

Abstract
Pseudoangiomatous stromal hyperplasia (PASH) is a benign mesenchymal tumor-like lesion of the breast. It is commonly seen as incidental background changes of the intralobular stroma in biopsy specimens performed for other breast lesions. Less frequently, it presents as a nodular form that has a benign morphology on imaging, mimicking fibroadenoma or as a diffuse form causing progressive massive gigantomastia. Diagnosis is established by biopsy. Knowledge of the imaging appearance of PASH not only facilitates proper assessment of radiopathological correlation but also helps in deciding further management of these lesions. Occasionally, nodular PASH may have a suspicious appearance on imaging wherein excision biopsy is indicated to exclude a coexisting carcinoma.
Keywords: pseudoangiomatous stromal hyperplasia, nodular form, diffuse form, incidental PASH changes
Introduction
Pseudoangiomatous stromal hyperplasia (PASH) is a rare benign mesenchymal tumor-like lesion of the breast with no malignant potential. PASH was first described by Vuitch et al as grossly circumscribed lesions with a distinct histological appearance of complex interanastomosing channels lined by spindle stromal cells in the breast parenchyma simulating the vascular spaces of low grade angiosarcoma. 1 The lesions consist of dense hyalinized collagen bundles that cause expansion of intralobular stroma and are dissected by slit-like pseudovascular spaces lined by myofibroblasts. Majority of the lesions are discovered as incidental microscopic findings in biopsy specimens of other benign breast diseases. Less frequently, they are identified on screening mammography or present as clinically palpable breast lumps. 2 In this case series, we report and discuss the spectrum of clinicoradiological manifestation of PASH including incidental PASH changes, nodular, and diffuse PASH.
Case Reports
We report 8 cases of PASH worked up at our hospital, of which cases 1 to 5 were nodular PASH, case 6 was diffuse PASH, and cases 7 and 8 were PASH changes seen in association with benign breast lesions.
Cases 1 to 5
Nodular PASH ( Figs. 1 , 2 , 3 , 4 , 5 )—All the patients in this group presented either for screening mammography with incidentally identified lesions or with palpable lumps. Except for one postmenopausal woman, all the others were in their fourth and fifth decades of life. On mammogram, all the lesions appeared as equal density masses and showed either circumscribed or obscured margins. Coarse calcification was noted in one of the lesions and no associated feature was seen in any of them. Contrast-enhanced mammography was performed in two lesions that showed heterogeneous persistent enhancement in one and minimal enhancement in the other. On ultrasound, the lesions appeared oval or irregular and showed either indistinct or circumscribed margins. Cystic spaces were observed in three of the lesions and all were soft on elastography. Minimal internal vascularity was observed in all the lesions.
Fig. 1.

Case 1. Incidentally detected nodular pseudoangiomatous stromal hyperplasia in a patient with mastalgia. Craniocaudal and mediolateral oblique images of left breast ( A, B ) show an oval equal density lesion with circumscribed margins in upper outer quadrant, showing no significant enhancement on recombined postcontrast images ( C, D ). On ultrasonography, the lesion appears hypoechoic with indistinct margins and cystic spaces ( E ), shows mild vascularity ( F ), and is soft on elastography ( G ). On magnetic resonance imaging, the lesion shows intermediate signal intensity on axial T1-weighted ( H ) and T2-weighted inversion recovery ( I ) images with no diffusion restriction on diffusion-weighted image and apparent diffusion coefficient map (arrow in J, K ). On early and delayed postcontrast subtracted images, minimal enhancement is observed (arrowhead in L, M ). ( N ) Photomicrograph (40× magnification; hematoxylin and eosin stain) showing collagenized sparsely cellular stroma with slit-like spaces (arrow) rimmed by spindled myofibroblasts (arrowhead).
Fig. 2.

Case 2. Nodular pseudoangiomatous stromal hyperplasia identified on screening mammogram. Craniocaudal and mediolateral oblique images ( A, B ) of left breast show oval equal density lesion (arrow) with obscured margins in outer central quadrant with heterogeneous enhancement in recombined postcontrast images ( C, D ). On ultrasound ( E ), the lesion appears oval, hypoechoic with indistinct margins and cystic spaces (arrow) and was soft on elastography (not shown). ( F ) Photomicrograph (40× magnification; hematoxylin and eosin stain) showing collagenized stroma with slit-like spaces (arrow) lined by slender myofibroblasts (arrowhead).
Fig. 3.

Case 3. Nodular pseudoangiomatous stromal hyperplasia presenting as a palpable lump. Craniocaudal and mediolateral oblique images ( A, B ) of the right breast show an equal density lesion with obscured margins in the retroareolar region (arrowhead). On ultrasound, the lesion appears hypoechoic with partly circumscribed and partly indistinct margins with a few cysts along the posterior aspect ( C ), shows mild vascularity ( D ), and appears soft on elastography ( E ).
Fig. 4.

Case 4. Nodular pseudoangiomatous stromal hyperplasia incidentally detected on screening mammogram. Craniocaudal and mediolateral oblique views of the right breast show an irregular equal density lesion with circumscribed margins and coarse calcification in the upper outer quadrant ( A, B ). On ultrasound, the lesion appears hypoechoic with circumscribed margins ( C ), no significant vascularity ( D ) and is soft on elastography ( E ) resembling a fibroadenoma.
Fig. 5.

Case 5. Nodular pseudoangiomatous stromal hyperplasia presenting as a breast lump. Craniocaudal and mediolateral oblique (MLO) views of the right breast (arrow in A, B ) show an oval equal density lesion with obscured margins in the upper outer quadrant. MLO view tomosynthesis image shows better definition of the lesion margins ( C ). On ultrasound, the lesion appears oval, isoechoic with circumscribed margins ( D ) and with mild internal vascularity ( E ).
All were categorized as BIRADS 4 either because of atypical imaging appearance (cases 1, 2, 3, 5) or because of the age at presentation (case 4) and biopsy was performed. Core biopsy specimens of the lesions revealed stromal hyalinization with slit-like spaces rimmed by spindled myofibroblasts consistent with PASH. Since the radiopathological findings were concordant, surgery was deferred and follow-up advised in all of them. Magnetic resonance imaging (MRI) was performed in case 1 that showed intermediate signal intensity of the lesion on T1-weighted (T1W) and T2-weighted (T2W) images with no diffusion restriction and minimal postcontrast enhancement.
Case 6
Diffuse PASH ( Fig. 6 )—A 47-year-old female presented with progressive painless increase in size of both breasts over the past few years. On examination, the breasts were massively enlarged with multiple vaguely palpable lumps. Mammogram showed increased density of both breasts with multiple oval and round equal density lesions showing circumscribed and obscured margins diffusely involving the parenchyma. Ultrasound correlation revealed multiple round and oval heterogeneous lesions of varying sizes with minimal vascularity diffusely involving both breasts and appearing soft on elastography. MRI was performed for further characterization that showed multiple lesions with circumscribed margins, replacing the breast parenchyma. The lesions appeared hypointense on T1W and T2W images and showed delayed progressive contrast enhancement. Interspersed hyperintense slit-like areas and cysts were seen in the lesions on T2W inversion recovery (IR) images. Biopsy from lesions in both breasts showed sparse terminal duct-lobular units and hyalinized collagenous stroma with many slit-like angulated spaces lined by spindled cells suggestive of PASH. The patient was not willing for surgery and hence was advised follow-up.
Fig. 6.

Case 6. Diffuse pseudoangiomatous stromal hyperplasia causing gigantomastia. Craniocaudal ( A, B ) and mediolateral oblique ( C, D ) images of both breasts show diffusely increased density with multiple equal density lesions having obscured margins extensively involving the parenchyma. Ultrasound images show circumscribed heterogeneous lesions with minimal vascularity involving the breast parenchyma ( E, F ). Multiple such lesions were seen diffusely involving the breasts. Magnetic resonance images demonstrate the lesions showing intermediate signal intensity on T1-weighted (T1W) and T2W (T2W) images with interspersed slit-like areas appearing hypointense on T1W image (arrow in G ), hyperintense on T2W image (arrow in H ). A cyst is also seen in the T2W image (arrowhead in H ). No diffusion restriction is observed in diffusion-weighted image and apparent diffusion coefficient map ( I, J ). The lesions show persistent heterogeneous enhancement in early and delayed subtracted postcontrast images ( K, L ). ( M ) Photomicrograph (40× magnification; hematoxylin and eosin stain) showing sparse terminal duct lobular units and hyalinized collagenous stroma with many slit-like spaces (arrow) lined by spindled myofibroblasts (arrowhead).
Cases 7 and 8
Benign lesions with incidental PASH changes ( Figs. 7 , 8 )—Both the patients presented with breast lumps that on mammogram and ultrasound showed benign features suggestive of fibroadenoma. Though the imaging appearance was benign, the patients opted to get the lesions removed because of palpability and hence vacuum-assisted excision was performed. Histopathology revealed ducts lined by bilayered epithelium and background collagenized stroma intervened by slit-like spaces rimmed by slender myofibroblasts suggestive of fibroadenoma with PASH like stroma.
Fig. 7.

Case 7. Fibroadenoma with pseudoangiomatous stromal hyperplasia changes. Craniocaudal and mediolateral oblique images ( A, B ) of the right breast show an oval equal density lesion (arrowhead in B ) with circumscribed margins in the lower inner quadrant. The lesion on ultrasound appears oval, hypoechoic and shows circumscribed margins ( C, D ).
Fig. 8.
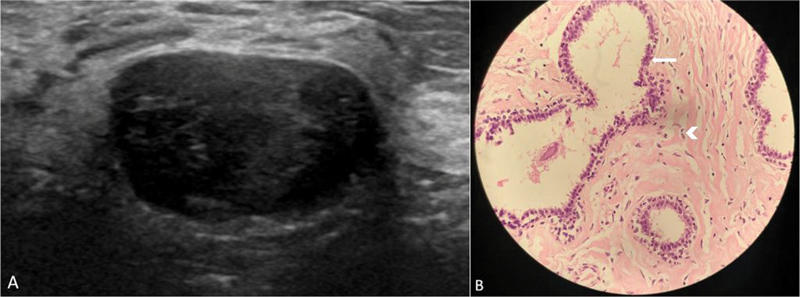
Case 8. Fibroadenoma with incidental pseudoangiomatous stromal hyperplasia changes. Ultrasound image ( A ) shows an oval hypoechoic lesion with circumscribed margins typical of fibroadenoma. ( B ) Photomicrograph (40× magnification; hematoxylin and eosin stain) showing ducts lined by bilayered epithelium (arrow) and intervening collagenized stroma with slit-like spaces lined by slender myofibroblasts (arrowhead).
Further details of the cases are presented in Table 1 .
Table 1. Case presentation and imaging findings.
| Age (in y) | Presentation | Mammogram | Ultrasound | Final diagnosis | |
|---|---|---|---|---|---|
| Case 1 | 42 | Right mastalgia with nipple discharge that was attributed to periductal mastitis on imaging. Mammogram further showed an incidental left breast lesion | Oval equal density lesion with circumscribed margins in upper outer quadrant of left breast | Oval hypoechoic lesion with indistinct margins and cystic spaces, showing minimal vascularity and appearing soft on elastography | Nodular PASH |
| Case 2 | 44 | Screen-detected | Oval equal density lesion with obscured margins in outer central quadrant of left breast | Oval hypoechoic mass with indistinct margins and a few cystic spaces, soft on elastography | Nodular PASH |
| Case 3 | 32 | Right breast lump | Oval equal density lesion with obscured margins in retroareolar region of left breast | Oval hypoechoic lesion with partly circumscribed and partly indistinct margins, soft on elastography | Nodular PASH |
| Case 4 | 60 | Screen-detected | Irregular equal density lesion with circumscribed margins and coarse calcification in the upper outer quadrant of right breast | Irregular hypoechoic lesion with circumscribed margins, soft on elastography | Nodular PASH |
| Case 5 | 46 | Right breast lump that was proven to be PASH on biopsy from a different hospital 2 years before, presented for screening | Oval equal density lesion with obscured margins in upper outer quadrant of right breast, stable since the previous mammogram | Oval hypoechoic lesion with circumscribed margins and minimal internal vascularity, soft on elastography | Nodular PASH |
| Case 6 | 47 | Progressive painless increase in size of both breasts over past few years | Bilateral enlarged breasts with increased density and multiple oval/round equal density lesions with circumscribed/obscured margins diffusely involving the parenchyma | Multiple oval heterogeneous masses of varying sizes diffusely involving both breasts with minimal vascularity and appearing soft on elastography | Diffuse PASH |
| Case 7 | 43 | Right breast lump | Oval equal density lesion with circumscribed margins in lower inner quadrant of right breast | Oval hypoechoic lesion with circumscribed margins, soft on elastography | Fibroadenoma with PASH like stroma |
| Case 8 | 26 | Left breast lump | – | Oval hypoechoic lesion with circumscribed margins, soft on elastography | Fibroadenoma with PASH like stroma |
Abbreviation: y, years
Discussion
PASH is a rare benign mesenchymal tumor of the breast. The name is derived from the characteristic histopathological stromal appearance of the lesion consisting of complex intercommunicating empty spaces lined by spindle shaped myofibroblasts simulating the endothelium lined vascular spaces seen in low-grade angiosarcoma. 1 Hormonal role has been postulated in the pathogenesis of PASH, evinced by the fact that it commonly occurs in premenopausal women and that the spindle cells in PASH demonstrate estrogen and progesterone receptor positivity. Less commonly, PASH occurs in postmenopausal women on hormonal replacement therapy and in men with gynecomastia. 3 Also, the stromal appearance of PASH consisting of pseudoangiomatous spaces resembles the normal changes observed in the hormone responsive intralobular stroma during the luteal phase of menstrual cycle.
It is hypothesized that PASH results from deviant response of myofibroblasts to the hormones resulting in abnormal expansion of intralobular stroma. Though a wide age range of involvement has been reported including premenarchal girls and postmenopausal women, women in the fourth and fifth decades are the most affected as was observed in our cases. 2 4 5 Clinicopathological spectrum of PASH includes the nodular and diffuse forms that are relatively rare entities and PASH changes of the mammary stroma that are common incidental background stromal findings in biopsy specimens of other benign and malignant breast pathologies.
Incidental PASH Changes
PASH is mostly seen as an incidental pathological finding in biopsy specimens performed for other breast lesions. In a retrospective analysis of 200 consecutive breast biopsy and mastectomy specimens, Ibrahim et al reported that 23% showed at least one microscopic focus of incidental PASH changes. 3 Kelten et al similarly reported that 37 out of 412 core needle biopsy specimens (9%) had background PASH changes. 6 Breast pathologies associated with PASH changes include fibrocystic changes, fibroadenoma, sclerosing lobular hyperplasia, benign breast parenchyma with stromal fibrosis, columnar cell hyperplasia, and invasive carcinoma. Though PASH is a benign entity and does not have increased risk of malignant transformation, there are reports of PASH occurring in the setting of invasive carcinoma. 7 In a large retrospective study of the Mayo Benign Breast Disease Cohort consisting of 9,087 women aged between 18 and 85 years, Degnim et al reported that PASH was identified in 6.4% biopsies and that PASH was not associated with increased risk of developing breast cancer in future. 8 Ferreira et al reported a case of invasive ductal carcinoma in the background of PASH; the malignant focus measured 9mm and was totally within the confines of PASH that was otherwise grossly well circumscribed on excision biopsy. The authors inferred it to be an incidental association rather than malignant degeneration of PASH. 5 PASH has also been reported as an incidental finding in 24 to 47% of men with gynecomastia. 9
Nodular PASH
Nodular PASH is a rare entity with an incidence of 0.4% in breast biopsies. 10 It may either present as a palpable breast lump or may be incidentally identified on imaging. The lesions are usually firm, nontender, and mobile on palpation and may either remain stable, enlarge, or regress in size on follow-up. They may be of varying size at presentation and lesions as large as 20 cm are reported in literature.
As was observed in our series, nodular PASH lesions frequently have a benign morphology on mammogram appearing as oval or round equal density lesions with circumscribed or obscured margins. Less commonly they present as focal asymmetries. Calcifications are rare. In the study by Celliers et al, most of the PASH lesions with calcifications had a primary diagnosis of other benign breast disease with incidental PASH changes in stroma. 11 Suspicious features like architectural distortion and microcalcification are usually absent. On ultrasound, the lesions appear round to oval, hypoechoic with circumscribed or indistinct margins.
Both on mammography and ultrasound, they are often misdiagnosed as fibroadenoma due to the overlapping imaging appearance. Occasionally, cystic changes may be seen as was observed in our first three cases and the lesions may appear hyperechoic or heterogeneous. Posterior acoustic features are variable, and the lesions are soft on elastography. At times, the lesions may present with suspicious imaging features like irregular shape and noncircumscribed margins both on mammogram and ultrasound and these warrant biopsy. Jones et al reported that 14% of the 56 lesions in their study had irregular or indistinct margins and were assigned as BIRADS category 4. 11 12 13 Though PASH does not upgrade to carcinoma, PASH may coincidentally occur at the site of carcinoma, and hence excision biopsy is recommended if clinical and radiological findings are discordant with pathological findings.
Limited literature is available on MRI appearance of PASH. The lesions are usually of intermediate signal intensity on T1W and T2W images with interspersed hyperintense slit-like spaces and cysts on T2W/IR images as discussed further under diffuse PASH. They show variable enhancement patterns, appearing either as a mass or nonmass enhancement. Rapid and persistent enhancement pattern is observed on dynamic postcontrast images. 14
Diagnosis is usually established by core needle biopsy. Surgical excision is preferred in lesions with suspicious imaging features, those which are rapidly increasing in size and to alleviate patient symptoms. Recurrence following surgery is reported in 15 to 22% cases, and hence wide local excision is preferred. Lesions managed conservatively are followed up clinically and with imaging. 2 The term tumoral PASH is used to describe circumscribed PASH lesions that grow to very large sizes causing asymmetric enlargement of the involved breast. 14
Diffuse PASH
PASH, in the least common form, presents as diffuse involvement of both breasts causing progressive asymmetric gigantomastia. Diffuse PASH either presents as multiple tumoral lesions replacing the breast parenchyma or as diffusely infiltrative lesions without forming discrete masses. 15
On mammography, diffuse PASH has the distinctive appearance of massively enlarged breasts with overall increased density. Additionally, multiple circumscribed or obscured lesions may be seen extensively involving the breast parenchyma as was noted in our case. On ultrasound, hypoechoic or heterogeneous lesions, either diffusely infiltrating or forming masses, are seen in the breast. Lace-like reticular hyperechoic areas and cysts may be seen and the lesions do not show increased vascularity.
Like nodular PASH, diffuse PASH shows intermediate signal intensity on T1W images and heterogeneous signal intensity on T2W/IR images with the slit-like areas and cysts appearing hyperintense on T2W and hypointense on T1W images. Teh et al described that the reticular lace-like pattern on imaging, appearing hyperechoic on ultrasound and as hyperintense slit-like areas on T2W/ IR images could potentially represent a specific imaging appearance of tumoral and diffuse PASH and is likely representative of empty clefts within the expanded collagenous stroma seen in PASH lesions. 16 The lesions show diffuse prominent enhancement with contrast with persistent enhancement kinetics in dynamic images. 14 The standard of care in diffuse and tumoral PASH is mastectomy or reduction mammoplasty for symptomatic relief and cosmetic purposes. 17 18 19
Conclusion
PASH is a rare noncancerous lesion of the breast with a wide spectrum of manifestations ranging from incidental microscopic changes to bilateral diffuse involvement causing gigantomastia. While diffuse PASH has a specific imaging appearance, nodular PASH mimics other benign breast lesions on imaging, commonly fibroadenoma. Irrespective of the imaging findings, provided there are no suspicious features of malignancy, a histopathologically proven nodular PASH can be safely followed up avoiding surgery.
Acknowledgment
Nil.
Funding Statement
Funding Nil.
Conflict of Interest None.
Meeting Presentation
No.
References
- 1.Vuitch M F, Rosen P P, Erlandson R A. Pseudoangiomatous hyperplasia of mammary stroma. Hum Pathol. 1986;17(02):185–191. doi: 10.1016/s0046-8177(86)80292-1. [DOI] [PubMed] [Google Scholar]
- 2.Estes A, Cao L, Miller M E. Pseudoangiomatous stromal hyperplasia: overview and clinical management. Ann Breast Surg. 2020;4:22–36. [Google Scholar]
- 3.Ibrahim R E, Sciotto C G, Weidner N. Pseudoangiomatous hyperplasia of mammary stroma. Some observations regarding its clinicopathologic spectrum. Cancer. 1989;63(06):1154–1160. doi: 10.1002/1097-0142(19890315)63:6<1154::aid-cncr2820630619>3.0.co;2-q. [DOI] [PubMed] [Google Scholar]
- 4.Jaunoo S S, Thrush S, Dunn P. Pseudoangiomatous stromal hyperplasia (PASH): a brief review. Int J Surg. 2011;9(01):20–22. doi: 10.1016/j.ijsu.2010.09.005. [DOI] [PubMed] [Google Scholar]
- 5.Ferreira M, Albarracin C T, Resetkova E. Pseudoangiomatous stromal hyperplasia tumor: a clinical, radiologic and pathologic study of 26 cases. Mod Pathol. 2008;21(02):201–207. doi: 10.1038/modpathol.3801003. [DOI] [PubMed] [Google Scholar]
- 6.Kelten Talu C, Boyaci C, Leblebici C, Hacihasanoglu E, Bozkurt E R. Pseudoangiomatous stromal hyperplasia in core needle biopsies of breast specimens. Int J Surg Pathol. 2017;25(01):26–30. doi: 10.1177/1066896916660763. [DOI] [PubMed] [Google Scholar]
- 7.Drinka E K, Bargaje A, Erşahin ÇH. Pseudoangiomatous stromal hyperplasia (PASH) of the breast: a clinicopathological study of 79 cases. Int J Surg Pathol. 2012;20(01):54–58. doi: 10.1177/1066896911418643. [DOI] [PubMed] [Google Scholar]
- 8.Degnim A C, Frost M H, Radisky D C. Pseudoangiomatous stromal hyperplasia and breast cancer risk. Ann Surg Oncol. 2010;17(12):3269–3277. doi: 10.1245/s10434-010-1170-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Milanezi M F, Saggioro F P, Zanati S G, Bazan R, Schmitt F C. Pseudoangiomatous hyperplasia of mammary stroma associated with gynaecomastia. J Clin Pathol. 1998;51(03):204–206. doi: 10.1136/jcp.51.3.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Polger M R, Denison C M, Lester S, Meyer J E. Pseudoangiomatous stromal hyperplasia: mammographic and sonographic appearances. AJR Am J Roentgenol. 1996;166(02):349–352. doi: 10.2214/ajr.166.2.8553945. [DOI] [PubMed] [Google Scholar]
- 11.Celliers L, Wong D D, Bourke A. Pseudoangiomatous stromal hyperplasia: a study of the mammographic and sonographic features. Clin Radiol. 2010;65(02):145–149. doi: 10.1016/j.crad.2009.10.003. [DOI] [PubMed] [Google Scholar]
- 12.Jones K N, Glazebrook K N, Reynolds C. Pseudoangiomatous stromal hyperplasia: imaging findings with pathologic and clinical correlation. AJR Am J Roentgenol. 2010;195(04):1036–1042. doi: 10.2214/AJR.09.3284. [DOI] [PubMed] [Google Scholar]
- 13.Raj S D, Sahani V G, Adrada B E. Pseudoangiomatous stromal hyperplasia of the breast: multimodality review with pathologic correlation. Curr Probl Diagn Radiol. 2017;46(02):130–135. doi: 10.1067/j.cpradiol.2016.01.005. [DOI] [PubMed] [Google Scholar]
- 14.Lee S J, Mahoney M C. Philadelphia: Elsevier Saunders; 2014. Benign findings in breast MRI; pp. 62–92. [Google Scholar]
- 15.Ryu E M, Whang I Y, Chang E D. Rapidly growing bilateral pseudoangiomatous stromal hyperplasia of the breast. Korean J Radiol. 2010;11(03):355–358. doi: 10.3348/kjr.2010.11.3.355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Teh H S, Chiang S H, Leung J W, Tan S M, Mancer J F. Rapidly enlarging tumoral pseudoangiomatous stromal hyperplasia in a 15-year-old patient: distinguishing sonographic and magnetic resonance imaging findings and correlation with histologic findings. J Ultrasound Med. 2007;26(08):1101–1106. doi: 10.7863/jum.2007.26.8.1101. [DOI] [PubMed] [Google Scholar]
- 17.Solomou E, Kraniotis P, Patriarcheas G. A case of a giant pseudoangiomatous stromal hyperplasia of the breast: magnetic resonance imaging findings. Rare Tumors. 2012;4(02):e23. doi: 10.4081/rt.2012.e23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Krawczyk N, Fehm T, Ruckhäberle E. Bilateral diffuse pseudoangiomatous stromal hyperplasia (PASH) causing gigantomastia in a 33-year-old pregnant woman: case report. Breast Care (Basel) 2016;11(05):356–358. doi: 10.1159/000450867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dai H, Connor C, Cui W, Gatewood J, Fan F. Bilateral diffuse tumorous pseudoangiomatous stromal hyperplasia: a case of bilateral mastectomy in a 29-year-old woman. Case Rep Pathol. 2014;2014:250608. doi: 10.1155/2014/250608. [DOI] [PMC free article] [PubMed] [Google Scholar]