated (Konstan 2010b).
Participants
All seven trials enroled both adults and children with age ranges from six to 56 years. With regard to the male/female split, in two trials there was an almost equal split between males and females (Assael 2013; Nikolaizik 2008) and in four trials there were more males than females (Elborn 2015; Schuster 2013; Konstan 2010b; Stead 1987). One trial did not specify the numbers of male and female participants (Bilton 2020).
All trials enroled participants with a confirmed diagnosis of CF and presence of P aeruginosa in the sputum (Assael 2013; Bilton 2020; Elborn 2015; Konstan 2010b; Nikolaizik 2008; Schuster 2013; Stead 1987).
Disease severity at baseline was measured in all trials. Four trials reported the number of participants whose FEV1 results at baseline were less than 50% of predicted: in the Assael trial 43.7% of participants (Assael 2013); in the Bilton trial 29.3% of participants (Bilton 2020); in the Schuster trial 47.3% of participants (Schuster 2013); Konstan reported separately for each arm of the trial, 41.6% and 42.6% (Konstan 2010b). Elborn reported that 55.9% and 52.9% of participants in the two arms had an FEV1 at baseline of less than 55% of predicted (Elborn 2015). One trial reported the mean (SD) FEV1 % predicted in each of the two arms of the trial, 48.4% (15.8) and 63.1% (21.6) (Nikolaizik 2008). Stead reported a median FVC at baseline of 53% of the predicted value (Stead 1987).
Interventions
Two trials compared different preparations of tobramycin (Konstan 2010b; Nikolaizik 2008). Konstan compared twice‐daily inhaled tobramycin powder (four capsules, total of 112 mg) with twice‐daily tobramycin for inhalation solution (TIS) (300 mg in 5 mL) for six months (Konstan 2010b). Over three months, Nikolaizik compared twice‐daily inhalations of the intravenous preparation of tobramycin (80 mg) and intermittent (four‐weekly on‐off cycles) TIS (300 mg) (Nikolaizik 2008).
A further four trials compared TIS to other inhaled antibiotics (Assael 2013; Bilton 2020; Elborn 2015; Schuster 2013). Assael compared 75 mg AZLI inhaled three times daily to 300 mg TIS inhaled twice daily (Assael 2013). Bilton compared once‐daily 590 mg/8.4 mL amikacin liposome inhalation suspension (ALIS) with twice‐daily 300 mg TIS (Bilton 2020). Elborn compared 240 mg levofloxacin for inhalation solution (LIS) (Aeroquin™, MP376, APT‐1026) with 300 mg TIS; both treatments were inhaled twice daily (Elborn 2015). In the fourth trial, Schuster compared twice‐daily 125 mg colistimethate dry powder for inhalation with twice‐daily 300 mg TIS for six months; the tobramycin regimen consisted of three cycles of 28 days on and 28 days off treatment (Schuster 2013).
Finally, over four months Stead compared twice‐daily inhalations of 1 g ceftazidine (in 2 mL to 4 mL solution) to twice‐daily inhalations of a combination of 80 mg gentamicin (in 2 mL solution) and 1 g carbenicillin (3 mL of sterile water) inhaled separately and also to placebo (2 mL to 4 mL of 3.5% saline solution) inhaled twice daily (Stead 1987).
Outcomes
All seven trials reported on FEV1 (Assael 2013; Bilton 2020; Elborn 2015; Konstan 2010b; Nikolaizik 2008; Schuster 2013; Stead 1987) and five reported FVC (Elborn 2015; Konstan 2010b; Nikolaizik 2008; Schuster 2013; Stead 1987). Four trials reported on sputum bacteriology (Assael 2013; Bilton 2020; Elborn 2015; Stead 1987) and two reported on participant preference (Nikolaizik 2008; Stead 1987). A further two trials measured treatment satisfaction (Assael 2013; Konstan 2010b) and one reported on treatment burden (Bilton 2020). Three trials reported on pulmonary exacerbations (Elborn 2015; Schuster 2013; Stead 1987), four reported the number of respiratory hospitalisations (Elborn 2015; Konstan 2010b; Schuster 2013; Stead 1987) and four reported on safety outcomes or adverse events (Bilton 2020; Elborn 2015; Konstan 2010b; Schuster 2013).
Continuous inhaled anti‐pseudomonal antibiotics versus intermittent inhaled anti‐pseudomonal antibiotics compared
One of the trials included at this update compared continuous treatment with a combination of inhaled anti‐pseudomonal antibiotics versus intermittent treatment with inhaled antibiotics (Flume 2016b). This trial included 90 participants.
Trial design
This multicentre trial (45 CF centres in the USA) employed a double‐blind parallel design with a run‐in period of 28 days of TIS followed by three 28‐day cycles of AZLI or placebo. The three treatment cycles were alternated with 28 days of TIS. Participants either received a continuous course of alternate antibiotics (AZLI alternating with TIS) or an intermittent course of TIS alternating with placebo.
The total duration of the trial was 28 weeks with the intervention period lasting 24 weeks. 90 participants were randomised and included in the intention‐to‐treat (ITT) analysis.
Participants
The trial enroled both adults and children with a mean (SD) age of 28.5 (12.1) years in the AZLI group and a mean (SD) age of 28.3 (10.8) years in the placebo group. Both arms of the trial were weighted towards females with only 42.9 % male in the AZLI group and 41.3 % male in the placebo group.
All enroled participants had a confirmed diagnosis of CF and presence of P aeruginosa in the sputum.
Disease severity at baseline was measured using the mean (SD) FEV1 % predicted at day one; in the AZLI group this was 49.9% (17.7) and in the placebo group it was 50.1% (15.3)
Interventions
All participants received a run‐in of 28 days of TIS 300 mg twice daily. In the comparison phase, participants were randomised to AZLI 75 mg three times daily (diluted in 0.17% sodium chloride (NaCl) solution) delivered by the eFlow nebuliser system (PARI) or placebo. The placebo treatment was lactose monohydrate and sodium chloride reconstituted with the same diluent used for AZLI (0.17% w/v NaCl solution) and given to the same schedule. The alternating treatment was 300 mg of TIS twice daily for each four‐week period.
Outcomes
The trial measured mean change from baseline in FEV1 % predicted where values at the end of weeks four, 12 and 20 (AZLI or placebo phases) were averaged. The primary outcome for the trial was rate of protocol‐defined exacerbations (PDEs) at the end of treatment. The trial also reported on median time (95% CI) to first exacerbation and rate of hospitalisation. Nutritional outcomes were not reported, although the change in weight was listed in adverse events. Investigators reported QoL using the CFQ‐R respiratory symptom score with scores averaged from weeks four, 12 and 20. The changes in Cystic Fibrosis Respiratory Symptom Diary (CFRSD) scores and Chronic Respiratory Infection Symptom Scores (CRISS) were also exploratory endpoints. The trial did not report on survival. Antibiotic resistance was measured by measuring change from baseline in P aeruginosa density, presence of other respiratory pathogens and change from baseline in minimum inhibitory concentrations (MIC) of aztreonam, tobramycin and other antibiotics active against P aeruginosa. Adverse events were reported for the comparative phase of the trial and included treatment‐emergent adverse events, severe adverse events and treatment‐related adverse events (Flume 2016b).
Excluded studies
There are 102 trials listed as excluded, and we present details in the tables (Characteristics of excluded studies). The reasons for exclusion varied and some had more than one exclusion factor, but we have presented the main reason for exclusion in the following text. The most frequent reason for exclusion was duration of the trial, which in the original review was a minimum of 28 days and after the post hoc change in 2018 was a minimum of three months of treatment. Duration of the intervention was less than three months in 67 trials (ACTRN12620000531910; Al‐Aloul 2004; Alothman 2000; Alothman 2005; App 2000; Bruinenberg 2008; Coates 2011; Chua 1990; Davies 2004; Dodd 1997; Dodd 1998; Dorkin 2015; Dupont 2008; Eisenberg 1997; EUCTR2005‐004103‐10‐DE; EUCTR2006‐006215‐68‐DE; EUCTR2007‐003868‐22‐FR; EUCTR2007‐005346‐20‐GB; EUCTR2008‐008314‐40‐DK; EUCTR2009‐013660‐39‐FR; EUCTR2010‐023533‐34‐FR; EUCTR2014‐001401‐41‐NL; Flume 2016a; Frost 2018; Galeva 2013; Geborek 2003; Geller 2004; Geller 2007; Geller 2011a; Geller 2011b; Gibson 2003; Gibson 2006; Goss 2013; Griese 2009; Griffith 2008; Gulliver 2003; Hodson 2002; IRCT2016100930233N1; Jenkins 1985; Knowles 1988; Konstan 2010a; Lenoir 2007; Mainz 2014; Maneshi 2019; Mazurek 2014; McCoy 2008; Mullinger 2005; Nasr 2006; NCT00420836; NCT00503490; NCT01315691; NCT02894684; NTR5211; Poli 2005; Ramsey 1993; Retsch‐Bogart 2007; Retsch‐Bogart 2008; Rietschel 2009; Sands 2014; Schaad 1987; Stass 2015; Stephens 1983; Trapnell 2012; Wainwright 2011; Westerman 2003; Westerman 2007; Yasmin 1974). A summary of the information contained in the trials that are more than 28 days in duration but less than three months can be found in the additional tables (Table 9). Nine trials were not RCTs (Fiel 2013; Franz 1985; Nikolaizik 1996; Oermann 2009; Smith 1989; Stass 2009; Steinkamp 1989; Wall 1984; Wang 1984) and in a further four trials the control was not appropriate for testing the effect of an inhaled antibiotic (Rosenfeld 2006; Ruddy 2013; Shatunov 2001; Stroobant 1985). In nine trials the antibiotic was not inhaled (Claut 2011; NCT00411736; NCT02677701; NCT02730793; Nichols 2020; Pradal 2002; Ramsey 2017; Steinkamp 2006; Wainwright 2008). Two trials did not examine an anti‐pseudomonal antibiotic treatment (Ledson 2002; Nolan 1982). Three trials looked at treatment to eradicate P aeruginosa (Proesmans 2016; Ramsey 2005; Ratjen 2010). Finally, seven trials compared a combination of antibiotics administered differently and not just inhaled (Carswell 1987; Cooper 1985; Frederiksen 1997; Noah 2007; Schaad 1997; Tramper‐Stranders 2010; Valerius 1991). One trial needed to recruit 200 participants, but only recruited 32 and of those, only five completed the trial; no results are available (NCT02015663).
1. Summary of excluded short‐term studies (28 days or longer).
| Trial | Trial characteristics | Participants | Interventions | Summary of results |
| Dorkin 2015 |
Duration: 28 days. Design: double‐blind, placebo‐controlled parallel RCT. Location: multicentre ‐ 73 sites in 9 countries (USA, Australia and Europe). Clinical trials identifier: NCT00645788 |
Number: estimated enrolment 245, 288 randomised but only 286 received 1 of the 4 treatments. Age: 12 years and older (split children 12 ‐ 17 years and adults 18 years and over). Gender: males or females. Disease status: chronic colonisation with P aeruginosa, clinically stable. |
Intervention 1: 32.5 mg ciprofloxacin betaine corresponding to 50 mg ciprofloxacin Pulmonsphere inhalation powder 2x daily. Intervention 2: placebo (50 mg matching placebo powder formulation) 2x daily. Intervention 3: 48.75 mg ciprofloxacin betaine corresponding to 75 mg ciprofloxacin Pulmonsphere inhalation powder 2x daily. Intervention 4: placebo (75 mg matching placebo powder formulation) 2x daily. Interventions 3 and 4 were introduced after amendment 2. |
No significant difference in change in FEV1 between ciprofloxacin dry powder inhalation at either dose (P = 0.154). In pooled analyses, FEV1 decline from baseline to treatment end was significantly lower with ciprofloxacin DPI than with placebo (pooled data; P = 0.02). There were positive effects on sputum bacterial load and quality of life which weren't maintained in the 4‐week follow‐up. There were no significant differences in type/incidence of treatment‐emergent adverse events by treatment group (P = 0.115). |
| Dupont 2008 |
Duration: 28 days. Design: placebo‐controlled phase IIa parallel RCT (stratified by baseline FEV1 (% predicted) and randomised 2:1 to Arikace™ or placebo). Location: multicentre ‐ 13 centres in Europe. |
Number: 66 participants enrolled. Age: 23 adults, 25 adolescents (13 ‐ 18 years) and 18 children (6 ‐ 12 years). Gender: no details. Disease status: chronic P aeruginosa infection; baseline FEV1 (% predicted) 40 ‐ 75% in 43 participants; >75% in 23 participants. |
Cohort 1: (n = 32) 280 mg Arikace™ or placebo (hypertonic saline solution (1.5% NaCl)) once daily.
Cohort 2: (n = 34) 560 mg Arikace™ or placebo (hypertonic saline solution (1.5% NaCl)) once daily. Inhaled with PARI eFlow® nebuliser. |
Relative change in FEV1 was higher in the 560 mg group at day 28 (P = 0.033) compared to placebo. The adverse event profile was similar among Arikace™ and placebo groups. |
| Galeva 2013 |
Duration: 28 days. Design: placebo‐controlled parallel RCT. Location: multicentre ‐ 17 centres in 8 countries. |
Number: 62 randomised (target was 100). Age: 6 to 21 years. Gender: no details. Disease status: diagnosed with CF by at least 1 clinical feature plus sweat test, FEV1 of 25 ‐ 80% predicted. |
Intervention 1: TIP (n = 32) 112 mg 2x daily. Intervention 2: placebo (n = 30) 2x daily. |
Mean treatment difference in absolute change in FEV1 between TIP ‐ placebo was 4.4 % (P < 0.05). Mean treatment difference in relative change in FEV1 between TIP ‐ placebo was 5.9 % (P < 0.0.184). TIP significantly reduced sputum density. |
| Geller 2011b |
Duration: 28 days. Design: double‐blind, placebo‐controlled parallel RCT (3 arms). Location: multicentre ‐ 51 centres across USA and Europe. |
Number: 151 randomised. Age: mean age 29 years. Gender: 85 males, 66 females. Disease status: diagnosed CF, chronic P aeruginosa airways infection, FEV1 between 25 ‐ 85% predicted, and 3 courses of inhaled antibiotics over the past 12 months. |
Intervention 1: (n = 38) MP‐376 120 mg daily. Intervention 2: (n = 37) MP‐376 240 mg daily. Intervention 3: (n = 39) MP‐376 240 mg 2x daily. Intervention 4: (n = 37) placebo. Delivered by a customized investigational PARI eFlow nebulizer. |
All doses of MP‐376 resulted in reduced sputum density at day 28 (240 mg twice a day showed a 0.96 log difference compared with placebo P = 0.001) There was a dose‐dependent increase in FEV1 for MP‐376. There was a difference of 8.7 % in FEV1 between MP‐376 240 mg twice a day and placebo (P = 0.003). There was a significant reduction in the need for other anti‐pseudomonal antibiotics compared to placebo. |
| Gibson 2003 |
Duration: 28 days. Design: double‐blind, placebo‐controlled parallel RCT. Early termination due to poor recruitment. |
Number: 21 randomised (planned 98). Age: 6 months ‐ 6 years. Gender: 11 males, 10 females. Disease status: positive P aeruginosa culture. |
Intervention 1: (n = 8) tobramycin 300 mg 2x daily. Intervention 2: (n = 13) placebo 2x daily. |
There was a significant difference between treatment groups and placebo in the reduction in P aeruginosa density (no P aeruginosa was detected at day 28 in 8 out of 8 active group patients compared to 1 out of 13 placebo patients). There were no significant differences between treatment groups for clinical indices or adverse events. |
| Goss 2013 |
Duration: 28 days (with 28‐day follow‐up). Design: placebo‐controlled parallel phase 2 RCT (stratified by baseline FEV1 (% predicted) and randomised 2:1 to Arikace™ or placebo). Location: multicentre ‐ 18 centres across USA. |
Number: 46 randomised. Age: mean (SD) Arikace™ 70 mg: 33.1 (9.7) years. Arikace™ 140 mg: 35.4 (6.0) years. Placebo 70 mg and 140 mg: 24.4 (6.3) years Arikace™ 560 mg: 31.5 (14.5) years. Placebo 560 mg: 26.3 (6.7) years. Gender: 27 males, 19 females. Disease status: Cohorts 1 and 2: baseline FEV1 % predicted 40 ‐ 75% n = 16 and > 75% n = 5. Cohort 3: baseline FEV1 % predicted 40 ‐ 75% n = 19 and > 75% n = 6. More details on lung function and BMI in supplementary papers |
Arikace™ or placebo (hypertonic saline (1.5% NaCl). Cohort 1: (n = 14) 70 mg Arikace™ or placebo 1x daily. Cohort 2: (n = 12) 40 mg Arikace™ or placebo 1x daily. Cohort 3: (n = 22) 560 mg Arikace™ or placebo 1x daily. Inhaled using eFlow nebulizer system (PARI Pharma GmbH). Follow‐up for 28 days after trial finish. Review of interim data in combination with data from similar European trial led to addition of Cohort 3 for a further 28 days with follow‐up of 56 days after trial finish. |
Arikace™ was well tolerated at doses of 70 mg, 140 mg and 560 mg. |
| Hodson 2002 |
Duration: 28 days. Design: open‐label parallel RCT (stratified by age and centre). Location: multcentre. |
Number: 126 randomised, 11 withdrew before treatment, 115 treated. Age: range 7 ‐ 50 years. Gender: males 45% of total. Disease status: criteria for diagnosis abnormal sweat electrolytes, gene mutation. |
Intervention 1: tobramycin 300 mg in 5 mL 2x daily, delivered by Pari LC plus nebuliser with CR50 compressor. Intervention 2: colistin 1MU in 3 mL in saline 2x daily, delivered by Ventstream nebuliser with CR50 compressor. |
Tobramycin significantly improved lung function (mean improvement in FEV1 % predicted from baseline to week 4 was 6.7 % P = 0.006). The mean change in FEV1 % predicted was not significant in the colistin group (0.37 %). Both antibiotic regimes produced a significant decrease in sputum density, there was no development of highly resistant strains and the safety profile for both antibiotics was good. |
| Konstan 2010a |
Duration: total of 24 weeks, 3 cycles each of 28 days on treatment followed by 28 days off treatment (only cycle 1 was double‐blind and randomised, cycles 2 and 3 were open‐label extension phases in which all participants received the same treatment). Design: double‐blind, placebo‐controlled parallel RCT. Location; multicentre ‐ 38 centres in Europe, Latin America and USA. Clinical trials identifier: NCT00125346. Known as the EVOLVE Trial. Trial terminated after showing a statistically significant benefit of TIP. |
Number: 102 randomised, 95 received intended treatment, unclear in which group 7 withdrawals were from. Age: mean (SD): TIP 13.4 (4.42) years; placebo 13.2 (3.91) years. Gender: 42 males, 53 females. Disease status: baseline lung function (FEV1 % predicted) (mean (SD)): TIP 54.7 (18.89)%; placebo 58.5 (20.03)%. |
Intervention1: (n = 46) TIP 112 mg 2x daily. Intervention 2: (n = 49) placebo 2x daily. Cycle 1 (28 days on and 28 days off treatment or placebo). Cycles 2 and 3: open‐label cycles of TIP for all participants. |
TIP significantly improved FEV1 % predicted from baseline to day 28 (difference 13.3, 95% CI 5.31 to 21.28 P = 0.0016). TIP reduced sputum P aeruginosa density, respiratory related hospitalisation and anti‐pseudomonal antibiotic use. The most common adverse event was cough but the frequency was higher in the placebo group (26.5 %) versus TIP (13.0%). No evidence of ototoxicity or nephrotoxicity. |
| Lenoir 2007 |
Duration: 4 weeks followed by a 4‐week run‐out phase. Design: double‐blind, placebo‐controlled parallel RCT. Location: multicentre ‐ 13 sites in 4 countries. |
Number: 59 participants. Age: range 6 ‐ 30 years. Gender: 32 males, 27 females. Disease status: participants diagnosed with CF and P aeruginosa. |
Intervention 1: tobramycin 300 mg (Bramitob®) 2x daily. Intervention 2: placebo 2x daily. Active drug and placebo both delivered by Pari LC Plus nebuliser and Pari TurboBoy compressor. |
There was a significant increase in FEV1 from baseline in the tobramycin group but not in the placebo group (absolute difference 13.3% P = 0.003). Similar improvements were also seen for FVC in the tobramycin group. Adverse events were lower in the in the tobramycin group. Microbiological outcomes were significantly improved. |
| Mainz 2014 |
Duration: 28 days. Design: double‐blind placebo‐controlled parallel RCT. Location: multicentre ‐ 2 centres in Germany (Jena and Tuebingen). |
Number: 9 participants. Age: mean (SD): 22.4 (7.6) years; range 10.6 to 38.7 years. Gender: 6 males, 3 females. Disease status: diagnosed with CF by 2 positive sweat tests or genetic analysis (or both) and with chronic P aeruginosa colonisation. |
Intervention 1: 80 mg tobramycin daily. Intervention 2: placebo (isotonic saline). Sinonasal inhalation using PARI Sinus™ compressor with a PARI LC SPRINT STAR™ nebuliser. Drug administered to each nostril for 4 minutes with the other nostril occluded, maximum volume of 1 mL per nostril. |
P aeruginosa quantity decreased in 4 out of 6 (67%) participants receiving tobramycin and in none of the placebo group. Sinonasal inhalation was well tolerated. |
| Mazurek 2014 |
Duration: single cycle of 28 days on and 28 days off (8 weeks total duration). Design: parallel RCT (non‐inferiority trial). Location: multicentre ‐ 38 centres in Europe. Clinical trials identifier: NCT00885365. Follow‐on 48 week extension of TNS4 only: ClinicalTrials ID: NCT01111383. |
Number: 406 individuals screened, 324 participants randomised. Age: mean (SD): TNS4 15.89 (6.25) years; TNS5 15.58 (7.31) years. Gender: no details. Disease status: diagnosed with CF. Chronic P aeruginosa infection and FEV1 ≥ 40% and ≤ 80% predicted. |
Intervention 1: (n = 156) TNS4 (Bramitob®) 300 mg/4 mL 2x daily. Intervention 2: (n = 168) TNS5 (TOBI®) 300 mg/5 mL 2x daily. Both interventions delivered via PARI Boy N® compressor and the PARI LC Plus® nebuliser. Other standard therapies allowed. |
TNS4 showed similar short‐term clinical benefits to TNS5. Adverse event reporting was similar between the 2 treatment groups. |
| McCoy 2008 |
Duration: 4 weeks. Design: double‐blind, placebo‐controlled parallel RCT. Location: multicentre ‐ 56 centres in USA. |
Number: 246 participants randomised; 173 completed 28‐day treatment phase; and 90 completed open‐label follow‐up for 56 days. Age: 7 to 65 years. Gender: 121 males. Disease status: documented diagnosis of CF and P aeruginosa, 3 or more courses of tobramycin in previous year, FEV1 between 25 and 75% predicted. |
Intervention 1: aztreonam 75 mg for 4 weeks, 2x or 3xdaily. Intervention 2: placebo (5 mg lactose in 1mL 0.17% NaCl) for 4 weeks, 2x or 3x daily. |
AZLI treatment increased the median time to need for additional anti‐pseudomonal antibiotics by 21 days compared to placebo (AZLI 92 days; placebo 71 days P = 0.007). AZLI improved mean CFQ‐R respiratory scores (P = 0.02) and sputum density (P = 0.006. Adverse events were reported in both groups but were consistent with CF lung disease. |
| Nasr 2006 |
Duration: 28 days. Design: double‐blind, placebo‐controlled parallel RCT. Location: single centre in USA. |
Number: 32 people with CF (31 completed). Age: mean (SD) and range ‐ TSI group 11.81 (7.46) years, 6.0 to 34.7 years; placebo group 15.86 (7.25) years, 7.4 to 28.8 years. Gender: 12 males, 20 females ‐ TSI group 6 males and 10 females, placebo group 6 males and 10 females. Disease status: CF diagnosis by sweat test or genotype testing. Colonised with P aeruginosa. Lung function FEV1 % predicted mean (SD) and range: TSI group 95.73 (17.21)%, 55.0% to 134.1%; placebo group 83.71 (21.07)%, 45.0% to 108.73%. |
Intervention 1: (n = 16) TSI 5 mL (solution of 300 mg tobramycin and 11.25 mg sodium chloride in sterile water) 2x daily. Intervention 2: (n = 16) placebo (solution of 1.25 quinine sulphate in normal saline) 2x daily. Interventions both administered using PARI LC Plus™ jet nebuliser and PulmoAide compressor. |
% predicted FEV1 increased slightly for both groups by mean (SD) 1.29 (3.33) for TSI and 1.17 (1.4) for placebo. |
| Ramsey 1993 |
Duration: 3x 28‐day periods (only results of first 28‐day parallel group comparison suitable for analysis). Design: double‐blind placebo‐controlled 3‐period cross‐over RCT. |
Number: 71 participants. Age: mean (SD): 17.7 (1.25) years and 16.6 (1.24) years in 2 groups. Gender: 37 males, 34 females. Disease status: CF diagnosed by sweat test. Sputum culture of P aeruginosa susceptible to tobramycin. Mean baseline FEV1 55% (SE 3.7) and 60% (SE 3.2) predicted in 2 treatment arms. |
Intervention 1: tobramycin 600 mg 3x daily for 28 days, then cross‐over for 2 further 28‐day periods. Intervention 2: placebo (0.5 normal saline) 3x daily for 28 days, then cross‐over for 2 further 28‐day periods. Delivered by Ultrasonic (Ultraneb 100/99) nebuliser with 30 mL solution and 200 inhalations. |
In the first 28‐day period there was an increase in % predicted FEV1 compared to placebo (P < 0.001) and FVC (P = 0.014). There was a decrease in the density of P aeruginosa in sputum (P < 0.001). |
| Retsch‐Bogart 2007 |
Duration: 28 days. Design: double‐blind, placebo‐controlled parallel Phase III RCT. Location: multicentre: 53 centres in USA, Canada, Australia and New Zealand. Clinical trials identifier: NCT00112359. Known as AIR‐CF1 Trial. |
Number: 164 participants. Age: mean (range)): AZLI 27.4 (7 – 54) years; placebo 31.7 (11 – 74) years. Gender: 93 males, 71 females. Disease status: stable condition. P aeruginosa in sputum or throat swab. No use of anti‐pseudomonal antibiotics in previous 14 days. Baseline lung function (FEV1 % predicted) (mean (SD)): AZLI 54.4 (13.4)%; placebo 54.8 (14.0)%. |
Intervention 1: AZLI 75 mg 3x daily. Intervention 2: placebo 3x daily. Doses administered at least 4 hours apart using PARI eFlow™ Electronic Nebuliser after pre‐treatment with bronchodilator. Concommitant standard CF therapies allowed except anti‐pseudomonal antibiotics, azithromycin or hypertonic saline. |
AZLI improved FEV1 % predicted (P < 0.001), CFQ‐R respiratory score (P < 0.001) and sputum P aeruginosa density (P < 0.001) compared to placebo. Adverse events were comparable between groups with the exception of productive cough. This outcome was reduced by half in AZLI‐treated participants. |
| Rietschel 2009 |
Duration: 20 weeks in total (8 weeks intervention 1, followed by 4 week washout, followed by 8 weeks intervention 2). Design: cross‐over. Location: multicentre in Germany. |
Number: 35 stated as randomised in first abstract, but 29 randomised and 24/29 as having completed in second abstract. Age: 6 years and over, mean (SD) age 19.8 (6.3) years, range 8 ‐ 35 years. Disease status: chronically infected with P aeruginosa. |
Intervention 1: continuous TIS 300 mg/d 1x daily. Intervention 2: continuous TIS 300 mg/d 2x daily. |
Mean FEV1 was not markedly different between treatment periods or from baseline. No audiological or nephrotoxic side effects were noted. Once or twice daily dose was shown to be safe and tolerable. |
| Sands 2014 |
Duration: 3 months in total, but only 4 weeks taking each intervention (4 weeks intervention 1, 4 weeks washout period, 4 weeks intervention 2). Design: Cross‐over. Location: multicentre in Poland. |
Number: 58 randomised, 54 in ITT population Age: 4 years and older. Mean (SD) age 15.4 (6.81) years, range 7 to 36 years. Gender: 25 males, 33 females. Disease status: mean (SD) FEV1 % predicted: VANTOBRA group 63.8 (17.1)%, range 30.0% to 82.8%; TIS group 64.2 (17.7)%, range 28.0% to 83.9%. |
Intervention 1 (n = 28): T100 also known as VANTOBRA (170 mg tobramycin in 1.7 mL solution) via drug‐specific eFlow nebuliser Tolero with an eBase controller 2x daily. Intervention 2 (n = 30): TOBI (300 mg tobramycin in 5 mL solution) via PARI LC Plus nebuliser with PARI BOY SX compressor 2x daily. |
Treatment with both products were comparable in terms of clinical efficacy (reduction of P aeruginosa density and improvement in lung function. Safety profiles were also comparable. |
| Trapnell 2012 |
Duration: 28 days. Design: placebo‐controlled parallel RCT. Location: multicentre ‐ 33 sites in the USA. |
Number: 119 participants randomised. Age: mean (SD)): FTI 80/20mg 35 (10.9) years; FTI 160/40mg 31 (10.2) years; placebo 31 (8.8) years. Gender: 68 males, 51 females. Disease status: lung function (FEV1 % predicted) (mean (SD)): FTI 80/20mg 50 (13.4)%; FTI 160/40mg 21 (51)%; placebo 48 (13.6)%. |
Intervention 1: (n = 38) FTI 80/20 mg 2x daily. Intervention 2: (n = 41) FTI 160/40 mg 2x daily. Intervention 3: (n = 40) placebo 2x daily. |
Improvements in mean FEV1 % predicted achieved in the AZLI run‐in period were maintained in the FTI group compared with placebo (P = 0.002). The treatment effect on P aeruginosa sputum density significantly favoured FTI compared to placebo. Respiratory symptoms were less common in the FTI group. |
| Wainwright 2011 | Duration: 28 days. Design: placebo‐controlled parallel RCT. Location: multicentre ‐ 40 centres in USA, Canada and Australia. |
Number: 160 people randomised, 157 received treatment. Age: mean (SD): AZLI 19.5 (9.1) years; placebo 18.9 (9.1) years. Gender: 90 males, 70 females. Disease status: FEV1 % predicted: AZLI 95.5 (12.7)%; placebo 94.7 (12.9)%. |
Intervention 1: (n = 76; 75 analysed, 1 discontinued trial) AZLI (75 mg aztreonam, 52.5 mg lysine monohydrate diluted in 0.17% saline (1 mL)) 3x daily. Intervention 2: (n = 81) placebo (5 mg lactose, 7.3 mg NaCl diluted in 0.17% saline (1 mL)) 3x daily. Both interventions self‐administered with the investigational eFlow® electronic nebulizer (PARI GmbH, Starnberg, Germany). |
Treatment effect at 28 days for relative FEV1 % predicted was 2.7 % (P = 0.021 favouring AZLI). Treatment effect for CFQ‐R respiratory symptom score at day 28 was modest at 1.8 points (95% CI ‐2.8 to 6.4 P = 0.443). Sputum density was improved in the AZLI group (P = 0.016). |
AZLI: aztreonam lysine for inhalation. CF: cystic fibrosis. FEV1: forced expiratory volume in one second. FTI: fosfomycin/tobramycin for inhalation. ITT: intention to treat. P aeruginosa: Pseudomonas aeruginosa. RCT: randomised controlled trial. SD: standard deviation. SE: standard error. TIP: tobramycin inhalation powder.
Studies awaiting classification
There are four trials listed as 'Studies awaiting classification'. Three trials are only presented in abstract or trial registration form and there is insufficient information to be able to include them at this stage (EUCTR2007‐004277‐26‐NL; Herrmann 2017; NCT03341741). EUCTR2007‐004277‐26‐NL compares inhaled aztreonam with nebulised tobramycin over 28‐day cycles, but results have not yet been published, although the trial is completed. The other two trials compare 28‐day cycles of inhaled tobramycin in combination with colistin alone; we are unclear of the duration of the trials at this stage (Herrmann 2017; NCT03341741). The final trial is a three‐arm parallel comparison of TIS, Bramitob and inhaled colistin (Nikonova 2010). In this trial treatment duration is not clear and some participants have chronic infection and some had initial isolates of P aeruginosa.
Risk of bias in included studies
We present a summary of the risk of bias found across all included trials (Figure 2) and describe the risks in the tables (Characteristics of included studies).
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
A total of 11 trials compared an inhaled anti‐pseudomonal antibiotic to placebo or to usual treatment (Chuchalin 2007; Day 1988; Hodson 1981; Jensen 1987; Kun 1984; MacLusky 1989; Murphy 2004; Nathanson 1985; Ramsey 1999; Stead 1987; Wiesemann 1998). Seven trials compared different inhaled anti‐pseudomonal antibiotics (Assael 2013; Bilton 2020; Elborn 2015; Konstan 2010b; Nikolaizik 2008; Schuster 2013; Stead 1987). Only one trial compared continuous inhaled anti‐pseudomonal antibiotics to intermittent inhaled anti‐pseudomonal antibiotics (Flume 2016b).
Allocation
Inhaled anti‐pseudomonal antibiotic compared to placebo or to usual treatment
Generation of sequence
In one trial, the treatment sequence in the cross‐over design used a 'Latin square' method and therefore has a low risk of bias (Stead 1987).
Five trials stated only that generation of allocation sequence was randomised, and so we rated these as having an unclear risk of bias (Chuchalin 2007; Hodson 1981; Jensen 1987; Murphy 2004; Ramsey 1999). In two further trials randomisation was not described, and we also rated these as having an unclear risk of bias (Day 1988; Nathanson 1985).
In three trials the method of generating the allocation sequence has a high risk of bias as a coin toss or chance was used for randomisation of only the first participant (Kun 1984; MacLusky 1989; Wiesemann 1998).
Concealment of allocation
One trial which used alternate allocation had a low risk of bias for allocation concealment as a trial nurse was responsible for randomisation and the trial physician was reported to be blind to treatment allocation throughout the trial (MacLusky 1989). In eight trials, the concealment of the allocation schedule was not described, and so we judged these trials to have an unclear risk of bias (Chuchalin 2007; Day 1988; Hodson 1981; Jensen 1987; Murphy 2004; Nathanson 1985; Ramsey 1999; Stead 1987). We rated two trials which allocated participants to alternate groups, as having a high risk of bias with regard to the concealment of treatment allocation schedule as it could be foretold which treatment the next participant would be allocated to (Kun 1984; Wiesemann 1998).
Inhaled anti‐pseudomonal antibiotics compared
Generation of sequence
We judged two trials to have a low risk of bias (Assael 2013; Stead 1987). One trial used an interactive voice or web response system using a code generated by the pharmaceutical company sponsoring the trial (Assael 2013); the second trial generated the treatment sequence in the cross‐over design using a Latin square method (Stead 1987). The method of allocation in the remaining five trials was not described in detail leading to an unclear risk of bias (Bilton 2020; Elborn 2015; Konstan 2010b; Nikolaizik 2008; Schuster 2013).
Concealment of allocation
One trial used an interactive voice or web response system and so had a low risk of bias (Assael 2013). None of the remaining six trials commented on the treatment allocation schedule, and so we rated all as having an uncertain risk of bias (Bilton 2020; Elborn 2015; Konstan 2010b; Nikolaizik 2008; Schuster 2013; Stead 1987).
Continuous inhaled anti‐pseudomonal antibiotics versus intermittent inhaled anti‐pseudomonal antibiotics compared
Generation of sequence
We judged the trial to have an unclear risk of bias because although eligible participants were stratified by disease severity and number of acute respiratory exacerbations and randomised 1:1, the method of randomisation was not described (Flume 2016b).
Concealment of allocation
There was no description of allocation concealment, and so we rated the trial as having an uncertain risk of bias (Flume 2016b).
Blinding
Inhaled anti‐pseudomonal antibiotic compared to placebo or to usual treatment
We judged three trials to have a low risk of performance bias (blinding of participants and clinicians) as they attempted to mask the taste of the antibiotic solutions (although it is possible that this may not have been achieved adequately); two trials reported using quinine to attempt to mask nebulised solutions adequately (Chuchalin 2007; Ramsey 1999) and one used the tobramycin preservative solution to saline as the placebo (Wiesemann 1998). We judged five trials to have an unclear risk of bias ‐ four of these were described as being double‐blind, but no further details were given (Day 1988; Hodson 1981; Jensen 1987; Nathanson 1985) and one did not give any details (Stead 1987). Three trials had a high risk of bias ‐ one trial stated that only trial physicians were blinded (MacLusky 1989), in one trial the participants and clinicians were not blinded since one group received treatment prior to physiotherapy and the second group received treatment both before and after physiotherapy (Kun 1984) and the third trial was described as open‐label (Murphy 2004).
With regard to detection bias (blinding of outcome assessors), two trials had a low risk of bias as they specified that outcome assessors were blinded (Kun 1984; MacLusky 1989). Eight trials had an unclear risk of bias ‐ seven of these were described as double‐blind but gave no details of who exactly had been blinded to treatment (Chuchalin 2007; Day 1988; Hodson 1981; Jensen 1987; Nathanson 1985; Ramsey 1999; Wiesemann 1998) and one trial did not give any details at all (Stead 1987). One trial was open‐label and had a high risk of bias for the blinding of outcome assessors (Murphy 2004).
Inhaled anti‐pseudomonal antibiotics compared
There was a high risk of performance bias (blinding of participants and clinicians) in four trials which were described as open‐label (Assael 2013; Konstan 2010b; Nikolaizik 2008; Schuster 2013;) and in two trials which used different treatment schedules (Bilton 2020) or explicitly stated that participants were not blinded (Elborn 2015). The Stead trial was partially‐blinded with one of the treatment arms being open, but the remaining treatment arm and placebo arm being blind to participants and investigators leading to a judgement of an unclear risk of bias (Stead 1987).
There was a high risk of detection bias (blinding of outcome assessors) in three open‐label trials (Assael 2013; Konstan 2010b; Nikolaizik 2008). The risk of bias was judged to be unclear due to a lack of information in two trials (Bilton 2020; Stead 1987). A further two trials specifically stated that the outcome assessors were blinded, and we judged them to have a low risk of detection bias (Elborn 2015; Schuster 2013).
Continuous inhaled anti‐pseudomonal antibiotics versus intermittent inhaled anti‐pseudomonal antibiotics compared
The authors report the trial as double‐blind and say that both participants and investigators are blinded. No further description of blinding is given therefore we have deemed this domain to be at an unclear risk of bias (Flume 2016b).
There was, however, a low risk of detection bias (blinding of outcome assessors) due to there being an independent, blinded adjudication committee to review outcome data.
Incomplete outcome data
Inhaled anti‐pseudomonal antibiotic compared to placebo or to usual treatment
The proportion of participants enroled who were not available for analysis varied from 0.8% (2 out of 247) (Chuchalin 2007) to 65% (118 of 181) (Murphy 2004).
Two trials stated the use of an ITT analysis, and we rated these as having a low risk of bias (Chuchalin 2007; Ramsey 1999). In seven trials, we judged the risk of bias from incomplete outcome data to be unclear (Hodson 1981; Jensen 1987; Kun 1984; MacLusky 1989; Murphy 2004; Stead 1987; Wiesemann 1998). In one of these, a parallel group trial, there was marked inequality in dropouts between the placebo group (9 out of 20) and the active treatment group (2 out of 20) (Jensen 1987).
Two trials did not state the number of participants enroled but not analysed, and therefore we rated these as having a high risk of bias (Day 1988; Nathanson 1985).
Inhaled anti‐pseudomonal antibiotics compared
Withdrawal rates (with full reasons) were given in the full reports for six trials and therefore indicates a low risk of bias (Assael 2013; Bilton 2020; Elborn 2015; Konstan 2010b; Schuster 2013; Stead 1987). In a further trial, the number of participants randomised was not stated, and therefore the dropout rate is unknown; we judged this trial to have an unclear risk of bias (Nikolaizik 2008).
Continuous inhaled anti‐pseudomonal antibiotics versus intermittent inhaled anti‐pseudomonal antibiotics compared
The withdrawal rate (with full reasons) was given for the trial but more than 15% of randomised participants failed to complete the trial, so we rated this domain as having an unclear risk of bias (Flume 2016b).
Selective reporting
Inhaled anti‐pseudomonal antibiotic compared to placebo or to usual treatment
Protocols were not available for the included trials, therefore we based our assessment upon the information in the trial reports and related abstracts. Three trials appeared free of selective reporting as all outcomes stated in the methods section were reported, and we rated these as having a low risk of bias (Kun 1984; MacLusky 1989; Stead 1987). We rated the risk of bias from selective reporting as unclear for four trials (Chuchalin 2007; Hodson 1981; Jensen 1987; Nathanson 1985). We judged the remaining four trials to have a risk of selective reporting as the results for outcomes stated in the methods section were either not reported at all or only partially reported (e.g. P value only) (Day 1988; Murphy 2004; Ramsey 1999; Wiesemann 1998).
It should be noted that there are a number of methods of expressing FEV1 as a parameter of lung function and of measuring rates of exacerbations, hospitalisation and additional antibiotic use. This raises the possibility that analyses were performed in a number of ways of expressing these outcomes and non‐significant results not reported.
Inhaled anti‐pseudomonal antibiotics compared
Six trials appear free of selective reporting based on the information taken from the trial reports, and we judged these to have a low risk of bias (Assael 2013; Bilton 2020; Elborn 2015; Konstan 2010b; Schuster 2013; Stead 1987). One trial measured oxygen saturation and sputum bacteriology, but did not report the results, giving a high risk of bias (Nikolaizik 2008).
Continuous inhaled anti‐pseudomonal antibiotics versus intermittent inhaled anti‐pseudomonal antibiotics compared
We deemed the Flume trial to be free of selective reporting bias as all the outcomes reported in the methods are subsequently reported in the results. We were also able to access the trial registration documentation to check that outcomes reported at the protocol stage were included in the full report (Flume 2016b).
Inhaled anti‐pseudomonal antibiotic compared to placebo or to usual treatment
With regard to publication bias, it was not possible to produce a funnel plot as we could not include 10 trials in any single meta‐analysis. We assessed outcome reporting bias by comparing the methods sections to the results sections for all articles as protocols were not available (see above). One trial had early termination for benefit (Murphy 2004), which may overestimate benefit (Montori 2005). Five trials reported pharmaceutical company support (Chuchalin 2007; Hodson 1981; Kun 1984; Murphy 2004; Stead 1987). Four trials were of cross‐over design with insufficient information regarding analysis, washout periods and carryover effects and therefore had an uncertain risk of bias (Day 1988; Hodson 1981; Kun 1984; Nathanson 1985).
Inhaled anti‐pseudomonal antibiotics compared
There were no additional sources of bias identified for two trials which we therefore considered to have a low risk of bias (Bilton 2020; Elborn 2015). Two trials had an unclear risk of bias on account of their cross‐over design coupled with insufficient information regarding washout periods, carryover effects and analysis (Nikolaizik 2008; Stead 1987). Five trials had a risk of bias due to reported pharmaceutical company support (Assael 2013; Konstan 2010b; Nikolaizik 2008; Schuster 2013; Stead 1987).
Continuous inhaled anti‐pseudomonal antibiotics versus intermittent inhaled anti‐pseudomonal antibiotics compared
Trial enrolment was limited for the trial, and it was therefore underpowered and at an unclear risk of bias for this domain (Flume 2016b).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7; Table 8
Not all outcomes reported results that can be analysed. Pooling of results for analysis is not possible for most outcomes because of differences in trial duration, methods of measuring and expressing results of the outcome and because of missing estimates of variance. A major problem was the high proportion of cross‐over trials, six out of 18 included trials. There must be doubt about the suitability of this design for trials of antibiotic treatment in people with CF (see 'Discussion'). Despite this doubt we have included such trials in the review. They are excluded from meta‐analyses unless the first‐period parallel group comparison was available. Outcomes not reported by any trial in a comparison are not listed below; we only present those outcomes that have been reported in the included trials.
The effects of interventions are summarised in the summary of findings tables, the certainty of the evidence has been graded for pre‐defined outcomes (see above) and definitions of these gradings provided (Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7; Table 8).
Inhaled anti‐pseudomonal antibiotics compared to placebo
Please refer to Table 1.
Primary outcomes
1. Lung function
a. FEV1
All 11 trials (n = 1130) reported on FEV1 (Chuchalin 2007; Day 1988; Hodson 1981; Jensen 1987; Kun 1984; MacLusky 1989; Murphy 2004; Nathanson 1985; Ramsey 1999; Stead 1987; Wiesemann 1998). Trials reported FEV1 using in different units of measurement and most lacked information needed for a meta‐analysis.
The analysis of data for FEV1 % predicted (absolute values) did not differ between groups in one trial (n = 29) at three months, MD ‐2.00% (95% CI ‐22.41 to 18.41) or in a further trial (n = 245) at up to one year, MD 3.10 (95% CI ‐2.35 to 8.55) (Analysis 1.1). Two trials reported simply that FEV1 % predicted was "not significantly different" between groups at three months (no data) (Nathanson 1985; Wiesemann 1998).
1.1. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 1: Mean absolute FEV1 (% predicted)
Two trials reported the mean change in FEV1 % predicted (Chuchalin 2007; Jensen 1987). At three months, the Jensen trial (n = 29) reported no difference in the mean change between inhaled antibiotics and placebo, MD 6.00% (95% CI ‐1.07 to 13.07) (Analysis 1.2). Chuchalin (n = 247) showed there to be a greater change in FEV1 after tobramycin than placebo, with a 6.38% difference between groups (95% CI 2.94 to 9.82) (Analysis 1.3) (Figure 3). The largest trial (n = 520) reported a 10% mean increase in FEV1 % predicted in the tobramycin group compared to a 2% mean decrease in FEV1 % predicted in the control group after 20 weeks (P < 0.001) (Ramsey 1999). A further trial (n = 33) reported that the difference in the change in FEV1 % predicted between groups was statistically significant, but provided no data for analysis (Kun 1984). One trial (n = 14) reported within‐group differences in FEV1 % predicted narratively, but did not report between‐group differences at the end of treatment (Day 1988).
1.2. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 2: Mean change in FEV1 (% predicted)
1.3. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 3: Mean change in % predicted FEV1
3.

Two trials lasting over 12 months reported the rate of decline in FEV1 as the primary endpoint (MacLusky 1989; Murphy 2004). In the MacLusky trial (n = 27), the difference in rate of change of FEV1 % predicted per year favoured inhaled antibiotics, MD 7.80% (95% CI 3.29 to 12.31) (Analysis 1.4). The second trial (n = 181) reported no difference in FEV1 decline; but in this trial only 57% of participants had the minimum number of measurements (Murphy 2004).
1.4. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 4: Rate of change of FEV1 (% predicted per year)
Two reports (n = 38) stated that the differences between groups (one measuring FEV1 in mL and one in L) were "statistically significant", but provided no data (Hodson 1981; Stead 1987).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 1).
b. FVC
A result for FVC was reported in 10 trials (n = 1097) (Chuchalin 2007; Day 1988; Hodson 1981; Jensen 1987; MacLusky 1989; Murphy 2004; Nathanson 1985; Ramsey 1999; Stead 1987; Wiesemann 1998). Again, trials reported FVC in different units and usually lacked information needed for meta‐analysis.
The Jensen trial (n = 29) reported absolute values for FVC % predicted at three months; the results were not different between the groups, MD 8.00 (95% CI ‐12.18 to 28.18) (Analysis 1.5). Day (n = 14) reported that FVC % predicted was "significantly greater" in the antibiotic group (74.0%) than the control group (67.5%) at the end of the trial (six months) (P < 0.05); no further data were provided, therefore we are unable to present the results from this cross‐over trial in the analysis (Day 1988). One 12‐month trial (n = 22) reported no difference in FVC % predicted between the treatment and control groups (Wiesemann 1998).
1.5. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 5: Mean absolute FVC (% predicted) at end of treatment
Data from the Jensen trial (n = 29) showed that the change in FVC % predicted at three months was greater for inhaled antibiotics compared to placebo, MD 11.00 (95% CI 1.94 to 20.06) (Jensen 1987) (Analysis 1.6). Data from the Chuchalin trial (n = 245) at up to 12 months also reported a difference in favour of the antibiotic group, MD 4.60 (95% CI 1.01 to 8.19) (Chuchalin 2007) (Analysis 1.6) (Figure 4). Ramsey was the largest trial (n = 520), but did not present any data we were able to analyse; at 20 weeks investigators reported a greater change in FVC % predicted in the antibiotic group (8%) compared to the control group (‐1%) (Ramsey 1999).
1.6. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 6: Mean change in FVC (% predicted)
4.

Forest plot of comparison: 1 Inhaled anti‐pseudomonal antibiotic versus placebo, outcome: 1.6 Mean change in FVC (% predicted).
Two trials had a duration of more than 12 months and measured the rate of decline of FVC % predicted (MacLusky 1989; Murphy 2004). In one trial (n = 27), the difference in rate of change of FVC % predicted per year favoured antibiotics, MD 5.40 (95% CI 0.86 to 9.94) (Analysis 1.7) (MacLusky 1989). In the remaining trial (n = 181), it was reported that no difference was found between groups, but only 57% of participants in the Murphy trial had the minimum number of measurements for analysis (Murphy 2004).
1.7. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 7: Rate of change of FVC (% predicted per year)
Nathanson and Stead measured FVC in L (Nathanson 1985; Stead 1987). Nathanson (n = 7) reported no difference between groups at three months (end of trial) (Nathanson 1985). Stead (n = 18) used different antibiotics compared to placebo in a three‐arm cross‐over trial and values for FVC were higher during each of the four‐month active treatment arms than when taking placebo; results were greater for the combination of gentamicin and carbenicillin compared to placebo, but not for ceftazidime compared to placebo (Stead 1987). Hodson reported the mean FVC in mL over six months; this was higher during antibiotic treatment for 16 out of 17 participants, for seven of these participants the difference was "significant" (Hodson 1981).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 1).
2. Exacerbation of respiratory infection
a. Hospital admissions
Hospital admission was measured in six trials (n = 1008), but reported using different methods or scores (Chuchalin 2007; Day 1988; MacLusky 1989; Murphy 2004; Ramsey 1999; Stead 1987). Where possible, data have been entered into the analysis (Analysis 1.8).
1.8. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 8: Frequency of one or more hospital admissions
Three trials (n = 946) reported data at over three months and up to 12 months (Chuchalin 2007; Murphy 2004; Ramsey 1999). When these were combined, data show a lower risk of one or more hospital admissions for the antibiotic group, RR 0.66 (95% CI 0.47 to 0.93) (Analysis 1.8). This analysis showed heterogeneity between the three included trials (I2 = 57 %), but they all favoured inhaled antibiotics compared to placebo. All three trials investigated the same drug (tobramycin) at the same dose (300 mg) in four‐week on‐off cycles with a jet nebuliser and air compressor. Severity of disease at baseline was greatest in the Ramsey trial which had a lower risk ratio for hospital admissions than the other two trials and this may be the cause of heterogeneity (Ramsey 1999). Two trials (n = 14) reporting hospital admission were cross‐over in design; one reported hospital admissions were "similar" (Day 1988) and the remaining trial (n = 18) reported that four out of five hospital admissions were during the four‐month placebo period (Stead 1987).
Neither of the longer trials reported differences between groups for the risk of one or more hospital admissions; in one trial (n = 181) at over 12 months and up to two years, RR 0.59 (95% CI 0.34 to 1.05) (Murphy 2004) and in the second (n = 27) at 32 months, RR 0.80 (95% CI 0.39 to 1.65) (MacLusky 1989) (Analysis 1.8).
We rated the certainty of the evidence for this outcome in our GRADE analysis as low due to the risk of bias within the trials, particularly with regard to randomisation, allocation concealment and blinding (Table 1).
b. Days in hospital
Four trials (n = 762) reported days in hospital in some form (Kun 1984; MacLusky 1989; Murphy 2004; Ramsey 1999), but only data from the longest trial (n = 28) could be analysed (MacLusky 1989). MacLuskey reported no difference between the antibiotic group (10.3 days) and the control group (13.5 days) at 32 months, MD ‐3.20 days (95% CI ‐9.04 to 2.64) (Analysis 1.9). Of the remaining trials, the largest trial (n = 520) reported that at six months the average number of days of hospitalisation in the treatment group was 5.1 and 8.1 in the control group (Ramsey 1999). In a two‐year cross‐over trial (n = 33), Kun reported fewer hospital inpatient days in the treatment group (15 days (range (0 to 68)) compared to the control group (26 days (range 0 to 92)) (Kun 1984). Murphy (n = 181) reported that the number of annualised days in hospital was similar for treatment (4.6 days per year) and control (4.5 days per year) groups (Murphy 2004).
1.9. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 9: Hospital admissions, mean number of days in hospital
Our GRADE analysis assessed the certainty of the evidence for this outcome to be very low due to high or unclear risks of bias within the trials and inconsistency of outcome measurement.
c. Courses of intravenous antibiotics
Six trials (n = 1023) reported information relevant to this outcome (Chuchalin 2007; Hodson 1981; Kun 1984; Murphy 2004; Ramsey 1999; Wiesemann 1998), but only three (n = 940) provided data for the analysis (Chuchalin 2007; Murphy 2004; Ramsey 1999).
Four trials (n = 968) reported the frequency of courses of intravenous antibiotics during the trial (Chuchalin 2007; Hodson 1981; Murphy 2004; Ramsey 1999). Combined data at over three and up to 12 months from two of these trials (n = 765) favoured inhaled antibiotics, RR 0.77 (95% CI 0.67 to 0.88) (Chuchalin 2007; Ramsey 1999) (Analysis 1.10). In contrast, data from one trial (n = 181) at over 12 months showed no difference, RR of 0.62 (95% CI 0.35 to 1.08) (Murphy 2004) (Analysis 1.10).
1.10. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 10: Frequency of one or more courses of intravenous antibiotics
The Hodson cross‐over trial (n = 20) reported that over six months the treatment group had three courses of antibiotics compared to seven in the control group (Hodson 1981).
Furthermore, one trial (n = 22) reported the need for intravenous antibiotics as the cause of withdrawal from the trial in two out of 11 participants using placebo (Wiesemann 1998). The final trial reporting on this outcome, provided an antibiotic score of uncertain validity which we have not presented here (Kun 1984).
GRADE analysis for this outcome showed the certainty of the evidence to be very low due to risk of bias within the trials and inconsistency of results (Table 1).
d. Pulmonary exacerbations
i. Frequency
One trial (n = 245) reported the frequency of pulmonary exacerbations, but did not give a definition of a pulmonary exacerbation used (Chuchalin 2007). After 24 weeks 39.8% of the tobramycin group and 51.2% of the control group had experienced at least one exacerbation; this result showed no difference between treatment and placebo, RR 0.78 (95% CI 0.59 to 1.03) (Chuchalin 2007) (Analysis 1.11).
1.11. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 11: Pulmonary exacerbations
GRADE deemed the certainty of the evidence to be very low due to the risk of bias within the trial and imprecision due to low participant numbers and only one trial measuring the outcome (Table 1).
Secondary outcomes
1. Nutrition
b. Weight
Four trials (n = 460) reported an increase in weight with antibiotic treatment, but did not have results available for meta‐analysis (Chuchalin 2007; Day 1988; Murphy 2004; Stead 1987); two of these were of cross‐over design (Day 1988; Stead 1987). Murphy also reported that the control group gained weight as well and there were no between‐group differences (Murphy 2004).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be very low due to risk of bias being high or unclear in the underlying trials and there being no data available for meta‐analysis (Table 1).
2. QoL
One trial (n = 245) reported significantly fewer lost school or working days in the tobramycin‐treated group than in the placebo control group, MD ‐5.30 (95% CI ‐8.59 to ‐2.01) (Analysis 1.12) (Chuchalin 2007). Murphy (n = 181) also reported on this outcome and found no difference between the treatment and control groups in the number of school days missed due to illness (Murphy 2004).
1.12. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 12: Lost school or working days
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 1).
3. Survival
Four trials reported on this outcome (n = 828) (Chuchalin 2007; Kun 1984; MacLusky 1989; Ramsey 1999). Nine deaths were reported in three parallel‐group trials with 795 participants (Chuchalin 2007; MacLusky 1989; Ramsey 1999). There were no differences in two trials (n = 767) at over three and up to 12 months, RR 0.17 (95% CI 0.03 to 1.09) or in one trial (n = 27) at over 24 months and up to 36 months, RR 0.27 (95% CI 0.01 to 6.11) (Analysis 1.13). In addition, Kun reported two deaths in 33 participants from a cross‐over design trial. These deaths occurred at three and six months after changing from gentamicin to the saline mixture (Kun 1984).
1.13. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 13: Deaths
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low, particularly due to low event rates (Table 1).
4. Antibiotic resistance in P aeruginosa or other organisms
a. Antibiotic‐resistant P aeruginosa
Three parallel‐design trials (n = 795) measured the MIC of tobramycin for isolates of P aeruginosa (Chuchalin 2007; MacLusky 1989; Ramsey 1999). Chuchalin (n = 247) reported that the frequency of isolates of mucoid strains of P aeruginosa (about 60 % of all participants) having an MIC90 greater than 16 mcg/mL for tobramycin changed from 9.7% to 23.6% in the tobramycin group and from 17% to 18.2% in the control group after 24 weeks (Chuchalin 2007). However, the different baseline rate should be noted which may indicate that the change post‐treatment may not be attributable to the treatment. Ramsey (n = 520) reported that the proportion of isolates of P aeruginosa resistant to tobramycin increased from 13% to 23% in the tobramycin group and decreased from 10% to 8% in the control group between Week 0 and Week 24 of the trial; the RR for frequency of tobramycin resistance at end of trial was "significant", RR 2.93 (95% CI 1.75 to 4.91) (Burns 1999; Ramsey 1999). When combined for the time‐point over three months and up to 12 months, while these data (n = 672) favoured the control group they did not show a result, RR 1.95 (95% CI 0.86 to 4.42) (Analysis 1.14). The I2 value showed that there was moderate heterogeneity between these two trials (I2 = 79 % ) with the Ramsey trial having a higher frequency of tobramycin‐resistant P aeruginosa at 12 months (Ramsey 1999). Both the Chuchalin trial and the Ramsey trial studied tobramycin at the same dose and regimen. The only difference and possible cause of the heterogeneity was that disease severity was greater in the Ramsey trial at baseline (Chuchalin 2007; Ramsey 1999). MacLusky (n = 26) reported that in the first 24 months of the trial, four out of 14 participants (28.5%) in the tobramycin group and in none of the 12 participants in the control group became resistant, i.e. an MIC greater than 16 mcg/mL, RR 7.80 (95% CI 0.46 to 131.62) (MacLusky 1989).
1.14. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 14: Frequency of tobramycin‐resistant P. aeruginosa at end of study
Interpretation of data for this outcome is difficult in the four trials (n = 78) using a cross‐over design, two of which used combinations of drugs (Hodson 1981; Kun 1984; Nathanson 1985; Stead 1987). In one trial, gentamicin resistance developed in three out of 25 participants during the treatment with gentamicin and in two out of 25 participants during treatment with placebo (Kun 1984). There was no information on gentamicin resistance in two trials (n = 27) (Hodson 1981; Nathanson 1985). Furthermore, Hodson (n = 20) reported only transient resistance to carbenicillin in two out of 17 participants (Hodson 1981). Stead reported partial resistance to ceftazidime in one out of 13 participants and to carbenicillin in two out of 13 participants (Stead 1987).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 1).
b. Other organisms
Data on B cepacia isolation were reported by two parallel trials of six and 32 months (n = 548) (MacLusky 1989; Ramsey 1999). No significant differences between treatment arms were found, RR 0.26 (95% CI 0.03 to 1.99) (Analysis 1.15). A subsequent report on the Ramsey trial indicated there were intermittent isolates of B cepacia (two in the tobramycin group and three in the placebo group), but none of the isolates of B cepacia were persistent, i.e. not present on all three sputum specimens during the six‐month trial (Burns 1999).
1.15. Analysis.
Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 15: Frequency of new isolates of drug resistant organisms (at end of study)
Persistent isolates of Stenotrophomonas maltophilia and Alcaligenes xylosoxidans were also uncommon, although intermittent isolates were more frequent in the Ramsey trial (n = 520) that reported this detail, RR 3.05 (95% CI 0.32 to 29.10) and RR 1.02 (95% CI 0.06 to 16.15), respectively (Burns 1999) (Analysis 1.15). Intermittent isolates in tobramycin and placebo groups for S maltophilia were 14.7% and 21.8% respectively and for A xylosoxidans were 7.4% and 9.2% respectively. For treatment‐emergent Aspergillus species there was a significant difference in favour of placebo (n = 389), RR 2.12 (95% CI 1.29 to 3.46) (Burns 1999) (Analysis 1.15).
No difference in isolation of new pathogens were found in trials using tobramycin (n = 767) (Chuchalin 2007; Ramsey 1999) or colistin (n = 40) (Jensen 1987).
Four cross‐over design trials (n = 78) reported that sputum was cultured during the trial (Hodson 1981; Kun 1984; Nathanson 1985; Stead 1987). There is little information on results other than a statement that no new pathogens were isolated during the trial.
5. Adverse events
a. Renal impairment
Four trials (n = 976) measured renal function (serum creatinine), but no data were available for meta‐analysis. They found no significant evidence of persistent renal impairment (Chuchalin 2007; MacLusky 1989; Murphy 2004; Ramsey 1999). In the largest trial (n = 520), nine people in both the tobramycin group (300 mg twice daily) and the placebo group had transient increases of 50% or more in the creatinine level (Ramsey 1999). Chuchalin (n = 247) reported that median creatinine levels in the tobramycin and placebo groups were similar both at baseline and at the end of the trial (Chuchalin 2007).
b. Auditory impairment
Five trials (n = 996) measured audiometry (Chuchalin 2007; Hodson 1981; MacLusky 1989; Murphy 2004; Ramsey 1999); and four (n = 968) stated that no abnormality was found (Chuchalin 2007; Hodson 1981; Murphy 2004; Ramsey 1999). MacLusky found a change in hearing in one participant which was a conductive loss attributed to auditory polyp and not related to the study drug (treatment group not stated); it was further stated that no significant ototoxicity was seen in either group (MacLusky 1989) (Analysis 1.16).
1.16. Analysis.

Comparison 1: Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo, Outcome 16: Number experiencing adverse event (at end of study)
Ramsey reported tinnitus more frequently in the tobramycin‐treated group (8 out of 258) than in the placebo group (0 out of 262), RR 17.26 (95% CI 1.00 to 297.54) (Ramsey 1999).
c. Bronchospasm
One trial (n = 520) measured FEV1 response to an inhalation of the nebulised solutions, at first dose and at Week 20 (Ramsey 1999). In both groups, the median FEV1 fell 30 minutes after the first dose, tobramycin ‐1.8% (range ‐34.4 to 22.1) and placebo ‐2.6% (range ‐43.6 to 34.1); results at Week 20 were similar (Ramsey 1999). MacLusky (n = 28) reported that three participants complained of dyspnoea after inhaling tobramycin, but had a negative challenge and continued the trial (MacLusky 1989). Stead (n = 18) reported one participant with transient chest tightness with gentamicin (Stead 1987).
d. Other
There was a significant increase in voice alteration in two trials using tobramycin 300 mg twice daily (n = 701), RR 2.66 (95% CI 1.14 to 6.25) (Analysis 1.16) (Murphy 2004; Ramsey 1999).
The best estimate of the risk of pneumothorax was from five episodes in 520 participants, RR 0.25 (95% CI 0.03 to 2.26), favouring tobramycin (Ramsey 1999). Two other cross‐over trials (n = 38) reported an episode of pneumothorax (Hodson 1981; Stead 1987). Hodson reported that the participant was in the third arm of the trial and receiving ceftazidime when the pneumothorax developed (Hodson 1981); and Stead did not specify which treatment arm the participant was in when this occurred (Stead 1987).
In one trial (n = 520) the risk for haemoptysis with tobramycin was reported as RR of 0.87 (95% CI 0.66 to 1.13), but this did not show a difference between groups (Analysis 1.16) (Ramsey 1999).
Murphy (n = 181) recorded the incidence of several adverse events which was significantly lower in the antibiotic group compared to the placebo group (Murphy 2004):
| Adverse event | Antibiotic Group | Placebo Group |
| Aggravated cough | 35.2% | 64.4% |
| Cough | 40.7% | 53.3% |
| Pyrexia | 26.4% | 46.7% |
| Nasal congestion | 22.0% | 36.7% |
| Pharyngitis | 17.6% | 28.9% |
| Rhinorrhoea | 14.3% | 26.7% |
| Increased sputum | 4.4% | 18.9% |
However, two participants were withdrawn from the trial due to treatment‐emergent adverse events (cough in one participant and cough, sneeze and sore throat in the second); a further six participants had the tobramycin dosing interrupted and in three of these the adverse events were considered treatment‐related (Murphy 2004).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be very low due to risk of bias within individual trials and low event rates (Table 1).
Individual anti‐pseudomonal drugs versus placebo
There was no subgroup analysis by any of the individual drugs or combinations because of the small number of trials, different duration of these trials, different methods of expressing results of outcomes and absence of variance in results.
Inhaled anti‐pseudomonal antibiotics compared
Colistimethate sodium dry powder for inhalation versus tobramycin for inhalation solution (TOBI®)
One six‐month parallel trial (n = 380) compared colistimethate sodium dry powder for inhalation (Colobreathe®) (one capsule of 1.6625 MU (125 mg) twice daily) to TIS (300 mg per 5 mL twice daily) (Schuster 2013). The paper reported that the data were not normally distributed and results were evaluated using log‐transformation analysis; we therefore present the results directly reported from the original paper (Schuster 2013). Please refer to Table 2.
Primary outcome
1. Lung function
a. FEV1
Schuster observed a mean change from baseline to Week 24 in FEV1 % predicted of 0.964 in the Colobreathe® group and 0.986 in the TIS group. Using the last observation carried forward (LOCF) for the ITT population, Schuster reported the adjusted MD between the groups for the change in FEV1 % predicted, MD ‐0.98% (95% CI‐2.74% to 0.86%). The online supplement also presented mean (SD) data for baseline and end of trial for FEV1 L; however, due to its limitations we are not able to calculate and present any results for the change in FEV1 L. The data show equally small decreases in FEV1 L for both the Colobreathe® and the TIS groups (Schuster 2013).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 2).
b. FVC
Schuster reported a non‐significant difference for FVC at 24 weeks in the ITT population (LOCF), MD 0.01 L (95% CI ‐0.09 to 0.10). Again, the online supplement presented absolute baseline and end of treatment data for FVC L and showed even smaller changes than for FEV1 L (Schuster 2013).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 2).
2. Exacerbation of respiratory infection
c. Courses of intravenous antibiotics
Schuster reported the number of additional anti‐pseudomonal antibiotics used, but not specifically if theses were intravenous. In the ITT population, the mean duration of additional anti‐pseudomonal antibiotic use was 13.6 days in the Colobreathe® group compared to 14.4 days in the TIS group (Schuster 2013).
d. Pulmonary exacerbations
i. Frequency
Schuster reported that 57 out of 183 participants in the Colobreathe® group and 50 out of 191 participants in the TIS group experienced a PDE (Schuster 2013). When analysed these data did not show a difference between groups, RR 1.19 (95% CI 0.86 to 1.64) (Analysis 2.1).
2.1. Analysis.

Comparison 2: Colistimethate sodium dry powder (CDPI) versus tobramycin for inhalation solution (TIS), Outcome 1: Number of pulmonary exacerbations
ii. Time to first recorded exacerbation
Schuster also provided data for the mean time in days until the first PDE which favoured Colobreathe®, but again found no difference between groups, MD 6.21 (95% CI ‐11.70 to 24.12) (Analysis 2.2).
2.2. Analysis.

Comparison 2: Colistimethate sodium dry powder (CDPI) versus tobramycin for inhalation solution (TIS), Outcome 2: Time to first pulmonary exacerbation
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 2).
Secondary outcomes
1. Nutrition
Schuster reported that there were no relevant changes in weight, body mass index (BMI) or growth in either group (Schuster 2013).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be very low due to unclear risk of bias within the trial and imprecision from small numbers.
2. QoL
While the trial was not powered to detect differences in overall QoL, there were no treatment differences for the change in overall QoL scores using the CFQ‐R, although the adjusted mean changes at the end of the trial favoured the Colobreathe® group in terms of treatment burden (P = 0.091). This difference was statistically significant at Week 4 (P < 0.001; figure 4 in paper). Data for the individual domains are reported in supplementary tables of the trial report (Schuster 2013).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 2).
3. Survival
Schuster reported that there were no deaths (out of 183 participants) in the Colobreathe® group and two deaths (out of 191 participants) in the TIS group (Schuster 2013), RR 0.21 (95% CI 0.01 to 4.32) (Analysis 2.3).
2.3. Analysis.

Comparison 2: Colistimethate sodium dry powder (CDPI) versus tobramycin for inhalation solution (TIS), Outcome 3: Deaths
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 2).
4. Antibiotic resistance in P aeruginosa and other organisms
a. Antibiotic‐resistant P aeruginosa
The supplementary data from the Schuster trial presented values for the mean MIC50 and MIC90 values of respiratory isolates of P aeruginosa in the ITT population at monthly intervals from baseline to the end of the trial. No SDs were reported, and we have calculated the changed data for each group from the data presented, but are not able to enter these data in the analysis. The mean MIC50 (breakpoint of ≥ 8 mg/L) changed in the Colobreathe® group by 0.0 compared to 0.5 in the TIS group. The mean MIC90 (breakpoint of ≥ 8 mg/L) changed in the both groups by 4.0 (Schuster 2013).
Our GRADE analysis assessed the evidence for this outcome to be low (Table 2).
5. Adverse events
The analysis of the adverse event data presented by Schuster in the supplementary data tables showed that there was no difference in the risk of experiencing any adverse event, RR 1.06 (95% CI 0.99 to 1.12), but there was a higher risk of a treatment‐related adverse event in the Colobreathe® group, RR 1.76 (95% CI 1.50 to 2.08) (Analysis 2.4).
2.4. Analysis.

Comparison 2: Colistimethate sodium dry powder (CDPI) versus tobramycin for inhalation solution (TIS), Outcome 4: Adverse events (at end of study)
Schuster also reported adverse events by severity; mild adverse events were most common and there was no difference in risk between the groups, RR 1.00 (95% CI 0.92 to 1.09). However, the risks of moderate or severe adverse events were higher in the Colobreathe® group, RR 1.32 (95% CI 1.11 to 1.57) and RR 3.83 (95% CI 2.15 to 6.83) (Analysis 2.4). Most adverse events (2302 out of 2426 (95%)) were mild to moderate and the majority resolved without sequelae. The incidence of treatment‐related adverse events was higher in the Colobreathe® group, 153 out of 186 participants (82.3%) compared with 90 out of 193 participants (46.6%); and discontinuations where the primary cause was an adverse event were also higher in this group (18 out of 186 participants (9.7%) compared with 3 out of 193 participants (1.6%)). A further six participants mentioned adverse events as a reason for discontinuation, but not as the main reason. Severe adverse events were higher in the TIS group (6.2% participants compared with 4.3% participants) (Schuster 2013).
|
Most frequent adverse events by preferred term (≥ 5% of total number of events) |
Colobreathe® (n = 186a) | TIS (n = 193) | Total (n = 379) |
| Participants experiencing an adverse event | 175 (93.6) | 172 (89.1) | 347 (91.3) |
| Participants experiencing a treatment‐related adverse event | 153 (81.8) | 90 (46.6) | 243 (63.9) |
| Withdrawals due to an adverse event | 22 (11.8) | 5 (2.6) | 27 (7.1) |
| Severity: mild | 159 (85.0) | 165 (85.5) | 324 (85.3) |
| Severity: moderate | 123 (65.8) | 97 (50.3) | 220 (57.9) |
| Severity: severe | 48 (25.7) | 13 (6.7) | 61 (16.1) |
| Total number of adverse events | 1232 | 1194 | 2426 |
| Cough | 193 (15.7) | 123 (10.3) | 316 (13.0) |
| Abnormal taste | 132 (10.7) | 62 (5.2) | 194 (8.0) |
| Dyspnoea | 81 (6.6) | 98 (8.2) | 179 (7.4) |
| Lower respiratory tract infection | 79 (6.4) | 85 (7.1) | 164 (6.8) |
| Throat irritation | 94 (7.6) | 63 (5.3) | 157 (6.5) |
| Productive cough | 62 (5.0) | 76 (6.4) | 138 (5.7) |
Data presented as n (%), safety population. aOne participant was randomised but received no treatment.
c. Sensitivity reactions
Schuster reported the number of adverse events rather than the number of participants experiencing each type of event for cough, productive cough and throat irritation, which precluded the analysis of the data here. Incidences of cough and throat irritation were more common in the Colobreathe® group than the TIS group, 193 versus 123 and 94 versus 63 respectively. However, there were more incidences of productive cough reported in the TIS group (76) compared to the Colobreathe® group (62) (Schuster 2013).
d. Other
Schuster also reported fewer incidences of abnormal taste in the TIS group (62) compared to the Colobreathe® group (132). However, there were more reports of dyspnoea and lower respiratory tract infections in the TIS group compared to the Colobreathe® group, 98 versus 81 and 85 versus 79 respectively. Haemoptysis was below the 5% reporting level, but was reported by more participants receiving Colobreathe® (10.7%) than TIS (6.7%) (Schuster 2013).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low due to low event rates and risk of bias (Table 2).
Inhaled tobramycin (intravenous preparation) versus tobramycin for inhalation solution (TOBI®)
One cross‐over trial with 32 participants compared continuous twice‐daily 80 mg inhaled tobramycin (intravenous‐preparation) for three months to intermittent (four‐weekly on‐off cycles) twice‐daily 300 mg/5 mL TIS for three months (Nikolaizik 2008). This trial reported on FEV1 % predicted, FVC % predicted, participant preference and oxygen saturation and the results from the published papers showed some variation, so we contacted the trial investigators for clarification. They have kindly provided individual participant data for lung function, and we have analysed the first‐period data ourselves using the generic inverse variance method in RevMan (Review Manager 2014). Please refer to Table 3.
Primary outcome
1. Lung function
a. FEV1
Analysis of the data provided by the trial investigators showed no difference in FEV1 % predicted between the groups, MD ‐1.07 (95% CI ‐11.20 to 9.06) (Analysis 3.1).
3.1. Analysis.

Comparison 3: Inhaled TOBI® (IV preparation) versus tobramycin for inhalation solution (TIS), Outcome 1: FEV1 % predicted
b. FVC
Analysis of the data provided by the trial investigators showed no difference in FVC % predicted between the groups, MD 0.01 (95% CI ‐9.48 to 9.50) (Analysis 3.2).
3.2. Analysis.

Comparison 3: Inhaled TOBI® (IV preparation) versus tobramycin for inhalation solution (TIS), Outcome 2: FVC
Our GRADE analysis assessed the certainty of the evidence for both these outcomes to be very low and was downgraded twice due to risk of bias and once due to imprecision (small sample size) (Table 3).
Tobramycin inhalation powder versus tobramycin for inhalation solution (TOBI®)
One large parallel trial (n = 553) compared tobramycin inhalation powder (TIP) (a total of 112 mg, four capsules) to 300 mg/5 mL TIS, both given twice daily (Konstan 2010b). Please refer to Table 4.
Primary outcome
1. Lung function
a. FEV1
Konstan reported the relative change in FEV1 % predicted between baseline and Day 28 of the third treatment cycle. When analysed, data showed no difference between treatments, MD 1.10 (95% CI ‐2.33 to 4.53) (Analysis 4.1).
4.1. Analysis.

Comparison 4: Tobramycin inhalation powder (TIP) versus tobramycin for inhalation solution (TIS), Outcome 1: FEV1 (% predicted) relative change
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 4).
2. Exacerbation of respiratory infection
a. Hospital admissions
Konstan reported that the number of participants hospitalised for respiratory‐related events was similar between groups (Konstan 2010b); 24.4% in the TIP group and 22.0% in the TIS group, RR 1.11 (95% CI 0.80 to 1.53) (Analysis 4.2).
4.2. Analysis.

Comparison 4: Tobramycin inhalation powder (TIP) versus tobramycin for inhalation solution (TIS), Outcome 2: Hospitalisations
c. Courses of intravenous antibiotics
Konstan reported the number of participants requiring additional anti‐pseudomonal antibiotics was significantly higher in the TIP group (64.9%) compared to the TIS group (54.5%) (P = 0.0148) although the average number of days of usage was less in the TIP group (Konstan 2010b). It was not explicitly stated how these additional antibiotics were administered, except to say that most were oral and were used in 55.5% and 39.7% of participants in the TIP and TIS groups, respectively; also, that the percentage of participants receiving intravenous anti‐pseudomonal antibiotics was well‐matched across groups.
d. Pulmonary exacerbations
i. Frequency
Konstan stated that lung disorders presented in the table of adverse events were generally reported as pulmonary exacerbations (Konstan 2010b); when analysed, we found no difference between groups, RR 1.12 (95% CI 0.86 to 1.45) (Analysis 4.3).
4.3. Analysis.

Comparison 4: Tobramycin inhalation powder (TIP) versus tobramycin for inhalation solution (TIS), Outcome 3: Pulmonary exacerbations
Konstan reported that 31.1% of participants in the TIP group and 30.4% of participants in the TIS group experienced a pulmonary exacerbation (Konstan 2010b).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 4).
Secondary outcomes
3. Survival
Konstan reported that there were three deaths in the TIP group and no deaths in the TIS group, RR 4.76 (95% CI 0.25 to 91.62) (Analysis 4.4).
4.4. Analysis.

Comparison 4: Tobramycin inhalation powder (TIP) versus tobramycin for inhalation solution (TIS), Outcome 4: Deaths
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 4).
4. Antibiotic resistance
Konstan reported that sputum densities showed a decrease from baseline in both groups at each time point. Mean change at the end of 24 weeks in P aeruginosa sputum density was ‐1.6 log10 CFU/g in the TIP group versus ‐0.92 log10 CFU/g in the TIS group (mucoid phenotype), and ‐1.77 log10 CFU/g in the TIP group versus ‐0.73 log10 CFU/g in the TIS group (non‐mucoid phenotype) (Konstan 2010b).
On day 28 of the last cycle of treatment (24 weeks), 11.6 % of TIP participants and 9.9 % of TIS participants had negative P aeruginosa cultures.
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 4).
5. Adverse events
Konstan reported the rates for any adverse event were 90.3% in the TIP group and 84.2% in the TIS group, most of which were mild or moderate. The proportion of participants experiencing adverse events was highest in the first cycle and decreased successively with each following cycle (Konstan 2010b).
a. Renal impairment
Konstan stated there were few reports of changes in renal function and the reported incidence of renal and urinary disorders was less than 1% in both groups (Konstan 2010b).
b. Auditory impairment
Audiology was only performed in a subgroup of participants (78 out of 308 in the TIP group and 45 out of 209 in the TIS group); 20 participants (25.6%) in the TIP group experienced a decrease from baseline at any visit compared to seven participants (15.6%) in the TIS group and the decrease was of a similar magnitude in both groups (Konstan 2010b).
c. Sensitivity reactions ‐ bronchospasm
Konstan reported incidences of clinically significant bronchospasm (defined as a decrease of at least 20% in FEV1 % predicted from pre‐dose to 30 minutes post‐dose) in 16 participants (5.2%) in the TIP group and 11 participants (5.3%) in the TIS group (Konstan 2010b).
d. Other
Konstan reported a range of adverse events, but only two showed differences between groups (both in favour of the TIS group): cough, RR 1.56 (95% CI 1.23 to 1.96); and hoarseness, RR 3.56 (95% CI 1.71 to 7.43) (Analysis 4.5).
4.5. Analysis.

Comparison 4: Tobramycin inhalation powder (TIP) versus tobramycin for inhalation solution (TIS), Outcome 5: Adverse events (at end of study)
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 4).
Aztreonam lysine versus tobramycin for inhalation solution (TOBI®)
One parallel trial (n = 273, 268 included in analysis) compared AZLI 75 mg three times daily to TIS 300 mg twice daily in three consecutive cycles of four weeks on and four weeks off treatment (Assael 2013). Please refer to Table 5.
Primary outcomes
1. Lung function
a. FEV1
Assael reported the mean relative change from baseline in FEV1 % predicted at Week 24 (end of the third cycle) (Assael 2013). The data provided at Week 24 are an average across the three cycles and favour AZLI, MD ‐3.40 (95% CI ‐6.63 to ‐0.17) (Analysis 5.1). Assael reported that the mean relative change across three cycles was MD 3.4%, P = 0.02 (Assael 2013).
5.1. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 1: FEV1 % predicted ‐ mean relative change from baseline
Assael also reported the mean actual change from baseline averaged across the three cycles; our analysis shows a difference in favour of AZLI at Week 24, MD 2.71 (95% CI 0.76 to 4.66) (Analysis 5.2), which is similar to the report in the paper (MD 2.70% (95% CI 0.98 to 4.43) (P = 0.002)); the slight discrepancies may be due to the fact that we calculated the SD from the SE presented in the original paper to allow us to enter the data into RevMan.
5.2. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 2: FEV1 % predicted ‐ mean actual change from baseline
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 5).
2. Exacerbation of respiratory infection
a. Hospital admissions
Assael reported that 84 out of 136 participants (61.76%) in the AZLI group and 121 out of 132 participants (91.67%) in the TIS group experienced a respiratory event (not defined) (Assael 2013). There were 40 hospitalisations due to respiratory events amongst the 136 participants in the AZLI group compared to 58 hospitalisations amongst the 132 participants in the TIS group (P = 0.044); however, it is not clear from the original paper if these data refer to total hospitalisations or number of participants who were hospitalised, therefore we do not present these data in the analysis.
c. Courses of intravenous antibiotics
Assael reported the number of participants requiring additional antibiotics (intravenous or inhaled, or both) for each group. When the data are analysed, the risk of requiring additional antibiotics was lower in the AZLI group, RR 0.66 (95% CI 0.51 to 0.86) (Analysis 5.3). Assael further reported the mean number of days of additional antibiotics which was lower for the AZLI group, MD ‐7.10 (95% CI ‐13.90 to ‐0.30) (Analysis 5.4).
5.3. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 3: Need for additional antibiotics
5.4. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 4: Number of days of additional antibiotics
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 5).
Secondary outcomes
1. Nutrition
b. Weight
At Week 24, Assael reported the mean (SE) relative change in weight from baseline for each group; 0.58% (0.41) in the AZLI group and 0.06% (0.43) in the TIS group. Our analysis of the data showed no difference between groups, MD 0.52 (95% CI ‐0.64 to 1.68) (Analysis 5.5).
5.5. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 5: Weight (relative change from baseline)
Our GRADE analysis deemed the certainty of the evidence from this trial to be of moderate certainty, downgraded once due to some risk of bias within the trial (Table 5).
2. QoL
Assael reported the mean (SE) change from baseline in CFQ‐R respiratory symptom scale at the end of the trial (average across three cycles of treatment) for each group (Assael 2013). The change was greater in the AZLI group at the end of the trial, but this did not reach statistical significance, MD 4.10 (95% CI ‐0.06 to 8.26) (Analysis 5.6).
5.6. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 6: Quality of Life ‐ CFQR respiratory symptom scale
Assael also used the Treatment Satisfaction Questionnaire for Medication (TSQM) and reported on the domains of effectiveness, side effects, convenience and global satisfaction at Week 24 (Assael 2013). Results for effectiveness and global satisfaction favoured AZLI: effectiveness, MD 15.50 (95% CI 8.84 to 22.16) (Analysis 5.7); global satisfaction, MD 14.10 (95% CI 0.93 to 27.27) (Analysis 5.8). However, for the remaining domains of side effects and convenience the results showed no difference between treatments: side effects, MD 1.80 (95% CI ‐2.77 to 6.37) (Analysis 5.9); convenience MD 1.90 (95% CI ‐4.48 to 8.28) (Analysis 5.10).
5.7. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 7: TSQM ‐ effectiveness
5.8. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 8: TSQM ‐ global satisfaction
5.9. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 9: TSQM ‐ side effects
5.10. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 10: TSQM ‐ convenience
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 5).
3. Survival
Assael reported that two participants died due to complications of CF disease, both were considered unrelated to treatment and the treatment group was not specified (Assael 2013).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 5).
4. Antibiotic resistance in P aeruginosa or other organisms
Assael reported on the change from baseline in P aeruginosa in sputum (colony forming units (CFU)/g) at Week 24 (Assael 2013). Results showed no difference, MD ‐0.23 (95% CI ‐0.76 to 0.30) (Analysis 5.11).
5.11. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 11: Log10Pseudomonas aeruginosa CFU/g sputum
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 5).
5. Adverse events
Assael reported more treatment‐related adverse events in the AZLI group compared to the TIS group, RR 1.77 (95% CI 1.03 to 3.04) and more serious adverse events in the AZLI group, although this result was not statistically significant. There were no differences between the groups for other adverse events (Analysis 5.12).
5.12. Analysis.

Comparison 5: Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS), Outcome 12: Adverse events (at end of study)
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 5).
Amikacin liposome inhalation suspension (ALIS) versus tobramycin for inhalation solution (TOBI®)
One parallel trial (n = 302) compared ALIS 590 mg once daily to TIS 300 mg twice daily (Bilton 2020). Please refer to Table 6.
Primary outcomes
1. Lung function
a. FEV1
Relative change from baseline in FEV1 (L) in the ITT analysis was comparable at the end of treatment in the ALIS and TIS arms in each of the three cycles: cycle 1 (day 28; LS mean, 4.33% and 7.32%, respectively; P = 0.08); cycle 2 (day 84; 4.39% and 6.65%, respectively; P = 0.18); and cycle 3 (day 140; 4.07% and 5.11%, respectively; P = 0.59). Relative change was consistent across subgroups regardless of sex, ethnicity or age. In the per protocol analysis the difference in LS mean FEV1 (L) adjusted for treatment and randomisation strata, at day 168 was MD –1.31% (95% CI, –4.95 to 2.34; P = 0.48). The lower bound of the 95% CI was above –5%, indicating non‐inferiority of ALIS to TIS (Bilton 2020).
FEV1 % predicted was also reported and there were comparable improvements in both groups in the ITT population at the end of treatment (cycle 1 (day 28; 4.14% and 7.00%, respectively; P = 0.09), cycle 2 (day 84; 3.37% and 5.48%, respectively; P = 0.20), and cycle 3 (day 140; 2.31% and 3.23%, respectively; P = 0.63).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 6).
2. Exacerbation of respiratory infection
a. Hospitalisations
The trial reported all‐cause hospitalisations and found that 24 out of 148 participants were admitted in the ALIS group compared to 29 out 146 participants in the TIS group, RR 0.82 (95% CI 0.50 to 1.33) (Analysis 6.1).
6.1. Analysis.

Comparison 6: Amikacin liposome inhalation suspension (ALIS) versus TOBI®, Outcome 1: Hospitalisations ‐ number of participants hospitalised (all‐cause)
d. Pulmonary exacerbations
i. Frequency of exacerbations
Exacerbations were defined by the Fuchs criteria. There were more participants in the ALIS group experiencing an exacerbation than in the TIS group (63.5% in the ALIS group compared to 51.4% in the TIS group, P = 0.02). We graded the certainty of evidence as moderate (Table 6).
ii. Time to first exacerbation
Participants in the ALIS arm of the trial had a reduced time to first pulmonary exacerbation, HR 1.51 (95% CI 1.07 to 2.13; P = 0.03) (Bilton 2020).
Secondary outcomes
2. QoL
Respiratory symptoms, treatment burden and health scales were measured by the CFQ‐R. There were no differences between groups for any domain at day 168 (Analysis 6.2).
6.2. Analysis.

Comparison 6: Amikacin liposome inhalation suspension (ALIS) versus TOBI®, Outcome 2: Change from baseline in CFQ‐R domain scores
A comparison of 'on treatment' versus 'off treatment' demonstrated that the mean (SE) effects were greater for ALIS for respiratory symptoms (2.80 (1.25); P = 0.03), treatment burden (2.53 (0.97); P < 0.01) and health scales (2.47 (1.23); P = 0.05) (Bilton 2020).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 6).
4. Antibiotic resistance to P aeruginosa or other organisms
There was no difference between ALIS and TIS with regard to reduction in sputum density of P aeruginosa (P = 0.13) (Bilton 2020).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 6).
5. Adverse events
In the ALIS group, 84.5% of participants experienced at least one treatment emergent‐adverse event, whilst 78.8 % of the TIS group experienced at least one treatment‐emergent adverse event. There was no difference between groups in the reporting of adverse events (Analysis 6.3) (Bilton 2020).
6.3. Analysis.

Comparison 6: Amikacin liposome inhalation suspension (ALIS) versus TOBI®, Outcome 3: Treatment‐emergent adverse events (TEAEs)
Our GRADE analysis assessed the certainty of the evidence for this outcome to be moderate (Table 6).
Levofloxacin for inhalation solution versus tobramycin for inhalation solution (TOBI®)
One trial (n = 282) compared LIS to TIS (Elborn 2015). Please refer to Table 7.
Primary outcomes
1. Lung function
a. FEV1
Elborn reported means and SDs for both the absolute and the relative changes in FEV1 % predicted from baseline at up to three months and up to six months (Elborn 2015). Our analysis of the data showed no difference in the absolute change in FEV1 % predicted either at up to three months, MD 1.50 (95% CI ‐0.20 to 3.20) or up to six months, MD 0.70 (95% CI ‐0.85 to 2.25) (Analysis 7.1). This was also true for the relative change at both time points; at up to three months, MD 2.70 (95% CI ‐0.74 to 6.14) and at up to six months, MD 0.30 (95% CI ‐3.02 to 3.62) (Analysis 7.2).
7.1. Analysis.

Comparison 7: Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS), Outcome 1: Absolute change in FEV1 % predicted
7.2. Analysis.

Comparison 7: Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS), Outcome 2: Relative change in FEV1 % predicted
Our GRADE analysis assessed the certainty of the evidence for this outcome to be high (Table 7).
b. FVC
Elborn also reported means and SDs for both the absolute and the relative changes in FVC % predicted from baseline at up to three months and up to six months (Elborn 2015). At three months (after two four‐week periods of the active treatment with four weeks off treatment in between) there was an absolute change in FVC in favour of LIS, MD 2.60 (95% CI 0.77 to 4.43), but this was not maintained at the six‐month time point, MD ‐0.10 (95% CI ‐1.91 to 1.71) (Analysis 7.3). Similarly, there was a greater relative change in FVC % predicted at three months withLIS, MD 3.50 (95% CI 0.92 to 6.08), which again was not maintained to the end of the trial, MD 0.60 (95% CI ‐2.23 to 3.43) (Analysis 7.4).
7.3. Analysis.

Comparison 7: Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS), Outcome 3: Absolute change in FVC % predicted
7.4. Analysis.

Comparison 7: Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS), Outcome 4: Relative change in FVC % predicted
Our GRADE analysis assessed the certainty of the evidence for this outcome to be high (Table 7).
2. Exacerbation of respiratory infection
a. Hospital admissions
Elborn reported that 17.5% of participants in the LIS group were hospitalised compared to 28% of participants in the TIS group (Elborn 2015). When analysed there was a lower risk of hospitalisation due to respiratory infection in the LIS group, RR 0.62 (95% CI 0.40 to 0.98) (Analysis 7.5).
7.5. Analysis.

Comparison 7: Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS), Outcome 5: Hospitalisations due to respiratory exacerbations
Our GRADE analysis assessed the certainty of the evidence for this outcome to be high (Table 7).
Secondary outcomes
1. Nutrition
b. Weight
Elborn reported the incidence of weight loss as an adverse event (Elborn 2015). There was no difference found between the two groups, RR 0.78 (95% CI 0.56 to 1.09) (Analysis 7.6).
7.6. Analysis.

Comparison 7: Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS), Outcome 6: Weight decrease
Our GRADE analysis for this outcome assessed the evidence to be high certainty (Table 7).
2. QoL
Elborn did not provide data we were able to analyse, but reported that scores in the respiratory domain of the CFQ‐R were similar at baseline; at Day 28 they increased in the LIS group and decreased in the TIS group (difference in LS means was 3.9 units, P = 0.05), but results were again similar by the end of the trial (Elborn 2015).
Our GRADE analysis for this outcome assessed the evidence to be low certainty (Table 7).
4. Antibiotic resistance in P aeruginosa or other organisms
Data showed that no difference between groups for the change in P aeruginosa sputum density (log10 CFU/g) at up to six months, MD 0.12 (95% CI ‐0.31 to 0.55) (Analysis 7.7). Least squares mean difference was reported to be 0.44 log 10 CFU/g; 95% CI ‐0.01 to 0.88) (Elborn 2015).
7.7. Analysis.

Comparison 7: Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS), Outcome 7: Change in P aeruginosa sputum density (log10 CFU/g)
Elborn also reported that the proportion of participants experiencing a greater than four‐fold increase in the levofloxacin MIC of their most levofloxacin‐resistant P aeruginosa isolate was similar in both groups (21% for LIS compared to 17% for TIS; P = 0.5). Investigators did not observe the significant emergence of other pathogens in either treatment group (Elborn 2015).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be high (Table 7).
5. Adverse events
Adverse event data are presented in the analysis (Analysis 7.8). No data were reported for renal or auditory impairment.
7.8. Analysis.

Comparison 7: Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS), Outcome 8: Adverse events (at end of study)
d. Other
There were significantly fewer participants in the LIS group who reported: epistaxis, RR 0.20 (95% CI 0.04 to 1.00); general malaise, RR 0.10 (95% CI 0.01 to 0.83); and increased blood glucose, RR 0.28 (95% CI 0.08 to 0.94). Significantly more participants in the LIS group reported dysgeusia, RR 46.25 (95% CI 2.88 to 741.95). None of the other reported adverse events showed differences between the groups (Analysis 7.8).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be high (Table 7).
Ceftazidime versus combined gentamicin and carbenicillin
We have not produced a summary of findings table for this comparison as combined gentamicin and carbenicillin are no longer in use. One trial reported on this comparison (n = 18) (Stead 1987).
Primary outcome
1. Lung function
This outcome was reported narratively as part of the three‐arm cross‐over trial that looked at this combination of antibiotics. Lung function was stated to be similar in both groups at the end of treatment (Stead 1987).
Secondary outcomes
1. Nutrition
b. Weight
Weight was stated to be similar in both groups at the end of treatment (Stead 1987).
Continuous inhaled anti‐pseudomonal antibiotics versus intermittent inhaled anti‐pseudomonal antibiotics compared
One 28‐week parallel trial (n = 90) compared a continuous antibiotic regimen (three cycles) of 28 days AZLI (75 mg three times daily) followed by 28 days TIS (300 mg twice daily) to an intermittent antibiotic regimen (three cycles) of 28 days of placebo (three times daily) followed by 28 days TIS (300 mg twice daily) (Flume 2016b). Please refer to Table 8.
Primary outcome
1. Lung function
a. FEV1
Values from the end of each treatment cycle (end of weeks four, 12 and 20) were averaged and the adjusted mean change from baseline was presented. The mean change in FEV1 % predicted was greater in the group that received AZLI alternating with TIS than the group that received placebo alternating with TIS, 1.37 (SE 0.67) versus 0.04 (SE 0.66). However, analysis showed no difference between the groups, MD 1.33 (95% CI ‐0.51 to 3.17) (Analysis 8.1).
8.1. Analysis.

Comparison 8: Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS), Outcome 1: Mean change from baseline ‐ FEV1 % predicted
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 8).
2. Exacerbation of respiratory infection
a. Hospital admissions
The rate of hospitalisations was reported to be higher in the placebo/TIS group (1.62 per participant year) than in the AZLI/TIS group (1.04 per participant year), but we found no difference between groups, RR 0.642 (95% CI 0.36 to 1.16) (P = 0.14) (Flume 2016b). We have entered the RR and CIs into our analysis (Analysis 8.2).
8.2. Analysis.

Comparison 8: Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS), Outcome 2: Rate of hospitalisation per participant year
c. Courses of intravenous antibiotics
Flume reported the number of participants needing additional antibiotics during the trial, but included intravenous or inhaled antibiotics, or both. A larger percentage of participants in the placebo/TIS group (n = 26 out of 47 (55.3%)) required non‐study antibiotics for exacerbations during the comparison phase than those in the AZLI/TIS group (n = 21 out of 43 (48.8%)), but the rates did not differ between groups, RR 0.88 (95% CI 0.59 to 1.32) (Analysis 8.3).
8.3. Analysis.

Comparison 8: Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS), Outcome 3: Need for additional antibiotics for an exacerbation
d. Pulmonary exacerbations
i. Frequency
The rate of PDEs was the primary outcome in the Flume trial and investigators found that the rate was lower in the AZLI/TIS group (1.31 PDEs per participant‐year) than in the placebo/TIS group (1.76 PDEs per participant year) (Flume 2016b). However, the difference between the groups was not reported to be "significant", RR 0.74 (95% CI 0.45 to 1.24) (P = 0.25) (Flume 2016b); we have entered this result into our analysis (Analysis 8.4).
8.4. Analysis.

Comparison 8: Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS), Outcome 4: Rate of protocol defined pulmonary exacerbations per participant year
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 8).
Secondary outcomes
1. Nutrition
b. Weight
A decrease in weight was recorded as an adverse event (see adverse events) (Flume 2016b).
2. QoL
Flume reported the change in adjusted mean CFQ‐R RSS scores from baseline for the continuous AZLI/TIS group and the placebo/TIS group using an average from weeks four, 12 and 20. Whilst the mean (SE) scores improved 1.00 (1.74) in the AZLI/TIS group, they decreased ‐2.06 (1.63) in the placebo/TIS group. When we entered this into our analysis, but found no difference between the groups, MD 3.06 (95% CI ‐1.61 to 7.73) (Analysis 8.5).
8.5. Analysis.

Comparison 8: Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS), Outcome 5: Quality of life ‐ CFQ‐R respiratory symptom score
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 8).
4. Antibiotic resistance in P aeruginosa or other organisms
a. Antibiotic‐resistant P aeruginosa
We were not able to enter data for this outcome into our analysis, but the authors state that the adjusted mean changes from baseline sputum P aeruginosa density after each course of inhaled treatment (AZLI or placebo or TIS) during the comparative phase were small (0.36 to ‐0.55 log10 CFU/g) and that differences between treatment groups were not statistically significant (Flume 2016b). The authors also reported that the MIC50 values for P aeruginosa isolates changed at least two‐fold from baseline for both treatment groups (Flume 2016b).
b. Other organisms
Flume reported the incidence of other organisms during the comparative phase of the trial although and found no difference between treatment groups (Analysis 8.6).
8.6. Analysis.

Comparison 8: Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS), Outcome 6: Incidence of other respiratory pathogens (at end of study)
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 8).
5. Adverse events
We have presented adverse events by severity in the analyses, none of which were different between groups (Analysis 8.7). There were only three participants in each group reporting treatment‐related adverse events and these were all grade 1 or 2 in severity (AZLI/TIS n = 3/42 (7.1 %); placebo/TIS n = 3/46 (6.5 %); RR 1.10 (95% CI 0.23 to 5.13)). None of the serious adverse events (AZLI/TIS n = 21/42 (50.0 %); placebo/TIS n = 24/46 (52.2 %)) were considered to be treatment‐related.
8.7. Analysis.

Comparison 8: Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS), Outcome 7: Adverse events (at end of study)
Treatment‐emergent adverse events were reported only for those participants who received the treatment (safety population n = 88). We have presented specific adverse events in the analysis (Analysis 8.8).
8.8. Analysis.

Comparison 8: Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS), Outcome 8: Treatment‐emergent adverse events (at end of study)
c. Sensitivity reactions
The most commonly reported adverse events (none of which showed a difference between groups) were cough (AZLI/TIS n = 32 out of 42 participants (76.2 %); placebo/TIS n = 33 out of 46 participants (71.7 %); RR 1.06 (95% CI 0.83 to 1.36)), increased sputum (AZLI/TIS n = 20 out of 42 participants (47.6 %); placebo/TIS n = 31 out of 46 participants (67.4 %); RR 0.71 (95% CI 0.49 to 1.03)) and dyspnoea (AZLI/TIS n = 13 out of 42 participants (31.0 %); placebo/TIS n = 24 out of 46 participants (52.2 %); RR 0.59 (95% CI 0.35 to 1.01)).
d. Other
Decreased exercise tolerance was reported to be significantly more common in the placebo/TIS group, (RR 0.27, 95% CI 0.08 to 0.90); this was also true for decreased appetite, RR 0.34 (95% CI 0.14 to 0.85) and nasal congestion, RR 3.01 (95% CI 1.04 to 8.74). No differences were found between groups for any of the other treatment‐emergent adverse events (Flume 2016b).
Our GRADE analysis assessed the certainty of the evidence for this outcome to be low (Table 8).
Discussion
Summary of main results
The purpose of this review was to determine the benefits and harms of inhaling antibiotics for longer‐term suppression of chronic lung infection with P aeruginosa in people with CF. We wanted to distinguish this pattern of use from inhaled antibiotics to treat pulmonary exacerbations or to eradicate P aeruginosa (Langton Hewer 2017; Ryan 2012).
We originally used an arbitrary definition of treatment for at least one month as the criteria for accepting trials to guide long‐term suppression. In retrospect, this criterion was judged to be erroneous and the 2018 update of the review onwards only includes trials where treatment lasted at least three months. The main reason for this was that treatment to suppress chronic infection with P aeruginosa in the lungs of people with CF will be used for more than a month, so there is a need to know the benefit and harms of inhaled antibiotic treatment used over a longer time period.
The review found 18 trials with 3042 participants that examined the effect of any inhaled antibiotic treatment as long‐term therapy (i.e. three to 33 months) in people with CF. Of these, 11 trials compared one or more antibiotics to placebo or usual treatment (n = 1130). There were four trials that compared two different antibiotics (n = 1237). Two trials compared two regimens of inhaled tobramycin (n = 585) and one trial (n = 90) compared intermittent treatment with tobramycin compared to continuous treatment with tobramycin and aztreonam. The Stead trial (n = 18) was a three‐arm trial which fell into to both groups as they compared different antibiotics and compared antibiotics to placebo (Stead 1987). Overall the most studied antibiotic is tobramycin and was reported in 12 of the included trials.
Inhaled anti‐pseudomonal antibiotics versus placebo
The review found some evidence that inhaled antibiotics improved lung function (FEV1 and FVC) and reduced the frequency of exacerbations of respiratory infection in people with CF when compared to placebo (Table 1). There were insufficient data for us to be able to report an effect on nutritional outcomes. There was no difference in the number of deaths between groups, but this was only reported in two trials (Chuchalin 2007; Ramsey 1999). The effect on QoL was again only reported in two trials, but one trial found that fewer lost school or work days were reported in the tobramycin treated group compared with placebo (Chuchalin 2007), whilst the second found no difference in the number of school days missed between tobramycin and placebo (Murphy 2004). There was no difference in antibiotic resistance seen in the two trials that were included in the meta‐analysis (Chuchalin 2007; Ramsey 1999).
Important adverse effects were not common in these trials although tinnitus and voice alteration were more common after inhaled antibiotics than placebo. It was difficult to know what the acceptability of treatment was to the individual.
Inhaled anti‐pseudomonal antibiotics compared
Each of the comparisons of different anti‐pseudomonal antibiotics that we report only included one trial. We report the findings in summary of findings tables (Table 2; Table 3; Table 4; Table 5; Table 7). Lung function only improved in the comparison of TIS and AZLI (n = 268) and this was in favour of AZLI (Assael 2013). No differences in this outcome were found in the remaining comparisons.
Pulmonary exacerbations were measured in different ways with hospital admissions, courses and duration of antibiotics and number of exacerbations being used as a measure of the effect of the intervention on exacerbations. Assael (n = 268) reported that both the number of people requiring antibiotics and the number of days they required them for were higher in those participants in the TIS group compared to the AZLI group (Assael 2013). The evidence from this trial was deemed to be of moderate certainty; the GRADE judgement was downgraded because of the risk of bias within the trial caused by the design being open‐label. When comparing LIS to TIS, Elborn found that the number of hospitalisations due to an exacerbation was lower in the LIS group compared to the TIS group (n = 282); the certainty of the evidence from this trial was deemed to be high (Elborn 2015).
Due to paucity of data we are unable to draw conclusions about QoL changes for these comparisons or for nutritional outcomes. Similarly, the low numbers of deaths in the trials precludes us from commenting on the effect of the interventions on this outcome.
Adverse events were common for all comparisons, but a few differences were reported. With regard to treatment‐related adverse events, there was a lower number reported in the TIS group compared to the AZLI group in the Assael trial (n = 268) and similarly in the TIS group compared to colistimethate group in the Schuster trial (n = 379) (Assael 2013; Schuster 2013).
Continuous inhaled anti‐pseudomonal antibiotics versus intermittent inhaled anti‐pseudomonal antibiotics compared
We only found one trial that compared continuous alternating treatment of AZLI/TIS with an intermittent course of TIS (n = 90) (Flume 2016b). The results are presented in the tables (Table 8). Few differences were reported for the outcomes in which we are interested and none reached statistical significance. The authors only conclusion was that the continuous alternating regimen was well‐tolerated and may provide additional clinical benefit (Flume 2016b).
Overall completeness and applicability of evidence
It is unlikely that any trials of inhaled antibiotics, particularly good‐quality trials, have not been identified and included. The search strategy was thorough and the selection of trials for inclusion in the review from those found in the search strategy has favoured inclusion rather than exclusion, e.g. quasi‐RCTs and trials in which the criteria for diagnosis of CF were not explicitly stated were included. For three of the included trials, we were only able to find an abstract to the trial. Two of these trials were published over 30 years ago, and it is unlikely that we will find any further details (Day 1988; Nathanson 1985). The Bilton trial was first published in abstract form in 2013 and there is now a full paper that we have included (Bilton 2020). Extra information obtained has been added at this update.
There was important heterogeneity amongst these trials in terms of design and outcome measures, which led to difficulties in performing the review and interpreting the results. In particular, we were only able to include a few trials in a meta‐analysis of any outcome, raising the possibility of bias.
The most frequently measured outcomes were lung function, hospitalisation and antibiotic use and a measure of pulmonary exacerbations experienced. Inhaled therapy is time‐consuming and this will have a negative impact on the QoL and the independence of people with CF. We were less able to make conclusions relating to QoL and survival, as these are longer‐term measures; particularly with QoL measures, some trials did not report the outcome at all.
Previous versions of this review included trials of at least one month duration and found there to be some evidence that inhaled antibiotics benefited participants in terms of improving lung function and reducing exacerbations (Ryan 1999; Ryan 2003; Ryan 2011). In this version of the review, we have changed the criteria and include only those where participants were treated for at least three months. The changing face of CF care in recent decades has lead to improved survival and as such, a greater focus on the long‐term risks and benefits of different treatments. With more than half of adults with CF culturing P aeruginosa on a chronic or intermittent basis (CF Trust 2021), and 90% of them on long‐term inhaled antibiotic therapy, the inclusion of short trials in the review does not provide evidence that is comparable to current clinical practise, which recommends three months of treatment with inhaled antibiotics even at the first isolation of P aeruginosa, and essentially lifelong treatment in cases of failed eradication.
Certainty of the evidence
The design, performance and reporting of trials has changed since the first included trial (n = 20) was reported 36 years ago; this first report of the use of inhaled antibiotics in CF renewed interest in this therapy (Hodson 1981). Following this, six trials (n = 140) were published between 1984 and 1989; these were all single‐centre trials with small sample sizes and with important problems in trial design (Day 1988; Jensen 1987; Kun 1984; MacLusky 1989; Nathanson 1985; Stead 1987). Furthermore, the doses of antibiotic used in these trials was relatively small and probably determined by the size of the ampoule for intravenous therapy, e.g. doses of gentamicin or tobramycin from 20 mg to 80 mg. In vitro data suggested much higher doses would be needed to ensure bacterial killing. The next development was the production of a preservative‐free tobramycin in a dose of 300 mg in 5 mL solution and able to be delivered by jet nebuliser (n = 520) (Ramsey 1999). This trial was multicentre with larger numbers of participants. It was performed at a time when there was more critical examination of trial design in trials involving people with CF and was of higher quality. There were two trials in children with early isolation of P aeruginosa or persistent isolation but with mild impairment of lung function (n = 203) (Murphy 2004; Wiesemann 1998).
Two design features that are problematic for trials of nebulised antibiotics in CF are cross‐over periods and double blinding. Cross‐over design for antibiotic therapy in CF is probably inappropriate. Firstly, the clinical course of lung disease in CF is unstable with a frequent pattern of progressive deterioration and exacerbations causing further temporary deterioration. Secondly, an effective antibiotic treatment may have a carry‐over effect. Thirdly, treatment of exacerbations with antibiotics and more physiotherapy and other treatment will cause an improvement in lung function that is likely to persist with time, with potential for carry‐over benefit. Six of our trials used a cross‐over design (n = 124) (Day 1988; Hodson 1981; Kun 1984; Nathanson 1985; Nikolaizik 2008; Stead 1987).
We assessed the certainty of the evidence using the GRADE system and evaluate our specified outcomes in the summary of findings tables (Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7; Table 8). The most common reason for downgrading the certainty of evidence in this review was the risk of bias in the included trials. Blinding is important for these trials, but care is needed to mask the taste of antibiotic solutions and this may not have been achieved in a number of trials using normal saline for placebo. In some cases blinding was not possible due to the difference in treatment regimens and seven trials were open‐label (Assael 2013; Bilton 2020; Elborn 2015; Konstan 2010b; Murphy 2004; Nikolaizik 2008; Schuster 2013), one trial was partially blinded (Stead 1987) and two were single‐blinded (observer) (Kun 1984; MacLusky 1989).
We also downgraded the certainty of the evidence due to imprecision with many trials reporting low event rates or small sample sizes, or both. Difficulty in recruiting and maintaining trial numbers was a challenge and some included trials were underpowered for some or all of the outcomes measured (n = 470) (Flume 2016b; Schuster 2013). The sample of trials gives an example for the debate on the relative validity of pooling results from a number of small trials with results that are prone to error or the results from a single, large, well‐designed trial. In this review, one well‐designed trial contributed 45% of all participants (n = 520) in the 11 trials comparing an inhaled antibiotic to placebo (Ramsey 1999).
Potential biases in the review process
We feel that all the relevant trials have been identified and data rigorously and independently extracted by two review authors. At least two review authors also assessed the risks of bias for each trial and a third review author was brought in to arbitrate if needed. There has been a change to the review team, and although data extraction has always been done by two review authors, it has not always been the same two review authors. This may have introduced an element of bias to the way which we have reported the results of the trials.
The original protocol for this review was written in 1997. A general objective was to include as much evidence as possible from controlled trials on the use of inhaled antibiotics to suppress infection with P aeruginosa. This resulted in a large review with much heterogeneity in trial design and reporting, meaning that the review was difficult to analyse and interpret. Two design features open to debate are the length of the trial that is needed to support long‐term use and the inclusion of cross‐over trials (see preceding discussion). In the current update we have amended the original protocol to include only trials of at least three months duration, and we have treated results from cross‐over trials with caution.
Agreements and disagreements with other studies or reviews
In the UK, the first‐line treatment for P aeruginosa is colistin followed by alternating therapy with tobramycin, as recommended by the UK CF Trust guidelines, supported by UK NICE guidance on the use of colistin or tobramycin dry powders for inhalation rather than nebuliser therapy and is also seen in local CF guidelines (CF Trust 2009; GOSH 2011; NICE 2013). In the USA, chronic suppression of P aeruginosa is treated with inhaled tobramycin due to the sustained improvement in pulmonary function outweighing the risk of resistance developing (Yankaskas 2004). Colistin is not recommended in US guidelines for chronic suppression of P aeruginosa, which is consistent with the findings of this review, i.e. that there is no adequate evidence to support its use (Mogayzel 2013).
Authors' conclusions
Implications for practice.
The practise of prescribing inhaled antibiotics for many years to suppress chronic infection in people with cystic fibrosis (CF) is widespread. At present, the most commonly‐used drugs are tobramycin and colistin (Colobreathe®). Other emerging treatments are aztreonam, ciprofloxacin, levofloxacin, amikacin and combined fosfomycin‐tobramycin.
This review is restricted to randomised trials designed to test the benefit of these drugs for periods of three months or more. The review found limited evidence that inhaled antibiotic treatment of chronic infection with Pseudomonas aeruginosa (P aeruginosa) is of some benefit in terms of improvement in lung function and reduction in exacerbations of respiratory infection for up to 33 months (the duration of the longest trial). In addition, there do not seem to be severe or frequent adverse effects. The best evidence is for the use of tobramycin which was studied in 12 trials.
However, the findings of this review raise some issues to consider when prescribing this treatment long‐term.
There is a lack of evidence of benefit in terms of survival, quality of life or nutritional outcomes.
The level of benefit is uncertain as some trials are small and prone to error. We have included several larger trials, but heterogeneity in measurement and reporting of outcomes is such that very little pooled analysis was possible.
The major evidence for benefit is for use for up to six months, hence uncertainty about any longer‐term benefit remains;
There is no adequate evidence from randomised controlled trials to support the use of colistin.
Implications for research.
It is likely that inhaled antibiotics will increasingly be used for the long‐term treatment of people with CF who are troubled by complications attributable to chronic lung infection with P aeruginosa.
This review raises some important issues concerning the recruitment and maintenance of participants. Large, well‐designed, randomised controlled trials would help to fill many of the evidence gaps, but this is likely to be impractical due to the relatively small number of people with CF who are able to participate in trials which could potentially add to their already burdensome treatment regimen. Although we increased the duration of intervention included in this review to at least three months, the longest trial duration was 33 months. Longer trial durations running into years would help to identify the longer‐term effectiveness and harms associated with inhaled antibiotic treatment regimens.
We have included cross‐over trials in this version of the review, but the design is problematic. The progressive deterioration of lung function in people with CF makes it likely that the groups will be inherently different at the baseline of successive treatment periods. Trials of a parallel design are much more appropriate for future trials. Similarly, we have included older trials in this review (over 20 years old), but with the rapidly changing face of CF treatment, it may be more appropriate to exclude trials more than 20 years old.
A future review of the literature would be much improved by more consistent measurement and reporting of outcomes between trials. Consistency, especially with lung function test results and in defining exacerbations of respiratory tract infection (in terms of hospitalisation and of antibiotic use), may lead to more definitive conclusions. There should also be information on the effect of long‐term use on the outcomes of quality of life and survival.
Some specific issues which should be the objectives of trials are to:
determine the optimum dose, daily frequency of administration and frequency of treatment with tobramycin;
compare antibiotics for benefits and harm; there should be a longer‐term comparison of tobramycin and other inhaled antibiotics, and perhaps combinations;
determine adverse effects of longer‐term use, particularly on the relevance and impact of drug resistance organisms.
What's new
| Date | Event | Description |
|---|---|---|
| 13 September 2022 | New citation required but conclusions have not changed | One author (Kate H Regan) has stepped down from the team. No new studies have been included to the review, therefore our conclusions have not changed. |
| 13 September 2022 | New search has been performed | A search of the Cystic Fibrosis and Genetic Disorders Review Group's Cystic Fibrosis Trials Register identified 85 references potentially eligible for inclusion in the review. An additional three references were identified from the trial registry searches. We added 15 references to four already included studies (Assael 2013; Bilton 2020; Konstan 2010b; Ramsey 1999). We added 26 references to 16 already excluded studies (Dupont 2008; Flume 2016a; Frost 2018; Galeva 2013; Geller 2011b; Goss 2013; Hodson 2002; Mainz 2014; Mazurek 2014; McCoy 2008; NCT02677701; Ramsey 2017; Retsch‐Bogart 2007; Sands 2014; Wainwright 2011; Westerman 2003). Two references were added to one study already listed as awaiting classification (Ramsey 2017). This has now been moved to excluded studies. There are 11 newly‐excluded studies (13 references) (ACTRN12620000531910; EUCTR2006‐006215‐68‐DE; EUCTR2014‐001401‐41‐NL; Griese 2009; IRCT2016100930233N1; Maneshi 2019; NCT00411736; NCT00503490; NCT01315691; NCT02015663; NCT02730793). Two studies are awaiting classification (EUCTR2007‐004277‐26‐NL; NCT03341741). We deleted the remaining 30 references as they were not even considered eligible to be listed as excluded studies. |
History
Protocol first published: Issue 1, 1998 Review first published: Issue 3, 1999
| Date | Event | Description |
|---|---|---|
| 15 March 2018 | New citation required and conclusions have changed | The title of the review has changed to focus on treatment of chronic infection with Pseudomonas aeruginosa and a new author team is now in place. Conclusions have changed due to the removal of shorter‐term trials. We have also included the need for harmonising of outcomes in trials to allow combining of results. |
| 15 March 2018 | New search has been performed |
Changes to the scope of the review We have now focused on inhaled anti‐pseudomonal antibiotics and as such have now excluded two previously included trials which looked at other antibiotic regimens (Ledson 2002; Nolan 1982). We have also changed the inclusion criteria so as to only include trials with a duration of three months or longer (previously 28 days and over). A total of 20 trials have been excluded due to insufficient duration and their characteristics and summary results presented in an additional table for the readers' reference; 11 of these were previously included in the review (Dupont 2008; Geller 2011b; Gibson 2003; Goss 2013; Hodson 2002; Konstan 2010a; Lenoir 2007; McCoy 2008; Ramsey 1993; Retsch‐Bogart 2007; Wainwright 2011), one was previously listed as 'Awaiting assessment' (Davies 2004) and eight were newly identified at this update (see below) (Dorkin 2015; Galeva 2013; Geller 2011a; Mainz 2014; Mazurek 2014; Nasr 2006; Sands 2014; Trapnell 2012). New search results A search of the Cystic Fibrosis and Genetic Disorders Review Group's Cystic Fibrosis Trials Register identified 123 references to 32 trials. Four new trials (25 references) were included (Assael 2013; Bilton 2020; Elborn 2015; Flume 2016b), 10 new trials (39 references) were excluded (Dorkin 2015; Flume 2016a; Galeva 2013; Geller 2011a; Mainz 2014; Mazurek 2014; Nasr 2006; Ruddy 2013; Sands 2014; Trapnell 2012) and 11 new references to four already excluded trials have been identified (Al‐Aloul 2004; McCoy 2008; Ramsey 2005; Stass 2015). Two new trials (two references) have been listed as 'Awaiting classification' (Herrmann 2017; Ramsey 2017a). Trials previously listed as 'Awaiting classification' Two new references were identified to one trial previously listed as 'Awaiting assessment' which has now been excluded (Coates 2011). 10 new references were identified to a further trial which has also now been excluded (Wainwright 2008). Finally, one additional reference to a trial previously listed as 'Awaiting classification' has been identified and the trial has been excluded (Wainwright 2011). The EVOLVE trial was previously listed in 'Awaiting classification' both under a clinical trials identifier and as the Konstan 2009 trial (two abstracts). An additional three references to this trial have been identified and all references are now listed under the trial which has been included (Konstan 2010b). A further 28 new references were added to seven trials previously listed as 'Awaiting classification'; one trial (four new references) has been included (Schuster 2013) and six trials (25 new references) excluded (Dupont 2008; Geller 2011b; Goss 2013; Konstan 2010a; Retsch‐Bogart 2007; Rietschel 2009). No new references were found to one trial listed as 'Awaiting classification', but it has been excluded on the grounds of insufficient duration after the change in inclusion criteria (Davies 2004). One trial remains in 'Awaiting classification' pending further information (Nikonova 2010). Trial previously listed as 'Ongoing' Two additional references were identified to one trial previously listed as ongoing under the study ID Bayer 2010; following publication of the new abstracts, this has now been excluded under a new trial ID (Dorkin 2015). We have added a summary of findings table for each of the comparisons we present within this review. |
| 1 February 2011 | New search has been performed | The search of the Group's Cystic Fibrosis Trials Register in April 2010 identified 62 new citations to 36 studies. A total of 11 citations to four new studies have been included (Ledson 2002a; McCoy 2008a; Nikolaizik 2008; Nolan 1982a). One citation was added to an already included study (Ramsey 1999). Two studies previously awaiting classification have now been included and one new citation added to each (Chuchalin 2007; Lenoir 2007a). Two previously excluded trials have now been included; a consequence of not restricting the review to nebulised anti‐pseudomonas antibiotics (Ledson 2002a; Nolan 1982a). Thirteen new studies (19 citations) have been excluded (Bruinenberg 2008; Dodd 1998; Geller 2007; Griffith 2008; Mullinger 2005; Noah 2007; Proesmans 2016; Rosenfeld 2006; Shatunov 2001; Stass 2015; Stass 2009; Steinkamp 2006; Tramper‐Stranders 2010). A total of eight citations were added to six already excluded studies (Al‐Aloul 2004; Poli 2005; Ratjen 2010; Ramsey 2005; Retsch‐Bogart 2008; Westerman 2007). One previously included study has now been excluded as it is not clear that the effects of the intervention were due to the inhaled antibiotic (Carswell 1987). Eleven new studies with a total of 21 citations have been listed as awaiting classification (Davies 2004a; Dupont 2008a; Flume 2010a; Goldman 2008a; Goss 2009a; Keller 2010a; Konstan 2010c; Nikonova 2010; Retsch‐Bogart 2007a; Rietschel 2009a; Wainwright 2010). The Plain Language Summary has also been updated in line with the latest guidance from The Cochrane Collaboration. |
| 1 February 2011 | New citation required but conclusions have not changed | The title of the review has been changed from 'Nebulised anti‐pseudomonal antibiotics for cystic fibrosis' to 'Inhaled antibiotics for long‐term therapy cystic fibrosis' to better reflect:
1. that organisms other than Pseudomonas aeruginosa may be the target of inhaled antibiotic treatment; and
2. methods to generate aerosols of antibacterial agents other than nebulisers are being developed. One co‐author, Somnath Mukhopadhyay, has stepped down from the review team. A new co‐author has joined the team, Kerry Dwan. |
| 12 November 2008 | Amended | Converted to new review format |
| 21 February 2007 | New search has been performed | The search of the Group's Cystic Fibrosis Trials Register to September 2006 identified 18 new citations to 11 trials: ADDITIONAL CITATIONS TO ALREADY INCLUDED TRIALS Gibson 2003 (1 citation added) Ramsey 1999 (1 citation added) Results for weight, a secondary outcome, is now reported for the Gibson 2003 citation and is included. NEW TRIALS Two trials have been published as abstracts and have been added to the section 'Awating Assessment' until the full papers have been published. Chuchalin 2005 (2 citations) Lenoir 2005 (2 citations) EXCLUDED TRIALS The remaining 12 citations to 7 trials have been excluded. |
| 26 January 2006 | New search has been performed | The search of the Group's Cystic Fibrosis Trials Register to September 2005 identified 32 new citations of 16 trials: ADDITIONAL CITATIONS TO ALREADY EXCLUDED TRIALS Chua 1990 (1 additional citation added) Dodd 1997 (1 additional citation added) Frederiksen 1997 (1 additional citation added) Alothman 2002 (1 additional citation added) ADDITIONAL CITATIONS TO ALREADY INCLUDED TRIALS Ramsey 1999 (10 additional citations added) Hodson 2002 (2 additional citations added) These additional reports of results from these two included trials did not add new results to the review compared to the reports already included. These citations either reported results already included in this review, or included outcomes that were not in the protocol for this review; or reported sub‐group analyses, or results from open‐label extension. NEWLY EXCLUDED Adeboyeku 2001(1 citation) Geborek 2003 (1 citation) Geller 2004 (2 citations) Gullliver 2003 (1 citation) Ledson 1998 (2 citations) Pradal 2002 ( 1 citation) Wainwright 2002 (1 citation) Westerman 2003 (2 citations) NEWLY INCLUDED Gibson 2003 (2 citations) Murphy 2004 (3 citations) Wiesemann 1998 (2 citations) Methodological quality of included studies This section has been revised by using a new method to classify quality criteria, describing the criteria for individual studies in a table and summarising the results in the text. The results of this quality assessment has not been used for study selection or in analysis. Results The inclusion of three studies has not significantly changed the results. Gibson 2003 reported only adverse effects, the primary outcome of the study was density of Pseudomonas aeruginosa, which was not an outcome of this review. Murphy 2004 added some results to respiratory tract exacerbations (hospitalisation, antibiotic use), lung function, adverse events. Wiesemann 1998 studied people with CF and early acquisition of Pseudomonas. The primary outcome was time to eradication of Pseudomonas; lung function was measured and reported as not different without numbers. |
| 28 May 2003 | New citation required and conclusions have changed | There has been an extensive rewrite of the review. This reflects: 1. inclusion of new trial (Hodson 2002), which is a comparison of two nebulised anti‐pseudomonal antibiotics (tobramycin and colistin); 2. revision of inclusion of cross‐over trials. The seven trials using this study design are included in the review. Elbourne 2000 has discussed issues of pooling results in meta‐analysis. Results from these trials were included in tables of results in previous versions of this review. This is invalid. Therefore, results are not entered into RevMan unless there are data from the first period and considered as a parallel group study. This has reduced the number of tables and graphs; 3. removal of totals from tables of studies of different duration. This has changed estimates of size of effect for "effect on exacerbation of respiratory infection". 4. Abstract: selection criteria and results changed. 5. Criteria: edited according to style policy of CRG. 6. Description of studies: new headings for single antibiotics versus placebo and for antibiotics compared. 7. Methodological quality of included studies: new heading for antibiotics compared. 8. Results: new heading for antibiotics compared. Results of cross‐over design described in text but not used for quantitative estimate of effect. The totals that included trials of different durations were removed. 9. Discussion: altered discussion on selection criteria and on place of cross‐over design trials in this review. 10. Comparisons: results taken from cross‐over trials removed from tables. Totals removed from analyses of trials of different duration. |
| 27 May 2003 | New search has been performed | The search carried out on the Collaborative review Group (CRG) cystic fibrosis controlled trials register found 13 references as potential trials for inclusion in this update of the review. Two were not considered further (case series and not Pseudomonas aeruginosa). One was selected for inclusion (Hodson 2002). Seven were further analyses of the trial reported and already included as Ramsay 1999. The other three were single dose studies. GR selected trials and extracted data for this update. |
| 17 May 2003 | New citation required and conclusions have changed | Substantive amendment |
| 29 August 2000 | New search has been performed | Minor update |
| 26 October 1999 | Amended | Review re‐formatted |
Acknowledgements
We would like to thank previous authors of this review for their input: Gerard Ryan (Sir Charles Gairdner Hospital, Perth, Australia), Meenu Singh, Kerry Dwan and Somnath Mukhopadhyay (University of Dundee) and Kate Regan (NHS Lothian, Edinburgh, UK).
This project was supported by the National Institute for Health and Care Research (NIHR), via Cochrane Infrastructure funding to the Cochrane Cystic Fibrosis and Genetic Disorders Group. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health and Social Care.
Appendices
Appendix 1. Electronic search strategies
| Database / Resource | Search strategy | Date searched |
| clinicaltrials.gov (clinicaltrials.gov/) |
cystic fibrosis and pseudomonas aeruginosa and inhaled antibiotics; study type: interventional |
7 June 2022 |
| WHO ICTRP (apps.who.int/trialsearch/) |
cystic fibrosis and pseudomonas aeruginosa and inhaled antibiotics | 7 June 2022 |
Data and analyses
Comparison 1. Inhaled anti‐pseudomonal antibiotic (IAPA) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Mean absolute FEV1 (% predicted) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1.1 At 3 months | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | ‐2.00 [‐22.41, 18.41] |
| 1.1.2 Over 3 months and up to 12 months | 1 | 245 | Mean Difference (IV, Fixed, 95% CI) | 3.10 [‐2.35, 8.55] |
| 1.2 Mean change in FEV1 (% predicted) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.2.1 At 3 months | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 6.00 [‐1.07, 13.07] |
| 1.3 Mean change in % predicted FEV1 | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.3.1 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 6.38 [2.94, 9.82] | |
| 1.4 Rate of change of FEV1 (% predicted per year) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.4.1 Over 24 months and up to 36 months | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | 7.80 [3.29, 12.31] |
| 1.5 Mean absolute FVC (% predicted) at end of treatment | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.5.1 At 1 to 3 months | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 8.00 [‐12.18, 28.18] |
| 1.6 Mean change in FVC (% predicted) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.6.1 At 1 to 3 months | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 11.00 [1.94, 20.06] |
| 1.6.2 Over 3 months and up to 12 months | 1 | 245 | Mean Difference (IV, Fixed, 95% CI) | 4.60 [1.01, 8.19] |
| 1.7 Rate of change of FVC (% predicted per year) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.7.1 Over 24 months and up to 36 months | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | 5.40 [0.86, 9.94] |
| 1.8 Frequency of one or more hospital admissions | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.8.1 Over 3 months and up to 12 months | 3 | 946 | Risk Ratio (M‐H, Random, 95% CI) | 0.66 [0.47, 0.93] |
| 1.8.2 Over 12 months and up to 24 months | 1 | 181 | Risk Ratio (M‐H, Random, 95% CI) | 0.59 [0.34, 1.05] |
| 1.8.3 Over 24 months and up to 36 months | 1 | 27 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.39, 1.65] |
| 1.9 Hospital admissions, mean number of days in hospital | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.9.1 Over 24 months and up to 36 months | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐3.20 [‐9.04, 2.64] |
| 1.10 Frequency of one or more courses of intravenous antibiotics | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.10.1 Over 3 months and up to 12 months | 2 | 765 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.67, 0.88] |
| 1.10.2 Over 12 months and up to 24 months | 1 | 175 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.35, 1.08] |
| 1.11 Pulmonary exacerbations | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.11.1 Over 3 months and up to 12 months | 1 | 245 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.59, 1.03] |
| 1.12 Lost school or working days | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.12.1 Over 3 months and up to 12 months | 1 | 245 | Mean Difference (IV, Fixed, 95% CI) | ‐5.30 [‐8.59, ‐2.01] |
| 1.13 Deaths | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.13.1 Over 3 months and up to 12 months | 2 | 767 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.17 [0.03, 1.09] |
| 1.13.2 Over 24 months and up to 36 months | 1 | 27 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.27 [0.01, 6.11] |
| 1.14 Frequency of tobramycin‐resistant P. aeruginosa at end of study | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.14.1 Over 3 months and up to 12 months | 2 | 672 | Risk Ratio (M‐H, Random, 95% CI) | 1.95 [0.86, 4.42] |
| 1.14.2 Over 24 months and up to 36 months | 1 | 26 | Risk Ratio (M‐H, Random, 95% CI) | 7.80 [0.46, 131.62] |
| 1.15 Frequency of new isolates of drug resistant organisms (at end of study) | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.15.1 Burkholderia cepacia | 2 | 536 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.26 [0.03, 1.99] |
| 1.15.2 Stenotrophomonas maltophilia | 1 | 520 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.05 [0.32, 29.10] |
| 1.15.3 Alcaligenes xylosoxidans | 1 | 520 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.06, 16.15] |
| 1.15.4 Aspergillus species | 1 | 389 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.12 [1.29, 3.46] |
| 1.16 Number experiencing adverse event (at end of study) | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.16.1 Auditory impairment | 4 | 540 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 1.16.2 Tinnitus | 1 | 520 | Risk Ratio (M‐H, Random, 95% CI) | 17.26 [1.00, 297.54] |
| 1.16.3 Voice alteration | 2 | 701 | Risk Ratio (M‐H, Random, 95% CI) | 2.66 [1.14, 6.25] |
| 1.16.4 Pneumothorax | 1 | 520 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.03, 2.26] |
| 1.16.5 Hemoptysis | 1 | 520 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.66, 1.13] |
Comparison 2. Colistimethate sodium dry powder (CDPI) versus tobramycin for inhalation solution (TIS).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 Number of pulmonary exacerbations | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1.1 Over 3 months and up to 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.2 Time to first pulmonary exacerbation | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.2.1 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.3 Deaths | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.3.1 Over 3 months and up to 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.4 Adverse events (at end of study) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.4.1 Total adverse events | 1 | 379 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.99, 1.12] |
| 2.4.2 Treatment‐related adverse events | 1 | 379 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.76 [1.50, 2.08] |
| 2.4.3 Mild adverse events | 1 | 379 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.92, 1.09] |
| 2.4.4 Moderate adverse events | 1 | 379 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.32 [1.11, 1.57] |
| 2.4.5 Severe adverse events | 1 | 379 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.83 [2.15, 6.83] |
Comparison 3. Inhaled TOBI® (IV preparation) versus tobramycin for inhalation solution (TIS).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 FEV1 % predicted | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.1.1 At 1 to 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.2 FVC | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.2.1 At 1 to 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Comparison 4. Tobramycin inhalation powder (TIP) versus tobramycin for inhalation solution (TIS).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 4.1 FEV1 (% predicted) relative change | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.1.1 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.2 Hospitalisations | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.2.1 Over 3 months and up to 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.3 Pulmonary exacerbations | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.3.1 Over 3 months and up to 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.4 Deaths | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5 Adverse events (at end of study) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.1 Any adverse event | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.2 Bronchospasm | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.3 Cough | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.4 Productive cough | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.5 Dyspnoea | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.6 Pyrexia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.7 Oropharyngeal pain | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.8 Dysphonia (hoarseness) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.9 Haemoptysis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.10 Headache | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.11 Nasal congestion | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.12 Nausea | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.13 Rales | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.14 Rhinorrhea | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.15 Pulmonary function test decreased | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.16 Upper respiratory tract infection | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.17 Wheezing | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.18 Chest discomfort | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.19 Fatigue | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.20 Vomiting | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.21 Sinusitis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.5.22 Pulmonary congestion | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
Comparison 5. Inhaled aztreonam lysine (AZLI) versus tobramycin for inhalation solution (TIS).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 5.1 FEV1 % predicted ‐ mean relative change from baseline | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1.1 At Week 24 (average across 3 cycles) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.2 FEV1 % predicted ‐ mean actual change from baseline | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.2.1 At Week 24 (averaged across 3 cycles) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.3 Need for additional antibiotics | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5.3.1 At Week 24 | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5.4 Number of days of additional antibiotics | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.4.1 At Week 24 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.5 Weight (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.5.1 At Week 24 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.6 Quality of Life ‐ CFQR respiratory symptom scale | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.6.1 At Week 24 (average across 3 cycles) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.7 TSQM ‐ effectiveness | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.7.1 At week 24 (average across 3 cycles) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.8 TSQM ‐ global satisfaction | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.8.1 At Week 24 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.9 TSQM ‐ side effects | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.9.1 At Week 24 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.10 TSQM ‐ convenience | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.10.1 At Week 24 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.11 Log10Pseudomonas aeruginosa CFU/g sputum | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.11.1 At Week 24 (average across 3 cycles) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.12 Adverse events (at end of study) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.12.1 Treatment‐related adverse events | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.77 [1.03, 3.04] |
| 5.12.2 Serious adverse events | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.94 [0.98, 3.84] |
| 5.12.3 Cough | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.78, 1.03] |
| 5.12.4 Productive cough | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.69, 1.07] |
| 5.12.5 Pyrexia | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.73, 1.49] |
| 5.12.6 Oropharyngeal pain | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.64, 1.40] |
| 5.12.7 Dyspnoea | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.57, 1.30] |
| 5.12.8 Haemoptysis | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.43 [0.87, 2.36] |
| 5.12.9 Rales | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.54, 1.27] |
| 5.12.10 Headache | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.65, 1.66] |
| 5.12.11 Nasal congestion | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.68, 1.74] |
| 5.12.12 Rhinorrhea | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.46, 1.17] |
| 5.12.13 Exercise tolerance decreased | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.55, 1.46] |
| 5.12.14 Fatigue | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.56, 1.55] |
| 5.12.15 Decreased appetite | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.54, 1.75] |
| 5.12.16 Abdominal pain | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.18 [0.98, 4.85] |
| 5.12.17 Respiratory tract congestion | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.44, 1.52] |
| 5.12.18 Wheezing | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.42, 1.43] |
| 5.12.19 Chest discomfort | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.51, 2.14] |
| 5.12.20 Nausea | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.36 [0.63, 2.95] |
| 5.12.21 Vomiting | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.48, 1.96] |
| 5.12.22 Pulmonary function decreased | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.31, 1.29] |
| 5.12.23 Breath sounds abnormal | 1 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.52 [0.23, 1.18] |
Comparison 6. Amikacin liposome inhalation suspension (ALIS) versus TOBI®.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 6.1 Hospitalisations ‐ number of participants hospitalised (all‐cause) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6.2 Change from baseline in CFQ‐R domain scores | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.2.1 Respiratory domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | ‐0.06 [‐4.55, 4.43] |
| 6.2.2 Body image domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | 1.16 [‐4.54, 6.86] |
| 6.2.3 Digestive domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | 1.15 [‐3.51, 5.81] |
| 6.2.4 Eating disturbances domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | ‐2.41 [‐6.50, 1.68] |
| 6.2.5 Emotions domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | 0.22 [‐2.95, 3.39] |
| 6.2.6 Energy and wellbeing | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | 1.15 [‐3.91, 6.21] |
| 6.2.7 Health perception domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | 2.05 [‐2.91, 7.01] |
| 6.2.8 Physical domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | ‐1.44 [‐6.66, 3.78] |
| 6.2.9 Role limitations domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | 0.55 [‐4.86, 5.96] |
| 6.2.10 Social limitations domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | ‐1.12 [‐4.79, 2.55] |
| 6.2.11 Treatment burden domain | 1 | 294 | Mean Difference (IV, Fixed, 95% CI) | 0.35 [‐4.10, 4.80] |
| 6.3 Treatment‐emergent adverse events (TEAEs) | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6.3.1 Number of participants with any TEAE | 1 | 294 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.47 [0.81, 2.66] |
| 6.3.2 Participants experiencing a mild TEAE | 1 | 294 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.64, 1.68] |
| 6.3.3 Participants experienciing a moderate TEAE | 1 | 294 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.67, 1.69] |
| 6.3.4 Participants experiencing a severe TEAE | 1 | 294 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.26 [0.77, 6.69] |
| 6.3.5 Participants experiencing treatment‐emergent SAEs | 1 | 294 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.48, 1.55] |
Comparison 7. Levofloxacin for inhalation solution (LIS) versus tobramycin for inhalation solution (TIS).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 7.1 Absolute change in FEV1 % predicted | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1.1 At three months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1.2 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.2 Relative change in FEV1 % predicted | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.2.1 At three months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.2.2 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.3 Absolute change in FVC % predicted | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.3.1 At three months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.3.2 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.4 Relative change in FVC % predicted | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.4.1 At three months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.4.2 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.5 Hospitalisations due to respiratory exacerbations | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.5.1 Over 3 months and up to 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.6 Weight decrease | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.6.1 Over 3 months and up to 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.7 Change in P aeruginosa sputum density (log10 CFU/g) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.7.1 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.8 Adverse events (at end of study) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.1 Cough | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.2 Increased sputum | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.3 Respiratory tract congestion | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.4 Increased viscosity of bronchial secretions | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.5 Paranasal sinus hypersecretion | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.6 Haemoptysis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.7 Discoloured sputum | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.8 Exertional dyspnoea | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.9 Rales | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.10 Dyspnoea | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.11 Oropharyngeal pain | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.12 Epistaxis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.13 Disease progression | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.14 Fatigue | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.15 Decreased exercise tolerance | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.16 Pyrexia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.17 Malaise | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.18 Increase in blood glucose | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.19 Dysgeusia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.20 Sinus headache | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.21 Headache | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.22 Nasopharyngitis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.23 Sinusitis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.24 Upper respiratory tract infection | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.25 Abdominal pain | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.26 Nausea | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.27 Arthralgia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.28 Decreased appetite | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.8.29 Rash | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
Comparison 8. Continuous aztreonam (AZLI)/tobramycin (TIS) versus intermittent tobramycin (TIS).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 8.1 Mean change from baseline ‐ FEV1 % predicted | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 8.1.1 Over 3 months and up to 12 months (values from end of 3 cycles averaged) | 1 | Mean Difference (IV, Fixed, 95% CI) | 1.33 [‐0.51, 3.17] | |
| 8.2 Rate of hospitalisation per participant year | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.35, 1.11] |
| 8.2.1 Over 3 months and up to 12 months | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.35, 1.11] |
| 8.3 Need for additional antibiotics for an exacerbation | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.59, 1.32] |
| 8.3.1 Over 3 months and up to 12 months | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.59, 1.32] |
| 8.4 Rate of protocol defined pulmonary exacerbations per participant year | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.43, 1.18] |
| 8.4.1 Over 3 months and up to 12 months | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.43, 1.18] |
| 8.5 Quality of life ‐ CFQ‐R respiratory symptom score | 1 | Mean Difference (IV, Fixed, 95% CI) | 3.06 [‐1.61, 7.73] | |
| 8.5.1 Over 3 months and up to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 3.06 [‐1.61, 7.73] | |
| 8.6 Incidence of other respiratory pathogens (at end of study) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 8.6.1 P aeruginosa | 1 | 87 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.94, 1.06] |
| 8.6.2 Achromobacter species | 1 | 87 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.42, 3.90] |
| 8.6.3 Stenotrophomonas maltophilia | 1 | 87 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.40, 1.90] |
| 8.6.4 Aspergillus spp. | 1 | 87 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.35, 1.22] |
| 8.6.5 MRSA | 1 | 87 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.35, 1.22] |
| 8.6.6 Burkholderia spp. | 1 | 87 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.21 [0.13, 76.67] |
| 8.6.7 MSSA | 1 | 76 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.35, 1.33] |
| 8.7 Adverse events (at end of study) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 8.7.1 Any comparative phase adverse event | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.90, 1.05] |
| 8.7.2 Adverse events grade 1‐2 severity | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.23, 5.13] |
| 8.7.3 Adverse events grade 3‐4 severity | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.54, 1.91] |
| 8.7.4 Serious adverse events | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.64, 1.44] |
| 8.8 Treatment‐emergent adverse events (at end of study) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 8.8.1 Cough | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.83, 1.36] |
| 8.8.2 Sputum increased | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.49, 1.03] |
| 8.8.3 Dyspnoea | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.59 [0.35, 1.01] |
| 8.8.4 Fatigue | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.38, 1.33] |
| 8.8.5 Haemoptysis | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.53, 2.26] |
| 8.8.6 Nasal congestion | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.01 [1.04, 8.74] |
| 8.8.7 Pulmonary function test decreased | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.57, 2.54] |
| 8.8.8 Respiratory tract congestion | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.53, 2.26] |
| 8.8.9 Infective pulmonary exacerbation of CF | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.19 [0.82, 5.89] |
| 8.8.10 Lung disorder | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.36, 1.59] |
| 8.8.11 Wheezing | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.48, 2.50] |
| 8.8.12 Chest discomfort | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.31, 1.46] |
| 8.8.13 Pyrexia | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.31, 1.46] |
| 8.8.14 Headache | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.38, 2.41] |
| 8.8.15 Diarrhoea | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.31 [0.43, 3.99] |
| 8.8.16 Nausea | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.26, 1.65] |
| 8.8.17 Oropharyngeal pain | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.31 [0.43, 3.99] |
| 8.8.18 Decreased Appetite | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.14, 0.85] |
| 8.8.19 Dyspnoea exertional | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.74 [0.56, 13.37] |
| 8.8.20 Rhinorrhoea | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.24, 1.93] |
| 8.8.21 Sputum discoloured | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.83 [0.46, 7.18] |
| 8.8.22 Vomiting | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.22, 1.67] |
| 8.8.23 Chest pain | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.20, 1.99] |
| 8.8.24 Weight decreased | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.25, 3.05] |
| 8.8.25 Chills | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.17, 2.58] |
| 8.8.26 Exercise tolerance decreased | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.27 [0.08, 0.90] |
| 8.8.27 Sinus congestion | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.13, 1.70] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Assael 2013.
| Study characteristics | ||
| Methods | Open‐label RCT (randomised 1:1). Parallel design. Duration: 6 months ‐ 3 cycles of 28 days on and 28 days off. Multicentre: 91 centres in Europe and USA. |
|
| Participants | 273 participants with documented CF diagnosis, aged 6 years and over, positive P aeruginosa sputum culture in previous 3 months, FEV1 75% or less at screening. Age (mean (SD)): AZLI 25.8 (9.1) years; TIS 25.1 (9.0) years. Gender split n (% males): AZLI 68 (50%); TIS 66 (50%). CFTR genotype (n (%)): homozygous for Δ508 ‐ AZLI 64 (54.7) and TIS 60 (54.1); heterozygous for Δ508 ‐ AZLI 36 (30.8) and TIS 30 (27.0); unidentified/other ‐ AZLI 17 (14.5) and TIS 21 (18.9). FEV1 % predicted at screening (n (%)): > 50% to ≤ 75% ‐ AZLI 76 (55.9) and TIS 75 (56.8); ≤ 50% ‐ AZLI 60 (44.1) and TIS 57 (43.2); < 25% ‐ AZLI 6 (4.4) and TIS 6 (4.5). Baseline FEV1 % predicted baseline values (mean (SD)): AZLI 52.3 (15.6); TIS 52.2 (14.6). Baseline FEV1 (L) (mean (SD)): AZLI 1.8 (0.6); TIS 1.8 (0.6). Baseline CFQ‐R respiratory symptom score (mean (SD)): AZLI 62.9 (20.4); TIS 58.0 (20.8). |
|
| Interventions |
Intervention 1 (n = 136): AZLI 75 mg 3x daily via PARI eFlow electronic nebuliser. Intervention 2 (n = 132): TIS 300 mg 2x daily via PARI LC Plus nebuliser with compressor or via another nebuliser compatible with country‐specified labelling. |
|
| Outcomes |
Primary outcomes: non‐inferiority of AZLI for relative change in FEV1 % predicted at day 28; superiority of AZLI for relative change in FEV1 % predicted over 3 treatment cycles. Secondary outcomes: time to need for additional IV antibiotics; CFQ‐R change from baseline for respiratory symptom scores; number of respiratory hospitalisations; additional anti‐pseudomonal use; change in weight from baseline; change in P aeruginosa sputum density; treatment satisfaction questionnaire. |
|
| Notes | 26‐week active comparator period followed by an optional 24‐week open‐label single‐arm extension period for 3 months. Additional antibiotics allowed for diagnosis of pulmonary exacerbations. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Paper states randomised using ratio of 1:1; supplementary paper confirms randomisation by interactive voice/web response system using a code generated by Gilead. |
| Allocation concealment (selection bias) | Low risk | Interactive voice/web response system used. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label design, first treatment given 2x daily and the other 3x daily. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Open‐label design. An independent data safety board monitored adverse events during the trial, and an independent, blinded review committee identified respiratory hospitalisations and IV and inhaled anti‐pseudomonal antibiotics used for respiratory events. Unclear as to how a blinded monitoring committee might affect results. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Statistical analyses were performed on the ITT population: randomised participants receiving at least 1 dose of trial drug. 268/273 randomised participants received at least 1 dose: AZLI 136/137 or TNS 132/136. 233/273 participants (85.3%) completed the active‐comparator period. Reasons for withdrawal given for all dropouts. |
| Selective reporting (reporting bias) | Low risk | Primary and secondary outcomes reported with 95% CIs (relative and actual change in FEV1 % predicted). No protocol available but all outcomes listed in the methods are reported in the results. |
| Other bias | Unclear risk | The trial was funded by Gilead Sciences. 4 authors had consultancies with them and 3 authors are shareholders and/or employees. |
Bilton 2020.
| Study characteristics | ||
| Methods | RCT. Parallel design. Duration: 6 months ‐ 3 cycles of 28 days on and 28 days off. Multicentre: 70 sites across 17 countries in Europe and Canada. |
|
| Participants | People with CF confirmed by a positive sweat test (i.e. ≥ 60 mmol/ L) or DNA analysis and chronic P aeruginosa infection (confirmed by 3 positive cultures within 2 years ( ≥ 1 obtained within 6 months) prior to screening and positive sputum cultures at screening. Aged 6 years and over. 302 randomised, 296 dosed. 152 patients were assigned to amikacin liposome inhalation suspension (ALIS) 590 mg and 150 patients to TIS. 59.2% were adults; ALIS 58.8%, TIS 59.6%. Mean (SD) age: ALIS 22.8 years (10.2), TIS 22.0 years (10.0). Gender (% male): ALIS 53.4%; TIS 52.1%; overall 52.7%. FEV1 % predicted mean (SD): ALIS 64.5% (21.5); TIS 61.9 (22.0). BMI mean (SD): ALIS 20.1 (4.0); TIS 19.7 (3.7). Use of bronchodilator n (%): ALIS 113 (76.4%); TIS 111 (76.0%). Use of azithromycin n (%): ALIS 76 (51.4%); TIS 73 (50.0%). Demographic and baseline characteristics were comparable between the 2 arms. |
|
| Interventions |
Intervention 1: ALIS amikacin 590 mg/8.4 mL once daily with eFlow® nebuliser (PARI Pharma GmbH, Munich, Ger‐ many). Intervention 2: TIS (TOBI®) 300 mg 2x daily via PARI LC® PLUS nebuliser dosed at approximately 12 hours apart and not < 6 hours apart. 1 treatment cycle was defined as 28 days on treatment followed by 28 days off treatment; all patients received 3 treatment cycles. |
|
| Outcomes | Primary endpoint: relative change from baseline to end of study in FEV 1 (L). Secondary endpoints: changes from baseline during therapy in FEV 1 (L) and FEV 1 % predicted; change from baseline in respiratory symptoms as measured by the Cystic Fibrosis Questionnaire‐Revised (CFQ‐R); time to first protocol‐defined exacerbation (any 4 of 12 signs and symptoms of the Fuchs criteria); change from baseline in log 10 colony‐forming units (CFU) of P aeruginosa; all‐cause hospitalisations. Safety endpoints: acute tolerability measured by treatment‐emergent adverse events (TEAEs); AEs leading to discontinuation, serious AEs, laboratory abnormalities, audiology, serum creatinine changes, need for concomitant medications, and predose‐to‐postdose changes in pulmonary function tests, vital signs, and SaO 2. Study visits at weeks 2 and 4 and monthly thereafter with telephone assessments between monthly visits. |
|
| Notes | Follow‐on open‐label trial, 75% of participants rolled over to this. Trial completed, but according to clinicaltrials.gov request to delay results was received in February 2015. Full paper published in 2020. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | States randomised in a 1:1 ratio; stratified by age and lung function. No further details. |
| Allocation concealment (selection bias) | Unclear risk | No description of allocation concealment given. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | First treatment given 1x daily and the other treatment given 2x daily, used different nebulisers. Open‐label study with no masking. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details given. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Less than 15% of participants dropped out of the study (ALIS 11%, TIS 7%). A total of 274 patients completed the study and 266 per protocol. A modified ITT was used to analyse the data in addition to a per‐protocol analysis. Little information given on reasons for withdrawal from the study although the most common reasons for discontinuation of the study drug were protocol‐defined safety criteria or AEs (ALIS 7.2%; TIS 2.0%) and other reasons (ALIS 7.2%; TIS 4.0%). |
| Selective reporting (reporting bias) | Low risk | All outcomes reported in the protocol were reported in the full paper. |
| Other bias | Low risk | No other risk of bias identified. |
Chuchalin 2007.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled RCT. Allocation used was 2:1 (tobramycin: placebo). Parallel design. Duration: 24 weeks (4 weeks 'on treatment' followed by 4 weeks 'off treatment'). Multicentre: 21 sites across Hungary, Poland and Russia. |
|
| Participants | Diagnosis of CF and P aeruginosa. 247 randomised; 245 included in ITT population. Gender split n (% males): 135 (55%) Age range: 6 to 31 years (tobramycin group), 6 to 45 (placebo group). Excluded if received antibiotic therapy in 4 weeks running up to enrolment. Baseline FEV1 % predicted (mean (SD)) tobramycin group 60.7 (14.8); placebo group 63.6 (15.0). |
|
| Interventions |
Intervention 1: tobramycin 300 mg (Bramitob®). Intervention 2: placebo (saline solution with quinine hydrochloride solution). Administered for 24 weeks (4 weeks 'on treatment' followed by 4 weeks 'off treatment') using a Pari LC Plus jet nebuliser and Pari Turbo Boy air compressor. |
|
| Outcomes | FEV1, FVC, FEF25-75, sputum (P aeruginosa density, tobramycin susceptibility), other pathogens, pulmonary exacerbations, use of parenteral anti‐pseudomonal antibiotics, number of hospitalisations, loss of school/work days, audiometric test, renal function, adverse events. | |
| Notes | Supported by Chiesi Famaceutici SpA (Italy), MDS Pharma Services (France). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised. Method not stated, ratio tobramycin to placebo 2:1. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. Multicentre. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind, quinine hydrochloride added to placebo to mask taste. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No specific details given about outcome assessors, but described as double‐blind. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 247 randomised, 245 ITT analysis, 215 PP analysis. 232 completed, 6.1% dropout rate (tobramycin group 7 dropouts (4.3%), placebo group 8 dropouts (9.3%)). Reasons given. |
| Selective reporting (reporting bias) | Unclear risk | Not clear if results for microbiology are ITT or PP. |
| Other bias | Unclear risk | Pharmaceutical industry support. |
Day 1988.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled trial. Allocation method not stated.
Cross‐over design. Duration: 6 months. |
|
| Participants | 14 participants. Criteria for diagnosis of CF not stated. All colonised with P aeruginosa and entered the trial following a course of IV anti‐pseudomonal antibiotics. Age range 5 to 16 years. Gender split n (% males): 7 (50%). Lung function at baseline (FEV1 % predicted): range 30% to 106%. |
|
| Interventions |
Intervention 1: Colomycin® 1 million units 2x daily for 6 months. Intervention 2: placebo (saline) 2x daily for 6 months. |
|
| Outcomes | Lung function (FEV1 and FVC), exacerbations (antibiotic use and hospital admissions), symptom score and weight. | |
| Notes | Nebuliser (type not stated) with 2.0 mL solution. FEV1 result not stated. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Unclear. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Reported as double‐blind, but not stated who was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Reported as double‐blind, but not stated who was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 1 participant withdrawn and results included in analysis. Dropout rate not clearly stated. |
| Selective reporting (reporting bias) | High risk | Outcomes partially reported as article is only in abstract form. P values or means available for cough, sputum quantity, FVC, FEV1. Weight, height, oral antibiotic usage and hospital admission are mentioned, but no results reported. |
| Other bias | Unclear risk | Cross‐over design. No information given on design of cross‐over or analysis. |
Elborn 2015.
| Study characteristics | ||
| Methods | Open‐label RCT (randomised 2:1). Parallel design. Duration: 6 months ‐ 3 cycles of 28 days on and 28 days off. Monthly trial visits. Multicentre: 125 centres in Europe, USA and Israel. |
|
| Participants | People with documented CF diagnosis and chronic lung infection (defined in paper) aged 12 years and over, mean baseline age 28.5 years; baseline FEV1 % predicted 25% to 85%. 282 randomised, although 10 did not even receive a single dose, 23/272 discontinued. Age (mean (SD) and median): LIS 28.1 (8.96) years, median 27.0 years; TIS 28.8 (10.94) years, median 26.0 years. Gender split n (% males): LIS 103 (54.5%); TIS 56 (60.2%). FEV1 % predicted (mean (SD)): LIS 54.8 (16.96)%; TIS 53.2 (15.70)%. |
|
| Interventions |
Intervention 1 (n = 189): LIS (Aeroquin™, MP376, APT‐1026) 240 mg (2.4 mL of 100 mg per mL solution of levofloxacin as Apt‐1026) 2x daily via PARI investigational eFlow nebuliser. Intervention 2 (n = 93): TIS 300 mg (5 mL) (TOBI) 2x daily via PARI LC Plus nebuliser. |
|
| Outcomes | FEV1 % predicted; time to next anti‐pseudomonal antibiotics, CFQ‐R respiratory domain score, time to next exacerbation (as defined by Fuchs), hospitalisation, adverse events. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised in a ratio of 2:1 using an Interactive Voice Response System and was stratified by geographical region, age and FEV1 % predicted (supplementary e‐information). |
| Allocation concealment (selection bias) | Low risk | Randomisation was carried out using an Interactive Voice Response System. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and trial coordinators were aware of the treatment assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Site investigators and medical monitors remained blinded in order to minimise treatment bias during the trial. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Statistical analysis was performed on the ITT population consisting of all randomised participants. In TIS group, 3/93 did not receive TIS at all, reasons given for 7 discontinuations (adverse event n = 1; withdrawal of consent n = 5; investigator decision n = 1); in LIS group 7/189 did not receive drug, reasons given for 16 discontinuations (adverse event n = 6; withdrawal of consent n = 7; investigator decision n = 2; lost to follow‐up n = 1). |
| Selective reporting (reporting bias) | Low risk | In the results section the authors report the results of categorical change in FEV1 % predicted but they do not state this in the methods. Outcomes listed in the methods are reported in the paper. |
| Other bias | Low risk | No other sources of bias found. |
Flume 2016b.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled RCT.
Parallel design. Duration: 28‐day run in with TIS, followed by 3 4‐week cycles of AZLI or placebo alternating with 28 days of TIS open label. Total treatment time 28 weeks. Multicentre trial: 45 US CF centres. |
|
| Participants | Males or females older than 6 years, with a diagnosis of CF (sweat test or genetic) and documented presence of P aeruginosa. Participants had to be able to perform reproducible pulmonary function tests, have an FEV1 between 25% and 75% and a history of at least 1 hospitalisation or 1 course of IV antibiotics in the 12 months prior to screening. 90 participants randomised; 88 received the intended treatment and were analysed. Age (mean (SD)): overall ‐ AZLI 28.5 (12.1), placebo 28.3 (10.8). Gender (n (%)) male: AZLI 18 (42.9), placebo 19 (42.3). FEV1 % predicted (mean(SD)): AZLI 49.9 (17.7), placebo 50.1 (15.3). CFQ‐R RSS score (mean (SD)): AZLI 60.2 (18.3), placebo 64.2 (15.2). Number of acute respiratory exacerbations requiring IV antibiotics during year before screening (n (%)): AZLI 1 exacerbation 22 (52.4), 2 exacerbations 9 (21.4), 3 exacerbations 11 (26.2); placebo 1 exacerbation 27 (58.7), 2 exacerbations 6 (13.0), 3 exacerbations 13 (28.3). |
|
| Interventions | All participants received 28 days of TIS 300 mg 2x daily in the run‐in period followed by 3 cycles (28‐days) of AZLI or placebo. The 3 treatment cycles were alternated with TIS 300 mg 2x daily. Intervention 1: AZLI (Cayston, Gilead Sciences Inc) 75 mg (diluted in 0.17% NaCL) 3x daily. Intervention 2: placebo: lactose monohydrate and sodium chloride reconstituted with the same diluent used for AZLI (0.17% w/v sodium chloride solution) 3x daily. TIS (Novartis Pharmaceuticals Corp): 300 mg 2x daily for 28 days in the run‐in period then 300 mg 2x daily in the comparative phase in between the 3 cycles of AZLI versus placebo. |
|
| Outcomes | FEV1 measured in L or % predicted. Exacerbation of respiratory infection (measured as a defined event or as the need for hospitalisation or parenteral antibiotics or both). |
|
| Notes | Azithromycin use at day 1 or during comparative phase (or both) (n (%)): AZLI 34 (81.0), placebo 36 (78.3). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Eligible participants were stratified by disease severity and number of acute respiratory exacerbations. 1:1 randomisation. Method of randomisation not described. |
| Allocation concealment (selection bias) | Unclear risk | No description of allocation concealment methods. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Double‐blind trial. Participants and investigators were blinded but no methods described. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Yes – there was an independent blinded adjudication committee to review outcome data. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 16 out of 90 randomised participants failed to complete the trial (> 15%). All withdrawals were described and accounted for: withdrew consent n = 10 (AZLI n = 3, placebo n = 7); non‐compliance with trial drug n = 1 (AZLI n = 1, placebo = 0); adverse event n = 2 (AZLI n = 1, placebo n = 1); death n = 1 (AZLI n = 1, placebo = 0); pregnancy n = 1 (AZLI n = 0, placebo = 1); investigators' discretion n = 1 (AZLI n = 0, placebo = 1); other n = 2 (AZLI n = 1, placebo n = 1). |
| Selective reporting (reporting bias) | Low risk | All outcomes reported in the methods and trial documentation are reported in the results. Trial registration documentation could be accessed. |
| Other bias | Unclear risk | Trial enrolment was limited and so the trial was underpowered. |
Hodson 1981.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled RCT. Cross‐over design. Duration: 6 months. | |
| Participants | Criteria for diagnosis of CF were clinical features and elevated sweat sodium. All with P aeruginosa in sputum culture. 20 participants randomised. Age: range 15 to 42 years. Gender split n (% males): 11 (55%). No participant received IV chemotherapy during the 2 weeks before the trial. |
|
| Interventions |
Intervention 1: carbenicillin 1 g and gentamicin 80 mg 2x daily for 6 months via Bird nebuliser. Intervention 2: placebo (hypertonic saline and lactose) 2x daily for 6 months via Bird nebuliser. |
|
| Outcomes | Lung function (FEV1, FVC, PEFR), exacerbations of infection (courses of IV antibiotics), sputum culture and sensitivity, audiogram. | |
| Notes | No baseline clinical features. Sponsor: Beecham and Roussel Laboratories. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as randomised, but no method stated. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Reported as double‐blind, but not stated who was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Reported as double‐blind, but not stated who was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 16/20 completed, 4 dropouts (intervention arm uncertain). 17 analysed. Attrition rate 15%. |
| Selective reporting (reporting bias) | Unclear risk | FEV1, reported as mean of monthly measurements for 6 months with no SD. Graphs of FEV1, FEV and PEFR were presented. |
| Other bias | Unclear risk | Possible unblinding of intervention. Cross‐over design, no information given regarding a washout period or how data were analysed. Sponsor Beecham and Roussel Laboratories. |
Jensen 1987.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled RCT. Parallel design. Duration: 3 months. | |
| Participants | Diagnostic criteria for CF not stated. 40 participants with chronic P aeruginosa infection. Age range 7 to 35 years. Gender split n (% males): 20 (50%). Baseline lung function (FEV1 % predicted) mean (SD): 71% (25) and 79% (29) predicted in 2 treatment groups. |
|
| Interventions |
Intervention 1: colistin (1 million units) 2x daily for 3 months, delivered by Raindrop nebuliser with 3.0 mL of solution. Intervention 2: placebo (normal saline) 2x daily for 3 months, delivered by Raindrop nebuliser with 3.0 mL of solution. Before entering the trial a 2‐week course of parenteral anti‐pseudomonal treatment was given to all participants. |
|
| Outcomes | Lung function (FEV1 and FVC), clinical score, sputum culture and sensitivity, blood tests (ESR, WCC). | |
| Notes | FEV1 result (% predicted) at end of treatment and as change from baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as randomised, but method not stated. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Reported as double‐blind, but not stated who was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Reported as double‐blind, but not stated who was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 29/40 completed; 2 from colistin group and 9 from placebo group dropped out (reasons given). Attrition rate 28%. |
| Selective reporting (reporting bias) | High risk | Tolerance, FEF, Shwachman score and nocturnal cough are partially reported so that data could not be included in a meta‐analysis i.e. 'no significant difference'. No protocol was available for a more thorough assessment. |
| Other bias | High risk | Uneven withdrawals; 2/20 in colistin group and 9/20 in placebo group. Mean baseline FEV1 71% predicted (colistin) and 79% predicted (placebo) in participants analysed. |
Konstan 2010b.
| Study characteristics | ||
| Methods | Open‐label safety RCT. Parallel design. Duration: 24 weeks. Multicentre: 127 sites in 15 countries. |
|
| Participants | Inclusion criteria: males or females aged at least 6 years old at screening with confirmed diagnosis of CF and presence of P aeruginosa within 6 months prior to and at screening. Clinically stable with FEV1 % predicted at screening between 25% and 75%. 553 participants randomised: TIP n = 308; TIS n = 209 (36 discontinued prior to treatment, reasons given but group not stated). 517 received at least 1 dose of trial medication. Age mean (SD): TIP 26 (11.4) years; TIS: 25 (10.2) years. Gender split n (% males): TIP 171 (55.5%); TIS 115 (55%). Baseline lung function (FEV1% predicted) (mean (SD)): TIP: 53 (14.2)%; TIS: 53 (15.9)%. |
|
| Interventions |
Intervention 1: TIP 4 capsules (total of 112 mg) 2x daily administered via T‐326 inhaler. Intervention 2: TIS 300 mg/5 mL (TOBI®) 2x daily administered via the PARI LC® PLUS jet nebuliser and DeVilbiss PulmoAide compressor or equivalent alternative. |
|
| Outcomes |
Primary outcome: safety assessed by incidence of treatment‐emergent adverse events (measured at weeks 1, 2, 3, 5, 7, 9, 13, 17, 21 and 25) and clinical laboratory results (measured at weeks ‐4, 1, 5, 9, 13, 17, 21 and 25). Secondary outcomes: serum tobramycin concentrations; audiology test results (at selected CF centres); change in FEV1 % predicted from baseline at weeks 2, 5, 9, 13, 17, 21 and 25; change in sputum P aeruginosa density; treatment satisfaction (assessed using the Treatment Satisfaction Questionnaire for Medication), hospitalisation, anti‐pseudomonal antibiotic use. |
|
| Notes | Official title: 'A randomized, open‐label multicentre Phase 3 trial to assess the safety of tobramycin inhalation powder compared to tobramycin solution for inhalation in cystic fibrosis subjects', also known as 'Safety of tobramycin inhalation powder (TIP) versus tobramycin solution for inhalation in patients with cystic fibrosis (EAGER)'. Sponsor: Novartis. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as randomised in a 3:2 ratio of TIP to TIS. No further details given. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open label. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open label. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | In total 121/517 (23.4%) dropped out with reasons given. TIP: 83/308 (26.9%) dropped out (AE n = 40, death n = 3, consent withdrawn n = 24, lost to follow‐up n = 5, administrative reason n = 1, protocol violation n = 6, other n = 4). TIS: 38/209 (18.2%) dropped out (AE n = 17, consent withdrawn n = 9, lost to follow‐up n = 3, inappropriate enrolment n = 1, protocol violation n = 5, other n = 3). |
| Selective reporting (reporting bias) | Low risk | Results presented for all outcomes. |
| Other bias | Unclear risk | 3 authors have received income from pharmaceutical companies for consulting activities. 5 authors are employees of Novartis Pharmaceuticals. |
Kun 1984.
| Study characteristics | ||
| Methods | RCT stratified into 3 severity groups. Cross‐over design. Duration: 12 months. | |
| Participants | 33 participants with CF (criteria for diagnosis not stated). Age range: 7.8 to 16 years. Gender split not stated. Baseline lung function (FEV1 % predicted): 29% to 105% predicted. Sputum culture at start of treatment (P aeruginosa): gentamicin group n = 12, control group n = 9. |
|
| Interventions |
Intervention 1: gentamicin 20 mg 2x daily after physiotherapy, delivered by Bennett twinjet nebuliser. Intervention 2: usual treatment i.e. no nebulised therapy after physiotherapy. |
|
| Outcomes | Lung function (FEV1), exacerbation (hospital days and antibiotic use), sputum culture, symptom score. | |
| Notes | FEV1 result as % predicted change from baseline (no SD). Sponsor: Essex Laboratories. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | First participant in each of 3 severity groups allocated by chance then subsequent participants alternated gentamicin or saline. |
| Allocation concealment (selection bias) | High risk | Used alternation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and clinicians were not blinded since one group received treatment prior to physiotherapy and the second group received treatment both before and after physiotherapy. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors who saw participants every 3 months were blinded to treatment group. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 29/33 analysed (4 dropouts). Attrition rate 12%. Reasons given. |
| Selective reporting (reporting bias) | Low risk | All stated outcome measures have been reported, although a protocol was not available for a more thorough assessment. |
| Other bias | High risk | Cross‐over design, no information given on washout periods and it seems as though the analysis did not take into account the paired data from the cross‐over design. Sponsor Essex Laboratories. |
MacLusky 1989.
| Study characteristics | ||
| Methods | Single‐blind, placebo‐controlled RCT. Parallel design. Duration: mean duration of trial of 33 months (tobramycin) and 30 months (saline control). | |
| Participants | Criteria for CF chronic lung disease, pancreatic insufficiency and elevated sweat chloride. 28 participants, all had P aeruginosa in sputum culture. Age range 7 to 24 years. Gender split n (% males): 14 ( 50%). Baseline lung function (FEV1 % predicted) (mean (SD)): 78% (21) and 70% (22) predicted in treatment groups. |
|
| Interventions |
Intervention 1: tobramycin 80 mg 2x daily for mean duration of trial (33 months), delivered by Hodson 1730 or Intec 3010 nebuliser with 2 mL of solution. Intervention 2: placebo (normal saline) 2x daily for mean duration of trial (30 months), delivered by Hodson 1730 or Intec 3010 nebuliser with 2 mL of solution. |
|
| Outcomes | Lung function (FEV1 and FVC), clinical scores, sputum culture and sensitivity (24 months), exacerbations (hospitalisation for respiratory deterioration), ototoxicity and renal toxicity. | |
| Notes | Lung function expressed as rate of decline of FEV1 as % predicted per year. Sponsor: Canadian CFF. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | First participant in 6 strata (age, sex) assigned by coin toss and then alternation. |
| Allocation concealment (selection bias) | Low risk | Alternate randomisation and allocation performed by a trial nurse and the trial physician was reported to be blind to treatment allocation throughout the trial. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants aware of treatment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | SIngle blind ‐ trial physicians blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 27/28 completed, 1 participant excluded from analysis. Reason given. |
| Selective reporting (reporting bias) | Low risk | All outcomes stated in the methods section seem to be reported, although a protocol was not available for a more thorough assessment. |
Murphy 2004.
| Study characteristics | ||
| Methods | Open‐label RCT, stratified by age and sex.
Parallel design.
Duration: 56 weeks (alternating 4‐weekly cycles). Multicentre: 43 centres in USA and Canada. |
|
| Participants | 184 participants enrolled with 2 or more cultures of P aeruginosa, but only 181 randomised (91 to TIS group and 90 to control group). Age mean (SD): TIS 10.2 (2.7) years; control 9.9 (2.4) years. Range for each group 6 to 15 years. Gender split: 52% male. Baseline mean FEV1 (SD) % predicted 6 to 10 year age group: tobramycin group 89.1 (12.7); placebo group 89.3 (10.2). Baseline mean FEV1 (SD) % predicted 11 to 15 year age group: tobramycin group 78.1 (6.0); placebo group 81.2 (4.8). |
|
| Interventions |
Intervention 1: TIS 300 mg 2x daily (alternating 4‐weekly cycles for 56 weeks) using Pari LC Plus jet nebuliser and Pulmo‐Aide compressor. Intervention 2: routine management determined by individual clinicians. |
|
| Outcomes | Lung function, hospitalisation, antibiotic use. | |
| Notes | Early termination. 63 of 181 randomised participants completed 56 weeks. Sponsor: Chiron Corporation. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as randomised, but no method described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label design. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open‐label design. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Planned sample size 400, 181 randomised, 63 completed 56 weeks. Attrition rate 65%. 88 sponsor requested withdrawals. Reasons given. |
| Selective reporting (reporting bias) | High risk | Many outcomes were not fully reported, only stating a non‐significant difference between groups, including number of missed school days and weight. Also for lung function measurements, although these were also shown graphically. |
| Other bias | High risk | Early termination for benefit, only 63 of 181 randomised participants completed 56 weeks. Trial sponsor tobramycin manufacturer (Chiron corporation). |
Nathanson 1985.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled trial, allocation method not stated. Cross‐over design. Duration: 3 months. | |
| Participants | 7 participants, diagnostic criteria for CF not stated. All with P aeruginosa in sputum culture sensitive to gentamicin. Age mean (SD): 15.6 (5.7) years. Gender split not stated. |
|
| Interventions |
Intervention 1: gentamicin 80 mg 3x daily for 3 months. Intervention 2: placebo (saline) 3x daily for 3 months. Nebuliser type not stated, 2 mL volume. |
|
| Outcomes | Lung function (FEV1, FVC), sputum culture, NIH clinical score, sputum and blood gentamicin level. | |
| Notes | FEV1 result (L) no SD, probably end of trial. Sponsor: Schering. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Described as double blind, but not stated who was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Described as double blind, but not stated who was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Stated number of participants enrolled but not how many were analysed. No dropouts specifically reported. |
| Selective reporting (reporting bias) | Unclear risk | Number of participants analysed not reported. All outcomes mentioned seem to be reported. Although this paper is only an abstract and hospitalisation is mentioned in the discussion but not reported. |
| Other bias | Unclear risk | Cross‐over design, no information given regarding washout period or analysis. Sponsor: Schering. |
Nikolaizik 2008.
| Study characteristics | ||
| Methods | RCT. Cross‐over design. Duration: 3 months. |
|
| Participants | 32 participants with a confirmed diagnosis of CF, with at least 2 positive cultures for P aeruginosa in last 6 months and clinically stable. Mean age 18.5 (8.6) years. Gender split n (% male): 15 (46.9%). Initially 18 participants took low continual dose and 14 took the higher intermittent dose. |
|
| Interventions |
Intervention 1: inhaled tobramycin (IV preparation) 80 mg 2x daily continuously for 3 months. Intervention 2: inhaled TIS 300 mg 2x daily intermittent (4‐weekly on‐off cycles) for 3 months. |
|
| Outcomes | FEV1, FVC, participant preference, oxygen saturation. | |
| Notes | Supported by Chiron, Germany. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | States "randomly allocated", but no further details given. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open label, could not blind due to difference in treatments ‐ 1 was continuous and the other was intermittent (4 weeks on and 4 weeks off treatment). |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open label, could not blind due to difference in treatments ‐ 1 was continuous and the other was intermittent (4 weeks on and 4 weeks off treatment). |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not stated how many participants were randomised. |
| Selective reporting (reporting bias) | High risk | Oxygen saturation and sputum bacteriology were mentioned, but results not reported. |
| Other bias | Unclear risk | Cross‐over trial, no washout period is described. Supported by Chiron, Germany. |
Ramsey 1999.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled RCT.
Parallel design.
Duration: 3x 28‐day on‐off cycles. Multicentre. |
|
| Participants | 520 participants diagnosed with CF according to CFF clinical practice guidelines. All infected with P aeruginosa. Age from 6 years, 54% 18 years or older. Gender split (% male): 54%. Criteria for exclusion were receipt of anti‐pseudomonal antibiotics within the previous 2 weeks. Baseline mean (SD) FEV1 % predicted tobramycin group 49.9 (15.5); placebo group 51.2 (16.8). |
|
| Interventions |
Intervention 1: TIS 300 mg 2x daily for 3 cycles of 28‐day on‐off, delivered by Pari LC plus nebuliser with 5 mL of solution and Pulmo‐aide compressor. Intervention 2: placebo (0.22% normal saline and 1.25 mg quinine) 2x daily for 3 cycles of 28‐day on‐off, delivered by Pari LC plus nebuliser with 5 mL of solution and Pulmo‐aide compressor. |
|
| Outcomes | Lung function (FEV1 and FVC), exacerbations (hospitalisation or IV antibiotics), sputum P aeruginosa colony count, renal toxicity, ototoxicity. | |
| Notes | FEV1 result as change from baseline as % predicted. Support NIH, CFF, FDA. Some investigators are patent holders. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as adaptive randomisation procedure, stratified by 7 criteria. No further details. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Used quinine to attempt to mask nebulised solutions adequately, described as double blind, but not stated who. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Described as double blind, but not stated who. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ITT analysis stated, 90% completed (56 participants did not complete the trial). Attrition rate 10%. |
| Selective reporting (reporting bias) | High risk | FVC is only partially reported in the many journal articles for this trial. Other results seem to be reported. No protocol was available for a more thorough assessment and there were multiple publications from this trial. |
| Other bias | Unclear risk | Some investigators are patent holders. |
Schuster 2013.
| Study characteristics | ||
| Methods | RCT.
Parallel design. Duration: 24 weeks. Multicentre: 66 centres in Europe, Russia and Ukraine. Antimicrobial testing done at centralised laboratory using E‐test methodology. |
|
| Participants | Participants had all received a minimum of 2 on/off cycles of nebulised tobramycin prior to randomisation. 380 participants with CF aged 6 years or more with chronic P aeruginosa lung infection and FEV1 25% to 75% predicted, randomised: colistimethate dry powder for inhalation n = 187; tobramycin for inhalation solution n = 193. ITT analysis = 183 participants; PP analysis = 141 participants. Age mean (SD): colistimethate dry powder for inhalation 21.3 (9.72) years; tobramycin for inhalation solution 20.9 (9.30) years. Gender split n (% male): colistimethate dry powder for inhalation 103 (56.3%); tobramycin for inhalation solution 101 (52.9%). Baseline lung function (FEV1 % predicted) mean (SD): colistimethate dry powder for inhalation 49.14 (14.895)%; tobramycin for inhalation solution 50.80 (6.336)%. |
|
| Interventions |
Intervention 1: 125 mg colistimethate dry powder for inhalation 2x daily continuously for 24 weeks. Intervention 2: 300 mg TIS (TOBI®) 2x daily for 24 weeks (3x 28‐day courses, 28 days on and 28 days off). |
|
| Outcomes | Primary outcome: change from baseline in FEV1 % predicted at week 24. Other outcomes: antimicrobial resistance (6‐monthly), lung function (FEV1 and FVC), nutrition, QoL, survival, adverse events, respiratory tract exacerbations, hospitalisation, additional antibiotics. |
|
| Notes | Known as Freedom Study. Participants underwent at least two 28‐day TIS on‐off cycles prior to randomisation. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Centrally randomised equally to 2 intervention groups. No information about process of sequence generation. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open label. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The paper states that the primary endpoint was assessed by independent assessors of pulmonary function unaware of each individual's therapy. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 32/187 in colistimethate group dropped out (reasons given); 21/172 out of TIS group dropped out (reasons given). In main paper, 21/193 dropped out, 172 is the number completed. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes are reported and online supplementary tables provided. Only the significant finding for the QoL outcome was reported in the paper, but full results are available online. |
| Other bias | Unclear risk | Funding was provided by Forest laboratories. 2 authors are consultants for Forest Laboratories and 1 author is an employee. |
Stead 1987.
| Study characteristics | ||
| Methods | Partially blinded, placebo‐controlled RCT. Cross‐over design with 3 periods. Duration: 4 months. | |
| Participants | 18 participants with CF, diagnosed by clinical features and sweat sodium more than 70 mmol/L. All had persistent P aeruginosa on sputum culture. Mean baseline FEV1 1.29 (0.53) L. None had received IV antibiotics within the previous 3 weeks. Age range 13 to 41 years. Gender split n (% male): 12 (66.7%). |
|
| Interventions |
Intervention 1: ceftazidime 1 g 2x daily for 4 months, delivered by DeVilbiss nebuliser with 2 mL to 4 mL of solution. Intervention2: combination of gentamicin solution 80 mg (2 mL) and carbenicillin 1 g dissolved in 3 mL of sterile water prior to nebulisation. Gentamicin and carbenicillin were nebulised separately 2x daily for 4 months. Intervention 3: placebo (3.5% saline) 2x daily for 4 months delivered by DeVilbiss nebuliser with 2 mL to 4 mL of solution. |
|
| Outcomes | Lung function (FEV1, FVC, PEF), exacerbations (admission to hospital for IV antibiotics), sputum bacteriology, sputum volume, and participant preference. | |
| Notes | FEV1 (L) result at end of treatment. Only 2 arms used for this comparison. Sponsor: Glaxo Group Research Limited. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Described as randomised, Latin‐square design. |
| Allocation concealment (selection bias) | Unclear risk | No description given. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | 1 arm open‐label, otherwise blinded for participants and investigators. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | 1 arm open‐label, otherwise blinded for participants and investigators. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 13/18 completed. Attrition rate 28%. Reasons given. |
| Selective reporting (reporting bias) | Low risk | All outcomes mentioned seem to be reported. Although, a protocol was not available for a more thorough assessment. |
| Other bias | Unclear risk | Only 2 arms of cross‐over trial used for this comparison. Lung function in the saline period was higher in the participants who received it in the second period. Sponsor: Glaxo Group Research Limited. |
Wiesemann 1998.
| Study characteristics | ||
| Methods | Placebo‐controlled RCT. Parallel design. Duration: 12 months. |
|
| Participants | 22 participants. Aged over 4 years, mean age 11.4 and 9.8 in 2 groups. Gender split n (% male): 13 (59.1%). |
|
| Interventions |
Intervention 1: tobramycin 80 mg 2x daily for 12 months, delivered by Pari Boy jet nebuliser, 4 mL of solution. Intervention 2: placebo (saline with same preservatives) 2x daily for 12 months, delivered by Pari Boy jet nebuliser, 4 mL of solution. |
|
| Outcomes | Eradication of P aeruginosa, lung function, inflammatory parameters. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Described as randomised, flipping a coin in blocks of 2. |
| Allocation concealment (selection bias) | High risk | A coin was flipped in blocks of 2. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Used saline with same tobramycin preservative solution as the placebo, described as double blind, but does not state who. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Described as double blind, but does not state who. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 14/22 completed. Attrition rate 36%. Reasons given. |
| Selective reporting (reporting bias) | High risk | VC and FEV1 are mentioned in the methods section but results are not reported. However it is unclear if baseline measurements were only recorded, although FEV1 is an important clinical outcome. Also the report states "there was no significant difference between the groups in lung function parameters, IgG, IgE and ESR during or after the treatment period". |
BAL: bronchoalveolar lavage. CF: cystic fibrosis. CFF: Cystic Fibrosis Foundation. CFQ‐R: cystic fibrosis questionnaire‐revised. CFU: colony forming units. ESR: erythrocyte sedimentation rate. FDA: Food and Drug Administration. FEF25-75: forced expiratory flow from 25% to 75% of vital capacity. FEV1: forced expiratory volume in 1 second. FVC: forced vital capacity. IgE: immunoglobulin E. IgG: immunoglobulin G. ITT: intention‐to‐treat. IV: intravenous. LAI: liposomal amikacin for inhalation solution. LIS: levofloxacin for inhalation solution. NaCl: sodium chloride. NIH: National Institutes of Health. P aeruginosa: Pseudomonas aeruginosa. PEF: peak expiratory flow. PEFR: peak expiratory flow rate. PP: per protocol. QoL: quality of life. RCT: randomised controlled trial. RTE: respiratory tract exacerbation. SD: standard deviation. SE: standard error. TIS: tobramycin for inhalation solution. VC: vital capacity. WCC: white cell count.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| ACTRN12620000531910 | Duration of treatment is less than 3 months. |
| Al‐Aloul 2004 | Duration less than 28 days. |
| Alothman 2000 | Single‐dose trial. Outcome adverse effect. |
| Alothman 2005 | Duration less than 28 days. |
| App 2000 | Single dose trial. Outcome tobramycin level. |
| Bruinenberg 2008 | Duration less than 28 days. |
| Carswell 1987 | Trial of tobramycin and flucloxacillin compared to double placebo, can not conclude that any change is due to inhaled antibiotic. |
| Chua 1990 | Duration less than 28 days, single dose only. |
| Claut 2011 | Not an inhaled therapy. |
| Coates 2011 | Duration less than 28 days. |
| Cooper 1985 | Comparison of inhaled (nebulised) with intravenous antibiotics in hospital. Duration of treatment not stated. |
| Davies 2004 | Dry powder form of colistin versus nebulised colistin, each treatment only 28 days with at least 3‐day washout. |
| Dodd 1997 | Duration less than 28 days. Single inhalation of colistin solution of 3 levels of tonicity to determine effect on FEV1 and symptoms. |
| Dodd 1998 | Duration less than 28 days. |
| Dorkin 2015 | Duration only 28 days. |
| Dupont 2008 | Duration only 28 days. |
| Eisenberg 1997 | Duration less than 1 month. A single inhalation of tobramycin by 3 nebuliser systems to determine amount delivered to the lung measured by sputum and serum concentrations. |
| EUCTR2005‐004103‐10‐DE | Duration of treatment less than 3 months. Safety and bioavailability study. |
| EUCTR2006‐006215‐68‐DE | Duration of treatment is less than 3 months. |
| EUCTR2007‐003868‐22‐FR | Duration of treatment is less than 3 months. |
| EUCTR2007‐005346‐20‐GB | Duration of treatment is less than 3 months. |
| EUCTR2008‐008314‐40‐DK | Duration of treatment is less than 3 months. |
| EUCTR2009‐013660‐39‐FR | Duration of treatment is less than 3 months. |
| EUCTR2010‐023533‐34‐FR | Duration of treatment is less than 3 months. |
| EUCTR2014‐001401‐41‐NL | Duration of treatment is less than 3 months. |
| Fiel 2013 | Not an RCT, it is a review paper. |
| Flume 2016a | Duration only 28 days. |
| Franz 1985 | Case series, no placebo or usual treatment control. |
| Frederiksen 1997 | Concurrent anti‐pseudomonal antibiotic therapy with ciprofloxacin. A trial to compare the effect of colistin and ciprofloxacin given for 3 weeks or for 3 months. |
| Frost 2018 | Not for long term therapy, it is treatment of exacerbations. |
| Galeva 2013 | Duration 28 days. |
| Geborek 2003 | Duration less than 28 days. Trial in respiratory tract exacerbations. |
| Geller 2004 | Duration less than 28 days. Outcome measure (pharmacokinetics and bioavailability of tobramycin) not in protocol. |
| Geller 2007 | Duration less than 28 days. |
| Geller 2011a | Duration less than 28 days, single‐dose trial. |
| Geller 2011b | Duration 28 days. |
| Gibson 2003 | Duration less than 28 days. |
| Gibson 2006 | Duration less than 28 days. |
| Goss 2013 | Duration 28 days. |
| Griese 2009 | Duration is 28 days. |
| Griffith 2008 | Duration less than 28 days (14 days). |
| Gulliver 2003 | Duration less than 28 days, single‐dose trial of tobramycin. |
| Hodson 2002 | Duration 28 days. |
| IRCT2016100930233N1 | Duration of treatment 28 days. |
| Jenkins 1985 | Duration less than 28 days. A randomised, placebo‐controlled, cross‐over trial of aerosol amikacin 500 mg 2x daily for 3 weeks. |
| Knowles 1988 | Duration less than 28 days. Aerosol tobramycin and piperacillin added to IV antibiotics compared to IV antibiotics alone for the hospital treatment of pulmonary exacerbations. |
| Konstan 2010a | Duration 28 days. |
| Ledson 2002 | Not anti‐pseudomonal antibiotic treatment. |
| Lenoir 2007 | Duration 28 days. |
| Mainz 2014 | Duration 28 days. |
| Maneshi 2019 | Duration 28 days. |
| Mazurek 2014 | Duration 28 days. |
| McCoy 2008 | Duration 28 days. |
| Mullinger 2005 | Duration less than 28 days, single‐dose trial. |
| Nasr 2006 | Duration 28 days. |
| NCT00411736 | The intervention is the addition of oral azithromycin or placebo to inhaled colistin so both arms get inhaled colistin. |
| NCT00420836 | Duration of treatment less than 3 months. |
| NCT00503490 | Duration of treatment less than 3 months. |
| NCT01315691 | Duration of treatment less than 3 months. |
| NCT02015663 | Study terminated early ‐ they needed to randomise 200 participants but only recruited 32. Of these only 5 completed the study. No results presented. |
| NCT02677701 | Intervention is oral and not inhaled. |
| NCT02730793 | Intervention is to treat CF nasal disease. |
| NCT02894684 | Not long‐term therapy, to treat exacerbations. |
| Nichols 2020 | The intervention is the addition of oral azithromycin to inhaled tobramycin. |
| Nikolaizik 1996 | Not an RCT. Duration less than 28 days. |
| Noah 2007 | Comparison of TOBI® and IV ceftazidime and tobramycin; comparator intervention includes a further anti‐pseudomonal drug. |
| Nolan 1982 | Cephaloridine not an anti‐pseudomonal antibiotic. |
| NTR5211 | Duration of treatment is less than 3 months. |
| Oermann 2009 | Non‐randomised follow‐up of 2 previously randomised trials. |
| Poli 2005 | Duration less than 28 days. |
| Pradal 2002 | Treatment not nebulised, duration less than 28 days. Outcomes not in protocol. |
| Proesmans 2016 | Eradication protocol, not comparing inhaled antibiotics. |
| Ramsey 1993 | Duration 28 days. |
| Ramsey 2005 | Trial investigating treatment of early colonisation with and eradication of P aeruginosa infection. |
| Ramsey 2017 | The intervention is oral azithromycin or placebo alongside TIS. Both arms get the inhaled therapy. |
| Ratjen 2010 | Trial objective is to estimate duration of eradication of P aeruginosa after treatment. |
| Retsch‐Bogart 2007 | Duration 28 days. |
| Retsch‐Bogart 2008 | Duration less than 28 days. |
| Rietschel 2009 | Insufficient duration ‐ total trial lasted over 3 months, but it was a cross‐over trial and each treatment only given for 4 weeks followed by a 4‐week washout period and a week's follow‐up at the end of the trial. |
| Rosenfeld 2006 | All participants received the same dose of TOBI®, the difference was how the sputum was obtained. |
| Ruddy 2013 | Both groups received the same treatment, randomisation related to different outcome measurements. |
| Sands 2014 | Insufficient duration ‐ total trial lasted over 3 months, but it was a cross‐over trial and each treatment only given for 8 weeks. |
| Schaad 1987 | Duration less than 28 days. A comparison of 2 weeks of nebulised amikacin (100 mg 2x daily) added to IV amikacin and ceftazidime with IV antibiotics alone for treatment of acute pulmonary exacerbations in CF. |
| Schaad 1997 | Concurrent anti‐pseudomonal antibiotic therapy. A comparison of ciprofloxacin and nebulised amikacin (500 mg daily) with ciprofloxacin alone for 3 months. |
| Shatunov 2001 | Comparison of inhaled versus IV antibiotics for exacerbations. |
| Smith 1989 | No placebo or usual treatment control. Case series to monitor for toxic effects of aerosolised tobramycin, using 600 mg 3x a day for 12 weeks. |
| Stass 2009 | Not an RCT, no comparator treatment. |
| Stass 2015 | Duration less than 28 days, single‐dose pharmacokinetic trial. |
| Steinkamp 1989 | No placebo or usual treatment control. An open non‐controlled trial comparing before‐after treatment effect of a course of nebulised tobramycin 80 mg twice daily. |
| Steinkamp 2006 | Not a nebulised antibiotic. |
| Stephens 1983 | Duration less than 28 days. Trial was a comparison of IV (tobramycin and ticarcillin) and inhaled (tobramycin) antibiotics with IV antibiotics alone for treatment of acute pulmonary exacerbations. |
| Stroobant 1985 | Anti‐pseudomonal antibiotic (azlocillin) compared to mistabron, a mucolytic. |
| Tramper‐Stranders 2010 | Test of combination of antibiotics and not just inhaled antibiotics. |
| Trapnell 2012 | Duration 28 days. |
| Valerius 1991 | Concurrent anti‐pseudomonal treatment. A comparison of the effect of 3‐week courses of nebulised colistin and oral ciprofloxacin compared to no anti‐pseudomonal antibiotic treatment on isolation rate of P aeruginosa. |
| Wainwright 2008 | Trial of bronchoalveolar lavage‐directed therapy, not of inhaled antibiotics. |
| Wainwright 2011 | Duration 28 days. |
| Wall 1984 | No placebo or usual treatment control. An open‐label, uncontrolled trial with before and after comparison of effect of nebulised tobramycin and ticarcillin. |
| Wang 1984 | No placebo or usual treatment control. |
| Westerman 2003 | Duration less than 28 days, single‐dose trial. |
| Westerman 2007 | Duration less than 28 days, single‐dose trial. |
| Yasmin 1974 | Duration less than 28 days (2 weeks) and control group received IV antibiotic treatment. |
FEV1: forced expired volume in 1 second. IV: intravenous. RCT: randomised controlled trial. P aeruginosa: Pseudomonas aeruginosa.
Characteristics of studies awaiting classification [ordered by study ID]
EUCTR2007‐004277‐26‐NL.
| Methods | Phase 3 open label randomised trial. Parallel design Multicentre: 73 sites in the UK, Europe and USA |
| Participants | Children (aged 6 years or over) and adults with diagnosed CF and P aeruginosa infection |
| Interventions |
Intervention: aztreonam 75 mg powder and diluent for nebuliser solution (AZLI) self‐administered for 28 days for each treatment cycle. AZLI (75 mg/1 mL aztreonam lysine when reconstituted in diluent (0.17% saline); sterile, pH 4.2 to 7.0, and osmolality 300 to 550 mOsmol/kg) self‐administered by inhalation 3 times a day (TID) using the PARI eFlow electronic investigational nebuliser Comparator: tobramycin nebuliser solution (TNS) self‐administered for 28 days for each treatment cycle. TNS (300 mg/5 mL) was self‐administered by inhalation twice a day (BID) using the PARI LC PLUS(TM) Nebuliser with Compressor |
| Outcomes | FEV1 (day 28); time to IV antibiotics; time to hospitalisation; adverse events |
| Notes | It is unclear of the duration of treatment as there is an initial randomised phase followed by an open label extension |
Herrmann 2017.
| Methods | Phase 3, randomised trial comparing combined TOBIⓇ Podhaler and colistin with monotherapy with colistin |
| Participants | People with CF infected with P aeruginosa. No further details |
| Interventions |
Group 1: 28 days TOBIⓇ Podhaler 2 x 112 mg for 2 x 28 days (on/off) and colistin solution 2 x 1 Mio I.U. continuously for 112 days Group 2: inhaled colistin 2 x 1 Mio I.U. continuously for at least 30 days (expected 112 days) |
| Outcomes | Colony forming units, biomarkers in sputa and lung function at 28 days Pulmonary exacerbations/iv treatments, change in inhalative regimen and bacterial resistances after 112 days |
| Notes | No information on participants or randomisation/blinding |
NCT03341741.
| Methods | Randomised open label parallel trial |
| Participants | 26 participants with diagnosed CF aged 12 years or over Participant's lung colonised with P aeruginosa |
| Interventions |
Intervention: TOBI®Podhaler 2 x 112 mg daily for 2 x 28 days (on/off); and Colistin solution 2 x daily 1 Mega continuously for 112 days Comparator: colistin solution 2 x daily 1 Mega continuously for at least 30 days |
| Outcomes | Amount of P aeruginosa in sputum; FVC; FEV1; MEF25‐75; number of exacerbations; use of antibiotics; cytokines |
| Notes | It is unclear how long the treatment was given for as outcomes are measured at 30 days but some outcomes are measured at 112 days |
Nikonova 2010.
| Methods | 3‐arm parallel trial. Duration not stated |
| Participants | 41 people with CF with first isolate and chronic P aeruginosa infection Bramitob® group − 21 participants (6 to 18 years) all with chronic infection TOBI® group − 11 participants (3 to 15 years) 2 of them with first isolate and 9 with chronic infection Colistin group − 9 participants (0 to 15 years) 6 of them with first isolate and 3 with chronic infection |
| Interventions |
Intervention 1: Bramitob® Intervention 2: TOBI® Intervention 3: colistin |
| Outcomes | Eradication of P aeruginosa infection, lung function, nutritional status, number of exacerbations of chronic bronchopulmonary process |
| Notes | Randomisation not clear. Only abstract published, await publication of full paper |
CF: cystic fibrosis FEV1: forced expiratory volume at 1 second FVC: forced vital capacity P aeruginosa: Pseudomonas aeruginosa RCT: randomised controlled trial TIS: tobramycin for inhalation solution
Differences between protocol and review
March 2018 The title of the review was revised again to 'Inhaled anti‐pseudomonal antibiotics for long‐term therapy in cystic fibrosis' and the duration of the intervention restricted to over three months and not over one month. This was to reflect the treatment for long‐term suppression rather than in acute exacerbations.
At this update, summary of findings tables were included for each comparison presented in the review.
February 2011 The title of the review has been changed from 'Nebulised anti‐pseudomonal antibiotics for cystic fibrosis' to 'Inhaled antibiotics for long‐term therapy in cystic fibrosis' to better reflect the interventions included in the review.
While updating the Methods section of the review the authors added a second planned sensitivity analysis (with and without cross‐over trials), as they felt this was relevant given that a combination of parallel and cross‐over trials are included in the review.
Contributions of authors
Previous contributions
Somnath Mukhopadhyay developed the protocol. Meenu Singh selected trials and assessed trial quality. Gerard Ryan was involved in all aspects of the protocol and the original review. Gerard Ryan completed the updates up to 2018 with Meenu Singh and Kerry Dwan and previously acted as guarantor of the review.
At the 2018 update, new references were screened by two authors (Sherie Smith and Nicola Rowbotham). Data from newly included trials were extracted by Sherie Smith, Nicola Rowbotham and Kate Regan and entered into Revman by Sherie Smith. SS (with advice from NJ) carried out analyses on the newly included trials.
All authors contributed to writing and reviewing the main text.
Current contributions
At this update all screening of new references and data extraction was carried out by SS and NR. The same authors updated the review to include extra data and contributed to writing and reviewing the text.
Sources of support
Internal sources
-
Clinical Staff Education Fund, Sir Charles Gairdner Hospital, Australia
Funding for original author to work on review.
External sources
-
National Institute for Health and Care Research (NIHR), UK
This systematic review was supported by the NIHR, via Cochrane Infrastructure funding to the Cochrane Cystic Fibrosis and Genetic Disorders Group.
Declarations of interest
Nicola Rowbotham: none known. Sherie Smith: none known.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Assael 2013 {published data only}PI257
- Assael B, Chiron R, Fischer R, Bresnik M, Lewis S, Montgomery AB, et al. Lung function improvement in cystic fibrosis (CF) subjects in response to treatment with aztreonam for inhalation solution (AZLI) in a single-arm extension study after multiple courses of inhaled antipseudomonal antibiotics. American Journal of Respiratory and Critical Care Medicine 2011;183(Meeting Abstracts):A1111. [CFGD REGISTER: PI257n] [Google Scholar]
- Assael BM, Chiron R, Fischer R, Bresnick M, Lewis S, Montgomery AB, et al. Lung function improvement with aztreonam 75mg powder and solvent for nebuliser solution (AZLI) in single-arm extension of a randomized trial of inhaled anti-pseudomonal antibiotics in patients with cystic fibrosis (CF) and Pseudomonas aeruginosa infection. Journal of Cystic Fibrosis 2011;10 Suppl 1:S22. [ABSTRACT NO: 86] [CFGD REGISTER: PI257e] [Google Scholar]
- Assael BM, Chiron R, Fischer R, Bresnik M, Lewis S, Pressler T, et al. Lung function improvement with aztreonam for inhalation solution (AZLI) in the single-arm extension of a randomized trials of inhaled anti-pseudomonal antibiotics in patients with cystic fibrosis (CF) and Pseudomonas aeruginosa infection. Pediatric Pulmonology 2011;46 Suppl 34:312. [ABSTRACT NO: 278] [CFGD REGISTER: PI257c] [Google Scholar]
- Assael BM, Pressler T, Bilton D, Fayon M, Fischer R, Chiron R, et al. Inhaled aztreonam lysine vs. inhaled tobramycin in cystic fibrosis: a comparative efficacy trial. Journal of Cystic Fibrosis 2013;12(2):130-40. [CFGD REGISTER: PI257f] [DOI] [PubMed] [Google Scholar]
- Assael BM, Pressler T, Bilton D, Fayon M, Fischer R, Chiron R, et al. Inhaled aztreonam lysine vs. inhaled tobramycin in cystic fibrosis: a comparative efficacy trial. Journal of Cystic Fibrosis 2013;12(2):130-40. Online figure 1. [CFGD REGISTER: PI257k] [DOI] [PubMed] [Google Scholar]
- Assael BM, Pressler T, Bilton D, Fayon M, Fischer R, Chiron R, et al. Inhaled aztreonam lysine vs. inhaled tobramycin in cystic fibrosis: a comparative efficacy trial. Journal of Cystic Fibrosis 2013;12(2):130-40. Online figure 2. [CFGD REGISTER: PI257L] [DOI] [PubMed] [Google Scholar]
- Assael BM, Pressler T, Bilton D, Fayon M, Fischer R, Chiron R, et al. Inhaled aztreonam lysine vs. inhaled tobramycin in cystic fibrosis: a comparative efficacy trial. Journal of Cystic Fibrosis 2013;12(2):130-40. Online figure 3. [CFGD REGISTER: PI257m] [DOI] [PubMed] [Google Scholar]
- Assael BM, Pressler T, Bilton D, Fayon M, Fischer R, Chiron R, et al. Inhaled aztreonam lysine vs. inhaled tobramycin in cystic fibrosis: a comparative efficacy trial. Journal of Cystic Fibrosis 2013;12(2):130-40. Online supplement. [CFGD REGISTER: PI257j] [DOI] [PubMed] [Google Scholar]
- Fayon M, Oermann CM, Pressler T, Wicklund J, Brekke J, Liu H, et al. Post-hoc review of outcomes in patients switching from tobramycin for nebulization solution (TNS) to aztreonam lysine for inhalation (AZLI). Journal of Cystic Fibrosis 2016;15 Suppl 1:S49. [ABSTRACT NO: ePS06.5] [CENTRAL: 1171479] [CFGD REGISTER: PI257h] [Google Scholar]
- NCT00757237. Aztreonam for inhalation solution vs tobramycin inhalation solution in patients with cystic fibrosis & pseudomonas aeruginosa. clinicaltrials.gov/show/NCT00757237 (first received 23 September 2008). [CFGD REGISTER: PI257n]
- Nick JA, Moskowitz SM, Chmiel JF, Forssen AV, Kim SH, Saavedra MT, et al. Azithromycin may antagonize inhaled tobramycin when targeting Pseudomonas aeruginosa in cystic fibrosis. Annals of the American Thoracic Society 2014;11(3):342-50. [CFGD REGISTER: PI257g] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oermann CM, Assael B, Nakamura C, Boas SR, Bresnik M, et al. Aztreonam for inhalation solution (AZLI) vs. tobramycin inhalation solution (TIS), a 6-month comparative trial in cystic fibrosis patients with pseudomonas aeruginosa. Pediatric Pulmonology 2010;45 Suppl 33:327. [ABSTRACT NO: 305] [CFGD REGISTER: PI257a] [Google Scholar]
- Oermann CM, Lewis S, Bresnik M, Assael B. Change in FEV1% predicted in response to aztreonam for inhalation solution (AZLI) vs. tobramycin inhalation solution (TIS) in an active comparator study: responder analyses. Pediatric Pulmonology 2011;46 Suppl 34:289. [ABSTRACT NO: 216] [CFGD REGISTER: PI257b] [Google Scholar]
- Pressler BM, Assael R, Fischer R, Bresnik M, Lewis S, McKevitt M, et al. In vitro susceptibility of pseudomonas aeruginosa (PA) does not predict clinical response to aztreonam 75mg powder and solvent for nebuliser solution (AZLI): a responder analysis in subjects with cystic fibrosis. Journal of Cystic Fibrosis 2011;10 Suppl 1:S27. [ABSTRACT NO: 107] [CFGD REGISTER: PI257d] [Google Scholar]
- Schechter MS, Trueman D, Farquharson R, Higuchi K, Daines C. An economic evaluation of aztreonam lysine for inhalation and tobramycin for inhalation, in an intermittent aerosolised antibiotic regime, among cystic fibrosis patients with chronic pulmonary Pseudomonas aeruginosa infection. American Journal of Respiratory and Critical Care Medicine 2012;185(Meeting Abstracts):no pagination. [ABSTRACT NO: A6733] [CENTRAL: 1135697] [CFGD REGISTER: PI257i] [DOI: ] [EMBASE: 71986991] [Google Scholar]
Bilton 2020 {published data only}PI271
- Bilton D, Pressler T, Fajac I, Clancy JP, Sands D, Minic P, et al. Amikacin liposome inhalation suspension for chronic Pseudomonas aeruginosa infection in cystic fibrosis. Journal of Cystic Fibrosis 2020;19(2):284-91. [CFGD REGISTER: PI333b] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bilton D, Pressler T, Fajac I, Clancy JP, Sands D, Minic P, et al. Once-daily liposomal amikacin for inhalation is non-inferior to twice-daily tobramycin inhalation solution in improving pulmonary function in cystic fibrosis patients with chronic infection due to Pseudomonas aeruginosa. Journal of Cystic Fibrosis 2014;13 Suppl 2:S15. [ABSTRACT NO: WS7.3] [CFGD REGISTER: PI271b] [Google Scholar]
- Bilton D, Pressler T, Fajac I, Clancy JP, Sands D, Minic PB, et al. Interim analysis of a long-term, open-label safety, tolerability, and efficacy study of liposomal amikacin for inhalation in cystic fibrosis patients with chronic infection due to pseudomonas aeruginosa. American Journal of Respiratory and Critical Care Medicine 2014;189(Meeting Abstracts):no pagination. [ABSTRACT NO: A6571] [CENTRAL: 1038420] [CFGD REGISTER: PI271c] [Google Scholar]
- Bilton D, Pressler T, Isabelle F, John Paul C, Sands D, Minic P, et al. Phase 3 efficacy and safety data from randomized, multicenter study of liposomal amikacin for inhalation (Arikace) compared with TOBI® in cystic fibrosis patients with chronic infection due to pseudomonas aeruginosa. Pediatric Pulmonology 2013;48 Suppl 36:290. [ABSTRACT NO: 235] [CFGD REGISTER: PI271a] [Google Scholar]
- EUCTR2011-000441-20-ES. Study to evaluate Arikayce™ in CF patients with chronic Pseudomonas aeruginosa infections [Estudio para evaluar la eficacia, seguridad y tolerabilidad de arikace en pacientes con fibrosis quistica con infeccion cronica por pseudomonas aeruginosa]. trialsearch.who.int/Trial2.aspx?TrialID=NCT01315678 (first received 14 March 2011). [CFGD REGISTER: PI271g]
- NCT01315678. Study to evaluate arikayce™ in CF patients with chronic pseudomonas aeruginosa infections. clinicaltrials.gov/show/NCT01315678 (first received 15 March 2011). [CFGD REGISTER: PI333a]
- Quittner AL, Barker DH, Constantine SE, Gupta R. Clinical benefit of liposomal amikacin for inhalation as assessed by the cystic fibrosis questionnaire-revised. American Journal of Respiratory and Critical Care Medicine 2014;189(Meeting Abstracts):no pagination. [ABSTRACT NO: A6685] [CENTRAL: 1136702] [CFGD REGISTER: PI271d] [EMBASE: 72047316] [Google Scholar]
Chuchalin 2007 {published data only}PI201
- Chuchalin A, Csiszer E, Gyurkovics K, Bartnicka MT, Sands D, Kapranov N, et al. A formulation of aerosolized tobramycin (Bramitob) in the treatment of patients with cystic fibrosis and Pseudomonas aeruginosa infection: a double-blind, placebo-controlled, multicenter study. Paediatric Drugs 2007;9 Suppl 1:21-31. [CFGD REGISTER: PI201c] [DOI] [PubMed] [Google Scholar]
- Chuchalin A, Gyurkovics K, Mazurek H, Varoli G, Monici Preti P. Long-term administration of aerosolised tobramycin in patients with cystic fibrosis. European Respiratory Journal 2005;26 Suppl 49:619s. [CFGD REGISTER: PI201a] [Google Scholar]
- Chuchalin A, Gyurkovics K, Mazurek HVG, Monici Preti PA. Long-term administration of nebulised tobramycin in patients with cystic fibrosis. Journal of Cystic Fibrosis 2006;5 Suppl:S42. [CFGD REGISTER: PI201b] [Google Scholar]
Day 1988 {published data only}PI85
- Day AJ, Williams J, McKeown C, Bruton A, Weller PH. Evaluation of inhaled colomycin in children with cystic fibrosis. In: 10th International Cystic Fibrosis Congress; 1988 March 5-10; Sydney. 1988:106. [CFGD REGISTER: PI85]
Elborn 2015 {published data only}PI262
- Elborn JS, Flume PA, Cohen F, Loutit J, Van Devanter DR. Safety and efficacy of prolonged levofloxacin inhalation solution (APT-1026) treatment for cystic fibrosis and chronic Pseudomonas aeruginosa airway infection. Journal of Cystic Fibrosis 2016;15(5):634-40. [CENTRAL: 1262260] [CFGD REGISTER: PI262d] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Elborn JS, Flume PA, Loutit J, Cohen F. Prolonged improvement in lung function and quality of life in cystic fibrosis: a 24-week extension study of levofloxacin nebulization solution (APT-1026) versus tobramycin nebulization solution in stable CF patients with chronic pseudomonas aeruginosa infection. Journal of Cystic Fibrosis 2014;13 Suppl 2:S16. [ABSTRACT NO: WS7.5] [CENTRAL: 1000055] [CFGD REGISTER: PI262b] [Google Scholar]
- Elborn JS, Geller D, Conrad D, Aaron S, Smyth AR, Fischer R, et al. Phase 3 trial of inhaled levofloxacin (Aeruquinâ™, MP-376, APT-1026) vs. tobramycin inhalation solution (TIS) in intensively treated CF patients over 6 months. Journal of Cystic Fibrosis 2013;12 Suppl 1:S35. [ABSTRACT NO: WS17.6] [CENTRAL: 867323] [CFGD REGISTER: PI262a] [Google Scholar]
- Elborn JS, Geller DE, Conrad D, Aaron SD, Smyth AR, Fischer R, et al. A phase 3, open-label, randomized trial to evaluate the safety and efficacy of levofloxacin inhalation solution (APT-1026) versus tobramycin inhalation solution in stable cystic fibrosis patients. Journal of Cystic Fibrosis 2015;14:507-14. Online supplementary material. [CFGD REGISTER: PI262e] [DOI] [PubMed] [Google Scholar]
- Elborn JS, Geller DE, Conrad D, Aaron SD, Smyth AR, Fischer R, et al. A phase 3, open-label, randomized trial to evaluate the safety and efficacy of levofloxacin inhalation solution (APT-1026) versus tobramycin inhalation solution in stable cystic fibrosis patients. Journal of Cystic Fibrosis 2015;14(4):507-14. [CENTRAL: 1038490] [CFGD REGISTER: PI262c] [DOI: 10.1016/j.jcf.2014.12.013] [JID:: 101128966] [PMID: ] [DOI] [PubMed] [Google Scholar]
- EUCTR2010-019634-26-IE. Trial of aeroquin versus tobramycin inhalation solution (TIS) in stable cystic fibrosis patients. trialsearch.who.int/Trial2.aspx?TrialID=NCT01270347 (first received 3 January 2011). [CFGD REGISTER: PI283h]
- Fischer R, Flume PA, Van Devanter DR, Polu K, Pecoraro M, Bhatt N, et al. Pulmonary exacerbations and changes in lung function in CF adults with P. aeruginosa treated with inhaled levofloxacin (Quinsair®) or tobramycin. Journal of Cystic Fibrosis 2016;51 Suppl 45:359. [ABSTRACT NO: 436] [CENTRAL: 1262259] [CFGD Register: PI283d] [Google Scholar]
- Flume P, Elborn JS, Polu K, Llorens L, Pecoraro ML, Bhatt N, et al. History of pulmonary exacerbations (PEx) as a predictor of response to nebulized levofloxacin compared with nebulized tobramycin. Journal of Cystic Fibrosis 2016;15 Suppl 1:S61. [ABSTRACT NO: 38] [CENTRAL: 1171477] [CFGD REGISTER: PI283e] [Google Scholar]
- Flume P, Van Devanter DR, Cohen F, Fleming R, Elborn JS. Safety profile of levofloxacin inhalation solution from 3 controlled cystic fibrosis trials. Journal of Cystic Fibrosis 2015;14 Suppl 1:S87. [ABSTRACT NO: 117] [CENTRAL: 1077213] [CFGD REGISTER: PI283c // PI240f // PI284c] [Google Scholar]
- NCT01270347. Trial of aeroquin versus tobramycin inhalation solution (TIS) in cystic fibrosis (CF) patients [Phase 3, open-label, randomized trial to evaluate the safety and efficacy of MP-376 inhalation solution (Aeroquin) vs. tobramycin Iihalation solution (TIS) in stable CF patients]. clinicaltrials.gov/ct2/show/NCT01270347 (first received 5 January 2011). [CENTRAL: 1012530] [CFGD REGISTER: PI283a]
- Van Devanter D, Flume PA, Fleming R, Elborn J. How often is pulmonary exacerbation defined by ≥4 Fuchs criteria associated with antibiotic treatment? Pediatric Pulmonology 2014;49 Suppl 38:356. [ABSTRACT NO: 388] [CENTRAL: 1012531] [CFGD REGISTER: PI283b // PI284b] [Google Scholar]
- Van Devanter DR, Elborn JS, Flume P, Polu K, LiPuma JJ. Microbiologic changes observed over 6 months in a randomized, open-label comparison of inhaled levofloxacin and inhaled tobramycin in persons with cystic fibrosis and chronic P. aeruginosa (Pa) airway infection. Journal of Cystic Fibrosis 2016;15:S60-1. [PI262f] [Google Scholar]
Flume 2016b {published data only}PI288
- Flume PA, Clancy JP, Retsch-Bogart GZ, Tullis DE, Bresnik M, Derchak PA, et al. Continuous alternating inhaled antibiotics for chronic pseudomonal infection in cystic fibrosis. Journal of Cystic Fibrosis 2016;15(6):809-15. [CENTRAL: 1262277] [CFGD REGISTER: PI288b] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Flume PA, Clancy JP, Retsch-Bogart GZ, Tullis E, Bresnik M, Derchak PA, et al. Aztreonam for inhalation solution (AZLI) and tobramycin inhalation solution (TIS) continuous alternating therapy (CAT) for cystic fibrosis (CF) patients with chronic pseudomonas aeruginosa (PA) infection: a randomized, double-blind, placebo-controlled trial. Pediatric Pulmonology 2015;50 Suppl 41:352. [ABSTRACT NO: 428] [CENTRAL: 1092171] [CFGD REGISTER: PI288a] [Google Scholar]
- NCT01641822. Phase 3 study of aztreonam for inhalation solution (AZLI) in a continuous alternating therapy regimen for the treatment of chronic pseudomonas aeruginosa infection in patients with CF. clinicaltrials.gov/show/NCT01641822 (first received 17 July 2012). [CFGD REGISTER: PI288c]
Hodson 1981 {published data only}PI24
- Hodson ME, Penketh ARL, Batten JC. Aerosol carbenicillin and gentamicin treatment of Pseudomonas aeruginosa infection in patients with cystic fibrosis. Lancet 1981;2(8256):1127-9. [CFGD REGISTER: PI24] [DOI] [PubMed] [Google Scholar]
Jensen 1987 {published data only}PI51
- Jensen T, Pederson SS, Garne S, Heilmann C, Hoiby N, Koch C. Colistin inhalation therapy in cystic fibrosis patients with chronic Pseudomonas aeruginosa lung infection. Journal of Antimicrobial Chemotherapy 1987;19(6):831-8. [CFGD REGISTER: PI51] [DOI] [PubMed] [Google Scholar]
Konstan 2010b {published data only}PI239
- Chiron R, Geller DE, Angyalosi G, Debonnett L, Yadao A, Bader G, et al. Tobramycin powder for inhalation is effective in advanced stage CF lung disease: the EAGER trial. Journal of Cystic Fibrosis 2014;13 Suppl 2:S57. [ABSTRACT NO: 42] [CENTRAL: 996576] [CFGD REGISTER: PI239k] [Google Scholar]
- EUCTR2005-003772-37-DE. A randomized, open-label, multicenter, phase 3 trial to assess the safety of tobramycin inhalation powder compared to TOBI® in cystic fibrosis subjects. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2005-003772-37-GB (first received 9 November 2005). [CFGD REGISTER: PI239q]
- Geller DE, Flume PA, Brockhaus F, Zhang J, Angyalosi G, He E, et al. Treatment convenience and satisfaction of tobramycin inhalation powder (TIPTM) versus TOBI® in cystic fibrosis (CF) patients. Journal of Cystic Fibrosis 2010;9 Suppl 1:S22. [ABSTRACT NO: 83] [CFGD REGISTER: PI239b] [Google Scholar]
- Geller DE, Flume PA, Konstan M, Angyalosi G, Higgins M. Microbiological and clinical response to tobramycin inhalation powder (TIPTM) in cystic fibrosis patients with chronic Pseudomonas aeruginosa (Pa) infection. Journal of Cystic Fibrosis 2011;10 Suppl 1:S21. [ABSTRACT NO: 82] [CFGD REGISTER: PI239g] [Google Scholar]
- Geller DE, Nasr S, Piggott S, Angyalosi G, Higgins M. Tobramycin inhalation powder vs tobramycin inhalation solution for cystic fibrosis: Response by age group in the eager trial. Pediatric Pulmonology 2011;46 Suppl:337-8. [CFGD REGISTER: PI239m] [Google Scholar]
- Geller DE, Nasr SZ, Piggott S, He E, Angyalosi G, Higgins M. Tobramycin inhalation powder in cystic fibrosis patients: response by age group. Respiratory Care 2014;59(3):388-98. [CFGD REGISTER: PI239l] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Konstan M, Flume PA, Brockhaus F, Angyalosi G, He E, Geller D. Safety and efficacy of tobramycin inhalation powder (TIP) in treating CF patients infected with Pseudomonas aeruginosa (Pa). Journal of Cystic Fibrosis 2010;9 Suppl 1:S22. [ABSTRACT NO: 82] [CFGD REGISTER: PI239a] [Google Scholar]
- Konstan MW, Flume PA, Brockhaus F, Angyalosi G, He E, Zhang J, et al. Tobramycin inhalation powder (TIP) versus tobramycin inhalation solution (TOBI®): the EAGER trial. Pediatric Pulmonology 2010;45 Suppl 33:303. [ABSTRACT NO: 235] [CFGD REGISTER: PI239c] [Google Scholar]
- Konstan MW, Flume PA, Kappler M, Chiron R, Higgins M, Brockhaus F, et al. Safety, efficacy and convenience of tobramycin inhalation powder in cystic fibrosis patients: the EAGER trial. Journal of Cystic Fibrosis 2011;10(1):54-61. [CFGD REGISTER: PI239e] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Konstan MW, Parkins M, Angyalosi G, Higgins M. Tobramycin inhalation powder is AS effective AS tobramycin inhalation solution in patients with cystic fibrosis: a subgroup analysis of the eager trial. American Journal of Respiratory and Critical Care Medicine 2013;187:A1178. [CFGD REGISTER: PI239n] [Google Scholar]
- McColley S, Rietschel E, Brockhaus F, Angyalosi G, Higgins M. Safety of inhaled tobramycin in patients with cystic fibrosis. Pediatric Pulmonology 2011;46 Suppl 34:344. [ABSTRACT NO: 365] [CFGD REGISTER: PI239h // PI258b] 5500100000010634 [Google Scholar]
- Nasr S, Nick J, Ezzet N, Gallo P, Debonnett L, Angyalosi G, et al. Reduced administration time for inhaled tobramycin in cystic fibrosis patients: results from the EAGER trial. Pediatric Pulmonology 2013;48 Suppl 36:283. [ABSTRACT NO: 219] [CENTRAL: 921693] [CFGD REGISTER: PI239j] [Google Scholar]
- NCT00388505. Safety of tobramycin inhalation powder (TIP) vs tobramycin solution for inhalation in patients with cystic fibrosis. clinicaltrials.gov/show/NCT00388505 (first received 17 October 2006). [CFGD REGISTER: PI239p]
- Regnault A, Balp MM, Kulich K, Esteve L, Viala-Danten M. Association of treatment satisfaction and compliance of cystic fibrosis (CF) patients using inhaled tobramycin treatment in the EAGER study. Journal of Cystic Fibrosis 2011;10 Suppl 1:S82. [ABSTRACT NO: 323] [CFGD REGISTER: PI239d] [Google Scholar]
- Regnault A, Balp MM, Kulich K, Esteve L, Viala-Danten M. Validation of the treatment satisfaction questionnaire for medication (TSQM) in cystic fibrosis (CF). Journal of Cystic Fibrosis 2011;10 Suppl 1:S85. [ABSTRACT NO: 332] [CFGD REGISTER: PI239f] [DOI] [PubMed] [Google Scholar]
- Regnault A, Balp MM, Kulich K, Viala-Danten M. Validation of the treatment satisfaction questionnaire for medication in patients with cystic fibrosis. Journal of Cystic Fibrosis 2012;11(6):494-501. [CFGD REGISTER: PI239i] 5500100000011297 [DOI] [PubMed] [Google Scholar]
Kun 1984 {published data only}PI106
- Kun P, Landau LI, Phelan PD. Nebulized gentamicin in children and adolescents with cystic fibrosis. Australian Paediatric Journal 1984;20(1):43-5. [CFGD REGISTER: PI106] [DOI] [PubMed] [Google Scholar]
MacLusky 1989 {published data only}PI62
- MacLusky IB, Gold R, Corey M, Levison H. Long-term effects of inhaled tobramycin in patients with cystic fibrosis colonized with pseudomonas aeruginosa. Pediatric Pulmonology 1989;7(1):42-8. [CFGD REGISTER: PI62] [DOI] [PubMed] [Google Scholar]
Murphy 2004 {published data only}PI175
- Anbar RD, Yu X, Colin AA. Reduction of pulmonary hospitalizations during a randomized, controlled, open-label study of tobramycin solution for inhalation in young CF patients with mild lung disease. Pediatric Pulmonology 2003;Suppl 25:296. [CFGD REGISTER: PI175b] [Google Scholar]
- Colin AA, Anbar RD, Yu X. Reduction in pulmonary hospitalizations during a randomized, controlled, open-label study of tobramycin solution for inhalation in young CF patients with mild lung disease. Journal of Cystic Fibrosis 2003;2 Suppl 1:S22. [CFGD REGISTER: PI175a] [Google Scholar]
- Murphy TD, Anbar RD, Lester LA, Nasr SZ, Nickerson B, Van Devanter DR, et al. Treatment with tobramycin solution for inhalation reduces hospitalizations in young CF subjects with mild lung disease. Pediatric Pulmonology 2004;38(4):314-20. [CFGD REGISTER: PI175c] [DOI] [PubMed] [Google Scholar]
Nathanson 1985 {published data only}PI130
- Nathanson I, Cropp GJA, Li P, Neter P. Effectiveness of aerosolized gentamicin in cystic fibrosis (CF). In: Cystic Fibrosis Club Abstracts; 1985. Vol. 28. 1985:145. [CFGD REGISTER: PI130]
Nikolaizik 2008 {published data only}PI191
- Nikolaizik WH, Vietzke D, Ratjen F. A pilot study to compare tobramycin 80 mg injectable preparation with 300 mg solution for inhalation in cystic fibrosis patients. Canadian Respiratory Journal 2008;15(5):259-62. [CFGD REGISTER: PI191c] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nikolaizik WH, Vietzke D, Ratjen F. Comparison of tobramycin 80 mg (IV- Preparation) and 300 mg solution for inhalation in cystic fibrosis patients. European Respiratory Journal 2005;26 Suppl 49:620s. [CFGD REGISTER: PI191b] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nikolaizik WH, Vietzke D, Ratjen F. Comparison of tobramycin 80 mg (IV-preparation) and 300 mg solution inhaled twice daily for chronic P aeruginosa infection. Journal of Cystic Fibrosis 2005;4 Suppl:S53. [CFGD REGISTER: PI191a] [Google Scholar]
Ramsey 1999 {published data only}PI120
- Birnbaum HG, Greenberg P, Finkelstein S, Berndt E, Otto KL, Montgomery AB, et al. Economic analysis of hospitalization and home IV anti-pseudomonal antibiotic use in CF patients on tobramycin solution for inhalation (TOBI). Pediatric Pulmonology 1998;Suppl 17:273. [CFGD REGISTER: PI120f] [Google Scholar]
- Bowman CM. The long-term use of inhaled tobramycin in patients with cystic fibrosis. Journal of Cystic Fibrosis 2002;1 Suppl 2:S194-8. [CFGD REGISTER: PI120cc] [DOI] [PubMed] [Google Scholar]
- Burns JL, Van Dalfsen JM, Shawar RM, Otto KL, Garber RL, Quan JM, et al. Effect of chronic intermittent administration of inhaled tobramycin on respiratory microbial flora in patients with cystic fibrosis. Journal of Infectious Diseases 1999;179(5):1190-6. [CFGD REGISTER: Pi120i] [DOI] [PubMed] [Google Scholar]
- Casey S, Ramsey B, Borowitz D. Nutritional benefits of chronic intermittent Pseudomonas aeruginosa suppression with tobramycin solution for inhalation in adolescents. In: 13th International Cystic Fibrosis Congress; 2000 June 4-8; Stockholm, Sweden. 2000:172. [CFGD REGISTER: PI120ff]
- Enger C, Rothman K, Kylstra JW. Mortality rates during two years of treatment with intermittent inhaled tobramycin (TOBI) in CF. Pediatric Pulmonology 1999;Suppl 19:339-40. [CFGD REGISTER: PI120m] [Google Scholar]
- Fiel S, Van Devanter DR, Yu X. Effect of tobramycin solution for inhalation on pulmonary function decline rates in exacerbating and stable CF patients. In: 24th European Cystic Fibrosis Conference; 2001 June 6-9; Vienna. 2001:P195. [CFGD REGISTER: PI120s]
- Fiel SB. Long term effect of tobramycin solution for inhalation on reduction of hospitalization of CF patients. European Respiratory Journal 2000;16 Suppl 31:1545. [CFGD REGISTER: PI120dd] [Google Scholar]
- Geller DE, Pitlick WH, Nardella PA, Tracewell WG, Ramsey BW. Pharmacokinetics and bioavailability of aerosolized tobramycin in cystic fibrosis. Chest 2002;122(1):219-26. [CFGD REGISTER: PI120bb] [DOI] [PubMed] [Google Scholar]
- Graff GR, Burns JL. Factors affecting the incidence of Stenotrophomonas maltophilia isolation in cystic fibrosis. Chest 2002;121(6):1754-60. [CFGD REGISTER: PI120gg] [DOI] [PubMed] [Google Scholar]
- Graff GR, Gordon DC, Van Dalfsen, Burns JL. Epidemiology of Stenotrophomonas maltophilia culture in cystic fibrosis (CF) patients during the tobramycin solution for inhalation (TOBI) study. Pediatric Pulmonology 2000;Suppl 20:283. [CFGD REGISTER: PI120p] [Google Scholar]
- Hazinski TA. Intermitent administration of inhaled tobramycin in patients with cystic fibrosis. Journal of Pediatrics 1999;135(1):130. [CFGD REGISTER: PI120j] [PubMed] [Google Scholar]
- Klystra JW, Bowman CM, Meyer U, Montgomery AB, Schaeffler B, Stewart P, et al. Who benefits more? An age-stratified analysis of lung function and weight gain in CF patients using inhaled tobramycin. Netherlands Journal of Medicine 1999;54 Suppl:S83. [CFGD REGISTER: PI120h] [Google Scholar]
- Konstan MW, Van Devanter DR. Peripheral white blood cell count as a surrogate marker for progression of lung disease in cystic fibrosis. Pediatric Pulmonology 2001;Suppl 22:305. [CFGD REGISTER: PI120v] [Google Scholar]
- LeLorier J, Perreault S, Birnbaum H, Greenberg P, Sheehy O. Savings in direct medical costs from the use of tobramycin solution for inhalation in patients with cystic fibrosis. Clinical Therapeutics 2000;22(1):140-51. [CFGD REGISTER: PI120o] [DOI] [PubMed] [Google Scholar]
- LiPuma JJ. Microbiological and immunologic considerations with aerosolized drug delivery. Chest 2001;120 Suppl 3:118S-23S. [CFGD REGISTER: PI120x] [DOI] [PubMed] [Google Scholar]
- MacLeod DL, Nelson LE, Shawar RM, Lin BB, Lockwood LG, Dirks JE, et al. Aminoglycoside-resistance mechanisms for cystic fibrosis Pseudomonas aeruginosa isolates are unchanged by long-term, intermittent, inhaled tobramycin treatment. Journal of Infectious Diseases 2000;181(3):1180-4. [CFGD REGISTER: PI120n] [DOI] [PubMed] [Google Scholar]
- Moss R, Klystra JW, Montgomery AB, Gibson R. Who benefits more? An analysis of FEV1 and weight in adolescents (age 13 - <18) CF patients using inhaled tobramycin (TOBI). Pediatric Pulmonology 1999;Suppl 19:243. [CFGD REGISTER: PI120k] [Google Scholar]
- Moss RB. Administration of aerosolized antibiotics in cystic fibrosis patients. Chest 2001;120 Suppl 3:107S-13S. [CFGD REGISTER: PI120y] [DOI] [PubMed] [Google Scholar]
- Moss RB. Long-term benefits of inhaled tobramycin in adolescent patients with cystic fibrosis. Chest 2002;121(1):55-63. [CFGD REGISTER: PI120aa] [DOI] [PubMed] [Google Scholar]
- NCT00004829. Phase III randomized study of the inhalation of tobramycin in patients with cystic fibrosis. clinicaltrials.gov/show/NCT00004829 (first received 25 February 2000). [CFGD REGISTER: PI341a]
- NCT00006280. A study of the safety and efficacy of tobramycin for inhalation in young children with cystic fibrosis. clinicaltrials.gov/show/NCT00006280 (first received 12 September 2000). [CFGD REGISTER: PI120hh]
- Nickerson B, Montgomery AB, Klystra JW, Ramsey BW. Safety and effectiveness of 2 years of treatment with intermittent inhaled tobramycin in CF patients. Pediatric Pulmonology 1999;Suppl 19:243-4. [CFGD REGISTER: PI120l] [Google Scholar]
- Otto KL, Montgomery AB, Lin A, Ramsey BW. Seasonality of hospitalisations for pulmonary exacerbations and lower respiratory tract infections in phase III tobramycin solution for inhalation trials. Pediatric Pulmonology 1998;4 Suppl 17:273. [CFGD REGISTER: PI120e] [Google Scholar]
- Quan JM, Vasiljev M, Schaeffler B, Phelps C, Burrington C, Meyer U. Treatment for exacerbation only does not arrest progressive lung function decline in CF. Netherlands Journal of Medicine 1999;54 Suppl:S84. [CFGD REGISTER: PI120g] [Google Scholar]
- Quittner A, Gordon D, Yu X. Convergence of quality of life assessments and clinical outcomes in patients enrolled in the tobramycin solution for inhalation (TSI) trials. In: 24th European Cystic Fibrosis Conference; 2001 June 6-9; Vienna. 2001:P326. [CFGD REGISTER: PI120t]
- Quittner AL, Buu A, Gordon D. Longitudinal changes in global ratings of quality of life for patients in the tobramycin solution for inhalation (TSI) trials. Pediatric Pulmonology 2001;Suppl 22:349. [CFGD REGISTER: PI120w] [Google Scholar]
- Quittner AL, Buu A. Effects of tobramycin solution for inhalation on global ratings of quality of life in patients with cystic fibrosis and Pseudomonas aeruginosa infection. Pediatric Pulmonology 2002;33(4):269-76. [CFGD REGISTER: PI120z] [DOI] [PubMed] [Google Scholar]
- Ramsey B, Burns J, Smith A. Safety and efficacy of tobramycin solution for inhalation in patients with cystic fibrosis: the results of two phase III placebo controlled clinical trial. Pediatric Pulmonology 1997;Suppl 14:137-8. [CFGD REGISTER: PI120c] [Google Scholar]
- Ramsey BW, Bowman MC, Montgomery AB, Smith AR, TOBI Study Group. Design of phase 3 aerosolized tobramycin studies for chronic intermittent therapy. In: 21st European Cystic Fibrosis Conference; 1997 Jun 1-6; Davos. 1997:144. [CFGD REGISTER: PI120b]
- Ramsey BW, Bowman MC, Vasiljev-K M, Smith AR, TOBI Study Group. Results of Phase 3 aerosolized tobramycin studies for chronic intermittent therapy. In: 21st European Cystic Fibrosis Conference; 1997 Jun 1-6; Davos. 1997:144. [CFGD REGISTER: PI120a]
- Ramsey BW, Pepe MS, Quan JM, Otto KL, Montgomery AB, Williams Warren J, et al. Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. New England Journal of Medicine 1999;340(1):23-30. [CFGD REGISTER: PI120d/PI341b] [DOI] [PubMed] [Google Scholar]
- Rosenfeld M, Emerson J, Williams-Warren J, Pepe M, Smith A, Montgomery AB, et al. Defining a pulmonary exacerbation in cystic fibrosis. Journal of Pediatrics 2001;139(3):359-65. [CFGD REGISTER: PI120ee] [DOI] [PubMed] [Google Scholar]
- Taylor CJ. Nebulised high dose tobramycin (TOBI) in adolescents with cystic fibrosis. Pediatric Pulmonology 2001;Suppl 22:291. [CFGD REGISTER: PI120u] [Google Scholar]
- Van Devanter D, Hou K, Yu X. Effect of tobramycin solution for inhalation (TOBI) on long term rates of lung function decline in Pseudomonas aeruginosa-infected cystic fibrosis (CF) patients with mild to moderate lung disease. Pediatric Pulmonology 2000;Suppl 20:298. [CFGD REGISTER: PI120q] [Google Scholar]
- Van Devanter DR, Yu X, Konstan MW. Effect of tobramycin solution for inhalation on circulating white blood cell counts in exacerbating and stable CF patients. In: 24th European Cystic Fibrosis Conference; 2001 Jun 6-9; Vienna. 2001:P172. [CFGD REGISTER: PI120r]
Schuster 2013 {published data only}PI214
- EUCTR2004-003675-36-BE. A randomised, open label study to compare the efficacy and safety of a dry powder formulation of inhaled Colistimethate Sodium and nebulised TNSFI (Tobramycin nebuliser solution for inhalation, TOBI®) in cystic fibrosis patients with pseudomonas aeruginosa lung infection. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2004-003675-36-DK (first received 6 December 2005). [CFGD: PI214h]
- Goldman M, Schuster A, Halliburn C, Doering G, for the Freedom Study Group. A randomised, open label phase 3 study to evaluate the efficacy and safety of a dry powder formulation of inhaled colistimethate sodium (Colobreanthe®) verus tobramycin nebuliser solution (TNS) in cystic fibrosis subjects with chronic Pseudomonas aeruginosa lung infection. Journal of Cystic Fibrosis 2012;11 Suppl 1:S12. [ABSTRACT NO: WS5.5] [CFGD REGISTER: PI214b] [Google Scholar]
- Goldman MH, Pitt T. Lack of emergence of antimicrobial resistance of Pseudomonas aeruginosa after six months inhalation of dry powder colistimethate. Pediatric Pulmonology 2008;43 Suppl 31:331. [CFGD REGISTER: PI214a] [Google Scholar]
- Goldman MH, Shuster A, Haliburn C, Doring G. A randomised, open label phase 3 study to evaluate the efficacy and safety of a dry powder formulation of colistimethate sodium (Colobreanthe®) verus tobramycin nebuliser solution (TNS) in cystic fibrosis subjects with chronic Pseudomonas aeruginosa lung infection. Pediatric Pulmonology 2012;47 Suppl 35:353. [ABSTRACT NO: 363] [CFGD REGISTER: PI214c] [Google Scholar]
- Goldman MH, Werner T, Schuster A. Does persistence with inhaled dry powder antibiotic treatment improve tolerability? Pediatric Pulmonology 2013;48 Suppl 36:347. [ABSTRACT NO: 389] [CENTRAL: 921669] [CFGD REGISTER: PI214f] [Google Scholar]
- Schuster A, Haliburn C, Doring G, Goldman MH, for the Freedom Study Group. Safety, efficacy and convenience of colistimethate sodium dry powder for inhalation (Colobreathe DPI) in patients with cystic fibrosis: a randomised study. Thorax 2013;68(4):344-350. Online data supplement. [CFGD REGISTER: PI214e] 5500100000011299 [EUDRACT: 2004-003675-36] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuster A, Haliburn C, Doring G, Goldman MH, for the Freedom Study Group. Safety, efficacy and convenience of colistimethate sodium dry powder for inhalation (Colobreathe DPI) in patients with cystic fibrosis: a randomised study. Thorax 2013;68(4):344-50. [CFGD REGISTER: PI214d] 5500100000011298 [EUDRACT: 2004-003675-36] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuster A, Pressler T, Zhu H, Haberman R. Efficacy and safety of colistimethate sodium in a paediatric population: results from the FREEDOM trial. Journal of Cystic Fibrosis 2015;14 Suppl 1:S87. [ABSTRACT NO: 118] [CENTRAL: 1077212] [CFGD REGISTER: PI214g] [Google Scholar]
Stead 1987 {published data only}PI53
- Stead RJ, Hodson ME, Batten JC. Inhaled ceftazidime compared with gentamicin and carbenicillin in older patients with cystic fibrosis infected with Pseudomonas aeruginosa. British Journal of Diseases of the Chest 1987;81(3):272-9. [CFGD REGISTER: PI53b] [DOI] [PubMed] [Google Scholar]
- Stead RJ, Hodson ME, Batten JC. Nebulised ceftazidime compared with gentamicin and carbenicillin in adults with cystic fibrosis infected with Pseudomonas aeruginosa. In: 13th Annual Meeting of the European Working Group for Cystic Fibrosis; 1985 Nov 3-8; Jerusalem. Vol. 2. 1985:51. [CFGD REGISTER: PI53a]
Wiesemann 1998 {published data only}PI101
- Ratjen F, Steinkamp G, Doring G, Bauernfeind A, Wiesemann HG, Von Der Hardt H. Prevention of chronic Pseudomonas aeruginosa infection by early inhalation therapy with tobramycin. Pediatric Pulmonology 1994;Suppl 10:250. [CFGD REGISTER: PI101a] [Google Scholar]
- Wiesemann HG, Steinkamp G, Ratjen F, Bauernfeind A, Przyklenk B, Doring G, et al. Placebo-controlled, double-blind, randomized study of aerosolized tobramycin for early treatment of Pseudomonas aeruginosa colonization in cystic fibrosis. Pediatric Pulmonology 1998;25:88-92. [CFGD REGISTER: PI101b] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
ACTRN12620000531910 {published data only}
- ACTRN12620000531910. A Phase IIb, single-centre, randomised, double-blind, comparator-controlled, parallel-group, pilot sudy to evaluate the safety and tolerability of CaEDTA added to inhaled tobramycin vs tobramycin alone as adjunctive therapy to a course of standard treatment for cystic fibrosis patients admitted to hospital with a Pseudomonas aeruginosa pulmonary exacerbation. anzctr.org.au/Trial/Registration/TrialReview.aspx?id=379484&isReview=true (first received 23 March 2020).
Al‐Aloul 2004 {published data only}PI186
- Al-Aloul M, Miller H, Browning P, Ledson MJ, Walshaw MJ. A randomised cross over trial of TOBI® vs IV tobramycin in acute pulmonary exacerbations in CF. Pediatric Pulmonology 2004;38 Suppl 27:249. [CFGD REGISTER: PI186a] [Google Scholar]
- Al-Aloul M, Miller H, Ledson MJ, Walshaw MJ. Tobramycin nebuliser solution (TOBI): a renal sparing alternative to intravenous (IV) tobramycin in acute pulmonary exacerbations in CF. Thorax 2004;59 Suppl II:ii79. [CENTRAL: 517107] [CFGD REGISTER: PI186d] [Google Scholar]
- Al-Aloul M, Miller H, Ledson MJ, Walshaw MJ. Tobramycin nebuliser solution in the treatment of cystic fibrosis pulmonary exacerbations: effect on sputum pseudomonas aeruginosa density. Thorax 2005;2 Suppl 2:ii92. [CFGD REGISTER: PI186b] [Google Scholar]
- Al-Aloul M, Nazareth D, Walshaw M. Nebulized tobramycin in the treatment of adult cf pulmonary exacerbations. Journal of Aerosol Medicine and Pulmonary Drug Delivery 2014;27(4):299-305. [CFGD REGISTER: PI186c] [DOI] [PubMed] [Google Scholar]
Alothman 2000 {published data only}PI157
- Alothman GA, Alsaadi MM, Ho BL, Ho SL, Dupuis A, Corey M, et al. Evaluation of bronchial constriction in children with cystic fibrosis after inhaling two different preparations of tobramycin. Chest 2002;122(3):930-4. [CFGD REGISTER: PI157b] [DOI] [PubMed] [Google Scholar]
- Alothman GA, Coates Al, Corey M, Dupuis A, Ho SL, Ho BL, et al. In cystic fibrosis (CF) patients, does the inhalation of an intravenous tobramycin preparation result in more bronchospasm than a preservative free tobramycin preparation? Pediatric Pulmonology 2000;Suppl 20:298-9. [CFGD REGISTER: PI157a] [Google Scholar]
Alothman 2005 {published data only}
- Alothman GA, Ho B, Alsaadi MM, Ho SL, O'Drowsky L, Louca E, et al. Bronchial constriction and inhaled colistin in cystic fibrosis. Chest 2005;127(2):522-9. [DOI] [PubMed] [Google Scholar]
App 2000 {published data only}PI156
- App EM, Huls G, Bittner-Dersch P, Stolz S, Lindemann H, Matthys H. Impaired lung function influences the serum concentration of inhaled drugs in cystic fibrosis. Pediatric Pulmonology 2000;Suppl 20:279-80. [CFGD REGISTER: PI156b] [Google Scholar]
- Huls G, App EM, Bittner-Dersch, Stolz S, Lindemann H. Impaired lung function influences the serum concentration of inhaled drugs in cystic fibrosis. In: 13th International Cystic Fibrosis Congress; 2000 Jun 4-8; Stockholm. 2000:177. [CFGD REGISTER: PI156a]
Bruinenberg 2008 {published data only}PI216
- Bruinenberg P, Otulana B, Blanchard J, Morishige R, Cipolla D, Wilson J, et al. The effect of once-a day inhaled liposomal ciprofloxacin hydrochloride on sputum bacterial density in cystic fibrosis patients with chronic pulmonary P aeruginosa colonization. Pediatric Pulmonology 2008;43 Suppl 31:344. [CFGD REGISTER: PI216] [Google Scholar]
Carswell 1987 {published data only}PI54
- Carswell F, Ward C, Cook DA, Speller DCE. A controlled trial of nebulized aminoglycoside and oral flucloxacillin versus placebo in the out-patient management of children with cystic fibrosis. British Journal of Diseases of the Chest 1987;81(4):356-60. [CFGD REGISTER: PI54] [DOI] [PubMed] [Google Scholar]
Chua 1990 {published data only}PI66
- Chua H, Collis G, Souef P. Bronchial response of children with cystic fibrosis to nebulised antibiotics. Australian and New Zealand Journal of Medicine 1990;20:537. [CFGD REGISTER: PI66b] [Google Scholar]
- Chua HL, Collis GG, Le Souef PN. Bronchial response to nebulised antibiotics in children with cystic fibrosis. European Respiratory Journal 1990;3(10):1114-6. [CFGD REGISTER: PI66a] [PubMed] [Google Scholar]
Claut 2011 {published data only}
- Claut L, DiCicco M, Cariani L, Defilippi G, Costantini D, Colombo C. Tobramycin and hyaluronic acid nasal solution: beyond antimicrobial effect. Pediatric Pulmonology 2011;46 Suppl 34:322. [ABSTRACT NO.: 304] [CFGD REGISTER: CO52a] [Google Scholar]
Coates 2011 {published data only}PI241
- Coates AL, Denk O, Leung K, Ribeiro N, Chan J, Green M, et al. Higher tobramycin concentration and vibrating mesh technology can shorten antibiotic treatment time in cystic fibrosis. Pediatric Pulmonology 2011;46(4):401-8. [CFGD REGISTER: PI241b] [DOI] [PubMed] [Google Scholar]
- Denk O, Caotes AL, Keller M, Leung K, Green M, Chan J, et al. Lung delivery of a new tobramycin nebuliser solution (150mg/1.5ml) by an investigational eFlow® nebuliser is equivalent to TOBI® but in a fraction of time. Journal of Cystic Fibrosis 2009;8 Suppl 2:S66. [ABSTRACT NO: 264] [CFGD REGISTER: PI241c] 5500100000003576 [Google Scholar]
- Keller M, Coates AL, Griese M, Denk O, Schierholz J, Knoch M. In-vivo data support equivalent therapeutic efficacy of a new tobramycin inhalation solution (150mg/1.5ml) administered by the eFlow® electronic nebuliser compared to TOBI® in the PARI LC PLUS®. Journal of Cystic Fibrosis 2010;9 Suppl 1:S22. [ABSTRACT NO: 84] [CFGD REGISTER: PI241a] [Google Scholar]
Cooper 1985 {published data only}PI129
- Cooper DM, Harris M, Mitchell I. Comparison of intravenous and inhalation antibiotic therapy in acute pulmonary deterioration in cystic fibrosis. American Review of Respiratory Disease 1985;131:no pagination. [ABSTRACT NO: A242] [CFGD REGISTER: PI129] [Google Scholar]
Davies 2004 {published data only}PI189
- Conway SP, Davies JC, Etherington C, Goldman HH, Howard E, Jaffe A, et al. Piloting the use of the cystic fibrosis questionnaire (CFQ) in CF patients changing to dry powder inhaled colistimethate. Journal of Cystic Fibrosis 2007;6 Suppl 1:S76. [ABSTRACT NO: 309] [CFGD REGISTER: PI189b] [Google Scholar]
- Davies JC, Hall P, Francis J, Scott S, Geddes DM, Conway S, et al. A dry powder formulation of colistimethate sodium is safe and well tolerated in adults and children with CF. Pediatric Pulmonology 2004;38 Suppl 27:283. [ABSTRACT NO: 278] [CFGD REGISTER: PI189a] [Google Scholar]
- Goldman MH, Howard E, Lard N. FEV1% predicted may not be a simple end point for CF studies. Journal of Cystic Fibrosis 2007;6 Suppl 1:S34. [ABSTRACT NO: 141] [CFGD REGISTER: PI189c] [Google Scholar]
Dodd 1997 {published data only}PI100
- Dodd M, Maddison J, Abbott J, Webb AK. The effect of the tonicity of nebulised colistin on lung function in adults with cystic fibrosis. In: 18th European Cystic Fibrosis Conference; 1993 May 21-26; Madrid. 1993:121. [CFGD REGISTER: PI100a]
- Dodd ME, Abbott J, Maddison J, Moorcroft AJ, Webb AK. Effect of tonicity of nebulised colistin on chest tightness and pulmonary function in adults with cystic fibrosis. Thorax 1997;52(7):656-8. [CFGD REGISTER: PI100b] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dodd ME, Maddison J, Abbot J, Webb AR. The effect of the tonicity of nebulised colistin on chest tightness and lung function in adults with cystic fibrosis. European Respiratory Journal 1993;6 Suppl 17:515s. [CFGD REGISTER: PI100c] [Google Scholar]
Dodd 1998 {published data only}PI237
- Dodd ME, Haworth CS, Moorcroft AJ, Miles J, Webb AK. Is medicine evidence-based when there is discrepancy between patient reported and objective measures of compliance in clinical trials? Pediatric Pulmonology 1998;26 Suppl 17:389-90. [CFGD REGISTER: PI237] [Google Scholar]
Dorkin 2015 {published data only}PI261
- Cystic Fibrosis Foundation. Inhaled ciprofloxacin. www.cff.org/clinicaltrials (accessed 17 February 2010). [CFGD REGISTER: PI261c]
- Dorkin H, Criollo M, Reimnitz P, Alder J, Hampel B. Randomized, double-blind, placebo-controlled, multicenter study to evaluate the safety and efficacy of inhaled ciprofloxacin compared with placebo in patients with cystic fibrosis- a phase IIB study of ciprofloxacin dry powder for inhalation (DPI). Pediatric Pulmonology 2011;46 Suppl 34:296. [ABSTRACT NO: 235] [CFGD REGISTER: PI261] [CFGD REGISTER: PI261a] 5500100000011264 [Google Scholar]
- Dorkin HL, Staab D, Operschall E, Alder J, Criollo M. Ciprofloxacin DPI: a randomised, placebo-controlled, phase IIb efficacy and safety study on cystic fibrosis. BMJ Open Respiratory Research 2015;2(1):e000100. [CFGD REGISTER: PI261d] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT00645788. Study to evaluate the safety and efficacy of ciprofloxacin (inhaled) in patients with cystic fibrosis [Randomized, double-blind, placebo-controlled, multicenter study to evaluate the safety and efficacy of inhaled ciprofloxacin compared to placebo in subjects with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT00645788 (first received 28 March 2008). [CFGD REGISTER: PI261b] [CLINICALTRIALS.GOV IDENTIFIER: NCT00645788]
Dupont 2008 {published data only}PI207
- Clancy JP, Dupont L, Konstan MW, Billings J, Fustik S, Goss CH, et al. Phase II studies of nebulised Arikace in CF patients with Pseudomonas aeruginosa infection. Thorax 2013;68(9):818-25. [CENTRAL: 876398] [CFGD REGISTER: PI207e // PI222c] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clancy JP, Dupont L, Konstan MW, Billings J, Fustik S, Goss CH, et al. Phase II studies of nebulised Arikace in CF patients with Pseudomonas aeruginosa infection. Thorax 2013;68(9):818-25. Online supplementary data. [CFGD REGISTER: PI222d // PI207f] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clancy JP, Minic P, Dupont L, Goss CH, Quittner AL, Lymp JF, et al. Full analysis of data from two phase II blinded & placebo-controlled studies of nebulized liposomal amikacin for inhalation (ArikaceTM) in the treatment of CF patients with Pseudomonas aeruginosa lung infection. Pediatric Pulmonology 2010;45 Suppl 33:299. [ABSTRACT NO: 227] [CFGD REGISTER: PI207d // PI255] 5500100000010628 [Google Scholar]
- Dupont L, Minic P, Fustic S, Mazurek H, Solyom E, Feketova A, et al. A randomised placebo-controlled study of nebulized liposomal amikacin (Arikace™) in the treatment of cystic fibrosis patients with chronic Pseudomonas aeruginosa lung infection. Journal of Cystic Fibrosis 2008;7 Suppl 2:S26. [ABSTRACT NO: 102] [CFGD REGISTER: PI207a] [Google Scholar]
- Dupont LJ, Clancy JP, Minic P, Goss CH, Fustic S, Mazurek Hetal. Evaluation of two phase II blinded and placebo-controlled studies of nebulized liposomal amikacin (Arikace") in the treatment of cystic fibrosis patients with Pseudomonas aeruginosa lung infection. American Journal of Respiratory and Critical Care Medicine 2010;181(Meeting Abstracts):no pagination. [ABSTRACT NO: A1836] [CENTRAL: 758757] [CFGD REGISTER: PI222e // PI207g] [Google Scholar]
- Dupont LJ, Minic P, Fustik S, Mazurek H, Solyom E, Feketeova A, et al. A randomized placebo-controlled study of nebulized liposomal amikacin (Arikace™) in the treatment of cystic fibrosis patients with chronic Pseudomonas aeruginosa lung infection. Pediatric Pulmonology 2008;43 Suppl 31:301. [ABSTRACT NO: 285] [CFGD REGISTER: PI207b] [Google Scholar]
- Gupta R, Dupont L, Minin P, Fustik S, Mazurek H, Solyom E. A randomized placebo-controlled study of nebulized liposomal amikacin (Arikace™) in the treatment of cystic fibrosis patients with chronic Pseudomonas aeruginosa lung infection (protocol TR02-105). American Journal of Respiratory and Critical Care Medicine 2009;179(Meeting Abstracts):no pagination. [ABSTRACT NO: A1199] [CFGD REGISTER: PI207c] [Google Scholar]
- NCT00777296. Multidose safety and tolerability study of dose escalation of liposomal amikacin for inhalation (ARIKACETM). clinicaltrials.gov/show/NCT00777296 (first received 22 October 2008). [CFGD REGISTER: PI207i]
- Okusanya OO, Bhavnani SM, Hammel J, Minic P, Dupont LJ, Forrest A, et al. Pharmacokinetic and pharmacodynamic evaluation of liposomal amikacin for inhalation in cystic fibrosis patients with chronic pseudomonal infection. Antimicrobial Agents and Chemotherapy 2009;53(9):3847-54. [CFGD REGISTER: PI207h] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okusanya OO, Bhavnani SM, Hammel JP, Forrest A, Bulik CC, Ambrose PG, et al. Evaluation of the pharmacokinetics and pharmacodynamics of liposomal amikacin for inhalation in cystic fibrosis patients with chronic pseudomonal infections using data from two phase 2 clinical studies. Antimicrobial Agents and Chemotherapy 2014;58(9):5005-15. [CFGD REGISTER: PI207j] [DOI] [PMC free article] [PubMed] [Google Scholar]
Eisenberg 1997 {published data only}PI117
- Eisenberg J, Pepe M, Williams-Warren J, Vasiliev M, Montgomery AB, Smith AL, et al. A comparison of peak sputum tobramycin concentration in patients with cystic fibrosis using jet and ultrasonic nebulizer systems. Chest 1997;111:955-62. [CFGD REGISTER: PI117] [DOI] [PubMed] [Google Scholar]
EUCTR2005‐004103‐10‐DE {published data only}
- EUCTR2005-004103-10-DE. Randomized, open labeled, multi center, active controlled, parallel 28 days safety and bioavailability study of Tobramycin 100 PARI nebulized with eFlow® versus TOBI® nebulized with PARI LC PLUS in cystic fibrosis patients with Pseudomonas Aeruginosa infections. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2005-004103-10-DE (first received 30 January 2006). [CFGD REGISTER: DT64]
EUCTR2006‐006215‐68‐DE {published data only}
- EUCTR2006-006215-68-DE. A multicentre,multinational, open-label, randomised, parallel group clinical trial of tobrineb®/actitob®/ bramitob® (tobramycin solution for nebulisation, 300 mg twice daily in 4 ml unit dose vials) compared to tobi® in the treatment of patients with cystic fibrosis and chronic infection with pseudomonas aeruginosa. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2006-006215-68-CZ (first received 16 June 2008).
EUCTR2007‐003868‐22‐FR {published data only}
- EUCTR2007-003868-22-FR. Assesment of efficacy and tolerability of inhaled tobramycin vs placebo in cystic fibrosis patients receiving antibiotherapy for 28 days for pseudomonas aeruginosa primo colonisation - nebcinal 01-07. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2007-003868-22-FR (first received 19 March 2007). [CFGD REGISTER: PI300]
EUCTR2007‐005346‐20‐GB {published data only}
- EUCTR2007-005346-20-GB. Does nebulised tobramycin (TOBI) via e-flow delivery systems cause a raised peak serum tobramycin level in children with Cystic Fibrosis? - TOBICF. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2007-005346-20-GB (first received 24 July 2007). [CFGD REGISTER: DT67]
EUCTR2008‐008314‐40‐DK {published data only}
- EUCTR2008-008314-40-DK. Randomized, double-blind, placebo-controlled, multicenter study to evaluate the safety and efficacy of inhaled ciprofloxacin compared to placebo in subjects with cystic fibrosis. trialsearch.who.int/Trial2.aspx?TrialID=NCT00645788 (first received 26 March 2009).
EUCTR2009‐013660‐39‐FR {published data only}
- EUCTR2009-013660-39-FR. Etude pharmacocinetique de l’equivalence de la biodisponibilite entre Nebcinal® 150mg/3ml administre par Aeroneb® Idehaler® et Tobi® 300mg/5ml administre par Pari LC Plus®. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2009-013660-39-FR (first received 10 September 2009). [CFGD REGISTER: DT68]
EUCTR2010‐023533‐34‐FR {published data only}
- EUCTR2010-023533-34-FR. Etude pharmacocinetique de l’equivalence de la biodisponibilite entre Nebcinal® 150mg/3ml administre par Aeroneb® Idehaler® et Tobi® 300mg/5ml administre par Pari LC Plus® /Pulmoaid® chez des patients atteints de mucoviscidose. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2010-023533-34-FR (first received 14 December 2010). [CFGD REGISTER: DT70]
EUCTR2014‐001401‐41‐NL {published data only}
- EUCTR2014-001401-41-NL. Once daily deep inhalation of tobramycin with smart nebulizer more effective to treat small airways disease in cystic fibrosis? www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2014-001401-41-NL (first received 29 July 2014). [CFGD REGISTER: DT71]
Fiel 2013 {published data only}
- Fiel S, Nasr S, Wan R, Angyalosi G, Brockhaus F, Maykut R, et al. Rate of hospitalizations due to respiratory events with tobramycin inhalation powder in patients with cystic fibrosis. Chest 2013;144(4 Meeting Abstracts):p756A. [CFGD REGISTER: PI239o // PI260h] [Google Scholar]
Flume 2016a {published data only}PI284
- Flume P, Van Devanter DR, Cohen F, Fleming R, Elborn JS. Safety profile of levofloxacin inhalation solution from 3 controlled cystic fibrosis trials. Journal of Cystic Fibrosis 2015;14 Suppl 1:S87. [ABSTRACT NO: 117] [CENTRAL: 1077213] [CFGD REGISTER: PI283c // PI240f // PI284c] [Google Scholar]
- Flume PA, Van Devanter DR, Morgan EE, Dudley MN, Loutit JS, Bell SC, et al. A phase 3, multi-center, multinational, randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of levofloxacin inhalation solution (APT-1026) in stable cystic fibrosis patients. Journal of Cystic Fibrosis 2016;15(4):495-502. [CFGD REGISTER: PI284d] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Flume PA, Van Devanter DR, Morgan EE, Dudley MN, Loutit JS, Bell SC, et al. A phase 3, multi-center, multinational, randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of levofloxacin inhalation solution (APT-1026) in stable cystic fibrosis patients. Journal of Cystic Fibrosis 2016;15(4):495-502. Online supplement. [CFGD REGISTER: PI284e] [DOI] [PubMed] [Google Scholar]
- NCT01180634. MP-376 (Aeroquin™, levofloxacin for inhalation) in patients with cystic fibrosis [A phase 3, multi-center, multinational, randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of MP-376 (Levofloxacin Inhalation Solution; Aeroquin™) in stable cystic fibrosis patients]. clinicaltrials.gov/show/NCT01180634 (first received 12 August 2010). [CENTRAL: 1012532] [CFGD REGISTER: PI284a]
- Schwarz C, Spinola M, Flume PA, Elborn JS. Potential taste disturbance is largely mild and diminishes with continuing treatment in cystic fibrosis patients treated with levofloxacin inhaled solution. Journal of Cystic Fibrosis 2018;17(Suppl 3):S81-2. [CFGD REGISTER: PI283f] [Google Scholar]
- Van Devanter D, Flume PA, Fleming R, Elborn J. How often is pulmonary exacerbation defined by ≥4 Fuchs criteria associated with antibiotic treatment? Pediatric Pulmonology 2014;49 Suppl 38:356. [ABSTRACT NO: 388] [CENTRAL: 1012531] [CFGD REGISTER: PI283b // PI284b] [Google Scholar]
- Vandevanter DR, Flume PA, Cohen F, Fleming R, Elborn JS. Lack of correlation between sputum Pseudomonas aeruginosa density and FEV1 changes among CF patients treated with inhaled antibiotics. Journal of Cystic Fibrosis 2014;13 Suppl:S6. [CFGD REGISTER: PI283g] [Google Scholar]
Franz 1985 {published data only}
- Franz MN, Spohn WA, Ronald PM. Evaluation of tobramycin aerosol therapy in cystic fibrosis. In: Cystic Fibrosis Club Abstracts; 1985. Vol. 26. 1985:143.
Frederiksen 1997 {published data only}PI118
- Frederiksen B, Hansen A, Koch C, Hoiby N. Delay of recurrence of Pseudomonas aeruginosa in patients with cystic fibrosis with inhaled colistin and oral ciprofloxacin; a comparison between 3 weeks and 3 months of treatment. Pediatric Pulmonology 1997;Supp 14:288. [CFGD REGISTER: PI118a] [Google Scholar]
- Frederiksen B, Pressler T, Koch C, Hoiby N. Endpoints for evaluating early anti-pseudomonal treatment: changes in pseudomonas prevalence and in pulmonary function. Pediatric Pulmonology 2003;Suppl 25:334. [CFGD REGISTER: PI118b] [Google Scholar]
Frost 2018 {published data only}
- Frost F, Fothergill J, Winstanley C, Nazareth D, Walshaw MJ. Inhaled aztreonam lysine recovers lung function and improves quality of life in acute pulmonary exacerbations of cystic fibrosis. Thorax 2019;74:A13-4. [CFGD REGISTER: PI310b] [Google Scholar]
- Frost F, Fothergill J, Winstanley C, Walshaw M, Nazareth D. Aztreonam lysine inhalation solution recovers lung function and improves quality of life in treatment of acute pulmonary exacerbation of cystic fibrosis. Pediatric Pulmonology 2019;54 Suppl 2:430. [CFGD REGISTER: PI310c] [Google Scholar]
- Frost F, Fothergill J, Winstanley C, Walshaw M, Nazareth D. Aztreonam lysine recovers lung function and improves quality of life in the treatment of acute exacerbations of cystic fibrosis: results from an open-label randomised crossover study (AZTEC-CF). Journal of Cystic Fibrosis 2020;19 Suppl:S98. [CFGD REGISTER: PI310e] [DOI] [PubMed] [Google Scholar]
- Frost F, Nazareth D, Walshaw M, Young G, Winstanley C, Fothergill J. Inhaled and intravenous treatment strategies exert different effects on the lung microbiome during acute pulmonary exacerbations of cystic fibrosis: results from the AZTEC-CF study. Journal of Cystic Fibrosis 2020;19 Suppl:S80. [CFGD REGISTER: PI310f] [Google Scholar]
- Frost F, Nazareth D, Walshaw M. Aztec-CF study: aztreonam lysine for inhalation in the treatment of pulmonary exacerbations of cystic fibrosis. Pediatric Pulmonology 2018;53(S2):330. [CFGD REGISTER: PI310a] [Google Scholar]
- Frost F, Young GR, Wright L, Miah N, Smith DL, Winstanley C, et al. The clinical and microbiological utility of inhaled aztreonam lysine for the treatment of acute pulmonary exacerbations of cystic fibrosis: an open-label randomised crossover study (AZTEC-CF). Journal of Cystic Fibrosis 2021;20(6):994-1002. [CFGD Register: PI310g] [DOI] [PubMed] [Google Scholar]
Galeva 2013 {published data only}PI260
- EUCTR2008-002318-22-LT. A randomized, double-blind, placebo-controlled, multi-center phase III study in cystic fibrosis (CF) subjects to assess efficacy, safety and pharmacokinetics of tobramycin inhalation powder from a modified manufacturing process (tipnew). trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2008-002318-22-LT (first received 22 January 2009). [CFGD REGISTER: PI260j]
- Galeva I, Angyalosi G, Perrin M-E, Thomas K, Prasad N, Higgins M. Long-term safety and efficacy of tobramycin inhalation powder-results from edit core and extension study e1 in cystic fibrosis patients aged 6-21 years. American Journal of Respiratory and Critical Care Medicine 2013;187 Suppl:A2070. [CFGD REGISTER: PI260i] [Google Scholar]
- Galeva I, Higgins M, Piggott S, Angyalosi G. A randomized, double-blind, placebo-controlled study of tobramycin inhalation powder in patients with cystic fibrosis: the edit trial. Pediatric Pulmonology 2011;46 Suppl 34:344. [ABSTRACT NO: 366] [CFGD REGISTER: PI260a] 5500100000011266 [Google Scholar]
- Galeva I, Konstan MW, Higgins M, Angyalosi G, Brockhaus F, Piggott S, et al. Tobramycin inhalation powder manufactured by improved process in cystic fibrosis: the randomized EDIT trial. Current Medical Research and Opinion 2013;29(8):947-56. [CFGD REGISTER: PI260e] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galeva I, Konstan MW, Higgins M, Piggott S, Angyalosi G, Brockhaus F, et al. A challenging double-blind, placebo-controlled study of tobramycin inhalation powder in cystic fibrosis: results of the EDIT trial. Journal of Cystic Fibrosis 2012;11 Suppl 1:S12. [ABSTRACT NO: WS5.6] [CFGD REGISTER: PI260b] 5500100000011250 [Google Scholar]
- Konstan M, Flume P, Wan R, Perrin M, Maykut R, Angyalosi G. Long-term safety and efficacy of tobramycin inhalation powder in cystic fibrosis patients with P. aeruginosa: the EDIT trials and its two open-label extension studies. Pediatric Pulmonology 2013;48 Suppl 36:344. [ABSTRACT NO: 381] [CFGD REGISTER: PI260d] [Google Scholar]
- Konstan MW, Flume PA, Galeva I, Wan R, Debonnett LM, Maykut RJ, et al. One-year safety and efficacy of tobramycin powder for inhalation in patients with cystic fibrosis. Pediatric Pulmonology 2016;51(4):372-8. [CENTRAL: 1260415] [CFGD REGISTER: PI260g] [PMID: ] [DOI] [PubMed] [Google Scholar]
- NCT00918957. A study of tobramycin inhalation powder from a modified manufacturing process versus placebo. clinicaltrials.gov/show/NCT00918957 (first received 11 June 2009). [CFGD REGISTER: PI260k]
- Quittner AL, Higgins ML, Angyalosi G, Brockhaus F, Thomas K, Zhang J. Trends in health-related quality of life (HRQoL) in cystic fibrosis with tobramycin inhalation powder: the EDIT trial. Journal of Cystic Fibrosis 2012;11 Suppl 1:S73. [ABSTRACT NO: 67] [CFGD REGISTER: PI260c] 5500100000011252 [Google Scholar]
Geborek 2003 {published data only}PI176
- Geborek A, Hjelte L, Lindblad A, Mared L, Eriksson L, Johannesson M, et al. Cross-over study of TOBI® vs. intravenous tobramycin in combination treatment of pulmonary exacerbations in cystic fibrosis patients. Journal of Cystic Fibrosis 2003;Suppl 1:S22. [CFGD REGISTER: PI176] [Google Scholar]
Geller 2004 {published data only}PI183
- Geller DE, Rodriguez CA, Howenstine M, Murphy T, Voter K, Nickerson B, et al. The effects of doubling concentration of tobramycin solution for inhalation on pharmacokinetics (PK), safety and delivery time in patients with cystic fibrosis (CF). American Journal of Respiratory and Critical Care Medicine 2004;169(7):no pagination. [ABSTRACT NO: A391] [CFGD REGISTER: PI183a] [Google Scholar]
- Rosenfeld M, Geller DE, Rodriguez CA, Howenstine M, Konstan M, Ordonez C, et al. Serum pharmacokinetics of two preparations of tobramycin solution for inhalation in young cystic fibrosis patients. American Journal of Respiratory and Critical Care Medicine 2004;169(7):no pagination. [ABSTRACT NO: A386] [CFGD REGISTER: PI183b] [Google Scholar]
Geller 2007 {published data only}PI187
- Geller DE, Howenstine M, Conrad C, Smith J, Mulye S, Shrewsbury SB. A phase 1 study to assess the tolerability of a novel tobramycin powder for inhalation (TPI) formulation in cystic fibrosis subjects. Pediatric Pulmonology 2004;38 Suppl 27:250. [CFGD REGISTER: PI187a] [Google Scholar]
- Geller DE, Konstan MW, Smith J, Noonberg SB, Conrad C. Novel tobramycin inhalation powder in cystic fibrosis subjects: pharmacokinetics and safety. Pediatric Pulmonology 2007;42(4):307-13. [CFGD REGISTER: PI187c] [DOI] [PubMed] [Google Scholar]
- Rodriguez CA, Shrewsbury SB, Potter SN, Nardella P, Geller DE. Single dose pharmacokinetics of tobramycin after administration of a novel dry powder formulation (TPI) in subjects with cystic fibrosis (CF). Pediatric Pulmonology 2004;38 Suppl 27:250. [CFGD REGISTER: PI187b] [Google Scholar]
Geller 2011a {published data only}PI254
- Geller DE, Flume PA, Griffith DC, Morgan E, White D, Loutit J, et al. Pharmacokinetics (PK) of aerosol MP-376 (Aeroquin; levofloxacin inhalation solution) in CF patients. Journal of Cystis Fibrosis 2010;9 Suppl 1:S23. [ABSTRACT NO: 87] [CFGD REGISTER: PI254a] 5500100000010626 [Google Scholar]
- Geller DE, Flume PA, Griffith DC, Morgan E, White D, Loutit JS, et al. Pharmacokinetics and safety of MP-376 (levofloxacin inhalation solution) in cystic fibrosis subjects. Antimicrobial Agents and Chemotherapy 2011;55(6):2636-40. [CFGD REGISTER: PI254b] 5500100000010627 [DOI] [PMC free article] [PubMed] [Google Scholar]
Geller 2011b {published data only}PI240
- Conrad D, Flume P, Sindel L, Andrews S, Morgan L, Loutit J, et al. Phase 2b study of inhaled MP-376 (Aeroquin, levofloxacin inhalation solution) in stable cystic fibrosis (CF) patients with chronic Pseudomonas aeruginosa (PA) lung infection. American Journal of Respiratory and Critical Care Medicine 2010;181(Meeting Abstracts):no pagination. [CENTRAL: 1031676] [CFGD REGISTER: PI240g] [EMBASE: 70839804] [Google Scholar]
- EUCTR2008-001728-30-NL. A phase 2, multi-center, randomized, double-blind, placebo-controlled study to evaluate the safety, tolerability and efficacy of three dosage regimens of MP- 376 solution for inhalation given for 28 days to stable cystic fibrosis patients. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2008-001728-30-DE (first received 7 May 2008). [CFGD REGISTER: PI240i]
- Flume P, Geller DE, Sindel L, Staab D, Fischer R, Riethmuller J, et al. Effects of inhaled MP-376 (Aeroquin, levofloxacin inhalation solution) on lung function in stable cystic fibrosis (CF) patients with chronic pseudomonas aeruginosa (PA) lung function. Journal of Cystic Fibrosis 2010;9 Suppl 1:S23. [ABSTRACT NO: 86] [CFGD REGISTER: PI240a] [Google Scholar]
- Flume P, Van Devanter DR, Cohen F, Fleming R, Elborn JS. Safety profile of levofloxacin inhalation solution from 3 controlled cystic fibrosis trials. Journal of Cystic Fibrosis 2015;14 Suppl 1:S87. [ABSTRACT NO: 117] [CENTRAL: 1077213] [CFGD REGISTER: PI240f // PI283c // PI284c] [Google Scholar]
- Flume PA, Geller DE, Loutit JS, Dudley MN, Conrad D, Mpex 204 Study Group. Effects of inhaled MP-376 (AeroquinTM, levofloxacin inhalation solution) on cystic fibrosis patients with both Staphylococcus aureus (SA) and Pseudomonas aeruginosa (PA) lung infection. Journal of Cystic Fibrosis 2011;10 Suppl 1:S22. [ABSTRACT NO: 87] [CFGD REGISTER: PI240b] [Google Scholar]
- Geller D, Flume PA, Sindel L, Staab D, Fischer R, Loutit J, et al. Effects of inhaled MP-376 (Aeroquin, levofloxacin inhalation solution) on the need for other anti-pseudomonal antimicrobials in stable CF patients with chronic Pseudomonas aeruginosa lung infection. Pediatric Pulmonology 2010;45 Suppl 33:301. [ABSTRACT NO: 232] [CFGD REGISTER: PI240c] [Google Scholar]
- Geller DE, Flume PA, Staab D, Fischer R, Loutit JS, Conrad DJ, et al. Levofloxacin inhalation solution (MP-376) in patients with cystic fibrosis with Pseudomonas aeruginosa. American Journal of Respiratory and Critical Care Medicine 2011;183(11):1510-6. [CFGD REGISTER: PI240d] [DOI] [PubMed] [Google Scholar]
- Geller DE, Flume PA, Staab D, Fischer R, Loutit JS, Conrad DJ. Levofloxacin inhalation solution (MP-376) in patients with cystic fibrosis with pseudomonas aeruginosa. American Journal of Respiratory and Critical Care Medicine 2011;183(11):1510-6. Online supplemental methods. [CENTRAL: 1073292] [CFGD REGISTER: PI240e] [DOI] [PubMed] [Google Scholar]
- NCT00677365. Safety, tolerability and efficacy of MP-376 given for 28 days to cystic fibrosis (CF) patients. clinicaltrials.gov/show/NCT00677365 (first received 14 May 2008). [CFGD REGISTER: PI240h]
Gibson 2003 {published data only}PI151
- Gibson RL, Emerson J, McNamara S, Burns JL, Rosenfeld M, Yunker A, et al. Significant microbiological effect of inhaled tobramycin in young children with cystic fibrosis. American Journal of Respiratory and Critical Care Medicine 2003;167(6):841. Online supplement. [CFGD REGISTER: PI151e] [DOI] [PubMed] [Google Scholar]
- Gibson RL, Emerson J, McNamara S, Burns JL, Rosenfeld M, Yunker A, et al. Significant microbiological effect of inhaled tobramycin in young children with cystic fibrosis. American Journal of Respiratory and Critical Care Medicine 2003;167(6):841-9. [CFGD REGISTER: PI151d] [DOI] [PubMed] [Google Scholar]
- Gibson RL, Emerson J, McNamara S. A randomized controlled trial of inhaled tobramycin in young children with cystic fibrosis: eradication of Pseudomonas from the lower airway. Pediatric Pulmonology 2002;Suppl 24:300. [CFGD REGISTER: PI151c] [Google Scholar]
- Rosenfeld M, Borowitz D, Emerson J, Gibson R, McCoy K, McNamara S, et al. Serum pharmacokinetics and safety of inhaled tobramycin in very young CF patients. Pediatric Pulmonology 1999;Suppl 19:262. [CFGD REGISTER: PI151s] [Google Scholar]
- Rosenfeld M. Serum and lower respiratory tract tobramycin concentrations produced by inhaled tobramycin (TOBI) in young children with cystic fibrosis. Pediatric Pulmonology 1999;Suppl 19:106-108. [CFGD REGISTER: PI151b] [Google Scholar]
Gibson 2006 {published data only}PI188
- Gibson RL, Retsch-Bogart G, Ahrens R, Clancy J, Daines C, Milla C, et al. Safety and tolerability of aztreonam for inhalation (AI) in cystic fibrosis patients. Pediatric Pulmonology 2004;38 Suppl 27:253. [CFGD REGISTER: PI188a] [Google Scholar]
- Gibson RL, Retsch-Bogart GZ, Oermann C, Milla C, Pilewski J, Daines C, et al. Microbiology, safety, and pharmacokinetics of aztreonam lysinate for inhalation in patients with cystic fibrosis. Pediatric Pulmonology 2006;41(7):656-65. [CFGD REGISTER: PI188b] [DOI] [PubMed] [Google Scholar]
Goss 2013 {published data only}PI222
- Clancy JP, Dupont L, Konstan MW, Billings J, Fustik S, Goss CH, et al. Phase II studies of nebulised Arikace in CF patients with Pseudomonas aeruginosa infection. Thorax 2013;68(9):818-25. [CFGD REGISTER: PI222c // PI207e] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clancy JP, Dupont L, Konstan MW, Billings J, Fustik S, Goss CH, et al. Phase II studies of nebulised Arikace in CF patients with pseudomonas aeruginosa infection. Thorax 2013;68(9):818-25. Online supplementary data. [CFGD REGISTER: PI222d // PI207f] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clancy JP, Minic P, Dupont L, Goss CH, Quittner AL, Lymp JF, et al. Full analysis of data from two phase II blinded & placebo-controlled studies of nebulized liposomal amikacin for inhalation (Arikace) in the treatment of CF patients with Pseudomonas aeruginosa lung infection. Pediatric Pulmonology 2010;45 Suppl 33:299. [ABSTRACT NO: 227] [CFGD REGISTER: PI222b // PI207d] 5500100000010628 [Google Scholar]
- Dupont LJ, Clancy JP, Minic P, Goss CH, Fustic S, Mazurek Hetal. Evaluation of two phase II blinded and placebo-controlled studies of nebulized liposomal amikacin (Arikace") in the treatment of cystic fibrosis patients with Pseudomonas aeruginosa lung infection. American Journal of Respiratory and Critical Care Medicine 2010;181(Meeting Abstracts):no pagination. [ABSTRACT NO: A1836] [CENTRAL: 758757] [CFGD REGISTER: PI222e // PI207g] [Google Scholar]
- Goss CH, Clancy JP, Nick JA, Billings J, Rubenstein RC, Young KR, et al. A phase 2 blinded and placebo-controlled study of nebulized liposomal amikacin (Arikace™) in the treatment of CF patients with pseudomonas aeruginosa lung infection. Pediatric Pulmonology 2009;44 Suppl 32:295. [ABSTRACT NO: 239] [CFGD REGISTER: PI222a] [Google Scholar]
- NCT00558844. Safety/tolerability study of arikayceâ„¢ in cystic fibrosis patients with chronic infection due to pseudomonas aeruginosa. clinicaltrials.gov/show/NCT00558844 (first received 15 November 2007). [CFGD REGISTER: PI222f]
Griese 2009 {published data only}
- Griese M, Kappler M, Eismann C, Mazurek H, Denk O, Goedings P, et al. Pulmonary delivery of tobramycin by an investigational Eflow® electronic nebulizer saves 50% of the drug, and results in equivalent or improved tobramycin safety levels in plasma and sputum. Pediatric Pulmonology 2009;44 Suppl 32(S32):300 (Abstract no 252). [Google Scholar]
Griffith 2008 {published data only}PI210
- Geller DE, Flume P, Schwab R, Fornos P, Conrad DJ, Morgan E, et al. A phase 1 safety, tolerability and pharmacokinetic (PK) study of MP-376 (levofloxacin solution for inhalation) in stable cystic fibrosis (CF) patients. Pediatric Pulmonology 2008;43 Suppl 31:315. [ABSTRACT NO: 321] [CFGD REGISTER: PI210b] [Google Scholar]
- Griffith DC, Hansen C, Pressler T, Balchen T, Jensen TJ, Geller DE, et al. Single-dose pharmacokinetics of aerosol MP-376 (levofloxacin solution for inhalation) in cystic fibrosis patients: PK-PD implications. Journal of Cystic Fibrosis 2008;7 Suppl 2:S26. [CFGD REGISTER: PI210a] [Google Scholar]
- Kearns GL, Rubino CM, Griffith DC, Geller DE, Forrest A, Bhavnani SM, et al. Levofloxacin pharmacokinetics (PK) after administration of MP-376 (levofloxacin inhalation solution; Aeroquin) in children with cystic fibrosis. Journal of Cystic Fibrosis 2011;10 Suppl 1:S23. [ABSTRACT NO: 88] [CFGD REGISTER: PI210d] [Google Scholar]
- Stockmann C, Hillyard B, Ampofo K, Spigarelli MG, Sherwin CM. Levofloxacin inhalation solution for the treatment of chronic Pseudomonasaeruginosa infection among patients with cystic fibrosis. Expert Review of Respiratory Medicine 2015;9(1):13-22. [CFGD REGISTER: PI210c] [DOI] [PubMed] [Google Scholar]
Gulliver 2003 {published data only}PI184
- Gulliver T, Wilson S, Williams G, Harris M, Cooper D. Nebulized tobramycin (intravenous solution) is tolerated without inducing cough and wheeze in cystic fibrosis patients. In: Thoracic Society of Australia & New Zealand Annual Scientific Meeting; 2003 April 4-9; Adelaide, Australia. 2003. [ABSTRACT NO: P139] [CFGD REGISTER: PI184]
Hodson 2002 {published and unpublished data}PI153
- Govan JR. Insights into cystic fibrosis microbiology from the European tobramycin trial in cystic fibrosis. Journal of Cystic Fibrosis 2002;1 Suppl 2:203-8. [CFGD REGISTER: PI153e] [DOI] [PubMed] [Google Scholar]
- Hodson ME, Gallagher CG, Govan JRW, PL TNDS 101 Clinical Trial Group. Randomised UK / Eire clinical trial of the efficacy and safety of tobramycin 300 mg/5 ml nebuliser solution or nebulised colistin in CF patients. Pediatric Pulmonology 2000;Suppl 20:248-9. [CFGD REGISTER: PI153b] [Google Scholar]
- Hodson ME, Gallagher CG, Govan JRW, the PL-TNDS-101 Clinical Trial Group. Randomised UK/Eire clinical trial of the efficacy and safety of tobramycin 300 mg/5 mL nebuliser solution or nebulised colistin. In: 13th International Cystic Fibrosis Congress; 2000 Jun 4-8; Stockholm. 2000:145. [CFGD REGISTER: PI153a]
- Hodson ME, Gallagher CG, Govan JRW. A randomised clinical trial of nebulised tobramycin or colistin in cystic fibrosis. European Respiratory Journal 2002;20(3):658-64. [CFGD REGISTER: PI153c] [DOI] [PubMed] [Google Scholar]
- Hodson ME, Gallagher CG. New clinical evidence from the European tobramycin trial in cystic fibrosis. Journal of Cystic Fibrosis 2002;1 Suppl 2:S199-S202. [CFGD REGISTER: PI153d] [DOI] [PubMed] [Google Scholar]
- Hodson ME. Randomised UK/Eire trial of efficacy and safety of tobramycin 300mg/5ml nebuliser solution or nebulised colistin. European Respiratory Journal 2000;16(Suppl 31):154s. [CFGD REGISTER: PI153f] [Google Scholar]
IRCT2016100930233N1 {published data only}
- IRCT2016100930233N1. Effect of nebulized azithromycin in cystic fibrosis disease. trialsearch.who.int/Trial2.aspx?TrialID=IRCT2016100930233N1 (first received 30 October 2016).
Jenkins 1985 {published data only}PI131
- Jenkins SG, Kelly WC, Mason WG, Peele JD, Cruse MA, Coludro EO, et al. Aerosolized amikacin administration to cystic fibrosis patients chronically infected with Pseudomonas aeruginosa. In: Cystic Fibrosis Club Abstracts; 1985. Vol. 28. 1985:147. [CFGD REGISTER: PI131]
Knowles 1988 {published data only}PI87
- Knowles NE, Hallberg TK, Colombe JL. Efficacy of aerosolized antibiotics combined with intravenous treatment of cystic fibrosis pulmonary exacerbation. Pediatric Pulmonology 1998;Suppl 2(1):120. [CFGD REGISTER: PI87] [Google Scholar]
Konstan 2010a {published data only}PI227
- Konstan MW, Geller DE, Brockhaus F, Zhang J, Angyalosi G. Tobramycin inhalation powder is effective and safe in the treatment of chronic pulmonary Pseudomonas aeruginosa (Pa) infection in patients with cystic fibrosis. American Journal of Respiratory and Critical Care Medicine 2009;179:no pagination. [ABSTRACT NO: A1186] [CFGD REGISTER: PI227a] [Google Scholar]
- Konstan MW, Geller DE, Minic P, Brockhaus F, Zhang J, Angyalosi G. Effective treatment of chronic Pseudomonas aeruginosa (Pa) infection with tobramycin inhalation powder in CF patients. Journal of Cystic Fibrosis 2009;8 Suppl 2:S27. [ABSTRACT NO: 105] [CFGD REGISTER: PI227b] [Google Scholar]
- Konstan MW, Geller DE, Minic P, Brockhaus F, Zhang J, Angyalosi G. Tobramycin inhalation powder for P. aeruginosa infection in cystic fibrosis: The EVOLVE trial. Pediatric Pulmonology 2010;46:230-8. [CFGD REGISTER: PI227e] 5500100000011272 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McColley S, Rietschel E, Brockhaus F, Angyalosi G, Higgins M. Safety of inhaled tobramycin in patients with cystic fibrosis. Pediatric Pulmonology 2011;46 Suppl 34:344. [ABSTRACT NO: 365] [CFGD REGISTER: PI239h // PI227d] 5500100000010634 [Google Scholar]
- NCT00125346. Tobramycin inhalation powder (TIP) in cystic fibrosis subjects (EVOLVE) [A randomized, double-blind, placebo-controlled, multicenter, phase 3 trial to assess the efficacy and safety of tobramycin inhalation powder (TIP) in cystic fibrosis (CF) subjects]. clinicaltrials.gov/ct2/show/NCT00125346 (first received 1 August 2005). [CFGD REGISTER: PI227c]
Ledson 2002 {published data only}PI128
- Ledson MJ, Gallagher MJ, Cowperthwaite C, Robinson M, Convery RP, Walshaw MJ. A randomised double blind placebo controlled crossover trial of nebulised taurolidine in adult CF patients colonised with B cepacia. In: 22nd European CF Conference; 1998 June 13-19; Berlin, Germany. 1998:120. [CFGD REGISTER: PI128a]
- Ledson MJ, Gallagher MJ, Robinson M, Cowperthwaite C, Willets T, Hart CA, et al. A randomized double-blinded placebo-controlled crossover trial of nebulized taurolidine in adult cystic fibrosis patients infected with Burkholderia cepacia. Journal of Aerosol Medicine 2002;15(1):51-7. [CFGD REGISTER: PI128b] [DOI] [PubMed] [Google Scholar]
Lenoir 2007 {published data only}PI196
- Lenoir G, Antypkin YG, Miano A, Moretti P, Zanda M, Varoli G, et al. Efficacy, safety, and local pharmacokinetics of highly concentrated nebulized tobramycin in patients with cystic fibrosis colonized with Pseudomonas aeruginosa. Paediatric Drugs 2007;9 Suppl 1:11-20. [CFGD REGISTER: PI196c] [DOI] [PubMed] [Google Scholar]
- Lenoir G, Aryayev N, Varoli G, Monici Preti P. Aerosolized tobramycin in the treatment of patients with cystic fibrosis and pseudomonas aeruginosa infection. Journal of Cystic Fibrosis 2006;5 Suppl:S42. [CFGD REGISTER: PI196b] [Google Scholar]
- Lenoir G, Aryayev N, Varoli G, Monici Preti P. Highly concentrated aerosolized tobramycin in the treatment of patients with cystic fibrosis and Pseudomonas aeruginosa infection. European Respiratory Journal 2005;26 Suppl 49:620s. [CFGD REGISTER: PI196a] [Google Scholar]
Mainz 2014 {published data only}PI248
- EUCTR2008-000164-17-DE. Nasal inhalation of tobramycin by the pari sinus nebulizer in patients with cystic fibrosis and pseudomonas aeruginosa colonization in the upper airways. - tobra nasal CF pilot [Nasale inhalation von tobramycin mit dem pari sinus-vernebler bei patienten mit mukoviszidose und pseudomonasnachweis IM nasen-nasennebenhohlenbereich]. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2008-000164-17-DE (first received 26 May 2008).
- Mainz JG, Schadlich K, Schien C, Michl R, Schelhorn-Neise P, Koitschev A, et al. Sinonasal inhalation of tobramycin vibrating aerosol in cystic fibrosis patients with upper airway Pseudomonas aeruginosa colonization: results of a randomized, double-blind, placebo-controlled pilot study. Drug Design, Development and Therapy 2014;8:209-17. [CFGD REGISTER: PI248b] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mainz JG, Schien C, Schadlich K, Pfister W, Schelhorn-Neise P, Koitschev A, et al. Sinonasal inhalation of tobramycin in cystic fibrosis patients with P. aeruginosa colonization of the upper airways - results of a multicentric placebo-controlled pilot study. Journal of Cystic Fibrosis 2011;10 Suppl 1:S21. [ABSTRACT NO: 83] [CFGD REGISTER: PI248a] [Google Scholar]
- Mainz JG, Schiller I, Ritschel C, Mentzel HJ, Riethmüller J, Koitschev A, et al. Sinonasal inhalation of dornase alfa in CF: A double-blind placebo-controlled cross-over pilot trial. Auris, Nasus, Larynx 2011;38(2):220-7. [CENTRAL: 781345] [CFGD Register: PI248c / BD131c] [PMID: ] [DOI] [PubMed] [Google Scholar]
- NCT00774072. Nasal inhalation of tobramycin in patients with cystic fibrosis and pseudomonas aeruginosa colonization. clinicaltrials.gov/show/NCT00774072 (first received 17 October 2008). [CFGD REGISTER: PI248c]
Maneshi 2019 {published data only}
- Maneshi A, Modaresi MR, Khalili H, Shojae L, Faghihi T. Nebulized azithromycin versus oral azithromycin as anti-inflammatory therapy in children with cystic fibrosis: a prospective randomized open-label trial. Iranian Journal of Pediatrics 2019;29(6):e96977. [Google Scholar]
Mazurek 2014 {published data only}PI249
- Cicirello H, Mazurek H, Chiron R, Pelikan L, Geidel C, Bolbas K, et al. Efficacy and safety of two inhaled tobramycin solutions in patients with cystic fibrosis and chronic Pseudomonas aeruginosa infection: results from a head to head comparison. American Journal of Respiratory and Critical Care Medicine 2011;183(Meeting Abstracts):A3121. [CENTRAL: 1031434] [CFGD REGISTER: PI249e] [EMBASE: 70850327] [Google Scholar]
- Mazurek H, Chiron R, Kucerova T, Geidel C, Bolbas K, Chuchalin A, et al. Long-term efficacy and safety of aerosolized tobramycin 300 mg/4 ml in cystic fibrosis. Pediatric Pulmonology 2014;49(11):1076-89. [CENTRAL: 1015252] [CFGD REGISTER: PI249d] [JID:: 8510590] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Mazurek H, Chiron R, Pelikan L, Geidel C, Bolbas K, Antipkin Y, et al. Comparison of two inhaled tobramycin solutions in cystic fibrosis patients with chronic pseudomonas aeruginosa infection: results in different age subgroups. Journal of Cystic Fibrosis 2011;10 Suppl 1:S28. [ABSTRACT NO: 111] [CFGD REGISTER: PI249b] 5500100000010714 [Google Scholar]
- Mazurek H, Chiron R, Varoli G, Santoro D, Cicirello H, Antipkin Y. Efficacy on lung function and safety of multiple courses of tobramycin 300mg/4 ml nebuliser solution (Bramitob) in patients with cystic fibrosis and chronic Pseudomonas aeruginosa infection: results from a 48-week extension phase. Journal of Cystic Fibrosis 2012;11 Suppl 1:S74. [ABSTRACT NO: 69] [CFGD REGISTER: PI249c] 5500100000011290 [Google Scholar]
- Mazurek H, Chiron R, Varoli G, Santoro D, Cicirello H, Antipkin Y. Long-term efficacy and safety of tobramycin 300mg/4mL nebuliser solution in patients with cystic fibrosis and chronic Pseudomonas aeruginosa infection. European Respiratory Journal 2012;40(Suppl 56):606s. [CFGD: PI249f] [Google Scholar]
- Mazurek H, Lenoir G, Pelikan L, Geidel C, Bolbas K, Antipkin Y, et al. Head-to-head comparison of two inhaled tobramycin solutions in cystic fibrosis (CF) patients with chronic pseudomonas aeruginosa (Pa) infection. Journal of Cystic Fibrosis 2011;10 Suppl 1:S28. [ABSTRACT NO: 110] [CFGD REGISTER: PI249a] 5500100000010713 [Google Scholar]
- NCT00885365. A study comparing the efficacy and tolerability of tobrineb®/actitob®/bramitob® versus TOBI®. clinicaltrials.gov/show/NCT00885365 (first received 21 April 2009). [CFGD REGISTER: PI249g]
McCoy 2008 {published data only}PI212
- McCoy K, Retsch-Bogart G, Gibson RL, Oermann C, Braff M, Montgomery AB. Investigation of susceptibility breakpoints for inhaled antibiotic therapies in cystic fibrosis. Pediatric Pulmonology 2010;45 Suppl 33:341. [ABSTRACT NO: 340] [CFGD REGISTER: PI212g/PI213i] 5500100000010623 [Google Scholar]
- McCoy K, Retsch-Bogart G, Oermann C, Gibson R, Montgomery AB. Aztreonam lysine for inhalation (AZLI) for CF patients with P. aeruginosa (PA) infection. Journal of Cystic Fibrosis 2007;6 Suppl 1:S10. [CFGD REGISTER: PI212a] [Google Scholar]
- McCoy KS, Quittner AL, Oermann CM, Gibson RL, Retsch-Bogart GZ, Montgomery AB. Inhaled aztreonam lysine for chronic airway Pseudomonas aeruginosa in cystic fibrosis. American Journal of Respiratory and Critical Care Medicine 2008;178(9):921-8, Online data supplement. [CFGD REGISTER: PI212d] [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCoy KS, Quittner AL, Oermann CM, Gibson RL, Retsch-Bogart GZ, Montgomery AB. Inhaled aztreonam lysine for chronic airway Pseudomonas aeruginosa in cystic fibrosis. American Journal of Respiratory Critical Care Medicine 2008;178(9):921-8. [CFGD REGISTER: PI212c] [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCoy KS, Retsch-Boagrt GZ, Gibson RL, Oermann CM, McKevitt M, Montgomery AB. Efficacy of aztreonam lysine for inhalation (AZLI) in patients with cystic fibrosis and drug resistant P. aeruginosa (DRPA). Journal of Cystic Fibrosis 2009;8 Suppl 2:S28. [ABSTRACT NO: 108] [CFGD REGISTER: PI212e // PI 213e] [Google Scholar]
- McCoy KS, Retsch-Bogart GZ, Gibson R, Oermann C, Braff MH, Montgomery AB. Relevance of established susceptibility breakpoints to clinical efficacy of inhaled antibiotic therapies in cystic fibrosis. Pediatric Pulmonology 2008;43 Suppl 31:351. [ABSTRACT NO: 418] [CFGD REGISTER: PI212b // PI213c] [Google Scholar]
- NCT00104520. Safety and efficacy study of aztreonam for inhalation solution (AZLI) in cystic fibrosis patients with P. Aeruginosa. clinicaltrials.gov/show/NCT00104520 (first received 2 March 2005). [CFGD REGISTER: PI212i]
- Nichols DP, Happoldt CL, Bratcher PE, Caceres SM, Chmiel JF, Malcolm KC, et al. Impact of azithromycin on the clinical and antimicrobial effectiveness of tobramycin in the treatment of cystic fibrosis. Journal of Cystic Fibrosis 2017;16(3):358-66. [CFGD REGISTER: PI212h] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plosker GL. Aztreonam lysine for inhalation solution in cystic fibrosis. Drugs 2010;70(14):1843-55. [CFGD REGISTER: PI212f] [DOI] [PubMed] [Google Scholar]
Mullinger 2005 {published data only}
- Mullinger B, Brand P, Fischer A, Haubermann S, Scheuch G, Seitz J, et al. Intra-pulmonal deposition of two different tobramycin formulations. Journal of Cystic Fibrosis 2005;4 Suppl 1:S53. [Google Scholar]
Nasr 2006 {published data only}DG2
- Nasr SZ, Gordon D, Sakmar E, Eckhardt BP, Strouse PJ. Comparison of high resolution computerized tomography (HRCT) of the chest and pulmonary function testing in evaluating the effect of tobramycin solution for inhalation in cystic fibrosis (CF) patients. European Respiratory Journal 2004;24 Suppl 48:P2403. [CFGD REGISTER: DG2a] [Google Scholar]
- Nasr SZ, Gordon D, Sakmar E, Yu X, Christodoulou E, Eckhardt BP, et al. High resolution computerized tomography of the chest and pulmonary function testing in evaluating the effect of tobramycin solution for inhalation in cystic fibrosis patients. Pediatric Pulmonology 2006;41(12):1129-37. [CFGD REGISTER: DG2c] [DOI] [PubMed] [Google Scholar]
- Nasr SZ, Gordon D, Yu X, Sakmar E, Eckhardt BP, Strause P. Comparison of high resolution computerized tomography (HRCT) of the chest and pulmonary function testing in evaluating of the effect of tobramycin solution for inhalation (TSI) in cystic fibrosis (CF) subjects with mild lung disease. Pediatric Pulmonology 2004;38 Suppl 27:299. [CFGD REGISTER: DG2b] [Google Scholar]
- Nasr SZ, Sakmar E, Christodoulou E, Eckhardt BP, Streetman DS, Strouse PJ. The use of high resolution computerized tomography (HRCT) of the chest in evaluating the effect of tobramycin solution for inhalation in cystic fibrosis lung disease. Pediatric Pulmonology 2010;45(5):440-9. [CFGD REGISTER: DG2e] [DOI] [PubMed] [Google Scholar]
- Nasr SZ, Sakmar E, Eckhardt BP, Strouse PJ. High resolution computerized tomography (HRCT) of the chest vs. pulmonary function testing utility in evaluating the effect of tobramycin solution for inhalation in cystic fibrosis. Pediatric Pulmonology 2008;43 Suppl 31:366. [CFGD REGISTER: DG2d] [Google Scholar]
NCT00411736 {published data only}
- EUCTR2006-003275-12-DK. Scandinavian Cystic Fibrosis Azithromycin Study Supplementary oral azithromycin in treatment of intermittent Pseudomonas aeruginosa colonization in CF-patients with inhaled colistin and oral ciprofloxacin; postponing next isolate of pseudomonas and prevention of chronic infection. A prospective, double-blinded, placebo-controlled scandinavian multi-centre study. A investigator initiated study - Scandinavian Cystic Fibrosis Azithromycin Study. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2006-003275-12-DK (first received 17 April 2007).
- NCT00411736. Scandinavian cystic fibrosis azithromycin study. clinicaltrials.gov/show/NCT00411736 (first received 15 December 2006).
NCT00420836 {published data only}
- NCT00420836. Tobramycin administered by eFlow rapid nebulizer: pharmacokinetic study. clinicaltrials.gov/show/NCT00420836 (first received 11 January 2007). [CFGD REGISTER: DT66]
NCT00503490 {published data only}
- NCT00503490. Safety, pharmacokinetic and pharmacodynamic study of MP-376 in patients with cystic fibrosis. clinicaltrials.gov/show/NCT00503490 (first received 18 July 2007).
NCT01315691 {published data only}
- NCT01315691. Study to evaluate arikaceTM in CF patients with chronic infection due to Pseudomonas aeruginosa. clinicaltrials.gov/show/NCT01315691 (first received 15 March 2011).
NCT02015663 {published data only}
- EUCTR2016-004318-82-Outside-EU/EEA. A study comparing tobramycin inhalation powder (TIP) administered once daily continuously versus TIP administered BID in 28 day on / 28 day off cycles for the treatment of pulmonary pseudomonas aeruginosa in patients with cystic fibrosis. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2016-004318-82-Outside-EU/EEA (first received 15 May 2017).
- NCT02015663. Tobramycin inhalation powder (TIP) administered once daily continuously versus TIP administered BID in 28 day on / 28 day off cycles. clinicaltrials.gov/show/NCT02015663 (first received 19 December 2013).
NCT02677701 {published data only}
- NCT02677701. Testing the effect of adding chronic oral azithromycin to inhaled tobramycin in people with cystic fibrosis (CF). clinicaltrials.gov/show/NCT02677701 (first received 9 February 2016). [CFGD REGISTER: PI323a]
- Nichols DP, Singh PK, Baines A, Caverly LJ, Chmiel JF, Gibson RL, et al. Testing the effects of combining azithromycin with inhaled tobramycin for P. aeruginosa in cystic fibrosis: a randomised, controlled clinical trial. Thorax 2022;77(6):581-8. [CFGD: PI323a] [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT02730793 {published data only}
- NCT02730793. Aztreonam aerosol to treat cystic fibrosis nasal disease. clinicaltrials.gov/show/NCT02730793 (first received 6 April 2015).
NCT02894684 {published data only}
- NCT02894684. Aztreonam for inhalation solution (AZLI) for the treatment of exacerbations of cystic fibrosis. clinicaltrials.gov/show/NCT02894684 (first received 9 September 2016). [CFGD REGISTER: PI310d]
Nichols 2020 {published data only}
- Nichols DP, Baines A, Chmiel JF, Nick JA, Saiman L, Singh P, et al. Teach: testing the effects of adding chronic azithromycin to inhaled tobramycin; a randomized, controlled, clinical trial. Pediatric Pulmonology 2020;55 Suppl 2:150. [CFGD REGISTER: PI323b] [Google Scholar]
Nikolaizik 1996 {published data only}PI144
- Nikolaizik WH, Jenni JV, Schoni MH. Bronchial constriction after nebulized tobramycin preparations and saline in patients with cystic fibrosis. European Journal of Pediatrics 1996;155:608-11. [CFGD REGISTER: PI144] [DOI] [PubMed] [Google Scholar]
Noah 2007 {published data only}PI205
- Noah T, Ivins S, Abode K, Harris W, Henry M, Leigh M. Comparison of antibiotics for early pseudomonas infection in CF: interim data analysis. Pediatric Pulmonology 2007;42 Suppl 30:332. [CFGD REGISTER: PI205a] [Google Scholar]
- Noah TL, Ivins SS, Abode KA, Stewart PW, Michelson PH, Harris WT, et al. Inhaled versus systemic antibiotics and airway inflammation in children with cystic fibrosis and Pseudomonas. Pediatric Pulmonology 2010;45(3):281-90. [CFGD REGISTER: PI205b] [DOI] [PubMed] [Google Scholar]
Nolan 1982 {published data only}
- Nolan G, McIvor P, Levison H, Fleming PC, Corey M, Gold R. Antibiotic prophylaxis in cystic fibrosis: inhaled cephaloridine as an adjunct to oral cloxacillin. Journal of Pediatrics 1982;101(4):626-30. [DOI] [PubMed] [Google Scholar]
NTR5211 {published data only}
- NTR5211. TAPAS study in patients with CF. trialsearch.who.int/Trial2.aspx?TrialID=NTR5211 (first received 4 May 2015).
Oermann 2009 {published data only}
- Oermann CM, McCoy KS, Retsch-Bogart GZ, Gibson R, McKevitt M, Montgomery B. Antibiotic susceptibility in Pseudomonas aeruginosa (PA) isolates following repeated exposure to aztreonam for inhalation solution (AZLI) in patients with cystic fibrosis. Pediatric Pulmonology 2009;44 Suppl 32:309. [ABSTRACT NO: 278] [Google Scholar]
- Oermann CM, McCoy KS, Retsch-Bogart GZ, Gibson R, McKevitt M, Montgomery B. Effect of repeated exposure to aztreonam for inhalation solution (AZLI) therapy on cystic fibrosis respiratory pathogens. Pediatric Pulmonology 2009;44 Suppl 32:335. [ABSTRACT NO: 353] [Google Scholar]
- Oermann CM, McCoy KS, Retsch-Bogart GZ, Gibson RL, Montgomery AB. Effect of multiple courses of aztreonam lysine for inhalation (AZLI) on FEV1 and weight in patients with cystic fibrosis (CF) and Pseudomonas aeruginosa (PA): analysis of 18 month data from CP-AI-006. Journal of Cystic Fibrosis 2009;8 Suppl 2:S28. [ABSTRACT NO: 107] [Google Scholar]
- Oermann CM, McCoy KS, Retsch-Bogart GZ, Gibson RL, Quittner AL, Montgomery AB. Adherence over multiple courses of Aztreonam for inhalation (AZLI): effect on disease-related end points in patients with cystic fibrosis (CF) and Pseudomonas aeruginosa (PA). Journal of Cystic Fibrosis 2009;8 Suppl 2:S28. [ABSTRACT NO: 109] [Google Scholar]
Poli 2005 {published data only}PI195
- Poli G, Acerbi D, Pennini R, Soliani Raschini A, Bianco F, et al. Clinical pharmacology study of a new tobramycin solution for nebulisation. Journal of Cystic Fibrosis 2006;5 Suppl:S43. [CFGD REGISTER: PI195b] [Google Scholar]
- Poli G, Acerbi D, Pennini R, Soliani Raschini A, Corrado M, Eichler HG, et al. Clinical pharmacology study of a new tobramycin solution for nebulisation. European Respiratory Journal 2005;26 Suppl 49:729s. [CFGD REGISTER: PI195a] [DOI] [PubMed] [Google Scholar]
- Poli G, Acerbi D, Pennini R, Soliani Raschini A, Corrado ME, Eichler HG, et al. Clinical pharmacology study of Bramitob, a tobramycin solution for nebulization, in comparison with Tobi. Paediatric Drugs 2007;9 Suppl 1:3-9. [CFGD REGISTER: PI195c] [DOI] [PubMed] [Google Scholar]
Pradal 2002 {published data only}BD145
- Pradal U, Casotti V, Delmarco A, Nicolis E, Livraghi A, Conese M, et al. Effects of gentamicin on ion transport, MRNA and protein CFTR expression in patients with R1162X: a double blind placebo controlled study. Pediatric Pulmonology 2002;Suppl 24:263. [CFGD REGISTER: BD145] [Google Scholar]
Proesmans 2016 {published data only}PI208
- Proesmans M, Boulanger L, Vermeulen F, De Boeck K. Eradication of recent pseudomonas aeruginosa infection: TOBI versus Colistineb®/ ciprofloxacin. Journal of Cystic Fibrosis 2011;10 Suppl 1:S26. [ABSTRACT NO: 102] [CFGD REGISTER: PI208c] [DOI] [PubMed] [Google Scholar]
- Proesmans M, Boulanger L, Vermeulen F, De Boeck K. Eradication of recent Pseudomonas aeruginosa isolation: TOBI versus colistin/ ciprofloxacin. Journal of Cystic Fibrosis 2008;7 Suppl 2:S64. [CFGD REGISTER: PI208a] [Google Scholar]
- Proesmans M, Boulanger L, Vermeulen F, De Boeck K. Eradication of recent Pseudomonas aeruginosa isolation: TOBI versus colistin/ciprofloxacin. Pediatric Pulmonology 2009;44 Suppl 32:321. [ABSTRACT NO: 311] [CFGD REGISTER: PI208b] [Google Scholar]
- Proesmans M, Vermeulen F, Boulanger L, Verhaegen J, De Boeck K. Comparison of two treatment regimens for eradication of pseudomonas aeruginosa infection in children with cystic fibrosis. Journal of Cystic Fibrosis 2016;12(1):29-34. [CFGD REGISTER: PI208d] [DOI] [PubMed] [Google Scholar]
Ramsey 1993 {published data only}PI75
- Fiel SB. Aerosol delivery of antibiotics to the lower airways of patients with cystic fibrosis. Chest 1995;107 Suppl 2:61S-4S. [CFGD REGISTER: PI75b] [DOI] [PubMed] [Google Scholar]
- Ramsey BW, Dorkin HL, Eisenberg JD, Gibson RL, Harwood IR, Kravitz RM, et al. Efficacy of aerosolized tobramycin in patients with cystic fibrosis. New England Journal of Medicine 1993;328(24):1740-6. [CFGD REGISTER: PI75a] [DOI] [PubMed] [Google Scholar]
Ramsey 2005 {published data only}PI202
- Anstead M, Heltshe SL, Khan U, Barbieri JT, Langkamp M, Doring G, et al. Pseudomonas aeruginosa serology and risk for re-isolation in the EPIC trial. Journal of Cystic Fibrosis 2013;12(2):147-53. [CENTRAL: 1089772] [CFGD REGISTER: PI202m] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anstead M, Lymp J, Khan U, Barbieri J, Langkamp M, Doring G, et al. Pseudomonas aeruginosa serology predicts response to treatment and re-infection in the EPIC clinical study. Pediatric Pulmonology 2001;46 Suppl 34:303. [ABSTRACT NO: 254] [CFGD REGISTER: PI202g] [Google Scholar]
- Anstead M, Saiman L, Mayer-Hamblett N, Lands LC, Kloster M, Goss CH, et al. Pulmonary exacerbations in CF patients with early lung disease. Journal of Cystic Fibrosis 2014;13(1):74-9. [CENTRAL: 961723] [CFGD REGISTER: PI202l] [EMBASE: 2013796396] [DOI] [PubMed] [Google Scholar]
- Hamblett NM, Retsch-Bogart GZ, Treggiari M, Kronmal RA, Khan U, Williams J, et al. Safety and efficacy of anti-pseudomonal therapy for early eradication of Pseudomonas aeruginosa: the EPIC study. Pediatric Pulmonology 2009;44 Suppl 32:183. [PI202b] [Google Scholar]
- Hoffman LR, Ramsey BW, Kulasekara HD, Retsch-Bogart GZ, Wolter DJ, Pope CE, et al. Pseudomonas aeruginosa (PA) phenotypes associated with persistent early infection in CF patients in the EPIC clinical trial. Pediatric Pulmonology 2012;47 Suppl 35:317. [ABSTRACT NO: 266] [CFGD REGISTER: PI202j] [Google Scholar]
- Jorth P, Hisert KB, Garudathri J, Wolter D, Hoffman L, Singh P. Studies on the effects of ciprofloxacin on pseudomonas aeruginosa evolution in cystic fibrosis patients. Pediatric Pulmonology 2014;49:349. [CENTRAL: 1057036] [CFGD REGISTER: PI202n] [EMBASE: 71616423] [Google Scholar]
- Jorth P, Rezayat A, Hisert KB, Garudathri J, Khan U, Hamblett NM, et al. Early evolution of pseudomonas aeruginosa during cystic fibrosis infection. Pediatric Pulmonology 2015;50 Suppl 41:304. [ABSTRACT NO: 300] [CENTRAL: 1092204] [CFGD REGISTER: PI202p] [Google Scholar]
- Khan U, Mayer-Hamblett N, Retsch-Bogart G, Treggiari M, Ramsey B. Association between baseline pseudomonas aeruginosa positivity in EPIC clinical trial participants & prior antibiotic exposure. Pediatric Pulmonology 2010;45 Suppl 33:335. [ABSTRACT NO: 326] [CFGD REGISTER: PI202f] [Google Scholar]
- Mayer-Hamblett N, Kloster M, Rosenfeld M, Gibson RL, Retsch-Bogart GZ, Emerson J, et al. Impact of sustained eradication of new pseudomonas aeruginosa Infection on long-term outcomes in cystic fibrosis. Clinical Infectious Diseases 2015;61(5):707-15. [CENTRAL: 1099084] [CFGD REGISTER: PI202o] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayer-Hamblett N, Kronmal RA, Gibson RL, Rosenfeld M, Retsch-Bogart G, Treggiari MM, et al. Initial Pseudomonas aeruginosa treatment failure is associated with exacerbations in cystic fibrosis. Pediatric Pulmonology 2012;47(2):125-34. [CFGD REGISTER: PI202i] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayer-Hamblett N, Rosenfeld M, Treggiari MM, Konstan MW, Retsch-Bogart G, Morgan W, et al. Standard care versus protocol based therapy for new onset Pseudomonas aeruginosa in cystic fibrosis. Pediatric Pulmonology 2013;48(10):943-53. [CENTRAL: 916577] [CFGD REGISTER: PI202k] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ramsey B. TOBI use in infants and children with early Pseudomonas aeruginosa infection - duration of effect and epic update. Pediatric Pulmonology 2005;40 Suppl 28:146. [CFGD REGISTER: PI202a] [Google Scholar]
- Treggiari M, Retsch-Bogart G, Mayer-Hamblett N, Khan U, Kronmal R, Ramsey B, et al. Comparative efficacy and safety of four randomized regimens to treat early Pseudomonas aeruginosa infection in children with cystic fibrosis. Journal of Cystic Fibrosis 2010;9 Suppl 1:S54. [ABSTRACT NO: 209] [CFGD REGISTER: PI202e] [Google Scholar]
- Treggiari M, Retsch-Bogart GZ, Mayer-Hamblett N, Kronmal R, Khan U, Williams J, et al. Early anti-pseudomonal infection in children with CF: study population and conduct of the "EPIC" clinical trial. Pediatric Pulmonology 2009;44 Suppl 32:316. [ABSTRACT NO: 299] [CFGD REGISTER: PI202c] [Google Scholar]
- Treggiari MM, Retsch-Bogart G, Mayer-Hamblett N, Khan U, Kulich M, Kronmal R, et al. Comparative efficacy and safety of 4 randomized regimens to treat early Pseudomonas aeruginosa infection in children with cystic fibrosis. Archives of Pediatric & Adolescent Medicine 2011;165(9):847-56. [CFGD REGISTER: PI202h] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Treggiari MM, Rosenfeld M, Mayer-Hamblett N, Retsch-Bogart G, Gibson RL, Williams J, et al. Early anti-pseudomonal acquisition in young patients with cystic fibrosis: rationale and design of the EPIC clinical trial and observational study. Contempory Clinical Trials 2009;30(3):256-68. [CFGD REGISTER: PI202d] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ramsey 2017 {published data only}
- Magaret AS, Salerno J, Deen JF, Kloster M, Mayer-Hamblett N, Ramsey BW, et al. Long-term azithromycin use is not associated with QT prolongation in children with cystic fibrosis. Journal of Cystic Fibrosis 2021;20(2):e16-8. [CFGD Register: MA31f] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayer-Hamblett N, Retsch-Bogart G, Kloster M, Accurso F, Rosenfeld M, Albers G, et al. Azithromycin for early Pseudomonas infection in cystic fibrosis. The OPTIMIZE randomized trial. American Journal of Respiratory and Critical Care Medicine 2018;198(9):1177-87. [CFGD Register: MA31b] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayer-Hamblett N, Retsch-Bogart G, Kloster M, Accurso F, Rosenfeld M, Albers G, et al. Erratum: azithromycin for early Pseudomonas infection in cystic fibrosis. The OPTIMIZE randomized trial. American Journal of Respiratory and Critical Care Medicine 2019;199(6):809. [CFGD REGISTER: MA31d] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02054156. Optimizing treatment for early pseudomonas aeruginosa infection in cystic fibrosis. clinicaltrials.gov/show/NCT02054156 (first received 4 February 2014). [CFGD REGISTER: MA31c]
- Pittman JE, Skalland MS, Sagel SD, Ramsey BW, Mayer-Hamblett N, Retsch-Bogart GZ. Impact of azithromycin on serum inflammatory markers in children with cystic fibrosis and new Pseudomonas. Journal of Cystic Fibrosis 2022 Mar 5 [Epub ahead of print]. [CFGD REGISTER: MA31g] [DOI: 10.1016/j.jcf.2022.02.015] [DOI] [PMC free article] [PubMed]
- Ramsey BW, Retsch-Bogart GZ, Kloster M, Buckingham R, Hamblett NM. Efficacy and safety of azithromycin for treatment of early pseudomonas in cystic fibrosis: the optimize trial. Pediatric Pulmonology 2017;52(Suppl 47):380-1. [CFGD REGISTER: MA31a] [Google Scholar]
Ratjen 2010 {published data only}PI197
- Ratjen F, Munck A, Campello V. Inhaled tobramycin nebuliser solution for treatment of early Pseudomonas aeruginosa infection: first results from the Elite study. Pediatric Pulmonology 2006;41 Suppl 29:318. [CFGD REGISTER: PI197b] [Google Scholar]
- Ratjen F, Munck A, Campello V. Safety of inhaled tobramycin nebuliser solution for treatment of early pseudomonas aeruginosa infection: first results from the ELITE study. Journal of Cystic Fibrosis 2006;5 Suppl:S22. [CFGD REGISTER: PI197a] [Google Scholar]
- Ratjen F, Munck A, Kho P, Angyalosi G. Treatment of early Pseudomonas aeruginosa infection in patients with cystic fibrosis: the ELITE trial. Thorax 2010;65(4):286-91. [CFGD REGISTER: PI197e] [DOI] [PubMed] [Google Scholar]
- Ratjen F, Munck A, Kho P. Short and long-term efficacy of inhaled tobramycin in early P. aeruginosa infection: the ELITE study. Pediatric Pulmonology 2008;43 Suppl 31:319. [CFGD REGISTER: PI197d] [Google Scholar]
- Ratjen F, Stenglein S, Munck A. Inhaled tobramycin nebulizer solution for treatment of early Pseudomonas aeruginosa infection; the ELITE study. Journal of Cystic Fibrosis 2008;7 Suppl 2:S26. [CFGD REGISTER: PI197c] [Google Scholar]
Retsch‐Bogart 2007 {published data only}PI213
- McCoy K, Retsch-Bogart G, Gibson RL, Oermann C, Braff M, Montgomery AB. Investigation of susceptibility breakpoints for inhaled antibiotic therapies in cystic fibrosis. Pediatric Pulmonology 2010;45 Suppl 33:341. [ABSTRACT NO: 340] [CFGD REGISTER: PI212g/PI213i] 5500100000010623 [Google Scholar]
- McCoy KS, Retsch-Boagrt GZ, Gibson RL, Oermann CM, McKevitt M, Montgomery AB. Efficacy of aztreonam lysine for inhalation (AZLI) in patients with cystic fibrosis and drug resistant P. aeruginosa (DRPA). Journal of Cystic Fibrosis 2009;8 Suppl 2:S28. [ABSTRACT NO: 108] [CFGD REGISTER: PI213e // PI212e] [Google Scholar]
- McCoy KS, Retsch-Bogart GZ, Gibson R, Oermann C, Braff MH, Montgomery AB. Relevance of established susceptibility breakpoints to clinical efficacy of inhaled antibiotic therapies in cystic fibrosis. Pediatric Pulmonology 2008;43 Suppl 31:351. [ABSTRACT NO: 418] [CFGD REGISTER: PI212b // PI213c] [Google Scholar]
- NCT00112359. International safety and efficacy study of aztreonam for inhalation solution (AZLI) in cystic fibrosis patients with P. Aeruginosa. clinicaltrials.gov/show/NCT00112359 (first received 2 June 2005). [CFGD REGISTER: PI213k]
- Plosker GL. Aztreonam lysine for inhalation solution in cystic fibrosis. Drugs 2010;70(14):1843-55. [CFGD REGISTER: PI213h] [DOI] [PubMed] [Google Scholar]
- Quitnner AL, Henig NR, Lewis S, Derchak PA, McCoy KS, Oermann CM, et al. Effects of chronic intermittent aztreonam for inhalation solution (AZLI) on health-related quality of life (HRQOL) in persons with cystic fibrosis (CF) and P. aeruginosa. Pediatric Pulmonology 2011;46 Suppl 34:299. [ABSTRACT NO: 240] [CFGD REGISTER: PI213j] 5500100000011261 [Google Scholar]
- Quittner AL, Retsch-Bogart GZ, McCoy KS, Oermann CM, Gibson R, Lewis S. Effect of a 28-day course of aztreonam for inhalation solution (AZLI) on responses to individual CFQ-R respiratory symptoms score questions among patients with CF. Pediatric Pulmonology 2009;44 Suppl 32:305. [ABSTRACT NO: 266] [CFGD REGISTER: PI213f] [Google Scholar]
- Retsch-Bogart GZ, McCoy KS, Gibson RL, Oermann C, Montgomery AB. Source of improvements in lung function in patients with cystic fibrosis (CF) following treatment with aztreonam lysine for inhalation (AZLI). Pediatric Pulmonology 2008;42 Suppl 30:320. [ABSTRACT NO: 336] [CFGD REGISTER: PI213d] [Google Scholar]
- Retsch-Bogart GZ, McCoy KS, Gibson RL, Oermann CM, Braff MH, Montgomery AB. Sustained improvement in pulmonary function following a 28-day course of 75 MG AZLI TID therapy. Pediatric Pulmonology 2008;43 Suppl 31:320. [ABSTRACT NO: 335] [CFGD REGISTER: PI213b] [Google Scholar]
- Retsch-Bogart GZ, Montgomery B, Gibson R, McCoy K, Oermann CM, Cooper P. Phase 3 trial (AIR-CF 1) measuring improvement in respiratory symptoms in patients with cystic fibrosis (CF) following treatment with aztreonam lysine for inhalation. Pediatric Pulmonology 2007;42 Suppl 30:310. [ABSTRACT NO: 308] [CFGD REGISTER: PI213a] [Google Scholar]
- Retsch-Bogart GZ, Quittner AL, Gibson RL, Oermann CM, McCoy KS, Montgomery AB, et al. Efficacy and safety of inhaled aztreonam lysing for airway pseudomonas in cystic fibrosis. Chest 2009;135(5):1223-32. [CFGD REGISTER: PI213g] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wainwright CE, Quittner AL, Geller DE, Nakamura C, Wooldridge JL, Gibson RL, et al. Aztreonam for inhalation solution (AZLI) in patients with cystic fibrosis, mild lung impairment, and P. aeruginosa. Journal of Cystic Fibrosis 2011;10(4):234-42. [CFGD REGISTER: PI213k] 5500100000011273 [DOI] [PubMed] [Google Scholar]
Retsch‐Bogart 2008 {published data only}PI211
- Burns JL, Stapp J, Lofland D, AI Phase 2 Study Group. Microbiology results from a phase 2 clinical study of aztreonam lysinate for inhalation (AI): a new inhaled antibiotic to treat CF patients with Pseudomonas aeruginosa (PA). Journal of Cystic Fibrosis 2005;4 Suppl:S55. [CFGD REGISTER: PI211a] [Google Scholar]
- Retsch-Bogart GZ, Burns JL, Otto KL, Liou TG, McCoy K, Oermann C, et al. A phase 2 study of aztreonam lysine for inhalation to treat patients with cystic fibrosis and Pseudomonas aeruginosa infection. Pediatric Pulmonology 2008;43(1):47-58. [CFGD REGISTER: PI211c] [DOI] [PubMed] [Google Scholar]
- Retsch-Bogart GZ, Gibson RL, AI Phase 2 Study Group. A phase 2 study of aztreonam lysinate for inhalation to treat cystic fibrosis patients with Pseudomonas aeruginosa infection. In: American Thoracic Society International Conference; 2005 May 20-25; San Diego, USA. 2005:A576. [CFGD REGISTER: PI211b]
- Retsch-Bogart GZ, McCoy KS, Gibson RL, Oermann CM, Braff MH, Montgomery AB. Sustained improvement in pulmonary function following a 28-day course of 75 MG AZLI TID therapy. Pediatric Pulmonology 2008;43 Suppl 31:320. [CFGD REGISTER: PI211d] [Google Scholar]
Rietschel 2009 {published data only}PI232
- Rietschel E, Posselt HG, Heuer HE, Merkel N, Staab D. Pharmacokinetics of tobramycin (TOBI™) after 4 and 8 weeks of continuous once daily or twice daily inhalation. Journal of Cystic Fibrosis 2009;8 Suppl 2:S27. [ABSTRACT NO: 106] [CFGD REGISTER: PI232a] [Google Scholar]
- Rietschel E, Staab D, Merkel N, Konigsbruggen S, Posselt H. Pharmacokinetics of continuous treatment with o.d. or b.i.d inhalation of tobramycin (TOBI™) via Pari EFlow™ Rapid. Pediatric Pulmonology 2010;45 Suppl 33:320. [ABSTRACT NO: 283] [CFGD REGISTER: PI232c] [Google Scholar]
- Rietschel E, Staab D, Konigsbruggen S, Merkel N, Heuer HE, Posselt HG. Pharmacokinetics of continuous treatment with o.d. or b.i.d. inhalation of tobramycin (TOBI™). Journal of Cystic Fibrosis 2010;9 Suppl 1:S23. [ABSTRACT NO: 85] [CFGD REGISTER: PI232b] [Google Scholar]
- Koningsbruggen-Rietschel S, Heuer HE, Merkel N, Posselt HG, Staab D, Sieder C, et al. Pharmacokinetics and safety of an 8 week continuous treatment with once-daily versus twice-daily inhalation of tobramycin in cystic fibrosis patients. Journal of Antimicrobial Chemotherapy 2016;71(3):711-7. [CENTRAL: 1199846] [CFGD REGISTER: PI232d] [PMID: ] [DOI] [PubMed] [Google Scholar]
Rosenfeld 2006 {published data only}PI203
- Rosenfeld M, Emerson J, Uh D, Anderson G, Genatossio A, McNamara S, et al. Does tobramycin accumulate in respiratory secretions with repeated aerosol administration: a pilot study. Pediatric Pulmonology 2006;41 Suppl 29:327. [CFGD REGISTER: PI203] [Google Scholar]
Ruddy 2013 {published data only}PI277
- Ruddy J, Emerson J, Moss R, Genatossio A, McNamara S, Burns JL, et al. Sputum tobramycin concentrations in cystic fibrosis patients with repeated administration of inhaled tobramycin. Journal of Aerosol Medicine and Pulmonary Drug Delivery 2013;26(2):69-75. [CFGD REGISTER: PI277] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sands 2014 {published data only}PI263
- Sands D, Sapiejka E, Gaszczyk G, Mazurek H, for the T100 Study Group. Comparison of two tobramycin nebuliser solutions: pharmacokinetic, efficacy and safety profiles of T100 and TNS. Journal of Cystic Fibrosis 2014;13:653-60. [CFGD REGISTER: PI263c] [DOI] [PubMed] [Google Scholar]
- Sands D, Sapiejka E, Mazurek H, Gaszczyk G. A randomised comparison of two tobramycin formulations in cystic fibrosis (CF) patients with chronic pseudomonas aeruginosa (PA) infection for pharmacokinetic and therapeutic equivalence. European Respiratory Journal 2013;42:423s. [CFGD REGISTER: PI263e] [Google Scholar]
- Sands D, Sapiejka E, Mazurek H, Gaszczyk G. A randomised comparison of VANTOBRA and TOBI in cystic fibrosis patients with chronic pseudomonas aeruginosa infection for pharmacokinetic and therapeutic equivalence. Journal of Cystic Fibrosis 2013;12 Suppl 1:S66. [ABSTRACT NO: 69] [CFGD REGISTER: PI263a] 5500100000011293 [Google Scholar]
- Sands D, Sapiejka E, Mazurek H, Gaszczyk G. Use of an electronic monitoring system to generate objective information on patients' adherence to taking treatments of a novel inhaled tobramycin solution. European Respiratory Journal 2013;42 Suppl 57:P1188. [ABSTRACT NO: 1497] [CENTRAL: 1099909] [CFGD REGISTER: PI263d] [EMBASE: 71843058] [Google Scholar]
- Sands D, Sapiejka E, Mazurek H, Gaszczyk G. Use of an electronic monitoring system to generate objective information on patients' adherence to taking treatments of a novel tobramycin solution (VANTOBRA). Journal of Cystic Fibrosis 2013;12 Suppl 1:S66. [ABSTRACT NO: 70] [CFGD REGISTER: PI263b] 5500100000011292 [Google Scholar]
Schaad 1987 {published data only}PI56
- Schaad UB, Wedgwood-Krucko J, Suter S, Kraemer R. Efficacy of inhaled amikacin as adjunct to intravenous combination therapy (ceftazidime and amikacin) in cystic fibrosis. Journal of Pediatrics 1987;111(4):599-605. [CFGD REGISTER: PI56] [DOI] [PubMed] [Google Scholar]
Schaad 1997 {published data only}PI116
- Schaad UB, Wedgwood J, Reuderberg A, Kraemer R, Hampel B. Ciprofloxacin as antipseudomonal treatment in patients with cystic fibrosis. Pediatric Infectious Disease Journal 1997;16(1):106-11. [CFGD REGISTER: PI116] [CFGD REGISTER: PI116] 5500100000000804 [DOI] [PubMed] [Google Scholar]
Shatunov 2001 {published data only}PI164
- Shatunov SM. Comparative efficacy of different methods of ceftazidime administration in children with cystic fibrosis. In: 11th European Respiratory Society Annual Congress; 2001 Sept 22-26; Berlin. 2001:860. [CFGD REGISTER: PI164]
Smith 1989 {published data only}
- Smith AL, Ramsey BW, Hedges DL, Hack B, Williams-Warren J, Weber A, et al. Safety of aerosol tobramycin administration for three months to patients with cystic fibrosis. Pediatric Pulmonology 1989;7:265-71. [DOI] [PubMed] [Google Scholar]
Stass 2009 {published data only}PI233
- Stass H, Nagelschmitz J, Posselt H. Safety, tolerability and pharmacokinetics of ciprofloxacin dry powder for inhalation in adolescent patients with CF. Pediatric Pulmonology 2009;44 Suppl 32:302. [ABSTRACT NO: 258] [CFGD REGISTER: PI233] [Google Scholar]
Stass 2015 {published data only}PI215
- Stass H, Delesen H, Nagelschmitz J, Staab D. Safety and pharmacokinetics of ciprofloxacin dry powder for inhalation in cystic fibrosis: a phase I, randomized, single-dose, dose-escalation study. Journal of Aerosol Medicine and Pulmonary Drug Delivery 2015;28(2):106-15. [CFGD REGISTER: PI215c] [DOI: 10.1089/jamp.2013.1056] [DOI] [PubMed] [Google Scholar]
- Stass H, Ludwig M, Nagelschmitz J, Stabb D. Safety and pharmacokinetics of inhaled dry powder ciprofloxacin after single and multiple inhalations in patients with cystic fibrosis. Pediatric Pulmonology 2008;43 Suppl 31:300. [CFGD REGISTER: PI215a] [Google Scholar]
- Stass H, Weimann B, Nagelschmitz J, Rolinck-Werninghaus C, Staab D. Tolerability and pharmacokinetic properties of ciprofloxacin dry powder for inhalation in patients with cystic fibrosis: a phase I, randomized, dose-escalation study. Clinical Therapeutics 2013;35(10):1571-81. [CFGD REGISTER: PI215b] [DOI] [PubMed] [Google Scholar]
Steinkamp 1989 {published data only}
- Gappa M, Steinkamp G, Tummler B, Von Der Hardt H. Long-term tobramycin aerosol therapy of chronic Pseudomonas aeruginosa infection in patients with cystic fibrosis. Scandinavian Journal of Gastroenterology 1988;23 Suppl 143:74-6. [PubMed] [Google Scholar]
- Steinkamp G, Tummler B, Gappa M, Albus A, Potel J, Doring G, et al. Long-term tobramycin aerosol therapy in cystic fibrosis. Pediatric Pulmonology 1989;6:91-8. [DOI] [PubMed] [Google Scholar]
Steinkamp 2006 {published data only}
- Steinkamp G, Schmitt-Grohe S, Doring G, Stabb D, Schubert R, Zielen S. Once weekly azithromycin in cystic fibrosis: a double-blind, randomised trial in patients with chronic Pseudomonas aeruginosa infection. Pediatric Pulmology 2007;42 Suppl 30:300. [Google Scholar]
- Steinkamp G, Schmitt-Grohe S, Doring G, Worlitzsch D, Staab D, Schubert R, et al. Clinical and immunomodulatory effects of once weekly azithromycin treatment in cystic fibrosis patients chronically infected with Pseudomonas aeruginosa. Journal of Cystic Fibrosis 2006;5 Suppl:S25. [Google Scholar]
Stephens 1983 {published data only}PI105
- Stephens D, Garey D, Isles A, Levison H, Gold R. Efficacy of inhaled tobramycin in the treatment of pulmonary exacerbations in children with cystic fibrosis. Pediatric Infectious Disease Journal 1983;2(3):209-11. [CFGD REGISTER: PI105] [DOI] [PubMed] [Google Scholar]
Stroobant 1985 {published data only}PI83
- Heaf DP, Tyson S, Dinwiddie R, Matthew D. A comparison of inhaled therapies in children with cystic fibrosis. In: 9th International Cystic Fibrosis Congress; 1984 June 9-15; Brighton, England. 1984:274. [CFGD REGISTER: PI83a]
- Stroobant J, Heaf DP, Tyson S, Matthew DJ. Effect of inhaled azlocillin, mistabron and combination therapy in children with cystic fibrosis. In: 13th Annual Meeting of European Working Group for Cystic Fibrosis; 1985 Nov 3-8; Jerusalem. 1985:47. [CFGD REGISTER: PI83b]
- Stroobant J, Heaf DP, Tyson S, Matthew DJ. Effect of inhaled azlocillin, mistabron and combination therapy in children with cystic fibrosis. Pediatric Research 1985;19:1099. [CFGD REGISTER: PI83c] [Google Scholar]
Tramper‐Stranders 2010 {published data only}PI239
- Tramper-Stranders G, Wolfs TFW, Aalderen W, Kouwenberg J, Nagelkerke A, Ent CK. Prevention of initial P. aeruginosa infection in children with cystic fibrosis: a multi-centre double-blind randomised controlled trial. Journal of Cystic Fibrosis 2009;8 Suppl 2:S37. [ABSTRACT NO: 148] [CFGD REGISTER: PI239a] [Google Scholar]
- Tramper-Stranders GA, Wolfs TF, Haren Noman S, Aalderen WM, Nagelkerke AF, Nuijsink M, et al. Controlled trial of cycled antibiotic prophylaxis to prevent initial Pseudomonas aeruginosa infection in children with cystic fibrosis. Thorax 2010;65(10):915-20. [CENTRAL: 761942] [CFGD REGISTER: PI239b] [PMID: ] [DOI] [PubMed] [Google Scholar]
Trapnell 2012 {published data only}PI247
- McColley SA, Trapnell B, Kissner D, McKevitt M, Montgomery B, Rosen J, et al. Fosfomycin/tobramycin for inhalation (FTI): microbiological results of a phase 2 placebo-controlled trial in patients with cystic fibrosis and pseudomonas aeruginosa. Pediatric Pulmonology 2010;45 Suppl 33:338. [ABSTRACT NO: 334] [CFGD REGISTER: PI247c] [CFGD REGISTER: PI247c] 5500100000010542 [Google Scholar]
- Trapnell BC, Kissner D, Montgomery AB, Newcomb T, Geller D. Fosfomycin/tobramycin for inhalation FTI): safety results of a phase 2 placebo-controlled trial in patients with cystic fibrosis and pseudomonas aeruginosa. Pediatric Pulmonology 2010;45 Suppl 33:302. [ABSTRACT NO: 234] [CFGD REGISTER: PI247b] 5500100000010541 [Google Scholar]
- Trapnell BC, McColley SA, Kissner DG, Rolfe MW, Rosen JM, McKevitt M, et al. Fosfomycin/tobramycin for inhalation in patients with cystic fibrosis with pseudomonas airway infection. American Journal of Respiratory and Critical Care Medicine 2012;185(2):171-8. [CFGD REGISTER: PI247d] 5500100000010632 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trapnell BC, Rolfe M, McColley S, Montgomery AB, Moorehead L, Geller D. Fosfomycon/tobramycin for inhalation (FTI): efficacy results of a phase 2 placebo-controlled trial in patients with cystic fibrosis and pseudomonas aeruginosa. Pediatric Pulmonology 2010;45 Suppl 33:302. [ABSTRACT NO: 233] [CFGD REGISTER: PI247a] 5500100000010712 [Google Scholar]
Valerius 1991 {published data only}PI70
- Valerius NH, Koch C, Hoiby N. Prevention of chronic colonization with Pseudomonas aeruginosa in patients with CF by early treatment with ciprofloxacin and colistin aerosol inhalations. Pediatric Pulmonology 1990;Suppl 5:219. [CFGD REGISTER: PI70a] [Google Scholar]
- Valerius NH, Koch C, Hoiby N. Prevention of chronic Pseudomonas aeruginosa colonisation in cystic fibrosis by early treatment. Lancet 1991;338(8769):725-6. [CFGD REGISTER: PI70b] [DOI] [PubMed] [Google Scholar]
Wainwright 2008 {published data only}PI167
- Byrnes CA, Vidmar S, Cheney JL, Carlin JB, Armstrong DS, Cooper PJ, et al. Prospective evaluation of respiratory exacerbations in children with cystic fibrosis from newborn screening to 5 years of age. Thorax 2013;68(7):643-51. [CENTRAL: 904924] [CFGD REGISTER: PE167i] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheney J, Vidmar S, Grimwood K, Carlin JB, Wainwright C, on behalf of ACFBAL Study Group. Interim outcomes of Pseudomonas aeruginosa (Pa) eradication protocol in young children in the Australasian Cystic Fibrosis Bronchoalveolar Lavage (ACFBAL) Study. Journal of Cystic Fibrosis 2009;8 Suppl 2:S39. [ABSTRACT NO: 157] [CENTRAL: 744130] [CFGD REGISTER: PE167c] [Google Scholar]
- Cheney J, Wainwright C, ACFBAL Study Group. Trials, tribulations and triumphs of a cystic fibrosis study - a behind the scenes look at the workings of an international multi-centre study. Journal of Cystic Fibrosis 2010;9 Suppl 1:S118. [ABSTRACT NO: 452] [CENTRAL: 790042] [CFGD REGISTER: PE167g] [Google Scholar]
- Kidd TJ, Ramsay KA, Vidmar S, Carlin JB, Bell SC, Wainwright CE, et al. Pseudomonas aeruginosa genotypes acquired by children with cystic fibrosis by age 5-years. Journal of Cystic Fibrosis 2015;14(3):361-9. [CENTRAL: 1131104] [CFGD REGISTER: PE167k] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Moodie M, Lal A, Vidmar S, Armstrong DS, Byrnes CA, Carlin JB, et al. Costs of bronchoalveolar lavage-directed therapy in the first 5 years of life for children with cystic fibrosis. Journal of Pediatrics 2014;165(3):564-9. [CFGD REGISTER: PE167j] [JID: 0375410] [PMID: ] [SI: ANZCTR/ACTRN12605000665639] [DOI] [PubMed] [Google Scholar]
- Wainwright C, Carlin J, Cooper P, Byrnes C, Martin J, Grimwood K, et al. Australasian cystic fibrosis BAL study interim analysis. Pediatric Pulmonology 2006;41 Suppl 29:317. [CENTRAL: 593082] [CFGD REGISTER: PE167a] [Google Scholar]
- Wainwright CE, Carlin J, Cooper P, Byrnes C, Whitehead B, Martin J, et al. Early infection with pseudomonas aeruginosa can be cleared in young children with cystic fibrosis. Pediatric Pulmonology 2002;Suppl 24:300-1. [CENTRAL: 404073] [CFGD REGISTER: PE167d] [Google Scholar]
- Wainwright CE, Grimwood K, Carlin JB, Vidmar S, Cooper PJ, Francis PW, et al. Safety of bronchoalveolar lavage in young children with cystic fibrosis. Pediatric Pulmonology 2008;43(10):965-72. [CENTRAL: 691446] [CFGD REGISTER: PE167b] [DOI] [PubMed] [Google Scholar]
- Wainwright CE, Kidd TJ, Ramsey KA, Bell SC, Grimwood K. Australasian CF bronchoalveolar lavage (ACFBAL) study: P. aeruginosa (PA) genotypes in pre-school CF children. Pediatric Pulmonology 2011;46 Suppl 34:320. [ABSTRACT NO: 299] [CENTRAL: 874662] [CFGD REGISTER: PE167h] [Google Scholar]
- Wainwright CE, Vidmar S, Armstrong DS, Byrnes CA, Carlin JB, Cheney J, et al. Effect of bronchoalveolar lavage-directed therapy on Pseudomonas aeruginosa infection and structural lung injury in children with cystic fibrosis: a randomized trial. JAMA 2011;306(2):163-71. [CENTRAL: 788878] [PE167e] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Wainwright CE, Vidmar S, Armstrong DS, Byrnes CA, Carlin JB, Cheney J, et al. Effect of bronchoalveolar lavage-directed therapy on Pseudomonas aeruginosa infection and structural lung injury in children with cystic fibrosis: a randomized trial. JAMA 2011;306(2):163-71. Online supplement. [CFGD REGISTER: PE167f] 5500100000011126 [DOI] [PubMed] [Google Scholar]
Wainwright 2011 {published data only}PI243
- EUCTR2015-000395-97-Outside-EU/EEA. A clinical trial to evaluate the effects of the drug aztreonam lysine for inhalation in patients with cystic fibrosis, mild lung disease, and infection with the bacteria pseudomonas aeruginosa (AIR-CF4). trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2015-000395-97-Outside-EU/EEA (first received 2 February 2015).
- NCT00712166. Safety and efficacy study of aztreonam for inhalation solution (AZLI) in patients with cystic fibrosis, mild lung disease, and P. Aeruginosa. clinicaltrials.gov/show/NCT00712166 (first received 9 July 2008). [CFGD REGISTER: PI243c]
- Wainwright C, Nakamura C, Geller D, Montgomery AB. A double-blind, multinational, randomized, placebo-controlled trial evaluating aztreonam for inhalation solution (AZLI) in patients with cystic fibrosis (CF), mild lung disease and P. aeruginosa. Journal of Cystic Fibrosis 2010;9 Suppl 1:S22. [ABSTRACT NO: 81] [CFGD REGISTER: PI243a] [DOI] [PubMed] [Google Scholar]
- Wainwright CE, Quittner AL, Geller DE, Nakamura C, Wooldridge JL, Gibson RL, et al. Aztreonam for inhalation solution (AZLI) in patients with cystic fibrosis, mild lung impairment, and P. aeruginosa. Journal of Cystic Fibrosis 2011;10:234-42. [CFGD REGISTER: PI243b] [AIR-CF4 Study Group] [DOI] [PubMed] [Google Scholar]
Wall 1984 {published data only}
- Wall MA, Steinbach S, McNamara M, Terry AB. Prophylactic inhaled antibiotics in cystic fibrosis. In: 25th Annual Meeting Cystic Fibrosis Club Abstracts;1984; San Jose. 1984:35.
- Wall MA, Terry AB, Eisenberg J, McNamara M, Cohen R. Inhaled antibiotics in cystic fibrosis. Lancet 1983;1(8337):1325. [DOI] [PubMed] [Google Scholar]
Wang 1984 {published data only}
- Wang CI, Roldan MA, Aufderheide M, Sehgal S. The effect of tobramycin aerosol to pulmonary infection from Pseudomonas aeruginosa in patients with cystic fibrosis. In: 25th Annual Meeting Cystic Fibrosis Club Abstracts;1984; San Jose. 1984:159.
Westerman 2003 {published data only}
- Westerman EM, Le Brun PP, Frijlink HW, Heijerman HG. Effect of nebulised colistin sulphate and colistin sulphomethate on lung function in patients with cystic fibrosis. Journal of Cystic Fibrosis 2003;2 Suppl 1:S55. [CFGD REGISTER: PI177a] [DOI] [PubMed] [Google Scholar]
- Westerman EM, Le Brun PP, Frijlink HW, Heijerman HG. Sulfate is unsatisfactory. Effect of nebulizing colistin sulfate and colistin sulfomethate on the lung function in patients with cystic fibrosis. Pharmaceutisch Weekblad 2003;138(20):703-7. [CFGD REGISTER: PI177c] [Google Scholar]
- Westerman EM, Le Brun PP, Touw DJ, Frijlink HW, Heijerman HG. Effect of nebulized colistin sulphate and colistin sulphomethate on lung function in patients with cystic fibrosis: a pilot study. Journal of Cystic Fibrosis 2004;3(1):23-8. [CFGD REGISTER: PI177b] [DOI] [PubMed] [Google Scholar]
Westerman 2007 {published data only}PI193
- Westerman EM, De Boer AH, Le Brun PP, Touw DJ, Roldaan AC, Frijlink HW, et al. Dry powder inhalation of colistin in cystic fibrosis patients: a single dose pilot study. Journal of Cystic Fibrosis 2007;6(4):284-92. [CFGD REGISTER: PI193b] [DOI] [PubMed] [Google Scholar]
- Westerman EM, Boer AH, Le Brun PPH, Touw DJ, Frijlink HW, Heijerman HGM. Colistin dry powder inhalation in cystic fibrosis: novel Twincer® inhaler compared to nebulization: a pilot study. Journal of Cystic Fibrosis 2005;4 Suppl 1:S64. [CFGD REGISTER: PI193a] [Google Scholar]
Yasmin 1974 {published data only}PI79
- Yasmin N, Laraya-Cuasay LR, Mueller S, Liberi P, Braverman S, Capitanio M, et al. A critical evaluation of antibiotic aerosol in patients with cystic fibrosis. In: 15th Annual Meeting of Cystic Fibrosis Club; 1974. 1974. [CFGD REGISTER: PI79]
References to studies awaiting assessment
EUCTR2007‐004277‐26‐NL {published data only}
- EUCTR2007-004277-26-NL. An open-label, randomized, phase 3 trial to evaluate the efficacy and safety of aztreonam 75 mg powder and diluent for nebuliser solution (AZLI) versus tobramycin nebuliser solution (TNS) in an intermittent aerosolized antibiotic regimen, in subjects with cystic fibrosis followed by an open-label, single arm extension. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2007-004277-26-BE (first received 20 December 2008).
Herrmann 2017 {published data only}
- Herrmann G, Freitag E, Kiefer L, Bender V, Adams C, Graepler-Mainka U, et al. Combined dry powder tobramycin and nebulized colistin versus colistin inhalation in CF patients - a randomised, open label phase III clinical study. Journal of Cystic Fibrosis 2017;16 Suppl 1:S54. [CFGD REGISTER: PI294] [Google Scholar]
NCT03341741 {published data only}
- NCT03341741. Combined dry powder tobramycin and nebulized colistin inhalation in CF patients. clinicaltrials.gov/show/NCT03341741 (first received 14 November 2017).
Nikonova 2010 {published data only}PI242
- Nikonova VS, Kashirskaya NY, Kapranov NI. Efficacy and safety of tobramycin and colistin for inhalation in children with cystic fibrosis from Moscow region. Journal of Cystic Fibrosis 2010;9 Suppl 1:S54. [ABSTRACT NO: 210] [CFGD REGISTER: PI242] [Google Scholar]
Additional references
Birnbaum 1998
- Birnbaum HG, Greenberg P, Finkelstein S, Berndt E, Otto KL, Montgomery AB, et al. Economic analysis of hospitalization and home IV anti-pseudomonal antibiotic use in CF patients on tobramycin solution for inhalation (TOBI). Pediatric Pulmonology 1998;Suppl 17:273. [Google Scholar]
Burns 1999
- Burns JL, Van Dalfsen JM, Shawar RM, Otto KL, Garber RL, Quan JM, et al. Effect of chronic intermittent administration of inhaled tobramycin on respiratory microbial flora in patients with cystic fibrosis. Journal of Infectious Diseases 1999;179(5):1190-6. [DOI] [PubMed] [Google Scholar]
CF Foundation 2019
- Cystic Fibrosis Foundation. About cystic fibrosis. www.cff.org/What-is-CF/About-Cystic-Fibrosis/ (accessed 22 August 2022).
CF Trust 2009
- Cystic Fibrosis Trust. Antibiotic treatment for cystic fibrosis. Consensus document; 3rd edition; 2009 May. www.cysticfibrosis.org.uk/~/media/documents/the-work-we-do/care/consensus-docs-with-new-address/anitbiotic-treatment.ashx?la=en (accessed prior to 8 November 2017).
CF Trust 2021
- Cystic Fibrosis Trust. UK cystic fibrosis 2020 registry annual data report. cysticfibrosis.org.uk/registryreports (accessed 22 August 2022).
Dodge 2007
- Dodge JA, Lewis PA, Stanton M, Wilsher J. Cystic fibrosis mortality and survival in the UK: 1947 - 2003. European Respiratory Journal 2007;29:522-6. [DOI] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne DR, Altman DG, Higgins JPT, Curtin F, Worthington HV, Vail A. Meta-analysis involving cross-over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140-9. [DOI] [PubMed] [Google Scholar]
Emerson 2002
- Emerson J, Rosenfeld M, McNamara S, Ramsey B, Gibson R L. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatric Pulmonology 2002;34(2):91-100. [DOI] [PubMed] [Google Scholar]
Flume 2007
- Flume PA, O'Sullivan BP, Robinson KA, Goss CH, Mogayzel PJ, Willey-Courand DB, et al. Cystic fibrosis pulmonary guidelines. Chronic medication for maintenance of lung health. American Journal of Respiratory and Critical Care Medicine 2007;176(10):957-69. [DOI] [PubMed] [Google Scholar]
GOSH 2011
- Great Ormond Street Hospital for Children NHS Trust. Handbook for the management of children with cystic fibrosis; September 2011. www.gosh.nhs.uk/file/745/download?token=pZK-Gnjs (accessed prior to 8 November 2017).
Higgins 2017
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (updated June 2017), Cochrane, 2017. Available from training.cochrane.org/handbook#previous-versions 2017.
Higgins 2021
- Higgins JP, Savović J, Page MJ, Elbers RG, Sterne JA. Chapter 8: Assessing risk of bias in a randomised trial. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook/archive/v6.2.
Langton Hewer 2017
- Langton Hewer SC, Smyth AR. Antibiotic strategies for eradicating Pseudomonas aeruginosa in people with cystic fibrosis. Cochrane Database of Systematic Reviews 2017, Issue 4. Art. No: CD004197. [DOI: 10.1002/14651858.CD004197.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mogayzel 2013
- Mogayzel PJ Jr, Naureckas ET, Robinson KA, Mueller G, Hadjiliadis D, Hoag JB, et al. Cystic fibrosis pulmonary guidelines. Chronic medications for maintenance of lung health. American Journal of Respiratory & Critical Care Medicine 2013;187(7):680-9. [DOI] [PubMed] [Google Scholar]
Montori 2005
- Montori VM, Devereaux PJ, Adhakiri NKJ et al. Randomized trials stopped early for benefit. JAMA 2005;294(17):2203-9. [DOI] [PubMed] [Google Scholar]
Newman 1985
- Newman SP. Aerosol deposition considerations in inhalational therapy. Chest 1985;88(2 Suppl):152S-60S. [DOI] [PubMed] [Google Scholar]
NICE 2013
- National Institute for Health and Care Excellence. Colistimethate sodium and tobramycin dry powders for inhalation for treating pseudomonas lung infection in cystic fibrosis. Technology appraisal guidance TA276; March 2013. www.nice.org.uk/Guidance/ta276 (accessed prior to 8 November 2017).
NICE 2017
- National Institute for Health and Clinical Excellence. Cystic fibrosis: diagnosis and management; 2017. Available at nice.org.uk/guidance/ng78. [PubMed]
Review Manager 2014 [Computer program]
- Review Manager 5 (RevMan 5). Version 5.3. The Cochrane Collaboration, 2014.
Rosenstein 1998
- Rosenstein BJ, Zeitlin PL. Cystic fibrosis. Lancet 1998;351(9098):277-82. [DOI] [PubMed] [Google Scholar]
Ryan 2012
- Ryan G, Jahnke N, Remmington T. Inhaled antibiotics for pulmonary exacerbations in cystic fibrosis. Cochrane Database of Systematic Reviews 2012, Issue 12. Art. No: CD008319. [DOI: 10.1002/14651858.CD008319.pub2] [DOI] [PubMed] [Google Scholar]
Touw 1995
- Touw DJ, Brimicombe RW, Hodson ME, Heijerman HGM, Bakker W. Inhalation of antibiotics in cystic fibrosis. European Respiratory Journal 1995;8(9):1594-604. [PubMed] [Google Scholar]
Wark 2009
- Wark P, McDonald VM. Nebulised hypertonic saline for cystic fibrosis. Cochrane Database of Systematic Reviews 2009, Issue 2. Art. No: CD001506. [DOI: 10.1002/14651858.CD001506.pub3] [DOI] [PubMed] [Google Scholar]
Yankaskas 2004
- Yankaskas JR, Marshall BC, Sufian B, Simon RH, Rodman D. Cystic fibrosis adult care: consensus conference report. Chest 2004;125((1 Suppl)):1S-39S. [DOI] [PubMed] [Google Scholar]
Zemanick 2015
- Zemanick ET, Emerson J, Thompson V, McNamara S, Morgan W, Gibson RL, et al. Clinical outcomes after initial pseudomonas acquisition in cystic fibrosis. Pediatric Pulmonology 2015;50(1):42-8. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Ryan 1999
- Ryan G, Mukhopadhyay S, Singh M. Nebulised anti-pseudomonal antibiotics for cystic fibrosis. Cochrane Database of Systematic Reviews 1999, Issue 3. Art. No: CD001021. [DOI: 10.1002/14651858.CD001021] [DOI] [PubMed] [Google Scholar]
Ryan 2003
- Ryan G, Mukhopadhyay S, Singh M. Nebulised anti-pseudomonal antibiotics for cystic fibrosis. Cochrane Database of Systematic Reviews 2003, Issue 3. Art. No: CD001021. [DOI: 10.1002/14651858.CD001021] [DOI] [PubMed] [Google Scholar]
Ryan 2011
- Ryan G, Singh M, Dwan K. Inhaled antibiotics for long-term therapy in cystic fibrosis. Cochrane Database of Systematic Reviews 2011, Issue Issue 3. Art. No.: CD001021. Art. No: CD001021. [DOI: 10.1002/14651858.CD001021.pub2] [DOI] [PubMed] [Google Scholar]
Smith 2018
- Smith S, Rowbotham NJ, Regan KH. Inhaled anti-pseudomonal antibiotics for long-term therapy in cystic fibrosis. Cochrane Database of Systematic Reviews 2018, Issue 3. Art. No: CD001021. [DOI: 10.1002/14651858.CD001021.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]