

Abstract
Background
The ketogenic diet is a therapeutic option to control drug-resistant epileptic seizures and has difficult compliance standards due to adverse effects, psychosocial factors, or dietary restriction.
Objective
To create and validate a ketogenic diet compliance questionnaire.
Methods
Methodological study, convergent care. The instrument was analyzed (construct validation) by five judges during two cycles of the Delphi technique. The judges assessed the relevance and clarity by using the Likert scale with three levels and made suggestions. The validation of the instrument was calculated using the agreement rate and content validity index (CVI). The application by two nutritionists made it possible to test reproducibility using the Kappa coefficient. When comparing the classification with a template developed by the health professionals who cared for the patients in question, the Pearson correlation and Fisher exact tests were used. For the reliability test, self-applied data were collected and evaluated using Cronbach Alpha coefficient.
Results
The questionnaire initially created with 11 multiple choice questions on a Likert scale was reduced to 10 questions with an agreement rate and the CVI classified as excellent after two rounds with judges. In the application of the tool, a kappa of 0.6087 was obtained, a Pearson that showed no significant difference between evaluators and a Cronbach α of 0.6483, with substantial consistency.
Conclusions
This work resulted in the creation of an unprecedented and reliable questionnaire on adherence to the national ketogenic diet. Further studies should be performed to extrapolate the use of this questionnaire in different populations.
Keywords: Diet, Ketogenic, Surveys and Questionnaires, Treatment Adherence and Compliance
Resumo
Antecedentes
A dieta cetogênica é um tratamento para epilepsia refratária e tem difícil adesão devido aos efeitos adversos, fatores psicossociais ou à própria restrição alimentar.
Objetivo
Criar e validar um questionário de adesão à dieta cetogênica.
Métodos
Estudo metodológico, convergente assistencial. O instrumento foi analisado (validação de constructo) por cinco juízes durante dois ciclos da técnica Delphi. Os juízes avaliaram a pertinência e a clareza com respostas na escala Likert com três níveis, além de sugestões. A validação do instrumento foi calculada pela taxa de concordância e índice de validade de conteúdo (IVC). Posteriormente, houve aplicação por duas nutricionistas (reprodutibilidade), sendo analisada a concordância pelo coeficiente de Kappa. Ao comparar a classificação com um gabarito, elaborado pelos profissionais da saúde responsáveis pelos pacientes em questão, foram utilizados os coeficientes de correlação de Pearson e teste exato de Fisher. Para teste de fidedignidade, a coleta de dados auto-aplicados foi avaliada pelo coeficiente de Alpha de Cronbach.
Resultados
O questionário inicialmente criado com 11 questões de múltipla escolha em escala Likert foi reduzido para 10 questões com taxa de concordância e IVC excelentes após 2 rodadas com juízes. Na aplicação da ferramenta obteve-se coeficiente de Kappa de 0,6087, o coeficiente de Pearson não demostrou diferença significativa entre avaliadores, e o coeficiente α de Cronbach de 0,6483, com consistência substancial.
Conclusões
Este trabalho resultou na criação do inédito questionário nacional de adesão à dieta cetogênica, válido e fidedigno. Outros estudos devem ser realizados para extrapolar a utilização deste questionário em diferentes populações.
Palavras-chave: Dieta Cetogênica, Inquéritos e Questionários, Cooperação e Adesão ao Tratamento
INTRODUCTION
The ketogenic diet (KD) is a treatment for drug-resistant epilepsy. It is not a recent treatment, having been used for a hundred years, since 1921. Although currently more widespread and better implemented, it is still little known by the general population, including doctors who still consider it a difficult-to-adhere-to and not a very palatable diet. Since the early 1990s, there has been a dramatic increase in scientific articles on KD, and it is now a well-established and proven effective treatment for epilepsy. 1,2
The KD has a 40 to 50% chance of reducing at least 50% of epileptic seizures. 3 It is indicated for patients from childhood to adulthood with drug-resistant epilepsy, often with daily or weekly seizures, who have failed treatment with two or three anti-seizure medications, correctly indicated, tolerated, used in adequate doses in monotherapy or polytherapy (3–5). The KD is considered the first line of treatment, regardless of the number of epileptic seizures in glucose transporter protein type 1 (GLUT-1) deficiency syndrome and pyruvate dehydrogenase complex deficiency. 3
The World Health Organization (WHO) defines as adherence the degree to which a person's behavior corresponds with the recommendations of health professionals regarding medication, dietary follow-up, or changes in lifestyle habits. 4
Adherence to treatment in KD is difficult. A meta-analysis with 11 KD studies indicated a combined patient compliance of 45%. Adherence failure is attributed to the adverse effects of the diet, psychosocial factors or the dietary restriction caused by the diet. 5
The KD is composed of foods rich in fat (sour cream, bacon, mayonnaise, and oils in general), protein (meat, eggs, cheese), and a small amount of food that contains carbohydrates (fruits, vegetables, and greens). Normally, KD is divided into 4 daily meals, which can vary from 3 to 5 meals a day, to adapt to family habits. Children under 1 year of age using infant formula should receive 6 meals a day. Food is weighed on a digital scale. The diet is calculated individually according to body weight, age, and the nutritional status of each child. The consistency must be modified according to the oromotor capacity of each child or use of ostomies. 2
Currently, the protocol for the care of patients with KD is made by a specialized nutritionist who guides the use of scales to weigh dietary ingredients, guides the way of preparing meals and options for substitutions. Even so, in clinical practice, patients with greater cognitive capacity still make mistakes and bring up several questions in the returns, showing an inability to understand the KD with theoretical explanations only.
To date, there is no validated instrument for checking the adherence to KD, and adherence is assessed by the professional team according to subjective methods. Thus, this study has as its primary justification the development and validation of a questionnaire for adherence to KD.
METHODS
This is a methodological study of a quantitative nature, developed in two stages: construction and validation of both the content and the reliability and reproducibility of a questionnaire for adherence to KD, which will be called “Keto-check,” to be applied by the therapeutic team (neurologists and nutritionists). In methodological research, the goal is to develop reliable, precise instruments that can be applied by the multiprofessional team. 6,7
The present study was performed at the outpatient clinic of KD, Instituto da Criança, Hospital das Clínicas, Medical School of Universidade de São Paulo (ICR-HCFMUSP), from January to July 2020. It was approved by the Research Ethics Committee (CEP) of the Medical School of Universidade de São Paulo, with Certificate of Presentation for Ethical Appreciation (CAAE) 19812919.2.0000.0068 and approval n. 3.735.637.
The first step was to build the content of the instrument. A brief bibliographic survey was performed on Pubmed with the terms questionnaire adherence or questionnaire compliance or questionnaire quality of life and ketogenic diet epilepsy to identify the main parameters that impact adherence to ketogenic therapy.
The tool was initially built by two professionals (nutritionist and child neurologist specialized in KD for epilepsy) with 11 statements related to factors associated with excellent adherence to treatment: improvement in quality of life, reduction of seizures, measurement of ketosis, weighing of food consumed, not cheating on the diet, using drugs without carbohydrates, always attending consultations, reading labels of processed foods and consulting a nutritionist about what you can consume, and cooking at home. The interviewee should indicate his/her level of agreement with the statement on a 5-point Likert scale: (1) Strongly disagree, (2) Partly disagree, (3) I do not know how to answer, (4) Partly agree, (5) Strongly agree. Each answer would subsequently have a score assigned (indicated above in parentheses) and the sum of all answers would lead to a score (minimum value 11, maximum 55). The higher the score, the better the adherence to treatment, being categorized as: insufficient adherence” from 11 to 35 points; good adhesion from 36 to 45 points; and excellent adhesion from 45 to 55 points.
To validate the instrument, the Delphi technique was used, with two cycles. (11) The tool was analyzed by a group of experts who acted as judges, composed of five professionals with the following inclusion criteria: (1) being a doctor or nutritionist; (2) having a title of specialist, master, or PhD; and (3) working in the areas of care, management or teaching and research in KD therapy, with more than 10 years of training and professional experience. The professionals were invited to participate by e-mail. We sent a form, prepared on Google Forms, which contained a brief text explaining the research and an informed consent form for participation. Next, we provided the new tool for verification of adherence to KD with questions in relation to each statement used as to the pertinence and ease of understanding. The responses were presented on a Likert scale with a score of 1 to 3: 1 = no; 2 = maybe; and 3 = yes. At the end of each question, we provided a field for suggestions, so that the judges could give feedback on the questions, as well as enrich the content with timely aspects. 8
For content validation, the agreement rate and the content validity index (CVI) were calculated. The latter is widely used to calculate the consensus among the judges, since it measures the agreement about the evaluated aspects. 9
The agreement rate was calculated by dividing the number of positive responses by the total number of responses. The CVI can be calculated following four steps. The first, based on the judges' scores (1–3), averages the scores for each item. In the second stage, based on the average, the initial CVI for each item is calculated, dividing by the maximum value that the question could receive for relevance or clarity. In the third stage, the error of each item is calculated, to discount possible biases by the judges. To calculate the error, one (1) is divided by the number of judges, raised by the same number of evaluators. In the fourth step, the final CVI of each item can be calculated from the subtraction of the initial CVI by the error. The acceptable rate of consensus in this study, for each item analyzed to be considered valid, was 90% or CVI of 0.9.
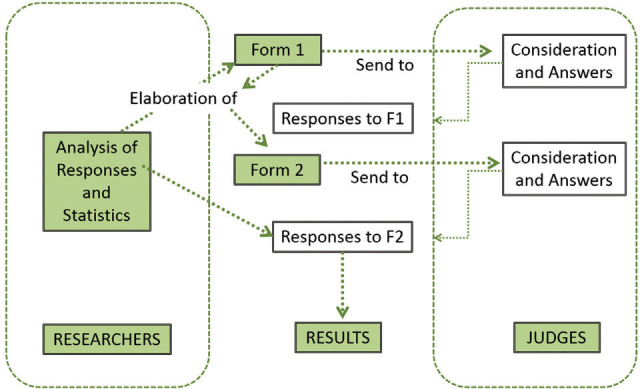
The validation of the content of the tool went through two cycles with the specialists so that it could reach the minimum value of the CVI for all items. The answers obtained were organized in a Microsoft Excel electronic spreadsheet (Microsoft Corp., Redmond, WA, USA), with the numerical and subjective information filled in by the judges. In the flowchart illustrated in ►Figure 1 , all Delphi phases used in this study are observed.
Figure 1. Delphi phases used in this study. Source: prepared by the authors. São Paulo. 2020.
In the first cycle, the five judges responded and made suggestions. The tool was reformulated according to opinions, after discussion among researchers. The tool for the analysis of all the judges was sent again. Calculations were performed, and the consensus initially proposed was obtained.
After validating the instrument's content, two nutritionists, who work in the care area and who had not participated in the previous stages of the study, were invited to apply the tool to 10 patients who have undergone or performed KD for at least 3 months, in follow-up at ICR-HCFMUSP. The questionnaire was applied in duplicate by the 2 nutritionists via telephone, individually, with an interval between applications longer than 1 week and shorter than 15 days, without the nutritionists having access to the previous answers of the same patient. The nutritionists were asked to classify patients according to the score obtained for the level of adherence to KD. To assess the agreement between the evaluators (reproducibility), the Kappa coefficient was used, characterized by different ranges, in which values greater than 0.75 represent excellent agreement; values below 0.40 represent low agreement; and values between 0.40 and 0.75 represent satisfactory agreement. 10
Without having access to the answers to the questionnaires applied by the nutritionists, two professionals (one doctor and another nutritionist) from the patient care team, with access to medical records (laboratory data, ketosis, nutritional status), indicated the correct answers, according to their knowledge of patient compliance. This was considered the gold standard to compare the correlation of the KD adherence questionnaire with the perception of the health professional. For that, the statistical test performed for comparisons between the classifications was the Fisher exact test, and for the total value of the questionnaire score, it was Pearson correlation coefficient.
To test the reliability of the questionnaire, data was collected in a convenience sample from patients using KD. The questionnaire was sent electronically for patients and caregivers all over Brazil. They self-completed the questionnaire. In this stage, reliability was verified through internal consistency using the Cronbach αcoefficient, which can be classified as: when it reaches values above 0.8, almost perfect; from 0.61 to 0.8, substantial; from 0.41 to 0.6, moderate; between 0.21 and 0.4, reasonable; and less than 0.21, a small consistency is considered. (11) The tests were performed using the Stata version 13 software (Stata Corp., College Station, TX, USA), 11 and the level of significance determined was p< 0.05.
RESULTS
A review of the literature approaching questionnaires of adherence (n= 3) or compliance (n= 5) or quality of life (n= 15) in KD for epilepsy showed few articles. The registered dietitian and neurologist created the keto-check based on reported quality of life questionnaires. 12,13,14
Although few judges participated, they could represent important reference centers of Brazil and followed all criteria of inclusion. In ►Table 1 , we can see the characterization of the judges who participated in the Delphi cycles, according to sex, place of professional practice, title of professional qualification, area of knowledge, and area of expertise. ►Table 2 shows the results of the two cycles referring to the content validation of the tool. All items were considered pertinent by the judges since the first Delphi cycle, despite presenting borderline values in question 10. Regarding clarity, question 7 did not initially reach consensus, and the writing was reformulated. In addition, questions 5 and 6 were combined, resulting in a reduction of one question.
Table 1. Characterization of the judges who participated in the validation of the instrument's content.
| Characteristics | n° | % | |
|---|---|---|---|
| Sex | F | 5 | 100.0 |
| Total | 5 | 100.0 | |
| Place of professional activity | São Paulo | 2 | 40.0 |
| Recife | 3 | 60.0 | |
| Total | 5 | 100.0 | |
| Professional qualification title | Doctorate degree | 2 | 40.0 |
| Master's degree | 1 | 20.0 | |
| Specialization | 2 | 40.0 | |
| Total | 5 | 100.0 | |
| Knowledge area | Doctor | 1 | 20.0 |
| Nutritionist | 4 | 80.0 | |
| Total | 5 | 100.0 | |
| Professional practice area | Assistance | 4 | 80.0 |
| Teaching and research | 1 | 20.0 | |
| Total | 5 | 100.0 |
Table 2. Percentage of agreement (%C) of the judges and the content validity index in the analysis of the instrument.
| Question | Pertinence | Clarity | |||
|---|---|---|---|---|---|
| First round | Second round | First round | Second round | ||
| 1 | CVI | 0.9997 | 0.9997 | 0,8663 | 0,9997 |
| % C | 100 | 100 | 60 | 100 | |
| 2 | CVI | 0.9997 | 0.9997 | 0.9330 | 0.9997 |
| % C | 100 | 100 | 80 | 100 | |
| 3 | CVI | 0.9997 | 0.9997 | 0.8663 | 0.9997 |
| % C | 100 | 100 | 60 | 100 | |
| 4 | CVI | 0.9997 | 0.9997 | 0.9330 | 0.9997 |
| % C | 100 | 100 | 80 | 100 | |
| 5 | CVI | 0.9997 | − | 0.9330 | − |
| % C | 100 | − | 80 | − | |
| 6 | CVI | 0.9997 | 0.9997 | 0.9330 | 0.8663 |
| % C | 100 | 80 | 80 | 100 | |
| 7 | CVI | 0.9997 | 0.9997 | 0.6663 | 0.9997 |
| % C | 100 | 100 | 40 | 100 | |
| 8 | CVI | 0.9997 | 0.9997 | 0.9330 | 0.9997 |
| % C | 100 | 100 | 80 | 100 | |
| 9 | CVI | 0.9997 | 0.9997 | 0.9330 | 0.9997 |
| % C | 100 | 100 | 80 | 100 | |
| 10 | CVI | 0.7997 | 0.9997 | 0.8663 | 0.9997 |
| % C | 60 | 100 | 80 | 100 | |
| 11 | CVI | 0.9997 | 0.9997 | 0.9330 | 0.9997 |
| % C | 100 | 100 | 80 | 100 | |
| Categorization | CVI | 0.9997 | 0.9997 | ||
| % C | 100 | 100 | |||
Abbreviation: CVI, Content Validity Index.
%C: Percentage of agreement among judges.
After this cycle, the adjustments suggested by the judges were made, and a new form was created for content validation. In this second round, the values obtained for the percentage of agreement between judges and the content validity index, as well as the relevance and clarity of the question, were excellent (►Table 2 ).
In view of the validated tool, two evaluators (nutritionists specialized in clinical nutrition, but not related to the elaboration or judgment of the instrument) were invited to apply the tool to a group of 10 patients who underwent KD for at least 3 months. Nutritionists contacted the patients by phone with a maximum interval of 15 days, without having access to previous answers. There was only one refusal to participate, so the sample number was nine, where is observed a greater adherence refered by the patient when compared with the gold standard (►Table 3 ). To verify the agreement between the professionals, the Kappa coefficient was performed, obtaining a value of k = 0.6087, which means there was a satisfactory agreement between evaluators.
Table 3. Application of the keto-check tool in nine patients undergoing treatment with ketogenic diet.
| Patient | Evaluator 1 | Evaluator 2 | Gold standard |
|---|---|---|---|
| 1 | Great | Great | Good |
| 2 | Great | Great | Good |
| 3 | Great | Good | Good |
| 4 | Great | Great | Good |
| 5 | Great | Great | Good |
| 6 | Great | Great | Good |
| 7 | Good | Good | Great |
| 8 | Great | Great | Good |
| 9 | Great | Great | Good |
After sending the questionnaire electronically for patients from all over Brazil, 47 answered questionnaires were obtained (►Table 4 shows some sample's details), and in this stage of the study, the internal consistency of the instrument was verified by means of the Cronbach αcoefficient, obtaining the value of 0.6483, which translates as substantial consistency. ►Table 5 shows the changes of values of the Cronbach coefficient in case of exclusion of each questionnaire's sentence.
Table 4. Characteristics of the sample (n= 47) who answered questionnaires electronically from all over Brazil.
| Characteristic | n | % | |
|---|---|---|---|
| Age | 0–2 years | 8 | 17 |
| 2–10 years | 28 | 60 | |
| 10–18 years | 8 | 17 | |
| Adults | 3 | 6 | |
| Time in the ketogenic diet | < 3 months | 0 | 0 |
| 3–6 months | 6 | 13 | |
| 6–12 months | 8 | 17 | |
| >12 months | 33 | 70 | |
Table 5. Values of α de Cronbach in case of exclusion of each question.
| Question | Cronbach α |
|---|---|
| Q1 | 0.6529 |
| Q2 | 0.6518 |
| Q3 | 0.5794 |
| Q4 | 0.5302 |
| Q5 | 0.6118 |
| Q6 | 0.6432 |
| Q7 | 0.6545 |
| Q8 | 0.5483 |
| Q9 | 0.6394 |
| Q10 | 0.6614 |
The comparison of the classification of adherence to KD performed by the questionnaire through the interview by professionals and the classification performed by the professionals who care for these patients (template) did not show any significant difference (p= 0.111), and when the Pearson correlation coefficient was performed in the total score of the questionnaire, this showed a result of 0.5917, which indicates a moderate correlation.
After validating the content and applicability of the proposed instrument, the keto-check was obtained, as shown in ►Table 6 (English version) and ►Table 7 (Portuguese version).
Table 6. Keto-check adherence assessment tool. Keto-check English version.
|
KETO-CHECK - ASSESSMENT TOOL FOR KETOGENIC DIET ADHESION
Next you will read 10 sentences. Circle the alternative that corresponds to how much you agree or disagree with the phrase in your reality and routine with your child or teenager. | |
| I. After the beginning of the ketogenic diet, I realize that my child/adolescent has improved the quality of life in general (considering physical health, communication, and emotional and social life; positive effects on family dynamics; and learning and performance in therapies). | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| II. After the beginning of the ketogenic diet, I realize that the number and/or duration and/or intensity of epileptic seizures in my child/adolescent has decreased. | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| III. After starting the ketogenic diet, I measure my child's/adolescent's ketosis (in the blood or urine), and it remains in frank ketosis (in the purple urine strip: ++ or 80 mg/dL to +++ or 160 mg / dL OR in blood: 2–5 mmol). | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| IV. After starting the ketogenic diet, I weigh all the foods (raw) offered to my child/adolescent. | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| V. After the beginning of the ketogenic diet, my child/adolescent never ate food that was not prescribed by the nutritionist (there was never a cheat meal: sneaking or having someone else offer food that is not allowed or using more or less of the ingredients then the recommended). | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| VI. After the beginning of the ketogenic diet, all medications that my child/adolescent uses were exchanged for sugar-free medicines. | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| VII. I attend all appointments scheduled with a nutritionist and neurologist. | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| VIII. After starting the ketogenic diet, I make notes in a notebook daily with food consumed, number of seizures, measured ketosis, and complications (fever, vomiting, refusal to eat). | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| IX. After starting the ketogenic diet, I always read the labels (carbohydrates, proteins, sugars) of all industrialized products and I always ask the nutritionist if such food/product is allowed before offering this product to my child/teenager. | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| X. I cook all my child's meals at home. I always try to vary preparations and look for new recipes. | 1- Strongly disagree 2- Partially disagree 3- I do not know how to answer 4- Partially agree 5- I totally agree |
| TOTAL POINTS - ADD CIRCULATED NUMBERS | |
| • Insufficient adherence: 10 to 35 points • Good adherence: 36 to 45 points • Excellent adherence: 45 to 50 points | |
Source: prepared by the authors. São Paulo. 2020.
Table 7. Keto-Check adherence assessment tool. Keto-check. Portuguese version.
|
KETO-CHECK - FERRAMENTA DE AVALIAÇÃO DA ADESÃO A DIETA CETOGENICA
A seguir você vai ler 10 frases. Circule a alternativa que corresponde ao quanto você concorda ou não com a frase na sua realidade e rotina com sua criança ou adolescente. | |
| I. Após o início da dieta cetogênica, eu percebo que minha criança/adolescente melhorou a qualidade de vida de maneira geral (considerando saúde física, comunicação, e vida emocional e social; efeitos positivos na dinâmica familiar; aprendizado e rendimento nas terapias). | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| II. Após o início da dieta cetogênica, eu percebo que diminuíram número e/ou duração e/ou intensidade de crises epilépticas na minha criança/adolescente. | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| III. Após o início da dieta cetogênica, eu realizo aferição da cetose (no sangue ou na urina) da minha criança/adolescente e esta mantém-se em cetose franca (na fita de urina roxinha: ++ ou 80 mg/dL a +++ ou 160 mg/dL OU no sangue: 2–5 mmol). | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| IV. Após o início da dieta cetogênica, eu realizo pesagem de todos os alimentos (crus) oferecidos para minha criança/adolescente. | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| V. Após o início da dieta cetogênica, minha criança/adolescente nunca comeu alimento fora da prescrição do nutricionista (nunca fugiu à dieta: comer escondido ou outra pessoa oferecer alimentos não permitidos ou usar maior ou menor quantidade de ingredientes do que o recomendade). | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| VI. Após o início da dieta cetogênica, todos os medicamentos que minha criança/adolescente utiliza foram trocados por versões sem açúcar. | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| VII. Eu compareço a todas as consultas agendadas com nutricionista e neurologista. | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| VIII. Após o início da dieta cetogênica, eu realizo anotações em um caderno diariamente com os alimentos consumidos, o número de crises, cetose aferida, e intercorrências (febre, vômito, recusa alimentar). | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| IX. Após o início da dieta cetogênica, eu sempre leio os rótulos (carboidratos, proteínas, açúcares) de todos os produtos industrializados e sempre questiono ao nutricionista se estes são permitidos antes de oferecê-los para minha criança/adolescente. | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| X. Eu cozinho em casa todas as refeições da minha criança. Sempre procuro variar preparações e buscar novas receitas. | 1- Discordo totalmente 2- Discordo parcialmente 3- Não sei responder 4- Concordo parcialmente 5- Concordo totalmente |
| TOTAL PONTOS – SOMAR NÚMEROS CIRCULADOS | |
| • Adesão insuficiente: 10 a 35 pontos • Boa adesão: 36 a 45 pontos • Excelente adesão: 45 a 50 pontos | |
Source: Prepared by the authors. São Paulo. 2020.
DISCUSSION
Adherence to treatment is essential to obtain positive results; however, no national instruments have been identified to assess adherence to KD therapy. This study made it possible to create a questionnaire to determine the adherence to KD with valid and reliable results, with these data being obtained through a complex methodological process and already applied in similar articles. 15
The creation of this questionnaire was based on topics addressed in other validated questionnaires for assessing quality of life, with some referring to the effectiveness of the KD in children with epilepsy. 12,16,17
Although related to the same theme and sometimes the same population regarding the pathology, the present questionnaire verifies a wider range of parameters for analyzing adherence to the treatment in question, encompassing issues such as making ketogenic recipes on a daily basis. In addition, it is the first questionnaire in the national scenario to address adherence to KD therapy in a systematic, valid, and reliable manner.
The health professional's perception of the patient's adherence to treatment is not always correlated with reality. In this study, we noticed that the perception of the professional tends to be of lower adherence than that reported by the patient, despite not reaching statistical significance. It can be considered that the patient's response might contain a bias of the fear of reporting poor adherence and losing access to treatment, even if the consent form to participate in the research guarantees confidentiality and access to the services independently of participation in the research.
Other published questionnaires had difficulties in achieving an excellent statistical result, either due to methodological biases, the number of questions, or the sample number. 12,15,16
Some limiting factors in this study are related to the sample number in the various data collections, which may have hindered the statistical analysis. Perhaps with a larger sample size, the analysis would be even more favorable to the validity and reliability of the instrument. In addition, the fact that it was applied in only a few reference centers may limit the extrapolations of this questionnaire to other populations, despite having been created with a jury of specialists from important reference centers in Brazil.
Despite that, this work resulted in the creation of an unprecedented and valid questionnaire to determine the adherence to the national KD. Further studies should be performed to cover the application of this questionnaire in other populations, with other realities of approaching KD therapy.
References
- 1.Kossoff EH, Zupec-Kania BA, Auvin S, Charlie Foundation. Matthew’s Friends. Practice Committee of the Child Neurology Society et al. Optimal clinical management of children receiving dietary therapies for epilepsy: Updated recommendations of the International Ketogenic Diet Study Group. Epilepsia Open. 2018;3(02):175–192. doi: 10.1002/epi4.12225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sampaio LPB. In: ABC da dieta cetogênica para epilepsia refratária. 1ª. Content D, editor. Rio de Janeiro: Liga Brasileira de Epilepsia; 2018. p. 220. [Google Scholar]
- 3.Kossoff EH, Zupec-Kania BA, Amark PE, Charlie Foundation. Practice Committee of the Child Neurology Society. International Ketogenic Diet Study Group et al. Optimal clinical management of children receiving the ketogenic diet: recommendations of the International Ketogenic Diet Study Group. Epilepsia. 2009;50(02):304–317. doi: 10.1111/j.1528-1167.2008.01765.x. [DOI] [PubMed] [Google Scholar]
- 4.Reyes-Flores E, Trejo-Alvarez R, Arguijo-Abrego S, et al. Adherencia terapéutica: conceptos, determinantes y nuevas estrategias. Rev Med Hondur. 2016;3/4(84):125–132. [Google Scholar]
- 5.Ye F, Li XJ, Jiang WL, Sun HB, Liu J. Efficacy of and patient compliance with a ketogenic diet in adults with intractable epilepsy: a meta-analysis. J Clin Neurol. 2015;11(01):26–31. doi: 10.3988/jcn.2015.11.1.26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Polit DF, Beck CT. Fundamentos de Pesquisa em Enfermagem: Avaliação de Evidências para a Prática da Enfermagem. 7th. Porto Alegre: Artmed; 2011. [Google Scholar]
- 7.Coluci MZO, Alexandre NMC, Milani D. Construção de instrumentos de medida na área da saúde. Cien Saude Colet. 2015;20(03):925–936. doi: 10.1590/1413-81232015203.04332013. [DOI] [PubMed] [Google Scholar]
- 8.Revorêdo LS, Maia RS, Torres GV, Maia EMC. O uso da técnica Delphi em saúde: uma revisão integrativa de estudos brasileiros. Arq. Ciênc Saúde (Porto Alegre) 2015;(22):16–21. [Google Scholar]
- 9.Alexandre NMC, Coluci MZO. Validade de conteúdo nos processos de construção e adaptação de instrumentos de medidas. Cien Saude Colet. 2011;16(07):3061–3068. doi: 10.1590/s1413-81232011000800006. [DOI] [PubMed] [Google Scholar]
- 10.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(01):159–174. [PubMed] [Google Scholar]
- 11.StataCorp . Stata Statistical Software: Release 13. College Station, TX: StataCorp LP; 2013. [Google Scholar]
- 12.Barwick K, Parker T, Murphy N, Todd A, Leveritt M, Wilkinson SA. Development and pilot testing of a parent-reported health-related quality of life measure for children on the ketogenic diet: The KetoQoL. Nutr Diet. 2017;74(05):521–528. doi: 10.1111/1747-0080.12348. [DOI] [PubMed] [Google Scholar]
- 13.Bruce S, Devlin A, Air L, Cook L. Changes in quality of life as a result of ketogenic diet therapy: A new approach to assessment with the potential for positive therapeutic effects. Epilepsy Behav. 2017;66(66):100–104. doi: 10.1016/j.yebeh.2016.10.001. [DOI] [PubMed] [Google Scholar]
- 14.Viana V, Sinde S, Saxton JC. Children’s eating behavior questionnaire: associations with BMI in Portuguese children. Br J Nutr. 2008;100(02):445–450. doi: 10.1017/S0007114508894391. [DOI] [PubMed] [Google Scholar]
- 15.Modi AC, Junger KF, Mara CA, et al. Validation of the PedsQL Epilepsy Module: A pediatric epilepsy-specific health-related quality of life measure. Epilepsia. 2017;58(11):1920–1930. doi: 10.1111/epi.13875. [DOI] [PubMed] [Google Scholar]
- 16.Schoeler NE, MacDonald L, Champion H, et al. Assessing parents’ attitudes towards ketogenic dietary therapies. Epilepsy Behav. 2014;39(39):1–5. doi: 10.1016/j.yebeh.2014.07.020. [DOI] [PubMed] [Google Scholar]
- 17.Richardson J, Iezzi A, Khan MA, Maxwell A. Validity and reliability of the Assessment of Quality of Life (AQoL)-8D multi-attribute utility instrument. Patient. 2014;7(01):85–96. doi: 10.1007/s40271-013-0036-x. [DOI] [PMC free article] [PubMed] [Google Scholar]