

Abstract
Ectopic and supernumerary parathyroid glands in the neck is a real surgical challenge especially in multi-gland pathologies. We report a supernumerary ectopic gland at a rare site in the neck in a chronic kidney disease patient which required a re-exploration following a deceptively successful bilateral neck dissection.
Keywords: Ectopic, Supernumerary, Parathyroid gland, 4D CT, Exploration
Introduction
Hyperparathyroidism (HPT) is a relatively common endocrine disorder after diabetes and thyroid disorders [1]. It can be broadly classified in to primary, secondary and tertiary HPT. Adenoma or hyperplasia of single or multiple glands and rarely carcinoma of a gland gives rise to any of these clinical subtypes. Secondary and tertiary HPT are more common in chronic kidney disease (CKD) patients and standard bilateral neck exploration (BNE) is required in these patients for symptom relief and avoiding complications [2].
Case Report
A 55-year-old male patient, CKD on haemodialysis, initially diagnosed to have secondary hyperparathyroidism with intact parathyroid hormone (i-PTH) level 2400 pg/ml on high frequency ultrasound (HFUS) examination showed a total of 4 parathyroid glands in either tracheo-oesophageal grooves. A Tc-99 m sestamibi scanning is not mandatory prior to a conventional BNE but the patient had done it one year back from another hospital which revealed greater uptake on left inferior pole of thyroid. All the 4 parathyroids concordant with the HFUS findings were successfully removed in a BNE which included a gland inferior to the left lobe of thyroid as well. i-PTH remained elevated next morning at 2100 pg/ml. and hence the sestamibi was repeated immediately. Left inferior activity was found to persist and a HFUS repeated in the afternoon revealed no additional information. A 4-dimensional computerized tomography (4D CT) of neck was performed on the same day evening which showed a 2 cm sized ectopic parathyroid gland behind the proximal common carotid artery on left side. On the second post-operative day morning, a repeat exploration was done and the ectopic gland was successfully removed from behind the common carotid artery on the left side at a level inferior to left lobe of thyroid and i-PTH came down to 10 pg/ml. after 10 min of surgery. Biopsy confirmed the successful removal of 4 hyperplastic glands in the initial surgery with a 5th gland showing adenoma at the ectopic position, making the final diagnosis tertiary HPT with a supernumerary ectopic adenoma.
Discussion
HPT is a relatively common endocrine disorder [1] and the secondary HPT with multi gland pathology is well known among CKD patients dependent on dialysis [2]. Ectopic and supernumerary glands though uncommon can pose real challenges to the surgical team. In single gland disease, focussed surgery is preferred over a standard BNE which is the rule in a multi gland disease [3, 4]. Preoperative localisation is mandatory in focussed surgeries and imaging studies include HFUS, 4D CT and Tc-99 Sestamibi scan. Notoriously operator dependent in parathyroid, HFUS is continues to be a useful basic test which can assess thyroid and other neck structures simultaneously and often helps in a guided aspiration if indicated. It can also be safely repeated as many times as needed and even during a surgery. Sestamibi is a functional test lacking anatomical details but shows high sensitivity and specificity in lateralizing the pathological gland to one side or even to unsuspected ectopic sites. 4D CT (a multiplanar CT scan with a fourth dimension consisting of changes in contrast attenuation over periods of time) combining great anatomical delineation and functional assessment is a more realistic tool especially in a redo procedure [6]. Concordance between two tests are more dependable than an advanced single imaging [5, 7]. Prior to BNE, a pre-operative imaging study or intraoperative i-PTH (intact parathyroid hormone) testing is not considered mandatory but surgeon often finds them useful.
In our case, HFUS and sestamibi appeared concordant and first surgery went well with recovery of all four parathyroids and hence intra operative i- PTH was not monitored. The uncalled for sestamibi (Fig. 1) appeared curiously deceptive in this case compared to a realistic picture of a 4D CT scan (Fig. 2). Thinking retrospectively, a more extensive first surgery based on persistent intra operative i-PTH values would have resulted in unwanted thyroid lobectomies, thymectomy and unnecessary carotid sheath explorations which would presumably fail to find out an ectopic in the rare site behind common carotid artery in the lower neck. Had the first surgery been extensive, there is also the possibility of 4D CT being not feasible after destruction of vascular supply which would impede the fourth vascular dimension of the imaging [8]. Though the patient had to undergo a second surgery immediately, he was fortunate to have an easy surgery without the complications of a second surgery at a later date in a scarred neck. Accurate localization is mandatory prior to a re exploration and this rule may be extrapolated to extensive blind neck explorations as well in the modern era where accurate anatomical delineation is possible with imaging like 4D CT which offers both anatomical and functional detail in a parathyroid gland whose vascularity is intact.
Fig. 1.

Tc-99 m sestamibi picture of ectopic parathyroid mimicking a left eutopic inferior gland
Fig. 2.
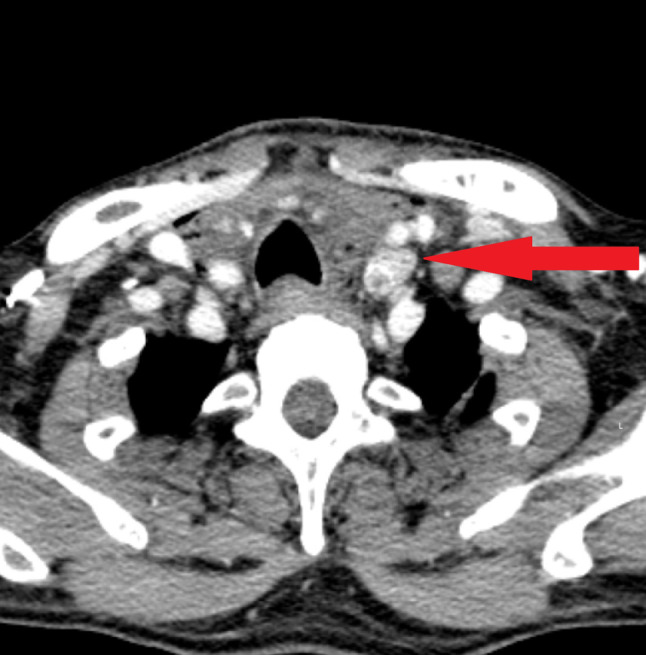
4D CT scan section of ectopic parathyroid gland behind common carotid artery, corresponding to the Sestamibi picture in Fig. 1
Compliance with ethical standards
Conflict of interest
They authors declare that they have no conflict of interest.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Muhammed Unais T, Email: muhammedunaisdr@gmail.com.
Prathosh Gangadhar, Email: prathosh@yahoo.com.
Shahul Hameed, Email: shahuldr@gmail.com.
Nejima Kolikkat, Email: drnejimakk2011@gmail.com.
References
- 1.DeLellis RA, Mazzaglia P, Mangray S. Primary hyperparathyroidism: a current perspective. Arch Pathol Lab Med. 2008;132(8):1251–1262. doi: 10.5858/2008-132-1251-PHACP. [DOI] [PubMed] [Google Scholar]
- 2.Bellasi A, Cozzolino M, Malberti F, Cancarini G, Esposito C, Guastoni CM, et al. New scenarios in secondary hyperparathyroidism: etelcalcetide. Position paper of working group on CKD-MBD of the Italian Society of Nephrology. J Nephrol. 2020;33(2):211–221. doi: 10.1007/s40620-019-00677-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Noureldine SI, Gooi Z, Tufano RP. Minimally invasive parathyroid surgery. Gland Surg. 2015;4(5):410–419. doi: 10.3978/j.issn.2227-684X.2015.03.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.van der Plas WY, Dulfer RR, Koh EY, Vogt L, Appelman-Dijkstra NM, Schepers A, et al. Safety and efficacy of subtotal or total parathyroidectomy for patients with secondary or tertiary hyperparathyroidism in four academic centers in the Netherlands. Langenbecks Arch Surg. 2018;403(8):999–1005. doi: 10.1007/s00423-018-1726-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kowa XY, Richards P, Waterhouse M, Parvanta L, Adams A. Atypical presentations of parathyroid gland pathology: a pictorial review. Eur J Radiol Open. 2019;6:320–329. doi: 10.1016/j.ejro.2019.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Malinzak MD, Sosa JA, Hoang J. 4D-CT for detection of parathyroid adenomas and hyperplasia: state of the art imaging. Curr Radiol Rep. 2017;5:8. doi: 10.1007/s40134-017-0198-8. [DOI] [Google Scholar]
- 7.Nasiri S, Soroush A, Hashemi AP, Hedayat A, Donboli K, Mehrkhani F. Parathyroid adenoma localization. Med J Islam Repub Iran. 2012;26(3):103–109. [PMC free article] [PubMed] [Google Scholar]
- 8.Hoang JK, Sung WK, Bahl M, Phillips CD. How to perform parathyroid 4D CT: tips and traps for technique and interpretation. Radiology. 2014;270(1):15–24. doi: 10.1148/radiol.13122661. [DOI] [PubMed] [Google Scholar]