

Abstract
OBJECTIVE
Reoperative thyroid surgery is technically difficult process with increased complications due to the adhesions and fibrosis caused by the previous surgery. In this experimental animal model, we planned to investigate the effect of ContracttubexTM, a mixture of Extractum cepae, Heparin sodium and Allantoin, on adhesion and fibrosis after neck surgery (thyroidectomy).
METHODS
The current study is an experimental animal model of post-thyroidectomy adhesion. Twelve Wistar-Albino male rats in two groups were used. Under sterile conditions, a midline incision on the neck was made. The anterior thyroid muscles were separated and the thyroid lodge was reached. As a minor interventional procedure, a sponge was applied to the thyroid tissue, and then a combination of 1 g Extractum capae, heparin, sodium, and allantoin was applied to the dissection site in the drug group. Rats in both groups were sacrificed on 30th day. Cervical regions were dissected and evaluated for macroscopic adhesion. Tissue samples were taken for microscopic evaluation for fibrosis and inflammation.
RESULTS
In the experimental group in which ContractubexTM was applied, inflammation was not detected in five (83.3%) of six rats while no inflammation was detected in four (66.7%) of six rats in the control group (p=0.505). Considering the fibrosis score, mild or moderate fibrosis was detected in four (66.7%) of six rats in the control group, while fibrosis was found in only two (33.3%) rats in the experimental group (p=0.264). When macroscopic adhesion was evaluated, two (33.3%) rats of the control group subjects were Grade 4, and one (16.7%) was Grade 3. No rats in the experimental group were Grade 4 (p=0.392).
CONCLUSION
ContractubexTM seems to be effective in preventing adhesions and fibrosis after thyroidectomy and neck surgery, but further research is needed for use in human studies.
Keywords: Adhesion, Extractum cepae, fibrosis, re-operative surgery, thyroidectomy
Highlight key points
ContractubexTM seems to be effective preventing adhesions and fibrosis in neck surgery.
No side effects related to ContractubexTM have been detected.
Anti-inflamatuary effects of ContractubexTM should be eveluated immuno-chemically.
Reoperative thyroid surgery is defined as thyroid surgeries performed after previous thyroid surgery, tracheostomy, anterior cervical discectomy, or operations in which the cervical compartments are dissected, such as carotid endarterectomy [1]. Thyroid re-operations are performed in case of recurrence of primary thyroid disease, residual thyroid disease or unexpected pathology results. With the abandonment of bilateral subtotal thyroidectomy in surgical treatment guidelines, the rates of completion thyroidectomy requiring dissection in the same region have decreased, but thyroid surgery is still the most common re-operation on the neck.
Compared to primary surgery, re-operation is technically difficult and open to more complications [2, 3]. Intense fibrosis and adhesions that develop due to the previous surgery both impair the anatomical recognition and complicate the preservation of the recurrent laryngeal nerve and the dissection of the parathyroid tissues in complementary thyroidectomy/parathyroidectomy operations [4]. Temporary or permanent recurrent nerve injury (2.6–24%) and temporary or permanent hypoparathyroidism rates (3–16%) after secondary surgeries are detected in increasing rates [5, 6]. Swallowing and phonation disorders without anatomical nerve injury can also be observed in patients undergoing neck surgery, which is associated with developing adhesions and fibrosis due to surgery [7, 8]. Contractubex™ consists of a mixture of Extractum capea, heparin, sodium, and allantoin. It has entered the standard treatment guidelines for the hypertrophic scars and keloids [9]. The anti-inflammatory and anti-fibrotic efficacy of this combination in epidural fibrosis and intra-abdominal adhesion models were examined and promising results were obtained [10, 11]. In this experimental animal model, we planned to investigate the effect of an E. capea, heparin sodium and allantoin combination on adhesion and fibrosis after neck surgery (thyroidectomy).
MATERIALS AND METHODS
Study Design
All experimental stages were carried out in accordance with the Helsinki Declaration Laboratory Animal Use and Care Rules after the approval of the Ankara University Animal Experiments Local Ethics Committee numbered 2015-18-202. All procedures were carried out in the Ankara University Experimental Animals Laboratory. Twelve Wistar-Albino male rats weighing 220±25 g were used in this study. Animals were randomized into two groups, with six animals in each group. Anesthesia was achieved with intraperitoneally administered xylazine hydrochloride (10 mg_kg) and ketamine hydrochloride (50 mg_kg). All surgical procedures were performed by two researchers (Balas, Yilmaz). Under sterile conditions, a midline incision on the neck was made, the anterior thyroid muscles were separated and the thyroid lodge was reached. As a minor interventional procedure, a sponge was applied to the thyroid tissue, and then a combination of 1 g E. capea, heparin, sodium, and allantoin was applied to the dissection site in the drug group. After the procedure, the muscles were brought back to the anatomical plan. The skin was closed with a non-absorbable 4.0 prolene suture. After the procedure, the animals were taken into single cages for post-op compilation. Rats were fed with standard feed and water. After sacrificing the rats with high-dose sodium thiopental anesthesia on the 30th day, their cervical regions were dissected and evaluated by a single-blind surgeon in terms of macroscopic adhesion (Akıncı). The Zühlke [12] macroscopic adhesion score was used for macroscopic evaluation (Table 1). Tissue samples were taken for microscopic evaluation of fibrosis and inflammation.
Table 1.
Zühlke adhesion score
| Grade 1 | Filmy adhesions: Easy to separate by blunt dissection (no vascularization) |
| Grade 2 | Minimally adhesions: Blunt dissection possible but partly sharp dissection possible (beginning of vascularization) |
| Grade 3 | Strong adhesions: Adhesions requiring sharp dissection (obvious vascularization) |
| Grade 4 | Dense adhesions: Lysis possible by sharp dissection only (organ strongly attached with severe adhesions and damage of organs hardly preventable) |
Pathological Evaluation
After routine formalin fixation, 4–5 µm thick sections prepared from tissues embedded in paraffin blocks were evaluated by light microscopy after Hematoxylin Eosin (HE) staining. In the microscopic evaluation, the levels of inflammation and fibrosis in the sections were evaluated. Inflammation was evaluated on the basis of chronic inflammatory cell infiltration (lymphocyte and plasmocyte) and was scored out of three. Fibrosis, which was evaluated on the basis of fibroblast proliferation, was also scored out of three using the same method. For both parameters, a semi-quantitative scoring method was used as: 0, none; 1, mild; and 2, moderate-severe. Then, a total score, which is the sum of the inflammation and fibrosis scores, was created for each case.
Statistical Analysis
Categorical data were expressed as numbers and percentages. Comparison between categorical data was made with the Chi-square test. Analyses were performed with IBM SPSS (Statistics Package Program for the Social Sciences) version 22.0 (IBM Corporation, Armonk, NY, USA). Statistical significance level was considered as p<0.05.
RESULTS
No complications and mortality were observed in either experimental group. In the experimental group in which ContractubexTM was applied, inflammation was not detected in five (83.3%) of six rats while no inflammation was detected in four (66.7%) of six rats in the control group (p=0.505). Considering the fibrosis score, mild, or moderate, fibrosis was detected in four (66.7%) of six rats in the control group, while fibrosis was found in only two (33.3%) rats in the experimental group (p=0.264) (Fig. 1–3). Considering the total microscopic score, in the six rats of the control group, one (16.7%) had mild inflammation, two (33.3%) had moderate inflammation, and one (16.7%) had severe inflammation+fibrosis, while half (50.0%) of the experimental group developed only mild inflammation+fibrosis (p=0.241). When macroscopic adhesion was evaluated, two (33.3%) rats of the control group subjects were Grade 4, and one (16.7%) was Grade 3 (Fig. 4). No rats in the experimental group were Grade 4 (p=0.392). The comparison of macroscopic and histopathological findings between the two groups is demostrated in Table 2.
Figure 1.
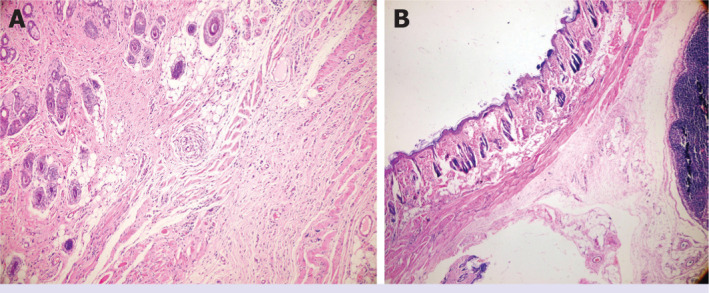
(A) Limited fibrosis focus in the subcutaneous tissue in two different samples in the control group (HE × 200). (B) Limited fibrosis focus in the subcutaneous tissue in two different samples in the control group (HE × 100).
Figure 3.
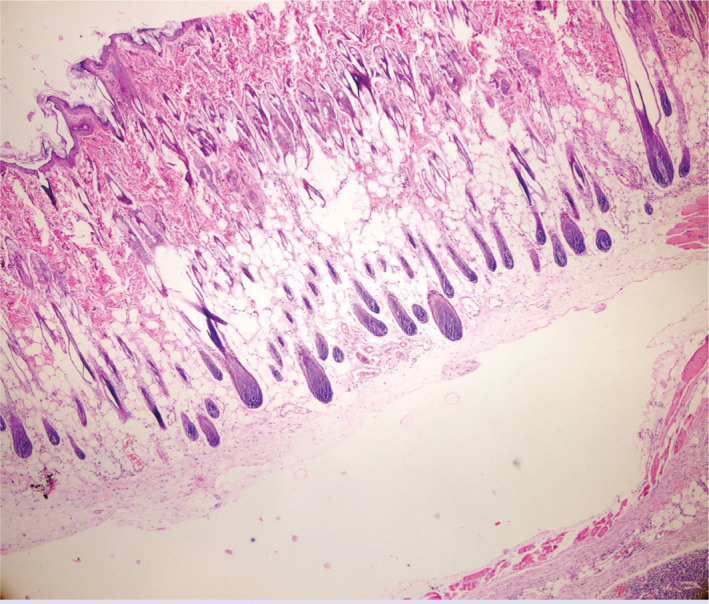
Loose subcutaneous tissue without fibrosis and inflammation in the drug group (HE × 100).
Figure 4.

Grade 3 adhesion in the control group.
Table 2.
Comparison of the ContractubexTM and control groups according to ınflammation, fibrosis, total microscopic score, and macroscopic grades
| Group I (control) (%) | Group II (ContractubexTM) (%) | |||
|---|---|---|---|---|
| Inflammation score | ||||
| No | 66.7 | 83.3 | 75.0 | 0.505* |
| Mild | 33.3 | 16.7 | 25.0 | |
| Fibrosis score | ||||
| No | 33.3 | 66.7 | 50.0 | 0.264* |
| Mild | 33.3 | 33.3 | 33.3 | |
| Moderate-severe | 33.3 | 0.0 | 16.7 | |
| Total microscopic score | ||||
| No | 33.3 | 50.0 | 41.7 | 0.241* |
| Mild | 16.7 | 50.0 | 33.3 | |
| Moderate-Severe | 33.3 | 0.0 | 16.7 | |
| Severe | 16.7 | 0.0 | 8.3 | |
| Macroscopic grade | ||||
| Grade 1 | 16.7 | 50.0 | 33.3 | 0.392* |
| Grade 2 | 33.3 | 33.3 | 33.3 | |
| Grade 3 | 16.7 | 16.7 | 16.7 | |
| Grade 4 | 33.3 | 0.0 | 16.7 | |
| Total | 100.0 | 100.0 | 100.0 |
: Chi-square test.
Figure 2.
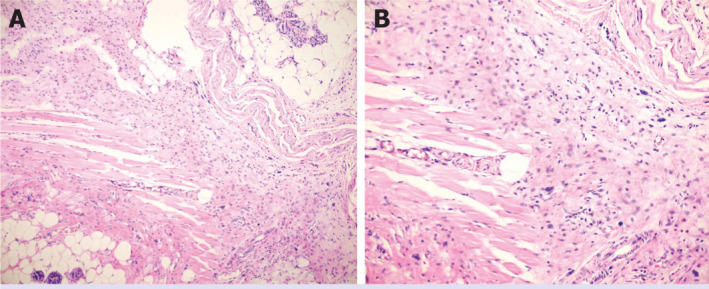
(A) Diffuse fibrosis and mild inflammation in the subcutaneous tissue in the control group (HE × 200). (B) Diffuse fibrosis and mild inflammation in the subcutaneous tissue in the control group (HE × 400).
DISCUSSION
In all surgical anatomical areas, secondary surgeries carry significant risks and technical difficulties due to adhesion and fibrosis caused by the previous surgery. The morbidity and mortality rates of secondary surgeries are exponential when compared to primary surgeries. For this reason, the indications of re-operative thyroid surgery should be determined meticulously and it is recommended that the surgery be performed by experienced teams [2]. Benek et al. [6] revealed that the rate of completion thyroidectomy decreased due to the primary surgical preference shifting to total thyroidectomy in their study on the change in completion thyroidectomy in the last decade. Gür et al. [5] showed that complications rates of completion thyroidectomy are at still high despite increasing technological developments. Medas et al. [4] performed 152 (3.3%) re-operative thyroidectomies in their thyroid surgery series of 4572 patients; the rate of transient hypoparathyroidism was 56%, permanent hypoparathyroidism was detected in 25%, and while nerve damage was reported as temporary in 10% and permanent in 2%. The most important goals of surgery for multinodular goiters are to prevent recurrence after surgery, to diagnose malignancy that could not be defined preoperatively, and to decrease re-operation rates. The relapse rates after bilateral subtotal thyroidectomies have been reported to be as high as 9–43% [13]. Complications of completion thyroidectomy increase in patients undergoing subtotal thyroidectomy. However, the risk increase in patients with completed opposite lobe after unilateral lobectomy is not as scary as entering the same area. Adhesion-related complications after completion thyroidectomy still maintain its current importance despite the use of nerve monitoring and developments in surgical technique. Although it has been reported that the complications related to reoperation have decreased with the use of intraoperative nerve monitoring, there are studies reporting that the risk continues [14, 15].
The importance of preventing post-thyroidectomy adhesions is not only because of the difficulty of secondary surgery, but also fibrosis and adhesions that develop after primary surgery disrupt the movements of the larynx and cause phonation and swallowing disorders. Cho et al. [7] measured the larynx movements of patients who underwent hemithyroidectomy and total thyroidectomy with the help of ultrasound and showed that the movements were impaired during swallowing, and this was attributed to adhesions secondary to the operation.
There are studies on the pathophysiology and prevention of adhesions in re-operative thyroid surgery. Although the shift of surgical techniques to minimally invasive methods, the use of anti-inflammatory drugs, heparin, fibronolytic agents, and membrane or fluid barriers is promising, they have not been fully successful. Alkan et al. [8] used hyaluronic acid carboxymethyl cellulose (Seprafilm) as an adhesion barrier in patients who underwent total thyroidectomy in their randomized prospective study; they checked the swallowing function with a post-operative electrophysiological study and showed that the application of seprafilm did not provide a significant benefit in the improvement of post-operative swallowing functions Bae et al. [16], in their prospective randomized controlled study, could not detect the antiadhesive effect of seprafilm application, but they showed that dysphagia and skin recession due to thyroidectomy tended to regress over time. Park et al. [17] used oxidized regenerated cellulose (Interceed) in their prospective randomized controlled study and showed that swallowing problems and neck skin shrinkage rates decreased in the early post-operative period. In the experimental study of Makay et al. [18], it was stated that the locally applied low-dose simvastatin had lower macroscopic adhesion scores compared to the control group and high-dose simvastatin group. However, it was determined that TGF-β1 levels, which control the anti-inflammatory effects of simvastatin, did not show a significant change. Idiz et al. [19] in their experimental studies investigating the effects of flaxseed oil and glycerol, showed that glycerol prevented adhesion more effectively, although it was not statistically significant. Yigit et al. [20], in their experimental study comparing the effects of seprafilm and interceed, showed that both materials reduced adhesion rates and did not cause foreign body reactions. Extractum cepae has anti-inflammatory and bactericidal effects. It is thought to be effective through the quercetin and kaempferol it contains. It has been shown that TGFβ-1, IGF-1 dependent pathways in keloid fibroblasts are inhibited when in contact with quercetin. In electron microscopic studies, it was determined that the extracellular matrix levels of keloid fibroblasts in contact with quercetin were much lower in density. It was observed that the production and accumulation of the extracellular matrix were inhibited in the group in which quercetin was administered [21]. In our experimental study to prevent adhesion and fibrosis after neck surgery (thyroidectomy), we used a mixture of E. Capea, heparin, and allantoin, ContractubexTM [10/100 g Extractum Cepae per, 40/100 mg (5000 IU) Heparin Sodium, 1/100 g allantoin] gel. Aysan et al. [11] determined that 1 g of ContractubexTM administered intraperitoneally did not form granulomas, and there was no toxicity in their study.
In our study, it was seen that ContractubexTM 1 g applied to the dissection lodge did not cause granuloma in the drug group. In our macroscopic evaluation, we found fewer adhesions in the ContractubexTM group than in the control group, although it was not statistically significant. We think that this is due to the small number of experimental animals, which is one of the most important limitations of our study. Since thyroidectomy was not applied in the adhesion formation technique, we used it in the experimental protocol. We believe that only the dissection of the fascial planes and then minor manipulation of the thyroid tissue with a sponge caused fewer adhesions in the control group. In the experimental study by Lim et al. [22], it was shown that more collagen was stored in the model in which istmectomy (thyroidectomy) was performed compared to the models in which only the fascial planes were dissected, and there was more intense fibrosis between the trachea and strap muscles. The reason we chose this experimental model is that the definition of re-operative thyroid surgery includes not only completion thyroidectomy but also other previous neck surgeries. Aksakal et al. [23] reported that the materials used as adhesion barriers with the liquid-gelatinous structure were more effective than others. In our study, we believe that the gel structure of ContractubexTM also contributes to the prevention of adhesion development as a physical barrier. In our study, the time of termination of the experiment was determined as the 30th day. This period is within the dangerous time period that Saleem et al. [24] showed in their meta-analysis examining the effect of timing of completion thyroidectomy on complications, so we tried to prevent the negative effect of spontaneous regression of developing adhesions in our study. Menekse et al. [25] showed that ContractubexTM decreased the amount and density of fibrosis in their study on epidural fibrosis. Ozay et al. [10] showed that ContractubexTM was effective in both the development of epidural fibrosis and its regression after revision surgery in the rat laminectomy model. In their peritoneal adhesion studies, Ozmen et al. [26] showed that the ContractubexTM mixture was more effective than the use of each of components separately Seref et al. [27] showed that ContractubexTM inhibited stricture development by preventing fibrosis in their experimental corrosive esophageal burn model. In our study, it was observed that fibrosis developed less in the drug group than in the control group. Ayengin and Kilic [28] showed that contractubex reduced the development of fibrosis in their experimental hypospadias model, but the inflammation detected histopathologically was higher than the control.
In our study, we detected a higher rate of inflammation in the control group, but we did not evaluate a parameter that immuno-chemically controls anti-inflammatory activity, which is an important limitation of our study.
Conclusion
This is the first study to prevent adhesion and fibrosis after neck surgery based on the anti-fibrotic effects of contractubex (a combination of E. capea, heparin sodium, and allantoin). ContractubexTM seems to be effective in preventing adhesions and fibrosis after thyroidectomy and neck surgery, but further research is needed for use in human studies.
Footnotes
Cite this article as: Balas S, Tokgoz S, Yilmaz KB, Onder E, Karabacak H, Akinci M, et al. Effect of Extractum cepae, heparin sodium and allantoin combination (ContractubexTM) on adhesion and fibrosis after neck surgery (thyroidectomy) in rats. North Clin Istanb 2022;9(5):495–500.
Ethics Committee Approval
The Ankara University Animal Experiments Ethics Committee granted approval for this study (date: 27.10.2015, number: 2015-18-202).
Conflict of Interest
No conflict of interest was declared by the authors.
Financial Disclosure
The authors declared that this study has received no financial support.
Authorship Contributions
Concept – KBY, SB; Design – KBY, MA, SB; Supervision – MA, AI, SB; Fundings – HK, BB, ST; Materials – ST, SB, HK; Data collection and/or processing – MA, SB, ST, EO; Analysis and/or interpretation – SB, KBY, HK, EO; Literature review – SB, BB, AI, HK; Writing – SB, KBY, MA; Critical review – SB, AI, BB.
References
- 1.Patel KN, Yip L, Lubitz CC, Grubbs EG, Miller BS, Shen W, et al. The American Association of Endocrine Surgeons Guidelines for the definitive surgical management of thyroid disease in adults. Ann Surg. 2020;271:e21–93. doi: 10.1097/SLA.0000000000003580. [DOI] [PubMed] [Google Scholar]
- 2.Lefevre JH, Tresallet C, Leenhardt L, Jublanc C, Chigot JP, Menegaux F. Reoperative surgery for thyroid disease. Langenbecks Arch Surg. 2007;392:685–91. doi: 10.1007/s00423-007-0201-6. [DOI] [PubMed] [Google Scholar]
- 3.Shaha AR. Revision thyroid surgery-technical considerations. Otolaryngol Clin North Am. 2008;41:1169–83. doi: 10.1016/j.otc.2008.05.002. [DOI] [PubMed] [Google Scholar]
- 4.Medas F, Tuveri M, Canu GL, Erdas E, Calò PG. Complications after reoperative thyroid surgery: retrospective evaluation of 152 consecutive cases. Updates Surg. 2019;71:705–10. doi: 10.1007/s13304-019-00647-y. [DOI] [PubMed] [Google Scholar]
- 5.Gür HÜ, Madenci C, Çıtlak G, Yüksel S, Ferlengez E, Erözgen F. Is morbidity high in completion thyroidectomy? Med Bull Haseki. 2019;57:69–74. [Google Scholar]
- 6.Benek S, Kocakuşak A, Özer B, Kızılkaya MC, Erözgen F, Çiftçi F, et al. The ever-changing configuration of the completion thyroidectomy in the last decade. Med Bull Haseki. 2015;53:225–8. [Google Scholar]
- 7.Cho JG, Byeon HK, Oh KH, Baek SK, Kwon SY, Jung KY, et al. Objective assessment of postoperative swallowing difficulty through ultrasound in patients undergoing thyroidectomy. Dysphagia. 2020;35:253–60. doi: 10.1007/s00455-019-10020-1. [DOI] [PubMed] [Google Scholar]
- 8.Alkan Z, Yigit O, Adatepe T, Uzun N, Kocak I, Sunter V, et al. Effect of anti-adhesive barrier use on laryngotracheal movement after total thyroidectomy: an electrophysiological study. Indian J Otolaryngol Head Neck Surg. 2014;66:71–7. doi: 10.1007/s12070-011-0319-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yuan X, Shen J, Chen L, Wang L, Yan Q, Zhang J. Onion extract gel is not better than other topical treatments in scar management: A meta-analysis from randomised controlled trails. Int Wound J. 2021;18:396–409. doi: 10.1111/iwj.13542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Özay R, Yavuz OY, Aktaş A, Yiğit F, Çetinalp NE, Özdemir HM, et al. Effects of cepae extract, allantoin, and heparin mixture on developing andalready formed epidural fibrosis in a rat laminectomy model. Turk J Med Sci. 2016;46:1233–9. doi: 10.3906/sag-1504-16. [DOI] [PubMed] [Google Scholar]
- 11.Aysan E, Bektas H, Ersoz F, Sari S, Huq G. Effects of contractubex on the prevention of postoperative peritoneal adhesion. J Surg Res. 2010;164:193–7. doi: 10.1016/j.jss.2010.05.045. [DOI] [PubMed] [Google Scholar]
- 12.Zühlke HV, Lorenz EM, Straub EM, Savvas V. Pathophysiology and classification of adhesions [Article in German] Langenbecks Arch Chir Suppl II Verh Dtsch Ges Chir. 1990:1009–16. [PubMed] [Google Scholar]
- 13.Dogan L, Karaman N, Yilmaz KB, Ozaslan C, Atalay C. Total thyroidectomy for the surgical treatment of multinodular goiter. Surg Today. 2011;41:323–7. doi: 10.1007/s00595-009-4272-6. [DOI] [PubMed] [Google Scholar]
- 14.Alesina PF, Rolfs T, Hommeltenberg S, Hinrichs J, Meier B, Mohmand W, et al. Intraoperative neuromonitoring does not reduce the incidence of recurrent laryngeal nerve palsy in thyroid reoperations: results of a retrospective comparative analysis. World J Surg. 2012;36:1348–53. doi: 10.1007/s00268-012-1548-6. [DOI] [PubMed] [Google Scholar]
- 15.Barczyński M, Konturek A, Pragacz K, Papier A, Stopa M, Nowak W. Intraoperative nerve monitoring can reduce prevalence of recurrent laryngeal nerve injury in thyroid reoperations: results of a retrospective cohort study. World J Surg. 2014;38:599–606. doi: 10.1007/s00268-013-2260-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bae DS, Woo JW, Paek SH, Kwon H, Chai YJ, Kim SJ, et al. Antiadhesive effect and safety of sodium hyaluronate-carboxymethyl cellulose membrane in thyroid surgery. J Korean Surg Soc. 2013;85:199–204. doi: 10.4174/jkss.2013.85.5.199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Park KS, Lee KE, Ku do H, Kim SJ, Park WS, Kim HY, et al. Antiadhesive effect and safety of oxidized regenerated cellulose after thyroidectomy: a prospective, randomized controlled study. J Korean Surg Soc. 2013;84:321–9. doi: 10.4174/jkss.2013.84.6.321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Makay O, Isik D, Erol V, Yenisey C, Kose T, Icoz G, et al. Efficacy of simvastatin in reducing postoperative adhesions after thyroidectomy: an experimental study. Acta Chir Belg. 2017;117:77–83. doi: 10.1080/00015458.2016.1242292. [DOI] [PubMed] [Google Scholar]
- 19.Idiz O, Aysan E, Firat D, Ersoy YE, Cengiz MB, Akbulut H, et al. Efficacy of glycerol and flax seed oil as anti-adhesive barriers after thyroidectomy. Med Sci Monit. 2014;20:1090–4. doi: 10.12659/MSM.890460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yigit O, Uslu Coskun B, Coskun H, Yilmaz B, Alkan S, Cinar U, et al. Efficacy of anti-adhesive barriers in secondary thyroidectomy: an experimental study. Laryngoscope. 2004;114:1668–73. doi: 10.1097/00005537-200409000-00031. [DOI] [PubMed] [Google Scholar]
- 21.Poetschke J, Gauglitz GG. Onion extract. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, editors. Textbook on Scar Management. Cham: Springer; 2020. pp. 209–13. [Google Scholar]
- 22.Lim YS, Kim HB, Park JH, Cho CG, Park SW, Lee JS, et al. Effects of excessive fibrin deposit and polylactide adhesion barrier on wound healing in thyroidectomy murine wound model. Head Neck. 2018;40:1207–13. doi: 10.1002/hed.25096. [DOI] [PubMed] [Google Scholar]
- 23.Aksakal N, Goksoy B, Onder SY, Dogan S, Gok AFK, Barbaros U. A new cross-linked hyaluronic acid gel for preventing adhesion after thyroid surgery: an animal study. J Surg Res. 2021;265:147–52. doi: 10.1016/j.jss.2021.03.044. [DOI] [PubMed] [Google Scholar]
- 24.Bin Saleem R, Bin Saleem M, Bin Saleem N. Impact of completion thyroidectomy timing on post-operative complications: a systematic review and meta-analysis. Gland Surg. 2018;7:458–65. doi: 10.21037/gs.2018.09.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Menekşe G, Çelik H, Erdem Y, Güvenç Y, Çıkla U, Kul H, et al. Anti-adhesion properties of contractubex® in a rat laminectomy model: a morphological and histopathological study. Journal of Neurological Sciences. 2015;32:46, 708–17. [Google Scholar]
- 26.Ozmen I, Gunal YD, Atasoy P, Kisa U, Yorubulut S, Aslan MK, et al. The effect of extractum cepae, heparin sodium, and allantoin in experimental peritoneal adhesion. Indian J Surg. 2020;82:892–8. [Google Scholar]
- 27.Seref K, Sonmez K, Gulburun MA, Ekinci O, Oge CB, Gulbahar O, et al. Protective effects of contractubex® on stricture formation after experimental corrosive esophageal burns in rats. Arch Med Res. 2020;51:664–9. doi: 10.1016/j.arcmed.2020.06.017. [DOI] [PubMed] [Google Scholar]
- 28.Ayengin K, Kılıç N. Use of contractubex® (allantoin, heparin, extractum cepae) to prevent scar formation in the rabbits to which primary closure has been applied after urethrotomy. East J Med. 2020;23:161–9. [Google Scholar]