

Abstract
There are many evidences showing diethylcarbamazine as a potential drug for the treatment of allergic rhinitis. This study evaluated the effectiveness of diethylcarbamazine in the treatment of allergic rhinitis and compared it with montelukast and levocetirizine. This parallel double-blind randomized clinical trial was done in allergic rhinitis patients. Seven hundred and twelve participants who met the inclusion criteria and provided informed written consent were randomized and divided into 2 equal groups. Diethylcarbamazine 300 mg/day orally in divided doses was given to group A, and montelukast 10 mg and levocetirizine 5 mg/day orally at night for 21 days was given to group B. Primary outcomes were the change in symptoms, absolute eosinophil count, serum total IgE, phadiatop and response in skin prick from baseline to 21 days and 3 months after treatment. Secondary outcome was to compare it with montelukast and levocetirizine. The mean (SD) age of the patients was 33 (10.6) years, with 374 (52.5%) males and 338 (47.5%) females. There was statistically significant improvement in all the parameters in both groups. Improvement was better with diethylcarbamazine compared to montelukast and levocetirizine and the effects were sustained for 3 months in diethylcarbamazine group. The findings suggest that diethylcarbamazine is effective in the treatment of allergic rhinitis. It gives better control and is cost-effective than montelukast and levocetirizine.
Trial Registration: https://www.ctri.nic.in Identifier: CTRI/2020/03/024145 registered on 20-03-2020.
Keywords: Allergic rhinitis, Allergens, Inhalation allergen challenge, Skin prick test, Therapeutics
Introduction
Allergic rhinitis is one of the most common but underdiagnosed disease of the nasal mucosa worldwide which persists throughout life. It is present in 0.8 and 39.7% of the world population (depending on location). It is characterised by symptoms like sneezing, itching, rhinorrhoea and nasal congestion [1]. It is mediated by early and late hypersensitivity responses and IgE mediated activation of mast cells in the nasal mucosa. This leads to mediator release and acute inflammatory reaction. T helper-2 cells and eosinophils also contribute to the pathology. Interleukin-17 and interleukin-33 also play a role in the inflammatory and immune response to allergen [2–4].
Allergic rhinitis is diagnosed based on history, nasal symptoms, nasal examination, and investigations like skin prick test and serum total and specific IgE according to BSACI guidelines [5]. Eosinophil count can be taken to monitor the response to treatment in allergic rhinitis [6–8]. There are many oral drugs and topical nasal medication to treat allergic rhinitis. Oral drugs like leukotriene receptor antagonists act on leukotriene pathway of allergic response [9]. Oral corticosteroids cannot be used continuously because of its side effects and topical corticosteroids have local effects like nasal irritation and dryness which leads to poor patient compliance [10, 11]. Allergen immunotherapy for allergic rhinitis gives excellent results but it is not cost-effective, needs long duration treatment, careful patient selection and lacks patient compliance [12–16].
Diethylcarbamazine is a commonly used anti-filarial drug. It has many other pharmacological actions. It is a potent leukotriene inhibitor. Leukotrienes have an important role in mechanism of asthma and allergic rhinitis [17]. Diethylcarbamazine also decreases the eosinophil synthesis in bone marrow and decreases its number in spleen which results in reduced response to allergen [18]. Diethylcarbamazine can be a cheaper and more potent alternative to the known drugs for allergic rhinitis. This study compares the effect of therapy with monteleukast plus levocetirizine and diethylcarbamazine in the symptoms, skin prick test, serum IgE and eosinophil count in allergic rhinitis patients.
Methods
Trial Design and Participants
This double blind randomised controlled trial evaluated the efficacy and safety of treatment with diethylcarbamazine in patients with allergic rhinitis. Trial protocol was approved by the institutional ethical committee (IEC Ref. No: KIMS/PG/2019/42) and the study was registered in clinical trials registry India (CTRI/2020/03/024,145). Patients above 18 years and below 60 years were included in the study. Patients with symptoms of allergic rhinitis, increased absolute eosinophil count and serum total IgE and positive skin prick test were included in the study. Patients with any other form of rhinitis, deviated septum, pregnancy, asthma, any lung pathology, mass or tumour of nose or para nasal sinuses and patients already taking any oral or nasal corticosteroids or any other anti-allergic medication were excluded from the study. Patients with any other medical disorder, renal or hepatic disorder or any other chronic illness were also excluded from the study.
Recruitment
Patients coming to ENT OPD in our institution, which is an academic tertiary care institution with symptoms of allergic rhinitis were screened and eligible participants were recruited. This study was done during the period of March 20–September 20, 2020. Informed written consent was obtained from all patients after explaining the study. After that, participants were randomized and treatment initiated within 2–3 days.
Randomization and Blinding
Patients were randomized using computer generated random numbers with 1:1 random allocation ratio. Participants and researchers were blind to the group in which the patient was allotted to avoid bias. Only the staff nurse who allotted the participant was aware of the group allocation.
Interventions
Sample size was calculated by a pilot study. Total 712 patients were recruited with 356 patients in each group. Patients were assigned to one of two treatment groups: diethylcarbamazine group (group A), or montelukast and levocetirizine group (group B). Patients in group A (n = 356) received oral tablet diethylcarbamazine 100 mg, thrice daily for 21 days and those in group B (n = 356) received oral tablet montelukast 10 mg and levocetirizine 5 mg, once daily for 21 days.
Outcomes and Measures
Before randomization, patients baseline demographic details, symptoms by Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) [19], absolute eosinophil count, serum total IgE, phadiatop and skin prick test were noted in a proforma. Patients were evaluated by RQLQ for sleep trouble, non-hay fever symptoms, practical problems, nasal symptoms, eye symptoms, activities and emotional trouble. It had 28 questions related to these problems which was scaled from 0 to 6. Absolute eosinophil count was assessed for all participants. Serum total IgE was assessed by electrochemiluminescence immunoassay using cobas e immunoassay analyser by sandwich principle. Serum was collected from the patient using standard sampling tubes. After the reaction with reagent IGE II, results were determined by measuring the chemiluminescent emission by a photomultiplier. Patients with values more than 100 IU/mL were included.
Skin prick test for house dust, Aspergillus fumigatus, pollen and Parthenium hysterophorus were done. A drop of allergen extract was placed on the volar aspect of the forearm 3 cm from the wrist. Location of each allergen was marked with a pen. Distance of 2 cm was maintained between 2 allergens to avoid false-positive reaction from nearby allergen. A metal lancet with single head was used to press through the allergen extract into the epithelial layer and held for one second. Separate lancet was used for each allergen to prevent cross contamination. Histamine dihydrochloride 0.1% was used as positive control and the diluent was used as negative control. The results were measured after 20 min. Positive and negative controls were measured. The largest diameter of wheal of each allergen test was measured. Size ≥ 3 mm was taken as positive result.
Presence of allergen specific IgE was confirmed by Phadiatop. It uses ImmunoCAP fluorescent-enzyme immunosorbent assay (FEIA) technology. Value more than 0.35 was taken as positive. Assessments were done at baseline before starting treatment, on completion of treatment at 21 days and after 3 months. The primary outcome was to see the change in the symptoms and other parameters in group A after treatment, so the efficacy of diethycarbamazine is known. The secondary outcome was to compare the change in parameters after treatment in both groups to find how diethylcarbamazine compares with the standard treatment.
Statistical Analysis
Statistical analysis was done using IBM SPSS Statistics for Windows, Version 20.0., IBM Corp., Chicago, IL. Demographic data were analysed by descriptive statistics. Descriptive statistics were reported as mean (SD) for continuous variables, frequencies (percentage) for categorical variables. Symptom score, absolute eosinophil count, serum total IgE, phadiatop and skin prick test before and after treatment were analysed. Student t test was used. p value less than 0.05 was taken as significant.
Results
Study Recruitment
Participant recruitment is presented in CONSORT diagram in Fig. 1. A total of 974 individuals with symptoms of allergic rhinitis were registered for screening. 216 (22.2%) did not meet inclusion criteria and 46 (4.7%) did not give consent and were excluded. A total of 712 patients with allergic rhinitis were included in the study.
Fig. 1.
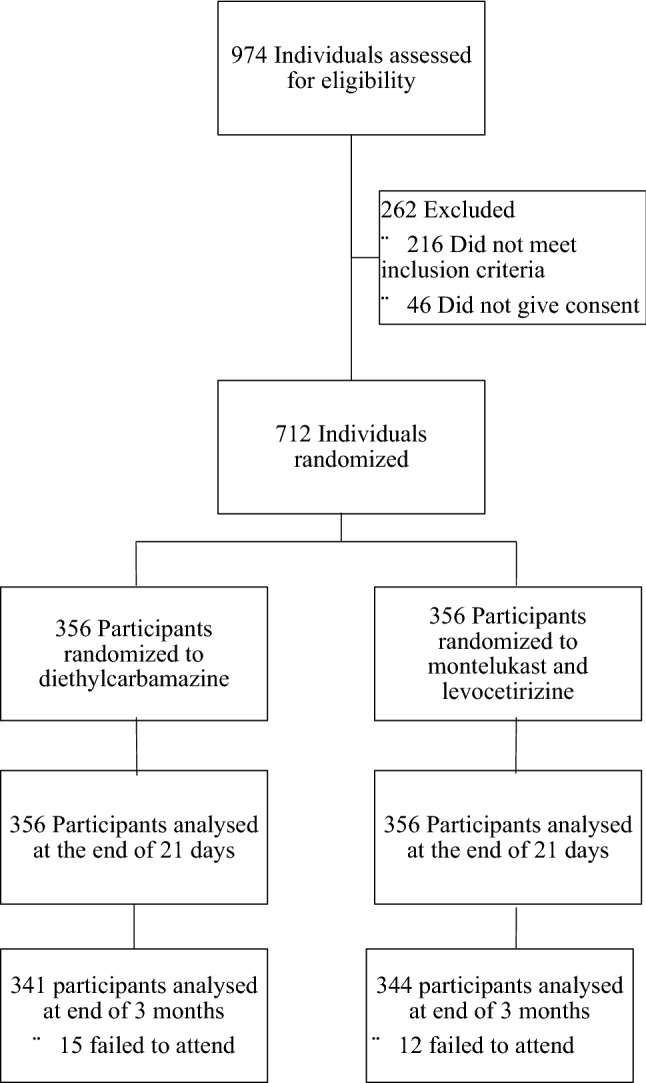
CONSORT flow diagram. Consolidated standards of reporting trials showing the number of participants initially assessed, enrolled and followed up for 21 days and 3 months
Demographic Baseline Characteristics
The mean (SD) age of the patients was 33 (10.6) years, with 374 (52.5%) males and 338 (47.5%) females. They were divided into 2 groups. Diethylcarbamazine group (group A) had 356 patients with mean (SD) age 32.1 (11.2) years, with 163 (45.8%) males and 193 (54.2%) females. Montelukast and levocetirizine group (group B) had 356 patients with mean (SD) age 33.9 (9.94), with 211 (59.3%) males and 145 (40.7%) females. The demographic characteristics are summarised in Table 1.
Table 1.
Demographic baseline characteristic of 712 patients
| Characteristic | Group A | Group B | Total |
|---|---|---|---|
| Age (mean ± SD) | 32.1 ± 11.2 | 33.9 ± 9.9 | 33 ± 10.6 |
| Sex, male/female | 163/193 | 211/145 | 374/338 |
| Sleep trouble (mean ± SD) | 2.74 ± 1.66 | 1.83 ± 1.33 | 2.29 ± 1.57 |
| Non-hayfever symptoms (mean ± SD) | 2.05 ± 1.59 | 1.71 ± 1.01 | 1.88 ± 1.34 |
| Practical problems (mean ± SD) | 3.6 ± 1.72 | 3.61 ± 1.61 | 3.61 ± 1.67 |
| Nasal symptoms (mean ± SD) | 4.39 ± 1.64 | 3.79 ± 1.88 | 4.09 ± 1.79 |
| Eye symptoms (mean ± SD) | 2.63 ± 1.07 | 2.78 ± 1.68 | 2.71 ± 1.41 |
| Activities trouble (mean ± SD) | 3.4 ± 1.54 | 3.76 ± 2.32 | 3.58 ± 1.98 |
| Emotional trouble (mean ± SD) | 2.91 ± 1.65 | 2.62 ± .26 | 2.76 ± 1.48 |
| RQLQ (mean ± SD) | 21.73 ± 4.65 | 20.12 ± 5.14 | 20.92 ± 4.97 |
| AEC (mean ± SD) | 1073.2 ± 657.46 | 1058.49 ± 532.29 | 1065.9 ± 597.78 |
| Serum total IgE (mean ± SD) | 804.73 ± 933.17 | 709.36 ± 741.22 | 757.04 ± 843.43 |
| SPT-House dust (mean ± SD) | 0.86 ± 0.34 | 0.74 ± 0.44 | 0.80 ± 0.40 |
| SPT-Aspergillus | 0.52 ± 0.5 | 0.60 ± 0.49 | 0.56 ± 0.50 |
| SPT-Pollen | 0.66 ± 0.47 | 0.65 ± 0.47 | 0.66 ± 0.47 |
| SPT-Parthenium | 0.64 ± 0.47 | 0.54 ± 0.5 | 0.59 ± 0.49 |
| Phadiatop | 3.73 ± 2.84 | 4.1 ± 3.3 | 3.92 ± 3.08 |
RQLQ, rhinoconjunctivitis quality of life questioner, AEC absolute eosinophil count, SPT skin prick test, Group A, diethyl carbamazine; Group B, montelukast and levocetirizine
RQLQ
All the parameters of RQLQ were statistically decreased in both the groups post 21 days treatment (Table 2). Patients reported better reduction in sleep trouble (p < 0.001), non-hay fever symptoms (p < 0.001), practical problems (p < 0.001), nasal symptoms (p < 0.001), eye symptoms (p < 0.001), activities trouble (p < 0.001) and emotional trouble (p < 0.001) in group A compared to group B (Table 2). Three months after treatment, all parameters of RQLQ were statistically decreased in diethylcarbamazine group compared to the baseline (p < 0.001) and in montelukast and levocetirizine group, improvement was seen in some patients while it worsened or became similar to baseline in some. Overall there was no statistically significant improvement (Table 3).
Table 2.
RQLQ before and 21 days after treatment
| RQLQ | Group | Baseline before treatment | 21 days after treatment | Difference | 95% CI | p value |
|---|---|---|---|---|---|---|
| Sleep trouble | Group A | 2.74 ± 1.66 | 0.7 ± 0.77 | 2 | 1.9–2.2 | < 0.001 |
| Group B | 1.83 ± 1.33 | 0.84 ± 0.7 | 0.99 | 0.89–1.09 | < 0.001 | |
| Non hayfever symptoms | Group A | 2.05 ± 1.59 | 0.58 ± 1.01 | 1.47 | 1.34–1.6 | < 0.001 |
| Group B | 1.71 ± 1.01 | 0.95 ± 0.77 | 0.76 | 0.69–0.84 | < 0.001 | |
| Practical problems | Group A | 3.6 ± 1.72 | 1.03 ± 0.78 | 2.57 | 2.41–2.73 | < 0.001 |
| Group B | 3.61 ± 1.61 | 1.47 ± 0.93 | 2.15 | 1.98–2.32 | < 0.001 | |
| Nasal symptoms | Group A | 4.39 ± 1.64 | 1.36 ± 0.88 | 3.02 | 2.87–3.18 | < 0.001 |
| Group B | 3.79 ± 1.88 | 1.64 ± 0.99 | 2.15 | 1.94–2.37 | < 0.001 | |
| Eye symptoms | Group A | 2.63 ± 1.07 | 0.41 ± 0.59 | 2.22 | 2.1–2.34 | < 0.001 |
| Group B | 2.78 ± 1.68 | 1.45 ± 1.17 | 1.34 | 1.23–1.44 | < 0.001 | |
| Activities trouble | Group A | 3.4 ± 1.54 | 0.76 ± 0.71 | 2.63 | 2.48–2.78 | < 0.001 |
| Group B | 3.76 ± 2.32 | 1.81 ± 1.59 | 1.95 | 1.81–2.08 | < 0.001 | |
| Emotional trouble | Group A | 2.91 ± 1.65 | 0.46 ± 0.68 | 2.45 | 2.29–2.61 | < 0.001 |
| Group B | 2.62 ± .26 | 1.15 ± 1.02 | 1.47 | 1.33–1.61 | < 0.001 | |
| RQLQ | Group A | 21.73 ± 4.65 | 5.31 ± 2.23 | 16.42 | 16.03–16.81 | < 0.001 |
| Group B | 20.12 ± 5.14 | 9.03 ± 3.28 | 10.81 | 10.45–11.17 | < 0.001 |
RQLQ, rhinoconjunctivitis quality of life questioner; Group A, diethyl carbamazine; Group B, montelukast and levocetirizine
Table 3.
RQLQ before and 3 months after treatment
| RQLQ | Group | Baseline before treatment | 3 months after treatment | Difference | 95% CI | p value |
|---|---|---|---|---|---|---|
| Sleep trouble | Group A | 2.71 ± 1.67 | 0.77 ± 0.7 | 1.94 | 1.8–2.08 | < 0.001 |
| Group B | 1.85 ± 1.33 | 1.73 ± 1.33 | 0.12 | 0.00–0.25 | 0.07 | |
| Non hayfever symptoms | Group A | 2.05 ± 1.6 | 0.69 ± 1.04 | 1.36 | 1.22–1.5 | < 0.001 |
| Group B | 1.71 ± 1 | 1.67 ± 1.05 | 0.03 | − 0.03–0.1 | 0.32 | |
| Practical problems | Group A | 3.61 ± 1.72 | 1.19 ± 1 | 2.43 | 2.25–2.6 | < 0.001 |
| Group B | 3.62 ± 1.62 | 3.53 ± 1.57 | 0.09 | − 0.04–0.21 | 0.16 | |
| Nasal symptoms | Group A | 4.38 ± 1.63 | 1.56 ± 0.81 | 2.82 | 2.68–2.96 | < 0.001 |
| Group B | 3.8 ± 1.86 | 3.7 ± 1.88 | 0.1 | − 0.05–0.23 | 0.19 | |
| Eye symptoms | Group A | 2.63 ± 1.07 | 0.45 ± 0.5 | 2.19 | 2.08–2.3 | < 0.001 |
| Group B | 2.8 ± 1.7 | 2.69 ± 1.59 | 0.12 | − 0.01–0.24 | 0.06 | |
| Activities trouble | Group A | 3.38 ± 1.53 | 0.65 ± 0.58 | 2.73 | 2.58–2.88 | < 0.001 |
| Group B | 3.77 ± 2.35 | 3.64 ± 2.34 | 0.13 | − 0.02–0.28 | 0.08 | |
| Emotional trouble | Group A | 2.93 ± 1.66 | 0.73 ± 1.27 | 2.2 | 2.02–2.38 | < 0.001 |
| Group B | 2.62 ± 1.27 | 2.51 ± 1.46 | 0.1 | − 0.04–0.25 | 0.16 | |
| RQLQ | Group A | 21.69 ± 4.58 | 6.03 ± 1.82 | 15.66 | 15.26–16.07 | < 0.001 |
| Group B | 20.17 ± 5.13 | 19.78 ± 5.57 | 0.38 | − 0.02–0.78 | 0.06 |
RQLQ, rhinoconjunctivitis quality of life questioner; Group A, diethyl carbamazine; Group B, montelukast and levocetirizine
Skin Prick Test
Skin prick test showed statistically significant decreased reaction after completion of 21 days treatment in both groups. It is summarized in Table 4. Difference in group A for house dust allergen skin prick test (77.9% difference; 95% CI, 0.62–0.71; p < 0.001) was better than group B (47.3% difference; 95% CI, 0.3– 0.4; p < 0.001), and it was statistically significant (p < 0.001). Difference in group A for aspergillus allergen skin prick test (78.8% difference; 95% CI, 0.36–0.46; p < 0.001) was better than group B (48.3% difference, 95% CI, 0.25–0.34; p < 0.001), and it was statistically significant (p < 0.001). Difference in group A for pollen allergen skin prick test (76.9% difference; 95% CI, 0.45–0.56; p < 0.001) was better than group B (45.4% difference, 95% CI, 0.25–0.34; p < 0.001), and it was statistically significant (p < 0.001). Difference in group A for Parthenium allergen skin prick test (73.3% difference; 95% CI, 0.42–0.52; p < 0.001) was better than group B (40.7% difference, 95% CI, 0.18–0.26; p < 0.001), and it was statistically significant (p < 0.001). Three months after treatment, skin prick test in group A showed statistically significant decreased response for all the allergens tested (p < 0.001). Group B showed similar response to baseline. It is summarized in Table 5.
Table 4.
Investigations before and 21 days after treatment
| Group | Baseline before treatment | 21 days after treatment | Difference | 95% CI | p value | |
|---|---|---|---|---|---|---|
| AEC | Group A | 1073.2 ± 657.46 | 391.84 ± 258.54 | 681.38 | 635.74–727.03 | < 0.001 |
| Group B | 1058.49 ± 532.29 | 810.11 ± 332.16 | 248.38 | 224.74–272.01 | < 0.001 | |
| STIgE | Group A | 804.73 ± 933.17 | 134.43 ± 97.95 | 670.3 | 582.23–758.36 | < 0.001 |
| Group B | 709.36 ± 741.22 | 434.55 ± 492.03 | 274.8 | 246.11–303.5 | < 0.001 | |
| SPT HD | Group A | 0.86 ± 0.34 | 0.2 ± 0.4 | 0.67 | 0.62–0.71 | < 0.001 |
| Group B | 0.74 ± 0.44 | 0.39 ± 0.49 | 0.35 | 0.3–0.4 | < 0.001 | |
| SPT ASPER | Group A | 0.52 ± 0.5 | 0.11 ± 0.31 | 0.41 | 0.36–0.46 | < 0.001 |
| Group B | 0.60 ± 0.49 | 0.3 ± 0.46 | 0.29 | 0.25–0.34 | < 0.001 | |
| SPT POLLEN | Group A | 0.65 ± 0.47 | 0.16 ± 0.36 | 0.5 | 0.45–0.56 | < 0.001 |
| Group B | 0.66 ± 0.47 | 0.36 ± 0.48 | 0.3 | 0.25–0.34 | < 0.001 | |
| SPT PART | Group A | 0.64 ± 0.47 | 0.18 ± 0.38 | 0.47 | 0.42–0.52 | < 0.001 |
| Group B | 0.54 ± 0.5 | 0.32 ± 0.47 | 0.22 | 0.18–0.26 | < 0.001 | |
| Phadiatop | Group A | 3.73 ± 2.84 | 0.37 ± 0.33 | 3.37 | 3.1–3.64 | < 0.001 |
| Group B | 4.1 ± 3.3 | 2.23 ± 2.03 | 1.87 | 1.72–2.02 | < 0.001 |
AEC absolute eosinophil count, STIgE serum total immunoglobulin E, SPT HD skin prick test for house dust, SPT ASPER skin prick test for aspergillosis, SPT POLLEN skin prick test for pollen, SPT PART skin prick test for parthenium, Group A: diethyl carbamazine, Group B: montelukast and levocetirizine
Table 5.
Investigations before and 3 months after treatment
| Group | Baseline before treatment | 3 months after treatment | Difference | 95% CI | p value | |
|---|---|---|---|---|---|---|
| AEC | Group A | 1074.26 ± 661.84 | 360.89 ± 201.23 | 713.38 | 659.74–767.01 | < 0.001 |
| Group B | 1060.8 ± 531.49 | 1049.82 ± 490.09 | 10.98 | − 1.31 ± 23.27 | 0.08 | |
| STIgE | Group A | 820.03 ± 947.62 | 179.41 ± 117.67 | 640.62 | 548.67–732.57 | < 0.001 |
| Group B | 711.75 ± 743.04 | 703.54 ± 694.55 | 8.21 | − 6.29–22.70 | 0.27 | |
| SPT HD | Group A | 0.87 ± 0.34 | 0.31 ± 0.46 | 0.55 | 0.5–0.6 | < 0.001 |
| Group B | 0.74 ± 0.44 | 0.7 ± 0.46 | 0.04 | − 0.01–0.08 | 0.1 | |
| SPT ASPER | Group A | 0.51 ± 0.5 | 0.21 ± 0.41 | 0.3 | 0.25–0.35 | < 0.001 |
| Group B | 0.60 ± 0.49 | 0.57 ± 0.5 | 0.03 | 0.00–0.06 | 0.06 | |
| SPT POLLEN | Group A | 0.65 ± 0.47 | 0.21 ± 0.41 | 0.45 | 0.4–0.51 | < 0.001 |
| Group B | 0.66 ± 0.47 | 0.65 ± 0.48 | 0.01 | − 0.01–0.02 | 0.26 | |
| SPT PART | Group A | 0.65 ± 0.48 | 0.29 ± 0.45 | 0.36 | 0.31–0.41 | < 0.001 |
| Group B | 0.53 ± 0.5 | 0.51 ± 0.5 | 0.02 | 0.00–0.04 | 0.06 | |
| Phadiatop | Group A | 3.7 ± 2.84 | 0.6 ± 0.55 | 3.11 | 2.84–3.37 | < 0.001 |
| Group B | 4.08 ± 3.29 | 4.04 ± 3.29 | 0.04 | − 0.08–0.16 | 0.49 |
AEC absolute eosinophil count, STIgE serum total immunoglobulin E, SPT HD skin prick test for house dust, SPT ASPER skin prick test for aspergillosis, SPT POLLEN skin prick test for pollen, SPT PART skin prick test for parthenium, Group A, diethyl carbamazine; Group B, montelukast and levocetirizine
Absolute Eosinophil Count
Absolute eosinophil count decreased significantly in both groups, on completion of 21 days treatment course. Improvement in group A (63.5% difference, 95% CI, 635.74–727.03; p < 0.001) was more than group B (23.5% difference, 95% CI, 224.74–272.01; p < 0.001), and it was statistically significant (p < 0.001). Three months after treatment, group A had statistically significant decreased absolute eosinophil count (66.4% difference, 95% CI, 659.74–767.01; p < 0.001). Group B had similar eosinophil count to baseline (p = 0.08).
Serum Total IgE and Phadiatop
Serum total IgE was reduced significantly in both groups, on completion of 21 days treatment. Reduction of serum total IgE in group A (83.3% difference, 95% CI, 582.23–758.36; p < 0.001) was more than group B (38.7% difference, 95% CI, 246.11–303.5; p < 0.001) and it was statistically significant (p < 0.001). Phadiatop was also reduced significantly in both groups. Reduction of phadiatop in group A (90.3% difference, 95% CI, 3.1–3.64; p < 0.001) was more than group B (45.6% difference, 95% CI, 1.72–2.02; p < 0.001), and it was statistically significant (p < 0.001). Three months after completion of treatment, there was statistically significant reduction in serum total IgE and phadiatop in group A (p < 0.001), when compared to baseline values. In group B, values of both the parameters were similar to baseline values (Table 5).
Adverse Events
There were 15 (4.2%) reports of headache and 7 (1.9%) reports of diarrhoea in diethylcarbamazine group. 97 (27.2%) reports of sleepiness in montelukast and levocetirizine group. There were no major adverse effects in both groups.
Discussion
Allergic rhinitis is due to specific immunoglobulin E (IgE) reaction to inhaled allergen. It is mediated by type 2 helper cells (Th2). There is mucosal inflammation and infiltration of eosinophils [20]. When there is exposure to allergen, specific IgE binds to high affinity IgE receptor which leads to release of histamine, leukotriene, prostaglandin, platelet activating factor and activates mast cells. These lead to early phase allergic response. These mediators also attract inflammatory cells leading to late phase reaction. Tumor necrosis factor α is released by activated mast cells which leads to eosinophil and lymphocyte influx into tissues [21]. Diethylcarbamazine acts in many levels in the mechanism of allergic rhinitis. So, it can be considered as a potential drug in the treatment of allergic rhinitis.
Diethylcarbamazine is used as an antifilarial drug for many years [22]. It is also being used in various other conditions like bronchial asthma, tropical pulmonary eosinophilia, type 2 diabetes, liver fibrosis, myocardial infarction, pulmonary hypertension and radiation induced acute lung injury and oxidative stress [23–30]. Recent studies have explored its effect in immunomodulation, arachidonic acid pathway, specific lipoxygenase pathway and leukotriene inhibition [31, 32]. The exact mechanism is not known [17]. Diethylcarbamazune is effective in treating the symptoms of bronchial asthma by blocking the pulmonary eosinophilic inflammation. It prevents airway resistance and suppresses interleukin 5 dependent eosinophilopoiesis [33].
Eosinophils release cytokines, granular cytotoxic proteins and lipid mediators in asthma [34, 35]. There is increase in eosinopoiesis in response to allergen challenge [36]. 5-lipoxygenase through specialized enxymes yields leukotriene B4 and cystinyl leukotrienes which has an important role in the pathophysiology of allergy and asthma [37–40]. In bone marrow, cystinyl leukotrienes enhance eosinopoiesis [41]. Diethylcarbamazine supresses leukotriene synthesis, prevents eosinophilic response to allergen challenge and prevents its accumulation in spleen [18, 42, 43]. Diethylcarbamazine also blocks Th2 cytokine production through attenuating nitric oxide synthase (iNOS) expression and inhibits tumor necrosis factor α [42].
In this study, we have compared diethylcarbamazine with montelukast and levocetirizine treated patients. On completion of 21 days treatment, we found a statistically significant decrease in all the parameters and significant reduction of symptoms in both groups. We found that diethylcarbamazine is better in controlling symptoms of allergic rhinitis and diethylcarbamazine treated patients had decreased absolute eosinophil count, serum total IgE and phadiatop values when compared to montelukast and levocetirizine treated patients. Response to skin prick test was significantly decreased in both groups with better results in diethylcarbamazine group. Three months after discontinuation of treatment, the results were maintained in diethylcarbamazine group, whereas the values in montelukast and levocetirizine group became similar to baseline values. Montelukast and levocetirizine are commonly used to treat allergic rhinitis but have limitations like sedation and it is not cost effective [43–46]. This study shows that diethylcarbamazine is comparable to montelukast and levocetirizine in the treatment of allergic rhinitis and can be a cost-effective alternative to montelukast and levocetirizine. Diethylcarbamazine is better than montelukast and levocetirizine in controlling the symptoms of allergic rhinitis in the acute phase and there is a better reduction in absolute eosinophil count and serum total IgE with diethylcarbamazine. The results of diethylcarbamazine therapy are sustained even 3 months after completion of treatment. The effects of montelukast and levocetirizine wane off on discontinuation of treatment. This study is the first to compare the effects of diethylcarbamazine with montelukast and levocetirizine in the treatment of allergic rhinitis.
The mechanism of montelukast and levocetirizine is cysteinyl leukotriene type 1 receptor antagonism and H1-antihistamine action [47–50]. Mechanism of diethylcarbamazine in allergic rhinitis may be by its suppression of interleukin 5 dependent eosinophilopoiesis, leukotriene synthesis, eosinophilic response to allergen challenge and its accumulation in spleen [17, 33], Th2 cytokine production through attenuating nitric oxide synthase (iNOS) expression and inhibition of tumor necrosis factor α [18]. In our study, there were lesser side effects in diethylcarbamazine compared to montelukast and levocetirizine. The limitation in our study is the exact mechanism of action of diethylcarbamazine in treating allergic rhinitis is not known and future research can be directed to that.
Conclusion
In conclusion, diethylcarbamazine is a safe and cost-effective alternative to montelukast and levocetirizine in treating allergic rhinitis. There is good symptomatic improvement and reduced response to allergen. Future studies should be done to evaluate the exact mechanism of action of diethylcarbamazine and its long-term effects. With this, clinicians may have a cost effective alternative drug in the treatment of allergic rhinitis.
Acknowledgements
We thank Dr. Meera Jothiraj, MD, for her expertise and assistance in all the investigations of our study. We thank Dr. Preethi Mithun, MD, for her assistance in the statistical analysis of our data.
Authors Contributions
MKS and NGN contributed equally to this work. Author order was determined by seniority.
Funding
None.
Compliance with Ethical Standards
Conflict of interest
The authors declare they have no financial interests.
Availability of Data and Material
Available.
Ethics Approval
Yes. Institutional ethics committee IEC Ref No: KIMS/PG/2019/42.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
S. Mohana Karthikeyan, Email: karthient@gmail.com
G. N. Nikisha, Email: nikimol@yahoo.co.in
References
- 1.Strachan D, Sibbald B, Weiland S, et al. Worldwide variations in prevalence of symptoms of allergic rhinoconjunctivitis in children: the international study of asthma and allergies in childhood (ISAAC) Pediatr Allergy Immunol. 1997;8:161–176. doi: 10.1111/j.1399-3038.1997.tb00156.x. [DOI] [PubMed] [Google Scholar]
- 2.Amin K, Issa SM, Ali KM, et al. Evidence for eosinophil and IL-17 mediated inflammation in allergic rhinitis. Clin Mol Allergy. 2020;18:1–7. doi: 10.1186/s12948-020-00117-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Charlesworth EN, Hood AF, Soter NA, Kagey-Sobotka A, Norman PS, Lichtenstein LM. Cutaneous late-phase response to allergen: mediator release and inflammatory cell infiltration. J Clin Invest. 1989;83(5):1519–1526. doi: 10.1172/JCI114047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wenzel S, Wilbraham D, Fuller R, Getz EB, Longphre M. Effect of an interleukin-4 variant on late phase asthmatic response to allergen challenge in asthmatic patients: results of two phase 2a studies. Lancet. 2007;370(9596):1422–1431. doi: 10.1016/S0140-6736(07)61600-6. [DOI] [PubMed] [Google Scholar]
- 5.Scadding GK, Kariyawasam HH, Scadding G, et al. BSACI guideline for the diagnosis and management of allergic and non-allergic rhinitis. Clin Exp Allergy. 2017;47(7):856–889. doi: 10.1111/cea.12953. [DOI] [PubMed] [Google Scholar]
- 6.Bentley AM, Jacobson MR, Cumberworth V, et al. Immunohistology of the nasal mucosa in seasonal allergic rhinitis: increases in activated eosinophils and epithelial mast cells. J Allergy Clin Immunol. 1992;89(4):877–883. doi: 10.1016/0091-6749(92)90444-7. [DOI] [PubMed] [Google Scholar]
- 7.Beppu T, Ohta N, Gon S, et al. Eosinophil and eosinophil cationic protein in allergic rhinitis. Acta Otolaryngol. 1994;114(sup511):221–223. doi: 10.3109/00016489409128337. [DOI] [PubMed] [Google Scholar]
- 8.Mullarkey MF, Hill JS, Webb DR. Allergic and nonallergic rhinitis: their characterization with attention to the meaning of nasal eosinophilia. J Allergy Clin Immunol. 1980;65(2):122–126. doi: 10.1016/0091-6749(80)90196-7. [DOI] [PubMed] [Google Scholar]
- 9.Wilson AM, O'Byrne PM, Parameswaran K. Leukotriene receptor antagonists for allergic rhinitis: a systematic review and meta-analysis. Am J Med. 2004;116(5):338–344. doi: 10.1016/j.amjmed.2003.10.030. [DOI] [PubMed] [Google Scholar]
- 10.Trangsrud AJ, Whitaker AL, Small RE. Intranasal corticosteroids for allergic rhinitis. Pharmacother J Hum Pharmacol Drug Ther. 2002;22(11):1458–1467. doi: 10.1592/phco.22.16.1458.33692. [DOI] [PubMed] [Google Scholar]
- 11.Stanbury RM, Graham EM. Systemic corticosteroid therapy: side effects and their management. Br J Ophthalmol. 1998;82(6):704–708. doi: 10.1136/bjo.82.6.704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Durham SR, Penagos M. Sublingual or subcutaneous immunotherapy for allergic rhinitis? J Allergy Clin Immunol. 2016;137(2):339–349. doi: 10.1016/j.jaci.2015.12.1298. [DOI] [PubMed] [Google Scholar]
- 13.Penagos M, Durham SR. Duration of allergen immunotherapy for inhalant allergy. Curr Opin Allergy Clin Immunol. 2019;19(6):594–605. doi: 10.1097/ACI.0000000000000585. [DOI] [PubMed] [Google Scholar]
- 14.Musa F, Al-Ahmad M, Arifhodzic N, Al-Herz W. Compliance with allergen immunotherapy and factors affecting compliance among patients with respiratory allergies. Hum Vaccin Immunother. 2017;13(3):514–517. doi: 10.1080/21645515.2016.1243632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Epstein TG, Liss GM, Murphy-Berendts K, Bernstein DI. Risk factors for fatal and nonfatal reactions to subcutaneous immunotherapy: national surveillance study on allergen immunotherapy (2008–2013) Ann Allergy Asthma Immunol. 2016;116(4):354–359. doi: 10.1016/j.anai.2016.02.001. [DOI] [PubMed] [Google Scholar]
- 16.Calderón MA, Casale TB, Togias A, Bousquet J, Durham SR, Demoly P. Allergen-specific immunotherapy for respiratory allergies: from meta-analysis to registration and beyond. J Allergy Clin Immunol. 2011;127(1):30–38. doi: 10.1016/j.jaci.2010.08.024. [DOI] [PubMed] [Google Scholar]
- 17.Peixoto CA, Silva BS. Anti-inflammatory effects of diethylcarbamazine: a review. Eur J Pharmacol. 2014;734:35–41. doi: 10.1016/j.ejphar.2014.03.046. [DOI] [PubMed] [Google Scholar]
- 18.Masid-de-Brito D, Queto T, Gaspar-Elsas MI, Xavier-Elsas P. Roles of 5-lipoxygenase and cysteinyl-leukotriene type 1 receptors in the hematological response to allergen challenge and its prevention by diethylcarbamazine in a murine model of asthma. Mediat Inflamm. 2014 doi: 10.1155/2014/403970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Juniper EF, Guyatt GH. Development and testing of a new measure of health status for clinical trials in rhinoconjunctivitis. Clin Exp Allergy. 1991;21(1):77–83. doi: 10.1111/j.1365-2222.1991.tb00807.x. [DOI] [PubMed] [Google Scholar]
- 20.Samitas K, Carter A, Kariyawasam HH, Xanthou G. Upper and lower airway remodelling mechanisms in asthma, allergic rhinitis and chronic rhinosinusitis: the one airway concept revisited. Allergy. 2018;73(5):993–1002. doi: 10.1111/all.13373. [DOI] [PubMed] [Google Scholar]
- 21.Bernstein DI, Schwartz G, Bernstein JA. Allergic rhinitis: mechanisms and treatment. Immunol Allergy Clin N Am. 2016;36(2):261–278. doi: 10.1016/j.iac.2015.12.004. [DOI] [PubMed] [Google Scholar]
- 22.Ottesen EA. Efficacy of diethylcarbamazine in eradicating infection with lymphatic-dwelling filariae in humans. Rev Infect Dis. 1985;7(3):341–356. doi: 10.1093/clinids/7.3.341. [DOI] [PubMed] [Google Scholar]
- 23.Nath K, Pandeya SN. Diethylcarbamazine therapy in tropical eosinophilia. Br Med J. 1960;1(5166):104–107. doi: 10.1136/bmj.1.5166.104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Florêncio MS, Saraiva KL, Peixoto CA. The effects of diethylcarbamazine on the ultrastructure of lung cells in vivo. Tissue Cell. 2005;37(3):241–246. doi: 10.1016/j.tice.2005.03.001. [DOI] [PubMed] [Google Scholar]
- 25.Segoviano-Ramirez JC, Lopez-Altamirano DF, Garcia-Juarez J, Aguirre-Garza JE, Cárdenas-Estrada E, Ancer-Rodriguez J. The diethylcarbamazine delays and decreases the netosis of polymorphonuclear cells of humans with DM Type 2. J Diabetes Res. 2020;2020:4827641. doi: 10.1155/2020/4827641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.El AE, Sokar SS, Shebl AM, Mohamed DZ. Antifibrotic effect of diethylcarbamazine combined with hesperidin against ethanol induced liver fibrosis in rats. Biomed Pharmacother. 2017;89:1196–1206. doi: 10.1016/j.biopha.2017.03.013. [DOI] [PubMed] [Google Scholar]
- 27.Jia G, Zao M, Liu X. Protective effect of diethylcarbamazine inhibits NF-κB activation in isoproterenol-induced acute myocardial infarction rat model through the PARP pathway. Mol Med Rep. 2017;16(2):1596–1602. doi: 10.3892/mmr.2017.6695. [DOI] [PubMed] [Google Scholar]
- 28.de França ME, Rocha SW, Oliveira WH, et al. Diethylcarbamazine attenuates the expression of pro-fibrogenic markers and hepatic stellate cells activation in carbon tetrachloride-induced liver fibrosis. Inflammopharmacology. 2018;26(2):599–609. doi: 10.1007/s10787-017-0329-0. [DOI] [PubMed] [Google Scholar]
- 29.Farzipour S, Amiri FT, Mihandoust E, et al. Radioprotective effect of diethylcarbamazine on radiation-induced acute lung injury and oxidative stress in mice. J Bioenerg Biomembr. 2020;52(1):39–46. doi: 10.1007/s10863-019-09820-9. [DOI] [PubMed] [Google Scholar]
- 30.Ribeiro EL, Fragoso IT, dos Santos Gomes FO, et al. Diethylcarbamazine: A potential treatment drug for pulmonary hypertension? Toxicol Appl Pharmacol. 2017;333:92–99. doi: 10.1016/j.taap.2017.08.015. [DOI] [PubMed] [Google Scholar]
- 31.Medina-De la Garza CE, Guerrero-Ramírez G, García-Hernández M, et al. Immunomodulatory activity of diethylcarbamazine on humoral, cellular cytokine response and respiratory burst in BALB/c mice. Immunopharmacol Immunotoxicol. 2012;34(3):477–483. doi: 10.3109/08923973.2011.630008. [DOI] [PubMed] [Google Scholar]
- 32.Masid-de-Brito D, Vieira BM, de Souza CC, Silva F, Gaspar-Elsas MI, Xavier-Elsas P. Allergen challenge-induced changes in bone-marrow responses to leukotriene D4, nonsteroidal anti-inflammatory drugs and cytokines. Immunopharmacol Immunotoxicol. 2020;42(3):199–210. doi: 10.1080/08923973.2020.1733598. [DOI] [PubMed] [Google Scholar]
- 33.Ribeiro EL, Barbosa KP, Fragoso IT, et al. Diethylcarbamazine attenuates the development of Carrageenan-induced lung injury in mice. Mediat Inflamm. 2014 doi: 10.1155/2014/105120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Liu W, Liu S, Verma M, et al. Mechanism of TH2/TH17-predominant and neutrophilic TH2/TH17-low subtypes of asthma. J Allergy Clin Immunol. 2017;139(5):1548–1558. doi: 10.1016/j.jaci.2016.08.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Suphioglu C, Singh MB, Taylor P, et al. Mechanism of grass-pollen-induced asthma. Lancet. 1992;339(8793):569–572. doi: 10.1016/0140-6736(92)90864-y. [DOI] [PubMed] [Google Scholar]
- 36.Cockcroft DW. Mechanism of perennial allergic asthma. Lancet. 1983;322(8344):253–256. doi: 10.1016/s0140-6736(83)90235-0. [DOI] [PubMed] [Google Scholar]
- 37.Flint KC, Leung KB, Hudspith BN, Brostoff J, Pearce FL, Johnson NM. Bronchoalveolar mast cells in extrinsic asthma: a mechanism for the initiation of antigen specific bronchoconstriction. Br Med J. 1985;291(6500):923–926. doi: 10.1136/bmj.291.6500.923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.McFadden ER, Jr, Luparello TH, Lyons HA, Bleecker E. The mechanism of action of suggestion in the induction of acute asthma attacks. Psychosom Med. 1969;31(2):134–143. doi: 10.1097/00006842-196903000-00007. [DOI] [PubMed] [Google Scholar]
- 39.Parnes SM. The role of leukotriene inhibitors in allergic rhinitis and paranasal sinusitis. Curr Allergy Asthma Rep. 2002;2(3):239–244. doi: 10.1007/s11882-002-0025-y. [DOI] [PubMed] [Google Scholar]
- 40.Denburg JA, Gauvreau GM. Hemopoietic progenitors: the role of eosinophil/basophil progenitors in allergic airway inflammation. Expert Rev Clin Immunol. 2005;1(1):87–101. doi: 10.1586/1744666X.1.1.87. [DOI] [PubMed] [Google Scholar]
- 41.Queto T, Xavier-Elsas P, Gardel MA, et al. Inducible nitric oxide synthase/CD95L-dependent suppression of pulmonary and bone marrow eosinophilia by diethylcarbamazine. Am J Respir Crit Care Med. 2010;181(5):429–437. doi: 10.1164/rccm.200905-0800OC. [DOI] [PubMed] [Google Scholar]
- 42.Vijayan VK, Rao KK, Sankaran K, Venkatesan P, Prabhakar R. Tropical eosinophilia: clinical and physiological response to diethylcarbamazine. Respir Med. 1991;85(1):17–20. doi: 10.1016/s0954-6111(06)80205-2. [DOI] [PubMed] [Google Scholar]
- 43.Snidvongs K, Seresirikachorn K, Khattiyawittayakun L, Chitsuthipakorn W. Sedative effects of levocetirizine: a systematic review and meta-analysis of randomized controlled studies. Drugs. 2017;77(2):175–186. doi: 10.1007/s40265-016-0682-0. [DOI] [PubMed] [Google Scholar]
- 44.Layton D, Wilton L, Boshier A, Cornelius V, Harris S, Shakir SA. Comparison of the risk of drowsiness and sedation between levocetirizine and desloratadine. Drug saf. 2006;29(10):897–909. doi: 10.2165/00002018-200629100-00007. [DOI] [PubMed] [Google Scholar]
- 45.Hay J, Jhaveri M, Tangirala M, Kaliner M. Cost and resource utilization comparisons of second-generation antihistamines versus montelukast for allergic rhinitis treatment. Allergy Asthma Proc. 2009;30(6):634–642. doi: 10.2500/aap.2009.30.3293. [DOI] [PubMed] [Google Scholar]
- 46.Goodman MJ, Jhaveri M, Saverno K, Meyer K, Nightengale B. Cost-effectiveness of second-generation antihistamines and montelukast in relieving allergic rhinitis nasal symptoms. Am Health Drug Benefits. 2008;1(8):26–34. [PMC free article] [PubMed] [Google Scholar]
- 47.Ciprandi G, Cirillo I, Vizzaccaro A, Tosca MA. Levocetirizine improves nasal obstruction and modulates cytokine pattern in patients with seasonal allergic rhinitis: a pilot study. Clin Exp Allergy. 2004;34(6):958–964. doi: 10.1111/j.1365-2222.2004.01960.x. [DOI] [PubMed] [Google Scholar]
- 48.Bachert C. Levocetirizine: a modern H1-antihistamine for the treatment of allergic rhinitis. Expert Rev Clin Immunol. 2005;1(4):495–510. doi: 10.1586/1744666X.1.4.495. [DOI] [PubMed] [Google Scholar]
- 49.Klimek L. Potential of levocetirizine in the relief of nasal congestion. Int J Clin Pract. 2005;59(6):721–729. doi: 10.1111/j.1368-5031.2005.00521.x. [DOI] [PubMed] [Google Scholar]
- 50.Ciebiada M, Górska-Ciebiada M, DuBuske LM, Górski P. Montelukast with desloratadine or levocetirizine for the treatment of persistent allergic rhinitis. Ann Allergy Asthma Immunol. 2006;97(5):664–671. doi: 10.1016/S1081-1206(10)61098-8. [DOI] [PubMed] [Google Scholar]