

Abstract
Background
Smartphone apps have the potential to address some of the current issues facing service provision for young people’s mental health by improving the scalability of evidence-based mental health interventions. However, very few apps have been successfully implemented, and consensus on implementation measurement is lacking.
Objective
This review aims to determine the proportion of evidence-based mental health and well-being apps that have been successfully adopted and sustained in real-world settings. A secondary aim is to establish if key implementation determinants such as coproduction, acceptability, feasibility, appropriateness, and engagement contribute toward successful implementation and longevity.
Methods
Following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, an electronic search of 5 databases in 2021 yielded 18,660 results. After full-text screening, 34 articles met the full eligibility criteria, providing data on 29 smartphone apps studied with individuals aged 15 to 25 years.
Results
Of 34 studies, only 10 (29%) studies were identified that were evaluating the effectiveness of 8 existing, commercially available mental health apps, and the remaining 24 (71%) studies reported the development and evaluation of 21 newly developed apps, of which 43% (9/21) were available, commercially or otherwise (eg, in mental health services), at the time of enquiry. Most studies addressed some implementation components including adoption, acceptability, appropriateness, feasibility, and engagement. Factors including high cost, funding constraints, and lengthy research processes impeded implementation.
Conclusions
Without addressing common implementation drivers, there is considerable redundancy in the translation of mobile mental health research findings into practice. Studies should embed implementation strategies from the outset of the planned research, build collaborations with partners already working in the field (academic and commercial) to capitalize on existing interventions and platforms, and modify and evaluate them for local contexts or target problems and populations.
Trial Registration
PROSPERO CRD42021224365; https://tinyurl.com/4umpn85f
Keywords: adolescent mental health, smartphones, mobile apps, apps, implementation science, mobile phone
Introduction
Background
There has been a proliferation in the number of smartphone apps being developed, both commercially and in academic research programs, which aim to improve mental health and well-being. Recent estimates suggest that anywhere from 10,000 [1] to 22,750 mental health apps exist [2]. Although many of these apps can be accessed directly by individuals in the commercial app marketplace as self-care tools, they are also playing an increasing role in clinical services, supplementing or enhancing traditional interventions [3]. The rapid expansion in the research and development of mental health and well-being apps highlights how much interest and potential there is thought to be in the mobile health arena.
Most common mental health disorders, including depression and anxiety, have their onset during adolescence and, if not successfully resolved, can lead to negative impacts well into adulthood [4,5]. Given the increasing number of young people (between the ages of 15 and 25 years) using digital technologies, smartphone-based interventions provide a scalable solution to support this group to manage their mental health and well-being [6]. Apps have the potential to address some of the accessibility issues in service provision for young people’s mental health, especially for underserved populations. Emerging evidence suggests that some apps may produce significant symptom improvement across multiple outcomes compared with waitlist or control conditions [7-9]. Despite this promise, empirical research often fails to translate into meaningful and sustained implementation in “real-world” settings [10,11]. This can be attributed, in part, to the complex and lengthy process of implementing and maintaining evidence-based approaches in practice, as well as the commercial and regulatory complexities of scaling up mobile technologies in health services [12,13]. Besides innovation and efficacy, other factors, including user engagement, usability, acceptability, accessibility, and low cost, are key prerequisites for adoption, scalability, and uptake [14-17].
Given these multifaceted challenges, it is important to identify what facilitates and inhibits the implementation of mobile mental health interventions [10]. Currently, our understanding of how mental health apps are implemented in real-world settings is limited in several ways. Foremost, implementation processes and outcomes from research trials are seldom recorded or reported, and implementation efforts often lack a solid theoretical or model-based approach, making it difficult to understand and explain how and why implementation succeeds or fails [18,19]. In the context of mobile mental health apps, successful implementation can be measured by the extent to which the intervention has been embedded into service provision, the number of app users, the frequency of app use, app engagement, and evidence of sustained use following the end of a research trial [20,21]. Assessing implementation outcomes using a conceptually grounded framework allows for a systematic assessment of outcomes while also supporting the rigor and reproducibility of implementation research and providing building blocks for the implementation of future interventions.
Existing scoping and systematic reviews have focused on reviewing and critically appraising the methodological rigor and quality of implementation effectiveness studies, reporting implementation outcomes as their primary outcomes [22,23]. To the best of our knowledge, no review has taken a systematic approach to assessing the successful implementation and sustainment of all evidence-based mental health apps for young people. In this review, we assessed the factors influencing implementation success according to a set of implementation outcome criteria based on a modified version of the implementation framework by Proctor et al [24]. In total, 10 implementation variables were examined, of which 8 were from the Proctor model: acceptability (perceived usefulness and satisfaction with a technology), appropriateness (fitness for purpose), feasibility (extent to which a technology was successfully used), fidelity (implementation as intended), cost (financial impact of technology implementation), adoption (technology uptake and use), penetration (spread or reach of the technology), and sustainability (sustained uptake by users or maintenance or integration of a technology within a health care service). Two additional relevant outcomes were added: coproduction (user involvement in intervention development and evaluation) and engagement (adherence and dropout) [25,26].
Although conceptually distinct constructs, the implementation variables listed above are dynamically interrelated and sequentially contingent on one another [24,27]. For an app to be engaging, widely adopted, and well sustained, it must first be acceptable, appropriate, and feasible. It may be that an app-based intervention is deemed highly relevant and applicable to young people’s needs (high appropriateness) but may be costly to download and time intensive (low feasibility). Similarly, an intervention may be considered by a mental health service as a good fit to address young people’s needs (high appropriateness); nevertheless, the service user may be reluctant to use it if they dislike a certain feature of the intervention (low acceptability). Given the potential benefits of smartphone apps in supporting the mental health and well-being of young people, it is critical that researchers and app developers place greater emphasis on enhancing the engagement, implementation, and scalability of efficacious interventions in local contexts or specific populations.
Research Questions
The aim of this review was to determine how successfully evidence-based mobile apps, which aim to promote well-being and mental health outcomes in young people, are adopted, scaled up, and sustained in real-world settings. The research questions of interest were as follows:
What proportion of evidence-based mental health apps are sustained and adopted after development?
What components are needed for successful implementation outcomes and what are the common barriers?
Methods
The systematic review protocol was registered in PROSPERO (CRD42021224365).
Literature Search and Search Strategy
An information specialist (EH) performed an electronic search of the following databases from January 1, 2011, to the search date on February 2, 2021: Ovid Embase, Ovid MEDLINE, Ovid PsycINFO, Cochrane Database of Systematic Reviews, and Cochrane Central Register of Controlled Trials. The search strategies used text words and relevant indexing to capture the concepts of studies on the effectiveness or trials of mental health apps for young people. The search strategy was guided by similar reviews exploring digital mental health interventions for young people [25], and the terms for apps were derived from Cochrane reviews [28,29]. The full search strategies are available in Multimedia Appendix 1. Duplicates were removed following the method described by Falconer [30], and records were then screened by titles and abstracts to complete the process manually. The reference lists of included studies and relevant systematic reviews were assessed for additional relevant studies. All references were exported to Endnote X9 (Clarivate) and then to the systematic review software Rayyan [31].
Inclusion and Exclusion Criteria
The focus of this review was the implementation of app-based interventions that aim to promote mental health and well-being, prevent mental health problems, and treat existing mental health problems in young people. Screened articles were included if (1) the study targeted young people with a mean age of 15 to 25 years, with or without a formal mental health or physical health diagnosis (eg, targeting anxiety in adolescents with diabetes); (2) the intervention was an efficacious “native” mobile app (ie, not on a web browser), whose primary aim was to promote well-being, prevent mental health problems, or treat existing mental health problems; (3) the primary outcome was a measure of mental health or well-being, including change in anxiety and depressive symptoms, diagnosis, problem severity, problem improvement, recovery, remission, or more general change in mental health or well-being across at least 2 time points (eg, baseline and after the intervention or follow-up); and (4) the intervention was efficacious, that is, it had beneficial mental health or well-being outcomes compared with any other type of digital intervention, usual care (eg, psychotherapy), waitlist control group, or no-intervention control group. Both randomized and nonrandomized studies were considered for inclusion.
Articles were excluded if (1) the mean age of participants was not 15 to 25 years; (2) the intervention was not a mobile app, such as other digital interventions, including therapy delivered by phone, SMS text message, video platforms, or PC (eg, computer-based cognitive behavioral therapy); (3) the apps used were not efficacious (ie, there was no significant improvement in mental health or well-being compared with a control group); (4) the apps used did not include an intervention component (ie, primarily focused on diagnosis or assessment); (5) the studies did not report mental health outcomes or the primary outcome was physical (eg, blood sugar levels or exercise); and (6) the studies did not have a control group. Gray literature was not included in the search.
Study Selection
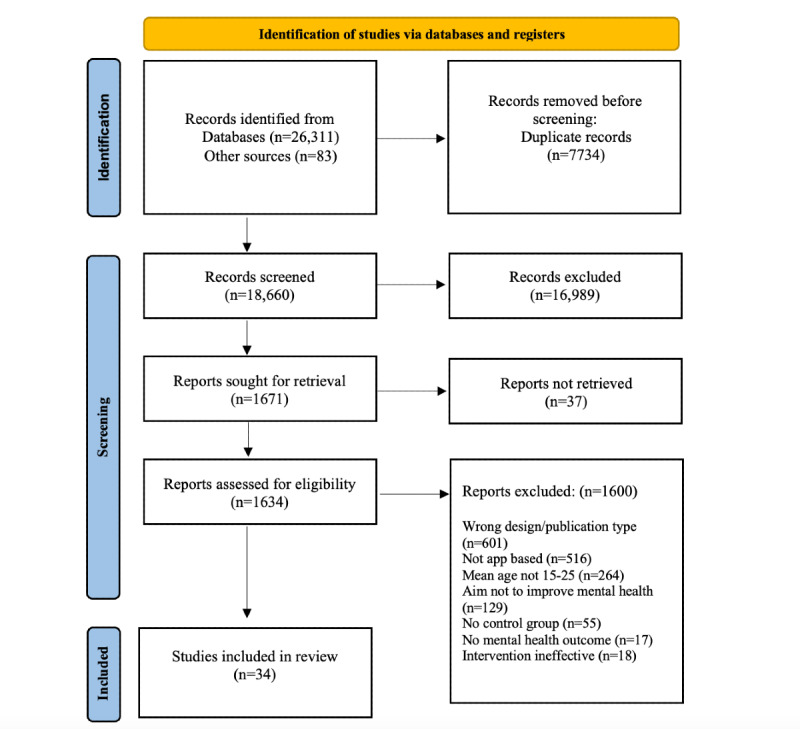
In accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [32], the flowchart presented in Figure 1 provides step-by-step details of the study selection procedure. The search strategy identified 18,660 citations after the removal of duplicates. Of these 18,660 studies, 1634 (8.75%) were considered potentially relevant based on their titles and abstracts. Three members of the review team (HB, LAN, and JD) screened the titles and abstracts against the inclusion criteria. The remaining full texts were screened by 6 members of the review team (HB, LAN, JD, SL, BM, and LN). At this stage, 20% of the texts were screened by at least 2 reviewers independently to ensure interrater reliability (intraclass correlation coefficient range 0.88-0.96). Any disagreements between the 2 reviewers were resolved through discussion with the wider review team.
Figure 1.
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the study selection process.
Data Extraction
Data were extracted by 1 reviewer (HB or LAN) and reviewed for accuracy and completeness by another. After verifying all the extracted data, discrepancies were resolved through discussion or adjudication by another party (MF). Extracted data included information on study characteristics (eg, authors, publication year, country, study design, and study population), intervention characteristics (eg, characteristics of the technology, app name, therapeutic modality, and intervention outcomes), and implementation constructs (eg, implementation objectives and implementation results). Textbox 1 provides a description of the implementation outcome criteria.
Description of implementation variables.
Outcome and definition
Coproduction: user involvement in the development or evaluation of the intervention through coproduction or another patient and public involvement activities.
Acceptability: perception among stakeholders that a given evidence-based practice is useful, agreeable, palatable, or satisfactory.
Appropriateness: appropriateness is the perceived fit, relevance, suitability, or compatibility of an innovation with a practice setting or context.
Feasibility: actual fit, utility, or suitability and the extent to which an evidence-based practice can be successfully used or conducted within a given context.
Fidelity: extent to which an evidence-based practice is being delivered as intended. This includes adherence and the quality of program delivery.
Adoption: intention, decision, or initiation to use or uptake an evidence-based practice.
Engagement: user enrollment, attendance, session participation, homework completion, adherence, and dropout.
Penetration: spread, reach, and integration of an evidence-based practice in “real-world” settings.
Implementation cost: costs associated with implementing an evidence-based practice. This includes cost-effectiveness and cost-benefit.
Sustainability: uptake by users and the extent to which a newly implemented evidence-based practice is maintained and continued within a service setting’s ongoing, stable operations.
Quality Assessment
The mixed methods appraisal tool (version 2018) was used to assess the methodological quality of the included studies [33]. It was developed by combining the core relevant methodological criteria found in different well-known and widely used qualitative and quantitative critical appraisal tools. It consists of 2 screening questions applicable to all types of study design and a further 5 questions applicable to specific study designs. Responses were rated on a categorical scale as “no,” “unclear,” or “yes” to any of the methodological quality criteria. Quality assessments were made by 1 of 3 reviewers (SL, BM, and LN). We did not exclude any studies based on quality assessment scores.
Data Synthesis and Analysis
The extracted data were collated and summarized to produce a narrative summary of the study, sample, and intervention characteristics. To determine the proportion of apps that were sustained or adopted after development, we contacted the corresponding author of the included articles to complete a brief survey about the development and implementation of the app described in their study (Multimedia Appendix 2). If they did not respond, the first or lead author was then contacted. In addition, we searched to check the availability and discoverability of the app in the Apple App Store (iPhone or Mac) and Google Play Store. A codebook approach was used to code and synthesize implementation data from all available sources according to the 10 implementation outcome categories [34].
Results
The systematic search identified 34 studies published between 2011 and 2021, corresponding to 29 unique apps that reported a beneficial intervention effect when compared with a control group. Figure 1 provides additional details on the screening and inclusion processes.
Study Characteristics
The characteristics of the included studies are presented in Multimedia Appendix 3 [35-68]. Of the 34 studies, 11 (32%) studies were conducted in the United States; 6 (18%) in the United Kingdom; 3 (9%) in Australia; 2 (6%) each in Italy, Japan, New Zealand, and Spain; and 1 (3%) each in Canada, Iceland, Iran, Israel, South Korea, and Sweden. Most studies (31/34, 91%) were published between 2018 and 2021. Regarding the evaluated sample populations, most studies (24/34, 71%) primarily recruited university students, followed by clinical samples (5/34, 15%), general population samples (5/34, 15%), school students (3/34, 9%), primary care patients (1/34, 3%), and those attending youth organizations (1/34, 3%). In terms of study design, 74% (25/34) of studies were randomized controlled trials (RCTs), 15% (5/34) were pilot RCTs, 6% (2/34) were quasi-experimental, and 6% (2/34) were feasibility trials. Notably, 29% (10/34) of the included studies evaluated the effectiveness of a commercially available app that was not developed by the evaluation study team.
Intervention Characteristics
Multimedia Appendix 4 [35-68] outlines the format and delivery of interventions assessed in the included studies. Of the 34 studies, 15 (44%) studies aimed to treat mental health problems or reduce symptoms, 14 (41%) aimed to promote well-being or mental health, and 5 (15%) aimed to prevent the onset of mental health problems. Most apps studied (29/34, 85%) were stand-alone, and the remainder (5/34, 15%) accompanied other therapeutic interventions.
Successful Implementation
The measurement of successful implementation, such as sustained use following the end of the research trial either commercially (eg, discoverable in app stores) or otherwise (including available to young people via schools or mental health services) varied based on unique features of the app itself, its recipients, and its context. To ascertain the proportion of apps that were sustained after development, we contacted the authors of the included articles to request additional information about the implementation of the app reported in their study. We did not contact the authors of the 18% (6/34) of studies testing existing apps that we knew were commercially available and discoverable to the public at the point of the review (eg, Headspace and Calm); that is, being successfully sustained. Of those contacted (28/34, 82%), we collected 23 survey responses (Multimedia Appendix 5 [35-43,48,50,51,54,55,57-61,63,65-67]), and 5 authors did not respond. However, on reviewing the survey responses, 17% (4/23) were evaluating other apps already available. In the absence of survey data for 5 studies, we checked if they were commercially available; 2 (40%) were discoverable on either the Apple App Store (iPhone or Mac) or Google Play Store (Google Inc) [45,62], and 3 (60%) were not available [52,53,64].
In summary, 10 articles evaluated the effectiveness of an existing app that was available for use at the time of the evaluation study [38,44,46,47,49,54,56,59,60,68]. Of the 10 articles, 8 (80%) evaluated an app still available on the market: Headspace [44,46,47,68], Calm [49], Pacifica/Sanvello [38], Smiling Mind [47], Stop Breathe Think [56], and Thrive [59]. The 2 major smartphone app markets (ie, App Store and Google Play) publicly list app ratings out of 5 on their store pages. Google Play also provides download count estimates. The consumer app ratings on a 5-point scale, from the App Store and Google Play, respectively, are as follows: Headspace (rating 4.9 and 4.25) and Calm (rating 4.8 and 4.25) were the most popular (>10 million downloads), followed by Sanvello (rating 4.8 and 4.5), Stop Breathe Think (rating 4.8 and 4.5), Smiling Mind (rating 4.5 and 3.75; >1 million downloads), and Thrive (rating 5.0 and 3.5; >50,000 downloads). Finally, 2 studies evaluated consumer apps that are no longer available: DeStressify [54] and Lantern [60]; therefore, their store statistics are not reported.
Of the 24 studies reporting on a newly developed app, 43% (9/21) are currently available, commercially or otherwise (eg, in mental health services), and 57% (12/21) are no longer available. Most respondents reported that it took several years to develop and test the app reported in their articles, ranging from 6 months to 6 years.
Markers of Successful Implementation
Adoption
Of the 20 apps sustained after development, several are available noncommercially and freely to users in local contexts, including in mental health services [37,42], for university students [36,59], and for corporate organizations [63]. Apps are also accessible to users via commercial channels, including Apple App Store (iPhone or Mac) and Google Play Store (Multimedia Appendix 6 [35-68]).
Coproduction
A total of 9 unique apps were reported as being coproduced with young people, 5 of which are either currently available or were previously available following the study but no longer available. The level of youth involvement in the coproduction of the apps varied across studies but involved activities such as a web-based survey, which was delivered to 150 young people (ie, the target end users) [61,69]; market research and beta testing [54]; design workshops with 15 key stakeholders, followed by a series of in-depth interviews [67,70]; focus groups with young people with lived experience that guided the development of app functionalities [42]; and study groups with teenagers and young people who were involved in all developmental phases of the app [43]. Coproduction data were not reported in 12 studies.
Acceptability and Appropriateness
Acceptability was generally well assessed with a variety of measures using both qualitative and quantitative methods (k=16). Most studies of implemented apps reported them as acceptable, with high user satisfaction and ease of use among young people and health care providers [43,45,61,69]. O’Dea et al [69] examined adolescents’ attitudes toward the concept of a mobile phone app for relationship help and support and reported that, overall, 60.7% (91/150) were likely to use an app for relationship problems, and this was not associated with demographics or social support (P>.05). Notably, the likelihood of app use was found to be influenced by the perceived need for help, personal beliefs about app effectiveness, and whether the app was engaging and easy to use. Overall, adolescents found the proposed app content helpful, with an average of 99.3% (149/150) rating the strategies provided as somewhat to very helpful. More than 90% of respondents reported that the app was enjoyable, easy to use and understand, and that they would recommend it to a friend [61,69]. The barriers most commonly experienced were mismatched need, forgetfulness, and being time-poor [61,69]. Acceptability was also assessed for the “Personalized Real-time Intervention for Motivational Enhancement (PRIME)” app designed to improve motivation in young people with early-onset schizophrenia during an exit interview 12 weeks after the trial. Participants rated their satisfaction with specific features of the app, such as the ability to interact with peers and the different goal categories, on a scale from 1 (not at all) to 10 (very much) [67]. Schlosser [67] reported that participants rated their overall satisfaction with “PRIME” highly. Similarly, Broglia et al [38] explored the feasibility and acceptability of supplementing college counselling with the “Pacifica” app and whether this, in turn, had positive clinical outcomes. This blended approach to their intervention was shown to be acceptable and feasible and showed the potential to maintain clinical improvement in anxiety following the completion of a brief counselling intervention [38]. Egilsson et al [43] assessed acceptability with the Systematic Usability Scale, a widely used and relatively well-studied 10-item questionnaire on app usability, where scores range from 0 to 100, and a total score of >70 indicates satisfactory usability and user acceptance [71]. The mean total score on the Systematic Usability Scale was satisfactory (mean 78.09, SD 9.82), indicating adequate usability of the app they tested to improve the emotional and physical health of adolescents [43]. Acceptability data were unavailable for 53% (18/34) of studies, and appropriateness data were unavailable for 68% (23/34) of studies.
Feasibility
The extent to which interventions were feasible (ie, the actual fit or practicality) was reported in 35% (12/34) of studies that used a broad range of metrics as indicators of utility and suitability, including log-in frequency, app activity, average number of sessions, recruitment duration, treatment preference, the percentage of participants who completed follow-up assessments, and randomization acceptability [38,42,43,56,67]. To evaluate the feasibility of “PRIME,” the authors examined the log-in frequency, challenges completed, spontaneous and goal achievement moments, peer and coach interactions, and active use rate [67]. Participants in the “Stop, Breathe and Think” trial, which evaluated a publicly available mindfulness app, provided high satisfaction ratings and reported regular use of the app, particularly in the first 2 weeks. However, the rate of recruitment was slow over the course of an academic year, indicating potential feasibility and long-term sustainability concerns [56]. Of the 34 studies, feasibility data were not available for 22 (65%) studies.
Fidelity
Fidelity, the extent to which the interventions were delivered as intended, is a less-prominent implementation determinant for apps, given the content control inherent in the structure of the delivery mechanism. However, it is relevant, for example, in one of the included studies, where fidelity outcomes were reported in transcripts from counselling audio recordings where the app was provided as an adjunct to face-to-face counselling [38]. Transcripts were scored to assess the following criteria: (1) number of times the app was discussed, (2) duration of app discussion, (3) whether therapist reviewed client app use, (4) number of app features therapist suggested, and (5) missed opportunities to discuss client app use [38].
Engagement
Engagement-related factors, including user enrollment, attendance, session participation, homework completion, adherence, study retention, and dropout, were widely reported outcomes across studies. Engagement data were reported in all but 1 study [37]. A consistent and noteworthy finding across several studies was that engagement decreased over time [43,54,67]. Unsurprisingly, young people identified that accessibility and engagement issues, including user experience, influenced their likelihood of using the intervention [61,69]. For example, engagement with 1 app dropped after the first month of the trial before leveling out over the second and third months [67]. Egilsson et al [43] noted a decrease in average exercises performed between the first week of the intervention and subsequent intervention weeks, with a significant 76% decrease in the total number of in-app health exercises from week 1 to week 2.
A total of 10 articles evaluated a consumer (ie, available on the App Store or Google Play) smartphone app at the time of their publication. Data collection methods and the degree of detail for app use differed across studies. Most studies (6/10, 60%) collected information regarding app use from participants’ self-reports [38,44,47,54,59,68], followed by passive activity tracking (2/10, 20%) provided by the official app teams [46,49], combined self-report and passive tracking (1/10, 10% [56]), or not specified (1/10, 10% [60]). Self-report measures were generally 1-item data points, varying from 10-point scales between “did not use at all” and “used as often as requested” [54] to number of times per week [56,59] and yes or no daily measures [47]. In total, 2 studies requested an in-app summary screenshot of completed minutes as a record [44,68], and Yang et al [68] further provided a paper calendar for record tracking. On the other hand, passive activity tracking provided greater detail, including the date, time, and duration of an in-app exercise [46,49,56]. Newman et al [60] did not specify app use data collection methods but recorded more details of use than other studies, such as total visits on the app, number of sessions on the app, and minutes on the app. It is noteworthy that Yang et al [68] reported that individuals in the experimental group who tried Headspace at least once had an average of 12 days of use over the course of their 30-day, laissez-faire (ie, use this app as you would normally) intervention without additional prompts or ongoing accountability. In addition, 74% of those who used the app during the 30-day intervention period continued to use it for an additional 30 days. These findings imply that motivating individuals to use an app just once may be an important step in retention.
Although app use measures provide straightforward indicators of attendance, session participation, homework completion, and adherence are unclear owing to variations in their definitions. Session participation may be synonymous with attendance for some researchers, whereas others operationalize it as meaningful, back-and-forth interactions between a user and agent (eg, app, coach, or counselor). A total of 20% (2/10) of studies reporting on consumer apps included an agent (therapists [38] and coaches [60]) as part of their intervention, but only 1 analyzed whether user-agent communication (ie, session participation) affected efficacy. Newman et al [60] reported “treatment usage” (a composite variable including user-agent interaction), which did not affect symptom outcomes. In addition, homework completion may be defined as completing the prescribed exercises in a study, whereas another study may define it as tasks in addition to the primary intervention. None of the included studies mentioned “session participation” or “homework.” In terms of adherence, 50% (5/10) of studies explicitly measured adherence (eg, app use data, including time spent and sessions using the app) [46,47,49,54,59]. An additional study [56] did not operationalize “adherence,” although they collected characteristic adherence data through self-report, asking users how many days in the past 2 weeks they had used the app. However, given the lack of conceptual clarity and consensus on adherence, it is difficult to assess whether adherence affects clinical health outcomes in the context of consumer app evaluation.
Implementation Cost
Data on the costs associated with implementing the apps, including cost-effectiveness and cost-benefit, are not readily available in the public domain. However, results from the survey indicate that, unsurprisingly, apps developed from scratch were the costliest to develop and test. Notably, several apps included in this review were developed from existing, ready-made platforms, which were modified for different interventions rather than building the app from the ground up. For example, the GGtude platform was developed in 2016 and hosts several apps designed for different populations and presenting problems [35,40,41,66]. This approach has been successful with several studies reporting that daily use of apps from the GGtude platform during a period of 2 weeks (3 minutes a day) is associated with significant beneficial effects on mental health in nonclinical and subclinical samples [40,41,66]. Similarly, Levin et al [55] have focused their efforts on developing app prototypes rapidly using easy-to-use website platforms to customize intervention content and develop generalizable knowledge about principles and processes that work in mobile apps rather than building and developing new apps from scratch [55,57]. However, the authors note that their platform was not set up for commercialization or broad deployment because the app is delivered within the LifeData system and lacks key features needed for a public launch, including budget and support for ongoing technical maintenance and monitoring user inquiries and data. It was also noted that ongoing updates are likely needed to remain relevant and competitive with other market products, which involves undertaking regular market scans and content refinement to ensure the product remains well positioned and effective in an increasingly saturated market [61].
Another approach taken by the authors of the included studies was to evaluate existing, publicly available apps for a specific local context and also as a potential adjunct to existing in-person therapies (eg, university students and college counselling centers) [38,54,56,59,60]. For example, Broglia et al [38] contacted the developers of a mood monitoring app to test its use in conjunction with usual care counselling sessions. Similarly, Levin et al [56] conducted a pilot RCT to evaluate the feasibility and acceptability of a publicly available mindfulness app for university students. Using existing, commercially available apps or building prototypes using adaptable web platforms provides a lower cost and quicker alternative to developing and evaluating new apps from the ground up. However, implementing apps in distinct local contexts requires well-thought-out and tailored implementation strategies, with consideration given to common barriers, especially acceptability and feasibility.
Sustainability and Penetration
Sustainability can be measured in several ways, including apps being fully integrated into service settings and a steady budget for app advertising, maintenance, and updates [21]. The number of app downloads and interactions over time also provides an indication of sustained uptake over time. However, none of the included studies reported data on the sustainability of the interventions evaluated in their study. As such, the literature is sparse regarding the long-term integration and penetration of mobile interventions within mental health and other support service settings.
Study Quality
Methodological quality varied across the included studies (Multimedia Appendix 7 [35-68]). Most studies (32/34, 94%) were judged as having possible limitations in at least 1 criterion. Most studies (29/34, 85%) clearly described the randomization of the study participants or the process for recruiting a representative sample. Most randomized trials reported complete outcome data (30/32, 94%) and described samples that were comparable at baseline (27/32, 84%). However, few studies described the process used to blind the outcome assessor to the intervention group (10/32, 31%). Only half of the studies (16/32, 50%) reported acceptable adherence rates to the intervention. Regarding the 2 nonrandomized trials, both studies used appropriate outcome measures. Of the 2 studies, 1 (50%) was judged as not clearly accounting for confounders in the study design and analysis. Both studies were judged as adhering to the intervention protocol [38,53].
Discussion
Principal Findings
The primary aim of this systematic review was to determine the proportion of evidence-based mental health and well-being apps that have been successfully adopted and sustained in “real-world” settings. In total, 29% (10/34) of studies were identified that evaluated the effectiveness of 8 existing, commercially available mental health apps. The remaining 71% (24/34) of included studies evaluated 21 newly developed apps, of which 43% (9/21) are currently available, commercially or otherwise (eg, in mental health services), and 57% (12/21) were no longer available at the time of enquiry. Therefore, these results not only indicate a 43% implementation success rate of new apps but also provide some information on how existing efficacious commercial apps are promoted and sustained in the field.
Broadly synthesized using 10 dimensions of implementation, our review suggests that measures of adoption, acceptability, appropriateness, and feasibility are more frequently reported than indicators of cost, fidelity, sustainability, and penetration. Implementation outcomes were unavailable for many of the studies, precluding direct comparisons between those apps that were implemented and those that were not across constructs. To partially address our second research question, most of the apps that had been implemented confirmed a degree of adoption, acceptability, appropriateness, feasibility, and engagement. These determinants are relevant to a range of interventions and would benefit from broad systematic incorporation into the development of a smartphone app. Other important factors identified included the coproduction of interventions with young people and the need to embed apps within local settings, such as schools, universities, and mental health services, rather than relying on commercial strategies. Although assessing implementation outcomes using an integrated framework allows for a more systematic assessment of outcomes, the review highlights a lack of measurement precision around implementation constructs in that an array of overlapping terms, such as acceptability and usability, are often used interchangeably, highlighting the need for greater consensus on how to measure and report implementation determinants. There is also a need to elucidate the relationship between different implementation constructs (eg, acceptability and engagement) and intervention effectiveness (eg, clinical change) [22]. Modeling these relationships was not possible in the current review because of data quality issues. Further empirical research is needed to model the interrelationships between implementation variables to better understand the nature of their connections and their impact on implementation success.
Confirming acceptability and engagement in the early phases of intervention development, before implementation commences, is an important step in ensuring that the intervention has potential longevity and may be important for saving time and money. As evidence suggests that engagement is the highest in the first days or weeks of downloading an app, it might be more appropriate for apps to be developed with this anticipated behavior in mind [72].
Research has identified that intervention- and person-specific factors that influence engagement with mobile mental health interventions should be considered [25]. For example, getting individuals to use an app just once is an important step in retention. It is likely that an initial hook is needed to catch the attention of young people to encourage them to identify and download the app. Thereafter, rewards and gamification are reported by young people as motivating factors for ongoing engagement and retention [25]. Similarly, usability has been reported as important for promoting engagement. Acceptability and engagement are critical elements of mental health apps that support users [73]. However, it is recognized that operationalizing meaningful app engagement is not straightforward, as many downloaded apps are never used and more work is needed to define sustained engagement, what leads to it, and how to create products that achieve it [73,74]. Further research may explore characteristics facilitating initial use, continued use, and the implications of changing the treatment structure during an intervention (eg, Do individuals find it motivating or overwhelming?).
Barriers to Successful Implementation
The importance of identifying mental health interventions that are efficacious needs to progress in concert with addressing implementation requirements from the outset of app development. This can be a complicated focus for researchers and funding bodies, as in the absence of efficacy, it might seem premature to address dissemination issues, but given the high redundancy of scientific studies—less than half of the efficacious apps were actually identified as being in sustained use—these questions must be paramount at the outset of the research cycle.
In addition to the markers of successful implementation, there are several extant barriers, including high cost, time, funding constraints, and lengthy research processes. The process of applying for funding, app development, data collection, data analysis, and app release is lengthy and expensive, taking up to 6 years [39]. The sustainability and penetration of apps is contingent on projects being funded or grants being successful, and even when funding is secured, it is often time limited [42,67,75]. The way in which funding streams are set up means that it is harder to secure funding for the follow-on implementation research than for the initial evaluation project.
Other challenges include the continuous, rapidly evolving development of technology, which results in the need for continued code updates and upgrades to allow for compatibility with smartphone operating systems [42,61]. Additional noted barriers include the rapidly changing nature of many commercial providers supplying the app technology, sometimes with significant staff movement, changes to the focus of work depending on commercial drivers, and short life spans of some tech companies [60]. Given that only a small proportion of existing, commercially based apps are being well sustained, rather than developing de novo apps, it might be that evaluating more successful apps and adapting them to specific contexts can propel implementation in the field. However, it is recognized that the commercial app marketplace is highly competitive, and research has identified that, based on our estimates of monthly active users, mindfulness and meditation apps appear to be the most popular: Headspace and Calm account for 13.4 million users, Replika and Wysa account for 1.5 million users, and Reflectly and Daylio account for 840,000 users [76]. In total, these 6 apps monopolize the marketplace, many of which have been made freely available to young people and extensively marketed; hence, they penetrate the market and account for 83% of the monthly active users of mental health and wellness apps [76]. As noted by others, currently, the mental health and well-being apps that have been rigorously evaluated struggle to attract users, and apps with many users are rarely evaluated [76,77].
There are several possible explanations for the success of these commercial apps. Fish and Saul [44] reported that Headspace, one of the most popular consumer apps in the market, applies gamification techniques, such as accomplishment, empowerment, social influence, and ownership to improve engagement and motivate individuals to enjoy meditations and find them rewarding. Several engagement design features in Headspace, such as user tracking, reminder function, and push notifications, can improve engagement, these features were not actively part of any of the evaluated studies and were left for use at the discretion of the individuals [46]. However, Huberty et al [49] report that these features may be critical for engagement and acceptability.
Groups at Risk of Exclusion
An interesting finding of this review is that there are certain groups that are less likely to access mental health and well-being apps. It is noteworthy that most studies included in this review recruited university students (24/34, 71%). There was a marked absence of youth samples from underserved or marginalized populations, including but not limited to migrants, asylum seekers and refugees, those experiencing homelessness, and those from socioeconomically deprived backgrounds. These potentially high-risk groups are typically underrepresented in research, face access and engagement barriers when navigating health care systems, and experience digital exclusion [78]. The studies included in this systematic review had not targeted these populations, and research exploring the acceptability, appropriateness, and feasibility of app-based interventions is lacking.
Limitations
Although this review was rigorous, carefully executed, and used a robust methodological approach, it was not without limitations. Foremost, although the review team attempted to identify and include as many articles as possible, some articles may have been missed because of the inconsistencies in how implementation outcomes are recorded and reported. It was also difficult to ensure that all apps for this age group were identified because those aged between 15 and 25 years are harder to differentiate in adolescent and adult studies, meaning we might have missed some relevant studies. Although the focus of this review was young people aged between 15 and 25 years, most of the included studies recruited university students, and most of the study samples had a mean age of >20 years. This finding suggests that there may be a lack of effective mental health apps targeted at mid to late teenagers. This may be a result of the ethical constraints of recruiting young people aged <18 years (16 years in the United Kingdom) to research studies, as it is easier to recruit those who are deemed able to independently consent to trial participation. Additional research is needed to determine whether mental health apps have been developed for this group; however, upon evaluation, they were deemed ineffective. Given the considerable heterogeneity in the social, emotional, and cognitive development and maturity of young people in this age range, research is needed to understand the potential differential impacts and utility of apps throughout adolescence and young adulthood.
In addition, the review included several apps that were delivered as an adjunct to in-person therapies. It is recognized that the reported successful implementation of these apps may in fact be a by-product of the success of the primary therapeutic intervention rather than the app itself. Research comparing face-to-face therapies with and without additional app support provides evidence to support the superiority of adjunctive interventions compared with standard intervention-only conditions [79]. However, additional research is needed to enable us to determine the role of apps in the successful implementation and sustainability of blended intervention programs.
Unpublished data were not included in the search, which may have affected the results of this review. Nevertheless, this approach was also seen as a further strength by ensuring that only peer-reviewed interventions were included. Given that the focus of our review was on apps that had been found to be efficacious, the publication bias effect was minimal. However, it is possible that companies that have developed the apps possess valuable data pertaining to some aspects of implementation. Commercial companies are likely to have collected a wealth of relevant and informative data on user engagement and app use over several years. However, owing to competing commercial interests and a lack of regulation in the mobile mental health app arena, these data are not publicly available or made openly accessible to researchers [80]. Nonetheless, an attempt was made to obtain implementation data when it was not included in the articles by contacting the study authors, most of whom responded.
Finally, more than two-thirds of the apps were not independently evaluated and, therefore, an important consideration is that “developer bias” may have impacted the analysis and subsequent findings of those trials. More independent and robust evaluation of apps is needed, and findings must be shared in a manner that is accessible to the scientific community as well as the users of the app. This will require time and resources but needs to become integral to the development process to mitigate potential bias in evaluations moving forward [81], be that within purely commercial or research contexts or for commercial-research collaborations.
Recommendations for Research and Practice
Coproduction With Young People
Coproducing interventions with young people may help improve the acceptability and feasibility of the end product, which, in turn, can improve intervention effectiveness [25,26]. Coproduction actively involves relevant stakeholder groups in the design process to help ensure that the technology developed meets their needs and is usable. In coproduction, intended users work with designers, developers, and researchers during the innovation and development process [82]. A range of methods have been used to enact young people’s involvement in health research, often under the umbrella of “Young People’s Advisory Groups” (YPAGs) [83]. This includes, but is not limited to, market research and beta testing, design workshops, in-depth interviews, and focus groups. Consistent reporting on the methods of involvement and outputs of YPAGs in publications will help develop a better understanding of the influence of YPAGs in youth mental health research, enabling better systems for meaningful youth involvement in research [83,84].
Cost-effective Prototyping
To address the lengthy and costly research and evaluation processes, adaptable and modifiable interventions can be developed from existing platforms, which can then be delivered quickly in a personalized way to meet a range of users’ needs. As noted by others, this is complicated by the need to balance scientific rigor with the fast pace with which technology advances to achieve the adoption of evidence-based practice [85]. To address some of the time, funding, and financial burdens, it may be that researchers and clinicians work collaboratively with industry partners to capitalize on existing interventions and platforms, modifying and evaluating them for their local context. However, it is acknowledged that working with developers involves its own set of complex challenges. Often, researchers invest time and resources in the initial stages in building prototypes with developers only to find out that the intervention is ineffective, not feasible, or not economically viable. As an alternative, researchers can take advantage of free or low-cost systems for rapid prototyping, such as Qualtrics, or an Ecological Momentary Assessment platform, such as LifeData or MetricWire.
Assess and Report Implementation Outcomes
Intervention evaluation should include key implementation determinants, such as acceptability, feasibility, appropriateness, and cost. Currently, implementation outcomes are poorly reported, and publications reporting the results of RCTs focus on clinical outcomes, often neglecting sustainability, cost, and the process of embedding the intervention into “real-world” clinical practice. It has been reported that psychological intervention articles report, at most, 64% of the information needed to implement interventions [86]. It is important that researchers use consistent implementation measurement and reporting to allow meaningful and accurate comparisons across studies and share the information required by implementers. Assessing implementation outcomes using a conceptually grounded framework allows for a more systematic assessment of outcomes while supporting the rigor and reproducibility of implementation research and providing the building blocks for implementation evaluation.
Hybrid Intervention Models
There has been increased attention toward “blended” approaches, where web-based support is provided as an adjunct to, rather than a replacement for, face-to-face treatment. The importance of human support in web-based therapies and the perceived value of blending mobile health interventions with traditional face-to-face treatment is well described in the literature [87-89]. A blended approach has the potential to reduce the relative load of costly face-to-face contact while boosting engagement, enhancing outcomes, and increasing treatment acceptability [88].
Early Consideration of Economic Sustainability
To support the implementation of evidence-based and efficacious interventions, early consideration of funding and costs are crucial. Funding bodies should endeavor to develop new, responsive funding streams, including implementation-specific grants, to focus on the implementation of existing evidence-based interventions, as the translation of evidence from feasibility to adoption is poorly realized, bringing considerable redundancy to the field of intervention research. Currently, it is harder for researchers to secure funding for follow-on work than for the initial evaluation project, and it is not possible to secure funding ahead of time for this in the initial app, as they are usually feasibility studies, and so effectiveness cannot be assumed. However, services are unable to adopt evidence-based practices until implementation drivers are tested and addressed. Furthermore, it is important that a clear business model is planned and in place, with consideration given to the potential market and how the implementation of the product will take place and any anticipated revenue generation [85].
Involvement of Vulnerable Groups
As in other areas of mental health research, young people from marginalized and underserved groups (eg, from low-income backgrounds, refugees, or asylum seekers; those not in education, employment, or training; members of ethnic and sexual minorities; and those under state care) were underrepresented in these studies, which typically focused on university students. Few attempts have been made in the literature to create new interventions or to adapt existing ones to meet the complex and heterogeneous needs of these young people [90]. Research exploring the acceptability, appropriateness, and feasibility of mental health app–based interventions for this group is lacking [89]. Work to assess the acceptability and feasibility of mental health apps for underserved young people is needed to ensure that they are not further excluded from research and to advance toward mental health provision that meets their support needs.
Conclusions
Despite the significant amount of funding that has been directed toward the development of mobile mental health interventions, few have published evidence-based data to support their use in real-world settings, and even fewer have been successfully transitioned into sustainable mental health interventions. Although it had been thought that smartphone apps held the potential to address many of the current issues facing service provision in youth mental health by improving the scalability and affordability of evidence-based mental health interventions for young people and addressing health disparities by providing wider access to underserved populations, more work is needed to improve key implementation drivers, such as uptake and adoption. Innovative and targeted funding mechanisms that are quick, responsive, and encouraging of broad stakeholder and industry partnerships, where data are openly shared, are essential to ensure mental health and well-being app development, evaluation, implementation, and sustainability proceeds in a direction that will enable evidence-based interventions to be made available quickly to young people who may benefit from them.
Acknowledgments
This project received funding from the European Union’s Horizon 2020 research and innovation program (grant 754657).
The authors are grateful to those authors who took the time to complete the survey in this review, including, but not limited to, Professor Michael E Levin, Jennifer Krafft, Professor Guy Doron, Dinur Aboody, Dr Bridianne O’Dea, Dr Erlendur Egilsson, Dr Emma Broglia, Dr Tayla McCloud, Dr Silvia Cerea, Professor Maria Roncero, Dr Martina Di Simplicio, Professor Sandra Bucci, Dr Sung-Won Choi, Dr Ji-Won Hur, Dr Somaieh Borjalilu, Professor Michelle G Newman, Dr Kristin Thomas, Dr Baland Jalal, Dr David Plans, Professor Danielle Schlosser, Dr Mary Elizabeth Jung, and Dr Lynnette Nathalie Lyzwinski. The authors would also like to thank Verity Westgate and Professor Andrea Cipriani for their helpful and insightful feedback on an earlier version of this manuscript.
Abbreviations
- PRIME
Personalized Real-time Intervention for Motivational Enhancement
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT
randomized controlled trial
- YPAG
Young People’s Advisory Groups
Systematic search strategy.
Author survey questions.
Study characteristics.
Intervention characteristics.
Implementation and sustainability.
Implementation variables.
Mixed methods appraisal tool.
Data Availability
The data extracted to support the findings of this review can be obtained from the corresponding author on reasonable request.
Footnotes
Conflicts of Interest: SL is a consultant at Paradym Ltd, an organization that developed Paradym, an app for supporting well-being (not included in the current review).
References
- 1.Torous J, Roberts LW. Needed innovation in digital health and smartphone applications for mental health: transparency and trust. JAMA Psychiatry. 2017 May 01;74(5):437–8. doi: 10.1001/jamapsychiatry.2017.0262.2616170 [DOI] [PubMed] [Google Scholar]
- 2.Schueller SM, Neary M, O'Loughlin K, Adkins EC. Discovery of and interest in health apps among those with mental health needs: survey and focus group study. J Med Internet Res. 2018 Jun 11;20(6):e10141. doi: 10.2196/10141. https://www.jmir.org/2018/6/e10141/ v20i6e10141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Muñoz RF. The efficiency model of support and the creation of digital apothecaries. Clin Psychol Sci Pract. 2017 Mar;24(1):46–9. doi: 10.1111/cpsp.12174. [DOI] [Google Scholar]
- 4.Clayborne ZM, Varin M, Colman I. Systematic review and meta-analysis: adolescent depression and long-term psychosocial outcomes. J Am Acad Child Adolesc Psychiatry. 2019 Jan;58(1):72–9. doi: 10.1016/j.jaac.2018.07.896.S0890-8567(18)31906-3 [DOI] [PubMed] [Google Scholar]
- 5.Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustün TB. Age of onset of mental disorders: a review of recent literature. Curr Opin Psychiatry. 2007 Jul;20(4):359–64. doi: 10.1097/YCO.0b013e32816ebc8c. https://europepmc.org/abstract/MED/17551351 .00001504-200707000-00010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aschbrenner KA, Naslund JA, Tomlinson EF, Kinney A, Pratt SI, Brunette MF. Adolescents' use of digital technologies and preferences for mobile health coaching in public mental health settings. Front Public Health. 2019 Jul 2;7:178. doi: 10.3389/fpubh.2019.00178. doi: 10.3389/fpubh.2019.00178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Leech T, Dorstyn D, Taylor A, Li W. Mental health apps for adolescents and young adults: a systematic review of randomised controlled trials. Child Youth Serv Rev. 2021 Aug;127:106073. doi: 10.1016/j.childyouth.2021.106073. [DOI] [Google Scholar]
- 8.Buttazzoni A, Brar K, Minaker L. Smartphone-based interventions and internalizing disorders in youth: systematic review and meta-analysis. J Med Internet Res. 2021 Jan 11;23(1):e16490. doi: 10.2196/16490. https://www.jmir.org/2021/1/e16490/ v23i1e16490 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Eisenstadt M, Liverpool S, Infanti E, Ciuvat RM, Carlsson C. Mobile apps that promote emotion regulation, positive mental health, and well-being in the general population: systematic review and meta-analysis. JMIR Ment Health. 2021 Nov 08;8(11):e31170. doi: 10.2196/31170. https://mental.jmir.org/2021/11/e31170/ v8i11e31170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lipschitz J, Hogan TP, Bauer MS, Mohr DC. Closing the research-to-practice gap in digital psychiatry: the need to integrate implementation science. J Clin Psychiatry. 2019 May 14;80(3):18com12659. doi: 10.4088/JCP.18com12659. http://www.psychiatrist.com/JCP/article/Pages/2019/v80/18com12659.aspx . [DOI] [PubMed] [Google Scholar]
- 11.Hollis C. Youth mental health: risks and opportunities in the digital world. World Psychiatry. 2022 Feb;21(1):81–2. doi: 10.1002/wps.20929. doi: 10.1002/wps.20929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Morris ZS, Wooding S, Grant J. The answer is 17 years, what is the question: understanding time lags in translational research. J R Soc Med. 2011 Dec;104(12):510–20. doi: 10.1258/jrsm.2011.110180. https://journals.sagepub.com/doi/abs/10.1258/jrsm.2011.110180?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .104/12/510 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Torous J, Haim A. Dichotomies in the development and implementation of digital mental health tools. Psychiatr Serv. 2018 Dec 01;69(12):1204–6. doi: 10.1176/appi.ps.201800193. https://europepmc.org/abstract/MED/30256182 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kenny R, Dooley B, Fitzgerald A. Developing mental health mobile apps: exploring adolescents' perspectives. Health Informatics J. 2016 Jun;22(2):265–75. doi: 10.1177/1460458214555041. https://journals.sagepub.com/doi/10.1177/1460458214555041?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .1460458214555041 [DOI] [PubMed] [Google Scholar]
- 15.Ng MM, Firth J, Minen M, Torous J. User engagement in mental health apps: a review of measurement, reporting, and validity. Psychiatr Serv. 2019 Jul 01;70(7):538–44. doi: 10.1176/appi.ps.201800519. https://europepmc.org/abstract/MED/30914003 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Temkin AB, Schild J, Falk A, Bennett SM. Mobile apps for youth anxiety disorders: a review of the evidence and forecast of future innovations. Prof Psychol Res Pract. 2020 Aug;51(4):400–13. doi: 10.1037/pro0000342. [DOI] [Google Scholar]
- 17.Szinay D, Jones A, Chadborn T, Brown J, Naughton F. Influences on the uptake of and engagement with health and well-being smartphone apps: systematic review. J Med Internet Res. 2020 May 29;22(5):e17572. doi: 10.2196/17572. https://www.jmir.org/2020/5/e17572/ v22i5e17572 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015 Apr 21;10:53. doi: 10.1186/s13012-015-0242-0. https://implementationscience.biomedcentral.com/articles/10.1186/s13012-015-0242-0 .10.1186/s13012-015-0242-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fleming T, Bavin L, Lucassen M, Stasiak K, Hopkins S, Merry S. Beyond the trial: systematic review of real-world uptake and engagement with digital self-help interventions for depression, low mood, or anxiety. J Med Internet Res. 2018 Jun 06;20(6):e199. doi: 10.2196/jmir.9275. https://www.jmir.org/2018/6/e199/ v20i6e199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Connolly SL, Hogan TP, Shimada SL, Miller CJ. Leveraging implementation science to understand factors influencing sustained use of mental health apps: a narrative review. J Technol Behav Sci. 2021;6(2):184–96. doi: 10.1007/s41347-020-00165-4. https://europepmc.org/abstract/MED/32923580 .165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hermes ED, Lyon AR, Schueller SM, Glass JE. Measuring the implementation of behavioral intervention technologies: recharacterization of established outcomes. J Med Internet Res. 2019 Jan 25;21(1):e11752. doi: 10.2196/11752. https://www.jmir.org/2019/1/e11752/ v21i1e11752 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wozney L, McGrath PJ, Gehring ND, Bennett K, Huguet A, Hartling L, Dyson MP, Soleimani A, Newton AS. eMental healthcare technologies for anxiety and depression in childhood and adolescence: systematic review of studies reporting implementation outcomes. JMIR Ment Health. 2018 Jun 26;5(2):e48. doi: 10.2196/mental.9655. https://mental.jmir.org/2018/2/e48/ v5i2e48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ellis LA, Augustsson H, Grødahl AI, Pomare C, Churruca K, Long JC, Ludlow K, Zurynski YA, Braithwaite J. Implementation of e-mental health for depression and anxiety: a critical scoping review. J Community Psychol. 2020 Apr;48(3):904–20. doi: 10.1002/jcop.22309. [DOI] [PubMed] [Google Scholar]
- 24.Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, Griffey R, Hensley M. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011 Mar;38(2):65–76. doi: 10.1007/s10488-010-0319-7. https://europepmc.org/abstract/MED/20957426 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Liverpool S, Mota CP, Sales CM, Čuš A, Carletto S, Hancheva C, Sousa S, Cerón SC, Moreno-Peral P, Pietrabissa G, Moltrecht B, Ulberg R, Ferreira N, Edbrooke-Childs J. Engaging children and young people in digital mental health interventions: systematic review of modes of delivery, facilitators, and barriers. J Med Internet Res. 2020 Jun 23;22(6):e16317. doi: 10.2196/16317. https://www.jmir.org/2020/6/e16317/ v22i6e16317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Moltrecht B, Patalay P, Bear HA, Deighton J, Edbrooke-Childs J. A transdiagnostic, emotion regulation app (Eda) for children: design, development, and lessons learned. JMIR Form Res. 2022 Jan 19;6(1):e28300. doi: 10.2196/28300. https://formative.jmir.org/2022/1/e28300/ v6i1e28300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kien C, Griebler U, Schultes M, Thaler KJ, Stamm T. Psychometric testing of the German versions of three implementation outcome measures. Glob Implement Res Appl. 2021 Aug 23;1(3):183–94. doi: 10.1007/s43477-021-00019-y. [DOI] [Google Scholar]
- 28.Marcano Belisario JS, Huckvale K, Greenfield G, Car J, Gunn LH. Smartphone and tablet self management apps for asthma. Cochrane Database Syst Rev. 2013 Nov 27;2013(11):CD010013. doi: 10.1002/14651858.CD010013.pub2. https://europepmc.org/abstract/MED/24282112 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Marcano Belisario JS, Jamsek J, Huckvale K, O'Donoghue J, Morrison CP, Car J. Comparison of self-administered survey questionnaire responses collected using mobile apps versus other methods. Cochrane Database Syst Rev. 2015 Jul 27;2015(7):MR000042. doi: 10.1002/14651858.MR000042.pub2. https://europepmc.org/abstract/MED/26212714 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Falconer J. Removing duplicates from an EndNote library. Library, Archives & Open Research Services Blog. 2018. Dec 7, [2021-02-02]. http://blogs.lshtm.ac.uk/library/2018/12/07/removing-duplicates-from-an-endnote-library/
- 31.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a Web and mobile app for systematic reviews. Syst Rev. 2016 Dec 05;5(1):210. doi: 10.1186/s13643-016-0384-4. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-016-0384-4 .10.1186/s13643-016-0384-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. doi: 10.1136/bmj.n71. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=33782057 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, Gagnon MP, Griffiths F, Nicolau B, O’Cathain A, Rousseau MC, Vedel I, Pluye P. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018 Dec 18;34(4):285–91. doi: 10.3233/efi-180221. [DOI] [Google Scholar]
- 34.Crabtree BE, Miller WF. A template approach to text analysis: developing and using codebooks. In: Crabtree BF, Miller WL, editors. Doing Qualitative Research. Thousand Oaks, CA, USA: Sage Publications; 1999. pp. 163–77. [Google Scholar]
- 35.Aboody D, Siev J, Doron G. Building resilience to body image triggers using brief cognitive training on a mobile application: a randomized controlled trial. Behav Res Ther. 2020 Nov;134:103723. doi: 10.1016/j.brat.2020.103723.S0005-7967(20)30177-7 [DOI] [PubMed] [Google Scholar]
- 36.Bendtsen M, Müssener U, Linderoth C, Thomas K. A mobile health intervention for mental health promotion among university students: randomized controlled trial. JMIR Mhealth Uhealth. 2020 Mar 20;8(3):e17208. doi: 10.2196/17208. https://mhealth.jmir.org/2020/3/e17208/ v8i3e17208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Borjalilu S, Mazaheri MA, Talebpour A. Effectiveness of mindfulness-based stress management in the mental health of Iranian university students: a comparison of blended therapy, face-to-face sessions, and mHealth app (Aramgar) Iran J Psychiatry Behav Sci. 2019 May 12;13(2):e84726. doi: 10.5812/ijpbs.84726. [DOI] [Google Scholar]
- 38.Broglia E, Millings A, Barkham M. Counseling with guided use of a mobile well-being app for students experiencing anxiety or depression: clinical outcomes of a feasibility trial embedded in a student counseling service. JMIR Mhealth Uhealth. 2019 Aug 15;7(8):e14318. doi: 10.2196/14318. https://mhealth.jmir.org/2019/8/e14318/ v7i8e14318 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bucci S, Barrowclough C, Ainsworth J, Machin M, Morris R, Berry K, Emsley R, Lewis S, Edge D, Buchan I, Haddock G. Actissist: proof-of-concept trial of a theory-driven digital intervention for psychosis. Schizophr Bull. 2018 Aug 20;44(5):1070–80. doi: 10.1093/schbul/sby032. https://europepmc.org/abstract/MED/29566206 .4939353 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cerea S, Ghisi M, Bottesi G, Carraro E, Broggio D, Doron G. Reaching reliable change using short, daily, cognitive training exercises delivered on a mobile application: the case of Relationship Obsessive Compulsive Disorder (ROCD) symptoms and cognitions in a subclinical cohort. J Affect Disord. 2020 Nov 01;276:775–87. doi: 10.1016/j.jad.2020.07.043.S0165-0327(20)32488-5 [DOI] [PubMed] [Google Scholar]
- 41.Cerea S, Ghisi M, Bottesi G, Manoli T, Carraro E, Doron G. Cognitive behavioral training using a mobile application reduces body image-related symptoms in high-risk female university students: a randomized controlled study. Behav Ther. 2021 Jan;52(1):170–82. doi: 10.1016/j.beth.2020.04.002.S0005-7894(20)30052-6 [DOI] [PubMed] [Google Scholar]
- 42.Di Simplicio M, Appiah-Kusi E, Wilkinson P, Watson P, Meiser-Stedman C, Kavanagh DJ, Holmes EA. Imaginator: a proof-of-concept feasibility trial of a brief imagery-based psychological intervention for young people who self-harm. Suicide Life Threat Behav. 2020 Jun;50(3):724–40. doi: 10.1111/sltb.12620. https://europepmc.org/abstract/MED/32057131 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Egilsson E, Bjarnason R, Njardvik U. Usage and weekly attrition in a smartphone-based health behavior intervention for adolescents: pilot randomized controlled trial. JMIR Form Res. 2021 Feb 17;5(2):e21432. doi: 10.2196/21432. https://formative.jmir.org/2021/2/e21432/ v5i2e21432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Fish MT, Saul AD. The gamification of meditation: a randomized-controlled study of a prescribed mobile mindfulness meditation application in reducing college students’ depression. Simul Gaming. 2019 Jun 04;50(4):419–35. doi: 10.1177/1046878119851821. [DOI] [Google Scholar]
- 45.Fitzpatrick KK, Darcy A, Vierhile M. Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (Woebot): a randomized controlled trial. JMIR Ment Health. 2017 Jun 06;4(2):e19. doi: 10.2196/mental.7785. https://mental.jmir.org/2017/2/e19/ v4i2e19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Flett JA, Conner TS, Riordan BC, Patterson T, Hayne H. App-based mindfulness meditation for psychological distress and adjustment to college in incoming university students: a pragmatic, randomised, waitlist-controlled trial. Psychol Health. 2020 Sep;35(9):1049–74. doi: 10.1080/08870446.2019.1711089. [DOI] [PubMed] [Google Scholar]
- 47.Flett JA, Hayne H, Riordan BC, Thompson LM, Conner TS. Mobile mindfulness meditation: a randomised controlled trial of the effect of two popular apps on mental health. Mindfulness (N Y) 2019;10(5):863–76. doi: 10.1007/s12671-018-1050-9. [DOI] [Google Scholar]
- 48.Franklin JC, Fox KR, Franklin CR, Kleiman EM, Ribeiro JD, Jaroszewski AC, Hooley JM, Nock MK. A brief mobile app reduces nonsuicidal and suicidal self-injury: evidence from three randomized controlled trials. J Consult Clin Psychol. 2016 Jun;84(6):544–57. doi: 10.1037/ccp0000093.2016-15311-001 [DOI] [PubMed] [Google Scholar]
- 49.Huberty J, Green J, Glissmann C, Larkey L, Puzia M, Lee C. Efficacy of the mindfulness meditation mobile app "Calm" to reduce stress among college students: randomized controlled trial. JMIR Mhealth Uhealth. 2019 Jun 25;7(6):e14273. doi: 10.2196/14273. https://mhealth.jmir.org/2019/6/e14273/ v7i6e14273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Hur JW, Kim B, Park D, Choi SW. A scenario-based cognitive behavioral therapy mobile app to reduce dysfunctional beliefs in individuals with depression: a randomized controlled trial. Telemed J E Health. 2018 Sep;24(9):710–6. doi: 10.1089/tmj.2017.0214. [DOI] [PubMed] [Google Scholar]
- 51.Jalal B, Brühl A, O'Callaghan C, Piercy T, Cardinal RN, Ramachandran VS, Sahakian BJ. Novel smartphone interventions improve cognitive flexibility and obsessive-compulsive disorder symptoms in individuals with contamination fears. Sci Rep. 2018 Oct 23;8(1):14923. doi: 10.1038/s41598-018-33142-2. doi: 10.1038/s41598-018-33142-2.10.1038/s41598-018-33142-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kageyama K, Kato Y, Mesaki T, Uchida H, Takahashi K, Marume R, Sejima Y, Hirao K. Effects of video viewing smartphone application intervention involving positive word stimulation in people with subthreshold depression: a pilot randomized controlled trial. J Affect Disord. 2021 Mar 01;282:74–81. doi: 10.1016/j.jad.2020.12.104.S0165-0327(20)33194-3 [DOI] [PubMed] [Google Scholar]
- 53.Kajitani K, Higashijima I, Kaneko K, Matsushita T, Fukumori H, Kim D. Short-term effect of a smartphone application on the mental health of university students: a pilot study using a user-centered design self-monitoring application for mental health. PLoS One. 2020 Sep 25;15(9):e0239592. doi: 10.1371/journal.pone.0239592. https://dx.plos.org/10.1371/journal.pone.0239592 .PONE-D-20-11603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lee RA, Jung ME. Evaluation of an mHealth app (DeStressify) on university students' mental health: pilot trial. JMIR Ment Health. 2018 Jan 23;5(1):e2. doi: 10.2196/mental.8324. https://mental.jmir.org/2018/1/e2/ v5i1e2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Levin ME, Krafft J, Seifert S, Lillis J. Tracking valued and avoidant functions with health behaviors: a randomized controlled trial of the acceptance and commitment therapy matrix mobile app. Behav Modif. 2022 Jan;46(1):63–89. doi: 10.1177/0145445520913987. [DOI] [PubMed] [Google Scholar]
- 56.Levin ME, Hicks ET, Krafft J. Pilot evaluation of the stop, breathe and think mindfulness app for student clients on a college counseling center waitlist. J Am Coll Health. 2022 Jan;70(1):165–73. doi: 10.1080/07448481.2020.1728281. [DOI] [PubMed] [Google Scholar]
- 57.Levin ME, Haeger J, An W, Twohig MP. Comparing cognitive defusion and cognitive restructuring delivered through a mobile app for individuals high in self-criticism. Cogn Ther Res. 2018 Jul 13;42(6):844–55. doi: 10.1007/s10608-018-9944-3. [DOI] [Google Scholar]
- 58.Lyzwinski LN, Caffery L, Bambling M, Edirippulige S. The mindfulness app trial for weight, weight-related behaviors, and stress in university students: randomized controlled trial. JMIR Mhealth Uhealth. 2019 Apr 10;7(4):e12210. doi: 10.2196/12210. https://mhealth.jmir.org/2019/4/e12210/ v7i4e12210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.McCloud T, Jones R, Lewis G, Bell V, Tsakanikos E. Effectiveness of a mobile app intervention for anxiety and depression symptoms in university students: randomized controlled trial. JMIR Mhealth Uhealth. 2020 Jul 31;8(7):e15418. doi: 10.2196/15418. https://mhealth.jmir.org/2020/7/e15418/ v8i7e15418 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Newman MG, Jacobson NC, Rackoff GN, Bell MJ, Taylor CB. A randomized controlled trial of a smartphone-based application for the treatment of anxiety. Psychother Res. 2021 Apr;31(4):443–54. doi: 10.1080/10503307.2020.1790688. https://europepmc.org/abstract/MED/32662323 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.O'Dea B, Han J, Batterham PJ, Achilles MR, Calear AL, Werner-Seidler A, Parker B, Shand F, Christensen H. A randomised controlled trial of a relationship-focussed mobile phone application for improving adolescents' mental health. J Child Psychol Psychiatry. 2020 Aug;61(8):899–913. doi: 10.1111/jcpp.13294. https://europepmc.org/abstract/MED/32683737 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Orosa-Duarte Á, Mediavilla R, Muñoz-Sanjose A, Palao Á, Garde J, López-Herrero V, Bravo-Ortiz M, Bayón C, Rodríguez-Vega B. Mindfulness-based mobile app reduces anxiety and increases self-compassion in healthcare students: a randomised controlled trial. Med Teach. 2021 Jun;43(6):686–93. doi: 10.1080/0142159X.2021.1887835. [DOI] [PubMed] [Google Scholar]
- 63.Ponzo S, Morelli D, Kawadler JM, Hemmings NR, Bird G, Plans D. Efficacy of the digital therapeutic mobile app BioBase to reduce stress and improve mental well-being among university students: randomized controlled trial. JMIR Mhealth Uhealth. 2020 Apr 06;8(4):e17767. doi: 10.2196/17767. https://mhealth.jmir.org/2020/4/e17767/ v8i4e17767 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Reid SC, Kauer SD, Hearps SJ, Crooke AH, Khor AS, Sanci LA, Patton GC. A mobile phone application for the assessment and management of youth mental health problems in primary care: a randomised controlled trial. BMC Fam Pract. 2011 Nov 29;12:131. doi: 10.1186/1471-2296-12-131. https://bmcfampract.biomedcentral.com/articles/10.1186/1471-2296-12-131 .1471-2296-12-131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Rodgers RF, Donovan E, Cousineau T, Yates K, McGowan K, Cook E, Lowy AS, Franko DL. BodiMojo: efficacy of a mobile-based intervention in improving body image and self-compassion among adolescents. J Youth Adolesc. 2018 Jul;47(7):1363–72. doi: 10.1007/s10964-017-0804-3.10.1007/s10964-017-0804-3 [DOI] [PubMed] [Google Scholar]
- 66.Roncero M, Belloch A, Doron G. Can brief, daily training using a mobile app help change maladaptive beliefs? Crossover randomized controlled trial. JMIR Mhealth Uhealth. 2019 Feb 13;7(2):e11443. doi: 10.2196/11443. https://mhealth.jmir.org/2019/2/e11443/ v7i2e11443 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Schlosser DA, Campellone TR, Truong B, Etter K, Vergani S, Komaiko K, Vinogradov S. Efficacy of PRIME, a mobile app intervention designed to improve motivation in young people with schizophrenia. Schizophr Bull. 2018 Aug 20;44(5):1010–20. doi: 10.1093/schbul/sby078. https://europepmc.org/abstract/MED/29939367 .5042996 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Yang E, Schamber E, Meyer RM, Gold JI. Happier healers: randomized controlled trial of mobile mindfulness for stress management. J Altern Complement Med. 2018 May;24(5):505–13. doi: 10.1089/acm.2015.0301. [DOI] [PubMed] [Google Scholar]
- 69.O'Dea B, Achilles MR, Werner-Seidler A, Batterham PJ, Calear AL, Perry Y, Shand F, Christensen H. Adolescents' perspectives on a mobile app for relationships: cross-sectional survey. JMIR Mhealth Uhealth. 2018 Mar 08;6(3):e56. doi: 10.2196/mhealth.8831. https://mhealth.jmir.org/2018/3/e56/ v6i3e56 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Schlosser D, Campellone T, Kim D, Truong B, Vergani S, Ward C, Vinogradov S. Feasibility of PRIME: a cognitive neuroscience-informed mobile app intervention to enhance motivated behavior and improve quality of life in recent onset schizophrenia. JMIR Res Protoc. 2016 Apr 28;5(2):e77. doi: 10.2196/resprot.5450. https://www.researchprotocols.org/2016/2/e77/ v5i2e77 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Bangor A, Kortum PT, Miller JT. An empirical evaluation of the system usability scale. Int J Hum Comput Interact. 2008 Jul 30;24(6):574–94. doi: 10.1080/10447310802205776. [DOI] [Google Scholar]
- 72.Baumel A, Muench F, Edan S, Kane JM. Objective user engagement with mental health apps: systematic search and panel-based usage analysis. J Med Internet Res. 2019 Sep 25;21(9):e14567. doi: 10.2196/14567. https://www.jmir.org/2019/9/e14567/ v21i9e14567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Kaveladze BT, Wasil AR, Bunyi JB, Ramirez V, Schueller SM. User experience, engagement, and popularity in mental health apps: secondary analysis of app analytics and expert app reviews. JMIR Hum Factors. 2022 Jan 31;9(1):e30766. doi: 10.2196/30766. https://humanfactors.jmir.org/2022/1/e30766/ v9i1e30766 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Lattie EG, Schueller SM, Sargent E, Stiles-Shields C, Tomasino KN, Corden ME, Begale M, Karr CJ, Mohr DC. Uptake and usage of IntelliCare: a publicly available suite of mental health and well-being apps. Internet Interv. 2016 May;4(2):152–8. doi: 10.1016/j.invent.2016.06.003. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(15)30029-4 .S2214-7829(15)30029-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Levin ME, Haeger J, Cruz RA. Tailoring acceptance and commitment therapy skill coaching in the moment through smartphones: results from a randomized controlled trial. Mindfulness (N Y) 2018 Jul 21;10(4):689–99. doi: 10.1007/s12671-018-1004-2. [DOI] [Google Scholar]
- 76.Wasil AR, Palermo EH, Lorenzo-Luaces L, DeRubeis RJ. Is there an app for that? A review of popular apps for depression, anxiety, and well-being. Cogn Behav Pract. 2022 Nov;29(4):883–901. doi: 10.1016/j.cbpra.2021.07.001.S0005-7967(19)30184-6 [DOI] [Google Scholar]
- 77.Lau N, O'Daffer A, Colt S, Yi-Frazier JP, Palermo TM, McCauley E, Rosenberg AR. Android and iPhone mobile apps for psychosocial wellness and stress management: systematic search in app stores and literature review. JMIR Mhealth Uhealth. 2020 May 22;8(5):e17798. doi: 10.2196/17798. https://mhealth.jmir.org/2020/5/e17798/ v8i5e17798 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Robards F, Kang M, Usherwood T, Sanci L. How marginalized young people access, engage with, and navigate health-care systems in the digital age: systematic review. J Adolesc Health. 2018 Apr;62(4):365–81. doi: 10.1016/j.jadohealth.2017.10.018.S1054-139X(17)30861-3 [DOI] [PubMed] [Google Scholar]
- 79.Linardon Jake, Cuijpers Pim, Carlbring Per, Messer Mariel, Fuller-Tyszkiewicz Matthew. The efficacy of app-supported smartphone interventions for mental health problems: a meta-analysis of randomized controlled trials. World Psychiatry. 2019 Oct;18(3):325–336. doi: 10.1002/wps.20673. doi: 10.1002/wps.20673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Singh Swarndeep, Sagar Rajesh. Time to Have Effective Regulation of the Mental Health Apps Market: Maximize Gains and Minimize Harms. Indian J Psychol Med. 2022 Jul;44(4):399–404. doi: 10.1177/02537176221082902. https://journals.sagepub.com/doi/abs/10.1177/02537176221082902?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .10.1177_02537176221082902 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Wolf R, Morrison J, Inns A, Slavin R, Risman K. Average Effect Sizes in Developer-Commissioned and Independent Evaluations. Journal of Research on Educational Effectiveness. 2020 Apr 06;13(2):428–447. doi: 10.1080/19345747.2020.1726537. [DOI] [Google Scholar]
- 82.Hill C, Creswell C, Vigerland S, Nauta MH, March S, Donovan C, Wolters L, Spence SH, Martin JL, Wozney L, McLellan L, Kreuze L, Gould K, Jolstedt M, Nord M, Hudson JL, Utens E, Ruwaard J, Albers C, Khanna M, Albano AM, Serlachius E, Hrastinski S, Kendall PC. Navigating the development and dissemination of internet cognitive behavioral therapy (iCBT) for anxiety disorders in children and young people: a consensus statement with recommendations from the #iCBTLorentz Workshop Group. Internet Interv. 2018 Jun;12:1–10. doi: 10.1016/j.invent.2018.02.002. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(17)30129-X .S2214-7829(17)30129-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Sellars E, Pavarini G, Michelson D, Creswell C, Fazel M. Young people's advisory groups in health research: scoping review and mapping of practices. Arch Dis Child. 2021 Jul;106(7):698–704. doi: 10.1136/archdischild-2020-320452.archdischild-2020-320452 [DOI] [PubMed] [Google Scholar]
- 84.Bevan Jones R, Stallard P, Agha SS, Rice S, Werner-Seidler A, Stasiak K, Kahn J, Simpson SA, Alvarez-Jimenez M, Rice F, Evans R, Merry S. Practitioner review: co-design of digital mental health technologies with children and young people. J Child Psychol Psychiatry. 2020 Aug;61(8):928–40. doi: 10.1111/jcpp.13258. https://europepmc.org/abstract/MED/32572961 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Hill C, Martin JL, Thomson S, Scott-Ram N, Penfold H, Creswell C. Navigating the challenges of digital health innovation: considerations and solutions in developing online and smartphone-application-based interventions for mental health disorders. Br J Psychiatry. 2017 Aug;211(2):65–9. doi: 10.1192/bjp.bp.115.180372.S0007125000281828 [DOI] [PubMed] [Google Scholar]
- 86.Premachandra B, Lewis Jr NA. Do we report the information that is necessary to give psychology away? A scoping review of the psychological intervention literature 2000-2018. Perspect Psychol Sci. 2022 Jan;17(1):226–38. doi: 10.1177/1745691620974774. [DOI] [PubMed] [Google Scholar]
- 87.Valentine L, McEnery C, Bell I, O'Sullivan S, Pryor I, Gleeson J, Bendall S, Alvarez-Jimenez M. Blended digital and face-to-face care for first-episode psychosis treatment in young people: qualitative study. JMIR Ment Health. 2020 Jul 28;7(7):e18990. doi: 10.2196/18990. https://mental.jmir.org/2020/7/e18990/ v7i7e18990 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Sanderson C, Kouzoupi N, Hall CL. Technology Matters: the human touch in a digital age - a blended approach in mental healthcare delivery with children and young people. Child Adolesc Ment Health. 2020 May;25(2):120–2. doi: 10.1111/camh.12385. [DOI] [PubMed] [Google Scholar]
- 89.Ramos G, Ponting C, Labao JP, Sobowale K. Considerations of diversity, equity, and inclusion in mental health apps: a scoping review of evaluation frameworks. Behav Res Ther. 2021 Dec;147:103990. doi: 10.1016/j.brat.2021.103990. https://linkinghub.elsevier.com/retrieve/pii/S0005-7967(21)00189-3 .S0005-7967(21)00189-3 [DOI] [PubMed] [Google Scholar]
- 90.Schueller SM, Hunter JF, Figueroa C, Aguilera A. Use of digital mental health for marginalized and underserved populations. Curr Treat Options Psych. 2019 Jul 5;6(3):243–55. doi: 10.1007/s40501-019-00181-z. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Systematic search strategy.
Author survey questions.
Study characteristics.
Intervention characteristics.
Implementation and sustainability.
Implementation variables.
Mixed methods appraisal tool.
Data Availability Statement
The data extracted to support the findings of this review can be obtained from the corresponding author on reasonable request.