

Highlights
-
•
The COVID-19 pandemic suppressed fertility desires among US women.
-
•
Impacts on fertility preferences persisted from summer 2020 to early 2021.
-
•
The fertility preferences of younger women, women of color and those facing financial stress were most impacted.
Keywords: Fertility, Reproduction, United States, Childbearing, Women
Abbreviations: aOR, Adjusted Odds Ratio; aRRR, Adjusted Relative Risk Ratio; US, United States
1. Background
The COVID-19 pandemic was accompanied by a decrease in births in the United States (US) between 2019 and 2020, with evidence of a small rebound between 2020 and 2021 that remained below pre-pandemic levels (Hamilton, 2022). This depression has been explained in part by evidence of early changes in fertility plans driven by the pandemic. In the spring of 2020, one-third of cisgender US women reported wanting children later or wanting fewer children because of the pandemic (Lindberg et al., 2020). Another study found that one-third of US individuals who were trying to conceive at the onset of the pandemic had changed their fertility preferences by the summer of 2020 (Naya et al., 2021). In New York City, a cross-sectional survey of women with young children conducted between April and August of 2020 found that half of those previously trying to or planning to conceive were no longer doing so (Kahn et al., 2021).
Although these studies have described changing fertility preferences after the pandemic began, inadequate attention has been paid to disparities in the impact of the pandemic on people's childbearing plans. In Spring 2020, suppressed fertility preferences during the pandemic were more common among those who face the most structural oppression: women of color, and women living on lower incomes (Lindberg et al., 2020). Evidence on changes in fertility during the pandemic has shown that while births among white and Latina women largely rebounded between 2020 and 2021, birth rates continued to fall for Black, American Indian/Native American, and Asian women (Hamilton, 2022). Such disparities may drive longer-term inequities in fertility outcomes, compounding the existing unequal health and socio-economic impacts of the pandemic. Understanding how and for whom fertility preferences have changed is key to contextualizing whether newly documented changes in birth rates during the pandemic are attributable to fertility preferences or to disruptions in access to reproductive health services.
Few studies have examined the impact of COVID-19 on fertility preferences beyond 2020. Lindberg et al. found that in Summer 2021, when lockdowns were less common and COVID-19 vaccines were readily available, only 22% of US women said the pandemic changed their fertility preferences—a sharp decline from 41% in May 2020, suggesting the pandemic may have depressed childbearing intentions only temporarily (Lindberg et al., 2021). The authors found that the pandemic continued to have suppressive effects on the fertility preferences of: people of color; sexual and gender minority respondents; people living on lower incomes; and people who experienced economic disruptions. Despite this evidence, there is little understanding of how preferences changed within individuals over the course of the pandemic, as fertility preferences have likely evolved as the pandemic has progressed. Rocca et al. is one exception. This study found that trends towards a greater desire for pregnancy over time were interrupted by the pandemic among a sample of people aged 15–34 years in the US Southwest between March 2019 and March 2021 (Rocca et al., 2022). The authors found that the pandemic's dampening of desire for pregnancy was stronger among those younger and earlier in their reproductive life course. For some groups of women, pandemic-related impacts may have persisted and compounded, especially among populations that were hit hardest by financial and employment difficulties.
Although an investigation of within-individual changes in fertility patterns provides critical information regarding the effect of the pandemic, opportunities to study fertility dynamics are rare. Here, we capitalize on one of the few national longitudinal data sources in the US to understand how the pandemic's initial impact on fertility preferences evolved over time and how these patterns differed across a diverse sample of US women using a cohort surveyed in July 2020 and January 2021.
2. Theoretical framework: COVID-19 and fertility preferences
Fertility preferences respond to changing economic situations at the individual, household, and societal levels (Comolli, 2017; Trinitapoli & Yeatman, 2018). Past large-scale economic uncertainty has been associated with downward shifts in fertility preferences—both a desire to delay the timing of future childbearing and suppression of overall desired fertility—in the short and longer-term. Pandemics, such as COVID-19, increase economic insecurity due to job or income loss, impact people's ability to balance work and childcare, and engender a sense of fear around bringing a child into an uncertain world. These crises introduce additional uncertainty into fertility decision-making due to potential impacts on maternal health and wellbeing, as well as the potential health of a fetus, especially earlier in the pandemic when the biological effects of COVID-19 on pregnancy where unknown. In a pandemic, people may thus choose to delay childbearing due to fears of the virus' health impacts, pandemic-related economic stressors, or other uncertainties that are perceived to be short-term, or they may change their overall fertility preferences, resulting in an increased or decreased desire for children, due to perceived longer-term factors or uncertainties.
Because childbearing determinants differ across demographic characteristics, any impact of the pandemic on fertility should be assessed for potential heterogeneous effects across the population. Further, because existing structural inequities and health disparities have been exacerbated in previous phases of economic uncertainty and crisis, we might expect differential impacts on fertility preferences by socioeconomic position and race/ethnicity.
3. Hypotheses
Based on prior literature, we aimed to test the following hypotheses:
-
•
H1: Women of color will be more likely to have a sustained desire to delay or decrease childbearing due to the pandemic compared to white women.
-
•
H2: Women with a previous birth will be more likely to have a sustained desire to delay or decrease childbearing due to the pandemic compared to those with no previous births at baseline.
-
•
H3: Women with lower household income levels will be more likely to have a sustained desire to delay or decrease childbearing due to the pandemic compared to those with higher household income levels.
-
•
H4: Women who experience COVID-19-related income loss in July 2020 will be more likely to have a sustained desire to delay or decrease childbearing due to the pandemic compared to those who do not experience COVID-19-related income loss.
4. Methods
4.1. Study population, setting, and data collection
Our analysis is part of a broader study of women's experiences with sexual and reproductive health services during the COVID-19 pandemic. We recruited our sample using Facebook and Instagram advertisements over one week in July 2020, as described in more detail elsewhere (Diamond-Smith et al., 2021). Eligible respondents identified as women, lived in the US, were 18–45 years old, and provided informed consent. At the end of the five-minute survey, respondents were asked to provide contact information if they were interested in participating in a follow-up survey. The follow-up survey was sent by email in January 2021, and those who completed both surveys received a $10 gift card by e-mail. To ensure data quality, we dropped baseline surveys from the same IP address, those completed in less than 60 seconds, and incomplete surveys. Since only women who answered both the baseline and follow-up surveys are included in our cohort, and because participants were contacted via email for the follow-up survey, we have a high degree of confidence that responses are from actual individuals. De-identified data were recorded in Qualtrics and stored on a secure network. The study received ethical approval from the University of California Institutional Review Board (#20-30994).
The baseline sample in July 2020 included 4,645 women; 3,186 (69%) completed the follow-up survey (Fig. 1). Since we were interested in changes in fertility preferences, we excluded participants who reported that they or their partner were sterilized at baseline (n = 119) and those who were pregnant at baseline (n = 862). We also excluded those whose responses to the select-all-that-apply fertility preference outcome at baseline or follow-up were missing or reported as “other”, and those who endorsed multiple response options to our fertility preference outcome that were contradictory (e.g., reporting both an increased and decreased desire for a child at either survey) (n = 118). This resulted in an analytic sample of 2,087 women.
Fig. 1.

Study Exclusion Criteria.
4.2. Measures
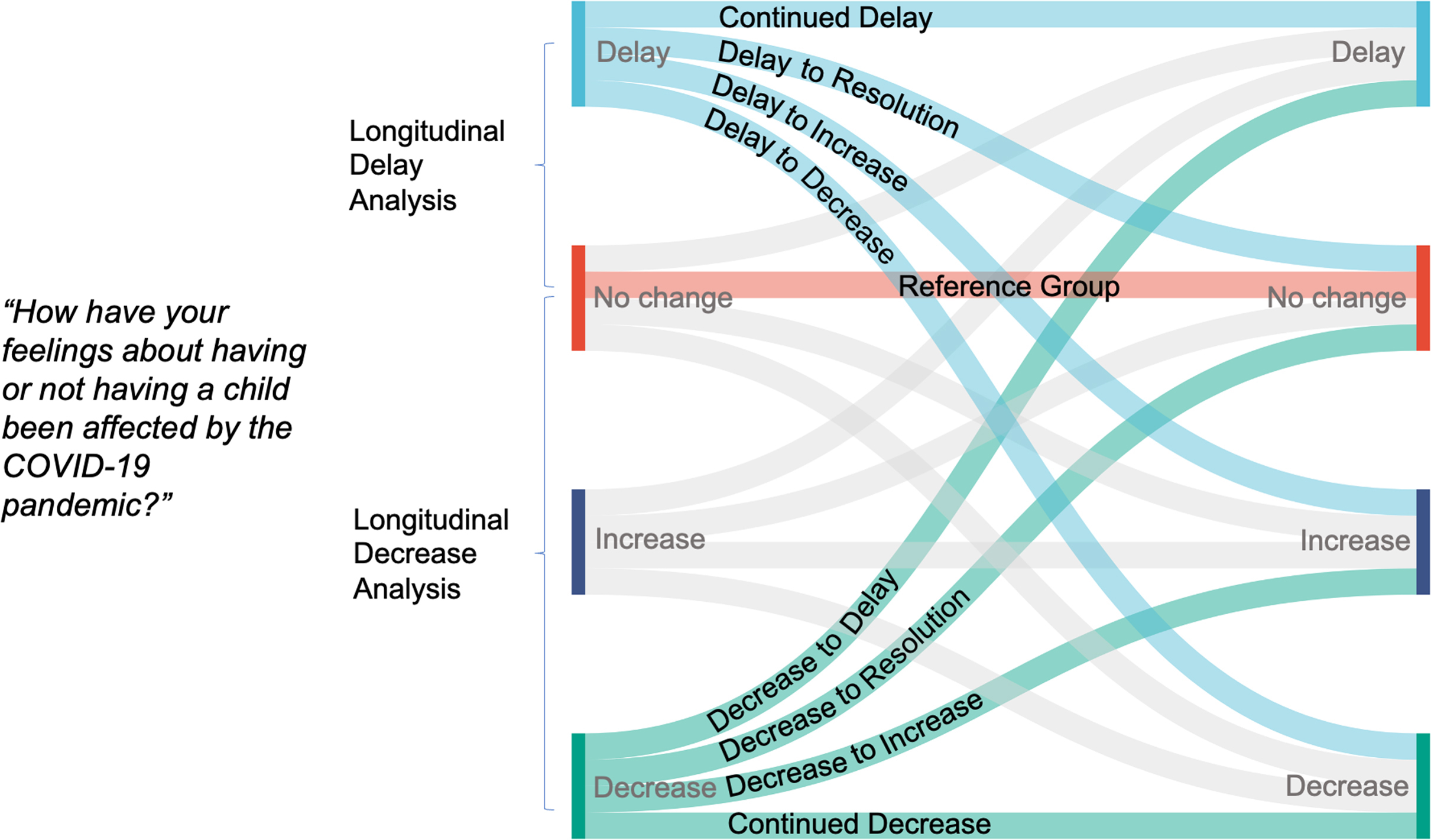
Our fertility preference outcomes were measured at both baseline and follow-up using a single select-all-that-apply item with the following prompt: “How have your feelings about having or not having a child been affected by the COVID-19 pandemic?” Participants could indicate whether the pandemic had: not changed how they felt about having a/another child; caused them to want to delay having a/another child; decreased their desire to have a/another child; increased their desire to have a/another child; or other. For our analysis, we categorized participants into four outcomes at each survey: no change, delay, decrease, or increase.
Our first set of dependent variables included three binary variables reflecting fertility preferences measured at baseline in July 2020: delay vs. no change; decrease vs. no change; and increase vs. no change. Because some participants (n = 204 at baseline) selected multiple responses (i.e., preferences to both increase and delay), some respondents were included in multiple measures.
Our second set of dependent variables measured changes in fertility preferences between July 2020 and January 2021. Here, we were interested in patterns in two groups: those who initially reported a preference to delay at baseline and those who initially reported a decreased desire to have a child at baseline. For these variables, participants who reported both a preference to delay and any other fertility preferences during either survey were categorized as having a preference to delay.
For the longitudinal analyses conducted among participants whose baseline preferences were to either delay having a child due to the pandemic or a decreased desire for childbearing due to the pandemic, we created two categorical variables to reflect changes in fertility preferences over time. The first compared changes over time among the group that preferred to delay childbearing due to the pandemic at baseline (delay to “resolution”, continued preference to delay, delay to decrease, and delay to increase) to a reference group of those whose fertility preferences were not impacted by the pandemic at both surveys. The second compared changes over time among the group that preferred to decrease childbearing due to the pandemic at baseline (decrease to “resolution”, sustained decrease, decrease to delay, and decrease to increase) to a reference group of those whose fertility preferences were not impacted by the pandemic at both surveys. The trajectories depicted in these variables are depicted in Figure A1.
Baseline covariates are outlined in detail in Table 1. Sociodemographic covariates included: respondent age; education; race/ethnicity; annual household income; parity; and partnership status. We included two COVID-related predictors in our models: whether the participant reported losing income due to the pandemic and the number of COVID-19 public health measures in place where the participants resided at the time of the baseline. Missing values were minimal (<1%), and therefore we imputed covariates at their mean (for numeric variables) or mode (for categorical variables), except for race/ethnicity, where missing responses were categorized as multiracial, Indigenous, other, or unknown.
Table 1.
Sample description overall and by baseline fertility preference (n = 2,087).
| Overall | Baseline fertility preference |
|||||
|---|---|---|---|---|---|---|
| No change | Desire to delay having a child | Decreased desire for a child | Increased desire for a child | |||
| N | 2,087 | 946 | 592 | 641 | 118 | |
| Age, mean (SD) | 30.2 (6.5) | 30.2 (7.0) | 29.4 (5.6) | 30.1 (6.5) | 31.2 (6.0) | |
| Race/ethnicity | White | 62.1% | 63.2% | 56.2% | 60.8% | 66.9% |
| Black or African American | 4.9% | 4.5% | 6.2% | 4.7% | 5.9% | |
| Asian or Pacific Islander | 13.5% | 16.5% | 12.5% | 11.9% | 3.4% | |
| Latina | 10.2% | 7.8% | 14.2% | 11.9% | 8.5% | |
| Multiracial, Indigenous, Other, or Unknown | 9.3% | 7.9% | 10.8% | 10.8% | 15.3% | |
| Education | Less than college | 31.8% | 32.6% | 31.2% | 32.4% | 30.5% |
| College or more | 68.2% | 67.4% | 68.8% | 67.6% | 69.5% | |
| Annual household income | <$25,000 | 16.2% | 16.9% | 16.7% | 17.5% | 15.3% |
| $25,000 - $49,999 | 18.8% | 18.0% | 18.2% | 19.7% | 17.8% | |
| $50,000 - $99,999 | 37.7% | 37.5% | 37.7% | 36.2% | 38.1% | |
| ≥$100,000 | 27.3% | 27.6% | 27.4% | 26.7% | 28.8% | |
| Parity | Nulliparous | 47.6% | 51.0% | 46.6% | 44.9% | 51.7% |
| 1 birth | 24.3% | 19.7% | 31.8% | 23.2% | 27.1% | |
| ≥2 births | 28.0% | 29.2% | 21.5% | 31.7% | 21.2% | |
| Partnership status | Not living with partner | 30.9% | 36.6% | 25.5% | 30.1% | 21.2% |
| Living with partner | 69.1% | 63.4% | 74.5% | 69.9% | 78.8% | |
| No | 56.4% | 61.8% | 51.2% | 52.4% | 45.8% | |
| Yes | 43.6% | 38.2% | 48.8% | 47.6% | 54.2% | |
| Number of COVID-19 restrictions in place (0-10), mean (SD) a | 5.1 (2.0) | 4.9 (2.0) | 5.3 (2.0) | 5.2 (2.1) | 5.1 (2.2) | |
– Types of COVID-19 related restrictions: social or physical distancing, masks required in public spaces, stay at home order, shelter in place, curfew, ban on non-essential gatherings, ban on large groups, restrictions on bars, restaurants, theaters, school closures, or recommended working from home.
4.3. Analysis
First, we described frequencies and proportions of participant characteristics overall, and by fertility preferences at baseline in July 2020. Second, we used multivariable logistic regression to identify correlates of each binary baseline fertility preference measured in July 2020. Third, we used multivariable multinomial logistic regression to identify correlates of longitudinal patterns of fertility preferences. We used two different dependent variables for these analyses based on whether respondents initially reported a preference for delayed or decreased childbearing. We also examined the baseline fertility preferences of women who were pregnant at the time of the follow-up survey. We used Stata version 17.0 (College Station, TX) for all analyses.
5. Results
The 2,087 participants in our sample were on average 30 years old. Most respondents (62%) were white. Two-thirds (68%) had completed college or more education, 48% were nulliparous, and 27% had an annual household income of over $100,000. Just under half (44%) reported lost income due to pandemic-related work changes as of July 2020. Table 1 provides more details on sample characteristics.
In July 2020, 44% of women said their fertility preferences were not impacted by the pandemic, 28% preferred to delay having a child, 23% said that the pandemic had decreased their desire to have a child, and 5% indicated an increased desire to have a child because of the pandemic (Fig. 2). In January 2021, 50% indicated that their preference for a child was not impacted by the pandemic, 24% indicated a preference to delay, 22% expressed a decreased desire, and 5% indicated an increased desire for a child due to the pandemic. Among women who reported a preference to delay having a child (N = 592) or a decreased desire (N = 476) to have a child in July 2020, two-thirds (N = 722, 68%, Appendix Table 1) still reported a desire to postpone or decrease childbearing due to the pandemic by January 2021. Meanwhile, desires to delay or decrease childbearing had transitioned into no impact of the pandemic on fertility preferences for a little over a quarter of women (N = 307, 29%) in the group that preferred to delay or decrease childbearing at baseline.
Fig. 2.

Changes in fertility preferences due to COVID-19 between July 2020 and January 2021 (n = 2,087).
Next, we compared the factors associated with each July 2020 fertility preference (delay, decrease, and increase) with the group that reported no change at baseline (Table 2). Participants who expressed a preference to delay or decrease childbearing were younger than those who reported no change in fertility preferences due to the pandemic at baseline. We also found differences in fertility preferences by race/ethnicity; Latina women, Black women, and women who reported a multiracial, Indigenous, other, or unknown race/ethnicity were more likely to report a preference to delay childbearing compared to white women. Latina women were more likely to express a decreased desire for a child than white women, and white women were more likely than Asian women to have an increased desire for a child. Women who identified as multiracial, Indigenous, other, or unknown race/ethnicities were more likely to report an increased desire for a child than white women. Income loss due to COVID-19 was associated with higher odds of all three forms of changes in fertility preferences due to the pandemic. Compared to women with one birth, nulliparous women were less likely to have either a decreased desire for or a desire to delay childbearing, and those with two or more births were less likely to experience an increased desire for or a desire to delay having a child due to the pandemic. Living with a partner was associated with greater odds of experiencing decreased or delayed fertility preferences due to the pandemic. Women who lived in areas with more pandemic restrictions were more likely to report a baseline preference to delay or decrease childbearing.
Table 2.
Results of logistic regression models examining associations between selected respondent characteristics and fertility preferences due to COVID-19 in July 2020.
| Decrease (n = 1564) |
Delay (n = 1513) |
Increase (n = 1054) |
||||
|---|---|---|---|---|---|---|
| aOR | 95% CI | aOR | 95% CI | aOR | 95% CI | |
| Age (continuous, scaled in 5-year intervals, centered at mean) | 0.88* | 0.80–0.97 | 0.79*** | 0.71–0.88 | 1.07 | 0.90–1.27 |
| Race/ethnicity | ||||||
| White | ref | |||||
| Black | 1.17 | 0.70–1.96 | 2.13** | 1.29–3.51 | 1.67 | 0.70–4.00 |
| Asian or Pacific Islander | 0.80 | 0.58–1.11 | 0.97 | 0.70–1.36 | 0.21** | 0.07–0.59 |
| Latina | 1.50* | 1.05–2.14 | 2.26*** | 1.56–3.27 | 1.00 | 0.48–2.08 |
| Multiracial, Alaska Native, Native American, Other, or Unknown | 1.45* | 1.01–2.09 | 1.76** | 1.20–2.59 | 2.05* | 1.13–3.72 |
| Education | ||||||
| Less than college | ref | |||||
| College or more | 1.18 | 0.92–1.51 | 1.20 | 0.92–1.55 | 1.02 | 0.63–1.64 |
| Household income | ||||||
| <$25,000 | ref | |||||
| $25,000 - $49,999 | 1.02 | 0.72–1.45 | 1.00 | 0.69–1.46 | 1.00 | 0.50–2.01 |
| $50,000 - $99,999 | 0.88 | 0.64–1.22 | 0.96 | 0.68–1.36 | 0.93 | 0.49–1.79 |
| ≥$100,000 | 0.93 | 0.66–1.32 | 1.02 | 0.70–1.48 | 1.21 | 0.60–2.43 |
| Parity | ||||||
| 1 birth | ref | |||||
| Nulliparous | 0.71* | 0.53–0.97 | 0.55*** | 0.40–0.74 | 1.15 | 0.68–1.95 |
| ≥2 births | 0.92 | 0.69–1.23 | 0.45*** | 0.33–0.61 | 0.46** | 0.26–0.82 |
| Partnership Status | ||||||
| Not living with partner | ref | |||||
| Living with partner | 1.06* | 1.01–1.12 | 1.10*** | 1.04–1.16 | 1.04 | 0.94–1.16 |
| Lost income due to COVID-19 | ||||||
| No | ref | |||||
| Yes | 1.49*** | 1.21–1.84 | 1.62*** | 1.30–2.02 | 2.02*** | 1.35–3.02 |
| Number of COVID restrictions in place, July 2020 a | 1.32* | 1.02–1.72 | 2.10*** | 1.58–2.79 | 2.36** | 1.39–3.98 |
* - p < 0.05 ** - p < 0.01 *** - p < 0.001.
– Types of COVID-19 related restrictions: social or physical distancing, masks required in public spaces, stay at home order, shelter in place, curfew, ban on non-essential gatherings, ban on large groups, restrictions on bars, restaurants, theaters, school closures, or recommended working from home.
Next, we turned to longitudinal analyses of fertility preferences, examining changes between July 2020 and January 2021. Among the 592 participants who preferred to delay having a child due to the pandemic in July 2020, half continued to prefer to delay having a child by January 2021 (Fig. 2). One-fourth reported a preference to delay having a child at baseline but reported no impact of COVID-19 on their desire for a child at follow-up, and 19% had their baseline preference to delay having a child translate into a decreased desire for a child 6 months later. Less than 5% had an increased desire for a child at follow-up. When we examined the 476 participants who indicated a decreased desire to have a child at baseline, we found that 46% had a continued decreased desire for a child in January 2021 and 31% indicated that the pandemic did not impact their desire for a child at follow-up. Meanwhile, 21% of those who initially experienced a decreased desire for a child preferred to delay childbearing at follow-up, and 3% had an increased desire for a child at follow-up.
In adjusted multinomial models that compared each of the baseline delay groups to the reference group of no change at either survey, we found that younger women, Latina women, those who had completed college or more education, women with one child (compared to nulliparous women), and those living in areas with more pandemic restrictions in place had higher risks of reporting a continued preference to delay having a child (Table 3). Compared to white women, we found that Black women, Latina women, and women who were multiracial, Indigenous, another, or unknown race/ethnicity, had a higher risk of their baseline delay translating to a decreased desire to have a child at follow-up compared to white women. In addition, women living with a partner and those who had lost income due to COVID-19 at baseline had higher risks of reporting a decreased desire to have a child at follow-up.
Table 3.
Results from multinomial regression models examining associations between selected respondent characteristics and longitudinal changes in fertility preferences due to COVID-19 between July 2020 and January 2021 among participants who had desired to delay childbearing in July 2020 (n = 1,300).
| No change | Delay to Resolution |
Continued Delay |
Delay to Decrease |
Delay to Increase |
|||||
|---|---|---|---|---|---|---|---|---|---|
| aRRR | 95% CI | aRRR | 95% CI | aRRR | 95% CI | aRRR | 95% CI | ||
| Age (continuous, scaled in 5-year intervals, centered at mean) | 0.82* | 0.69–0.97 | 0.71*** | 0.62–0.83 | 0.89 | 0.74–1.07 | 0.75 | 0.50–1.11 | |
| Race/ethnicity | |||||||||
| White | ref | ||||||||
| Black | 2.18* | 1.02–4.67 | 2.02 | 0.97–4.21 | 2.91* | 1.22–6.94 | 7.01** | 1.94–25.41 | |
| Asian or Pacific Islander | 0.71 | 0.40–1.26 | 0.84 | 0.53–1.33 | 1.55 | 0.84–2.85 | 1.50 | 0.49–4.60 | |
| Latina | 2.39** | 1.31–4.35 | 3.34*** | 2.01–5.57 | 3.81*** | 1.96–7.39 | 2.80 | 0.73–10.80 | |
| Multiracial, Alaska Native, Native American, Other, or Unknown | 1.09 | 0.57–2.07 | 1.61 | 0.96–2.70 | 3.13*** | 1.69–5.78 | 0.70 | 0.09–5.62 | |
| Education | |||||||||
| Less than college | ref | ||||||||
| College or more | 0.74 | 0.49–1.12 | 1.60* | 1.11–2.30 | 1.19 | 0.74–1.92 | 2.50 | 0.87–7.20 | |
| Household income | |||||||||
| <$25,000 | ref | ||||||||
| $25,000 - $49,999 | ref | 1.12 | 0.61–2.04 | 0.84 | 0.49–1.43 | 1.37 | 0.71–2.65 | 0.62 | 0.18–2.13 |
| $50,000 - $99,999 | 0.94 | 0.53–1.66 | 0.85 | 0.53–1.37 | 0.99 | 0.52–1.86 | 0.29* | 0.09–0.96 | |
| ≥$100,000 | 1.28 | 0.70–2.35 | 0.81 | 0.48–1.35 | 0.81 | 0.39–1.65 | 0.36 | 0.10–1.25 | |
| Lost income due to COVID-19 | |||||||||
| No | ref | ||||||||
| Yes | 1.51* | 1.06–2.17 | 1.58** | 1.17–2.13 | 1.98** | 1.31–2.98 | 1.40 | 0.62–3.19 | |
| Parity | |||||||||
| 1 birth | ref | ||||||||
| Nulliparous | 1.01 | 0.59–1.70 | 0.41*** | 0.28–0.61 | 0.87 | 0.48–1.57 | 0.40 | 0.15–1.07 | |
| ≥2 births | 1.00 | 0.60–1.65 | 0.23*** | 0.15–0.36 | 0.74 | 0.41–1.33 | 0.11** | 0.02–0.54 | |
| Partnership Status | |||||||||
| Not living with partner | ref | ||||||||
| Living with partner | 2.02** | 1.27–3.22 | 2.84*** | 1.91–4.21 | 1.71* | 1.02–2.86 | 2.43 | 0.88–6.73 | |
| Number of COVID restrictions in place, July 2020 a | 1.11* | 1.02–1.22 | 1.18*** | 1.09–1.28 | 1.00 | 0.90–1.11 | 1.17 | 0.95–1.44 | |
* - p < 0.05 ** - p < 0.01 *** - p < 0.001.
– Types of COVID-19 related restrictions: social or physical distancing, masks required in public spaces, stay at home order, shelter in place, curfew, ban on non-essential gatherings, ban on large groups, restrictions on bars, restaurants, theaters, school closures, or recommended working from home.
Compared to those who did not experience a change in fertility preferences at both baseline and follow-up, Latina women and women who identified as multiracial, Indigenous, other, or whose race/ethnicity was unknown, younger women, those who were nulliparous or had two or more children, women living with a partner, and those who had lost income because of the pandemic were more likely to have their baseline decreased desire for a child change to a preference to delay in January 2021 (Table 4). Participants who had a baseline decreased desire for a child were more likely to maintain a decreased desire for childbearing six months later if they: were Latina; had one child; experienced income loss at baseline due to the pandemic; or lived in an area with more pandemic restrictions in place.
Table 4.
Results from multinomial regression models examining associations between selected respondent characteristics and longitudinal changes in fertility preferences due to COVID-19 between July 2020 and January 2021 among participants who had a decreased desire for childbearing in July 2020 (n = 1353).
| No change | Decrease to Resolution |
Decrease to delay |
Continued Decrease |
Decrease to Increase |
|||||
|---|---|---|---|---|---|---|---|---|---|
| aRRR | 95% CI | aRRR | 95% CI | aRRR | 95% CI | aRRR | 95% CI | ||
| Age (continuous, scaled in 5-year intervals, centered at mean) | 0.95 | 0.82–1.11 | 0.77** | 0.66–0.91 | 0.91 | 0.79–1.04 | 0.81 | 0.52–1.27 | |
| Race/ethnicity | |||||||||
| White | ref | ||||||||
| Black | 0.68 | 0.25–1.83 | 1.72 | 0.76–3.89 | 1.39 | 0.69–2.81 | 2.34 | 0.27–20.14 | |
| Asian or Pacific Islander | 0.80 | 0.48–1.31 | 0.91 | 0.54–1.55 | 0.63 | 0.38–1.04 | 1.43 | 0.42–4.90 | |
| Latina | 1.28 | 0.68–2.41 | 2.62*** | 1.48–4.65 | 2.10** | 1.27–3.48 | 2.14 | 0.44–10.26 | |
| Multiracial, Alaska Native, Native American, Other, or Unknown | 0.94 | 0.51–1.74 | 2.02* | 1.18–3.47 | 1.29 | 0.78–2.13 | 0.78 | 0.10–6.24 | |
| Education | |||||||||
| Less than college | ref | ||||||||
| College or more | 1.13 | 0.76–1.69 | 1.17 | 0.78–1.74 | 1.23 | 0.87–1.75 | 1.74 | 0.50–6.00 | |
| Household income | |||||||||
| <$25,000 | ref | ||||||||
| $25,000 - $49,999 | ref | 0.90 | 0.51–1.61 | 0.85 | 0.49–1.49 | 1.15 | 0.70–1.89 | 1.31 | 0.21–8.34 |
| $50,000 - $99,999 | 0.79 | 0.46–1.33 | 0.72 | 0.43–1.20 | 0.82 | 0.51–1.32 | 1.36 | 0.26–7.09 | |
| ≥$100,000 | 0.95 | 0.54–1.65 | 0.71 | 0.40–1.23 | 0.86 | 0.51–1.43 | 1.15 | 0.20–6.77 | |
| Lost income due to COVID-19 | |||||||||
| No | ref | ||||||||
| Yes | 1.18 | 0.84–1.66 | 1.67** | 1.19–2.36 | 1.80*** | 1.34–2.43 | 0.60 | 0.21–1.71 | |
| Parity | |||||||||
| 1 birth | ref | ||||||||
| Nulliparous | 1.28 | 0.75–2.20 | 0.59* | 0.37–0.93 | 0.60* | 0.38–0.93 | 1.39 | 0.38–5.09 | |
| ≥2 births | 1.64 | 0.99–2.72 | 0.34*** | 0.20–0.56 | 1.03 | 0.69–1.53 | 0.91 | 0.23–3.54 | |
| Partnership Status | |||||||||
| Not living with partner | ref | ||||||||
| Living with partner | 1.16 | 0.76–1.78 | 1.87** | 1.22–2.86 | 1.24 | 0.85–1.82 | 3.62* | 1.02–12.84 | |
| Number of COVID restrictions in place, July 2020 a | 1.07 | 0.98–1.16 | 1.05 | 0.97–1.14 | 1.09* | 1.01–1.17 | 1.06 | 0.84–1.33 | |
* - p < 0.05 ** - p < 0.01 *** - p < 0.001.
– Types of COVID-19 related restrictions: social or physical distancing, masks required in public spaces, stay at home order, shelter in place, curfew, ban on non-essential gatherings, ban on large groups, restrictions on bars, restaurants, theaters, school closures, or recommended working from home.
We then examined the July 2020 pregnancy preferences of the 97 women who were pregnant at the January 2021 survey but not in July 2020. Most (37%) had reported no impact of COVID-19 on their pregnancy preferences at baseline. Meanwhile, one-third (32%) had reported a desire to delay pregnancy at baseline. Smaller proportions indicated an increased (24%) or decreased (7%) desire to have a child in July 2020.
6. Discussion
In this longitudinal study, we found that the COVID-19 pandemic impacted the fertility preferences of many women in our sample, with evidence of sustained shifts in fertility preferences for some women between the summer of 2020 and winter of 2021. We found that most women (68%) who initially experienced a reduced desire for childbearing in the summer of 2020 continued to feel that way six months later, suggesting that the pandemic could have long-lasting impacts on fertility.
This study aimed to examine inequities in fertility preference trajectories over the first year of the pandemic. Our results revealed two divergent experiences. In the first, 43% of women in our sample experienced no impact of the pandemic on their fertility plans–a proportion that increased to nearly half by the follow-up survey. Women whose fertility preferences were not impacted by the pandemic in July 2020 were more likely to be older, white, nulliparous, have two or more children, and not cohabiting with a partner. They were less likely to have experienced financial hardship due to the pandemic and more likely to have lived in areas with fewer pandemic restrictions.
On the other hand, about half of women surveyed at baseline and again six months later expressed a decreased desire to have a child or wanted to delay childbearing until a later point. These women's experiences align with existing evidence that demonstrates that people prefer not to have a child during times of economic crisis or epidemics (Sobotka et al., 2011; Vrachnis et al., 2014). These women were disproportionately younger, women of color, those who experienced recent income loss, and women who were parenting one child.
Elevated rates of COVID-19 infection and death (Riley et al., 2021), job loss (The Employment Situation, 2021), and intensified tension around racial injustice are likely to contribute to these concentrated impacts of the pandemic on women of color. We found divergent effects of the pandemic on women based on their partnership and family structures. Women with one child were more likely than nulliparous women or women with two or more children to have a continued preference to decrease or delay childbearing. This may reflect a lesser impact of the pandemic on the fertility preferences of women who are not yet considering childbearing or who had decided to forego childbearing as women who already had a child were navigating challenges of school closures, loss of family and social support, and increased emotional and mental distress (Brown et al., 2020; Calvano et al., 2021; Russell et al., 2020; Taubman-Ben-Ari et al., 2021; Weeland et al., 2021). Meanwhile, women with two or more children may have been less susceptible to the pandemic's impact on fertility preferences because they have already completed childbearing. This finding suggests that the pandemic may have decreased preferred family size for women who were parenting one child, compared to those with two or more children (Hartnett & Gemmill, 2020). Women living with a partner were more likely to experience shifts towards delaying or decreasing childbearing, perhaps because cohabiting women were more concretely considering their childbearing options than those not living with a partner (Bachrach & Morgan, 2013; Hashemzadeh et al., 2021; Pietromonaco & Overall, 2021). In addition, the pandemic was documented to have disrupted partnership quality and status for many couples, which may have influenced fertility intentions (Jones et al., 2021; Luetke et al., 2020).
Contrary to our hypotheses, we did not find an association between income level and changes in fertility preferences. However, women who lost income due to the pandemic were more likely to experience suppressed childbearing preferences because of to the pandemic. This finding echoes prior evidence about the impact of financial insecurity on suppressing people's childbearing plans and their fertility, both preceding and during the pandemic (Geist et al., 2021; Kahn et al., 2021; Lin et al., 2021). It also suggests that perceptions of financial insecurity and hardship may be more strongly linked to changes in fertility preferences than absolute income level (Vignoli et al., 2020).
Recent evidence has suggested that an initial suppression in fertility preferences and births due to the pandemic rebounded as people adjusted to the pandemic and resumed their prior plans (Hamilton, 2022; Rocca et al., 2022). Among women in our sample who wanted to delay or postpone childbearing at baseline, two-thirds did not experience a rebound in their fertility preferences, and instead continued to prefer to decrease or delay childbearing in January 2021. Again, these sustained preferences to decrease or delay childbearing because of the pandemic were more common among younger women, women of color, those experiencing income loss, and those already parenting, as well as among more educated women. Our results reveal important and sustained inequities in the suppressive effects of the pandemic on fertility preferences that fall disproportionately on the women who already face the greatest challenges in actualizing their reproductive goals. These unequal effects are likely to further drive longstanding reproductive inequities in the US. While prior research has demonstrated inequities in the effects of widescale shocks on fertility (Berberian et al., 2022; Seltzer & Nobles, 2017), our research is among the first to our knowledge to highlight the longitudinal inequities in the impact of the COVID-19 pandemic on fertility across the US.
These shifts in fertility preferences highlight family planning and abortion needs among those for whom the pandemic has caused a decreased desire for children. It also signals shifting maternal and fertility care needs among the people for whom the pandemic has caused a sustained desire to delay childbearing. These changes are particularly important in light of pandemic-related disruptions in and widespread legal restrictions on access to abortion and other forms of sexual and reproductive health care in the US, most critically the US Supreme Court's overturning of Roe v. Wade in June 2022 (Diamond-Smith et al., 2021).
When we examined the July 2020 fertility preferences of the women who had later become pregnant, we found that nearly a third had indicated a desire to delay childbearing in the summer of 2020, suggesting that the extended duration of the pandemic may have led those who initially intended to delay childbearing to resume their fertility plans by the winter of 2021. While we were not able to identify the intendedness of all pregnancies, disruptions in access to reproductive health services may have led to unintended pregnancies. While a small subsample, this evidence can provide insight into how trends in birth rates may rebound over time during the COVID-19 pandemic.
This paper contributes to the literature by following a cohort of women over time from across the US to understand the impact of COVID-19 on fertility preferences, a strength given the existing literature is mostly narrow in geographic focus and cross-sectional. However, there are several limitations. While social media platforms allowed us to collect data quickly, inexpensively, and from a dispersed geographic sample during a global crisis, this may limit the external validity of our sample, which had lower proportions of Black and Latina respondents and greater proportions of respondents with higher levels of education and income than the US overall (Schneider & Harknett, 2022). Our recruitment script asked respondents to self-identify as women; thus, our results are not informative about the experiences of individuals with other gender identities. The survey did not capture sexual orientation; therefore we were unable to explore its impact on fertility preferences.
Additionally, we lacked a pre-pandemic baseline measurement of fertility preferences. Therefore, our outcomes of interest asked respondents for their perceptions of how the pandemic had influenced their fertility preferences. Participants may have mistakenly attributed other changes in preferences to the pandemic, so their responses in the survey may have reflected stressors or other factors beyond the pandemic that influence their fertility preferences. This may have overestimated the proportion of the sample who reported any impact of the pandemic on their fertility preferences. Further, participants may not have accurately recalled their pre-pandemic fertility desires. However, other research that included pre-pandemic measurements of fertility preferences, and that looked at changes in preferences during the pandemic, have demonstrated similar patterns, bolstering the validity of our findings (Lindberg et al., 2021; Rocca et al., 2022). Our analysis may also be limited by differences in interpretation regarding the survey response options for delayed versus decreased fertility preferences and the lack of a validated measure of the impact of COVID-19 on fertility preferences. Future analyses should explore a range of changes in fertility timing and overall desired number of children due to the pandemic, including how other factors contribute to changes in fertility preferences that are perceived to be due to the pandemic.
7. Implications for public health
Our findings suggest that the impact of the COVID-19 pandemic on fertility preferences in the US has been sustained over time, and the pandemic has disproportionately impacted populations that already face major structural inequities. As the effects of the pandemic persist, and in the face of the next crisis, it is critical that healthcare resources, including abortion access, family planning, maternal health, and fertility care, are directed to populations most at risk of long-term consequences.
Ethical statement
This study received ethical approval from the University of California, San Francisco Institutional Review Board.
Author statement
Koenig: Conceptualization, Methodology, Data Analysis, Writing – Original Draft Smith Hughes: Conceptualization, Methodology, Writing, Reviewing and Editing Gemmill: Reviewing and Editing Diamond-Smith: Data curation, Supervision, Methodology, Reviewing and Editing.
Acknowledgements
The authors would like to thank the co-Principal Investigator Jennifer Kerns, co-Investigators Rachel Logan and Cassondra Marshall for the overall study. We appreciate research support from Aliza Adler and Sirena Gutierrez. Ms. Koenig is funded by a training grant from the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Number T32MD015070. Dr. Gemmill is supported by a grant from the National Institute of Child Health and Human Development and the Johns Hopkins University Population Center (P2CHD042854). The authors appreciate support from The Commonwealth Fund (20213165), Stan and Mary Friedman, and the University of California, San Francisco Department of Epidemiology and Biostatistics.
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ssmph.2022.101305.
Appendix A. Supplementary data
The following are the Supplementary data to this article:
{kind=link}
Data availability
The authors do not have permission to share data.
References
- Bachrach C.A., Morgan S.P. A cognitive-social model of fertility intentions. Population and Development Review. 2013;39(3):459–485. doi: 10.1111/j.1728-4457.2013.00612.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berberian A.G., Gonzalez D.J.X., Cushing L.J. Racial disparities in climate change-related health effects in the United States. Curr Environ Health Rep. 2022;9(3):451–464. doi: 10.1007/s40572-022-00360-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown S.M., Doom J.R., Lechuga-Peña S., Watamura S.E., Koppels T. Stress and parenting during the global COVID-19 pandemic. Child Abuse & Neglect. 2020;110(Pt 2) doi: 10.1016/j.chiabu.2020.104699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calvano C., Engelke L., Di Bella J., Kindermann J., Renneberg B., Winter S.M. Families in the COVID-19 pandemic: Parental stress, parent mental health and the occurrence of adverse childhood experiences-results of a representative survey in Germany. European Child & Adolescent Psychiatry. 2021 doi: 10.1007/s00787-021-01739-0. Published online March 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Comolli C.L. The fertility response to the great recession in europe and the United States. Demographic Research. 2017;36:1549–1600. [Google Scholar]
- Diamond-Smith N, Logan R, Marshall C, et al. COVID-19's impact on contraception experiences: Exacerbation of structural inequities in women's health. Contraception. Published online August 2021:S0010782421003693. doi:10.1016/j.contraception.2021.08.011. [DOI] [PMC free article] [PubMed]
- The Employment Situation — January 2021. U.S. Bureau of Labor Statistics https://www.bls.gov/news.release/archives/empsit_02052021.htm.
- Geist C., Everett B.G., Simmons R.G., et al. Changing lives, dynamic plans: Prospective assessment of 12-month changes in pregnancy timing intentions and personal circumstances using data from HER Salt Lake. Pienta A.M., editor. PLoS One. 2021;16(9) doi: 10.1371/journal.pone.0257411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton B.E. Vol. 20. 2022. (Births: Provisional data for 2021). [DOI] [Google Scholar]
- Hartnett C.S., Gemmill A. Recent trends in U.S. Childbearing intentions. Demography. 2020;57(6):2035–2045. doi: 10.1007/s13524-020-00929-w. [DOI] [PubMed] [Google Scholar]
- Hashemzadeh M., Shariati M., Mohammad Nazari A., Keramat A. Childbearing intention and its associated factors: A systematic review. Nurs Open. 2021;8(5):2354–2368. doi: 10.1002/nop2.849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones H.E., Yoon D.B., Theiss J.A., Austin J.T., Lee L.E. Assessing the effects of COVID-19 on romantic relationships and the coping strategies partners use to manage the stress of a pandemic. Journal of Family Communication. 2021;21(3):152–166. doi: 10.1080/15267431.2021.1927040. [DOI] [Google Scholar]
- Kahn L.G., Trasande L., Liu M., Mehta-Lee S.S., Brubaker S.G., Jacobson M.H. Factors associated with changes in pregnancy intention among women who were mothers of young children in New York city following the COVID-19 outbreak. JAMA Network Open. 2021;4(9) doi: 10.1001/jamanetworkopen.2021.24273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindberg L.D., Mueller J., Kirstein M., VandeVusse A. Guttmacher Institute; 2021. The continuing impacts of the COVID-19 pandemic in the United States: Findings from the 2021 guttmacher survey of reproductive health experiences. [DOI] [Google Scholar]
- Lindberg L.D., VandeVusse A., Mueller J., Kirstein M. Guttmacher Institute; 2020. Early impacts of the COVID-19 pandemic: Findings from the 2020 guttmacher survey of reproductive health experiences. [DOI] [Google Scholar]
- Lin T.K., Law R., Beaman J., Foster D.G. The impact of the COVID-19 pandemic on economic security and pregnancy intentions among people at risk of pregnancy. Contraception. 2021;103(6):380–385. doi: 10.1016/j.contraception.2021.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luetke M., Hensel D., Herbenick D., Rosenberg M. Romantic relationship conflict due to the COVID-19 pandemic and changes in intimate and sexual behaviors in a nationally representative sample of American adults. Journal of Sex & Marital Therapy. 2020;46(8):747–762. doi: 10.1080/0092623X.2020.1810185. [DOI] [PubMed] [Google Scholar]
- Naya C.H., Saxbe D.E., Dunton G.F. Early effects of the COVID-19 pandemic on fertility preferences in the United States: An exploratory study. Fertility and Sterility. 2021;116(4):1128–1138. doi: 10.1016/j.fertnstert.2021.05.092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pietromonaco P.R., Overall N.C. Applying relationship science to evaluate how the COVID-19 pandemic may impact couples' relationships. American Psychologist. 2021;76(3):438–450. doi: 10.1037/amp0000714. [DOI] [PubMed] [Google Scholar]
- Riley A.R., Chen Y.H., Matthay E.C., et al. Excess death among Latino people in California during the COVID-19 pandemic. MedRxiv Prepr Serv Health Sci. Published online January. 2021;25 doi: 10.1101/2020.12.18.20248434. 2020.12.18.20248434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rocca CH, Parra M, Muñoz I, Foster DG, Boscardin WJ, Ralph LJ. Comparison of pregnancy preferences preceding vs year 1 of the COVID-19 pandemic. JAMA Network Open. 2022;5(7) doi: 10.1001/jamanetworkopen.2022.20093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell B.S., Hutchison M., Tambling R., Tomkunas A.J., Horton A.L. Initial challenges of caregiving during COVID-19: Caregiver burden, mental health, and the parent-child relationship. Child Psychiatry and Human Development. 2020;51(5):671–682. doi: 10.1007/s10578-020-01037-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schneider D., Harknett K. What's to like? Facebook as a tool for survey data collection. Sociological Methods & Research. 2022;51(1):108–140. doi: 10.1177/0049124119882477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seltzer N., Nobles J. Post-disaster fertility: Hurricane katrina and the changing racial composition of new orleans. Population and Environment. 2017;38(4):465–490. doi: 10.1007/s11111-017-0273-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sobotka T., Skirbekk V., Philipov D. Economic recession and fertility in the developed world. Population and Development Review. 2011;37(2):267–306. doi: 10.1111/j.1728-4457.2011.00411.x. [DOI] [PubMed] [Google Scholar]
- Taubman-Ben-Ari O., Ben-Yaakov O., Chasson M. Parenting stress among new parents before and during the COVID-19 pandemic. Child Abuse & Neglect. 2021;117 doi: 10.1016/j.chiabu.2021.105080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trinitapoli J., Yeatman S. The flexibility of fertility preferences in a context of uncertainty: Flexibility of fertility preferences in a context of uncertainty. Population and Development Review. 2018;44(1):87–116. doi: 10.1111/padr.12114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vignoli D., Guetto R., Bazzani G., Pirani E., Minello A. A reflection on economic uncertainty and fertility in Europe: The Narrative Framework. Genus. 2020;76(1):28. doi: 10.1186/s41118-020-00094-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vrachnis N., Vlachadis N., Iliodromiti Z., Vlachadi M., Creatsas G. Greece's birth rates and the economic crisis. The Lancet. 2014;383(9918):692–693. doi: 10.1016/S0140-6736(14)60252-X. [DOI] [PubMed] [Google Scholar]
- Weeland J., Keijsers L., Branje S. Introduction to the special issue: Parenting and family dynamics in times of the COVID-19 pandemic. Developmental Psychology. 2021;57(10):1559–1562. doi: 10.1037/dev0001252. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The authors do not have permission to share data.