

Abstract
Integrated recreational programs designed to support neurodiverse children and their families are important vehicles for community participation. In this mixed-methods study, we investigated the mechanisms by which parent–child music classes for autistic and neurotypical children can support community participation. Parents of autistic (n = 33) and typically developing (TD; n = 28) preschoolers were interviewed about their expectations for and experiences of participating in a 12-week psychoeducational parent–child music program. Parents completed ratings of momentary affect and social connection, and researchers coded children’s behavioral engagement during classes at multiple time points throughout the program. Primary motivations for enrolling in an integrated music class included children’s interest in music and opportunities for child socialization. Parent-focused reasons were less frequently endorsed as primary motivations for participation. Yet, momentary ratings indicated that music classes supported parents’ affect regulation and social connection with other parents at the level of individual classes and across the program. These in-class experiences were echoed by interviews following program completion, which additionally highlighted the use of new parenting strategies through the musical activities. Since parental emotional experiences of activities, supportive community relationships, and parenting confidence are all linked with increased community participation, integrated music classes may support participation and satisfaction with community experiences.
Keywords: affect, autism, community participation, music, parent training, social connection
INTRODUCTION
Integrated recreational community programs, which are designed to support the social and physical engagement of children with diverse developmental needs and their parents, provide opportunities for community participation and support family well-being.1–3 Reduced community participation is frequently observed among families of young children with autism spectrum disorder (ASD),a a common neurodevelopmental disorder characterized by difficulties with social interaction and communication.4–6 Parents of autistic children express interest in increased child and family participation in community activities, and positive involvement in community activities is increasingly being highlighted as a meaningful outcome of interventions for families of autistic children.7–10 Community activities can foster social support and relationships, increase child and parent well-being, and reduce parenting stress, which is often elevated in parents of autistic children.2,5,11,12 Community activities also provide opportunities for skill development and generalization for individuals with disabilities.2,5,13 Moreover, integrated community activities can shape attitudes of other community members and their understanding of disability.1,2
Community participation is influenced by a variety of factors related to the child, parent, community members, activity demands, accessibility, and the setting/environment.1,4,6,14–16 During the preschool period, community participation includes family involvement in recreational activities. Parents of autistic children are generally more involved in their child’s community participation than parents of typically developing (TD) children.16 Parents of autistic preschoolers report that they are equally willing to take their children to community activities as parents of TD children but are less satisfied with their child’s participation.4,10,16 For recreational activities, parents of young autistic children report fewer positive and more negative emotions, and participation is also more difficult compared to parents of TD children.16 Parents’ negative or positive emotional experiences of activities can lead to parents’ reduced or increased willingness, respectively, to participate in future activities.16 Increased family participation and satisfaction with their child’s participation is observed when parents feel more competent in their parenting skills, when parents are more involved and satisfied with their own participation, and when families experience more positive attitudes and interactions from other community members.2,16–19 Thus, positive and supportive community experiences can impact families’ current and future willingness to participate in community recreational activities.
Musical activities may provide a promising pathway for positive community participation experiences for families of young children with ASD due to their potential impacts on both child and parent behavior.20 Musical activities, such as parent–child music classes, are common in early childhood, and many autistic children are interested in musical activities.21 The PRESS-Play Framework highlights how aspects of musical activities, including predictability, reinforcement, emotion regulation, shared attention, and social play, can scaffold participation of children with ASD and their parents or peers.20 Indeed, beyond traditional parent–child recreational music classes, music therapy focuses on the use of music in the context of a therapeutic relationship to support nonmusical goals.22,23 In autism, this has included using family-centered, parent coaching, and improvisational music therapy approaches to support children’s social communication skills, such as joint engagement and joint attention, as well as the parent–child relationship.24–28
Music can be a powerful tool for emotion regulation. It elicits emotional responses in part due to psychoacoustic properties like mode and tempo, as well as by fostering positive shared social experiences.29,30 Music engages the dopaminergic reward system and modulates the activity of the autonomic nervous system and hypothalamic–pituitary–adrenal axis.30–32 These physiological effects can occur during parent–child musical experiences, suggesting that musical activities may be a platform for increasing positive emotions during a community activity.21,33–35 Joint music activities also support social connection and bonding,36,37 including between parents and their children, and between unfamiliar adults or children.21,33,38,39
While both group and individual singing are associated with decreases in the production of the stress-related hormone cortisol, only group singing is associated with increases in oxytocin, a neuropeptide associated with social bonding.37 Joint music activities impact social connection in part by increasing interpersonal synchrony, which occurs due to music’s predictable melodic and rhythmic structure.36 The predictability and repetition of musical activities can also serve as a support for child participation, especially for autistic children who benefit from predictable structures and routines.20 Additionally, musical activities naturally support positive parenting practices, such as nonverbal responsiveness and shared attention, and can also provide a platform for teaching parenting skills and increasing parent competence.38,40–42 These changes in parenting behaviors may in turn contribute to increased community participation.38, 40
Initial studies of therapeutic music groups primarily focused on the effects on the child or the parent–child relationship. Understanding the expectations and experience of parents participating in integrated parent–child music programs, including how these may differ for families of autistic and TD children, may inform successful implementation of such music programs. In a small pilot study of an integrated psychoeducational parent–child music class program, qualitative coding of parent interviews about their program experience demonstrated the feasibility of such a setting for promoting components known to be important for increasing community participation (e.g., enjoyable and meaningful activity, supportive community and environment, increased skills and competence in using musical activities).38 In the current mixed-methods study of the same psychoeducational music program,b we extend prior findings by directly assessing parents’ perceptions during music classes in real time, combined with qualitative analyses of parent interviews both prior to and following their experience in the music class program. These results will advance the understanding of mechanisms by which such a program may promote community participation.
METHODS
Participants
Participants in the current study included preschool-aged children with ASD (n = 33) or TD (n = 28) and their parents/caregivers who attended at least six classes of the 12-week Serenade parent–child music class program offered as part of a research study (mean [SD]: 9.8 [1.5] classes were attended per family [range: 6–12]). There were two autistic sibling pairs, one TD sibling pair, and one sibling pair with one autistic and one TD child, resulting in a total of 57 unique families participating.c For data analysis purposes, all child participants underwent assessments and behavior coding of class engagement (see below); however, parent questionnaires and interviews were only collected one time per family via the primary parent/caregiver. Demographic information for the primary parent/caregiver and child participants is presented in Tables 1 and 2. Children with ASD were somewhat older than children with TD but had lower nonverbal and language scores. Participating families were not involved in concurrent music therapy or other community parent–child music programs.
TABLE 1.
Demographic information for primary parent participants
| ASD (n = 31) | TD (n = 26) | Difference | |
|---|---|---|---|
| Relationship to child | 26 mothers, four fathers, and one grandmother | 23 mothers and three fathers | χ2 = 0.25, p = 0.62 |
| Age (years; mean [SD]) | 38.0 (5.6) | 34.3 (4.9) | t = 2.57, p = 0.013 |
| Education (# with 4-year college degree) | 23 | 23 | χ2 = 1.85, p = 0.17 |
| Family income (n) | χ2 = 4.67, p = 0.10 | ||
| >$70,000/year | 22 | 16 | |
| $30,000–$70,000/year | 5 | 9 | |
| <$30,000/year | 3 | 0 | |
| Race (n) | χ2 = 4.25, p = 0.51 | ||
| Caucasian | 20 | 21 | |
| Asian | 5 | 1 | |
| Black/African-American | 3 | 1 | |
| More than one race | 2 | 2 | |
| American Indian/Alaskan Native | 2 | 1 | |
| Native Hawaiian/Pacific Islander | 1 | 0 | |
| Ethnicity (# Hispanic/Latinx) | 2 | 1 | - |
Note: Two parents (n = 2 ASD) declined to report education level; three parents (n = 1 ASD; n = 2 TD) declined to provide age; and two parents (n = 1 ASD; n = 1 TD) declined to report income level.
TABLE 2.
Characterization information for child participants
| ASD | TD | Difference | |
|---|---|---|---|
| n (M:F) | 33 (27:6) | 28 (15:13) | χ2 = 4.7, p = 0.03 |
| Chronological age (months; mean [SD]) | 43.8 (9.3) | 37.2 (8.7) | t = 2.88, p = 0.005 |
| MSEL Nonverbal Age Equivalence (months; mean [SD]) | 30.6 (15.6) | 42.0 (12.3) | t = 3.08, p = 0.003 |
| MSEL Language Age Equivalence (months; mean [SD]) | 25.1 (14.4) | 39.8 (10.2) | t = 4.73, p < 0.001 |
| ADOS-2 Comparison Score | 7.8 (1.8) | - | - |
Note: Nonverbal (visual reception) and language (average of receptive and expressive language skills) derived from the Mullen Scales of Early Learning (MSEL).
Abbreviation: ADOS-2, Autism Diagnostic Observation Schedule, 2nd edition.
The study was approved by the university’s Institutional Review Board. Written, informed consent was obtained by a parent or guardian of the children. Children above the age of 3 years and with appropriate language level provided verbal assent.
Procedures
Families participated in the 12-week Serenade parent–child music class program. Families attended the same session weekly so the class makeup was consistent across weeks. Parents completed interviews before and after the music class program with an unfamiliar study team member. Parents completed study surveys (see below) at the start and end of an early, middle, and late class week. Children’s engagement during music class was coded during the early and late class week. Early, middle, and late class week typically corresponded to the first, sixth, and twelfth class week; however, if a family was not present at class during these weeks, surveys/behavior were collected at an adjacent week as possible.
Serenade parent–child music class
Serenade is a 12-week parent–child music class program led by a board-certified music therapist that provides music-based parent training and peer interaction in a musical play context following a manualized curriculum. During Serenade’s weekly class sessions, groups of four to six families (~half with child with ASD) participate in joint music-making activities that are designed to facilitate children’s engagement while also teaching parents behavioral strategies to promote children’s social engagement and positive behavior. Each week of the program focuses on a different theme targeting the use of specific musical strategies, with families receiving weekly handouts on the topic and related supports (e.g., visual schedules and audio recordings) (Table S1).
The Serenade music class format and sample session activities have been described previously38 (Table S2). In brief, each class involves a warm-up period during which children engage in free play, while the music therapist leads parents in a discussion of their home practice goals and introduces the theme for the week. The music therapist then leads families in ~30–40 min of eight structured group music activities, throughout which the therapist demonstrates ways in which the music activities connect with the session theme. At the end of each class, the therapist reviews the theme, and families set individual goals for at-home practice. All families participate in all class aspects such that the program incorporates aspects of community music classes, parent training/psychoeducation, and parent support groups. The music therapist is supported by approximately two research assistants who provide behavioral or technical support (e.g., video cameras) as needed. The music therapist and a research assistant completed fidelity checklists after each session to ensure high fidelity to program curriculum (>97% by each rater).
MEASURES
Parent interviews
Before and after their participation in the music class program, parents completed an individual semistructured interview about their expectations for (pre-interview) and experiences with (post-interview) the program. In the pre-interview, parents were asked about prior experience with children with autism or other developmental disabilities, how they envisioned their family (including child and parents) potentially benefitting from the program, and any concerns they had about participating. In the post-interview, parents were asked about their general impressions of the class, including positive and negative aspects, perceived impact of the program on their family (including child and parents), and if the program impacted their thoughts about parenting, autism, and their own child. Interviews were recorded and transcribed offline.d
Parent momentary affect
Parents completed the Positive and Negative Affect Schedule (PANAS)43 at the start and end of the first, middle, and last weeks’ sessions. The PANAS consists of 10 positive and 10 negative affect items that are rated on a 5-point scale from “not at all” to “very much.” Parents were asked to rate the extent to which they felt each emotion “right now, that is, at the present moment.” A total score is generated for each scale (PANAS Positive; PANAS Negative) with possible score ranges from 10 to 50.
Parent momentary sense of connection
After completing the PANAS, parents completed two Inclusion of the Other in the Self (IOS) scales to measure parents’ perceived social connection to their child and to other members of the class.44 Parents selected one of seven Venn diagrams with circles labeled as “self” or “other” that ranged from not overlapping at all to nearly entirely overlapping to represent how “connected or close” they felt to their child or other members of the class, respectively, at that moment (i.e., at start and end of class). Possible scores for each IOS scale (their child; other class members) range from 1 to 7.
Children’s class engagement
Children’s engagement during class music activities was manually coded using a 15-s momentary coding scheme from videos of the music classes. Engagement was determined based on children’s song-related movements/singing and gaze direction. For every 15-s interval, each child’s behavior was scored hierarchically as active engagement (child overtly participating in class through movement and/or singing while attending to class activities), facilitated engagement (parent or staff physically prompting child while child attended to class activities), passive engagement (child attending to class activities but no overt movement/singing), unengaged (child not attending to class, including off-task behavior), or disruptive (e.g., child screaming). Due to the low number of unengaged and disruptive intervals, unengaged/disruptive were combined. If the child was not visible on the video, the interval was marked as uncodable. Engagement was coded throughout each active music activity except for the lullaby (because children were not expected to actively move/sing during the lullaby) and book activities (because different books provided different opportunities for movement/singing) (Table S2). Proportions for each engagement state were calculated by dividing the number of intervals in each engagement state by the total number of codable intervals across all activities. Videos were coded using ProcoderDV™45 by two trained coders masked to video week. The two coders double coded 12% of the videos (randomly selected) for reliability (ICC’s: active = 0.973; facilitated = 0.980, passive = 0.897; disruptive/unengaged = 0.623).
DATA ANALYSIS
Parent interview coding and analysis
A thematic analysis approach was used to illuminate parent expectations for and experiences of participation.46 All interview transcripts were first reviewed by two coders for familiarity with their contents and to determine and discuss emerging themes. The coders then rereviewed all transcripts to assess for any additional themes so that saturation was achieved (i.e., the data set was fully represented by the themes). One coder (different coders for pre- and post-interviews) then rereviewed all transcripts line-by-line and labeled all relevant lines with codes; a second coder co-coded 28% of transcripts. In places of disagreement (5.7% of codes), the reviewers discussed and came to a consensus. Subthemes were clustered together, and names of overarching and subthemes were refined to best reflect participant responses.
Parent momentary ratings and child engagement
Parent class experience focused on four dependent variables: parent positive affect (PANAS positive), negative affect (PANAS negative), connection to child (IOS child), and connection to other class members (IOS others). For each dependent variable, we conducted separate linear mixed models with within-subjects fixed factors of class timepoint (2: start and end) and week (3: early, middle, and late) nested with the random factor of parent, and between-subjects factor of child diagnosis (2: ASD and TD). Both timepoint and week were included in analyses because we hypothesized that changes could occur within and across class sessions. Linear mixed models were conducted using the lmerTest package in jamovi (v. 1.6.23.0).47,48 Factors were contrast coded centered on 0, so that model estimates reflect the main effects across entire sample/time points. Child engagement analyses focused on children’s active engagement during the music program. We conducted a repeated measures ANOVA to examine change in children’s active engagement over weeks (2: early and late) by diagnostic group (2: ASD and TD).
RESULTS
Parent interviews
Pre-interviews
During the pre-interviews, parents’ responses addressed the topics of (1) child-related reasons for participating; (2) parent-related reasons for participating; and (3) participation concerns; within these overarching themes, specific subthemes emerged (Figure S1A).
Nearly, all families (90% ASD; 100% TD) reported on child-related reasons for participating. The majority of ASD (83.3%) and TD (61.5%) families specifically commented on the musical experience as motivating their participation because of their child’s love of music. Parents wanted their children to enjoy a fun musical experience and also wanted to expand their child’s musical knowledge (e.g., by broadening child’s musical repertoire). A second subtheme that emerged was child socialization (63.3% ASD; 88.5% TD). Parents of autistic children expressed interest in opportunities for their children to interact with others, including children with and without autism. Parents of TD children often commented on their child engaging with neurodiverse populations. The third subtheme to emerge reflected other nonmusical skill development. This theme was expressed less often and primarily by ASD families (40.0% ASD; 7.7% TD). Some parents hoped that the music classes might help the child with, for example, their speech and communication skills.
Parent-related themes were less frequently discussed by parents. Approximately a third of parents (46.7% ASD; 23.1% TD) expressed interested in having a shared experience/activity with their child. A similar percentage (36.7% ASD; 34.6% TD) expressed interest in learning new activities or strategies through the program, with parents primarily focused on opportunities to broaden their own knowledge of musical activities. The third subtheme to emerge related to parent-to-parent connections (20.0% ASD; 19.2% TD).
Participation concerns primarily focused around child behaviour (60.0% ASD; 19.2% TD). Some parents expressed concerns about their child having behavior difficulties, being overwhelmed, or not participating in class activities. Approximately one-third of parents expressed other eclectic concerns, such as potential scheduling issues, parents’ own self-perceived lack of musical skills, and if the music would be interesting to their child.
Post-interviews
Five main themes emerged from the post-interview regarding experience in the program. These themes were generally consistent with themes previously identified in a smaller pilot study of the music program:38 (1) importance of a positive and supportive activity (100% of parents); (2) community connections and autism awareness (71.0% ASD; 84.0% TD); (3) within family connections (54.8% ASD; 84.0% TD); (4) parenting strategies (100% ASD; 92.0% TD); and (5) perceived child behavior changes (87.1% ASD; 68.0% TD) (Figure S1B).
Within these themes, parents frequently reflected upon the importance of having a “fun” activity for both their child and themselves, incorporation of structure and clear expectations (including predictable routines and visual supports), and adequate staffing to support participation. Some parents, particularly those of autistic children, commented on the importance of knowing that other families would be understanding of differences in their child’s engagement and behavior during classes, though they noted feeling concerned at times about their child’s behavior (e.g., when a child would not engage in class activities). At the same time, many parents expressed pride in seeing their own child and other children in the class increase their engagement in activities over the program. Parents also appreciated the opportunity to learn from and connect with other parents and the opportunity for their children to interact with other children. Consistent with the psychoeducational components of the curriculum, parents reported on increased musical parenting skills that supported both parent–child connections (e.g., shared musical games during class and at home) and specific child behavioral needs (e.g., ways to use music in daily living routines).
Parent momentary ratings and child engagement
Parent positive affect significantly increased from the start to end of music classes (B = 1.28, t = 2.90, p = 0.004; Figure 1A). Though effect of child diagnosis on parent positive affect was not significant (B = −3.70, t = −1.86, p = 0.07), there was a significant interaction between week and diagnosis (B = −2.64, t = −2.37, p = 0.02; Figure 2A). Follow-up simple effects testing suggested increased positive affect in parents of autistic children at the late versus early week (B = 1.45, t = 1.93, p = 0.05) but no change in parents of TD children. For parent negative affect, the only significant factor was class, with negative affect decreasing from start to end of classes (B = −1.54, t = −5.83, p < 0.001; Figure 1B).
FIGURE 1.
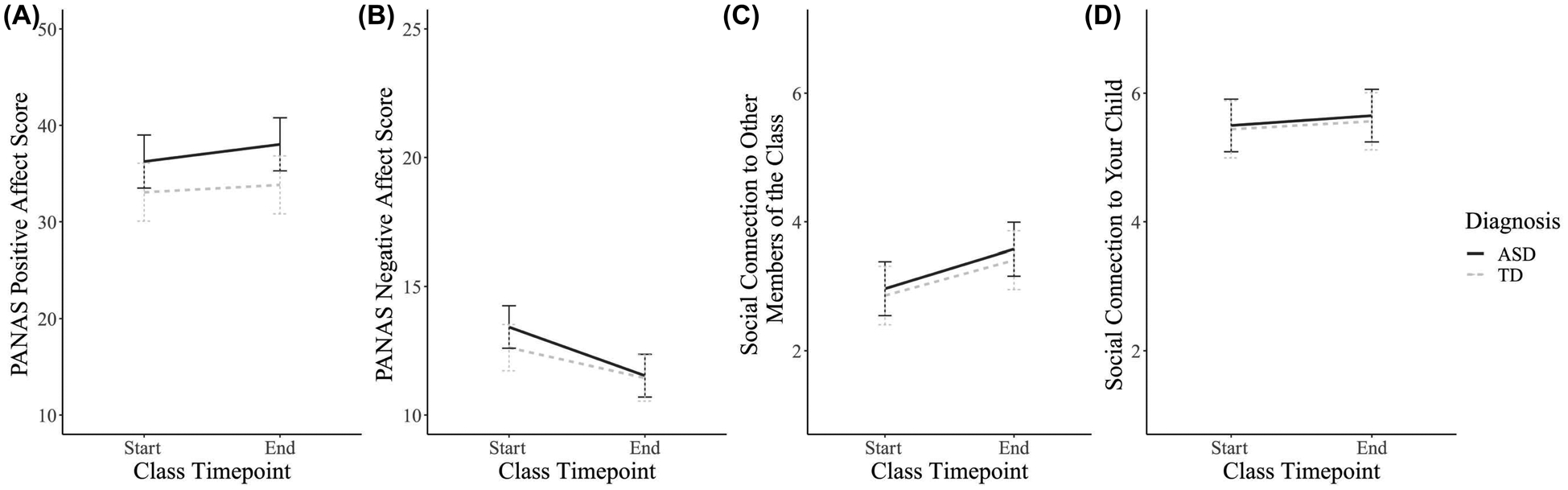
Model score plots showing change in momentary ratings by parents of autistic (ASD) and TD children from start to end of individual music class sessions, controlling for week of program. (A) PANAS positive affect, (B) PANAS negative affect, (C) social connection to other class members (IOS others), and (D) social connection to own child (IOS child). Error bars portray 95% confidence intervals.
FIGURE 2.
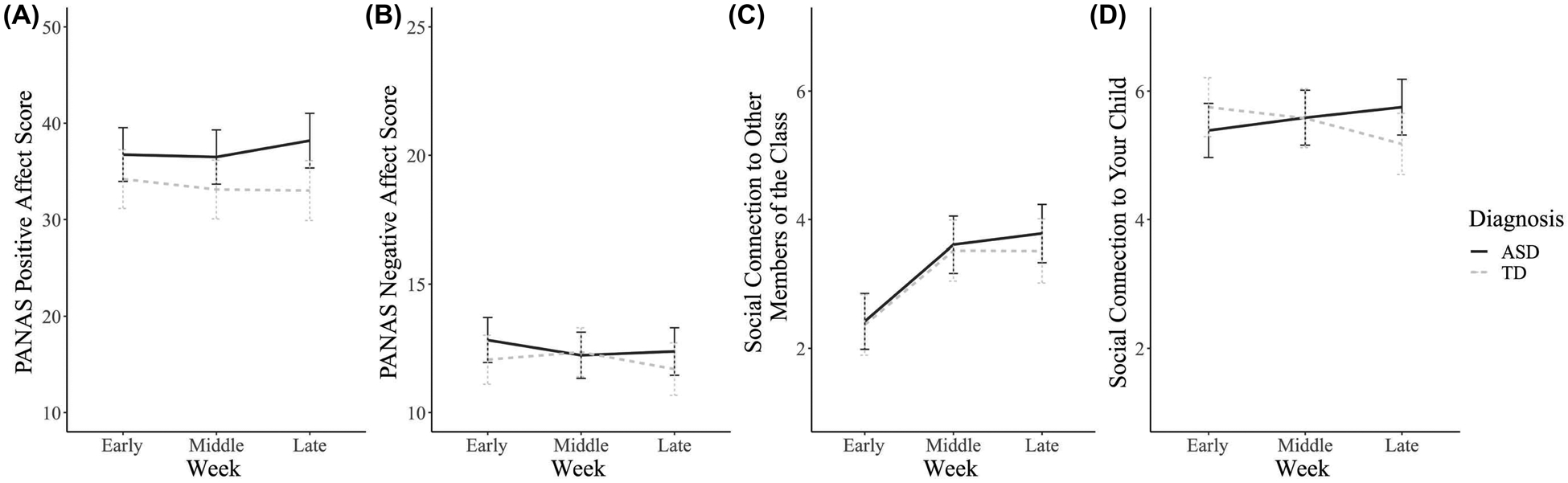
Model score plots showing change in momentary ratings by parents of autistic (ASD) and TD children across early, middle, and late weeks of music class program, controlling for class timepoint. (A) PANAS positive affect, (B) PANAS negative affect, (C) social connection to other class members (IOS others), and (D) social connection to own child (IOS child). Error bars portray 95% confidence intervals.
At the start of the first class, before parents had the opportunity to engage with others, sense of connection to others was low (ASD: 2.1 [1.4]; TD: 2.0 [1.4]). Parents’ connection to others increased significantly from start to end of individual classes (B = 0.58, t = 5.37, p < 0.001; Figure 1C) and across the weeks of the program (middle vs. early week: B = 1.17, t = 9.03, p < 0.001; late vs. early week: B = 1.26, t = 9.17, p < 0.001; middle and late weeks did not differ; Figure 2C). There were no effects related to child diagnosis.
Parents’ sense of connection to their own child was already high at the start of the first class (ASD: 5.4 [1.5]; TD: 5.7 [1.0]). While there were no main effects for class, week, or diagnosis, there was a significant interaction between child diagnosis and program week for the late versus early week (B = −0.94, t = −4.09, p < 0.001; Figure 2D). Parents of autistic children reported greater sense of connection to their child at the late versus early week (B = 0.36, t = 2.36, p = 0.02), while parents of TD children reported reduced sense of connection to their child (B = −0.57, t = −3.37, p < 0.001), though overall connection remained high.
The different patterns for parents’ sense of connection to their child between the ASD and TD groups over the repeated weeks in the program may in part relate to how children participate in the music classes. There were substantial individual differences in children’s active engagement in the classes (Table 3). TD children were more actively engaged than autistic children (repeated measures ANOVA: F(1,49) = 4.33, p = 0.04, η2G = 0.07) but both groups increased their active engagement from the early to late week (F(1,49) = 49.16, p < 0.001, η2G = 0.16). We conducted a linear mixed model to examine the possibility that active engagement differentially impacted parents’ social connection to their child depending on diagnostic group. There was a significant interaction between child diagnosis and child active engagement (B = −3.27, t = −3.45, p < 0.001). As children’s active engagement increased, parents of autistic children reported increased connection to their child (B = 1.79, t = 2.77, p = 0.006), while parents of TD children reported decreased connection to their child (B = −1.49, t = −2.09, p = 0.038).
TABLE 3.
Proportion of time in each engagement state during an early and late class in the ASD and TD groups (mean [SD])
| ASD | TD | |||
|---|---|---|---|---|
| Early | Late | Early | Late | |
| Active | 0.18 (0.17) | 0.33 (0.23) | 0.28 (0.18) | 0.46 (0.16) |
| Passive | 0.61 (0.16) | 0.53 (0.19) | 0.56 (0.16) | 0.48 (0.15) |
| Facilitated | 0.17 (0.16) | 0.12 (0.13) | 0.14 (0.13) | 0.04 (0.04) |
| Unengaged/disruptive | 0.03 (0.05) | 0.02 (0.03) | 0.02 (0.05) | 0.01 (0.03) |
DISCUSSION
Integrated community experiences may benefit both typical and neurodiverse populations by fostering opportunities for skill development, increasing parent and child emotional well-being and social relationships, and impacting perceptions of and understanding of disability.1,2,13 The current study focuses on parent expectations for and experiences with an integrated parent–child music class program. By combining real-time ratings of parent affect and social connections during music classes with parent interviews, the current study sheds light on the mechanisms by which music programs may impact community participation of families of autistic children.
The primary motivations of parents of autistic and TD children for participating in the music program were their child’s interest in musical activities and opportunities for peer socialization. Parents also expressed interest in shared parent–child activities. As musical activities are a common form of positive social interaction between parents and children and children and their peers,21,49 integrated music classes provide a context aligned with parents’ goals for community participation. Parents typically seek out recreational community activities that are enjoyable, aligned with children’s interests, and meaningful for families.50 Interests in child social experiences were not limited to parents of autistic children. The majority of families of TD children wanted their child to have experiences with children of diverse developmental profiles, perhaps reflecting growing interest and awareness of neurodiversity. While some families, particularly of autistic children, commented about the potential for their child to develop additional nonmusical skills (e.g., communication skills), this was expressed by less than half of participants. At post-interviews, some parents of autistic children noted the tension they sometimes felt between treating all activities as interventions versus the music class as an opportunity to “be in something he could just enjoy and have fun.”
Though specific parent-driven motivations for participation were less frequently endorsed at pre-interview, parents’ real-time ratings during music classes and post-interviews indicate specific impacts on parent emotions, social connections, and parenting skills. Parent affect was modulated within single classes and to some degree--for parents of autistic children--across program duration. For parents of autistic and TD children, social connection to others increased within single classes and across the program. These findings expand upon prior surveys, interviews, and physiological measurements conducted in other populations and settings, such as parent–infant music classes and adult singing activities.28,33,37,39,51 Changes in affect and social connection across single classes are consistent with joint music making as a “fast-acting” conduit for social bonding and emotion regulation.33,37,51 These effects at the timescale of single classes may be important in providing immediate reinforcement to families to support their continued participation in the program. Increased social connection across the program may relate to continual impact of the shared music-making activities as well as reflect an additional source of social support (e.g., from parent discussion components) for parents of TD and autistic children. For parents of autistic children in particular, social support contributes to increased parent well-being.12
Parents’ connection to their own children was high throughout the program and may reflect the characteristics of families interested in enrolling in parent–child music classes. On their momentary class ratings, parents of TD and autistic children reported different patterns of social connection to their child across the program, with modest decreases in TD and increases in autistic groups. Though speculative, perhaps as children became increasingly actively engaged in class music activities, parents of TD children perceived their child as more independent, while parents of autistic children perceived their child as more participating in a shared experience. In the post-interview, parents of both autistic and TD children reported increased connections within their family in response to the music program.
Parenting competence is another attribute associated with increased community participation.16 Though sense of competence was not measured in real time, parent post-interviews revealed perceived gains in parenting skills and perceived changes in child behavior. Over time, children increased their active engagement during classes, and parents learned specific parenting skills through the psychoeducational curriculum embedded in the music program. These advances may have helped parents feel more confident in the music class setting and could potentially extend to new circumstances. For example, many parents spoke of applying musical strategies to assist in non-musical activities (e.g., using a song to help with transitions), as well as incorporating non-musical supports (e.g., visual schedules) in their home environment.
Limitations of the current study include the sample demographics as participants were primarily well-educated, white, and had relatively high earnings. Future studies need to include more diverse families to study the generalizability of findings. At the same time, there was substantial variability in the developmental level and autism symptom severity among child participants. The data are limited to self-report and behavioral observation given the importance of parents’ own perceptions of their experiences in shaping their participation.4 Future studies could elect to include physiological measurements (e.g., cortisol and oxytocin) from parents and/or children to examine biological correlates of these behavioral measures. The current study focused on real-time ratings, which captured parents’ class experiences in the moment. Additional studies will be needed to examine if there are any long-term effects of integrated music programming on frequency, experience of, and satisfaction with future community participation activities.
Although parents’ statements may explicitly focus on the interests and needs of their child, parent-related factors greatly determine the degree of a family’s current and future community involvement.4,16 The parent-related effects of parent–child music class participation--such as parent affect regulation, social connection between parents, and parenting skills--all align with frameworks for supporting parents’ well-being.38,52 These effects were apparent for parents of both autistic and TD children, suggesting that integrated music class activities may engage mechanisms important for supporting community participation across diverse families. Integrated music class programs may hold promise for increasing the frequency of and satisfaction with meaningful community participation during early childhood.
Supplementary Material
ACKNOWLEDGMENTS
We thank the families for their participation in the study. We thank the students and staff of the Vanderbilt Music Cognition Lab for assistance with data collection and coding, as well as Adam Summers, MT-BC, and Marisa Fisher for their helpful feedback and discussions. This work was supported in part by the National Endowment for the Arts Award #1844332-38-C-18 and a Vanderbilt University Office for Equity, Diversity, and Inclusion Seed Grant, as well as the Vanderbilt Kennedy Center and VUMC Department of Otolaryngology—Head and Neck Surgery. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Endowment for the Arts (NEA). The NEA does not guarantee the accuracy or completeness of the information included in this report and is not responsible for any consequence of its use. The use of RED-Cap was made possible by the Vanderbilt CTSA grant UL1 TR000445 from the National Center for Advancing Translational Science/National Institute of Health.
Funding information
National Center for Advancing Translational Sciences, Grant/Award Number: UL1 TR000445; National Endowment for the Arts, Grant/Award Number: 1844332-38-C-18; Vanderbilt University Office for Equity, Diversity, and Inclusion Seed Grant; Vanderbilt Kennedy Center; VUMC Department of Otolaryngology–Head and Neck Surgery
Footnotes
COMPETING INTERESTS
The authors declare no competing interests.
SUPPORTING INFORMATION
Additional supporting information can be found online in the Supporting Information section at the end of this article.
We use both identity-first (i.e., “autistic children”) and person-first (i.e., “children with ASD”) language, in line with preferences expressed by self-advocates, caregivers, and professionals and APA guidelines for terminology around disability.53,54
The current study uses the same curriculum as the pilot study38 but is an entirely separate cohort of participants. The pilot study used a 10-week version of the curriculum; the current study extended the curriculum to 12 weeks due to family feedback in the pilot study.
As part of the overall Serenade program and associated research, we aimed to enroll a minimum of 50 unique participants (n = 25 ASD, n = 25 TD). Enrollment goals were informed by sample size recommendations for the qualitative analysis approach, including when applied with families/participants with ASD given the heterogeneity in this population,55–57 as well as to be well-powered to detect medium effect sizes for quantitative analyses (group × time interactions). Due to family interest in the program and group session scheduling availability, we were able to meet and somewhat exceed this minimum sample size requirement during the time period the Serenade program was offered.
Due to audio device malfunction, interviews were not available for one family at pre (ASD) and one family at post (TD).
REFERENCES
- 1.WHO. (2011). World Report on Disability 2011. World Health Organization. [PubMed] [Google Scholar]
- 2.King G, Lawm M, King S, Rosenbaum P, Kertoy MK, & Young NL (2003). A conceptual model of the factors affecting the recreation and leisure participation of children with disabilities. Physical & Occupational Therapy in Pediatrics, 23, 63–90. [PubMed] [Google Scholar]
- 3.Weaver LA, Bingham E, Luo K, Juárez AP, & Taylor JL (2021). What do we really mean by “inclusion?”: The importance of terminology when discussing approaches to community engagement. Autism, 25, 2149–2151. [DOI] [PubMed] [Google Scholar]
- 4.Lam S-F, Wong BPH, Leung D, Ho D, & Au-Yeung P (2010). How parents perceive and feel about participation in community activities. Autism, 14, 359–377. [DOI] [PubMed] [Google Scholar]
- 5.Askari S, Anaby D, Bergthorson M, Majnemer A, Elsabbagh M, & Zwaigenbaum L (2015). Participation of children and youth with autism spectrum disorder: A scoping review. Review Journal of Autism and Developmental Disorders, 2, 103–114. [Google Scholar]
- 6.Egilson ST, Jakobsdóttir G, Ólafsson K, & Leósdóttir T (2017). Community participation and environment of children with and without autism spectrum disorder: Parent perspectives. Scandinavian Journal of Occupational Therapy, 24, 187–196. [DOI] [PubMed] [Google Scholar]
- 7.Karst JS, & Van Hecke AV (2012). Parent and family impact of autism spectrum disorders: A review and proposed model for intervention evaluation. Clinical Child and Family Psychology Review, 15, 247–277. [DOI] [PubMed] [Google Scholar]
- 8.Wainer AL, Hepburn S, & Mcmahon Griffith E (2017). Remembering parents in parent-mediated early intervention: An approach to examining impact on parents and families. Autism, 21, 5–17. [DOI] [PubMed] [Google Scholar]
- 9.Stahmer AC, & Pellecchia M (2015). Moving towards a more ecologically valid model of parent-implemented interventions in autism. Autism, 19, 259–261. [DOI] [PubMed] [Google Scholar]
- 10.Simpson K, Keen D, Adams D, Alston-Knox C, & Roberts J (2018). Participation of children on the autism spectrum in home, school, and community. Child: Care, Health and Development, 44, 99–107. [DOI] [PubMed] [Google Scholar]
- 11.Bromley JO, Hare DJ, Davison K, & Emerson E (2004). Mothers supporting children with autistic spectrum disorders: Social support, mental health status and satisfaction with services. Autism, 8, 409–423. [DOI] [PubMed] [Google Scholar]
- 12.Ekas NV, Lickenbrock DM, & Whitman TL (2010). Optimism, social support, and well-being in mothers of children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40, 1274–1284. [DOI] [PubMed] [Google Scholar]
- 13.Dunst CJ, Bruder MB, Trivette CM, & Hamby DW (2006). Everyday activity settings, natural learning environments, and early intervention practices. Journal of Policy and Practice in Intellectual Disabilities, 3, 3–10. [Google Scholar]
- 14.Di Marino E, Tremblay S, Khetani M, & Anaby D (2018). The effect of child, family and environmental factors on the participation of young children with disabilities. Disability and Health Journal, 11, 36–42. [DOI] [PubMed] [Google Scholar]
- 15.Lavesser P, & Berg C (2011). Participation patterns in preschool children with an autism spectrum disorder. OTJR Occupation, Participation and Health, 31, 33–39. [Google Scholar]
- 16.Avrech Bar M, Shelef L, & Bart O (2016). Do participation and self-efficacy of mothers to children with ASD predict their children’s participation? Research in Autism Spectrum Disorders, 24, 1–10. [Google Scholar]
- 17.Anaby D, Hand C, Bradley L, Direzze B, Forhan M, Digiacomo A, & Law M (2013). The effect of the environment on participation of children and youth with disabilities: A scoping review. Disability and Rehabilitation, 35, 1589–1598. [DOI] [PubMed] [Google Scholar]
- 18.Kramer JM, Olsen S, Mermelstein M, Balcells A, & Liljenquist K (2012). Youth with disabilities’ perspectives of the environment and participation: A qualitative meta-synthesis. Child: Care, Health and Development, 38, 763–777. [DOI] [PubMed] [Google Scholar]
- 19.Bedell GM, Khetani MA, Cousins MA, Coster WJ, & Law MC (2011). Parent perspectives to inform development of measures of children’s participation and environment. Archives of Physical Medicine and Rehabilitation, 92, 765–773. [DOI] [PubMed] [Google Scholar]
- 20.Lense MD, & Camarata S (2020). PRESS-Play: Musical engagement as a motivating platform for social interaction and social play in young children with ASD. Music & Science, 3, 10.1177/2059204320933080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Steinberg S, Shivers CM, Liu T, Cirelli LK, & Lense MD (2021). Survey of the home music environment of children with various developmental profiles. Journal of Applied Developmental Psychology, 75, 101296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Marquez-Garcia AV, Magnuson J, Morris J, Iarocci G, Doesburg S, & Moreno S (2021). Music therapy in autism spectrum disorder: A systematic review. Review Journal of Autism and Developmental Disorders, 9, 91–107. [Google Scholar]
- 23.Mayer-Benarous H, Benarous X, Vonthron F, & Cohen D (2021). Music therapy for children with autistic spectrum disorder and/or other neurodevelopmental disorders: A systematic review. Frontiers in Psychiatry, 12, 643234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kim J, Wigram T, & Gold C (2008). The effects of improvisational music therapy on joint attention behaviors in autistic children: A randomized controlled study. Journal of Autism and Developmental Disorders, 38, 1758–1766. [DOI] [PubMed] [Google Scholar]
- 25.Hernandez-Ruiz E (2020). Parent coaching of music interventions for children with ASD: A conceptual framework. Nordic Journal of Music Therapy, 29, 200–221. [Google Scholar]
- 26.Carpente J, Casenhiser DM, Kelliher M, Mulholland J, Sluder HL, Crean A, & Cerruto A (2021). The impact of imitation on engagement in minimally verbal children with autism during improvisational music therapy. Nordic Journal of Music Therapy, 31, 44–62. [Google Scholar]
- 27.Thompson GA, Mcferran KS, & Gold C (2014). Family-centred music therapy to promote social engagement in young children with severe autism spectrum disorder: A randomized controlled study. Child: Care, Health and Development, 40, 840–852. [DOI] [PubMed] [Google Scholar]
- 28.Williams KE, Berthelsen D, Nicholson JM, Walker S, & Abad V (2012). The effectiveness of a short-term group music therapy intervention for parents who have a child with a disability. Journal of Music Therapy, 49, 23–44. [DOI] [PubMed] [Google Scholar]
- 29.Juslin PN, & Västfjäll D (2008). Emotional responses to music: The need to consider underlying mechanisms. Behavioral and Brain Sciences, 31, 559–575. discussion 575–621. [DOI] [PubMed] [Google Scholar]
- 30.Chanda ML, & Levitin DJ (2013). The neurochemistry of music. Trends in Cognitive Sciences, 17, 179–193. [DOI] [PubMed] [Google Scholar]
- 31.Ferreri L, Mas-Herrero E, Zatorre RJ, Ripollés P, Gomez-Andres A, Alicart H, Olivé G, Marco-Pallarés J, Antonijoan RM, Valle M, Riba J, & Rodriguez-Fornells A (2019). Dopamine modulates the reward experiences elicited by music. Proceedings of the National Academy of Sciences of the United States of America, 116, 3793–3798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Zatorre RJ, & Salimpoor VN (2013). From perception to pleasure: Music and its neural substrates. Proceedings of the National Academy of Sciences of the United States of America, 110, 10430–10437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Fancourt D, & Perkins R (2018). The effects of mother–infant singing on emotional closeness, affect, anxiety, and stress hormones. Music & Science, 10.1177/2059204317745746 [DOI] [Google Scholar]
- 34.Cirelli LK, Jurewicz ZB, & Trehub SE (2019). Effects of maternal singing style on mother–infant arousal and behavior. Journal of Cognitive Neuroscience, 32, 1213–1220. [DOI] [PubMed] [Google Scholar]
- 35.Trehub SE, Plantinga J, & Russo FA (2016). Maternal vocal interactions with infants: Reciprocal visual influences. Social Development, 25, 665–683. [Google Scholar]
- 36.Savage PE, Loui P, Tarr B, Schachner A, Glowacki L, Mithen S, & Fitch WT (2020). Music as a coevolved system for social bonding. Behavioral and Brain Sciences, 44, e59. [DOI] [PubMed] [Google Scholar]
- 37.Good A, & Russo F (2022). Changes in mood, oxytocin, and cortisol following group and individual singing: A pilot study. Psychology of Music, 50, 1340–1347. [Google Scholar]
- 38.Lense MD, Beck S, Liu C, Pfeiffer R, Diaz N, Lynch M, Goodman N, Summers A, & Fisher MH (2020). Parents, peers, and musical play: Integrated parent–child music class program supports community participation and well-being for families of children with and without autism spectrum disorder. Frontiers in Psychology, 11, 555717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Perkins R, Yorke S, & Fancourt D (2018). How group singing facilitates recovery from the symptoms of postnatal depression: A comparative qualitative study. BMC Psychology, 6, 41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Teggelove K, Thompson G, & Tamplin J (2019). Supporting positive parenting practices within a community-based music therapy group program: Pilot study findings. Journal of Community Psychology, 47, 712–726. [DOI] [PubMed] [Google Scholar]
- 41.Boorom O, Muñoz V, Xin R, Watson M, & Lense MD (2020). Parental responsiveness during musical and non-musical engagement in preschoolers with ASD. Research in Autism Spectrum Disorders, 78, 101641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Liu T, Schultz BG, Dai D, Liu C, & Lense MD (2021). Parent–child nonverbal engagement during read versus sung book-sharing in preschoolers with and without ASD. Psychology of Music, 10.1177/03057356211058781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Watson D, Clark LA, & Tellegen A (1988). Development and validation of brief measures of positive and negative affect: The PANAS Scales. Journal of Personality and Social Psychology, 54, 1063–1070. [DOI] [PubMed] [Google Scholar]
- 44.Aron A, Aron EN, & Smollan D (1992). Inclusion of Other in the Self Scale and the structure of interpersonal closeness. Journal of Personality and Social Psychology, 63, 596–612. [Google Scholar]
- 45.Tapp J, & Walden T (1993). PROCODER: A professional tape control, coding, and analysis system for behavioral research using videotape. Behavior Research Methods, Instruments, & Computers, 25, 53–56. [Google Scholar]
- 46.Braun V, & Clarke V (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3, 77–101. [Google Scholar]
- 47.Jamovi. (2021). The jamovi project.
- 48.Kuznetsova A, Brockhoff PB, & Christensen RHB (2017). lmerTest Package: Tests in linear mixed effects models. Journal of Statistical Software, 82, 1–26. [Google Scholar]
- 49.Politimou N, Stewart L, Müllensiefen D, & Franco F (2018). Music@Home: A novel instrument to assess the home musical environment in the early years. PLoS One, 13, e0193819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Langa LA, Monaco P, Subramaniam M, Jaeger PT, Shanahan K, & Ziebarth B (2013). Improving the museum experiences of children with autism spectrum disorders and their families: An exploratory examination of their motivations and needs and using web-based resources to meet them. Curator: The Museum Journal, 56, 323–335. [Google Scholar]
- 51.Pearce E, Launay J, & Dunbar RIM (2015). The ice-breaker effect: Singing mediates fast social bonding. Royal Society Open Science, 2, 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Seligman MEP (2011). Flourish: A visionary new understanding of happiness and well-being. Free Press. [Google Scholar]
- 53.Bottema-Beutel K, Kapp SK, Lester JN, Sasson NJ, & Hand BN (2021). Avoiding ableist language: Suggestions for autism researchers. Autism in Adulthood, 3, 18–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.American Psychological Association. (2020). Publication manual of the American Psychological Association 2020: The official guide to APA style. 7th ed. [Google Scholar]
- 55.Cridland EK, Jones SC, Caputi P, & Magee CA (2015). Qualitative research with families living with autism spectrum disorder: Recommendations for conducting semistructured interviews. Journal of Intellectual & Developmental Disability, 40, 78–91. [Google Scholar]
- 56.Moser A, & Korstjens I (2018). Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. European Journal of General Practice, 24, 9–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.van Schalkwyk GI, & Dewinter J (2020). Qualitative research in the Journal of Autism and Developmental Disorders. Journal of Autism and Developmental Disorders, 50, 2280–2282. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.