

Abstract
Background:
Advance care planning (ACP) and involving family are particularly important in dementia, and primary care is a key setting. The purpose of this trial is to examine the impact and implementation of SHARING Choices, an intervention to improve communication for older adults with and without dementia through proactively supporting ACP and family engagement in primary care.
Methods:
We cluster-randomized 55 diverse primary care practices across two health systems to the intervention or usual care. SHARING Choices is a multicomponent intervention that aims to improve communication through patient and family engagement in ACP, agenda setting, and shared access to the patient portal for all patients over 65 years of age. The primary outcomes include documentation of an advance directive or medical orders for life-sustaining treatment in the electronic health record (EHR) at 12 months for all patients and receipt of potentially burdensome care within 6 months of death for the subgroup of patients with serious illness. We plan a priori sub-analysis for patients with dementia. Data sources include the health system EHRs and the Maryland health information exchange. We use a mixed-methods approach to evaluate uptake, fidelity and adaptation of the intervention and implementation facilitators and barriers.
Conclusions:
This cluster-randomized pragmatic trial examines ACP with a focus on the key population of those with dementia, implementation in diverse settings and innovative approaches to trial design and outcome abstraction. Mixed-methods approaches enable understanding of intervention delivery and facilitators and barriers to implementation in rapidly changing health care systems.
ClinicalTrials.gov Identifier: NCT04819191
Keywords: Advance care planning, Advance directives, Primary care, Dementia
1. Introduction
Alzheimer’s Disease and Related Dementias (ADRD) are among the most profoundly disabling and costly health conditions [1] and a leading cause of death in the United States. [2] ACP can be defined as a communication process to understand and share personal values, life goals, and preferences for future medical care and designate health care surrogates, that many experts and US organizations recommend throughout the course of serious illness. [3,4] Although persons with ADRD often meaningfully participate in ACP, [6,7] they are less likely than those without to participate in ACP and complete advance directives. [8,9] As a result, persons with ADRD are at greater risk for lack of concordance of preferences with end-of-life care. [10]
Family and close friends (family, as broadly defined by each person, referred to as “family” hereafter) are foundational in managing ADRD. Because family is particularly important in clinical decision-making for persons with ADRD, [11] engaging them in primary care and ACP is critical. [12–15] [16–20] Almost all community-living persons with ADRD rely on help from family [21,22] to coordinate information and care, and participate increasingly in shared decision-making as disease progresses. [21–23] Yet ambiguity about families’ roles and primary care clinician time and skill limitations amplify ACP challenges for persons with ADRD. [15,24]
Across populations, support and education can increase ACP [10,25] and systematic reviews of ACP show effectiveness for increasing advance directive documentation. [25,26] However, most interventional research has been limited to evaluation of participation and advance directive documentation rather than patient-centered outcomes such as end-of-life care. Moreover, key reviews found that ACP interventions alone improve advance directive documentation but have not shown effectiveness for person-centered outcomes; one potential reason is that these interventions do not address the wide scope of communication and systems issues needed to improve end-of-life care. [3,27–29] Prior studies of ACP in primary care have mostly targeted general populations [10,25,30] and generally excluded those with ADRD; most interventions in persons with ADRD have been in nursing homes. [31,32]
With this backdrop, we undertook the SHARING Choices study with the goal of improving communication for older adults with and without ADRD through proactively engaging family in interactions with primary care and supporting ACP and attention to ADRD in primary care. Our aims were [1] to test the effects of SHARING Choices in 3 patient groups: all older adults, those with ADRD, and those who die, and [2] to evaluate implementation and contextual factors, using mixed methods. Our hypothesis is based on evidence that older adults and families appreciate and expect primary care practices to initiate ACP [33] but that patient, family, and system factors often limit these conversations. [10] As a pragmatic trial, we addressed ACP for all older adults in intervention practices with particular attention for those with ADRD, given that cognitive impairment is common and often challenging to discern from medical records and that improving end-of-life communication and outcomes requires system-level changes. [34]
2. Methods
2.1. Conceptual framework and development of the intervention and trial
The design of SHARING Choices was informed by the fields of patient-provider communication, [17,35] family caregiving, [36,37] health services, [38,39] and health informatics, [40,41] acknowledging multiple ways that interpersonal relationships influence decision-making and end-of-life care. Our study design and evaluation are grounded in the Consolidated Framework for Implementation Research, a widely applied conceptual framework of contextual factors for adoption and spread of complex interventions in practice, as adapted for primary care, complex interventions and implementation outcomes. [42,43] The intervention is based on extensive research on feasibility and implementation of ACP and incorporation of ACP facilitators (staff trained in ACP that work with patients and families) and the other components of the intervention (Table 1). [44,45] The intervention also builds on health behavior change models of ACP that incorporate preparation to enhance uptake, [46,47] and is aligned with broader quality improvement approaches in our health systems and advanced primary care models. [48] Finally, the intervention and approach involved extensive stakeholder engagement, including patient and family interviews and patient advocate involvement, piloting with patients and families to refine the intervention, and model development within partner systems. [33,49–53] Groups of both local and national advisors also guide the trial.
Table 1.
SHARING choices components, content, rationale, evidence.
| Content | Rationale | Evidence |
|---|---|---|
| 1. Primary care engagement in voluntary advance care planning (ACP) | Most older adults and families appreciate when primary care practices engage them in ACP. Proactively introducing ACP through postal mailings normalizes these conversations. | Primary care initiatives to increase ACP are well-received. [52,66] |
| 2. ACP information and availability of facilitator- led ACP conversations | ACP education increases patient & family awareness, knowledge and skill. Respecting Choices™ is a structured educational program to train facilitators to facilitate ACP conversations. In SHARING Choices, ACP facilitators initiate outreach and/or respond to clinician referrals. | ACP and Respecting Choices™ are associated with increased advance directive documentation and patient satisfaction in primary care and for those with serious illness. [26,44,45] |
| 3. Person-Family Agenda Setting | Individuals & families often have different concerns. Agenda-setting stimulates conversations about ACP & the role of family. In SHARING Choices, agenda-setting tools are included in initial mailed outreach and can be supported by ACP facilitators. | Agenda-setting helps clarify concerns, goals, and expectations, and increase engagement in care. [67–69] |
| 4. Patient/Family Access to Electronic Health Record | The patient portal facilitates timely and accurate information about health care issues, including ACP. In many health systems, with patient permission, families can have their own identity credentials to access information and communicate with clinicians. In SHARING Choices, information about the patient portal is included in initial mailed outreach and can be supported by ACP facilitators. | The patient portal operates through mechanisms of convenience, continuity, activation, and understanding. [40] Prior studies find benefit of supporting family through technology such as portals. [70] |
| 5. Alzheimer’s Disease and Related Dementias (ADRD) Resources and Training of Staff and Clinicians | Patients and family appreciate when primary care practices provide ADRD information but practices often do not incorporate this into care. [71,72] [73] In SHARING Choices, ACP facilitators are provided additional training and support to engage in conversations in the context of ADRD. | Training curricula [74] and referral resources [75] support ADRD-friendly primary care practice. |
2.2. Intervention: components of SHARING Choices
The intervention comprises 5 components (rationale and evidence in Table 1):
outreach from the primary care practice introducing SHARING Choices to prepare patients and families to engage in ACP conversations (Fig. 1),
access to a facilitator trained in all elements of SHARING Choices, including Respecting CHOICES and leading ACP for persons with ADRD and their families,
person-family agenda-setting to align perspectives about the role of family and stimulate conversation about health care issues and ACP (Fig. 2),
information about registration for the patient portal to enable and extend electronic interactions and information access to patients and family, and.
ADRD educational materials and resources for staff and clinicians.
Fig. 1.
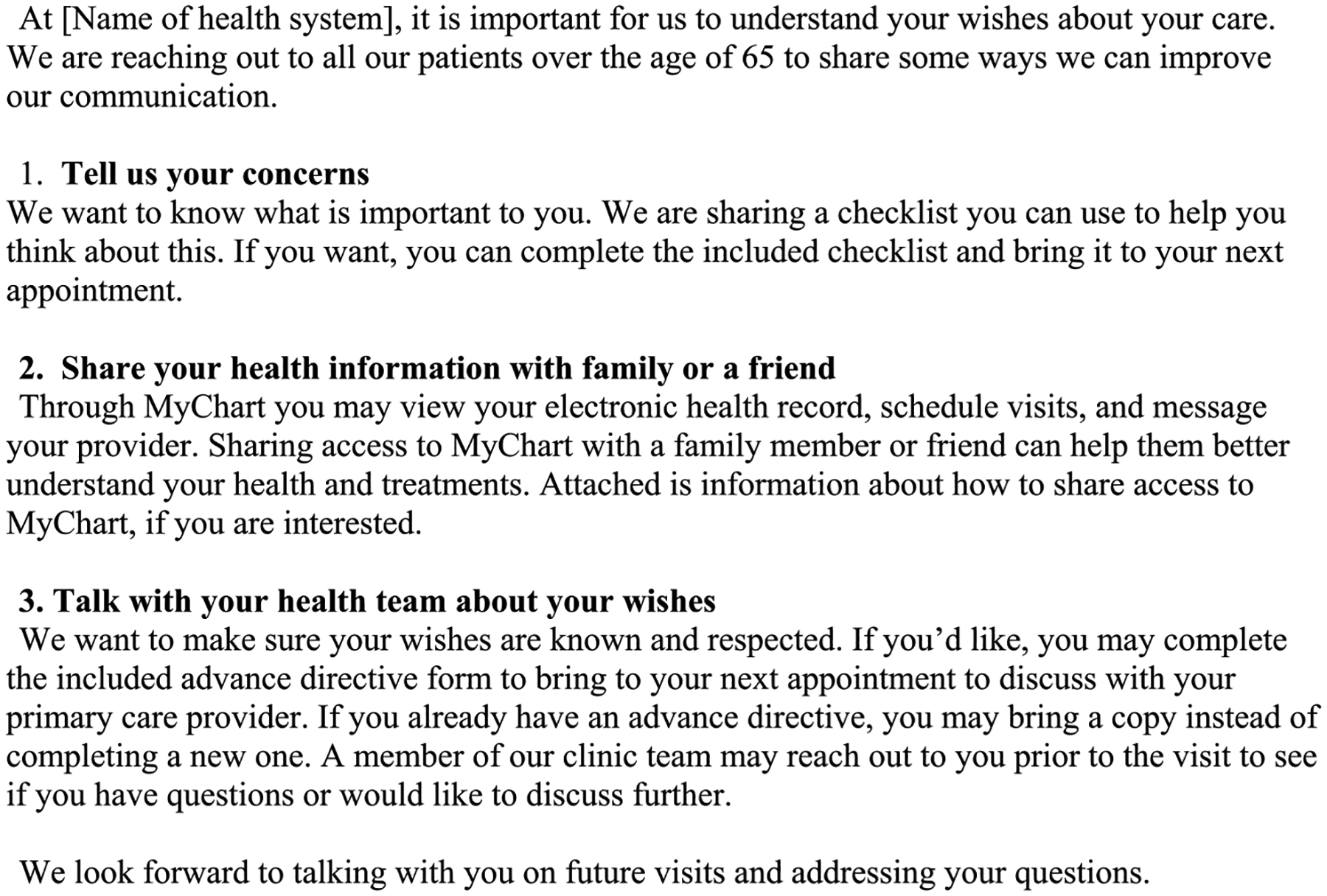
Content of outreach letter to patients [Johns Hopkins version).
Fig. 2.
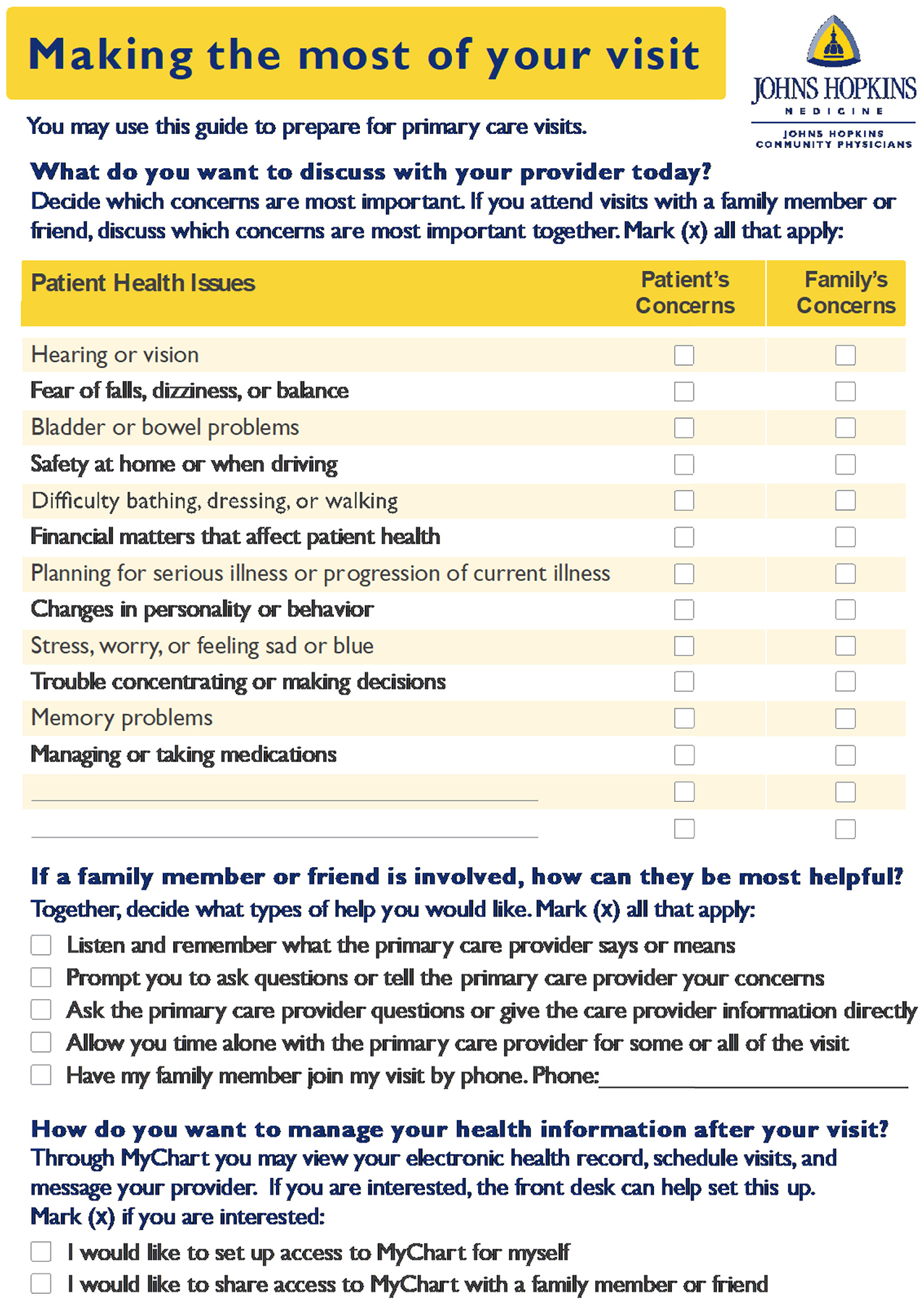
Agenda-setting checklist (Johns Hopkins version).
2.3. Study overview
We implement and evaluate the effectiveness of SHARING Choices on advance directive documentation and end-of-life outcomes by conducting a cluster-randomized pragmatic trial in 55 diverse primary care practices from the two partner health systems. We use a mixed-methods evaluation to examine not only “if” the intervention is effective but also “how” and “why” it had successes and limitations and to identify facilitators and barriers of implementation. We test the effects of SHARING Choices on ACP outcomes for all older patients, including persons with ADRD diagnoses in their electronic health record (EHR). Using information collected during routine care, we assess primary outcomes of advance directive documentation for all included patients and potentially burdensome care (defined as specific life-sustaining procedures that may not always be appropriate or consistent with patient preferences) within 6 months of death53 for the subgroup of patients with serious illness (defined as those with at-risk diagnoses or conditions that may limit prognosis, capacity or function or increase disease burden) who die [54,55] (Appendix). We evaluate participation by patients and families in each element of the intervention overall and for those with ADRD. After the trial, we also conduct key informant interviews to assess various stakeholder perspectives (patient, family, primary care teams, administrators) on SHARING Choices.
2.4. Setting
We are conducting the study in partnership with primary care health systems operated by MedStar Health System and Johns Hopkins Community Physicians (JHCP) which together operate >75 primary care practices in the Baltimore-Washington DC area. Baseline population characteristics are in Table 3. Both systems have established EHRs with consumer-facing patient/family portals and many practices participating in the advanced primary care models that encourage ACP and advance directive documentation as part of value-based care. MedStar Health operates a centralized palliative care program in which the new grant-funded ACP facilitators were embedded. [48] The new JHCP grant-funded ACP facilitators functioned in a mixed centralized and local primary care environment with staff from JHCP’s Department of Education, building on many years of incorporating ACP into care management programs and primary care. [49,50,56]
Table 3.
Baseline Characteristics by Health System and Practice.
| Johns Hopkins Community Physicians | MedStar Health | |
|---|---|---|
| Number of Clinics Randomized | 20 | 35 |
| Location | ||
| Urban | 4 (20%) | 10 (28.6%) |
| Rural | 6 (30%) | 5 (14.3%) |
| Suburban | 10 (50%) | 20 (57.1%) |
| Primary care clinicians, total (range by practice) | 143 (4, 18) | 342(5, 50) |
| Number of Patients | 204,607 | 175,558 |
| Number of Patients Age 65+ | 35,898 | 49,183 |
| Percent Female (range by practice) | 61% (55, 73) | 61% (47, 73) |
| Percent Age 65+ (range by practice) | 20% (5, 34) | 30% (02, 95) |
| Race and Ethnicitv | ||
| Percent Hispanic/Latino (range by practice) | 6% (2, 11) | 2% (0, 8) |
| Percent White (range by practice) | 60% (25,90) | 53% (4, 90) |
| Percent Black (range by practice) | 24% (4, 64) | 34% (4, 90) |
| Percent Other Race (range by practice) Paver Mix | 10% (3, 21) | 13% (3, 36) |
| Percent Commercial (range by practice) | 83% (57,91) | 51% (6, 85) |
| Percent Medicare (range by practice) | 14% (6, 29) | 32% (01, 92) |
| Percent Medicaid (range by practice) | 2% (0, 9) | 12% (1, 43) |
| Percent with Advance Directive in Electronic Health Record (EHR) | 4% (5, 10) | 19% (7, 44) |
| Percent with Dementia Diagnosis in EHR (range by practice) | 6% (2, 23) | 8% (2, 49) |
| Percent Registered for EHR portal (range by practice) | 65% (50, 82) | 31% (11, 60) |
2.5. Inclusion criteria
Eligible primary care practices have at least 2 clinicians whose panels collectively include >400 older adults. In this pragmatic trial, we target all new and established primary care patients ages 65 and over with a scheduled visit to the practice for an annual or follow-up in-person or telehealth appointment, including those with and without ADRD. There is no formal enrollment or consent as this is a practice-level initiative offered to all eligible patients at intervention practices.
3. ACP facilitation
Facilitators include lay facilitators, medical assistants, nurses or social workers embedded within partner health systems. Grant-funded intervention facilitators were trained in all elements of SHARING Choices, including The Respecting Choices™ First Steps™ curriculum for ACP, documenting advance directives, using the person-family agenda-setting checklist, and registering and accessing the patient portal (for both patients and family) (Table 1). The core of the required ACP training is Respecting Choices™ (https://respectingchoices.org), a structured educational curriculum to train non-physicians in ACP. [57] Prior studies have shown that Respecting Choices™ improves advance directive documentation, including in diverse communities. [44,45,57,58]
We reinforced facilitators’ ACP competency with traditional didactics, case scenarios, and modeling and mentored role play in one-hour biweekly mandatory meetings. Facilitators needed to successfully conduct at least one conversation before facilitating intervention conversations and received regular mentoring, monitoring and feedback, tailored to each health system. We also supplemented the Respecting Choices curriculum with targeted content on ADRD and ACP for persons with ADRD (Table 2). This supplemental training included communication techniques for a person-centered approach and supported decision making, recognition of limited patient understanding and need for communication with the primary care clinician on the need for further ACP conversation. We also trained facilitators on language and engagement of Black patients and their family.
Table 2.
Supplemental Alzheimer’s Disease and Related Dementias Training.
| Topic | Content | Methods |
|---|---|---|
| Living with Dementia: The Person | Patient experience in early-stage dementia | Video; discussion; reading |
| How to Talk so Alzheimer’s can Hear You | Patient experience in moderate- to late-stage dementia Recognizing and facilitating communication challenges between patient, family, and advance care planning facilitator |
Video; discussion |
| Family | Adult family experience with dementia from early to moderate stages of dementia | Video; discussion |
| Communication | Reflective listening Empathy Facilitating conversation with patient and family |
Videos; discussion; case examples; role play |
| Communication with Diverse Patients and Engagement with Black Patients | Use of language and avoidance of medical jargon Potential influence of religiousness/spirituality Cultural sensitivity |
Discussion; case examples |
| Repetitive Behaviors | Understanding family experience with repetitive questions, phone calls | Video; discussion |
| The Role of Medical Orders for Life-Sustaining Treatment (POLST) in the Care of People with Dementia | Symptoms and staging of dementia Overview of MOLST MOLST role in decision making |
Video; discussion |
4. Intervention embedding
We presented information on SHARING Choices to practice leaders before the study addressing intervention components, planning support and timeline, and resources and support for implementation and program monitoring. SHARING Choices champions were primary contacts for the investigators during implementation for intervention practices. At JHCP, the investigators worked with practice leadership to identify champions (practitioners, nurses and case managers); at Medstar Health, champions were practice management and medical director quality improvement leaders. Intervention components and workflows were tailored with practice champions over 2–3 meetings in the three months preceding the trial. Champions connected SHARING Choices staff with key practice staff to guide processes for interacting with patients and communicating about ACP with clinicians. We invited champions and leadership to bi-monthly meetings in the trial’s first six months to review progress and potential adaptations.
5. Intervention delivery characteristics and processes
SHARING Choices is designed for compatibility with primary care and balances core elements with adaptability to health system context and practice preferences. We modified the protocol for COVID-19 pandemic logistical issues (mainly focusing on remote facilitation). All patients 65 years of age and older under care of intervention practice clinicians with an upcoming new, physical, or follow-up visit within the next month are mailed SHARING Choices information. Working with practice stakeholders, grant-funded facilitators prioritize patients for outreach based on Annual Wellness Visit eligibility, lack of advance directive in the EHR, or an ADRD diagnosis. Approximately two weeks before the visit, facilitators contact pattients by phone or portal messaging about an ACP conversation. Intervention practice clinicians and case managers can also refer patients to facilitators.
ACP conversations occur by phone or telehealth or at the practice and are not necessarily linked to a visit. The facilitator follows the Respecting Choices™ structured conversation guide and employs motivational interviewing techniques to evaluate readiness and facilitate discussion of SHARING Choices components with patients (and family when available), focusing on communication techniques for those with ADRD. The facilitator records the duration (which varies per patient preferences) and content of ACP meetings and resulting decisions in the EHR. Advance directive documentation, if brought to a visit or sent in, is uploaded to the EHR.
6. Fidelity monitoring and adaptations
Guided by the NIH Behavior Change Consortium [59] we address fidelity through a.) design, by selecting distinct intervention elements based on theory, b.) training, by relying on a protocolized curriculum to train facilitators in ACP and other elements of SHARING Choices, c.) monitoring measures of implementation, and d.) ongoing training and resources to support facilitators and maximize fidelity to procedures within the pragmatic nature of the trial.
As a pragmatic trial, tracking of processes is monitored through data collected in routine interactions. The study team uses reporting systems to regularly monitor measures of implementation such as number of mailings and scheduled and completed ACP facilitator meetings. ACP facilitators document meeting content using structured EHR fields, including structure (presence of family, meeting duration) and ACP topics discussed. EHR Data monitored includes documented facilitator conversations, completed advance directives, and patient portal use. Additionally, the study team collects limited information from ACP facilitators related to safety monitoring and practice-level field observations during routine check-ins with managers and the study team for the implementation evaluation. Key stakeholders including administrators, champions, facilitators, patients (including those with ADRD) and families will participate in interviews after the trial to evaluate implementation processes and facilitators and barriers. We will conduct interviews using an interview guide based on our pilot work, literature review and stakeholder input. We will use a concurrent mixed-methods approach, with quantitative evaluation of measures of implementation (Table 4) and a reflexive thematic analysis approach for evaluation of interviews.
Table 4.
Schedule of data elements, purpose and sources.
| Purpose and Timing | |||
|---|---|---|---|
| Assessment (Data Source) | Practice Eligibility and Randomization (Day – 180) | Patient eligibility and Intervention: Day 0–456 | Outcomes at 12 Months (±30 Days) |
| Primary Care Practice Characteristics, including size and age and race distributions (Health Systems) | X | ||
| Patient Characteristics, including age, race and ADRD diagnosis (Health System EHR) | X | ||
| Measures of Implementation (ACP Facilitators contacts, ACP conversations, family presence, content, and AD completion or uploading) (Health System EHR and facilitator field notes) | X | ||
| Primary Outcome: Advance Directive or MO(L)ST Documentation in EHR (Health System EHR) | X | ||
| Primary Outcome: Potentially burdensome Care, last 6 months of life (Health System EHR/Health Information Exchange) | X | ||
| Adverse Events | X | ||
| Implementation Interviews | X | ||
ACP = Advance care planning, ADRD = Alzheimer’s Disease and Related Dementias, EHR = Electronic Health Record, MO(L)ST = Medical Orders for Life-Sustaining Treatment/Medical Orders for Scope of Treatment.
The Chair, ACP Facilitator Training and Oversight Workgroup (VC) regularly convenes ACP facilitators. Frequency and content of meetings varied based on study phase and facilitators’ specific needs. Before trial launch, the focus was educating facilitators about study objectives, workflows, and protocols and building ACP skills. After launch, we provided facilitators with study updates and asked them to present cases, troubleshoot challenges, engage in collaborative problem-solving, and discuss strategies for resolution. Ad-hoc support is available from investigators (VC, KS, KW) and the health systems. Through ongoing supervision, investigators probe for feedback regarding practice-level systems and workflows that work well or pose barriers, identifying needs for adaptations.
We evaluated facilitators’ skills mid-trial using observation of standardized patient encounters evaluating communication skills for ACP in those with ADRD. Each facilitator completed two case-based simulations, one with cognitive impairment and one with ADRD and a family member, followed by a debrief and structured assessment to evaluate adherence to the intervention, quality of delivery, and areas for improvement, which were incorporated into supplemental training.
7. Description of evaluations
7.1. Outcomes
We selected measures based on: 1.) known reliability and validity, 2.) sensitivity to change, 3.) clinical relevance, 4.) reflection of objective indicators of domains of interest, and 5.) feasibility of data extraction within the pragmatic trial mechanism. Our primary outcomes of advance directive documentation or MO(L)ST at 12 months and receipt of potentially burdensome care for those with serious illness within 6 months of death are extracted from JHCP and MedStar Health EHRs and the regional health information exchange (Table 4). We additionally assess measures of implementation, including facilitators’ patient contacts, ACP conversations, inclusion of family, and conversation content.
Advance directive or MO(L)ST documentation
Advance directive or MO(L)ST documentation is defined as a composite measure of EHR documentation of either [1] advance directive: a health care agent form (durable medical power of attorney/surrogate) or living will, or [2] MO(L)ST: Maryland Medical Order for Life-Sustaining Treatment (MOLST), or District of Columbia Medical Order for Sustaining Treatment (MOST). Documentation is based on audited data fields available through each health system’s EHR 12 months after study entry.
Although our primary outcome is operationalized as a composite measure, we exoamine advance directives and MO(L)ST in parallel for older adults ages 65 and older with and without a diagnosis of ADRD as defined by ICD-10-CM diagnosis codes (Appendix). By separately examining between-group differences in advance directive and MO(L)ST completion, we assess whether the study differentially affected these two outcomes for relevant subgroups.
Potentially burdensome care
Potentially burdensome care is measured as any (yes/no) life-sustaining procedures within the 6 months preceding death using dates and validated ICD-10-CM codes for hospital services (Appendix). Specific validated codes for potentially burdensome care include intubation and mechanical ventilation, tracheostomy, gastrostomy feeding tube placement, hemodialysis, enteral and parenteral nutrition, and cardiopulmonary resuscitation (Appendix). [60] The measure denominator comprises patients who died during the 12 months post-analytic sample with serious illness (as defined above, under study overview) using a modified list of validated ICD-10-CM codes (Appendix). [56]
7.2. Sample size
Sample size estimates use the following considerations: (a) the cluster-randomized trial design, (b) ability to detect effect sizes comparable to treatment effect estimates from published literature, [25] and (c) two-tailed type 1 error rate of 0.025 given two trial primary outcomes. We expect approximately 87,000 older adults from 55 primary care practices to be eligible, of whom approximately 9200 will have a diagnosis of ADRD (10.6%) and 7000 will die within 12 months of study entry. Power calculations incorporate two features of SHARING Choices: 1) that practices are randomized to intervention versus control at a 1:2 ratio, and 2) that effects of clustering are accounted for by assuming variability in the control group success rate (analogous to an intraclass correlation assumption for a continuous outcome). We performed power calculations using the Optimal Design software package for cluster randomized trials. [61,62]
For our primary outcome, advance directive or MO(L)ST documentation, preliminary data indicates that advance directive documentation in the EHR is relatively low and varies by practice across our two health system partners. If we assume advance directive documentation in the EHR of 15% at baseline (reported base rate at JHCP at the time of trial design) [56] and a plausible range of ±10% (i.e. from 5% to 25%) based on nationally-representative estimates, we have power of 0.80 to detect an increase from 15% to 21% or greater. Because 29,000 patients are expected to be eligible for the intervention, an increase from 15% (4350 persons) to 21% (6090 persons) represents an increase in advance directive documentation among 1740 older adults at intervention practices. For the 9200 older adults expected to have an ADRD diagnosis, we have power of 0.80 to detect an increase from 15% to 22% or greater. Of these patients, 3064 are expected to be randomized to the intervention, and an increase from 15% (460 persons) to 22% (674 persons) represents an increase in advance directive documentation for 214 ADRD patients in intervention practices.
Based on US data, we project that 7000 of the 87,000 patients in the trial (8%) will die within 12 months of study entry, [63] and assume a base rate of potentially burdensome care of 18%, with a plausible range of ±5% (i.e., from 13% to 23%). [9] From these assumptions, we have power of 0.80 to detect a reduction in potentially burdensome care from 18% to 15% for the patients who die.
7.3. Randomization
The unit of randomization is the primary care practice, which reduces potential for contamination of controls and enables practice-wide deployment. We randomized practices to intervention or control in a 1:2 ratio because control practices incur no study cost and having more control practices affords greater precision in study outcome estimates. We first stratified practices by participating health system (JHCP or Medstar Health) since variation in system-level processes, culture, and intervention implementation could affect outcomes. Second, we balanced intervention and control groups on practice characteristics: geography (urban, suburban, rural location), percent of patients of Black race, percent of patients age ≥ 65, and number of primary care clinicians.
Because we include 20 JHCP and 35 Medstar Health practices, notable and problematic imbalances on practice-level characteristics may occur by chance in a single randomization. Methodological innovations are needed to achieve balance on multiple practice-level characteristics while maintaining the experimental rigor and inferential value of true random assignment.
Therefore, we used a covariate-constrained randomization (CCR) method to assure approximate balance on selected site characteristics across intervention and control groups. In this CCR, for each organization (JHCP and Medstar Health), 1000 randomizations were undertaken using a 1:2 assignment ratio. We then identified a subset of randomizations meeting 5 balancing characteristics (urban vs. suburban, rural vs. suburban, # of clinicians, % age ≥ 65, and % Black) and the following 3 criteria (Table 3):
The overall balance index, I, based on the half-normal distribution of the absolute value of SHARING Choices vs. Control differences on the balancing variables, was in the bottom 10%. That is, only the best 100 of the 1000 randomizations were further considered, following Huang and Roth. [64]
The p-value from a non-parametric test, the Kruskal-Wallis test, had to be >0.30 for each balancing variable, as recommended by Ciolino et al. for CCR. [65]
For JHCP, 1–2 urban and 2–3 rural practices were assigned to SHARING Choices; for MedStar Health, 3–4 urban and 2–3 rural practices were assigned to SHARING Choices.
For JHCP, 79 of the 1000 randomizations met all three criteria, and for MedStar Health, 41 of the 1000 randomizations met all three criteria. From the 79 JHCP and 41 MedStar Health eligible randomizations, one was randomly selected for each organization for preliminary randomization. Of the 55 practices, 20 were randomized to SHARING Choices and 35 to control.
7.4. Data analyses for primary outcomes
We compare SHARING Choices and control practices by analyzing the distribution of practice-level characteristics at baseline using appropriate graphical procedures, summary statistics, and multivariate methods. We examine consistency of effects stratified by patient age group, gender, race, ADRD diagnosis, and primary care practice.
We test the effects of SHARING Choices on all patients and on a subsample of patients with a diagnosis of ADRD, defined by ICD-10-CM diagnosis codes, as described above. For both analyses, we hypothesize that patients at intervention practices are more likely to have a documented advance directive and/or MO(L)ST in the EHR than patients at control practices at 12 months. We additionally hypothesize that among patients who die, those at intervention (versus control) practices are less likely to experience potentially burdensome end-of-life care within 6 months of death. All analyses are performed using SAS statistical software and account for the cluster design, with the patient as the unit of analysis. All primary analyses comparing the effect of SHARING Choices to usual care follow the principle of intention-to-treat, including all eligible study subjects with measurements at all available time points as appropriate to the outcome. The primary independent variable is group assignment at the initial time point that eligible patients are identified, consistent with intention-to-treat.
We assess comparability of patients in intervention and control groups by comparing the distribution of practice-level and patient-level characteristics at baseline using appropriate graphical procedures, summary statistics, and multivariate methods. The study is designed to produce balance on important covariates at the practice level (unit of randomization) but not necessarily at the patient level. Baseline patient and practice characteristics that differ between groups are included in our models of between-group differences. We use SAS Proc GLIMMIX to examine binary primary outcomes. The model includes practice variables as fixed effect practice-level covariates. Initial analyses examine baseline variables distributions and differences by intervention and control group. We build multilevel models accounting for practice-level randomization and group assignment and clustering of outcome distributions within practices. Multilevel models also include and control for baseline patient and practice-level covariates. In addition to overall effects of the intervention, we examine consistency of effects stratified by patient age group (< 75, ≥ 75) and primary care practice. We conduct parallel analyses to determine whether effects vary by primary outcome definition (AD alone versus AD+MOLST combined).
8. Conclusion
The design of this pragmatic trial of SHARING Choices has several advantages for evaluating potential improvements in processes and care for older adults with and without ADRD in primary care. First, the pragmatic nature of the trial allows for a flexible approach to fidelity at the practice level and adaptations as the trial continues. This was particularly important as many COVID-19 restrictions were still in place at trial launch, and as health system, local and federal initiatives to improve ACP and changes in EHR and portal and proxy systems and use evolve during the trial. Second, emphasizing training facilitators and incorporating strategies for those with ADRD is particularly important since these patients are often excluded and may require additional time to engage in effective ACP and document advance directives and/or MO (L)ST for the EHR. Finally, although EHR data has many limitations in outcome measurement, monitoring advance directive documentation and potentially burdensome care in EHRs across health systems and health information exchanges is an important advance in trials of care for large populations with serious illness.
The pragmatic nature of the trial also has limitations. Some parts of the intervention may be less successfully implemented than others given emerging health system priorities, measurement of implementation outcomes may be less complete and differ across health systems, and many aspects of ongoing ACP and related initiatives already integrated into health systems are not easily measurable, [27] but the randomized design should account for these issues.
Given these strengths and limitations, evaluating the impact of SHARING Choices will contribute to knowledge to better equip primary care in effective communication and team-based ACP, particularly for the critically important population with ADRD.
Acknowledgments
Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number R33AG061882. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We would also like to acknowledge the input of the translational advisory committee: Rachelle Bernacki, Mary Ersek, Rosemary Gibson (Patient Advisory Board member), Gabrielle Rocque and David Rolston.
The authors have no competing interests to disclose.
Appendix
Table.
Codes for potential burdensome care and serious illness.
| Codes for Potentially Burdensome Care at the End of Life (Numerator) [60] | ||
|---|---|---|
| Procedure | CPT/HCPCS Code | ICD-10-CM |
| Intubation and Mechanical Ventilation | 31,500 | OBH17EZ, OBH18EZ, OB717DZ, OB718DZ, 0BH07DZ, OBH07YZ, OBH172Z, OBH17YZ, OBH182Z, OBH18YZ, OBHK7YZ, OBHK8YZ, OBHL7YZ, OBHL7YZ, OBHL8YZ, OWHQ7YZ, 5A19, 5A1935Z, 5A1945Z, 5A1955Z, 5A12012, 5A19054 |
| Tracheostomy | 31,600, 31,601, 31,603 | OB11, OB110F4, OB11OZ4, OB113F4, OB113Z4, OB114F4, OB114Z4, |
| Gastrostomy Tube Insertion | 49,440, 43,761 | |
| Hemodialysis | 90,935, 90,937 | 5A1D, 5A1D00Z, 5A1D60Z |
| Enteral or Parenteral Nutrition | 43,750, 43,246, 44,372, 44,373, 74,350, 43,832, 43,830, 43,653, 49,440, 49,441, 49,446 | 0DH67UZ, 0DH68UZ, 3E0G36Z |
| Cardiopulmonary Resuscitation | 92,950 | 5A120012, 5A19054 |
| Codes for Serious Illness and Conditions (Denominator) [54,55] | |
|---|---|
| ICD-10-CM Code | |
| Cancer | ICD-10-CM liver excluding HCC (C22.1–4), esophagus (C15.3–5, C158–9), stomach (C16.0–6, C16.8–9), pancreas (C25.0–3, C25.7–9), peritoneum (C48.0–2, C48.8), brain (C71, C71.0–9), secondary malignant neoplasms (C78.00, C78.1–2, C78.39, C78.4–7, C78.89, C79.00, C79.11, C79.19, C79.2, C79.31–2, C79.49, C79.51–2, C79.60, C79.70, C79.81, C79.82, C79.89, C79.9), malignant pleural effusion (J91.0), malignant ascites (R18.0), disseminated malignant neoplasm (C80.0), leptomeningeal carcinomatosis (G96.12), heme malignancy (C81.09, C81.19, C81.29, C81.39, C81.49, C81.79, C81.99, C85.19, C85.29, C85.89, C91.02, C91.12, C91.52, C91.62, C91.92, C91.A2, C92.02, C92.12, C95.12). |
| Heart failure | ICD-10-CM (I09.81, I11.0, I13.0, I13.2, I50.1, I50.9, I50.20–23, I50.30–33, I50.40–43). |
| Chronic obstructive lung disease | ICD-10-CM (J43.9, J44.0, J44.1, J44.9). Home oxygen: ICD-10-CM (J95.850, Z99.1, Z99.11–12, Z99.81). |
| Cirrhosis | ICD-10-CM (K70.3, K70.30, K70.31, K70.4, K70.40, K70.41, K74.3–5, K74.60, K74.69). |
| Hepatic decompensation | ICD-10-CM (K65.9, K67, K65.0, K65.2, K65.8); esophageal varices: ICD-9 (456, 456.2, 456.21); ICD-10-CM (I85.01, I85.10, I85.11); ascites: ICD-9 (789.5, 789.51, 789.59); ICD-10-CM (R18.8). |
| End-stage renal disease | ICD-10-CM (N18.5, N18.6, Z94.0, Z99.2, Z91.15, Z49.31, Z49.01, Z49.02, Z49.32). |
| Amyotrophic Lateral Sclerosis | ICD-10-CM (G12.21). |
| Alzheimer’s Disease and Related Dementias (ADRD) | ICD-10-CM (F01.50, F01.51, F02.80, F02.81, F03.90, F03.91, G30.0, G30.1, G30.9, G31.01, G31.09, G31.83, G31.84, R41.81) (includes code G31.84, Mild Cognitive Impairment) |
Footnotes
CRediT authorship contribution statement and full SHARING Choices authorship group
Sydney M. Dy: Conceptualization, Methodology, Project administration, Writing – original draft, Supervision, Funding acquisition. Daniel L. Scerpella: Conceptualization, Project administration, Resources, Writing – review & editing. Valerie Cotter: Writing – review & editing, Supervision. Jessica Colburn: Conceptualization, Methodology, Project administration, Supervision. David L. Roth: Conceptualization, Methodology, Writing – original draft. Maura McGuire: Conceptualization, Writing – review & editing. Erin Rand Giovannetti: Methodology, Writing – review & editing. Kathryn A. Walker: Methodology, Project administration, Resources, Supervision. Naaz Hussain: Methodology. Danetta H. Sloan: Methodology, Project administration. Cynthia M. Boyd: Methodology, Supervision. Kimberley Cockey: Project administration. Neha Sharma: Methodology, Project administration, Supervision. Martha Abshire Saylor: Methodology. Kelly M. Smith: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing, Funding acquisition. Jennifer L. Wolff: Conceptualization, Methodology, Project administration, Resources, Supervision, Writing – original draft, Funding acquisition. Ryan Anderson: Conceptualization, Project administration, Resources. Diane Echavarria: Methodology, Project administration. Tara Funk-houser: Methodology. Karyn Lee Carlson Nicholson: Project administration, Resources. Christine Rawlinson: Project administration, Resources, Supervision. Sri Ribala: Methodology. Meena Seshamani: Conceptualization, Methodology, Resources. Laura Torres: Project administration.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- [1].Hurd MD, Martorell P, Delavande A, Mullen KJ, Langa KM, Monetary costs of dementia in the United States, N. Engl. J. Med 368 (14) (2013) 1326–1334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].CDC, Pages. Accessed at U.S. Government Printing Office at https://www.cdc.gov/nchs/data/hus/hus17.pdf, 2017.
- [3].Bernacki RE, Block SD, For the American College of Physicians High Value Care Task F. Communication about serious illness care goals: a review and synthesis of best practices, JAMA Intern. Med 174 (12) (2014) 1994–2003. [DOI] [PubMed] [Google Scholar]
- [4].Sudore RL, Lum HD, You JJ, Hanson LC, Meier DE, Pantilat SZ, et al. , Defining advance care planning for adults: a consensus definition from a multidisciplinary Delphi panel, J. Pain Symptom Manag 53 (5) (2017) 821–32 e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Song MK, Ward SE, Hepburn K, Paul S, Kim H, Shah RC, et al. , Can persons with dementia meaningfully participate in advance care planning discussions? A mixed-methods study of SPIRIT, J. Palliat. Med 22 (11) (2019) 1410–1416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Wendrich-van Dael A, Bunn F, Lynch J, Pivodic L, Van den Block L, Goodman C, Advance care planning for people living with dementia: an umbrella review of effectiveness and experiences, Int. J. Nurs. Stud 107 (2020), 103576. [DOI] [PubMed] [Google Scholar]
- [8].Harrison KL, Adrion ER, Ritchie CS, Sudore RL, Smith AK, Low completion and disparities in advance care planning activities among older Medicare beneficiaries, JAMA Intern. Med 176 (12) (2016) 1872–1875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Nicholas LH, Bynum JP, Iwashyna TJ, Weir DR, Langa KM, Advance directives and nursing home stays associated with less aggressive end-of-life care for patients with severe dementia, Health Aff (Millwood). 33 (4) (2014) 667–674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Lakin JR, Block SD, Billings JA, Koritsanszky LA, Cunningham R, Wichmann L, et al. , Improving communication about serious illness in primary care: a review, JAMA Intern. Med 176 (9) (2016) 1380–1387. [DOI] [PubMed] [Google Scholar]
- [11].Piers R, Albers G, Gilissen J, De Lepeleire J, Steyaert J, Van Mechelen W, et al. , Advance care planning in dementia: recommendations for healthcare professionals, BMC Palliat Care. 17 (1) (2018) 88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Karlawish J, Casarett D, James B, Xie S, Kim S, The ability of persons with Alzheimer disease (AD) to make a decision about taking an AD treatment, Neurology. 64 (9) (2005) 1514–1519. [DOI] [PubMed] [Google Scholar]
- [13].Hirschman K, Xie S, Feudtner C, Karlawish J, How does an Alzheimer’s disease patient’s role in medical decision making change over time? J. Geriatr. Psychiatry Neurol 17 (2) (2004) 55–60. [DOI] [PubMed] [Google Scholar]
- [14].Vick J, Amjad H, Smith KC, Boyd CM, Gitlin LN, Roth DL, et al. , “Let him speak:” a descriptive qualitative study of the roles and behaviors of family companions in primary care visits among older adults with cognitive impairment, Int J Geriatr Psychiatry. 33 (1) (2018) e12–e103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Hirschman KB, Kapo JM, Karlawish JH, Identifying the factors that facilitate or hinder advance planning by persons with dementia, Alzheimer Dis. Assoc. Disord 22 (3) (2008) 293–298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Wolff JL, Roter DL, Hidden in plain sight: medical visit companions as a quality of care resource for vulnerable older adults, Arch. Intern. Med 168 (13) (2008) 1409–1415. [DOI] [PubMed] [Google Scholar]
- [17].Wolff JL, Roter DL, Family presence in routine medical visits: a meta-analytical review, Soc. Sci. Med 72 (6) (2011) 823–831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Wolff JL, Roter DL, Older adults’ mental health function and patient-centered care: does the presence of a family companion help or hinder communication? J. Gen. Intern. Med 27 (6) (2012) 661–668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].van der Steen JT, van Soest-Poortvliet MC, Hallie-Heierman M, Onwuteaka-Philipsen BD, Deliens L, de Boer ME, et al. , Factors associated with initiation of advance care planning in dementia: a systematic review, J. Alzheimers Dis 40 (3) (2014) 743–757. [DOI] [PubMed] [Google Scholar]
- [20].Sharp T, Moran E, Kuhn I, Barclay S, Do the elderly have a voice? Advance care planning discussions with frail and older individuals: a systematic literature review and narrative synthesis, Br. J. Gen. Pract 63 (615) (2013) e657–e668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Kasper JD, Freedman VA, Spillman BC, Wolff JL, The disproportionate impact of dementia on family and unpaid caregiving to older adults, Health Aff (Millwood). 34 (10) (2015) 1642–1649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Friedman EM, Shih RA, Langa KM, Hurd MD, US prevalence and predictors of informal caregiving for dementia, Health Aff (Millwood). 34 (10) (2015) 1637–1641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Alzheimer’s Association, Alzheimer’s Disease: Facts and Figures, 2013, p. 2013. [DOI] [PubMed]
- [24].Fetherstonhaugh D, McAuliffe L, Bauer M, Shanley C, Decision-making on behalf of people living with dementia: how do surrogate decision-makers decide? J. Med. Ethics 43 (1) (2017) 35–40. [DOI] [PubMed] [Google Scholar]
- [25].Oczkowski SJ, Chung HO, Hanvey L, Mbuagbaw L, You JJ, Communication tools for end-of-life decision-making in ambulatory care settings: a systematic review and meta-analysis, PLoS One 11 (4) (2016), e0150671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Sloan DH, Hannum SM, DeGroot L, Dy SM, Waldfogel J, Chyr LC, et al. , Advance care planning shared decision-making tools for non-cancer chronic serious illness: a mixed method systematic review, Am J Hosp Palliat Care. 38 (12) (2021) 1526–1535. [DOI] [PubMed] [Google Scholar]
- [27].Morrison RS, Meier DE, Arnold RM, What’s wrong with advance care planning? JAMA. 326 (16) (2021) 1575–1576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Sudore RL, Fried TR, Redefining the “planning” in advance care planning: preparing for end-of-life decision making, Ann. Intern. Med 153 (4) (2010) 256–261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].IOM, Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life, National Academy Press, Washington DC, 2014. [PubMed] [Google Scholar]
- [30].Walczak A, Butow PN, Bu S, Clayton JM, A systematic review of evidence for end-of-life communication interventions: who do they target, how are they structured and do they work? Patient Educ. Couns 99 (1) (2016) 3–16. [DOI] [PubMed] [Google Scholar]
- [31].Mitchell SL, Black BS, Ersek M, Hanson LC, Miller SC, Sachs GA, et al. , Advanced dementia: state of the art and priorities for the next decade, Ann. Intern. Med 156 (1 Pt 1) (2012) 45–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Jones K, Birchley G, Huxtable R, Clare L, Walter T, Dixon J, End of life care: a scoping review of experiences of advance care planning for people with dementia, Dementia (London). 18 (3) (2019) 825–845. [DOI] [PubMed] [Google Scholar]
- [33].Abu Al Hamayel N, Isenberg SR, Sixon J, Smith KC, Pitts SI, Dy SM, et al. , Preparing older patients with serious illness for advance care planning discussions in primary care, J. Pain Symptom Manag 58 (2) (2019) 244–51 e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Institute of Medicine (U.S.). Committee on Approaching Death: Addressing Key End-of-Life Issues. Dying in America : Improving Quality and Honoring Individual Preferences near the End of Life, The National Academies Press, Washington, D.C., 2015. [PubMed] [Google Scholar]
- [35].Epstein RM, Street RL Jr., Shared mind: communication, decision making, and autonomy in serious illness, Ann. Fam. Med 9 (5) (2011) 454–461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Yates M, Tennstedt S, Chang B, Contributors to and mediators of psychological well-being for informal caregivers, J Gerontol B Psychol. Sci 54B (12–22) (1999). [DOI] [PubMed] [Google Scholar]
- [37].Pearlin L, Mullan J, Semple S, Skaff M, Caregiving and the stress process: an overview of concepts and their measures, Gerontologist. 30 (5) (1990) 583–594. [DOI] [PubMed] [Google Scholar]
- [38].Aday L, Andersen R, A framework for the study of access to medical care, Health Serv. Res 208–20 (1974). [PMC free article] [PubMed] [Google Scholar]
- [39].Andersen RM, Revisiting the behavioral model and access to medical care: does it matter? J. Health Soc. Behav 36 (1) (1995) 1–10. [PubMed] [Google Scholar]
- [40].Otte-Trojel T, de Bont A, Rundall TG, van de Klundert J, How outcomes are achieved through patient portals: a realist review, J. Am. Med. Inform. Assoc 21 (4) (2014) 751–757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].de Lusignan S, Mold F, Sheikh A, Majeed A, Wyatt JC, Quinn T, et al. , Patients’ online access to their electronic health records and linked online services: a systematic interpretative review, BMJ Open 4 (9) (2014), e006021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Rojas Smith L, Ashok M, Morss Dy S, Wines RC, Teixeira-Poit S, Contextual Frameworks for Research on the Implementation of Complex System Interventions, Rockville (MD), 2014. [PubMed] [Google Scholar]
- [43].Damschroder L, Aron D, Keith S, Kirsh J, Alexander B, Lowery J, Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science, Implement. Sci 50 (4) (2009). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Detering KM, Hancock AD, Reade MC, Silvester W, The impact of advance care planning on end of life care in elderly patients: randomised controlled trial, BMJ. 340 (2010), c1345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Rocque GB, Dionne-Odom JN, Sylvia Huang CH, Niranjan SJ, Williams CP, Jackson BE, et al. , Implementation and impact of patient lay navigator-led advance care planning conversations, J. Pain Symptom Manag 53 (4) (2017) 682–692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Prochaska J, Velicer W, The transtheoretical model of health behavior change, Am. J. Health Promot 12 (1) (1997) 38–48. [DOI] [PubMed] [Google Scholar]
- [47].Sudore RL, Schickedanz AD, Landefeld CS, Williams BA, Lindquist K, Pantilat SZ, et al. , Engagement in multiple steps of the advance care planning process: a descriptive study of diverse older adults, J. Am. Geriatr. Soc 56 (6) (2008) 1006–1013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].Maryland Department of Health. health.maryland.gov/mdpcp/Pages/home.aspx, 2021. on November 24, 2021.
- [49].Seow H, Piet L, Kenworthy CM, Jones S, Fagan PJ, Dy SM, Evaluating a palliative care case management program for cancer patients: the Omega Life Program, J. Palliat. Med 11 (10) (2008) 1314–1318. [DOI] [PubMed] [Google Scholar]
- [50].Wang L, Piet L, Kenworthy CM, Dy SM, Association between palliative case management and utilization of inpatient, intensive care unit, emergency department, and hospice in Medicaid beneficiaries, Am J Hosp Palliat Care. 32 (2) (2015) 216–220. [DOI] [PubMed] [Google Scholar]
- [51].Abu Al Hamayel N, Isenberg SR, Hannum SM, Sixon J, Smith KC, Dy SM, Older patients’ perspectives on quality of serious illness care in primary care, Am J Hosp Palliat Care. 35 (10) (2018) 1330–1336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Luu NP, Nigrin C, Peairs K, Dy SM, Sawyer M, Pitts S, et al. , Increasing advance care planning completion at an academic internal medicine outpatient clinic, J. Pain Symptom Manag 54 (3) (2017) 383–386. [DOI] [PubMed] [Google Scholar]
- [53].Wolff JL, Scerpella D, Cockey K, Hussain N, Funkhouser T, Echavarria D, et al. , SHARING choices: a pilot study to engage family in advance care planning of older adults with and without cognitive impairment in the primary care context, Am J Hosp Palliat Care. 38 (11) (2021) 1314–1321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].Walling AM, Sudore RL, Bell D, Tseng CH, Ritchie C, Hays RD, et al. , Population-based pragmatic trial of advance care planning in primary care in the University of California health system, J. Palliat. Med 22 (S1) (2019) 72–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Alzheimer’s Association, Medicare’s Cognitive Impairment Assessment and Care Planning Codes, 2017.
- [56].Hussain NA, McGuire M, Colburn JL, Advance Care Planning Workflow Implementation for Older Adults in Primary Care, Society for General Internal Medicine, Denver CO, 2018. [Google Scholar]
- [57].Hammes BJ, Rooney BL, Death and end-of-life planning in one midwestern community, Arch. Intern. Med 158 (4) (1998) 383–390. [DOI] [PubMed] [Google Scholar]
- [58].Huang CH, Crowther M, Allen RS, DeCoster J, Kim G, Azuero C, et al. , A pilot feasibility intervention to increase advance care planning among African Americans in the deep south, J. Palliat. Med 19 (2) (2016) 164–173. [DOI] [PubMed] [Google Scholar]
- [59].Bellg AJ, Borrelli B, Resnick B, Hecht J, Minicucci DS, Ory M, et al. , Enhancing treatment fidelity in health behavior change studies: best practices and recommendations from the NIH behavior change consortium, Health Psychol. 23 (5) (2004) 443–451. [DOI] [PubMed] [Google Scholar]
- [60].Wasp GT, Alam SS, Brooks GA, Khayal IS, Kapadia NS, Carmichael DQ, et al. , End-of-life quality metrics among medicare decedents at minority-serving cancer centers: a retrospective study, Cancer Med. 9 (5) (2020) 1911–1921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [61].Raudenbush SW, Liu X, Statistical power and optimal design for multisite randomized trials, Psychol. Methods 5 (2) (2000) 199–213. [DOI] [PubMed] [Google Scholar]
- [62].Spybrook J, Raudenbush SW, Liu X, Congdon R, Martinez A, Optimal Design for Longitudinal and Multilevel Research: Documentation for the “Optimal Design” Software, University of Michigan School of Education, Hierarchical Models Project, Ann Arbor, 2006. [Google Scholar]
- [63].Carey EC, Walter LC, Lindquist K, Covinsky KE, Development and validation of a functional morbidity index to predict mortality in community-dwelling elders, J. Gen. Intern. Med 19 (10) (2004) 1027–1033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [64].Huang J, Roth DL, Using the half normal distribution to quantify covariate balance in cluster-randomized pragmatic trials, Trials. 22 (1) (2021) 190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [65].Ciolino JD, Diebold A, Jensen JK, Rouleau GW, Koloms KK, Tandon D, Choosing an imbalance metric for covariate-constrained randomization in multiple-arm cluster-randomized trials, Trials. 20 (1) (2019) 293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [66].Heiman H, Bates DW, Fairchild D, Shaykevich S, Lehmann LS, Improving completion of advance directives in the primary care setting: a randomized controlled trial, Am. J. Med 117 (5) (2004) 318–324. [DOI] [PubMed] [Google Scholar]
- [67].Haywood K, Marshall S, Fitzpatrick R, Patient participation in the consultation process: a structured review of intervention strategies, Patient Educ. Couns 63 (1–2) (2006) 12–23. [DOI] [PubMed] [Google Scholar]
- [68].Kinnersley P, Edwards A, Hood K, Ryan R, Prout H, Cadbury N, et al. , Interventions before consultations to help patients address their information needs by encouraging question asking: systematic review, BMJ. 337 (2008), a485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [69].Wolff JL, Roter DL, Barron J, Boyd CM, Leff B, Finucane T, et al. , A tool to strengthen the older patient-companion partnership in primary care: results from a pilot study, J. Am. Geriatr. Soc 62 (2) (2014) 312–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [70].Wolff JL, Berger A, Clarke D, Green JA, Stametz RA, Yule C, et al. , Patients, care partners, and shared access to the patient portal: online practices at an integrated health system, J. Am. Med. Inform. Assoc 23 (6) (2016) 1150–1158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [71].Peterson K, Hahn H, Lee AJ, Madison CA, Atri A, In the information age, do dementia caregivers get the information they need? Semi-structured interviews to determine informal caregivers’ education needs, barriers, and preferences, BMC Geriatr. 16 (1) (2016) 164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [72].McCabe M, You E, Tatangelo G, Hearing their voice: a systematic review of dementia family Caregivers’ needs, Gerontologist. 56 (5) (2016) e70–e88. [DOI] [PubMed] [Google Scholar]
- [73].Handley M, Bunn F, Goodman C, Dementia-friendly interventions to improve the care of people living with dementia admitted to hospitals: a realist review, BMJ Open 7 (7) (2017), e015257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [74].Health Resources and Services Administration. bhw.hrsa.gov/grants/geriatrics/alzheimers-curriculum, 2017.
- [75].Reuben D, Levin J, Frank J, Hirsch S, McCreath H, Roth C, et al. , Closing the dementia care gap: can referral to Alzheimer’s Association chapters help? Alzheimers Dement. 5 (6) (2009) 498–502. [DOI] [PMC free article] [PubMed] [Google Scholar]