

Abstract
Case Summary
A 27 years old female presented to gynae OPD with foul smelling discharge per vaginum off and on for a year and was given treatment for PID (Pelvic inflammatory disease) and cervicitis. Pap smear was taken and was reported unsatisfactory due to inflammation. Colposcopy was planned later due to her bothersome complaints and suspicious looking cervix. A white worm popped out of cervix while doing colposcopy which turned out to be Trichuris trichiura. Deworming was done for the patient and her family members. Patient reported again with similar complaints and this time colposcopy and guided biopsy was done that showed Tubercular Granulomatous cervicitis hence, she was put on category I ATT (Anti-tubercular treatment) that relieved her symptoms and improved cervical findings.
Conclusion
People living in tropical and subtropical areas are at highest risk of infection by T. trichiura. This is the first case of T. trichiura in ectopic location and first case of a live worm found in female genital tract. Previous studies have shown that helminthic infection can reactivate latent TB and aggravate the disease expression.
Keywords: Trichuris trichiura, Vaginal discharge, Genital helminthiasis, Granulomatous cervicitis, Tuberculosis
Introduction
Trichuris trichiura is an intestinal helminth belonging to Phylum Nematode that causes trichuriasis in humans. It is referred to as the whipworm because it looks like a whip with a short and broad posterior end and a very long and narrow anterior end. It is one of the three most prevalent STHs (soil-transmitted helminth) in the world along with Ascaris lumbricoides and hookworms. It is estimated that more than two billion people in the world are infected with at least one of these STHs [1].
Genital tract infection of helminthic worms is extremely rare and this case of trichuriasis of genital tract is the first reported case of extraintestinal trichuriasis. This is the first case of live worm detected in the female genital tract and the first case report of whipworm seen in an ectopic location.
Case Summary
A 27-year-old multiparous female reported in gynae OPD with complaints of pain in the lower abdomen and excessive foul-smelling discharge per vaginum for the past one year which was associated with backache and itching in perineum. Her general physical and systemic examination was unremarkable. Her per speculum examination revealed hypertrophied cervix and copious mixed discharge. This was associated with forniceal tenderness on vaginal examination. She was given treatment for Pelvic inflammatory disease (Tablet Doxycycline and Tablet Metronidazole for 2 weeks) along with vaginal pessaries based on her clinical findings and was asked to follow up after 2 weeks. On follow-up visit, she was only partially relieved of her symptoms. Her Pap smear was taken which was reported unsatisfactory obscured by inflammatory cells. Because of the troublesome complaints of persistent discharge despite antibiotic course and suspicious-looking cervix, the decision for colposcopy was taken. During colposcopy, as soon as acetic acid was applied, which is a known irritant, a whitish long worm popped out of the ectocervix and started wriggling over the cervix. It could be taken out completely off the cervix with great difficulty by wrapping it on a swab-stick as it was trying to burrow itself back into its abode. The worm was sent to the microbiology department for the identification (Fig. 1a and b-video) and was reported as Trichuris trichiura. History was reviewed again but there was no history of perineal itching or passage of worms in stool in patients or in family members. Once the diagnosis of whipworm was made, we did deworming of the patient along with her family members. Tab Mebendazole 100 mg twice a day for 3 days was given to the patient along with a repeat course after 2 weeks in consultation with the microbiologist. To our surprise, the patient came back again with similar complaints of discharge per vaginum and now colposcopy, and directed cervical biopsy was taken which came out to be tubercular granulomatous cervicitis (Fig. 2). She was given ATT for 6 months, following which she was relieved of her symptoms along with improvement in her cervical findings.
Fig. 1.

a Whipworm wriggling over the cervix. b video of a wriggly worm
Fig. 2.
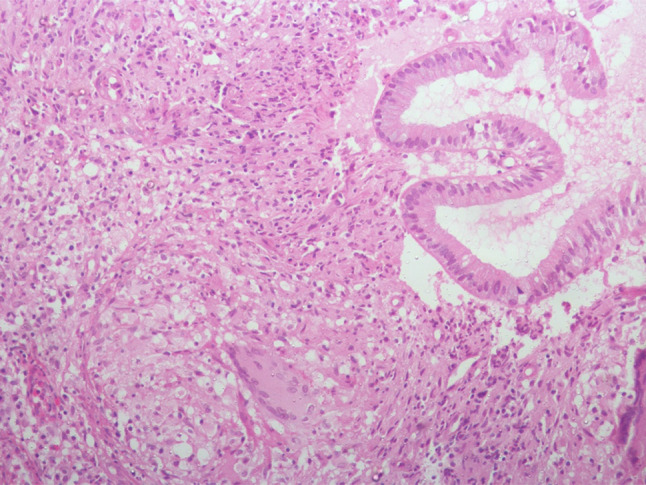
Granulomatous cervicitis
Discussion
Trichuris trichiura is an intestinal helminth belonging to phylum Nematode. It has a worldwide distribution with areas of hyper-endemicity located in tropical and subtropical regions. However, populations without access to safe water and sanitation elsewhere are also at increased risk of infection [1].
Humans are the only known hosts of T. trichiura. Life cycle in the human host starts with oral ingestion of embryonated eggs and in the small intestine, larvae are released from the embryonated eggs. Larvae mature through four phases to develop into large intestine-dwelling adults (both male and female). The adult worm resides in either the cecum and/or the ascending colon. Sixty to seventy days after infection, females start laying eggs that are released along with the feces, and then, in soil at appropriate temperature and humidity, these eggs become embryonated, and the cycle repeats itself.
Clinical manifestations may vary and depend on the degree of infestation. Mild infestations are usually asymptomatic, only 10% have symptoms, whereas heavy infections may manifest with watery, mucus-laden, bloody, painful diarrhea, which may progress into anemia and growth retardation if not treated. Rectal prolapse is also associated with heavy infections. WHO recommends the use of the Kato–Katz method to examine stool samples by direct microscopy for the identification of unembryonated eggs. Eosinophilia, if present, is usually mild. Treatment includes tablet Albendazole 400 mg single dose or tablet Mebendazole 100 mg twice daily for 3 days. In recurrent infection, a second course is recommended [2].
On searching the literature, we found that Genital helminthiasis is a known entity though a rare one. However, most of the reported cases of genital helminthiasis are with pinworm infestation, i.e., Enterobious vermicularis and very few with. S. stercoralis, Entamoeba histolytica. Cases have been reported in literature involving the vagina, cervix, uterus, ovaries, and peritoneum. Patients with the symptomatic disease have been reported to present with clinical features of vulvovaginitis, cervicitis, salpingitis, endometriosis, urinary tract infections, postmenopausal bleeding, pelvic mass, tubo-ovarian abscess, and generalized peritonitis. We could not find any case of Trichuris trichiura in ectopic location in the reproductive tract. All of the previously reported cases of worm infestation involved an accidental finding of ova on cervical or vaginal smears or generally diagnosed as granuloma containing the parasite or ova with variable degrees of necrosis and fibrosis in surgical or autopsy tissue specimens [3]. Never ever a live worm has been reported from the genital tract. This is the first case where a live worm had been retrieved from the female genital tract. We all know the specific affinity of these worms to poor hygiene. The worm came in search of new pastures and found one in the dirty diseased cervix of our patient.
Tuberculosis patients are commonly found to have co-infection with helminth species such as Trichuris trichiura and Ascaris lumbricoides. Helminthic infection can reactivate latent Tuberculosis and aggravate the disease expression. Limited epidemiological studies in Ethiopia have shown that chronic parasitic infection could increase the risk of Tuberculosis. High tubercular—intestinal parasitic co-infection prevalence rate has been reported from parts of Ethiopia in Gondar (33.3%) and Arba Minch (26.3%) and north-east ethopia (10%) [4]. We noted a similar finding in our patient who was later diagnosed with cervical TB and she responded well with ATT. Therefore, a possibility of helminthic infestation should always be kept in mind while dealing with patients of chronic vaginal discharge, especially in tropical and subtropical regions which are endemic to soil-transmitted helminths.
Conclusion
Genital helminthiasis is a known but rare entity. We should always keep in mind the possibility of helminthic infestation in patients with chronic vaginal discharge in tropical countries. Helminthic infection can reactivate latent TB and aggravate the disease expression. Proper knowledge about the disease will help in managing such cases with adequate patients’ satisfaction.
Richa Aggarwal
She is graduate from Maulana Azad Medical college. She did her postgraduation and senior residency from UCMS and GTB hospital Delhi. Currently she is working as Associate Professor at UCMS and GTB Hospital. Her area of interest are colposcopy and fetal medicine. 
Funding
None.
Declarations
Conflict of interest
The authors declared that they have no conflict of interest.
Informed consent
Informed consent was taken from the individual who participated in the study and also for reproducing the images and histopathology report.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. This is a case report where the patient was managed according to the treatment protocol, and informed consent was taken from the patient for the case report as well as for reproducing images and histopathology report.
Footnotes
Dr. Richa Aggarwal, Associate Professor, Obstetrics and Gynaecology, UCMS and GTB Hospital; Dr. Abha Sharma, Senior Specialist, Obstetrics and Gynaecology, UCMS and GTB Hospital; Dr. Preeti Sharma. Senior Resident, Obstetrics and Gynaecology, UCMS and GTB Hospital; Dr. Archana Chaudhary, Specialist, Obstetrics and Gynaecology, UCMS and GTB Hospital; Dr Amita Suneja, Director Professor & Head of Department, Obstetrics and Gynaecology, UCMS & GTB Hospital.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Richa Aggarwal, Email: richa.agg77@gmail.com.
Abha Sharma, Email: drabhasharma.obg@gmail.com.
Preeti Sharma, Email: medicalgroup101@gmail.com.
Archana Choudhary, Email: drarchana.73@gmail.com.
Amita Suneja, Email: amita_suneja@yahoo.co.in.
References
- 1.Bansal R, Huang T, Chun S. Trichuriasis. Am J Med Sci. 2018;2:355. doi: 10.1016/j.amjms.2017.09.003. [DOI] [PubMed] [Google Scholar]
- 2.Yu W, Ross AG, Olveda RM, Harn DA, Li Y, Chy D, et al. Risk of human helminthiases: geospatial distribution and targeted control. Int J Infect Dis. 2017;55:131–138. doi: 10.1016/j.ijid.2016.12.013. [DOI] [PubMed] [Google Scholar]
- 3.Anand KV, Mishra GA, Pimple SA, Pathuthara S, Kulkarni VY. Detection of rare parasite on Pap smear. Cytojournal. 2020;17:18. doi: 10.25259/Cytojournal_74_2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gashaw F, Bekele S, Mekonnen Y, et al. High helminthic co-infection in tuberculosis patients with undernutritional status in northeastern Ethiopia. Infect Dis Poverty. 2019;8:88. doi: 10.1186/s40249-019-0600-2. [DOI] [PMC free article] [PubMed] [Google Scholar]