

Abstract
Purpose:
To retrospectively evaluate the treatment outcomes of thermal ablation for renal metastatic tumors.
Materials and Methods:
Thirteen consecutive patients with small renal metastatic tumors (≤3 cm), who underwent thermal ablation between 2009 and 2020, were included in this study. Eight patients had extra-renal tumors during renal ablation. The primary tumors were adenoid cystic carcinoma in four patients, lung cancer in three, hemangiopericytoma in three, leiomyosarcoma in two, and thyroid cancer in one. The therapeutic effects, safety, survival rate, prognostic factor, and renal function were evaluated.
Results:
We performed 18 ablation sessions (cryoablation, n = 13; radiofrequency ablation, n = 5) on 19 renal metastases with a mean diameter of 1.7 cm, which resulted in a primary technique efficacy rate of 100% without procedure-related deaths or major complications. Renal function significantly declined 6 months after ablation (P = 0.0039). During the mean follow-up period of 31.2 ± 22.4 months (range, 2.7-71.4 months), one patient had local tumor progression at 11.9 months following radiofrequency ablation. The overall survival rates at 1 and 3 years after ablation were 76.9% (95% confidence interval [CI], 54.0%-99.8%) and 59.3% (95% CI, 31.3%-87.3%), respectively. Tumor size ≥ 2 cm (P = 0.02) and metastasis from non-small cell lung cancer (P = 0.001) were significant worse prognostic factors in univariate analysis, and metastasis from non-small cell lung cancer (P = 0.01) was significant in multivariate analysis.
Conclusions:
Percutaneous thermal ablation for small renal metastases is safe and feasible and can control local tumors.
Keywords: renal metastasis, radiofrequency ablation, cryoablation
Introduction
Advances in cancer treatment, including systemic chemotherapy, have prolonged the prognosis of patients with malignant tumors; however, multi-organ metastases and multiple primary malignancies can occur during their survival [1]. Renal metastases are neither common nor rare and are the twelfth most frequent to occur with a reported frequency of 7%-12.6% [2-4]. Furthermore, improvements in imaging modalities and the widespread use of cross-sectional imaging have enabled more frequent detection of small renal masses [5, 6]. Renal cell carcinoma, as a second primary cancer concurrent with the first primary cancer, has been detected 4.5 times more commonly than renal metastases [7]. Additionally, previous reports have demonstrated that renal metastases are typically only radiologically detected as small masses [4, 5]. Caution must be exercised when diagnosing new renal masses in patients with cancer. Tumor biopsy is also crucial for diagnosing small renal masses [8-12].
For renal metastases, lung cancer; breast cancer; tumors of the gastrointestinal, genitourinary, and gynecologic tracts; and melanoma are known primary lesions of metastatic renal tumors [2-4]. However, reports on the local treatment of renal metastases are scarce, and surgical treatment of renal metastases can be beneficial for patients with limited tumor burden, such as isolated renal metastases and oligometastases [13, 14]. However, indications for the local treatment of renal metastases have not been established.
Thermal ablation, either as cryoablation (CA) or radiofrequency (RF) ablation, is an established approach for the local treatment of small primary renal tumors in patients who cannot undergo surgery [8,15-20]. Because renal metastasis is associated with systemic disseminated cancer in most cases [3, 4, 21], minimally invasive local treatment using thermal ablation represents an attractive alternative. Hence, the treatment outcomes of thermal ablation for metastatic renal tumors were retrospectively evaluated in this study.
Material and Methods
Study design and patients
This study was approved by our institutional review board, and informed consent was obtained for data usage in this retrospective study. Additionally, informed consent was obtained from all patients undergoing tumor biopsy and thermal ablation.
The indication for the thermal ablation for renal metastases was determined after multidisciplinary discussion with interventional radiologists, medical and radiation oncologists, and urologists. Thermal ablation was performed on patients who were not suitable candidates for surgical resection or those who declined to undergo surgical treatment. All patients included in this study (13/13) declined surgical treatment and preferred thermal ablation. The inclusion criteria were (i) patients who had one or two renal metastatic tumors measuring ≤3 cm, (ii) patients without extra-renal tumor or with extra-renal tumors that did not significantly increase in size on serial computed tomography (CT) scans taken 3-4 months before the initial thermal ablation, (iii) patients with Eastern Cooperative Oncology Group performance status of 0 or 1, and (iv) patients with a life expectancy of 6 months or longer.
Between January 2009 and December 2020, 683 consecutive patients underwent thermal ablation for renal tumors in our institute. Of these patients, 13 (1.9%, 13/683) with 19 metastatic renal tumors (1.46 tumors/patient) were included in this retrospective study. The patient demographics and tumor characteristics of this study are presented in Table 1. The study included 6 men and 7 women with a mean age of 54.0 ± 12.1 years (mean ± standard deviation [SD]; range, 36-75 years). The primary sites of renal metastases were salivary gland in 4 (30.8%, 4/13), meningeal mesenchyme in 3 (23.1%, 3/13), lung in 3 (23.1%, 3/13), and thyroid gland, omental bursa, and extremity in 1 each (7.7%, 1/13). Pathological diagnoses of these primary tumors were adenoid cystic carcinoma (ACC) in 4 (30.8%, 4/13), hemangiopericytoma in 3 (23.1%, 3/13), non-small cell lung cancer (NSCLC) in 3 (23.1%, 3/13), leiomyosarcoma in 2 (15.4%, 2/13), and follicular thyroid cancer in 1 patient (7.7%, 1/13). The median period from primary tumor diagnosis to renal ablation was 66.4 months (25%-75% quartile range [QR]: 29.9-107.5 months). All patients (100%, 13/13 patients) had a history of extra-renal tumors before renal ablation. At the time of the initial renal ablation, eight patients (61.5%, 8/13 patients) had extra-renal tumors in the lung (61.5%, 8/13, and ≤30 mm in diameter), liver (7.7%, 1/13, and multiple tumors ≤ 6 mm in diameter), bone (7.7%, 1/13, and 14 mm in diameter), and retroperitoneum (7.7%, 1/13, and 10 mm in diameter). All extra-renal tumors were smaller than the metastatic renal tumors except for the bone metastasis in one patient. For the bone metastasis of this patient, radiation therapy with curative intent had planned, thus, locoregional therapy of renal ablation was planned for renal metastatic tumor (10 mm in diameter). Ten patients (76.9%, 10/13) had a total number of systemic metastases ≤ 5 at the time of initial renal ablation. No patient had undergone local renal treatment, including radical or partial nephrectomy or radiation therapy before thermal ablation. At the time of initial thermal ablation for the renal metastases, primary tumors had been resected (n = 12, 92.3%, and 12/13) or treated with radiation therapy (n = 1, 7.7%, and 1/13). Five patients (38.5%, 5/13) had two renal tumors before the initial renal ablation. Of the five patients, one had two renal tumors treated in a single session of RF ablation, but this patient developed another renal metastasis, which was also treated with RF ablation. In the remaining four patients, single tumor was ablated in each session. Thus, thermal ablation was performed for 19 renal metastases, and five patients received two sessions of renal ablation.
Table 1.
Patient and Tumor Demographics.
| Characteristics | |||||
|---|---|---|---|---|---|
| Patient characteristics | |||||
| No. of patients | n = 13 | ||||
| Gender | |||||
| Male | 6 (46.2%) | ||||
| Female | 7 (53.8%) | ||||
| Age (years) | |||||
| Mean ± SD | 54.0 ± 12.1 | ||||
| <55 | 7 (53.8%) | ||||
| ≥55 | 6 (46.2%) | ||||
| History of extra-renal tumor | |||||
| Yes | 13 (100%) | ||||
| No | 0 (0%) | ||||
| Previous local renal treatment | |||||
| Yes | 0 (0%) | ||||
| No | 13 (100%) | ||||
| Previous chemotherapy | |||||
| Yes | 4 (30.8%) | ||||
| No | 9 (69.2%) | ||||
| Renal tumor number | |||||
| Single | 8 (61.5%) | ||||
| Multiple | 5 (38.5%) | ||||
| Extra-renal tumor at the time of initial ablation | |||||
| Yes | 8 (61.5%) | ||||
| No | 5 (38.5%) | ||||
| Total no. of systemic metastatic tumor | |||||
| 5 or less | 10 (76.9%) | ||||
| 6 or more | 3 (23.1%) | ||||
| Tumor origin | |||||
| Organ | Pathology | ||||
| Salivary gland | ACC | 4 (30.8%) | |||
| Lung | NSCLC | 3 (23.1%) | |||
| Meningeal mesenchyme | Hemangiopericytoma | 3 (23.1%) | |||
| Omental bursa, Extremity | Leiomyosarcoma | 2 (15.4%) | |||
| Thyroid gland | Follicular thyroid cancer | 1 (7.7%) | |||
| Tumor characteristics | |||||
| No. of renal tumors | n = 19 | ||||
| Maximum tumor size (cm) | |||||
| Mean ± SD | 1.7 ± 0.6 | ||||
| Range | 0.7–3.0 | ||||
| No. of the tumors <2 cm | 14 (73.7%) | ||||
| No. of the tumors ≥2 cm | 5 (26.3%) | ||||
| Location | |||||
| Right | 13 (68.4%) | ||||
| Left | 6 (36.2%) | ||||
| Type of thermal ablation | |||||
| Cryoablation | 14 (73.7%) | ||||
| RF ablation | 5 (26.3%) | ||||
Data are number of patients or tumors, with percentages in parentheses. No, number; SD, standard deviation; ACC, adenoid cystic carcinoma; NSCLC, non-small cell lung cancer; RF, radiofrequency.
Systemic chemotherapy for renal metastases was administered to four patients (30.8%, 4/13) before thermal ablation; specifically, while carboplatin (Sandoz K.K., Tokyo, Japan) and paclitaxel (Nippon Kayaku Co., Ltd., Tokyo, Japan) were prescribed to one patient with ACC and two patients with lung cancer, cisplatin (Nichi-Iko Pharmaceutical Co., Ltd., Toyama, Japan) and 5-fluorouracil (Fluorouracil; Kyowa Kirin Co., Ltd., Tokyo, Japan) were administered to another patient with ACC. Of these four patients who underwent thermal ablation, two developed renal metastases 1 and 9 years after systemic chemotherapy, whereas the other two developed renal metastases during chemotherapy.
Pretreatment work-up
Before thermal ablation, routine physical examination; blood tests (blood count, blood biochemistry; coagulation fibrinolysis examination); and CT of the chest, abdomen, and pelvis, with and without contrast material, were performed. Renal metastases were diagnosed predominantly based on radiological findings, i.e., renal metastases were defined as emerging renal masses in patients with malignant neoplasms, which increased in size on CT scans obtained every 3-4 months. All patients (100%, 13/13) underwent CT scans with intravenous contrast material in the early and delayed phases. In seven patients (53.8%, 7/13), magnetic resonance (MR) images were also obtained with intravenous contrast material in the early and delayed phases before renal thermal ablation. Percutaneous biopsy of the renal tumor was performed in all patients (100%, 13/13) suspected of renal metastasis based on radiological findings. Metastatic renal tumor was pathologically confirmed in 12 patients (92.3%, 12/13). In one patient with leiomyosarcoma (7.7%, 1/13), the renal tumor was biopsied immediately after CA and resulted in a non-diagnostic result.
Thermal ablation for renal metastases
Two interventional radiologists with approximately 13 and 14 years of experience in interventional oncology, respectively, performed all thermal ablation procedures. The procedures were executed under the guidance of real-time CT fluoroscopy (Aquilion ONE, Canon Medical Systems Corporation, Otawara, Japan) and conscious sedation. Puncture sites and access routes for the ablation needles were determined based on reference images obtained using contrast-enhanced CT or MR. For local anesthesia, lidocaine (Xylocaine; Astellas Pharma Inc., Tokyo, Japan) was used. For analgesia, fentanyl (Fentanest; Janssen-Kyowa, Tokyo, Japan) at a dose of 0.1-0.2 mg was administered during RF ablation.
CA was performed using Cryoprobes of IceSeed or IceRod (Galil Medical Ltd., Israel) with a gas-based cryoablation system (CryoHit, Galil Medical Ltd., Israel). The freeze-thaw cycle numbers required to cover the renal tumor with an ice-ball margin of 6 mm or more were 2 ± 0.26 (mean ± SD; range, 2-3 cycles) [22].
For RF ablation, 17-gauge internally cooled electrodes (Cool-tip RF Ablation System; Medtronic, Minneapolis, MN) were used. With an impedance control algorithm, RF energy was applied using a generator (Cool-tip RF generator or Cool-tip RF Ablation System E-series; Medtronic, Minneapolis, Minnesota) for 10-12 min.
Complications
Procedure-related complications were evaluated based on the Society of Interventional Radiology grading [23]; specifically, major complications (classes C-E) were defined as adverse events leading to substantial morbidity, disability, or an increased level of care, requiring hospitalization or a substantially lengthened hospital stay, whereas all other complications were defined as minor complications (class A/B).
Follow-up
Two interventional radiologists followed up treated patients for a median period of 24.3 months (range, 2.7-71.4 months). Contrast-enhanced CT or MR images of the early and delayed phases were obtained in 12 patients (92.3%, 12/13) within 1 week following thermal renal ablation, and 1 patient (7.7%, 1/13) underwent plain CT within 1 week after ablation due to decreased renal function. Abdominal CT or MR image evaluations, with and/or without contrast enhancement, and routine physical examination and blood tests, including an estimated glomerular filtration rate (eGFR), were completed within 1 week following thermal ablation and repeated every 3-4 months thereafter. Two diagnostic radiologists interpreted the CT or MR images, and eGFR was derived using the abbreviated equation developed from the Modification of Diet in Renal Disease Study [24].
Complete coverage of the renal tumor by the ablative zone with no signs of residual tumor after the initial procedure was defined as technique efficacy [25]. The development of tumor foci at the edge of the ablated zone despite technical efficacy evident on follow-up CT or MR images was defined as local tumor progression [25]. Distant tumor recurrence was defined as the emergence of new tumors in the untreated renal parenchyma or extra-renal regions. Progression-free survival was defined as the period from renal thermal ablation to local tumor progression, new distant recurrence, or a ≥20% increase in the size of remaining tumors. The pretreatment glomerular filtration rate (GFR) and GFR at 6 months after ablation were compared. In five patients (38.5%, 5/13) in whom two sessions of renal ablation were required, the GFR at 6 months after the last ablation was compared with the pretreatment GFR. Follow-up was completed at the time of death or at the last visit of the patient until June 2021.
Statistical analyses
Categorical and continuous variables are expressed as frequencies and percentages and means and SD, respectively. Student's t-test was applied to evaluate the differences in the continuous variables. The chi-squared test was applied to evaluate the differences between the categorical variables. The Kaplan-Meier method was employed to evaluate local tumor progression and overall and progression-free survival rates. Univariate and multivariate Cox proportional hazards regression models were used to evaluate the factors affecting the overall and recurrence-free survival. IBM SPSS statistics 25 (IBM Co. Armonk, NY, USA) was used for all statistical analyses. A P-value < 0.05 was regarded as significant.
Results
Initial therapeutic results
Eighteen ablation sessions were performed on nineteen metastatic renal tumors (1.05 tumors per session). The maximum tumor diameter was 1.7 ± 0.6 cm (mean ± SD; range, 0.7-3 cm). Before the introduction of CA in April 2012, RF ablation was applied to all thermal ablations. After May 2012, all metastatic renal tumors were ablated using CA. Of the 19 tumors, 14 (73.7%, 14/19) were detected in 10 patients (76.9%, 10/13) and were treated with CA; the remaining 5 (26.3%, 5/19) were detected in 4 patients (30.8%, 4/13) and were subjected to RF ablation. The needles for CA and RF ablation were positioned at the planned sites for each renal tumor, and thermal ablation was performed with a planned protocol in all tumors. Eight sessions (42.1%, 8/19) of hydrodissection were performed to dislocate the heat-sensitive critical organs. Technical success was achieved in all tumors (technical success rate, 100%; 19/19 tumors), all renal metastases were ablated with a sufficient margin, and the primary technique efficacy rate was 100% (19/19 tumors).
Adverse Events and changes in renal function
No procedure-related deaths or major complications were recorded in any session. Minor complications, such as self-limiting retroperitoneal hematomas (class A adverse event), developed after nine thermal ablation sessions (50.0%, 9/18 sessions), seven CA sessions (53.8%, 7/13 sessions), and two RF ablation sessions (40.0%, 2/5 sessions).
Five patients (38.5%, 5/13) underwent two sessions of renal ablation for multiple renal tumors, 6 days to 1 year apart, and the renal function data at 6 months after the last renal ablation was available for 11 patients (84.6%, 11/13). The pretreatment mean eGFR for these patients was 86.4 ± 27.0 mL/min/1.73 m2 (range: 34.6-128.3 mL/min/1.73 m2), and the eGFR decreased by 10.7 ± 9.6 mL/min/1.73 m2 (range: −3.6 to 29.7 mL/min/1.73 m2) to 75.7 ± 25.5 mL/min/1.73 m2 (range: 15.2-101.3 mL/min/1.73 m2) by 6 months after the last ablation. The percentage reduction in eGFR was 14.1% ± 16.4% (range: −5.0% to 56.1%). Thus, the eGFR significantly decreased by 6 months after the last thermal ablation (P = 0.0039) (Fig. 1). The chronic kidney disease (CKD) classification based on eGFR [26] led to nine patients (81.8%, 9/11) remaining in CKD stage 1 or 2 and one patient each (9.1%, 1/11) progressing from stages 2 to 3a and from stages 3b to 4 by 6 months after the last ablation.
Figure 1.

Changes in renal function before and 6 months after thermal ablation. The mean eGFR was 86.4 ± 27.0 mL/min/1.73 m2 (range: 34.6–128.3 mL/min/1.73 m2), and eGFR decreased significantly to 75.7 ± 25.5 mL/min/1.73 m2 (range: 15.2–101.3 mL/min/1.73 m2) at 6 months after thermal ablation.
Tumor progression and survival
During follow-up (median: 24.3 months; range: 2.7-71.4 months), 12 patients (92.3%, 12/13) were followed with contrast-enhanced CT or MR images, and one patient with reduced renal function (7.7%, 1/13) was followed with CT and MR images without contrast enhancement. One patient (7.7%, 1/13) had local tumor progression 11.9 months after RF ablation; the primary cancer was NSCLC. Because of systemic tumor dissemination, repeat thermal ablation was not recommended for treating locally progressing renal tumor. The local tumor control rates were 93.3% (95% CI, 80.7%-100%) at 1, 3, and 5 years (Fig. 2). The distant tumor recurrence following renal ablation was 92.3% (12/13 patients), with lesions in the lung (53.8%, 7/13 patients), liver (23.1%, 3/13 patients), and bone (30.8%, 4/13 patients). The progression-free survival rate was 7.7% (95% CI, 0%-22.2%) at 1 and 3 years (Fig. 3).
Figure 2.
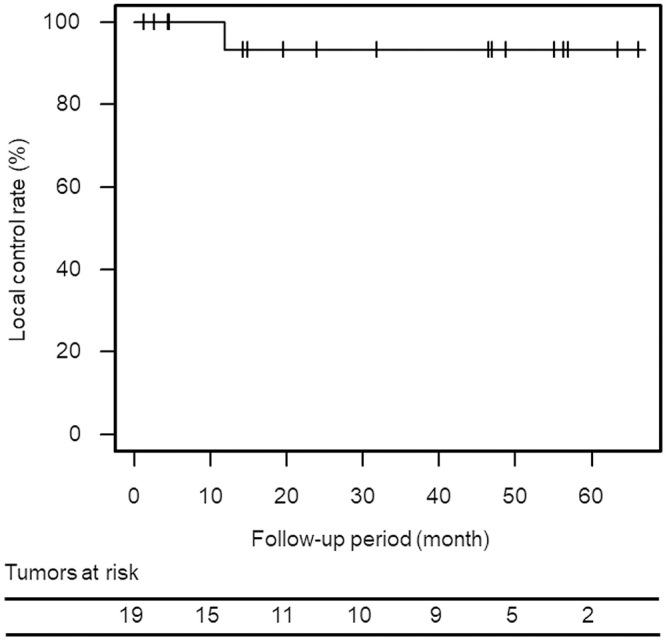
Kaplan–Meier curve of the local tumor control rate after thermal ablation for renal metastasis. The local tumor control rate was 93.3% (95% confidence interval [CI], 80.7%–100%) at 1, 3, and 5 years.
Figure 3.

Kaplan–Meier curve of progression-free survival after the initial thermal ablation for renal metastasis. The progression-free survival rate was 7.7% (95% confidence interval [CI], 0%–22.2%) at 1 and 3 years.
Furthermore, 9 of the 13 patients died (69.2%, 9/13 patients) during follow-up, and the cause of death was tumor progression (61.5%, 8/13) or pneumonia (7.7%, 1/13). The median survival time after thermal ablation was 24.3 months (25%-75% QR; 12.5-49.1 months). The overall survival rates at 1 and 3 years after the initial renal ablation were 76.9% (95% CI, 54.0%-99.8%) and 59.3% (95% CI, 31.3%-87.3%), respectively (Fig. 4). The prognosis of treated patients based on tumor origin is presented in Table 2. The median survival times after thermal ablation in patients with ACC, hemangiopericytoma, NSCLC, and leiomyosarcoma were 18.1, 57.3, 4.7, and 51.9 months, respectively, whereas those after the initial primary tumor diagnosis in patients with ACC, hemangiopericytoma, NSCLC, and leiomyosarcoma were 59.0, 230.9, 10.8, and 78.9 months, respectively.
Figure 4.
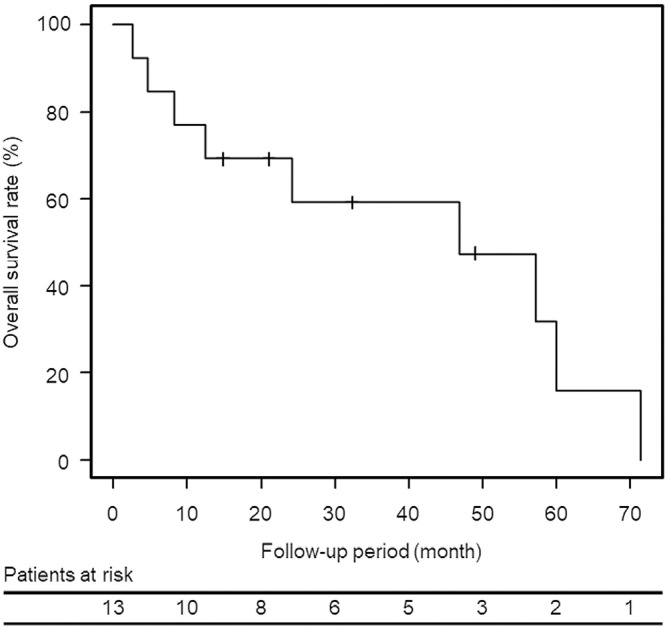
Kaplan–Meier curve of overall survival after the initial thermal ablation for renal metastasis. The median survival time was 24.3 months. The overall survival rates after renal ablation were 76.9% (95% confidence interval [CI], 54.0%–99.8%) and 59.3% (95% CI, 31.3%–87.3%) at 1 and 3 years, respectively.
Table 2.
Patient Prognosis According to Tumor Origin.
| Tumor origin | No. of patients | MST after renal thermal ablation (mo) | MST from the initial diagnosis of tumor origin (mo) |
|---|---|---|---|
| Adenoid cystic carcinoma | 4 (30.8%) | 18.1 | 59.0 |
| NSCLC | 3 (23.1%) | 4.7 | 10.8 |
| Hemangiopericytoma | 3 (23.1%) | 57.3 | 230.9 |
| Leiomyosarcoma | 2 (15.4%) | 51.9 | 78.9 |
No, number; mo, months; MST, median survival time; and NSCLC, non-small cell lung cancer.
Univariate analysis was conducted using the factors listed in Table 1; of these, the history of extra-renal tumor and previous local renal treatment was excluded because one side was 100%. Factors, such as tumor location and type of thermal ablation, were also excluded because both kidneys were affected in three patients and one underwent CA and RF ablation. Tumor size (P = 0.02) and NSCLC metastasis (P = 0.001) were significant factors for a worse prognosis during univariate analysis (Table 3). In the multivariate analysis, NSCLC metastasis (P = 0.01; hazard ratio: 19.6; 95% CI: 2.0-196.2) was a significant independent factor that affected the overall survival. No significant prognostic factors affected the progression-free survival rates.
Table 3.
Univariate Analysis of Variables Relevant to Overall Survival.
| Variable | n (%) | Overall survival rate (%) | MST
(mo) |
P value | |||
|---|---|---|---|---|---|---|---|
| 1-year | 3-years | 5-years | |||||
| Gender | |||||||
| Male | 6 (46.2%) | 83.3% (95% CI, 53.5%–100%) | 83.3% (95% CI, 53.5%–100%) | 31.3% (95% CI, 0%–79.3%) | 48.0 | 0.29 | |
| Female | 7 (53.8%) | 71.4% (95% CI, 38.0%–100%) | 38.1% (95% CI, 0%–77.2%) | 38.1% (95% CI, 0%–77.2%) | 21.1 | ||
| Age (years) | |||||||
| <55 | 7 (53.8%) | 85.7% (95% CI, 59.8%–100%) | 64.3% (95% CI, 23.1%–100%) | - | 24.3 | 0.79 | |
| ≥55 | 6 (46.2%) | 66.7% (95% CI, 29.1%–100%) | 50.0% (95% CI, 10.0%–90.0%) | 50.0% (95% CI, 10.0%–90.0%) | 30.8 | ||
| Previous chemotherapy | |||||||
| Yes | 4 (30.8%) | 75.0% (95% CI, 32.5%–100%) | - | - | 16.8 | 0.10 | |
| No | 9 (69.2%) | 77.8% (95% CI, 50.6%–100%) | 77.8% (95% CI, 50.6%–100%) | 41.5% (95% CI, 0.9%–82.1%) | 46.9 | ||
| Renal tumor number | |||||||
| Single | 8 (61.5%) | 75.0% (95% CI, 45.0%–100%) | 46.9% (95% CI, 10.2%–83.6%) | 23.4% (95% CI, 0%–60.6%) | 22.7 | 0.18 | |
| Multiple | 5 (38.5%) | 80.0% (95% CI, 44.9%–100%) | 80.0% (95% CI, 44.9%–100%) | 53.3% (95% CI, 4.7%–100%) | 57.3 | ||
| Extra-renal tumor at the time of initial ablation | |||||||
| Yes | 8 (61.5%) | 75.0% (95%CI, 45.0%–100%) | 75.0% (95%CI, 45.0%–100%) | 28.1% (95%CI, 0%–71.6%) | 39.7 | 0.40 | |
| No | 5 (38.5%) | 80.0% (95%CI, 44.9%–100%) | 30.0% (95%CI, 0%–76.8%) | 30.0% (95%CI, 0%–76.8%) | 21.1 | ||
| Total no. of systemic metastatic tumor | |||||||
| <5 | 10 (76.9%) | 80.0% (95%CI, 55.3%–100%) | 56.0% (95%CI, 22.5%–89.5%) | 56.0% (95%CI 22.5%–89.5%) | 22.7 | 0.38 | |
| ≥6 | 3 (21.1%) | 66.7% (95%CI, 13.4%–100%) | 66.7% (95%CI, 13.4%–100%) | - | 46.9 | ||
| Tumor origin | |||||||
| NSCLC | 3 (23.1%) | 33.3% (95% CI, 0%–86.6%) | - | - | 4.7 | 0.001 | |
| Others | 10 (76.9%) | 90.0% (95% CI, 71.4%–100%) | 77.1% (95% CI, 48.9%–100%) | 41.1% (95% CI, 0.7%–81.5%) | 40.0 | ||
| Tumor size (cm) | |||||||
| <2 | 8 (61.5%) | 100% (95% CI, 100%) | 83.3% (95% CI, 53.5%–100%) | 41.7% (95% CI, 0%–85.2%) | 39.7 | 0.02 | |
| ≥2 | 5 (38.5%) | 40.0% (95% CI, 0%–82.9%) | 20.0% (95% CI, 0%–55.1%) | 20.0% (95% CI, 0%–55.1%) | 8.3 | ||
| Total | 13 | ||||||
Data are numbers of patients. MST, median survival time; mo, months; CI, confidence interval; No., number; and NSCLC, non-small cell lung cancer.
Discussion
Our retrospective analysis revealed that thermal ablation for renal metastases is a safe and feasible treatment option that can provide a high rate of localized tumor control.
After renal ablation, 58.3% (7/12) of the patients with metastatic tumors were prescribed systemic chemotherapy; the remaining 41.7% (5/12) were not administered chemotherapy because no effective systemic chemotherapy options were available. Although thermal ablation for renal metastases decreased the renal function by 12.5 ± 9.0% (range: −5.0% to 23.2%) in these seven patients who were administered systemic chemotherapy, 85.7% (6/7) of them remained in CKD stage 1 or 2 at 6 months following treatment, indicating that renal function was preserved. Importantly, decreased renal function did not prevent the administration of requisite systemic chemotherapy after renal ablation in these patients.
Small renal metastases do not typically result in clinical symptoms [4]. In addition, patients with renal metastases were reported to have extensive disease in other organs [3, 4, 21], and all patients in our cohort had extra-renal metastases. Therefore, less-invasive and nephron-sparing treatment might be preferred for subsequent systemic chemotherapy. Owing to the advantages of thermal ablation, such as less invasiveness and preservation of postoperative renal function than partial renal resection and nephrectomy [15], local treatment with thermal ablation was selected after consultation with medical oncologists.
In this study, the overall survival rates were 76.9% and 59.3% at 1 and 3 years, respectively, and multivariate analysis revealed that metastases from NSCLC were an unfavorable prognostic factor of overall survival. Renal metastases from cancers other than NSCLC (ACC, hemangiopericytoma, leiomyosarcoma, and thyroid cancer) had higher overall survival (OS) rates of 90.0% and 77.1% at 1 and 3 years, respectively. Given the small number of patients in our study, higher survival rates were observed compared with those reported previously for the surgical resection of renal metastases [14], thereby indicating that in patients with slow-growing tumors, local treatment of renal metastases can be a promising treatment option that prolongs survival.
Adamy et al. [13] reported the treatment outcomes of radical or partial nephrectomy for larger renal metastases of 4.5-cm median tumor diameter and 30.7% of the patients (4/13) were alive without evidence of disease at the last follow-up. Their primary diseases were NSCLC (2/4), ACC (1/4), and breast lobular carcinoma (1/4). The results of our study indicated a high local control rate of thermal ablation for metastatic renal tumors (92%) likewise reported rates for primary renal cell carcinoma (95%-100%) [8]. Despite the promising local tumor control rates, only one patient (7.7%, 1/13) achieved a disease-free status, and distant tumor progression decreased the progression-free survival rate to 7.7% at 1 year following renal ablation. In the report by Adamy et al.[13], all patients had a single isolated renal metastasis, and 53.8% of the patients (7/13) had renal tumors as an initial metastasis. However, all patients in our study had a history of extra-renal tumor before renal ablation. The renal tumors in our study might not be a limited disease but are among the manifestations of systemic disseminated disease, and this might be a reason for the low progression-free survival rate. Thermal ablation for renal metastases can be a promising local treatment option for patients with limited tumor burden, especially those with low renal function reserve, but careful patient selection and further research is required.
This study has several limitations. First is the retrospective nature of the study, second is the small sample size of patients, third is heterogeneity in primary tumor(s), and fourth is that our results were not compared with those of other local treatments of surgical resection or radiation treatment.
Conclusion
Thermal ablation for small renal metastatic tumors is safe and feasible. It can be a useful treatment option for the local control of renal metastases. The prognostic factors detected in this study can help maximize the therapeutic benefit and determine the indication for renal metastases ablation.
Conflict of Interest
One of the authors (H.S.) has received research grants from DAIICHI SANKYO COMPANY, LIMITED, Fuji Pharma Co., Ltd., FUJIFILM RI Pharma Co., Ltd., and Eisai Co., Ltd. All other authors declare that there are no relevant conflicts of interest. This study was not supported by any funding.
Author Contribution
All authors contributed to the study conception and design. Material preparation and data collection were performed by Chisami Nagata, Masashi Fujimori, Takashi Yamanaka, Yuichi Sugino, Naritaka Matsushita, Seiya Kishi, Hikari Fukui, Yuki Omari, Kohei Nishikawa, and Hajime Sakuma. Data analysis was conducted by Chisami Nagata, Masashi Fujimori, and Takashi Yamanaka. The first draft of the manuscript was written by Chisami Nagata, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
A part of this study was presented in CIRSE2020.
Acknowledgement
One of the authors (H.S.) has received research grants from DAIICHI SANKYO COMPANY, LIMITED, Fuji Pharma Co., Ltd., FUJIFILM RI Pharma Co., Ltd., and Eisai Co., Ltd.
References
- 1.Vogt A, Schmid S, Heinimann K, et al. Multiple primary tumours: challenges and approaches, a review. ESMO Open. 2017; 2: e000172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma. Analysis of 1000 autopsied cases. Cancer. 1950; 3: 74-85. [DOI] [PubMed] [Google Scholar]
- 3.Bracken RB, Chica G, Johnson DE, Luna M. Secondary renal neoplasms: an autopsy study. South Med J. 1979; 72: 806-807. [DOI] [PubMed] [Google Scholar]
- 4.Choyke PL, White EM, Zeman RK, Jaffe MH, Clark LR. Renal metastases: clinicopathologic and radiologic correlation. Radiology. 1987; 162: 359-363. [DOI] [PubMed] [Google Scholar]
- 5.Pagani JJ. Solid renal mass in the cancer patient: second primary renal cell carcinoma versus renal metastasis. J Comput Assist Tomogr. 1983; 7: 444-448. [DOI] [PubMed] [Google Scholar]
- 6.Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Rising incidence of small renal masses: a need to reassess treatment effect. J Natl Cancer Inst. 2006; 98: 1331-1334. [DOI] [PubMed] [Google Scholar]
- 7.Pagani JJ, Bernardino ME. Incidence and significance of serendipitous CT findings in the oncologic patient. J. Comput. Assist. Tomogr. 1982; 6: 268-275. [DOI] [PubMed] [Google Scholar]
- 8.Park BK, Shen SH, Fujimori M, Wang Y. Asian conference on tumor ablation guidelines for renal cell carcinoma. Investig Clin Urol. 2021; 62: 378-388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Silverman SG, Gan YU, Mortele KJ, Tuncali K, Cibas ES. Renal masses in the adult patient: the role of percutaneous biopsy. Radiology. 2006; 240: 6-22. [DOI] [PubMed] [Google Scholar]
- 10.Krokidis ME, Orsi F, Katsanos K, Helmberger T, Adam A. CIRSE guidelines on percutaneous ablation of small renal cell carcinoma. Cardiovasc Intervent Radiol. 2017; 40: 177-191. [DOI] [PubMed] [Google Scholar]
- 11.Silverman SG, Israel GM, Herts BR, Richie JP. Management of the incidental renal mass. Radiology. 2008; 249: 16-31. [DOI] [PubMed] [Google Scholar]
- 12.Takafuji M, Fujimori M, Nakatsuka A, et al. Computed tomography-guided biopsy for small renal masses before or immediately after tumor ablation: factors affecting diagnostic yield. Jpn J Radiol. 2021; 39: 283-292. [DOI] [PubMed] [Google Scholar]
- 13.Adamy A, Von Bodman C, Ghoneim T, Favaretto RL, Bernstein M, Russo P. Solitary, isolated metastatic disease to the kidney: Memorial Sloan-Kettering Cancer Center experience. BJU Int. 2011; 108: 338-342. [DOI] [PubMed] [Google Scholar]
- 14.Zhou C, Urbauer DL, Fellman BM, et al. Metastases to the kidney: a comprehensive analysis of 151 patients from a tertiary referral centre. BJU Int. 2016; 117: 775-782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fujimori M, Yamanaka T, Sugino Y, Matsushita N, Sakuma H. Percutaneous image-guided thermal ablation for renal cell carcinoma. Interv Radiol. 2020; 5: 32-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Campbell S, Uzzo RG, Allaf ME, et al. Renal mass and localized renal cancer: AUA guideline. J Urol. Elsevier Ltd; 2017; 198: 520-529. [DOI] [PubMed] [Google Scholar]
- 17.Motzer RJ, Jonasch E, Agarwal N, et al. Kidney cancer, version 2.2017: clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2017; 15: 804-834. [DOI] [PubMed] [Google Scholar]
- 18.Ljungberg B, Bensalah K, Canfield S, et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur Urol. 2015; 67: 913-924. [DOI] [PubMed] [Google Scholar]
- 19.Desai MM, Gill IS. Current status of cryoablation and radiofrequency ablation in the management of renal tumors. Curr Opin Urol. 2002; 12: 387-393. [DOI] [PubMed] [Google Scholar]
- 20.Carraway WA, Raman JD, Cadeddu JA. Current status of renal radiofrequency ablation. Curr Opin Urol. 2009; 19: 143-147. [DOI] [PubMed] [Google Scholar]
- 21.Pollack HM, Banner MP, Amendola MA. Other malignant neoplasms of the renal parenchyma. Semin Roentgenol. 1987; 22: 260-274. [DOI] [PubMed] [Google Scholar]
- 22.Yamanaka T, Yamakado K, Yamada T, et al. CT-guided percutaneous cryoablation in renal cell carcinoma: factors affecting local tumor control. J Vasc Interv Radiol. 2015; 26: 1147-1153. [DOI] [PubMed] [Google Scholar]
- 23.Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of Interventional Radiology clinical practice guidelines. J Vasc Interv Radiol. 2003; 14: 199-202. [DOI] [PubMed] [Google Scholar]
- 24.Matsuo S, Imai E, Horio M, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009; 53: 982-992. [DOI] [PubMed] [Google Scholar]
- 25.Ahmed M, Solbiati L, Brace CL, et al. Image-guided tumor ablation: standardization of terminology and reporting criteria-A 10-year update. J Vasc Interv Radiol. 2014; 25: 1691-1705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Goolsby MJ. National Kidney Foundation Guidelines for chronic kidney disease: evaluation, classification, and stratification. J Am Acad Nurse Pract. 2002; 14: 238-242. [DOI] [PubMed] [Google Scholar]