

Abstract
Urolithiasis is a worldwide spread condition that affects patients’ Health-Related Quality of Life (HRQOL), which measurement is an important tool for routine clinical and research practice. Disease-specific HRQOL measures demonstrated to perform better in assessing the effects of specific conditions. A disease-specific questionnaire for kidney stones, the WISQOL, has been validated in different languages, but an Italian version is still missing. Our aim is to produce and validate the Italian version of WISQOL (IT-WISQOL). Patients undergoing any elective treatment for upper urinary tract stones were enrolled. A multi-step process with forward- and back-translation was used to translate WISQOL into Italian. Patients were evaluated within 15 days pre-operatively and then at 30-, 90 days post-operatively and administered both IT-WISQOL and SF-36v2. Post-operative data such as 30 days postoperative complications, late stone-related events, successful status, and stone complexity were collected. Cronbach’s α was used to evaluate the internal consistency of IT-WISQOL, while Spearman’s rho was used for item and inter-domain correlations and IT-WISQOL with SF-36v2 correlation. We found excellent internal consistency across all domains (α ≥ 0.88), particularly when the total score is considered (α = 0.960). Test–retest reliability showed excellent results for the total questionnaire (Pearson correlation value: 0.85). The Inter-domain association ranged from 0.497 to 0.786. Convergent validity was confirmed by a good correlation with subdomains of the SF-36v2 measures. IT-WISQOL is a reliable tool to measure HRQOL in stone patients. It shows analog characteristics if compared to English WISQOL.
Supplementary Information
The online version contains supplementary material available at 10.1007/s00240-022-01382-7.
Keywords: Health-related quality of life, WISQOL, SF-36v2, Kidney stones, Urolithiasis, Questionnaire
Introduction
Urolithiasis is a worldwide spread condition with a prevalence ranging from 1 to 20% [1] and it is expected to represent a rising global challenge [2]. Additionally, the high risk of recurrence may determine the need to repeat periodically investigations and/or surgical treatments, and may as well expose patients to bothersome symptoms, including pain, infections, haematuria, etc. [3]. These events may affect patients’ Quality of Life (QOL) under many aspects, from social to working life. In fact, kidney stones have been shown to be associated with stress, anxiety, and depression even between acute episodes [4, 5]. As expected, Health-related QOL (HRQOL) of stone formers was found to be reduced compared to healthy adults [6].
HRQOL measurements are important tools for routine clinical and research practice, as they provide a better understanding of the specific disease’s impact, and they allow to standardize elements that are difficult to balance. In recent years, they have gained growing attention and influenced treatment strategies. In terms of urolithiasis, urologists rely on surrogates of surgical adequacy, like the absence of residual fragments or complication rates, to determine the success of different treatments. Patients’ perspectives are frequently different and consider also different elements including the invasiveness of the procedure, the peri-operative discomfort, the length and complexity of postoperative recovery. All these elements have to be measured and balanced before treatment planning and should be discussed during patients’ counseling [7]. Additionally, the evaluation and comparison of HRQOL may play an important role in data comparison and research purposes.
Different generic questionnaires have been created to evaluate the effect of surgeries on patients’ general HRQOL [8]. However, they might not be sufficient to gain a deep understanding of the impact of urinary stone disease. Furthermore, it is demonstrated that disease-specific HRQOL measures perform better than their generic equivalents in assessing the effects of specific conditions [9].
To fill this gap, a disease-specific questionnaire for kidney stones, the “wisconsin stone quality of life questionnaire” (WISQOL), was recently developed and validated by Penniston et al. [7, 10].
The WISQOL has already been translated and validated in different languages, i.e., Spanish, Turkish, Korean, French,German, Chinese, Japanese and Slovak [11–18], but an Italian version has not been developed and tested yet.
Aim of our study is to produce and validate the Italian version of WISQOL (IT-WISQOL). We will also test its reliability using for comparison the 36-Item Short Form Health Survey (SF-36v2), a validated questionnaire to evaluate HRQOL.
Materials and methods
Study design
Six different Italian urological centers sited in different regions of the peninsula were involved in this prospective observational study. The initial study period was 2019–2020. Due to the advent of the COVID-19 outbreak and related difficulties in recruiting patients, we extended it to September 2021.
Patients undergoing any elective treatment for upper urinary tract stones with curative intent were enrolled in the study. Surgical treatments included Extracorporeal Shock Wave Lithotripsy (SWL), ureterolithotripsy (URS), Retrograde Intra-Renal Surgery (RIRS) or Percutaneous Nephrolithotomy (PCNL). All cases have been carried out by surgeons beyond their learning curve. Patients treated in an emergency setting were excluded from the study.
To be eligible, patients had to be older than 18 years, native Italian speakers, with a computed tomography (CT) scan performed pre-operatively within 3 months and willing and able to give informed consent. Exclusion criteria included any of the following: contraindications to surgical treatment; no preoperative CT scan available within 3 months before surgery; pregnant patients; American Society of Anesthesiologists (ASA) [19] score ≥ 3 or any other ongoing medical conditions causing pain or deterioration of general health.
Questionnaires in use
The WISQOL questionnaire is composed of 28 items and it measures disease-specific impact identifying four different domains: social impact, emotional impact, disease impact, and impact on vitality [10]. Each item of the questionnaire is scored on a Likert scale ranging from 1 to 5, with the maximum score being 140 and, thus, a high score correlates to high HRQOL [7]. The WISQOL only refers to events or symptoms occurring in the previous four weeks.
SF-36v2 is a multipurpose, short-form health survey, widely adopted because of its shortness and comprehensiveness, and differently from WISQOL it is a generic measure. It is built on three levels: (1) 36 items, each of those is used in scoring only one scale; (2) eight scales that can be grouped by four according to the physical and mental health variance they have in common to form (3) two summary measures, called “Physical Health” and “Mental Health” [20].
Questionnaire preparation
The translation process followed the multi-step process recommended by Hutchinson [21].
The original version of WISQOL was reviewed and translated into Italian by two native Italian-speaking urologists. Both surgeons were specialized in urolithiasis management and fluent in English. A meeting was held to review both versions and consensus was achieved on an initial version of the questionnaire. Subsequently, the questionnaire was administered to a different urologist not familiar with WISQOL to carry out the back-translation in English. This back-translated version and the original English version were reviewed together for comparison. Few further modifications were introduced to render it easier to read and understand. A final consensus was reached after two rounds of meetings. Five patients were recruited and administered the questionnaire to test its readability and comprehension. All participants were able to understand and fill in the questionnaire correctly, so no further modifications were included.
Patients were evaluated within 15 days pre-operatively and then at 30-, 90-days post-operatively and administered both IT-WISQOL and the SF-36v2.
30 days postoperative complications were collected and graded using Clavien-Dindo classification System [22]. In the case of PCNL, the modified version by de la Rosette et al. was utilized [23]. Late stone-related events were also recorded. Successful status, defined as no residual fragment ≥ 2 mm, was assessed either by performing non-contrast-enhanced CT or by an ultrasound scan of the urinary tract plus kidney-ureter-bladder (KUB) radiogram within 3 months after treatment. The stone complexity was calculated using Guy’s and S.T.O.N.E. nephrolithometry scores [24, 25].
Sample size population
Previous studies validating different language versions of the questionnaire documented a Spearman’s rank correlation between WISQOL and SF-36v2 varying between 0.5 and 0.7 [10, 12–14]. Expecting similar results, considering a 95% Fisher confidence interval, a sample size population of about 150–200 patients was calculated to obtain adequate results.
Statistical analysis
All the data were analyzed with the IBM Statistical Package for the Social Sciences Statistics version 25.0 (IBM SPSS Statistics; Armonk, NY, USA). Continuous variables are presented as means (SD) in cases of normal distribution and compared using the independent Student’s t test, while in cases of skewed distributions they are presented as median and interquartile range (IQR) and compared using the Mann–Whitney U test. Categorical variables are presented as numbers with percentages and compared using chi-square or Fisher’s exact tests. Cronbach’s α was used to evaluate internal consistency of IT-WISQOL between Centers. Test–retest reliability was evaluated by comparing the 30-day-postoperative questionnaire and the 3-month-postoperative questionnaire. Spearman test was used for item and inter-domain correlations and for IT-WISQOL Total Score. As Penniston et al. [10] did, IT-WISQOL was divided into four domains describing social impact, emotional impact, disease impact and impact on vitality, and matched with the relative domains of SF-36v2, namely “Role Physical”, “Mental Health”, “Body Pain”, “Vitality”. Correlation of total Scores of IT-WISQOL and SF-36v2 was assessed to determine convergent validity using Spearman rank correlation. Correlations between clinical variables and results from IT-WISQOL and SF-36v2 were analyzed to assess the effect of these on results. Cronbach’s α and correlation coefficients results were interpreted as in the original WISQOL development study. Statistical significance will be considered for two-tailed P values of < 0.05.
Results
A total of 226 patients were enrolled in the study. Patients’ characteristics and preoperative outcomes are reported in Supplementary Table 1. Among them 141 (62.4%) were male and 85 (37.6%) were female. Most of them (68.1%) had a high school degree or higher. A minority of patients were stented (24.8%) or had a nephrostomy placed (6.2%) before treatment. Stone’s cumulative diameter was in median (IQR) 12.5 (8.2–20.0) mm. Median (IQR) Guy’s score was 2 (1–2), median (IQR) S.T.O.N.E. score was 7 (5–8). Perioperative data are reported in Supplementary Table 2. Majority of patients (49.5%) underwent retrograde treatments (URS or RIRS), 28.3% underwent SWL and 22.12% PCNL. Most patients (68.6%) were discharged with indwelling ureteral stent or nephrostomy tube, that were removed after a median of 21(1–45) days. 22 patients (9.7%) experienced minor complications (Clavien–Dindo ≤ 2) during in-hospital stay, mostly haematuria. In the following month, 23 (9.3%) patients experienced complications and stent-related pain was the most common complication reported. 32 (14.2) experienced a stone-related event within 3 months from discharge. Overall SFR at 3 months was 86.7%.
Questionnaires
The average preoperative IT-WISQOL score of 226 patients was 96.16 ± 23.86. It raised to 103.66 ± 19.87 at 30 days postoperative and 109.07 ± 19.56 at 3 months postoperative. Fig. 1a, b, c describe the correlation between IT-WISQOL and SF-36v2 preoperative, 30- and 90 days separately. The total score of IT-WISQOL and SF-36v2 had significant correlation in all three preoperative (r = 0.836, p < 0.001), 30 days postoperative (r = 0.827, p < 0.001) and 90 days postoperative (r = 0.817, p < 0.001) questionnaires.
Fig. 1.
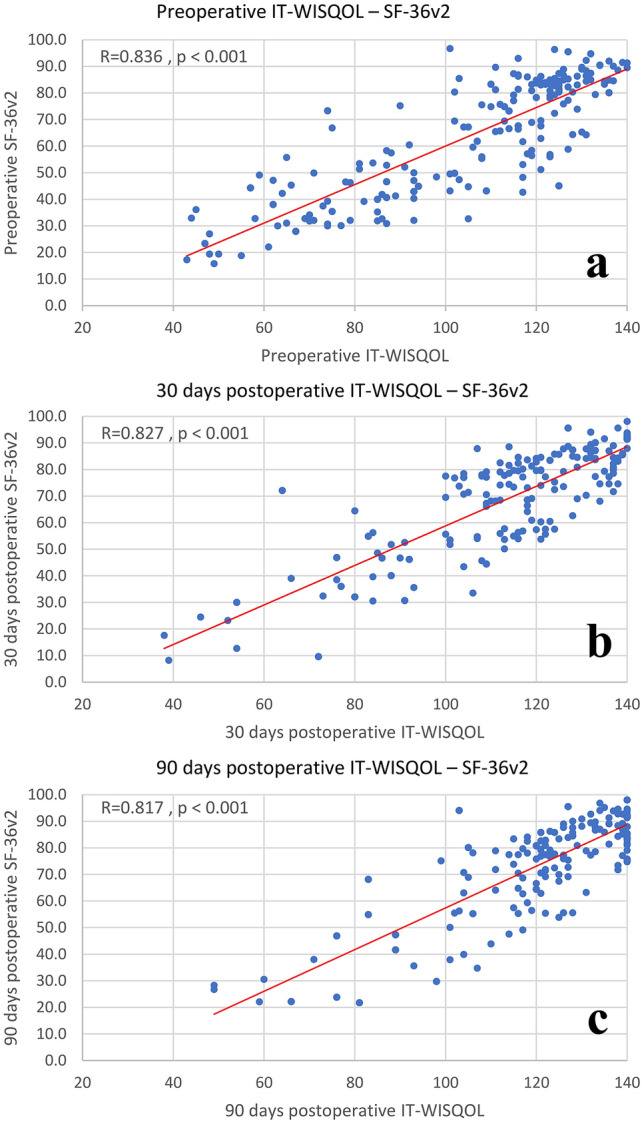
Correlation of WISQOL and SF-36v2 a Preoperative; b 30 days postoperative; c 3 months postoperative. Min–Max of IT-WISQOL score is 28–140 respectively
The internal consistency of each domain was evaluated by Cronbach’s α of the preoperative questionnaire. The α values were all > 0.8, representing excellent internal consistency. Test–retest reliability was evaluated by comparing the 30-day-postoperative questionnaire and the 3-month-postoperative questionnaire. The value of Pearson correlation of each domain was > 0.6 and no significant differences were observed (p < 0.01) (Table 1).
Table 1.
Internal Consistency and Test–retest reliability
| Internal consistency | Test | Retest | Pearson correlation value (p < 0.01) | |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| D1-social impact | 0.899 | 32.66 ± 7.55 | 34.91 ± 5.68 | 0.66 |
| D2-emotional impact | 0.888 | 27.58 ± 6.33 | 29.14 ± 5.69 | 0.67 |
| D3-stone-related impact | 0.903 | 31.43 ± 7.35 | 33.49 ± 6.57 | 0.70 |
| D4-vitality impact | 0.929 | 11.99 ± 3.44 | 12.79 ± 2.92 | 0.65 |
| Total score | 0.960 | 83.45 ± 45.69 | 84.94 ± 49.41 | 0.85 |
D1 domain 1-social impact (WISQOL items: 3a, 3b, 3c, 3d, 3e, 6a, 6b, 6c), D2 domain 2-emotional impact (WISQOL items: 4c, 7a, 7b, 7c, 7d, 7e, 7f), D3 domain 3-disease impact (WISQOL items: 2a, 2b, 2c, 2d, 5a, 5b, 5c, 5d), D4 domain 4-impact on vitality (WISQOL items: 1a, 1b, 1c)
The value of the inter-domain association ranged from 0.497 to 0.786, showing a moderate difference and correlation among domains. Different domains of all three questionnaires demonstrated a significant correlation to the total score (Table 2).
Table 2.
Spearman rank correlations: inter-domain association and convergent validity
| Domains | Preoperative | 30 days postoperative | 3 months postoperative |
|---|---|---|---|
| Inter-domain association | |||
| D1-D2 | 0.721 | 0.771 | 0.733 |
| D1-D3 | 0.614 | 0.723 | 0.699 |
| D1-D4 | 0.681 | 0.633 | 0.650 |
| D2-D3 | 0.593 | 0.640 | 0.573 |
| D2-D4 | 0.636 | 0.606 | 0.497 |
| D3-D4 | 0.786 | 0.709 | 0.704 |
| D1-TOTAL | 0.847 | 0.728 | 0.736 |
| D2-TOTAL | 0.810 | 0.626 | 0.620 |
| D3-TOTAL | 0.849 | 0.719 | 0.726 |
| D4-TOTAL | 0.850 | 0.695 | 0.712 |
| Convergent Validity* | |||
| D1-Role physical | 0.668 | 0.570 | 0.531 |
| D2-Mental health | 0.605 | 0.425 | 0.347 |
| D3-Body pain | 0.624 | 0.646 | 0.559 |
| D4-Vitality | 0.709 | 0.639 | 0.604 |
D1 domain 1-social impact (WISQOL items: 3a, 3b, 3c, 3d, 3e, 6a, 6b, 6c), D2 domain 2-emotional impact (WISQOL items: 4c, 7a, 7b, 7c, 7d, 7e, 7f), D3 domain 3-disease impact (WISQOL items: 2a, 2b, 2c, 2d, 5a, 5b, 5c, 5d), D4 domain 4-impact on vitality (WISQOL items: 1a, 1b, 1c)
*Correlations between corresponding domains in the WISQOL and SF-36v2 questionnaires
All domains of IT-WISQOL significantly correlate with the corresponding domains of SF-36v2, though the value of Spearman rank test turned weaker at two postoperative questionnaires (Table 2).
Discussion
Urolithiasis is a common condition with increasing incidence worldwide [2]. Patients’ HRQOL was found to be decreased, particularly with respect to their physical and mental states [5, 6, 26–28]. Penniston et al. [7, 10] developed a stone-specific questionnaire, the WISQOL, with robust psychometric properties, which has been already translated and validated in different languages [11–15]. Worldwide, we are observing an increasing interest in publishing high-quality papers on urolithiasis. In fact, Abedi et al. [29], during the decade 2010–2020 if compared with the previous decade, reported an increased volume of publications corresponding to 133, 103.5 and 70.4% for ureteroscopies, PCNLs and SWL respectively. This fact highlights the need for tools to objectively report, analyze and compare HRQOL parameters. Therefore, in our opinion, the IT-WISQOL will provide important support for this purpose.
This study demonstrates that IT-WISQOL is a reliable assessment tool for the evaluation of symptoms in patients suffering from urolithiasis. IT-WISQOL showed satisfactory validation results, with excellent internal consistency across all domains (α ≥ 0.88), particularly when the total score is considered (α = 0.960). Similar results were also found with the original WISQOL [10] and the French version [13], both with a total score α = 0.970. The test–retest reliability showed good values for each domain and excellent results for the total questionnaire (Pearson correlation value for total score: 0.85) (Table 1). Comparison with other studies is not easy as test–retest reliability has been measured with different tools, like Spearman rank correlation or Cronbach’s α in the German and Turkish validation studies respectively [12, 14].
Inter-domain reliability analysis showed analogous results to other validation studies [10, 12, 13]. Consistently with previous works [10, 12, 13] we found a strong correlation between the vitality domain (D4) and the emotional domain (D2) at 3-month follow-up (Spearman’s rho correlation coefficient = 0.497), but not at preoperative and 30-days postoperative questionnaires. The reason for these findings remains to be clarified. According to Bhojani et al. [13], this weaker correlation suggests that patients with lower HRQOL in the context of nephrolithiasis also tend to experience higher levels of stress (Table 2).
Convergent validity of IT-WISQOL was confirmed by a good correlation with subdomains of the SF-36v2 measures (Table 2). Figure 1 shows how the total score of IT-WISQOL and SF-36v2 were significantly correlated at any of the follow-up times the questionnaire has been administered. This makes IT-WISQOL a dedicated reliable tool and comparable with the Italian SF-36v2 questionnaire.
This is the first study aiming to evaluate the reliability and adequacy of the Italian version of WISQOL. The questionnaire demonstrated to be reliable if compared to other versions. We included 6 Centers located in different parts of Italy with different dialects and in all of them the questionnaire resulted to be adequately usable.
Our study has some limitations. First of all, the number of patients involved is limited. Studies using IT-WISQOL in larger populations are desirable. Additionally, most of the patients had a high educational level, thus further testing on patients with low education may further improve the readability of the questionnaire. Patients have been recruited in Academic centers, thus they might have more complex stone disease than the general population, affecting our results. Furthermore, the study has been conducted during two COVID-19 outbreaks. This limited our capacity in recruiting patients and a certain amount of distress on patients could be expected, potentially affecting final results.
Future perspectives for this field of study may be the evaluation of the differences of IT-WISQOL scores among sexes or patients of different age as well as to investigate whether HRQOL differs in patients with different preoperative (history of prior stones, stone burden), operative (type of surgery received) or postoperative (presence of residual fragments, stent) characteristics.
Conclusion
The IT-WISQOL has demonstrated to be a reliable tool to measure HRQOL in stone patients. It also showed analog characteristics if compared to English WISQOL. In our opinion it represents an important tool for treatment counseling, monitoring patients’ conditions and also research purposes.
Supplementary Information
Below is the link to the electronic supplementary material.
Author contributions
GM: protocol and project development, manuscript writing, data analysis and interpretation ES: manuscript writing, data collection, data management, data analysis and interpretation WZ: statistical analysis SF, FC, CF, GC, GGG, DZ, AP, MC, NL, RD, NP, CB, MAC, AA, AC: data collection, supervision and critical revision All authors read and approved the final version of the manuscript.
Funding
The authors did not receive financial support.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the ethics committee of each participating center and performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Türk C, Neisius A, Petřík A et al (2021). EAU Guidelines on Urolithiasis. In: EAU Guidelines, edn. presented at the EAU Annual Congress Milan 2021, European Association of Urology Guidelines Office: Arnhem, the Netherlands, (ISBN 978-94-92671-13-4)
- 2.Sorokin I, Mamoulakis C, Miyazawa K, et al. (2017) Epidemiology of stone disease across the world. World J Urol. 2017;359(35):1301–1320. doi: 10.1007/S00345-017-2008-6. [DOI] [PubMed] [Google Scholar]
- 3.Khan SR, Pearle MS, Robertson WG, et al. Kidney stones. Nat Rev Dis Prim. 2016;21(2):1–23. doi: 10.1038/nrdp.2016.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Diniz DHMP, Schor N, Blay SL. stressful life events and painful recurrent colic of renal lithiasis. J Urol. 2006;176:2483–2487. doi: 10.1016/J.JURO.2006.07.156. [DOI] [PubMed] [Google Scholar]
- 5.Angell J, Bryant M, Tu H, et al. Association of depression and urolithiasis. Urology. 2012;79:518–525. doi: 10.1016/J.UROLOGY.2011.10.007. [DOI] [PubMed] [Google Scholar]
- 6.Kartha G, Calle JC, Marchini GS, Monga M. Impact of stone disease: chronic kidney disease and quality of life. Urol Clin North Am. 2013;40:135–147. doi: 10.1016/J.UCL.2012.09.004. [DOI] [PubMed] [Google Scholar]
- 7.Penniston KL, Nakada SY. Development of an instrument to assess the health related quality of life of kidney stone formers. J Urol. 2013;189:921–930. doi: 10.1016/J.JURO.2012.08.247. [DOI] [PubMed] [Google Scholar]
- 8.Urbach DR. Measuring quality of life after surgery. Surg Innov. 2005;12:161–165. doi: 10.1177/155335060501200216. [DOI] [PubMed] [Google Scholar]
- 9.Wiebe S, Guyatt G, Weaver B, et al. Comparative responsiveness of generic and specific quality-of-life instruments. J Clin Epidemiol. 2003;56:52–60. doi: 10.1016/S0895-4356(02)00537-1. [DOI] [PubMed] [Google Scholar]
- 10.Penniston KL, Antonelli JA, Viprakasit DP, et al. Validation and reliability of the wisconsin stone quality of life questionnaire. J Urol. 2017;197:1280–1288. doi: 10.1016/J.JURO.2016.11.097. [DOI] [PubMed] [Google Scholar]
- 11.Basulto-Martínez M, Olvera-Posada D, Velueta-Martínez IA, et al. (2020) Quality of life in patients with kidney stones: translation and validation of the Spanish wisconsin stone quality of life questionnaire. Urolithiasis. 2020;485(48):419–424. doi: 10.1007/S00240-020-01192-9. [DOI] [PubMed] [Google Scholar]
- 12.Atalay HA, Ülker V, Canat L, et al. Validation of the Turkish version of the wisconsin stone-quality of life questionnaire. Turkish J Urol. 2019;45:118–123. doi: 10.5152/TUD.2018.35305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bhojani N, Moussaoui G, Nguyen DD, et al. Validation of the French version of the wisconsin quality of life (WISQOL) questionnaire for patients with nephrolithiasis. Can Urol Assoc J. 2020;15:227–231. doi: 10.5489/cuaj.6552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gottstein M, Pratsinis M, Güsewell S, et al. The German linguistic validation of the wisconsin stone quality of life questionnaire (WisQoL. World J Urol. 2020;396(39):2163–2168. doi: 10.1007/S00345-020-03405-7. [DOI] [PubMed] [Google Scholar]
- 15.Yoon YE, Cho SY. Translation and linguistic validation of the korean version of the wisconsin stone quality of life questionnaire. Int Neurourol J. 2020;24:77–83. doi: 10.5213/INJ.1836238.119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhong W, Xu J, Mazzon G et al (2022) Translation and validation of the Chinese version of wisconsin stone quality of life questionnaire in patients with kidney stones. Minerva Urol Nephrol (online ahead of print). 10.23736/S2724-6051.22.04905-9 [DOI] [PubMed]
- 17.Okada T, Hamamoto S, Taguchi K, et al. Validation of the Japanese version of the wisconsin stone quality of life questionnaire: results from SMART study Group. J Endourol. 2021 doi: 10.1089/END.2021.0292. [DOI] [PubMed] [Google Scholar]
- 18.Svihra J, Sopilko I, Svihrova V, et al. Is health-related quality of life of patients after single-use flexible ureteroscopy superior to extracorporeal shock wave lithotripsy? a randomised prospective study. Urolithiasis. 2021;49:73–79. doi: 10.1007/S00240-020-01224-4. [DOI] [PubMed] [Google Scholar]
- 19.Dripps RD, Lamont A, Eckenhoff JE. The role of anesthesia in surgical mortality. JAMA. 1961;178:261–266. doi: 10.1001/JAMA.1961.03040420001001. [DOI] [PubMed] [Google Scholar]
- 20.Ware JEJ. SF-36 Health survey update. Spine. 2000;25:3130–3139. doi: 10.1097/00007632-200012150-00008. [DOI] [PubMed] [Google Scholar]
- 21.Hutchinson A, Bentzen N, König-Zahn C (1997) Cross-cultural health outcome assessment: a user’s guide. ERGHO (European Research Group on Health Outcomes), (ISBN 9789036707480)
- 22.Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–213. doi: 10.1097/01.sla.0000133083.54934.ae. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.De La Rosette JJMCH, Opondo D, Daels FPJ, et al. Categorisation of complications and validation of the clavien score for percutaneous nephrolithotomy. Eur Urol. 2012;62:246–255. doi: 10.1016/J.EURURO.2012.03.055. [DOI] [PubMed] [Google Scholar]
- 24.Thomas K, Smith NC, Hegarty N, Glass JM. The guy’s stone score—grading the complexity of percutaneous nephrolithotomy procedures. Urology. 2011;78:277–281. doi: 10.1016/J.UROLOGY.2010.12.026. [DOI] [PubMed] [Google Scholar]
- 25.Okhunov Z, Friedlander JI, George AK, et al. S.T.O.N.E. nephrolithometry: novel surgical classification system for kidney calculi. Urology. 2013;81:1154–1160. doi: 10.1016/J.UROLOGY.2012.10.083. [DOI] [PubMed] [Google Scholar]
- 26.Raja A, Hekmati Z, Joshi HB (2016) How do urinary Calculi influence health-related quality of life and patient treatment preference: a systematic review. https://home.liebertpub.com/end 30:727–743. 10.1089/END.2016.0110 [DOI] [PubMed]
- 27.Bryant M, Angell J, Tu H, et al. Health related quality of life for stone formers. J Urol. 2012;188(2):436–440. doi: 10.1016/J.JURO.2012.04.015. [DOI] [PubMed] [Google Scholar]
- 28.Miyaoka R, Ortiz-Alvarado O, Kriedberg C et al (2012) Correlation between stress and kidney stone disease. https://home.liebertpub.com/end 26:551–555. 10.1089/END.2010.0536 [DOI] [PubMed]
- 29.Abedi AR, Razzaghi M, Montazeri S, Allameh F. The trends of urolithiasis therapeutic interventions over the last 20 years: a bibliographic study. J Lasers Med Sci. 2021;12:1–6. doi: 10.34172/jlms.2021.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.