

Abstract
Background
Dancers are at high risk of musculoskeletal disorders. There has been a growing interest in the last few years in pre-season screening using tools to evaluate movement competency, among which is the Movement Competency Screen (MCS). It is currently scored using a categorical 3-level rating system, but this method does not seem to take into account the load level of movements. A 5-level scoring system could potentially alleviate this problem.
Hypothesis/Purpose
For each scoring system, to investigate (1) the internal consistency, and (2) the association with transversus abdominis activation (TrA), hip muscle strength and with Functional Movement screen (FMSTM) total score.
Study design
Secondary analyses of a prospective cohort study.
Methods
One hundred and eighteen professional and preprofessional dancers evolving in ballet or contemporary dance were recruited. The MCS was performed and was scored according to the 3- and 5-level scoring systems. The key variables for movement competency that were considered for convergent validity were the activation ratio of the TrA evaluated with ultrasound imaging and hip strength assessed with a handheld dynamometer. Movement competency was also measured with the FMSTM.
Results
Internal consistency was higher for the 5-level scoring of the MCS items (=0.548) compared to the 3-level scoring system (=0.494). Multiple linear regressions showed that TrA activation, hip adductor strength, and FMSTM could significantly explain 24.0% of the variance for the 5-level scoring system of the MCS whereas hip internal rotator strength and FMSTM could explain only 16.4% of the variance for the 3-level scoring system.
Conclusion
The 5-level scoring system showed better metrologic properties in terms of internal consistency and concurrent validity and therefore, should be preferred over the 3-level scoring system in future research.
Level of Evidence
Level III
Keywords: movement competency, dance, athlete, pre-season screening, musculoskeletal disorder
BACKGROUND
Musculoskeletal injuries among dancers represent a major concern.1–4 In addition to being associated with serious physical and psychological disabilities in athletes, injuries can represent an extensive financial burden on health care systems.5 In order to better understand the underlying pathokinesiology of non-traumatic injuries among dancers, researchers have focused on specific, segmental impairments identified as potential risk factors in other athlete populations.6–9 These risk factors include lower or delayed activation of the transversus abdominis muscle (TrA),6–8 as well as reduced hip and knee muscle strength.9 However, with prevention of injuries in mind, there has been a continued interest in the evaluation of movement competency in recent years, as opposed to specific segmental impairments assessments.10 This shift in approach has given rise to the development of movement competency screening tools.11–14 Movement competency can be defined as the ability to achieve fundamental movements without any functional deficits.15 Strength and motor control are key to preventing faulty movement patterns. For instance, the activation of the TrA and having stronger lower limb muscles have been linked to movement competency.16 The evaluation of movement competency using screening tools has enabled the identification of athletes and workers at risk of injuries.17,18
Among the multiple movement competency screening tools that have been developed, the Functional Movement Screen (FMSTM) and the Movement Competency Screen (MCS) have been investigated.16–21 The MCS was developed and validated for athletes and dancers.16,17,21 It has the interesting characteristic of evaluating different load levels during the performance of movements used in rehabilitation and training programs. Out of 11 movement competency assessment tools reported in the literature, the MCS was identified among the most promising to assess performance capabilities in terms of applicability and the rigor with which it was developed.22 In the original version of the MCS, Kritz described load grades as being scored using a 5-level scoring system : (1) assisted loading, (2) bodyweight loading, (3) external loading, (4) eccentric loading, and (5) plyometric loading.21 According to the currently accepted method for scoring the MCS, those five levels are regrouped into three levels as follows : (1) assisted and bodyweight loading, (2) external and eccentric loading, and (3) plyometric loading.21
The 3-level scoring system thus collapses the five levels into three levels. For example, a movement performed with certain compensations could be rated as a 3 or a 4 on the 5-level system, while on the 3-level scoring system it would be rated as a 2. This appears to be less than optimal since the merging of load levels results in a loss of detailed information. The 5-level scoring system would allow greater precision and, as a result, would more accurately characterize movement competency. The strength of the MCS compared to other movement competency screening tools is the use of load levels. It should therefore be accounted for in detail in the scoring method.
The aim of this technical note was to investigate, in a sample of dancers, and for each MCS scoring system (1) the internal consistency between items and (2) their association with TrA activation, hip strength, and FMSTM total score. It was hypothesized that the 5-level scoring system would show better psychometric properties in terms of internal consistency and concurrent validity as assessed by association with key components of movement competency and another validated movement competency tool.
DESCRIPTION
Data for this study were gathered at one time point prior to the beginning of the 2018-2019 and 2019-2020 dance season and were derived from a prospective cohort study involving 118 dancers, varying in dance style (ballet and contemporary) and status (professional and pre-professional). Dancers were recruited following a presentation of the research project in multiple dance schools and companies. This study was approved by the institutional review board and each participant gave written informed consent. Participants had to be at least 16 years old and had to dance professionally or pre-professionally for at least 10 hours per week. They were excluded if they were pregnant because of the impact on the lumbopelvic muscles, or if they had a musculoskeletal disorder that restricted dancing at the time of the evaluation. Participants underwent an assessment conducted by an experienced physiotherapist who has been a dancer for 17 years, a dance educator for eight years and who treats dancers in her regular practice. The assessment included the evaluation of TrA activation, hip strength, and movement competency. The evaluation was done on-site in dance schools or companies, either in a dance studio or in a physiotherapist’s office if one was available.
Independent variables
The preferential activation ratio of the TrA was evaluated using ultrasound imaging (GE LOGIQ E, GE Healthcare, Milwaukee, Wisconsin, 13 MHz linear probe in B-mode) in a standardized position.23–25 Dancers were in a supine position with both knees at a 90° flexion. The probe was positioned between the axillary and mamillary lines, at mid-distance between the iliac crest and 12th rib in a transverse plane. The preferential activation ratio is calculated to take into account the activation of the internal and external obliques. This method thus considers the possible compensations of these muscles. Both sides were assessed three times and a mean value was obtained.
The strength of the hip flexors, extensors, abductors, adductors, and external and internal rotators were measured in a standardized position using a handheld dynamometer secured with straps.26 The exact positions used are described in a previous study.16 Both sides were assessed three times with a 30 second break in between each measurement. A mean value was obtained and used for analysis.
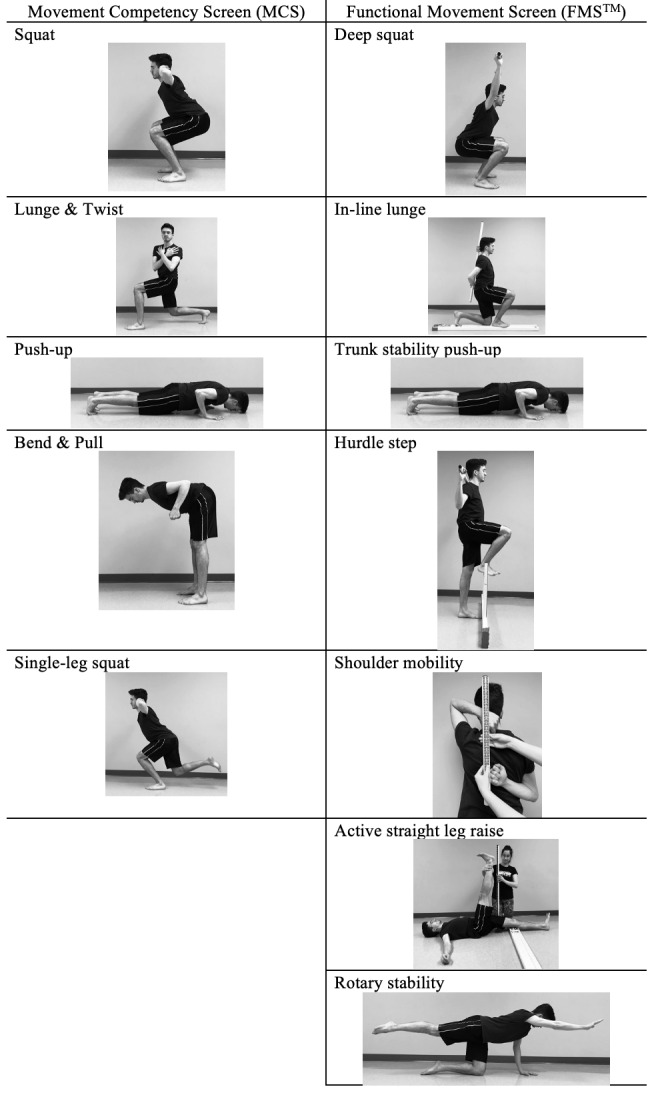
Movement competency was screened using two distinct instruments, the FMSTM and the MCS.17–21 The MCS is composed of five tasks designed to assess global movement competency: (1) squat, (2) lunge and twist, (3) bend and pull, (4) push-up and (5) single-leg squat. The lunge and twist, and the bend and pull are subdivided into the individual components of each movement. Therefore, there are seven items to be evaluated. Each item has a set of possible primary and secondary compensations. The scoring is completed by evaluating the number of compensations observed. More frequent compensations result in a lower score. Additionally, primary compensations are more detrimental to the score than secondary compensations. The tasks of the MCS can be completed with multiple load levels, according to the evaluator’s judgement. The movement can be completed slowly, rapidly, or using plyometrics. As per the accepted scoring system, the 3-level score is attributed only according to the compensations observed, with no discrimination between assisted and bodyweight loading or external and eccentric loading. The MCS was scored using both the 5-level scoring system that uses separate load levels (assisted, bodyweight, external, eccentric, and plyometric) and the 3-level scoring system in which they are grouped as described above. The FMSTM does not include different load levels. Each movement is done at a slow pace. Figure 1 shows a comparison between the movements from the MCS and the FMSTM.
Figure 1. Comparison between MCS and FMSTM .
Statistical analysis
Statistical analyses were conducted in SPSS 28.0. Cronbach’s alpha was first calculated for items scored with the 5-level system and then, for items scored with the 3-level system, to assess internal consistency. To identify the scoring system that best suited the variables, simple linear regressions were first used for the 5-level and then for the 3-level scoring system. FMS scores, TrA activation, and hip strength were used as independent variables. Each independent variable’s association with movement competency was examined, as well as the proportion of variance for the total MCS score that they each explained. A multiple regression model was built which included the variables significantly associated with the MCS score for each scoring system. Therefore, a different model was built for the 5-level and 3-level systems since the results from the simple regression analyses identified different variables as being associated with the dependent variables. Since dance hours could be a potential confounder in the analyses, each linear regression was controlled for this variable. The level of significance for all statistical analyses was set at p≤0.05. Statistical assumptions were met for each linear regression completed.
OUTCOMES
The sample was composed of 118 preprofessional and professional dancers. Table 1 presents demographic information. No adverse events occurred during the evaluations.
Table 1. Demographics.
| N(%) or Mean ± SD | |
| Sample | 118 (100) |
| Age (years) | 21.6 ± 5.2 |
| Gender (female / male / nonbinary) | 92 (78) / 24 (20) / 2 (2) |
| Style (contemporary / ballet) | 66 (57) / 49 (43) |
| Status (preprofessional / professional) | 91 (78) / 25 (22) |
Table 2 presents the results of separate linear regressions between each independent variable and the MCS total score, where each item was scored using either the 5-level system or the 3-level system.
Table 2. Simple linear regressions.
| MCS total score /5 as dependent variable | |||||
| Independent variables | Adjusted R2 | Standardized β | 95% C.I. | p | |
| TrA activation Dominant side |
0.033 | 0.203 | [0.281, 4.800] | 0.028 | |
| Hip flexor strength Non dominant side |
0.024 | 0.180 | [-0.001, 0.168] | 0.052 | |
| Hip extensor strength Non dominant side |
0.081 | 0.301 | [0.029, 0.136] | 0.003 | |
| Hip abductor strength Non dominant side |
0.075 | 0.288 | [0.035, 0.146] | 0.002 | |
| Hip adductor strength Non dominant side |
0.084 | 0.303 | [0.039, 0.145] | 0.001 | |
| Hip external rotator strength Non dominant side |
0.038 | 0.215 | [0.022, 0.250] | 0.019 | |
| Hip internal rotator strength Non dominant side |
-0.009 | 0.010 | [-0.083, 0.093] | 0.913 | |
| FMSTM total score | 0.200 | 0.455 | [0.758, 1.610] | <0.001 | |
| MCS total score /3 as dependent variable | |||||
| Independent variables | Adjusted R2 | Standardized β | 95% C.I. | p | |
| TrA activation Dominant side |
0.005 | 0.116 | [-0.433, 1.936] | 0.211 | |
| Hip flexor strength Non dominant side |
-0.005 | 0.063 | [-0.029, 0.059] | 0.498 | |
| Hip extensor strength Non dominant side |
-0.001 | 0.098 | [-0.015, 0.42] | 0.342 | |
| Hip abductor strength Non dominant side |
-0.005 | 0.063 | [-0.020, 0.040] | 0.499 | |
| Hip adductor strength Non dominant side |
-0.008 | 0.031 | [-0.024, 0.034] | 0.738 | |
| Hip external rotator strength Non dominant side |
0.001 | -0.098 | [-0.092, 0.028] | 0.293 | |
| Hip internal rotator strength Non dominant side |
0.037 | -0.214 | [-0.097, -0.008] | 0.020 | |
| FMSTM total score | 0.054 | 0.250 | [0.096, 0.575] | 0.006 | |
MCS : Movement Competency Screen; FMSTM : Functional Movement Screen; TrA : transversus abdominis
The 5-level scoring system as the dependent variable
The internal consistency assessed with Cronbach’s alpha for the seven items of the MCS scored with the 5-level system was 0.548. It was found using simple linear regressions that TrA activation, hip extensor, abductor, adductor, and external rotator strength, as well as FMSTM total score (β=0.455, p<0.001) were statistically significantly associated with the MCS total score as measured by the 5-level scoring system. Given multicollinearity between hip strength variables in the multiple linear regression model, only hip adductor strength was introduced in the model. This variable was chosen since it was the most significantly and strongly associated with the MCS total score. As seen in Table 3, the multivariate model accounted for 24% of the variance for the MCS scored on the 5-level system (F=13.324, p<0.001).
Table 3. Multiple linear regression.
| MCS total score /5 as dependent variable | |||||
| Independent variables | Adjusted R2 | Standardized β | 95% C.I. | p | |
| TrA activation Dominant side |
0.240 | 0.115 | [-0.595, 3.482] | 0.163 | |
| Hip adductor strength Non dominant side |
0.195 | [0.009, 0.109] | 0.021 | ||
| FMSTM total score | 0.389 | [0.582, 1.446] | <0.001 | ||
| MCS total score /3 as dependent variable | |||||
| Independent variables | Adjusted R2 | Standardized β | 95% C.I. | p | |
| Hip internal rotator strength Non dominant side |
0.133 | -0.303 | [-0.118, -0.031] | <0.001 | |
| FMSTM total score | 0.332 | [0.208, 0.684] | <0.001 | ||
MCS: Movement Competency Screen; TrA : transversus abdominis; FMSTM : Functional Movement Screen.
The 3-level scoring system as the dependent variable
Regarding the internal consistency, Cronbach’s alpha for the seven items of the 3-level scoring system was 0.494. Simple linear regression analyses revealed significant associations with hip internal rotator strength and FMSTM total score (β=0.250, p=0.006) with the MCS total scored on a 3-level system. Results showed that the multiple linear regression model built accounted for 13.3% of the variance for the MCS on a 3-level scoring system (F=9.959, p<0.001).
DISCUSSION
The purpose of this study was to examine the internal consistency for the items scored with each system and to explore if the association of TrA activation, hip muscle strength, and FMS score was higher with the 5-level scoring system, as opposed to the 3-level scoring system.
Although both point systems did not have a Cronbach’s alpha that exceeded the generally accepted value of 0.7 as acceptable internal consistency,27 the 5-level system showed a moderate internal consistency (≥0.5) and the 3-level scoring system showed a poor internal consistency (<0.5).28 This supports the hypothesis that the 5-level scoring system would show higher internal consistency than the 3-level scoring system.
Findings from a previous study on the correlations between the MCS total score (3-level scoring) and TrA activation, hip strength, and FMS showed significant associations.16 However, linear regressions for the 3-level scoring system in the current study did not reveal significant association with TrA activation or hip strength, with the exception of internal rotators.16 In the present study, the model with the 3-level system as the dependent variable explained only 13.3% of the variance. In a previous model using the 3-level system, similar independent variables could explain only 10.8% of the variance.16 In the current study, it was found that 24% of the variance for the total MCS score using the 5-level system could be explained by the independent variables selected. These results are of particular interest because they show that the variance of the 5-level scoring system is explained in a greater proportion by components that have been identified as key to movement competency. This supports the assumption that the 5-level scoring system shows higher concurrent validity.
This study is not the first to reconsider the MCS scoring. Instead of using the common 3-level scoring for only the weaker side, Lee et al. used the 3-level scoring system for both sides and added up the points, giving a 6-level score for each task.17 The reasoning behind this choice is unfortunately not explained in the article. Considering both sides when evaluating each MCS item could lead to a higher score and to an overestimation of the athlete’s physical abilities when one side scores higher than the other. This method using the 3-level scoring system still presents the problem of grouping the five initial load levels. Results from the current study support the use of a 5-level scoring system to obtain more precise measurement of movement competency. Taking both sides into account when evaluating athletes could be considered; but to group this information in a total score could also mean overestimation of the athlete’s movement competency. Future research should consider the benefits and risks associated with an inflated movement competency score when considering both sides.
The main limitation of this study is the inclusion of dancers practicing various types of dance. Indeed, the inclusion of ballet and contemporary, as well as preprofessional and professional dancers could lead to increased heterogeneity in the dancers’ characteristics that are inherent to dance style and/or level of experience. The sample size could not allow analysis of these subgroups. However, this heterogeneity increased external validity.
CONCLUSION
The items scored with the 5-level system showed higher internal consistency of the test scores than with the 3-level system. Simple and multiple linear regressions used in the present technical note indicate that a 5-level system is more representative of the essential components of movement competency than the commonly used 3-level system because of its higher and more significant association with TrA activation, hip strength, and FMSTM score. For these reasons, health professionals and researchers should consider using the 5-level scoring system of the MCS in future clinical settings and research.
CONFLICTS OF INTEREST
The authors report no conflicts of interest.
Funding Statement
This study was funded by a partnership between the Institut de recherche Robert-Sauvé en santé et sécurité du travail (IRSST) and REPAR (03SNT007).
References
- A survey of injuries affecting pre-professional ballet dancers. Caine Dennis, Bergeron Glen, Goodwin Brett J., Thomas Jessica, Caine Caroline G., Steinfeld Sam, Dyck Kevin, André Suzanne. Sep 15;2016 Journal of Dance Medicine & Science. 20(3):115–126. doi: 10.12678/1089-313x.20.3.115. https://doi.org/10.12678/1089-313x.20.3.115 [DOI] [PubMed] [Google Scholar]
- Injuries in pre-professional ballet dancers: Incidence, characteristics and consequences. Ekegren Christina L., Quested Rachele, Brodrick Anna. May;2014 Journal Of Science And Medicine In Sport. 17(3):271–275. doi: 10.1016/j.jsams.2013.07.013. https://doi.org/10.1016/j.jsams.2013.07.013 [DOI] [PubMed] [Google Scholar]
- Potential predictors of injury among pre-professional ballet and contemporary dancers. Yau Rebecca K., Golightly Yvonne M., Richardson David B., Runfola Cristin D., Waller Anna E., Marshall Stephen W. Jun 15;2017 Journal of Dance Medicine & Science. 21(2):53–63. doi: 10.12678/1089-313x.21.2.53. https://doi.org/10.12678/1089-313x.21.2.53 [DOI] [PubMed] [Google Scholar]
- Psychological risk factors and outcomes of dance injury: a systematic review. Mainwaring Lynda M., Finney Caitlin. Sep 15;2017 Journal of Dance Medicine & Science. 21(3):87–96. doi: 10.12678/1089-313x.21.3.87. https://doi.org/10.12678/1089-313x.21.3.87 [DOI] [PubMed] [Google Scholar]
- Field-expedient screening and injury risk algorithm categories as predictors of noncontact lower extremity injury. Lehr M. E., Plisky P. J., Butler R. J., Fink M. L., Kiesel K. B., Underwood F. B. Mar 20;2013 Scandinavian Journal of Medicine & Science in Sports. 23(4):e225–e232. doi: 10.1111/sms.12062. https://doi.org/10.1111/sms.12062 [DOI] [PubMed] [Google Scholar]
- Altered lumbopelvic movement control but not generalized joint hypermobility is associated with increased injury in dancers. A prospective study. Roussel Nathalie Anne, Nijs Jo, Mottram Sarah, Van Moorsel Annouk, Truijen Steven, Stassijns Gaetane. Dec;2009 Manual Therapy. 14(6):630–635. doi: 10.1016/j.math.2008.12.004. https://doi.org/10.1016/j.math.2008.12.004 [DOI] [PubMed] [Google Scholar]
- Motor control and low back pain in dancers. Roussel N., De Kooning M., Schutt A., Mottram S., Truijen S., Nijs J., Daenen L. Feb;2013 International Journal of Sports Medicine. 34(2):138–143. doi: 10.1055/s-0032-1321722. [DOI] [PubMed] [Google Scholar]
- Morphology of the abdominal muscles in ballet dancers with and without low back pain: a magnetic resonance imaging study. Gildea Jan E., Hides Julie A., Hodges Paul W. Sep;2014 Journal of Science and Medicine in Sport. 17(5):452–456. doi: 10.1016/j.jsams.2013.09.002. https://doi.org/10.1016/j.jsams.2013.09.002 [DOI] [PubMed] [Google Scholar]
- The relationship between muscular strength and dance injuries: a systematic review. Moita João P, Nunes Alexandre, Esteves José, Oliveira Raul, Xarez Luis. Mar 1;2017 Medical Problems of Performing Artists. 32(1):40–50. doi: 10.21091/mppa.2017.1002. https://doi.org/10.21091/mppa.2017.1002 [DOI] [PubMed] [Google Scholar]
- Pre-participation screening: the use of fundamental movements as an assessment of function - part 1. Cook Gray, Burton Lee, Hoogenboom Barb. May;2006 North American journal of sports physical therapy: NAJSPT. 1(2):62–72. PMID: 21522216 PMCID: PMC2953313. [PMC free article] [PubMed] [Google Scholar]
- Proposed model to assess an athlete’s physical competency and capacity. Culhane PEter M. 2019Journal of Australien Strength and Conditioning. 27(7):38–61. [Google Scholar]
- The association between sport specialisation and movement competency in youth: a systematic review. Zoellner Anja, Whatman Chris, Read Paul, Sheerin Kelly. Mar 3;2021 International Journal of Sports Science & Coaching. 16(4):1045–1059. doi: 10.1177/1747954121998456. https://doi.org/10.1177/1747954121998456 [DOI] [Google Scholar]
- A musculoskeletal approach to the preparticipation physical examination. Preventing injury and improving performance. Kibler W.B., Chandler T. Jeff, Uhl Tim, Maddux Robin E. Jul;1989 The American Journal of Sports Medicine. 17(4):525–531. doi: 10.1177/036354658901700413. https://doi.org/10.1177/036354658901700413 [DOI] [PubMed] [Google Scholar]
- National athletic trainers’ association position statement: preparticipation physical examinations and disqualifying conditions. Conley Kevin M., Bolin Delmas J., Carek Peter J., Konin Jeff G., Neal Timothy L., Violette Danielle. Jan 1;2014 Journal of Athletic Training. 49(1):102–120. doi: 10.4085/1062-6050-48.6.05. https://doi.org/10.4085/1062-6050-48.6.05 [DOI] [PMC free article] [PubMed] [Google Scholar]
- The back squat: A proposed assessment of functional deficits and technical factors that limit performance. Myer Gregory D., Kushner Adam M., Brent Jensen L., Schoenfeld Brad J., Hugentobler Jason, Lloyd Rhodri S., Vermeil Al, Chu Donald A., Harbin Jason, McGill Stuart M. Dec;2014 Strength & Conditioning Journal. 36(6):4–27. doi: 10.1519/ssc.0000000000000103. https://doi.org/10.1519/ssc.0000000000000103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Does the Movement Competency Screen correlate with deep abdominals activation and hip strength for professional and pre-professional dancers? Benoît-Piau Justine, Morin Mélanie, Fortin Sylvie, Guptill Christine, Gaudreault Nathaly. Feb 1;2021 International Journal of Sports Physical Therapy. 16(1):31–40. doi: 10.26603/001c.18792. https://doi.org/10.26603/001c.18792 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Injury incidence, dance exposure and the use of the Movement Competency Screen (MCS) to identify variables associated with injury in full-time pre-professional dancers. Lee Linda, Reid Duncan, Cadwell Jill, Palmer Priya. Jun;2017 International Journal of Sports Physical Therapy. 12(3):352–370. PMID: 28593089 PMCID: PMC5455185. [PMC free article] [PubMed] [Google Scholar]
- Reliability, validity, and injury predictive value of the functional movement screen: a systematic review and meta-analysis. Bonazza Nicholas A., Smuin Dallas, Onks Cayce A., Silvis Matthew L., Dhawan Aman. 2017The American Journal of Sports Medicine. 45(3):725–732. doi: 10.1177/0363546516641937. https://doi.org/10.1177/0363546516641937 [DOI] [PubMed] [Google Scholar]
- Do Functional Movement Screen (FMS) composite scores predict subsequent injury? A systematic review with meta-analysis. Moran Robert W, Schneiders Anthony G, Mason Jesse, Sullivan S John. Mar 30;2017 British Journal Of Sports Medicine. 51(23):1661–1669. doi: 10.1136/bjsports-2016-096938. https://doi.org/10.1136/bjsports-2016-096938 [DOI] [PubMed] [Google Scholar]
- Functional Movement Screen normative values and validity in high school athletes: can the FMSTM be used as a predictor of injury? Bardenett Sean M., Micca Joseph J., DeNoyelles John T., Miller Susan D., Jenk Drew T., Brooks Gary S. Jun;2015 International Journal of Sports Physical Therapy. 10(3):303–308. PMID: 26075145 PMCID: PMC4458917. [PMC free article] [PubMed] [Google Scholar]
- Kritz Matthew. Development, reliability and effectiveness of the Movement Competency Screen (MCS) AUT University; Doctorate Thesis: [Google Scholar]
- Multicomponent musculoskeletal movement assessment tools: a systematic review and critical appraisal of their development and applicability to professional practice. Bennett Hunter, Davison Kade, Arnold John, Slattery Flynn, Martin Max, Norton Kevin. Oct;2017 Journal of Strength and Conditioning Research. 31(10):2903–2919. doi: 10.1519/jsc.0000000000002058. https://doi.org/10.1519/jsc.0000000000002058 [DOI] [PubMed] [Google Scholar]
- Reliability of ultrasound imaging measures of transverse abdominis and lumbar multifidus in various positions. Mangum L. Colby, Sutherlin Mark A., Saliba Susan A., Hart Joseph M. 2016PM&R. 8(4):340–347. doi: 10.1016/j.pmrj.2015.09.015. https://doi.org/10.1016/j.pmrj.2015.09.015 [DOI] [PubMed] [Google Scholar]
- Measurement of muscle contraction with ultrasound imaging. Hodges P.W., Pengel L.H.M., Herbert R.D., Gandevia S.C. May 19;2003 Muscle & Nerve. 27(6):682–692. doi: 10.1002/mus.10375. https://doi.org/10.1002/mus.10375 [DOI] [PubMed] [Google Scholar]
- Rehabilitative ultrasound imaging is a valid measure of trunk muscle size and activation during most isometric sub-maximal contractions: a systematic review. Koppenhaver Shane L., Hebert Jeffrey J., Parent Eric C., Fritz Julie M. 2009Australian Journal of Physiotherapy. 55(3):153–169. doi: 10.1016/s0004-9514(09)70076-5. https://doi.org/10.1016/s0004-9514(09)70076-5 [DOI] [PubMed] [Google Scholar]
- Effects of examiner strength on reliability of hip-strength testing using a handheld dynamometer. Krause David A., Neuger Mathew D., Lambert Kimberly A., Johnson Amanda E., DeVinny Heather A., Hollman John H. Feb;2014 Journal of Sport Rehabilitation. 23(1):56–64. doi: 10.1123/jsr.2012-0070. https://doi.org/10.1123/jsr.2012-0070 [DOI] [PubMed] [Google Scholar]
- Making sense of Cronbach's alpha. Tavakol Mohsen, Dennick Reg. Jun 27;2011 International Journal of Medical Education. 2:53–55. doi: 10.5116/ijme.4dfb.8dfd. https://doi.org/10.5116/ijme.4dfb.8dfd [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hinton Perry R., McMurray Isabella, Brownlow Charlotte. SPSS Explained; London ; New York. London ; New York: Routledge; [Google Scholar]