

Abstract
Background
Systemic corticosteroids are used to treat people with COVID‐19 because they counter hyper‐inflammation. Existing evidence syntheses suggest a slight benefit on mortality. Nonetheless, size of effect, optimal therapy regimen, and selection of patients who are likely to benefit most are factors that remain to be evaluated.
Objectives
To assess whether and at which doses systemic corticosteroids are effective and safe in the treatment of people with COVID‐19, to explore equity‐related aspects in subgroup analyses, and to keep up to date with the evolving evidence base using a living systematic review approach.
Search methods
We searched the Cochrane COVID‐19 Study Register (which includes PubMed, Embase, CENTRAL, ClinicalTrials.gov, WHO ICTRP, and medRxiv), Web of Science (Science Citation Index, Emerging Citation Index), and the WHO COVID‐19 Global literature on coronavirus disease to identify completed and ongoing studies to 6 January 2022.
Selection criteria
We included randomised controlled trials (RCTs) that evaluated systemic corticosteroids for people with COVID‐19.
We included any type or dose of systemic corticosteroids and the following comparisons: systemic corticosteroids plus standard care versus standard care, different types, doses and timings (early versus late) of corticosteroids.
We excluded corticosteroids in combination with other active substances versus standard care, topical or inhaled corticosteroids, and corticosteroids for long‐COVID treatment.
Data collection and analysis
We followed standard Cochrane methodology. To assess the risk of bias in included studies, we used the Cochrane 'Risk of bias' 2 tool for RCTs. We rated the certainty of the evidence using the GRADE approach for the following outcomes: all‐cause mortality up to 30 and 120 days, discharged alive (clinical improvement), new need for invasive mechanical ventilation or death (clinical worsening), serious adverse events, adverse events, hospital‐acquired infections, and invasive fungal infections.
Main results
We included 16 RCTs in 9549 participants, of whom 8271 (87%) originated from high‐income countries. A total of 4532 participants were randomised to corticosteroid arms and the majority received dexamethasone (n = 3766). These studies included participants mostly older than 50 years and male. We also identified 42 ongoing and 23 completed studies lacking published results or relevant information on the study design.
Hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19
Systemic corticosteroids plus standard care versus standard care plus/minus placebo
We included 11 RCTs (8019 participants), one of which did not report any of our pre‐specified outcomes and thus our analyses included outcome data from 10 studies.
Systemic corticosteroids plus standard care compared to standard care probably reduce all‐cause mortality (up to 30 days) slightly (risk ratio (RR) 0.90, 95% confidence interval (CI) 0.84 to 0.97; 7898 participants; estimated absolute effect: 274 deaths per 1000 people not receiving systemic corticosteroids compared to 246 deaths per 1000 people receiving the intervention (95% CI 230 to 265 per 1000 people); moderate‐certainty evidence).
The evidence is very uncertain about the effect on all‐cause mortality (up to 120 days) (RR 0.74, 95% CI 0.23 to 2.34; 485 participants). The chance of clinical improvement (discharged alive at day 28) may slightly increase (RR 1.07, 95% CI 1.03 to 1.11; 6786 participants; low‐certainty evidence) while the risk of clinical worsening (new need for invasive mechanical ventilation or death) may slightly decrease (RR 0.92, 95% CI 0.84 to 1.01; 5586 participants; low‐certainty evidence).
For serious adverse events (two RCTs, 678 participants), adverse events (three RCTs, 447 participants), hospital‐acquired infections (four RCTs, 598 participants), and invasive fungal infections (one study, 64 participants), we did not perform any analyses beyond the presentation of descriptive statistics due to very low‐certainty evidence (high risk of bias, heterogeneous definitions, and underreporting).
Different types, dosages or timing of systemic corticosteroids
We identified one RCT (86 participants) comparing methylprednisolone to dexamethasone, thus the evidence is very uncertain about the effect of methylprednisolone on all‐cause mortality (up to 30 days) (RR 0.51, 95% CI 0.24 to 1.07; 86 participants). None of the other outcomes of interest were reported in this study.
We included four RCTs (1383 participants) comparing high‐dose dexamethasone (12 mg or higher) to low‐dose dexamethasone (6 mg to 8 mg).
High‐dose dexamethasone compared to low‐dose dexamethasone may reduce all‐cause mortality (up to 30 days) (RR 0.87, 95% CI 0.73 to 1.04; 1269 participants; low‐certainty evidence), but the evidence is very uncertain about the effect of high‐dose dexamethasone on all‐cause mortality (up to 120 days) (RR 0.93, 95% CI 0.79 to 1.08; 1383 participants) and it may have little or no impact on clinical improvement (discharged alive at 28 days) (RR 0.98, 95% CI 0.89 to 1.09; 200 participants; low‐certainty evidence). Studies did not report data on clinical worsening (new need for invasive mechanical ventilation or death).
For serious adverse events, adverse events, hospital‐acquired infections, and invasive fungal infections, we did not perform analyses beyond the presentation of descriptive statistics due to very low‐certainty evidence.
We could not identify studies for comparisons of different timing and systemic corticosteroids versus other active substances.
Equity‐related subgroup analyses
We conducted the following subgroup analyses to explore equity‐related factors: sex, age (< 70 years; ≥ 70 years), ethnicity (Black, Asian or other versus White versus unknown) and place of residence (high‐income versus low‐ and middle‐income countries). Except for age and ethnicity, no evidence for differences could be identified. For all‐cause mortality up to 30 days, participants younger than 70 years seemed to benefit from systemic corticosteroids in comparison to those aged 70 years and older. The few participants from a Black, Asian, or other minority ethnic group showed a larger estimated effect than the many White participants.
Outpatients with asymptomatic or mild disease
There are no studies published in populations with asymptomatic infection or mild disease.
Authors' conclusions
Systemic corticosteroids probably slightly reduce all‐cause mortality up to 30 days in people hospitalised because of symptomatic COVID‐19, while the evidence is very uncertain about the effect on all‐cause mortality up to 120 days. For younger people (under 70 years of age) there was a potential advantage, as well as for Black, Asian, or people of a minority ethnic group; further subgroup analyses showed no relevant effects. Evidence related to the most effective type, dose, or timing of systemic corticosteroids remains immature. Currently, there is no evidence on asymptomatic or mild disease (non‐hospitalised participants). Due to the low to very low certainty of the current evidence, we cannot assess safety adequately to rule out harmful effects of the treatment, therefore there is an urgent need for good‐quality safety data. Findings of equity‐related subgroup analyses should be interpreted with caution because of their explorative nature, low precision, and missing data.
We identified 42 ongoing and 23 completed studies lacking published results or relevant information on the study design, suggesting there may be possible changes of the effect estimates and certainty of the evidence in the future.
Plain language summary
Are corticosteroids (anti‐inflammatory medicines) given orally or by injection an effective treatment for people with COVID‐19?
Key messages
• Corticosteroids (anti‐inflammatory medicines) given orally or by injection (systemic) are evaluated for the treatment of coronavirus disease 2019 (COVID‐19).
• Corticosteroids are effective in reducing mortality slightly.
• We do not know whether a specific type or dose of corticosteroid is effective.
• There are no data for people who were not hospitalised.
• We found 42 ongoing and 23 completed studies lacking published results or relevant information on the study design, so our findings may change in the future.
What are corticosteroids?
Corticosteroids are anti‐inflammatory drugs that reduce redness and swelling that arises due to an insult (e.g. injury, irritation) to the body. They also reduce the activity of the immune system, which defends the body against disease and infection. Corticosteroids are used to treat a variety of conditions, such as asthma, eczema, joint strains, and rheumatoid arthritis. Systemic corticosteroids can be swallowed or taken as an injection to treat problems anywhere in the body. Short‐term intake of high doses can increase the risk of further infections (including fungal infections) as well as high blood sugar and blood pressure. Furthermore, it can cause swelling of the body and psychiatric side effects such as steroid psychosis and delirium.
Why are corticosteroids possible treatments for COVID‐19?
COVID‐19 affects the lungs and airways. As the immune system fights the virus, the lungs and airways become injured and inflamed, causing breathing difficulties, and hinder oxygen transport to other vital organs. Some patients’ immune systems overreact against the invading virus causing further inflammation and tissue damage in the whole body; corticosteroids may help to control this response.
We wanted to know:
• whether and in which doses systemic corticosteroids are an effective treatment for people with COVID‐19;
• whether they cause unwanted effects; and
• whether the benefits and harms differ with respect to equity‐related aspects (e.g. age, sex, ethnicity, income by country).
We were interested in:
• deaths from any cause up to 30 and 120 days after treatment start;
• whether people got better or worse after treatment;
• unwanted effects, for example infections caught in hospital.
What did we do?
We looked for studies that investigated systemic corticosteroids for people with COVID‐19. People could be of any age, sex, or ethnicity.
Studies could compare corticosteroids:
• plus usual care versus usual care with or without placebo (sham medicine); • versus another type of corticosteroid; • versus a different medicine; • in different doses; • given as early versus late treatment.
We compared and summarised the results of the studies and rated our confidence in the evidence, based on factors such as study methods and sizes.
What did we find?
We found 16 studies with 9549 people. About 4532 people received corticosteroids, mostly dexamethasone (3766 people). These studies included participants mostly older than 50 years, male, and from high‐income countries.
We also found 42 ongoing and 23 completed studies lacking published results or relevant information on the study design.
Main results
Eleven studies compared corticosteroids plus usual care versus usual care with or without a placebo. Only one study compared two types of corticosteroids. Four studies compared different dosing of a corticosteroid named dexamethasone. The studies included only hospitalised people with confirmed or suspected COVID‐19. No studies looked at non‐hospitalised people or different timing of treatment.
Systemic corticosteroids plus usual care compared to usual care with or without placebo:
• probably reduce the number of deaths from any cause slightly, up to 30 days after treatment;
• may slightly increase the chance of being discharged alive from hospital and may slightly decrease the risk of needing breathing support or dying;
• we don't know if corticosteroids increase or decrease the number of deaths from any cause up to 120 days after treatment, any unwanted effects, or infections caught in the hospital.
Methylprednisolone versus dexamethasone:
The evidence for the number of deaths up to 30 days is very uncertain (one small study only).
High‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8 mg)
High‐dose dexamethasone:
• may reduce the number of deaths from any cause up to 30 days after treatment; • may make little to no difference to the chance of being discharged alive from hospital; • we don't know if high‐dose dexamethasone increases or decreases the number of deaths from any cause up to 120 days after treatment, any unwanted effects, or infections caught in the hospital.
Equity‐related subgroup analyses
We examined the following equity‐related aspects: ethnicity (Black, Asian or other versus White versus unknown) and place of residence (high‐income versus low‐ and middle‐income countries). For most of the subgroups, except for age and ethnicity, no evidence for differences could be identified. For death from any cause up to 30 days, participants younger than 70 years seem to benefit from corticosteroids in contrast to participants who were aged 70 years and older. Furthermore, the few participants from a Black, Asian, or minority ethnic group had a larger estimated effect than the many White participants, but these subgroup results need cautious interpretation.
What are the limitations of the evidence?
We are moderately confident in the evidence about the effect of corticosteroids on deaths from any cause within 30 days after treatment. However, our confidence in the other evidence is low to very low, because studies did not use the most robust methods, and the way results were recorded and reported differed across studies.
How up‐to‐date is this evidence?
This review updates our previous review. The evidence is up‐to‐date to 6 January 2022.
Summary of findings
Summary of findings 1. Summary of findings table ‐ Corticosteroids plus standard care compared to standard care (plus/minus placebo) for hospitalised and unvaccinated individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Corticosteroids plus standard care compared to standard care (plus/minus placebo) for hospitalised and unvaccinated individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19 | ||||||
| Patient or population: hospitalised and unvaccinated individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19 Setting: inpatient, ICU Intervention: corticosteroids plus standard care Comparison: standard care (plus/minus placebo) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with standard care (plus/minus placebo) | Risk with corticosteroids plus standard care | |||||
| All‐cause mortality up to 30 days | 274 per 1000 | 246 per 1000 (230 to 265) | RR 0.90 (0.84 to 0.97) | 7898 (9 RCTs) | ⊕⊕⊕⊝ Moderatea | Systemic corticosteroids probably reduce all‐cause mortality up to 30 days slightly. |
| All‐cause mortality up to 120 days | 402 per 1000 | 298 per 1000 (93 to 942) | RR 0.74 (0.23 to 2.34) | 485 (3 RCTs) | ⊕⊝⊝⊝ Very lowb | The evidence is very uncertain about the effect of systemic corticosteroids on all‐cause mortality up to 120 days. |
| Clinical improvement: discharged alive (follow‐up: 28 days) | 620 per 1000 | 664 per 1000 (639 to 688) | RR 1.07 (1.03 to 1.11) | 6786 (3 RCTs) | ⊕⊕⊝⊝ Lowc | Systemic corticosteroids may slightly increase the chance of clinical improvement: discharged alive. |
| Clinical worsening: new need for invasive mechanical ventilation or death | 282 per 1000 | 260 per 1000 (237 to 285) | RR 0.92 (0.84 to 1.01) | 5586 (2 RCTs) | ⊕⊕⊝⊝ Lowd | Systemic corticosteroids may slightly decrease the risk of clinical deterioration: new need for invasive mechanical ventilation or death. |
| Serious adverse events (follow‐up: during treatment) | We did not perform meta‐analyses because of high risk of bias, heterogeneous definitions, and underreporting. Therefore, we only present descriptive statistics: Angus 2020 shock‐dependent hydrocortisone: RR 4.11 (95% CI 0.23 to 72.98); Angus 2020 fixed‐dose hydrocortisone: RR 1.43 (95% CI 0.16 to 12.49); Tomazini 2020: RR 0.54 (95% CI 0.19 to 1.59). | 678 (2 RCTs) | ⊕⊝⊝⊝ Very lowe | The evidence is very uncertain about the effect of systemic corticosteroids on serious adverse events. | ||
| Adverse events (any grade) (follow‐up: during treatment) | We did not perform meta‐analyses because of high risk of bias, heterogeneous definitions, and underreporting. We only present descriptive statistics: Edalatifard 2020: RR 0.82 (95% CI 0.12 to 5.48); Tang 2021: RR 0.63 (95% CI 0.22 to 1.76); Tomazini 2020: RR 0.99 (95% CI 0.89 to 1.10). | 447 (3 RCTs) | ⊕⊝⊝⊝ Very lowf | The evidence is very uncertain about the effect of systemic corticosteroids on adverse events. | ||
| Hospital‐acquired infections (follow up: during treatment) | We did not perform meta‐analyses because of high risk of bias, heterogeneous definitions, and underreporting. We present descriptive statistics only: Corral‐Gudino 2021: RR 4.14 (95% CI 0.51 to 33.49); Dequin 2020: RR 0.90 (95% CI 0.60 to 1.34); Tang 2021: RR 2.00 (95% CI 0.19 to 21.24); Tomazini 2020: RR 0.75 (95% CI 0.50 to 1.15). | 598 (4 RCTs) | ⊕⊝⊝⊝ Very lowf | The evidence is very uncertain about the effect of systemic corticosteroids on hospital‐acquired infections. | ||
| Invasive fungal infections (follow‐up: during treatment) | We present descriptive statistics only because of high risk of bias: Corral‐Gudino 2021: RR 2.50 (95% CI 0.11 to 59.15). | 64 (1 RCT) | ⊕⊝⊝⊝ Very lowf | The evidence is very uncertain about the effect of systemic corticosteroids on invasive fungal infections. | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
| See interactive version of this table: https://gdt.gradepro.org/presentations/#/isof/isof_question_revman_web_424096272361428897. | ||||||
a We downgraded one level for serious risk of bias (partly deviations from the intended intervention, selection of the reported results, missing information about the allocation concealment, baseline differences) b We downgraded one level for serious risk of bias (partly deviations from the intended intervention, selection of the reported results, missing information about the allocation concealment), one level for serious inconsistency and one level for serious imprecision (wide confidence interval, low number of participants) c We downgraded one level for serious risk of bias (partly deviations from the intended intervention, selection of the reported results, missing information about the allocation concealment) and one level for serious inconsistency. d We downgraded one level for serious risk of bias (deviations from the intended intervention, measurement of the outcome) and one level for serious inconsistency. e We downgraded two levels for very serious risk of bias (deviations from the intended intervention, missing adjustment for competing risk of death, reporting bias (the safety‐relevant outcome was not reported)) and one level for serious imprecision (fewer than 500 events). f We downgraded two levels for very serious risk of bias (deviations from the intended intervention, missing adjustment for competing risk of death, missing information about the allocation concealment, reporting bias (the safety‐relevant outcome was not reported) and one level for serious imprecision (fewer than 500 events).
Summary of findings 2. Summary of findings table ‐ Methylprednisolone compared to dexamethasone for hospitalised and unvaccinated individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Methylprednisolone compared to dexamethasone for hospitalised and unvaccinated individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19 | ||||||
| Patient or population: hospitalised and unvaccinated individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19 Setting: inpatient, ICU Intervention: methylprednisolone Comparison: dexamethasone | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with dexamethasone | Risk with methylprednisolone | |||||
| All‐cause mortality up to 30 days | 357 per 1000 | 182 per 1000 (86 to 382) | RR 0.51 (0.24 to 1.07) | 86 (1 RCT) | ⊕⊝⊝⊝ Very lowa | The evidence is very uncertain about the effect of methylprednisolone on all‐cause mortality up to 30 days. |
| All‐cause mortality up to 120 days ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
| Clinical improvement: discharged alive ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
| Clinical worsening: new need for invasive mechanical ventilation or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
| Serious adverse events ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
| Adverse events ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
| Hospital‐acquired infections ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
| Invasive fungal infections ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
| See interactive version of this table: https://gdt.gradepro.org/presentations/#/isof/isof_question_revman_web_424391243004646489. | ||||||
a We downgraded one level for serious risk of bias for missing pre‐specification/protocol/statistical analysis plan and two levels for very serious imprecision (fewer than 50 events).
Summary of findings 3. Summary of findings table ‐ High‐dose dexamethasone (12 mg or higher) compared to low‐dose dexamethasone (6 mg to 8 mg) for hospitalised individuals with unknown vaccination status and a confirmed diagnosis of symptomatic COVID‐19.
| High‐dose dexamethasone (12 mg or higher) compared to low‐dose dexamethasone (6 mg to 8 mg) for hospitalised individuals with unknown vaccination status and a confirmed diagnosis of symptomatic COVID‐19 | ||||||
| Patient or population: hospitalised individuals with unknown vaccination status and a confirmed diagnosis of symptomatic COVID‐19 Setting: inpatient Intervention: high‐dose dexamethasone (12 mg or higher) Comparison: low‐dose dexamethasone (6 mg to 8 mg) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with low‐dose dexamethasone (6 mg to 8 mg) | Risk with high‐dose dexamethasone (12 mg or higher) | |||||
| All‐cause mortality up to 30 days | 285 per 1000 | 248 per 1000 (208 to 297) | RR 0.87 (0.73 to 1.04) | 1269 (3 RCTs) | ⊕⊕⊝⊝ Lowa | High‐dose dexamethasone may further reduce all‐cause mortality up to 30 days compared to low‐dose dexamethasone (6 mg to 8 mg). |
| All‐cause mortality up to 120 days | 329 per 1000 | 306 per 1000 (260 to 355) | RR 0.93 (0.79 to 1.08) | 1383 (4 RCTs) | ⊕⊝⊝⊝ Very lowb | The evidence is very uncertain about the effect of high‐dose dexamethasone (12 mg or higher) on all‐cause mortality up to 120 days compared to low‐dose dexamethasone (6 mg to 8 mg). |
| Clinical improvement: discharged alive (follow‐up: 28 days) | 882 per 1000 | 865 per 1000 (785 to 962) | RR 0.98 (0.89 to 1.09) | 200 (1 RCT) | ⊕⊕⊝⊝ Lowc | High‐dose dexamethasone (12 mg or higher) may have little or no impact on the chance of clinical improvement: discharged alive compared to low‐dose dexamethasone (6 mg to 8 mg). |
| Clinical worsening: new need for invasive mechanical ventilation or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No study reported this outcome. |
| Serious adverse events (follow‐up: during treatment) | We did not perform meta‐analyses because of high risk of bias arising from the missing adjustment for competing risk of death. We present descriptive data only: Munch 2021b: RR 0.80 (95% CI 0.60 to 1.07); Maskin 2021: RR 1.05 (95% CI 0.88 to 1.25). | 1080 (2 RCTs) | ⊕⊝⊝⊝ Very lowd | The evidence is very uncertain about the effect of high‐dose dexamethasone (12 mg or higher) on serious adverse events compared to low‐dose dexamethasone (6 mg to 8 mg). | ||
| Adverse events (any grade) (follow‐up: during treatment) | We did not perform meta‐analyses because of high risk of bias arising from the missing adjustment for competing risk of death. We present descriptive data only: Maskin 2021: RR 1.02 (95% CI 0.96 to 1.08). | 98 (1 RCT) | ⊕⊝⊝⊝ Very lowe | The evidence is very uncertain about the effect of high‐dose dexamethasone (12 mg or higher) on adverse events compared to low‐dose dexamethasone (6 mg to 8 mg). | ||
| Hospital‐acquired infections (follow‐up: during treatment) | We did not perform meta‐analyses because of high risk of bias arising from the missing adjustment for competing risk of death. We present descriptive data only: Maskin 2021: RR 0.89 (95% CI 0.70 to 1.14); Munch 2021b: RR 0.80 (95% CI 0.56 to 1.14). | 1080 (2 RCTs) | ⊕⊝⊝⊝ Very lowf | The evidence is very uncertain about the effect of high‐dose dexamethasone (12 mg or higher) on hospital‐acquired infections compared to low‐dose dexamethasone (6 mg to 8 mg). | ||
| Invasive fungal infections (follow‐up: during treatment) | We did not perform meta‐analyses because of high risk of bias arising from the missing adjustment for competing risk of death. We present descriptive data only: Munch 2021b: RR 0.70 (95% CI 0.36 to 1.34); Maskin 2021: RR 1.00 (95% CI 0.21 to 4.71). | 1080 (2 RCTs) | ⊕⊝⊝⊝ Very lowf | The evidence is very uncertain about the effect of high‐dose dexamethasone (12 mg or higher) on invasive fungal infections compared to low‐dose dexamethasone (6 mg to 8 mg). | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
| See interactive version of this table: https://gdt.gradepro.org/presentations/#/isof/isof_question_revman_web_431226044092715996. | ||||||
a We downgraded one level for serious risk of bias (deviations from the intended intervention, no information about the allocation concealment) and one level for serious imprecision (wide confidence interval, low number of participants/events). b We downgraded one level for serious risk of bias (no information about the allocation concealment; deviations from the protocol), one level for serious imprecision (wide confidence interval, low number of participants/events) and one level for serious inconsistency (Toroghi 2021 differs from the other studies). c We downgraded one level for serious risk of bias (no information about the allocation concealment) and one level for serious imprecision (wide confidence interval, low number of participants/events). d We downgraded one level for serious risk of bias (missing adjustment of competing risk of death) and two levels for very serious imprecision (very low number of events/participants). e We downgraded one level for serious risk of bias (missing adjustment for competing risk of death, deviations from the intended intervention), two levels for very serious imprecision (very low number of events/participants). f We downgraded one level for serious risk of bias (missing adjustment for competing risk of death, protocol deviations, measurement of the outcome, no information about the allocation concealment), two levels for very serious imprecision (very low number of events/participants).
Background
This work is part of a series of Cochrane Reviews investigating treatments and therapies for coronavirus disease 2019 (COVID‐19). Reviews in this series share information in the background section and methodology with the first published reviews about monoclonal antibodies (Kreuzberger 2021), and convalescent plasma (Piechotta 2021).
Description of the condition
COVID‐19 is a rapidly spreading infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) (WHO 2020a). On 11 March 2020, the World Health Organization (WHO) declared the current COVID‐19 outbreak a pandemic, which is unprecedented in comparison to previous coronavirus outbreaks (severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), which each caused fewer than 1000 deaths; WHO 2007; WHO 2019). Despite intensive international efforts to contain its spread, SARS‐CoV‐2 has resulted in an ongoing increase of new weekly cases and deaths in several regions around the globe (WHO 2021a; WHO 2022a). In the meantime, the emergence of SARS‐CoV‐2 variants, with the potential for altered transmission or disease characteristics, or to impact the effectiveness of vaccines, therapeutics, diagnostics, or public health and social measures, challenge strategies to control disease spread (WHO 2022b).
Apart from age and co‐morbidities, vaccination status substantially influences the risk of a severe course of disease, hospitalisation, and mortality. In patients without effective immunisation (individuals who are unvaccinated, incompletely vaccinated, or individuals who fail to develop an immunological response despite being fully vaccinated) this risk is higher among those aged 65 years or older, smokers and those with certain underlying medical conditions such as cancer, chronic kidney disease, chronic obstructive pulmonary disease (COPD), heart conditions, immunocompromised state, obesity, sickle cell disease or type 2 diabetes mellitus (Huang 2020; Liang 2020; WHO 2020a; Williamson 2020). COVID‐19 case fatality ratios vary widely between countries and reporting periods, from 0.0% to more than 18% (Johns Hopkins University 2022). However, these numbers may be misleading as variability in reporting and testing certainly contributed to inaccuracy in case fatality ratios due to varying testing frequency, a lack of reporting dates, and variations in case definitions, especially at the beginning of the pandemic when the main focus was on severe cases (WHO 2020b).
The median incubation time and time to symptom onset depends on the virus variant and is estimated to be three days (range zero to eight days) in the case of the Omicron variant of concern, which is shorter compared with previous reports for the Delta variant and other previously circulating non‐Delta SARS‐CoV‐2 (five to six days) (Brandal 2021; Lauer 2020). Sore throat, cough, fever, headache, fatigue, and myalgia or arthralgia are the most commonly reported symptoms (Brandal 2021; Struyf 2020). Other symptoms include dyspnoea, chills, nausea or vomiting, diarrhoea, and nasal congestion (WHO 2020a). The reported frequency of asymptomatic infections varies greatly, depending on the time of the investigation, the cohort investigated, and the virus variant, and ranges between 6% and 96% (Buitrago‐Garcia 2020; Funk 2021; Lewnard 2022; Oran 2020; Wolter 2022).
A smaller proportion of people are affected by severe (approximately 11% to 20%) or critical (approximately 1% to 5%) disease with hospitalisation and intensive care unit (ICU) admission due to respiratory failure, septic shock, or multiple organ dysfunction syndrome (Ferguson 2021; Funk 2021; Lewnard 2022; Wolter 2022; Wu 2020). In one systematic review and meta‐analysis of international studies, the proportion of patients who died among those treated in the ICU was estimated to be 34% and for those who received invasive mechanical ventilation it was 83% (Potere 2020). However, the hospitalisation and ICU treatment rates seem to depend on the virus variant. Analyses from the United Kingdom show a significant reduction in the relative risk of hospitalisation for adult Omicron cases compared to Delta (Ferguson 2021). There may also have been a different threshold for admission to hospital or ICU during the course of the pandemic. Depending on the local pressure on ICU resources, some normal wards will have learned to provide continuous positive airway pressure (CPAP) therapy equivalent to ICU support in other healthcare systems. It is unclear whether triage criteria in some healthcare systems may have influenced admission to hospital or ICU (or both).
As the evidence on many of the substances that were investigated for the treatment of COVID‐19 increased over the course of the pandemic, national and international guidelines emerged to support daily clinical decisions (NICE 2021; NIH 2021; WHO 2021b). However, so far there are only a few substances with clearly proven benefits and clear recommendations as well as approval by national and international authorities for the treatment of COVID‐19 (EMA 2022; FDA 2022; WHO 2021b; WHO 2021c). In light of the extent of the COVID‐19 pandemic and the scarcity of effective treatments, there is still an urgent need for effective therapies to save lives and to reduce the high burden on healthcare systems (either with a high workload caused by COVID‐19 or staff shortages due to infected health care providers), especially in the face of evolving variants of the virus with the potential for increased transmissibility and the limited global availability of vaccines.
Description of the intervention
Corticosteroids are a group of stress hormones produced from the adrenal cortex. In addition to their stress‐mediated mechanisms for generating energy substrates, corticosteroids have anti‐inflammatory and immunosuppressive properties in higher doses and are applied in a wide variety of ways in almost all fields of medicine (Barnes 2006; Rhen 2005). For example, corticosteroids are used at high doses of more than 6 mg/kg up to 30 mg/kg methylprednisolone corresponding to more than 30 mg/kg up to 150 mg/kg hydrocortisone equivalents daily for short‐term, high‐dose pulse therapy against solid organ transplant rejection, or about 0.5 mg/kg hydrocortisone equivalents daily for prolonged therapy in different inflammatory lung diseases. A major representative of synthetic corticosteroids is the long‐acting compound dexamethasone. Examples of other synthetic corticosteroids with weaker and shorter activity are methylprednisolone and hydrocortisone (Bourdeau 2003). To obtain comparable effects, dosage equivalents are needed for the different corticosteroids. However, patients may have a higher risk of infections (including fungal infections) and can suffer from blood glucose problems, hypertension, oedema, and psychiatric side effects such as steroid psychosis and delirium (Schreiber 2014; Waljee 2017). The therapeutic use of higher doses of corticosteroids over a longer time suppresses the hypothalamic‐pituitary‐adrenal axis such that dosage‐tapering may be needed (Taves 2011; Yasir 2022).
How the intervention might work
It has been proposed that corticosteroids could be clinically effective against severe and critical COVID‐19. A substantial percentage of patients develop severe and critical COVID‐19 that requires hospitalisation, with dyspnoea, hypoxia, or relevant lung involvement based on imaging, as well as respiratory failure, shock, or multi‐organ dysfunction requiring ventilator support (Thibeault 2021; Wu 2020). In COVID‐19, an insufficient host defence and unbalanced inflammation is thought to play a key role in the pathophysiology of hypoxaemic respiratory failure (Schulte‐Schrepping 2020). A systemic inflammatory response with the excessive release of cytokines and inflammation mediators can lead to lung injury with the development of acute respiratory distress syndrome (ARDS). The potent anti‐inflammatory effects of corticosteroids might prevent or mitigate these deleterious effects by modulating cytokine release (Villar 2020). Corticosteroids have been widely used in syndromes closely related to COVID‐19, including SARS, MERS, severe influenza, and community‐acquired pneumonia. The evidence to support or discourage the use of corticosteroids under these conditions has been weak. Corticosteroids can induce harm through immunosuppressive effects during the treatment of infection. In SARS‐CoV‐2 infection, viral shedding appears early in the illness and declines thereafter. The effect of corticosteroid therapy on virus clearance in COVID‐19 needs to be taken into consideration as well as the unwanted adverse events. In acutely critically ill people, dexamethasone has comparatively few side effects (Rochwerg 2018). However, patients may suffer from blood glucose variations and potential invasive fungal infections. The therapeutic use of higher doses of corticosteroids over a longer time (more than 21 days) suppresses the hypothalamic‐pituitary‐adrenal axis such that dosage‐tapering may be needed.
Why it is important to do this review
Systemic corticosteroids are now part of the standard therapy for COVID‐19 in patients having additional oxygen supply and/or mechanical ventilation, and are recommended in national and international guidelines (NICE 2021; NIH 2021; WHO 2021b), based on systematic reviews regarding interventions for COVID‐19, including corticosteroids. For example, several systematic reviews investigated the association between the use of corticosteroids and COVID‐19‐related mortality based on randomised controlled trials (RCTs) and non‐randomised studies (e.g. Chaudhuri 2021; Sterne 2020; Van Paassen 2020). Comparison of different corticosteroids, dosages, and time points of administration in terms of clinical progression, or comparison with other active substances, especially other anti‐inflammatory substances, appears necessary in order to define the role of corticosteroids in the treatment of COVID‐19. This not only relates to effectiveness but also the risk profile, especially with regard to a potential risk of systemic fungal infections. This, moreover, is interconnected with the equity considerations that this updated systematic review is addressing: do participant characteristics such as age, sex, place of residence, or ethnicity stratify clinical outcomes and influence how large a benefit a participant can expect in terms of mortality reduction, or should certain subgroups not receive systemic corticosteroids at all?
We were encouraged by Tomlinson 2021 to not only present the baseline characteristics of participants but also to analyse outcome data with respect to equity‐related aspects. We aimed to perform subgroup analyses stratified by age group, sex, income group of the country of origin, and ethnicity for mortality outcomes in all comparisons. We used PROGRESS‐Plus to consider the equity‐related stratifying factors below (Welch 2012):
Sex: sex of study participants might influence the outcome and potentially access to care (Ahrenfeldt 2020).
Age: age is a known risk factor for severe disease and potentially access to care (Ahrenfeldt 2020).
Ethnicity: existing studies have indicated that some ethnicities might have a worse outcome (e.g. people of colour, including in a high‐income country), therefore it is important to evaluate whether intervention effects are consistent across all ethnicities (Navar 2021).
Place of residence: we did not evaluate at country‐level, but by income ranking (low‐ and middle‐income versus high‐income countries). One reason for this was to see whether this effective treatment has also been evaluated in low‐ and middle‐income countries and whether the results are comparable, as this intervention is cheap and available almost everywhere (Oke 2020).
The 'living' approach in evidence synthesis is necessary in order to incorporate new knowledge into the data evaluation, to keep the evidence assessment up‐to‐date and thus to offer a better basis for recommendations and everyday clinical decisions. This Cochrane Review is the first update of our published review (Wagner 2021a). The update was necessary because important new studies have been published in the meantime. It will fill current evidence gaps by identifying, describing, evaluating, and meta‐analysing RCTs of systemic corticosteroids in relation to clinical outcomes in COVID‐19. Unlike other systematic reviews in this field, it considers the outcome clinical improvement (defined as Discharged alive) and worsening (defined as a combined endpoint New need for invasive ventilation or death), and provides equity‐relevant subgroup analyses and methodologically critical sensitivity analyses. This living systematic review will be updated once new evidence becomes available.
Objectives
To assess whether and at which doses systemic corticosteroids are effective and safe in the treatment of people with COVID‐19, and to keep up‐to‐date with the evolving evidence base using a living systematic review approach. Apart from adding newly published evidence to existing and new comparisons, we would like to assess equity‐related aspects quantitatively in subgroup analyses where possible.
Methods
Criteria for considering studies for this review
Types of studies
The main description of methods is based on Cochrane Haematology's standard template and is in line with a series of Cochrane Reviews investigating treatments and therapies against COVID‐19. We made specific adaptations related to the research question if necessary. The protocol for this review was registered with PROSPERO on 21 December 2020 (Wagner 2021b).
To assess the efficacy and safety of systemic corticosteroids against COVID‐19, we included RCTs, as this study design, if performed appropriately, provides the best evidence for experimental therapies in highly controlled therapeutic settings. We used the methods recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2022a). We would also have accepted cluster‐randomised trials for inclusion, if we had found any.
We included the following formats if sufficient information was available on study design, characteristics of participants, interventions, and outcomes:
full‐text publications;
preprint articles.
For our previous version of the review (Wagner 2021a), we included preprints for a complete overview of ongoing research activity, especially for tracking newly emerging studies about the use of systemic corticosteroids against COVID‐19, but in this updated version all studies that contributed to data/analyses are peer‐reviewed RCTs.
We did not apply any limitation with respect to the length of follow‐up. The types of study designs remained the same as in the first version of this review, and we did not include any additional study designs that may be more suited for conducting equity‐related analyses.
Types of participants
We included adults with a suspected or confirmed diagnosis of COVID‐19 (as described in the study) and we did not exclude any studies based on sex, ethnicity, disease severity, or setting.
We excluded studies evaluating the use of corticosteroids against coronavirus diseases such as SARS or MERS, or other viral diseases, such as influenza. If studies enrolled populations with or exposed to mixed viral diseases, we had planned to only include these if the study authors provided subgroup data for SARS‐CoV‐2 infection.
Types of interventions
We included the following interventions:
any type or dose of systemic corticosteroids;
oral or intravenous application.
We had planned to include the following comparisons:
systemic corticosteroids plus standard care versus standard care (plus/minus placebo);
dose comparisons;
timing comparisons (early versus late);
different types of corticosteroids;
systemic corticosteroid versus other active substances.
However, comparisons of different timings (early versus late) and systemic corticosteroids versus other active substances were not available.
Standard care in both arms should be similar.
We excluded the following interventions:
corticosteroid plus other active substance versus standard care;
topical corticosteroids;
inhaled corticosteroids;
corticosteroids for long‐COVID treatment.
Types of outcome measures
We evaluated core outcomes in accordance with the Core Outcome Measures in Effectiveness Trials (COMET) Initiative for COVID‐19 patients (COMET 2020; Marshall 2020), and additional outcomes that have been prioritised by consumer representatives and the panel of the German 'National Treatment Guidance for Hospitalised COVID‐19 Patients' (Kluge 2022).
We defined this outcome set for hospitalised individuals with a confirmed or suspected diagnosis of COVID‐19 and moderate to severe disease, according to the WHO clinical progression scale stage 4 to 9 (Marshall 2020); that is, all patients who were hospitalised because of symptomatic COVID‐19 treated with all different levels of respiratory support (no additional oxygen, low‐flow oxygen prongs or mask ('low‐flow oxygen' only hereafter), high‐flow oxygen or non‐invasive ventilation (NIV), invasive mechanical ventilation including extracorporeal membrane oxygenation (ECMO)), and individuals with a confirmed or suspected diagnosis of SARS‐CoV‐2 infection and asymptomatic or mild disease, according to the WHO clinical progression scale (Marshall 2020). Of note, readers may encounter respiratory support both as a baseline characteristic and as an outcome measure ‐ in the latter case we used changes in the level of support.
Individuals with a suspected or confirmed diagnosis of COVID‐19 and moderate to severe disease
Prioritised outcomes (included in the summary of findings tables)
-
Mortality:
-
All‐cause mortality
Up to day 30 (from here on for simplicity in this version of the review All‐cause mortality up to 30 days)
Any longer observation period from day 31 on (from here on All‐cause mortality up to 120 days)
-
-
Improvement of clinical status during the longest observation period available:
Participants discharged alive (without clinical worsening or death)
-
Worsening of clinical status during the longest observation period available:
New need for invasive mechanical ventilation or death
Serious adverse events, defined as the number of participants with any serious adverse event (serious as defined according to CTCAE (Common Terminology Criteria for Adverse Events))
Adverse events (any grade), defined as the number of participants with any adverse event
Specific adverse events: hospital‐acquired infections, defined as the number of participants with an event
Specific adverse events: invasive fungal infections, defined as the number of participants with an event
Prioritised outcomes (not included in the summary of findings tables):
Quality of life, including fatigue and neurological status, assessed with standardised scales (e.g. WHOQOL‐100) during the longest period available
Additional outcomes (not included in the summary of findings tables)
New need for dialysis during the longest period available
Viral clearance, assessed with reverse transcription polymerase chain reaction (RT‐PCR) test for SARS‐CoV‐2 at baseline, up to 3, 7, and 15 days
Individuals with a suspected or confirmed diagnosis of SARS‐CoV‐2 infection and asymptomatic or mild disease
Prioritised outcomes (included in the summary of findings tables)
Mortality: all‐cause mortality up to day 30 or any longer observation period
Admission to hospital or death within 28 days
Quality of life, including fatigue and neurological status, assessed with standardised scales (e.g. WHOQOL‐100) during the longest period available
Serious adverse events, defined as the number of participants with any serious adverse event (serious as defined according to CTCAE (Common Terminology Criteria for Adverse Events)
Adverse events (any grade), defined as the number of participants with any adverse event
Specific adverse events: infections, defined as the number of participants with an event
Specific adverse events: invasive fungal infections, defined as the number of participants with an event
Additional outcomes (not included in the summary of findings tables)
Viral clearance, assessed with RT‐PCR test for SARS‐CoV‐2 at baseline, up to 3, 7, and 15 days
Timing of outcome measurement
In the case of time‐to‐event analysis, for example, for time to clinical improvement, we included the outcome measure based on the longest follow‐up time. We also collected information on outcomes from all other time points reported in the publications.
Search methods for identification of studies
Electronic searches
Our information specialist (MIM) conducted systematic searches in the following sources from the inception of each database to 6 January 2022 (search date for all databases) and did not place restrictions on the language of publication.
-
Cochrane COVID‐19 Study Register (CCSR) (www.covid-19.cochrane.org), comprising:
MEDLINE (PubMed), weekly updates;
Embase.com, weekly updates;
ClinicalTrials.gov (www.clinicaltrials.gov), daily updates;
WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/trialsearch), weekly updates;
medRxiv (www.medrxiv.org), weekly updates;
Cochrane Central Register of Controlled Trials (CENTRAL), monthly updates.
-
Web of Science Core Collection (Clarivate), from 1 January 2020 onwards:
Science Citation Index Expanded (1945 to present);
Emerging Sources Citation Index (2015 to present).
WHO COVID‐19 Global literature on coronavirus disease (search.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/).
Database search results for Web of Science were restricted to publications from 2020 to the present date, as no treatment studies on COVID‐19 were registered prior to January 2020. For detailed search strategies, see Appendix 1 (previous review version) and Appendix 2 (current review version).
We did not conduct separate searches of the databases required by the Methodological Expectations of Cochrane Intervention Reviews (MECIR) standards (Higgins 2022), since these databases are already being regularly searched for the production of the CCSR.
Searching other resources
We identified other potentially eligible studies or ancillary publications by searching the reference lists of included studies and systematic reviews.
Data collection and analysis
Selection of studies
Two out of three review authors (MSp, CW, ALF) independently screened the results of the search strategies for eligibility for the review by reading the titles and abstracts using Ouzzani 2016. We coded the abstracts as either 'include' or 'exclude'. In the case of disagreement or if it was unclear whether we should retrieve the abstract or not, we obtained the full‐text publication for further discussion. Two review authors assessed the full‐text articles of selected studies. If the two review authors were unable to reach a consensus, they consulted a senior review author to reach a final decision.
We documented the study selection process in a flow chart, as recommended in the PRISMA statement (Moher 2009), and showed the total numbers of retrieved references and the numbers of included and excluded studies. We listed all studies that we excluded after full‐text assessment and the reasons for their exclusion in the Characteristics of excluded studies section.
Data extraction and management
We conducted data extraction according to the guidelines proposed by Cochrane (Li 2021). Two out of five review authors (CW, MSp, JD, ALF, MG) extracted data independently and in duplicate, using a customised data extraction form developed in Microsoft Excel (Microsoft 2018). We resolved disagreements by discussion. If we were unable to reach agreement, we involved a third review author.
Two review authors (CW, MSp) independently assessed eligible studies obtained in the process of study selection (as described above) for methodological quality and risk of bias. If the review authors were unable to reach a consensus, they consulted a third review author.
We extracted the following information if reported:
General information: author, title, source, publication date, country, language, duplicate publications
Study characteristics: trial design, setting and dates, source of participants, inclusion/exclusion criteria, comparability of groups, treatment cross‐overs, compliance with assigned treatment, length of follow‐up
Participant characteristics: age, sex, ethnicity, number of participants recruited/allocated/evaluated, number of participants with positive, negative or unknown RT‐PCR test result, additional diagnoses, severity of disease, previous treatments, concurrent treatments, co‐morbidities (e.g. diabetes, immunosuppression), vaccination status
Interventions: type of corticosteroid, dose, frequency, timing, duration and route of administration, setting (e.g. inpatient, outpatient), duration of follow‐up
Control interventions: placebo, no treatment or other intervention; dose, frequency, timing, duration and route of administration, setting, duration of follow‐up
Outcomes: as specified under Types of outcome measures
Risk of bias assessment: randomisation process, deviations from the intended interventions, missing outcome data, measurement of the outcome, selection of the reported results
-
Equity‐related aspects as per the PROGRESS‐Plus approach (Welch 2012): place of residence, race/ethnicity, occupation, sex, religion, education, socioeconomic status, social capital and personal characteristics associated with discrimination (e.g. age, disability); features of relationships; time‐dependent relationships
Countries were classified socio‐economically based on the World Bank's latest version of the Country and Lending Groups (World Bank 2021)
Assessment of risk of bias in included studies
We used the RoB 2 tool (version of 22 August 2019) to analyse the risk of bias of study results (Sterne 2019). Of interest for this review is the effect of the assignment to the intervention (the intention‐to‐treat (ITT) effect); thus, we performed all assessments with RoB 2 on this effect. The outcomes that we assessed are those specified for inclusion in the summary of findings table.
Two out of six review authors (CW, MSp, MG, ALF, AAN, JD) independently assessed the risk of bias for each outcome. In case of discrepancies among their judgements and inability to reach consensus, we consulted the third review author to reach a final decision. We assessed the following types of bias as outlined in Chapter 8 (Higgins 2022b) and for cluster‐RCTs as outlined in Chapter 23 (Table 23.1.a; Higgins 2022c) of the Cochrane Handbook for Systematic Reviews of Interventions:
For RCTs:
bias arising from the randomisation process;
bias due to deviations from the intended interventions;
bias due to missing outcome data;
bias in measurement of the outcome;
bias in selection of the reported result.
For cluster‐RCTs:
bias arising from the randomisation process;
bias arising from the timing of identification and recruitment of participants;
bias due to deviations from intended interventions;
bias due to missing outcome data;
bias in measurement of the outcome;
bias in selection of the reported result.
To address these types of bias we used the signalling questions recommended in RoB 2 and made a judgement using the following options.
'Yes': if there is firm evidence that the question is fulfilled in the study (i.e. the study is at low or high risk of bias for the given the direction of the question).
'Probably yes': a judgement has been made that the question is fulfilled in the study (i.e. the study is at low or high risk of bias given the direction of the question).
'No': if there is firm evidence that the question is unfulfilled in the study (i.e. the study is at low or high risk of bias for the given the direction of the question).
'Probably no': a judgement has been made that the question is unfulfilled in the study (i.e. the study is at low or high risk of bias given the direction of the question).
'No information': if the study report does not provide sufficient information to allow any judgement.
We used the algorithms proposed by RoB 2 to assign each domain one of the following levels of bias:
low risk of bias;
some concerns;
high risk of bias.
Subsequently, we derived an overall risk of bias rating for each pre‐specified outcome in each study in accordance with the following suggestions.
'Low risk of bias': we judge the trial to be at low risk of bias for all domains for this result.
'Some concerns': we judge the trial to raise some concerns in at least one domain for this result, but not to be at high risk of bias for any domain.
'High risk of bias': we judge the trial to be at high risk of bias in at least one domain for the result, or we judge the trial to have some concerns for multiple domains in a way that substantially lowers confidence in the results.
We used the RoB 2 Excel tool to implement RoB 2 (available on the riskofbias.info website), and stored and presented our detailed RoB 2 assessments in the analyses section and as supplementary online material.
As we collected the data from the studies and assessed RoB 2, we noticed an issue with competing risk of death (Columbia Public Health 2021 as easily accessible introduction), which we discussed in Quality of the evidence of the first version of the review. We dealt with this issue within domain 3 of RoB 2 (Higgins 2019). For risk of bias in the subgroup analyses of mortality we applied the same assessments as for the respective studies' main mortality result, irrespective of whether data were primarily published or sent in upon request.
Additionally, we pioneered critical appraisal of specific sources of bias in platform trials using the Park 2020 checklist. Sources of bias were not assessed on result but at study level and this did not have a direct impact on GRADEing of the evidence.
Measures of treatment effect
For continuous outcomes, we recorded the mean, standard deviation (SD), and total number of participants in both treatment and control groups. Where continuous outcomes used the same scale, we performed analyses using the mean difference (MD) with 95% confidence intervals (CIs). For continuous outcomes measured with different scales, we had planned to perform analyses using the standardised mean difference (SMD). For interpreting SMDs, we would have re‐expressed SMDs in the original units of a particular scale with the most clinical relevance and impact.
For dichotomous outcomes, we recorded the number of events and total number of participants in both treatment and control groups. We reported the pooled risk ratio (RR) with a 95% CI (Deeks 2022).
If available, we had planned to extract and report hazard ratios (HRs) for time‐to‐event outcomes (e.g. time to liberation from invasive ventilation), but we did not find data to estimate them using the methods proposed by Parmar and Tierney (Parmar 1998; Tierney 2007).
Unit of analysis issues
The aim of this review is to summarise studies that analyse data at the level of the individual. We would also have accepted cluster‐randomised trials for inclusion, if we had found any. We collated multiple reports of one study so that the study, and not the report, is the unit of analysis. In case of adverse events, serious adverse events, hospital‐acquired infections, and invasive fungal infections only the number of events and not the number of participants are counted in most of the studies. We therefore asked the authors if they could provide us with the data as the number of participants with at least one event, i.e. as dichotomous data.
Studies with multiple treatment groups
As recommended in Chapter 6 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2022d), for studies with multiple treatment groups of the same intervention (i.e. dose, route of administration), we planned to evaluate whether study arms were sufficiently homogeneous to be combined. If arms could not be pooled, we planned to compare each arm with the common comparator separately. For pair‐wise meta‐analysis, we planned to split the ‘shared’ group into two or more groups with smaller sample size, and include two or more (reasonably independent) comparisons. For this purpose, for dichotomous outcomes, we planned to divide both the number of events and the total number of participants, and for continuous outcomes, we planned to divide the total number of participants with unchanged means and SDs.
Dealing with missing data
Chapter 10 of the Cochrane Handbook for Systematic Reviews of Interventions suggests a number of potential sources for missing data, which we took into account at study level, at outcome level, and at summary data level (Deeks 2022). At all levels, it is important to differentiate between data 'missing at random', which may often be unbiased, and 'not missing at random', which may bias study and thus review results.
Missing outcome data on general safety and corticosteroid‐specific safety, and missing adjustment for competing risk of death, had a negative impact on the certainty of the evidence in the first version of this review. Moreover, the influence of equity‐related aspects on mortality had not been examined quantitatively. Therefore, we requested from all corresponding authors data for Serious adverse events, Adverse events, Hospital‐acquired infections, and Invasive fungal infections standardised on the nominal scale as a dichotomous outcome, Participants with at least one event/patients at risk. Additionally, we requested safety data adjusted for competing risk of death and mortality data stratified by age group, sex, and ethnicity to explore equity‐related aspects. Finally, we asked corresponding authors of studies awaiting classification to clarify registration, protocol, and randomisation issues (Gautam 2021; Ghanei 2021; Rashad 2021), and make available the manuscript where only an abstract was published (Montalvan 2021).
Assessment of heterogeneity
We assessed heterogeneity of treatment effects between trials using a Chi² test with a significance level at P < 0.1. We used the I² statistic (Higgins 2003), and visual examination, to assess possible heterogeneity (I² statistic > 30% to signify moderate heterogeneity, I² statistic > 75% to signify considerable heterogeneity; Deeks 2022). If the I² statistic was above 80%, we had planned to explore potential causes through sensitivity and subgroup analyses (see Sensitivity analysis and Subgroup analysis and investigation of heterogeneity). For future updates, if we cannot identify reasons for heterogeneity in subgroup or sensitivity analysis, we will not perform a meta‐analysis but, instead, provide outcome data for all studies without an overall effect estimate.
Assessment of reporting biases
As mentioned above, we searched trials registries to identify completed studies that have not been published elsewhere, to minimise or determine publication bias. We intended to explore potential publication bias by generating a funnel plot and statistically testing this by conducting a linear regression test for meta‐analyses involving at least 10 trials (Sterne 2019). We considered P < 0.1 as significant for this test. We planned to generate a funnel plot, but had fewer than 10 studies reporting a comparable outcome.
Data synthesis
If the clinical and methodological characteristics of individual studies were sufficiently homogeneous, we pooled the data in a meta‐analysis. We performed analyses according to the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2022). Additionally, we analysed studies that included different severities of disease separately, grouping them with respect to disease severity according to need for respiratory support at randomisation (see Types of outcome measures). We treated placebo and standard care as the same intervention, as well as standard care at different institutions and time points.
We used Review Manager Web (RevMan Web) software for analyses (RevMan Web 2019). One review author entered the data into RevMan Web, and a second review author checked the data for accuracy. For most of our analyses we used the random‐effects model as planned and as required to take into account differences, for example, in settings, disease severity, and co‐medications. However, in rare cases (i.e. Analysis 1.3; Analysis 1.4; Analysis 9.2), we decided to report the fixed‐effect model as the primary analysis so that very small studies with few events did not receive extraordinary weight compared to very large studies with many events. If we deemed meta‐analysis inappropriate for a certain outcome because of heterogeneity of the included studies both statistically or conceptually or due to too high a risk of bias, we presented descriptive statistics only.
1.3. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 3: Clinical improvement: discharged alive
1.4. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 4: Clinical worsening: new need for IMV or death
9.2. Analysis.

Comparison 9: High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 2: All‐cause mortality up to 120 days
If meta‐analysis was possible, we assessed the effects of potential biases in sensitivity analyses (see Sensitivity analysis). For binary outcomes, we based the estimation of the between‐study variance on the Mantel‐Haenszel method. We explored heterogeneity above 80% with subgroup and sensitivity analyses.
Subgroup analysis and investigation of heterogeneity
Our focus was on both clinical relevance and equity, therefore we performed subgroup analyses for all‐cause mortality based on participant characteristics that may stratify health outcomes for every comparison in which data were available, irrespective of observed statistical heterogeneity.
Clinical relevance
Respiratory support at randomisation
Type of systemic corticosteroid: dexamethasone versus (methyl‐)prednisolone versus hydrocortisone
Equity‐related aspects
Sex: female versus male
Age: < 70 years versus ≥ 70 years
Ethnicity: Black, Asian, or other versus White versus unknown
Place of residence: high‐income countries (HIC) versus low‐ and middle‐income countries (LMIC)
We also performed subgroup analyses for clinical improvement (discharged alive) because the I² statistic was found to be above 80%. We made our decision on subgroup definitions before performing the first analyses. For future updates, if the I² statistic is found to be above 80% for the other outcomes, we will also conduct subgroup analyses for these outcomes (see also Assessment of heterogeneity).
Sensitivity analysis
We performed the following sensitivity analysis for all‐cause mortality up to 30 and 120 days as well as for clinical improvement (discharged alive) because I² statistic for the latter was found to be above 80%:
Risk of bias assessment components (studies with a low risk of bias or some concerns versus studies with a high risk of bias).
Platform trials versus no platform trials.
Fixed‐effect model versus random‐effects model.
Preprint versus journal publication.
Summary of findings and assessment of the certainty of the evidence
We used the GRADE approach to assess the certainty of the evidence for the following outcomes, and prepared one summary of findings table per population.
Summary of findings
We used the GRADEpro GDT software to create summary of findings tables. For time‐to‐event outcomes, we would have calculated absolute effects at specific time points, as recommended in the GRADE guidance (Skoetz 2020).
According to Chapter 14 of the Cochrane Handbook for Systematic Reviews of Interventions, the “most critical and/or important health outcomes, both desirable and undesirable, limited to seven or fewer outcomes” should be included in the summary of findings table(s) (Schünemann 2021). We included outcomes prioritised according to the core outcome sets for studies for the treatment of patients with confirmed or suspected COVID‐19 (COMET 2020), and patient relevance. These outcomes were as follows.
Individuals with a suspected or confirmed diagnosis of COVID‐19 and moderate to severe disease
-
All‐cause mortality
Up to day 30 (from here on for simplicity in this version of the review All‐cause mortality up to 30 days)
Any longer observation period from day 31 on (from here on for simplicity in this version of the review All‐cause mortality up to 120 days)
-
Improvement of clinical status during the longest observation period available:
Participants discharged alive (without clinical worsening or death)
-
Worsening of clinical status during the longest observation period available:
New need for invasive mechanical ventilation or death; that is, transition to WHO 7 to 9 if 6 or lower at baseline (Figure 1)
Serious adverse events, defined as the number of participants with any serious adverse event (serious as defined according to CTCAE (Common Terminology Criteria for Adverse Events)
Adverse events (any grade), defined as the number of participants with any adverse event
Specific adverse events: hospital‐acquired infections
Specific adverse events: invasive fungal infections
1.
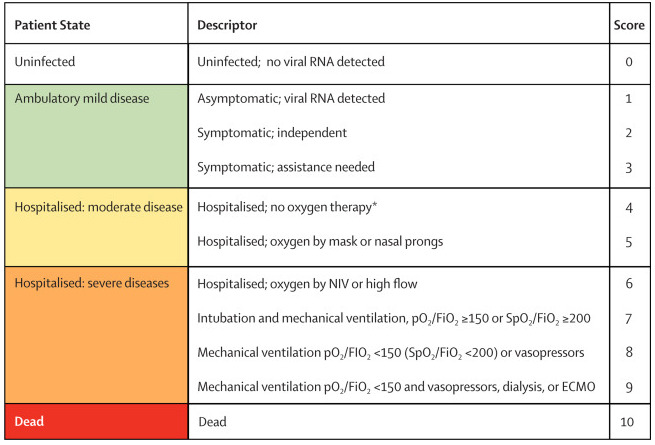
WHO Clinical Progression Scale (Marshall 2020). Copyright © 2020 Elsevier Ltd. All rights reserved: reproduced with permission.
ECMO = extracorporeal membrane oxygenation; FiO2 = fraction of inspired oxygen; NIV = non‐invasive ventilation; pO2 = partial pressure of oxygen; RNA = ribonucleic acid; SpO2 = oxygen saturation.
*If hospitalised for isolation only, record status for ambulatory patients.
Individuals with a suspected or confirmed diagnosis of SARS‐CoV‐2 infection and asymptomatic or mild disease
-
All‐cause mortality
Up to day 30
Any longer observation period
Admission to hospital or death within 28 days
Quality of life, including fatigue and neurological status, assessed with standardised scales (e.g. WHOQOL‐100) during the longest period available
Serious adverse events, defined as the number of participants with any serious adverse event (serious as defined according to CTCAE (Common Terminology Criteria for Adverse Events)
Adverse events (any grade), defined as the number of participants with any adverse event
Specific adverse events: infections
Assessment of the certainty of the evidence
We used the GRADE approach to assess the certainty of the evidence for the outcomes listed in the previous section.
The GRADE approach uses five domains (risk of bias, inconsistency, imprecision, indirectness, and publication bias) to assess certainty in the body of evidence for each prioritised outcome.
We downgraded our certainty of the evidence for:
serious (‐1) or very serious (‐2) risk of bias;
serious (‐1) or very serious (‐2) inconsistency;
serious (‐1) or very serious (‐2) uncertainty about directness;
serious (‐1) or very serious (‐2) imprecise or sparse data;
serious (‐1) or very serious (‐2) probability of reporting bias.
The GRADE system uses the following criteria for assigning grade of evidence.
'High': we are very confident that the true effect lies close to that of the estimate of the effect.
'Moderate': we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different.
'Low': our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.
'Very low': we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
We followed the current GRADE guidance for these assessments in its entirety as recommended in the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 14 (Schünemann 2021).
We used the overall risk of bias judgement, derived from the RoB 2 Excel tool, to inform our decision on downgrading for risk of bias. We phrased the findings and certainty in the evidence as suggested in the informative statement guidance (Santesso 2020).
Methods for future updates
Living systematic review considerations
Our Information Specialist (MIM) will provide us with new search records each week, which two review authors will screen, extract, evaluate, and integrate following the guidance for Cochrane living systematic reviews (Living Evidence Network 2019).
We will manually check platform trials that were previously identified and listed as 'studies awaiting classification' for additional treatment arms.
We will wait until the accumulating evidence changes our conclusions in the implications for research and practice before republishing the review. We will consider one or more of the following components to inform this decision:
findings of one or more prioritised outcomes;
credibility (e.g. GRADE rating) of one or more prioritised outcomes;
new settings, populations, interventions, comparisons, or outcomes studied.
In case of emerging policy relevance because of global controversies around the intervention, we will consider republishing an updated review even though our conclusions remain unchanged. We will review the review scope and methods approximately monthly, or more frequently if appropriate, in light of potential changes in COVID‐19 research (for example, when additional comparisons, interventions, subgroups or outcomes, or new review methods become available).
Results
Description of studies
Results of the search
We searched all databases and screened the resulting records up to 6 January 2022. We identified 3552 records. After removing duplicates, we screened 2682 records based on their titles and abstracts. We excluded 2546 records that did not meet the inclusion criteria. Of the remaining 136 records, we included 105 records:
16 RCTs (in 32 records) for inclusion in this review of which five were newly included in this second version (Maskin 2021; Munch 2021a; Munch 2021b; Taboada 2021; Toroghi 2021);
42 RCTs (in 47 records) are ongoing;
23 RCTs (in 26 records) are awaiting classification as they have been reported as being completed, but the results have not yet been published or they lack relevant information on the study design.
The study flow diagram in Figure 2 illustrates the study selection process according to the PRISMA guidelines (Moher 2009).
2.
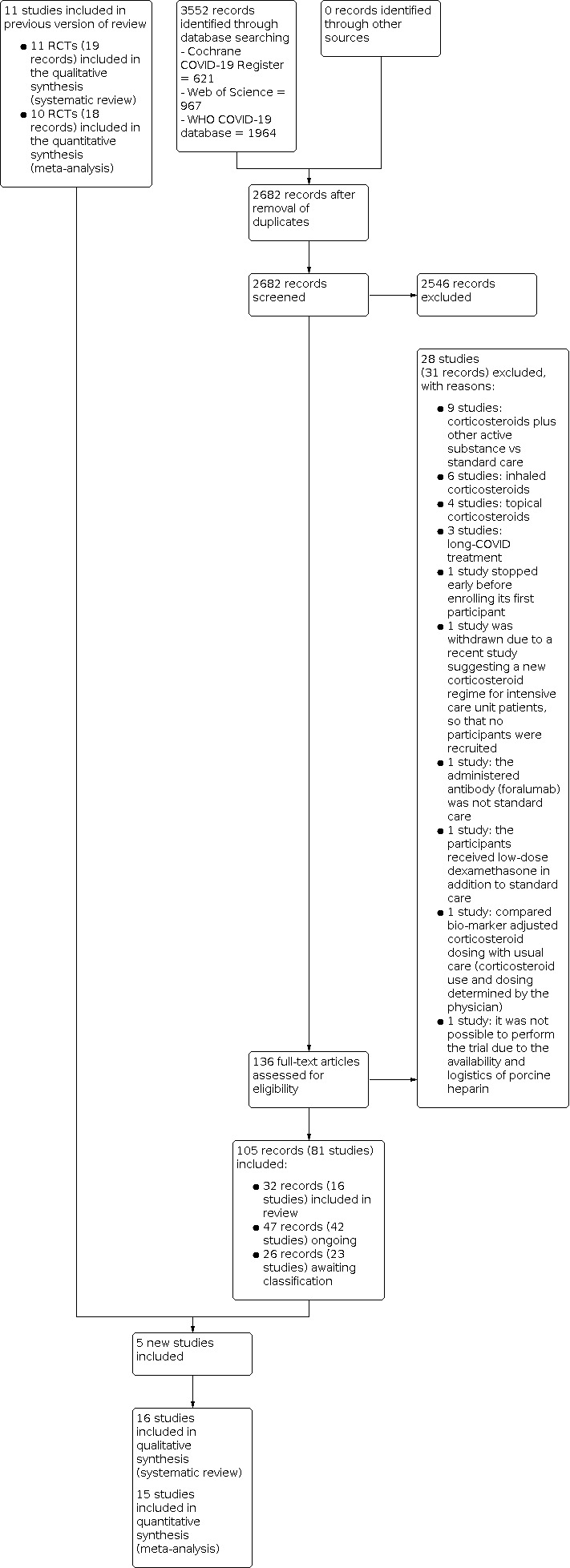
PRISMA flow diagram illustrating our study selection process.
Included studies
Design and sample size
We included 16 RCTs, of which two were multicentre platform RCTs (Horby 2021; Angus 2020), eight were multicentre RCTs (Corral‐Gudino 2021; Dequin 2020; Edalatifard 2020; Maskin 2021; Munch 2021a; Munch 2021b; Tang 2021; Tomazini 2020), and six were single‐centre RCTs (Farahani 2021; Jamaati 2021; Jeronimo 2020; Ranjbar 2021; Taboada 2021; Toroghi 2021).
Setting
Of 9549 participants in the included studies, 8418 (88%) originated from seven studies from high‐income countries (Angus 2020; Corral‐Gudino 2021; Dequin 2020; Horby 2021; Munch 2021a; Munch 2021b; Taboada 2021); 1131 (12%) participants originated from nine studies from upper‐ and lower‐middle‐income countries (Edalatifard 2020; Farahani 2021; Jamaati 2021; Jeronimo 2020; Maskin 2021; Ranjbar 2021; Tang 2021; Tomazini 2020; Toroghi 2021). There were no studies from low‐income countries.
Participants
All participants were adults hospitalised for either acute proven COVID‐19 or, as in the case of Angus 2020, Dequin 2020, Horby 2021, Jeronimo 2020, and Tomazini 2020, suspected acute COVID‐19. Positive RT‐PCR rates within the studies ranged from 100% in Maskin 2021, Munch 2021a, and Munch 2021b to about 80% in Angus 2020. All included participants were hospitalised because of symptomatic (suspected) COVID‐19 and were treated with different levels of respiratory support (no oxygen, low‐flow oxygen, high‐flow oxygen or non‐invasive ventilation (NIV), or invasive mechanical ventilation including extracorporeal membrane oxygenation (ECMO)). Based on the different levels of respiratory support at baseline, disease severity ranged from 4 to 9 on the WHO Clinical Progression Scale (Marshall 2020).
Shares of female participants ranged between 20% in Munch 2021a and 52% in Tang 2021. Means of age ranged between 54 years (standard deviation (SD) 15) in the intervention group in Jeronimo 2020 and 73 years (SD 11) in the intervention group in Corral‐Gudino 2021. No explicit information could be found regarding the proportion of vaccinated participants in any included study. However, recruitment of all studies in the comparisons 1 and 2 had ended before the first human was injected a vaccine dose outside a clinical trial worldwide on 8 December 2020 so that we deem it reasonable to declare all those participants in comparison 1 and 2 (Table 1; Table 2) "unvaccinated" with consequences for the applicability of the evidence today (Watson 2022). However, recruitment in comparison 3 (Table 3) took place until May 2021 so that we declared the vaccination status of these participants "unknown".
Interventions
Of the included completed studies, 11 compared systemic corticosteroids, which were hydrocortisone, prednisolone, methylprednisolone, and dexamethasone, to standard care (plus/minus placebo), one compared methylprednisolone to dexamethasone (Ranjbar 2021), and four directly compared different doses of dexamethasone (Maskin 2021; Munch 2021b; Taboada 2021; Toroghi 2021). The route of administration was intravenous except in Horby 2021, where both oral and intravenous administration were allowed, and Farahani 2021, with oral dose‐tapering after intravenous initiation. Doses as hydrocortisone equivalents were ≤ 200 mg/day in Angus 2020, Dequin 2020, Horby 2021, and Munch 2021a; 201 to 500 mg/day in Corral‐Gudino 2021, Jamaati 2021, Jeronimo 2020, Tang 2021, and Tomazini 2020; 1250 mg/day hydrocortisone equivalent and more as pulse dose regimen in Edalatifard 2020 and Farahani 2021. Durations of treatment differed between the studies, depending on the type of corticosteroid used, in a range between 3 days (methylprednisolone 250 mg/day, in Edalatifard 2020) and 14 days (hydrocortisone 200 mg/day tapered to 50 mg/day, in Dequin 2020). All the studies investigating the effects of dexamethasone reported treatment durations limited to 10 days (Horby 2021; Jamaati 2021; Maskin 2021; Munch 2021b; Taboada 2021; Tomazini 2020; Toroghi 2021). None of the included studies stratified data analyses according to treatment duration.
Equity‐related aspects
No study data were available for the following equity‐related elements: occupation, religion, education, socioeconomic status, and social capital. Data regarding place of residence, age, and sex were reported in all studies. Angus 2020, Horby 2021, and Jeronimo 2020 are the only trials reporting ethnicity. For details please see Table 4.
1. Equity elements of the included studies.
| Study/equity‐element | Place of residence (World Bank 2021) | Age | Ethnicity (%) | Occupation | Sex (% female) | Religion | Education | Socioeconomic status | Social capital |
| Angus 2020 | High‐income country (Australia, Canada, France, Ireland, the Netherlands, New Zealand, UK, USA) | Mean (years, SD)
|
Fixed‐dose intervention group:
Shock‐dependent intervention group:
Control group:
|
NR |
|
NR | NR | NR | NR |
| Corral‐Gudino 2021 | High‐income country (Spain) | Mean (years, SD)
|
NR | NR |
|
NR | NR | NR | NR |
| Dequin 2020 | High‐income country (France) | Median (years, IQR)
|
NR | NR |
|
NR | NR | NR | NR |
| Edalatifard 2020 | Middle‐income country (Iran) | Mean (years, SD)
|
NR | NR |
|
NR | NR | NR | NR |
| Farahani 2021 | Middle‐income country (Iran) | Mean (years, SD):
|
NR | NR |
|
NR | NR | NR | NR |
| Horby 2021 | High‐income country (UK) | Mean (years, SD):
|
Intervention group:
Control group:
|
NR |
|
NR | NR | NR | NR |
| Jamaati 2021 | Middle‐income country (Iran) | Median (years, IQR)
|
NR | NR |
|
NR | NR | NR | NR |
| Jeronimo 2020 | Middle‐income country (Brazil) | Mean (years, SD)
|
Intervention group:
Control group:
|
NR |
|
NR | NR | NR | NR |
| Maskin 2021 | Middle‐income country (Argentina) | Mean age (years, SD)
|
NR | NR |
|
NR | NR | NR | NR |
| Munch 2021a | High‐income country (Denmark) | Median (years, IQR)
|
NR | NR |
|
NR | NR | NR | NR |
| Munch 2021b | High‐income country (Denmark, India, Sweden, Switzerland) | Median (years, IQR)
|
NR | NR |
|
NR | NR | NR | NR |
| Ranjbar 2021 | Middle‐income country (Iran) | Mean (years, SD)
|
NR | NR |
|
NR | NR | NR | NR |
| Taboada 2021 | High‐income country (Spain) | Mean age (years, SD)
|
NR | NR |
|
NR | NR | NR | NR |
| Tang 2021 | Middle‐income country (China) | Median (years, IQR)
|
NR | NR |
|
NR | NR | NR | NR |
| Tomazini 2020 | Middle‐income country (Brazil) | Mean (years, SD)
|
NR | NR |
|
NR | NR | NR | NR |
| Toroghi 2021 | Middle‐income country (Iran) | Mean age (years, SD)
|
NR | NR |
|
NR | NR | NR | NR |
NR: not reported; SD: standard deviation; IQR: interquartile range
Included studies for comparison of systemic corticosteroids plus standard care to standard care (plus/minus placebo)
We included 11 studies describing 8019 participants in this comparison, of whom 3002 were randomised to corticosteroids and 5017 to standard care (plus/minus placebo). Daily hydrocortisone equivalents of the initial doses ranged from 150 mg to 5000 mg and durations of treatment ranged from zero to approximately 20 days. The majority of participants (n = 2577; 86%) randomised to corticosteroids received equivalents of 200 mg/day or less, 463 (15%) received 201 mg/day to 500 mg/day, and 48 (2%) received 501 mg/day to 5000 mg/day. Please see Table 5 for details, but note that no outcome data from Farahani 2021 (29 participants) were applicable for further analysis, resulting in quantitative analysis of 10 trials only in this comparison.
2. Characteristics of the included studies for the comparison: systemic corticosteroids versus placebo or standard care for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Study ID | Intervention and regimen | Hydrocortisone equivalent of initial dose: for 80 kg bodyweight if applicable (Stoelting 2006) | Control | Randomised to corticosteroids | Randomised to control | Study design | Place of residence (World Bank 2021) and recruitment period | Age | Sex (% female) | Population/disease severity at randomisation on WHO Clinical Progression Scale (Marshall 2020) |
| Angus 2020 | Hydrocortisone, IV, 150 mg daily for 7 days | 150 mg/d | Standard care | 143 (fixed‐dose) and 152 (shock‐dependent dose)a | 108 |
|
High‐income country (Australia, Canada, France, Ireland, the Netherlands, New Zealand, United Kingdom, USA) between March and June 2020 |
Mean (years, SD)
|
|
Severe ≥ 6 |
| Corral‐Gudino 2021 | Methylprednisolone, IV 80 mg for 3 days + 40 mg for 3 days | 400 mg/d | Standard care | 35 | 29 |
|
High‐income country (Spain) between April and May 2020 |
Mean (years, SD)
|
|
Moderate to severe 5 to 6 |
| Dequin 2020 | Hydrocortisone, IV 200 mg for 7 days, 100 mg for 4 days + 50 mg for 3 days | 200 mg/d | Placebo | 76 | 73 |
|
High‐income country (France) between March and June 2020 |
Median (years, IQR)
|
|
Moderate to severe ≥ 5 |
| Edalatifard 2020 | Methylprednisolone, IV, 250 mg for 3 days | 1250 mg/d | Standard care | 34 | 34 |
|
Middle‐income country (Iran) between March and May 2020 |
Mean (years, SD)
|
|
Moderate to severe 5 to 6 |
| Farahani 2021 | Methylprednisolone, IV 1000 mg/d for 3 days + tapering with 1 mg/kg prednisolone for 10 days | 5000 mg/d | Standard care | 14 | 15 |
|
Middle‐income country (Iran) between March and May 2020 |
Mean (years, SD):
|
|
Moderate to severe 5 to 6 |
| Horby 2021 | Dexamethasone, IV or oral 6 mg daily for 10 days | 150 mg/d | Standard care | 2104 | 4321 |
|
High‐income country (United Kingdom) between May and June 2020 |
Mean (years, SD):
|
|
Moderate to severe 4 to 9 |
| Jamaati 2021 | Dexamethasone, IV, 20 mg for 5 days + 10 mg for 5 days | 500 mg/d | Standard care | 25 | 25 |
|
Middle‐income country (Iran) in March 2020 |
Median (years, IQR)
|
|
Most likely moderate 5; no IMV at randomisation |
| Jeronimo 2020 | Methylprednisolone (as sodium succinate), IV 1 mg/kg for 5 days | 400 mg/d | Placebo | 209 | 207 |
|
Middle‐income country (Brazil) between April and June 2020 |
Mean (years, SD)
|
|
Moderate to severe 5 to 9 |
| Munch 2021a | Hydrocortisone, IV, 200 mg per day, for 7 days or until hospital discharge | 200 mg/d | Placebo | 16 | 14 |
|
High‐income country (Denmark) between April and June 2020 |
Median (years, IQR)
|
|
Severe ≥ 6 |
| Tang 2021 | Methylprednisolone, IV, 1 mg/kg for 7 days | 400 mg/d | Placebo | 43 | 43 |
|
Middle‐income country (China) between February and March 2020 |
Median (years, IQR)
|
|
Moderate 4 to 5 |
| Tomazini 2020 | Dexamethasone, IV, 20 mg for 5 days + 10 mg for 5 days | 500 mg/d | Standard care | 151 | 148 |
|
Middle‐income country (Brazil) between April and June 2020 |
Mean (years, SD)
|
|
Severe 7 to 9 |
| d: day;IMV: invasive mechanical ventilation; IV: intravenous; SD: standard deviation; IQR: interquartile range | ||||||||||
a Shock‐dependent dose: shock‐dependent dosing strategy was that restricting hydrocortisone to the period when the patient had overt shock would maximise the risk‐benefit ratio. Shock was defined as the requirement for intravenous vasopressor infusion for the treatment of shock presumed due to COVID‐19. Hydrocortisone was discontinued in the shock‐dependent group once shock was considered to have resolved or vasopressors had been discontinued for 24 hours.
Included studies for comparison of different types of systemic corticosteroids
We included Ranjbar 2021 describing 86 participants in this comparison, of whom 44 were randomised to methylprednisolone and 42 to dexamethasone. For details please see Table 6.
3. Characteristics of the included studies for the comparison: methylprednisolone versus dexamethasone for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19.
| Study ID | Intervention A | Hydrocortisone equivalent of initial dose (for 80 kg bodyweight if applicable) | Intervention B | Randomised to intervention A | Randomised to Intervention B | Study design | Place of residence (World Bank 2021) and recruitment period | Age | Sex (% female) | Population/disease severity at randomisation on WHO Clinical Progression Scale (Marshall 2020) |
| Ranjbar 2021 | Methylprednisolone 2 mg/kg, i.e. for an 80 kg participant: IV 160 mg for 5 days + 80 mg for 5 days + 40 mg for 5 days + 20 mg for 5 days (approximation of tapering scheme) | 800 mg/d in the methylprednisolone arm for an 80 kg participant 1000 mg/d in the dexamethasone arm fixed |
Dexamethasone, IV, 6 mg for 10 days | 44 | 42 |
|
Middle‐income country (Iran) between August and November 2020 |
Mean (years, SD)
|
|
Moderate 4 to 5 |
| IV: intravenous, d: day, SD: standard deviation | ||||||||||
Included studies for comparison of high‐dose dexamethasone to low‐dose dexamethasone
We included Maskin 2021, Munch 2021b, Taboada 2021, and Toroghi 2021 describing 1444 participants in this comparison, of whom 746 were randomised to high‐dose (12 mg/day or higher) dexamethasone and 698 to low‐dose (6 mg to 8 mg/day) dexamethasone. For details please see Table 7.
4. Characteristics of the included studies for the comparison: high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8 mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19.
| Study ID | Intervention dose and regimen | Hydrocortisone equivalent of initial dose: for 80 kg bodyweight if applicable (Stoelting 2006) | Control | Randomised to high‐dose dexamethasone | Randomised to low‐dose dexamethasone | Study design | Place of residence (World Bank 2021) and recruitment date | Age | Sex (% female) | Population/disease severity at randomisation on WHO Clinical Progression Scale (Marshall 2020) |
| Munch 2021b | Dexamethasone, IV, 12 mg/day for up to 10 days | 300 mg/d vs 150 mg/d | Dexamethasone, IV, 6 mg/day for up to 10 days | 503 | 497 |
|
Mainly high‐income countries (Denmark, India, Sweden, Switzerland) between August 2020 and May 2021 |
Median age (years, IQR)
|
|
Moderate to severe ≥5 |
| Maskin 2021 | Dexamethasone + standard care, IV, 16 mg once daily for 5 days, followed by 8 mg administered once daily for additional 5 days | 400 mg/d vs 150 mg/d | Dexamethasone + standard care, IV, 6 mg per day for 10 days | 49 | 51 |
|
Middle‐income country (Argentina) between June 2020 and March 2021 |
Mean age (years, SD)
|
|
Severe ≥ 7 |
| Toroghi 2021 | Arm 2: Dexamethasone, IV, 8 mg twice a day for up to 10 days or until hospital discharge Arm 3: 8 mg 3 times a day for up to 10 days or until hospital discharge |
Arm 2: 400 mg/d or Arm 3: 600 mg/d vs 200 mg/d | Dexamethasone, IV, 8 mg once a day for up to 10 days or until hospital discharge | 96 | 48 |
|
Middle‐income country (Iran) between October 2020 and January 2021 |
Mean age (years, SD)
|
|
Moderate to severe ≥ 5 |
| Taboada 2021 | Dexamethasone, IV, 20 mg once daily for 5 days, followed by 10 mg once daily for additional 5 days | 500 mg/d vs 150 mg/d | Dexamethasone, IV, 6 mg once daily for 10 days | 98 | 102 |
|
High‐income country (Spain) between January and May 2021 |
Mean age (years, SD)
|
|
Moderate to severe ≥ 5 |
| IV: intravenous; d: day; SD: standard deviation; IQR: interquartile range | ||||||||||
Outcome summary
All studies except Farahani 2021 reported utilisable dichotomous mortality data: for 7898 participants with follow‐up of up to 30 days and 485 participants with follow‐up between 31 and 120 days in the comparison of corticosteroids versus standard care (plus/minus placebo), 86 participants in the direct comparison of methylprednisolone and dexamethasone, and 1269 participants with follow‐up up to 30 days and 1399 participants with follow‐up between 31 and 120 days in the comparison of different corticosteroid doses. In the setting of acute COVID‐19 with immediate risk of death, we assumed in‐hospital mortality and all‐cause mortality with follow‐up of 14 to 30 days similar enough for meta‐analysis. For intermediate‐term survival we considered observation periods of 31 to 120 days equivalent and ready for meta‐analysis.
Other efficacy outcomes were reported heterogeneously.
The reporting of safety data was heterogeneous both in terms of whether reported at all (missing outcome data) and the underlying definitions. Including recent data requests for all studies, only four studies explicitly reported adverse events regardless of their nature and suspected relation to the intervention (Angus 2020; Edalatifard 2020; Tomazini 2020; Toroghi 2021). Another eight studies reported specific serious adverse events and adverse events related to the expected side effects of corticosteroids in both arms (Corral‐Gudino 2021; Dequin 2020; Jeronimo 2020; Maskin 2021; Munch 2021a; Munch 2021b; Taboada 2021; Tang 2021).
Apart from that, by far the largest study with 6425 participants reported safety outcomes only for the intervention arm as suspected drug reactions (Horby 2021), and three studies with 165 participants did not report safety outcomes at all (Farahani 2021; Jamaati 2021; Ranjbar 2021).
Beware that only dichotomous safety data (participants with at least one event/participants at risk) is presented narratively in the summary of findings tables, while additional discrete continuous data (number of events/participants at risk) is presented in an overview of safety data reporting with additional information (Table 8).
5. Reporting of safety data.
| Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) | |||||
| Study | Definition as published | Way of counting | Intervention group | Control group | Study design |
| Angus 2020 | Any SAE | SAE: participants with at least one event/participants at risk |
Shock‐dependent hydrocortisone: SAE: 5/141 Fixed‐dose hydrocortisone: SAE: 4/137 |
SAE: 0/52 SAE: 1/49 |
Open‐label |
| Corral‐Gudino 2021 | Microbiology‐proven infection and hyperglycaemia | AE, HAI: events/participants at risk HAI, FI: participants with at least one event/participants at risk |
AE: 14/35 HAI: 5/35 (events and participants) FI: 1/35 |
AE: 1/29 HAI: 1/29 (events and participants) FI: 0/29 |
Open‐label |
| Dequin 2020 | Nosocomial infections until day 28 defined by need for antibiotics. No other SAEs/AEs. | AE, HAI: events/participants at risk HAI: participants with at least one event/participants at risk |
AE: 40/76 HAI: 40/76 (events), 28/76 (participants) |
AE: 50/73 HAI: 50/73 (events), 30/73 (participants) |
Double‐blind |
| Edalatifard 2020 | All undesirable effects (adverse events) | HAI: events/participants at risk AE: participants with at least one event/participants at risk |
AE: 2/34 HAI: 1/34 |
AE: 2/28 HAI: 0/28 |
Single‐blind |
| Farahani 2021 | Not reported | Not applicable | — | — | Double‐blind |
| Horby 2021 | Suspected drug reactions reported | Not applicable | — | — | Open‐label |
| Jamaati 2021 | Not reported | Not applicable | — | — | Open‐label |
| Jeronimo 2020 | AE/SAE not explicitly reported Positive blood culture, need for insulin therapy, sepsis reported |
Not applicable | — | — | Double‐blind |
| Munch 2021a | Serious adverse reaction reported | Not applicable | — | — | Triple‐blind |
| Tang 2021 | Hyperglycaemia, ventilator‐associated pneumonia, stress ulcer, gastrointestinal haemorrhage | AE, HAI: participants with at least one event/participants at risk | AE: 5/43 HAI: 2/43 |
AE: 8/43 HAI: 1/43 |
Single‐blind |
| Tomazini 2020 | Glycaemic control, nosocomial infection, other AEs | SAE, AE, HAI: participants with at least one event/participants at risk | SAE: 5/151 AE: 122/151 HAI: 30/151 |
SAE: 9/148 AE: 121/148 HAI: 39/148 |
Open‐label |
| Comparison 2: Methylprednisolone versus dexamethasone | |||||
| Study | Definition as published | Way of counting | Methylprednisolone | Dexamethasone | Study design |
| Ranjbar 2021 | Not reported | Not applicable | — | — | Triple‐blind |
| Comparison 3: High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) | |||||
| Study | Definition as published | Way of counting | High‐dose | Low‐dose | Study design |
| Maskin 2021 | SAE: effects causing disability (defined as muscular weakness with a MRC scale < 48) or death AE: hyperglycaemia (≥ 200 mg/dL), delirium (positive CAM‐ICU or requirement of neuroleptic drugs), hospital‐acquired infections (according to investigator judgement) HAI: as defined by the attending physician FI: candidemia (documented as Candida sp. in blood cultures), aspergillosis (documented as Aspergillus sp. in cultures) |
SAE, FI, AE, HAI: participants with at least one event/participants at risk | SAE: 42/49 AE: 49/49 HAI: 34/49 FI: 3/49 |
SAE: 40/49 AE: 48/49 HAI: 38/49 FI: 3/49 |
Open‐label |
| Munch 2021b | Serious adverse reaction (i.e. new episodes of septic shock, invasive fungal infection, clinically important gastrointestinal bleeding, or anaphylactic reaction to dexamethasone) HAI: either new episode of septic shock OR invasive fungal infection, as per the elements of the composite outcome of ≥ 1 serious adverse reaction at day 28 FI: not further defined |
SAE, FI, HAI: participants with at least one event/participants at risk HAI, FI: events/participants at risk |
SAE: 70/497 HAI: 27/497 (events), 50/497 (participants) FI: 15/497 |
SAE: 85/485 HAI: 35/485 (events), 61/485 (participants) FI: 21/485 |
Triple‐blind |
| Taboada 2021 | AE: nosocomial infection, insuline use for hyperglycaemia, thrombosis, death at day 28 and death at day 60 | AE, HAI: events/participants at risk | AE: 58/98 HAI: 10/98 |
AE: 65/102 HAI: 10/102 |
Open‐label |
| Toroghi 2021 | AE: not further defined HAI: secondary infections |
AE, HAI: events/participants at risk | AE: 252/86 HAI: 5/86 |
AE: 122/47 HAI: 1/47 |
Open‐label |
| AE: adverse event; ICU: intensive care unit; FI: fungal infection; SAE: serious adverse event; HAI: hospital‐acquired infection; SAP: statistical analysis plan | |||||
Ongoing studies
We identified 42 ongoing RCTs with systemic application of steroids for acute COVID‐19 (details listed in Table 9), of which 25 were classified as 'recruiting' or 'ongoing' according to the study registrations. One was classified as 'active, not recruiting', for one study recruitment was completed, and one was 'temporarily halted'. Thirteen were classified as 'not yet recruiting' and one as 'not recruiting'. The majority of studies were conducted in high‐income countries (about 62%). For further characteristics of ongoing studies please see Table 9.
6. Characteristics of ongoing studies.
| Study | Sponsor/developer | Design | Place of residence (World Bank 2021) | Population/disease severity | Setting | Drug | Route of administration | Number of participants | Status |
| ACTRN12621001200875 | Royal Prince Alfred Hospital | RCT | High‐income country (Australia) |
Exhibiting mild/moderate COVID‐19 symptoms (fever, respiratory tract symptoms, dyspnoea, headache, gastrointestinal symptoms), with no requirement for oxygen or hospitalisation | Outpatient | Dexamethasone | Oral | 650 | Recruiting |
| ACTRN12621001603808 | Monash Health Hospital Victoria | RCT | High‐income country (Australia) |
Women pregnant > 16 weeks with COVID‐19 hospitalised with an oxygen requirement | Inpatient | Prednisolone, dexamethasone | Oral | 192 | Not yet recruiting |
| ChiCTR2000029386 | Chongqing Public Health Medical Center | RCT | Middle‐income country (China) |
Severe | Inpatient | Methylprednisolone | IV | 48 | Recruiting |
| ChiCTR2000029656 | Wuhan Pulmonary Hospital | RCT | Middle‐income country (China) |
Severe | Inpatient | Methylprednisolone | IV | 100 | Not yet recruiting |
| ChiCTR2000030481 | Zhongnan Hospital of Wuhan University | RCT | Middle‐income country (China) |
Diagnosed COVID‐19 infection | Inpatient | Early corticosteroid intervention, middle‐late corticosteroid intervention | Unclear, most likely systemic | 200 | Recruiting |
| CTRI/2020/07/026608 |
Dr Ananthakumar PK, Chettinad Hospital and Research Institute Kelambakkam Kancheepuram Dist Pin 603103 | RCT | Middle‐income country (India) |
Diagnosed COVID‐infection + ARDS | Inpatient | Dexamethasone, methylprednisolone | IV | 40 | Not yet recruiting |
| CTRI/2020/12/029894 | SRM Medical College Hospital and Research Centre | RCT | Middle‐income country (India) |
SpO2 < 94% under room air and requiring supplemental oxygen for hypoxaemia, respiratory rate 24 to 30/min | Inpatient | Dexamethasone, methylprednisolone | IV | 50 | Not yet recruiting |
| CTRI/2020/12/030143 | Maulana Azad Medical College and associated Lok Nayak Hospital | RCT | Middle‐income country (India) |
Admitted to ICU within 14 days of onset of symptoms; receiving invasive or non‐invasive positive pressure ventilation or respiratory support through HFNC | Inpatient | Dexamethasone, methylprednisolone | IV | 500 | Not yet recruiting |
| CTRI/2021/05/033873 | JK Hospital and LN Medical College | RCT | Middle‐income country (India) |
Excluded: moderate to severe type of disease; eligible for home isolation | Outpatient | Methylprednisolone | Oral | 500 | Not yet recruiting |
| CTRI/2021/08/035822 | Animesh Ray | RCT | Middle‐income country (India) |
Severe COVID‐19 pneumonia (SpO2 < 94%; PaO2/FiO2 < 300 mm Hg or respiratory rate (RR) > 30 breaths/min) with lack of response to dexamethasone 6 mg after 48 hours (defined as similar or worsening oxygen requirement (margin of error is 5% Fio2 for high‐flow nasal cannula, 2 L/min for NRBM, and 1 L/min for low flow oxygen devices) | Inpatient | Dexamethasone high‐dose, dexamethasone low‐dose | IV or oral | 120 | Not yet recruiting |
| EUCTR2020‐001413‐20‐ES |
Fundació Clínic per a la Recerca Biomèdica | RCT | High‐income country (Spain) |
Non‐critical patient with pneumonia in radiological progression and/or patient with progressive respiratory failure in the last 24 to 48 h | Inpatient | Methylprednisolone | IV | 100 | Temporarily halted |
| EUCTR2020‐001457‐43‐FR |
APHP | RCT | High‐income country (France) |
Admitted to ICU | Inpatient | Dexamethasone | IV | 550 | Ongoing |
| EUCTR2020‐001622‐64‐ES |
Dra Ana Pueyo Bastida | RCT | High‐income country (Spain) |
Clinical diagnosis of pulmonary involvement (respiratory symptoms ± pathological auscultation ± O2 desaturation) + chest X‐ray with mild‐moderate or normal alterations | Outpatient | Prednisone | Oral | 200 | Ongoing |
| EUCTR2020‐001707‐16‐ES |
Iis Biodonostia | RCT | High‐income country (Spain) |
Bilateral pneumonia caused by SARS‐CoV‐2 without response to the treatment: defined as persistence of fever (above 37.5 ºC without other focus) and respiratory worsening (more dyspnoea, more cough, oxygen therapy at increasing doses, worsening of the degree of respiratory distress according to the PaO2/FiO2 ratio in categories 'mild, moderate or serious') or absence of improvement with respect to the previous state | Inpatient | Methylprednisolone | IV | 60 | Ongoing |
| EUCTR2020‐001921‐30 | Azienda Ospedaliero‐Universitaria Policlinico di Modena | RCT | High‐income country (Italy) |
Positive pressure ventilation (either non‐invasive or invasive) from > 24 h, IMV from < 96 h, PaO2/FiO2 ratio < 150 | Inpatient | Methylprednisolone | IV | 200 | Ongoing |
| EUCTR2020‐003363‐25‐DK |
Department of Intensive Care, Rigshospitalet | RCT | High‐income country (Denmark) |
Severe, IMV/NIV | Inpatient | Dexamethasone (high dose and low dose) | IV | 1000 | Ongoing |
| EUCTR2020‐006054‐43‐IT | Università degli Studi di Trieste | RCT | High‐income country (Italy) |
PaO2 ≤ 60 mmHg or SpO2 ≤ 90% or on HFNC, CPAP or NPPV at randomisation | Inpatient | Methylprednisolone, dexamethasone | IV | 680 | Ongoing |
| EUCTR2021‐001416‐29‐ES | Fundación para la Investigación e Innovación Biomédica (FIIB) del Hospital Universitario Infanta Leonor y Hospital Unive | RCT | High‐income country (Spain) |
With need for oxygen therapy in NG = 1 lpm to maintain saturation = 94% | Inpatient | Dexamethasone high‐dose, dexamethasone low‐dose | IV | 200 | Ongoing |
| EUCTR2021‐004021‐71 | University Medical Center Utrecht | RCT | High‐income country (Netherlands) |
Recent COVID‐19 infection (< 3 months) | Outpatient | Prednisolone | Oral | 116 | Ongoing |
| IRCT20190606043826N2 | Esfahan University of Medical Sciences | RCT | Middle‐income country (Iran) |
Hospitalised patients with COVID‐19 | Inpatient | Dexamethasone high‐dose, dexamethasone low‐dose | IV | 60 | Recruitment completed |
| NCT04329650 | Judit Pich Martínez, Fundacion Clinic per a la Recerca Biomédica | RCT | High‐income country (Spain) |
Non‐critical patient with pneumonia in radiological progression and/or patient with progressive respiratory failure in the last 24 to 48 h | Inpatient | Methylprednisolone | IV | 200 | Recruiting |
| NCT04344730 | Assistance Publique ‐ Hôpitaux de Paris | RCT | High‐income country (France) |
Admitted to ICU | Inpatient | Dexamethasone | IV | Actual enrolment 550 | Not recruiting |
| NCT04345445 | University of Malaya | RCT | Middle‐income country (Malaysia) |
Excluded: receipt of mechanical ventilation | Inpatient | Methylprednisolone | IV | 310 | Not yet recruiting |
| NCT04377503 | Hospital Sao Domingos | RCT | Middle‐income country (Brazil) |
COVID diagnosis confirmed by real time PCR, PaO2/FIO2 < 200, laboratory: high sensitivity CRP > 5 mg/L; LDH > 245 U/L; ferritin > 300; D‐dimer > 1500; interleukin‐6 > 7.0 pg/mL | Inpatient | Methylprednisolone | Oral | 40 | Not yet recruiting |
| NCT04452565 | NeuroActiva, Inc. | RCT | High‐income country (USA) |
Excluded: IMV | Inpatient | Dexamethasone | Oral | 525 | Recruiting |
| NCT04499313 | Chattogram General Hospital | RCT | Middle‐income country (Bangladesh) |
Moderate to severe COVID‐19 infection | Inpatient | Dexamethasone, methylprednisolone | IV | 60 | Recruiting |
| NCT04509973 | Scandinavian Critical Care Trials Group | RCT | High‐income country (Denmark) |
IMV OR NIV or continuous use of CPAP for hypoxia OR oxygen supplementation with an oxygen flow of at least 10 L/min independent of delivery system | Inpatient | Dexamethasone | IV | 1000 | Active, not recruiting |
| NCT04513184 | Edda Sciutto Conde | RCT | Middle‐income country (Mexico) |
Hospitalised patients with moderate to severe respiratory complications that have not received mechanical ventilation | Inpatient | Dexamethasone | IV vs nasal | 60 | Recruiting |
| NCT04528329 | ClinAmygate | RCT | Middle‐income country (Egypt) |
Mild to moderate severity | Unclear | Dexamethasone | Unclear, most likely systemic | 300 | Recruiting |
| NCT04528888 | Massimo Girardis, University of Modena and Reggio Emilia | RCT | High‐income country (Italy) |
Included: positive pressure ventilation (IMV/NIV) for > 24 h, IMV from < 96 h, PaO2/FiO2 ratio < 150 | Inpatient | Methylprednisolone | IV | 210 | Recruiting |
|
NCT04545242 |
Dr. Negrin University Hospital | RCT | High‐income country (Spain) |
Intubated and mechanically ventilated | Inpatient | Dexamethasone | IV | 980 | Not yet recruiting |
| NCT04636671 | University of Trieste | RCT | High‐income country (Italy) |
Excluded: on IMV Included: PaO2 ≤ 60 mmHg or SpO2 ≤ 90% or on HFNC, CPAP or NPPV at randomisation |
Inpatient | Dexamethasone, methylprednisolone | IV | 680 | Recruiting |
| NCT04663555 | Brno University Hospital | RCT | High‐income country (Czech Republic) |
Intubation/mechanical ventilation or ongoing HFNC oxygen therapy; admission to ICU | Inpatient | Dexamethasone | IV | 300 | Recruiting |
| NCT04673162 | Azienda Unità Sanitaria Locale Reggio Emilia | RCT | High‐income country (Italy) |
Need for supplemental oxygen in any delivery mode with the exception of IMV | Inpatient | Methylprednisolone | IV | 260 | Not yet recruiting |
| NCT04707534 | University of Oklahoma | RCT | High‐income country (USA) |
Positive pressure ventilation (non‐invasive or invasive) or HFNC or need supplemental oxygen with oxygen mask or nasal cannula | Inpatient | Dexamethasone | Unclear, most likely systemic | 300 | Recruiting |
| NCT04765371 | Centre Hospitalier René Dubos | RCT | High‐income country (France) |
Patient with SpaO2 ≤ 94 % in room air (90% for patient with respiratory failure) and requiring an oxygen therapy | Inpatient | Dexamethasone, prednisolone | Unclear, most likely systemic | 220 | Recruiting |
| NCT04780581 | Fundación Instituto de Estudios de Ciencias de la Salud de Castilla y León | RCT | High‐income country (Spain) |
Requires supplementary oxygen due to basal saturation ≤ 93% (with ambient O2, 21%), excluded if IMV, NIV, HFNC | Inpatient | Dexamethasone, methylprednisolone | Unclear, most likely systemic | 290 | Recruiting |
| NCT04795583 | University of Alberta | RCT | Middle‐income country (Colombia, Mexico) |
Ambulatory, confirmed SARS‐CoV‐2. Clinical symptoms compatible with COVID‐19 for ≤ 14 days before randomisation. Oxygen saturation ≥ 95% | Outpatient | Prednisone | Oral | 1526 | Not yet recruiting |
| NCT04834375 | Northwell Health | RCT | High‐income country (USA) | Hypoxaemia defined by an oxygen saturation < 94% or the need for supplemental oxygen | Inpatient | Dexamethasone | IV | 142 | Recruiting |
| NCT04836780 | Hospital Universitario Infanta Leonor | RCT | High‐income country (Spain) | Peripheral capillary oxygen saturation (SpO2) ≥ 94% and < 22 breaths per minute (bpm) breathing room air. High risk of developing ARDS | Inpatient | Dexamethasone | IV |
126 | Recruiting |
| NCT04860518 | Faron Pharmaceuticals Ltd | RCT | High‐income country (USA) | Admitted to hospital with respiratory symptoms of COVID‐19 requiring hospital care and oxygen supplementation (≤ 8L/min) | Inpatient | Dexamethasone and human intravenous interferon beta‐Ia | IV | 140 | Recruiting |
| TCTR20211017001 | Faculty of Medicine Ramathibodi Hospital | RCT | Middle‐income country (Thailand) |
Resting oxygen saturation between 90% and 94% | Inpatient | Methylprednisolone, dexamethasone | IV | 120 | Not yet recruiting |
| ARDS: acute respiratory distress syndrome; CPAP: continuous positive airway pressure; CRP: c‐reactive protein; FiO2: fraction of inspired oxygen; HFNC: high‐flow nasal cannula; ICU: intensive care unit; IMV: invasive mechanical ventilation; IV: intravenous; LDH: lactic dehydrogenase; NIV: non‐invasive ventilation; NPPV: non‐invasive positive pressure ventilation; PaO2: partial pressure oxygen; PCR: polymerase chain reaction RCT: randomised; controlled trial; RT‐PCR: reverse transcription polymerase chain reaction; SpO2: blood oxygen saturation | |||||||||
On excluding the studies that were 'not recruiting', 'not yet recruiting', and 'active, not recruiting' the 27 studies that were recruiting, ongoing, temporarily halted and that completed recruitment comprised a total of 7617 expected participants. Most of the potentially eligible ongoing studies identified intend to recruit people who are admitted to hospital and require varying levels of respiratory support. Of the 42 ongoing studies, 15 planned to test dexamethasone, 11 methylprednisolone, and three prednisolone or prednisone. Four studies planned to compare different dexamethasone dosing regimens. Eight studies planned to compare dexamethasone to methylprednisolone, and one study dexamethasone to prednisolone, another dexamethasone to human intravenous interferon beta‐Ia. One study planned to compare corticosteroids at different time points.
Studies awaiting classification
We identified 23 RCTs with systemic application of steroids for acute COVID‐19 (details listed in Table 10). Of the 23 studies comprising 5608 expected participants, 15 were classified as ‘completed’, four as ‘prematurely ended’, and four as 'terminated' (due to lack of enrolment, too few participants, local recommendations or corticosteroid use approval), according to the study registrations. For four studies, the full‐text publications are available, but the methodology is unclear. For one study only the abstract is available, which does not provide any information on the randomisation process. The majority of studies were conducted in low‐ and middle‐income countries (about 56%; for details see Table 10).
7. Characteristics of studies awaiting classification.
| Study | Sponsor/developer | Design | Place of residence (World Bank 2021) | Population/disease severity | Setting | Drug | Route of administration | Number of participants | Status |
| EUCTR2020‐001333‐13‐FR | Groupe Hospitalier Paris Saint‐Joseph | RCT | High‐income country (France) |
Included: patient diagnosed COVID positive by RT‐PCR and/or scanner (patients admitted with already mechanical ventilation and sedation, or with acute respiratory failure evolving very quickly) | Inpatient | Dexamethasone | IV | 122 | Prematurely ended |
| EUCTR2020‐001307‐16‐ES |
Fundación para la Investigación Biomédica Hospital Ramón y Cajal | RCT | High‐income country (Spain) |
ARDS | Inpatient | Methylprednisolone | IV | 104 | Prematurely ended |
| EUCTR2020‐001553‐48‐FR | Hospices Civils de Lyon | RCT | High‐income country (France) |
Peripheral saturation by pulse oximeter SpO2 ≤ 94% in ambient air measured twice at 5‐ to 15‐min intervals, or PaO2/FiO2 < 300 mmHg | Inpatient | Prednisone | Oral | 304 | Prematurely ended |
| IRCT20081027001411N3 | Teheran University of Medical Sciences | RCT | Middle‐income country (Iran) |
Blood oxygen saturation < 93%; with ARDS | Inpatient | Prednisolone | Not stated | 60 | Completed |
| IRCT20120215009014N354 | Hamedan University of Medical Sciences | RCT | Middle‐income country (Iran) |
Hospitalised in ICU, bilateral pulmonary infiltration in chest X‐ray or CT‐scan; respiratory distress with > 24 breaths per minute | Inpatient | Hydrocortisone, methylprednisolone, dexamethasone | IV | 81 | Completed |
| IRCT20160118026097N4 | Ghoum University of Medical Sciences | RCT | Middle‐income country (Iran) |
Hypoxia requires supplemental oxygen to maintain oxygen saturation > 90% | Inpatient | Dexamethasone | Not stated | 64 | Completed |
| IRCT20200611047727N3 | Shahid Beheshti University of Medical Sciences | RCT | Middle‐income country (Iran) | Oxygen saturation level < 93 | Inpatient | Methylprednisolone | IV | 60 | Completed |
| IRCT20201015049030N1 | Teheran University of Medical Sciences | RCT | Middle‐income country (Iran) | Blood oxygen saturation between 90% and 95% | Outpatient | Dexamethasone | Not stated | 200 | Completed |
|
ISRCTN33037282 |
Clínica Medellín ‐ Grupo Quirónsalud | RCT | Middle‐income country (Colombia) |
PaO2 ≤ 60 mmHg or SpO2 ≤ 90% or on HFNC, CPAP or NPPV at randomisation Excluded: on IMV |
Inpatient | Methylprednisolone, dexamethasone | IV | 680 | Completed |
| NCT04244591 | Peking Union Medical College Hospital | RCT | Middle‐income country (China) | PaO2/FiO2 < 200 mmHg; positive pressure ventilation (non‐invasive or invasive) or HFNC > 45 L/min for < 48 h; requiring ICU admission | Inpatient | Methylprednisolone | Not stated | 80 | Completed |
| NCT04325061 | Dr. Negrin University Hospital | RCT | High‐income country (Spain) | Intubated and mechanically ventilated | Inpatient | Dexamethasone | IV | 19 | Terminated (lack of enrolment) |
| NCT04530409 | ClinAmygate | RCT | Middle‐income country (Egypt) |
Mild and moderate severity | Unclear | Dexamethasone | Unclear, most likely systemic | 450 | Completed |
| NCT04746430 | General Practitioners Research Institute | RCT | High‐income country (Netherlands) | Exercise‐induced desaturation, defined as SpO2 < 92% (< 90% for COPD patients) and/or an absolute drop of ≥ 4% in SpO2 after a 1‐min sit‐to‐stand test or SpO2 < 92% (< 90% for COPD patients) at rest with GP's and patient's shared decision to keep patient at home despite this in itself being an indication for referral to hospital | Outpatient | Dexamethasone | Unclear, most likely systemic | 2000 | Terminated (too few patients) |
| EUCTR2020‐002186‐34‐ES | Fundació Hospital Universitari Vall d'Hebron ‐ Institut de Recerca (VHIR) | RCT | High‐income country (Spain) | Air oxygen saturation > 90 and < 94%; PaO2/FiO2 > 200 and ≤ 300 mmHg; Sa:FiO2 (O2 saturation measured with pulse oximeter/inspired O2 fraction) ≤ 350 | Inpatient | Methylprednisolone | IV | 100 | Prematurely ended |
| EUCTR2020‐004323‐16 |
Azienda Ospedaliera Arcispedale Santa Maria Nuova/IRCCS di Reggio Emilia | RCT | High‐income country (Italy) | Need for supplemental oxygen in any delivery mode with the exception of IMV | Inpatient | Methylprednisolone | IV | 260 | Completed |
| NCT04347980 | Centre Chirurgical Marie Lannelongue | RCT | High‐income country (France) | Admitted to ICU | Inpatient | Dexamethasone | IV | 122 | Terminated (ANSM (Agence nationale de sécurité du médicament et des produits de santé) Recommendation) |
| NCT04438980 | Fundacion Miguel Servet | RCT | High‐income country (Spain) | Hospitalised Excluded: SpO2 < 90% (in air ambient) or PaO2 < 60 mmHg (in ambient air) or PaO2/FiO2 < 300 mmHg |
Inpatient | Methylprednisolone | IV | 72 | Completed |
| NCT04451174 | University of Chile | RCT | High‐income country (Chile) | Excluded: requirements of mechanical ventilation (IMV/NIV) Included: oxygen requirements until 35 % by Venturi mask or 5 L/min by nasal cannula |
Inpatient | Prednisone | IV | 184 | Terminated (corticosteroid use approval) |
| Salukhov 2021 | Not stated | RCT (unclear randomisation process) | Middle‐income country (Russia) | Moderate to severe course with process prevalence according to computed tomography without hypoxaemia (saturation SpO2 > 93%) with a duration of hyperthermia > 38 °C for 3 days or more and C‐reactive protein levels of 15 to 50 mg/L | Inpatient | Methylprednisolone | oral | 40 | Completed and published (but unclear randomisation process) |
| Ghanei 2021 | Not stated | RCT | Middle‐income country (Iran) | Oxygen saturation (Spo2) less than 94% | Inpatient | Prednisolone | Not stated | 236 | Completed and published (not pre‐registered, no ethics vote named, no patient informed consent) |
| Gautam 2021 | None | RCT | Middle‐income country (India) | Moderate to severe COVID‐19, oxygen saturation < 93% on room air | Inpatient | Methylprednisolone, dexamethasone | IV | 140 | Completed and published (not pre‐registered, no ethics vote named, no patient informed consent, no information about randomisation) |
| Montalvan 2021 | Not stated | RCT (unclear randomisation process) | Middle‐income country (Honduras) |
Not stated | Inpatient | Dexamethasone | Not stated | 81 | Completed and abstract published (no registration number, no information about randomisation process), only abstract available |
| Rashad 2021 | South Valley University | RCT (unclear randomisation process) | Middle‐income country (Egypt) | Moderate to severe ≥ 5 | Inpatient | Dexamethasone | IV | 149 | Completed and published (no pre‐registration, unclear randomisation process) |
| ARDS: acute respiratory distress syndrome; COPD: chronic obstructive pulmonary disease; CT: computed tomography; HFNC: high‐flow nasal cannula;ICU: intensive care unit; RCT: randomised controlled trial; RT‐PCR: reverse transcription polymerase chain reaction. | |||||||||
Only one of the studies awaiting classification was placebo‐controlled and compared methylprednisolone in addition to standard care to standard care plus placebo. Four studies planned to compare dexamethasone, four methylprednisolone, and three prednisolone or prednisone (each in addition to standard care) to standard care only. One open‐label study planned to compare methylprednisolone without specification of the control. Two studies planned to compare dexamethasone to methylprednisolone, one study methylprednisolone to prednisolone, and one study hydrocortisone to methylprednisolone to dexamethasone. Two other studies planned to compare dexamethasone plus hydroxychloroquine to hydroxychloroquine only and one prednisolone plus hydroxychloroquine plus azithromycin plus naproxen to hydroxychloroquine plus azithromycin plus naproxen. One study planned to compare two different treatment regimes: an early versus a late treatment with dexamethasone. One study planned to compare different doses of dexamethasone. Another study compared dexamethasone to tocilizumab.
Excluded studies
We excluded 28 studies (31 references) that did not meet our inclusion criteria.
Nine studies investigated corticosteroids plus other active substances versus standard care (EUCTR2020‐001445‐39‐ES; IRCT20120225009124N4; IRCT20190312043030N2; NCT04341038; NCT04411667; NCT04468646; NCT04561180; NCT04640168; NCT04826822).
Six studies examined inhaled corticosteroids (EUCTR2020‐001616‐18‐ES; EUCTR2020‐001889‐10; ISRCTN86534580; NCT04355637; NCT04381364; NCT04416399).
Four studies investigated topical corticosteroids (IRCT20200522047542N1; NCT04361474; NCT04484493; NCT04569825).
Three studies considered corticosteroids for long‐COVID treatment (NCT04551781; NCT04534478; NCT04657484).
One study stopped early before enrolling its first participant (NCT04359511).
One study was withdrawn due to a recent study suggesting a new corticosteroid regime for intensive care unit patients, so that no participants were recruited (NCT05133635).
In one study the administered antibody (foralumab) was not standard care (Moreira 2021).
In one study the participants received low‐dose dexamethasone in addition to standard care (Naik 2021).
One study compared bio‐marker adjusted corticosteroid dosing with usual care (corticosteroid use and dosing determined by the physician) (Odeyemi 2021).
For one study it was not possible to perform the trial due to the availability and logistics of porcine heparin (NCT04485429).
Risk of bias in included studies
We assessed the risk of bias of results from 15 RCTs that contributed to our analyses (Angus 2020; Corral‐Gudino 2021; Dequin 2020; Edalatifard 2020; Horby 2021; Jamaati 2021; Jeronimo 2020; Maskin 2021; Munch 2021a; Munch 2021b; Ranjbar 2021;Taboada 2021; Tang 2021; Tomazini 2020; Toroghi 2021), using the RoB 2 tool (version 22 August 2019) recommended in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2022b). We made no assessment of bias for Farahani 2021 as it did not report any outcomes relevant to this review.
The 15 studies contributed 47 study results to eight outcomes in the respective summary of findings tables and three more in additional analyses for inpatient individuals. The completed RoB 2 tool with responses to all assessed signalling questions is available online at: https://zenodo.org/record/6500842.
Overall judgements for studies that included individuals with a confirmed diagnosis of moderate to severe COVID‐19
Overall risk of bias by study
From 47 study results, we rated 5 (11%) at low risk of bias, noted some concerns in 20 (43%) study results, and rated 22 (47%) at high risk of bias. Regarding the respective studies we included the following:
Angus 2020 ‐ two study results with some concerns and one with high risk.
Corral‐Gudino 2021 ‐ one study result with some concerns and two with high risk.
Dequin 2020 ‐ one study result with some concerns and one with high risk.
Edalatifard 2020 ‐ two study results with some concerns and one with high risk.
Horby 2021 ‐ three study results with some concerns and one with high risk.
Jamaati 2021 ‐ one study result with some concerns.
Jeronimo 2020 ‐ two study results with some concerns and three with high risk.
Maskin 2021 ‐ two study results with some concerns and four with high risk.
Munch 2021a ‐ two study results with low risk.
Munch 2021b ‐ two study results with low risk and three with high risk.
Ranjbar 2021 ‐ one study result with some concerns.
Taboada 2021 ‐ three study results with some concerns.
Tang 2021 ‐ one study result with low risk and two with high risk.
Tomazini 2020 ‐ two study results with some concerns and three with high risk.
Toroghi 2021 ‐ one study result with high risk.
Overall risk of bias by outcome
Systemic corticosteroids (plus standard care) versus standard care (plus/minus placebo)
We had some concerns about all‐cause‐mortality up to 30 days (Table 84) and all‐cause‐mortality up to 120 days (Table 85) because of issues with randomisation, deviations from intended interventions, and pre‐specification of the outcomes. We also applied the respective risk of bias assessments to the six subgroup analyses (Table 95; Table 96; Table 97; Table 98; Table 99; Table 100; Table 101; Table 102). We also had some concerns about clinical improvement (discharged alive) because of issues with randomisation, deviations from intended intervention, assessment, and pre‐specification of the outcome (Table 86). There were some concerns about clinical worsening (new need for invasive mechanical ventilation (IMV) or death) because of deviations from intended interventions and assessment of the outcome only (Table 87). We judged all safety outcomes (serious adverse events, adverse events, hospital‐acquired infections, and invasive fungal infections), need for dialysis, and viral clearance to be at high risk of bias mainly due to missing adjustment for competing risk of death (Table 88; Table 89; Table 90; Table 91; Table 93; Table 94).
Risk of bias for analysis 1.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | 15% of the participants in the no hydrocortisone group received hydrocortisone | Low risk of bias | Data were available for this outcome. 238 participants were randomised and 238 were analysed. | Low risk of bias | Mortality is an observer‐reported outcome not involving judgement. | Low risk of bias | Protocol and SAP are available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention |
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | 15% of the participants in the no hydrocortisone group received hydrocortisone | Low risk of bias | Data were available for this outcome. 238 participants were randomised and 238 were analysed. | Low risk of bias | Mortality is an observer‐reported outcome not involving judgement. | Low risk of bias | Protocol and SAP are available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention |
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | Open‐label design (participants and clinicians were aware of the assigned treatment). ITT data presented. | Low risk of bias | No substantial data missing. | Low risk of bias | Both groups were measured at the same time and the measurements were similar between groups. | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results and missing information about the allocation concealment. |
| Dequin 2020 | Low risk of bias | Randomisation was centralised and performed electronically. Allocation sequences were generated in a 1:1 ratio by a computer‐generated random number using a blocking schema. There were no baseline differences between the groups. | Low risk of bias | Protocol: Patients, investigators and care providers will be blinded for the patient‐arm. ITT was used. | Low risk of bias | Data were available for this outcome. | Low risk of bias | The measurements were similar between groups. | Some concerns | The protocol and statistical analysis plan were available. 21‐day mortality was a post hoc outcome. | Some concerns | Overall judged some concerns due to selection of reported results. |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone. | Low risk of bias | 6425 participants were randomised and 6425 were analysed. | Low risk of bias | Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Jamaati 2021 | Some concerns | The selected patients were allocated to either the dexamethasone group or the control group by block randomisation. Ten blocks were generated by the Online Randomiser website. Pulmonary disease was highly significantly more prevalent in the control group. Additionally, baseline level of respiratory support was not reported so that we can only assume the most likely circumstance, i.e. that no support beyond oxygen insufflation had been given until randomisation. |
Low risk of bias | No deviations mentioned. ITT data reported. | Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups. | Some concerns | Trial registered after recruitment stop. No analysis plan published beyond registry entry. | Some concerns | Potential bias through probably problematic block randomisation with significant baseline imbalance for pulmonary disease, very delayed registration, and potentially not pre‐specified stop for futility raise some concerns. The issues were not discussed. Potential mild bias towards experimental. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment Control group: 5 excluded before starting treatment, 3 excluded after starting treatment |
Low risk of bias | 416 participants randomised and 416 participants analysed. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | Some concerns | Overall judged some concerns due to protocol deviations. |
| Munch 2021a | Low risk of bias | No issues with randomisation process. | Low risk of bias | Withdrawals with consecutive open‐label steroids may have affected the outcome, but withdrawals and non‐compliance was rather balanced after all. | Low risk of bias | No missing data. | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with the reported result. | Low risk of bias | Withdrawals because of the experimental context lead to some concerns (but it is less than 10% of all patients). |
| Tang 2021 | Low risk of bias | Randomisation was stratified by the statistician of the leading site, who produced computer‐generated block randomisation lists with a block size of 4 patients. | Low risk of bias | Single‐blind design (participants), ITT data presented. No deviations reported. | Low risk of bias | No missing data. | Low risk of bias | The data collection and end point judgement were blinded, and the statisticians were also blinded during the statistical analysis. The measurements were similar between groups | Low risk of bias | 30‐day mortality as pre‐specified in the trial registration was not explicitly reported, but could reliably derive from a synopsis of full text, figures, and supplemental material. | Low risk of bias | All domains were rated low risk of bias. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | No missing data. | Low risk of bias | Individuals who assessed the outcomes were not blinded for the assigned treatment. Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall judged some concerns because of protocol deviations |
Risk of bias for analysis 1.2 All‐cause mortality up to 120 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Edalatifard 2020 | Some concerns | No information about the allocation concealment. | Some concerns | 6 patients in the control group received the intervention drug and were excluded from the analyses (17%). | Low risk of bias | The data were requested from the authors because the follow‐up time was not clearly visible from the publication. | Low risk of bias | The measurements were similar between groups. | Some concerns | Neither the protocol nor the SAP were available | Some concerns | Overall judged some concerns due to the randomisation process, protocol deviations and the selection of the reported results. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment Control group: 5 excluded before starting treatment, 3 excluded after starting treatment |
Low risk of bias | 416 participants randomised and 416 participants analysed. | Low risk of bias | The measurements were similar between groups. | Some concerns | Protocol and statistical plan available. Outcome was not pre‐specified. | Some concerns | Overall judged some concerns due to protocol deviations and selective reporting. |
| Munch 2021a | Low risk of bias | No issues with randomisation process. | Low risk of bias | Withdrawals with consecutive open‐label steroids may have affected the outcome, but withdrawals and non‐compliance was rather balanced after all. | Low risk of bias | No missing data. | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with the reported result. | Low risk of bias | Withdrawals because of the experimental context lead to some concerns (below 10% of all patients). |
Risk of bias for analysis 2.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 2.1.1 No oxygen | ||||||||||||
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | 6425 randomised, 6425 analysed | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Subgroup 2.1.2 Low‐flow oxygen only | ||||||||||||
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | No protocol deviations. ITT data presented. | Low risk of bias | We requested the data from the authors, as the data was not broken down by our subgroups of interest in the publication | Low risk of bias | The measurements were similar between groups | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment Control group: 5 excluded before starting treatment, 3 excluded after starting treatment |
Low risk of bias | 416 participants randomised and 416 participants analysed. | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | Some concerns | Overall judged some concerns due to protocol deviations. |
| Subgroup 2.1.3 NIV, high‐flow, and low‐flow oxygen combined | ||||||||||||
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | 6425 randomised, 6425 analysed | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Subgroup 2.1.4 NIV or high‐flow oxygen only | ||||||||||||
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | No protocol deviations. ITT data presented. | Low risk of bias | We requested the data from the authors, as the data was not broken down by our subgroups of interest in the publication | Low risk of bias | The measurements were similar between groups | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment Control group: 5 excluded before starting treatment, 3 excluded after starting treatment |
Low risk of bias | 416 participants randomised and 416 participants analysed. | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | Some concerns | Overall judged some concerns due to protocol deviations. |
| Subgroup 2.1.5 Invasive ventilation | ||||||||||||
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | 6425 randomised, 6425 analysed | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment Control group: 5 excluded before starting treatment, 3 excluded after starting treatment |
Low risk of bias | 416 participants randomised and 416 participants analysed. | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | Some concerns | Overall judged some concerns due to protocol deviations. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall judged some concerns because of protocol deviations. |
Risk of bias for analysis 3.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 3.1.1 Dexamethasone | ||||||||||||
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | 6425 randomised, 6425 analysed | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available | Some concerns | Overall judged some concerns due to protocol deviations. |
| Jamaati 2021 | Some concerns | The selected patients were allocated to either the dexamethasone group or the control group by block randomisation. Ten blocks were generated by the Online Randomiser website. Pulmonary disease was highly significantly more prevalent in the control group. Additionally, baseline level of respiratory support was not reported so that we can only assume the most likely circumstance, i.e. that no support beyond oxygen insufflation had been given until randomisation. |
Low risk of bias | No deviations mentioned. ITT data reported. | Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups. | Some concerns | Trial registered after recruitment stop. No analysis plan published beyond registry entry. | Some concerns | Overall judged some concerns due to selective reporting and baseline differences. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall judged some concerns due to protocol deviations. |
| Subgroup 3.1.2 Methylprednisolone | ||||||||||||
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | Open‐label study. ITT data presented. | Low risk of bias | No substantial data missing. | Low risk of bias | The measurements were similar between groups | Some concerns | Endpoint was registered in Eudra‐CT as in‐hospital mortality but reported as 28d‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selective reporting. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment Control group: 5 excluded before starting treatment, 3 excluded after starting treatment |
Low risk of bias | 416 participants randomised and 416 participants analysed. | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | Some concerns | Overall judged some concerns due to protocol deviations. |
| Tang 2021 | Low risk of bias | Randomisation was stratified by the statistician of the leading site, who produced computer‐generated block randomisation lists with a block size of 4 patients. | Low risk of bias | ITT data presented. No deviations reported. | Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | 30‐day mortality as pre‐specified in the trial registration could was not explicitly reported, but could reliably derive from a synopsis of full text, figures, and supplemental material. | Low risk of bias | All domains were rated low. |
| Subgroup 3.1.3 Hydrocortisone | ||||||||||||
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | 15% of the participants in the no hydrocortisone group received corticosteroids | Low risk of bias | No missing data. | Low risk of bias | Mortality is an observer‐reported outcome not involving judgement. | Low risk of bias | Protocol and SAP available | Some concerns | Overall judged some concerns due to protocol deviations |
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | 15% of the participants in the no hydrocortisone group received corticosteroids | Low risk of bias | No missing data. | Low risk of bias | Mortality is an observer‐reported outcome not involving judgement. | Low risk of bias | Protocol and SAP available | Some concerns | Overall judged some concerns due to protocol deviations |
| Dequin 2020 | Low risk of bias | Randomisation was centralised and performed electronically. Allocation sequences were generated in a 1:1 ratio by a computer‐generated random number using a blocking schema. There were no baseline differences between the groups. | Low risk of bias | Protocol: Patients, investigators and care providers will be blinded for the patient‐arm ITT was used |
Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups. | Some concerns | The protocol and statistical analysis plan were available. 21‐day mortality was a post hoc outcome | Some concerns | Overall judged some concerns due to selective reporting. |
| Munch 2021a | Low risk of bias | No issues with randomisation process. | Low risk of bias | Withdrawals with consecutive open‐label steroids may have affected the outcome, but withdrawals and non‐compliance was rather balanced after all. | Low risk of bias | No missing data. | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with the reported result. | Low risk of bias | Withdrawals because of the experimental context lead to some concerns (below 10% of all patients). |
Risk of bias for analysis 3.2 All‐cause mortality up to 120 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 3.2.1 Hydrocortisone | ||||||||||||
| Munch 2021a | Low risk of bias | No issues with randomisation process. | Low risk of bias | Withdrawals with consecutive open‐label steroids may have affected the outcome, but withdrawals and non‐compliance was rather balanced after all. | Low risk of bias | No missing data | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with the reported result. | Low risk of bias | Withdrawals because of the experimental context lead to some concerns (below 10% of all patients). |
| Subgroup 3.2.2 Methylprednisolone | ||||||||||||
| Edalatifard 2020 | Some concerns | No information about the allocation concealment. | Some concerns | 6 patients in the control group received the intervention drug and were excluded from the analyses (17%). | Low risk of bias | The data were requested from the authors because the follow‐up time was not clearly visible from the publication. | Low risk of bias | The measurements were similar between groups. | Some concerns | Neither the protocol nor the SAP were available | Some concerns | Overall judged some concerns due to the randomisation process, protocol deviations and the selection of the reported results. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment ; Control group: 5 excluded before starting treatment, 3 excluded after starting treatment | Low risk of bias | Data is available for all participants. | Low risk of bias | The measurements were similar between groups, | Some concerns | No pre‐specification of the outcome in the protocol. | Some concerns | Overall we judged some concern due to protocol deviations and selective reporting |
Risk of bias for analysis 3.3 Clinical improvement: discharged alive.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 3.3.1 Dexamethasone | ||||||||||||
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | Data for this outcome was available for all participants randomised. | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement. | Low risk of bias | No issue with selective reporting. | Some concerns | Overall judged some concerns due to the randomisation process, protocol deviations and limited bias in measurement. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | Data for this outcome was available for all participants randomised | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall rated some concerns due to protocol deviations and measurement of the outcome. |
| Subgroup 3.3.2 Methylprednisolone | ||||||||||||
| Edalatifard 2020 | Some concerns | No information about the allocation concealment. | Some concerns | In this study, patients did not know which group of them used medicine Physicians and clinicians team know about the medicine and intervention groups. 6 patients in the control group received the intervention drug and were excluded from the analyses Intention‐to‐treat |
Low risk of bias | Data for this outcome was available for all participants randomised | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement.No protocol or SAP available. | Some concerns | Neither the protocol nor the SAP were available | Some concerns | Overall judged some concerns due to missing information about the allocation concealment, deviations from the intended interventions, measurement of the outcome and selection of the reported result |
Risk of bias for analysis 4.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 4.1.1 Female | ||||||||||||
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | Open‐label design (participants and clinicians were aware of the assigned treatment). ITT data presented. | Low risk of bias | No substantial data missing. | Low risk of bias | Both groups were measured at the same time and the measurements were similar between groups. | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results and missing information about the allocation concealment. |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone. | Low risk of bias | 6425 participants were randomised and 6425 were analysed. | Low risk of bias | Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | No missing data. We requested the data from the authors. | Low risk of bias | Individuals who assessed the outcomes were not blinded for the assigned treatment. Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall judged some concerns because of protocol deviations |
| Subgroup 4.1.2 Male | ||||||||||||
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | Open‐label design (participants and clinicians were aware of the assigned treatment). ITT data presented. | Low risk of bias | No substantial data missing. | Low risk of bias | Both groups were measured at the same time and the measurements were similar between groups. | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results and missing information about the allocation concealment. |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone. | Low risk of bias | 6425 participants were randomised and 6425 were analysed. | Low risk of bias | Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | No missing data. We requested the data from the authors. | Low risk of bias | Individuals who assessed the outcomes were not blinded for the assigned treatment. Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall judged some concerns because of protocol deviations |
Risk of bias for analysis 5.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 5.1.1 < 70 years | ||||||||||||
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | Open‐label design (participants and clinicians were aware of the assigned treatment). ITT data presented. | Low risk of bias | We requested data from the authors. No substantial data missing. | Low risk of bias | Both groups were measured at the same time and the measurements were similar between groups. | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results and missing information about the allocation concealment. |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone. | Low risk of bias | 6425 participants were randomised and 6425 were analysed. | Low risk of bias | Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | No missing data. We requested the data from the authors. | Low risk of bias | Individuals who assessed the outcomes were not blinded for the assigned treatment. Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall judged some concerns because of protocol deviations |
| Subgroup 5.1.2 ≥ 70 years | ||||||||||||
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | Open‐label design (participants and clinicians were aware of the assigned treatment). ITT data presented. | Low risk of bias | We requested data from the authors. No substantial data missing. | Low risk of bias | Both groups were measured at the same time and the measurements were similar between groups. | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results and missing information about the allocation concealment. |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone. | Low risk of bias | 6425 participants were randomised and 6425 were analysed. | Low risk of bias | Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | No missing data. We requested the data from the authors. | Low risk of bias | Individuals who assessed the outcomes were not blinded for the assigned treatment. Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall judged some concerns because of protocol deviations |
Risk of bias for analysis 6.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 6.1.1 White | ||||||||||||
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | Open‐label design (participants and clinicians were aware of the assigned treatment). ITT data presented. | Low risk of bias | No substantial data missing. | Low risk of bias | Both groups were measured at the same time and the measurements were similar between groups. | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results and missing information about the allocation concealment. |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone. | Low risk of bias | 6425 participants were randomised and 6425 were analysed. | Low risk of bias | Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Subgroup 6.1.2 Black, Asian or minority ethnic group | ||||||||||||
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone. | Low risk of bias | 6425 participants were randomised and 6425 were analysed. | Low risk of bias | Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Subgroup 6.1.3 Unknown | ||||||||||||
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone. | Low risk of bias | 6425 participants were randomised and 6425 were analysed. | Low risk of bias | Both groups were measured at the same time. The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
Risk of bias for analysis 7.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 7.1.1 High‐income countries | ||||||||||||
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | 15% of the participants in the no hydrocortisone group received hydrocortisone | Low risk of bias | Data were available for this outcome. 238 participants were randomised and 238 were analysed. | Low risk of bias | Mortality is an observer‐reported outcome not involving judgement. | Low risk of bias | Protocol and SAP are available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention |
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | 15% of the participants in the no hydrocortisone group received hydrocortisone | Low risk of bias | Data were available for this outcome. 238 participants were randomised and 238 were analysed. | Low risk of bias | Mortality is an observer‐reported outcome not involving judgement. | Low risk of bias | Protocol and SAP are available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention |
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | No protocol deviations. ITT data presented. | Low risk of bias | We requested the data from the authors, as the data was not broken down by our subgroups of interest in the publication | Low risk of bias | The measurements were similar between groups | Some concerns | Outcome was registered in Eudra‐CT as in‐hospital mortality but reported as 28‐day‐mortality in the supplemental material. | Some concerns | Overall judged some concerns due to selection of reported results. |
| Dequin 2020 | Low risk of bias | Randomisation was centralised and performed electronically. Allocation sequences were generated in a 1:1 ratio by a computer‐generated random number using a blocking schema. There were no baseline differences between the groups. | Low risk of bias | Protocol: Patients, investigators and care providers will be blinded for the patient‐arm. ITT was used. | Low risk of bias | Data were available for this outcome. | Low risk of bias | The measurements were similar between groups. | Some concerns | The protocol and statistical analysis plan were available. 21‐day mortality was a post hoc outcome. | Some concerns | Overall judged some concerns due to selection of reported results. |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | 6425 randomised, 6425 analysed | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group. |
| Munch 2021a | Low risk of bias | No issues with randomisation process. | Low risk of bias | Withdrawals with consecutive open‐label steroids may have affected the outcome, but withdrawals and non‐compliance was rather balanced after all. | Low risk of bias | No missing data. | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with the reported result. | Low risk of bias | Withdrawals because of the experimental context lead to some concerns (but it is less than 10% of all patients). |
| Subgroup 7.1.2 Low‐ and middle‐income countries | ||||||||||||
| Jamaati 2021 | Some concerns | The selected patients were allocated to either the dexamethasone group or the control group by block randomisation. Ten blocks were generated by the Online Randomiser website. Pulmonary disease was highly significantly more prevalent in the control group. Additionally, baseline level of respiratory support was not reported so that we can only assume the most likely circumstance, i.e. that no support beyond oxygen insufflation had been given until randomisation. |
Low risk of bias | No deviations mentioned. ITT data reported. | Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups. | Some concerns | Trial registered after recruitment stop. No analysis plan published beyond registry entry. | Some concerns | Potential bias through probably problematic block randomisation with significant baseline imbalance for pulmonary disease, very delayed registration, and potentially not pre‐specified stop for futility raise some concerns. The issues were not discussed. Potential mild bias towards experimental. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment Control group: 5 excluded before starting treatment, 3 excluded after starting treatment |
Low risk of bias | 416 participants randomised and 416 participants analysed. | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | Some concerns | Overall judged some concerns due to protocol deviations. |
| Tang 2021 | Low risk of bias | Randomisation was stratified by the statistician of the leading site, who produced computer‐generated block randomisation lists with a block size of 4 patients. | Low risk of bias | Single‐blind design (participants), ITT data presented. No deviations reported. | Low risk of bias | No missing data. | Low risk of bias | The data collection and end point judgement were blinded, and the statisticians were also blinded during the statistical analysis. The measurements were similar between groups | Low risk of bias | 30‐day mortality as pre‐specified in the trial registration was not explicitly reported, but could reliably derive from a synopsis of full text, figures, and supplemental material. | Low risk of bias | All domains were rated low risk of bias. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall judged some concerns because of protocol deviations. |
Risk of bias for analysis 1.3 Clinical improvement: discharged alive.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Edalatifard 2020 | Some concerns | No information about the allocation concealment. | Some concerns | In this study, patients did not know which group of them used medicine Physicians and clinicians team know about the medicine and intervention groups. 6 patients in the control group received the intervention drug and were excluded from the analyses Intention‐to‐treat |
Low risk of bias | Data for this outcome was available for all participants randomised | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement.No protocol or SAP available. | Some concerns | Neither the protocol nor the SAP were available | Some concerns | Overall judged some concerns due to missing information about the allocation concealment, deviations from the intended interventions, measurement of the outcome and selection of the reported result |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | Data for this outcome was available for all participants randomised | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement. | Low risk of bias | No issue with selective reporting | Some concerns | Overall judged some concerns due to the randomisation process, protocol deviations and limited bias in measurement. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | Data for this outcome was available for all participants randomised | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall rated some concerns due to protocol deviations and measurement of the outcome. |
Risk of bias for analysis 1.4 Clinical worsening: new need for IMV or death.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | Participants and clinicians were aware of the assigned treatment. Furthermore, 15% of the participants in the no hydrocortisone group received hydrocortisone, and although we deem it rather unlikely that a larger part of these deviations arose from the experimental context, we see some concerns. | Low risk of bias | Since the data were available for all participants, we arrive at the following assessment of domain 3: Low | Some concerns | Assessment of new need for IMV is partly subjective, but we deem it unlikely that large efforts were made or feasible to treat one arm different from another. | Low risk of bias | Because the data were analysed in accordance with a pre‐specified analysis plan we judged this domain low. | Some concerns | Overall judged some concerns because of some degree of deviations and some concerns arising from assessment of the outcome. |
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | Participants and clinicians were aware of the assigned treatment. Furthermore, 15% of the participants in the no hydrocortisone group received hydrocortisone, and although we deem it rather unlikely that a larger part of these deviations arose from the experimental context, we see some concerns. | Low risk of bias | Since the data were available for all participants, we arrive at the following assessment of domain 3: Low | Some concerns | Assessment of new need for IMV is partly subjective, but we deem it unlikely that large efforts were made or feasible to treat one arm different from another. | Low risk of bias | Because the data were analysed in accordance with a pre‐specified analysis plan we judged this domain low. | Some concerns | Overall judged some concerns because of some degree of deviations and some concerns arising from assessment of the outcome. |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | Because data is available for all participants we judged this domain low. | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement. | Low risk of bias | The analysis for this result was prespecified in the protocol | Some concerns | Overall judged some concerns due to deviations from the intended intervention in the control group and limited bias in measurement. |
Risk of bias for analysis 1.5 Serious adverse events.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | Participants and clinicians were aware of the assigned treatment. Further 15% of the participants in the no hydrocortisone group received hydrocortisone, and although we deem it rather unlikely that a larger part of these deviations arose from the experimental context, we see some concerns. | High risk of bias | Since data were not adjusted for competing risk of death in the presence of a relevant death rate, risk of bias is high. | Low risk of bias | The measurement method was appropriate. | Low risk of bias | Protocol and SAP available. | High risk of bias | Because of the issue of competing risk of death all data for this outcome might not be available. There was no adjustment in the analysis for competing risk of death. |
| Angus 2020 | Low risk of bias | Participants were randomised to each locally available group using balanced assignment. Participants were randomly assigned via a computer software program to each locally available group using proportional assignment (e.g., 1:1 if 2 groups available and 1:1:1 if 3 groups available) Protocol: The RAR will occur centrally as part of the computerised randomisation process. Sites will receive the allocation status and will not be informed of the randomisation proportions. Each region will maintain its own computer‐based randomisation program that is accessed by sites in that region but the RAR proportions will be determined by a SAC and provided monthly to the administrator of each region's randomisation program who will update the RAR proportions Baseline characteristics were similar across groups. |
Some concerns | Participants and clinicians were aware of the assigned treatment. Further 15% of the participants in the no hydrocortisone group received hydrocortisone, and although we deem it rather unlikely that a larger part of these deviations arose from the experimental context, we see some concerns. | High risk of bias | Since data were not adjusted for competing risk of death in the presence of a relevant death rate, risk of bias is high. | Low risk of bias | The measurement method was appropriate. | Low risk of bias | Protocol and SAP available. | High risk of bias | Because of the issue of competing risk of death all data for this outcome might not be available. There was no adjustment in the analysis for competing risk of death. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | High risk of bias | Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | High risk of bias | Occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias, so overall we judged high risk of bias. |
Risk of bias for analysis 1.6 Adverse events.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Edalatifard 2020 | Some concerns | No information about the allocation concealment. | Some concerns | 6 patients in the control group received the intervention drug and were excluded from the analyses (17%) | High risk of bias | 6 patients in the control group were not included in the analysis because of deviations from the protocol (17%) Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. |
Low risk of bias | The measurements were similar between groups. | Some concerns | Neither the protocol nor statistical analysis plan were available | High risk of bias | Overall judged high because 6 patients in the control group received the intervention drug and were excluded from the analyses. Moreover, occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias. |
| Tang 2021 | Low risk of bias | Randomisation was stratified by the statistician of the leading site, who produced computer‐generated block randomisation lists with a block size of 4 patients. | Low risk of bias | ITT presented. The participants were blinded, and the physicians were aware of the treatment assignment. No protocol deviations. | High risk of bias | Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Some concerns | Endpoint including its subitems were not named in NCT registration. | High risk of bias | Occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias, so overall we judged high risk of bias. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | High risk of bias | We requested data from the authors. Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | High risk of bias | Occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias, so overall we judged high risk of bias. |
Risk of bias for analysis 1.7 Hospital‐acquired infections.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | No deviations from the protocol. | High risk of bias | We request data from the authors. Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Some concerns | Endpoint and definition is not pre‐specified in Eudra‐CT registration. | High risk of bias | Occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias, so overall we judged high risk of bias. |
| Dequin 2020 | Low risk of bias | Randomisation was centralised and performed electronically. Allocation sequences were generated in a 1:1 ratio by a computer‐generated random number using a blocking schema. There were no baseline differences between the groups. | Low risk of bias | Protocol: Patients, investigators and care providers will be blinded for the patient‐arm | High risk of bias | Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. | High risk of bias | Occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias, so overall we judged high risk of bias. |
| Tang 2021 | Low risk of bias | Randomisation was stratified by the statistician of the leading site, who produced computer‐generated block randomisation lists with a block size of 4 patients. | Low risk of bias | Single‐blind design, ITT data presented. No deviations reported. | High risk of bias | Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Some concerns | Endpoint was not named in NCT registration. | High risk of bias | Occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias, so overall we judged high risk of bias. |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | High risk of bias | We requested data from the authors. Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | High risk of bias | Occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias, so overall we judged high risk of bias. |
Risk of bias for analysis 1.8 Invasive fungal infections.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Corral‐Gudino 2021 | Some concerns | We judged the domain some concerns due to missing information about the allocation concealment. | Low risk of bias | Participants and clinicians were aware of the assigned treatment. The intention‐to‐treat‐analysis was used to estimate the effect of the assignment to intervention. All this leads us to the following judgement for domain 2: Low. | High risk of bias | Because of the issue of competing risk of death all data for this outcome might not be available. There was no adjustment in the analysis for competing risk of death. | Low risk of bias | No issues with measurement. | Some concerns | We judged some concerns as the outcome was not pre‐specified but requested from the authors. | High risk of bias | Overall we judged risk of bias to be high mainly because of missing adjustment for competing risk of death in domain 3. |
Risk of bias for analysis 1.10 New need for dialysis.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | High risk of bias | Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. | High risk of bias | Occurrence of non‐terminal events can be precluded by death as a competing risk. Without adjustment this leads to high risk of bias, so overall we judged high risk of bias. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment; Control group: 5 excluded before starting treatment, 3 excluded after starting treatment | High risk of bias | Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | High risk of bias | Overall judged high due to missing outcome data. |
Risk of bias for analysis 1.11 Viral clearance.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment; Control group: 5 excluded before starting treatment, 3 excluded after starting treatment | High risk of bias | Unknown amount of missing data because of competing risk, and no analysis to adjust for this was made. | Low risk of bias | The measurements were similar between groups. | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | High risk of bias | Overall judged high due to missing outcome data. |
Methylprednisolone versus dexamethasone
We had some concerns about all‐cause‐mortality up to 30 days because of questionable pre‐specification, the only outcome included in this version of the review (Table 105).
Risk of bias for analysis 8.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Ranjbar 2021 | Low risk of bias | Random allocation using the block randomisation method was performed in all four branches of the strata, based on two prognostic factors such as age (< 55 and ≥55) and disease severity based on O2 saturation (<85 and ≥85). The patient, assessor, and analyser in the two groups did not have access to the randomisation list and type of administered drug (Triple blind). No major differences in the baseline characteristics. | Low risk of bias | The patient, assessor, and analyser in the two groups did not have access to the randomisation list and type of administered drug (Triple blind). ITT analysis was used. | Low risk of bias | No missing data. | Low risk of bias | The measurements were similar between groups | Some concerns | Protocol and SAP are not available. | Some concerns | Overall judged some concerns due to selective reporting. |
High‐dose dexamethasone versus low‐dose dexamethasone
We had some concerns about all‐cause‐mortality up to 30 days because of issues with randomisation and deviations from intended interventions (Table 106). We judged all‐cause mortality up to 120 days to be at high risk of bias mainly because of deviations from intended interventions (Table 107). We also applied the respective risk of bias assessments to the four subgroup analyses, although it has to be noted that thereby the age‐stratified analysis could be assessed to be at low risk of bias (Table 113; Table 114; Table 115; Table 116; Table 117; Table 118). We had some concerns about clinical improvement (discharged alive) because of issues with randomisation (Table 108). We judged all safety outcomes (serious adverse events, adverse events, hospital‐acquired infections, and invasive fungal infections) to be at high risk of bias due to missing adjustment for competing risk of death (Table 109; Table 110; Table 111; Table 112).
Risk of bias for analysis 9.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | Few, balanced, and blinded exclcusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
| Taboada 2021 | Some concerns | There are no further information regarding the concealment of the allocation sequence | Low risk of bias | Both participants and those delivering the intervention were aware of intervention received, but there was no information on deviations from intended intervention. The analysis was appropriate. | Low risk of bias | Data for this outcome was available for all 200 participants randomised. | Low risk of bias | The measurement of the outcome was appropriate, and it is unlikely that it differed between intervention groups. The outcome assessors were aware of the intervention received, but it is unlikely that knowledge of intervention received could have affected outcome measurement | Low risk of bias | Outcome is pre‐specified. | Some concerns | However, there are some concerns for bias in the randomisation process. |
Risk of bias for analysis 9.2 All‐cause mortality up to 120 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | Few, balanced, and blinded exclcusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
| Taboada 2021 | Some concerns | There are no further information regarding the concealment of the allocation sequence | Low risk of bias | Both participants and those delivering the intervention were aware of intervention received, but there was no information on deviations from intended intervention. The analysis was appropriate. | Low risk of bias | Data for this outcome was available for all 200 participants randomised. | Low risk of bias | The measurement of the outcome was appropriate and it is unlikely that it differed between intervention groups. The outcome assessors were aware of the intervention received, but it is unlikely that knowledge of intervention received could have affected outcome measurement | Low risk of bias | Protocol available. Outcome pre‐specified. | Some concerns | For this outcome, there is low risk of bias due to deviations from intended interventions, due to missing outcome data and in measurement of the outcome. However, there are some concerns for bias in the randomisation process. |
| Toroghi 2021 | Low risk of bias | Participants were block randomised, and the allocation sequence was concealed. There are no baseline differences that would suggest a problem with randomisation. | High risk of bias | The study design was blind on patient level, but there were no arrangements that ensured blinding. Therefore, we do not know whether the higher dropout rate in the intermediate/high‐dose groups occurred due to the assigned intervention. No information on treatment adherence was reported. | Low risk of bias | Data was available for nearly all participants. | Low risk of bias | The measurement of the outcome was appropriate, and it is unlikely that it differed between intervention groups. The outcome assessors were unaware of the intervention received. | Some concerns | There was a trial register entry, which provided details of the pre‐specified outcomes, but "mortality" was not pre‐specified at trial registration and in the protocol | High risk of bias | The study design was blind on patient level, but there were no arrangements that ensured blinding. Therefore, we do not know whether the higher dropout rate in the intermediate/high‐dose groups occurred due to the assigned intervention. No information on treatment adherence was reported. |
Risk of bias for analysis 10.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 10.1.1 Female | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | We requested the data from the authors. No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | We requested data from the authors. Few, balanced, and blinded exclusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
| Subgroup 10.1.2 Male | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | We requested the data from the authors. No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | We requested data from the authors. Few, balanced, and blinded exclusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
Risk of bias for analysis 10.2 All‐cause mortality up to 120 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 10.2.1 Female | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | We requested data from the authors. Few, balanced, and blinded exclcusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
| Subgroup 10.2.2 Male | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | We requested data from the authors. Few, balanced, and blinded exclcusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
Risk of bias for analysis 11.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 11.1.1 <70 years | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | We requested data from the authors. Few, balanced, and blinded exclusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
| Subgroup 11.1.2 ≥ 70 years | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | We requested data from the authors. Few, balanced, and blinded exclusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
Risk of bias for analysis 11.2 All‐cause mortality up to 120 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 11.2.1 <70 years | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | We requested data from the authors. No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | We requested data from the authors. Few, balanced, and blinded exclusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
| Subgroup 11.2.2 ≥ 70 years | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | We requested data from the authors. No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | We requested data from the authors. Few, balanced, and blinded exclusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
Risk of bias for analysis 12.1 All‐cause mortality up to 30 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 12.1.1 High‐income countries | ||||||||||||
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | Few, balanced, and blinded exclusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
| Taboada 2021 | Some concerns | There are no further information regarding the concealment of the allocation sequence | Low risk of bias | Both participants and those delivering the intervention were aware of intervention received, but there was no information on deviations from intended intervention. The analysis was appropriate. | Low risk of bias | Data for this outcome was available for all 200 participants randomised. | Low risk of bias | The measurement of the outcome was appropriate, and it is unlikely that it differed between intervention groups. The outcome assessors were aware of the intervention received, but it is unlikely that knowledge of intervention received could have affected outcome measurement | Low risk of bias | Outcome is pre‐specified. | Some concerns | However, there are some concerns for bias in the randomisation process. |
| Subgroup 12.1.2 Low‐ and middle‐income countries | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
Risk of bias for analysis 12.2 All‐cause mortality up to 120 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 12.2.1 High‐income countries | ||||||||||||
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | Low risk of bias | Few, balanced, and blinded exclusions for similar reasons in both arms. | Low risk of bias | No issues with measurement | Low risk of bias | No issues with potential selection. | Low risk of bias | Low risk of bias in all domains. |
| Taboada 2021 | Some concerns | There are no further information regarding the concealment of the allocation sequence | Low risk of bias | Both participants and those delivering the intervention were aware of intervention received, but there was no information on deviations from intended intervention. The analysis was appropriate. | Low risk of bias | Data for this outcome was available for all 200 participants randomised. | Low risk of bias | The measurement of the outcome was appropriate, and it is unlikely that it differed between intervention groups. The outcome assessors were aware of the intervention received, but it is unlikely that knowledge of intervention received could have affected outcome measurement | Low risk of bias | Protocol available. Outcome pre‐specified. | Some concerns | For this outcome, there is low risk of bias due to deviations from intended interventions, due to missing outcome data and in measurement of the outcome. However, there are some concerns for bias in the randomisation process. |
| Subgroup 12.2.2 Low‐ and middle‐income countries | ||||||||||||
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with deviations (2/51 patients from the control received not intended intervention) and appropriate analysis. | Low risk of bias | No relevant amount of missing data. | Low risk of bias | No relevant issues with measurement. | Low risk of bias | No relevant issues with reporting. | Some concerns | Some minor concerns regarding deviations in about 5% of patients and their exclusion from analysis. |
| Toroghi 2021 | Low risk of bias | Participants were block randomised, and the allocation sequence was concealed. There are no baseline differences that would suggest a problem with randomisation. | High risk of bias | The study design was blind on patient level, but there were no arrangements that ensured blinding. Therefore, we do not know whether the higher dropout rate in the intermediate/high‐dose groups occurred due to the assigned intervention. No information on treatment adherence was reported. | Low risk of bias | Data was available for nearly all participants. | Low risk of bias | The measurement of the outcome was appropriate, and it is unlikely that it differed between intervention groups. The outcome assessors were unaware of the intervention received. | Some concerns | There was a trial register entry, which provided details of the pre‐specified outcomes, but "mortality" was not pre‐specified at trial registration and in the protocol | High risk of bias | The study design was blind on patient level, but there were no arrangements that ensured blinding. Therefore, we do not know whether the higher dropout rate in the intermediate/high‐dose groups occurred due to the assigned intervention. No information on treatment adherence was reported. |
Risk of bias for analysis 9.3 Clinical improvement: discharged alive.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Taboada 2021 | Some concerns | There are no further information regarding the concealment of the allocation sequence | Low risk of bias | Both participants and those delivering the intervention were aware of intervention received, but there was no information on deviations from intended intervention. The analysis was appropriate. | Low risk of bias | Data for this outcome was available for all 200 participants randomised. | Low risk of bias | The measurement of the outcome was appropriate and it is unlikely that it differed between intervention groups. The outcome assessors were aware of the intervention received, but it is unlikely that knowledge of intervention received could have affected outcome measurement | Low risk of bias | Protocol available. Outcome pre‐specified. | Some concerns | For this outcome, there is low risk of bias due to deviations from intended interventions, due to missing outcome data and in measurement of the outcome. However, there are some concerns for bias in selection of the reported result and the randomisation process. |
Risk of bias for analysis 9.4 Serious adverse events.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with appropriate analysis but no relevant number of deviations or exclusions from analysis. | High risk of bias | Missing adjustment for competing risk of death in a trial with relevant death rate. | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with reporting | High risk of bias | High risk of bias due to missing adjustment for competing risk of death in domain 3. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | High risk of bias | Few, balanced, and blinded exclusions for similar reasons in both arms. Missing adjustment for competing risk of death. | Low risk of bias | No issues with measurement | Low risk of bias | No extraordinary issues with potential selection. | High risk of bias | High risk of bias due to missing adjustment for competing risk of death. |
Risk of bias for analysis 9.5 Adverse events.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with appropriate analysis but no relevant number of deviations or exclusions from analysis. | High risk of bias | Missing adjustment for competing risk of death in a trial with relevant death rate. | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with reporting. | High risk of bias | High risk of bias due to missing adjustment for competing risk of death in domain 3. |
Risk of bias for analysis 9.6 Hospital‐acquired infections.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with appropriate analysis but no relevant number of deviations or exclusions from analysis. | High risk of bias | Missing adjustment for competing risk of death in a trial with relevant death rate. | Some concerns | Some concerns because also subjective clinical assessment was allowed but not deemed of major concern. | Low risk of bias | No relevant issues with reporting | High risk of bias | High risk of bias due to missing adjustment for competing risk of death in domain 3. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions | High risk of bias | We requested data from the authors. No adjustment for competing risk of death done or supported. | Low risk of bias | No issues with measurement | Low risk of bias | No extraordinary issues with potential selection. | High risk of bias | High risk of bias due to missing adjustment for competing risk of death. |
Risk of bias for analysis 9.7 Invasive fungal infections.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Maskin 2021 | Low risk of bias | No issues with randomisation. | Some concerns | Minor issues with appropriate analysis but no relevant number of deviations or exclusions from analysis. | High risk of bias | Missing adjustment for competing risk of death in a trial with relevant death rate. | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with reporting | High risk of bias | High risk of bias due to missing adjustment for competing risk of death in domain 3. |
| Munch 2021b | Low risk of bias | No issues with randomisation process. | Low risk of bias | No issues with deviations from intended interventions. | High risk of bias | Adjustment for competing risk of death missing or not possible on time‐to‐event scale. | Low risk of bias | No issues with measurement. | Low risk of bias | No issues with potential selection, extraction initiated by review authors. | High risk of bias | High risk of bias due to missing data or adjustment regarding competing risk of death in circumstances of relevant mortality. |
Effects of interventions
See: Table 1; Table 2; Table 3
Hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19
From 16 RCTs in this population (Angus 2020; Corral‐Gudino 2021; Dequin 2020; Edalatifard 2020; Farahani 2021; Horby 2021; Jamaati 2021; Jeronimo 2020; Maskin 2021; Munch 2021a; Munch 2021b; Ranjbar 2021; Taboada 2021; Tang 2021; Tomazini 2020; Toroghi 2021), the study of Farahani 2021 did not report any of the prioritised outcomes of interest.
We received data for serious adverse events, adverse events, hospital‐acquired infections, invasive fungal infections, age‐stratified, sex‐stratified and ethnicity‐stratified mortality from four studies upon request (Corral‐Gudino 2021; Maskin 2021; Munch 2021b; Tomazini 2020).
Systemic corticosteroids plus standard care versus standard care (plus/minus placebo)
The evidence profile is presented in Table 1.
All‐cause mortality up to 30 days
Data on all‐cause mortality up to 30 days were available from nine studies with a total of 7898 participants (Angus 2020; Corral‐Gudino 2021; Dequin 2020; Horby 2021; Jamaati 2021; Jeronimo 2020; Munch 2021a; Tang 2021; Tomazini 2020). The observation periods ranged from 21 to 28 days. Overall, 764 of 2937 participants in the intervention groups died compared with 1357 of 4961 participants in the control groups. The risk ratio (RR) of this dichotomous outcome of death was 0.90 (95% confidence interval (CI) 0.84 to 0.97; I² = 0%; random‐effects model; Analysis 1.1). We downgraded the certainty of the evidence for this outcome from high to moderate due to serious risk of bias.
1.1. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
Subgroup analyses: clinical relevance
Respiratory support at randomisation: the test for subgroup differences indicated no difference (P = 0.11) (Analysis 2.1). In contrast with the beneficial effect on mortality in all those subgroups needing respiratory support, a higher risk of death with systemic corticosteroids was seen among symptomatic COVID‐19 participants who did not need any respiratory support (RR 1.27, 95% CI 1.00 to 1.61). A single large study contributed data for participants without the need for respiratory support (Horby 2021).
Dexamethasone versus methylprednisolone versus hydrocortisone indirectly compared for their effects relative to placebo/standard care: the test for subgroup differences indicated no difference (P = 0.71) (Analysis 3.1). However, the effect estimates for each subgroup were in favour of corticosteroid use.
2.1. Analysis.

Comparison 2: Subgroup analysis: respiratory support for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
3.1. Analysis.

Comparison 3: Subgroup analysis: dexamethasone versus methylprednisolone versus hydrocortisone for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
Subgroup analyses: equity‐related aspects
Sex ‐ female versus male: the test for subgroup differences indicated no difference (P = 0.44) (Analysis 4.1). However, the effect estimates for each subgroup were in favour of corticosteroid use.
Age ‐ < 70 years versus ≥ 70 years: the test for subgroup differences indicated differences (P = < 0.0001) (Analysis 5.1). Participants younger than 70 years seem to benefit from corticosteroids in contrast to participants who were aged 70 years and older. Furthermore, the degree of heterogeneity in each of the subgroups is much lower (< 10 %) than in the set of the combined subgroups (77%). This might be a sign for identifying one of the causes of overall heterogeneity.
Ethnicity ‐ White versus Black, Asian or minority ethnic group versus unknown: the test for subgroup differences indicated differences (P = 0.01) (Analysis 6.1). The few participants from a Black, Asian, or minority ethnic group had a larger estimated effect than the many White participants.
Place of residence ‐ high‐income versus low‐ and middle‐income countries: the test for subgroup differences indicated no difference (P = 0.42) (Analysis 7.1). However, the effect estimates for both subgroups were in favour of corticosteroid use.
4.1. Analysis.

Comparison 4: Subgroup analysis: female versus male for the comparison of systemic corticosteroids versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
5.1. Analysis.

Comparison 5: Subgroup analysis: < 70 years versus ≥ 70 years for the comparison of systemic corticosteroids versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
6.1. Analysis.

Comparison 6: Subgroup analysis: White versus Black, Asian or minority ethnic group versus unknown for the comparison of systemic corticosteroids versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
7.1. Analysis.

Comparison 7: Subgroup analysis: high‐income countries versus low‐ and middle‐income countries for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
Sensitivity analyses
We summarised the effects of sensitivity analyses in Table 11. Reported effects in our main analysis were robust when removing platform trials and using the fixed‐effect model. As we found only a low risk of bias or some concerns in our included RCTs for this outcome, there was no opportunity to exclude studies at high risk of bias for sensitivity analysis. Furthermore, none of the included studies for this comparison were preprints.
8. Sensitivity analyses for the comparison: systemic corticosteroids plus standard care versus standard care (plus/minus placebo).
| Outcome | Main analyses | Risk of bias (excluding studies at high risk of bias) | Fixed‐effect model or random‐effects model | Preprint (excluding preprints) | Platform trial (excluding platform trialsa) |
| All‐cause mortality up to 30 days | RR 0.90, 95% CI 0.84 to 0.97; 9 studies, 7898 participants | There were no RCTs with high risk of bias concerning this outcome | RR 0.90, 95% CI 0.83 to 0.97; 9 studies, 7898 participants | There were no RCTs as a preprint concerning this outcome | RR 0.94, 95% CI 0.82 to 1.08; 7 studies, 1094 participants |
| All‐cause mortality up to 120 days | RR 0.74, 95% CI 0.23 to 2.34; 3 studies, 485 participants | There were no RCTs with high risk of bias concerning this outcome | RR 0.92, 95% CI 0.73 to 1.15; 3 studies, 485 participants | There were no RCTs as a preprint concerning this outcome | There were no platform trials concerning this outcome |
| Clinical improvement: discharged alive | RR 1.07, 95% CI 1.03 to 1.11; 3 studies, 6786 participantsb | There were no RCTs with high risk of bias concerning this outcome | RR 1.36, 95% CI 0.95 to 1.96; 3 studies, 6786 participantsc | There were no RCTs as a preprint concerning this outcome | RR 1.65, 95% CI 1.23 to 2.21; 2 studies, 361 participants |
aExcluding platform trials: Angus 2020; Horby 2021.
bUsing the fixed‐effect model.
c Using the random‐effects model.
CI: confidence interval; RR: risk ratio
All‐cause mortality up to 120 days
Data on all‐cause mortality up to 120 days were available from three studies with a total of 485 participants (Edalatifard 2020; Jeronimo 2020 (matched with long‐term data from Barros 2021); Munch 2021a). Overall, 89 of 244 participants in the intervention groups died compared with 97 of 241 participants in the control groups. The RR of death was 0.74 (95% CI 0.23 to 2.34; I² = 79%; random‐effects model; Analysis 1.2). We downgraded the certainty of the evidence for this outcome from high to very low due to serious risk of bias, serious inconsistency, and serious imprecision.
1.2. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 2: All‐cause mortality up to 120 days
Subgroup analyses: clinical relevance
Respiratory support at randomisation: We refrained from performing this analysis because only a single study would have contributed 62 participants.
Methylprednisolone versus hydrocortisone indirectly compared for their effect relative to placebo/standard care: the test for subgroup differences indicated no difference (P = 0.17) (Analysis 3.2) and description of different directions of effects appears misleading, taking into account the small sample size.
3.2. Analysis.

Comparison 3: Subgroup analysis: dexamethasone versus methylprednisolone versus hydrocortisone for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 2: All‐cause mortality up to 120 days
Subgroup analyses: equity‐related aspects
High‐income versus low‐ and middle‐income countries: the test for subgroup differences indicated no difference (P = 0.14) (Analysis 7.2) and the description of different directions of effects appears misleading, taking into account the small sample size.
7.2. Analysis.

Comparison 7: Subgroup analysis: high‐income countries versus low‐ and middle‐income countries for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 2: All‐cause mortality up to 120 days
We could not perform the subgroup analyses for sex, age, and ethnicity due to missing data.
Sensitivity analyses
We summarised the effects of the two sensitivity analyses in Table 11. When using the random‐effects and fixed‐effect model, we found different effects with broad confidence intervals pointing in the same direction (random‐effects model: RR 0.74, 95% CI 0.23 to 2.34; fixed‐effect model: RR 0.92, 95% CI 0.73 to 1.15). There were no study results with high risk of bias and none of the included RCTs were published as preprints for this comparison. Hence, we did not perform the further two planned analyses.
Clinical improvement: discharged alive (at 28 days)
Data on clinical improvement were available from three studies with a total of 6786 participants (Edalatifard 2020; Horby 2021; Tomazini 2020). Overall, 1490 of 2289 participants in the intervention groups were discharged alive compared with 2789 of 4497 participants in the control groups. The RR of being discharged alive was 1.07 (95% CI 1.03 to 1.11; I² = 81%; fixed‐effect model; Analysis 1.3). We downgraded the certainty of the evidence for this outcome from high to low due to serious risk of bias, serious inconsistency, and serious imprecision. Although this is not a critical outcome, because of the high statistical heterogeneity we performed subgroup and sensitivity analyses as pre‐specified:
Subgroup analyses: clinical relevance
Methylprednisolone versus hydrocortisone indirectly compared for their effect relative to placebo/standard care: the test for subgroup differences indicated a difference (P = 0.01) (Analysis 3.3), but large heterogeneity (I2 = 85%). In both groups, the risk ratio favoured treatment with glucocorticoids, while the effect estimate in the trial evaluating methylprednisolone was stronger, but the number of the included participants very low.
3.3. Analysis.

Comparison 3: Subgroup analysis: dexamethasone versus methylprednisolone versus hydrocortisone for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 3: Clinical improvement: discharged alive
Subgroup analyses: equity‐related aspects
High‐income versus low‐ and middle‐income countries: the test for subgroup differences indicated a difference (P = 0.003) (Analysis 7.3), but large heterogeneity (I2 = 88%). In both groups, the risk ratio favoured treatment with glucocorticoids, while the effect estimate in the trial evaluating low‐ and middle‐income countries was stronger, but the number of the included participants very low.
7.3. Analysis.

Comparison 7: Subgroup analysis: high‐income countries versus low‐ and middle‐income countries for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 3: Clinical improvement: discharged alive
We could not perform the subgroup analyses for sex, age, and ethnicity because of missing data.
Sensitivity analyses
We summarised the effects of the sensitivity analyses in Table 11. When using the random‐effects and fixed‐effect model, we found different effects with broad confidence intervals pointing in the same direction (random‐effects model: RR 1.36, 95% CI 0.95 to 1.96; fixed‐effect model: RR 1.07, 95% CI 1.03 to 1.11). When removing the platform trial we found a different effect with a broader confidence interval pointing in the same direction as the main analysis (main analysis: RR 1.07, 95% CI 1.03 to 1.11; excluding Horby 2021: RR 1.65, 95% CI 1.23 to 2.21). As we found only a risk of bias of 'some concerns' in our included RCTs for this outcome, there was no opportunity to exclude studies at high risk of bias for sensitivity analysis. Furthermore, all included RCTs were published in full in peer‐reviewed journals for this comparison.
Clinical worsening: new need for invasive mechanical ventilation or death
Data on clinical worsening were available from two studies with a total of 5586 participants (Angus 2020; Horby 2021). Overall, 527 of 1900 participants in the intervention groups needed invasive mechanical ventilation or died compared with 1040 of 3686 participants in the control groups. The RR of needing invasive mechanical ventilation or death was 0.92 (95% CI 0.84 to 1.01; I² = 72%; fixed‐effect model; Analysis 1.4). We downgraded the certainty of the evidence for this outcome from high to low due to serious risk of bias and serious inconsistency.
Serious adverse events
Two studies reported serious adverse events for 678 participants (Angus 2020; Tomazini 2020). In Angus 2020 (shock‐dependent hydrocortisone group) 5 of 141 participants in the intervention group and 0 of 52 participants in the control group developed a serious adverse event (RR 4.11, 95% CI 0.23 to 72.98). In Angus 2020 (fixed‐dose hydrocortisone group), 4 of 137 participants in the intervention group and 1 of 49 participants in the control group developed a serious adverse event (RR 1.43, 95% CI 0.16 to 12.49). In Tomazini 2020, 5 of 151 participants in the intervention group and 9 of 148 participants in the control group developed a serious adverse event (RR 0.54, 95% CI 0.19 to 1.59). Data on serious adverse events can be taken from Analysis 1.5 and additional information from Table 8. We decided not to carry out a meta‐analysis because we are highly uncertain about the size and direction of the effects not adjusted for competing risk of death. However, a cautious analysis of the descriptive statistics suggested little to no difference between the groups. We downgraded the certainty of the evidence for this outcome from high to very low due to very serious risk of bias and serious imprecision.
1.5. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 5: Serious adverse events
Adverse events (any grade)
Three studies reported adverse events amongst 447 participants (Edalatifard 2020; Tang 2021; Tomazini 2020). In Edalatifard 2020, 2 of 34 participants in the intervention group and 2 of 28 participants in the control group developed an adverse event (RR 0.82, 95% CI 0.12 to 5.48). In Tang 2021, 5 of 43 participants in the intervention group and 8 of 43 participants in the control group developed an adverse event (RR 0.63, 95% CI 0.22 to 1.76). In Tomazini 2020, 122 of 151 participants in the intervention group and 121 of 148 participants in the control group developed an adverse event (RR 0.99, 95% CI 0.89 to 1.10). Data on adverse events are presented in Analysis 1.6 and Table 8. We decided not to carry out meta‐analysis because we are highly uncertain about size and the direction of the effects not adjusted for competing risk of death. However, a cautious analysis of the descriptive statistics suggested little to no difference between the groups. We downgraded the certainty of the evidence for this outcome from high to very low due to very serious risk of bias and serious imprecision.
1.6. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 6: Adverse events
Hospital‐acquired infections
Four studies involving 598 participants reported hospital‐acquired infections (Corral‐Gudino 2021; Dequin 2020; Tang 2021; Tomazini 2020). In Corral‐Gudino 2021, 5 of 35 participants in the intervention group and 1 of 29 participants in the control group developed a hospital‐acquired infection (RR 4.14, 95% CI 0.51 to 33.49). In Dequin 2020, 28 of 76 participants in the intervention group and 30 of 73 participants in the control group developed a hospital‐acquired infection (RR 0.90, 95% CI 0.60 to 1.34). In Tang 2021, 2 of 43 participants in the intervention group and 1 of 43 participants in the control group developed a hospital‐acquired infection (RR 2.00, 95% CI 0.19 to 21.24). In Tomazini 2020, 30 of 151 participants in the intervention group and 39 of 148 participants in the control group developed a hospital‐acquired infection (RR 0.75, 95% CI 0.50 to 1.15). Data on hospital‐acquired infections can be taken from Analysis 1.7 and additional information from Table 8. We decided not to carry out meta‐analysis because we are highly uncertain about size and the direction of the effects not adjusted for competing risk of death. However, a cautious analysis of the descriptive statistics suggested little to no difference between the groups. We downgraded the certainty of the evidence for this outcome from high to very low due to very serious risk of bias and serious imprecision.
1.7. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 7: Hospital‐acquired infections
Invasive fungal infections
One study reported this outcome for 64 participants (Corral‐Gudino 2021), where 1 of 35 participants in the intervention group and 0 of 29 participants in the control group developed an invasive fungal infection (RR 2.50, 95% CI 0.11 to 59.15). Data on invasive fungal infections can be taken from Analysis 1.8 and additional information from Table 8. We are highly uncertain about size and the direction of the effects not adjusted for competing risk of death. We downgraded the certainty of the evidence for this outcome from high to very low due to very serious risk of bias and serious imprecision.
1.8. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 8: Invasive fungal infections
Quality of life (up to 120 days)
One study reported quality of life for 118 participants with the Duke activity status index (DASI) (Jeronimo 2020). The score ranged from 0 to 58.2, with higher scores indicating greater levels of fitness. Participants in the intervention group reached a mean score of 43.3 (SD 14.2) and participants in the control group reached a mean score of 40.6 (SD 13.9). The mean difference was 2.70 (95% CI ‐2.38 to 7.78). Data on quality of life can be taken from Analysis 1.9. However, a cautious analysis of the descriptive statistics suggested little to no difference between the groups. We would downgrade the certainty of the evidence from high to very low due to serious risk of bias and very serious imprecision.
1.9. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 9: Quality of life up to 120 days
New need for dialysis
Two studies reported data on new need for dialysis for 6613 participants (Horby 2021; Jeronimo 2020). In Horby 2021, 89 of 2034 participants in the intervention group and 314 of 4194 participants in the control group needed dialysis (RR 0.58, 95% CI 0.46 to 0.74). In Jeronimo 2020, 29 of 191 participants in the intervention group and 33 of 194 participants in the control group needed dialysis (RR 0.89, 95% CI 0.57 to 1.41). Data on the new need for dialysis can be taken from Analysis 1.10. We decided not to carry out a meta‐analysis because we are highly uncertain about the size and direction of the unadjusted effects. We would downgrade the certainty of the evidence from high to very low due to serious risk of bias and very serious imprecision.
1.10. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 10: New need for dialysis
Viral clearance
One study reported data on viral clearance (Jeronimo 2020). Viral clearance was defined as the presence of viral RNA detected through RT‐PCR in the naso‐/oropharyngeal swab on day seven. In Jeronimo 2020, no viral load was detected in 61 of 117 participants in the intervention group and in 50 of 95 in the control group (RR 0.99, 95% CI 0.77 to 1.28). Data on viral clearance can be taken from Analysis 1.11. We would downgrade the certainty of the evidence from high to very low due to serious risk of bias and very serious imprecision.
1.11. Analysis.

Comparison 1: Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 11: Viral clearance
Different types of systemic corticosteroids: methylprednisolone versus dexamethasone
The evidence profile is presented in Table 2.
All‐cause mortality up to 30 days
Data on all‐cause mortality up to 30 days were available from one trial with 86 participants (Ranjbar 2021), where 8 of 44 participants in the intervention group died compared with 15 of 42 participants in the control group. The RR of death was 0.51 (95% CI 0.24 to 1.07; Analysis 8.1), favouring methylprednisolone. We downgraded the certainty of the evidence for this outcome to very low due to serious risk of bias and very serious imprecision.
8.1. Analysis.

Comparison 8: Methylprednisolone versus dexamethasone for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
Subgroup and sensitivity analyses
We could not perform any of our planned subgroup and sensitivity analyses for the comparison of methylprednisolone versus dexamethasone and the outcome of all‐cause mortality up to 30 days.
Other outcomes
No further outcome of interest was available from Ranjbar 2021 nor could we identify any other study for this comparison.
High‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8 mg)
The evidence profile is presented in Table 3.
All‐cause mortality up to 30 days
Data on all‐cause mortality up to 30 days were available from three studies involving a total of 1269 participants (Maskin 2021; Munch 2021b; Taboada 2021). The observation period in the studies was 28 days. Overall, 159 of 638 participants in the intervention group died compared with 180 of 631 participants in the control group. The RR of death was 0.87 (95% CI 0.73 to 1.04; I² = 0%; random‐effects model; Analysis 9.1). We downgraded the certainty of the evidence for this outcome from high to low due to serious risk of bias and serious imprecision.
9.1. Analysis.

Comparison 9: High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
Subgroup analyses: equity‐related aspects
Female versus male: the test for subgroup differences indicated no difference (P = 0.92) between subgroups stratified by the sex of the participants (Analysis 10.1). However, the effect estimates for each subgroup were in favour of high‐dose dexamethasone.
< 70 years versus ≥ 70 years: the test for subgroup differences indicated no difference (P = 0.55) between subgroups stratified by the age of the participants (Analysis 11.1). However, the effect estimates for each subgroup were in favour of high‐dose dexamethasone.
High‐income versus low‐ and middle‐income countries: the test for subgroup differences indicated no difference (P = 0.41) between subgroups stratified by income of the country (Analysis 12.1).
10.1. Analysis.

Comparison 10: Subgroup analysis: female versus male for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
11.1. Analysis.

Comparison 11: Subgroup analysis: < 70 years versus ≥ 70 years for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
12.1. Analysis.

Comparison 12: Subgroup analysis: high‐income countries versus low‐ and middle‐income countries for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 1: All‐cause mortality up to 30 days
We could not perform the subgroup analyses for respiratory support at randomisation and ethnicity due to insufficient data.
Sensitivity analyses
We summarised the effects of sensitivity analyses in Table 12. Reported effects of our main analysis were robust when using the fixed‐effect model. We found no preprints, platform trials, or trials with high risk of bias concerning this outcome, so we could not exclude them.
9. Sensitivity analyses for the comparison: high‐dose dexamethasone versus low‐dose dexamethasone.
| Outcome | Main analyses | Risk of bias (excluding studies at high risk of bias)b | Fixed‐effect model or random‐effects model | Preprint (excluding preprints) | Platform trials (excluding platform trials) |
| All‐cause mortality up to 30 days | RR 0.87, 95% CI 0.73 to 1.04; 3 studies, 1269 participants | There were no RCTs with high risk of bias concerning this outcome | RR 0.87, 95% CI 0.73 to 1.04; 3 studies, 1269 participants | There were no RCTs as a preprint concerning this outcome | There were no platform trials concerning this outcome |
| All‐cause mortality up to 120 days | RR 1.05, 95% CI 0.74 to 1.48; 4 studies, 1399 participantsa | RR 0.87, 95% CI 0.74 to 1.02; 3 studies, 1266 participants | RR 0.93, 95% CI 0.79 to 1.08; 4 studies, 1399 participantsc | There were no RCTs as a preprint concerning this outcome | There were no platform trials concerning this outcome |
aUsing the fixed‐effect model.
bExcluded studies with high risk of bias: Toroghi 2021.
cUsing the random‐effects model.
CI: confidence interval; RR: risk ratio
All‐cause mortality up to 120 days
Data on all‐cause mortality up to 120 days were available from four studies with a total of 1383 participants (Maskin 2021; Munch 2021b; Taboada 2021; Toroghi 2021). The observation periods ranged from 60 to 90 days. Overall, 218 of 717 participants in the intervention group died compared with 219 of 666 participants in the control group. The RR of death was 0.93 (95% CI 0.79 to 1.08; I² = 54%; fixed‐effect model; Analysis 9.2). We downgraded the certainty of the evidence for this outcome from high to very low due to serious risk of bias, serious inconsistency, and serious imprecision.
Subgroup analyses: equity‐related aspects
Female versus male: the test for subgroup differences indicated no difference (P = 0.59) between subgroups stratified by the sex of the participants (Analysis 10.2). However, the effect estimates for each subgroup were in favour of high‐dose dexamethasone.
< 70 years versus ≥ 70 years: the test for subgroup differences indicated no difference (P = 0.30) between subgroups stratified by the age of the participants (Analysis 11.2). However, the effect estimates for each subgroup were in favour of high‐dose dexamethasone.
High‐income versus low‐ and middle‐income countries: the test for subgroup differences indicated differences (P = 0.03) between subgroups stratified by income of the country (Analysis 12.2) favouring high‐dose dexamethasone in high‐income countries, while the effect estimate in low‐income countries favoured low‐dose dexamethasone. However, the estimated effect for low‐ and middle‐income countries was fully carried by Toroghi 2021, the only study result at high risk of bias in this analysis.
10.2. Analysis.

Comparison 10: Subgroup analysis: female versus male for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 2: All‐cause mortality up to 120 days
11.2. Analysis.

Comparison 11: Subgroup analysis: < 70 years versus ≥ 70 years for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 2: All‐cause mortality up to 120 days
12.2. Analysis.

Comparison 12: Subgroup analysis: high‐income countries versus low‐ and middle‐income countries for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 2: All‐cause mortality up to 120 days
We could not perform the subgroup analyses for respiratory support at randomisation and ethnicity due to insufficient data.
Sensitivity analyses
We summarised the effects of sensitivity analyses in Table 12. When using the random‐effects and fixed‐effect models, we found different effects with broad confidence intervals pointing in opposite directions (random‐effects model: RR 0.93, 95% CI 0.79 to 1.08; fixed‐effect model: RR 1.05, 95% CI 0.74 to 1.48). When excluding the study with high risk of bias (Toroghi 2021), we found effects with broad confidence intervals also pointing in different directions (main analysis: RR 1.05, 95% CI 0.74 to 1.48; excluding study at high risk of bias: RR 0.87, 95% CI 0.74 to 1.02). No preprints nor platform trials contributed to this outcome for this comparison, and thus we did not pursue the respective sensitivity analyses.
Clinical improvement: discharged alive
Data on clinical improvement were available from one study with a total of 200 participants (Taboada 2021). Overall, 85 of 98 participants in the intervention group were discharged alive compared with 90 of 102 participants in the control group. The RR of being discharged alive was 0.98 (95% CI 0.89 to 1.09; I² = not applicable; random‐effects model; Analysis 9.3). We downgraded the certainty of the evidence for this outcome from high to low due to serious risk of bias and serious imprecision.
9.3. Analysis.

Comparison 9: High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 3: Clinical improvement: discharged alive
Clinical worsening: new need for invasive mechanical ventilation or death
We did not identify any study reporting this outcome.
Serious adverse events
Two studies reported serious adverse events for 1080 participants (Munch 2021b; Maskin 2021). In Maskin 2021, 42 of 49 participants in the high‐dose group and 40 of 49 participants in the low‐dose group developed a serious adverse event (RR 1.05, 95% CI 0.88 to 1.25). In Munch 2021b, 70 of 497 participants in the high‐dose group and 85 of 485 participants in the low‐dose group developed a serious adverse event (RR 0.80, 95% CI 0.60 to 1.07). Data on serious adverse events can be taken from Analysis 9.4 and additional information from Table 8. We decided not to carry out a meta‐analysis because we are highly uncertain about the size and direction of the effects not adjusted for competing risk of death. However, a cautious analysis of the descriptive statistics suggested little to no difference between the groups. We downgraded the certainty of the evidence for this outcome from high to very low due to serious risk of bias and very serious imprecision.
9.4. Analysis.

Comparison 9: High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 4: Serious adverse events
Adverse events (any grade)
One study reported data for 98 participants for this outcome (Maskin 2021), where all 49 participants in the high‐dose group and 48 of 49 participants in the low‐dose group developed an adverse event (RR 1.02, 95% CI 0.96 to 1.08). Data on adverse events can be taken from Analysis 9.5 and Table 8. Without adjustment for competing risk of death, a cautious analysis of the descriptive statistics nonetheless suggested little to no difference between the groups. We downgraded the certainty of the evidence for this outcome from high to very low due to serious risk of bias and very serious imprecision.
9.5. Analysis.

Comparison 9: High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 5: Adverse events
Hospital‐acquired infections
Two studies reported this outcome for 1080 participants (Maskin 2021; Munch 2021b). In Maskin 2021, 34 of 49 participants in the high‐dose group and 38 of 49 participants in the low‐dose group developed a hospital‐acquired infection (RR 0.89, 95% CI 0.70 to 1.14). In Munch 2021b, 50 of 497 participants in the high‐dose group and 61 of 485 participants in the low‐dose group developed a hospital‐acquired infection (RR 0.80, 95% CI 0.56 to 1.14). Data on hospital‐acquired infections can be taken from Analysis 9.6 and additional information from Table 8. We decided not to carry out a meta‐analysis because we are highly uncertain about the size and direction of the effects not adjusted for competing risk of death. However, a cautious analysis of the descriptive statistics suggested little to no difference between the groups. We downgraded the certainty of the evidence for this outcome from high to very low due to serious risk of bias and very serious imprecision.
9.6. Analysis.

Comparison 9: High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 6: Hospital‐acquired infections
Invasive fungal infections
Two studies reported this outcome for 1080 participants (Maskin 2021; Munch 2021b). In Maskin 2021, 3 of 49 participants in the high‐dose group and 3 of 49 participants in the low‐dose group developed an invasive fungal infection (RR 1.00, 95% CI 0.21 to 4.71). In Munch 2021b, 15 of 497 participants in the high‐dose group and 21 of 485 participants in the low‐dose group developed an invasive fungal infection (RR 0.70, 95% CI 0.36 to 1.34). Data on invasive fungal infections can be taken from Analysis 9.7 and Table 8. We decided not to carry out a meta‐analysis because we are highly uncertain about the size and direction of the effects not adjusted for competing risk of death. However, a cautious analysis of the descriptive statistics suggested little to no difference between the groups. We downgraded the certainty of the evidence for this outcome from high to very low due to serious risk of bias and very serious imprecision.
9.7. Analysis.

Comparison 9: High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19, Outcome 7: Invasive fungal infections
Other outcomes
No further outcome of interest was available from Maskin 2021, Munch 2021b, Taboada 2021, and Toroghi 2021.
Timing comparisons (early versus late)
No studies provided data for this comparison.
Systemic corticosteroids versus other active substances
No studies provided data for this comparison.
Outpatients with asymptomatic or mild disease
We did not identify any study that investigated the effects of systemic corticosteroids in people with asymptomatic infection or mild disease (i.e. non‐hospitalised individuals).
Discussion
Summary of main results
This review aimed to assess the efficacy and safety of systemic corticosteroids for the treatment of COVID‐19, as well as equity‐related aspects quantitatively in subgroup analyses where possible. We found no studies for people with asymptomatic infection or mild COVID‐19 disease.
For hospitalised people with a confirmed or suspected diagnosis of symptomatic COVID‐19, we identified 16 RCTs (9549 participants). Eleven trials (8019 participants) evaluated systemic corticosteroids plus standard care compared to standard care (with or without placebo), one trial compared different types of corticosteroids (86 participants), and four studies compared different doses of dexamethasone (1444 participants). We identified 42 ongoing studies evaluating systemic corticosteroids and 23 completed studies lacking published results or relevant information on the study design, which we categorised as 'studies awaiting classification'. We checked the proportion of PCR‐positive tests in each study, as some studies included confirmed or suspected COVID‐19 infections, or both. The study with the lowest PCR‐positive rate of approximately 80% was Angus 2020.
Effects of interventions
Hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19
Systemic corticosteroids plus standard care versus standard care (plus/minus placebo)
Systemic corticosteroids probably slightly reduce all‐cause mortality up to 30 days (moderate‐certainty evidence).
The evidence is very uncertain about the effect of systemic corticosteroids on all‐cause mortality up to 120 days (very low‐certainty evidence).
Systemic corticosteroids may slightly increase the chance of clinical improvement (discharged alive) and may slightly decrease the risk of clinical worsening (new need for invasive mechanical ventilation or death) (both low‐certainty evidence).
We are uncertain of the effects of systemic corticosteroids on serious adverse events, adverse events, hospital‐acquired infections, and invasive fungal infections (very low‐certainty evidence).
Direct comparisons of different types and different dosages
The evidence is of low and mostly very low certainty.
Overall completeness and applicability of evidence
Diagnosis of COVID‐19 was confirmed by positive SARS‐CoV‐2 PCR testing in 93.8% of the participants. Regarding virological aspects, all participants included in this review were enrolled up to 26 May 2021 and none of the studies reported information on vaccination status. Thus, it is important to consider that the findings of this review might no longer be directly applicable to the current (i.e. late 2022) treatment situation of patients who are infected with later variants of SARS‐CoV‐2 including Delta and Omicron, and, at the same time, with an increasing proportion being vaccinated with different types and dosage regimens of SARS‐CoV‐2 vaccines or having recovered from prior infections. Specifically, these limitations regarding variants and vaccination apply most importantly to data comparison 1 (Systemic corticosteroids plus standard care versus standard care (plus/minus placebo)) for which recruitment of the majority of patients had ended in mid 2020 (Table 5).
In addition, a considerable share of participants also received various COVID‐19 treatment options such as antibiotics with potential antiviral and anti‐inflammatory properties (i.e. azithromycin), established antiviral drugs (e.g. remdesivir, lopinavir/ritonavir), hydroxychloroquine, convalescent plasma, or combinations of these drugs, mostly balanced between the arms. None of the trials evaluated participants with asymptomatic infections or mild disease (non‐hospitalised participants, WHO clinical progression scale 0 to 3); at this point we would like to refer the reader to the Cochrane Review Griesel 2022, addressing the use of inhaled corticosteroids against COVID‐19, which were mostly studied in outpatient participants with mild disease.
Considering the severity of COVID‐19 at the beginning of corticosteroid treatment, the difficult issue remains of the different scales of severity and progression used across studies and in the different guidelines and consensus statements (Marshall 2020; WHO 2021b). Similar to the first version of this review (Wagner 2021a), we used the need for respiratory support (no oxygen, low‐flow oxygen support, non‐invasive ventilation/high‐flow nasal cannula, and invasive ventilation) at randomisation and its changes as a surrogate for COVID‐19 disease severity. Among the 9314 of 9549 participants from all three comparisons for whom we could extract respiratory support information at randomisation, 16% did not receive any additional oxygen, 61% received any non‐invasive respiratory support, and 22% received invasive ventilation.
Regarding our equity‐related analyses, firstly we would like to highlight the fact that study participants in this version of the review mainly originated from high‐income countries. The share of participants from middle‐income countries has sunk from 13% in the first version of this review (Wagner 2021a) to 12% in this version, and again none came from low‐income countries although about 80% of the world's population lives in a low‐ or middle‐income country (Allen 2017). These numbers are quite similar to the findings of a systematic review on representation of low‐ and middle‐income countries in all COVID‐19‐related RCTs in high‐ranking journals, so the inequality extends beyond corticosteroids to the structural level (Ramanan 2022). Regarding the applicability of the evidence in this version of the review, unfortunately we must reiterate that it might only partially apply to people with COVID‐19 who are treated under different circumstances to those of most studies included in our review: there might be a more severe shortage of hospital beds in both ordinary wards and intensive care units, shortage of oxygen, and other resource constraints on the delivery of respiratory support, and other aspects of care labelled as standard care in this review.
Benefits
Effects on all‐cause mortality
As the main result of our analysis, we found that systemic corticosteroid treatment probably reduces all‐cause mortality (up to 30 days) in hospitalised patients with moderate to severe COVID‐19 from estimated absolute mortality of 27.4 % (standard of care, plus/minus placebo) to 24.6% (95% CI 23% to 26.5%). Considering this small effect size on all‐cause mortality (absolute mortality reduction 2.8%, RR 0.90), we aimed by additional subgroup analyses to identify subsets of patients potentially benefiting most and, further, to ascertain the types and doses of steroids that are more or less beneficial in treating COVID‐19 patients.
Disease severity by level of respiratory support
Since none of the newly included studies contained corresponding data subsets, the result of the subgroup analysis regarding respiratory support as an indicator for disease severity at baseline did not change: subgroup analysis did not reveal a significant difference in all‐cause mortality up to 30 days between the different levels of respiratory support. Despite missing statistical significance for a subgroup difference on 5% alpha error level, we observed a gradient of harm to benefit as the level of respiratory support increased at randomisation, which could be plausible from a biological perspective and might indicate harm in COVID‐19 patients without clinical signs of COVID‐19‐associated pulmonary gas exchange impairment, i.e. no oxygen at baseline. Nonetheless, for scientific rigour we kept our approach to subgroup analysis as per the first version of this review (Wagner 2021a), i.e. with the highest possible level of respiratory support (reported in each trial or through data request) at randomisation and refrained from a posteriori data‐driven pooling of all participants with any need for respiratory support. We acknowledge that this approach may lead to some overlap of subgroups and reduce statistical power; however, we would like to point out again that the observed consistent trend along with the increasing need for respiratory support and the negative effect among those without respiratory support is of informative value, too. However, there is a widely read pre‐planned analysis of combined respiratory support subgroups of the many participants of Horby 2021 in their referenced publication showing a clearer subgroup difference.
Comparison of different types of corticosteroids
Compared to the first version of this review (Wagner 2021a), our subgroup analysis of different types of corticosteroids included only one additional study with a very low number of participants treated with hydrocortisone (Munch 2021a). Hence, the majority of the participants (about 86%) included in this analysis were treated with dexamethasone. Again, we did not detect any significant differences between the estimated effects of dexamethasone, methylprednisolone, or hydrocortisone on all‐cause mortality in COVID‐19. We did an additional subgroup analysis regarding the different types of corticosteroids for the newly included outcomes all‐cause mortality up to 120 days and clinical improvement (discharged alive), but the certainty of the evidence was low to very low. Furthermore, equivalence of dosages could not be ensured. Hence, we refrain from further interpretation of those analyses. Further, unchanged from the first version of this review, in the direct comparison of two different types of corticosteroids the certainty of the evidence remains very low and interpretation of data unwarranted.
Dose escalation
Most participants in the RCTs included for the comparison of systemic corticosteroids versus standard care received daily doses of corticosteroids of hydrocortisone equivalent ≤ 200 mg/day, and we again refrained from subgroup analyses stratified by dosing because data for the high‐dose pulse regimens were very few. However, in this version of the review we were able to include a new comparison encompassing 1444 participants from four RCTs, in which different doses of dexamethasone were directly compared ‐ this had been identified as a research gap in the first version of this review (Wagner 2021a). Low‐certainty evidence showed that dexamethasone dosed at least twice as high (12 mg/day and higher, 300 mg hydrocortisone equivalent) as in Horby 2021 (6 mg/day, 150 mg hydrocortisone equivalent) may add to the probable slight reduction in All‐cause mortality up to 30 days from Analysis 1.1 when compared to low‐dose hydrocortisone equivalents (6 mg to 8 mg dexamethasone/day). Still, the decision for dose escalation based on our evidence should be critically scrutinised, taking into account the low‐certainty evidence basis for the cited result and that safety data on dose escalation are even more scarce in this comparison and of very low certainty. Moreover, large patient groups and settings peculiar to constrained resources and climate are again underrepresented, and harm through fungal secondary infections as discussed below can increase. Finally, the benefits and harms of corticosteroids do not only depend on dose but on treatment duration and regimens; the included studies only examined pulse dose and short‐term regimens of up to 10 days (or up to 14 days when dose tapering was part of the regimen).
Equity‐related subgroup analyses
Here we discuss the equity‐related subgroup analyses of the only moderate‐certainty outcome, All‐cause mortality up to 30 days in the comparison of systemic corticosteroids plus standard care versus standard care (plus/minus placebo).
It should be noted that all the subgroup analyses are only useful for generation of hypotheses, are not adjusted for multiple testing, suffer heavily from missing outcome data, and most likely lack statistical power.
Sex
In the analyses of sex, estimated effects of both groups were in favour of corticosteroid use without a large difference (Analysis 4.1).
Age
Participants younger than 70 years seem to benefit from corticosteroids in contrast to participants who are aged 70 years and older (Analysis 5.1), which might be attributable to the fact that the immune system's activity generally declines with entering the senium (Aw 2007). Consequently, targetting hyper‐inflammation in COVID‐19 in this older population with systemic corticosteroids could be less effective but more harmful due to known adverse effects of corticosteroids, including hyperglycaemia, further immunosuppression, and consequent vulnerability to secondary infection, which might outweigh the modest benefits as seen in our meta‐analysis (Analysis 1.1). Moreover, the degree of heterogeneity in each of the subgroups is much lower (below 10%) than in the analysis of the two subgroups combined (77%), which could be a hint for identifying one of the causes of overall heterogeneity.
Ethnicity
Black, Asian or minority ethnic group participants seem to benefit from corticosteroids in contrast to White participants, which we struggle to explain based on our own data without the possibility of multiple regression analysis (Analysis 6.1). However, these subgroup data were mainly from Horby 2021 and it is known from a pre‐COVID‐19, large prospective cohort study in the UK that first emergency hospital admissions in patients of Black and Asian ethnicity took place at a significantly earlier age than in Whites (Wan 2021), which might link this finding with the above discussed age‐stratified analysis. It is unclear why details on ethnicity were unavailable for some study participants, or whether they were missing at random or because of specific ethnicity.
Place of residence
In our own subgroup analysis, estimated effects were slightly in favour of corticosteroid use without a large difference (Analysis 7.1), but there are compelling signs from non‐RCT studies that widespread corticosteroid use in COVID‐19 might do substantial harm. Data from low‐ and middle‐income countries were relatively scarce, but we felt it was important to explore geographical and economical inequities and hence hypothesised beyond our approach that systemic corticosteroids might have a different impact on outcomes amongst people with COVID‐19 in low‐ and middle‐income countries. Related factors such as ethnicity and climatic zone have been shown to influence COVID‐19 outcomes (Liu 2021). Studies from the UK have consistently shown that ethnic minorities have a higher chance of having poorer COVID‐19 outcomes ‐ including hospitalisation and mortality (Aldridge 2020; Mathur 2021). Similar findings were made in Brazil where the Pardo and Preto ethnicities had a higher risk of COVID‐19‐related mortality (Baqui 2020). There were possible confounding factors such as larger family size, poor access to quality health care, and higher prevalence of co‐morbidities, which could have played a role in the association between ethnicity and COVID‐19 outcomes (Morales 2021). Regarding co‐morbidities, type 2 diabetes mellitus is of high importance: the prevalence varies significantly among various ethnicities and is exceptionally high among Asians and middle‐eastern countries (El‐Kebbi 2021; Ramachandran 2012). Hence, administration of systemic (gluco‐)corticosteroids like the one under study in this review could be associated with higher diabetes‐related adverse effects in populations with a higher prevalence of diabetes and less resources to diagnose and control the condition both acutely and chronically (Alessi 2020; Caughey 2013). Before the second wave of COVID‐19 began globally in March 2021 (WHO 2022a), it was hypothesised that countries with higher temperatures, relative humidity, and those closer to the equator would have fewer daily cases of COVID‐19, possibly due to unfavourable aerosol transmission, particularly in summer (Chen 2021). However, at the end of the second wave (July 2021), no such apparent dissimilarities across countries were noted in COVID‐19 prevalence. Despite the climatic factors, the implementation of public health policies such as social distancing and vaccination programmes could have played a part in the prevention of SARS‐CoV‐2 infections. This argument continues in the following discussion of the potential harms of systemic corticosteroid use.
Potential harms
In general, there is still a relevant underreporting of safety data (serious adverse events, adverse events, hospital‐acquired infections and fungal infections) from the included studies: only two evaluated serious adverse events for 678 participants, five reported partly selected adverse events for 660 participants, five studies provided information on hospital‐acquired infections for 660 participants, and only one study including 64 participants reported data on invasive fungal infections. Unfortunately, the largest included study did not report any adverse event data, but only four suspected drug reactions from the 1996 participants that received at least one dose of dexamethasone. Hence, the certainty of the evidence about potential harmful effects of corticosteroid treatment remains low and the few results from individual trials regarding safety outcomes should not be readily applied to the current clinical treatment situation of COVID‐19 patients.
Invasive fungal infections
As mentioned above, the certainty of the evidence about the safety outcome fungal infections and hospital‐acquired infections is very low. Nevertheless, specific difficult to treat fungal infections like mucormycosis and invasive aspergillosis increasingly draw attention in the context of widespread usage of corticosteroids in critical ill COVID‐19 patients. Even before the onset of COVID‐19, the prevalence of mucormycosis was high in Asian countries, particularly India (Prakash 2019). However, mucormycosis cases were on an unprecedented rapid rise in India during the second wave of COVID in April 2021. It throttled the already struggling health care machinery as the disease was invariably fatal either due to morbid surgery or highly nephrotoxic antifungal therapy. After COVID‐19, there was a sudden increase in the prevalence of mucormycosis. A single‐centre study from South India reported that poorly controlled diabetes (odds ratio of 4.6), previously undiagnosed diabetes (odds ratio of 3.3), and unwarranted steroid use (odds ratio of 28.4) were the three main risk factors that were associated with increased risk of mucormycosis in COVID‐19. The authors have highlighted that almost all the patients who had mucormycosis only had mild COVID‐19, which did not warrant corticosteroids in the management of COVID‐19 (Bhanuprasad 2021). From a global perspective, mucormycosis cases have been reported in various countries, including Europe. The high prevalence of diabetes among mucormycosis patients was a common factor across all countries (Hoenigl 2022). It is well known that corticosteroid therapy is associated with a higher risk of fungal infections. However, a retrospective study from Berlin, Germany reported more than twice the prevalence of aspergillosis in severe and critical COVID‐19 patients receiving corticosteroids compared to those who did not receive them. Diabetes, inappropriate use of steroids, oxygen, and antibiotics are all associated with mucormycosis in COVID‐19 patients (Aaranjani 2021). We tried to obtain these data for our review, particularly from Gautam 2021; however, the data were unavailable. In summary, while the certainty of the evidence about fungal and other secondary infections from prospective randomised trials remains very low, observational data from various countries indicate potential clinically relevant harmful effects of corticosteroid therapy in COVID‐19 patients.
Prospect of studies ongoing and awaiting classification
With regard to additional evidence from future publications, we identified 42 ongoing, recruiting, or temporarily halted studies (compared to 31 as identified in the first version of the review) (Wagner 2021a), encompassing approximately 13,500 participants. The number of studies described as completed, prematurely ended, or terminated grew from 16 to 23, encompassing approximately 5500 participants. Most of the studies intend to recruit people treated with different levels of respiratory support and a growing number seek to investigate different dexamethasone doses or different types of steroids. With the publication of even parts of these data, possible publication bias would be countered and changes to the precision and effect estimates themselves are not unlikely, although we do not expect a relevant difference or even a change of direction in the effect of mortality in the first comparison but rather more precise estimates for subgroup analyses, subordinate and safety outcomes, regarding dosing, and for outpatients. At this point we would like to emphasise that there are five completed and partially published studies from low‐ and middle‐income countries, for which we have so far unsuccessfully contacted the authors for full publication or additional information (Gautam 2021; Ghanei 2021; Montalvan 2021; Rashad 2021).
Quality of the evidence
Systemic corticosteroids plus standard care versus standard care (plus/minus placebo)
We included data from 10 RCTs in the analysis of the efficacy and safety of systemic corticosteroids. The population of interest was hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19 when compared to treatment with standard care (plus/minus placebo).
We rated the certainty of the evidence as moderate to very low (see Table 1). We downgraded the certainty of the evidence due to risk of bias arising from deviations from the intended intervention for all outcomes, missing adjustment for competing risk of death for all safety outcomes, selection of the reported results (all‐cause mortality up to 30 and 120 days and clinical improvement: discharged alive), missing information about allocation concealment (all‐cause mortality up to 30 and 120 days, clinical improvement: discharged alive, adverse events, hospital‐acquired infections, invasive fungal infections), baseline differences (all‐cause mortality up to 30 days), measurement of the outcome (new need for invasive mechanical ventilation or death), and reporting bias (serious adverse events, adverse events, hospital‐acquired infections, invasive fungal infections). Moreover, we downgraded for inconsistency for the following outcomes: all‐cause mortality up to 120 days, clinical improvement (discharged alive), and new need for invasive mechanical ventilation or death. Low numbers of events/imprecision affected all‐cause mortality up to 120 days and all safety outcomes.
Comparison of different types of corticosteroids
Methylprednisolone versus dexamethasone
We included data from one RCT assessing the efficacy and safety of methylprednisolone for individuals with a confirmed diagnosis of COVID‐19 when compared to treatment with dexamethasone.
We rated the certainty of the evidence as very low (see Table 2). We downgraded the certainty of the evidence due to risk of bias arising from the missing pre‐specification of the outcome and the missing protocol, and due to very serious imprecision.
High‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8 mg)
We included data from four RCTs assessing the efficacy and safety of different doses of dexamethasone for individuals with a confirmed diagnosis of COVID‐19.
We rated the certainty of the evidence as low to very low (see Table 3). We downgraded the certainty of the evidence due to risk of bias arising from deviations from the intended intervention (All‐cause mortality up to 30 and 120 days, Adverse events, Hospital‐acquired infections, Invasive fungal infections), missing information about the allocation concealment (All‐cause mortality up to 30 and 120 days, Clinical improvement: Discharged alive, Hospital‐acquired infections, Invasive fungal infections), missing adjustment for competing risk of death (all safety outcomes) and measurement of the outcome (Hospital‐acquired infections, Invasive fungal infections). Furthermore, we downgraded for inconsistency for All‐cause mortality up to 120 days and Hospital‐acquired infections. Low numbers of events/imprecision affected all outcomes.
Critical appraisal of selected outcome parameters
Outcomes with death as competing risk
Death and our exploratory endpoints in the domain of clinical improvement and worsening, as well as safety data, have to be seen as semi‐competing risks for each other: death precludes the occurrence of non‐terminal outcomes if participants die early. We discussed the issue extensively in the first version of this review, and it still has an impact on the risk of bias assessment and decisions not to meta‐analyse non‐terminal endpoints that were not adjusted by design or modelling (Brock 2011; Columbia Public Health 2021; Wu 2020).
Composite outcomes
Conceptual peculiarity of composite outcomes like New need for invasive mechanical ventilation or death and Discharged alive with inherent quasi‐adjustment for competing risk of death were discussed in the first version of this review.
Importance of platform trials and their specific sources of bias
Without a doubt, platform trials such as the included studies Angus 2020 and Horby 2021 offered great chances for rapid and adaptive generation of evidence involving huge numbers of participants in the pandemic. A few platform trials have extraordinarily contributed to the evidence base of pharmacotherapy in COVID‐19, which can be illustrated by their weight in the main RCT‐only mortality analyses in selected Cochrane Reviews: 99.6% regarding colchicine (Mikolajewska 2021), 77% regarding remdesivir (Ansems 2021), > 90% overall regarding convalescent plasma (Piechotta 2021), 100% regarding inhaled corticosteroids (Griesel 2022), and 51% regarding systemic corticosteroids in the first version of this review (Wagner 2021a). Thus, by impacting evidence synthesis their results have significantly influenced treatment guideline recommendations on COVID‐19 treatment. Nevertheless, they inherently have specific sources of risk of bias through their adaptive, multi‐arm, and often pragmatic (e.g. missing source data verification in Horby 2021) and open‐label designs, which are under‐ or unrepresented in the latest tools for risk of bias assessment in randomised trials, e.g. RoB 2 (Sterne 2019). In an attempt to address these issues and since there is not yet an established tool for critically appraising platform trials, we pioneered a checklist (Park 2020), with results available at https://zenodo.org/record/7015269#.YwOn43HP2Ul. In summary, easily detectable bias risk arose from the combination of open‐label and pragmatic design, leading to questionable allocation concealment. However, it was not feasible to sufficiently review and judge the different protocol versions and statistical architecture with its main pillars of multiple interim analyses, adaptive randomisation, and case‐count reducing compilation of control groups within factorial trial design from the outside without employing additional expert resources. The scientific community needs to build up expertise in reviewing platform trials and research groups conducting them should ensure high‐quality standards of data acquisition despite the pragmatic approaches and support the understanding of their architecture in comparison to traditionally performed RCTs in their respective fields of research.
Potential biases in the review process
In addition to peer‐reviewed, full‐text articles, we also included preprints. We are aware of the potentially lower quality of preprint publications, and that the results could change once the peer‐reviewed journal publications are available. In cases of missing data, we contacted study authors for additional data or relevant details if we needed more information. We are confident that we identified all relevant studies and will monitor ongoing studies as well as full publications of preprints closely after the publication of this review.
We decided on definitions of subgroups before running the first analyses based on the availability of data and based on clinical considerations. Subgroup analyses are exploratory only and confounding variables may have impacted their influence through biology, equity, or both. Our equity‐related subgroup analyses, like the other meta‐analyses, were not adjusted for multiple testing.
Agreements and disagreements with other studies or reviews
In the first version of this review (Wagner 2021a), we compared our findings to the four RCT‐only reviews: Chaudhuri 2021; Pasin 2021; Siemieniuk 2020; Sterne 2020. Since then no updates on these nor other high‐quality, RCT‐only systematic reviews of compelling relevance for discussion in this field have been published.
Once again, the open‐label adaptive and pragmatic platform study Horby 2021 must be discussed due to its huge impact. Not only was it the largest contributor to our review in terms of events and participants, but it also had an immense influence on treatment guidelines and ongoing studies in 2020 when its preliminary report became available (WHO 2021c). The direction and size of the effect on 30‐day mortality is congruent with our overall findings as well as the findings in the subgroup analysis stratified by respiratory support at randomisation. It is worth highlighting that this statement is based on analyses of unadjusted dichotomous 30‐day mortality data, including Horby 2021, in this review, while the authors of Horby 2021 in their publication presented rate ratios of time‐to‐event data from age‐adjusted Cox regression.
Authors' conclusions
Implications for practice.
Based on the current evidence, we are moderately certain that systemic corticosteroids probably slightly reduce All‐cause mortality up to 30 days amongst hospitalised, symptomatic COVID‐19 patients while level of respiratory support might play a critical role in patient selection. This finding is supported by low‐certainty evidence for a slightly increased chance of clinical improvement and a slightly decreased risk of worsening. Subgroup analyses suggest that the beneficial effect of the intervention might vanish for patients aged 70 years and older, but could be stronger in patients of Black, Asian, or other non‐White ethnicity. Long‐term survival data up to 120 days is of very low certainty and hence inconclusive.
Direct evidence on types of corticosteroids in the second comparison is of very low certainty and hence also inconclusive. Dose escalation may add to the slight benefit on All‐cause mortality up to 30 days, but the certainty of the evidence is low. It is most important to state that evidence on safety throughout the comparisons is of very low certainty because of underreporting and missing adjustment for competing risk of death.
The applicability of the data is limited. Data primarily came from European high‐income countries and are therefore limited in their applicability to settings different from that with regard to resources, climate, and other infectious diseases. Our own subgroup analyses are inconclusive in that regard but non‐RCT data raise suspicion of a potential for harm. Moreover, even in this update of the review the data were generated from unvaccinated participants and before the first occurrence of the recent variants of SARS‐CoV‐2, so the evidence may not be fully transferable to patients in 2022 and beyond.
Currently, there is no evidence to characterise the benefits and harms of corticosteroids in patients with asymptomatic or mild disease (non‐hospitalised) and regarding timing of the intervention.
Implications for research.
To address large uncertainties in the already existing analyses, we would prioritise the following:
Applicability: RCT data from low‐ and middle‐income countries and diverse environments is needed. All publishers should support timely and adequate reporting of already completed studies.
Safety data (adverse events/serious adverse events, detailed reporting of secondary infections): study authors should consistently measure and report adverse events, serious adverse events, and infections for both study arms.
Survival data: there is an urgent need for more long‐term data (up to 120 days and beyond) to improve the certainty of the evidence.
Patient‐centred outcomes: quality of life, neurological function, and independence in daily activities should be examined and reported.
Regimens: treatment dosing and duration are likely to influence both benefits and harms and the latter remains unaddressed in RCTs.
Interpretation of the current evidence warrants a call for new RCTs in the main comparison of systemic steroids plus standard care to standard care alone (plus/minus placebo) directly investigating the following:
Age: as there are some hints in the subgroup analysis that older people (above 70 years) might benefit less, study authors should report subgroup analyses for different age groups.
Immunological effects of recent variants and vaccination: re‐applying study designs from 2020 in contemporary and vaccinated populations.
We identified 42 ongoing and 23 completed RCTs lacking publication or important information in trials registries and databases, which will probably increase the certainty of the evidence in the future. In accordance with the living systematic review approach, we will continually update our search and include eligible trials.
What's new
| Date | Event | Description |
|---|---|---|
| 29 April 2022 | New citation required and conclusions have changed | New studies included, new comparisons, equity aspects considered. |
| 28 April 2022 | New search has been performed | Update search on January 6, 2022, inclusion of new studies, and introduction of new methods and focus on health equity. |
History
Review first published: Issue 8, 2021
Notes
Parts of the review's methods section and of the background were adopted from Cochrane Haematology templates (Kreuzberger 2021; Piechotta 2021).
Risk of bias
Risk of bias for analysis 1.9 Quality of life up to 120 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment; Control group: 5 excluded before starting treatment, 3 excluded after starting treatment As the study is meant to detect a positive effect of corticosteroids, participants in the control group receiving the experimental medication lead to expected bias towards null. Hence, we only see a slight tendency of under‐estimating the effect, but there is no increase in the risk to mistakenly introduce a medication for its beneficial effect. |
High risk of bias | Because of the issue of competing risk of death all data for this outcome might not be available. There was no adjustment in the analysis for competing risk of death. | Low risk of bias | We judged this domain low because the measurements were similar between groups. | Some concerns | The outcome was presented on a single scale and with one analysis only, but was not prespecified which leads to some concerns. | High risk of bias | Overall we see high risk bias due to missing adjustment for competing risks |
Risk of bias for analysis 7.2 All‐cause mortality up to 120 days.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 7.2.1 High‐income countries | ||||||||||||
| Munch 2021a | Low risk of bias | No issues with randomisation process. | Low risk of bias | Withdrawals with consecutive open‐label steroids may have affected the outcome, but withdrawals and non‐compliance was rather balanced after all. | Low risk of bias | No missing data. | Low risk of bias | No issues with measurement. | Low risk of bias | No relevant issues with the reported result. | Low risk of bias | Withdrawals because of the experimental context lead to some concerns (but it is less than 10% of all patients). |
| Subgroup 7.2.2 Low‐ and middle‐income countries | ||||||||||||
| Edalatifard 2020 | Some concerns | No information about the allocation concealment. | Some concerns | 6 patients in the control group received the intervention drug and were excluded from the analyses (17%). | Low risk of bias | The data were requested from the authors because the follow‐up time was not clearly visible from the publication. | Low risk of bias | The measurements were similar between groups. | Some concerns | Neither the protocol nor the SAP were available | Some concerns | Overall judged some concerns due to the randomisation process, protocol deviations and the selection of the reported results. |
| Jeronimo 2020 | Low risk of bias | An independent statistician prepared an electronically generated randomisation list with 14 blocks of 30 participants per block, generated via R software version 3.6.1 (blockrand package). The list was accessible only to non‐blinded pharmacists in the study. Participants were randomised by the study pharmacist to their designated treatment regimen at the time of inclusion and were subsequently identified throughout the study only by their allocated study number. There were no major differences in baseline characteristics between the intervention and placebo groups |
Some concerns | Intervention group: 14 excluded before starting treatment, 1 excluded after starting treatment Control group: 5 excluded before starting treatment, 3 excluded after starting treatment |
Low risk of bias | 416 participants randomised and 416 participants analysed. | Low risk of bias | The measurements were similar between groups | Low risk of bias | Protocol and statistical plan available. Data analysed and presented according to a pre‐specified plan. | Some concerns | Overall judged some concerns due to protocol deviations. |
Risk of bias for analysis 7.3 Clinical improvement: discharged alive.
| Study | Bias | |||||||||||
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall | |||||||
| Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | Authors' judgement | Support for judgement | |
| Subgroup 7.3.1 High‐income country | ||||||||||||
| Horby 2021 | Low risk of bias | Randomisation was performed with the use of a web‐based system with concealment of the trial‐group assignment. No baseline differences between the groups. | Some concerns | 8% of the participants in the control group received dexamethasone | Low risk of bias | Data for this outcome was available for all participants randomised. | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement. | Low risk of bias | No issue with selective reporting. | Some concerns | Overall judged some concerns due to the randomisation process, protocol deviations and limited bias in measurement. |
| Subgroup 7.3.2 Low‐ and middle‐income country | ||||||||||||
| Edalatifard 2020 | Some concerns | No information about the allocation concealment. | Some concerns | In this study, patients did not know which group of them used medicine Physicians and clinicians team know about the medicine and intervention groups. 6 patients in the control group received the intervention drug and were excluded from the analyses Intention‐to‐treat |
Low risk of bias | Data for this outcome was available for all participants randomised | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement.No protocol or SAP available. | Some concerns | Neither the protocol nor the SAP were available | Some concerns | Overall judged some concerns due to missing information about the allocation concealment, deviations from the intended interventions, measurement of the outcome and selection of the reported result |
| Tomazini 2020 | Low risk of bias | Randomisation was performed through an online web‐based system using computer‐generated random numbers and blocks of 2 and 4, unknown to the investigators, and was stratified by centre. The group treatment was disclosed to the investigator only after all information regarding patient enrolment was recorded in the online system. Baseline characteristics were well‐balanced between groups. |
Some concerns | 25 deviations from protocol in the intervention arm (16.55%); 1 patient received a corticosteroid other than dexamethasone. In the control arm, 52 patients received corticosteroids, of which 14 were protocol deviations (9.4%). | Low risk of bias | Data for this outcome was available for all participants randomised | Some concerns | Outcome assessors were aware of the treatment assignments. Knowledge of intervention received could have affected ascertainment only in patients who had not died. So the influence of the unblinded assessor is limited but existing ‐ therefore deviation between algorithm and judgement. | Low risk of bias | The protocol and statistical analysis plan were available. Outcomes reported as prespecified. | Some concerns | Overall rated some concerns due to protocol deviations and measurement of the outcome. |
Acknowledgements
We thank the investigators of four studies for providing us with additional data for this version of the review: Luis Corral‐Gudino for Corral‐Gudino 2021, Bruno Tomazini for Tomazini 2020, Anders Granholm for Munch 2021b, and Agostina Velo for Maskin 2021. The early phase of this research was supported by the German Federal Ministry of Education and Research (NaFoUniMedCovid19, funding number: 01KX2021; part of the project "CEOSys"). The contents of this document reflect only the authors' views and the German Ministry is not responsible for any use that may be made of the information it contains. We would like to thank the individuals who have contributed to this review through their work on the first version: Karoline Kley, Anika Mueller, Monika Nothacker, and Marco Kopp.
Disclaimer: CW, MG, MIM, and ALF personnel costs were partly covered by the German Federal Ministry of Education and Research (NaFoUniMedCovid19, funding number: 01KX2021; part of the project "CEOSys"). The contents of this document reflect only the authors' views and the German Ministry is not responsible for any use that may be made of the information it contains.
Cochrane Haematology supported the development of this review update. Nicole Skoetz and Carina Wagner are members of Cochrane Haematology but were not involved in the editorial process or decision‐making for this review. The following people conducted the editorial process for this review:
Sign‐off Editor (final editorial decision): Harald Herkner, Medical University of Vienna, Austria; Co‐ordinating Editor of the Cochrane Emergency and Critical Care Group
Managing Editor (selected peer reviewers, provided comments, collated peer reviewer comments, provided editorial guidance to authors, edited the article): Joey Kwong, Cochrane Central Editorial Service
Editorial Assistant (conducted editorial policy checks and supported editorial team): Leticia Rodrigues, Cochrane Central Editorial Service
Copy Editor (copy‐editing and production): Jenny Bellorini, Central Production Service
Peer reviewers (provided comments and recommended an editorial decision): Jennifer Petkovic, University of Ottawa (Equity Methods Reviewer); Robert Walton, Cochrane UK (Summary Versions Reviewer); Robin Featherstone, Cochrane Central Editorial Service (Information Specialist Reviewer); Nuala Livingstone, Cochrane Evidence Production and Methods Directorate (Methods Reviewer); Konstantinos Kostikas, Respiratory Medicine Department, University of Ioannina, Greece (Clinical/Content Reviewer); Alireza FakhriRavari, Loma Linda University School of Pharmacy (Clinical/Content Reviewer); Nida Qadir, Division of Pulmonary and Critical Care Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA (Clinical/Content Reviewer); Annabel Dawson (Consumer Reviewer)
Appendices
Appendix 1. Search strategies (previous review published on 16 August 2021)
Cochrane COVID‐19 Study Register
Search string:
corticosteroid* OR corticoid* OR prednison* OR dehydrocortison* OR deltason* OR decortin* OR orasone* OR deltra* OR meticorten* OR cortancyl* OR deltacorten* OR dacortin* OR adasone* OR "delta‐cortison" OR panasol* OR decorton* OR metacortandracin* OR paracort* OR predicor* OR decortisyl* OR delta‐1‐cortison* OR "delta‐dome" OR deltadehydrocortison* OR ofisolon* OR panafcort* OR predicorten* OR predni* OR econonson* OR promifen* OR servison* OR deltison* OR lisacort* OR meproson* OR rayos OR sterapred* OR "liquid pred" OR cortan* OR rectodelt* OR predeltin* OR prednisolon* OR methylprednisolon* OR medrol OR "pred forte" OR medrone OR urbason OR wyacort OR "Delta‐F" OR duralon* OR medrate OR omnipred OR adlone OR caberdelta OR depmedalon* OR "Depo Moderin" OR "Depo‐Nisolone" OR Emmetipi OR esameton* OR firmacort OR medlon* OR "Mega‐Star" OR meprolon* OR metilbetason* OR metrocort OR metypresol OR metysolon* OR orapred OR "Predni‐M‐Tablinen" OR radilem OR sieropresol OR solpredon* OR "A‐MethaPred" OR prelone OR medrone OR aprednislon OR pediapred OR hostacortin OR "Di‐Adreson‐F" OR adnisolon* OR capsoid OR cortalon* OR cortisolon* OR deltacortril OR estilsona OR panafcortelone OR sterane OR "Delta‐Cortef" OR econopred OR dacortin OR decaprednil OR "Delta‐Diona" OR "Delta‐Phoricol" OR deltahydrocortison* OR deltasolon* OR deltidrosol OR dhasolone OR fisopred OR frisolona OR gupison* OR hydeltra OR hydeltrasol OR klismacort OR kuhlprednon OR lenisolon* OR "Lepi‐Cortinolo" OR "Linola‐H" OR longiprednil OR metacortandralon* OR "Meti Derm" OR meticortelon* OR opredsone Or precortisyl OR "Pred‐Clysma" OR predeltilon* OR prenilone OR hydrocortancyl OR "Solu Moderin" OR predonin* OR metypred OR prednisol OR dexamethason* OR "BB 1101" OR decadron OR hexadrol OR fortecortin OR dexameth OR dexone OR hexadecadrol OR desamethason* OR ozurdex OR deronil OR baycuten OR aacidexam OR spersadex OR dexacortal OR gammacorten OR visumetazon* OR adexone OR "Alba‐Dex" OR cortidexason OR decacort OR decadrol OR dectancyl OR desameton OR loverine OR millicorten OR orgadrone OR alin OR auxiloson OR cortisumman OR decalix OR decameth OR decasone OR dekacort OR deltafluorene OR "Dexa‐Mamallet" OR dexafluorene OR dexalocal OR dexamecortin OR dexamonozon OR dexapos OR dexinoral OR fluorodelta OR lokalison OR methylfluorprednisolon* OR mymethason* OR "Dexa‐Rhinosan" OR "Dexa‐Scheroson" OR "Dexa‐sine" OR dexacortin OR dexafarma OR dinormon OR baycadron OR "Aeroseb‐Dex" OR Maxidex OR Dextenza OR dexasone OR dexpak OR hydrocortison* OR cortisol OR cortef OR hydrocorton* OR cetacort OR barseb OR aeroseb OR "Cort‐Dome" OR cortenema OR cortril OR cortifan OR cortispray OR dermacort OR domolene OR eldecort OR hautosone OR "Heb‐Cort" OR hytone OR Komed OR Nutracort OR Proctocort OR Rectoid OR Hydrocort OR locoid OR Solu‐Glyc
Study characteristics: 1) "Intervention assignment": “Randomised” OR 2) "Study type": "Interventional" AND "Study design": "Parallel/Crossover" OR 3) "Study type": "Interventional" AND "Study design": "Unclear"
Web of Science Core Collection (Advanced search)
#1 TI=( corticosteroid* OR corticoid* OR prednison* OR dehydrocortison* OR deltason* OR decortin* OR orasone* OR deltra* OR meticorten* OR cortancyl* OR deltacorten* OR dacortin* OR adasone* OR "delta‐cortison" OR panasol* OR decorton* OR metacortandracin* OR paracort* OR predicor* OR decortisyl* OR delta‐1‐cortison* OR "delta‐dome" OR deltadehydrocortison* OR ofisolon* OR panafcort* OR predicorten* OR predni* OR econonson* OR promifen* OR servison* OR deltison* OR lisacort* OR meproson* OR rayos OR sterapred* OR "liquid pred" OR cortan* OR rectodelt* OR predeltin* OR prednisolon* OR methylprednisolon* OR medrol OR "pred forte" OR medrone OR urbason OR wyacort OR "Delta‐F" OR duralon* OR medrate OR omnipred OR adlone OR caberdelta OR depmedalon* OR "Depo Moderin" OR "Depo‐Nisolone" OR Emmetipi OR esameton* OR firmacort OR medlon* OR "Mega‐Star" OR meprolon* OR metilbetason* OR metrocort OR metypresol OR metysolon* OR orapred OR "Predni‐M‐Tablinen" OR radilem OR sieropresol OR solpredon* OR "A‐MethaPred" OR prelone OR medrone OR aprednislon OR pediapred OR hostacortin OR "Di‐Adreson‐F" OR adnisolon* OR capsoid OR cortalon* OR cortisolon* OR deltacortril OR estilsona OR panafcortelone OR sterane OR "Delta‐Cortef" OR econopred OR dacortin OR decaprednil OR "Delta‐Diona" OR "Delta‐Phoricol" OR deltahydrocortison* OR deltasolon* OR deltidrosol OR dhasolone OR fisopred OR frisolona OR gupison* OR hydeltra OR hydeltrasol OR klismacort OR kuhlprednon OR lenisolon* OR "Lepi‐Cortinolo" OR "Linola‐H" OR longiprednil OR metacortandralon* OR "Meti Derm" OR meticortelon* OR opredsone Or precortisyl OR "Pred‐Clysma" OR predeltilon* OR prenilone OR hydrocortancyl OR "Solu Moderin" OR predonin* OR metypred OR prednisol OR dexamethason* OR "BB 1101" OR decadron OR hexadrol OR fortecortin OR dexameth OR dexone OR hexadecadrol OR desamethason* OR ozurdex OR deronil OR baycuten OR aacidexam OR spersadex OR dexacortal OR gammacorten OR visumetazon* OR adexone OR "Alba‐Dex" OR cortidexason OR decacort OR decadrol OR dectancyl OR desameton OR loverine OR millicorten OR orgadrone OR alin OR auxiloson OR cortisumman OR decalix OR decameth OR decasone OR dekacort OR deltafluorene OR "Dexa‐Mamallet" OR dexafluorene OR dexalocal OR dexamecortin OR dexamonozon OR dexapos OR dexinoral OR fluorodelta OR lokalison OR methylfluorprednisolon* OR mymethason* OR "Dexa‐Rhinosan" OR "Dexa‐Scheroson" OR "Dexa‐sine" OR dexacortin OR dexafarma OR dinormon OR baycadron OR "Aeroseb‐Dex" OR Maxidex OR Dextenza OR dexasone OR dexpak OR hydrocortison* OR cortisol OR cortef OR hydrocorton* OR cetacort OR barseb OR aeroseb OR "Cort‐Dome" OR cortenema OR cortril OR cortifan OR cortispray OR dermacort OR domolene OR eldecort OR hautosone OR "Heb‐Cort" OR hytone OR Komed OR Nutracort OR Proctocort OR Rectoid OR Hydrocort OR locoid OR Solu‐Glyc) OR AB=( corticosteroid* OR corticoid* OR prednison* OR dehydrocortison* OR deltason* OR decortin* OR orasone* OR deltra* OR meticorten* OR cortancyl* OR deltacorten* OR dacortin* OR adasone* OR "delta‐cortison" OR panasol* OR decorton* OR metacortandracin* OR paracort* OR predicor* OR decortisyl* OR delta‐1‐cortison* OR "delta‐dome" OR deltadehydrocortison* OR ofisolon* OR panafcort* OR predicorten* OR predni* OR econonson* OR promifen* OR servison* OR deltison* OR lisacort* OR meproson* OR rayos OR sterapred* OR "liquid pred" OR cortan* OR rectodelt* OR predeltin* OR prednisolon* OR methylprednisolon* OR medrol OR "pred forte" OR medrone OR urbason OR wyacort OR "Delta‐F" OR duralon* OR medrate OR omnipred OR adlone OR caberdelta OR depmedalon* OR "Depo Moderin" OR "Depo‐Nisolone" OR Emmetipi OR esameton* OR firmacort OR medlon* OR "Mega‐Star" OR meprolon* OR metilbetason* OR metrocort OR metypresol OR metysolon* OR orapred OR "Predni‐M‐Tablinen" OR radilem OR sieropresol OR solpredon* OR "A‐MethaPred" OR prelone OR medrone OR aprednislon OR pediapred OR hostacortin OR "Di‐Adreson‐F" OR adnisolon* OR capsoid OR cortalon* OR cortisolon* OR deltacortril OR estilsona OR panafcortelone OR sterane OR "Delta‐Cortef" OR econopred OR dacortin OR decaprednil OR "Delta‐Diona" OR "Delta‐Phoricol" OR deltahydrocortison* OR deltasolon* OR deltidrosol OR dhasolone OR fisopred OR frisolona OR gupison* OR hydeltra OR hydeltrasol OR klismacort OR kuhlprednon OR lenisolon* OR "Lepi‐Cortinolo" OR "Linola‐H" OR longiprednil OR metacortandralon* OR "Meti Derm" OR meticortelon* OR opredsone Or precortisyl OR "Pred‐Clysma" OR predeltilon* OR prenilone OR hydrocortancyl OR "Solu Moderin" OR predonin* OR metypred OR prednisol OR dexamethason* OR "BB 1101" OR decadron OR hexadrol OR fortecortin OR dexameth OR dexone OR hexadecadrol OR desamethason* OR ozurdex OR deronil OR baycuten OR aacidexam OR spersadex OR dexacortal OR gammacorten OR visumetazon* OR adexone OR "Alba‐Dex" OR cortidexason OR decacort OR decadrol OR dectancyl OR desameton OR loverine OR millicorten OR orgadrone OR alin OR auxiloson OR cortisumman OR decalix OR decameth OR decasone OR dekacort OR deltafluorene OR "Dexa‐Mamallet" OR dexafluorene OR dexalocal OR dexamecortin OR dexamonozon OR dexapos OR dexinoral OR fluorodelta OR lokalison OR methylfluorprednisolon* OR mymethason* OR "Dexa‐Rhinosan" OR "Dexa‐Scheroson" OR "Dexa‐sine" OR dexacortin OR dexafarma OR dinormon OR baycadron OR "Aeroseb‐Dex" OR Maxidex OR Dextenza OR dexasone OR dexpak OR hydrocortison* OR cortisol OR cortef OR hydrocorton* OR cetacort OR barseb OR aeroseb OR "Cort‐Dome" OR cortenema OR cortril OR cortifan OR cortispray OR dermacort OR domolene OR eldecort OR hautosone OR "Heb‐Cort" OR hytone OR Komed OR Nutracort OR Proctocort OR Rectoid OR Hydrocort OR locoid OR Solu‐Glyc)
#2 TI=(COVID OR COVID19 OR "SARS‐CoV‐2" OR "SARS‐CoV2" OR SARSCoV2 OR "SARSCoV‐2" OR "SARS coronavirus 2" OR "2019 nCoV" OR "2019nCoV" OR "2019‐novel CoV" OR "nCov 2019" OR "nCov 19" OR "severe acute respiratory syndrome coronavirus 2" OR "novel coronavirus disease" OR "novel corona virus disease" OR "corona virus disease 2019" OR "coronavirus disease 2019" OR "novel coronavirus pneumonia" OR "novel corona virus pneumonia" OR "severe acute respiratory syndrome coronavirus 2") OR AB=(COVID OR COVID19 OR "SARS‐CoV‐2" OR "SARS‐CoV2" OR SARSCoV2 OR "SARSCoV‐2" OR "SARS coronavirus 2" OR "2019 nCoV" OR "2019nCoV" OR "2019‐novel CoV" OR "nCov 2019" OR "nCov 19" OR "severe acute respiratory syndrome coronavirus 2" OR "novel coronavirus disease" OR "novel corona virus disease" OR "corona virus disease 2019" OR "coronavirus disease 2019" OR "novel coronavirus pneumonia" OR "novel corona virus pneumonia" OR "severe acute respiratory syndrome coronavirus 2")
#3 #1 AND #2
#4 TI=(random* OR placebo OR trial OR groups OR "phase 3" or "phase3" or p3 or "pIII") OR AB=(random* OR placebo OR trial OR groups OR "phase 3" or "phase3" or p3 or "pIII")
#5 #3 AND #4
Indexes=SCI‐EXPANDED, ESCI Timespan=2020‐2021
WHO COVID‐19 Global literature on coronavirus disease
(corticosteroid* OR corticoid* OR prednis* OR hydrocorti* OR methylpredni* OR deltahydrocorti* OR dehydrocorti* OR dexameth* OR desameth*) AND (random* OR placebo OR trial OR groups OR "phase 3" or "phase3" or p3 or "pIII")
Appendix 2. Search strategies (update)
Cochrane COVID‐19 Study Register
Search string:
(corticosteroid* OR glucocorticoid* OR corticoid* OR cloprednol* OR methylpredni* OR metilpredni* OR predni* OR triamcinol* OR beclomet* OR betamet* OR dexamethas* OR dexametas* OR paramethas* OR parametas* OR prednyli* OR budesonid* OR deflazacort OR hydrocortis* OR cortison* OR fludrocortison*)
Study characteristics: 1) "Intervention assignment": “Randomised” OR “Quasi‐Randomised” OR 2) "Study design": "Parallel/Crossover" OR "Unclear" = 356 studies (621 references) Web of Science Core Collection (Advanced search)
#1 TI=(corticosteroid* OR glucocorticoid* OR corticoid* OR cloprednol* OR methylpredni* OR metilpredni* OR predni* OR triamcinol* OR beclomet* OR betamet* OR dexamethas* OR dexametas* OR paramethas* OR parametas* OR prednyli* OR budesonid* OR deflazacort OR hydrocortis* OR cortison* OR fludrocortison*) OR AB=(corticosteroid* OR glucocorticoid* OR corticoid* OR cloprednol* OR methylpredni* OR metilpredni* OR predni* OR triamcinol* OR beclomet* OR betamet* OR dexamethas* OR dexametas* OR paramethas* OR parametas* OR prednyli* OR budesonid* OR deflazacort OR hydrocortis* OR cortison* OR fludrocortison*)
#2 TI=(COVID OR COVID19 OR "SARS‐CoV‐2" OR "SARS‐CoV2" OR SARSCoV2 OR "SARSCoV‐2" OR "SARS coronavirus 2" OR "2019 nCoV" OR "2019nCoV" OR "2019‐novel CoV" OR "nCov 2019" OR "nCov 19" OR "severe acute respiratory syndrome coronavirus 2" OR "novel coronavirus disease" OR "novel corona virus disease" OR "corona virus disease 2019" OR "coronavirus disease 2019" OR "novel coronavirus pneumonia" OR "novel corona virus pneumonia" OR "severe acute respiratory syndrome coronavirus 2") OR AB=(COVID OR COVID19 OR "SARS‐CoV‐2" OR "SARS‐CoV2" OR SARSCoV2 OR "SARSCoV‐2" OR "SARS coronavirus 2" OR "2019 nCoV" OR "2019nCoV" OR "2019‐novel CoV" OR "nCov 2019" OR "nCov 19" OR "severe acute respiratory syndrome coronavirus 2" OR "novel coronavirus disease" OR "novel corona virus disease" OR "corona virus disease 2019" OR "coronavirus disease 2019" OR "novel coronavirus pneumonia" OR "novel corona virus pneumonia" OR "severe acute respiratory syndrome coronavirus 2")
#3 #1 AND #2
#4 TI=(random* OR placebo OR trial OR groups OR "phase 3" or "phase3" or p3 or "pIII") OR AB=(random* OR placebo OR trial OR groups OR "phase 3" or "phase3" or p3 or "pIII")
#5 #3 AND #4 Indexes=SCI‐EXPANDED, ESCI Timespan=2020‐2022 = 967 WHO COVID‐19 Global literature on coronavirus disease
Title, abstract, subject: (corticosteroid* OR glucocorticoid* OR corticoid* OR cloprednol* OR methylpredni* OR metilpredni* OR predni* OR triamcinol* OR beclomet* OR betamet* OR dexamethas* OR dexametas* OR paramethas* OR parametas* OR prednyli* OR budesonid* OR deflazacort OR hydrocortis* OR cortison* OR fludrocortison*) AND (random* OR placebo OR trial OR groups OR "phase 3" or "phase3" or p3 or "pIII") =1964
Data and analyses
Comparison 1. Systemic corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 All‐cause mortality up to 30 days | 9 | 7898 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.84, 0.97] |
| 1.2 All‐cause mortality up to 120 days | 3 | 485 | Risk Ratio (M‐H, Random, 95% CI) | 0.74 [0.23, 2.34] |
| 1.3 Clinical improvement: discharged alive | 3 | 6786 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [1.03, 1.11] |
| 1.4 Clinical worsening: new need for IMV or death | 2 | 5586 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.84, 1.01] |
| 1.5 Serious adverse events | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.6 Adverse events | 3 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.7 Hospital‐acquired infections | 4 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.8 Invasive fungal infections | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.9 Quality of life up to 120 days | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.10 New need for dialysis | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.11 Viral clearance | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 2. Subgroup analysis: respiratory support for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 All‐cause mortality up to 30 days | 4 | 7137 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.81, 1.03] |
| 2.1.1 No oxygen | 1 | 1535 | Risk Ratio (M‐H, Random, 95% CI) | 1.27 [1.00, 1.61] |
| 2.1.2 Low‐flow oxygen only | 2 | 85 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.50, 1.63] |
| 2.1.3 NIV, high‐flow, and low‐flow oxygen combined | 1 | 3883 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.79, 1.00] |
| 2.1.4 NIV or high‐flow oxygen only | 2 | 195 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.53, 1.58] |
| 2.1.5 Invasive ventilation | 3 | 1439 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.70, 1.04] |
Comparison 3. Subgroup analysis: dexamethasone versus methylprednisolone versus hydrocortisone for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 All‐cause mortality up to 30 days | 9 | 7898 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.84, 0.97] |
| 3.1.1 Dexamethasone | 3 | 6774 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.83, 0.98] |
| 3.1.2 Methylprednisolone | 3 | 566 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.77, 1.24] |
| 3.1.3 Hydrocortisone | 3 | 558 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.56, 1.21] |
| 3.2 All‐cause mortality up to 120 days | 3 | 485 | Risk Ratio (M‐H, Random, 95% CI) | 0.74 [0.23, 2.34] |
| 3.2.1 Hydrocortisone | 1 | 30 | Risk Ratio (M‐H, Random, 95% CI) | 2.04 [0.65, 6.43] |
| 3.2.2 Methylprednisolone | 2 | 455 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.06, 3.04] |
| 3.3 Clinical improvement: discharged alive | 3 | 6786 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [1.03, 1.11] |
| 3.3.1 Dexamethasone | 2 | 6724 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [1.03, 1.11] |
| 3.3.2 Methylprednisolone | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.65 [1.18, 2.29] |
Comparison 4. Subgroup analysis: female versus male for the comparison of systemic corticosteroids versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 4.1 All‐cause mortality up to 30 days | 3 | 6788 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.83, 0.98] |
| 4.1.1 Female | 3 | 2475 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.81, 1.10] |
| 4.1.2 Male | 3 | 4313 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.80, 0.97] |
Comparison 5. Subgroup analysis: < 70 years versus ≥ 70 years for the comparison of systemic corticosteroids versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 5.1 All‐cause mortality up to 30 days | 3 | 6781 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.71, 1.10] |
| 5.1.1 < 70 years | 3 | 3885 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.60, 0.82] |
| 5.1.2 ≥ 70 years | 3 | 2896 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.92, 1.12] |
Comparison 6. Subgroup analysis: White versus Black, Asian or minority ethnic group versus unknown for the comparison of systemic corticosteroids versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 6.1 All‐cause mortality up to 30 days | 2 | 6489 | Risk Ratio (M‐H, Random, 95% CI) | 0.79 [0.60, 1.04] |
| 6.1.1 White | 2 | 4753 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.87, 1.06] |
| 6.1.2 Black, Asian or minority ethnic group | 1 | 1147 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.52, 0.93] |
| 6.1.3 Unknown | 1 | 589 | Risk Ratio (M‐H, Random, 95% CI) | 0.60 [0.41, 0.88] |
Comparison 7. Subgroup analysis: high‐income countries versus low‐ and middle‐income countries for the comparison of corticosteroids plus standard care versus standard care (plus/minus placebo) for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 7.1 All‐cause mortality up to 30 days | 9 | 7898 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.84, 0.97] |
| 7.1.1 High‐income countries | 5 | 7047 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.81, 0.97] |
| 7.1.2 Low‐ and middle‐income countries | 4 | 851 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.82, 1.09] |
| 7.2 All‐cause mortality up to 120 days | 3 | 485 | Risk Ratio (M‐H, Random, 95% CI) | 0.74 [0.20, 2.75] |
| 7.2.1 High‐income countries | 1 | 30 | Risk Ratio (M‐H, Random, 95% CI) | 2.62 [0.63, 10.98] |
| 7.2.2 Low‐ and middle‐income countries | 2 | 455 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.06, 3.04] |
| 7.3 Clinical improvement: discharged alive | 3 | 6786 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [1.03, 1.11] |
| 7.3.1 High‐income country | 1 | 6425 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [1.02, 1.10] |
| 7.3.2 Low‐ and middle‐income country | 2 | 361 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.65 [1.23, 2.21] |
Comparison 8. Methylprednisolone versus dexamethasone for hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 8.1 All‐cause mortality up to 30 days | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 9. High‐dose dexamethasone (12 mg/d or higher) versus low‐dose dexamethasone (6 to 8 mg/d) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 9.1 All‐cause mortality up to 30 days | 3 | 1269 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.73, 1.04] |
| 9.2 All‐cause mortality up to 120 days | 4 | 1383 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.79, 1.08] |
| 9.3 Clinical improvement: discharged alive | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 9.4 Serious adverse events | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 9.5 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 9.6 Hospital‐acquired infections | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 9.7 Invasive fungal infections | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 10. Subgroup analysis: female versus male for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 10.1 All‐cause mortality up to 30 days | 2 | 1069 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.72, 1.04] |
| 10.1.1 Female | 2 | 333 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.65, 1.22] |
| 10.1.2 Male | 2 | 736 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.62, 1.34] |
| 10.2 All‐cause mortality up to 120 days | 2 | 1066 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.74, 1.02] |
| 10.2.1 Female | 2 | 333 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.70, 1.23] |
| 10.2.2 Male | 2 | 733 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.70, 1.03] |
Comparison 11. Subgroup analysis: < 70 years versus ≥ 70 years for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 11.1 All‐cause mortality up to 30 days | 2 | 1069 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.73, 1.04] |
| 11.1.1 <70 years | 2 | 707 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.63, 1.07] |
| 11.1.2 ≥ 70 years | 2 | 362 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.73, 1.15] |
| 11.2 All‐cause mortality up to 120 days | 2 | 1066 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.76, 1.03] |
| 11.2.1 <70 years | 2 | 706 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.63, 1.02] |
| 11.2.2 ≥ 70 years | 2 | 360 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.78, 1.14] |
Comparison 12. Subgroup analysis: high‐income countries versus low‐ and middle‐income countries for the comparison of high‐dose dexamethasone (12 mg or higher) versus low‐dose dexamethasone (6 mg to 8mg) for hospitalised individuals with a confirmed diagnosis of symptomatic COVID‐19.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 12.1 All‐cause mortality up to 30 days | 3 | 1269 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.73, 1.04] |
| 12.1.1 High‐income countries | 2 | 1171 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.70, 1.02] |
| 12.1.2 Low‐ and middle‐income countries | 1 | 98 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.65, 1.71] |
| 12.2 All‐cause mortality up to 120 days | 4 | 1383 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.79, 1.08] |
| 12.2.1 High‐income countries | 2 | 1152 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.72, 1.01] |
| 12.2.2 Low‐ and middle‐income countries | 2 | 231 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.35 [0.93, 1.94] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Angus 2020.
| Study characteristics | ||
| Methods | Trial design: multicentre, open‐label, platform RCT Type of publication: journal publication Setting: inpatient Recruitment dates: 9 March to 17 June 2020 Country: Australia, Canada, France, Ireland, the Netherlands, New Zealand, UK, USA Language: English Number of centres: 121 clinical sites Trial registration number: NCT02735707 Date first posted: 13 April 2016 |
|
| Participants | Age: mean age of
Gender
Proportion of confirmed infections
Ethnicity
Number of participants (recruited/allocated/evaluated)
Severity of condition according to study definition
Severity of condition according to WHO score: severe ≥ 6 Co‐morbidities: diabetes, respiratory disease, kidney disease, severe cardiovascular disease, immunosuppressive disease Inclusion criteria
Exclusion criteria
|
|
| Interventions | Treatment details of intervention group (e.g dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses)
Duration of follow‐up: follow‐up ended 12 August 2020 Treatment cross‐overs: no Compliance with assigned treatment: yes |
|
| Outcomes | Primary study outcome: respiratory and cardiovascular organ support‐free days up to day 21, with subcomponents in‐hospital deaths and organ support‐free days among survivors Review outcomes: inpatient setting
Additional study outcomes: time to death, cardiovascular organ support–free days, length of ICU stay, WHO scale at day 14 |
|
| Identification | ||
| Notes | Date of publication: 2 September 2020 Sponsor/funding: Platform for European Preparedness Against (Re‐) emerging Epidemics (PREPARE) consortium by the European Union, FP7‐HEALTH‐2013‐INNOVATION‐1 (grant 602525), the Australian National Health and Medical Research Council (grant APP1101719), the New Zealand Health Research Council (grant 16/ 631), the Canadian Institute of Health Research Strategy for Patient‐Oriented Research Innovative Clinical Trials Program (grant 158584), the UK National Institute for Health Research (NIHR) and the NIHR Imperial Biomedical Research Centre, the Health Research Board of Ireland (grant CTN 2014‐012), the UPMC Learning While Doing Program, the Breast Cancer Research Foundation, the French Ministry of Health (grant PHRC‐20‐0147), and the Minderoo Foundation Risk of bias table presents two entries for analysis 1.1 All‐cause mortality and analysis 1.5 Serious adverse events: one entry for fixed‐dose arm and one for shock‐dependent arm |
|
Corral‐Gudino 2021.
| Study characteristics | ||
| Methods | Trial design: multicentre, open‐label, RCT Type of publication: journal publication Setting: inpatient Recruitment dates: April to May 2020 Country: Spain Language: English Number of centres: 5 hospitals Trial registration number: EUCTR 2020‐001934‐37 Date of trial registration: 8 May 2020 |
|
| Participants | Age: mean age of:
Gender:
Proportion of confirmed infections: PCR positivity inclusion criterion Ethnicity: not reported Number of participants (recruited/allocated/evaluated):
Severity of condition according to study definition
Severity of condition according to WHO score: moderate to severe 5 to 6 Co‐morbidities: hypertension, cardiac disease, respiratory disease, diabetes Inclusion criteria
Exclusion criteria:
|
|
| Interventions | Treatment details of intervention group (e.g dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses): standard care
Duration of follow‐up: until hospital discharge or day 28 after inclusion Treatment cross‐overs: no Compliance with assigned treatment: yes |
|
| Outcomes | Primary study outcome: composite endpoint including in‐hospital all‐cause mortality, escalation to ICU admission or progression of respiratory insufficiency that required noninvasive ventilation Review outcomes: inpatient setting
Additional study outcomes: composite endpoint included in‐hospital all‐cause mortality, escalation to ICU admission, or progression of respiratory insufficiency that required noninvasive ventilation |
|
| Identification | ||
| Notes | Date of publication: 3 February 2021 Sponsor/funding: IDIVAL Instituto de Investigación Sanitaria Valdecilla |
|
Dequin 2020.
| Study characteristics | ||
| Methods | Trial design: multicentre, double‐blind, randomised trial Type of publication: journal publication Setting: inpatient Recruitment dates: 7 March to 1 June 2020 Country: France Language: English Number of centres: 9 Trial registration number: NCT02517489 Date first posted: 7 August 2015 |
|
| Participants | Age:
Gender:
Proportion of PCR‐confirmed infections
Ethnicity: not reported Number of participants (recruited/allocated/evaluated):
Severity of condition according to study definition
Severity of condition according to WHO score: moderate to severe ≥ 5 Co‐morbidities: diabetes, COPD/asthma, immunosuppression Inclusion criteria
Exclusion criteria
|
|
| Interventions | Treatment details of intervention group (e.g dose, route of administration, number of doses):
Treatment details of control group (e.g. dose, route of administration, number of doses): placebo Concomitant therapy (e.g. description of standard care): not reported Duration of follow‐up: last follow‐up on 29 June 2020 Treatment cross‐overs: no Compliance with assigned treatment: yes |
|
| Outcomes | Primary study outcome: treatment failure on day 21 (death or persistent dependence of mechanical ventilation or high‐flow oxygen therapy) Review outcomes: Inpatient setting:
Additional study outcomes: endotracheal intubation (for patients noninvasively ventilated at inclusion), prone position, ECMO, inhaled nitric oxide |
|
| Identification | ||
| Notes | Date of publication: 6 October 2020 Sponsor/funding: University Hospital, Tours |
|
Edalatifard 2020.
| Study characteristics | ||
| Methods | Trial design: RCT Type of publication: journal publication Setting: inpatient Recruitment dates: 28 March to 28 May 2020 (study register entry) Country: Iran Language: English Number of centres: 4 Trial registration number: IRCT20200404046947N1 Date of trial registration: 15 April 2020 |
|
| Participants | Age
Gender:
Proportion of confirmed infections: PCR positivity inclusion criterion Ethnicity: not reported Number of participants (recruited/allocated/evaluated)
Severity of condition according to study definition
Severity of condition according to WHO score: moderate to severe 5 to 6 Co‐morbidities: diabetes, hypothyroidism, cancer, respiratory disorder, renal disorder, cardiovascular disorder, hypertension, autoimmune, and neurodegenerative diseases Inclusion criteria
Exclusion criteria
|
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses):
Treatment details of control group (e.g. dose, route of administration, number of doses): standard care
Duration of follow‐up: 3 days Treatment cross‐overs: no Compliance with assigned treatment: 6 patients in the control group received the intervention drug |
|
| Outcomes | Primary study outcome: time to event (discharge or death), time to improvement Review outcomes: inpatient setting
Additional study outcomes: blood SO2 level, BORG score, heart rate, temperature, respiratory rate |
|
| Identification | ||
| Notes | Date of publication: 7 September 2020 Sponsor/funding: Tehran University of Medical Sciences |
|
Farahani 2021.
| Study characteristics | ||
| Methods | Trial design: open‐label, single‐centre RCT Type of publication: preprint Setting: inpatient Recruitment dates: 30 March to 18 May 2020 (only estimated dates from registry entry) Country: Iran Language: English Number of centres: 1 Trial registration number: IRCT20200406046963N1 Date of trial registration: 22 April 2020 |
|
| Participants | Age (mean, SD): intervention group: 61.07 ± 12.83, control group: 66.80 ± 14.03 Gender (female, n (%)): intervention group: 4 (28,6), control group: 6 (40) Proportion of confirmed infections: PCR positivity inclusion criterion Ethnicity: no ethnicities excluded Number of participants (recruited/allocated/evaluated): 14 intervention group, 15 control group Severity of condition according to study definition:
Severity of condition according to WHO score: moderate‐severe 5 to 6 Co‐morbidities: not reported Inclusion criteria
Exclusion criteria
Previous treatments: not specified |
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses): 1000 mg methylprednisolone IV for 3 days followed by 1 mg/kg oral prednisolone with dose tapering for 7 days + standard care Treatment details of control group (e.g. dose, route of administration, number of doses): standard care Concomitant therapy (e.g. description of standard care):
Duration of follow‐up: not specified Treatment cross‐overs: none reported Compliance with assigned treatment: no deviations reported |
|
| Outcomes | Primary study outcome: mortality rate, blood O2 saturation and need for further oxygen therapy Review outcomes: inpatient setting
Additional study outcomes
|
|
| Identification | ||
| Notes | Date of publication: 9 September 2020 Sponsor/funding: Artesh University of Medical Sciences |
|
Horby 2021.
| Study characteristics | ||
| Methods | Trial design: open‐label RCT Type of publication: journal publication Setting: inpatient Recruitment dates: recruitment ended on 8 June 2020 Country: UK Language: English Number of centres: 176 Trial registration number: NCT04381936 Date of trial registration: 11 May 2020 |
|
| Participants | Age: mean age
Gender
Proportion of PCR test results
Ethnicity: not reported Number of participants (recruited/allocated/evaluated):
Severity of condition according to study definition
Severity of condition according to WHO score: moderate to severe 4 to 9 Co‐morbidities: diabetes, heart disease, chronic lung disease, tuberculosis, HIV infection, severe liver disease, severe kidney impairment Inclusion criteria
Exclusion criteria
Previous treatments: not reported |
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses)
Concomitant therapy (e.g. description of standard care): none Duration of follow‐up: until discharge or death, or 28 days after randomisation Treatment cross‐overs: no Compliance with assigned treatment: 8% in the control group received intervention drug |
|
| Outcomes | Primary study outcome: 28‐day mortality Review outcomes: inpatient setting
Additional study outcomes: composite outcome IMV or death |
|
| Identification | ||
| Notes | Date of publication: 17 July 2020 Sponsor/funding: University of Oxford |
|
Jamaati 2021.
| Study characteristics | ||
| Methods | Trial design: RCT Type of publication: journal publication Setting: inpatient Recruitment dates: March 2020 Country: Iran Language: English Number of centres: 1 Trial registration number: IRCT20151227025726N17 Date of trial registration: 31 May 2020 |
|
| Participants | Age: median age
Gender (male, n(%)):
Proportion of confirmed infections: PCR positivity inclusion criterion Ethnicity: not reported Number of participants (recruited/allocated/evaluated):
Severity of condition according to study definition: PaO2/FiO2 between 100 and 300 mmHg Severity of condition according to WHO score: most likely 5, no invasive ventilation at randomisation Co‐morbidities: diabetes, hypertension, cardiovascular disease Inclusion criteria
Exclusion criteria
Previous treatments: not reported |
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses)
Concomitant therapy (e.g. description of standard care): oxygen support, fluid support, lopinavir/ritonavir (200/50 mg, 2 tablets twice a day) Duration of follow‐up: 28 days Treatment cross‐overs: no Compliance with assigned treatment: yes |
|
| Outcomes | Primary study outcome: need for IMV, death rate Review outcomes: inpatient setting
Additional study outcomes: duration of clinical improvement, radiological changes in the CT scan |
|
| Identification | ||
| Notes | Date of publication: 16 February 2021 Sponsor/funding: Shahid Beheshti University of Medical Sciences |
|
Jeronimo 2020.
| Study characteristics | ||
| Methods | Trial design: double‐blind RCT Type of publication: journal publication Setting: inpatient Recruitment dates: 18 April to 16 June 2020 Country: Brazil Language: English Number of centres: 1 Trial registration number: NCT04343729 Date of trial registration: 13 April 2020 |
|
| Participants | Age: mean age
Gender
Proportion of PCR test results
Ethnicity: white, black, admixed, Asian, Amerindian Number of participants (recruited/allocated/evaluated)
Severity of condition according to study definition
Severity of condition according to WHO score: moderate to severe: 5 to 9 Co‐morbidities: diabetes, hypertension, alcohol use disorder, heart disease, asthma, rheumatic disease, liver disease, previous tuberculosis, COPD Inclusion criteria
Exclusion criteria
Previous treatments: not reported |
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses):
|
|
| Outcomes | Primary study outcome: 28‐day mortality Review outcomes: inpatient setting
Additional study outcomes: none |
|
| Identification | ||
| Notes | Date of publication: 12 August 2020 Sponsor/funding: Fundação de Medicina Tropical Dr. Heitor Vieira Dourado |
|
Maskin 2021.
| Study characteristics | ||
| Methods |
|
|
| Participants |
|
|
| Interventions |
|
|
| Outcomes | Primary study outcome: ventilator‐free days during the first 28 days (defined as the number of days alive and free from mechanical ventilation up to the 28th day from randomisation), co‐primary outcome: the time to complete and successful discontinuation of mechanical ventilation or death Review outcomes: inpatient setting
Additional study outcomes: the daily value of glucose and insulin dose, muscle strength score, and the frequency of delirium within 28 days of randomisation |
|
| Identification | ||
| Notes | Date of publication: 29 November 2021 Sponsor/funding: — |
|
Munch 2021a.
| Study characteristics | ||
| Methods |
|
|
| Participants |
|
|
| Interventions |
|
|
| Outcomes | Primary study outcome: days alive without the use of life support (i.e. invasive mechanical ventilation, circulatory support, or renal replacement therapy, including days in between intermittent renal replacement therapy) at day 28 Review outcomes: inpatient setting
Additional study outcomes: clinically important gastrointestinal bleeding, or anaphylactic reaction; days alive without life support at day 90; days alive and out of hospital at day 90 |
|
| Identification | ||
| Notes | Date of publication: 17 June 2021 Sponsor/funding: Novo Nordisk Foundation | |
Munch 2021b.
| Study characteristics | ||
| Methods |
|
|
| Participants |
|
|
| Interventions |
|
|
| Outcomes | Primary study outcome: the number of days alive without life support (invasive mechanical ventilation, circulatory support, or kidney replacement therapy) at 28 days after randomisation Review outcomes: inpatient setting
Additional study outcomes: the number of days alive without life support at 90 days, the number of days alive out of the hospital at 90 days, health‐related quality of life measured using the 5‐dimension, 5‐level European Quality of Life questionnaire and the European Quality of Life visual analogue scale, will be assessed at 180 days after randomisation |
|
| Identification | ||
| Notes | Date of publication: 21 October 2021 Sponsor/funding: Novo Nordisk Foundation | |
Ranjbar 2021.
| Study characteristics | ||
| Methods | Trial design: triple‐blind RCT Type of publication: preprint Setting: inpatient Recruitment dates: 10 August 2020 to 15 November 2020 Country: Iran Language: English Number of centres: 1 Trial registration number: IRCT20200204046369N1 Date of trial registration: 8 April 2020 |
|
| Participants | Age: mean age
Gender
Proportion of confirmed infections: PCR positivity inclusion criterion Ethnicity: not reported Number of participants (recruited/allocated/evaluated):
Severity of condition according to study definition: patients with SpO2 < 92 in room air Severity of condition according to WHO score: moderate 4 to 5 Co‐morbidities: diabetes, cardiovascular disease, hypertension, renal diseases, liver diseases Inclusion criteria
Exclusion criteria: Pregnancy
Previous treatments: not reported |
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses): 6 mg of dexamethasone IV daily for 10 days Concomitant therapy (e.g. description of standard care): no Duration of follow‐up: 28 days Treatment cross‐overs: no Compliance with assigned treatment: yes |
|
| Outcomes | Primary study outcome: all‐cause mortality in 28 days, clinical status after 5 and 10 days after enrolment with 9‐point WHO scale Review outcomes: inpatient setting
Additional study outcomes: intubation, admission to ICU, hospital death during 28 days after enrolment |
|
| Identification | ||
| Notes | Date of publication: 1 February 2021 Sponsor/funding: Shiraz University of Medical Sciences Dr. Mohsen Moghadami |
|
Taboada 2021.
| Study characteristics | ||
| Methods | Trial design: open‐label, randomised controlled trial Type of publication: journal publication Setting: inpatient Recruitment dates: 15 January to 26 May 2021 Country: Spain Language: English Number of centres: 1 Trial registration number: NCT04726098, EUCTR2020‐ 005702‐25 Date first posted: 27 January 2021 |
|
| Participants | Age: mean age
Gender:
Proportion of confirmed infections: confirmed SARS‐CoV‐2 infection by nasopharyngeal swab polymerase chain reaction was inclusion criterion Ethnicity: not stated Number of participants (recruited/allocated/evaluated)
Severity of condition according to study definition: receiving supplemental oxygen in order to maintain an oxygen saturation greater than 92% Severity of condition according to WHO score: moderate to severe ≥ 5 Co‐morbidities: hypertension, hyperlipidaemia, obesity, diabetes, chronic pulmonary disease, asthma, cardiovascular disease, history of cancer, chronic kidney disease Inclusion criteria:
Exclusion criteria:
Previous treatments (e.g. experimental drug therapies, oxygen therapy, ventilation): ACE inhibitors, antihypertensive, anticoagulants, antiplatelet, inhaled corticosteroids, statins, immunosuppressants, insulin |
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses): dexamethasone, IV, 6 mg once daily for 10 days Concomitant therapy (e.g. description of standard care): no Duration of follow‐up: 28 days Treatment cross‐overs: no Compliance with assigned treatment: yes |
|
| Outcomes | Primary study outcome: clinical worsening within 11 days since randomisation, defined as worsening of the patient's condition during treatment (need to increase fraction of inspired oxygen > 0.2, need for fraction of inspired oxygen > 0.5, respiratory rate > 25) or score higher than 4 on the 7‐point ordinal scale WHO‐CIS Review outcomes: inpatient setting
Additional study outcomes: time to recovery (defined as the first day after enrollment, on which a patient attained category 1, 2, or 3 on the 7‐point ordinal scale WHO‐CIS), clinical status of patients using the 7‐point ordinal scale WHO‐CIS at day 5, 11, 14, 28, and 60 days after randomisation, adverse drug reactions, number of patients admitted to the ICU, number of patients who needed mechanical ventilation, duration of mechanical ventilation, length of ICU and hospital stay, mortality during hospitalisation |
|
| Identification | ||
| Notes | Date of publication: 16 December 2021 Sponsor/funding: Manuel Taboada Muñiz |
|
Tang 2021.
| Study characteristics | ||
| Methods | Trial design: prospective, multicentre, single‐blind RCT Type of publication: journal publication Setting: inpatient Recruitment dates: 19 February 2020 to 31 March 2020 Country: China Language: English Number of centres: 7 Trial registration number: NCT04273321 Date of trial registration: 15 February 2020 |
|
| Participants | Age: median age
Gender
Proportion of confirmed infections: PCR positivity inclusion criterion Ethnicity: not reported Number of participants (recruited/allocated/evaluated):
Severity of condition according to study definition:
Severity of condition according to WHO score: moderate to severe 4 to 6 Co‐morbidities: COPD, asthma, hypertension, coronary heart disease, diabetes, chronic renal failure Inclusion criteria
Exclusion criteria
Previous treatments: not reported |
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses)
Concomitant therapy (e.g. description of standard care): standard therapy of COVID‐19: according to the Chinese Diagnosis and Treatment Plan for COVID‐19 (trial version 6); antivirals: 67 (77.9%) of patients, antibiotics: 61 (70.9%) of patients Duration of follow‐up: at least 14 days after randomisation or until hospital discharge Treatment cross‐overs: none documented Compliance with assigned treatment: yes |
|
| Outcomes | Primary study outcome: clinical deterioration 14 days after randomisation Review outcomes: inpatient setting
Additional study outcomes: clinical deterioration 14 days after randomisation (defined as deterioration of clinical signs and symptoms, new pulmonary or extrapulmonary lesions, progress in chest CT, ICU admission or death); clinical cure 14 days after randomisation (defined as improvement of clinical signs and symptoms of COVID‐19 and no need of additional therapy); time from randomisation to clinical cure, median (IQR), days; ICU admission |
|
| Identification | ||
| Notes | Date of publication: 22 January 2021 Sponsor/funding: Beijing Chao Yang Hospital |
|
Tomazini 2020.
| Study characteristics | ||
| Methods | Trial design: multicentre, open‐label RCT Type of publication: journal publication Setting: inpatient Recruitment dates: 17 April to 23 June 2020 Country: Brazil Language: English Number of centres: 41 Trial registration number: NCT04327401 Date of trial registration: 31 March 2020 |
|
| Participants |
|
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses):
Treatment details of control group (e.g. dose, route of administration, number of doses): standard care Concomitant therapy (e.g. description of standard care): hydroxychloroquine, azithromycin, other antibiotics, oseltamivir Duration of follow‐up: 28 days Treatment cross‐overs: no Compliance with assigned treatment
|
|
| Outcomes | Primary study outcome: number of days alive and free from mechanical ventilation for at least 48 consecutive hours Review outcomes: inpatient setting
Additional study outcomes: Sequential Organ Failure Assessment (SOFA) scores |
|
| Identification | ||
| Notes | Date of publication: 2 September 2020 Sponsor/funding: this trial was funded and supported by the Coalition COVID‐19 Brazil. The Laboratórios Farmacêuticos provided the study drug, distribution logistics, and insurance for the study patients |
|
Toroghi 2021.
| Study characteristics | ||
| Methods | Trial design: open‐label, randomised clinical trial Type of publication: journal publication Setting: inpatient Recruitment dates: 26 October 2020 to 25 January 2021 Country: Iran Language: English Number of centres: 1 Trial registration number: IRCT20100228003449N31 Date of trial registration: 8 October 2020 |
|
| Participants | Age: mean 59 years (SD 14) in the low‐dose group, mean 59 years (SD 17) in the intermediate‐dose group and mean 56 years (SD 16) in the high‐dose group Gender: 28 (59.6%) male in the low‐dose group, 21 (52.5%) male in the intermediate‐dose group, and 31 (58.6%) male in the high‐dose group Proportion of confirmed infections: PCR positivity inclusion criterion Ethnicity: not reported Number of participants (recruited/allocated/evaluated):
Severity of condition according to study definition: moderate to severe; moderate COVID‐19 was considered when clinical signs of pneumonia (fever, cough, dyspnoea, and high respiratory rate) were positive along with SpO2 between 90% and 93% on room air. Severe COVID‐19 was described as clinical signs of pneumonia plus respiratory rate > 30 breaths/min or SpO2 < 90% on room air. Severity of condition according to WHO score: moderate to severe ≥ 5 Co‐morbidities: hypertension, diabetes mellitus, ischaemic heart disease, hypothyroidism, respiratory disorders, cerebrovascular accident, dyslipidaemia, neuropsychiatric disorders, rheumatoid arthritis, Parkinson's disease, depression, malignancy, renal disorders, liver disorders, heart failure Inclusion criteria
Exclusion criteria
Previous treatments: aspirin, angiotensin receptor blockers, statin, beta blocker, metformin, azithromycin, levothyroxine, sofosbuvir‐ledipasvir, insulin, doxycycline, hydroxychloroquine, immunosuppressants, supplements, other antibiotics, angiotensinogen converting enzyme inhibitors |
|
| Interventions | 3 groups comparing different doses of dexamethasone Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses):
Concomitant therapy (e.g. description of standard care): administration of antivirals, anticoagulants, antibiotics, analgesics, fluids, electrolytes, supplemental oxygen, vitamins, minerals, nutritional supports, and stress ulcer prophylaxis Duration of follow‐up: probably 60 days Treatment cross‐overs: no Compliance with assigned treatment: yes |
|
| Outcomes | Primary study outcome: time to a clinical response that was described as improvement of at least 2 scores in the 8‐category ordinal scale of the National Institute of Health (NIH): (1) discharge, with no limitations in usual activity, (2) discharge, with some limitations in usual activity, (3) hospital admission without the requirement of supplemental oxygen, (4) hospital admission, requiring oxygen by mask or nasal cannula, (5) hospital admission requiring non‐invasive ventilation or high‐flow oxygen, (6) intubation and mechanical ventilation, (7) mechanical ventilation and additional organ support like vasopressors, renal replacement therapy (RRT) or extracorporeal membrane oxygenation (ECMO), and (8) death. Review outcomes: inpatient setting
Additional study outcomes: time to 50% decrease in serum CRP level, time to respiratory rate ≤ 20 breaths per minute, time to peripheral oxygen saturation ≥ 93%, hospital readmission, need for ICU admission, duration of hospital and ICU stay, need for mechanical ventilation |
|
| Identification | ||
| Notes | Date of publication: 27 November 2021 Sponsor/funding: the authors did not receive any funds for this work |
|
AE: adverse event; ARDS: acute respiratory distress syndrome; COPD: chronic obstructive pulmonary disease; CPK: creatine phosphokinase; CT: computed tomography; ECMO: extracorporeal membrane oxygenation; FiO2: fraction of inspired oxygen; GI: gastrointestinal; h: hours; ICU: intensive care unit; IMV: invasive mechanical ventilation; IQR: interquartile range: IV: intravenous; LDH: lactate dehydrogenase; LMIC: low‐ and middle‐income countries; NIV: non‐invasive ventilation; PaO2: partial pressure of oxygen; PEEP: positive end‐expiratory pressure; RCT: randomised controlled trial; RT‐PCR: reverse transcription polymerase chain reaction; SAE: serious adverse event; SaO2: arterial oxygen saturation; SpO2: blood oxygen saturation; SD: standard deviation; WHO: World Health Organization
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| EUCTR2020‐001445‐39‐ES | Corticosteroid plus other active substances versus standard care |
| EUCTR2020‐001616‐18‐ES | Inhaled corticosteroids |
| EUCTR2020‐001889‐10 | Inhaled corticosteroids |
| IRCT20120225009124N4 | Corticosteroid plus other active substances versus standard care |
| IRCT20190312043030N2 | Corticosteroid plus other active substances versus standard care |
| IRCT20200522047542N1 | Topical corticosteroids |
| ISRCTN86534580 | Inhaled corticosteroids |
| Moreira 2021 | The administered antibody (foralumab) was not standard care |
| Naik 2021 | The participants received low‐dose dexamethasone in addition to standard care |
| NCT04341038 | Corticosteroid plus other active substances versus standard care |
| NCT04355637 | Inhaled corticosteroids |
| NCT04359511 | Withdrawn (competitor test RECOVERY) |
| NCT04361474 | Topical corticosteroids |
| NCT04381364 | Inhaled corticosteroids |
| NCT04411667 | Corticosteroid plus other active substances versus standard care |
| NCT04416399 | Inhaled corticosteroids |
| NCT04468646 | Corticosteroid plus other active substances versus standard care |
| NCT04484493 | Topical corticosteroids |
| NCT04485429 | Withdrawn (it was not possible to perform the trial due to the availability and logistics of porcine heparin) |
| NCT04534478 | Corticosteroids for long‐COVID treatment |
| NCT04551781 | Corticosteroids for long‐COVID treatment |
| NCT04561180 | Corticosteroid plus other active substances versus standard care |
| NCT04569825 | Topical corticosteroids |
| NCT04640168 | Corticosteroid plus other active substances versus standard care |
| NCT04657484 | Corticosteroids for long‐COVID treatment |
| NCT04826822 | Corticosteroid plus other active substance versus standard care |
| NCT05133635 | Study was withdrawn because a recent study suggested a new corticosteroid regime for intensive care unit patients, so that no participants were recruited |
| Odeyemi 2021 | Compared bio‐marker adjusted corticosteroid dosing with usual care (corticosteroid use and dosing determined by the physician) |
Characteristics of studies awaiting classification [ordered by study ID]
EUCTR2020‐001307‐16‐ES.
| Methods | Trial design: open RCT Sample size: 104 Setting: inpatient Language: Spanish, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: methylprednisolone
Treatment details of control group (e.g. dose, route of administration): no information Concomitant therapy: no information |
| Outcomes | Primary study outcome: death for any cause in the first 28 days after randomisation |
| Notes | Recruitment status: prematurely ended Prospective completion date: 6‐month duration Date last update was posted: unclear Sponsor/funding: Fundación para la Investigación Biomédica Hospital Ramón y Cajal |
EUCTR2020‐001333‐13‐FR.
| Methods | Trial design: open RCT Sample size: 122 Setting: inpatient Language: French, English Number of centres: 18 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Concomitant therapy: no information |
| Outcomes | Primary study outcome: mortality on day 28 |
| Notes | Recruitment status: prematurely ended Date of the global end of the trial: 7 August 2020 Date last update was posted: unclear Sponsor/funding: Groupe Hospitalier Paris Saint‐Joseph |
EUCTR2020‐001553‐48‐FR.
| Methods | Trial design: open RCT Sample size: 304 Setting: inpatient Language: French Number of centres: 17 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): standard care Concomitant therapy: no information |
| Outcomes | Primary study outcome
|
| Notes | Recruitment status: prematurely ended Prospective completion date: 7 months predicted Date last update was posted: unclear Sponsor/funding: Hospices Civils de Lyon |
EUCTR2020‐002186‐34‐ES.
| Methods | Trial design: open‐label, randomised trial Sample size: 100 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: methylprednisolone
Treatment details of control group (e.g. dose, route of administration): standard care Concomitant therapy: no |
| Outcomes | Primary outcome: incidence of a combined variable made up of the variables death, ICU admission, non‐IMV, or need for high‐flow oxygen therapy (defined as SaFi < 200 with FiO2 ≥ 50%) (day 90) |
| Notes | Recruitment status: prematurely ended Prospective completion date: estimated duration 1 year Date last update was posted: no information Sponsor/funding: Fundació Hospital Universitari Vall d'Hebron ‐ Institut de Recerca (VHIR) |
EUCTR2020‐004323‐16.
| Methods | Trial design: randomised, multicentre, double‐blind study Sample size: 260 Setting: inpatient Language: Italian, English Number of centres: 5 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): placebo, IV Concomitant therapy: no information |
| Outcomes | Primary study outcome: length of hospitalisation, calculated as the interval between randomisation and discharge from the hospital without the need for supplemental oxygen |
| Notes | Recruitment status: completed Prospective completion date: 4‐month trial duration planned Date last update was posted: 25 November 2020 Sponsor/funding: Azienda Ospedaliera Arcispedale Santa Maria Nuova/IRCCS Di Reggio Emilia |
Gautam 2021.
| Methods | Trial design: randomised controlled trial Type of publication: journal publication Setting: inpatient Recruitment dates: 15 April to 15 June 2021 Country: India Language: English Number of centres: 1 Trial registration number: not stated Date first posted: not stated |
| Participants | Age: mean age
Gender:
Proportion of confirmed infections: PCR positivity inclusion criterion Ethnicity: not stated Number of participants (recruited/allocated/evaluated)
Severity of condition according to study definition: moderate‐to‐severe COVID‐19 cases according to definition, patients having oxygen saturation < 93% on room air Severity of condition according to WHO score: moderate to severe ≥ 5 Co‐morbidities: diabetes mellitus, chronic kidney disease, hypertension, chronic obstructive pulmonary disease, hypothyroidism, heart disease, obesity, malignancy Inclusion criteria:
Exclusion criteria:
Previous treatments (e.g. experimental drug therapies, oxygen therapy, ventilation): not stated |
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses): dexamethasone, 8 mg/day intravenously daily in divided dose up to 10 days Concomitant therapy (e.g. description of standard care): patients were given oxygen by nasal cannula, face mask, and non‐rebreathing mask Duration of follow‐up: day 0, 5, 10 Treatment cross‐overs: no Compliance with assigned treatment: yes |
| Outcomes | Primary study outcome: not stated Additional study outcomes: all‐cause mortality, hospital‐acquired infections, radiological improvement, transfer to intensive care unit, hyperglycaemic coma, clinical improvement |
| Notes | Date of publication: 1 December 2021 Sponsor/funding: none |
Ghanei 2021.
| Methods |
|
| Participants |
|
| Interventions |
|
| Outcomes | Primary study outcome: number of admissions to intensive care unit Additional study outcomes: all‐cause mortality, the length of hospital stay (LOS), death during admission, intubation in ICU, and time to clinical recovery. Clinical recovery was defined as being medically stable and ready for discharge from the hospital, determined by the attending physician |
| Notes | Date of publication: 15 September 2021 Sponsor/funding: not applicable |
IRCT20081027001411N3.
| Methods | Trial design: single‐blinded RCT Sample size: 60 Setting: inpatient Language: English Number of centres: 4 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): control group receives standard treatment for COVID‐19 disease Concomitant therapy: not stated |
| Outcomes | Primary study outcome
|
| Notes | Recruitment status: completed Prospective completion date: 30 June 2020 Date last update was posted: 1 June 2020 Sponsor/funding: Teheran University of Medical Sciences |
IRCT20120215009014N354.
| Methods | Trial design: double‐blind, phase II RCT Sample size: 81 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention group 1
Details of intervention group 2
Details of intervention group 3
Treatment details of control group (e.g. dose, route of administration): Concomitant therapy: routine care |
| Outcomes | Primary study outcome
|
| Notes | Recruitment status: completed Prospective completion date: 5 August 2020 Date last update was posted: 1 May 2020 Sponsor/funding: Hamedan University of Medical Sciences |
IRCT20160118026097N4.
| Methods | Trial design: unblinded, RCT Sample size: 60 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): treatment according to Ministry of Health's protocol Concomitant therapy: no information |
| Outcomes | Primary study outcome: mortality rate or recovery within 30 days after hospitalisation |
| Notes | Recruitment status: completed Prospective completion date: no information Date last update was posted: 13 September 2020 Sponsor/funding: Ghoum University of Medical Sciences |
IRCT20200611047727N3.
| Methods | Trial design: single‐blinded, RCT Sample size: 60 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): standard care Concomitant therapy: no |
| Outcomes | Primary study outcome: radiological changes (before the intervention and 6 weeks later) |
| Notes | Recruitment status: completed Prospective completion date: no information Date last update was posted: 3 January 2021 Sponsor/funding: Shahid Beheshti University of Medical Sciences |
IRCT20201015049030N1.
| Methods | Trial design: single‐blind, RCT Sample size: 200 Setting: outpatient Language: English Number of centres: 4 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): standard care Concomitant therapy: no |
| Outcomes | Primary study outcome
|
| Notes | Recruitment status: completed Prospective completion date: no information Date last update was posted: 7 November 2020 Sponsor/funding: Teheran University of Medical Sciences |
ISRCTN33037282.
| Methods | Trial design: open‐label, RCT Sample size: 680 Setting: inpatient Language: English Number of centres: 3 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: per‐protocol methylprednisolone administration and tapering
Treatment details of control group: per‐protocol dexamethasone administration
Concomitant therapy: no |
| Outcomes | Primary study outcome
|
| Notes | Recruitment status: completed Prospective completion date: 30 April 2021 Date last update was posted: 19 November 2020 Sponsor/funding: Clínica Medellín ‐ Grupo Quirónsalud |
Montalvan 2021.
| Methods | Trial design: single‐centre, randomised, non‐blinded control trial pilot study Type of publication: abstract only Setting: hospitalised participants Recruitment dates: 81 randomised (40 low‐dose, 41 high‐dose dexamethasone) Country: Honduras Language: English Number of centres: single‐centre Trial registration number: not reported Date first posted: October 2021 |
| Participants | Age: (mean ± SD) of 56.9 ± 14.9 and 57.5 ± 16.5 for low and high‐dose dexamethasone respectively Gender: low‐dose n = 17 (42.5%) male and n = 23 (57.5%) female vs the high‐dose n = 29(70.7%) male and n = 12(29.3%) female Proportion of confirmed infections: not reported Ethnicity: not reported Number of participants (recruited/allocated/evaluated): not reported/81/81 (40 low‐dose, 41 high‐dose dexamethasone) Severity of condition according to study definition: not reported Severity of condition according to WHO score: not reported Co‐morbidities: not reported Inclusion criteria: not reported Exclusion criteria: not reported Previous treatments (e.g. experimental drug therapies, oxygen therapy, ventilation): not reported |
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses): dexamethasone 6 mg /day Concomitant therapy (e.g. description of standard care): not reported Duration of follow‐up: not reported Treatment cross‐overs: not reported Compliance with assigned treatment: not reported |
| Outcomes | Primary study outcome: reduction in mortality and intubation Additional study outcomes: hospital‐acquired infections, risk of becoming critically ill and requiring intubation |
| Notes | Date of publication: October 2021 Sponsor/funding: not reported |
NCT04244591.
| Methods | Trial design: randomised, open‐label Sample size: 80 Setting: inpatient Language: English Number of centres: multicentre Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria:
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): standard care Concomitant therapy: no information |
| Outcomes | Primary study outcome
|
| Notes | Recruitment status: completed Prospective completion date: 13 April 2020 Date last update was posted: 13 April 2020 Sponsor/funding: Peking Union Medical College Hospital |
NCT04325061.
| Methods | Trial design: open‐label RCT Sample size: 19 Setting: inpatient Language: English Number of centres: multicentre Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): patients will be treated with standard intensive care Concomitant therapy: no information |
| Outcomes | Primary study outcome: all‐cause mortality at 60 days after enrolment |
| Notes | Recruitment status: terminated (lack of enrolment) Prospective completion date: June 2020 Date last update was posted: February 2021 Sponsor/funding: Dr. Negrin University Hospital |
NCT04347980.
| Methods | Trial design: single‐blinded (participants) RCT Sample size: 122 Setting: inpatient Language: French, English Number of centres: multicentre, no concrete information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): 200 mg x 3/d enterally from J1 of the hydroxychloroquine for 10 days. If the patient is extubated before the 10th day, he will receive his last dose of hydroxychloroquine before. Concomitant therapy: no information |
| Outcomes | Primary study outcome: day 28 mortality |
| Notes | Recruitment status: terminated (ANSM (Agence nationale de sécurité du médicament et des produits de santé) Recommendation) Prospective completion date: August 2020 Date last update was posted: 17 April 2020 Sponsor/funding: Centre Chirurgical Marie Lannelongue |
NCT04438980.
| Methods | Trial design: double‐blinded RCT Sample size: 72 Setting: inpatient Language: Spanish, English Number of centres: 2 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
|
| Outcomes | Primary outcome
|
| Notes | Recruitment status: completed Prospective completion date: February 2021 Date last update was posted: 22 July 2020 Sponsor/funding: Fundacion Miguel Servet |
NCT04451174.
| Methods |
|
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): no intervention Concomitant therapy: no information |
| Outcomes | Primary outcome
|
| Notes | Recruitment status: terminated (corticosteroid use approval) Prospective completion date: 3 December 2020 Date last update was posted: 20 October 2020 Sponsor/funding: University of Chile |
NCT04530409.
| Methods | Trial design: open‐label RCT Sample size: 450 Setting: no information Language: Arabic, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): dexamethasone is to be used upon the deterioration of cases Concomitant therapy: no information |
| Outcomes | Primary outcome
|
| Notes | Recruitment status: completed Prospective completion date: estimated primary completion date 1 April 2021 Estimated study completion date: 1 May 2021 Date last update was posted: 16 February 2021 Sponsor/funding: ClinAmygate |
NCT04746430.
| Methods | Trial design: open‐label RCT Sample size: 2000 Setting: outpatient Language: Dutch, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): only remote monitoring Concomitant therapy: no information |
| Outcomes | Primary outcome: time to first hospital admission or death (time frame: 28 days) |
| Notes | Recruitment status: terminated (too few patients) Prospective completion date: March 2022 Date last update was posted: 5 April 2021 Sponsor/funding: General Practitioners Research Institute |
Rashad 2021.
| Methods |
|
| Participants |
|
| Interventions |
|
| Outcomes | Primary study outcome: time to failure, defined as death, within 14 days from ICU admission Additional study outcomes: all‐cause mortality, hospital‐acquired infections |
| Notes |
|
Salukhov 2021.
| Methods | Trial design: probably randomised controlled trial (uncertainties regarding the randomisation process) Sample size: 40 Setting: inpatient Language: Russian Number of centres: 1 Trial registration number: not stated Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Treatment details of intervention group (e.g. dose, route of administration, number of doses)
Treatment details of control group (e.g. dose, route of administration, number of doses): standard care Concomitant therapy (e.g. description of standard care): no |
| Outcomes | Primary study outcome: composite score of: COVID‐19 progression to extreme severity, a decrease in SpO2 ≤ 93% and the need for oxygen therapy, occurrence of pulmonary and extrapulmonary complications requiring transfer to ICU, and death |
| Notes | Date of publication: 2021 Sponsor/funding: not stated |
ALT: alanine transaminase; ARDS: acute respiratory distress syndrome; COPD: chronic obstructive pulmonary disease; CPAP: continuous positive airway pressure; CPK: creatine phosphokinase; CRP: C‐reactive protein; CT: computed tomography; d: days; FiO2: fraction of inspired oxygen; h: hours; HFNC: high‐flow nasal cannula; ICU: intensive care unit; IMV: invasive mechanical ventilation; IQR: interquartile range: IV: intravenous; LDH: lactate dehydrogenase; NPPV: non‐invasive positive pressure ventilation; PaO2: partial pressure of oxygen; PEEP: positive end‐expiratory pressure; RCT: randomised controlled trial; RT‐PCR: reverse transcription polymerase chain reaction; SD: standard deviation; SpO2: blood oxygen saturation
Characteristics of ongoing studies [ordered by study ID]
ACTRN12621001200875.
| Study name | A randomised controlled trial of dexamethasone for emergency and life‐threatening admissions due to COVID‐19 in virtual care: the DELTA study |
| Methods | Trial design: triple‐blind, randomised controlled trial Sample size: 650 Setting: outpatient Language: English Number of centres: not stated Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Details of intervention: dexamethasone plus usual care
Treatment details of control group (e.g. dose, route of administration): probably placebo (not explicitly explained) Concomitant therapy: not stated |
| Outcomes | Primary study outcome: COVID‐19 related hospitalisation, defined as COVID‐19 related emergency presentation (excluding injuries and presentations for social reasons), or hospital admission or intensive care unit admission or death |
| Starting date | 20 September 2021 |
| Contact information | Prof Michael Dinh Royal Prince Alfred Hospital Level 10, King George V Building, Camperdown, New South Wales 2050 Australia Telephone: +61 419620654 Email: Michael.Dinh@health.nsw.gov.au |
| Notes | Recruitment status: recruiting Prospective completion date: not stated Date last update was posted: 10 December 2021 Sponsor/funding: Royal Prince Alfred Hospital |
ACTRN12621001603808.
| Study name | The effect of prednisolone vs dexamethasone on Covid‐19 in pregnancy: an open labelled randomised control trial |
| Methods | Trial design: open‐label, randomised controlled trial Sample size: 192 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria: women aged 18 to 50 years, pregnant > 16 weeks with COVID‐19, hospitalised with an oxygen requirement
Co‐morbidities are included, not limited to obesity, hypertension, diabetes, pre‐existing illnesses Exclusion criteria: pregnancy < 16 weeks gestation, not requiring oxygen, contraindications to receiving corticosteroids |
| Interventions | Details of intervention: prednisolone
Treatment details of control group (e.g. dose, route of administration): dexamethasone, dose and route of administration not explicitly explained Concomitant therapy: not stated |
| Outcomes | Primary study outcome: WHO ordinal scale of clinical improvement compared at day 5 and at day 10 |
| Starting date | 1 December 2021 |
| Contact information | Dr Carole‐Anne Whigham, Monash Health 246 Clayton Road Clayton 3168 Vic, Australia Phone: +61 404644029 Email: carole‐anne.whigham@monashhealth.org |
| Notes | Recruitment status: not yet recruiting Prospective completion date: not stated Date last update was posted: 24 November 2021 Sponsor/funding: Monash Health Hospital Victoria, Australia |
ChiCTR2000029386.
| Study name | Effectiveness of glucocorticoid therapy in patients with severe coronavirus disease 2019: protocol of a randomised controlled trial |
| Methods | Trial design: open‐label RCT Sample size: 48 Setting: inpatient Language: Chinese, English Number of centres: single‐centre Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): no glucocorticoid use Concomitant therapy: no information |
| Outcomes | Primary study outcome
|
| Starting date | No information |
| Contact information | Dr. Yao‐Kai Chen, Division of Infectious Diseases, Chongqing Public Health Medical Center, Chongqing 400036, China E‐Mail: yaokaichen@hotmail.com |
| Notes | Recruitment status: recruiting Prospective completion date: unclear Date last update was posted: 5 May 2020 Sponsor/funding: Chongqing Special Research Project for Prevention and Control of Novel Coronavirus Pneumonia |
ChiCTR2000029656.
| Study name | A randomised, open‐label study to evaluate the efficacy and safety of low‐dose corticosteroids in hospitalised patients with novel coronavirus pneumonia (COVID‐19) |
| Methods | Trial design: randomised, open‐label Sample size: 100 Setting: inpatient Language: Chinese, English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): standard treatment Concomitant therapy: no information |
| Outcomes | Primary study outcome
|
| Starting date | 14 February 2020 |
| Contact information | Ronghui Du: +86 15337110926 Email: bluesearh006@sina.com |
| Notes | Recruitment status: not yet recruiting Prospective completion date: 14 April 2020 Date last update was posted: 12 February 2020 Sponsor/funding: Wuhan Pulmonary Hospital |
ChiCTR2000030481.
| Study name | The clinical value of corticosteroid therapy timing in the treatment of novel coronavirus pneumonia (COVID‐19): a prospective randomised controlled trial |
| Methods |
|
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): no corticosteroid Concomitant therapy: no information |
| Outcomes | Primary study outcome: the time of duration of COVID‐19 nucleic acid RT‐PCR test results of respiratory specimens (such as throat swabs) or blood specimens change to negative Among secondary outcomes: 21‐day all‐cause mortality |
| Starting date | 1 March 2020 |
| Contact information | Chen Zhenshun: +86 13627288300 Email: chzs1990@163.com |
| Notes | Recruitment status: recruiting Prospective completion date: 30 April 2020 Date last update was posted: 3 March 2020 Sponsor/funding: Science and Technology Department of Hubei Province |
CTRI/2020/07/026608.
| Study name | A clinical trial to study the effects of two drugs methylprednisolone and dexamethasone in patients with severe COVID‐19 |
| Methods | Trial design: randomised, parallel‐group trial Sample size: 40 Setting: inpatient Language: English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): injection dexamethasone 6 mg IV once a day for 3 days Concomitant therapy: no information |
| Outcomes | Primary study outcome
|
| Starting date | 27 July 2020 |
| Contact information | Prof V R Mohan Rao, India: 9841210011 Email: medicinehod@chettinadhealthcity.com |
| Notes | Recruitment status: not yet recruiting Prospective completion date: estimated duration of trial 3 months Date last update was posted: 15 July 2020 Sponsor/funding: Chettinad Hospital and Research Institute Kelambakkam, Dr Ananthakumar PK |
CTRI/2020/12/029894.
| Study name | Comparing the effectiveness of dexamethasone versus methylprednisolone in patients with moderate COVID 19 ‐ a randomised controlled trial |
| Methods | Trial design: open‐label, RCT Sample size: 50 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: dexamethasone
Treatment details of control group (e.g. dose, route of administration): methylprednisolone 32 mg/60 mg intravenous, 6 days Concomitant therapy: no |
| Outcomes | Primary outcome: mortality during hospital stay (day 1 to day 7) |
| Starting date | No information |
| Contact information | DR R Nivetha, Department of General Medicine 1st floor SRM Medical College Hospital and Research Centre SRM University Potheri Kattankulathur, India Email: nivethamdr@gmail.com |
| Notes | Recruitment status: not yet recruiting Prospective completion date: estimated duration 6 months Date last update was posted: no information Sponsor/funding: SRM Medical College Hospital and Research Centre |
CTRI/2020/12/030143.
| Study name | Evaluation of different steroid regimes in critically ill adult patients of COVID‐19 admitted to intensive care units |
| Methods | Trial design: randomised controlled trial Sample size: 500 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: dexamethasone
Treatment details of control group (e.g. dose, route of administration): methylprednisolone, 1 to 2 mg/kg body weight, IV, frequency: daily for 10 days Concomitant therapy: no |
| Outcomes | Primary outcome: 28‐day mortality |
| Starting date | No information |
| Contact information | Dr Sukhyanti Kerai, Maulana Azad Medical College New Delhi, India Email: drsukhi25@gmail.com |
| Notes | Recruitment status: not yet recruiting Prospective completion date: estimated duration 6 months Date last update was posted: no information Sponsor/funding: Maulana Azad Medical College and associated Lok Nayak Hospital |
CTRI/2021/05/033873.
| Study name | Pre‐emptive steroids to alter the disease course in COVID‐19 patients |
| Methods | Trial design: open‐label, randomised controlled trial Sample size: 500 Setting: outpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Details of intervention: methylprednisolone plus standard care
Treatment details of control group (e.g. dose, route of administration): standard care Concomitant therapy: not stated |
| Outcomes | Primary study outcome: number of patients requiring hospitalisation, supplemental oxygen and/or ICU care as compared to standard of care protocol (time points: baseline, 7 days, 14 days and, if applicable, ICU status/hospitalisation time) |
| Starting date | 2 May 2022 |
| Contact information | Prakhar Gupta, JK Hospital and LN Medical College, Department of Medicine, Third floor JK Hospital and LN Medical college, Bhopal MADHYA PRADESH 462042, India Email: itsme.prakhar@gmail.com |
| Notes | Recruitment status: not yet recruiting Prospective completion date: not stated Date last update was posted: 28 May 2021 Sponsor/funding: JK Hospital and LN Medical College |
CTRI/2021/08/035822.
| Study name | Assessment of doubling dose of dexamethasone in progressively worsening severe COVID‐19 pneumonia ‐ a randomised controlled trial |
| Methods | Trial design: open‐label, randomised controlled trial Sample size: 120 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria: patients aged 18 to 99 years, hospitalised, confirmed SARS‐CoV‐2 infection by nucleic acid based testing (RT‐PCR, CB‐NAAT, or TrueNAT) or antigen testing, severe COVID‐19 pneumonia (SpO2 < 94%; PaO2/FiO2 < 300 mm Hg or respiratory rate (RR) > 30 breaths/min) with lack of response to dexamethasone 6 mg after 48 hours (defined as similar or worsening oxygen requirement (margin of error is 5% Fio2 for high flow nasal cannula, 2 L/min for NRBM, and 1 L/min for low flow oxygen devices)) Exclusion criteria: patient already on corticosteroid therapy for an unrelated indication; patient with impending death or respiratory failure necessitating ICU care within 24 hours including inability to maintain SpO2 ≥ 90% despite HFNC with flow 60 L/min and FiO2 1.0 or, if available, NIV with PEEP of up to 8 cm H2O and FiO2 1.0; patients who have received ≥ 2 day of steroids outside hospital care or within the hospital outside of wards that are involved in the study. These doses must be no greater than 12 mg dexamethasone or 64 mg methylprednisolone cumulatively; patients with a known contraindication to corticosteroids including untreated bacterial sepsis, diabetic keto‐acidosis, and invasive fungal infections such as mucormycosis; medical history that might, in the opinion of the attending clinician, put the patient at significant risk if he/she were to participate in the trial; pregnancy; recruitment in another therapeutic trial; use of immunosuppressive drugs, cytotoxic chemotherapy in the past 21 days; neutropenia due to haematological or solid malignancies with bone marrow invasion; refusal of consent. |
| Interventions | Details of intervention: dexamethasone
Treatment details of control group (e.g. dose, route of administration): dexamethasone, 6 mg, once daily, through intravenous or oral route, for 10 days or till discharge, whichever is earlier Concomitant therapy: not stated |
| Outcomes | Primary study outcome: supplemental oxygen‐free days at day 28 from hospitalisation, proportion of patients requiring non‐invasive ventilation by NIV mask or invasive mechanical ventilation |
| Starting date | 1 September 2021 |
| Contact information | Animesh Ray, All India Institute of Medical Sciences, New Delhi, Room no. 3070A, Department of Medicine, 3rd floor teaching block, All India Institute of Medical Sciences, New Delhi‐110029 South West DELHI 110029, India Phone: 01126593963 Email: doctoranimeshray@gmail.com |
| Notes | Recruitment status: not yet recruiting Prospective completion date: not stated Date last update was posted: 16 August 2021 Sponsor/funding: All India Institute of Medical Sciences, New Delhi |
EUCTR2020‐001413‐20‐ES.
| Study name | Efficacy and safety of siltuximab vs. corticosteroids in hospitalised patients with COVID‐19 pneumonia |
| Methods | Trial design: phase 2, randomised, open‐label Sample size: 100 Setting: inpatient Language: Spanish, English Number of centres: single‐centre Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: siltuximab
Treatment details of control group (e.g. dose, route of administration): methylprednisolone 250 mg/kg Concomitant therapy: no information |
| Outcomes | Primary study outcome: proportion of patients requiring ICU admission at any time within the study period (time frame 29 days) |
| Starting date | No information |
| Contact information | Felipe García: +349322754002884 Email: fgarcia@clinic.cat |
| Notes | Recruitment status: temporarily halted Prospective completion date: prospective duration of trial 45 days Date last update was posted: no information Sponsor/funding: Fundació Clínic per a la Recerca Biomèdica |
EUCTR2020‐001457‐43‐FR.
| Study name | Dexamethasone and oxygen support strategies in ICU patients with COVID‐19 pneumonia |
| Methods | Trial design: double‐blind (phase III) RCT Sample size: 550 Setting: inpatient Language: French, English Number of centres: 12 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
For patients without mechanical ventilation other exclusion criteria are:
|
| Interventions | Details of intervention: dexamethasone
Treatment details of control group (e.g. dose, route of administration): placebo, IV Concomitant therapy: no information |
| Outcomes | Primary study outcome
|
| Starting date | No information |
| Contact information | Email: fadila.amerali@aphp.fr |
| Notes | Recruitment status: ongoing Prospective completion date: October 2020 Date last update was posted: 2 April 2020 Sponsor/funding: APHP (An ancillary study CACAO (Covidicus air contamination) will be performed in 4 centres aiming at assessing the environmental contamination by SARS‐CoV‐2 according to the oxygen support modality. Additional funding will be searched for these analyses (submitted for ANR call)) |
EUCTR2020‐001622‐64‐ES.
| Study name | Outpatient treatment of COVID‐19 with early pulmonary corticosteroids as an opportunity to modify the course of the disease (TAC‐COVID‐19) |
| Methods | Trial design: open (phase IV) RCT Sample size: 200 Setting: outpatient Language: Spanish, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: prednisone
Treatment details of control group (e.g. dose, route of administration): concomitant therapy Concomitant therapy: symptomatic treatment + hydroxychloroquine + azithromycin |
| Outcomes | Primary study outcome: the aim of this study is to explore the effectiveness and safety of oral corticosteroids (prednisone) in the treatment of early stage SARS‐Cov‐2 pneumonia in patients who do not yet meet hospital admission criteria: admission after 30 days |
| Starting date | 19 April 2020 |
| Contact information | María Jesús Coma: 0034610620180 Email: mjcoma@hubu.es |
| Notes | Recruitment status: ongoing Prospective completion date: 3‐month estimated duration of trial Date last update was posted: 20 April 2020 Sponsor/funding: Dra Ana Pueyo Bastida, Hospital Universitario de Burgos |
EUCTR2020‐001707‐16‐ES.
| Study name | Outpatient treatment of COVID‐19 with early pulmonary corticosteroids as an opportunity to modify the course of the disease (TOCICOVID) |
| Methods |
|
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: tocilizumab
Treatment details of control group (e.g. dose, route of administration): methylprednisolone, 331 mg, IV Concomitant therapy: no information |
| Outcomes | Primary study outcome: respiratory situation at 24 hours, 3 and 7 days based on PaO2/FiO2 ratio that graduates respiratory distress from mild (200 to 300), moderate (100 to 200) and severe (< 100). In addition, it will include: presence of dyspnoea and grade according to the New York Health Association (NYHA) scale, presence of respiratory work and respiratory rate (FR) |
| Starting date | 22 July 2020 |
| Contact information | IIS BIODONOSTIA 943006288 |
| Notes | Recruitment status: ongoing Prospective completion date: 20‐month estimated duration of trial Date last update was posted: 20 April 2020 Sponsor/funding: IIS BIODONOSTIA |
EUCTR2020‐001921‐30.
| Study name | Steroids and unfractionated heparin in critically‐ill patients with pneumonia from COVID‐19 infection. A multicenter, interventional, randomised, three arms study design |
| Methods | Trial design: open RCT Sample size: 200 Setting: inpatient Language: Italian, English Number of centres: 9 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention: methylprednisolone + unfractionated heparin (Eparina)
Treatment details of control group (e.g. dose, route of administration): heparin subcutaneous (25,000 international units) Concomitant therapy: no information |
| Outcomes | Primary study outcome: all‐cause mortality at day 28 |
| Starting date | 14 May 2020 |
| Contact information | Clinical Trials Quality Team: 0594225868 Email: mighali.pasquale@aou.mo.it |
| Notes | Recruitment status: ongoing Prospective completion date: 1 year later, so May 2021 Date last update was posted: 26 June 2020 Sponsor/funding: AZIENDA OSPEDALIERO‐UNIVERSITARIA POLICLINICO DI MODENA |
EUCTR2020‐003363‐25‐DK.
| Study name | Higher vs. lower doses of dexamethasone in patients with COVID‐19 and severe hypoxia: the COVID STEROID 2 trial |
| Methods | Trial design: double‐blinded RCT Sample size: 1000 Setting: inpatient Language: English Number of centres: 36 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): dexamethasone 6 mg, IV Concomitant therapy: no information |
| Outcomes | Primary study outcome: days alive without life support (i.e. IMV, circulatory support or renal replacement therapy) from randomisation to day 28 |
| Starting date | 18 August 2020 |
| Contact information | Department of Intensive Care, Rigshospitalet: +4535457237 Email: covid‐steroid@cric.nu |
| Notes | Recruitment status: ongoing Prospective completion date: 18‐month duration planned Date last update was posted: 18 August 2020 Sponsor/funding: Department of Intensive Care, Rigshospitalet, Novo Nordisk Foundation |
EUCTR2020‐006054‐43‐IT.
| Study name | Randomised controlled trial of methylprednisolone versus dexamethasone in COVID‐19 pneumonia ‐ methylprednisolone vs dexamethasone in COVID‐19 |
| Methods | Trial design: open‐label, randomised controlled trial Sample size: 680 Setting: inpatient Language: English Number of centres: not stated Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Details of intervention: methylprednisolone
Treatment details of control group (e.g. dose, route of administration): dexamethasone, 8 mg, IV Concomitant therapy: not stated |
| Outcomes | Primary study outcome: survival proportion at 28 days in both arms |
| Starting date | 3 March 2021 |
| Contact information | Università degli Studi di Trieste, Strada di Fiume, 447 Trieste 34129, Italy Email: mconfalonieri@units.it |
| Notes | Recruitment status: ongoing Prospective completion date: not stated Date last update was posted: 26 July 2021 Sponsor/funding: Università degli Studi di Trieste |
EUCTR2021‐001416‐29‐ES.
| Study name | Early treatment strategy with high‐dose versus standard‐dose dexamethasone in patients with SARS‐CoV‐2 pneumonia (COVID‐19) |
| Methods | Trial design: open‐label, randomised controlled trial Sample size: 200 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria: patients admitted with SARS‐CoV‐2 pneumonia (COVID‐19) confirmed by antigenic test or PCR, age = 18 years, presents with a PCR = 66 mg/L and = 150 mg/L at inclusion or pandemic score at admission > 200 with PCR 9.7 to 149 mg/L at inclusion, WHO scale level 4, with need for oxygen therapy in NG = 1 lpm to maintain saturation = 94%, onset of symptoms = 10 days before the date of inclusion Exclusion criteria: patients with criteria of respiratory distress at the time of randomisation, understood as need for OCNAF/NIMV/MIV (levels 5 and 6 of the WHO scale) or O2 saturation = 92% and/or RF = 30 despite oxygen in NG at 4 litres, patients with allergy or contraindication to the use of systemic corticosteroids, patients with severe asthma or chronic lung disease with home oxygen requirements and active corticosteroid therapy, patients on chronic corticosteroid therapy, use of corticosteroids daily in the 15 days prior to hospital admission, indication for steroid use due to other clinical conditions of the patient (e.g. septic shock), pregnant or actively breastfeeding women, patients with suspected or confirmed bacterial, fungal, or viral infection other than SARS‐CoV‐2 itself at time of randomisation, patients with confirmed past or latent tuberculosis infection prior to inclusion, patients with known HIV infection with CD4 below 500 cells/mm3 or on active treatment with protease inhibitors or boosters such as cobicistat or ritonavir, patients with active oncological processes in the last year or on active treatment with chemotherapy, patients with life expectancy < 3 months at inclusion due to clinical conditions other than SARS‐CoV‐2 pneumonia, patients expected to die within 48 to 72 hours, patients included in another clinical trial |
| Interventions | Details of intervention: dexamethasone
Treatment details of control group (e.g. dose, route of administration): dexamethasone, IV, 4 mg Concomitant therapy: not stated |
| Outcomes | Primary study outcome: requirement of respiratory therapy with NIV/MIV/OCNAF, need for respiratory support with NIMV/MIV/OCNAF, days of hospitalisation counted from signature of informed consent to time of discharge from hospital |
| Starting date | 31 August 2021 |
| Contact information | Ángel Pueyo, Calle Puerto de Lumbreras, 5 28031 Madrid Spain, Fundación para la Investigación e Innovación Biomédica (FIIB) del Hospital Universitario Infanta Leonor Telephone: +34911919855 Email: pueyo.angel@investiganet.es |
| Notes | Recruitment status: ongoing Prospective completion date: not stated Date last update was posted: 7 September 2021 Sponsor/funding: Fundación para la Investigación e Innovación Biomédica (FIIB) del Hospital Universitario Infanta Leonor y Hospital Unive |
EUCTR2021‐004021‐71.
| Study name | Corticosteroids for COVID‐19 induced loss of smell – COCOS trial |
| Methods | Trial design: double‐blind, randomised controlled trial Sample size: 116 Setting: outpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria: recent COVID‐19 infection (< 3 months), confirmed with a positive test (PCR of antigen by GGD), persistent loss of smell after one month, objectified by TDI < 30.5 on Sniffin’ Stick test, age 18 years or older, capable of giving informed consent, good understanding of the Dutch language Exclusion criteria: pre‐existing olfactory disorders, chronic rhinitis or rhinosinusitis (with or without nasal polyps), corticosteroids (nasal, oral or intravenously) since positive test, pregnancy, contra‐indications of steroid use (Insulin dependent diabetes mellitus, Ulcus pepticum) |
| Interventions | Details of intervention: prednisolone
Treatment details of control group (e.g. dose, route of administration): placebo, oral (capsule) Concomitant therapy: not stated |
| Outcomes | Primary study outcome: objective olfactory function means of Sniffin’ Sticks, combining olfactory detection threshold (T), discrimination (D) and identification (I) ability into a composite TDI score (ranging from 1 to 48 points) that can be categorised into normosmia, hyposmia and anosmia, clinical improvement is set at > 5.5 points |
| Starting date | Not stated |
| Contact information | University Medical Center Utrecht, Otorhinolaryngology Department, Heidelberglaan 100, Utrecht, 3584 CX, Netherlands Telephone number: +310887555555 |
| Notes | Recruitment status: ongoing Prospective completion date: not stated Date last update was posted: not stated Sponsor/funding: University Medical Center Utrecht |
IRCT20190606043826N2.
| Study name | Comparison of the effectiveness and complication of dexamethasone at doses of 8 and 24 mg in the treatment of in hospitalised patients with Covid‐19 |
| Methods | Trial design: double‐blind, randomised controlled trial Sample size: 60 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria: hospitalised patients with COVID‐19 Exclusion criteria: pregnancy, immunodeficiency diseases, chronic liver and kidney diseases, or gastrointestinal bleeding, glucocorticoid use in the last month |
| Interventions | Details of intervention: dexamethasone
Treatment details of control group (e.g. dose, route of administration): dexamethasone, 8 mg daily, IV Concomitant therapy: not stated |
| Outcomes | Primary study outcome: determination of mean arterial blood oxygen saturation with and without oxygen therapy (at the beginning of hospitalisation and 3, 5, 7, and 10 days later), shortness of breath score based on modified Borg scale (at the beginning of hospitalisation and 3, 5, 7, and 10 days later), number of days required for mechanical ventilation, measurement of serum levels of C‐reactive protein (at the beginning of hospitalisation and 3, 5, 7, and 10 days later) |
| Starting date | 6 July 2021 |
| Contact information | Marzieh Mollaei Ardestani Phone: +98 31 5558 0931 Email: mollaei‐m@kaums.ac.ir |
| Notes | Recruitment status: recruitment completed Prospective completion date: not stated Date last update was posted: July 1, 2021 Sponsor/funding: Esfahan University of Medical Sciences |
NCT04329650.
| Study name | Efficacy and safety of siltuximab vs. corticosteroids in hospitalised patients with COVID‐19 pneumonia |
| Methods | Trial design: phase 2, randomised, open‐label Sample size: 200 Setting: inpatient Language: Spanish, English Number of centres: 4 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration)
Concomitant therapy: no information |
| Outcomes | Primary study outcome: proportion of patients requiring ICU admission at any time within the study period (time frame: 29 days) |
| Starting date | |
| Contact information | Contact: Felipe García, MD+34932275400 ext 2884 Email: fgarcia@clinic.ca |
| Notes | Recruitment status: recruiting Prospective completion date: 20 May 2020 Date last update was posted: 17 April 2020 Sponsor/funding: Judit Pich Martínez |
NCT04344730.
| Study name | Dexamethasone and oxygen support strategies in ICU patients with COVID‐19 pneumonia (COVIDICUS) |
| Methods | Trial design: quadruple‐masked RCT Sample size: 550 Setting: inpatient Language: French, English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): placebo Concomitant therapy: study stratified according to subgroups (only oxygen therapy, CPAP, HFNC, IMV) |
| Outcomes | Primary study outcome
|
| Starting date | 10 April 2020 |
| Contact information | Jean François TIMSIT, Pr |
| Notes | Recruitment status: active, not recruiting Prospective completion date: 31 December 2021 Date last update was posted: 9 February 2021 Sponsor/funding: Assistance Publique ‐ Hôpitaux de Paris |
NCT04345445.
| Study name | Study to evaluate the efficacy and safety of tocilizumab versus corticosteroids in hospitalised COVID‐19 patients with high risk of progression |
| Methods | Trial design: open‐label, randomised, cross‐over interventional study Sample size: 310 Setting: inpatient Language: English Number of centres: 4 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): methylprednisolone 120 mg/day for 3 days IV Concomitant therapy: no information |
| Outcomes | Primary study outcome
|
| Starting date | 14 April 2020 |
| Contact information | Adeeba Kamarulzaman, MBBS: +603‐79492050 Email: adeeba@um.edu.my |
| Notes | Recruitment status: not yet recruiting Prospective completion date: 31 October 2020 Date last update was posted: 14 April 2020 Sponsor/funding: University of Malaya |
NCT04377503.
| Study name | Tocilizumab versus methylprednisolone in the cytokine release syndrome of patients with COVID‐19 |
| Methods | Trial design: phase II trial (open‐label), RCT Sample size: 40 Setting: inpatient Language: English Number of centres: 1 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): methylprednisolone at a dose of 1.5 mg/kg/d divided into 2 daily doses for 7 days. Then 1 mg/kg/day for another 7 days in 2 daily doses. Finally, 0.5 mg/kg/d for another 7 days. Concomitant therapy: no information |
| Outcomes | Primary outcome: patient clinical status 15 days after randomisation on a 7‐category ordinal scale (time frame: 15 days after randomisation) |
| Starting date | No information |
| Contact information | Jose A Azevedo, MD, PhD: +559832168110 Email: jrazevedo47@gmail.com |
| Notes | Recruitment status: not yet recruiting Prospective completion date: no information Date last update was posted: 6 May 020 Sponsor/funding: Hospital Sao Domingos |
NCT04452565.
| Study name | NA‐831, atazanavir and dexamethasone combination therapy for the treatment of COVID‐19 infection (NATADEX) |
| Methods |
|
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions |
|
| Outcomes | Primary outcome
|
| Starting date | First posted: 30 June 2020 |
| Contact information | Brian Tran, MD: 1‐415‐941‐3133 Email: BTran@neuroactiva.com |
| Notes | Recruitment status: recruiting Prospective completion date: 15 February 2021 Date last update was posted: 7 September 2020 Sponsor/funding: NeuroActiva, Inc. |
NCT04499313.
| Study name | Dexamethasone versus methylprednisolone for the treatment of patients with ARDS caused by COVID‐19 |
| Methods |
|
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): methylprednisolone sodium succinate at a dose of 0.5 mg/kg (injectable solution) Concomitant therapy: no information |
| Outcomes | Primary outcome
|
| Starting date | 2 August 2020 |
| Contact information | Abu Taiub Mohammed Mohiuddin Chowdhury, MBBS, MD: +88 01817711079 Email: dr_mohiuddinchy@yahoo.com |
| Notes | Recruitment status: recruiting Prospective completion date: 30 November 2020 Date last update was posted: 18 August 2020 Sponsor/funding: Chattogram General Hospital |
NCT04509973.
| Study name | Higher vs. lower doses of dexamethasone for COVID‐19 and severe hypoxia (COVIDSTEROID2) |
| Methods | Trial design: quadruple‐blinded, multicentre, clinical RCT Sample size: 1000 Setting: inpatient Language: Swedish, Danish, English Number of centres: 53 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): dexamethasone 6 mg once daily in addition to standard care for up to 10 days. We will allow the use of betamethasone 6 mg at sites where dexamethasone is not available. Concomitant therapy: no information |
| Outcomes | Primary outcome: days alive without life support (i.e. IMV, circulatory support or renal replacement therapy) from randomisation to day 28 |
| Starting date | 27 August 2020 |
| Contact information | Anders Perner, MD, PhD, Professor: +4535458333 Email: anders.perner@regionh.dk |
| Notes | Recruitment status: active, not recruiting Prospective completion date: 17 February 2022 Date last update was posted: 1 September 2020 Sponsor/funding: Scandinavian Critical Care Trials Group |
NCT04513184.
| Study name | Randomised clinical trial of intranasal dexamethasone as an adjuvant in patients with COVID‐19 |
| Methods | Trial design: multicentre, double‐masked (participant, care provider), RCT Sample size: 60 Setting: inpatient Language: Spanish, English Number of centres: 3 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): nasal dexamethasone 0.12 mg/kg/daily for 3 days from day 1, followed by 0.06 mg/kg/daily from day 4 to 10 after randomisation Concomitant therapy: no information |
| Outcomes | Primary outcome
|
| Starting date | 14 July 2020 |
| Contact information | Graciela A Cárdenas‐Hernández, PhD: +525556063822 ext 2012 Email: gracielacardenas@yahoo.com.mx |
| Notes | Recruitment status: recruiting Prospective completion date: primary completion date 30 March 2021 estimated study completion date 31 July 2021 Date last update was posted: 12 November 2020 Sponsor/funding: Edda Sciutto Conde |
NCT04528329.
| Study name | Anosmia and / or ageusia in COVID‐19: timeline, treatment with early corticosteroid and recovery |
| Methods | Trial design: open‐label RCT Sample size: 300 Setting: no information Language: Arabic, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): dexamethasone is to be used lately upon the deterioration of cases Concomitant therapy: no information |
| Outcomes | Time to recovery (time frame: 1 to 6 weeks) from anosmia and/or ageusia |
| Starting date | 30 August 2020 |
| Contact information | Emad R Issak, MD: 01272228989 Email: dr.emad.r.h.issak@gmail.com |
| Notes | Recruitment status: recruiting Prospective completion date: 15 April 2021 Date last update was posted: 29 March 2021 Sponsor/funding: ClinAmygate |
NCT04528888.
| Study name | Steroids and unfractionated heparin in critically ill patients with pneumonia from COVID‐19 infection (STAUNCH‐19) |
| Methods | Trial design: multicentre, national, interventional, randomised, open‐label Sample size: 210 Setting: inpatient Language: Italian, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions |
|
| Outcomes | Primary outcome: all‐cause mortality at day 28, defined as the comparison of proportions of patients' death for any cause at day 28 from randomisation |
| Starting date | 1 September 2020 |
| Contact information | Massimo Girardis, PD: 0594225878 ext 0039 Email: massimo.girardis@unimore.it |
| Notes | Recruitment status: recruiting Prospective completion date: 30 July 2021 Date last update was posted: 27 August 2020 Sponsor/funding: Massimo Girardis, University of Modena and Reggio Emilia |
NCT04545242.
| Study name | Efficacy of dexamethasone in patients with acute hypoxemic respiratory failure caused by infections (DEXA‐REFINE) |
| Methods | Trial design: multicentre, open‐label, clinical RCT Sample size: 980 Setting: inpatient Language: English Number of centres: 40 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): dexamethasone: 20 mg/IV/ daily from day of randomisation (day 1) during 5 days, followed by 10 mg/IV/ daily from day 6 to 10 of randomisation Concomitant therapy: no information |
| Outcomes | Primary outcome: all‐cause mortality at 60 days after randomisation |
| Starting date | 8 February 2021 |
| Contact information | Jesús Villar, MD: +34606860027 Email: jesus.villar54@gmail.com |
| Notes | Recruitment status: not yet recruiting Prospective completion date: 30 December 2023 Date last update was posted: 22 January 2021 Sponsor/funding: Dr. Negrin University Hospital |
NCT04636671.
| Study name | Methylprednisolone vs. dexamethasone in COVID‐19 pneumonia (MEDEAS RCT) (MEDEAS) |
| Methods | Trial design: open‐label RCT Sample size: 680 Setting: inpatient Language: Italian, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): A. dexamethasone 6 mg IV in 30 min or orally from day 1 to 10 or until hospital discharge (if sooner). B. After day 10 study treatment is interrupted. Concomitant therapy: no information |
| Outcomes | Primary outcome: survival proportion at 28 days in both arms |
| Starting date | 25 November 2020 |
| Contact information | Marco Confalonieri, MD: +390403994667 Email: mconfalonieri@units.it |
| Notes | Recruitment status: recruiting Prospective completion date: estimated primary completion date 31 March 2021; estimated study completion date 30 April 2021 Date last update was posted: 19 November 2020 Sponsor/funding: University of Trieste and Centro di Riferimento Oncologico ‐ Aviano and National Institute for the Infectious Diseases (L. Spallanzani) ‐ Rome |
NCT04663555.
| Study name | Effect of two different doses of dexamethasone in patients with ARDS and COVID‐19 (REMED) |
| Methods | Trial design: prospective, phase II, open‐label, RCT Sample size: 300 Setting: inpatient Language: Czech, English Number of centres: 11 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): dexamethasone 6 mg day 1 to 10 Concomitant therapy: no information |
| Outcomes | Primary outcome: number of ventilator‐free days at 28 days after randomisation, defined as being alive and free from mechanical ventilation (> 48 h) |
| Starting date | |
| Contact information | Jan Maláska, MD, PhD, EDIC: +420723784101 Email: jan.malaska@gmail.com |
| Notes | Recruitment status: recruiting Prospective completion date: 31 March 2021 Date last update was posted: 4 February 2021 Sponsor/funding: Brno University Hospital |
NCT04673162.
| Study name | Evaluation of the efficacy of high doses of methylprednisolone in SARS‐CoV2 (COVID‐19) pneumonia patients |
| Methods | Trial design: quadruple‐blind, multicentre, randomised study Sample size: 260 Setting: inpatient Language: Italian, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): standard treatment (currently dexamethasone 6 mg/daily for 10 days) plus placebo Concomitant therapy: no information |
| Outcomes | Primary study outcome
|
| Starting date | |
| Contact information | Massimo Costantini, MD: +390522296986 Email: massimo.costantini@ausl.re.it |
| Notes | Recruitment status: not yet recruiting Prospective completion date: estimated primary completion date April 2021; estimated study completion date June 2021 Date last update was posted: 17 December 2020 Sponsor/funding: Azienda Unità Sanitaria Locale Reggio Emilia |
NCT04707534.
| Study name | Dexamethasone for COVID‐19 |
| Methods | Trial design: open‐label RCT Sample size: 300 Setting: inpatient Language: English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): dexamethasone 6 mg daily for 10 days Concomitant therapy: no information |
| Outcomes | Primary outcome: 8‐point World Health Organization ordinal scale at day 28 |
| Starting date | 21 January 2021 |
| Contact information | Huimin Wu, MD MPH: (405) 271‐6173 Email: Huimin‐Wu@ouhsc.edu |
| Notes | Recruitment status: recruiting Prospective completion date: 21 June 2021 Date last update was posted: 8 January 2021 Sponsor/funding: University of Oklahoma |
NCT04765371.
| Study name | Comparison between prednisolone and dexamethasone on mortality in patients on oxygen therapy, with COVID‐19 (COPreDex) |
| Methods | Trial design: open‐label RCT Sample size: 220 Setting: inpatients Language: French, English Number of centres: 6 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): 60 mg/d of prednisolone during 10 days Concomitant therapy: no information |
| Outcomes | Primary outcome: mortality assessment at day 28 |
| Starting date | March 2021 |
| Contact information | Maryline Delattre: +33 130754131 Email: maryline.delattre@ght‐novo.fr |
| Notes | Recruitment status: recruiting Prospective completion date: October 2021 Date last update was posted: 1 March 2021 Sponsor/funding: Centre Hospitalier René Dubos |
NCT04780581.
| Study name | Glucocorticoid therapy in coronavirus disease COVID‐19 patients |
| Methods | Trial design: open‐label RCT Sample size: 290 Setting: inpatient Language: Spanish, English Number of centres: 5 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): high‐dose methylprednisolone bolus (250 mg/4 h, 3 days) Concomitant therapy: no information |
| Outcomes | Primary outcome: mortality rate in COVID‐19 patients after high‐dose methylprednisolone bolus administration versus mortality rate intermediate‐dose dexamethasone pattern (time frame: 28 days) |
| Starting date | 1 February 2021 |
| Contact information | Luis Corral Gudino: 983 420400 Email: lcorral@saludcastillayleon.es |
| Notes | Recruitment status: recruiting Prospective completion date: 31 December 2021 Date last update was posted: 3 March 2021 Sponsor/funding: Fundación Instituto de Estudios de Ciencias de la Salud de Castilla y León |
NCT04795583.
| Study name | Corticosteroids for COVID‐19 (CORE‐COVID) |
| Methods | Trial design: interventional, randomised, placebo‐controlled, triple‐blinded, adaptive clinical trial Sample size: 1526 Setting: outpatient Language: English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): capsules with the same appearance as prednisone Concomitant therapy: no information |
| Outcomes | Primary outcome
|
| Starting date | April 2021 |
| Contact information | Carlos Cervera, MD, PhD: 780‐492‐5346 Email: cerveraa@ualberta.ca |
| Notes | Recruitment status: not yet recruiting Prospective completion date: August 2022 Date last update was posted: 18 March 2021 Sponsor/funding: University of Alberta |
NCT04834375.
| Study name | Randomised open investigation determining steroid dose (ROIDS‐Dose) |
| Methods | Trial design: randomised, open‐label trial Sample size: 142 Setting: probably inpatient Language: English Number of centres: single‐centre Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention
Treatment details of control group (e.g. dose, route of administration): dexamethasone 0.2 mg/kg/d IV (maximum 20 mg daily) for 10 days Concomitant therapy: no information |
| Outcomes | Primary outcome: all‐cause mortality at 28 days |
| Starting date | 19 March 2021 |
| Contact information | Carlos X Rabascall, MD: 5164655400 Email: crabascallay@northwell.edu |
| Notes | Recruitment status: recruiting Prospective completion date: 19 April 2022 Date last update was posted: 8 April 2021 Sponsor/funding: Northwell Health |
NCT04836780.
| Study name | Dexamethasone early administration in hospitalised patients with COVID‐19 pneumonia (EARLYDEXCoV2) |
| Methods | Trial design: prospective, multicentre, phase‐4, parallel‐group, open‐label RCT Sample size: 126 Setting: inpatient Language: Spanish, English Number of centres: no information Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Details of intervention:
Treatment details of control group (e.g. dose, route of administration): standard care therapy Concomitant therapy: no information |
| Outcomes | Primary outcome
|
| Starting date | No information |
| Contact information | Anabel Franco Moreno, MD, PhD: +34 911 918000 Email: afranco278@hotmail.com |
| Notes | Recruitment status: recruiting Prospective completion date: 30 June 2021 Date last update was posted: 8 April 2021 Sponsor/funding: Hospital Universitario Infanta Leonor |
NCT04860518.
| Study name | Human intravenous interferon beta‐Ia safety and preliminary efficacy in hospitalised subjects with Coronavirus (HIBISCUS) |
| Methods | Trial design: double‐blind, randomised controlled trial Sample size: 140 Setting: inpatient Language: English Number of centres: 4 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Details of intervention: interferon beta‐Ia
Treatment details of control group (e.g. dose, route of administration): dexamethasone, IV, daily for 6 days while hospitalised, dose not stated Concomitant therapy: n.i. |
| Outcomes | Primary study outcome: clinical status at day 14 (first day of study drug is day 1) as measured by WHO 9‐point ordinal scale WHO 9‐point ordinal scale: 0 ‐ no detectable infection
|
| Starting date | 23 August 2021 |
| Contact information | Jarna Hannukainen, PhD: +358 02 469 5151 Email: jarna.hannukainen@faron.com Gerd Tötterman: +358 02 469 5151 Email: gerd.totterman@faron.com |
| Notes | Recruitment status: recruiting Prospective completion date: April 2023 Date last update was posted: 3 January 2022 Sponsor/funding: Faron Pharmaceuticals Ltd |
TCTR20211017001.
| Study name | A comparative study of the effectiveness between pulse regimen methylprednisolone versus high dose dexamethasone as the initial treatment of moderate Covid‐19 pneumonia: an open‐label randomised controlled trial |
| Methods | Trial design: open‐label, randomised controlled trial Sample size: 120 Setting: inpatient Language: English Number of centres: 2 Type of intervention (treatment/prevention): treatment |
| Participants | Inclusion criteria: age over 18 years old, visited within 48 hours, respiratory sample was confirmed Covid‐19 by RT‐PCR, evidence of pneumonia by chest imaging, resting oxygen saturation between 90% and 94%, voluntary consent Exclusion criteria: received high flow nasal cannula, non‐invasive mechanical ventilation or invasive mechanical ventilation, high risk for corticosteroid such as current active infection or poor glycaemic control, immunocompromised host such as end stage liver disease, end stage renal disease without renal replacement therapy, HIV CD4 less than 200 or cancer with ongoing chemotherapy, pregnant women, psychiatric problems, current use of corticosteroid (more than 20 mg of prednisolone equivalent dose and consecutively more than 14 day) |
| Interventions | Details of intervention: methylprednisolone
Treatment details of control group (e.g. dose, route of administration): dexamethasone, IV, 20 mg per day for 3 days, then intravenous or oral dexamethasone 20 mg per day for 2 days, then intravenous or oral dexamethasone 10 mg per day for 5 days Concomitant therapy: not stated |
| Outcomes | Primary study outcome: mean of WHO clinical progression scale at day 5 |
| Starting date | 18 October 2021 |
| Contact information | Jakkrit Laikitmongkhon: 270 Rama 6 Rd. Phayatai Ratchathewi Bangkok 10400, Thailand |
| Notes | Recruitment status: not yet recruiting Prospective completion date: 31 December 2022 Date last update was posted: 16 November 2021 Sponsor/funding: Faculty of Medicine Ramathibodi Hospital |
AHRF: acute hypercapnic respiratory failure; ALT: alanine transaminase; APPT: activated partial thromboplastin time; ARDS: acute respiratory distress syndrome; AST: aspartate transaminase; CT: computed tomography; d: days; ECG: echocardiogram; ECMO: extracorporeal membrane oxygenation; FiO2: fraction of inspired oxygen; HFNC: high‐flow nasal cannula; HFNO: high‐flow nasal oxygen; ICU: intensive care unit; IMV: invasive mechanical ventilation; IV: intravenous; LMWH: low molecular weight heparin; NLR: neutrophil‐lymphocyte ratio; NPPV: non‐invasive positive pressure ventilation; PCR: polymerase chain reaction; PEEP: positive end‐expiratory pressure; RCT: randomised controlled trial; RT‐PCR: reverse transcription polymerase chain reaction; SC: subcutaneously; SpO2: blood oxygen saturation; ULN: upper limit of normal; WHO: World Health Organization
Differences between protocol and review
Differences between protocol and first review version
Types of participants
For the different endpoints of interest and treatment settings, we excluded participants treated for symptoms of long‐COVID. However, treatments for long‐COVID should soon be addressed outside this review.
Types of outcome measures
Due to heterogeneous reporting and high bias through death as competing risk, we omitted most endpoints with regard to clinical improvement and worsening, and length of hospital stay. As a compromise and because of their importance to patients, data availability in trials, and strong implications for resource usage, we kept in the first publication of this living review the following outcome measures: new need for invasive ventilation, liberation from invasive ventilation, ventilator‐free days, need for dialysis, viral clearance, quality of life/neurological outcome.
We counted adverse events regardless of their grades because the included studies did not report grades for adverse events.
If not specified otherwise, the observation period for outcomes other than mortality was the longest period available. Where this differed between arms of a trial, risk of bias assessment would be adjusted.
Types of intervention
After discussion with clinical experts we added comparisons to meet questions arising in daily routine practice:
dose comparisons;
time comparisons (early versus late) but indirectly in terms of disease severity as described below;
two different types of corticosteroids;
corticosteroid versus another active substance (e.g. remdesivir, tocilizumab).
On the other hand, we excluded topical and inhaled steroids from this review because of inherently different pharmacokinetics and treatment settings. However, their role is critical and inhaled steroids were addressed in another review by our review group (Griesel 2022).
Analysis
We made calculations with RevMan Web instead of RevMan 5.4 software.
We omitted subgroup analysis for treatment settings; that is, outpatient, inpatient, and intensive care unit, because we deemed triage criteria, definition of intensive care or high‐dependency units, and available resources too heterogeneous. Taking away a degree of indirectness, we instead performed subgroup analysis stratified by the level of respiratory support needed at randomisation. This allowed for the fact that levels of respiratory support can at least partially be delivered independent of the treatment setting and hence rendered a more valid conclusion about disease severity.
Differences between first and second review version
This version of the review puts more focus on health equity‐related aspects. We examined participant characteristics more closely and analysed mortality data with respect to equity (see below). Moreover, we put emphasis on possible harm through secondary infections especially in tropical low‐ and middle‐income settings in the discussion section. Finally, we strengthened the authoring team (previously solely authors from Germany and therefore with a high‐income background) with two Indian clinician scientists and guideline authors, and we adjusted the title of the review.
In addition, competing risk of death was extensively discussed in the first version of the review. The respective section was very much shortened but the impact on risk of bias assessments remains where the outcomes could not be changed or adjusted (see below).
To address additional sources of bias arising from platform trials we pioneered a checklist for their critical appraisal and added sensitivity analyses (see below).
Because we suspect a different immune response in vaccinated participants, we added vaccination status as an item for data extraction.
Types of outcome measures
Individuals with a suspected or confirmed diagnosis of COVID‐19 and moderate to severe disease: In line with the research gap identified in the first version of the review we added All‐cause mortality up to 120 days and retained All‐cause mortality up to 30 days for optimal evidence robustness. To reach a certain level of adjustment for competing risk of death, we added Discharged alive and changed New need for invasive mechanical ventilation (IMV) to New need for IMV or death. Because of compelling clinical and equity implications, we added Invasive fungal infections as a prioritised outcome included in the summary of findings tables while Quality of life is a prioritised outcome but no longer included in the summary of findings table. Need for dialysis and Viral clearance are categorised as additional outcomes. We deleted ventilator‐free days from the outcome set, because there is now New need for IMV or death as another outcome quasi‐adjusted for competing risk of death, which is more widely reported.
Certain outcomes are no longer additionally defined as changes in the COVID‐19‐specific WHO clinical progression scale (WHO 2020c), but as simple descriptions.
The outcome Need for dialysis was renamed New need for dialysis to clarify that participants with pre‐existing need for dialysis were excluded from this analysis. Data remained unchanged.
Individuals with a suspected or confirmed diagnosis of SARS‐CoV‐2 infection and asymptomatic or mild disease: To better adjust our review to the priorities of outpatients after publication of a Cochrane Review on inhaled corticosteroids in COVID‐19 (Griesel 2022), we added Admission to hospital or death within 28 days and Quality of life as prioritised outcomes.
Subgroup analysis
We added all‐cause mortality subgroup analyses stratified by age group, sex, and ethnicity in all comparisons.
Sensitivity analysis
We added a new sensitivity analysis excluding platform trials from the mortality outcomes' analyses. Moreover, following Chapter 10 of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2022), we performed sensitivity analysis with a fixed‐effect versus a random‐effects model in this version of the review.
Contributions of authors
CW: screening, data extraction, characteristics of included studies/ongoing studies/studies awaiting classification, risk of bias assessment, meta‐analysis, conception and writing of the review, taking responsibility for reading and checking the review before submission
MG: data extraction, risk of bias assessment, appraisal of platform trials, meta‐analysis, conception and writing of the review, taking responsibility for reading and checking the review before submission
AM: clinical expertise, writing of the review, taking responsibility for reading and checking the review before submission
MIM: design and conduct of searches, drafting of search methods section, taking responsibility for reading and checking the review before submission
MSp: screening, data extraction, risk of bias assessment, appraisal of platform trials, taking responsibility for reading and checking the review before submission
ALF: data extraction, risk of bias assessment, clinical expertise, writing of the review, taking responsibility for reading and checking the review before submission
AAN: data extraction, risk of bias assessment, clinical expertise, writing of the review, taking responsibility for reading and checking the review before submission
JD: data extraction, risk of bias assessment, clinical expertise, writing of the review, taking responsibility for reading and checking the review before submission
MS: clinical expertise, writing of the review, taking responsibility for reading and checking the review before submission
NS: methodological expertise and advice, conception and writing of the review, taking responsibility for reading and checking the review before submission
FF: clinical expertise, writing of the review, taking responsibility for reading and checking the review before submission
Sources of support
Internal sources
-
University Hospital of Cologne, Germany
Cochrane Cancer, Department I of Internal Medicine
-
University of Leipzig Medical Center, Germany
Department of Anesthesiology and Intensive Care
-
Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt‐Universität zu Berlin, Berlin, Germany, Germany
Department of Infectious Diseases and Respiratory Medicine
-
Christian Medical College, Vellore, Tamil Nadu, India
Department of Respiratory Medicine and Department of Pulmonary Medicine
External sources
-
Federal Ministry of Education and Research, Germany
NaFoUniMedCovid19 (funding number: 01KX2021) part of the project „CEO‐Sys“
Declarations of interest
CW: Federal Ministry of Education and Research (grant/contract); staff of Cochrane Haematology.
MG: Bundesministerium für Bildung und Forschung (grant/contract); published Cochrane‐initiated Twitter posts and an upcoming Cochrane‐initiated podcast on systemic corticosteroids; Resident at the Department of Anesthesiology and Critical Care, University of Leipzig Medical Service; Member of the German Society of Anaesthesia and Intensive Care Medicine (Deutsche Gesellschaft für Anästhesiologie & Intensivmedizin, DGAI), which supports and promotes the German Clinical Practice Guideline on COVID‐19 Inpatient Therapy.
AM: no relevant interests; co‐ordination of Section COVRIIN and work in the office of STAKOB (Competence and Treatment Centres for high‐consequence infectious diseases) at Robert Koch‐Institute Centre for Biological Threats and Special Pathogens (ZBS), Section Clinical Management and Infection Control.
MIM: no relevant interests; performs editorial activities for reviews overseen by Cochrane Metabolic and Endocrine Disorders.
MSp: no relevant interests; Resident, Universitätsklinikum Leipzig.
ALF: Universitätsklinikum Leipzig AöR (employment); Fellowship in University Hospital Leipzig, 04103 Leipzig, Germany.
AAN: no relevant interests; part of Indian COVID guidelines, worked in the evidence synthesis team for inhaled steroids and HFNC versus NIV in COVID; works at the Department of Respiratory Medicine, Christian Medical College, Vellore.
JD: no relevant interests; Pulmonologist, Department of Pulmonary Medicine, CMC Vellore, India.
MS: no relevant interests; Medical Doctor, Charité – Universitätsmedizin Berlin, Germany.
NS: no relevant interests; Editor of Cochrane Haematology but was not involved in the editorial process for this review.
FF: no relevant interests; Intensive Care Consultant, University Hospital, University of Leipzig Medical Faculty.
contributed equally (first author)
contributed equally (last author)
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
Angus 2020 {published data only}
- Angus DC, Berry S, Lewis RJ, Al-Beidh F, Arabi Y, Van Bentum-Puijk W, et al. The randomised embedded multifactorial adaptive platform for community-acquired pneumonia (REMAP-CAP) study: rationale and design. Annals of the American Thoracic Society 2020;17(7):879-91. [DOI: 10.1513/AnnalsATS.202003-192SD] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Angus DC, Derde L, Al-Beidh F, Annane D, Arabi Y, Beane A, et al. Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19: the REMAP-CAP COVID-19 corticosteroid domain randomised clinical trial. JAMA 2020;324(13):1317-29. [DOI: 10.1001/jama.2020.17022] [NCT02735707] [DOI] [PMC free article] [PubMed] [Google Scholar]
Corral‐Gudino 2021 {published data only}
- Corral-Gudino L, Bahamonde A, Arnaiz-Revillas F, Gómez-Barquero J, Abadía-Otero J, García-Ibarbia C, et al. Methylprednisolone in adults hospitalised with COVID-19 pneumonia: an open-label randomised trial (GLUCOCOVID). Wiener Klinische Wochenschrift 2021;133(7-8):303-11. [DOI: 10.1007/s00508-020-01805-8] [EUCTR2020-001934-37-ES] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corral L, Bahamonde A, Arnaiz delas Revillas F, Gomez-Barquero J, Abadia-Otero J, Garcia-Ibarbia C, et al. GLUCOCOVID: a controlled trial of methylprednisolone in adults hospitalised with COVID-19 pneumonia. medRxiv [Preprint]. [DOI: 10.1101/2020.06.17.20133579] [EUCTR2020-001934-37-ES] [DOI]
Dequin 2020 {published data only}
- Dequin PF, Gouge AL, Tavernier E, Giraudeau B, Zohar S. Embedding a COVID-19 group sequential clinical trial within an ongoing trial: lessons from an unusual experience. Statistics in Biopharmaceutical Research 2020:1-5. [EMBASE: https://www.embase.com/search/results?subaction=viewrecord&id=L2005906375&from=export] [DOI] [PMC free article] [PubMed]
- Dequin PF, Heming N, Meziani F, Plantefève G, Voiriot G, Badié J, et al. Effect of hydrocortisone on 21-day mortality or respiratory support among critically ill patients with COVID-19: a randomised clinical trial. JAMA 2020;324(13):1298-306. [DOI: 10.1001/jama.2020.16761] [NCT02517489] [DOI] [PMC free article] [PubMed] [Google Scholar]
Edalatifard 2020 {published data only}
- Edalatifard M, Akhtari M, Salehi M, Naderi Z, Jamshidi A, Mostafaei S, et al. Intravenous methylprednisolone pulse as a treatment for hospitalised severe COVID-19 patients: results from a randomised controlled clinical trial. European Respiratory Journal 2020;56(6):1-13. [DOI: 10.1183/13993003.02808-2020] [IRCT20200404046947N1] [DOI] [PMC free article] [PubMed] [Google Scholar]
Farahani 2021 {published data only}
- Farahani RH, Mosaed R, Nezami-Asl A, Chamanara M, Soleiman-Meigooni S, Kalantar S, et al. Evaluation of the efficacy of methylprednisolone pulse therapy in treatment of COVID-19 adult patients with severe respiratory failure: randomised, clinical trial. Research Square 2021;Version 1:1-19. [DOI: 10.21203/rs.3.rs-66909/v1] [IRCT20200406046963N1] [DOI] [Google Scholar]
Horby 2021 {published data only}
- Horby P, Lim WS, Emberson J, Mafham M, Bell J, Linsell L, et al. Effect of dexamethasone in hospitalised patients with COVID-19: preliminary report. medRxiv [Preprint] 2020. [DOI: ]
- Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, Linsell L, et al. Dexamethasone in hospitalised patients with COVID-19. New England Journal of Medicine 2021;384(8):693-704. [DOI: 10.1056/NEJMoa2021436] [NCT04381936] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oxford University. Low-cost dexamethasone reduces death by up to one third in hospitalised patients with severe respiratory complications of COVID-19. University of Oxford 2020.
Jamaati 2021 {published data only}
- Jamaati H, Hashemian SM, Farzanegan B, Malekmohammad M, Tabarsi P, Marjani M, et al. No clinical benefit of high dose corticosteroid administration in patients with COVID-19: a preliminary report of a randomised clinical trial. European Journal of Pharmacology 2021;897:173947. [DOI: 10.1016/j.ejphar.2021.173947] [IRCT20151227025726N17] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jeronimo 2020 {published data only}
- Barros CMSS, Freire RS, Frota E, Santos AGR, Farias MAL, Rodrigues MGA, et al. Short-course of methylprednisolone improves respiratory functional parameters after 120 days in hospitalised COVID-19 patients (Metcovid Trial): a randomised clinical trial. Frontiers in Medicine 2021;8(758405):1-9. [DOI: 10.3389/fmed.2021.758405] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeronimo CM, Farias ME, Val FF, Sampaio VS, Alexandre MA, Melo GC, et al. Methylprednisolone as adjunctive therapy for patients hospitalised with COVID-19 (metcovid): a randomised, double-blind, phase IIb, placebo-controlled trial. Clinical Infectious Diseases 2020;72(9):e373–e81. [DOI: 10.1093/cid/ciaa1177] [NCT04343729] [DOI] [PMC free article] [PubMed] [Google Scholar]
Maskin 2021 {published data only}
- Maskin LP, Bonelli I, Olarte GL, Palizas F Jr, Velo AE, Lurbet MF, et al. High- versus low-dose dexamethasone for the treatment of COVID-19-related acute respiratory distress syndrome: a multicenter and randomised open-label clinical trial. medRxiv 2021;Version 1:1-21. [DOI: 10.1101/2021.09.15.21263597] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maskin LP, Bonelli I, Olarte GL, Palizas Jr F, Velo AE, Lurbet MF, et al. High- versus low-dose dexamethasone for the treatment of COVID-19-related acute respiratory distress syndrome: a multicenter, randomised open-label clinical trial. Journal of Intensive Care Medicine 2021;Version 1:1-9. [DOI: 10.1177/08850666211066799] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maskin LP, Olarte GL, Palizas F Jr, Velo AE, Lurbet MF, Bonelli I, et al. High dose dexamethasone treatment for acute respiratory distress syndrome secondary to COVID-19: a structured summary of a study protocol for a randomised controlled trial. Trials 2020;21(1):743. [DOI: 10.1186/s13063-020-04646-y] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT04395105. Dexamethasone for COVID-19 related ARDS: a multicenter, randomised clinical trial. clinicaltrials.gov/show/NCT04395105 (first received 20 May 2020).
Munch 2021a {published data only}
- Munch MW, Meyhoff TS, Helleberg M, Kjær M-BN, Granholm A, Hjortsø CJ, et al. Low-dose hydrocortisone in patients with COVID-19 and severe hypoxia: the COVID STEROID randomised, placebo-controlled trial. Acta Anaesthesiologica Scandinavica 2021;65(10):1421-30. [DOI: 10.1111/aas.13941] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT04348305. Hydrocortisone for COVID-19 and severe hypoxia. clinicaltrials.gov/show/NCT04348305 (first received 16 April 2020).
- Petersen MW, Meyhoff TS, Helleberg M, Nørregaard Kjær MB, Granholm A, Steensen Hjortsø CJ, et al. Low-dose hydrocortisone in patients with COVID-19 and severe hypoxia (COVID STEROID) trial-protocol and statistical analysis plan. Acta Anaesthesiologica Scandinavica 2020;64(9):1365-75. [DOI: 10.1111/aas.13673] [DOI] [PMC free article] [PubMed] [Google Scholar]
Munch 2021b {published data only}
- Granholm A, Munch MW, Myatra SN, Vijayaraghavan BKT, Cronhjort M, Wahlin RR, et al. Dexamethasone 12 mg versus 6 mg for patients with COVID-19 and severe hypoxaemia: a pre-planned, secondary Bayesian analysis of the COVID STEROID 2 trial. Intensive Care Medicine 2022;48(1):45-55. [DOI: 10.1007/s00134-021-06573-1] [DOI] [PMC free article] [PubMed] [Google Scholar]
- The COVID STEROID 2 trial group. Effect of 12 mg vs 6 mg of dexamethasone on the number of days alive without life support in adults with COVID-19 and severe hypoxemia The COVID STEROID 2 randomised trial. JAMA 2021;326(18):1807–17. [DOI: 10.1001/jama.2021.18295] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ranjbar 2021 {published data only}
- Ranjbar K, Shahriarirad R, Erfani A, Khodamoradi Z, Saadi MHG, et al. Methylprednisolone or dexamethasone, which one is the superior corticosteroid in the treatment of hospitalised COVID-19 patients: a triple-blinded randomised controlled trial. Research Square (Preprint). [DOI: ] [IRCT20200204046369N1]
Taboada 2021 {published data only}
- NCT04726098. Low or high dose of dexamethasone in patients with respiratory failure by COVID-19. clinicaltrials.gov/ct2/show/record/NCT04726098 (first received 27 January 2021).
- Taboada M, Rodríguez N, Varela PM, Rodríguez MT, Abelleira R, González A, et al. Effect of high versus low dose of dexamethasone on clinical worsening in patients hospitalised with moderate or severe COVID-19 pneumonia: an open-label, randomised clinical trial. European Respiratory Journal 2021;59(1):1-43. [DOI: 10.1183/13993003.02518-2021] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tang 2021 {published data only}
- Tang X, Feng YM, Ni JX, Zhang JY, Liu LM, Hu K, et al. Early use of corticosteroid may prolong SARS-CoV-2 shedding in non-intensive care unit patients with COVID-19 pneumonia: a multicenter, single-blind, randomised control trial. Respiration 2021;100(2):116-26. [DOI: 10.1159/000512063] [NCT04273321] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tomazini 2020 {published data only}
- Tomazini BM, Maia IS, Bueno FR, Silva Mvao Baldassare FP, Costa EL, Moura RA, et al. COVID-19-associated ARDS treated with DEXamethasone (CoDEX): study design and rationale for a randomised trial. medRxiv [Preprint] 2020. [DOI: ] [DOI] [PMC free article] [PubMed]
- Tomazini BM, Maia IS, Bueno FR, Silva Mvao Baldassare FP, Costa EL, Moura RA, et al. COVID-19-associated ARDS treated with dexamethasone (CoDEX): study design and rationale for a randomised trial. Revista Brasileira de Terapia Intensiva 2020;32(3):354-62. [DOI: 10.5935/0103-507X.20200063] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomazini BM, Maia IS, Cavalcanti AB, Berwanger O, Rosa RG, Veiga VC, et al. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: the CoDEX randomised clinical trial. JAMA 2020;324(13):1307-16. [DOI: 10.1001/jama.2020.17021] [NCT04327401] [DOI] [PMC free article] [PubMed] [Google Scholar]
Toroghi 2021 {published data only}
- IRCT20100228003449N31. Corticosteroids in COVID-19. irct.ir/trial/51163 (first received 8 October 2020).
- Toroghi N, Abbasian L, Anahid Nourian A, Davoudi-Monfared E, Khalili H, Hasannezhad M, et al. Comparing efficacy and safety of different doses of dexamethasone in the treatment of COVID-19: a three-arm randomized clinical trial. Pharmacological Reports 2021;Version 1:1-12. [DOI: 10.1007/s43440-021-00341-0] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
EUCTR2020‐001445‐39‐ES {published data only}
- EUCTR2020-001445-39-ES. Clinical trial to evaluate methylprednisolone pulses and tacrolimus in hospitalized patients with severe pneumonia secondary to COVID-19 (tacrovid). www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001445-39 (first received 31 March 2020).
EUCTR2020‐001616‐18‐ES {published data only}
- TACTIC-COVID. www.clinicaltrialsregister.eu/ctr-search/search?query=2020-001616-18.
- Treatment with inhaled corticoids in patients with COVID-19 and pneumonia. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2020-001616-18-ES.
EUCTR2020‐001889‐10 {published data only}
- EUCTR2020-001889-10. Use of inhaled corticosteroids as treatment of early COVID-19 infection to prevent clinical deterioration and hospitalisation. www.clinicaltrialsregister.eu/ctr-search/trial/2020-001889-10/GB (first received 15 May 2020).
IRCT20120225009124N4 {published data only}
- IRCT20120225009124N4. Letter to the editor: efficacy of different methods of combination regimen administrations including dexamethasone, intravenous immunoglobulin, and interferon-beta to treat critically ill COVID-19 patients: a structured summary of a study protocol for a randomized controlled trial. Trials 2020;21(1):549. [DOI: 10.1186/s13063-020-04499-5] [DOI] [PMC free article] [PubMed] [Google Scholar]
IRCT20190312043030N2 {published data only}
- IRCT20190312043030N2. The effect of selenium, vitamin C and methylprednisolone combination on mortality and morbidity of COVID-19 patients. en.irct.ir/trial/49508 (first received 19 August 2020).
IRCT20200522047542N1 {published data only}
- IRCT20200522047542N1. Effect of corton on olfactory dysfunction in COVID-19 patients. en.irct.ir/trial/48379 (first received 4 August 2020).
ISRCTN86534580 {published data only}
- ISRCTN86534580. PRINCIPLE: a trial evaluating treatments for suspected COVID-19 in people aged 50 years and above with pre-existing conditions and those aged 65 years and above. www.isrctn.com/ISRCTN86534580 (first received 20 March 2020).
Moreira 2021 {published data only}
- Moreira TG, Matos KTF, De Paula GS, Santana TMM, Da Mata RG, Pansera FC, et al. Nasal administration of anti-CD3 monoclonal antibody (foralumab) reduces lung inflammation and blood inflammatory biomarkers in mild to moderate COVID-19 patients: a pilot study. Frontiers in Immunology 2021;12:3255. [DOI: 10.3389/fimmu.2021.709861] [DOI] [PMC free article] [PubMed] [Google Scholar]
Naik 2021 {published data only}
- Naik NB, Puri GD, Kajal K, Mahajan V, Bhalla A, Kataria S, et al. High-dose dexamethasone versus tocilizumab in moderate to severe COVID-19 pneumonia: a randomised controlled trial. Cureus 2021;13(12):e20353. [DOI: 10.7759/cureus.20353] [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT04341038 {published data only}
- NCT04341038. Clinical trial to evaluate methylprednisolone pulses and tacrolimus in patients with COVID-19 lung injury. clinicaltrials.gov/show/NCT04341038 (first received 10 April 2020).
- NCT04341038. Pragmatic, open-label, single-center, randomized, phase II clinical trial to evaluate the efficacy and safety of methylprednisolone pulses and tacrolimus in patients with severe pneumonia secondary to COVID-19: the TACROVID trial protocol. medRxiv [Preprint] 2021;21(100716):1-8. [DOI: 10.1016/j.conctc.2021.100716] [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT04355637 {published data only}
- NCT04355637. Inhaled corticosteroid treatment of COVID-19 patients with pneumonia. clinicaltrials.gov/show/NCT04355637 (first received 21 April 2020).
NCT04359511 {published data only}
- NCT04359511. Efficacy and safety of corticosteroids in oxygen-dependent patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04359511 (first received 24 April 2020).
NCT04361474 {published data only}
- Daval M, Corre A, Palpacuer C, Houssette J, Poillon G, Eliezer M, et al. Efficacy of local budesonide therapy in the management of persistent hyposmia in COVID-19 patients without signs of severity: a structured summary of a study protocol for a randomised controlled trial. Trials 2020;21(666):1-3. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT04361474. Trial evaluating the efficacy of local budesonide therapy in the management of hyposmia in COVID-19 patients without signs of severity. clinicaltrials.gov/show/NCT04361474 (first received 24 April 2020).
NCT04381364 {published data only}
- NCT04381364. Inhalation of ciclesonide for patients with COVID-19: a randomised open treatment study (HALT COVID-19). clinicaltrials.gov/show/NCT04381364 (first received 8 May 2020).
NCT04411667 {published data only}
- Sakoulas G, Geriak M, Kullar R, Greenwood KL, Habib M, Vyas A, et al. Intravenous immunoglobulin plus methylprednisolone mitigate respiratory morbidity in coronavirus disease 2019. Critical Care Explorations 2020;2(11):e0280. [DOI: 10.1097/CCE.0000000000000280] [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT04416399 {published data only}
- Ramakrishnan S, Nicolau DV Jr, Langford B, Mahdi M, Jeffers H, Mwasuku C, et al. Inhaled budesonide in the treatment of early COVID-19 illness: a randomised controlled trial. medRxiv [Preprint]. [DOI: ] [DOI] [PMC free article] [PubMed]
NCT04468646 {published data only}
- Riffat M, Fridoon A, Ahad Q, Muhammad AR, Syed AG, Muhammad AT, et al. Aprepitant as a combinant with dexamethasone reduces the inflammation via neurokinin 1 receptor antagonism in severe to critical COVID-19 patients and potentiates respiratory recovery: a novel therapeutic approach. medRxiv [Preprint]. [DOI: ]
NCT04484493 {published data only}
- Abdelalim AA, Mohamady AA, Elsayed RA, Elawady MA, Ghallab AF. Corticosteroid nasal spray for recovery of smell sensation in COVID-19 patients: a randomised controlled trial. American Journal of Otolaryngology 2021;42(2):1-6. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT04485429 {published data only}
- NCT04485429. Efficacy assessment of methylprednisolone and heparin in patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04485429 (first received 24 July 2020).
NCT04534478 {published data only}
- NCT04534478. Oral prednisone regimens to optimise the therapeutic strategy in patients with organising pneumonia post-COVID-19. clinicaltrials.gov/show/NCT04534478 (first received 1 September 2020).
NCT04551781 {unpublished data only}
- NCT04551781. Short term low dose corticosteroids for management of post COVID19 pulmonary fibrosis. clinicaltrials.gov/show/NCT04551781 (first received 16 September 2020).
NCT04561180 {published data only}
- NCT04561180. Study to evaluate the efficacy and safety of EG-HPCP-03a compared to DEX in patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04561180 (first received 23 September 2020).
NCT04569825 {published data only}
- NCT04569825. Effect of nasal steroid in the treatment of anosmia due to COVID-19 disease. clinicaltrials.gov/ct2/show/NCT04569825 (first received 30 September 2020).
NCT04640168 {published data only}
- NCT04640168. Adaptive COVID-19 treatment trial 4 (ACTT-4). clinicaltrials.gov/show/NCT04640168 (first received 23 November 2020).
NCT04657484 {published data only}
- NCT04657484. Comparison of two corticosteroid regimens for post-COVID diffuse lung disease. clinicaltrials.gov/show/NCT04657484 (first received 8 December 2020).
NCT04826822 {published data only}
- NCT04826822. Spironolactone and dexamethasone in patients hospitalised with COVID-19 (SPIDEX-II). clinicaltrials.gov/show/NCT04826822 (first received 1 April 2021).
NCT05133635 {published data only}
- NCT05133635. High-dose corticosteroid or tocilizumab for clinical worsening of COVID-19. https://clinicaltrials.gov/show/NCT05133635 (first received 11 January 2021).
Odeyemi 2021 {published data only}
- Odeyemi YE, Chalmers SJ, Barreto EF, Jentzer JC, Gajic O, Yadav H. Early, biomarker-guided steroid dosing in COVID-19 pneumonia: a pilot randomised controlled trial. Critical Care 2022;26(9):1-3. [DOI: 10.1186/s13054-021-03873-2] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
EUCTR2020‐001307‐16‐ES {published data only}
- EUCTR2020-001307-16-ES. Efficacy and safety of corticoids in patients with adult respiratory distress syndrome (ARDS) secondary to coronavirus infection. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001307-16 (first received 1 April 2020).
EUCTR2020‐001333‐13‐FR {published data only}
- EUCTR2020-001333-13-FR. Dexamethasone associated with hydroxychloroquine vs. hydroxychloroquine alone for the early treatment of severe ARDS caused by COVID-19: a randomised controlled trial. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001333-13 (first received 9 April 2020).
EUCTR2020‐001553‐48‐FR {published data only}
- EUCTR2020-001553-48-FR. Corticoids in COVID-19 viral pneumonia in infection with SARS-CoV-2 (translation by the review authors) [Corticoides au cours de la pneumonie virale COVID-19 liee a linfection par le SARS-CoV-2]. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001553-48 (first received 13 April 2020).
EUCTR2020‐002186‐34‐ES {published data only}
- EUCTR2020-002186-34-ES. Efficacy of the early use of corticotherapy in CoV-2 infection to prevent the progression of acute respiratory distress syndrome (ARDS). www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-002186-34 (first received 22 July 2020).
EUCTR2020‐004323‐16 {published data only}
- EUCTR2020-004323-16. Evaluation of the efficacy of high doses of methylprednisolone in SARS-CoV2 pneumonia patients. www.clinicaltrialsregister.eu/ctr-search/trial/2020-004323-16/IT (first received 23 November 2020).
Gautam 2021 {published data only}
- Gautam PB, Kumar A, Kannojia BL, Chaudhary R. A comparative study of the efficacy and outcome of methylprednisolone and dexamethasone in moderate to severe COVID-19 disease. Asian Journal of Medical Sciences 2021;12(12):17-22. [DOI: 10.3126/ajms.v12i12.39294] [DOI] [Google Scholar]
Ghanei 2021 {published data only}
- Ghanei M, Solaymani‑Dodaran M, Qazvini A, Ghazale AH, Setarehdan SA, Saadat SH, et al. The efficacy of corticosteroids therapy in patients with moderate to severe SARS-CoV-2 infection: a multicenter, randomized, open-label trial. Respiratory Research 2021;22(245):1-14. [DOI: 10.1186/s12931-021-01833-6] [DOI] [PMC free article] [PubMed] [Google Scholar]
IRCT20081027001411N3 {published data only}
- IRCT20081027001411N3. Effect of prednisolone on treatment of COVID-19. irct.ir/trial/46975 (first received 6 January 2020).
IRCT20120215009014N354 {published data only}
- IRCT20120215009014N354. Evaluating the effect of intravenous hydrocortisone, methylprednisolone, and dexamethasone in treatment of patients with moderate to severe acute respiratory distress syndrome caused by COVID-19. irct.ir/trial/48043 (first received 12 May 2020).
IRCT20160118026097N4 {published data only}
- IRCT20160118026097N4. The effect of dexamethasone in the treatment of high-risk COVID-19 patients. irct.ir/trial/48310 (first received 13 September 2020).
IRCT20200611047727N3 {published data only}
- IRCT20200611047727N3. Evaluation of efficacy and safety of low dose corticosteroid with severe pneumonia COVID-19. irct.ir/trial/49116 (first received 3 January 2021).
IRCT20201015049030N1 {published data only}
- IRCT20201015049030N1. Effect of dexamethasone on treatment of COVID-19. www.irct.ir/trial/51736 (first received 7 November 2020).
ISRCTN33037282 {published data only}
- ISRCTN33037282. Comparing two medications (dexamethasone and methylprednisolone high dose) for the treatment of pneumonia in patients with COVID-19. www.isrctn.com/ISRCTN33037282 (first received 26 November 2020).
Montalvan 2021 {published data only}
- Montalvan E, Carcamo B, Palacion D, Rivera S, Estevez R, Norwood D, et al. High-dose vs low-dose dexamethasone in patients with COVID-19 in a tertiary hospital in Western Honduras. Chest 2021;160(4):A1117-8. [DOI: 10.1016/j.chest.2021.07.1027] [DOI] [Google Scholar]
NCT04244591 {published data only}
- NCT04244591. Glucocorticoid therapy for novel coronavirus critically ill patients with severe acute respiratory failure. www.clinicaltrials.gov/ct2/show/NCT04244591 (first received 28 January 2020).
NCT04325061 {published data only}
- NCT04325061. Efficacy of dexamethasone treatment for patients with ARDS caused by COVID-19. clinicaltrials.gov/ct2/show/NCT04325061 (first received 27 March 2020).
NCT04347980 {published data only}
- NCT04347980. Dexamethasone treatment for severe acute respiratory distress syndrome. clinicaltrials.gov/show/NCT04347980 (first received 15 April 2020).
NCT04438980 {published data only}
- Les Bujanda I, Loureiro-Amigo J, Capdevila Bastons F, Elejalde Guerra I, Anniccherico Sánchez J, Murgadella-Sancho A, et al. Treatment of COVID-19 pneumonia with glucocorticoids (CORTIVID): a structured summary of a study protocol for a randomised controlled trial. Trials 2021;22(1):43. [DOI: 10.1186/s13063-020-04999-4] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT04438980. Glucocorticoids in COVID-19 (CORTIVID). clinicaltrials.gov/show/NCT04438980 (first received 19 June 2020).
NCT04451174 {published data only}
- NCT04451174. Early use of corticosteroids in hospitalised patients with moderate COVID19 pneumonia. clinicaltrials.gov/show/NCT04451174 (first received 30 June 2020).
- Salinas M, Andino P, Palma L, Valencia J, Figueroa E, Ortega J. Early use of corticosteroids in non-critical patients with COVID-19 pneumonia (PREDCOVID): a structured summary of a study protocol for a randomised controlled trial. Trials 2021;22(1):92. [DOI: 10.1186/s13063-021-05046-6.] [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT04530409 {published data only}
- NCT04530409. Timing of corticosteroids in COVID-19. clinicaltrials.gov/show/NCT04530409 (first received 28 August 2020).
NCT04746430 {published data only}
- NCT04746430. COVID-19 primary care platform for early treatment and recovery (COPPER) study. clinicaltrials.gov/show/NCT04746430 (first received 9 February 2021).
Rashad 2021 {published data only (unpublished sought but not used)}
- NCT04519385. Tocilizumab versus dexamethasone in severe COVID19 cases. clinicaltrials.gov/show/NCT04519385 (first received 19 August 2020).
- Rashad A, Mousa S, Nafady‑Hego H, Nafady A, Elgendy H. Short term survival of critically ill COVID‑19 Egyptian patients on assisted ventilation treated by either dexamethasone or tocilizumab. Scientific Reports 2021;11(8816):1-7. [DOI: 10.1038/s41598-021-88086-x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Salukhov 2021 {published data only}
- Salukhov VV, Kryukov EV, Chugunov AA, Kharitonov MA, Rudakov YV, Lakhin RE, et al. The role and place of glucocorticosteroids in treatment of COVID-19 pneumonia without hypoxemia [Роль и место глюкокортикостероидов в терапии пневмоний, вызванных COVID-19, без гипоксемии]. Meditsinskiy Sovet = Medical Council 2021;16(60):162-72. [DOI: 10.21518/2079- 701X-2021-12-162-172] [Google Scholar]
References to ongoing studies
ACTRN12621001200875 {published data only}
- ACTRN12621001200875. A randomised controlled trial of dexamethasone for emergency and life-threatening admissions due to COVID-19 in virtual care: the DELTA study. http://www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12621001200875 (first received 8 September 2021).
ACTRN12621001603808 {published data only}
- ACTRN12621001603808. The effect of prednisolone vs dexamethasone on Covid-19 in pregnancy: an open labelled randomised control trial. https://trialsearch.who.int/Trial2.aspx?TrialID=ACTRN12621001603808 (first received 24 November 2021).
ChiCTR2000029386 {published data only}
- Qin YY, Zhou YH, Lu YQ, Sun F, Yang S, Harypursat V, et al. Effectiveness of glucocorticoid therapy in patients with severe novel coronavirus pneumonia: protocol of a randomised controlled trial. Chinese Medical Journal 2020;133(9):1080-6. [DOI: 10.1097/CM9.0000000000000791] [ChiCTR2000029386] [DOI] [PMC free article] [PubMed]
ChiCTR2000029656 {published data only}
- ChiCTR2000029656. A randomised, open-label study to evaluate the efficacy and safety of low-dose corticosteroids in hospitalised patients with novel coronavirus pneumonia (COVID-19). www.chictr.org.cn/showprojen.aspx?proj=49086 (first received 9 February 2020).
ChiCTR2000030481 {published data only}
- ChiCTR2000030481. The clinical value of corticosteroid therapy timing in the treatment of novel coronavirus pneumonia (COVID-19): a prospective randomised controlled trial. www.chictr.org.cn/showprojen.aspx?proj=50453 (first received 3 March 2020).
CTRI/2020/07/026608 {published data only}
- CTRI/2020/07/026608. A clinical trial to study the effects of two drugs methylprednisolone and dexamethasone in patients with severe COVID-19. www.ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=45638 (first received 15 July 2020).
CTRI/2020/12/029894 {published data only}
- Comparing the effectiveness of dexamethasone versus methylprednisolone in patients with moderate COVID 19 - a randomised controlled trial. ctri.nic.in/Clinicaltrials/showallp.php?mid1=49273&EncHid=&userName=029894 (first received 18 December 2020).
- CTRI/2020/12/029894. A study to compare the effectiveness of two drugs, dexamethasone versus methylprednisolone in the treatment of moderate Covid 19 patients. www.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2020/12/029894.
CTRI/2020/12/030143 {published data only}
- CTRI/2020/12/030143. Comparison of different steroid regimes in critically ill adult patients of COVID-19. www.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2020/12/030143.
- CTRI/2020/12/030143. Evaluation of different steroid regimes in critically ill adult patients of COVID-19 admitted to intensive care units. ctri.nic.in/Clinicaltrials/showallp.php?mid1=50886&EncHid=&userName=30143 (first received 31 December 2020).
CTRI/2021/05/033873 {published data only}
- CTRI/2021/05/033873. Pre-emptive steroids to alter the disease course in COVID-19 patients. http://www.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2021/05/033873 (first received: 31 May 2021).
CTRI/2021/08/035822 {published data only}
- CTRI/2021/08/035822. Assessment of doubling dose of dexamethasone in progressively worsening severe COVID-19 pneumonia - a randomised controlled trial. http://www.ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=57048 (first received 19 August 2021).
EUCTR2020‐001413‐20‐ES {published data only}
- EUCTR2020-001413-20-ES. Efficacy and safety of siltuximab vs. corticosteroids in hospitalized patients with COVID-19 pneumonia. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001413-20 (first received 7 April 2020).
EUCTR2020‐001457‐43‐FR {published data only}
- EUCTR2020-001457-43-FR. Dexamethasone and oxygen support strategies in ICU patients with COVID-19 pneumonia. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001457-43 (first received 10 April 2020).
EUCTR2020‐001622‐64‐ES {published data only}
- EUCTR2020-001622-64-ES. Outpatient treatment of COVID-19 with early pulmonary corticosteroids as an opportunity to modify the course of the disease. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001622-64 (first received 19 April 2020).
- Saiz-Rodríguez M, Peña T, Lázaro L, González A, Martínez A, Cordero JA, et al. Outpatient treatment of COVID-19 with steroids in the phase of mild pneumonia without the need for admission as an opportunity to modify the course of the disease: a structured summary of a randomised controlled trial. Trials 2020;21(632):1-3. [DOI: 10.1186/s13063-020-04575-w] [DOI] [PMC free article] [PubMed] [Google Scholar]
EUCTR2020‐001707‐16‐ES {published data only}
- EUCTR2020-001707-16-ES. Phase III randomised, unicentric open, controlled clinical trial to demonstrate the effectiveness of tocilizumab against systemic corticotherapy in patients entered by COVID-19 with bilateral pneumonia and bad evolution. www.clinicaltrialsregister.eu/ctr-search/trial/2020-001707-16/ES (first received 25 June 2020).
EUCTR2020‐001921‐30 {published data only}
- Busani S, Tosi M, Mighali P, Vandelli P, D'Amico R, Marietta M, et al. Multi-centre, three arm, randomised controlled trial on the use of methylprednisolone and unfractionated heparin in critically ill ventilated patients with pneumonia from SARS-CoV-2 infection: a structured summary of a study protocol for a randomised controlled trial. Trials 2020;21(1):724. [DOI: 10.1186/s13063-020-04645-z] [DOI] [PMC free article] [PubMed] [Google Scholar]
- EUCTR2020-001921-30. Steroids and unfractionated heparin in critically-ill patients with pneumonia from COVID-19 infection. A multicenter, interventional, randomised, three arms study design. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001921-30 (first received 26 June 2020).
EUCTR2020‐003363‐25‐DK {published data only}
- EUCTR2020-003363-25-DK. Higher vs. lower doses of dexamethasone in patients with COVID-19 and severe oxygen deficiency: the COVID STEROID 2 trial. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-003363-25 (first received 18 August 2020).
EUCTR2020‐006054‐43‐IT {published data only}
- EUCTR2020-006054-43-IT. Randomised controlled trial to evaluate the efficacy of per-protocol administration of methylprednisolone compared to dexamethasone in SARS-CoV-2 infections requiring respiratory support. http://www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2020-006054-43-IT (first received 22 March 2021).
EUCTR2021‐001416‐29‐ES {published data only}
- EUCTR2021-001416-29-ES. High-dose dexamethasone treatment for SARS-COV-2. http://www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2021-001416-29-ES (first received 26 May 2021).
EUCTR2021‐004021‐71 {published data only}
- EUCTR2021-004021-71. Corticosteroids for loss of smell by COVID-19 infection – COCOS trial. https://www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2021-004021-71 (first received 12 October 2021).
IRCT20190606043826N2 {published data only}
- IRCT20190606043826N2. Comparison of the effectiveness and complication of dexamethasone at doses of 8 and 24 mg in the treatment of in hospitalised patients with Covid-19. http://www.who.int/trialsearch/Trial2.aspx?TrialID=IRCT20190606043826N2 (first received 1 July 2021).
NCT04329650 {published data only}
- NCT04329650. Efficacy and safety of siltuximab vs. corticosteroids in hospitalised patients with COVID19 pneumonia. clinicaltrials.gov/show/NCT04329650 (first received 1 April 2020).
NCT04344730 {published data only}
- NCT04344730. Dexamethasone and oxygen support strategies in ICU patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04344730 (first received 14 April 2020).
NCT04345445 {published data only}
- NCT04345445. Study to evaluate the efficacy and safety of tocilizumab versus corticosteroids in hospitalised COVID-19 patients with high risk of progression. clinicaltrials.gov/show/NCT04345445 (first received 14 April 2020).
NCT04377503 {published data only}
- NCT04377503. Tocilizumab versus methylprednisolone in the cytokine release syndrome of patients with COVID-19. clinicaltrials.gov/show/NCT04377503 (first received 6 May 2020).
NCT04452565 {published data only}
- NCT04452565. NA-831, atazanavir and dexamethasone in the treatment of SARSCov-2 infection (NATADEX). clinicaltrials.gov/show/NCT04452565 (first received 30 June 2020).
NCT04499313 {published data only}
- NCT04499313. Dexamethasone versus methylprednisolone for the treatment of patients with ARDS caused by COVID-19. clinicaltrials.gov/show/NCT04499313 (first received 5 August 2020).
NCT04509973 {published data only}
- Munch MW, Granholm A, Myatra SN, Vijayaraghavan BK, Cronhjort M, Wahlin RR, et al. Higher vs. lower doses of dexamethasone in patients with COVID-19 and severe hypoxia (COVID STEROID 2) trial: protocol and statistical analysis plan. Acta Anaesthesiologica Scandinavica 2021;00:1-12. [DOI: 10.1111/aas.13795] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT04509973. Higher vs. lower doses of dexamethasone for COVID-19 and severe hypoxia. clinicaltrials.gov/show/NCT04509973 (first received 12 August 2020).
NCT04513184 {published data only}
- NCT04513184. Randomised clinical trial of nasal dexamethasone as an adjuvant in patients with COVID-19. clinicaltrials.gov/show/NCT04513184 (first received 14 August 2020).
NCT04528329 {published data only}
- NCT04528329. Anosmia and / or ageusia and early corticosteroid use. clinicaltrials.gov/show/NCT04528329 (first received 27 August 2020).
NCT04528888 {published data only}
- NCT04528888. Steroids and unfractionated heparin in critically ill patients with pneumonia from COVID-19 infection. clinicaltrials.gov/show/NCT04528888 (first received 27 August 2020). [EUDRA-CT: https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-001921-30/IT] [NCT: https://clinicaltrials.gov/ct2/show/study/NCT04528888]
NCT04545242 {published data only}
- NCT04545242. Efficacy of dexamethasone in patients with acute hypoxemic respiratory failure caused by infections. clinicaltrials.gov/show/NCT04545242 (first received 10 September 2020).
NCT04636671 {published data only}
- NCT04636671. Methylprednisolone vs. dexamethasone in COVID-19 pneumonia (MEDEAS RCT). clinicaltrials.gov/show/NCT04636671 (first received 19 November 2020).
NCT04663555 {published data only}
- NCT04663555. Effect of two different doses of dexamethasone in patients with ARDS and COVID-19. clinicaltrials.gov/show/NCT04663555 (first received 11 December 2020).
NCT04673162 {published data only}
- NCT04673162. Evaluation of the efficacy of high doses of methylprednisolone in SARS-CoV2 (COVID-19) pneumonia patients. clinicaltrials.gov/show/NCT04673162 (first received 17 December 2020).
NCT04707534 {published data only}
- NCT04707534. Dexamethasone for COVID-19. clinicaltrials.gov/show/NCT04707534 (first received 13 January 2021).
NCT04765371 {published data only}
- NCT04765371. Comparison between prednisolone and dexamethasone on mortality in patients on oxygen therapy, with COVID-19. clinicaltrials.gov/ct2/show/NCT04765371 (first received 21 February 2021).
NCT04780581 {published data only}
- NCT04780581. Glucocorticoid therapy in coronavirus disease COVID-19 patients. clinicaltrials.gov/show/NCT04780581 (first received 3 March 2021).
NCT04795583 {published data only}
- NCT04795583. Corticosteroids for COVID-19. clinicaltrials.gov/show/NCT04795583 (first received 12 March 2021).
NCT04834375 {published data only}
- NCT04834375. Randomised open investigation determining steroid dose. clinicaltrials.gov/show/NCT04834375 (first received 8 April 2021).
NCT04836780 {published data only}
- NCT04836780. Dexamethasone early administration in hospitalised patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04836780 (first received 8 April 2021).
NCT04860518 {published data only}
- NCT04860518. Human intravenous interferon beta-Ia safety and preliminary efficacy in hospitalised subjects with coronavirus (HIBISCUS). https://clinicaltrials.gov/ct2/show/NCT04860518 (first received 22 April 2021).
TCTR20211017001 {published data only}
- TCTR20211017001. A comparative study of the effectiveness between pulse regimen methylprednisolone versus high dose dexamethasone as the initial treatment of moderate Covid-19 pneumonia: an open-label randomised controlled trial. http://www.thaiclinicaltrials.org/show/TCTR20211017001 (first received 17 October 2021).
Additional references
Aaranjani 2021
- Aranjani JM, Manuel A, Abdul Razack HI, Mathew ST. COVID-19–associated mucormycosis: evidence-based critical review of an emerging infection burden during the pandemic’s second wave in India. PLOS Neglected Tropical Diseases 2021;15(11):e0009921. [DOI: 10.1371/journal.pntd.0009921] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ahrenfeldt 2020
- Ahrenfeldt LJ, Otavova M, Christensen K, Lindahl-Jacobsen R. Sex and age differences in COVID-19 mortality in Europe. Wiener Klinische Wochenschrift 2021;133:393-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Aldridge 2020
- Aldridge RW, Lewer D, Katikireddi SV, Mathur R, Pathak N, Burns R, et al. Black, Asian and Minority Ethnic groups in England are at increased risk of death from COVID-19: indirect standardisation of NHS mortality data. Wellcome Open Research 2020;5(88):1-20. [DOI: 10.12688/wellcomeopenres.15922.2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Alessi 2020
- Alessi J, Oliveira GB, Schaan BD, Telo GH. Dexamethasone in the era of COVID-19: friend or foe? An essay on the effects of dexamethasone and the potential risks of its inadvertent use in patients with diabetes. Diabetology and Metabolic Syndrome 2020;12(80):1-11. [DOI: 10.1186/s13098-020-00583-7] [DOI] [PMC free article] [PubMed] [Google Scholar]
Allen 2017
- Allen L, Cobiac L, Townsend N. Quantifying the global distribution of premature mortality from non-communicable diseases. Journal of Public Health December 2017;49(4):698–703. [DOI: ] [DOI] [PubMed] [Google Scholar]
Ansems 2021
- Ansems K, Grundeis F, Dahms K, Mikolajewska A, Thieme V, Piechotta V, et al. Remdesivir for the treatment of COVID-19. Cochrane Database of Systematic Reviews 2021, Issue 8. Art. No: CD014962. [DOI: 10.1002/14651858.CD014962] [DOI] [PMC free article] [PubMed] [Google Scholar]
Aw 2007
- Aw, D, Silva AB, Palmer DB. Immunosenescence: emerging challenges for an ageing population. Immunology 2007;120(4):435-46. [DOI: 10.1111/j.1365-2567.2007.02555.x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Baqui 2020
- Baqui P, Bica I, Marra V, Ercole A, Schaar M. Ethnic and regional variations in hospital mortality from COVID-19 in Brazil: a cross-sectional observational study. Lancet Global Health 2020;8(8):e1018-e26. [DOI: 10.1016/S2214-109X(20)30285-0] [DOI] [PMC free article] [PubMed] [Google Scholar]
Barnes 2006
- Barnes PJ. How corticosteroids control inflammation: quintiles prize lecture. British Journal of Pharmacology 2005;148(3):245-54. [DOI: 10.1038/sj.bjp.0706736] [DOI] [PMC free article] [PubMed] [Google Scholar]
Barros 2021
- Barros CMSS, Freire RS, Frota E, Santos AGR, Farias MAL, Rodrigues MGA, et al. Short-course of methylprednisolone improves respiratory functional parameters after 120 days in hospitalised COVID-19 patients (Metcovid Trial): a randomised clinical trial. Frontiers in Medicine 2021;8(758405):1-9. [DOI: 10.3389/fmed.2021.758405] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bhanuprasad 2021
- Bhanuprasad K, Manesh A, Devasagayam E, Varghese L, Cherian LM, Kurien R, et al. Risk factors associated with the mucormycosis epidemic during the COVID-19 pandemic. International Journal of Infectious Diseases 2021;111:267-70. [DOI: 10.1016/j.ijid.2021.08.037] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bourdeau 2003
- Bourdeau I, Stratakis CA. Glucocorticoids, Pharmacology of. In: Henry H, Norman A, editors(s). Encyclopedia of Hormones. Cambridge, MA: Academic Press, 2003:142-50. [DOI: ] [Google Scholar]
Brandal 2021
- Brandal LT, MacDonald E, Veneti L, Ravlo T, Lange H, Naseer U, et al. Outbreak caused by the SARS-CoV-2 Omicron variant in Norway, November to December 2021. European Surveillance 2021;26(50):2101147. [DOI: 10.2807/1560-7917.ES.2021.26.50.2101147] [DOI] [PMC free article] [PubMed] [Google Scholar]
Brock 2011
- Brock GN, Barnes C, Ramirez JA, Myers J. How to handle mortality when investigating length of hospital stay and time to clinical stability. BMC Medical Research Methodology 2011;11:144. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Buitrago‐Garcia 2020
- Buitrago-Garcia D, Egli-Gany D, Counotte MJ, Hossmann S, Imeri H, Ipekci Aziz M, et al. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: a living systematic review and meta-analysis. PLOS Medicine 2020;17(9):e1003346. [DOI] [PMC free article] [PubMed] [Google Scholar]
Caughey 2013
- Caughey GE, Preiss AK, Vitry AI, Gilbert AL, Roughead EE. Comorbid diabetes and COPD: impact of corticosteroid use on diabetes complications. Diabetes Care 2013;36(10):3009-14. [DOI: 10.2337/dc12-2197] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chaudhuri 2021
- Chaudhuri D, Sasaki K, Karkar A, Sharif S, Lewis K, Mammen MJ, et al. Corticosteroids in COVID-19 and non-COVID-19 ARDS: a systematic review and meta-analysis. Intensive Care Medicine 2021;47:521–37. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chen 2021
- Chen S, Prettner K, Kuhn M, Geldsetzer P, Wang C, Bärnighausen T, et al. Climate and the spread of COVID-19. Scientific Reports 2021;11(1):9042. [DOI: 10.1038/s41598-021-87692-z] [DOI] [PMC free article] [PubMed] [Google Scholar]
Columbia Public Health 2021
- Competing Risk Analysis. Columbia University Mailman School of Public Health Website. Available from www.publichealth.columbia.edu/research/population-health-methods/competing-risk-analysis (accessed 13 July 2021). [ACCESSED JULY 13 2021: https://www.publichealth.columbia.edu/research/population-health-methods/competing-risk-analysis]
COMET 2020
- Core outcome set developers’ response to COVID-19. www.comet-initiative.org/Studies/Details/1538 (accessed 2 November 2020).
Deeks 2022
- Deeks JJ, Higgins JP, Altman DG, editor(s). Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook.
El‐Kebbi 2021
- El-Kebbi IM, Bidikian NH, Hneiny L, Nasrallah MP. Epidemiology of type 2 diabetes in the Middle East and North Africa: challenges and call for action. World Journal of Diabetes 2021;12(9):1401-25. [DOI: 10.4239/wjd.v12.i9.1401] [DOI] [PMC free article] [PubMed] [Google Scholar]
EMA 2022
- European Medicines Agency (EMA). COVID-19 treatments. Available at: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/covid-19-treatments (accessed 12 December 2021).
FDA 2022
- FDA US Food & Drug Administration. Coronavirus Disease 2019 (COVID-19). Available at: https://www.fda.gov/emergency-preparedness-and-response/counterterrorism-and-emerging-threats/coronavirus-disease-2019-covid-19 (accessed 12 December 2021). [PubMed]
Ferguson 2021
- Ferguson N, Ghani A, Hinsley W, Volz E. Hospitalisation risk for Omicron cases in England. Imperial College London 2021;www.gov.uk:1-12. [DOI: 10.25561/93035] [DOI]
Funk 2021
- Funk T, Pharris A, Spiteri G, Bundle N, Melidou A, Carr M, et al. Characteristics of SARS-CoV-2 variants of concern B.1.1.7, B.1.351 or P.1: data from seven EU/EEA countries, weeks 38/2020 to 10/2021. Eurosurveillance 2021;26(16):2100348. [DOI: 10.2807/1560-7917.ES.2021.26.16.2100348] [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- GRADEpro GDT. Hamilton (ON): McMaster University (developed by Evidence Prime), accessed 18 July 2021. Available at gradepro.org.
Griesel 2022
- Griesel M, Wagner C, Mikolajewska A, Stegemann M, Fichtner F, Metzendorf MI, et al. Inhaled corticosteroids for the treatment of COVID-19. Cochrane Database of Systematic Reviews 2022, Issue 3. Art. No: CD015125. [DOI: 10.1002/14651858.CD015125] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2019
- Higgins JP, Savovic J, Page MJ, Sterne JA. Revised Cochrane risk-of-bias tool for randomized trials (RoB 2). www.riskofbias.info/welcome/rob-2-0-tool/current-version-of-rob-2 (accessed 7 July 2021).
Higgins 2022
- Higgins JP, Lasserson T, Chandler J, Tovey D, Thomas J, Flemyng E, et al. Methodological expectations of Cochrane intervention reviews. www.community.cochrane.org/mecir-manual/ (accessed 6 January 2022).
Higgins 2022a
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from: training.cochrane.org/handbook 2022.
Higgins 2022b
- Higgins JP, Savović J, Page MJ, Elbers RG, Sterne JA. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook.
Higgins 2022c
- Higgins J, Eldridge S, Li T. Chapter 23: Including variants on randomised trials. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 202s). Cochrane, 2022. Available from training.cochrane.org/handbook.
Higgins 2022d
- Higgins JP, Li T, Deeks JJ, editor(s). Chapter 6: Choosing effect measures and computing estimates of effect. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook.
Hoenigl 2022
- Hoenigl M, Seidel D, Carvalho A, Rudramurthy SM, Arastehfar A, Gangneux JP, et al. The emergence of COVID-19 associated mucormycosis: a review of cases from 18 countries. Lancet Microbe 2022;21:00237-8. [DOI: 10.1016/S2666-5247(21)00237-8] [DOI] [PMC free article] [PubMed] [Google Scholar]
Huang 2020
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020;395(10223):497-506. [DOI: 10.1016/S0140-6736(20)30183-5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Johns Hopkins University 2022
- Johns Hopkins University. Mortality analyses. coronavirus.jhu.edu/data/mortality (accessed 4 April 2022).
Kluge 2022
- Kluge S, Janssens U, Welte T, Weber-Carstens S, Schälte G, Spinner CD, et al. S3 Guideline – recommendations for inpatient therapy of patients with COVID-19 [S3-Leitlinie – Empfehlungen zur stationären Therapie von Patienten mit COVID-19]. www.awmf.org/uploads/tx_szleitlinien/113-001LGl_S3_Empfehlungen-zur-stationaeren-Therapie-von-Patienten-mit-COVID-19_2022-03.pdf (accessed 7 April 2022). [DOI] [PubMed]
Kreuzberger 2021
- Kreuzberger N, Hirsch C, Chai KL, Tomlinson E, Khosravi Z, Popp M, et al. SARS‐CoV‐2‐neutralising monoclonal antibodies for treatment of COVID‐19. Cochrane Database of Systematic Reviews 2021, Issue 9. Art. No: CD013825. [DOI: 10.1002/14651858.CD013825] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lauer 2020
- Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, Meredith HR, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Annals of Internal Medicine 2020;172(9):577–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lewnard 2022
- Lewnard JA, Hong VX, Patel MM, Kahn R, Lipsitch M, Tartof SY. Clinical outcomes among patients infected with Omicron (B.1.1.529) SARS-CoV-2 variant in southern California. Preprint server MedRxiv 2022. [DOI: 10.1101/2022.01.11.22269045] [DOI] [PMC free article] [PubMed]
Li 2021
- Li T, Higgins JP, Deeks JJ (editors). Chapter 5: Collecting data. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 6.1 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook.
Liang 2020
- Liang W, Guan W, Chen R, Wang W, Li J, Xu K, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncology 2020;21(3):335-7. [DOI: 10.1016/S1470-2045(20)30096-6] [DOI] [PMC free article] [PubMed] [Google Scholar]
Liu 2021
- Liu Z, Zhu L, Wang X, Zhou Z, Guo Y. The correlation between COVID-19 activities and climate factors in different climate types areas. Journal of Occupational and Environmental Medicine 2021;63(8):e-533-41. [DOI: DOI: 10.1097/JOM.0000000000002274] [DOI] [PMC free article] [PubMed] [Google Scholar]
Living Evidence Network 2019
- Living Evidence Network. Guidance for the production and publication of Cochrane living systematic reviews: Cochrane Reviews in living mode (Version December 2019). Available from community.cochrane.org/review-production/production-resources/living-systematic-reviews (accessed 22 March 2021).
Marshall 2020
- Marshall JC, Murthy S, Diaz J, Adhikari NK, Angus DC, Arabi YM, et al. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infectious Diseases 2020;20(8):e192-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mathur 2021
- Mathur R, Rentsch CT, Morton CE, Hulme WJ, Schultze A, MacKenna B, et al. Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: an observational cohort study using the OpenSAFELY platform. Lancet 2021;397(10286):1711-24. [DOI: 10.1016/S0140-6736(21)00634-6] [DOI] [PMC free article] [PubMed] [Google Scholar]
Microsoft 2018 [Computer program]
- Microsoft Excel. Microsoft Corporation. Microsoft Corporation, 2018. office.microsoft.com/excel.
Mikolajewska 2021
- Mikolajewska A, Fischer AL, Piechotta V, Mueller A, Metzendorf MI, Becker M, et al. Colchicine for the treatment of COVID-19. Cochrane Database of Systematic Reviews 2021, Issue 10. Art. No: CD015045. [DOI: 10.1002/14651858.CD015045] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Journal of Clinical Epidemiology 2009;62(10):1006-12. [DOI] [PubMed] [Google Scholar]
Morales 2021
- Morales D, Ali SN. COVID-19 and disparities affecting ethnic minorities. Lancet 2021;397(10286):1684-5. [DOI: 10.1016/S0140-6736(21)00949-1] [DOI] [PMC free article] [PubMed] [Google Scholar]
Navar 2021
- Navar AM, Purinton SN, Hou Q, Taylor RJ, Peterson ED. The impact of race and ethnicity on outcomes in 19,584 adults hospitalised with COVID-19. PLOS One 2021;16(7):e0254809. [DOI] [PMC free article] [PubMed] [Google Scholar]
NICE 2021
- NICE. COVID-19 rapid guideline: managing COVID-19. https://www.nice.org.uk/guidance/ng191/resources/covid19-rapid-guideline-managing-covid19-pdf-51035553326.
NIH 2021
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available at https://www.covid19treatmentguidelines.nih.gov/. [PubMed]
Oke 2020
- Oke J, Heneghan C. Global Covid-19 case fatality rates. https://www.cebm.net/covid-19/global-covid-19-case-fatality-rates/ (accessed 17 August 2022).
Oran 2020
- Oran DP, Topol EJ. Prevalence of Asymptomatic SARS-CoV-2 Infection. Annals of Internal Medicine 2020;173(5):362-7. [DOI: 10.7326/M20-3012] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ouzzani 2016
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan — a web and mobile app for systematic reviews. Systematic Reviews 2016;5(1):210. [DOI: 10.1186/s13643-016-0384-4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Park 2020
- Park JJ, Harari O, Dron L, Lester RT, Thorlund K, Mills EJ. An overview of platform trials with a checklist for clinical readers. Journal of Clinical Epidemiology 2020;125:1-8. [DOI: 10.1016/j.jclinepi.2020.04.025] [DOI] [PubMed] [Google Scholar]
Parmar 1998
- Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17(24):2815-34. [DOI] [PubMed] [Google Scholar]
Pasin 2021
- Pasin L, Navalesi P, Zangrillo A, Kuzovlev A, Likhvantsev V, Hajjar LA, et al. Corticosteroids for patients with coronavirus disease 2019 (COVID-19) with different disease severity: a meta-analysis of randomized clinical trials. Journal of Cardiothoracic and Vascular Anesthesia 2021;35(2):578-84. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Piechotta 2021
- Piechotta V, Iannizzi C, Chai KL, Valk SJ, Kimber C, Dorando E, et al. Convalescent plasma or hyperimmune immunoglobulin for people with COVID‐19: a living systematic review. Cochrane Database of Systematic Reviews 2021, Issue 5. Art. No: CD013600. [DOI: 10.1002/14651858.CD013600.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Potere 2020
- Potere N, Valeriani E, Candeloro M, Tana M, Porreca E, Abbate A, et al. A higher mortality rate and long ventilation times differentiate COVID-19 from severe respiratory infections in flu waves [Eine höhere Letalität und lange Beatmungsdauer unterscheiden COVID-19 von schwer verlaufenden Atemwegsinfektionen in Grippewellen]. Critical Care 2020;24(1):389. [DOI: 10.25646/7111] [DOI] [PMC free article] [PubMed] [Google Scholar]
Prakash 2019
- Prakash H, Chakrabarti A. Global epidemiology of mucormycosis. Journal of Fungi 2019;5(1):26. [DOI: 10.3390/jof5010026] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ramachandran 2012
- Ramachandran A, Snehalatha C, Shetty AS, Nanditha A. Trends in prevalence of diabetes in Asian countries. World Journal of Diabetes 2012;3(6):110-7. [DOI: 10.4239/wjd.v3.i6.110] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ramanan 2022
- Ramanan M, Tong SYC, Kumar A, Venkatesh B. Geographical representation of low- and middle-income countries in randomized clinical trials for COVID-19. JAMA Network Open 2022;5(2):e220444. [PMID: 10.1001/jamanetworkopen.2022.0444] [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan Web 2019 [Computer program]
- Review Manager Web (RevMan Web). The Cochrane Collaboration, 2019. revman.cochrane.org.
Rhen 2005
- Rhen T, Cidlowski JA. Antiinflammatory action of glucocorticoids - new mechanisms for old drugs. New England Journal of Medicine 2005;353(16):1711-23. [DOI: 10.1056/NEJMra050541] [DOI] [PubMed] [Google Scholar]
Rochwerg 2018
- Rochwerg B, Oczkowski SJ, Siemieniuk RA, Agoritsas T, Belley-Cote E, D'Aragon F, et al. Corticosteroids in sepsis: an updated systematic review and meta-analysis. Critical Care Medicine 2018;46(9):1411-20. [PMID: ] [DOI] [PubMed] [Google Scholar]
Santesso 2020
- Santesso N, Glenton C, Dahm P, Garner P, Akl A, Alper B, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. Journal of Clinical Epidemiology 2020;119:126-35. [DOI] [PubMed] [Google Scholar]
Schreiber 2014
- Schreiber MP, Colantuoni E, Bienvenu OJ, Neufeld KJ, Chen KF, Shanholtz C, et al. Corticosteroids and transition to delirium in patients with acute lung injury. Critical Care Medicine 2014;42(6):1480-6. [DOI: 10.1097/CCM.0000000000000247] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schulte‐Schrepping 2020
- Schulte-Schrepping J, Reusch N, Paclik D, Baßler K, Schlickeiser S, Zhang B, et al. Severe COVID-19 is marked by a dysregulated myeloid cell compartment. Cell 2020;182(6):1419-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schünemann 2021
- Schünemann HJ, Higgins JP, Vist GE, Glasziou P, Akl EA, Skoetz N, et al. Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). Cochrane, 2021. Available from www.training.cochrane.org/handbook.
Siemieniuk 2020
- Siemieniuk RA, Bartoszko JJ, Ge L, Zeraatkar D, Izcovich A, Kum E, et al. Drug treatments for COVID-19: living systematic review and network meta-analysis. BMJ 2020;370:m2980. [BMJ: https://www.bmj.com/content/370/bmj.m2980] [DOI] [PMC free article] [PubMed] [Google Scholar]
Skoetz 2020
- Skoetz N, Goldkuhle M, Van Dalen EC, Akl EA, Trivella M, Mustafa RA, et al. GRADE guidelines 27: how to calculate absolute effects for time-to-event outcomes in summary of findings tables and evidence profiles. Journal of Clinical Epidemiology 2020;118:124-31. [DOI] [PubMed] [Google Scholar]
Sterne 2019
- Sterne JA, Savovic J, Page MJ, Elbers RG, Blencowe N, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:l4898. [DOI] [PubMed] [Google Scholar]
Sterne 2020
- Sterne JA. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA 2020;324(13):1330-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stoelting 2006
- Stoelting RK, Hiller SC (editors). Pharmacology. In: Pharmacology & Physiology in Anesthetic Practice. 4 edition. Philadelphia: Lippincott Williams & Wilkins, 2006:462. [Google Scholar]
Struyf 2020
- Struyf T, Deeks JJ, Dinnes J, Takwoingi Y, Davenport C, Leeflang MM, et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database of Systematic Reviews 2020, Issue 7. Art. No: CD013665. [DOI: 10.1002/14651858.CD013665] [DOI] [PMC free article] [PubMed] [Google Scholar]
Taves 2011
- Taves MD, Gomez-Sanchez CE, Soma KK. Extra-adrenal glucocorticoids and mineralocorticoids: evidence for local synthesis, regulation and function. American Journal of Physiology - Endocrinology and Metabolism 2011;301(1):E11-24. [DOI: 10.1152/ajpendo.00100.2011] [DOI] [PMC free article] [PubMed] [Google Scholar]
Thibeault 2021
- Thibeault C, Mühlemann B, Helbig ET, Mittermaier M, Lingscheid T, Tober-Lau P, et al. Clinical and virological characteristics of hospitalised COVID-19 patients in a German tertiary care centre during the first wave of the SARS-CoV-2 pandemic: a prospective observational study. Infection 2021;49(4):703-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tierney 2007
- Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007;8:16. [DOI: 10.1186/1745-6215-8-16] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tomlinson 2021
- Tomlinson E, Petkovic J, Welch V, Tugwell P. It's time to increase the global relevance of Cochrane Reviews by applying an ‘equity lens’. Cochrane Database of Systematic Reviews 2021;8. [DOI: ] [DOI] [PMC free article] [PubMed]
Van Paassen 2020
- Van Paassen J, Vos JS, Hoekstra EM, Neumann KM, Boot PC, Arbous SM. Corticosteroid use in COVID-19 patients: a systematic review and meta-analysis on clinical outcomes. Critical Care 2020;24(696):1-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Villar 2020
- Villar J, Ferrando C, Martínez D, Ambrós A, Muñoz T, Soler JA, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respiratory Medicine 2020;8(3):267-76. [DOI] [PubMed] [Google Scholar]
Waljee 2017
- Waljee AK, Rogers MAM, Lin P, Singal AG, Stein JD, Marks RM, et al. Short term use of oral corticosteroids and related harms among adults in the United States: population based cohort study. BMJ 2017;357(j1415):1-8. [DOI: 10.1136/bmj.j1415] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wan 2021
- Wan YI, Robbins AJ, Apea VJ, Orkin CM, Pearse RM, Puthucheary ZA, et al. Ethnicity and acute hospital admissions: multi-center analysis of routine hospital data. EClinicalMedicine 2021;39:101077. [DOI: 10.1016/j.eclinm.2021.101077] [DOI] [PMC free article] [PubMed] [Google Scholar]
Watson 2022
- Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infectous Diseases 2022;22(9):1293-302. [DOI: 10.1016/S1473-3099(22)00320-6] [DOI] [PMC free article] [PubMed] [Google Scholar]
Welch 2012
- Welch V, Petticrew M, Tugwell P, Moher D, O'Neill J, Waters E, et al. PRISMA-equity 2012 extension: reporting guidelines for systematic reviews with a focus on health equity. PLOS Medicine 2012;9(10):e1001333. [DOI: 10.1371/journal.pmed.1001333] [DOI] [PMC free article] [PubMed] [Google Scholar]
WHO 2007
- World Health Organization. Cumulative number of reported probable cases of SARS. www.who.int/csr/sars/country/2003_07_11/en (accessed 22 March 2021).
WHO 2019
- World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV). www.who.int/emergencies/mers-cov/en (accessed 22 March 2021).
WHO 2020a
- World Health Organization. Report of the WHO‐China joint mission on coronavirus disease 2019 (COVID‐19). www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report (accessed 22 March 2021).
WHO 2020b
- World Health Organization. Estimating mortality from COVID-19 - scientific brief. www.who.int/publications/i/item/WHO-2019-nCoV-Sci-Brief-Mortality-2020.1 (accessed 22 March 2021).
WHO 2020c
- WHO working group on the clinical characterisation and management of COVID-19 infection. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infectious Diseases 2020;20(8):e192-7. [DOI] [PMC free article] [PubMed]
WHO 2021a
- World Health Organization. Weekly epidemiological update - 23 February 2021. www.who.int/publications/m/item/weekly-epidemiological-update---23-february-2021 (accessed 1 March 2021).
WHO 2021b
- World Health Organization. Therapeutics and COVID-19: living guideline. 6 July 2021. 6. Who do the recommendations apply to? www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1.
WHO 2021c
- WHO. Therapeutics and COVID-19: living guideline. 6 July 2021. 7. Recommendations for therapeutics. 7.6 Systemic corticosteroids (published 2 September 2020). www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2021.2.
WHO 2022a
- World Health Organization. WHO coronavirus disease (COVID-19) dashboard. covid19.who.int (accessed 31 March 2022).
WHO 2022b
- World Health Organization. SARS-CoV-2 variants. https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed 4 April 2022). [PubMed]
Williamson 2020
- Williamson E, Walker AJ, Bhaskaran KJ, Bacon S, Bates C, Morton CE, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020;584:430-6. [DOI: 10.1038/s41586-020-2521-4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wolter 2022
- Wolter N, Jassat W, Walaza S, Welch R, Moultrie H, Groome M, et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: a data linkage study. Lancet 2022;399(10323):437-46. [DOI: 10.1016/S0140-6736(22)00017-4] [DOI] [PMC free article] [PubMed] [Google Scholar]
World Bank 2021
- World Bank Country and Lending Groups. datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed 15 April 2021). [WEBSITE: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups]
Wu 2020
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020;323(13):1239-42. [DOI: 10.1001/jama.2020.2648] [DOI] [PubMed] [Google Scholar]
Yasir 2022
- Yasir M, Goyal A, Sonthalia S. Corticosteroid adverse effects. StatPearls Publishing 2022. [https://www.ncbi.nlm.nih.gov/books/NBK531462/] [PubMed]
References to other published versions of this review
Wagner 2021a
- Wagner C, Griesel M, Mikolajewska A, Mueller A, Nothacker M, Kley K, et al. Systemic corticosteroids for the treatment of COVID-19. Cochrane Database of Systematic Reviews 16 August 2021, Issue 8. Art. No: CD015125. [DOI: 10.1002/14651858.CD015125] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wagner 2021b
- Wagner C, Griesel M, Micholajewska A, Fichtner F, Skoetz N. Corticosteroids for the treatment of COVID-19 (part of German Ecosystem CEO-Sys). PROSPERO 1 February 2021 (available from www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=227450). [PROSPERO: CRD42020227450]