

Abstract
Laryngopharyngeal Reflux Disease (LPRD) is form of extra-oesophageal reflux due to the backflow of gastric contents into the upper aero digestive tract leading to throat symptoms. World over, the prevalence rate of LPRD, ranges from 5 to 30%. The aim of this study was to find the prevalence rate of LPRD in Indian population. This was an observational study whereby the RSI questionnaire was circulated amongst the population and records collected. All subjects who had RSI score more than 13 were considered to be suffering from LPRD. 2300 responses were collected from almost all strata of population. Out of 2300 people who responded 253 had RSI score > 13, and were considered as suffering from LPRD. Thus the prevalence rate of LPRD in population was 11%. The prevalence rate of LPRD in females was 11.2% and in males was 10.6%. The difference in prevalence among both the genders was not significant.The most common symptom of LPR reported by subjects was heartburn followed by clearing of throat and excess throat mucous. The prevalence of LPRD in Indian population as assessed by RSI score > 13 was 11%. The prevalence is same in males and females.
Keywords: LPRD, Prevalence, RSI, Reflux laryngitis
Introduction
Laryngopharyngeal Reflux Disease (LPRD) is due to the backflow of gastric contents into the upper aerodigestive tract leading to throat symptoms [1].
It is a form of extra-oesophageal reflux (EOR). Usually occurs in upright position and is mainly due to reflux of gaseous gastric contents, containing fine droplets [2]. Tissue damage in LPRD is quicker as there are no mechanisms to physically remove or chemically neutralize the acid.
LPRD is clinically diagnosed by history taking and laryngoscopic examination. Common presenting symptoms include dysphonia, swallowing difficulty, cough, frequent throat clearing, sore throat, thick mucus in throat and feeling of lump in throat [1].
If it remains undiagnosed it can lead to various chronic laryngeal conditions like subglottic stenosis, laryngeal carcinoma, granulomas, contact ulcers and vocal nodules [3].
Sedentary lifestyle, tobacco, alcohol has been an important risk factor for this disease [4].
High variability is present world over for the prevalence of LPRD, which ranges between 7.1% [4] to 30% [5, 6]. Studies have even reported prevalence to be 64% in people above age of 40 years [7] and around 50% in patients with laryngeal and voice disorder [8]
Reports suggest that up to 10% of patients presenting to an otolaryngologist’s office may be suffering from LPRD [9].
In 2002, Belafsky et al. developed the Reflux Symptom Index (RSI), a self-administered nine-item questionnaire, designed to assess various symptoms related to LPR. RSI ≥ 13 was considered abnormal and strongly indicative of LPR [10].
Literature does say that RSI scoring have the same value in diagnosing LPRD as that of pH monitoring.[11]. RSI scoring system is simple reliable questionnaire good for population screening.
Indian data is not available about prevalence of LPRD and this study primarily aims to find the same using the RSI score. This will also help to know the burden of LPR disease in Indian population.
Materials and Methods
This observational study was done over six months at a tertiary care center in India.
A questionnaire was prepared. Before the start of questionnaire there was a consent form. This consent described the name, institute and contact details of principle investigator, purpose of study and assured confidentiality of personal data.
The main questionnaire consisted of the RSI questions, to gather data about LPR symptoms and along with this, there were questions related to age, sex and profession to have basic demographic data.
The RSI consists of 9 questions. Each symptom scored by the subject themselves, from 0 to 5 based on severity, with a maximum score of 45. Those with a score of 13 or more are considered to be suffering from LPRD.[Table 1] [10]
Table 1.
Reflux Symptom Index (RSI) according to Belfasky et al.
| Within the last MONTH, how did the following problems affect you ? | |||||||
| 0 = no problem, 5 = severe problem | |||||||
| 1 | Hoarseness or a problem with your voice | 0 | 1 | 2 | 3 | 4 | 5 |
| 2 | Clearing your throat | 0 | 1 | 2 | 3 | 4 | 5 |
| 3 | Excess throat mucous or postnasal drip | 0 | 1 | 2 | 3 | 4 | 5 |
| 4 | Difficulty swallowing food, liquids, or pills | 0 | 1 | 2 | 3 | 4 | 5 |
| 5 | Coughing after you ate or after lying down | 0 | 1 | 2 | 3 | 4 | 5 |
| 6 | Breathing difficulties or choking episodes | 0 | 1 | 2 | 3 | 4 | 5 |
| 7 | Troublesome or annoying cough | 0 | 1 | 2 | 3 | 4 | 5 |
| 8 | Sensations of something sticking in your throat or a lump in your throat | 0 | 1 | 2 | 3 | 4 | 5 |
| 9 | Heartburn, chest pain, indigestion, or stomach acid coming up | 0 | 1 | 2 | 3 | 4 | 5 |
| Total | |||||||
The study protocol was approved by institutional ethical committee. The idea was to circulate this questionnaire to as many individuals as possible and try to analyze the data. Children less than 16 years of age were not included in the study. Besides this all willing subjects were included in the study.
This questionnaire was circulated as Google forms on various Indian social media platforms. Responses were also collected on hard copy randomly from relatives coming to this tertiary care hospital. Besides responses were also collected by interns, from villages during community trips, A wide publicity and effort was given to get maximum responses. After the mammoth effort 2300 responses were collected from almost all strata of population.
The data collected was compiled in excel sheet and then was analyzed
Results
The questionnaire was given a wide publicity and after all the effort, data was received from 2420. After screening the data 2300 were found to have all the desired information and were included for the purpose of analysis.
Of 2300 respondents, 1242 were females and 1058 were males. (Fig. 1)
Fig. 1.
Gender distribution of subjects who responded to questionnaire
The subjects were well distributed across all age group. Majority of subjects were in the age group 21–30 ( 42%), followed by 31–40 ( 19%) and the rest data of responders as between 12 and 14% across all age groups as per Fig. 2.
Fig. 2.
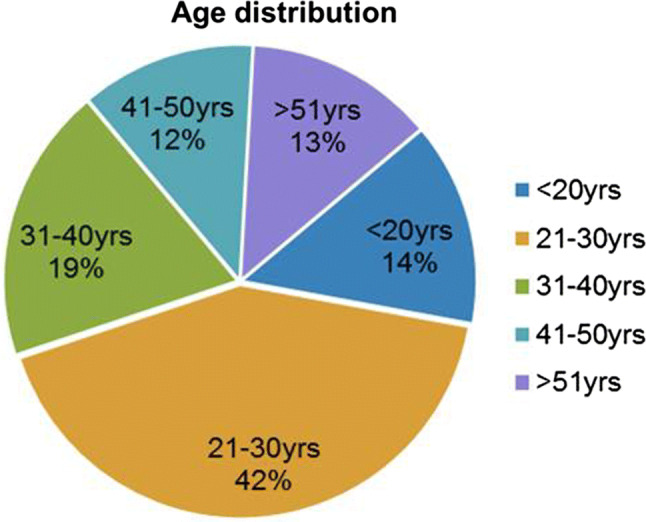
Age distribution of subjects who responded to questionnaire
Prevalence Data
Out of 2300 people who responded 253 had RSI score > 13, and were considered as suffering from LPRD, as compared to 2047 who had RSI score < 13 were without LPRD. Thus the prevalence rate of LPRD in population was 11%. (Fig. 3). Out of total positive patients of LPRD, 55% (139) of these were females, whereas 45% (114) were males. The prevalence rate of LPRD in females was 11.2% and in males was 10.6%. Thus the difference in prevalence among both the genders was not significant. (P value was > 0.05 using t test).
Fig. 3.
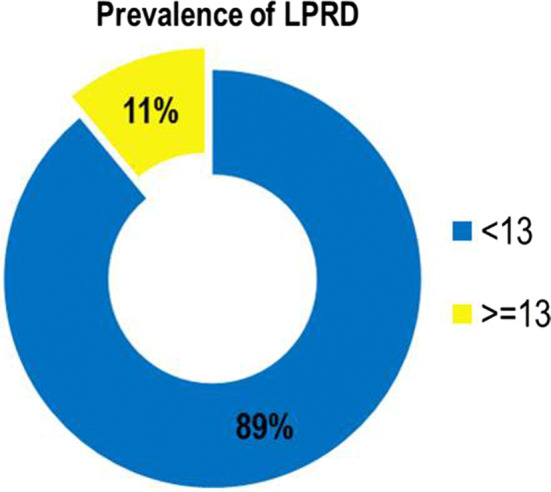
Prevalence of LPRD in Indian population
On further analysis regarding the major symptoms of LPRD patients, it was found that majority of patients had heart burn, repeated throat clearing post nasal drip and sensation of something stuck in throat were seen. The details are as per Table 2.
Table 2.
Frequency of symptoms reported by LPRD patients
| Sr. No | Symptoms | No. of patients | Percentage |
|---|---|---|---|
| 1 | Heartburn, chest pain, indigestion, or stomach acid coming up | 95 | 38 |
| 2 | Clearing your throat | 82 | 33 |
| 3 | Excess throat mucous or postnasal drip | 71 | 28 |
| 4 | Sensations of something sticking in your throat or a lump in your throat | 57 | 23 |
| 5 | Coughing after you ate or after lying down | 56 | 22 |
| 6 | Troublesome or annoying cough | 56 | 22 |
| 7 | Hoarseness or a problem with your voice | 48 | 19 |
| 8 | Breathing difficulties or choking episodes | 43 | 17 |
| 9 | Difficulty swallowing food, liquids, or pills | 36 | 14 |
Discussion
Laryngopharyngeal reflux (LPR) is defined as the retrograde flow of stomach content to the larynx and pharynx whereby this material comes in contact with the upper aero-digestive tract [1]. Literature search gives a very variable prevalence of LPRD world over, ranging from 5% in China as per Chen XM et al. [12], 7.1% as per Sone M et al. [4], 18.8 in Greek population as per Spantideas et al. [6] and up to 30% in English population study by Kamani et al. [5].
The most common symptoms of LPR are excessive throat clearing, coughing, hoarseness, and globus pharyngeus (“lump in the throat sensation”) [13]. These are common symptoms with which patients regularly present to ENT OPD and it becomes essential to diagnose LPRD. Besides according to El-Serag, the prevalence of reflux diseases has increased by 4% every year since 1976 [14]. A Study by Altman et al. reports that, between 1990 and 2001, the LPR visits to ENT OPD has increased by 500% [15].
Considering the common symptoms it does become difficult to know the prevalence of LPR in the general population since the suggested gold standard of 24 h pHmetry is not available for large scale epidemiological studies [6, 9]. At the same time it is also essential not to miss out diagnosis as besides the typical symptoms of LPR that affect the quality of life, studies have shown LPR as a possible risk factor for laryngitis, subglottic stenosis,, granulomas, contact ulcers, vocal nodules and even laryngeal carcinoma [9, 16, 17].
Knowing this it was essential to know the exact prevalence of LPRD in Indian population and thus the burden of this disease.
In present study out of 2300 subjects who answered the questionnaire 253 had LPRd based on RSI score > 13. Thus the prevalence rate of LPR in Indian population is 11%. This means almost 1 in every 10 adult in India is suffering from LPR. No significant difference was observed between males and females in the prevalence of LPR.
The rates in present study are in between the prevalence rates in different studies as quoted above.
The difference in prevalence rate world over definitely will vary knowing the fact that LPR is mainly a quality of life disease [18]. All the prevalence studies have used RSI score to find patients with LPRD thus the results are well comparable. Study by Kamini et al. [5] on English population had taken RSI score more than 10 as positive for LPRD and this might have led to higher prevalence rate of 30% in their study. Study by Spantideas et al. on Greek population who got a prevalence rate of 18.8% also had no difference in prevalence between male and females [6], however they had derived the data from 340 subjects whereas in present study its derived form 2300 subjects.
In present study the most common symptom of LPR reported by subjects was heartburn followed by excessive clearing your throat and excess throat mucous which was similar to various other studies.
Literature search till date did not reveal any Indian study showing the prevalence of LPRD thus the design and finding of this study becomes important. A possible limitation of this study can be not using the 24Hr PH metry for diagnosis of LPRD, however using ph metry for epidemiological study may not be feasible at present considering invasive nature of the test and studies does show that diagnosis by RSI and ph metry are comparable [11].
Conclusion
The prevalence of LPRD in Indian population as assessed by RSI score > 13 was 11%. The prevalence is same in males and females. Most common reported symptom was heart burn, clearing of throat, mucus in throat. Thus with prevalence LPRD being that of more than 1 in every 10 person makes this a disease very important and it needs to be understood and treated well not only by ENT surgeons but equally well by family physicians.
Compliance with Ethical standards
Conflict of interest
The authors declare that they have no conflict of interest
Institutional Ethical Clearance
Obtained
Consent
Taken from all before filling questionnaire
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Prasun Mishra, Email: entprasun@gmail.com.
Deeksha Agrawal, Email: 48deeksha@gmail.com.
Kartikeya Chauhan, Email: c.kartikeya@gmail.com.
Maitri Kaushik, Email: tre.kaushik@gmail.com.
References
- 1.Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery. Otolaryngol Head Neck Surg. 2002;127(1):32–35. doi: 10.1067/mhn.2002.125760. [DOI] [PubMed] [Google Scholar]
- 2.Wiener GJ, Tsukashima R, Kelly C, et al. Oropharyngeal pH monitoring for the detection of liquid and aerosolized supraoesophageal gastric reflux. J Voice. 2009;23(4):498–504. doi: 10.1016/j.jvoice.2007.12.005. [DOI] [PubMed] [Google Scholar]
- 3.Campagnolo AM, Priston J, Thoen RH, Medeiros T, Assunção AR. Laryngopharyngeal reflux: diagnosis, treatment, and latest research. Int Arch Otorhinolaryngol. 2014;18(2):184–191. doi: 10.1055/s-0033-1352504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sone M, Katayama N, Kato T, Izawa K, Wada M, Hamajima N, et al. Prevalence of laryngopharyngeal reflux symptoms: comparison between health checkup examinees and patients with otitis media. Otolaryng Head Neck Surg. 2012;146:562–566. doi: 10.1177/0194599811434049. [DOI] [PubMed] [Google Scholar]
- 5.Kamani T, Penney S, Mitra I, Pothula V. The prevalence of laryngopharyngeal reflux in the English population. Eur Arch Otorhinolaryngol. 2012;269(10):2219–2225. doi: 10.1007/s00405-012-2028-1. [DOI] [PubMed] [Google Scholar]
- 6.Spantideas N, Drosou E, Bougea A, et al. Laryngopharyngeal reflux disease in the Greek general population, prevalence and risk factors. BMC Ear Nose Throat Disord. 2015;15:7. doi: 10.1186/s12901-015-0020-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Reulbach TR, Belafsky PC, Blalock PD, Koufman JA, Postma GN. Occult laryngeal pathology in a community-based cohort. Otolaryngol Head Neck Surg. 2001;124:448–450. doi: 10.1067/mhn.2001.114256. [DOI] [PubMed] [Google Scholar]
- 8.Koufman JA, Amin MR, Panetti M. Prevalence of reflux in 113 consecutive patients with laryngeal and voice disorders. Otolaryngol Head Neck Surg. 2000;123(4):385–388. doi: 10.1067/mhn.2000.109935. [DOI] [PubMed] [Google Scholar]
- 9.Kοufman JA. The Otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24 h pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope. 1991;101(Suppl 52):1–78. doi: 10.1002/lary.1991.101.s53.1. [DOI] [PubMed] [Google Scholar]
- 10.Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the reflux finding score (RFS) The laryngoscope. 2001;111(8):1313–1317. doi: 10.1097/00005537-200108000-00001. [DOI] [PubMed] [Google Scholar]
- 11.Feng GJ, Zhang LH, Zhao LL, Liu YL. A pilot study on diagnosing laryngopharyngeal reflux disease by pH monitoring in laryngopharynx. Zhonghua Yi Xue Za Zhi. 2008;88(12):805–808. [PubMed] [Google Scholar]
- 12.Chen XM, Li Y, Guo WL, Wang WT, Lu M. Prevalence of laryngopharyngeal reflux disease in Fuzhou region of China. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2016;51(12):909–913. doi: 10.3760/cma.j.issn.1673-0860.2016.12.006. [DOI] [PubMed] [Google Scholar]
- 13.Ford CN. Review evaluation and management of laryngopharyngeal reflux. JAMA. 2005;294(12):1534–1540. doi: 10.1001/jama.294.12.1534. [DOI] [PubMed] [Google Scholar]
- 14.El-Serag HB. Review time trends of gastroesophageal reflux disease: a systematic review. Clin Gastroenterol Hepatol. 2007;5(1):17–26. doi: 10.1016/j.cgh.2006.09.016. [DOI] [PubMed] [Google Scholar]
- 15.Altman KW, Stephens RM, Lyttle CS. Weiss KB changing impact of gastroesophageal reflux in medical and otolaryngology practice. Laryngoscope. 2005;115(7):1145–1153. doi: 10.1097/01.MLG.0000165464.75164.E5. [DOI] [PubMed] [Google Scholar]
- 16.Tae K, Jin BJ, Ji YB, Jeong JH, Cho SH, Lee SH. The role of laryngopharyngeal reflux as a risk factor in laryngeal cancer: a preliminary report. Clin Exp Otorhinolaryngol. 2011;4(2):101–104. doi: 10.3342/ceo.2011.4.2.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tan JJ, Wang L, Mo TT, Wang J, Wang MG, Li XP. Pepsin promotes IL-8 signaling-induced epithelial-mesenchymal transition in laryngeal carcinoma. Cancer Cell Int. 2019;19:64. doi: 10.1186/s12935-019-0772-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kesari SP, Chakraborty S. Sharma B evaluation of risk factors for Laryngopharyngeal reflux among sikkimese population. Kathmandu Univ Med J. 2017;15(57):29–34. [PubMed] [Google Scholar]