

Abstract
Background: Buerger's disease (thromboangiitis obliterans) may be a rare peripheral vascular disease that sometimes affects young male smokers. This study presents surgical treatment options for 315 Buerger's patients during a period of 18 years from 2002 to 2020.
Methods: In this cross-sectional study, 315 newly diagnosed Buerger patients in a period of 18 years (by Census sampling) were evaluated. Data included age, sex, cigarette smoking status, clinical presentation, the affected limb (right or left, upper or lower extremities), and the performed therapeutic procedures such as angiography of limb arteries, amputation, sympathectomy, and vascular bypass surgery, which were collected in a data sheet. Vascular reconstruction was done if there were suitable inflow and outflow arteries. Sympathectomy was performed for the patients who were unsuitable for revascularization. All analyzes were performed using SPSSV.18 software package (SPSS Inc., Chicago, IL). Data are presented as frequency, mean ± variance (SD).
Results: The mean age of patients was 42.6±9 years old, ranging from (26-75). There were 309 (98.1%) males and 6 (1.9%) females. The most common symptom was ulcer 252 (80%), and the most commonly involved arteries were the dorsal pedis (N=231; 73.4%) and posterior tibialis (N=225; 71.5%). Vascular bypass surgery, sympathectomy, and amputation were performed for patients who met surgical indications. Aortofemoral (N=9) and femoropopliteal (N=24) bypass procedures were done in 2.8% and 7.6% of patients respectively. Of nine patients who underwent aorto-femoral bypass procedure, 6 cases presented with leg claudication, 3 with an ulcer, and 3 with the Raynaud phenomenon. The digital loss rate was 9.6% (N=9) in toes and 1% (N=3) in fingers.
Conclusion: As most of the Buerger patients have multi arterial involvement, bypass surgery or sympathectomy can’t help treat these patients more than cigarette smoking or pharmaceutical therapy.
Keywords: Thromboangiitis Obliterans, Sympathectomy, Surgery, Amputation
↑What is “already known” in this topic:
Although the definitive cause is yet unknown, tobacco use seems to be a trigger for what appears to be an autoimmune mechanism in this group of patients.
→What this article adds:
The most common symptom in this survey is ulcers. Due to the low socioeconomic state of the patients, they would request treatment by delay. Surgery or sympathectomy can’t help treat these patients more than cigarette smoking or pharmaceutical therapy.
Introduction
Buerger's disease (thromboangiitis obliterans) may be a rare peripheral vascular disease that sometimes affects young male smokers. It is characterized by multiple occlusions distal to the knee and elbow (1). The disease is more prevalent in the Mediterranean, Middle East, and Asia (2). It is a relentless and devastating vasculitis causing significant loss of digits and limbs and is mor e commonly observed in males of age between 35 to 50 years (3). Disease characteristics and prognosis do not differ between males and females. In contrast to North America and Western Europe, the Mediterranean, the near and far East, and the Indian subcontinent are high prevalence regions (4). The incidence of Buerger's disease is high in the Iranian population, but there is not a nationwide epidemiological study in Iran. Surgical sympathectomy, amputation, and arterial plastic surgery are widely applied to Burger's patients. However, these approaches appear to be markedly changed recently and the number of the surgery have been declining (3-5). A systematic review published in the Cochrane database in 2016 declared in patients with chronic limb ischemia and poor chances of revascularization, as seen in many patients diagnosed with Buerger's disease, pharmacological treatment is given to improve the blood flow (perfusion) in the affected extremity (6). Sina Hospital, as a university hospital, is one of the referral centers known for vascular surgery in Iran. This study presents 315 Buerger patients during a period of 18 years from 2002 to 2020.
Methods
From March 2002 to March 2020, 315 newly diagnosed patients with ischemic limb symptoms caused by Buerger's disease were admitted to the Department of vascular surgery, Sina hospital of Tehran University of Medical Sciences. The diagnosis of Buerger's disease was made based on the clinical criteria proposed by Shionoya et al. 7 and has remained the same for 20 years: (1) onset of the symptoms before the age of 50 years, (2) smoking positive history of smoking, (3) infra popliteal arterial occlusive lesions, (4) either upper limb involvement or thrombophlebitis migrans, and (5) absence of atherosclerotic risk factors other than smoking. In this study, the exclusion criteria were collagen vascular disease, popliteal entrapment syndrome, cystic adventitial disease, hypercoagulable state, thoracic outlet syndrome, and atrial fibrillation. Infrapopliteal and upper limb arterial involvements had been determined by using arteriography and physical findings (e.g., Allen's test), respectively. Data included age, sex, cigarette smoking status, clinical presentation, the affected limb (right or left, upper or lower extremities), and the performed therapeutic procedures such as angiography of limb arteries, amputation, sympathectomy, and vascular bypass surgery collected in a data sheet.
The patients with critical ischemic complaints such as rest pain, non-healing ulcer, and gangrene without popliteal artery pulse underwent arteriography to find a suitable segment for arterial revascularization. Vascular reconstruction was performed if there were suitable inflow and outflow arteries. Sympathectomy was performed for patients who were unsuitable for revascularization when there were limited ischemia complaints such as rest pain and non-healing ulcers without infection. Ethics approval and consent to participate: This study was approved by the ethics committee of Tehran University of Medical Sciences (No: 19785) and a written consent form was obtained from all the participants. All analyzes were performed using SPSSV.18 software package (SPSS Inc., Chicago, IL). Data are presented as frequency, mean ± variance (SD).
Results
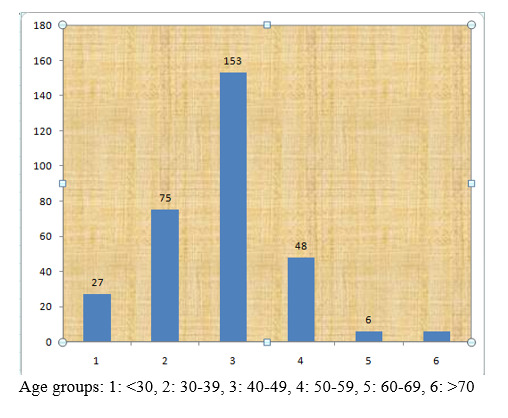
Between March 2002 to March 2020, 315 newly diagnosed patients with Buerger’s disease who were admitted for vascular intervention in Sina Hospital, Tehran University of Medical Sciences (TUMS) were enrolled in this study. There were 309 (98.1%) males and 6 (1.9%) females. The mean age of patients was 42.69±9.09 (Figure 1). The mean age of females and males was 49.00±5.47 and 42.54±9.11 years, respectively.
Figure 1.
Buerger’s disease distribution
The mean smoking pack/year was 18.22±11.68. Angiography was performed in 141 (44.8%) patients. The most common symptom in men was an ulcer, 252(80%), and all six females experienced paresthesia (100%). Calf and thigh claudication were observed in all the females. Table 1 shows the frequency of patients’ symptoms.
Table 1. Frequency of patients’ symptoms.
| Symptom | Frequency | Percent |
|---|---|---|
| Ulcer | 252 | 80 |
| Rest pain | 225 | 71.4 |
| Gangrene | 219 | 69.5 |
| Paresthesia | 210 | 66.7 |
| Leg claudication | 195 | 61.9 |
| Calf claudication | 177 | 56.2 |
| Raynaud | 81 | 25.7 |
| Migratory Phlebitis | 24 | 7.6 |
The most common involved artery in men was the dorsal pedis artery (73.4%) (Table 2). There was no upper extremity involvement in women, and all six female patients had bilateral lower extremity involvement.
Table 2. Diseased arteries in Buerger’s patients.
| Diseased Artery | % | N |
|---|---|---|
| Dorsal Pedis | 73.4% | 231 |
| Posterior Tibialis | 71.5% | 225 |
| Popliteal | 33.3% | 104 |
| Ulnar | 11.5% | 36 |
| Radial | 11.4% | 35 |
| Femoral | 3.8% | 12 |
| Anterior tibialis | 3.8% | 12 |
Vascular bypass surgery, sympathectomy, and amputation were performed for patients according to the criteria described in the methods. Aortofemoral and femoropopliteal bypass procedures were done in 7.6% of patients.
Three above-knee, 27 below-knee, nine trans-metatarsal, and 33 digital amputations were carried out in the entire series, with a limb salvage rate of 90.4 % (Table 3). Of nine patients who underwent an aortofemoral bypass procedure, six cases presented with leg claudication, three with an ulcer, and three with the Raynaud phenomenon. Threetoe amputations happened in patients after femoropopliteal bypass surgery.
Table 3. Different Procedures in Buerger's patients.
| Bypass surgery | Frequency (%) | N |
|---|---|---|
| Vascular surgery bypass | (13.3%) | 42 |
| Aortofemoral | (2.8%) | 9 |
| Femoropopliteal | (7.6%) | 24 |
| Femoroproneal | (1.9%) | 6 |
| Femoroanteriortibialis | (1%) | 3 |
| Femoroposteriortibialis | - | - |
| Sympathectomy | (49.5%) | 156 |
| Lumbar | (36.1%) | 114 |
| Thoracic | (13.3%) | 42 |
| Amputation | (22.8%) | 72 |
| Toe | (9.6%) | 30 |
| Transmetatarsal | (2.9%) | 9 |
| Below knee | (8.6%) | 27 |
| Above knee | (1%) | 3 |
| Finger | (1%) | 3 |
The mean duration of migratory phlebitis, Raynaud, and calf claudication was 42 (±30.53), 35 (±29.53), and 24 (±20.58) days, respectively. Right, and left upper extremity involvement was observed in 69 (21.9%) and 57 (18.1%) patients, respectively. While there were 210 (66.7%) and 204 (64.8%) right and left lower extremity involvement. 213 patients (67.6%) had more than one arterial involvement.
Discussion
In this study, the mean age of patients was 42.6±9, which was similar to previous studies (3-8). There is an upward trend of Buerger's disease in women, which is attributable to the increased number of female smokers in the past few decades. Accordingly, six females were observed in this study. Also, it is an increase compared to the previous large study in Iran, where all the patients were men (9).
Although the definitive cause is yet unknown, tobacco use seems to be a trigger for what appears to be an autoimmune mechanism in a group of patients, and there was a seasonal variation with most cases admitted during winter for admission with winter being significantly the most common (9, 10).
Buerger’s disease typically occurs in patients with a low social status. Some authors even described a Buerger-type personality with manipulative and auto-aggressive tendencies often matched with denial, negligence, or tendencies to minimize their illness, while others even presumed typical morphological characteristics (4). In this study, most of the patients presented with ulcers and they may sought medical help by the delay because of their low socio-economical status.
In this survey, the most common presentations were ulcer (80%), rest pain (71.4%), and gangrene (69.5%). There were 25.7% Raynaud's phenomenon and 7.6% thrombophlebitis in this study. In a Similar study in Iran, Raynaud’s phenomenon and thrombophlebitis were reported at 8.7% and 2.5%, respectively (3). In Cleveland Clinic, during 1970-1978, 76% suffered from ischemic ulcers,44% revealedRaynaud‘s phenomenon and 38% had thrombophlebitis (11).
In a study that investigated the short-term outcomes of sympathectomy, it was found that marked improvement, in general, was predicted in 60% of total patients who received it. Twenty-five percent of patients responded as improved in symptoms, 13% were unchanged but only 1.5% of patients exhibited aggravation. It was noted that even the advanced and aggravated symptom such as rest pain and ulcer formation pretty well responded to this treatment (5).
In a systematic review published in 1990, sympathectomy was evaluated as one of the oldest treatments for patients with Buerger’s disease in critical limb ischemia. The main evidence found in this study refers to the greater effectiveness of iloprost (prostacyclin analog) in comparison to the lumbar sympathectomy on the healing of ischaemic ulcers and pain at rest (11). In Iran, iloprost is not easily accessible due to sanctions thus, it can’t be prescribed for Buerger’s patients.
Although smoking is a trigger to exhibit Beurger’s symptoms, abnormal microcirculation, systemic factors (hormonal or immune logical), the interaction between the coagulation system proteins and vascular endothelium may be involved in Buerger’s disease. 3Therefore TAO improvement in the absence of a history of smoking can be explained as there were ten patients (3.1%) without a positive history of smoking.
In this study, the amputation rate was 22.8% which is similar to Sasaki (25.2%) and Olin (27%) studies (10, 11).
The digital loss was seen at 9.6% in toes and 1% in fingers, which compromised half (46%) of the limb loss cases in the studied patients, compared to one-third of all amputations in the Cleveland clinic (11).
There has been a marked shift in treatment courses from the surgical approach to medical pharmaceutical therapy (5, 6). Prostaglandin, sympathetic ganglion blockage technique, and sympathectomy under endoscopic guidance may be the reasons for declining surgical procedures (5).
The main limitation of this study is the lack of follow-up, which is crucial for evaluating the short- and long-term outcomes of the therapy. Future studies should be designed to compare sympathectomy versus drugs such as iloprost, cilostazol, pentoxifylline, clopidogrel, and other therapeutic options (use of stem cells, omental transplantation, foot venous arch arterialization, acupuncture (6).
Conclusion
As most of the Buerger patients have multi arterial involvement, bypass surgery or sympathectomy can’t help treat these patients more than cigarette smoking or pharmaceutical therapy.
Consent for publication
The patients provided written informed consent for publication.
Availability of data and materials.
Patients data are available in the electronic database of Sina Hospital of Tehran University of Medical sciences
Conflict of Interests
The authors declare that they have no competing interests.
Cite this article as : Salimi J, Cheraghali R, Omrani Z, Farshidmehr P, Afghani R. Surgical Treatment Options for Buerger's Disease (Experience with 315 Cases in Iran). Med J Islam Repub Iran. 2022 (14 Nov);36:134. https://doi.org/10.47176/mjiri.36.134
References
- 1.Sayin A, Bozkurt AK, Tüzün H, Vural FS, Erdog G, Ozer M. Surgical treatment of Buerger's disease: experience with 216 patients. Cardiovasc Surg. 1993 Aug:377. doi: 10.1177/096721099300100412. [DOI] [PubMed]
- 2.Ates A, Yekeler I, Ceviz M, Erkut B, Pac M, Basoglu A. et al. One of the most frequent vascular diseases in northeastern of Turkey: Thromboangiitis obliterans or Buerger's disease (experience with 344 cases) Int J Cardiol. 2006 Jul 28:147. doi: 10.1016/j.ijcard.2005.12.002. [DOI] [PubMed]
- 3.Salami J, Zafarghandi MR, Khashayar P. Buerger’s disease in Tehran university of medical sciences hospitals: A fifteen years study. Acta Med Iran. 2009
- 4.Klein-Weigel P, Volz TS, Zange L, Richter J. Buerger's disease: providing integrated care. J Multidiscip Healthc. 2016 doi: 10.2147/JMDH.S109985. [DOI] [PMC free article] [PubMed]
- 5.Nakajima N. The change in concept and surgical treatment on Buerger's disease--personal experience and review. Int J Cardiol. 1998 Oct 1 doi: 10.1016/s0167-5273(98)00179-x. [DOI] [PubMed]
- 6.Cacione DG, Macedo CR, Baptista-Silva JC. Pharmacological treatment for Buerger's disease. Cochrane Database Syst Rev. 2016:CD011033. doi: 10.1002/14651858.CD011033.pub3. [DOI] [PMC free article] [PubMed]
- 7.Shionoya S. Surgical treatment. In: Shionoya S, editor. Buerger’s disease
- 8.Bozkurt AK, Beşirli K, Köksal C, Sirin G, Yüceyar L, Tüzün H. et al. Surgical treatment of Buerger's disease. Vascular. 2004 May-Jun:192. doi: 10.1258/rsmvasc.12.3.192. [DOI] [PubMed]
- 9.Tavakoli H, Rezaii J, Esfandiari K, Salimi J, Rashidi A. Buerger's disease: a 10-year experience in Tehran, Iran. Clin Rheumatol. 2008 Mar:369. doi: 10.1007/s10067-007-0784-x. [DOI] [PubMed]
- 10.Sasaki S, Sakuma M, Yasuda K. Current status of thromboangiitis obliterans (Buerger's disease) in Japan. Int J Cardiol. 2000 doi: 10.1016/s0167-5273(00)00190-x. [DOI] [PubMed]
- 11.Olin JW, Young JR, Graor RA, Ruschhaupt WF, Bartholomew JR. The changing clinical spectrum of thromboangiitis obliterans (Buerger’s disease) Circulation. 1990:IV3. [PubMed]