

This cross-sectional study examines rates of organ donation and transplants during major US motorcycle rallies vs 4 weeks before and after the rallies.
Key Points
Question
Is the incidence of organ donation and transplants higher during major US motorcycle rallies?
Findings
In this cross-sectional study of 10 798 organ donors and 35 329 recipients of these organs from a national transplant registry from 2005 to 2021, there were 21% more organ donors and 26% more transplant recipients per day during motorcycle rallies in regions near those rallies compared with the 4 weeks before and after the rallies.
Meaning
While safety measures to minimize morbidity and mortality during motorcycle rallies should be prioritized, this study showed the downstream association of these events with organ donation and transplants.
Abstract
Importance
Large-scale motorcycle rallies attract thousands of attendees and are associated with increased trauma-related morbidity and mortality.
Objective
To examine the association of major US motorcycle rallies with the incidence of organ donation and transplants.
Design, Setting, and Participants
This population-based, retrospective cross-sectional study used data from the Scientific Registry of Transplant Recipients for deceased organ donors aged 16 years or older involved in a motor vehicle crash and recipients of organs from these donors from March 2005 to September 2021.
Exposure
Dates of 7 large US motorcycle rallies and regions near these events.
Main Outcomes and Measures
The main outcomes were incidence of motor vehicle crash–related organ donation and number of patients receiving a solid organ transplant from these donors. An event study design was used to estimate adjusted rates of organ donation during the dates of 7 major US motorcycle rallies compared with the 4 weeks before and after the rallies in rally-affected and rally-unaffected (control) regions. Donor and recipient characteristics and metrics of organ quality were compared between rally and nonrally dates.
Results
The study included 10 798 organ donors (70.9% male; mean [SD] age, 32.5 [13.7] years) and 35 329 recipients of these organs (64.0% male; 49.3 [15.5] years). During the rally dates, there were 406 organ donors and 1400 transplant recipients. During the 4 weeks before and after the rallies, there were 2332 organ donors and 7714 transplant recipients. Donors and recipients during rally and nonrally dates were similar in demographic and clinical characteristics, measures of organ quality, measures of recipient disease severity, and recipient waiting time. During rallies, there were 21% more organ donors per day (incidence rate ratio [IRR], 1.21; 95% CI, 1.09-1.35; P = .001) and 26% more transplant recipients per day (IRR, 1.26; 95% CI, 1.12-1.42; P < .001) compared with the 4 weeks before and after the rallies in the regions where they were held.
Conclusions and Relevance
In this cross-sectional study, major motorcycle rallies in the US were associated with increased incidence of organ donation and transplants. While safety measures to minimize morbidity and mortality during motorcycle rallies should be prioritized, this study showed the downstream association of these events with organ donation and transplants.
Introduction
The shortage of organs available for transplant remains a public health challenge in the US. In January 2022, there were more than 106 000 patients on a solid organ transplant waiting list.1 Yet, with only 33 000 transplants performed in 2021, demand exceeds supply, and 16 patients die each day waiting for a transplant.1 Deceased donation accounts for 84% of all organ transplants, and a common source of deceased donor organs is traumatic injury from motor vehicle accidents, which have increased over the past decade1,2 and accounted for 11% of all organ donors in 2021.1
Motorcyclists are disproportionately more likely to die in a crash compared with passenger vehicle motorists, and unhelmeted motorcyclists are 3 times as likely to become organ donors when involved in fatal crashes.3 In states where motorcycle helmets were previously required by law, helmet law repeal was associated with greater motor vehicle crash–related deceased organ donation.4
An unexplored mechanism by which traffic systems and motorcycle trauma may impact organ donation is through large-scale motorcycle rallies. There are several large motorcycle rallies, or “Bike Weeks,” organized annually in the US that attract hundreds of thousands of participants. The largest and most widely known motorcycle rally is the Sturgis Motorcycle Rally in Sturgis, South Dakota, which attracts more than 400 000 people annually.5 Given the injury risk associated with motorcycle use and the large scale of these events, these rallies can strain local trauma systems through increased traumatic morbidity and mortality.6,7 However, the effect of this excess mortality on availability of organ donation is unknown.
We assessed changes in incidence of organ donation and transplants during dates of large-scale US motorcycle rallies using a national registry of organ donors and transplant recipients. We compared rates of motor vehicle trauma–related organ donation and transplant for all solid organs in the 4 weeks before and after 7 major US motorcycle rallies, hypothesizing that the rates of motor vehicle trauma–associated organ donation and transplant would be higher during motorcycle rallies and in their associated regions compared with surrounding weeks.
Methods
Data Sources
Motorcycle rally dates were identified by a historical review of rally websites and local news sources. This cross-sectional study used data from the Scientific Registry of Transplant Recipients (SRTR).8 The SRTR data system includes data on all donors, wait-listed candidates, and transplant recipients in the US that are submitted by the members of the Organ Procurement and Transplantation Network (OPTN). The Health Resources and Services Administration, US Department of Health and Human Services provides oversight to the activities of the OPTN and SRTR contractors. This study was approved by the institutional review board of Mass General Brigham. All transplant candidates, recipients, and donors nationally consent to their data being collected and made publicly available for research purposes. Thus, for this study of deidentified registry data, the informed consent requirement was waived. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Motorcycle Rallies
We identified dates of the 7 largest motorcycle rallies in the US from 2005 to 2021 (eTable 1 in the Supplement). The rallies, all estimated to have between 200 000 to 500 000 annual attendees, included the Sturgis Motorcycle Rally (Sturgis, South Dakota), Daytona Bike Week (Daytona Beach, Florida), Laconia Motorcycle Week (Laconia, New Hampshire), Myrtle Beach Bike Week Spring Rally (Myrtle Beach, South Carolina), Atlantic Beach Bikefest (also in Myrtle Beach, South Carolina, following the former rally), Republic of Texas Biker Rally (Austin, Texas), and Bikes, Blues & BBQ (Fayetteville, Arkansas). These rallies occur across a range of seasons from March through September. Figure 1 shows the location of each rally relative to the OPTN regions, which are administrative boundaries used to organize OPTN governance and operations (procured organs have historically been prioritized locally first, then by OPTN region, and lastly, nationally).
Figure 1. Locations of Motorcycle Rallies and Their Corresponding Organ Procurement and Transplantation Network (OPTN) Regions.

Locations of the 7 motorcycle rallies included in our analysis: Sturgis Motorcycle Rally (Sturgis, South Dakota), Daytona Bike Week (Daytona Beach, Florida), Laconia Motorcycle Week (Laconia, New Hampshire), Myrtle Beach Bike Week Spring Rally (Myrtle Beach, South Carolina), Atlantic Beach Bikefest (Myrtle Beach, South Carolina), Republic of Texas Biker Rally (Austin, Texas), and Bikes Blues & BBQ (Fayetteville, Arkansas). The OPTN regions are outlined in bold black lines, and the regions containing the motorcycle rallies are shaded.
Organ Donations and Transplants
We identified all donors aged 16 years or older involved in a motor vehicle crash between March 2005 and September 2021 (dates chosen for complete data availability). Overall, 14.5% of donors aged 16 years or older in the SRTR were involved in a crash. The date of organ procurement and the OPTN region from which the donor originated were used to link donors temporally and geographically to a specific motorcycle rally. Donors who originated from an OPTN region that did not contain a motorcycle rally were used in a control group analysis described below.
Outcome Measures
Our primary outcome measures were the number of distinct organ donors per day and transplant recipients per day per OPTN region. The transplant recipient outcome was a count of the total number of recipients receiving 1 or more organs from each given donor and was linked temporally and geographically relative to the donor (ie, agnostic to the location of the ultimate recipients). The analysis was performed at the level of the region-day to account for motorcycle rallies of variable duration.
Donor and Recipient Characteristics
Donor characteristics included demographics, comorbidities, and the following metrics of organ quality or risk: donation after circulatory death, organ ischemia time, expanded criteria donor (defined as age >60 years or >50 years with 2 of the following conditions: hypertension, serum creatinine level ≥1.5 mg/dL [to convert to μmol/L, multiply by 88.4], or stroke as cause of death), steatotic liver (≥30% macrosteatosis on biopsy), high risk for infectious disease transmission, and hepatitis C antibody positivity. Demographic data were ascertained by self-report, and age, sex, race, and ethnicity were reported in this study for demographic purposes. Race and ethnicity are reported separately in the transplant registry. Race is dichotomized (White and racial minority groups [American Indian or Alaska Native, Arab or Middle Eastern, Asian, Black or African American, Indian subcontinent, Native Hawaiian or other Pacific Islander, other multiracial, and unknown]). Ethnicity is dichotomized as Latinx and not Latinx and is not mutually exclusive from the race categories. Recipient characteristics included demographics, time on waiting list, and metrics of recipient illness severity (dialysis, life support, mechanical circulatory support, and model for end-stage liver disease score).
Statistical Analysis
We first examined donor and recipient characteristics for organs procured on motorcycle rally dates compared with the 4 weeks before or after the rallies to test for possible differences in transplantation practices that occur during rally dates. During a transient increase in organ supply, it may be possible for transplant teams to be more conservative in their organ selection (ie, less inclined to transplant marginal quality organs), and transplant teams may also be able to provide transplants to patients with lower disease severity who are further down the waiting lists. Moreover, donor characteristics and organ quality might be expected to differ since any additional organs procured because of motorcycle rallies would presumably draw heavily from a specific group of individuals—motorcyclists—for whom health may differ from the general population of motorists. Differences in characteristics were tested using Fisher exact tests for binary variables and Wilcoxon rank-sum tests for continuous variables.
Next, we examined the rates of organ donation and transplants in motorcycle rally–affected areas during the dates of rallies compared with the 4 weeks before and after the rallies—an event study design. An event study design is an econometric approach that combines the period surrounding multiple similar events into a single analysis.9,10,11,12,13 Because within a season (eg, spring or summer), the specific dates of motorcycle rallies should be as-good-as-randomly timed with respect to regional demand for organ donations, a natural experiment occurs that permits an analysis of whether rallies are associated with an increase in organ donations through increases in the number of motorcyclists in rally-affected regions.
We estimated region-day–level multivariable Poisson regression models with robust SEs to generate estimated daily outcome counts adjusted for OPTN region, day of week, week of year, and year. In addition, to evaluate whether changes in donation or transplant rates occurring during rally dates were associated with the rallies themselves as opposed to other temporal factors, we also included in the same model a control group of distant regions (all regions not sharing a border with the rally region) that did not have a motorcycle rally in that same period. Rally and control region-days were included in the same model using an interaction term to estimate the main effects separately in rally-affected vs rally-unaffected (ie, control) regions. Although all weeks of the calendar year were included in the analysis to account for seasonal trends, we graphed adjusted mean daily counts of organ donors and transplant recipients per region (rally affected and rally unaffected) by week relative to the motorcycle rally, focusing on the week of the rally (defined as week 0) and the 4 weeks immediately preceding (weeks −4 to −1) and following (weeks 1-4) it. We expected to see no increase in donation and transplant rates during rally dates in the control regions.
To facilitate interpretation of effect sizes associated with the rallies, we also estimated a similar region-day–level multivariable Poisson regression model with the aforementioned covariates and an indicator variable equal to 1 for calendar days occurring in rally weeks and 0 for days in the 4 weeks before or after a rally (all other weeks of the year were also included in the regression to account for seasonal trends). In this model, we similarly included an interaction term between rally week and rally-affected regions to estimate the main effects separately in rally-affected vs control regions. We computed the adjusted incidence rate ratio (IRR) to estimate the proportional change in the daily number of organ donors or transplant recipients per region (rally affected and rally unaffected) for motorcycle rally dates compared with the 4 weeks before and after the rally combined.
We performed several sensitivity analyses to check the robustness of our findings to various assumptions and to residual confounding. First, we repeated the primary analyses for a separate group of comparison regions—those sharing a border with the rally region. This is not a true control group given the proximity of these regions to the rally regions and the potential for rally attendees (and potential donors) to cross between regions.
Second, in a random permutation test, we repeated the primary analyses using randomly selected rally weeks (“placebo rally dates”) instead of actual rally dates in the rally-containing regions to assess in a nonparametric manner the probability of obtaining similar effect sizes due to chance alone.14,15 After assigning randomly selected weeks to each motorcycle rally region, we repeated the analysis with these placebo rally dates for 1000 iterations and compared our observed effect size (IRR) with the distribution of effect sizes obtained from this simulation.
In addition, we repeated the analyses excluding more distant dates (ie, considered only dates within 4 weeks of the rallies) and separately by excluding 2020 and 2021 rallies (during the COVID-19 pandemic). Finally, we repeated the analyses for nonmotor vehicle–related donor deaths to assess whether there was an increase in organ donations associated with other factors (eg, medical, drug overdose).
Analyses were performed using Stata, version 14.1 (StataCorp LLC). The 95% CIs represent a 2-tailed P = .05.
Results
Study Population
Overall, 10 798 organ donors (70.9% male; mean [SD] age, 32.5 [13.7] years) and 35 329 transplant recipients (64.0% male; 49.3 [15.5] years) were analyzed (5128 heart, 2749 lung, 8916 liver, 17 201 kidney, 614 pancreas, 1951 kidney-pancreas, and 104 intestinal transplant recipients). A total of 30 074 region-days were analyzed, of which 854 region-days (2.8%) involved a motorcycle rally. During the rally dates, there were 406 organ donors (29.3% female; 70.7% male; mean [SD] age, 31.7 [13.1] years) and 1400 transplant recipients (34.8% female; 65.2% male; mean [SD] age, 49.0 (15.7) years). During the surrounding weeks, there were 2332 organ donors (29.4% female; 70.6% male; mean [SD] age, 32.2 [13.7] years) and 7714 transplant recipients (35.5% female; 64.5% male; mean [SD] age, 49.5 [15.3] years) (Table 1 and Table 2). Donors during rally and nonrally dates were similar in both demographic and clinical characteristics with the exception that donors during rally dates were more likely to be from racial minority groups compared with donors during nonrally dates in the surrounding weeks (19.0% [77 of 406] vs 14.1% [329 of 2332]; P = .01) (Table 1). Among transplant recipients, there were no statistically significant differences in demographic characteristics, time spent on the waiting list, disease severity, or organ ischemia time between those receiving a transplant on rally dates and those receiving a transplant on nonrally dates (Table 2).
Table 1. Characteristics of Organ Donors.
| Characteristic | Motorcycle rally dates | 4 wk Before and after rally | P valuea |
|---|---|---|---|
| Region-days, No. | 854 | 5541 | NA |
| Donor and organ volume and yield | |||
| Donors, No. | 406 | 2332 | NA |
| Donors per region-day, mean (SD) | 0.48 (0.70) | 0.42 (0.67) | .03 |
| Organs transplanted, No. | 1445 | 7983 | NA |
| Organs transplanted per region-day, mean (SD) | 1.69 (2.66) | 1.44 (2.43) | .02 |
| Organs transplanted per donor, mean (SD) | 3.56 (1.19) | 3.42 (1.21) | .051 |
| Donor characteristics | |||
| Age, mean (SD), y | 31.7 (13.1) | 32.2 (13.7) | .57 |
| Sex, No. (%) | |||
| Female | 119 (29.3) | 685 (29.4) | >.99 |
| Male | 287 (70.7) | 1647 (70.6) | |
| Latinx | 77 (19.0) | 329 (14.1) | .01 |
| Racial minority groupsb | 42 (10.3) | 342 (14.7) | .02 |
| Height, mean (SD), cm | 174.1 (9.0) | 174.4 (9.5) | .61 |
| Weight, mean (SD), kg | 81.2 (19.4) | 82.5 (18.6) | .054 |
| Organ donations after circulatory death, No. (%) | 49 (12.1) | 328 (14.1) | .31 |
| Warm ischemia time, mean (SD), min | 20.1 (9.5) | 20.5 (13.3) | .66 |
| Expanded criteria donors, No. (%)c | 18 (4.4) | 118 (5.1) | .71 |
| Liver steatosis, No. (%)d | 7 (2.0) | 58 (2.8) | .48 |
| Diabetes, No. (%) | 14 (3.4) | 77 (3.3) | .88 |
| Hypertension, No. (%) | 45 (11.1) | 242 (10.4) | .66 |
| High risk for disease transmission, No. (%) | 74 (18.2) | 341 (14.6) | .07 |
| Hepatitis C antibody positivity, No. (%) | 19 (4.7) | 70 (3.0) | .09 |
| ≥20 Pack-years smoking, No. (%) | 67 (16.5) | 366 (15.7) | .66 |
| Alcohol use ≥2 drinks/d, No. (%) | 53 (13.1) | 316 (13.6) | .88 |
| Out-of-state residence, No. (%) | 308 (75.9) | 1700 (72.9) | .22 |
Abbreviation: NA, not applicable.
SI conversion factor: To convert serum creatinine level to micromoles per liter, multiply by 88.4.
P values were obtained from the Fisher exact test for binary variables and the Wilcoxon rank-sum test for continuous variables.
American Indian or Alaska Native, Arab or Middle Eastern, Asian, Black or African American, Indian subcontinent, Native Hawaiian or other Pacific Islander, other multiracial, and unknown.
Refers to donors aged 60 years or older or donors aged 50 years or older with 2 or more of the following conditions: hypertension, serum creatinine level of 1.5 mg/dL or higher, or stroke as cause of death.
Among 8916 liver donors.
Table 2. Characteristics of Transplant Recipients.
| Characteristic | Motorcycle rally dates | 4 wk Before and after rally | P valuea |
|---|---|---|---|
| Recipients, No. | 1400b | 7714b | NA |
| Age, mean (SD), y | 49.0 (15.7) | 49.5 (15.3) | .52 |
| Sex, No. (%) | |||
| Female | 487 (34.8) | 2737 (35.5) | .63 |
| Male | 913 (65.2) | 4977 (64.5) | |
| Latinx | 430 (30.7) | 2318 (30.0) | .61 |
| Racial minority groupsc | 127 (9.1) | 1022 (13.2) | <.001 |
| Time on waiting list, mean (SD), d | 491.4 (694.6) | 475.7 (665.8) | .82 |
| Organwise transplant characteristic | |||
| Heart | |||
| Transplant recipients, No. | 205 | 1096 | NA |
| Time on waiting list, mean (SD), d | 207.8 (340.8) | 221.7 (389.8) | .55 |
| Dialysis, No. (%) | 10 (4.9) | 43 (3.9) | .56 |
| Life support, No. (%) | 156 (76.8) | 870 (79.7) | .35 |
| Mechanical circulatory support, No. (%) | 97 (47.3) | 515 (47.0) | .94 |
| Total ischemia time, mean (SD), min | 198.7 (71.5) | 199.1 (66.8) | .93 |
| Lung | |||
| Transplant recipients, No. | 115 | 561 | NA |
| Time on waiting list, mean (SD), d | 136.2 (220.4) | 182.6 (440.8) | .42 |
| Dialysis, No. (%) | 1 (0.9) | 1 (0.2) | .31 |
| Life support, No. (%) | 12 (10.4) | 53 (9.5) | .73 |
| Total ischemia time, mean (SD), min | 295.2 (83.3) | 306.3 (106.1) | .46 |
| Liver | |||
| Transplant recipients, No. | 353 | 1986 | NA |
| Time on waiting list, mean (SD), d | 197.9 (481.3) | 190.8 (401.4) | .92 |
| Calculated MELD, mean (SD) | 22.4 (9.6) | 22.6 (9.8) | .75 |
| Allocation MELD, mean (SD)d | 26.1 (7.7) | 26.5 (7.8) | .72 |
| Dialysis, No. (%) | 43 (12.2) | 286 (14.4) | .32 |
| Life support, No. (%) | 34 (9.7) | 154 (7.8) | .24 |
| Cold ischemia time, mean (SD), h | 6.2 (2.6) | 6.4 (2.7) | .33 |
| Kidney | |||
| Transplant recipients, No. | 671 | 3774 | NA |
| Time on waiting list, mean (SD), d | 796.9 (806.5) | 741.6 (764.2) | .14 |
| Cold ischemia time, h | 18.2 (10.9) | 17.7 (9.2) | .75 |
| Pancreas | |||
| Transplant recipients, No. | 27 | 123 | NA |
| Time on waiting list, mean (SD), d | 342.1 (279.7) | 326.8 (356.4) | .40 |
| Kidney-Pancreas | |||
| Transplant recipients, No. | 73 | 424 | NA |
| Time on waiting list, mean (SD), d | 273.7 (295.3) | 329.3 (454.7) | .93 |
| Cold ischemia time, mean (SD), h | 11.9 (4.7) | 11.7 (5.0) | .44 |
| Intestines | |||
| Transplant recipients, No. | 4 | 25 | NA |
| Time on waiting list, mean (SD), d | 19.5 (21.9) | 121.5 (152.1) | .07 |
| Total ischemia time, mean (SD), h | 6.9 (1.1) | 7.5 (1.4) | .54 |
Abbreviations: MELD, model for end-stage liver disease; NA not applicable.
P values were obtained from the Fisher exact test for binary variables and the Wilcoxon rank-sum test for continuous variables.
Column totals (number of distinct recipients) are less than the sum for individual organs because a given recipient can receive multiple transplanted organs.
American Indian or Alaska Native, Arab or Middle Eastern, Asian, Black or African American, Indian subcontinent, Native Hawaiian or other Pacific Islander, other multiracial, and unknown.
Allocation MELD accounts for exception points.
Organ Donors and Transplants During Dates of Motorcycle Rallies
There were more organ donors (mean [SD], 0.48 [0.70] vs 0.42 [0.67] per region-day; P = .03) and more transplanted organs (mean [SD], 1.69 [2.66] vs 1.44 [2.43] per day; P = .02) in rally regions during the rally dates compared with the surrounding 4 weeks in the same regions (Table 1). Organ yield, defined as the number of organs procured and transplanted from a single donor, was similar during rally and nonrally dates (mean [SD], 3.56 [1.19] vs 3.42 [1.21]; P = .05).
Incidence of organ donation was higher on rally dates compared with surrounding nonrally dates after adjustment for OPTN region, day of week, week of year, and year (Figure 2A and eTable 2 in the Supplement). In regions containing a motorcycle rally, there were 21% more organ donors per day during rally dates compared with the 4 weeks before and after the rally (IRR, 1.21; 95% CI, 1.09-1.35; P = .001; absolute increase, 0.08 donors per region-day; 95% CI, 0.03-0.12 donors per region-day). Across 9 days (the mean duration of a motorcycle rally), this reflected 0.7 (95% CI, 0.3-1.1) additional organ donors for a typical rally. In comparison, in control (distant) regions (29 999 region-days), there was no significant difference in the number of organ donors per day during motorcycle rally dates compared with the 4 weeks before and after the rally (IRR, 1.06; 95% CI, 0.98-1.14; P = .14; absolute change, 0.02 donors per region-day; 95% CI, −0.01 to 0.04 donors per region-day). The net effect of motorcycle rallies (rally effect minus control effect) was 14% more organ donors per day during rally dates compared with nonrally dates (IRR, 1.14; 95% CI, 1.01-1.30; P = .04).
Figure 2. Adjusted Number of Organ Donors and Organ Transplants per Region per Day by Weeks Relative to Motorcycle Rally.
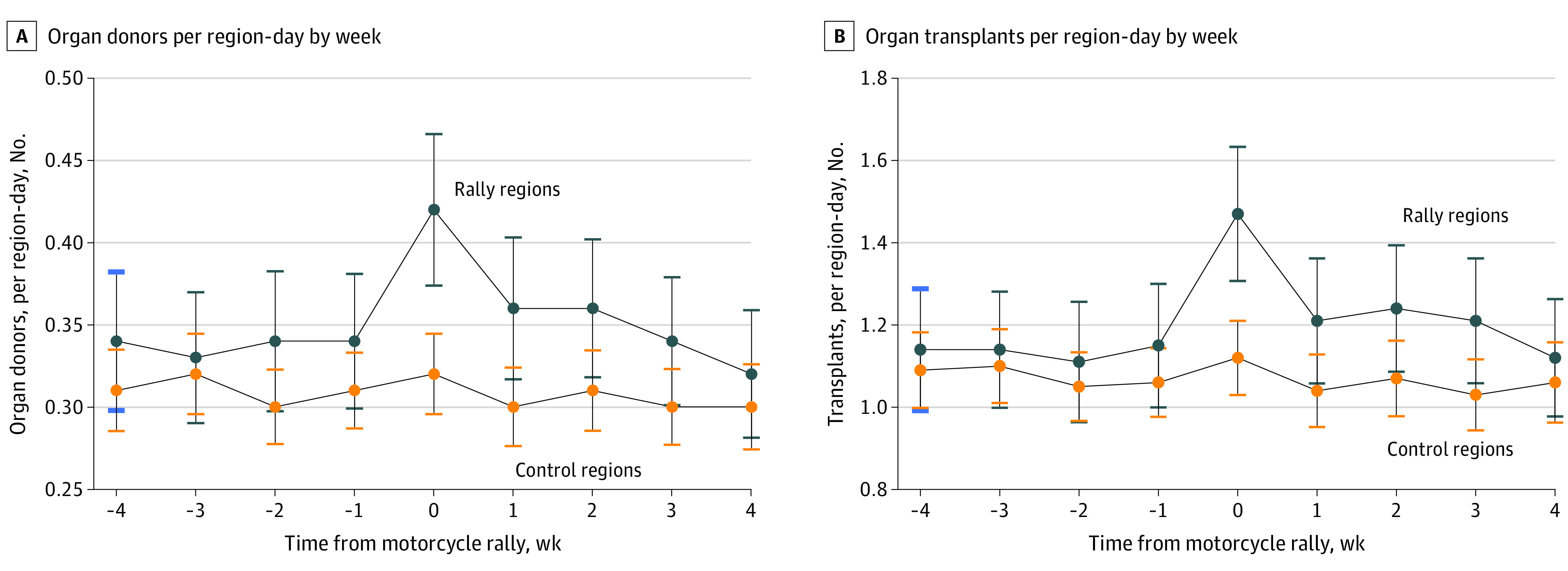
Data are from the event study model described in the Methods section. Control regions were regions distant from the rally region. Week 0 indicates the week of the motorcycle rally. Error bars indicate 95% CIs.
More patients received organ transplants on rally dates compared with surrounding nonrally dates after adjustment for OPTN region, day of week, week of year, and year (Figure 2B and eTable 2 in the Supplement). In regions containing a rally, there were 26% more transplant recipients per day during rally dates compared with nonrally dates (IRR, 1.26; 95% CI, 1.12-1.42; P < .001; absolute change, 0.34 transplant recipients per region-day; 95% CI, 0.15-0.52 transplant recipients per region-day), reflecting 3.1 (95% CI, 1.2-4.7) additional transplant recipients for a typical motorcycle rally. In comparison, in control (distant) regions, there was no significant difference in the number of transplant recipients per day during motorcycle rally dates compared with nonrally dates (IRR, 1.06; 95% CI, 0.97-1.15; P = .18; absolute change, 0.06 transplant recipients per region-day; 95% CI, −0.03 to 0.14 transplant recipients per region-day). The net effect of motorcycle rallies was 19% more transplant recipients per day during rally dates compared with nonrally dates (IRR, 1.19; 95% CI, 1.04-1.37; P = .01).
Additional Analyses
In a random permutation sensitivity analysis with randomly assigned placebo rally dates, only 7 of 1000 simulations (0.7%) produced an IRR for organ donors greater than our observed effect size of 1.21, and 2 of 1000 simulations produced an IRR for organ transplants greater than our observed effect size of 1.26 (eFigure in the Supplement). In nearby regions not containing a motorcycle rally, there were 11% fewer organ donors (IRR, 0.89; 95% CI, 0.82-0.98; P = .02) and 10% fewer transplant recipients (IRR, 0.90; 95% CI, 0.82-0.99; P = .04) per day during motorcycle rally dates compared with nonrally dates.
Results were similar when excluding weeks more distant than 4 weeks before or after the rallies (IRR of organ donation, 1.14; 95% CI, 1.00-1.30; P = .05; and IRR of transplant recipients, 1.18; 95% CI, 1.02-1.36; P = .02). When excluding 2020 and 2021 (years coincident with the COVID-19 pandemic), the results were also largely unchanged (among 27 390 region-dates, IRR of organ donation, 1.23; 95% CI, 1.10-1.38; P < .001; and IRR of transplant recipients, 1.27; 95% CI, 1.12-1.43; P < .001). When we separately analyzed donors with non–motor vehicle crash–related deaths (n = 122 488), there was no change in the number of organ donors (IRR, 0.98; 95% CI, 0.92-1.04; P = .50) or transplant recipients (IRR, 1.00; 95% CI, 0.95-1.05; P = .94) during rally weeks compared with the surrounding weeks.
Discussion
In this study, major motorcycle rallies in the US were associated with increased incidence of organ donation and transplants. Because the timing of these rallies is plausibly unrelated to demand for organs and because we found no such effect for non–motor vehicle–related donor deaths, our findings are likely due to an increase in motorcycle use in areas where large rallies are held. In regions where rallies are held, we estimated 21% more organ donors and 26% more transplant recipients per day during the rally dates compared with the 4 weeks before and after the rallies. This amounts to approximately 1 additional donor or 6 additional transplant recipients in these regions for every 2 major motorcycle rallies.
During motorcycle rally weeks in distant regions not containing motorcycle rallies, there was no increase in the number of organ donations or transplants, suggesting that our observed main effect was associated with the rallies rather than other temporal factors such as vacation travel. A portion of this increase in organ donors may represent individuals who would have died and become donors in other regions had they not traveled to the rallies—a displacement effect. For instance, in an analysis of the surrounding regions, we observed a 11% decrease in organ donations during rallies, possibly owing to would-be donors being displaced to the nearby motorcycle rally regions. This decrease is smaller than the increase seen in rally regions, and no effect was seen in the distant control regions. The overall net effect on the national organ supply attributable to motorcycle rallies is not readily quantifiable with this analysis of 7 of the largest rallies.
There were no differences observed in donor characteristics during motorcycle rally dates compared with nonrally dates, suggesting that any changes in the regional composition of donors that might result from those attending large rallies did not translate into differences in donor characteristics. For example, compared with the typical donor, motorcyclists involved in crashes tend to be older and are more likely to be male and engage in risky behaviors (alcohol was involved in 42% of motorcycle crashes in 2019).3 However, we found no significant differences in age, sex, alcohol use, or smoking between donors on rally and donors on nonrally dates. In addition, we found no differences in other measures of organ quality between rally and nonrally dates. This increase in organ supply without a decrease in quality of organs may be a reflection of donor selection criteria remaining constant during these rallies.
We also found no difference between rally and nonrally dates in wait times or severity of illness for transplant recipients. A large and sudden surge in organ availability might be expected to provide organs to patients further down the waiting list who are less sick, leading to shorter wait times (for organs such as heart, lung, or liver, which are allocated based on disease severity). The incremental increase in organ availability coupled with high demand for organs was likely not sufficient to lead to detectable differences in recipient characteristics or wait times in our analysis. The absolute effect size—3.1 additional transplants per rally week in affected regions—is small relative to the national organ shortage. Yet, a 26% increase in organ availability may still be significant to patients and transplant teams in motorcycle rally–affected areas.
Large-scale motorcycle rallies are associated with a surge in trauma volume at local hospitals as well as excess motor vehicle fatalities.6,16 A study of the Daytona Bike Week in 2000, which attracted 500 000 people, reported that 570 people were involved in 281 motorcycle crashes, which led to 72 hospitalizations and 11 deaths.6 There are no comprehensive estimates of mortality associated with large motorcycle rallies, to our knowledge, although the injury risk associated with motorcycle use is well established. For example, motorcyclists are 29 times more likely to die in a crash per mile traveled compared with occupants of passenger vehicles, and helmet use can prevent 37% of motorcycle crash fatalities.3 Unhelmeted motorcyclists are 3 times more likely than helmeted motorcyclists to become organ donors in a fatal crash,17 and an estimated 1 life is saved through transplant for every 3 unhelmeted motorcyclist deaths.4 Our study is the first, to our knowledge, to report organ donation and transplant rates during major motorcycle rallies.
The increase in organ transplants during motorcycle rallies may be associated with several factors including greater overall motorcycle use, inherent risk associated with these events (eg, congested roads), fatigue among motorcyclists driving long distances, or health system factors such as improved performance of organ procurement organizations during these events (eg, in identifying potential donors and optimizing yield of organ donors per death). We did not find an increase in donations associated with non–motor vehicle trauma–related deaths, suggesting that our observations were associated with traffic fatalities. From a public health standpoint, efforts to prevent excess morbidity and mortality associated with these events should remain the priority. However, to the extent that these events remain a source of increased mortality, the potential for these deaths to be turned into a gift of life through organ donation should be recognized, and efforts should be taken to anticipate and translate eligible deaths from these events into organ donations. The process of identifying potential donors and seeing them through to organ donation is resource intensive, and by identifying discrete events associated with increased availability of organ donors, organ procurement organizations may be able to augment staffing to maximize donation rates during events such as motorcycle rallies. In addition, large events may be useful venues for hosting organ donation education, outreach, and registration activities.
Although these findings are specific to the 7 largest motorcycle rallies in the US, they show the potential of large events, altered traffic patterns, and concentrations of motorcyclists or motor vehicles to have downstream associations with organ donation and transplant. As a related example, increased travel volume and riskier behaviors of travelers during spring break are associated with increased traffic fatalities18 and may similarly be associated with increased organ donation. Of the 7 motorcycle rallies included in our study, only 2 occur around holiday times (eg, spring break and Memorial Day weekend); however, no effects were seen around these same rally dates in distant control regions, and thus our results were unlikely to have been confounded by these temporal factors.
Limitations
This study has several limitations. First, our study was observational and residual confounding was possible. However, we relied on the plausibly exogenous timing of motorcycle rallies to address unmeasured confounding. Second, our analysis was unable to assess whether the increase in organ transplants during rallies led to improved transplant outcomes arising from earlier transplants. Third, our data set could not distinguish between motorcycle and car or truck crashes as the mechanism of death, and we could not identify specific dates of accidents, which would be useful to temporally link donors to rallies. Rather, we used the date of procurement for this linkage. For some patients, the progression to brain death and ultimately to donation may be prolonged, and thus these patients may have been coded as nonrally donors if their date of procurement was delayed by 1 to 2 weeks from their accident. This, however, would bias our findings toward the null. Fourth, exact donor hospital location was not available, precluding analysis on a smaller geographical level. Nevertheless, using OPTN regions as the unit of analysis reflects actual practice during most of the study period as organs were allocated within their OPTN region before being allocated to outside regions. Fifth, this study does not represent every motorcycle rally in the US, but only 7 of the largest rallies. Sixth, we could not identify rates of donation among all eligible deaths as the transplant registry does not report deaths that did not lead to donation. Seventh, it is possible that our findings were due to chance alone. However, the observed effect size for the association between rally dates and rates of organ transplant was larger in magnitude than 99% of estimates obtained from a simulation that randomly assigned placebo rally dates to rally regions.
Conclusions
In this cross-sectional study, an increase in motor vehicle crash–related organ donors and an increase in the number of organs transplanted was observed during dates of major US motorcycle rallies in regions where these rallies were held. Motorcycle rallies and other large-scale events are common, and though the priority must be public safety and minimizing excess morbidity and mortality during these events, the potential downstream association with organ donation should be recognized.
eTable 1. Motorcycle Rally Locations and Dates
eTable 2. Adjusted Number of Organ Donors and Organ Transplants Per Day Per Region, for Motorcycle Rally Dates Compared With Non-Rally Dates
eFigure 1. Comparison of Observed Effect Sizes to Effect Sizes Obtained From a Simulation of Randomly Assigned “Pseudo-Rally” Dates
References
- 1.Organ Procurement and Transplantation Network. National data reports. Accessed February 1, 2022. https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/.
- 2.National Highway Traffic Safety Administration . Fatality Analysis Reporting System (FARS) data tables. Accessed April 27, 2022. https://www-fars.nhtsa.dot.gov/Main/index.aspx.
- 3.National Center for Statistics and Analysis National Highway Traffic Safety Administration . Motorcycles: 2019 data (Traffic Safety Facts. Report No. DOT HS 813 112). 2021. Accessed October 6, 2022. https://crashstats.nhtsa.dot.gov/Api/Public/Publication/813112
- 4.Dickert-Conlin S, Elder T, Moore B. Donorcycles: motorcycle helmet laws and the supply of organ donors. J Law Econ. 2011;54(4):907-935. doi: 10.1086/661256 [DOI] [Google Scholar]
- 5.South Dakota Department of Transportation. Sturgis Motorcycle Rally Traffic Counts 2011–2020. August 2020. Accessed March 22, 2022. https://dot.sd.gov/media/documents/traffic/2020RallyTrafficReport.pdf
- 6.Kanny D, Schieber RA, Jones BH, Ryan GW, Sorensen BJ. Motorcycle casualties sustained during Daytona Beach Bike Week 2000: lessons learned. Ann Emerg Med. 2003;41(6):792-797. doi: 10.1067/mem.2003.191 [DOI] [PubMed] [Google Scholar]
- 7.DuPree C, Pinnola A, Gibson S, Muertos K, Davis JM, Sciarretta JD. Can planned traffic patterns improve survival among the injured during mass casualty motorcycle rallies? J Surg Res. 2019;234:262-268. doi: 10.1016/j.jss.2018.09.014 [DOI] [PubMed] [Google Scholar]
- 8.Massie AB, Kucirka LM, Segev DL. Big data in organ transplantation: registries and administrative claims. Am J Transplant. 2014;14(8):1723-1730. doi: 10.1111/ajt.12777 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.MacKinlay AC. Event studies in economics and finance. J Econ Lit. 1997;35(1):13-39. [Google Scholar]
- 10.Khullar D, Jena AB. “Natural experiments” in health care research. JAMA Health Forum. 2021;2(6):e210290. doi: 10.1001/jamahealthforum.2021.0290 [DOI] [PubMed] [Google Scholar]
- 11.Zou E, Worsham C, Miller NH, Molitor D, Reif J, Jena AB. Emergency visits for thunderstorm-related respiratory illnesses among older adults. JAMA Intern Med. 2020;180(9):1248-1250. doi: 10.1001/jamainternmed.2020.1672 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kato H, Jena AB, Tsugawa Y. Patient mortality after surgery on the surgeon’s birthday: observational study. BMJ. 2020;371:m4381. doi: 10.1136/bmj.m4381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Worsham CM, Woo J, Kearney MJ, Bray CF, Jena AB. Carbon monoxide poisoning during major U.S. power outages. N Engl J Med. 2022;386(2):191-192. doi: 10.1056/NEJMc2113554 [DOI] [PubMed] [Google Scholar]
- 14.Jena AB, Mann NC, Wedlund LN, Olenski A. Delays in emergency care and mortality during major U.S. marathons. N Engl J Med. 2017;376(15):1441-1450. doi: 10.1056/NEJMsa1614073 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barnett ML, Olenski AR, Jena AB. Patient mortality during unannounced accreditation surveys at US hospitals. JAMA Intern Med. 2017;177(5):693-700. doi: 10.1001/jamainternmed.2016.9685 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pinnola A, Sciarretta JD, Gibson S, et al. The vicious cycle of motorcycle rally casualties: a single center’s experience. Am Surg. 2018;84(1):114-117. doi: 10.1177/000313481808400131 [DOI] [PubMed] [Google Scholar]
- 17.Thorp SD, Le J, Adams NS, et al. Are motorcycles really “donorcycles”? examining organ donation rates between unhelmeted and helmeted motorcyclists. J Safety Res. 2020;75:173-177. doi: 10.1016/j.jsr.2020.09.006 [DOI] [PubMed] [Google Scholar]
- 18.French MT, Gumus G. Fast times during spring breaks: are traffic fatalities another consequence? Econ Inq. 2015;53(1):745-757. doi: 10.1111/ecin.12157 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Motorcycle Rally Locations and Dates
eTable 2. Adjusted Number of Organ Donors and Organ Transplants Per Day Per Region, for Motorcycle Rally Dates Compared With Non-Rally Dates
eFigure 1. Comparison of Observed Effect Sizes to Effect Sizes Obtained From a Simulation of Randomly Assigned “Pseudo-Rally” Dates