

Abstract
Millions of Americans struggle with depression, a condition characterized by feelings of sadness and motivation loss. To understand how individuals managing depression conceptualize their self-management activities, we conducted visual elicitations and semi-structured interviews with 30 participants managing depression in a large city in the U.S. Midwest. Many depression support tools are focused on the individual user and do not often incorporate social features. However, our analysis showed the key importance of sociality for self-management of depression. We describe how individuals connect with specific others to achieve expected support and how these interactions are mediated through locations and communication channels. We discuss factors influencing participants’ sociality including relationship roles and expectations, mood state and communication channels, location and privacy, and culture and society. We broaden our understanding of sociality in CSCW through discussing diffuse sociality (being proximate to others but not interacting directly) as an important activity to support depression self-management.
Keywords: Depression, sociality, diffuse sociality, self-management, location, communication channels, mental health support technology, relationship roles
1. INTRODUCTION
Approximately 16.2 million U.S. adults experienced a depressive episode in 2016 [143]. Symptoms of depression include negative thoughts, feelings of sadness, lack of enjoyment of activities, agitation, sleep disruption, and lack of motivation [11]. Individuals often experience depression alongside other mental and physical health conditions, most commonly anxiety. Further, individuals with depression can experience difficulty establishing and maintaining social relationships [122,131]. Feelings of isolation and loneliness may lead to reoccurring challenges in symptom management [67]. Addressing these challenges requires ongoing work to prevent or reduce the intensity of future depressive episodes.
Self-management includes the day-to-day practices of an individual to control or reduce the impact of their condition within daily life [27]. Individuals manage their depression symptoms to get through their day, compete tasks, and engage in various life activities. The “self” in self-management practices may imply that these are solitary activities, but as we will explore in this work, these practices often happen within a social context and can involve other people. Some individuals also seek professional mental health care. However, there are barriers to receiving such professional care including cost, availability, and stigma [93]. For example, individuals in the U.S. seeking treatment for their depression often face significant wait times due to unavailability of clinical psychologists and other mental health services, particularly in rural areas [64]. Given these barriers, self-management is a way that individuals address their symptoms. However, these practices go beyond “treating” symptoms. Individuals with depression engage in these activities to improve their overall quality of life. Consequently, understanding the activities individuals do to self-manage their condition are of particular importance.
To support self-management practices, researchers and designers in CSCW, Human-Computer Interaction (HCI), and Psychology have begun to investigate the potential for technology-based approaches to mental health treatment (e.g., [24,39,95,120]). However, these tools do not yet integrate well into the daily lives and routines of users and have so far not been sustainable [127]. To start to address these issues of integration and sustainability, we undertook a “bottom-up” investigation to understand how individuals conceptualized their own depression self-management activities. We conducted interviews and visual elicitations with 30 individuals managing depression living in a large city in the U.S. Midwest. We primarily draw on the visual elicitation activity for this paper. We encouraged participants to build a holistic picture of the values, behaviors, and preferences that informed their individual, day-to-day activities managing the symptoms and effects of depression. We provide more details about this activity in the methods section.
We found that a key ingredient for effective self-management is sociality. Sociality refers to the social interactions and relationships within an individual’s life [93]. Within CSCW, researchers are beginning to investigate the role that social relationships play in the self-management of mental health conditions, particularly the supportive practices that individuals enact through these relationships (e.g., sharing personal health data to support bipolar disorder management [98]). By using the lens of sociality to understand our participants’ day-to-day activities, we highlight how social relationships factor into mood and symptom
In this paper, we use sociality to better understand and unpack the social self-management activities of individuals managing depression. We present the professional and non-professional ties with whom they connect and detail locations where they conduct these activities. We also analyze the in-person and technology-mediated communication channels they select to enable their sociality. In our discussion, we unpack factors influencing participant sociality including relationship roles and expectations, mood state and communication channel selection, location and privacy, and culture and society. Finally, we extend the CSCW discussion of sociality by presenting the benefits of “diffuse sociality” – being in proximate location to others but not directly interacting (e.g., studying at a coffee shop; playing online games).
2. RELATED WORK
Health has long been of interest to the CSCW community. As Fitzpatrick and Ellingson [48] highlight, CSCW researchers have investigated work practices and technologies (i.e., electronic health records) within clinical settings for many years. More recently, the research space has widened to include the home context, and wellness. This growing interest regarding how individuals manage their health outside the clinical context highlights opportunities to explore health conditions that often have to be self-managed by individuals [43]. One such condition is depression. In this section, we overview research regarding self-management tools for depression. We then discuss CSCW research on sociality and mental health†.
2.1. Toward Collaborative Self-Management Tools for Depression
Much of the self-management literature in CSCW (and more broadly in HCI) focuses on chronic physical disease(s) (e.g., diabetes [86,124,125]; cancer [32,42,56]; chronic kidney disease [41,133]). This literature describes important care activities supported by family members or healthcare professionals. Work in this area strongly underlines the often essential collaborative nature of supporting long-term health management [119,139,140].
However, most tools for depression self-management have limited, if any, social interaction-based features. Current technologies focus largely on individual psychoeducation and skills practice such as cognitive reframing using smartphone apps [95,120]. A few technologies offer occasional interaction with clinicians, but this is usually for crisis support or as an extension to therapy. For example, Internet-based Cognitive-Behavioral Therapy (iCBT), delivered through module-based online programs, has demonstrated efficacy in reducing symptoms of depression, both with and without clinician guidance [68,73]. Researchers have also explored context sensing to help predict episodes of depression with tools such as Mobilyze! [23]. Other tools encourage novel visualizations of the mind such as neurofeedback [24], or enable individuals to monitor emotions over time [39,78]. Many of these tools adapt techniques used in therapeutic practice to online and smartphone applications and, therefore, lack support for broader social interaction (e.g., [90,115]).
Furthermore, despite the growing number of tools for depression support, adherence to and long-term engagement with digital mental health tools remains a major challenge. Many of these resources have been developed and delivered in a “top-down” manner following clinical practices that may not align with the day-to-day routines, needs, or motivations of users [127]. While many of these tools have been shown to be efficacious, adoption has been low [94,96]. Consequently, there is a need to better understand how individuals managing mental health needs conceptualize their own self-management activities to improve the design of these tools.
In other areas of mental health research, scholars have begun to investigate the potential of social features integration into support technologies. For example, HORYZON [1] uses peer-to-peer social networking and expert moderation features to support first-episode psychosis recovery. Similarly, in a twist on common tracking features, the MONARCA system [8], designed for individuals managing bipolar disorder, captures not only biometric data such as hours slept, but also collects data regarding an individual’s amount of texting and social activities to recognize early warning signs of a manic or depressive episode.
Social feature integration is a promising future avenue for depression self-management support. However, further research is needed to deeply understand current contexts and conceptualizations of self-management to create effective tools sensitive to the needs of these individuals. We explore these topics in this study. In summary, the majority of current self-management technologies for depression (e.g., [24,39,95,120]) do not support the social interactions and nuances of relationships within an individual’s wider support network. This is a missed opportunity because connecting with close relationships has been shown in the chronic physical disease literature to be key to sustainable self-management [101,124,133] and has been shown in numerous social support studies to be beneficial for mental health [16,18,29,104]. Current technology tools for self-management of depression were designed to deliver mental health support services based on clinical best practices, however these tools have not yet fully envisioned the role that the user’s support network can play in the self-management process.
In the next section we discuss current work regarding sociality in health and wellness-focused CSCW research.
2.2. Sociality in CSCW
Sociality is a core part of CSCW. Within health and wellness-focused CSCW research, sociality is discussed as the various ways that people interact socially, their social goals, and their challenges in achieving those goals [7,45,46,81]. Sociality is mediated through verbal and nonverbal cultural cues (e.g., norms of conversation) and artifacts including technologies such as computer-mediated communication tools [92,93]. Sociality is also connected to both individual and community well-being [52].
Much of the current research on sociality as it relates to health and wellness in CSCW and HCI has focused on direct interaction explored in three key ways: deliberate communication, spontaneous communication, and the location of social interactions. First, researchers have studied how deliberate communication activities (e.g., conversations; messages) promote health. Researchers have investigated these activities within the context of individuals having face-to-face conversations with peers [118] and healthcare providers [12,13,82], and individuals communicating through digital technologies including mobile communication [10,66], and online interactions [15,87] particularly within online communities [21,63,79,99,110,141]. Second, there is growing interest in understanding how “accidental” encounters can also be beneficial to individuals. In research focused on older adults, Light et al. [80] describe the importance of protecting and maintaining social aspects of one’s life and engagement in meaningful activities in retirement. The authors extend our understanding of sociality from deliberate direct communication to include “serendipitous sociality while out and about.” They note how incidental connections made with others throughout the day, in addition to expected planned interactions, are also important for wellbeing. While Light et al.’s study begins to highlight the breadth of meaningful social activities for health and wellbeing, it still focuses on direct social connections. Finally, recent work has started to shift our focus on sociality by exploring where these interactions are taking place. For example, in the context of individuals with autism, Ringland et al. [114] critique the presumed superiority of face-to-face social interaction and show the essential nature of digital play spaces for children with autism. Their work shows the importance of attending to people’s social interactions in both physical and online locations and asserts that these online social interactions have the same meaning and importance as those made face-to-face. Collectively, these studies highlight how sociality encompasses direct social interactions, which may be spontaneous or deliberate and may occur in physical or virtual space. However, we currently lack an understanding of how indirect social interactions beyond conversations and messages may be useful for individuals’ health and wellness.
CSCW researchers have also explored the challenges of being social, particularly for populations where social interactions may be difficult, and have sought to support their social needs. For example, researchers have illuminated some of the challenges of social interactions in the context of the work of caregivers supporting individuals with chronic disease and cognitive conditions including diabetes [75,119] and dementia [130]. For these caregivers, the often reduced ability to communicate face-to-face with their care recipient(s) and difficulty maintaining previous routines of social interaction (e.g., connecting with friends) outside care settings can be particularly exhausting and isolating. Chen et al. [26] note that for their caregiver participants “socializing is an important aspect of life that has been deeply disrupted by the work of caregiving.”
To begin to address challenging social interaction contexts, researchers have created novel ways to create opportunities for sociality [81,113]. Unbehaun et al. [130] created novel video games to create opportunities for conversation and richer social interaction between individuals with dementia and their caregivers, overcoming often strained social relations. Ringland et al. [111] found that online communities and worlds provide essential spaces to support social play in contexts where the physical environment and cultures of the playground made sociality difficult for children with autism. In another study about young adults with autism, Hong et al. [60] demonstrate how technology can support movement toward independence by receiving advice and feedback from a supportive network.
In general, wellbeing and, more specifically, mental health is impacted by the ability to access desired forms of social interaction. Yet much of the previous wellness research has focused narrowly on the concept of social support [16,72,83,105]. Here we follow Liu et al. [83], who used Barrera and Ainley [9] to define social support as encompassing six categories: material aid, behavioral assistance, intimate interaction, guidance, feedback, and positive social interaction. CSCW researchers have explored social support within varied contexts including parenting [2], gender transitioning [53], and grieving and loss of a loved one [19]. However, while these studies have focused on “positive interpersonal relationships” [9], we know less about the role that social interactions more broadly influence individual’s mental health and wellbeing. Specifically, we still need to better understand sociality for self-management purposes, particularly within the sensitive and nuanced context of mental health. Our research helps to develop an understanding of socially-oriented depression self-management practices, and the contextual factors that influence the social activities of these individuals and their social networks.
In the following section we describe CSCW research regarding mental health and social interactions.
2.2.1. Mental Health and Sociality.
Current mental health research in CSCW has largely analyzed social media. Several studies have used social media scraping to gather and classify activities of individuals managing mental health needs. For example, researchers have created classification algorithms to detect activity potentially indicative of depression on Twitter [34,128] and Facebook [33]. Other studies have investigated disclosures of mental illness on social media using computer vision techniques [88], machine learning algorithms [35], and content analysis methods to investigate images, text, and commenting behaviors. However, Feuston and Piper [46] critique these approaches to behavior classification, highlighting that to understand the nuanced goals of expression by individuals managing mental illness, we need to also focus on the individuals themselves.
Other work has examined peer support enacted through online forums and other technologies. Peers with shared experience managing mental health concerns are often a key resource for discussing problems and sharing information [102]. For instance, research has shown that women with concerns about postpartum depression use public forums to seek emotional support and to ask and answer questions related to symptoms, diagnosis, treatment, and care [44]. However, in an online community for LGBTQ youth, Homan et al. [59] found that users who were less woven into the social fabric of the community were more likely to be experiencing depression. Online peer support can be useful, but may not be as helpful for all users.
Critically, very little research thus far focuses on understanding the social interactions of individuals who are managing mental health needs together with their support networks. A few studies have shed light on the sociality of family members and caregivers of individuals with depression [14,129,139,140]. However, while this work provides some insights into understanding the social activities of the individuals managing depression, there needs to be more focus on how these individuals self-conceptualize their own sociality. This is particularly important in order to effectively incorporate sociality into self-management technologies.
Park’s investigation of young adults’ practices of social support for mental health starts to explore this question [104]. Park found that college students reach out to close friends, parents, and acquaintances expecting different types of interactions such as empathetic listening or reassurance of unconditional support. The focus of this study was managing general mental health needs during college. For bipolar disorder participants sharing personal informatics, Murnane et al. [98] also noted the importance of connecting to different roles (e.g., healthcare providers; family members) to understand and take action regarding their data. However, beyond these few studies, researchers have not yet examined the role of social activities for individuals with mental health challenges from their own perspective.
2.3. Summary
As this section highlights, there is a range of CSCW and broader HCI research pertaining to health and well-being and specifically mental health. While as a field, we have started to improve our understanding of mental health and how we can support individuals managing their mental health, there are still a number of issues we need to more deeply explore. In this paper, we turn our attention to better understanding how individuals conceptualize their self-management activities to address symptoms of depression, and the role that social interactions play in helping them to address these symptoms.
3. METHOD
Qualitative researchers have a long history of using various types of elicitation to gather reactions and explore new lines of questioning with participants [28,51,54,144]. Visual elicitation in particular has been used as a constructionist and emotionalist [132] approach to gathering information from individuals about how they see and interpret elements of the world and how they think about relationships between those elements.
Here, we use a specific form of visual elicitation called graphic elicitation [31] which involves “presenting interviewees with a diagrammatic representation of the domain with which they are involved.” Diagrams can provide a “common conceptual foundation” [31] to guide discussion in qualitative research. We used this method to provide a common framework for discussing self-management activities to help participants think through the interrelated aspects of their self-management and to enable the research team to compare across participant responses.
3.1. Participants
This research, and our recruitment practices, were approved by the authors’ university institutional review board. Participants were recruited through four means: (1) online posts to local Facebook groups; (2) flyers posted to local libraries and public spaces; and (3) a study recruitment email from a patient registry through a partner research group in the University’s clinical psychology department; and (4) via an email to a local Meetup group for depression peer support.
We recruited participants who were comfortable conducting the interview in English, were 18 years or older, and currently managing depression or had received a diagnosis of depression within the last 12 months. All participants lived or worked in the geographic area of the large Midwestern city where the University is located. From our demographic survey of participants, 57% of our sample self-reported as white, 43% were mixed race or people of color, and 30% indicated Hispanic origin. Participants ranged in age from 18 to 72. Less than half (40%) reported full-time employment, 20% were full-time students, 17% worked part-time, 13% were unemployed or underemployed, and 10% indicated “other” (e.g., retired, or on disability). As highlighted in Table 1, participants had been self-managing depression for varying lengths of time, some newly-diagnosed and others for many years (min a few months; max 25 years).
Table 1.
Study Participants
| Participant Number | Age | Gender | Years managing condition | Participant Number | Age | Gender | Years managing condition |
|---|---|---|---|---|---|---|---|
| P01 | 22 | Male | 5 | P16 | 51 | Female | 16 |
| P02 | 32 | Female | 3 | P17 | 18 | Female | 1 |
| P03 | 32 | Male | 6 | P18 | 52 | Male | 1 |
| P04 | 24 | Female | 7 | P19 | 21 | Female | 1 |
| P05 | 44 | Female | 12 | P20 | 72 | Female | 10 |
| P06 | 36 | Female | 15 | P21 | 34 | Female | 6 |
| P07 | 32 | Female | 1 | P22 | 28 | Male | 3 |
| P08 | 48 | Male | 19 | P23 | 52 | Female | 25 |
| P09 | 31 | Male | 2 | P24 | 21 | Male | 1 |
| P10 | 40 | Male | 1 | P25 | 33 | Female | 17 |
| P11 | 29 | Female | 8 | P26 | 44 | Left blank | 1 |
| P12 | 21 | Female | A few months | P27 | 48 | Female | 2 |
| P13 | 20 | Female | A few months | P28 | 31 | Female | 2 |
| P14 | 20 | Female | 2 | P29 | 18 | Left blank | 2 |
| P15 | 54 | Female | 25 | P30 | 36 | Female | 22 |
3.2. Data Collection
We coordinated via email to meet with each participant for data collection in a location of their preference. Our aim was always to maximize participant comfort. Therefore, we met some participants in public libraries and coffee shops, some participants came to our lab across our two campus locations, and we also conducted a few interviews in participant homes. We compensated each individual $25 for their time. Study lengths among participants ranged from 75 to 90 minutes.
3.2.1. Study Session Process.
After completing a short demographic survey, each participant completed a 45-minute semi-structured interview. We used an interview protocol with a variety of questions about technology and self-management routines. After the interview, participants took part in a visual elicitation activity for the final 30 to 40 minutes of the session. The visual elicitation data is the main focus of the analysis for this paper. The visual elicitation for each participant consists of two structured worksheets, completed in response to prompted scenarios we detail below.
Structured worksheets.
Researchers provided each participant with two worksheets, each with 5 boxes labeled Spaces, Resources, People, Technologies, Actions, & Results (see Figure 1). The boxes were chosen to provide data to guide (re)design of systems for supporting self-management. We did not expect comprehensive coverage, but used the worksheet structure to obtain a consistent “picture” of activities as they were described by our participants. We were particularly curious about outcomes in our research because we wanted to understand what goals and outcomes might look like from our participant’s perspective. Clinical outcomes and participant-perceived outcomes may be different or overlap, but critically they are often expressed using different language (i.e., clinical vs. patient). Therefore, we sought to capture their activities and management expectations in their own words. The visual elicitation created a reliable avenue to gain diagrams of daily management support while allowing flexibility for participants to define their own “success” in the outcomes space. The worksheet was offered as a space for participants to respond to two scenario prompts, given in the following order for each participant. Below, we provide more details about each scenario.
Figure 1.
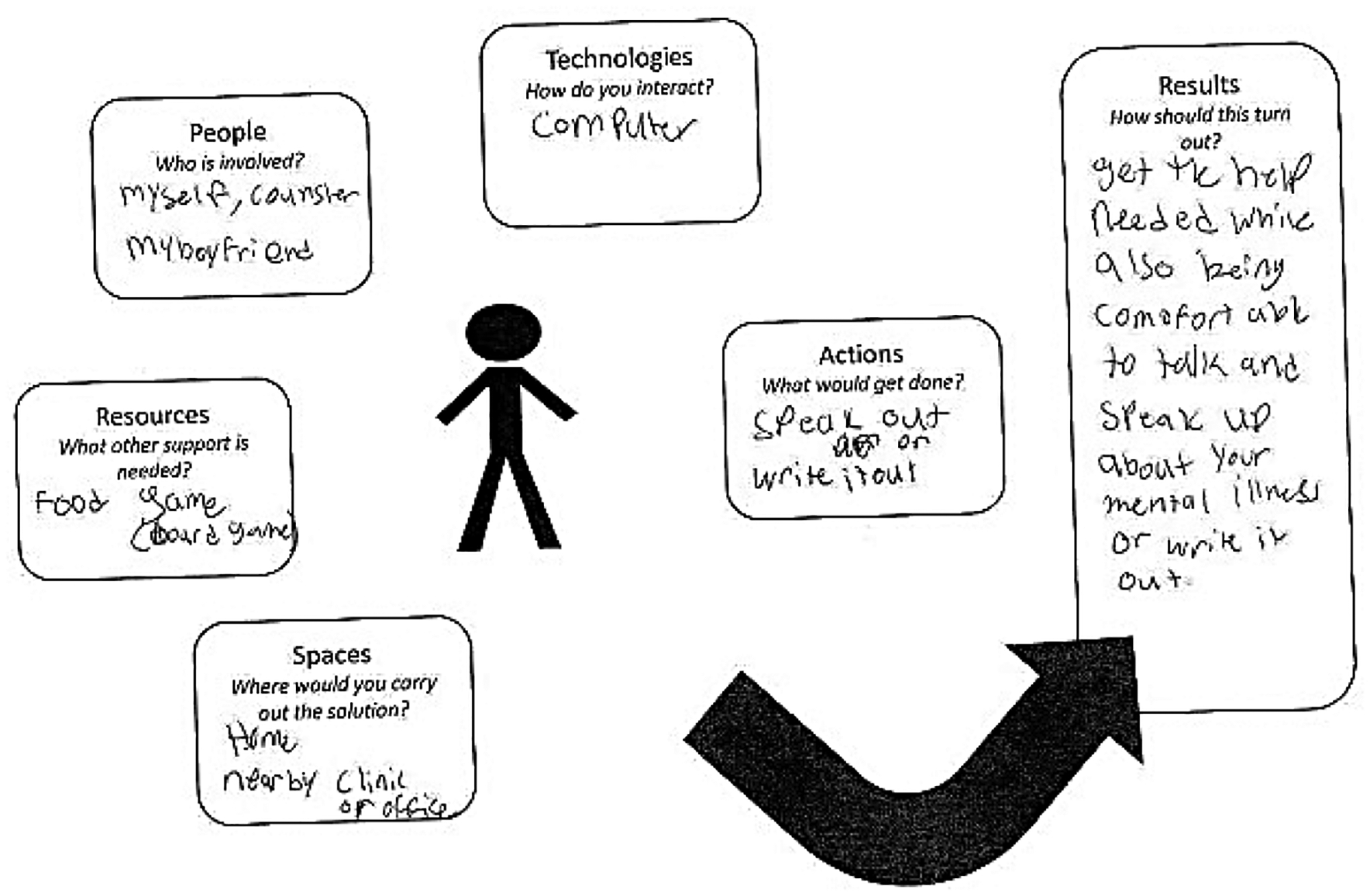
Scenario 2 Worksheet for P01
Prompted scenario 1.
“Imagine you’re having a bad day, feeling anxious or tired. How do you best take care of yourself in that situation? How would you try and improve your day and your feelings using the worksheet to illustrate your solution?” We designed this to investigate participant’s current self-management routines (e.g., their response to a problem situation without access to clinical resources, or a mental health expert).
Prompted scenario 2:
“On days you’re struggling with your moods or motivation, you are given the opportunity to get instant, on-demand support from someone who can provide you expert counseling. What would you like that support to be like, using the worksheet to illustrate it?” We designed this scenario to investigate how participants would conceptualize a management routine with access to clinical resources (e.g., connection with a mental health expert; we left the concept of “expert” vague, as individuals with depression may view a member of the clergy, or other influential person in their life, a preferable source of support than a clinical expert).
Participants completed their response to scenario 1 before moving on to scenario 2. Researchers directed participants to respond to the scenarios by writing text on their worksheets as they saw fit. Some participants spoke aloud during the exercise, and other participants who were silent as they completed the worksheet were prompted to walk the researcher through each section, providing more detail. One participant was not willing to put his handwriting on study materials other than the consent form; in this case we used his audio transcript in lieu of the visual elicitation document.
After both scenarios were completed, the researchers placed the scenarios side by side, facing the participant. At this point, the researcher asked the participant questions to compare and contrast responses to each scenario. Such questions included: What are some differences between the two solutions you made up? Looking at the results box, how do you know when you achieve good results? What is the most important element of the scenario? Participant interview and visual elicitation descriptions were audio-recorded and transcribed, and scenario worksheets for each participant were scanned and digitized for analysis alongside the transcripts.
3.3. Data Analysis
Four members of the research team used qualitative data analysis methods to analyze the last two questions of the semi-structured interview component (Who do you consider to be an expert about managing moods or emotions? and, Who do you consider to be an expert in managing your moods or emotions?), the visual elicitation documents, and audio transcripts of the visual elicitation activities. We describe our process below.
Beginning with a sorting exercise to examine initial patterns across the visual elicitation documents, we organized all the documents within Scenario 1 and then Scenario 2 separately developing several categories including types of technologies, and how many people were involved in desired social interactions, among others. We recorded these categories in Excel. During the sorting process, we realized that there was significant overlap in many aspects of the documents, and therefore conducted our following analysis across both scenarios.
We followed the Braun & Clarke thematic analysis process [17], starting with open coding of the elicitation transcripts across both scenarios examining 40% of the data corpus. We followed a consensus process among the multiple coders. All reviewers independently coded all of the transcripts and met to compare their coding to arrive at consensus judgments through open dialogue [37,57,58]. Consensus coding captures data complexity, avoids errors, reduces groupthink, and circumvents some researcher biases. To conduct our coding, we utilized Dedoose, a qualitative coding software system [145].
Through a collaborative process, the researchers developed a consensus set of axial codes such as “past and ongoing relationships,” “locations,” and “creating action plans and learning tools,” among others. We then applied these axial codes across the dataset. This coding process resulted in the main themes explored in the following section.
3.4. Positionality
In this work, the research team represents a variety of backgrounds including behavioral scientists and human-computer interaction researchers; all who had prior experience working with individuals with mental health concerns. The two HCI researchers were attuned to common understandings of technology and routines of technology use. The other two researchers had a psychology background, and, therefore, were able to explain issues that participants raised that had a clinical nature. At least one author has a mental health condition. These varied perspectives allowed us to be more sensitive to the nuances in our participants’ data.
4. FINDINGS
In this section, we present the results of our analysis of participants’ descriptions of their self-management of symptoms of depression. First, we describe participant socially-focused self-management activities, with whom they interact, and related expectations. We then describe characteristics influencing these activities, including locations and selected technology channels.
4.1. Role of Sociality in Participant Self-management Activities & Expectations
Participants described a variety of self-management activities to help mitigate negative emotions or deal with challenging situations. We detail three common activities below: expressing moods, creating solutions, and de-escalating moods. While we separate these activities in our findings for analytical purposes, in practice, participants often interwove a variety of these activities in their daily lives. They also had several expectations of their self-management activities. These included changing feeling state, achieving a specific outcome, and learning about or enacting control over symptoms. Below, we describe each of these major categories of activities, followed by a brief discussion of participant self-management expectations.
4.1.1. Expressing Moods.
Participants expressed their moods through sharing stories and conversations about their issues and feelings. Being able to put words to an internal mood and describe a challenging situation helped participants to feel better, especially when speaking or writing to a sympathetic listener. Although a few participants journaled their moods individually, the majority of participants expressed their moods to other people. By expressing moods to others, participants felt heard and validated in their emotional experiences, such as, “letting my frustrations out and venting…hopefully I will gain a little peace of mind. It is never healthy to keep it all in” (P07).
During their sharing process, participants expected to receive understanding and empathy from the person listening to them. Importantly, while expressing their moods, participants explicitly stated that they did not want to receive advice or solutions; they simply desired to “vent” and be heard. P14 highlights what she is looking for in this type of interaction, “have someone just listen and not interrupt or tell me what they think I should do.” Expressing feelings and moods to others helped to normalize participant experiences of dealing with symptoms of their condition and to “feel supported” (P19) in their condition management.
Participants expressed moods primarily to others with whom they had an ongoing relationship. These individuals possessed knowledge of the participant’s life and circumstances, particularly through knowledge developed over time. They included close family, friends, and those who shared similar experiences with depression. Therapists also built relationships over time with participants, but were viewed in different context by participants because of their professional knowledge and formal relationship with the participants.
P27 describes that shared history is an important reason why she is comfortable expressing her moods to her long-time friend: “[My best friend] and I have known each other for 20 years, so I can tell her something, and she has enough history to get it without me even saying it the right way.” Similarly, P09 described how his therapist used the knowledge developed over the course of their clinical relationship to know when to probe further to help him to express his feelings, “one time when I tried to just say everything’s fine, and then he could tell – he’s like, ‘I don’t think everything is fine.’” Relationships that build over time, such as described by P27 and P09 enable a trusting and predictable connection. Predictability is important, providing participants the ability to better expect the response that they will receive when connecting with supportive others for self-management. This also means that lack of history may be viewed as a barrier. For example, P16 contrasted the idea of connecting with supportive individuals she knew versus someone new such as the on-demand expert in scenario 2: “well, I trust these people. I don’t trust this [expert]. And I have a history with them, so I know they will respond in a way that will help.” P16 exemplifies the frequent wariness of participants when considering connecting with a new person for support.
Participants were comfortable expressing their moods to individuals who had a shared experience of depression and believed they would receive appropriate support from them. P07 described her perceived benefits of connecting based on shared experience of depression: “Just knowing somebody that has been there done that, that may be able to offer me solutions, maybe not, but also will just be like, ‘Oh, girl, I’ve been there.’” P07 found the empathetic understanding from someone who has also experienced depression to be particularly meaningful. An additional benefit of receiving support from others with depression was knowing that they are not alone through access to a supportive community. This aligns with findings of previous research about online peer support for depression [103].
4.1.2. Creating Solutions.
Some participants wanted to connect with others to help them identify a solution to issues underlying their negative mood(s). Through conversation, participants went into details about their mood with others, and asked them for help coming up with solutions. These solutions took several forms ranging from advice, personalized tools and strategies, to detailed next step plans. For example, if she is struggling to self-manage, P13 would connect with others to develop “a plan of [a] series of things to do that’ll get you back on track.” Solutions meant different things to different participants. Some participants sought to understand what caused or might have triggered their current mood. Other people knew what caused their mood and wanted to know how to address the issue, for example, how to resolve a fight with a friend which was causing their bad mood.
Across these different solution-seeking approaches, people who knew participants well were seen to offer better solutions than others because of their knowledge of the participant. However, weaker connections including work colleagues were also helpful to a few participants. For example, over lunch breaks, P08 frequently would “throw” problems to his work colleagues, get feedback from them regarding what he should do next, and then recompose himself: “If it’s a lunch hour, I’ve managed to get it down to a mad science.”
Although participants turned to their non-professional network for general help, they sought professionals with mental health training for best-practice solutions to challenging issues. For example, P23 wanted to receive a prioritized list of next step tasks for her mental health management through connecting with a therapist. While most mental health professionals were described as therapists, others had a variety of backgrounds (e.g., wellness/life coach). The perceived benefits of connecting with a mental health professional for support included knowledge of best practices and the ability to provide unique support for creating solutions e.g., “offer tools or insights that I may not have on my own” (P02). Participants expected professionals to offer solutions and plans beyond the validating and comforting activities largely conducted with family members and friends. They often expected professionals to possess better knowledge and advice about depression management than other people in their social circle:
“if I, right now, am feeling anxious or depressed, I can reach out to my wife, my brother, my friends, etc., and just tell them – and they can empathize with me, but they can’t say ‘try this.’ And if they do, I’m like, ‘You don’t know what you’re talking about.’ They’re not experts. And so I think [connecting with an expert] would make my life easier by providing at-the-ready solutions to some of the biggest problems I deal with day in and day out.”
(P03)
Some participants discussed how their therapist could be warm, but at the same time be an effective change agent, “[my therapist] calls me out on my shit, but is also a really kind person and so that helps me manage my stuff” (P19). Therapists managed their professional relationships with participants to support and encourage participants’ ongoing self-management. However, participants voiced frustrations about timelines for connecting with therapists. P24 discussed how the timeline of therapy did not match up with when he experienced challenges, “you have to take all your problems that you have during the week and then address them in 50 minutes.” Instead, he said, “you want real time advice.” Therapists were not always available when desired or needed by participants, and having to wait and ruminate on issues over the course of a week or more meant that participants were not able to act on issues as quickly as they would desire.
4.1.3. De-escalating moods: Distracting & Self-soothing.
Participants often reduced acute feelings of distress through distracting and self-soothing activities. These activities helped to create distance from the troubling problem or emotion. Participants used distracting activities such as going out to dinner with friends or watching a comedy show on Netflix to help them “get out” of their heads and take a break from their negative thoughts and mood. For example, “Focus on one thing, instead of what’s going on in my head” (P01).
Other research has shown that distractions can be perceived as meaningful or a waste of time depending on the user’s intentions [85]. This research describes how people might perceive using social media to pass the time as “mindless” or without deeper meaning, but the activity may also hold benefit as a “micro-break” from larger tasks. Additionally, psychology literature shows there are instances when distraction can offer a positive respite, especially to de-escalate intense moods when they occur [36,70,71,109,121]. Some participants described that they distracted themselves when they could not deal with a mood in the moment, for example, if experiencing a negative mood at work, “Compartmentalize; assure self that the issues will be attended to later” (P08). In tandem or in complement to distraction, participants engaged in self-soothing activities such as meditation, going for a walk, practicing reiki (a Japanese energy healing practice), getting a massage, taking a nap, or listening to music. P26 described self-soothing activities including a calming inner voice narration, “I would first exercise/meditate, drink water, calm myself down by thinking through things slowly, smile at other people instead of frown, talk to myself ‘it’s not the end of the world.’” Some activities served dual distracting and self-soothing purposes, for example, sharing a meal with friends.
During mood de-escalation activities, participants’ social responses were varied. Some sought interactions with others, and others explicitly sought solitude. Participants described hanging out with friends or family, cuddling with a significant other, scheduling meals with friends, playing video games together, or otherwise interacting without discussing their mood or problems as a way of distracting themselves. Conversely, others spoke about the importance of being able to tackle their own problems in order to start to calm themselves without waiting for others to help. In both cases, participants wanted to distract themselves from their current mood.
4.1.4. Expectations of Self-management Activities.
Many participants conducted self-management activities to achieve a change in feeling state, such as reducing stress or anxiety or becoming relaxed. These expectations or hoped-for outcomes motivated participants to engage in activities to self-manage their depression symptoms. For example, one participant wanted to “feel more grounded and less frantic” (P19), and another wanted to “[gain] confidence to get through the day” (P30). Being able to move from a negative mood to a calm mood led to an improved state that allowed participants to carry out their other daily activities such as getting out of bed, grooming themselves, and going to work. Improving their own productivity was a major goal, such as, “finding some peace or energy to keep doing my things or activities” (P10). P03 described specific outcomes of his socially-oriented self-management – to first achieve self-care, and then work toward improving his psychological health:
“I’d be motivated to apply these self-care tips as they’re needed with the promise of accountability keeping me on top of things; I’d be able to get over the hump, so to speak, and get back on more level psychological ground”
(P03)
Finally, a few participants expressed a desire to manage their condition longer-term. While this was not the expectation for the majority of our participants, for individuals who already had many self-directed activities, for example deep breathing, and tracking daily positive behaviors, this was the next step. P25 felt that gaining input and solutions from others as “tools to deal” with her condition would help prepare her for future self-management. Others desired “control over emotions” (P06), “not using maladaptive coping mechanisms, e.g., self-harm” (P13), and “in the future, be able to control my depression more effectively” (P17). These participants were particularly interested in gaining a better knowledge of their condition and long-term self-management skills through conversations with therapists and other trained professionals.
When asked about the most important element supporting her self-management, P15 noted that it was the people she connects with, saying, “I think people are powerful.” Through connecting with others, participants felt heard and understood, validated in their emotions, and assisted with reframing or deciding to let go of a situation. To achieve the expectations described in this section, individuals, as part of their self-management, reached out to others to express moods, create solutions, and enable distraction from feelings. Some participants described employing one or more of these activities, often mixing and matching depending on the situation.
In summary, these findings present a nuanced picture of the variety of participant expectations of self-management and their activities in pursuit of these expectations. Interestingly, the majority of participants, even when responding to a scenario prompt (Scenario 2) that included an on-demand expert, did not seek long-term management of their condition. Instead, participants focused much more on mood alleviation, mood expression, and shorter-term (more immediate) problem-solving.
In the following section, we describe characteristics of locations and its impact on sociality.
4.2. Locations of Sociality
Participants had specific ideas about where and how supportive interactions should occur. As has been found in other HCI research (e.g., [55,111,117,138]), location is a key component in participants’ descriptions of social activities. Participants chose locations in which they could regroup, reflect, and engage in their preferred sociality. They described a variety of locations including home, work, and public areas where they conducted self-management activities. The ability to control their location improved their interactions and helped them reach their expected outcomes, as stated by P25:
“if I was uncomfortable in a setting, I would want to change that as much as possible with like what I’m wearing, where I’m sitting, so that I could just be receptive to whatever they and I were gonna talk about.”
(P25)
Four key themes were important to participants in choosing their location: privacy, comfort, a new perspective, and social interaction.
4.2.1. Ensuring Privacy.
Participants often cited privacy as a reason for choosing a particular location for self-management. For example, “I would wanna be somewhere, whether that’s home, or at work, or even driving home in my car, or whatever, I would want it to be private” (P21). This desire for privacy is unsurprising given the sensitive nature of discussions about one’s moods and circumstances and was important in helping participants reach their expected outcomes. Participants largely associated their homes and vehicles with privacy.
However, for participants living with roommates, partners, or spouses, the ability of nearby individuals to potentially overhear conversations had to be taken into consideration. This was a particular consideration when preparing to talk with others for self-management support because of the likelihood of sharing private and sensitive information. Specifically, being in an intimate relationship, a friendship, or living with another did not mean that participants were automatically comfortable with them knowing about the participant’s conversations about their mental health. As such, participants sought privacy to safeguard against unwanted disclosure of their mental health.
4.2.2. Enabling Comfort.
Participants often cited comfort as a reason for choosing a particular location. Being comfortable and feeling relaxed and safe allowed individuals to lower their inhibitions and interact more freely with others. Comfort was closely related to helping individuals achieve self-soothing activities, but also was often a pre-requisite for undertaking the work of understanding moods and coming up with solutions. Home was most often the place participants wanted to be as they carried out self-management activities. When at home, they could more easily connect with a significant other, or call parents or friends. For example, P18 said, “My comfort zone, other than my car, is my home.” For some participants, safety was closely linked to comfort, “An escape, I guess, from everything from the outside world, going somewhere else were you feel comfortable and safe” (P01). Comfort could encompass feelings of safety, familiar surroundings, and the ability to feel relaxed and secure.
4.2.3. Shifting Perspective.
Because certain environments or social situations were described as triggering or exacerbating of their negative moods, several participants described a need to get away from their current location and change context, particularly to de-escalate their moods. Going outside, sitting in one’s car, or taking a walk were common activities, and connecting with supportive others helped to enhance these context shifts. For example, participants described talking with others during perspective-shifting walks to express and de-escalate their mood through conversation and change in location. Participants described wanting to go “away from work, house, stuff. And just be somewhere else” (P08) or to just “get the hell out of the situation” (P05) that was triggering or worsening their mood. However, shifting perspective did not always have to be accomplished by physically moving. A perspective shift could also involve simply changing activities, for example, from doing homework to watching a show on Netflix and brushing one’s hair. Therefore “location” for depression self-management can mean an individual staying in one location but shifting activities, or an individual moving between multiple locations to enhance and enable their self-management activities.
4.2.4. Managing Social Interactions.
Participants chose their location based on their desired social interactions with others. In some cases, they wanted to be around other people in busy, public places without directly engaging with them. We label this “diffuse sociality.” For example, P19 explains frequently working on homework at a coffee chain: “I put in my headphones and I like being surrounded by people, but feeling like not hearing any sounds.” P19 is still engaging in a social experience but not explicitly interacting with others. Importantly, she does this when she is experiencing a negative mood in order to accomplish her other daily required tasks. Being in public and busy places helped several participants to focus on their work while avoiding negative mood spirals and unwanted behaviors.
P13 described how the public nature of her favorite coffee chain helped her to avoid isolating herself and attendant unwanted self-harm behaviors, “I’m in public, so it’s a little easier to resist.” Diffuse sociality also occurred in other locations. P01 liked to sit next to his boyfriend while playing games but did not need to directly interact with him to feel the comfort of his presence. Being near other people but not necessarily needing to interact with them was important to some of our participants. Being near others allowed participants to accomplish their own tasks, but also enjoy the benefits of a social location. Consequently, while direct interaction was certainly a major component of sociality for our participants, so was diffuse sociality – focusing on their own activities while being around others.
In summary, these findings prompt reflection on how locations influence interactions for social support. The ability of people to participate in self-management and to interact in ways where they can feel safe and secure relates to how well their environment matches the intent of their interactions. In the following section, we describe ways participants adapted technology use to meet their needs.
4.3. Collaborative Technologies and Sociality
Technologies enabled participants to connect with their supportive network. Participants selected technologies according to their desired type of interaction, using different options depending on their location, their mood, and their expected outcomes. They communicated with others through a variety of technologies including texting, phone calls, voice calls, social media, and online games. Technology offered an opportunity for in-the-moment support. Addressing a bad mood earlier is often beneficial for mental health management [11].
No single mode of communication was preferred; participants were flexible and multimodal in their use, making choices about the technology based on the need for privacy, the content of the interaction, or the locations of those with whom they were communicating. For example, P02 described texting for support if she was having an issue with her boyfriend: “If I’m complaining about my boyfriend and he’s sitting right next to me, I’m not going to want to say it out loud.” Current moods and emotions guided other participants’ technology choices. For instance, if someone was anxious, “typing things out…lets them say what they want to say without using their voice” (P01). Similarly, not wanting to cry led P02 to switch communication modes to something less likely to evoke that response. Flexibility in their mode of communication was important for handling participants’ multiple different situations and communication desires.
At times, participants also switched communication medium based on the subject matter. For example, to communicate via “instant messaging with an option to escalate to video chatting” (P13) if a richer connection experience was desired. Others desired visual communication for better communication of emotion with their listener. P30 thought that FaceTime would be best for interaction because, “you can see and hear what people are feeling.” P10 concurred, “texting takes too much more time than actually talking and can be so much colder than a visual interaction.”
While technology was used to mediate direct interactions, participants also used technology to plan physically co-located interactions and to de-escalate their moods. Participants would often text their social support network in order to arrange face-to-face meetings or call a therapist to arrange an in-person appointment. For example, P06 explained how she would contact her friend via “messenger, and we are potentially [going] to make plans to go out to dinner or have drinks.” P22 described more broadly searching for social connection by looking for upcoming Facebook events, Meetups, and using OKCupid to set up interactions with others. Participants also used technology for mood de-escalation. They used headphones for music, computers and TVs for streaming services, and gaming consoles for games with others online. P01 described often having “headphones on because I like the music of the games…It gives me something to focus on, rather than focusing on how I’m feeling.” Therefore, technologies were used both to support social and individual-focused self-management.
Although technology was crucial to successfully being social in the ways that our participants desired, a few participants mistrusted technology-mediated communication. They viewed technology as potentially leading to less honest connections with others, “It’s kind of easier to lie behind technology…you can convince someone you’re fine via text so easily” (P13). Others found technology-mediated communication to lack the warm personal qualities of in-person interactions, “I rely more on the person experience, rather than the virtual experience” (P10). Finally, some participants were skeptical that technology-mediated support could work in an immediate way. P27 described how on-demand therapy would need a prohibitive amount of background information to work, in her perspective:
“you can’t give your life story in an instant. And unless they have enough of your back story, they can’t give you a good answer to go forward. So, the technology – the idea is good, but the input from the individual would need to be massive”
Technology clearly played an essential role in mediating sociality for the majority of our participants, however technology also created challenges for some participants.
In summary, participants connected to their support network through a diversity of channels, including technology-mediated channels and physical face-to-face channels. Additionally, these channels were often used in tandem or in sequence with one another. This variety allowed participants to choose which social activities to engage with in any given situation.
5. DISCUSSION
In our findings above, we unpacked how sociality is interwoven into individual’s self-management practices. Previous literature has found that social interactions can be challenging for individuals managing depression [93]. While this is true, and our study participants did talk about their challenges, we also found that they turned to others for several reasons and in a variety of ways as a key aspect of their self-management. In the following section, we discuss ways to conceptualize and situate core aspects of sociality for individuals managing depression. First, we present sociality as a lens through which we can better understand self-management of mental health needs by discussing factors that influenced sociality in our study. Second, we broaden our understanding of sociality in CSCW through discussing diffuse sociality.
5.1. Factors Influencing Sociality for Self-Management of Depression
The nuances of participants’ social activities highlight the tensions between, as well as the importance of, the interplay between factors influencing sociality for depression self-management. We identify four influencing factors which include: (1) relationship roles and expectations, (2) mood state and technology channels, (3) location and privacy, and (4) culture and sociality.
5.1.1. Relationship Roles and Expectations.
Participants selected who they wanted to connect with based on both the expertise of and their ongoing relationship with individuals in their social network. Reaching out to particular individuals for specific supportive reasons resonates with findings from Park’s college student participants [104] and Murnane et al.’s participants managing bipolar disorder [98]. To aid self-management, participants in our study sought social activities with close supportive relationships including friends, significant others, family members, and others also managing depression. For example, participants socialized with people who shared experience managing depression to receive empathetic listening, similar to findings of O’Leary et al. [102]. Participants also sought interactions with individuals with professional training, (e.g., therapists) to gain solution-focused support based on clinical best-practices. Many participants viewed interacting with professionals as particularly beneficial because it did not require reciprocal sharing. For individuals managing depression who may have limited energy and motivation, the tiring nature of managing relationship challenges including burden and reciprocity can influence to whom they reach out [18]. Furthermore, for some participants, hearing problems shared by others made them feel worse, similar to findings of depression symptom contagion [69]. Consequently, while these relationships are generally beneficial to participants, there are issues that affect who these participants want to turn to for support.
In particular, trust played a critical role in these supportive relationships. While participants viewed topic-based expertise as important (e.g., perceptions of expertise motivated people to connect with trained professionals), we found that other factors also encouraged trust within supportive relationships. Participants’ support networks included people who were close to the participant and who had built a deep understanding with them over the course of their relationship. Thus, while some supportive individuals had mental health expertise (e.g., a sister who is a trained social worker), importantly, these individuals also had participant-specific expertise. They knew the participant’s preferences, past activities, and common ways of thinking. Participants trusted the ability of these individuals to provide useful support based on their background knowledge of the participant and their ability to deliver support in comfortable and pleasant ways.
We can use our findings in the context of human-human relationships to consider what they might imply for human-technology “relationships” for self-management support. Previous CSCW research has identified digital elements that can support trust, including quantification of expertise in online games [77] and activity traces and profiles on GitHub [89]. However, better understanding trust in the mental health support context may be particularly essential given the current steep attrition rates associated with mental health technologies [91]. When considering potential future solutions, some of our participants were excited about tools to assist their self-management. However, others were wary of or held negative views regarding the efficacy and impact on mood of mental health support technologies [108]. This was largely because participants were skeptical about the ability of any new person or technology tool to possess the appropriate background knowledge of their life and circumstances, viewed as necessary for effective support.
5.1.2. Mood Influencing Communication Channel Selection.
Participants’ emotional states in-the-moment often influenced their interaction and technology choices. To self-manage, participants used multiple forms of technological mediation including social media, texting, video conferencing, and video games in distinct ways and in specific combinations. Technology-mediated channels to connect with others were often selected based on a collection of considerations such as location (e.g., work or home), emotion state (e.g., sad, anxious), and the availability and location of the person with whom they were connecting. Technology allowed participants the flexibility to receive in-the-moment support through different channels. Indeed, in-the-moment context-based channel-switching enabled by technology-mediated communication has also been found useful beyond the mental health context to enable communication with deaf and hard-of-hearing individuals [134]. These social interactions can take place both in physical and digital spaces, which is in line with other recent work in the autism context on understanding virtual and physical interactions in tandem for sociality [111].
Our findings described how participants used technology to enable and augment their social interactions. While the literature reports a lack of user engagement with current largely individual-focused tools to support user mental health [94,96,127], we found that participants creatively appropriated mainstream technologies to support their desired sociality. Technology ecosystems [38,114,136,137] (e.g., SMS, Facebook messenger, and video chat) provided essential access to supportive relationships and social network resources. These tools were unlikely to have been created with supporting user mental health in mind and indeed some have been correlated with negative trends in mental health [65]. However, as shown by research investigating the well-being of social technology users, meaningful connections within these social technologies including directly writing to others [20,22] and showing effort in communication [76] beyond simply “liking” content can positively influence mental health. Thinking toward a future of technologies for assisting depression self-management, we need to consider incorporation into existing management routines and communication structures where people are already sharing support.
As highlighted in other areas such as assistive technology [112,123], we can learn much from user appropriation. Understanding how users are appropriating technology can provide insight regarding what users want or need. For example, many participants described selecting among different channels of communication including texting, voice, or video calls, depending on their mood. A few participants noted that texting was particularly attractive when they were having difficulty regulating their emotions because even a voice call seemed too difficult to manage. Our findings align with other CSCW literature on selecting between multiple channels of communication [3,134]. However, channel selection was not only based on static individual preference, but also on the dynamic needs of our participants in the moment. Location and channel selection are also importantly intertwined. For our participants, even though technology was useful to quickly connect people in rich forms (e.g., video chat), these uses still suffered from privacy challenges. For instance, while video chat was prioritized by some participants, privacy of conversations at work and on the go (e.g., between classes), and in shared households was not a given. We discuss these challenges further in 5.1.3. Technology solutions that enable in-the-moment adaptation, for example, by allowing switching between text, voice, and video-based channels is one way to enable users to adapt their sociality to their current environment.
5.1.3. Locations and Privacy.
Participants made choices regarding socially-oriented self-management activities based on their location. As shown in previous HCI studies, location impacts interactions with technologies, as well as interactions with others (e.g., [55,111,117,138]). However, much of the prior CSCW literature has not focused on location in the context of mental health. For example, work analyzing social media communication and expression (e.g., [7,33,34,59,88]) may be “severing [posts] from other aspects of life and experience” [47]. In contrast, our findings deepen our understanding of participant experiences of self-management across a variety of locations in physical and technology-mediated environments.
For individuals seeking support, locations can take on new dimensions because of the social stigma associated with mental health challenges [30] and the difficultly in managing moods and emotions. For example, as described in our findings, location can affect an individual’s sense of security. A person may feel more or less secure disclosing to others about their challenges depending on their location (e.g., therapist’s office; workplace; public setting). Similar concerns have been raised in online environments. Previous research by Andalibi et al. [4] regarding disclosure of mental health and other sensitive topics on social media has also shown that privacy can affect intent to disclose [5–7] and other’s response(s) to disclosure.
Participants described the challenges of being in certain locations such as their workplaces when experiencing negative moods. An important way they self-managed in these locations was to seek comfortable and safe environments to communicate within places where they could avoid being overheard. For example, while at work, some participants headed to their car, went on a short walk, or connected with friends over lunch to talk through issues. Others used technology such as mobile phone games and music to reduce the intensity of their mood until they could manage it later. While the use of distraction as a self-management strategy to remediate low mood is often reported by individuals with depression [36,70,71,109,121] understanding more deeply what prompts people to ‘transport’ themselves physically and mentally in order to manage their mood is less understood. Comfort, privacy, and moving one’s body and/or mind to a new location (through physical movement or technology use) are key elements that enable the difficult work of self-management. Particularly with an eye to supporting self-management, we should seek to better understand the barriers to moving location when desired, such as workplace demands or fatigue and loss of energy common to depression. Understanding these location preferences is important for developing solutions that are sensitive to a user’s current context.
One way that researchers and designers have begun to use location information to support mental health management is through the use of smartphone sensors and passive tracking (e.g., [84,135,142]). A potential design direction from our research relates to passive sensing solutions. For example, a hypothetical application could combine sensed location data with user input, allowing sensors to detect frequent locations [116], and request users to annotate them (e.g., work; coffee shop; home), noting channels that are socially acceptable and most useful for the user to connect with others for support. For example, using texting but not video chat during work hours. However, such solutions have limitations and require more nuanced thinking before implementation. First, as shown in our findings, locations are not necessarily used for the same social activities all the time. For example, a home might be used sometimes to have alone time away from people and at other times to host a gathering of friends. Given the diverse interactions of daily life, mood management, location, and other people, it is difficult to predict a person’s social needs in any given moment solely based on sensing data.
Furthermore, location-based technologies necessitate privacy considerations. For many reasons a user may not want to disclose their location. Indeed, vulnerabilities from this type of data are cited as a concern regarding many digital mental health technologies [118]. In their study with individuals managing depression and anxiety, Nicholas et al. [100] noted distinct differences in individuals’ comfort sharing “health data” including sleep, mood, and physical activity versus “personal data” including communication logs, location, and social activity. Further, safety is an important concern for many individuals and was brought up by our participants. We need to consider who has access to location and other personal and sensitive data. The case of domestic violence exemplifies a need for great care to be taken in the design of these technologies [49]. The concept of “safety” is deeply intertwined with how each person chooses to be social, where they are being social, and who they are being social with. Future work needs to address these more nuanced concerns when designing digital mental health technologies, particularly if they involve tracking sensitive personal data such as location.
5.1.4. Culture and Society.
“Depression” has a specific meaning and definition within society. The important social needs of our participants to maintain productive self-management influenced the many ways they actively sought out human connection. In many cases, participant’s networks were able to support their needs. However, participants also spoke about some social challenges they experienced including both the tiring nature of self-management work and relationship aspects of burden [74] and reciprocity [62]. When designing future tools or new supportive social connections for this population, it is important to keep in mind that the concept of “mental health” is socially constructed and, as such, the definitions and meanings of labels such as “depression” are fluid and situational [40,110]. In creating new systems of support, these complex interplays between how labels and/or identities are interpreted, reified, and redefined will influence design and deployment of these new systems.
Furthermore, the term depression also held certain power within the culture of these participants. For example, a study examining online support groups for depression in China [141], highlights that cultural contexts and societal understandings of depression strongly affect an individual’s goals and behaviors of social connection. The importance of saving “face” both for oneself and one’s family prevented many people from being comfortable disclosing and discussing their mental health needs. Cultural understanding mediates and shapes the conversations our participants have when they connect with others and where self-management activities take place. We need to be sensitive to this issue because tools and technologies for mental health become a part of the larger societal “conversation” about depression. As we integrate tools into people’s lives, this conversation about their mental health is influenced by and in concert with the different interactions they have with medical professionals, friends, family, and cultural artifacts. Therefore, understanding the social activities and social goals of individuals managing mental health needs is essential to properly support the nuances of human connection for these individuals and their support networks.
In their recent book, Positive Computing [25], Calvo and Peters write that “there is obviously much we need to learn about which technologies can support wellbeing, when, in what circumstances, in what combinations, and why.” Our findings regarding the nuances of social interactions, technology use, and relationships in the context of individuals self-managing depression may have broader implications toward these questions. CSCW has a history of supporting the needs of individuals who are vulnerable and may have challenges with social interactions (e.g., [75,114,119,130]). Attention to these groups, such as our participants managing depression, can provide important considerations and design directions which may be useful for designing for and supporting mental health and wellbeing beyond this group of people.
5.2. Diffuse Sociality
Participants used both direct and indirect connections to others as part of their self-management activities. When faced with a bad day or a negative mood, many participants reached out and directly connected with others through texting, video chat, or face-to-face conversations. This is similar to social media use research that found connecting online to close others improved symptoms of depression [20,22]. Direct human connection enabled participants to feel heard, understood, and validated in their emotions and the experience of their condition, helping to lighten their load of managing depression. Direct connection with others largely centered on conversation (empathetic listening, some problem-solving), resonating with the social support literature [18,104], but also encompassed affectionate physical contact. Our findings regarding the direct connection activities of our participants resonates with previous conceptualizations of sociality in CSCW as highlighted in our related work section.
Through our study we extend this literature to highlight the importance of indirect social connection. Indirect social connection – diffuse sociality – was important in participants’ self-management practices. As described in the findings, several participants specifically planned time to be in the proximity of others, either in public locations such as working in a busy coffee shop, or in private locations such as playing video games while sitting next to a significant other. Participants intentionally chose to not directly connect, but still gained some of the social benefits of these indirect connections by being proximate to others.
Being around others helped participants to focus and avoid potential negative behaviors and moods that would appear if they were alone. Therefore, through indirect social connection, participants could still be social and gain benefits, such as being distracted from their moods, without requiring the same level of effort as potentially emotionally taxing direct interactions. The effort required for direct social interactions and the expectations surrounding these interactions may be reasons why some participants occasionally sought these indirect social connections. Indeed, direct social interaction with others can be tiring and time-consuming [146], consequently, indirect social interaction was one way participants met some of their self-management needs without the potential costs. However, no participant exclusively engaged in this type of sociality, because activities such as expressing moods and creating solutions required direct interaction with others.
Diffuse sociality provides a lens to consider when designing to support the breadth of an individual’s social interactions. For example, although individuals dealing with depression may not want to directly interact with others, this does not mean that they want to fully exclude themselves from social interactions. Rather, what diffuse sociality points us toward is the variety of social interactions that these individuals look for and participate in as part of their self-management. Taken together, direct and indirect human connection begins to show the broad range of sociality. Understanding the nuances of this spread of social activities allows us to better understand the context(s) in which participants engage in self-management practices. For instance, in online space, many individuals participate in “lurking” activities – logging into a virtual world, game, or online community without directly interacting with others [50,97,106,107,126]. It is possible that lurking may provide some level of depression self-management benefit that is worth investigating further.
The concept of diffuse sociality can help us explore and understand similar indirect social interactions that occur in-person and in online environments. It may also be a useful area to explore in other mental health and wellness-focused research. To support people with depression across the variety of physical and digital contexts in which they participate and interact with others socially, it will be essential to understand and support the full range of sociality as part of their self-management activities.
In summary, we have discussed the complexity of sociality that includes direct and indirect connections with others. Our work brings us closer to Miller’s assertion of sociality from his anthropological perspective as the state of being social [114], including an individual’s social interactions, communications, relationships, and nonverbal interactions with others [61,93]. Therefore, to extend the definition of sociality for CSCW, we propose that sociality is comprised of direct and indirect social interactions and is mediated by verbal and nonverbal cultural cues and technologies, across a variety of physical and virtual contexts.
6. LIMITATIONS
While we did conduct interviews in the home for some participants, we realize that our recruiting strategy may have excluded those with symptoms of depression severe enough to prevent them from participating in the study. In our future work, we plan to extend this research to more explicitly involve individuals with severe depression to examine whether the issues we identified in this study extend to that population. In addition, this study only covers the experiences of people within the United States of America. It is clear that experiences of depression and self-management may differ significantly in other cultures (e.g., [141]) and further studies should investigate self-management activities in other national and cultural contexts.
7. CONCLUSION
To study the self-management activities of individuals managing depression, we conducted visual elicitations and semi-structured interviews with 30 participants managing depression in a large city in the U.S. Midwest. We found that sociality was a key aspect of self-management for our participants, who connected with others through direct and indirect methods and used technologies and locations in diverse ways. We extend previous literature that has largely focused on the online activities of individuals managing depression [34,46,103] by showing how individuals conceptualize connecting with others both digitally and physically as part of their self-management activities. We expand our understanding of sociality in CSCW through the addition of diffuse sociality, being in proximate location to others but not interacting directly. We can better support individuals’ self-management of depression by considering factors influencing their sociality including relationship roles and expectations, mood state and communication channels, location and privacy, and culture and society. Future design of mental health support tools for this population should consider approaches and solutions that facilitate social connection to meet a range of user expectations, across a variety of communication channels and digital and physical environments.
CCS Concepts: • Human-centered computing → Human computer interaction (HCI); HCI theory, concepts and models
ACKNOWLEDGMENTS
We thank our participants for sharing their stories. We also thank Michael T. Hendon for his assistance. Ashley Knapp’s and Kate Ringland’s participation in this work is supported by the National Institute of Mental Health (T32MH115882). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Footnotes
Some authors [46] differentiate between the terms mental illness and mental health. In our paper, we refer to mental health as an umbrella term encompassing the work individuals do to manage their mental health needs and reach their health goals.
Contributor Information
ELEANOR R. BURGESS, Northwestern University, USA.
KATHRYN E. RINGLAND, Northwestern University, USA.
JENNIFER NICHOLAS, Northwestern University, USA.
ASHLEY A. KNAPP, Northwestern University, USA
JORDAN ESCHLER, Northwestern University, USA.
DAVID C. MOHR, Northwestern University, USA
MADHU C. REDDY, Northwestern University, USA
REFERENCES
- [1].Alvarez-Jimenez M, Bendall S, Lederman R, Wadley G, Chinnery G, Vargas S, Larkin M, Killackey E, McGorry PD, and Gleeson JF. 2013. On the HORYZON: Moderated online social therapy for long-term recovery in first episode psychosis. Schizophrenia Research 143, 1: 143–149. 10.1016/j.schres.2012.10.009 [DOI] [PubMed] [Google Scholar]
- [2].Ammari Tawfiq and Schoenebeck Sarita. 2015. Understanding and Supporting Fathers and Fatherhood on Social Media Sites. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems (CHI ‘15), 1905–1914. 10.1145/2702123.2702205 [DOI] [Google Scholar]
- [3].Andalibi Nazanin. 2019. What Happens After Disclosing Stigmatized Experiences on Identified Social Media: Individual, Dyadic, and Social/Network Outcomes. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems (CHI ‘19), 137:1–137:15. 10.1145/3290605.3300367 [DOI] [Google Scholar]
- [4].Andalibi Nazanin and Forte Andrea. 2018. Responding to Sensitive Disclosures on Social Media: A Decision-Making Framework. ACM Transactions on Computer-Human Interaction (TOCHI) 25, 6: 31. 10.1145/3241044 [DOI] [Google Scholar]
- [5].Andalibi Nazanin, Haimson Oliver L., De Choudhury Munmun, and Forte Andrea. 2018. Social Support, Reciprocity, and Anonymity in Responses to Sexual Abuse Disclosures on Social Media. ACM Trans. Comput.-Hum. Interact 25, 5: 28:1–28:35. 10.1145/3234942 [DOI] [Google Scholar]
- [6].Andalibi Nazanin, Morris Margaret E., and Forte Andrea. 2018. Testing Waters, Sending Clues: Indirect Disclosures of Socially Stigmatized Experiences on Social Media. Proc. ACM Hum.-Comput. Interact 2, CSCW: 19:1–19:23. 10.1145/3274288 [DOI] [Google Scholar]
- [7].Andalibi Nazanin, Ozturk Pinar, and Forte Andrea. 2017. Sensitive Self-disclosures, Responses, and Social Support on Instagram: The Case of #Depression. In Proceedings of the 2017 ACM Conference on Computer Supported Cooperative Work and Social Computing (CSCW ‘17), 1485–1500. 10.1145/2998181.2998243 [DOI] [Google Scholar]
- [8].Bardram Jakob E., Frost Mads, Szántó Károly, Faurholt-Jepsen Maria, Vinberg Maj, and Kessing Lars Vedel. 2013. Designing Mobile Health Technology for Bipolar Disorder: A Field Trial of the Monarca System. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ‘13), 2627–2636. 10.1145/2470654.2481364 [DOI] [Google Scholar]
- [9].Barrera Manuel and Ainlay Sheila L. 1983. The structure of social support: A Conceptual and empirical analysis. Journal of Community Psychology 11: 11. [DOI] [PubMed] [Google Scholar]
- [10].Baumer Eric P.S., Katz Sherri Jean, Freeman Jill E., Adams Phil, Gonzales Amy L., Pollak John, Retelny Daniela, Niederdeppe Jeff, Olson Christine M., and Gay Geri K.. 2012. Prescriptive Persuasion and Open-ended Social Awareness: Expanding the Design Space of Mobile Health. In Proceedings of the ACM 2012 Conference on Computer Supported Cooperative Work (CSCW ‘12), 475–484. 10.1145/2145204.2145279 [DOI] [Google Scholar]
- [11].Beck Aaron T.. 1979. Cognitive Therapy of Depression. Guilford Press. [Google Scholar]
- [12].Berry Andrew B.L., Lim Catherine, Hirsch Tad, Hartzler Andrea L., Wagner Edward H., Ludman Evette, and Ralston James D.. 2017. Getting Traction When Overwhelmed: Implications for Supporting Patient-Provider Communication. In Companion of the 2017 ACM Conference on Computer Supported Cooperative Work and Social Computing (CSCW ‘17 Companion), 143–146. 10.1145/3022198.3026328 [DOI] [Google Scholar]
- [13].Berry Andrew BL, Lim Catherine Y., Hartzler Andrea L., Hirsch Tad, Ludman Evette, Wagner Edward H., and Ralston James D.. 2017. “It’s Good to Know You’Re Not a Stranger Every Time”: Communication About Values Between Patients with Multiple Chronic Conditions and Healthcare Providers. Proc. ACM Hum.-Comput. Interact 1, CSCW: 23:1–23:20. 10.1145/3134658 [DOI] [Google Scholar]
- [14].Biegel David E., Sales Esther, and Schulz Richard. 1991. Family caregiving in chronic illness: Alzheimer’s disease, cancer, heart disease, mental illness, and stroke. Sage Publications, Inc, Thousand Oaks, CA, US. [Google Scholar]
- [15].Binda Jomara, Georgieva Elitza, Yang Yujing, Gui Fanlu, Beck Jordan, and Carroll John M.. 2018. PhamilyHealth: A Photo Sharing System for Intergenerational Family Collaboration on Health. In Companion of the 2018 ACM Conference on Computer Supported Cooperative Work and Social Computing (CSCW ‘18), 337–340. 10.1145/3272973.3274091 [DOI] [Google Scholar]
- [16].Braithwaite Dawn O., Waldron Vincent R., and Finn Jerry. 1999. Communication of Social Support in Computer-Mediated Groups for People With Disabilities. Health Communication 11, 2: 123–151. 10.1207/s15327027hc1102_2 [DOI] [PubMed] [Google Scholar]
- [17].Braun Virginia and Clarke Victoria. 2013. Successful Qualitative Research: A Practical Guide for Beginners. SAGE. [Google Scholar]
- [18].Brown GW, Andrews B, Harris T, Adler Z, and Bridge L. 1986. Social support, self-esteem and depression. Psychological Medicine 16, 4: 813–831. 10.1017/S0033291700011831 [DOI] [PubMed] [Google Scholar]
- [19].Brubaker Jed R., Hayes Gillian R., and Dourish Paul. 2013. Beyond the Grave: Facebook as a Site for the Expansion of Death and Mourning. The Information Society 29, 3: 152–163. 10.1080/01972243.2013.777300 [DOI] [Google Scholar]
- [20].Burke Moira and Kraut Robert E.. 2016. The Relationship Between Facebook Use and Well-Being Depends on Communication Type and Tie Strength. Journal of Computer-Mediated Communication 21, 4: 265–281. 10.1111/jcc4.12162 [DOI] [Google Scholar]
- [21].Burke Moira, Kraut Robert, and Williams Diane. 2010. Social Use of Computer-mediated Communication by Adults on the Autism Spectrum. In Proceedings of the 2010 ACM Conference on Computer Supported Cooperative Work (CSCW ‘10), 425–434. 10.1145/1718918.1718991 [DOI] [Google Scholar]
- [22].Kraut Robert Moira Burke. Internet Use and Psychological Well-Being: Effects of Activity and Audience. Retrieved February 13, 2019 from https://cacm.acm.org/magazines/2015/12/194633-internet-use-and-psychological-well-being/fulltext
- [23].Burns Michelle Nicole, Begale Mark, Duffecy Jennifer, Gergle Darren, Karr Chris J., Giangrande Emily, and Mohr David C.. 2011. Harnessing Context Sensing to Develop a Mobile Intervention for Depression. Journal of Medical Internet Research 13, 3: e55. 10.2196/jmir.1838 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Cai Hanshu, Wang Ziyang, Zhang Yanhao, Chen Yunfei, and Hu Bin. 2017. A Virtual-Reality Based Neurofeedback Game Framework for Depression Rehabilitation Using Pervasive Three-Electrode EEG Collector. In Proceedings of the 12th Chinese Conference on Computer Supported Cooperative Work and Social Computing (ChineseCSCW ‘17), 173–176. 10.1145/3127404.3127433 [DOI] [Google Scholar]
- [25].Calvo Rafael A. and Peters Dorian. 2014. Positive Computing: Technology for Well-Being and Human Potential. The MIT Press. [Google Scholar]
- [26].Chen Yunan, Ngo Victor, and Park Sun Young. 2013. Caring for caregivers: designing for integrality. 91–102. 10.1145/2441776.2441789 [DOI] [Google Scholar]
- [27].Clark Noreen M., Becker Marshall H., Janz Nancy K., Lorig Kate, Rakowski William, and Anderson Lynda. 1991. Self-Management of Chronic Disease by Older Adults: A Review and Questions for Research. Journal of Aging and Health 3, 1: 3–27. 10.1177/089826439100300101 [DOI] [Google Scholar]
- [28].Clark-IbáÑez Marisol. 2004. Framing the Social World With Photo-Elicitation Interviews. American Behavioral Scientist 47, 12: 1507–1527. 10.1177/0002764204266236 [DOI] [Google Scholar]
- [29].Cohen Sheldon and Wills Thomas A.. 1985. Stress, social support, and the buffering hypothesis. Psychological Bulletin 98, 2: 310–357. 10.1037/0033-2909.98.2.310 [DOI] [PubMed] [Google Scholar]
- [30].Corrigan Patrick W., Druss Benjamin G., and Perlick Deborah A.. 2014. The Impact of Mental Illness Stigma on Seeking and Participating in Mental Health Care The Impact of Mental Illness Stigma on Seeking and Participating in Mental Health Care. Psychological Science in the Public Interest 15, 2: 37–70. 10.1177/1529100614531398 [DOI] [PubMed] [Google Scholar]
- [31].Crilly Nathan, Blackwell Alan F., and Clarkson P. John. 2006. Graphic elicitation: using research diagrams as interview stimuli. Qualitative Research 6, 3: 341–366. 10.1177/1468794106065007 [DOI] [Google Scholar]
- [32].Czaja Ronald, Manfredi Clara, and Price Jammie. 2003. The Determinants and Consequences of Information Seeking Among Cancer Patients. Journal of Health Communication 8, 6: 529–562. 10.1080/716100418 [DOI] [PubMed] [Google Scholar]
- [33].De Choudhury Munmun, Counts Scott, Horvitz Eric J., and Hoff Aaron. 2014. Characterizing and Predicting Postpartum Depression from Shared Facebook Data. In Proceedings of the 17th ACM Conference on Computer Supported Cooperative Work & Social Computing (CSCW ‘14), 626–638. 10.1145/2531602.2531675 [DOI] [Google Scholar]
- [34].Munmun De Choudhury Michael Gamon, Counts Scott, and Horvitz Eric. 2013. Predicting Depression via Social Media. In Seventh International AAAI Conference on Weblogs and Social Media. Retrieved October 24, 2013 from http://www.aaai.org/ocs/index.php/ICWSM/ICWSM13/paper/view/6124 [Google Scholar]
- [35].Munmun De Choudhury Sanket S. Sharma, Logar Tomaz, Eekhout Wouter, and Nielsen René Clausen. 2017. Gender and Cross-Cultural Differences in Social Media Disclosures of Mental Illness. In Proceedings of the 2017 ACM Conference on Computer Supported Cooperative Work and Social Computing (CSCW ‘17), 353–369. 10.1145/2998181.2998220 [DOI] [Google Scholar]
- [36].Dekker Rebecca L., Peden Ann R., Lennie Terry A., Schooler Mary P., and Moser Debra K.. 2009. Living With Depressive Symptoms: Patients With Heart Failure. American journal of critical care : an official publication, American Association of Critical-Care Nurses 18, 4: 310–318. 10.4037/ajcc2009672 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].DeSantis L and Ugarriza DN. 2000. The concept of theme as used in qualitative nursing research. Western Journal of Nursing Research 22, 3: 351–372. 10.1177/019394590002200308 [DOI] [PubMed] [Google Scholar]
- [38].DeVito Michael A., Walker Ashley Marie, and Birnholtz Jeremy. 2018. “Too Gay for Facebook”: Presenting LGBTQ+ Identity Throughout the Personal Social Media Ecosystem. Proc. ACM Hum.-Comput. Interact 2, CSCW: 44:1–44:23. 10.1145/3274313 [DOI] [Google Scholar]
- [39].Dickerson Robert F., Gorlin Eugenia I., and Stankovic John A.. 2011. Empath: A Continuous Remote Emotional Health Monitoring System for Depressive Illness. In Proceedings of the 2Nd Conference on Wireless Health (WH ‘11), 5:1–5:10. 10.1145/2077546.2077552 [DOI] [Google Scholar]
- [40].Eisenberg L. 1988. The social construction of mental illness. Psychological Medicine 18, 01: 1. 10.1017/S0033291700001823 [DOI] [PubMed] [Google Scholar]
- [41].Burgess Eleanor R., Reddy Madhu C., Davenport Andrew, Laboi Paul, and Blandford Ann. 2019. “Tricky to get your head around”: Information Work of People Managing Chronic Kidney Disease. In 2019 CHI Conference on Human Factors in Computing Systems Proceedings (CHI 2019), 14. 10.1145/3290605.3300895 [DOI] [Google Scholar]
- [42].Eschler Jordan, Dehlawi Zakariya, and Pratt Wanda. 2015. Self-Characterized Illness Phase and Information Needs of Participants in an Online Cancer Forum. In Ninth International AAAI Conference on Web and Social Media. Retrieved June 14, 2018 from https://www.aaai.org/ocs/index.php/ICWSM/ICWSM15/paper/view/10546 [Google Scholar]
- [43].Eschler Jordan, Kendall Logan, O’Leary Kathleen, Vizer Lisa M., Lozano Paula, McClure Jennifer B., Pratt Wanda, and Ralston James D.. 2015. Shared Calendars for Home Health Management. In Proceedings of the 18th ACM Conference on Computer Supported Cooperative Work & Social Computing - CSCW ‘15, 1277–1288. 10.1145/2675133.2675168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Evans Marilyn, Donelle Lorie, and Hume-Loveland Laurie. 2012. Social support and online postpartum depression discussion groups: A content analysis. Patient Education and Counseling 87, 3: 405–410. 10.1016/j.pec.2011.09.011 [DOI] [PubMed] [Google Scholar]
- [45].Feuston Jessica L., Marshall-Fricker Charlotte G., and Piper Anne Marie. 2017. The Social Lives of Individuals with Traumatic Brain Injury. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems (CHI ‘17), 182–194. 10.1145/3025453.3025784 [DOI] [Google Scholar]
- [46].Feuston Jessica L. and Piper Anne Marie. 2018. Beyond the Coded Gaze: Analyzing Expression of Mental Health and Illness on Instagram. Proceedings of the ACM on Human-Computer Interaction 2, CSCW: 1–21. 10.1145/3274320 [DOI] [Google Scholar]
- [47].Feuston Jessica L. and Piper Anne Marie. 2019. Everyday Experiences: Small Stories and Mental Illness on Instagram. In CHI 2019. [Google Scholar]
- [48].Fitzpatrick Geraldine and Ellingsen Gunnar. 2013. A Review of 25 Years of CSCW Research in Healthcare: Contributions, Challenges and Future Agendas. Comput. Supported Coop. Work 22, 4–6: 609–665. 10.1007/s10606-012-9168-0 [DOI] [Google Scholar]
- [49].Freed Diana, Palmer Jackeline, Minchala Diana Elizabeth, Levy Karen, Ristenpart Thomas, and Dell Nicola. 2017. Digital Technologies and Intimate Partner Violence: A Qualitative Analysis with Multiple Stakeholders. Proceedings of the ACM on Human-Computer Interaction 1, CSCW: 46. 10.1145/3134681 [DOI] [Google Scholar]
- [50].Gong Wei, Lim Ee-Peng, and Zhu Feida. 2015. Characterizing Silent Users in Social Media Communities. International AAAI Conference on Web and Social Media. Retrieved June 21, 2019 from https://www.aaai.org/ocs/index.php/ICWSM/ICWSM15/paper/view/10462 [Google Scholar]
- [51].Gorm Nanna and Shklovski Irina. 2017. Participant Driven Photo Elicitation for Understanding Activity Tracking: Benefits and Limitations. In Proceedings of the 2017 ACM Conference on Computer Supported Cooperative Work and Social Computing (CSCW ‘17), 1350–1361. 10.1145/2998181.2998214 [DOI] [Google Scholar]
- [52].Grimes Andrea, Bednar Martin, Bolter Jay David, and Grinter Rebecca E.. 2008. EatWell: Sharing Nutrition-related Memories in a Low-income Community. In Proceedings of the 2008 ACM Conference on Computer Supported Cooperative Work (CSCW ‘08), 87–96. 10.1145/1460563.1460579 [DOI] [Google Scholar]
- [53].Haimson Oliver L., Brubaker Jed R., Dombrowski Lynn, and Hayes Gillian R.. 2015. Disclosure, Stress, and Support During Gender Transition on Facebook. In Proceedings of the 18th ACM Conference on Computer Supported Cooperative Work & Social Computing (CSCW ‘15), 1176–1190. 10.1145/2675133.2675152 [DOI] [Google Scholar]
- [54].Harrison C. Keith and Lawrence Suzanne Malia. 2003. African American Student Athletes’ Perceptions of Career Transition in Sport: a qualitative and visual elicitation. Race Ethnicity and Education 6, 4: 373–394. 10.1080/1361332032000146384 [DOI] [Google Scholar]
- [55].Harrison Steve and Dourish Paul. 1996. Re-place-ing space: the roles of place and space in collaborative systems. In Proceedings of the 1996 ACM conference on Computer supported cooperative work, 67–76. Retrieved April 27, 2015 from http://dl.acm.org/citation.cfm?id=240193 [Google Scholar]
- [56].Helgeson Vicki S., Cohen Sheldon, and Fritz Heidi L.. 1998. Social ties and cancer. Psycho-oncology: 99–109. [Google Scholar]
- [57].Hill Clara E., Thompson Barbara J., and Williams Elizabeth Nutt. 1997. A Guide to Conducting Consensual Qualitative Research. The Counseling Psychologist 25, 4: 517–572. 10.1177/0011000097254001 [DOI] [Google Scholar]
- [58].Hill Clara, Knox Sarah, Thompson Barbara, Williams Elizabeth, Hess Shirley, and Ladany Nicholas. 2005. Consensual Qualitative Research: An Update. Journal of Counseling Psychology. Retrieved from https://epublications.marquette.edu/edu_fac/18 [Google Scholar]
- [59].Homan Christopher M., Lu Naiji, Tu Xin, Lytle Megan C., and Silenzio Vincent M.B.. 2014. Social Structure and Depression in TrevorSpace. In Proceedings of the 17th ACM Conference on Computer Supported Cooperative Work & Social Computing (CSCW ‘14), 615–625. 10.1145/2531602.2531704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [60].Hong Hwajung, Kim Jennifer G., Abowd Gregory D., and Arriaga Rosa I.. 2012. SocialMirror: Motivating Young Adults with Autism to Practice Life Skills in a Social World. In Proceedings of the ACM 2012 Conference on Computer Supported Cooperative Work Companion (CSCW ‘12), 41–42. 10.1145/2141512.2141533 [DOI] [Google Scholar]
- [61].Horst Heather A. and Miller Daniel (eds.). 2012. Digital Anthropology. Berg Publishers, London ; New York. [Google Scholar]
- [62].Horwitz Allan V., Reinhard Susan C., and Howell-White Sandra. 1996. Caregiving as Reciprocal Exchange in Families with Seriously Mentally Ill Members. Journal of Health and Social Behavior 37, 2: 149–162. 10.2307/2137270 [DOI] [PubMed] [Google Scholar]
- [63].Huh Jina. 2015. Clinical Questions in Online Health Communities: The Case of “See Your Doctor” Threads. In Proceedings of the 18th ACM Conference on Computer Supported Cooperative Work & Social Computing (CSCW ‘15), 1488–1499. 10.1145/2675133.2675259 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [64].Human Jeffrey and Wasem Cathy. 1991. Rural mental health in America. American Psychologist 46, 3: 232–239. 10.1037/0003-066X.46.3.232 [DOI] [PubMed] [Google Scholar]
- [65].Hunt Melissa G., Marx Rachel, Lipson Courtney, and Young Jordyn. 2018. No More FOMO: Limiting Social Media Decreases Loneliness and Depression. Journal of Social and Clinical Psychology 37, 10: 751–768. 10.1521/jscp.2018.37.10.751 [DOI] [Google Scholar]
- [66].Jacobs Maia, Johnson Jeremy, and Mynatt Elizabeth D.. 2018. MyPath: Investigating Breast Cancer Patients’ Use of Personalized Health Information. Proc. ACM Hum.-Comput. Interact 2, CSCW: 78:1–78:21. 10.1145/3274347 [DOI] [Google Scholar]
- [67].Jaremka Lisa M., Andridge Rebecca R., Fagundes Christopher P., Alfano Catherine M., Povoski Stephen P., Lipari Adele M., Agnese Doreen M., Arnold Mark W., Farrar William B., Yee Lisa D., Carson William E. III, Bekaii-Saab Tanios, Martin Edward W. Jr., Schmidt Carl R., and Kiecolt-Glaser Janice K.. 2014. Pain, depression, and fatigue: Loneliness as a longitudinal risk factor. Health Psychology 33, 9: 948–957. 10.1037/a0034012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [68].Johansson Robert and Andersson Gerhard. 2012. Internet-based psychological treatments for depression. Expert Review of Neurotherapeutics 12, 7: 861–869; quiz 870. 10.1586/ern.12.63 [DOI] [PubMed] [Google Scholar]
- [69].Joiner Thomas E. and Katz Jennifer. 1999. Contagion of Depressive Symptoms and Mood: Meta-analytic Review and Explanations From Cognitive, Behavioral, and Interpersonal Viewpoints. Clinical Psychology: Science and Practice 6, 2: 149–164. 10.1093/clipsy.6.2.149 [DOI] [Google Scholar]
- [70].Joormann Jutta, Siemer Matthias, and Gotlib Ian H.. 2007. Mood regulation in depression: Differential effects of distraction and recall of happy memories on sad mood. Journal of Abnormal Psychology 116, 3: 484–490. 10.1037/0021-843X.116.3.484 [DOI] [PubMed] [Google Scholar]
- [71].Kadam UT, Croft P, McLeod J, and Hutchinson M. 2001. A qualitative study of patients’ views on anxiety and depression. The British Journal of General Practice: The Journal of the Royal College of General Practitioners 51, 466: 375–380. [PMC free article] [PubMed] [Google Scholar]
- [72].Kang Jin and Wei Lewen. 2018. “Give Me the Support I Want!”: The Effect of Matching an Embodied Conversational Agent’s Social Support to Users’ Social Support Needs in Fostering Positive User-Agent Interaction. In Proceedings of the 6th International Conference on Human-Agent Interaction (HAI ‘18), 106–113. 10.1145/3284432.3284462 [DOI] [Google Scholar]
- [73].Karyotaki Eirini, Riper Heleen, Twisk Jos, Hoogendoorn Adriaan, Kleiboer Annet, Mira Adriana, Mackinnon Andrew, Meyer Björn, Botella Cristina, Littlewood Elizabeth, Andersson Gerhard, Christensen Helen, Klein Jan P., Johanna Schröder Juana Bretón-López, Scheider Justine, Griffiths Kathy, Farrer Louise, Huibers Marcus J. H., Phillips Rachel, Gilbody Simon, Moritz Steffen, Berger Thomas, Pop Victor, Spek Viola, and Cuijpers Pim. 2017. Efficacy of Self-guided Internet-Based Cognitive Behavioral Therapy in the Treatment of Depressive Symptoms: A Meta-analysis of Individual Participant Data. JAMA psychiatry 74, 4: 351–359. 10.1001/jamapsychiatry.2017.0044 [DOI] [PubMed] [Google Scholar]
- [74].Kawachi Ichiro and Berkman Lisa F.. 2001. Social ties and mental health. Journal of Urban Health 78, 3: 458–467. 10.1093/jurban/78.3.458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [75].Kaziunas Elizabeth, Ackerman Mark S., and Veinot Tiffany C. E.. Localizing chronic disease management: Information work and health translations. Proceedings of the American Society for Information Science and Technology 50, 1: 1–10. 10.1002/meet.14505001090 [DOI] [Google Scholar]
- [76].Kelly Ryan, Gooch Daniel, Patil Bhagyashree, and Watts Leon. 2017. Demanding by Design: Supporting Effortful Communication Practices in Close Personal Relationships. In Proceedings of the 2017 ACM Conference on Computer Supported Cooperative Work and Social Computing (CSCW ‘17), 70–83. 10.1145/2998181.2998184 [DOI] [Google Scholar]
- [77].Kou Yubo and Gui Xinning. 2018. Entangled with Numbers: Quantified Self and Others in a Team-Based Online Game. Proc. ACM Hum.-Comput. Interact 2, CSCW: 93:1–93:25. 10.1145/3274362 [DOI] [Google Scholar]
- [78].Lee Kwangyoung and Hong Hwajung. 2017. Designing for Self-Tracking of Emotion and Experience with Tangible Modality. In Proceedings of the 2017 Conference on Designing Interactive Systems (DIS ‘17), 465–475. 10.1145/3064663.3064697 [DOI] [Google Scholar]
- [79].Li Guo, Zhou Xiaomu, Lu Tun, Yang Jiang, and Gu Ning. 2016. SunForum: Understanding Depression in a Chinese Online Community. In Proceedings of the 19th ACM Conference on Computer-Supported Cooperative Work & Social Computing (CSCW ‘16), 515–526. 10.1145/2818048.2819994 [DOI] [Google Scholar]
- [80].Light Ann, Howland Kate, Hamilton Tom, and Harley David A.. 2017. The Meaning of Place in Supporting Sociality. 1141–1152. 10.1145/3064663.3064728 [DOI] [Google Scholar]
- [81].Light Ann, Leong Tuck W., and Robertson Toni. 2015. Ageing Well with CSCW. In ECSCW 2015: Proceedings of the 14th European Conference on Computer Supported Cooperative Work, 19–23 September 2015, Oslo, Norway, 295–304. [Google Scholar]
- [82].Lim Catherine, Berry Andrew B.L., Hirsch Tad, Hartzler Andrea L., Wagner Edward H., Ludman Evette, and Ralston James D.. 2016. “It Just Seems Outside My Health”: How Patients with Chronic Conditions Perceive Communication Boundaries with Providers. In Proceedings of the 2016 ACM Conference on Designing Interactive Systems (DIS ‘16), 1172–1184. 10.1145/2901790.2901866 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [83].Liu Leslie S., Hirano Sen H., Tentori Monica, Cheng Karen G., George Sheba, Park Sun Young, and Hayes Gillian R.. 2011. Improving communication and social support for caregivers of high-risk infants through mobile technologies. In Proceedings of the ACM 2011 conference on Computer supported cooperative work, 475–484. Retrieved August 15, 2015 from http://dl.acm.org/citation.cfm?id=1958897 [Google Scholar]
- [84].Lu Jin, Shang Chao, Yue Chaoqun, Morillo Reynaldo, Ware Shweta, Kamath Jayesh, Bamis Athanasios, Russell Alexander, Wang Bing, and Bi Jinbo. 2018. Joint Modeling of Heterogeneous Sensing Data for Depression Assessment via Multi-task Learning. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol 2, 1: 21:1–21:21. 10.1145/3191753 [DOI] [Google Scholar]
- [85].Lukoff Kai, Yu Cissy, Kientz Julie, and Hiniker Alexis. 2018. What Makes Smartphone Use Meaningful or Meaningless? Proc. ACM Interact. Mob. Wearable Ubiquitous Technol 2, 1: 22:1–22:26. 10.1145/3191754 [DOI] [Google Scholar]
- [86].Mamykina Lena, Mynatt Elizabeth, Davidson Patricia, and Greenblatt Daniel. 2008. MAHI: investigation of social scaffolding for reflective thinking in diabetes management. 477–486. 10.1145/1357054.1357131 [DOI] [Google Scholar]
- [87].Mamykina Lena, Nakikj Drashko, and Elhadad Noemie. 2015. Collective Sensemaking in Online Health Forums. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems (CHI ‘15), 3217–3226. 10.1145/2702123.2702566 [DOI] [Google Scholar]
- [88].Manikonda Lydia and De Choudhury Munmun. 2017. Modeling and Understanding Visual Attributes of Mental Health Disclosures in Social Media. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems (CHI ‘17), 170–181. 10.1145/3025453.3025932 [DOI] [Google Scholar]
- [89].Marlow Jennifer, Dabbish Laura, and Herbsleb Jim. 2013. Impression Formation in Online Peer Production: Activity Traces and Personal Profiles in Github. In Proceedings of the 2013 Conference on Computer Supported Cooperative Work (CSCW ‘13), 117–128. 10.1145/2441776.2441792 [DOI] [Google Scholar]
- [90].Matthews Mark and Doherty Gavin. 2011. In the Mood: Engaging Teenagers in Psychotherapy Using Mobile Phones. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ‘11), 2947–2956. 10.1145/1978942.1979379 [DOI] [Google Scholar]
- [91].Melville Katherine M., Casey Leanne M., and Kavanagh David J.. 2010. Dropout from Internet-based treatment for psychological disorders. The British Journal of Clinical Psychology 49, Pt 4: 455–471. 10.1348/014466509X472138 [DOI] [PubMed] [Google Scholar]
- [92].Miller Daniel. The Internet: Provocation — Cultural Anthropology. Retrieved January 12, 2019 from https://culanth.org/fieldsights/847-the-internet-provocation
- [93].Miller Daniel and Sinanan Jolynna. 2014. Webcam. Polity Press, Cambridge. [Google Scholar]
- [94].Mohr David C., Riper Heleen, and Schueller Stephen M.. 2018. A Solution-Focused Research Approach to Achieve an Implementable Revolution in Digital Mental Health. JAMA Psychiatry 75, 2: 113–114. 10.1001/jamapsychiatry.2017.3838 [DOI] [PubMed] [Google Scholar]
- [95].Mohr David C, Tomasino Kathryn Noth, Lattie Emily G, Palac Hannah L, Kwasny Mary J, Weingardt Kenneth, Karr Chris J, Kaiser Susan M, Rossom Rebecca C, Bardsley Leland R, Caccamo Lauren, Stiles-Shields Colleen, and Schueller Stephen M. 2017. IntelliCare: An Eclectic, Skills-Based App Suite for the Treatment of Depression and Anxiety. Journal of Medical Internet Research 19, 1. 10.2196/jmir.6645 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [96].Mohr David C., Weingardt Ken R., Reddy Madhu, and Schueller Stephen M.. 2017. Three Problems With Current Digital Mental Health Research … and Three Things We Can Do About Them. Psychiatric Services 68, 5: 427–429. 10.1176/appi.ps.201600541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [97].Muller Michael. 2012. Lurking As Personal Trait or Situational Disposition: Lurking and Contributing in Enterprise Social Media. In Proceedings of the ACM 2012 Conference on Computer Supported Cooperative Work (CSCW ‘12), 253–256. 10.1145/2145204.2145245 [DOI] [Google Scholar]
- [98].Murnane Elizabeth L., Walker Tara G., Tench Beck, Voida Stephen, and Snyder Jaime. 2018. Personal Informatics in Interpersonal Contexts: Towards the Design of Technology That Supports the Social Ecologies of Long-Term Mental Health Management. Proc. ACM Hum.-Comput. Interact 2, CSCW: 127:1–127:27. 10.1145/3274396 [DOI] [Google Scholar]
- [99].Newman Mark W., Lauterbach Debra, Munson Sean A., Resnick Paul, and Morris Margaret E.. 2011. It’s Not That I Don’T Have Problems, I’m Just Not Putting Them on Facebook: Challenges and Opportunities in Using Online Social Networks for Health. In Proceedings of the ACM 2011 Conference on Computer Supported Cooperative Work (CSCW ‘11), 341–350. 10.1145/1958824.1958876 [DOI] [Google Scholar]
- [100].Nicholas Jennifer, Shilton Katie, Schueller Stephen M., Gray Elizabeth L., Kwasny Mary J., and Mohr David C.. 2019. The Role of Data Type and Recipient in Individuals’ Perspectives on Sharing Passively Collected Smartphone Data for Mental Health: Cross-Sectional Questionnaire Study. JMIR mHealth and uHealth 7, 4: e12578. 10.2196/12578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [101].Nunes Francisco, Verdezoto Nervo, Fitzpatrick Geraldine, Kyng Morten, Grönvall Erik, and Storni Cristiano. 2015. Self-Care Technologies in HCI: Trends, Tensions, and Opportunities. ACM Trans. Comput.-Hum. Interact 22, 6: 33:1–33:45. 10.1145/2803173 [DOI] [Google Scholar]
- [102].O’Leary Kathleen, Bhattacharya Arpita, Munson Sean A., Wobbrock Jacob O., and Pratt Wanda. 2017. Design Opportunities for Mental Health Peer Support Technologies. In Proceedings of the 2017 ACM Conference on Computer Supported Cooperative Work and Social Computing (CSCW ‘17), 1470–1484. 10.1145/2998181.2998349 [DOI] [Google Scholar]
- [103].O’Leary Kathleen, Schueller Stephen M., Wobbrock Jacob O., and Pratt Wanda. 2018. “Suddenly, We Got to Become Therapists for Each Other”: Designing Peer Support Chats for Mental Health. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems (CHI ‘18), 331:1–331:14. 10.1145/3173574.3173905 [DOI] [Google Scholar]
- [104].Park Sun Young. 2018. Social Support Mosaic: Understanding Mental Health Management Practice on College Campus. In Proceedings of the 2018 Designing Interactive Systems Conference (DIS ‘18), 121–133. 10.1145/3196709.3196787 [DOI] [Google Scholar]
- [105].Qin Yang, Xu Bin, and Cosley Dan. 2017. Designing the Interplay Between Anonymity and Publicity for Online Social Support. In Companion of the 2017 ACM Conference on Computer Supported Cooperative Work and Social Computing (CSCW ‘17 Companion), 283–286. 10.1145/3022198.3026318 [DOI] [Google Scholar]
- [106].Rafaeli Sheizaf, Ravid Gilad, and Soroka Vladimir. De-lurking in virtual communities: a social communication network approach to measuring the effects of social and cultural capital. 10.1109/hicss.2004.1265478 [DOI] [Google Scholar]
- [107].Pei-Luen Patrick Rau Qin Gao, and Ding Yinan. 2008. Relationship between the level of intimacy and lurking in online social network services. Computers in Human Behavior 24: 2757–2770. 10.1016/j.chb.2008.04.001 [DOI] [Google Scholar]
- [108].Stefan Rennick-Egglestone Sarah Knowles, Toms Gill, Bee Penny, Lovell Karina, and Bower Peter. 2016. Health Technologies “In the Wild”: Experiences of Engagement with Computerised CBT. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems (CHI ‘16), 2124–2135. 10.1145/2858036.2858128 [DOI] [Google Scholar]
- [109].Reynolds Frances. 2000. Managing depression through needlecraft creative activities: A qualitative study. The Arts in Psychotherapy 27, 2: 107–114. 10.1016/S0197-4556(99)00033-7 [DOI] [Google Scholar]
- [110].Ringland Kathryn E.. 2019. “Autsome”: Fostering an Autistic Identity in an Online Minecraft Community for Youth with Autism. In iConference 2019 Proceedings. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [111].Ringland Kathryn E.. 2019. A Place to Play: The (Dis)Abled Embodied Experience for Autistic Children in Online Spaces. In CHI 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [112].Ringland Kathryn E., Wolf Christine T., Boyd LouAnne E., Baldwin Mark S., and Hayes Gillian R.. 2016. Would You Be Mine: Appropriating Minecraft As an Assistive Technology for Youth with Autism. In Proceedings of the 18th International ACM SIGACCESS Conference on Computers and Accessibility (ASSETS ‘16), 33–41. 10.1145/2982142.2982172 [DOI] [Google Scholar]
- [113].Ringland Kathryn E., Wolf Christine T., Dombrowski Lynn, and Hayes Gillian R.. 2015. Making “Safe”: Community-Centered Practices in a Virtual World Dedicated to Children with Autism. In Proceedings of the 18th ACM Conference on Computer Supported Cooperative Work & Social Computing (CSCW ‘15), 1788–1800. 10.1145/2675133.2675216 [DOI] [Google Scholar]
- [114].Ringland Kathryn E., Wolf Christine T., Faucett Heather, Dombrowski Lynn, and Hayes Gillian R.. 2016. “Will I always be not social?”: Re-Conceptualizing Sociality in the Context of a Minecraft Community for Autism. In CHI 2016. [Google Scholar]
- [115].Robertson Lucy, Smith Michael, and Tannenbaum Dennis. 2005. Case management and adherence to an online disease management system. Journal of Telemedicine and Telecare 11, 2_suppl: 73–75. 10.1258/135763305775124885 [DOI] [PubMed] [Google Scholar]
- [116].Saeb Sohrab, Lattie Emily G, Kording Konrad P, and Mohr David C. 2017. Mobile Phone Detection of Semantic Location and Its Relationship to Depression and Anxiety. JMIR mHealth and uHealth 5, 8. 10.2196/mhealth.7297 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [117].Scheuerman Morgan Klaus, Branham Stacy M., and Hamidi Foad. 2018. Safe Spaces and Safe Places: Unpacking Technology-Mediated Experiences of Safety and Harm with Transgender People. Proceedings of the ACM on Human-Computer Interaction 2, CSCW: 1–27. 10.1145/3274424 [DOI] [Google Scholar]
- [118].Schmitt Zachary and Yarosh Svetlana. 2018. Participatory Design of Technologies to Support Recovery from Substance Use Disorders. Proc. ACM Hum.-Comput. Interact 2, CSCW: 156:1–156:27. 10.1145/3274425 [DOI] [Google Scholar]
- [119].Schorch Marén, Wan Lin, Randall David William, and Wulf Volker. 2016. Designing for Those Who Are Overlooked: Insider Perspectives on Care Practices and Cooperative Work of Elderly Informal Caregivers. In Proceedings of the 19th ACM Conference on Computer-Supported Cooperative Work & Social Computing (CSCW ‘16), 787–799. 10.1145/2818048.2819999 [DOI] [Google Scholar]
- [120].Schroeder Jessica, Wilkes Chelsey, Rowan Kael, Toledo Arturo, Paradiso Ann, Czerwinski Mary, Mark Gloria, and Linehan Marsha M.. 2018. Pocket Skills: A Conversational Mobile Web App To Support Dialectical Behavioral Therapy. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems (CHI ‘18), 398:1–398:15. 10.1145/3173574.3173972 [DOI] [Google Scholar]
- [121].Searle Aidan, Calnan Michael, Lewis Glyn, Campbell John, Taylor Adrian, and Turner Katrina. 2011. Patients’ views of physical activity as treatment for depression: a qualitative study. British Journal of General Practice 61, 585: e149–e156. 10.3399/bjgp11X567054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [122].Segrin Chris. 2000. Social skills deficits associated with depression. Clinical Psychology Review 20, 3: 379–403. 10.1016/S0272-7358(98)00104-4 [DOI] [PubMed] [Google Scholar]
- [123].Shinohara Kristen and Wobbrock Jacob O.. 2011. In the shadow of misperception: assistive technology use and social interactions. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, 705–714. Retrieved April 27, 2014 from http://dl.acm.org/citation.cfm?id=1979044 [Google Scholar]
- [124].Storni Cristiano. 2014. Design Challenges for Ubiquitous and Personal Computing in Chronic Disease Care and Patient Empowerment: A Case Study Rethinking Diabetes Self-monitoring. Personal Ubiquitous Comput. 18, 5: 1277–1290. 10.1007/s00779-013-0707-6 [DOI] [Google Scholar]
- [125].Storni Cristiano. 2015. Patients’ lay expertise in chronic self‐care: a case study in type 1 diabetes. Health Expectations : An International Journal of Public Participation in Health Care and Health Policy 18, 5: 1439–1450. 10.1111/hex.12124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [126].Sun Na. 2014. Understanding lurkers in online communities: A literature review. Computers in Human Behavior: 8. [Google Scholar]
- [127].Torous John, Nicholas Jennifer, Larsen Mark E., Firth Joseph, and Christensen Helen. 2018. Clinical review of user engagement with mental health smartphone apps: evidence, theory and improvements. Evidence-Based Mental Health 21, 3: 116–119. 10.1136/eb-2018-102891 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [128].Tsugawa Sho, Kikuchi Yusuke, Kishino Fumio, Nakajima Kosuke, Itoh Yuichi, and Ohsaki Hiroyuki. 2015. Recognizing Depression from Twitter Activity. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems (CHI ‘15), 3187–3196. 10.1145/2702123.2702280 [DOI] [Google Scholar]
- [129].Tuli Anupriya, Singh Pushpendra, Sood Mamta, Deb Koushik Sinha, Jain Siddharth, Jain Abhishek, Wason Manan, Chadda Rakesh, and Verma Rohit. 2016. Harmony: Close Knitted Mhealth Assistance for Patients, Caregivers and Doctors for Managing SMIs. In Proceedings of the 2016 ACM International Joint Conference on Pervasive and Ubiquitous Computing: Adjunct (UbiComp ‘16), 1144–1152. 10.1145/2968219.2968301 [DOI] [Google Scholar]
- [130].Unbehaun David, Aal Konstantin, Daryoush Daniel Vaziri Rainer Wieching, Tolmie Peter, and Wulf Volker. 2018. Facilitating Collaboration and Social Experiences with Videogames in Dementia: Results and Implications from a Participatory Design Study. Proc. ACM Hum.-Comput. Interact 2, CSCW: 175:1–175:23. 10.1145/3274444 [DOI] [Google Scholar]
- [131].Vanderhorst RK and McLaren S. 2005. Social relationships as predictors of depression and suicidal ideation in older adults. Aging & Mental Health 9, 6: 517–525. 10.1080/13607860500193062 [DOI] [PubMed] [Google Scholar]
- [132].Varga‐Atkins Tünde and O’Brien Mark. 2009. From drawings to diagrams: maintaining researcher control during graphic elicitation in qualitative interviews. International Journal of Research & Method in Education 32, 1: 53–67. 10.1080/17437270902759998 [DOI] [Google Scholar]
- [133].Veinot Tiffany C. E., Meadowbrooke Chrysta C., Newman Mark W., Zheng Kai, and Perry Erica E.. 2010. Routines That Ease the Pain: The Information World of a Dialysis Clinic. In Proceedings of the 73rd ASIS&T Annual Meeting on Navigating Streams in an Information Ecosystem - Volume 47 (ASIS&T ‘10), 23:1–23:4. Retrieved April 16, 2018 from http://dl.acm.org/citation.cfm?id=1920331.1920364 [Google Scholar]
- [134].Wang Emily Q. and Piper Anne Marie. 2018. Accessibility in Action: Co-Located Collaboration Among Deaf and Hearing Professionals. Proc. ACM Hum.-Comput. Interact 2, CSCW: 180:1–180:25. 10.1145/3274449 [DOI] [Google Scholar]
- [135].Wang Rui, Wang Weichen, daSilva Alex, Huckins Jeremy F., Kelley William M., Heatherton Todd F., and Campbell Andrew T.. 2018. Tracking Depression Dynamics in College Students Using Mobile Phone and Wearable Sensing. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol 2, 1: 43:1–43:26. 10.1145/3191775 [DOI] [Google Scholar]
- [136].Wang Yiran, Niiya Melissa, Mark Gloria, Reich Stephanie M., and Warschauer Mark. 2015. Coming of Age (Digitally): An Ecological View of Social Media Use among College Students. 571–582. 10.1145/2675133.2675271 [DOI] [Google Scholar]
- [137].Williams David L., Crittenden Victoria L., Keo Teeda, and McCarty Paulette. 2012. The use of social media: an exploratory study of usage among digital natives: The use of social media. Journal of Public Affairs 12, 2: 127–136. 10.1002/pa.1414 [DOI] [Google Scholar]
- [138].Wolf Christine T. and Veinot Tiffany C.. 2015. Struggling for space and finding my place: An interactionist perspective on everyday use of biomedical information: Struggling for Space and Finding My Place. Journal of the Association for Information Science and Technology 66, 2: 282–296. 10.1002/asi.23178 [DOI] [Google Scholar]
- [139].Yamashita Naomi, Kuzuoka Hideaki, Hirata Keiji, and Kudo Takashi. 2013. Understanding the conflicting demands of family caregivers caring for depressed family members. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, 2637–2646. Retrieved November 8, 2013 from http://dl.acm.org/citation.cfm?id=2481365 [Google Scholar]
- [140].Yamashita Naomi, Kuzuoka Hideaki, Kudo Takashi, Hirata Keiji, Aramaki Eiji, and Hattori Kazuki. 2018. How Information Sharing about Care Recipients by Family Caregivers Impacts Family Communication. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems - CHI ‘18, 1–13. 10.1145/3173574.3173796 [DOI] [Google Scholar]
- [141].Zhang Renwen, Eschler Jordan, and Reddy Madhu. 2018. Online Support Groups for Depression in China: Culturally Shaped Interactions and Motivations. Computer Supported Cooperative Work: CSCW: An International Journal: 1–28. 10.1007/s10606-018-9322-4 [DOI] [Google Scholar]
- [142].Zhang Xiao, Li Wenzhong, Chen Xu, and Lu Sanglu. 2018. MoodExplorer: Towards Compound Emotion Detection via Smartphone Sensing. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol 1, 4: 176:1–176:30. 10.1145/3161414 [DOI] [Google Scholar]
- [143].NIMH » Major Depression. Retrieved January 2, 2019 from https://www.nimh.nih.gov/health/statistics/major-depression.shtml
- [144].Harper Douglas. 2002. Talking about pictures: A case for photo elicitation: Visual Studies: Vol 17, No 1. Retrieved February 18, 2019 from https://www.tandfonline.com/doi/abs/10.1080/14725860220137345 [Google Scholar]
- [145].Home | Dedoose. Retrieved January 16, 2019 from https://www.dedoose.com/
- [146].Depression (major depressive disorder) - Symptoms and causes. Mayo Clinic. Retrieved April 2, 2019 from https://www.mayoclinic.org/diseases-conditions/depression/symptoms-causes/syc-20356007 [Google Scholar]