

Abstract
Introduction
The incidence of degenerative disorders, including osteoarthritis (OA), increases rapidly in women after menopause. However, the influence of the menopause is still insufficiently investigated due to the slowness of menopausal transition. In this study, a novel human model is used in which it is expected that menopausal-related changes will occur faster. This is the Females discontinuing Oral Contraceptives Use at Menopausal age model. The ultimate aim is to link these changes to OA and other degenerative disorders, including cardiovascular diseases, diabetes, osteoporosis and tendinopathies.
Methods and analysis
This is a pilot observational prospective cohort study with 2 years of follow-up. Fifty women aged 50–60 who use oral contraceptive (OC) and have the intention to stop are included. Measurements are performed once before stopping OC, and four times thereafter at 6 weeks, 6 months, 1 year and 2 years. At every time point, a questionnaire is filled in and a sample of blood is drawn. At the first and final time points, a physical examination, hand radiographs and a MRI scan of one knee are performed. The primary OA outcome is progression of the MRI Osteoarthritis Knee Score. Secondary OA outcomes are the development of clinical knee and hand OA, development of knee OA according to the MRI definition, and progression of radiographic features for hand OA. Principal component analysis will be used to assess which changes occur after stopping OC. Univariate and multivariate generalised estimating equation models will be used to test for associations between these components and OA.
Ethics and dissemination
The study has been approved by the Medical Ethics Committee of the Erasmus MC University Medical Center Rotterdam (MEC-2019-0592). All participants must give informed consent before data collection. Results will be disseminated in national and international journals.
Trial registration number
NL70796.078.19.
Keywords: Musculoskeletal disorders, INTERNAL MEDICINE, Magnetic resonance imaging
STRENGTHS AND LIMITATIONS OF THIS STUDY.
In this study, a novel human model (Females discontinuing Oral Contraceptives Use at Menopausal age) will be used to explore the influence of the menopause on the development of osteoarthritis and other degenerative disorders.
This model does not have the limitations in generalisability of animal models, nor does it have the limitations of subsequent hormonal support in other human models.
The model consists of women who stop oral contraceptive use at menopausal age, whereby it is not known in advance whether the woman will then directly enter the menopausal state.
Because the model has never been used before, this model will be used in a pilot study first with a small number of participants.
Introduction
Background and rationale
In the Netherlands, the prevalence of degenerative disorders, including osteoarthritis (OA), will increase due to population growth and ageing. In 2020, approximately 1.5 million people in the Netherlands were registered in primary care with OA and it is estimated that OA will be the most prevalent chronic disease in the Netherlands by 2040.1 2 OA is an age-related degenerative disorder of the joint which causes chronic pain, stiffness and disability. Until now, no disease-modifying therapy or prevention strategy exists for OA due to the complex multifactorial nature of the disease.3
Because the incidence of OA, and other degenerative disorders, increases rapidly after the age of 50 in women, it has been suggested that the menopause, and the change in hormones during the menopausal transition, influences the development of these disorders. Not only do hormone levels change during the menopausal transition, but so do the metabolism and inflammatory responses. Because these changes occur slowly, the role of the menopause is still insufficiently investigated.4 However, identifying possible causal relationships is crucial to developing novel, female-specific prevention strategies and therapies for these disorders.
In this study, a novel human model will be used to investigate the influence of the menopause on the development of OA and other degenerative disorders by modelling a ‘sudden menopause‘ in which it is expected that menopause-related changes will occur faster. This is the Females discontinuing Oral Contraceptives Use at Menopausal age (FOCUM) model. In this model, a ‘sudden menopause’ is defined as a rapid change in hormonal levels due to stopping oral contraceptive (OC) use at ‘menopausal’ age.
Objectives
The first aim of the FOCUM study is to develop the FOCUM model as a disease model for the development of OA. The second aim is to identify changes, specifically in proteins, that occur after a ‘sudden menopause’ and to identify which of these changes are associated with the development of OA after 2 years. The third aim is to explore whether the model can also be used to learn more about the development of other degenerative disorders, including cardiovascular diseases, diabetes, osteoporosis and tendinopathies.
Methods
Study design and setting
The FOCUM study is a pilot observational prospective cohort study in the Netherlands, with 2 years of follow-up. The study is being conducted by the department of general practice at the Erasmus MC University Medical Center in Rotterdam. Participants are recruited through pharmacies in and around Rotterdam by sending an invitation letter to women who meet the age and OC use criteria, with information about the study and the general advice to stop OC use at the age of 52. Women who are interested in participating and have the intention to stop OC use can fill in a response form and send it to Erasmus MC. All further screening, informed consent and study procedures will be performed by a clinical researcher at Erasmus MC. Participants are invited to visit the centre five times in total for measurements at baseline and during 2 years of follow-up. The recruitment of participants for this study started in July 2020 and, with a follow-up period of 2 years, this study is expected to be completed in August 2023.
Eligibility criteria
Women are eligible to participate in the FOCUM study if they have the intention to stop OC use and meet the following inclusion and exclusion criteria.
Inclusion criteria
Between 50 and 60 years of age.
Currently using a combined OC (with Anatomical Therapeutic Chemical code G03AA or G03AB).
Started OC use before the age of 45.
Exclusion criteria
Already known to have OA (self-reported or registered by their general practitioner).
Already known to have another inflammatory rheumatic condition (including rheumatoid arthritis, gout and psoriatic arthritis).
Contraindication for MRI.
Terminal or mental illness.
Unable to give informed consent.
Study procedures
After giving informed consent, baseline measurements (T0) are performed just before (0–30 days) stopping OC use. After stopping OC use, measurements are performed at four additional time points (T1=6 weeks; T2=6 months; T3=1 year; T4=2 years). At every time point a digital questionnaire is filled in, a normal photograph is taken of both hands and a sample of blood is drawn. In addition, at T0 and T4 a physical examination, a posterior–anterior radiograph of both hands, an MRI scan of one knee, a dual energy X-ray absorptiometry (DXA) scan and an ultrasound tissue characterisation (UTC) of one Achilles tendon are performed (see figure 1). All physical examinations and measurements are performed by the same clinical researcher at Erasmus MC.
Figure 1.
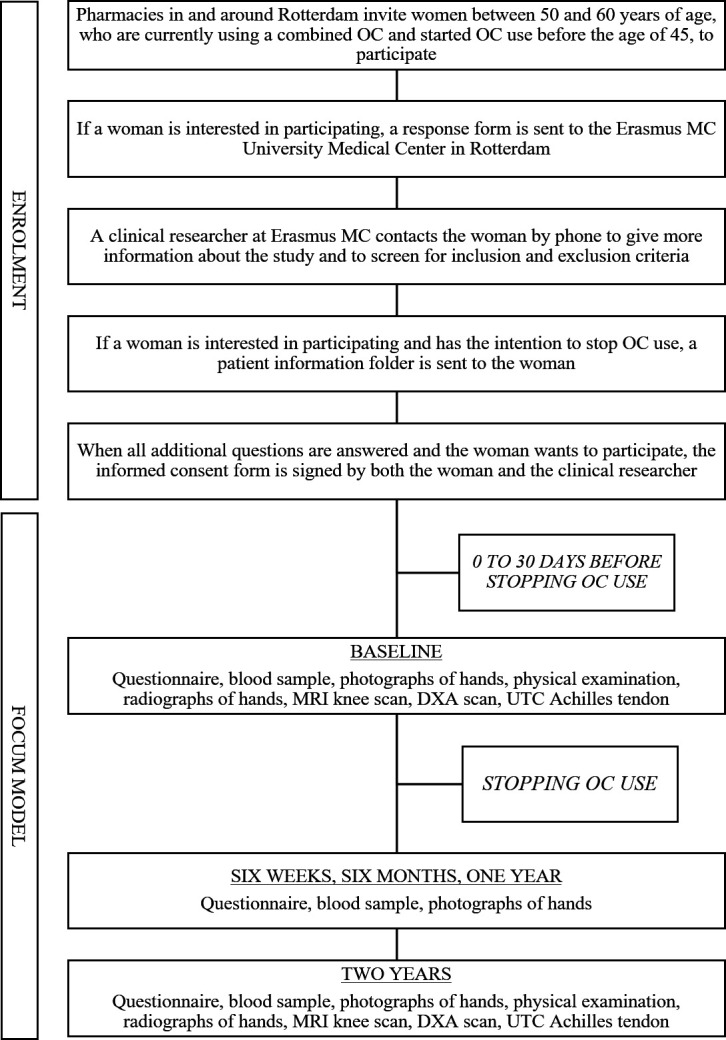
Flow chart of the FOCUM study. DXA, dual energy X-ray absorptiometry; OC, oral contraceptive; UTC, ultrasound tissue characterisation.
Data collection
Data collection methods
Questionnaires
Standardised questionnaires are used, including the Knee injury and Osteoarthritis Outcome Score5 and Australian Canadian Osteoarthritis Hand Index,6 to obtain information about the presence of and changes in knee and hand symptoms, respectively. The Short Questionnaire to Assess Health-enhancing physical activity7 is used to obtain information about physical activity and the Menopause Rating Score8 to obtain information about menopausal symptoms. Further questions are asked to obtain information about participants’ background characteristics (eg, level of education, profession and smoking), pain locations (manikin), reproductive factors (eg, age at menarche, parity and first and final start of OC use), medical history and current medical problems, medication use, family history and cardiovascular symptoms. Furthermore, additional questions are asked about tendon (Achilles and gluteus medius) and joint symptoms (including morning stiffness, activity-related pain and pain duration) to assess the development of tendinopathies and OA according to the clinical American College of Rheumatology (ACR)9 10 and National Institute for Health and Care Excellence.11
Physical examination
The physical examination of the participant includes: (1) measurements of body height and weight; (2) inspection and palpation of deformities, swelling, warmth, pain and bony enlargements of the hand and knee joints to assess the development of knee and hand OA according to the clinical ACR criteria9 10; (3) measurements of the strength of the quadriceps; (4) pain pressure threshold of both knees and one forearm with a handheld dynamometer (MicroFET2, Hoggan Health Industries, Salt Lake City, Utah, USA)12; (5) measurements of the range of motion of the knees with a goniometer and (6) assessment of the presence of tendinopathies by looking for swelling and pain on palpation of the Achilles and gluteus medius tendon and plantar fascia.
Blood measurements
Cholesterol (including low-density lipoprotein-cholesterol, high-density lipoprotein-cholesterol), total cholesterol and triglyceride), glucose and hormone levels (including estradiol, testosterone, androstenedione and 17-hydroxyprogesterone) are measured to investigate changes over time. Also, DNA methylation changes and immunological aspects of blood cells are assessed. To establish which time points are most relevant to find changes in proteins after a ‘sudden menopause’, changes in serum levels of inflammation and cardiometabolic-related proteins are examined.
Photographs of hands
The photographs of both hands of the participant are taken by the clinical researcher at baseline and after 2 years of follow-up. At the other time points, the photographs are taken by the participant and sent as a digital attachment to their completed questionnaire. The clinical researcher and participants are instructed to take the photograph with the palm of the hand on a dark and solid background. These images will be used to assess the development of structural changes in the hands by looking at joint deformities, bony enlargement and swelling.
Radiographs of hands
The posterior–anterior radiograph of both the participant’s hands is taken using a clinical X-ray system (Ysio Max, Siemens Healthcare, Erlangen, Germany). Each hand is placed on a separate cassette with the palm of the hand on the detection plate, the fingers extended and adducted and the forearm resting on the X-ray table. These radiographs are used to assess the progression of radiographic features of hand OA with reference to the Osteoarthritis Research Society International (OARSI) atlas. This atlas allows semiquantitative assessment of the presence and severity of hand OA features, such as osteophytes, joint space narrowing, subchondral erosions/sclerosis, cysts and malalignment.13–15
MRI knee scan
The MRI scan of one knee (the knee with the most symptoms or the right knee if asymptomatic at baseline) is performed using a clinical 3.0T MRI system (SIGNA Premier, General Electric (GE) Company, Boston, Massachusetts, USA) with a dedicated knee coil. The scan of the knee includes: (1) conventional MRI sequences (proton density and T2-weighted with fat suppression) to allow semi-quantitative assessment of the presence and severity of knee OA features using the MRI Osteoarthritis Knee Score (MOAKS)16 and (2) T2 mapping of articular cartilage, which provides a quantitative assessment of cartilage collagen content and network integrity. MOAKS scores are used to define the progression of MRI features for knee OA and the development of knee OA according to the MRI definition.17 18
DXA scan
The DXA scan of the total body, hip and lumbar and lateral spine is performed using a clinical DXA scanner (Lunar iDXA, GE Company). These scans are used to assess changes in bone mineral density (BMD) of the total body, hip and lumbar spine, Trabecular Bone Score, fat and muscle mass/distribution and development of osteoporosis and vertebral fractures through vertebral fracture assessment.
UTC Achilles tendon
The UTC scan of one Achilles tendon (the tendon with most symptoms or the right tendon if asymptomatic at baseline) is performed using a specific UTC device (UTC System, UTC Imaging BV, Stein, the Netherlands), which consists of an ultrasound scanner and a connected transducer.19 For this scan, the participant lies in a prone position on a research table with both feet over the edge of the table. The Achilles tendon is stretched by passive maximum dorsiflexion of the ankle, which is applied by the researcher. The transducer is placed in a transverse position and perpendicular to the tendon and moves automatically from proximal to distal over a distance of twelve centimetres. These images result in a three-dimensional scan, which is used for tomographical visualisation of the tendon in three planes of view. These images are used to assess the integrity (percentage aligned tendon structure), maximum anterior to posterior distance, maximum cross-sectional area and volume of the Achilles tendon mid-portion.20
Outcomes
Primary and secondary outcomes
The primary outcome of the FOCUM study is the progression of MRI features for knee OA scored with the MOAKS.16 17 Secondary outcomes of the study are as follows: (1) the development of knee OA according to the clinical ACR criteria9; (2) the development of knee OA according to the MRI definition18; (3) the progression of radiographic features for hand OA scored with the OARSI atlas13–15 and (4) the development of hand OA according to the clinical ACR criteria.10 Table 1 gives an overview of all the measurements that are performed during the study.
Table 1.
Overview of the measurements
| Time point | Baseline (T0) | 6 weeks (T1) | 6 months (T2) | 1 year (T3) | 2 years (T4) |
| Measurement | |||||
| PRIMARY OUTCOME | |||||
| MRI of knee | X | X | |||
| |||||
| SECONDARY OUTCOMES | |||||
| Questionnaire + physical examination | X | X | |||
| |||||
| MRI of knee | X | X | |||
| |||||
| Radiograph of hands | X | X | |||
| |||||
| OTHER VARIABLES | |||||
| Questionnaires | X | X | X | X | X |
| |||||
| |||||
| |||||
| |||||
| |||||
| |||||
| |||||
| |||||
| Physical examination | X | X | |||
| |||||
| |||||
| |||||
| |||||
| |||||
| Blood measurements | X | X | X | X | X |
| |||||
| |||||
| |||||
| |||||
| Photograph of hands | X | X | X | X | X |
| |||||
| Dual energy X-ray absorptiometry scan | X | X | |||
| |||||
| |||||
| |||||
| |||||
| Ultrasound Tissue Characterisation of Achilles tendon | X | X | |||
|
*Glucose, low-density lipoprotein, high-density lipoprotein, total cholesterol, triglyceride, estradiol, testosterone, androstenedione and 17-hydroxyprogesterone.
ACR, American College of Rheumatology; AP, anterior to posterior; AUSCAN, Australian Canadian Osteoarthritis Hand Index; BMD, bone mineral density; KOOS, Knee injury and Osteoarthritis Outcome Score; MOAKS, MRI Osteoarthritis Knee Score; MRS, Menopause Rating Scale; OA, osteoarthritis; OARSI, Osteoarthritis Research Society International; PPT, pain pressure threshold; SQUASH, Short Questionnaire to Assess Health-enhancing physical activity; TBS, Trabecular Bone Score.
Data management
Each participant receives a unique research identifier, which is used for all the measurements of the participant. All data are collected under this unique identifier in protected patient systems approved by Erasmus MC.
Study population size
For this pilot study, a total of 50 participants are included. It is known from another cohort study (PROOF study)21 that about 27% of women between 50 and 60 years of age will develop knee OA according to the MRI definition. For progression of the main knee OA features as measured with the MOAKS, this percentage is in the same range. With these numbers, we will be able to investigate which measurement time points are most valuable to assess the association between changes after a ‘sudden menopause’ and changes in disease features of OA after 2 years.
Statistical methods
The statistical analysis for this pilot study will be divided into two stages. In the first stage, the focus will be to establish which time points of measurements are most relevant to find changes in protein levels after a ‘sudden menopause’ (hormone change). Therefore, principal components analysis will be used on the delta in protein levels over time. Next, associations between the principal components and hormone change will be examined. In the second stage, these principal components will be related to the primary (progression of MRI features for knee OA) and secondary (development of clinical knee and hand OA, development of MRI-defined knee OA, progression of radiographic features for hand OA) outcomes of this study using generalised estimating equation models. First, associations will be assessed in univariate logistic regression models. If the p value of a variable is smaller than 0.1, the variable will be included in a multivariate logistic regression model.
Monitoring
A senior researcher in the department of general practice at Erasmus MC who is not directly related to the study has been assigned as monitor of the study. At various points during the study, meetings are held to monitor the study using a checklist. If there is sufficient ground to believe that continuation of the study will jeopardise the health or safety of a participant, or if it does not prove possible to include the minimum required number of participants, or if there is no additional funding for the study after 2 years, the study will be terminated earlier.
Harms
The time burden for the participants will be 9 hours spread over 2 years. There is little risk to their health from the radiographs and DXA scans (0.01 mSv in 2 years). All adverse events (AEs) and serious adverse events (SAEs) will be recorded and, in the event of an SAE, it will be reported to the accredited Medical Ethics Committee of Erasmus MC.
Patient and public involvement
In the prephase of this study, three patients from the OA patient panel of the department of general practice were asked about the relevance of this study. Although there was no direct relevance with respect to their own disease status, they were all excited about this study. During the preparation phase, one possibly eligible woman was asked about the recruitment of participants and the duration and burden of the measurements. After completion of this pilot study, we will ask five participants to think with us about future perspectives and dissemination.
Ethics and dissemination
Research ethics approval
The study was approved by the institutional review board (Medical Ethics Committee) of Erasmus MC (MEC-2019-0592) in December 2019.
Protocol amendments
Amendments are changes made to the study after the accredited Medical Ethics Committee of Erasmus MC has approved the study.
Consent or assent
If a woman is eligible to participate in the study, a patient information folder is sent. The woman is instructed to read the folder carefully and to contact the clinical researcher if there are any questions. After all additional questions have been answered and if the woman is still willing to participate, the informed consent form is signed by both the woman and the clinical researcher. In the informed consent form, participants can specify whether they want their data and body materials stored for future research.
Confidentiality
Each participant receives a unique identifier. Each identifier is linked to the personal information of the participant. The key for this link is stored at the department of general practice at Erasmus MC and is only available to persons who are directly involved in the study or who are monitoring the study.
Access to data
All data relating to the participants are collected under their unique identifiers in protected patient systems approved by Erasmus MC. Only those persons who are part of the research team have access to the data.
Ancillary and post-trial care
Erasmus MC has an insurance to cover damage to participants caused by the study, during or within 4 years after the end of the study.
The participant’s general practitioner will be informed about the participation of his/her patient in the study. In case of an incidental finding that could have medical consequences for the participants, the general practitioner will be informed about this finding.
Dissemination policy
The results of this study will be presented at national conferences (for example for general practitioners, orthopaedic specialists, physical therapists and rheumatologists) and at international conferences (eg, the OARSI World Congress on Osteoarthritis). In addition, the results will be disseminated in national and international scientific journals.
Discussion
This pilot observational cohort study will investigate the use of a novel human model, called FOCUM, for the development of OA and other degenerative disorders. The model consists of women who stop OC use at menopausal age (mean menopausal age is 50 to 51, SD±4–5 years).
In general, women in the Netherlands are advised by their general practitioner to stop OC use at the age of 52 as there is only a small chance of pregnancy but an increasing risk of health problems when continuing at a higher age (including venous tromboembolism, ischaemic cardiovascular disease and breast cancer).22 When these women stop OC use, it is expected that menopausal-related changes will occur faster due to a rapid change in hormones. Hopefully, with this study it will be possible to assess what changes occur and which of these changes are associated with the development of OA and other degenerative disorders after 2 years. As far as is known, this type of human model has never been used in prior studies.
A rapid change in hormone levels also occurs after an ovariectomy, but as a human model it is mostly of limited use due to the subsequent start of hormone replacement therapy, a malignancy or its associated treatments (eg, chemotherapy). Animal models are also often used to simulate a rapid change in hormones, but the generalisability to humans is one of the biggest limitations in these models.23
As mentioned before, the model consists of women who stop OC use at menopausal age, so it is expected that the majority of the participating women will enter menopausal status after stopping OC use. But given the range of 4–5 years around the mean menopausal age of 50–51, there will be some participants who will not enter menopausal status during follow-up. For this pilot study, no additional tests are used to ensure that all women enter menopausal state after stopping OC.
Because the FOCUM model has never been used before, little is known about what to expect exactly. Therefore, this model will be used in a pilot study first with a small number of participants and a large range of measurements. With this number of participants it will be difficult to give robust or conclusive results, but the explorative statistics will give us some direction for the future. If this pilot study shows that (1) the study is feasible, meaning that it is possible to include the targeted number of participants and the lost of follow-up at 6 weeks is less than 5% and (2) the model is feasible and promising, it may become possible to obtain extra funding, which can be used to create a more powerful model by adding more participants and in-depth measurements to the study (eg, assessing markers of bone metabolism, arterial stiffness and atherosclerosis of the carotid arteries). In addition, an extension of the number of participants gives the opportunity to investigate other degenerative disorders in more detail as well.
Supplementary Material
Footnotes
Contributors: SMAB-Z, JBJvM, EHGO and EL participated in the initial design of the study. All authors (EM, DS, EHGO, R-JdV, PKB, JBJvM, EL, MCZ, BCJvdE, MK, BWVS, MIBdR-D, SMAB-Z) contributed to the final design of the study. SMAB-Z, DS and EM are coordinating the study and are responsible for the data collection. DS and EM prepared the article. All other authors (EHGO, R-JdV, PKB, JBJvM, EL, MCZ, BCJvdE, MK, BWVS, MIBdR-D, SMAB-Z) have read and approved the final manuscript.
Funding: The study is funded by the Dutch Arthritis Society (ReumaNederland). Grant number: 18-2-204.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review: Not commissioned; externally peer reviewed.
Ethics statements
Patient consent for publication
Not applicable.
References
- 1.VTV-18 . Aandoeningen, 2018. Rijksinstituut voor Volksgezondheid en Milieu (RIVM). Available: https://www.vtv2018.nl/aandoeningen
- 2.Nielen MMJ, MJJC P, Gommer AM. Artrose - Leeftijd en geslacht, 2022. Rijksinstituut voor Volksgezondheid en Milieu (RIVM). Available: https://www.vzinfo.nl/artrose
- 3.Belo JN, Bierma-Zeinstra SMA, Kuijpers T. Niet-traumatische knieklachten, 2016. Nederlands Huisartsen Genootschap (NHG). Available: https://richtlijnen.nhg.org/standaarden/niet-traumatische-knieklachten#volledige-tekst
- 4.de Klerk BM, Schiphof D, Groeneveld FPMJ, et al. No clear association between female hormonal aspects and osteoarthritis of the hand, hip and knee: a systematic review. Rheumatology 2009;48:1160–5. 10.1093/rheumatology/kep194 [DOI] [PubMed] [Google Scholar]
- 5.de Groot IB, Favejee MM, Reijman M, et al. The dutch version of the knee injury and osteoarthritis outcome score: a validation study. Health Qual Life Outcomes 2008;6:16. 10.1186/1477-7525-6-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kroon FPB, Ramiro S, Royston P, et al. Reference curves for the Australian/Canadian hand osteoarthritis index in the middle-aged dutch population. Rheumatology 2017;56:kew483–52. 10.1093/rheumatology/kew483 [DOI] [PubMed] [Google Scholar]
- 7.Wendel-Vos GCW, Schuit AJ, Saris WHM, et al. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J Clin Epidemiol 2003;56:1163–9. 10.1016/S0895-4356(03)00220-8 [DOI] [PubMed] [Google Scholar]
- 8.Heinemann K, Ruebig A, Potthoff P, et al. The menopause rating scale (MRS) scale: a methodological review. Health Qual Life Outcomes 2004;2:45. 10.1186/1477-7525-2-45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Arthritis & Rheumatism 1986;29:1039–49. 10.1002/art.1780290816 [DOI] [PubMed] [Google Scholar]
- 10.Altman R, Alarcón G, Appelrouth D, et al. The American College of rheumatology criteria for the classification and reporting of osteoarthritis of the hand. Arthritis Rheum 1990;33:1601–10. 10.1002/art.1780331101 [DOI] [PubMed] [Google Scholar]
- 11.National Clinical Guideline Centre (UK) . Osteoarthritis: care and management in adults, 2014 [PubMed]
- 12.van der Heijden RA, Rijndertse MM, Bierma-Zeinstra SMA, et al. Lower pressure pain thresholds in Patellofemoral pain patients, especially in female patients: a cross-sectional case-control study. Pain Med 2018;19:184–92. 10.1093/pm/pnx059 [DOI] [PubMed] [Google Scholar]
- 13.Altman RD, Gold GE. Atlas of individual radiographic features in osteoarthritis, revised. Osteoarthritis Cartilage 2007;15 Suppl A:A1–56. 10.1016/j.joca.2006.11.009 [DOI] [PubMed] [Google Scholar]
- 14.Botha-Scheepers S, Riyazi N, Watt I, et al. Progression of hand osteoarthritis over 2 years: a clinical and radiological follow-up study. Ann Rheum Dis 2009;68:1260–4. 10.1136/ard.2008.087981 [DOI] [PubMed] [Google Scholar]
- 15.Bijsterbosch J, Haugen IK, Malines C, et al. Reliability, sensitivity to change and feasibility of three radiographic scoring methods for hand osteoarthritis. Ann Rheum Dis 2011;70:1465–7. 10.1136/ard.2010.143479 [DOI] [PubMed] [Google Scholar]
- 16.Hunter DJ, Guermazi A, Lo GH, et al. Evolution of semi-quantitative whole joint assessment of knee oa: moaks (MRI osteoarthritis knee score). Osteoarthritis Cartilage 2011;19:990–1002. 10.1016/j.joca.2011.05.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Runhaar J, Schiphof D, van Meer B, et al. How to define subregional osteoarthritis progression using semi-quantitative MRI osteoarthritis knee score (MOAKS). Osteoarthritis Cartilage 2014;22:1533–6. 10.1016/j.joca.2014.06.022 [DOI] [PubMed] [Google Scholar]
- 18.Hunter DJ, Arden N, Conaghan PG, et al. Definition of osteoarthritis on MRI: results of a Delphi exercise. Osteoarthritis Cartilage 2011;19:963–9. 10.1016/j.joca.2011.04.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.van Schie HTM, de Vos RJ, de Jonge S, et al. Ultrasonographic tissue characterisation of human Achilles tendons: quantification of tendon structure through a novel non-invasive approach. Br J Sports Med 2010;44:1153–9. 10.1136/bjsm.2009.061010 [DOI] [PubMed] [Google Scholar]
- 20.de Vos RJ, Weir A, Tol JL, et al. No effects of PRP on ultrasonographic tendon structure and neovascularisation in chronic midportion achilles tendinopathy. Br J Sports Med 2011;45:387–92. 10.1136/bjsm.2010.076398 [DOI] [PubMed] [Google Scholar]
- 21.Runhaar J, van Middelkoop M, Reijman M, et al. Prevention of knee osteoarthritis in overweight females: the first preventive randomized controlled trial in osteoarthritis. Am J Med 2015;128:888–95. 10.1016/j.amjmed.2015.03.006 [DOI] [PubMed] [Google Scholar]
- 22.Barnhoorn PC, Bruinsma ACA, Bouma M. Anticonceptie, 2020. Nederlands Huisartsen Genootschap (NHG). Available: https://richtlijnen.nhg.org/standaarden/anticonceptie#volledige-tekst
- 23.Sniekers YH, Weinans H, Bierma-Zeinstra SM, et al. Animal models for osteoarthritis: the effect of ovariectomy and estrogen treatment - a systematic approach. Osteoarthritis Cartilage 2008;16:533–41. 10.1016/j.joca.2008.01.002 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.