

Abstract
Many adolescents experience or witness aggression by peers at school. The purpose of the current study was to examine associations between exposure to peer aggression (i.e., peer victimization and witnessing school violence) and sleep problems and whether these associations are moderated by parental acceptance. Participants included 272 adolescents attending high school (M age = 17.27 years; 49% female; 59% White/European American, 41% Black/African American). Adolescents reported on exposure to peer aggression, parental acceptance, and two key sleep domains: sleep quality problems and daytime sleepiness. Results indicated that exposure to peer aggression was directly associated with poor sleep quality and sleepiness. Furthermore, peer victimization and witnessing school violence interacted with parental acceptance to predict sleep quality. Specifically, exposure to peer aggression was associated with sleep quality problems at higher (but not lower) levels of parental acceptance. The lowest levels of sleep quality problems were apparent at low levels of peer aggression and high levels of parental acceptance, but parental acceptance did not protect adolescents with high exposure to peer aggression against sleep problems. Findings illustrate the importance of considering moderators of effects and the conjoint roles of family and peer processes when considering individual differences in adolescents’ sleep. Future research should examine whether parental strategies targeted to address peer victimization are protective against the detrimental effects of exposure to peer aggression.
Keywords: peer victimization, school violence, parental acceptance, sleep, sleepiness
Exposure to peer aggression at school (i.e., experiencing or witnessing peer victimization) is prevalent among adolescents (Basch, 2011), with one study reporting that over half of adolescents experienced peer victimization in the past year (Salmon et al., 2018). Exposure to school violence is consistently associated with poor academic outcomes (Basch, 2011), and meta-analyses show that peer victimization robustly predicts internalizing (Hawker & Boulton, 2000) and externalizing (Reijntjes et al., 2011) problems. Although less is known about the impact of exposure to peer aggression on adolescents’ sleep, research has increased over the past decade, and a recent meta-analysis documented links between peer victimization and sleep problems among children and adolescents (van Geel et al., 2016).
According to Dahl’s (1996) sleep-arousal framework, sleep and vigilance are opposing regulatory processes. Sleep requires attenuation of arousal and responsiveness to the environment and can be disrupted under threatening conditions that evoke vigilance. Social experiences are salient environmental circumstances that enable or undermine the sense of safety that facilitates sleep (Worthman & Melby, 2002). Peer victimization leads to emotional distress (Nishina & Juvonen, 2005) as well as increased physiological arousal and dysregulation of stress response systems (Murray-Close, 2013), which could disrupt sleep. The connection between peer victimization and sleep may be particularly strong during adolescence when concerns about peer experiences escalate (Parker et al., 2006) and developmental changes in the sleep-arousal regulatory system occur (Crowley et al., 2018).
Although growing evidence suggests that being the victim of peer aggression is associated with sleep problems (e.g., Lepore & Kliewer, 2013; Tu et al., 2019), no known studies have examined associations between witnessing peer aggression and sleep among youth, despite that witnessing violence is much more common than experiencing violence as a victim (Lepore & Kliewer, 2013). Witnessing and directly experiencing peer victimization are both associated with poorer adjustment, yet each mode may have distinct effects (Nishina & Juvonen, 2005), and the effects of personal victimization on adjustment may be attenuated when youth witness the victimization of others (Schacter & Juvonen, 2019). Although no known study has examined the impact of witnessing school violence on sleep, witnessing community violence has uniquely predicted sleep problems, beyond the effects of victimization in the community (Kliewer & Lepore, 2015). Toward a more extensive assessment of relations between modes (i.e., experiencing or witnessing) of exposure to peer aggression and sleep, the current study examined whether witnessing violence in school and experiencing peer victimization is associated with sleep problems among adolescents.
In addition to a need to examine modes of exposure to peer aggression, the existing literature on relations between peer aggression and sleep is restricted by limited assessments of sleep. Although a few studies have adopted multi-item measures of sleep quality (e.g., Tu et al., 2019), much of the existing research has utilized single-item assessments of sleep (van Geel et al., 2016). Individual items do not always correlate with more established measures of sleep (Spruyt & Gozal, 2011), and assessment of multiple sleep parameters with established measures is critical to better understand the relation between sleep and youth adjustment (Sadeh, 2015).
Building on this literature, we examined two key sleep domains: sleep–wake problems and sleepiness. Sleep–wake problems are also referred to as sleep quality problems and include difficulties with falling asleep, maintaining sleep, and waking in the morning. Sleep quality problems are common among adolescents (Gradisar et al., 2011) and are associated with many salient indices of adjustment including internalizing symptoms (Palmer et al., 2018), externalizing problems (Denis et al., 2017), and poor school performance (Adelantado-Renau et al., 2019). Sleepiness involves struggling to stay awake or falling asleep during daily activities. Sleep–wake problems and sleepiness are related yet distinct constructs that frequently show differential associations with various developmental outcomes. Daytime sleepiness increases during adolescence, irrespective of the quality and duration of nighttime sleep (Campbell et al., 2007). Like sleep quality problems, sleepiness is associated with internalizing and externalizing outcomes (Shimizu et al., 2020), and sleepiness may be more strongly associated with academic and cognitive functioning than sleep quality or duration (Philbrook et al., 2018). Notably, concerns about community violence were associated with higher levels of sleepiness (Bagley et al., 2016), yet research is needed to determine whether exposure to peer aggression at school is associated with adolescents’ daytime sleepiness.
Parental Acceptance as a Protective Factor
Given emerging evidence of a relationship between exposure to peer aggression and sleep, it is important to investigate potential moderating factors to explicate for whom and under which conditions peer aggression may be associated with sleep. Parental acceptance refers to parental expressions of affection and enjoyment and appreciation of their child (Schaefer, 1965). Parental acceptance and closely related constructs (e.g., warmth and closeness) are robust predictors of psychological adjustment, including higher self-worth and emotional stability (Khaleque, 2013). Parental acceptance may provide protection in the context of peer victimization by fostering adolescents’ feelings of worth and belongingness as well as their receptivity to parental support and guidance (Gregson et al., 2016).
Although parental acceptance specifically has not been examined as a protective factor in associations between peer victimization and adolescents’ well-being, studies that have examined similar constructs have provided mixed evidence. For instance, studies of community violence have shown that parental acceptance generally does not buffer against the effects of violence exposure (Davis et al., 2015), although one study found that high levels of parental acceptance protected youth with low levels of violence exposure from internalizing symptoms (Kliewer et al., 2004). Studies of peer aggression have not examined parental acceptance per se, but an examination of similar parenting constructs has yielded inconsistent results. High-quality parent–child relationships can attenuate the association between peer victimization and depressive symptoms and antisocial behavior (Rudolph et al., 2020). Although some studies have failed to find a protective effect of parental support (defined by parental warmth and involvement; Burke et al., 2017), other evidence suggests that parental support may mitigate general mental health problems (Stadler et al., 2010) as well as internalizing symptoms (Thompson & Leadbeater, 2013), though the effects varied across adolescent age and gender. Only one known study has examined whether a form of parental support moderates the association between exposure to peer aggression and sleep. Morin et al. (2015) found that youths’ perceptions of parents’ engagement in school activities interacted with peer victimization to predict sleep problems (examined with a two-item scale), and the pattern of effects demonstrated that parental engagement was associated with fewer sleep problems among youth with low, but not high, levels of peer victimization.
The Current Study
We examined relations between exposure to peer aggression and sleep problems, and the role of parental acceptance as a moderator of these associations. We assessed whether associations were corroborated across two modes of exposure—direct victimization and witnessing school violence. To more fully examine a range of severity of peer victimization experiences, we created a composite measure of peer victimization that encompasses relational and verbal victimization, as well as both mild and severe forms of physical victimization. Witnessed school violence refers to seeing a peer physically victimized or threatened with physical harm at school. We examined effects across two important dimensions of adolescent sleep–wake processes: sleep quality problems (i.e., difficulty falling or staying asleep or trouble waking in the morning) and sleepiness (i.e., difficulty staying awake during daily activities), which we collectively refer to as sleep problems. Given associations between anxiety and both peer victimization (Hawker & Boulton, 2000) and sleep (Palmer et al., 2018), we controlled for anxiety in all main analyses. We hypothesized that each mode and type of exposure to peer aggression would be associated with more sleep–wake problems and more sleepiness. Furthermore, we expected that parental acceptance would serve as a moderator of risk and attenuate the associations between exposure to peer aggression and sleep problems.
Method
Participants
Data for the current study come from a larger, longitudinal study that focuses on sleep and health of youth (Auburn University Sleep Study). Most adolescents (62%) were recruited through previous waves of data collection, and 38% of adolescents participated for the first time at the current wave. Recruitment strategies were the same in both cases; letters requesting participation in an investigation of sleep, development, and health were sent home with students at school. All participants were recruited from the same school districts in small towns and semirural communities in the southeastern United States. Exclusion criteria included a parental report of a diagnosed sleep or learning disorder. For more information regarding recruitment and the initial waves of the study, see El-Sheikh et al. (2020). A sample of 323 adolescents and their families participated in the current wave, which occurred during the academic school year of 2017–2018. Only participants who were physically attending high school (84%) were included in the analytic sample to reduce potential confounds associated with sleep–wake schedules; one Latino participant was excluded given the larger study aims of examining sleep among White/European American (EA) and Black/African American (AA) youth.
The final analytic sample includes 272 high school students (51% male; M age = 17.27 years, SD = 0.76; 59% EA, 41% AA). African American youth were oversampled to address the aims of the larger study, and thus the racial composition of our sample reflects a somewhat higher percentage of AA and a lower percentage of EA adolescents than those represented in their community (65% EA, 30% AA). According to their families’ income-to-needs ratio (US Department of Commerce, 2019), 16% of participants were living in poverty (income-to-needs ratio ≤1), 19% were near the poverty line, 19% were lower middle class, and 46% were middle class. Approximately 63.6% of adolescents were living with two parents, 27.9% lived primarily with mom, 3.3% primarily with dad, 2.6% spent equal time with both parents, 2.2% lived with a grandparent or other guardian, and one participant (0.4%) lived with a fiancé.
Procedure
Following approval by Auburn University’s Institutional Review Board, consent from parents or guardians and adolescent assent were obtained. Adolescents received a Qualtrics link via email and completed the questionnaires online at home or in a university lab. Parents reported on demographic variables during a brief phone interview at the time of enrollment.
Measures
Exposure to Peer Aggression
To assure inclusion of a wide range of victimization experiences, a composite of two measures was used to assess peer victimization. Adolescents completed eight items from the Social Experiences Questionnaire (SEQ; Crick & Grotpeter, 1996), which assesses the frequency of various victimization experiences at school. Specifically, five items assess the frequency of relational victimization by peers (e.g., “left out on purpose when it’s time to do an activity”; “told lies about you to make other kids not like you anymore”), and three items assess the frequency of overt (i.e., verbal and mild physical) victimization (“other kids tease or make fun of you”; “get pushed or shoved by other peers at school”). The SEQ has been established as a reliable and valid measure of peer victimization in adolescence (Storch et al., 2005). Adolescents rated how often each experience occurred at school on a 5-point scale (1 = almost never to 5 = almost always). No time frame was specified for this measure. Internal consistency in the current sample was good (α = .87), and items were summed to form a peer victimization score.
Adolescents also completed the Recent Exposure to Violence Scale (REVS; Van Dulmen et al., 2008), which assesses violence exposure at home, at school, and in the neighborhood over the past year. Following Spilsbury et al. (2014), additional questions were added to specify the context of violence across all items. Five items assessed being a victim of school violence (“Have you been beaten up at school?”; “Have you yourself been slapped, punched, or hit by someone at school?”; “Did anyone at school tell you they were going to hurt you?”; “Have you yourself been attacked or stabbed with a knife at school?”; “Has someone pointed a real gun at you at school?”). Adolescents reported the frequency of victimization at school on a 4-point scale (1 = never, 2 = sometimes, 3 = often, 4 = almost every day). Items were summed to form a victim of school violence subscale (α = .76). The SEQ peer victimization and REVS school victimization scores were each standardized and averaged to form a Peer Victimization composite; higher scores reflect higher levels of peer victimization.
Adolescents reported the frequency of witnessing school violence via five analogous items on the REVS (e.g., “Have you seen someone else getting beat up at school?”; “Have you seen someone else being slapped, punched, or hit by someone at school?”) using the same 4-point scale (1 = never to 4 = almost every day). Items were summed to form a Witnessed School Violence composite (α = .72); higher scores reflect higher levels of witnessed school violence.
Parental Acceptance
Adolescents completed the Acceptance subscales of the Parental Behavior Inventory (Schaefer, 1965). The eight-item subscales for mothers and fathers were examined (e.g., “seems to see my good points more than my faults”; “enjoys going on drives, trips, or visits with me”; “has a good time at home with me”; “makes me feel better after talking over my worries with her/him”). Participants reported the similarity of the items to their parents’ behavior on a 3-point scale (1 = not like to 3 = like). Within families, mothers’ and fathers’ levels of acceptance are similarly rated by adolescents and have similar effects on adjustment (Miranda et al., 2016). The acceptance subscales for mothers and fathers in the current study were correlated (r = .52, p < .001) and averaged to form a Parental Acceptance composite, which demonstrated excellent internal consistency (α = .93). Higher scores index higher levels of acceptance. Participants were asked to complete the scales for their fathers and mothers (or in a few instances primary male and female caregivers), even if they were not living with both parents. For the 14 participants (5.1%) who reported on just one parent, only responses for the one parent were used. Sensitivity analyses excluding these cases revealed no appreciable differences from the reported results.
Sleep Problems
Adolescents completed the School Sleep Habits Survey (Wolfson & Carskadon, 1998), which has excellent reliability and validity (Lewandowski et al., 2011; Wolfson et al., 2003). Two scales were used: sleep–wake problems and sleepiness. The sleep–wake problems scale consists of 10 items that assess the frequency of difficulties with initiating and maintaining sleep at night and waking in the morning over the past 2 weeks (e.g., “had an extremely hard time falling asleep”; “needed more than 1 reminder to get up in the morning”; “fallen asleep in a morning class”). Responses were scored on a 5-point scale (1 = never to 5 = every day).
The sleepiness scale includes nine items that measure whether participants have struggled to stay awake during various activities over the past 2 weeks (e.g., “watching T.V. or listening to music”; “in a class at school”). Because many adolescents were not driving, one item regarding sleepiness while driving was not administered. Responses were scored on a 4-point scale (1 = did not struggle to stay awake to 4 = both struggled to stay awake and fell asleep) and were summed to derive the sleepiness score. Internal consistency was good for both scales (α = .83 and .84 for sleep–wake problems and sleepiness, respectively).
Covariates
Parents reported on adolescents’ sex, race, and age, as well as family income and the number of people living in the household, which was used to calculate the income-to-needs ratio, an index of the family’s socioeconomic status (SES; US Department of Commerce, 2019). Adolescents completed the 40-item Revised Children’s Manifest Anxiety Scale (Reynolds & Richmond, 2008), which assesses whether adolescents felt anxious in various situations (0 = no, 1 = yes). Five items pertaining to sleep problems were removed before responses were summed to yield an anxiety composite (α = .94). Initial analyses controlled for depressive symptoms, but they were not correlated with sleep and their inclusion did not meaningfully change the results.
Analysis Plan
A series of four regression models were fit to examine the moderating role of parental acceptance in the associations between both peer victimization and witnessing school violence and each sleep domain (sleep–wake problems and sleepiness). All analyses are cross-sectional, and thus predict is used in the statistical, rather than the causal, sense. The predictor, moderator, and covariates were mean-centered before creating interaction terms so that the intercept has a meaningful value. Exogenous variables (predictor, moderator, interaction term, and control variables) were allowed to covary. Statistically significant (p < .05) interactions were plotted at high and low (±1 SD) levels of parental acceptance, and simple slope analyses were conducted to probe significant interactions. Further, the regions of significance on X were identified (Roisman et al., 2012) to determine the regions of each predictor over which parental acceptance was associated significantly with each outcome.
All models were fit in Mplus Version 8 (Muthén & Muthén, 2017). Data that exceeded 4 SDs above or below the mean were winsorized (i.e., recoded to the value corresponding to 4 SDs; Cousineau & Chartier, 2010), including three peer victimization scores, one witnessed school violence score, two sleepiness scores, and two SES scores. Mplus uses full information maximum likelihood (FIML) estimation to handle missing data, which produces less biased estimates and lower Type I error rates than other methods for handling missing data (Raykov, 2005). Missingness for study variables ranged from 0% to 20.2%, which is within the acceptable range for use of FIML with the current sample size (McNeish, 2017). Models were fully saturated, and thus model fit is not reported.
Results
Preliminary Analyses and Descriptive Statistics
Table 1 presents the means, standard deviations, and correlations among all study variables. There were no sex differences in any of the primary variables. Exposure to peer aggression did not differ by race, yet AA adolescents (M = 22.88, SD = 8.81) reported more sleep–wake problems than EA adolescents (M = 20.45, SD = 6.98; t = −2.37, p < .05). Each mode of exposure to peer aggression was positively correlated with sleep–wake problems and sleepiness. Peer victimization and sleep–wake problems were negatively associated with parental acceptance.
Table 1.
Means, Standard Deviations, and Correlations Among Study Variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| 1. Sex | ||||||||||
| 2. Race | .01 | |||||||||
| 3. Age | .12 | −.06 | ||||||||
| 4. SES | .03 | −.42*** | .11 | |||||||
| 5. Anxiety | −.23*** | −.19** | −.04 | −.02 | ||||||
| 6. Peer Victimization | .10 | .08 | .04 | −.11 | .34*** | |||||
| 7. Witnessed School Violence | .13 | .00 | −.08 | −.06 | .26*** | .61*** | ||||
| 8. Parental Acceptance | −.01 | −.10 | .05 | .12 | −.20** | −.15* | −.04 | |||
| 9. Sleep-Wake Problems | −.06 | .15* | .03 | −.25*** | .38*** | .28*** | .24*** | −.28*** | ||
| 10. Sleepiness | .04 | .06 | .01 | −.08 | .28*** | .34*** | .43*** | −.12 | .45*** | |
|
| ||||||||||
| Mean | — | — | 17.27 | 2.90 | 10.16 | 0.00 | 6.32 | 18.62 | 21.43 | 14.35 |
| SD | — | — | 0.76 | 1.82 | 8.43 | 0.84 | 1.90 | 4.27 | 7.84 | 4.44 |
Note. N = 272. Sex was coded as 0 = female, 1 = male; race was coded as 0 = White/EA, 1 = Black/AA. SES = socioeconomic status (income-to-needs ratio).
p < .05.
p < .01.
p < .001.
Regarding exposure to peer aggression, 45% of adolescents reported relational or mild overt victimization via the SEQ (i.e., more than “almost never” on at least one item), 20% reported being a victim of school violence via the REVS (i.e., more than “never” on at least one item), and 47% reported witnessing at least one instance of violence at school. A small percentage of adolescents reported experiencing the most serious (i.e., weapon-involved) forms of peer aggression as either a victim (knife attack, 2.3%; had a gun pointed at them, 1.8%) or a witness (knife, 3.2%; gun, 1.4%). Regarding sleep problems, the majority of adolescents (86%) reported sleepiness in at least one context, and 92% reported at least one sleep–wake problem in the past 2 weeks. On average and based on adolescent self-report, adolescents went to sleep at 10:55 p.m. and woke up at 6:57 a.m. Adolescents slept for an average of 7 hr and 59 min per night (SD = 67 min), not accounting for awakenings during the night.
Primary Analyses
Sleep–Wake Problems
As shown in Table 2, regression models indicated that peer victimization and parental acceptance each significantly predicted sleep–wake problems. Further, peer victimization interacted with parental acceptance to predict sleep–wake problems. As shown in Figure 1a, simple slope analyses revealed that the association between peer victimization and sleep–wake problems was significant among adolescents with higher but not lower levels of parental acceptance. At lower levels of peer victimization, adolescents who reported high levels of acceptance had lower sleep–wake problems (predicted M = 17.46) compared to adolescents who reported low levels of acceptance (predicted M = 22.95), a difference of 0.70 SD. At higher levels of peer victimization, adolescents reported relatively high levels of sleep–wake problems regardless of parental acceptance. Regions of significance on X showed that acceptance was negatively associated with sleep–wake problems at peer victimization scores of 0.36 SDs above the mean and lower.
Table 2.
Sleep Regressed on Exposure to Peer Aggression, Parental Acceptance, and Their Interaction
| Predictor | Sleep-wake problems |
Sleepiness |
||||||
|---|---|---|---|---|---|---|---|---|
| B | SE | β | R 2 | B | SE | β | R 2 | |
|
| ||||||||
| Sex | −0.18 | 0.97 | −.01 | 0.81 | 0.58 | .09 | ||
| Race | 1.36 | 1.08 | .08 | 0.07 | 0.65 | .01 | ||
| Age | 0.77 | 0.61 | .07 | 0.13 | 0.36 | .02 | ||
| SES | −0.87 | 0.28 | −.21** | −0.19 | 0.17 | −.08 | ||
| Anxiety | 0.30 | 0.06 | .32*** | 0.09 | 0.04 | .18* | ||
| 23.0% | 9.7% | |||||||
| Peer Victimization | 1.43 | 0.61 | .15* | 1.30 | 0.37 | .25*** | ||
| Parental Acceptance | −0.34 | 0.11 | −.18** | −0.03 | 0.07 | −.03 | ||
| 26.7% | 15.1% | |||||||
| Victimization × Acceptance | 0.38 | 0.12 | .19** | 0.00 | 0.07 | .00 | ||
| 30.0% | 15.1% | |||||||
|
| ||||||||
| Sex | −0.44 | 0.98 | −.03 | 0.53 | 0.55 | .06 | ||
| Race | 1.92 | 1.08 | .12 | 0.17 | 0.61 | .02 | ||
| Age | 1.02 | 0.62 | .10 | 0.42 | 0.34 | .08 | ||
| SES | −0.83 | 0.28 | −.20** | −0.20 | 0.16 | −.09 | ||
| Anxiety | 0.30 | 0.06 | .31*** | 0.08 | 0.04 | .16* | ||
| 23.0% | 9.7% | |||||||
| Witnessed School Violence | 0.67 | 0.26 | .16** | 0.90 | 0.14 | .40*** | ||
| Parental Acceptance | −0.34 | 0.11 | −.18** | −0.05 | 0.06 | −.05 | ||
| 27.7% | 23.9% | |||||||
| Witnessed × Acceptance | 0.12 | 0.05 | .13* | 0.01 | 0.03 | .02 | ||
| 29.2% | 24.0% | |||||||
Note. Coefficients reported are from the final model. R2 reported is from the step of entry. N = 272. Sex was coded as 0 = female, 1 = male; race was coded as 0 = White/EA, 1 = Black/AA. SE = standard error, SES = socioeconomic status (income-to-needs ratio).
p < .05.
p < .01.
p < .001.
Figure 1. Peer Victimization (a) and Witnessed School Violence (b) Interact With Parental Acceptance to Predict Sleep–Wake Problems.
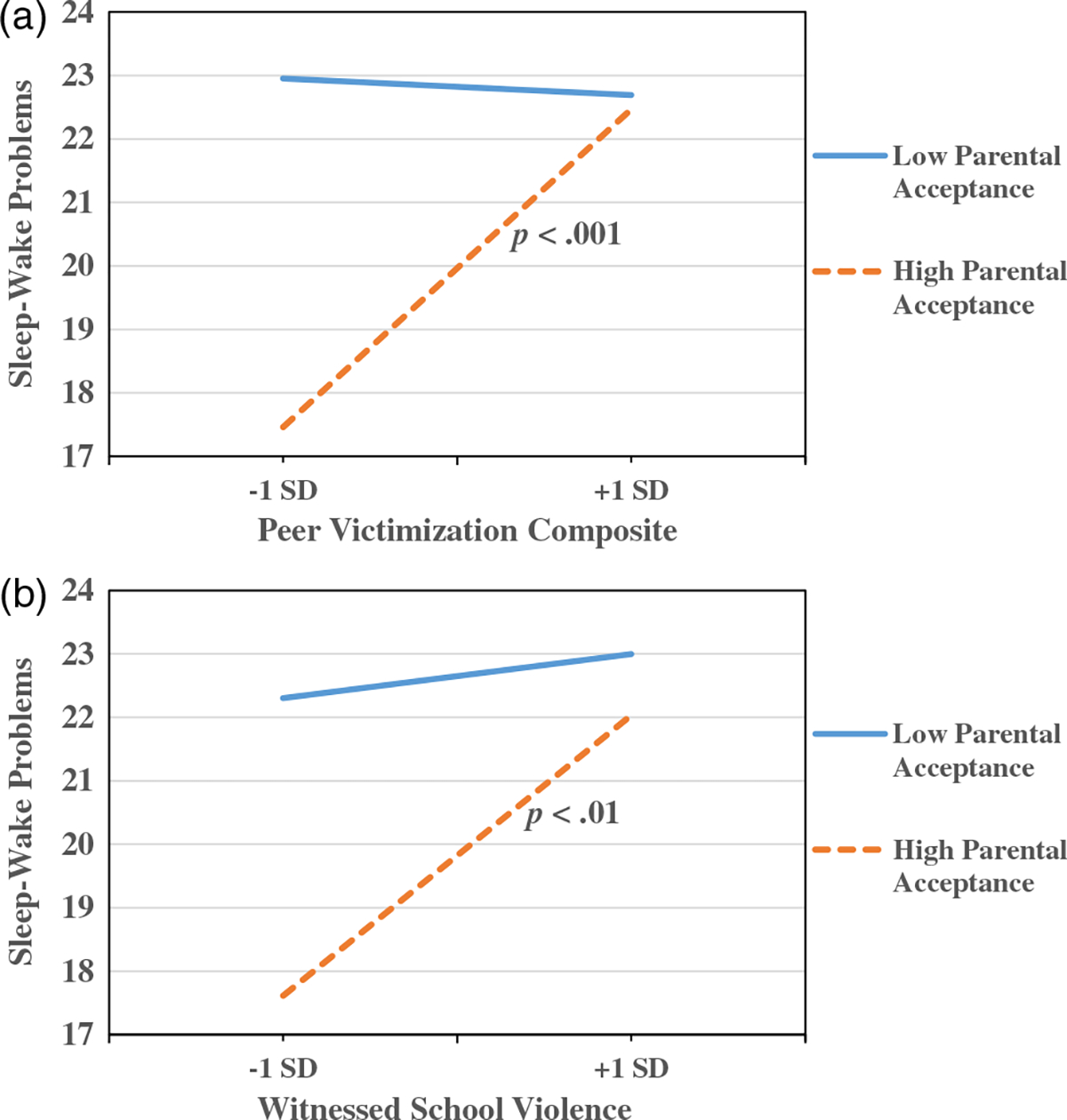
Witnessed school violence, parental acceptance, and their interaction also each significantly predicted sleep–wake problems (Table 2). As shown in Figure 1b, the association between witnessed school violence and sleep–wake problems was significant among adolescents with higher but not lower levels of parental acceptance. At lower levels of witnessed school violence, there was a 0.60 SD difference in predicted means of sleep–wake problems among adolescents with high levels of acceptance (predicted M = 17.61) compared to adolescents with low levels of acceptance (predicted M = 22.30). At higher levels of witnessed school violence, adolescents had higher levels of sleep–wake problems regardless of parental acceptance. Regions of significance on X showed that parental acceptance was negatively associated with sleep–wake problems at witnessed school violence scores of 0.44 SDs above the mean and lower.
Sleepiness
Peer victimization was significantly associated with higher levels of sleepiness, but parental acceptance and the Peer Victimization × Parental Acceptance interaction were not significant predictors of sleepiness (Table 2). Similarly, witnessing school violence predicted sleepiness, but parental acceptance and the Witnessed School Violence × Parental Acceptance interaction were not significant predictors.
Supplementary Analyses
Although not a primary aim of the study, we wished to ascertain whether associations between exposure to peer aggression and sleep problems differed for White/EA and Black/AA youth. In doing so, we examined two- and three-way interactions involving exposure to peer aggression, parental acceptance, and race. Findings are presented in Supplemental Materials. Race moderated associations between exposure to peer aggression and sleep–wake problems (see Supplemental Table S1 and Figure S1). Race did not interact with parental acceptance in the prediction of sleep problems, and no three-way interactions were significant.
Discussion
We examined whether exposure to peer aggression was associated with sleep–wake problems and sleepiness and whether parental acceptance moderated these associations. Peer victimization and witnessing school violence each interacted with parental acceptance to predict sleep quality. Specifically, the combination of both high parental acceptance and low exposure to peer aggression was associated with the lowest levels of sleep–wake problems. More exposure to peer aggression was associated with more sleep–wake problems among adolescents who felt accepted by their parents, whereas adolescents who did not feel accepted by their parents experienced high levels of sleep–wake problems regardless of exposure to peer aggression. Peer victimization and witnessing school violence were directly associated with sleepiness regardless of parental acceptance.
Across models, more exposure to peer aggression was directly associated with greater sleep problems, suggesting that such exposure during the school day continues to affect adolescents when they are trying to sleep at night. The present study expands the literature by examining a composite measure of peer victimization that spans mild to more severe instances of physical and nonphysical peer aggression and by illustrating that both experiencing and witnessing peer aggression are similarly associated with well-established measures of sleep quality problems and sleepiness. These findings are consistent with a sleep-arousal framework, in which anxiety or anger about social stressors can interfere with the sense of security and downregulation of arousal systems that enable good quality sleep (Dahl, 1996).
Given associations between anxiety and both peer victimization (Hawker & Boulton, 2000) and sleep (Palmer et al., 2018) in adolescence, we controlled for the effects of anxiety in all main analyses. Anxiety was a robust predictor of sleep quality problems and sleepiness in the current study, yet exposure to peer aggression uniquely predicted sleep problems even after accounting for anxiety, suggesting additional mechanisms. Other negative emotions that result from peer aggression (e.g., anger; Nishina & Juvonen, 2005) could be examined as potential mechanisms through which exposure to peer aggression impacts adolescents’ sleep.
The main effects of parental acceptance on adolescents’ sleep quality problems also can be interpreted within a sleep-arousal framework (Dahl, 1996). Although parental acceptance may have little bearing on adolescents’ physical safety, accepting parents provide security with respect to salient developmental concerns in adolescence, such as social and cognitive competence and autonomy (Steinberg, 2001). Parental acceptance can promote adolescents’ emotional security (Khaleque, 2013), in turn, facilitating sleep (Worthman & Melby, 2002). Despite robust associations with sleep–wake problems, parental acceptance was not directly associated with adolescents’ sleepiness, nor did it operate as a moderator of effects. These results, along with the moderate correlations between the two sleep parameters, are consistent with prior research showing that sleep quality and sleepiness are distinct constructs that are differentially related to development (e.g., Shimizu et al., 2020).
Associations between exposure to peer aggression and sleep quality problems were qualified by interactions with parental acceptance, and the interactions suggested promotive rather than protective effects of acceptance (Luthar & Goldstein, 2004). Parental acceptance was associated with better sleep in the context of low peer aggression, but the benefits of acceptance were not apparent for adolescents exposed to high levels of peer aggression. In other words, adolescents with little exposure to peer aggression and high levels of parental acceptance exhibited the lowest levels of sleep quality problems. Similar findings were reported by Morin et al. (2015), who found that parents’ engagement in school activities was associated with lower sleep problems among less victimized students, but not among highly victimized students. Although parental acceptance is generally beneficial, parenting approaches may function differently for youth with better and poorer peer experiences (Tu et al., 2017).
The hypothesis that parental acceptance would provide protection against sleep problems in the context of elevated peer aggression was not supported. Evidence that positive parent–child relationships and other forms of positive parenting provide protection is mixed (e.g., Burke et al., 2017; Rudolph et al., 2020; Stadler et al., 2010; Thompson & Leadbeater, 2013), and exposure to peer aggression is robustly associated with negative emotions (e.g., Nishina & Juvonen, 2005) that can interfere with sleep. Parents of adolescents are often unaware of peer victimization (Fekkes et al., 2005), and they have limited access to the peer group processes that drive peer aggression (e.g., peer bystanders’ reinforcement of aggression), raising further questions about their protective potential. One direction for future research is to examine whether specific parental responses to peer aggression—rather than general parenting styles or practices—can provide protection against sleep or psychological problems. For example, parents’ deliberate efforts to convey increased (i.e., more than usual) acceptance and support in response to peer victimization may promote positive self-appraisals and protect against psychological maladjustment, even if parental responses do not prevent peer aggression (Erath et al., 2020).
Strengths of the study include the socioeconomic diversity of the sample and a relatively even distribution of White/EA and Black/AA adolescents. The effects of parental acceptance did not differ for White/EA and Black/AA youth, yet the association between exposure to peer aggression and sleep quality problems was significant only for Black/AA adolescents (as shown in Supplemental Materials). Although this is beyond the scope of the current study, it is important for future research to consider how exposure to peer aggression may differ for adolescents of different races/ethnicities. Many African American adolescents’ experiences of peer victimization are linked to perceived racial discrimination (Seaton et al., 2013), which in turn is associated with sleep problems (Majeno et al., 2018). Thus, an avenue for future research is the consideration of discrimination when examining associations between exposure to peer aggression and sleep problems in racially diverse samples.
The present study is limited in that it is comprised of youth living in semirural communities and small towns, and races/ethnicities other than White/EA and Black/AA were not represented. Given that school violence is more prevalent in cities compared to towns and rural areas (Basch, 2011), it is important to examine associations between exposure to peer aggression and sleep, as well as the moderating effect of parenting, among populations who are more frequently exposed to violence in school. Indeed, in the current sample, rates of all forms of peer aggression were low, and thus results may not generalize to populations of youth with frequent exposure to peer aggression. Furthermore, findings may not generalize to youth with clinically significant sleep problems.
Other limitations of the current study include the reliance on self-report measures and the cross-sectional nature of analyses. Although prior longitudinal work has revealed that peer victimization predicts later sleep–wake problems among adolescents (Tu et al., 2019), it is also possible that youth who have sleep problems or are sleepy during the day are more likely to be exposed to peer aggression. Adolescents’ reports of maternal and paternal acceptance were combined to form a parental acceptance composite, precluding conclusions regarding potential distinct associations involving mothers and fathers.
In conclusion, the results suggest that exposure to peer aggression, through witnessing or direct victimization, is associated with more sleep quality problems and more sleepiness among late adolescents attending high school. Although adolescents who felt accepted by their parents and were not exposed to peer aggression slept relatively well, acceptance did not buffer against sleep problems among adolescents with high levels of exposure to peer aggression. General parental acceptance appeared to be most effective among low-risk youth, although future research should examine whether parents’ specific responses to peer victimization can protect against sleep problems among youth exposed to high levels of peer aggression.
Supplementary Material
Acknowledgments
This research was supported by Grant R01-HL136752 from the National Heart, Lung, and Blood Institute awarded to Mona El-Sheikh.
Footnotes
Supplemental materials: https://doi.org/10.1037/fam0000713.supp
References
- Adelantado-Renau M, Beltran-Valls MR, Migueles JH, Artero EG, Legaz-Arrese A, Capdevila-Seder A, & Moliner-Urdiales D (2019). Associations between objectively measured and self-reported sleep with academic and cognitive performance in adolescents: DADOS study. Journal of Sleep Research, 28(4), 1–9. 10.1111/jsr.12811 [DOI] [PubMed] [Google Scholar]
- Bagley EJ, Tu KM, Buckhalt JA, & El-Sheikh M (2016). Community violence concerns and adolescent sleep. Sleep Health, 2, 57–62. 10.1016/j.sleh.2015.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Basch CE (2011). Aggression and violence and the achievement gap among urban minority youth. The Journal of School Health, 81(10), 619–625. 10.1111/j.1746-1561.2011.00636.x [DOI] [PubMed] [Google Scholar]
- Burke T, Sticca F, & Perren S (2017). Everything’s gonna be alright! The longitudinal interplay among social support, peer victimization, and depressive symptoms. Journal of Youth and Adolescence, 46, 1999–2014. 10.1007/s10964-017-0653-0 [DOI] [PubMed] [Google Scholar]
- Campbell IG, Higgins LM, Trinidad JM, Richardson P, & Feinberg I (2007). The increase in longitudinally measured sleepiness across adolescence is related to the maturational decline in low-frequency EEG power. Sleep, 30(12), 1677–1687. 10.1093/sleep/30.12.1677 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cousineau D, & Chartier S (2010). Outliers detection and treatment: A review. International Journal of Psychological Research, 3(1), 58–67. 10.21500/20112084.844 [DOI] [Google Scholar]
- Crick NR, & Grotpeter JK (1996). Children’s treatment by peers: Victims of relational and overt aggression. Development and Psychopathology, 8, 367–380. 10.1017/S095457900007148 [DOI] [Google Scholar]
- Crowley SJ, Wolfson AR, Tarokh L, & Carskadon MA (2018). An update on adolescent sleep: New evidence informing the perfect storm model. Journal of Adolescence, 67, 55–65. 10.1016/j.adolescence.2018.06.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dahl RE (1996). The regulation of sleep and arousal: Development and psychopathology. Development and Psychopathology, 8, 3–27. 10.1017/S0954579400006945 [DOI] [Google Scholar]
- Davis T, Ammons C, Dahl A, & Kliewer W (2015). Community violence exposure and callous–unemotional traits in adolescents: Testing parental support as a promotive versus protective factor. Personality and Individual Differences, 77, 7–12. 10.1016/j.paid.2014.12.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Denis D, Akhtar R, Holding BC, Murray C, Panatti J, Claridge G, Sadeh A, Barclay N, O’Leary R, Maughan B, McAdams TA, Rowe R, Eley TC, Viding E, & Gregory AM (2017). Externalizing behaviors and callous-unemotional traits: Different associations with sleep quality. Sleep, 40(8). Advance online publication. 10.1093/sleep/zsx070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- El-Sheikh M, Shimizu M, Philbrook LE, Erath SA, & Buckhalt JA (2020). Sleep and development in adolescence in the context of socioeconomic disadvantage. Journal of Adolescence, 83, 1–11. 10.1016/j.adolescence.2020.06.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Erath SA, Pettit GS, & Troop-Gordon W (2020). Direct and compensatory parental responses to peer victimization. The Journal of Early Adolescence. Advance online publication. 10.1177/0272431620940386 [DOI]
- Fekkes M, Pijpers FI, & Verloove-Vanhorick SP (2005). Bullying: Who does what, when and where? Involvement of children, teachers and parents in bullying behavior. Health Education Research, 20(1), 81–91. 10.1093/her/cyg100 [DOI] [PubMed] [Google Scholar]
- Gradisar M, Gardner G, & Dohnt H (2011). Recent worldwide sleep patterns and problems during adolescence: A review and meta-analysis of age, region, and sleep. Sleep Medicine, 12(2), 110–118. 10.1016/j.sleep.2010.11.008 [DOI] [PubMed] [Google Scholar]
- Gregson KD, Erath SA, Pettit GS, & Tu KM (2016). Are they listening? Parental social coaching and parenting emotional climate predict adolescent receptivity. Journal of Research on Adolescence, 26(4), 738–752. 10.1111/jora.12222 [DOI] [PubMed] [Google Scholar]
- Hawker DS, & Boulton MJ (2000). Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 41(4), 441–455. 10.1111/1469-7610.00629 [DOI] [PubMed] [Google Scholar]
- Khaleque A (2013). Perceived parental warmth, and children’s psychological adjustment, and personality disposetions: A meta-analysis. Journal of Child and Family Studies, 2, Article e297. 10.1007/s10826-012-9579-z [DOI] [Google Scholar]
- Kliewer W, Cunningham JN, Diehl R, Parrish KA, Walker JM, Atiyeh C, Neace B, Duncan L, Taylor K, & Mejia R (2004). Violence exposure and adjustment in inner-city youth: Child and caregiver emotion regulation skill, caregiver-child relationship quality, and neighborhood cohesion as protective factor. Journal of Clinical Child and Adolescent Psychology, 33(3), 477–487. 10.1207/s15374424jccp3303_5 [DOI] [PubMed] [Google Scholar]
- Kliewer W, & Lepore SJ (2015). Exposure to violence, social cognitive processing, and sleep problems in urban adolescents. Journal of Youth and Adolescence, 44(2), 507–517. 10.1007/s10964-014-0184-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lepore SJ, & Kliewer W (2013). Violence exposure, sleep disturbance, and poor academic performance in middle school. Journal of Abnormal Child Psychology, 41, 1179–1189. 10.1007/s10802-013-9709-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewandowski AS, Toliver-Sokol M, & Palermo TM (2011). Evidence-based review of subjective pediatric sleep measures. Journal of Pediatric Psychology, 36(7), 780–793. 10.1093/jpepsy/jsq119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luthar SS, & Goldstein A (2004). Children’s exposure to community violence: Implications for understanding risk and resilience. Journal of Clinical Child and Adolescent Psychology, 33(3), 499–505. 10.1207/s15374424jccp3303_7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Majeno A, Tsai KM, Huynh VW, McCreath H, & Fuligni AJ (2018). Discrimination and sleep difficulties during adolescence: The mediating roles of loneliness and perceived stress. Journal of Youth and Adolescence, 47(1), 135–147. 10.1007/s10964-017-0755-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McNeish D (2017). Missing data methods for arbitrary missingness with small samples. Journal of Applied Statistics, 44, 24–39. 10.1080/02664763.2016.1158246 [DOI] [Google Scholar]
- Miranda M, Affuso G, Esposito C, & Bacchini D (2016). Parental acceptance-rejection and adolescent maladjustment: Mothers’ and fathers’ combined roles. Journal of Child and Family Studies, 25(4), 1352–1362. 10.1007/s10826-015-0305-5 [DOI] [Google Scholar]
- Morin HK, Bradshaw CP, & Berg JK (2015). Examining the link between peer victimization and adjustment problems in adolescents: The role of connectedness and parent engagement. Psychology of Violence, 5(4), 422–432. 10.1037/a0039798 [DOI] [Google Scholar]
- Murray-Close D (2013). Psychophysiology of adolescent peer relations I: Theory and research findings. Journal of Research on Adolescence, 2, 236–259. 10.1111/j.1532-7795.2012.00828.x [DOI] [Google Scholar]
- Muthén LK, & Muthén BO (2017). Mplus user’s guide (8th ed.). Muthén & Muthén. [Google Scholar]
- Nishina A, & Juvonen J (2005). Daily reports of witnessing and experiencing peer harassment in middle school. Child Development, 76(2), Article e435. 10.1111/j.1467-8624.2005.00855x [DOI] [PubMed] [Google Scholar]
- Palmer CA, Oosterhoff B, Bower JL, Kaplow JB, & Alfano CA (2018). Associations among adolescent sleep problems, emotion regulation, and affective disorders: Findings from a nationally representative sample. Journal of Psychiatric Research, 96, 1–8. 10.1016/j.jpsychires.2017.09.015 [DOI] [PubMed] [Google Scholar]
- Parker JG, Rubin KH, Erath SA, Wojslawowicz JC, & Buskirk AA (2006). Peer relationships, child development, and adjustment: A developmental psychopathology perspective. In Cicchetti D & Cohen DJ (Eds.), Theory and method. Developmental psychopathology (pp. 419–493). Wiley. [Google Scholar]
- Philbrook LE, Shimizu M, Buckhalt JA, & El-Sheikh M (2018). Sleepiness as a pathway linking race and socioeconomic status with academic and cognitive outcomes in middle childhood. Sleep Health, 4(5), 405–412. 10.1016/j.sleh.2018.07.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raykov T (2005). Analysis of longitudinal studies with missing data using covariance structure modeling with full-information maximum likelihood. Structural Equation Modeling, 12(3), 493–505. 10.1207/s15328007sem1203_8 [DOI] [Google Scholar]
- Reijntjes A, Kamphuis JH, Prinzie P, Boelen PA, van der Schoot M, & Telch MJ (2011). Prospective linkages between peer victimization and externalizing problems in children: A meta-analysis. Aggressive Behavior, 37, 215–222. 10.1002/ab.20374 [DOI] [PubMed] [Google Scholar]
- Reynolds CR, & Richmond BO (2008). Revised Children’s Manifest Anxiety Scale (RCMAS-2) (2nd ed.). Western Psychological Services. [Google Scholar]
- Roisman GI, Newman DA, Fraley RC, Haltigan JD, Groh AM, & Haydon KC (2012). Distinguishing differential susceptibility from diathesis–stress: Recommendations for evaluating interaction effects. Development and Psychopathology, 24(2), 389–409. 10.1017/S0954579412000065 [DOI] [PubMed] [Google Scholar]
- Rudolph KD, Monti JD, Modi H, Sze WY, & Troop-Gordon W (2020). Protecting youth against the adverse effects of peer victimization: Why do parents matter? Journal of Abnormal Child Psychology, 48(2), 163–176. 10.1007/s10802-019-00576-9 [DOI] [PubMed] [Google Scholar]
- Sadeh A (2015). III. Sleep assessment methods. Monographs of the Society for Research in Child Development, 80(1), 33–48. 10.1111/mono.12143 [DOI] [PubMed] [Google Scholar]
- Salmon S, Turner S, Taillieu T, Fortier J, & Afifi TO (2018). Bullying victimization experiences among middle and high school adolescents: Traditional bullying, discriminatory harassment, and cybervictimization. Journal of Adolescence, 63, 29–40. 10.1016/j.adolescence.2017.12.005 [DOI] [PubMed] [Google Scholar]
- Schacter HL, & Juvonen J (2019). Dynamic changes in peer victimization and adjustment across middle school: Does friends’ victimization alleviate distress? Child Development, 90(5), 1738–1753. 10.1111/cdev.13038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaefer ES (1965). Children’s reports of parental behavior: An inventory. Child Development, 36, 413–434. [PubMed] [Google Scholar]
- Seaton EK, Neblett EW, Cole DJ, & Prinstein MJ (2013). Perceived discrimination and peer victimization among African American and Latino youth. Journal of Youth and Adolescence, 42(3), 342–350. 10.1007/s10964-012-9848-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shimizu M, Gillis BT, Buckhalt JA, & El-Sheikh M (2020). Linear and nonlinear associations between sleep and adjustment in adolescence. Behavioral Sleep Medicine. Advance online publication. 10.1080/15402002.2019.1665049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spilsbury JC, Babineau DC, Frame J, Juhas K, & Rork K (2014). Association between children’s exposure to a violent event and objectively and subjectively measured sleep characteristics: A pilot longitudinal study. Journal of Sleep Research, 23(5), 585–594. 10.1111/jsr.12162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spruyt K, & Gozal D (2011). Pediatric sleep questionnaires as diagnostic or epidemiological tools: A review of currently available instruments. Sleep Medicine Reviews, 15(1), 19–32. 10.1016/j.smrv.2010.07.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stadler C, Feifel J, Rohrmann S, Vermeiren R, & Poustka F (2010). Peer-victimization and mental health problems in adolescents: Are parental and school support protective? Child Psychiatry and Human Development, 41, 371–386. 10.1007/s10578-010-0174-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L (2001). We know some things: Parent–adolescent relationships in retrospect and prospect. Journal of Research on Adolescence, 11, 1–19. 10.1111/1532-7795.00001 [DOI] [Google Scholar]
- Storch EA, Crisp H, Roberti JW, Bagner DM, & Masia-Warner C (2005). Psychometric evaluation of the social experience questionnaire in adolescents: Descriptive data, reliability, and factorial validity. Child Psychiatry and Human Development, 36, 167–176. 10.1007/s10578-005-3495-z [DOI] [PubMed] [Google Scholar]
- Thompson RSY, & Leadbeater BJ (2013). Peer victimization and internalizing symptoms from adolescence into young adulthood: Building strength through emotional support. Journal of Research on Adolescence, 23(2), 290–303. 10.1111/j.1532-7795.2012.00827.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tu KM, Gregson KD, Erath SA, & Pettit GS (2017). Custom-fit parenting: How low- and well-accepted young adolescents benefit from peer-related parenting. Parenting: Science and Practice, 17(3), 157–176. 10.1080/15295192.2017.1332298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tu KM, Spencer CW, El-Sheikh M, & Erath SA (2019). Peer victimization predicts sleep problems in early adolescence. The Journal of Early Adolescence, 39(1), 67–80. 10.1177/0272431617725199 [DOI] [Google Scholar]
- US Department of Commerce. (2019). How the Census Bureau measures poverty. https://www.census.gov/topics/income-poverty/poverty/guidance/poverty-measures.html
- Van Dulmen MH, Belliston LM, Flannery DJ, & Singer M (2008). Confirmatory factor analysis of the recent exposure to violence scale. Children & Schools, 30(2), 93–102. [Google Scholar]
- van Geel M, Goemans A, & Vedder PH (2016). The relation between peer victimization and sleeping problems: A meta-analysis. Sleep Medicine Reviews, 27, 89–95. 10.1016/j.smrv.2015.05.004 [DOI] [PubMed] [Google Scholar]
- Wolfson AR, & Carskadon MA (1998). Sleep schedules and daytime functioning in adolescents. Child Development, 69, 875–887. [PubMed] [Google Scholar]
- Wolfson AR, Carskadon MA, Acebo C, Seifer R, Fallone G, Labyak SE, & Martin JL (2003). Evidence for the validity of a sleep habits survey of adolescents. Sleep, 26(2), 213–216. 10.1093/sleep/26.2.213 [DOI] [PubMed] [Google Scholar]
- Worthman CM, & Melby MK (2002). Toward a comparative developmental ecology of human sleep. In Carskadon M (Ed.), Adolescent sleep patterns: Biological, social, and psychological influences (pp. 69–117). Cambridge University Press. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.