

Abstract
Introduction:
A case report of small bowel obstruction related to barbed suture in a postoperative patient of laparoscopic sacrocolpopexy.
Case Description:
A 61 -year-old female with a body mass index of 27 with vault prolapse underwent laparoscopic sacrocolpopexy. The patient was discharged on postoperative day two. She presented again in the emergency department on the fifth postoperative day with complaints of frequent vomiting episodes with intermittent and colicky pain in the abdomen. Her imaging (computed tomography abdomen/pelvis with oral contrast) suggested distal small bowel mechanical obstruction at midileum with significant free fluid in the peritoneum. Emergency laparoscopic exploration was done. Peroperative V-LocTM 180 suture tail end barbs were found anchored to the mesentery of midileum causing a loop that led to compression and occlusion of distal bowel. The barbed suture tail end was detached from the mesentery and thus relieving the compression. No additional procedure was required for the bowel wall. The excess barbed suture tail end outside the peritoneum was trimmed. The postoperative course was uneventful.
Conclusion:
Bowel complication is an uncommon but serious issue following the use of barbed sutures. It should be used with utmost caution as none of the preventive measures are completely safe. Further studies need to be done for preventive measures.
Keywords: Barbed suture, Laparoscopic sacrocolpopexy, Small bowel obstruction
INTRODUCTION
Laparoscopy has evolved tremendously over time, with numerous advanced technologies that enhance our surgical skills and increase precision. Endo suturing, especially knots tying in laparoscopic surgery, is still a challenging procedure and requires a significant learning curve to perform accurately. The barbed suture was introduced as a boon for laparoscopic surgeons to overcome this arduous work of endo suturing with knot tying. This new technique involves the use of the standard suture material with axially spaced barbed segments on each side of a midpoint. At the midpoint, the barbs change direction allowing self-anchoring and a more uniform distribution of the tension, without the need to tie any knots.1 This allows for a dependable substitute for conventional sutures during laparoscopic surgery.
However, any new advancement has its pros and cons. Several cases2,3 have been reported regarding the potential drawbacks of the use of barbed sutures. Exposed suture barbs may anchor to adjacent small bowel mesentery or omentum and cause serosal injury, obstruction leading to volvulus, necrosis, and even perforation. We report a case of small bowel obstruction related to barbed suture in a postoperative patient of laparoscopic sacrocolpopexy.
CASE DESCRIPTION
A female of 61 years of age with a body mass index of 27 presented to our outpatient department with chief complaints of vault prolapse. She was planned and posted for laparoscopic sacrocolpopexy after proper clinical examination and detailed pre-operative evaluation. Intraoperatively, the right retroperitoneal space was opened starting from the sacral promontory to the vault. The right medial pararectal space (Okabayashi space), rectovaginal, and vesicovaginal space were dissected. The vagina was freed off the bladder anteriorly and rectum posteriorly to achieve adequate space for mesh placement and suturing. Prolene mesh was anchored at the vault and sacral promontory with Ethicon Ethibond ExcelTM polyester suture, maintaining adequate tension along the mesh. The further peritoneal defect was completely closed with V-LocTM 180, taking two reverse stitches in the backward direction as given in the instruction for the user pamphlet and the mesh was thoroughly shielded. The barbed suture tail end was cut flushed to the peritoneum with almost zero remanent length (Figure 1). The patient passed flatus and stool on the second postoperative day. The patient was discharged on the second postoperative day in stable condition with no complaints. The patient presented in the emergency department on the fifth postoperative day with complaints of frequent vomiting episodes during the last 24 hours associated with intermittent and colicky pain in the abdomen. She also complained of constipation for the previous two to three days. Clinical examination revealed abdominal distention and mild guarding with deteriorating vital condition. Her imaging (computed tomography abdomen/pelvis with oral contrast) findings were consistent with distal small bowel mechanical obstruction at midileum, with proximal small bowel dilatation with significant free fluid in the peritoneal cavity (Figure 2). Pre-operative nasogastric tube delivered fluid with bilious component (approximately 1200 ml). The decision was made for emergency laparoscopic exploration. Intraoperative exploration revealed V-LocTM suture tail end barbs anchored to the mesentery of mid ileum causing a loop which led to compression and occlusion of distal bowel (Figure 3). The affected bowel loop was significantly distended with an oedematous bowel wall (Figure 4). The barbed suture tail end was detached from the mesentery and thus relieving the compression over the affected bowel loop. Further bowel wall was checked for its vascularity and integrity and no additional intervention was required. Approximately 5 cm of barbed suture tail end was seen outside the peritoneum which was trimmed (Figure 5). The postoperative course was uneventful and the patient was discharged after three days in a stable condition.
Figure 1.
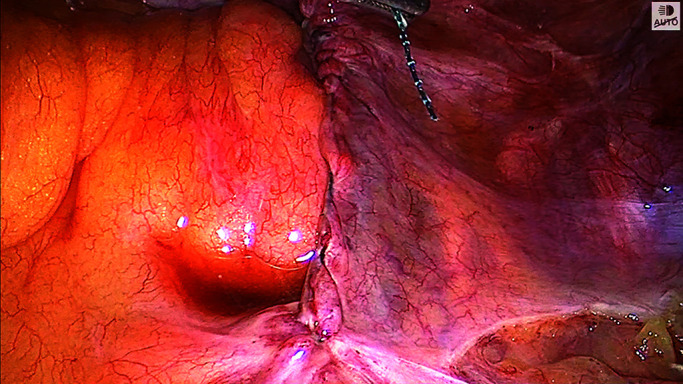
Laparoscopic intra operative image of primary surgery showing that the The V-LocTM 180 suture was cut flush to the peritoneum.
Figure 2.

Abdominal CT image with contrast showing arrow at small bowel obstruction at distal jejunal and proximal-mid ileum loop in left lumbar region.
Figure 3.

Laparoscopic intra operative image of secondary surgery showing tail of V-LocTM 180 suture anchored to mesentery of mid ileum.
Figure 4.
Laparoscopic intra operative image of secondary surgery showing extended tail of V-LocTM 180 suture after releasing it from mesentery of bowel.
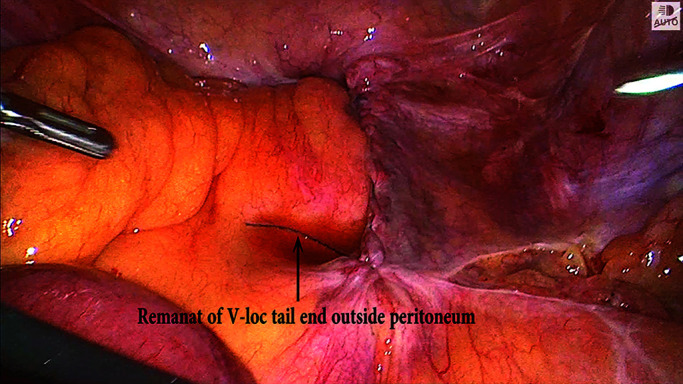
Figure 5.
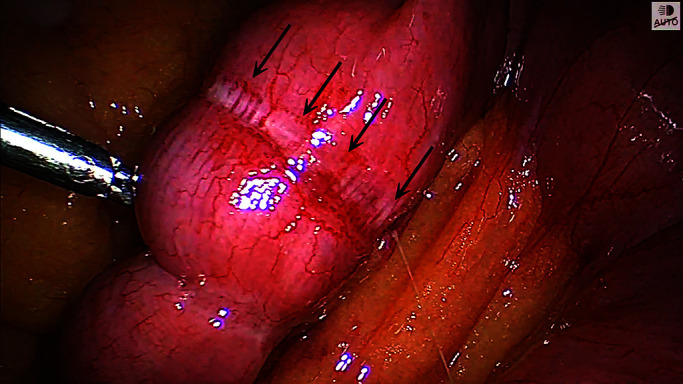
Laparoscopic intra operative image of secondary surgery with arrow showing impression of V-LocTM 180 suture over bowel wall after release of stricture and oedematous bowel wall.
DISCUSSION
Barbed suture is frequently used in various laparoscopic gynecologic procedures as in myoma bed closure, peritonization of mesh in sacrocolpopexy, or vaginal cuff closure in hysterectomy. Its knotless property and built-in barb anchors to tissue, thus avoiding slippage and maintaining a uniform tensile strength throughout the stitch line.4
The barbed suture has been very beneficial and rewarding, especially during laparoscopic suturing. It leads to a faster closure with subsequent decreased operative time. But every newer advancement has its snag. Numerous cases of bowel obstruction following the use of barbed sutures have been documented in the literature. As per a review of literature total of 24 cases3,5 of small bowel obstruction associated with barbed suture use have been documented to date in gynecological and surgical procedures. All the reported cases had a common finding of barbed suture tail end anchored to bowel mesentery or omentum leading to obstruction, volvulus, necrosis, and perforation.2
In this case report, barbed suture was used per the instructions and safety profile. Two reverse stitches were taken in the backward direction, as instructed by the user pamphlet, and the suture was cut flush to the tissue. The peritoneum possibly contracts during the healing of tissue, so the barbed suture tail end is squeezed out unidirectionally. Other mechanisms possibly causing the same might be due to the comparative more adhesive nature of barbed sutures to other conventional sutures. Incidentally, if barbed suture is anchored to the mesentery or bowel wall; the length of secured tail end further increases due to subsequent pulls by intestinal peristalsis. The same mechanism was explained in studies by Sakata et al.6 and Api et al.7 A similar case report as ours was reported in various other studies.3,8–10
Bowel obstruction has been reported as early as postoperative day 3 to as late as 122 days. Also, the absorbable time for barbed suture is prolonged, ranging from 90 – 180 days. An extended follow-up is advisable in all patients in whom barbed suture was used.11
A review of the literature suggests preventive measures to preclude adhesion of barbed suture to tissue that include: complete burying of the suture tail end into the tissue through two backward stitches, application of a surgical clip at the tail end of the suture, or use of anti-adhesive material over suture to prevent direct contact of tissue with the suture.3,5 Burying of the suture tail end into the tissue through two backward stitches has been used in the mentioned index case, which was not effective enough to prevent small bowel obstruction. Surgical clip or use of Lapra-Ty suture clip application at the tail end of the suture has also been associated with bowel obstruction.12,13 The role of anti-adhesive material as a preventive measure for bowel obstruction is still not proven. There was a case report documenting bowel wall obstruction even after the use of antiadhesive material.8 On the contrary, use of anti-adhesive material also increases the surgical cost. Alternatively, polyglactin 910 (Vicryl 2-0) can be used for peritoneal closure. It does not have any documented significant complication as per our knowledge. The same is opined by other studies.3
The authors have experience with 959 cases of barbed sutures over the last five years in various laparoscopic gynecological procedures such as vaginal cuff closure, myomectomy, and sacrocolopexy. We have experienced only one case (approximately 00.1%) of bowel obstruction following the use of barbed sutures till now, which makes it comparatively safer with all precautions duly taken. Other studies in the literature also have a similar complication rate of bowel obstruction following the use of barbed sutures (1/400, 00.5%).3
According to other studies,3,5 one should exercise caution with barbed sutures where there is direct exposure of barb to tissue in the peritoneal cavity as in peritonization procedures, vaginal cuff closure, or hernia repair. It is our opinion that barbed sutures can be used with caution with comparable safety. A high index of suspicion should be exercised especially while working with barbed sutures for any features suggestive of bowel obstruction. These cases should be under strict supervision with a plan for active management rather than conservative treatment.
CONCLUSION
Bowel complication is an uncustomary yet serious complication following the use of barbed sutures. It should be used with utmost caution as none of the preventive measures are completely safe. Thus, a long follow-up is required in all cases of barbed suture usage, especially where there is intraperitoneal exposure. Further studies are needed to decipher the measures that will intercept this catastrophic complication associated with the use of barbed sutures in surgical procedures. Further clinical trials need to be done for preventive measures.
Footnotes
Disclosure: none.
Funding sources: none.
Conflict of interests: none.
Informed consent: Dr. Dipak Limbachiya declares that written informed consent was obtained from the patient/s for publication of this study/report and any accompanying images.
Contributor Information
Dipak Limbachiya, Department of Gynaecological Endoscopy, Eva Women's Hospital, Ahmedabad, India..
Rajnish Tiwari, Department of Gynaecological Endoscopy, Eva Women's Hospital, Ahmedabad, India..
Rashmi Kumari, Department of Gynaecological Endoscopy, Eva Women's Hospital, Ahmedabad, India..
Manoj Aggarwal, Department of Gynaecological Endoscopy, Eva Women's Hospital, Ahmedabad, India..
References:
- 1.Alessandri F, Remorgida V, Venturini PL, Ferrero S. Unidirectional barbed suture versus continuous suture with intracorporeal knots in laparoscopic myomectomy: a randomized study. J Minim Invasive Gynecol. 2010;17(6):25–729. [DOI] [PubMed] [Google Scholar]
- 2.Segura-Sampedro JJ, Ashrafian H, Navarro-Sánchez A, Jenkins JT, Morales-Conde S, Martínez-Isla A. Small bowel obstruction due to laparoscopic barbed sutures: an unknown complication? Rev Esp Enferm Dig. 2015;107(11):677–680.Nov [DOI] [PubMed] [Google Scholar]
- 3.Stabile G, Romano F, De Santo D, et al. Case report: bowel occlusion following the use of barbed sutures in abdominal surgery. A single-center experience and literature review. Front Surg. 2021;8:626505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Greenberg JA, Goldman RH. Barbed suture: a review of the technology and clinical uses in obstetrics and gynecology. Rev Obstet Gynecol. 2013;6(3–4):107–115. [PMC free article] [PubMed] [Google Scholar]
- 5.Wang L, Maejima T, Fukahori S, et al. Bowel obstruction and perforation secondary to barbed suture after minimally invasive inguinal hernia repair: report of two cases and literature review. Surg Case Rep. 2021;7(1):161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sakata S, Kabir S, Petersen D, Doudle M, Stevenson AR. Are we burying our heads in the sand? Preventing small bowel obstruction from the V-loc® suture in laparoscopic ventral rectopexy. Colorectal Dis. 2015;17(9):O180–O183. [DOI] [PubMed] [Google Scholar]
- 7.Api M, Boza A, Cikman MS, Aker FV, Onenerk M. Comparison of barbed and conventional sutures in adhesion formation and histological features in a rat myomectomy model: randomized single blind controlled trial. Eur J Obstet Gynecol Reprod Biol. 2015;185:121–125. [DOI] [PubMed] [Google Scholar]
- 8.Chen H, Hong MK, Ding DC. Acute small bowel obstruction caused by barbed suture on the second day after laparoscopic hysterosacropexy: a case report and literature review. Taiwan J Obstet Gynecol. 2017;56(2):247–249. [DOI] [PubMed] [Google Scholar]
- 9.Buchs NC, Ostermann S, Hauser J, Roche B, Iselin CE, Morel P. Intestinal obstruction following use of laparoscopic barbed suture: a new complication with new material? Minim Invasive Ther Allied Technol. 2012;21(5):369–371. [DOI] [PubMed] [Google Scholar]
- 10.Thubert T, Pourcher G, Deffieux X. Small bowel volvulus following peritoneal closure using absorbable knotless device during laparoscopic sacral colpopexy. Int Urogynecol J. 2011;22(6):761–763. [DOI] [PubMed] [Google Scholar]
- 11.Clapp B, Klingsporn W, Lodeiro C, et al. Small bowel obstructions following the use of barbed suture: a review of the literature and analysis of the MAUDE database. Surg Endosc. 2020;34(3):1261–1269. [DOI] [PubMed] [Google Scholar]
- 12.Jang SH, Jung YK, Choi SJ, Ha TK. Postoperative mechanical small bowel obstruction induced by V-Loc barbed absorbable suture after laparoscopic distal gastrectomy. Ann Surg Treat Res. 2017;92(5):380–382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Donnellan NM, Mansuria SM. Small bowel obstruction resulting from laparoscopic vaginal cuff closure with a barbed suture. J Minim Invasive Gynecol. 2011;18(4):528–530. [DOI] [PubMed] [Google Scholar]