

Abstract
Ossification of the anterior longitudinal ligament (OALL) in the cervical spine is a common entity but rarely causes dysphagia, dyspnea, and dysphonia. We report an OALL case which causes such symptoms. A 47-year-old female patient had a complaint of progressive difficulty swallowing for 2 months. A cervical X-ray and computerized tomography scan were taken afterward, which showed OALL at the C3–7 level. She then had esophageal endoscopy to rule out other dysphagia-related disorders. The patient underwent anterior osteotomy via anterior cervical approach with significant relief of dysphagia postoperatively. Surgical management in symptomatic OALL improves dysphagia and prevents its secondary complications.
Keywords: ossification of the anterior longitudinal ligament (OALL), diffuse idiopathic skeletal hyperostosis (DISH), dysphagia, cervical
Introduction
Hypertrophic abnormalities and osteophytes, including ossification of the anterior longitudinal ligament (OALL), could be found in degenerative cervical spine or diffuse idiopathic skeletal hyperostosis (DISH), also known as Forestier's disease. 1 DISH is a noninflammatory joint disorder characterized by calcification and ossification of spinal ligaments and entheses, resulting in the development of osteophytes across the anterolateral side of the spine. DISH is diagnosed by ossification along the anterior aspect of at least four adjacent vertebrae without obvious signs of the involved intervertebral disc or apophyseal degenerative modification, and absence of facet joint ankylosis. 2
Its incidence ranges from 20 to 30% of the elderly population, but the disease rarely produces dysphagia. 3 The dysphagia caused by cervical OALL, although not commonly seen, is a primary complaint especially when osteophytes are extraordinarily large. 2 The ideal solution of symptomatic OALL remains controversial. While the majority of patients have been successfully managed by observation and medication, a surgical approach also shows benefits on some occasions. 4
This study illustrates an uncommon cervical OALL case causing dysphagia without any evidence of comorbid ossification of the posterior longitudinal ligament. The patient has made a successful recovery after the osteotomy. We will focus on the diagnostic criteria and the management strategy of this entity.
Case Presentation
A 47-year-old female was brought to the hospital with a complaint of solid food swallowing difficulty for 2 months. She denied hoarseness, dyspnea, sore throat, acid reflux, or unintentional weight loss. She did not have any neurological deficits. The blood work result was noncontributory.
The lateral view of the cervical spine radiograph revealed an extensive and continuous calcification area at the anterior longitudinal ligament along the anterolateral aspect of vertebral bodies from C3 to C7 ( Fig. 1A ). The three-dimensional reconstructed computerized tomography (CT) scan of the cervical spine showed OALL at C3-C7 vertebral levels ( Fig. 2 ).
Fig. 1.
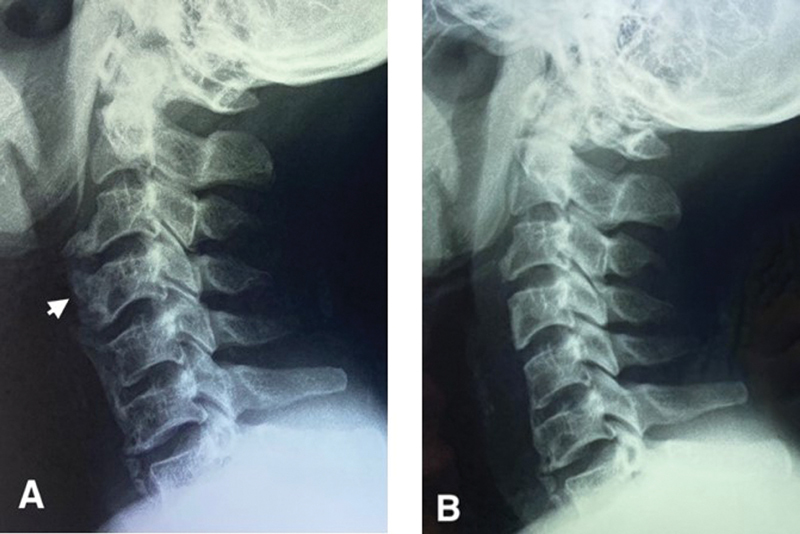
( A ) The preoperation lateral plain radiograph showed an extensive calcification extent from C3 to C7 ( arrow ). ( B ) Postoperation image revealed the calcifications were removed almost totally.
Fig. 2.
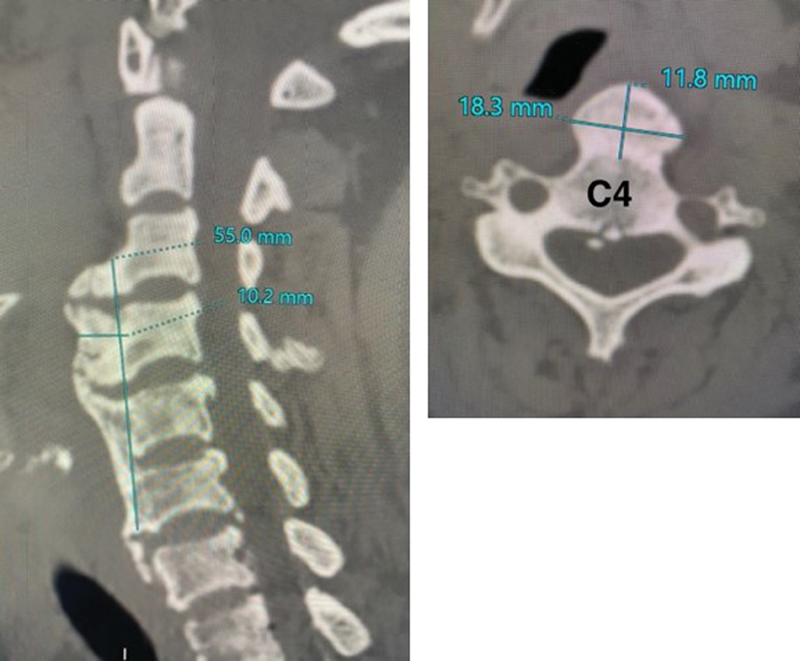
Cervical computed tomography (CT) scan showed the calcification at anterolateral aspect of C3-C7.
The esophageal endoscopy demonstrated the protrusion of the posterior pharyngeal wall causing partial obstruction of the esophageal inlet and deviating the esophagus toward the right ( Fig. 3 ). Also, there was no evidence of intrinsic lesions within the esophageal lumen. The barium radiography has also yielded the same impression.
Fig. 3.
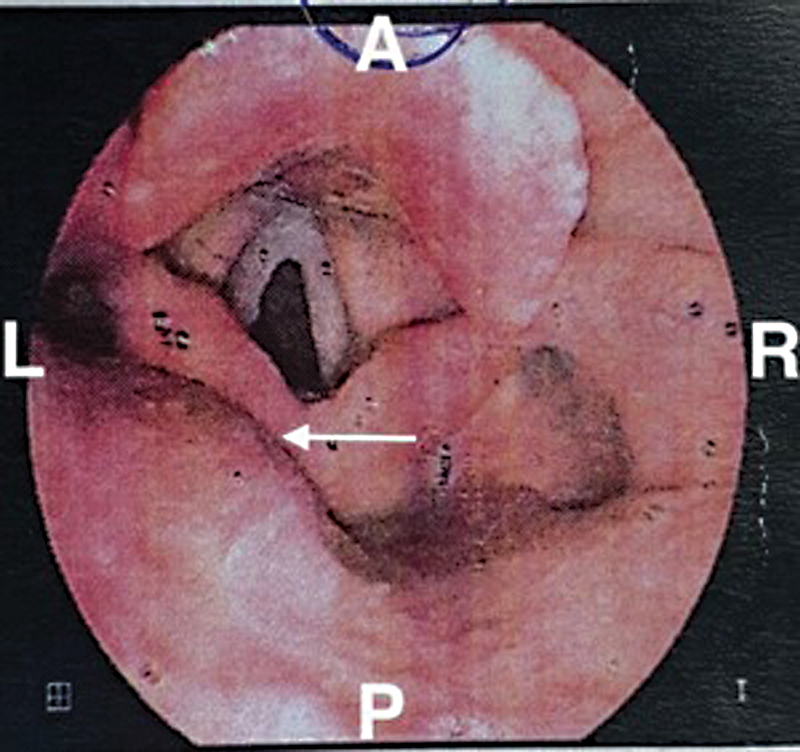
The esophageal endoscopy revealed the ossification of the anterior longitudinal ligament (OALL) protruded the posterior pharyngeal wall from the left ( arrow ).
The patient was diagnosed with OALL complicated with an esophageal stricture. She consequently underwent a left-sided anterior cervical approach to the spine. Intraoperatively, we confirmed the esophagus had been pushed toward the right side by a large OALL at C3-C6 vertebral levels. Fortunately, there was no adhesion between the esophagus and OALL; hence, we could retract the esophagus to the right quite easily. The OALL was largely removed with an osteotome and then smoothed using a high-speed drill under operative microscope magnification ( Fig. 4 ). The histological result was chronic ligamentitis with osteochondral metaplasia ( Fig. 5 ).
Fig. 4.
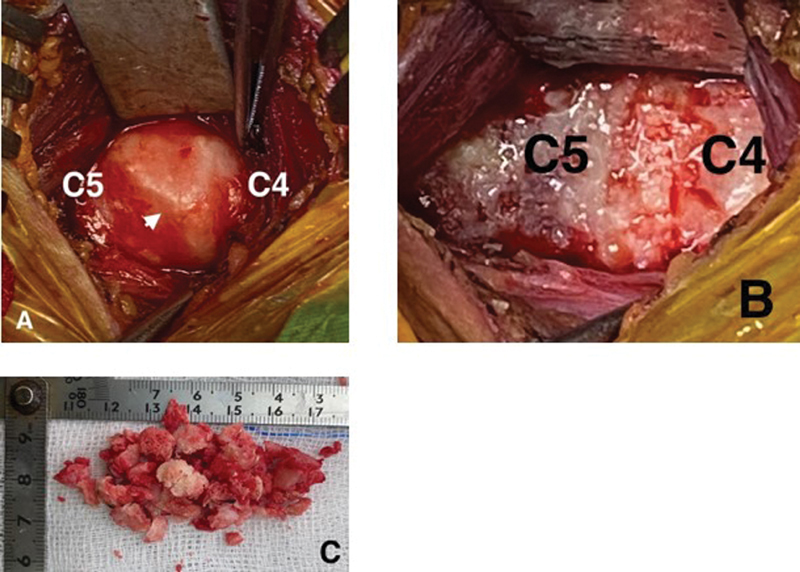
Intraoperation images. ( A ) The ossification of the anterior longitudinal ligament (OALL) ( arrow ), ( B ) the ossification was taken out, ( C ) the calcification.
Fig. 5.
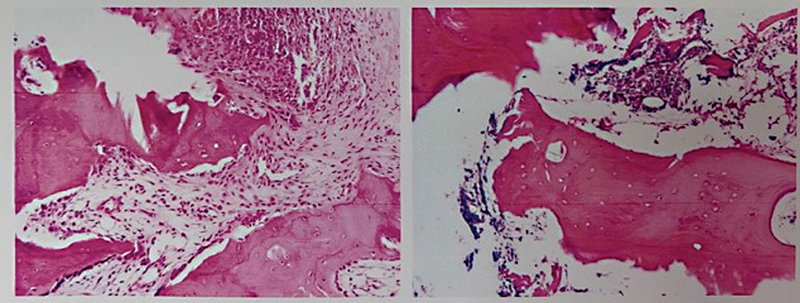
Histological result was chronic ligamentitis with osteochondral metaplasia.
The patient has experienced an improvement in swallowing since the second day after surgery. The postoperative radiograph showed the OALL has been near-complete removed ( Fig. 1B ).
Discussion
Osteophyte and cervical OALL originating from degenerative changes are usually asymptomatic. The most common symptom in symptomatic OALL is progressive dysphagia with solid food. In severe cases, patients can even experience difficulty swallowing liquids. Malnutrition and severe weight loss have been frequently reported with this entity. 5
Upper respiratory tract compression may lead to dyspnea, stridor, and cough. Other sequelae include musculoskeletal and neurological symptoms, sleep apnea, aspiration pneumonia, and sudden death due to complete airway obstruction. 3 There are several etiologies potentially leading to the dysphagia sequelae in addition to a direct esopharyngeal compression. 4 In OALL, dysphagia related to an osteophyte can be explained by various mechanisms, including: (1) the esophageal lumen being compressed by a huge osteophyte; (2) periesophageal edema from the physical irritation by osteophytes; (3) a small osteophyte but crucially located at the fixed segment of the esophagus; (4) pain and muscle spasm from the irritation; and (5) the combination of any of those above mechanisms. 3 In our case, there was no significant adhesion between the OALL and the esophagus, representing a noninflammatory esophageal compression.
A plain radiograph and CT scan can efficiently detect and differentiate OALL caused by DISH from those caused by degenerative osteophytes. 6 DISH is known as one of the most frequent causes of anterior cervical hyperosteophytosis resulting in dysphagia that requires surgical management. 7 8 Carlson et al reported that 3% of the population over 40 years of age have DISH and 0.1 to 6% of them will develop dysphagia. 9 In this case, we made a diagnosis of DISH because the CT imaging of our patient showed the mixture of globular OALL with a beak-like projection at the C3-5 level, and the C5-T2 vertebral bodies were fused by the anterior osteophyte, the disc height has been relatively preserved, and facet joints were not ankylosis.
Esophageal endoscopy has an important role in ruling out other dysphagia-related casualties such as cancer, neurological deficit, diverticula, pharyngeal, or esophageal stenosis. 10 If lateral video fluoroscopy or esophageal endoscopy suggests evidence of pharyngeal compression, CT imaging is recommended to further investigate potential OALL and other disturbances.
The management of dysphagia in cervical OALL includes medication-based or surgical approaches. We can reasonably postpone treatment in asymptomatic patients. In patients with mild dysphagia, swallowing therapy and anti-inflammatory agents may be beneficial to control the symptoms and decrease the risk of aspiration. 2 3 However, patients may need surgery when these conservative treatments are ineffective or the osteophytes enlarge significantly. A recent review article reported that only 35 (20.7%) of 169 OALL cases were treated by nonoperative methods. 11 Surgical interventions were used for the rest of the cases and the most common operative technique was removing ossification without spinal fusion. 11 In severe cases, OALL removal may instantly resolve dysphagia. However, taking the ossification area out alone portends the long-term risk of spinal instability and does not prevent recurrence in the future. 12 In symptomatic patients, especially those with a mechanical obstruction, timely surgical management would tremendously cease the chronic inflammatory and local fibrosis process. A delayed intervention may result in a less responsive outcome. 4
Complications regarding the anterior approach for osteophyte resection include vocal cord palsy, Horner syndrome, and esophageal/tracheal perforation or fistula. 7
A thorough evaluation should be conducted on any patient with dysphagia. Other etiologies of this problem except cervical OALL include tumors in the esophagus, lungs, or larynx, esophageal motility disorders, esophageal webs, benign strictures, esophagitis, and infections. 3 Physicians should always indicate esophageal and laryngeal endoscopy to precisely rule out other causes of dysphagia in patients with OALL; otherwise, a misdiagnosis could lead to disastrous sequelae. Valadka et al reported a 68-year-old male presenting with severe dysphagia, which was initially being concluded as a complication of cervical OALL; the patient then has been through a surgical resection without any symptom improvement postoperatively. Ten days later, the laryngoscopy showed a friable mass in the right vallecula, which turned out to be squamous cell carcinoma. 13 Again, cervical OALL should only be confirmed after eliminating all other potential differential diagnoses.
Conclusion
We suggest evaluating cervical X-rays of patients with dysphagia when we could not find any causes coming from the gastrointestinal system. Nevertheless, cervical OALL is an exclusive diagnosis and can only be confirmed after a detailed investigation. In patients with severe symptoms or in those who have failed with medication-based treatment, early osteophyte resection yields a promising outcome.
Funding Statement
Funding None.
Footnotes
Conflict of Interest None declared.
References
- 1.Resnick D, Shaul S R, Robins J M. Diffuse idiopathic skeletal hyperostosis (DISH): Forestier's disease with extraspinal manifestations. Radiology. 1975;115(03):513–524. doi: 10.1148/15.3.513. [DOI] [PubMed] [Google Scholar]
- 2.Hwang J S, Chough C K, Joo W I. Giant anterior cervical osteophyte leading to dysphagia. Korean J Spine. 2013;10(03):200–202. doi: 10.14245/kjs.2013.10.3.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kim S B, Oh S H, Yi H J. Dysphasia caused by ossification of the cervical anterior longitudinal ligament. J Korean Neurosurg Soc. 2003;34:474–476. [Google Scholar]
- 4.Sundeep M, Hirano Y, Iketani S, Konno A. Surgical management of symptomatic ossified anterior longitudinal ligament: a case report. Surg Neurol Int. 2017;8:108. doi: 10.4103/sni.sni_102_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chen Y-R, Sung K, Tharin S. Symptomatic anterior cervical osteophyte causing dysphagia: case report, imaging, and review of the literature. Cureus. 2016;8(02):e473. doi: 10.7759/cureus.473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Song J, Mizuno J, Nakagawa H.Clinical and radiological analysis of ossification of the anterior longitudinal ligament causing dysphagia and hoarseness Neurosurgery 20065805913–919., discussion 913–919 [DOI] [PubMed] [Google Scholar]
- 7.Oppenlander M E, Orringer D A, La Marca F.Dysphagia due to anterior cervical hyperosteophytosis Surg Neurol 20097203266–270., discussion 270–271 [DOI] [PubMed] [Google Scholar]
- 8.Calisaneller T, Ozdemir O, Tosun E, Altinors N.Dysphagia due to diffuse idiopathic skeletal hyperostosis Acta Neurochir (Wien) 2005147111203–1206., discussion 1206 [DOI] [PubMed] [Google Scholar]
- 9.Carlson M L, Archibald D J, Graner D E, Kasperbauer J L. Surgical management of dysphagia and airway obstruction in patients with prominent ventral cervical osteophytes. Dysphagia. 2011;26(01):34–40. doi: 10.1007/s00455-009-9264-6. [DOI] [PubMed] [Google Scholar]
- 10.Fattori B, Giusti P, Mancini V. Comparison between video fluoroscopy, fiberoptic endoscopy and scintigraphy for diagnosis of oro-pharyngeal dysphagia. Acta Otorhinolaryngol Ital. 2016;36(05):395–402. doi: 10.14639/0392-100X-829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Verlaan J J, Boswijk P F, de Ru J A, Dhert W J, Oner F C. Diffuse idiopathic skeletal hyperostosis of the cervical spine: an underestimated cause of dysphagia and airway obstruction. Spine J. 2011;11(11):1058–1067. doi: 10.1016/j.spinee.2011.09.014. [DOI] [PubMed] [Google Scholar]
- 12.Miyamoto K, Sugiyama S, Hosoe H, Iinuma N, Suzuki Y, Shimizu K. Postsurgical recurrence of osteophytes causing dysphagia in patients with diffuse idiopathic skeletal hyperostosis. Eur Spine J. 2009;18(11):1652–1658. doi: 10.1007/s00586-009-1133-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Valadka A B, Kubal W S, Smith M M. Updated management strategy for patients with cervical osteophytic dysphagia. Dysphagia. 1995;10(03):167–171. doi: 10.1007/BF00260972. [DOI] [PubMed] [Google Scholar]