

Abstract
Objective
Exercise has beneficial effects on mood and anxiety symptoms. However, the impact of aquatic exercise on mood and anxiety symptoms has not been clearly confirmed. Therefore, this study aimed to synthesize and systematically analyze evidence available on boosting mental health through aquatic exercise.
Method
A systematic review and meta-analysis were conducted under the PRISMA 2020 guidelines. PubMed, BIOSIS Previews, PsycINFO, Medline, SPORTDiscus, Education Source, and Web of Science Core Collection (WoSCC) were searched in May 2022. The research included the influence of aquatic exercises on mood and anxiety symptoms. After assessing trial quality and completing data extraction, a meta-analysis was carried out through R software. The results were presented as a standardized mean difference (SMD) and the corresponding 95% confidence interval.
Results
A total of 18 original trials were included. People who received aquatic exercise intervention had a statistically significant reduction in mental disorder symptoms compared with before. The results were aquatic exercise [SMD = −0.77, 95% CI (−1.08, −0.47), I2 = 77%, P < 0.01], swimming [SMD = −0.51, 95% CI (−1.14, 0.12), I2 = 78%, P < 0.01], aquatic aerobics [SMD = −0.92, 95% CI (−1.32, −0.53), I2 = 78%, P < 0.01], moderate intensity [SMD = −0.75, 95% CI (−1.07, −0.43), I2 = 67%, P < 0.01], and low intensity [SMD = −1.07, 95% CI (−1.08, −0.47), I2 = 85%, P < 0.01].
Conclusion
Aquatic exercise could statistically significantly improve mental health. Light aquatic aerobics probably has a better effect on mood and anxiety symptoms. However, given the number and quality of included research, verifying the aforementioned conclusions requires a larger sample of high-quality studies.
Keywords: swimming, mental health, anxiety, depression, aquatic exercise, mood
Introduction
Mental health is critically important to everyone, everywhere (1). Mood and anxiety significantly diminish the quality of life and happiness of those who suffer from them (2). Some psychological problems become so severe that they can even lead to suicide. More than 90% of suicides in the West have been attributed to mood disorders (3). The prevalence of these conditions has a significant economic impact on society because of the difficulties they cause for affected individuals on a daily basis (4–6). One study from China found that in January and February 2020, 54% of subjects expressed psychological symptoms as severe or moderate, 29% of subjects reported moderate to serious anxiety, and approximately 17% of subjects reported moderate to severe depression (7). Therefore, finding some effective and acceptable intervention methods that can improve mood and anxiety symptoms is significant.
As a non-drug treatment for mental disorders, exercise has become the focus of more and more researchers' attention. Recent studies support that exercise, especially aerobic exercise (8) and physical activity, has beneficial effects on mental health (9). Exercise was promoted as the first level in the Canadian Clinical Guidelines 2016 emotional therapy (10).
Aquatic exercise, as a special aerobic exercise, has been shown to potentially benefit mood and anxiety (11–14). Aquatic exercise has many physiological benefits compared to land-based workouts because of the water's unique properties, such as buoyancy, pressure, resistance, and protection from skin irritation due to temperature and touch (15). As a result, when compared to other forms of exercise, aquatic exercise may prove to be the most effective in terms of its positive impact on mood. However, to our knowledge, no study has been conducted to synthesize the research on the psychological benefits of aquatic exercise. A systematic review of the studies and a meta-analysis are necessary to elaborate on the effect of aquatic exercise on mood and anxiety.
Furthermore, the effect of exercise on mental health is affected by many factors, including differences in individual characteristics and specific parameters of exercise intervention. Aging of both the body and mind may be associated with an increased probability of developing mood disorders (16). Exercise as an intervention to treat chronic diseases is associated with mood elevations in patients with various chronic diseases and disabilities (17). The type, intensity, and duration of exercise also affect the effect of exercise on mood. Specifically, long-time relaxing aerobic exercise may promote greater mood benefits (18–20). Although little evidence supports greater mood improvements in response to exercise among women, (21) some previous studies showed that exercise (dance, yoga, aerobic games, etc.) reduced depressive symptoms, with no moderating effect of sex (22–25). However, it is unclear whether there are differences in age, sex, disease, intensity, and duration in the impact of aquatic exercise on mood.
This study aimed to synthesize and systematically analyze the available evidence to determine the effect of aquatic exercise on mental health.
Methods
The systematic review and meta-analysis followed the guidance of the PRISMA 2020 statement (26).
Eligibility criteria
The eligibility and inclusion criteria of the article are as follows: 1) The study design must only include randomized controlled trials and quasi-experimental studies. 2) The article's full text must be available. 3) The article must be written in English. 4) It must only include peer-reviewed journal articles. 5) The subjects must be limited to humans. 6) Interventions must have included any type of aquatic exercise. 7) Mental health, mood, anxiety symptoms, depression, or related parameters in the study could be clearly extracted.
Aquatic exercise in the encyclopedia was defined as “an activity,” and the activity site must be in the water, such as a pool, lake, or ocean (27). Based on this, all types of exercise in water (such as swimming, aquatic exercise, and floating in water) were included in this study. Additionally, demographic restrictions were waived.
Information sources and search strategy
PubMed, BIOSIS Previews, PsycINFO, Medline, SPORTDiscus, Education Source, and Web of Science Core Collection were searched on May 28, 2022, for studies using the following combination of terms: “mental health,” “depression,” “anxiety,” “mood,” “POMS,” “BDI,” “BAI” in combination with “swim,” “aquatic,” “water sport,” and “aquatic exercise.” Table 1 shows the search strategies used for database searches (e.g., PubMed).
Table 1.
Search strategy in PubMed.
| Step | Search strategies |
|---|---|
| #1 | “swim” OR “aquatic” OR “water sport” [Mesh] |
| #2 | “swim” OR “aquatic exercise” OR “water sport” [Text Word] |
| #3 | #1 OR #2 |
| #4 | “mental health” OR “depression” OR “anxiety” OR “mood” [Mesh] |
| #5 | “mental health” OR “depression” OR “anxiety” OR “mood” [Text Word] |
| #6 | “POMS” OR “BDI” OR “BAI” [Text Word] |
| #7 | #4 OR #5 OR #6 |
| #8 | #3 AND #7 |
Study selection
All of the search results were imported into Endnote. The duplicate was searched by year, title, and author. After removing duplicates, two authors (ZYT and JML) independently screened the studies based on the title and the abstract. Only experimental articles defining the effect of aquatic exercise on human mood and anxiety symptoms were included. Following the initial screening, two authors searched the full text and further evaluated the research according to the eligibility criteria. We resolved differences through discussion with another author (YW). The selection process of the study was exhibited by a PRISMA 2020 flow diagram.
Assessment of trial quality and data extraction
Trial quality was assessed from the selected full-text articles by two authors—the studies' risk of bias was in accordance with the Cochrane Handbook for Systematic Reviews of Interventions. At the same time, the data for the article were extracted. The information from the included articles (author, date of publication, country, and study design), the characteristics of subjects (sample size, age, sex, health condition, etc.), and intervention (types of exercises, duration, frequency) were extracted from the included articles. Furthermore, outcomes measured (mean, SD) and measurement tools used (type of questionnaire) were extracted.
Synthesis and analysis
The meta-analysis was performed by R 4.2.1 software (“meta” package). The Chi-square test was performed to determine whether or not there were statistically significant differences between the research results. Multiple similar homogenous studies were considered if P ≥ 0.1, I2 < 50%, and meta-analysis using a fixed-effect model. If P < 0.1, I2 ≥ 50%, the random-effects model was used. Because of the different ranges and measurement methods of mental health in these studies, standardized mean difference (SMD) and a 95% confidence interval (CI) were used for continuous data.
Subgroup analysis
Subgroup analyses were grouped based on the following factors: age, disease, mode of exercise, type of mental health, duration of exercise, and intensity.
Results
Search strategy results
The PRISMA flow chart (Figure 1) shows the search strategy and details the selection of articles for this review. A total of 8,764 articles were retrieved on a database search. After removing duplicates, 6,715 were removed through reviewing the title and abstract. Afterward, of the remaining 45 articles, through the full-text review, 27 were eliminated, and 18 were included.
Figure 1.

PRISMA flow chart. The figure shows the search strategy and selection of articles in this study (18 articles were included at the end).
Study characteristics
Table 2 displays the general characteristics of the 18 articles, including the date of publication, the country, the study design, and the population of subjects.
Table 2.
General characteristics.
| No. | Year | Author | Country | N | Population characters | Age | Mode | Measurement tool | Duration (week) | Frequency (d/week) | Intensity | Duration of sessions (min) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1992 | Berger and Owen. (28) | United States | 39 | College students | 21 | Swim | Profile of Mood State (POMS) | 14 | 2 | Moderate | 40 |
| 2 | 1997 | Berger et al. (29) | Australia | 39 | Swimmers | 15 | Swim | POMS | 1 | 12 | High | 180 |
| 3 | 1999 | Tanaka et al. (30) | United States | 12 | Obese subjects with stages 1 to 2 essential hypertension | 48 | Swim | POMS | 10 | 3 | Moderate | 60 |
| 4 | 2001 | Webb and Drummond. (31) | Australia | 19 | Beach swimming participants | 26 | Swim | Spielberger State-Trait Anxiety questionnaire | 2 | N/Ra | Moderate | 240 |
| 5 | 2002 | Lindeman et al. (32) | Finland | 25 | Winter swimming | 50 | Winter swim | Crown Crisp Experimental Index (CCEI) | 32 | N/R | N/R | N/R |
| 6 | 2004 | Huttunen et al. (33) | Finland | 36 | Winter swimming | 53 | Winter swim | POMS | 16 | 4 | N/R | N/R |
| 7 | 2015 | Kim et al. (34) | Korea | 25 | Elderly women | 72 | Aquatic aerobics | POMS | 24 | 3 | Moderate | 60 |
| 8 | 2016 | Razazian et al. (35) | Switzerland | Female patients with multiple sclerosis | 34 | Aquatic aerobics | Beck's Depression Inventory (BDI) | 8 | 3 | Moderate | 60 | |
| 9 | 2018 | Aidar et al. (36) | Brazil | 19 | Persons with stroke | 52 | Aquatic aerobics | StateTrait Anxiety Inventory & BDI | 12 | 2 | Moderate | 60 |
| 10 | 2018 | Da Silva et al. (37) | Brazil | 29 | Hypertensive adults & health adults | 53 | Aquatic aerobics | BDI & Beck's Anxiety Inventory (BAI) | 12 | 2 | light | 45 |
| 11 | 2018 | Delevatti et al. (38) | Brazil | 17 | Patients with type 2 diabetes | 54 | Aquatic aerobics | BDI | 12 | 3 | high | 45 |
| 12 | 2019 | da Silva et al. (39) | United States | 30 | Nondepression elderly & elderly with depression | 58 | Aquatic aerobics | BDI & BAI | 12 | 2 | light | 45 |
| 13 | 2019 | de Oliveira et al. (38) | Brazil | 10 | Elderly women | 67 | Swim | Geriatric Anxiety Inventory (GAI) & Perceived Stress Scale | 12 | 2 | light | 45 |
| 14 | 2019 | Perez et al. (40) | Brazil | 10 | Patients with Parkinson's disease | 67 | Aquatic aerobics | Short Geriatric Depression Scale | 15 | 2 | light | 45 |
| 15 | 2019 | Sahin et al. (14) | Turkey | 30 | People with osteoarthritis | 63 | Aquatic aerobics | Hospital Anxiety and Depression Scale (HAD) | 3 | 5 | Moderate | 60 |
| 16 | 2020 | Useros et al. (41) | Chile | 15 | People with cervical dystonia | 48 | Aquatic aerobics | BDI & State-Trait Anxiety Inventory (STAI) | 4 | 1 | light | 50 |
| 17 | 2021 | da Silva et al. (42) | United States | 30 | Health adults &people with Type 2 diabetes mellitus | 64 | Aquatic aerobics | BDI & BAI | 12 | 0.5 | light | 41 |
| 18 | 2021 | Lee et al. (43) | Korea | 20 | Pre-frailty elderly women | 73 | Aquatic aerobics | POMS | 12 | 3 | Moderate | 60 |
N/R, Not reported.
Quality of the evidence
The assessment of trial quality was performed independently by two authors, according to Version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2) (44). All discrepancies were discussed or consulted with another author. After evaluating the risk of bias in studies, seven studies were considered to have a high bias risk arising from the randomization process, three studies were found to have an ambiguous bias risk due to deviations from intended interventions, and 12 studies were found to have complete data (Figure 2). Overall, six studies have low risk, five have some concerns, and seven have a high risk (Figure 3).
Figure 2.

Risk of bias summary.
Figure 3.

Risk of bias graph.
Effects of aquatic exercise on mental health
According to meta-analysis, people who were treated with aquatic exercise showed a statistically significant reduction in mental disorder symptoms compared to pro-intervention [SMD = −0.77, 95% CI (−1.08, −0.47), I2 = 77%, P < 0.01]. As depicted in Figure 4, aquatic exercise improves mood and anxiety symptoms.
Figure 4.

Forest plot of aquatic exercise effects on mood. The overall effect of aquatic exercise: [SMD = −0.77, 95% CI (−1.08, −0.47), I2 = 77%, P < 0.01].
Subgroup analysis
Subgroup: Age
Based on the age of the subjects, studies were divided into three groups, with an age range of <18 years, 18–64 years, and>64 years, respectively. Age groups were classified according to WHO standards (45). It can be observed that 18–64 years [SMD = −0.94, 95% CI (−1.34, −0.54), I2 = 80%, P < 0.01] were statistically significant through the subgroup analysis (Figure 5). There was no statistical significance in other groups. There was a statistically significant subgroup effect (P = 0.02).
Figure 5.

Forest plot of age. By subgroup analysis of the age, 18–64 years [SMD = −0.94, 95% CI (−1.34, −0.54), I2 = 80%, P < 0.01] were statistically significant.
Subgroup: Disease
Studies were divided into ten groups based on the subjects' physical health. It can be observed that the Health group [SMD = −0.64, 95% CI (−1.03,−0.25), I2 = 74%, P < 0.01], Hypertension group [SMD = −1.20, 95% CI (−3.31, 0.91), I2 = 92%, P < 0.01], and Depression group [SMD = −2.49, 95% CI (−6.47, 1.49), I2 = 96%, P < 0.01] were statistically significant through the subgroup analysis (Figure 6). There was no statistical significance in other groups. There was a statistically significant subgroup effect (P = 0.02).
Figure 6.

Forest plot of disease. By subgroup analysis of the disease, the Health group [SMD = −0.64, 95% CI (−1.03, −0.25), I2 = 74%, P < 0.01], Hypertension group [SMD = −1.20, 95% CI (−3.31, 0.91), I2 = 92%, P < 0.01], and Depression group [SMD = −2.49, 95% CI (−6.47, 1.49), I2 = 96%, P < 0.01] were statistically significant.
Subgroup: Mode of exercise
Based on the exercise mode of intervention, studies were divided into three groups. The swimming group included swimming learning courses, leisure swimming, and swimming training. The aquatic aerobics group included water walking, water gymnastics, and any form of aerobic exercise in water, except swimming. It can be observed that swim [SMD = −0.51, 95% CI (−1.14, 0.12), I2 = 78%, P < 0.01] and aquatic aerobics [SMD = −0.92, 95% CI (−1.32, −0.53), I2 = 78%, P < 0.01] were statistically significant through the subgroup analysis (Figure 7). There was no statistical significance in the winter swim. There was a statistically significant subgroup effect (P = 0.02).
Figure 7.

Forest plot of the mode of exercise. By subgroup analysis of the disease, swimming [SMD = −0.51, 95% CI (−1.14, 0.12), I2 = 78%, P < 0.01], and aquatic aerobics [SMD = −0.92, 95% CI (−1.32, −0.53), I2 = 78%, P < 0.01] were statistically significant.
Subgroup: Type of mental health
Based on the type of mental health intervention, studies were divided into three groups. It can be observed that anxiety [SMD = −1.28, 95% CI (−2.04, −0.53), I2 = 87%, P < 0.01] and depression [SMD = −0.52, 95% CI (−0.74, −0.30), I2 = 55%, P < 0.01] were statistically significant through the subgroup analysis (Figure 8). There was a statistically significant subgroup effect (P = 0.07).
Figure 8.

Forest plot of the type of mental health. By subgroup analysis of the disease, Anxiety [SMD = −1.28, 95% CI (−2.04, −0.53), I2 = 87%, P < 0.01] and Depression [SMD = −0.52, 95% CI (−0.74, −0.30), I2 = 55%, P < 0.01] were statistically significant.
Subgroup: Duration
Based on the duration of the subjects, studies were divided into three groups, with an age range of <4 weeks, 4–12 weeks, and>12 weeks, respectively. It can be observed that <4 weeks [SMD = −0.74, 95% CI (−1.11, −0.37), I2 = 70%, P < 0.01] and 4–12 weeks [SMD = −0.95, 95% CI (−1.45, −0.45), I2 = 82%, P < 0.01] were statistically significant through the subgroup analysis (Figure 9). There was no statistical significance in the> 12-week group. There was a statistically significant subgroup effect (P = 0.01).
Figure 9.

Forest plot of duration of exercise. By subgroup analysis of the disease, <4 weeks [SMD = −0.74, 95% CI (−1.11, −0.37), I2 = 70%, P < 0.01] and 4–12 weeks [SMD = −0.95, 95% CI (−1.45, −0.45), I2 = 82%, P < 0.01] were statistically significant through the subgroup analysis.
Subgroup: Intensity
Intensity was one of the most important parameters of exercise intervention. Heart rate, as the main indicator of intensity, was measured in most studies. Based on the report of the American College of Sports Medicine, < 64% of the maximum was considered low intensity, 64–76% of the heart rate maximum was regarded as moderate intensity, and 77–95% of the heart rate maximum was considered high intensity (46). However, a few studies did not report the measurement of intensity.
According to the intensity of the subjects, studies were divided into three groups, light, moderate, and high, respectively. It can be observed that moderate [SMD = −0.75, 95% CI (−1.07, −0.43), I2 = 67%, P < 0.01] and light [SMD = −1.07, 95% CI (−1.08, −0.47), I2 = 85%, P < 0.01] were statistically significant through the subgroup analysis (Figure 10). There was no statistical significance in the high group. There was a statistically significant subgroup effect (P = 0.04).
Figure 10.

Forest plot of the intensity of exercise. By subgroup analysis of the disease, moderate [SMD = −0.75, 95% CI (−1.07,−0.43), I2 = 67%, P < 0.01] and light [SMD = −1.07, 95% CI (−1.08, −0.47), I2 = 85%, P < 0.01] were statistically significant through the subgroup analysis.
Publication bias
The funnel plot indicates the possible publication bias (Figure 11). Furthermore, the Egger method was used for analysis. When the linear regression test was P < 0.01, the publication bias of studies was statistically significant.
Figure 11.
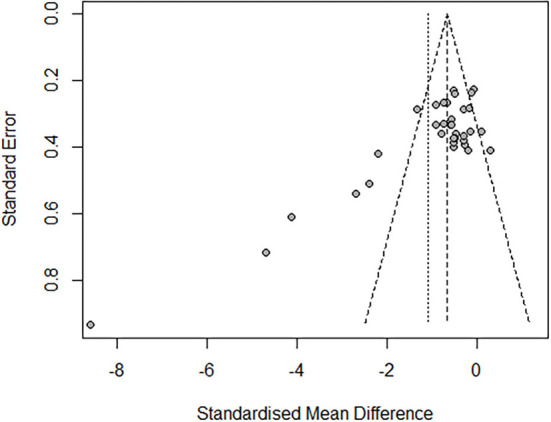
Funnel plot of publishing bias.
A sensitivity analysis was also conducted. A leave-one-out meta-analysis was used to test the publication bias of a single study (Figure 12). After sequentially removing each study, no studies affecting heterogeneity were found (I2 = 72%−78%). This analysis confirmed the stability of the results.
Figure 12.

Sensitivity analysis plot. A leave-one-out meta-analysis was used to test the publication bias of a single study. No studies affecting heterogeneity were found (I2 = 72–78%).
Discussion
This meta-analysis included 423 people who received aquatic exercise intervention; 18 studies synthesized the benefits of aquatic exercise, and the results revealed that aquatic exercise could statistically significantly improve mood and anxiety symptoms. The overall SMD = −0.77, [95% CI (−1.08, −0.47), I2 = 77%, P < 0.01].
Ten different states of physical health are included in this review. Few comparable studies of a particular disorder made it difficult to determine which states would reap the most benefits from aquatic exercise. Nevertheless, this review found that aquatic exercise may be effective for general states of physical health observed, especially depression and hypertension. It is possible that the exercise increases the secretion of the related release of b-endorphin and dopamine and provides a soothing effect (47), while the muscular resistance of the water is more than ten times higher than the resistance of land. Hence, it requires more activation of the motor cortex in the elderly (39). Besides, people with type 2 diabetes are usually not sufficiently active. Activation of the brain and mood improvement are potentially important motivators for exercise (48). For patients with hypertension, the levels of the cytokines (TNF-α and IL-6) could be reduced by participating in the aquatic exercise program, suggesting the inhibitory effect of aquatic exercise on the production of pro-inflammatory cytokines (37).
Aquatic exercise is particularly effective in reducing anxiety. Comparing the results of this study with other studies, a meta-analysis conducted by Song (49) found the effect of land-based aerobic exercise on anxiety (SMD:−0.50), traditional Chinese exercise (SMD:−0.03), and meditation (SMD: −0.15). The above three exercises are lower than aquatic exercises (SMD: −1.28). Several studies have also shown that aquatic exercise can boost mood (35, 40, 50). However, those studies were relatively narrow, focusing primarily on relatively menial land aerobic exercise. The effect of aquatic exercise is different from that of land exercise and needs further research.
Compared with land-based aerobic exercise, aquatic exercise shows its particularity. The sensation of water flowing through the skin when moving in water is difficult to obtain when moving on land. Several studies indicated that touch could reduce stress and improve mood (51–54). The reduction in gravity also reduces the load on the spine, knees, and other pain-prone areas. In addition to physical factors, aquatic exercises are difficult for some people, especially in the sea and other special environments; thus, “confronting challenges” was key to the impact of mood (55). Moreover, aquatic exercise serves to connect and convey a sense of nature. With the function of re-orientating and changing the sense of body, space, and gravity, people can expand their perspectives (56).
Regarding the intervention type of exercise, aquatic aerobics (SMD: −0.92) is better than swimming (SMD: −0.51), but these studies lack consistency. Swimming includes swim-learning programs (28, 38), swimming training for competition (29, 57), and leisure swimming (31, 58, 59). Swimming in different situations affects people's moods differently. Similarly, aquatic aerobics includes various forms. This may be one of the reasons for the high heterogeneity of research. In general, most of the aquatic aerobics' subjects are older or have ordinary diseases. Regarding safety and feasibility, older individuals prefer light, easy, and fun exercises over hard and stressful exercises (60). Therefore, they are more likely to benefit from water aerobics for their mental health than young, healthy adults. However, the trials in this study are insufficient for comparison. The specific impact needs further comparative study through similar samples. Winter swimming has little effect on improving mental health, which may be because the temperature stimulus of cold water is too strong, and then the body tends to remain tense (32, 33). For this reason, winter swimming may not be an effective way to improve mental health.
Based on the results of this study, the low intensity of aquatic exercise causes greater benefits for mental health. It may be that lower intensity makes people more relaxed (49). However, the acceptability of people of different ages and disease conditions to the intensity should also be considered, making it necessary to judge the research results carefully.
The influence of age and sex is not fully reflected in this study. In this study, the impact of exercise on the moods of the elderly was not statistically significant. The influence of age on the effect of exercise intervention is still controversial. A study of land-based exercise intervention shows that there were no significant differences in the amount of improvement between the younger and older exercise groups (61). However, some researchers find that exercise has greater distinct effects on brain activity and mood improvement in young people than in older people (62). Although the trials included in this investigation indicated the sex of the subjects, most studies were not classified by sex in the results, making sex-specific subgroup analysis challenging. Although some research (19, 25, 63, 64) suggests no difference in the positive effects of exercise based on sex, some evidence suggests that males may get greater advantages from exercise on their mood than females (65). Thus, more study is required to determine whether aerobic exercise has different effects on mood depending on gender and age.
There are a few limitations to this study. First, the between-study heterogeneity is significant, and our subgroup and sensitivity analyses cannot entirely account for it. Second, this study only selected articles published in English to limit the risk of bias. There may be influential publications written in languages other than English that were not included. Finally, non-randomized controlled trials were included, which may lead to selection bias. Given the limitations in our review, more large-scale research should be conducted in the future.
Conclusion
Aquatic exercise could statistically significantly improve mental health. Light aquatic aerobics may have a better effect on mood and anxiety symptoms. However, given the number and quality of included research, verifying the above conclusions requires a larger sample size of high-quality studies.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
ZT and YW conceived of the idea and designed the study protocol. YL conducted statistical analysis. ZT and JL drafted the manuscript. ZT, YW, JL, and YL participated in the revision of the manuscript of the study. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Tsinghua University Initiative Scientific Research Program 2021THZWJC15.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
- 1.World Health Organization . World Mental Health Report: Transforming Mental Health for All. WHO. (2022). [Google Scholar]
- 2.Boehm MA, Lei QM, Lloyd RM, Prichard JR. Depression, anxiety, and tobacco use: Overlapping impediments to sleep in a national sample of college students. J Am Colleg Health. (2016) 64:565–74. 10.1080/07448481.2016.1205073 [DOI] [PubMed] [Google Scholar]
- 3.Li N, Zhang J, Wang HY, Yang FR. Comparing suicide attempters with and without mental disorders: a study of young adults in Rural China. Community Ment Health J. (2020) 56:1372–9. 10.1007/s10597-020-00576-w [DOI] [PubMed] [Google Scholar]
- 4.Abdin E, Chong SA, Ragu V, Vaingankar JA, Shafie S, Verma S, et al. The economic burden of mental disorders among adults in Singapore: evidence from the 2016 Singapore Mental Health Study. J Mental Health. (2021). 10.1080/09638237.2021.1952958 [DOI] [PubMed] [Google Scholar]
- 5.Bebbington PE, McManus S. Revisiting the one in four: the prevalence of psychiatric disorder in the population of England 2000-2014. Br J Psychiatry. (2020) 216:55–7. 10.1192/bjp.2019.196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tan XW, Chong SA, Abdin E, Vaingankar J, Shafie S, Zhang Y, et al. Comorbidities within mental illnesses in a multiethnic urban population. Asian J Psychiatry. (2020) 51:102018. 10.1016/j.ajp.2020.102018 [DOI] [PubMed] [Google Scholar]
- 7.Wang CY, Pan RY, Wan XY, Tan YL, Xu LK, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. 10.3390/ijerph17051729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Morres ID, Hatzigeorgiadis A, Stathi A, Comoutos N, Arpin-Cribbie C, Krommidas C, et al. Aerobic exercise for adult patients with major depressive disorder in mental health services: a systematic review and meta-analysis. Depress Anxiety. (2019) 36:39–53. 10.1002/da.22842 [DOI] [PubMed] [Google Scholar]
- 9.Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry. (2005) 18:189–93. 10.1097/00001504-200503000-00013 [DOI] [PubMed] [Google Scholar]
- 10.Ravindran AV, Balneaves LG, Faulkner G, Ortiz A, McIntosh D, Morehouse RL, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 5. complementary and alternative medicine treatments. Can J Psychiatr. (2016) 61:576–87. 10.1177/0706743716660290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Da Silva LA, Doyenart R, Salvan PH, Rodrigues W, Lopes JF, Gomes K, et al. Swimming training improves mental health parameters, cognition and motor coordination in children with attention deficit hyperactivity disorder. Int J Environ Health Res. (2020) 30:584–92. 10.1080/09603123.2019.1612041 [DOI] [PubMed] [Google Scholar]
- 12.Lloret J, Gomez S, Rocher M, Carreno A, San J, Ingles E. The potential benefits of water sports for health and wellbeing in marine protected areas: a case study in the Mediterranean. Annal Leisure Res. (2021). 10.1080/11745398.2021.2015412 [DOI] [Google Scholar]
- 13.Neville C, Henwood T, Beattie E, Fielding E. Exploring the effect of aquatic exercise on behaviour and psychological well-being in people with moderate to severe dementia: A pilot study of the Watermemories Swimming Club. Aust Ageing. (2014) 33:124–7. 10.1111/ajag.12076 [DOI] [PubMed] [Google Scholar]
- 14.Sahin HG, Kunduracilar Z, Sonmezer E, Ayas S. Effects of two different aquatic exercise trainings on cardiopulmonary endurance and emotional status in patients with knee osteoarthritis. J Back Musculoskelet Rehabil. (2019) 32:539–48. 10.3233/BMR-171116 [DOI] [PubMed] [Google Scholar]
- 15.Noh DK, Lim J-Y, Shin H-I, Paik N-J. The effect of aquatic therapy on postural balance and muscle strength in stroke survivors - a randomized controlled pilot trial. Clin Rehabil. (2008) 22:966–76. 10.1177/0269215508091434 [DOI] [PubMed] [Google Scholar]
- 16.Cassilhas RC, Antunes HKM, Tufik S, de Mello MT. Mood. anxiety, and serum IGF-1 in elderly men given 24 weeks of high resistance exercise. Percept Mot Skills. (2010) 110:265–76. 10.2466/pms.110.1.265-276 [DOI] [PubMed] [Google Scholar]
- 17.Weinstein AA, Chin LMK, Collins J, Goel D, Keyser RE, Chan L. Effect of aerobic exercise training on mood in people with traumatic brain injury: a pilot study. J Head Trauma Rehabil. (2017) 32:E49–56. 10.1097/HTR.0000000000000253 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lane AM, Jackson A, Terry PC. Preferred modality influences on exercise-induced mood changes. J Sports Sci Med. (2005) 4:195–200. [PMC free article] [PubMed] [Google Scholar]
-
19.Oh S.
 . Effects of mood state change before and after exercising according to type and duration of exercise. Korean J Measurement Evaluation Physical Educat Sports Sci. (2005) 7:1–14. [Google Scholar]
. Effects of mood state change before and after exercising according to type and duration of exercise. Korean J Measurement Evaluation Physical Educat Sports Sci. (2005) 7:1–14. [Google Scholar] - 20.Rocheleau CA, Webster GD, Bryan A, Frazier J. Moderators of the relationship between exercise and mood changes: Gender, exertion level, and workout duration. Psychol Health. (2004) 19:491–506. 10.1080/08870440310001613509 [DOI] [Google Scholar]
- 21.McDowell CP, Campbell MJ, Herring MP. Sex-related differences in mood responses to acute aerobic exercise. Med Sci Sports Exerc. (2016) 48:1798–802. 10.1249/MSS.0000000000000969 [DOI] [PubMed] [Google Scholar]
- 22.Petty KH, Davis CL, Tkacz J, Young-Hyman D, Waller JL. Exercise effects on depressive symptoms and self-worth in overweight children: a randomized controlled trial. J Pediatr Psychol. (2009) 34:929–39. 10.1093/jpepsy/jsp007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Reigal R, Videra A. Effect of a physical activity session on mood. states. Rev Int Med Cienc Act Fis Dep. (2013) 13:783–98. [Google Scholar]
- 24.Oh S. The effects of the dance sports on mood states. Korea Sport Research. (2005) 16:197–204. [Google Scholar]
- 25.Kmiecik A, Bakota D, Plominski A. The level of mood regulation in practicing hatha yoga in the background of people who do not practice this physical activity. Physical Activity Review. (2020) 8:95–103. 10.16926/par.2020.08.11 [DOI] [Google Scholar]
- 26.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. 10.1136/bmj.n71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Donna B, Amy K, Jeffrey W. Gale Encyclopedia of Senior Health: A Guide for Seniors and Their Caregivers. Michigan, MI: Gale; (2009). p. 1873. [Google Scholar]
- 28.Berger BG, Owen DR. Mood alteration with yoga and swimming: aerobic exercise may not be necessary. Percept Mot Skills. (1992) 75:1331–43. 10.2466/pms.1992.75.3f.1331 [DOI] [PubMed] [Google Scholar]
- 29.Berger BG, Prapavessis H, Grove JR, Butki BD. Relationship of swimming distance, expectancy, and performance to mood states of competitive athletes. Percept Mot Skills. (1997) 84:1210. 10.2466/pms.1997.84.3c.1199 [DOI] [PubMed] [Google Scholar]
- 30.Tanaka H, Dale GA, Bassett DR. Influence of regular swimming on profile of mood states in obese subjects with essential hypertension. J pn J Phys Fit Sports Med. (1999) 48:447–52. 10.7600/jspfsm1949.48.447 [DOI] [Google Scholar]
- 31.Webb NL, Drummond PD. The effect of swimming with dolphins on human well-being and anxiety. Anthrozoos. (2001) 14:81–5. 10.2752/089279301786999526 [DOI] [Google Scholar]
- 32.Lindeman S, Hirvonen J, Joukamaa M. Neurotic psychopathology and alexithymia among winter swimmers and controls–a prospective study. Int J Circumpolar Health. (2002) 61:123–30. 10.3402/ijch.v61i2.17444 [DOI] [PubMed] [Google Scholar]
- 33.Huttunen P, Kokko L, Ylijukuri V. Winter swimming improves general well-being. Int J Circumpolar Health. (2004) 63:144. 10.3402/ijch.v63i2.17700 [DOI] [PubMed] [Google Scholar]
- 34.Kim I-M, Kim S-J, Park H-R, Lim J-H, Kim S-W. The long-term effect of aquarobics exercise program on physical function and mental health in elderly women. Indian J Sci Technol. (2015) 8:80987. 10.17485/ijst/2015/v8i26/80987 [DOI] [Google Scholar]
- 35.Razazian N, Yavari Z, Farnia V, Azizi A, Kordavani L, Bahmani DS, et al. Exercising impacts on fatigue, depression, and paresthesia in female patients with multiple sclerosis. Med Sci Sports Exer. (2016) 48:796–803. 10.1249/MSS.0000000000000834 [DOI] [PubMed] [Google Scholar]
- 36.Aidar FJ, Jaco de, Oliveira R, Gama de Matos D, Chilibeck PD, de Souza RF, Carneiro AL, et al. A randomized trial of the effects of an aquatic exercise program on depression, anxiety levels, and functional capacity of people who suffered an ischemic stroke. J Sports Med Physical Fitness. (2018) 58:1171–7. 10.23736/S0022-4707.17.07284-X [DOI] [PubMed] [Google Scholar]
- 37.Da Silva LA, Menguer L, Motta J, Dieke B, Mariano S, Tasca G, et al. Effect of aquatic exercise on mental health, functional autonomy, and oxidative dysfunction in hypertensive adults. Clin Exp Hypertens. (2018) 40:547–53. 10.1080/10641963.2017.1407331 [DOI] [PubMed] [Google Scholar]
- 38.de Oliveira DV, Muzolon LG, Antunes MD, Andrade do Nascimento Junior JR. Impact of swimming initiation on the physical fitness and mental health of elderly women. Acta Scientiarum-Health Sci. (2019) 41:43221. 10.4025/actascihealthsci.v41i1.43221 [DOI] [Google Scholar]
- 39.da Silva LA, Tortelli L, Motta J, Menguer L, Mariano S, Tasca G, et al. Effects of aquatic exercise on mental health, functional autonomy and oxidative stress in depressed elderly individuals: a randomized clinical trial. Clinics. (2019) 74:e322. 10.6061/clinics/2019/e322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Perez-de la Cruz S. Mental health in Parkinson's disease after receiving aquatic therapy: a clinical trial. Acta Neurologica Belgica. (2019) 119:193–200. 10.1007/s13760-018-1034-5 [DOI] [PubMed] [Google Scholar]
- 41.Useros-Olmo AI, Martinez-Pernia D, Huepe D. The effects of a relaxation program featuring aquatic therapy and autogenic training among people with cervical dystonia (a pilot study). Physiother Theory Pract. (2020) 36:488–97. 10.1080/09593985.2018.1488319 [DOI] [PubMed] [Google Scholar]
- 42.da Silva LA, Menguer LdS, Doyenart R, Boeira D, Milhomens YP, Dieke B, et al. Effect of aquatic exercise on mental health, functional autonomy, and oxidative damages in diabetes elderly individuals. Int J Environ Health Res. (2021) 32. 10.1080/09603123.2021.1943324 [DOI] [PubMed] [Google Scholar]
- 43.Lee E, Lim S-T, Kim W-N. Aquatic exercise for improving immune function and mental stress in pre-frailty elderly women. J Women Aging. (2021) 33:611–9. 10.1080/08952841.2020.1735287 [DOI] [PubMed] [Google Scholar]
- 44.Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ-Br Med J. (2019) 2019:366. 10.1136/bmj.l4898 [DOI] [PubMed] [Google Scholar]
- 45.World Health Organization . Global Recommendations on Physical Activity for Healthl WHO. (2010). [PubMed] [Google Scholar]
- 46.Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. (2011) 43:1334–59. 10.1249/MSS.0b013e318213fefb [DOI] [PubMed] [Google Scholar]
- 47.Salmon P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: a unifying theory. Clin Psychol Rev. (2001) 21:33–61. 10.1016/S0272-7358(99)00032-X [DOI] [PubMed] [Google Scholar]
- 48.O'Halloran PD. Mood changes in weeks 2 and 6 of a graduated group walking program in previously sedentary people with type 2 diabetes. Aust J Prim Health. (2007) 13:68–73. 10.1071/PY07009 [DOI] [Google Scholar]
- 49.Song J, Liu Z-z, Huang J, Wu J-s, Tao J. Effects of aerobic exercise, traditional Chinese exercises, and meditation on depressive symptoms of college student A meta-analysis of randomized controlled trials. Medicine. (2021) 100:23819. 10.1097/MD.0000000000023819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Delevatti RS, Schuch FB, Kanitz AC, Alberton CL, Marson EC, Lisboa SC, et al. Quality of life and sleep quality are similarly improved after aquatic or dry-land aerobic training in patients with type 2 diabetes: a randomized clinical trial. J Sci Med Sport. (2018) 21:483–8. 10.1016/j.jsams.2017.08.024 [DOI] [PubMed] [Google Scholar]
- 51.Espi-Lopez GV, Serra-Ano P, Cuenca-Martinez F, Suso-Marti L, Ingles M. Comparison between classic and light touch massage on psychological and physical functional variables in athletes: a randomized pilot trial. Int J Ther Massage Bodywork. (2020) 13:30–7. 10.3822/ijtmb.v13i3.551 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Roberts NA, Burleson MH, Pituch K, Flores M, Woodward C, Shahid S, et al. Affective experience and regulation via sleep, touch, and “sleep-touch” among couples. Affective Sci. (2022) 3:353–69. 10.1007/s42761-021-00093-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Lafreniere KD, Mutus B, Cameron S, Tannous M, Giannotti M, Abu-Zahra H, et al. Effects of therapeutic touch on biochemical and mood indicators in women. J Altern Complement Med. (1999) 5:367–70. 10.1089/acm.1999.5.367 [DOI] [PubMed] [Google Scholar]
- 54.von Mohr M, Kirsch LP, Fotopoulou A. The soothing function of touch: affective touch reduces feelings of social exclusion. Sci Rep. (2017) 7:13516. 10.1038/s41598-017-13355-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Burlingham A, Denton H, Massey H, Vides N, Harper M. Sea swimming as a novel intervention for depression and anxiety-A feasibility study exploring engagement and acceptability. Ment Health Physical Activity. (2022) 23:100472. 10.1016/j.mhpa.2022.100472 [DOI] [Google Scholar]
- 56.Denton H, Aranda K. The wellbeing benefits of sea swimming. Is it time to revisit the sea cure? qualitative research in sport. Exerc Health. (2020) 12:647–63. 10.1080/2159676X.2019.1649714 [DOI] [Google Scholar]
- 57.Boadas A, Osorio M, Gibraltar A, Rosas MM, Berges A, Herrera E, et al. Favourable impact of regular swimming in young people with haemophilia: experience derived from 'Desafio del Caribe' project. Haemophilia. (2015) 21:E12–E8. 10.1111/hae.12576 [DOI] [PubMed] [Google Scholar]
- 58.Driver S, Rees K, O'Connor J, Lox C. Aquatics, health-promoting self-care behaviours and adults with brain injuries. Brain Injury. (2006) 20:133–41. 10.1080/02699050500443822 [DOI] [PubMed] [Google Scholar]
- 59.Dundar U, Solak O, Toktas H, Demirdal US, Subasi V, Kavuncu V, et al. Effect of aquatic exercise on ankylosing spondylitis: a randomized controlled trial. Rheumatol Int. (2014) 34:1505–11. 10.1007/s00296-014-2980-8 [DOI] [PubMed] [Google Scholar]
- 60.Hyodo K, Suwabe K, Yamaguchi D, Soya H, Arao T. Comparison between the effects of continuous and intermittent light-intensity aerobic dance exercise on mood and executive functions in older adults. Front Aging Neurosci. (2021) 13:23243. 10.3389/fnagi.2021.723243 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Annesi JJ. Mood states of formerly sedentary younger and older women at weeks 1 and 10 of a moderate exercise program. Psychol Rep. (2004) 94:1337–42. 10.2466/PR0.94.3.1337-1342 [DOI] [PubMed] [Google Scholar]
- 62.Moraes H, Deslandes A, Silveira H, Ribeiro P, Cagy M, Piedade R, et al. The effect of acute effort on EEG in healthy young and elderly subjects. Eur J Appl Physiol. (2011) 111:67–75. 10.1007/s00421-010-1627-z [DOI] [PubMed] [Google Scholar]
- 63.Sexton H, Sogaard AJ, Olstad R. How are mood and exercise related? Results from the Finnmark study. Soc Psychiatry Psychiatr Epidemiol. (2001) 36:348–53. 10.1007/s001270170040 [DOI] [PubMed] [Google Scholar]
- 64.McLafferty CL, Wetzstein CJ, Hunter GR. Resistance training is associated with improved mood in healthy older adults. Percept Mot Skills. (2004) 98:947–57. 10.2466/pms.98.3.947-957 [DOI] [PubMed] [Google Scholar]
- 65.Williams CF, Bustamante EE, Waller JL, Davis CL. Exercise effects on quality of life, mood, and self-worth in overweight children: the SMART randomized controlled trial. Transl Behav Med. (2019) 9:451–9. 10.1093/tbm/ibz015 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.