

ABSTRACT
Humankind has lived with the danger of endemic, epidemic and pandemic disease for thousands of years. The effects of these outbreaks have often devastated human populations. Sixteen pandemic events causing an estimated 147 million deaths have occurred since the eighth century, The Black Death and the influenza pandemic of 1918-1920 probably having the greatest impact.
Animal populations, both wild and domestic, have similarly suffered devastating outbreaks of disease which, on occasions, have translated into serious effects on human health. The deliberate or accidental introduction of animals into virgin areas has given rise to unforeseen disease events occasionally leading to extinction. Similarly, human intent or negligence and the vagaries of nature itself has resulted in ill health and loss of life. This paper describes the history of pandemics, epidemics and disasters, and the attempts to bring them under control.
INTRODUCTION
Major outbreaks of disease have blighted humankind ever since the establishment of sedentary villages and small towns, and by the introduction of domesticated farm and work animals. Spread of disease was enhanced by the close proximity of housing and their inhabitants and livestock, and accentuated by the establishment of national and international trade.1
It is now generally accepted that there is a significant chance of the occurrence of future pandemics and of health systems collapse, especially in poorer countries. It is estimated that any pandemic arising from natural or animal causes could lead to as many as 10 million deaths worldwide, a figure already surpassed by the current SARS-CoV-2 pandemic.
It is also expected that climate change and global warming will increase the exposure of populations to vectors and pathogens previously not encountered in certain countries.2 Identifying the origins of zoonotic pathogens and their transmission will be crucial for early detection and prevention.3
Many diseases have a devastating impact on wild and economically important animals. Deliberate or accidental introduction of animals such as cats, mice, rabbits and rats into new habitats has led them to become the origin of plagues in their own right as predators or as sources of disease. The use of animals for biological control has also produced unforeseen adverse effects.
Examples of events caused by human intent or negligence have led to damage to the habitat and property. These have resulted in ill health and loss of life owing to the release of biological agents, toxic chemicals or radiation into the environment.
HUMAN PANDEMICS AND EPIDEMICS
There are five stages through which pathogens from animals evolve into pathogens in humans.4 Pathogens that occur in animals only then undergo the transfer of the pathogen to humans. Limited outbreaks may then occur in the human population followed by a prolonged human outbreak. Pandemics may then occur as a result of this exclusive outbreak amongst humans becoming country and worldwide.
Eight of the 15 temperate diseases possibly reached humans from domestic animals, three from apes or rodents, the remaining four still of unknown origin. Eighteen of the 25 major human pathogens originated in the Old World and possibly one-third of all emerging diseases have originated from changes in land use thereby increasing animal-human interaction.
The first probable epidemic occurred in China around 3000 BCE as evidenced by the presence of mass graves (Fig 1). Three pandemics of The Plague have occurred in history. The Plague of Justinian occurred from 541 to 747 CE, The Black Death from 1346 to 1844 and during the year 1894 originating in the Canton province of China. Major trade routes decided the major hot spots of Plague, with navigable rivers determining the geographical pattern of sporadic cases. Further studies by Yue et al.5 reveal that Plague penetrated further into Europe through local trade route networks. Table 1 lists the routes by which pandemics are spread.
Fig 1.

Ancient mass grave in China.
Table 1.
Spread of pandemics through trade and travel.
| Route of spread | Examples |
|---|---|
| Overland trade routes | The Silk Road: Far East to Middle East Overland routes between Constantinople and Western Europe Siberia and Russia to Europe (via Vienna) |
| Oceanic and sea routes | Trade: China to India Trade: India to Africa via Indian Ocean then to Egypt and Europe via the Red and Mediterranean seas Trade: Europe to the Americas via the Atlantic Ocean including the transport of slaves Cruise ships: Country to country; continent to continent |
| Air travel | Global air travel |
Throughout history there have been a number of other notable epidemics. Mediaeval leprosy is an example of relationships that developed between disease, social stigma and various theological interpretations. Between 1500 and 1600, syphilis, an apparently new disease, appeared among the army of Charles VIII during the siege of Naples and reached as far as China in the early part of the 16th century. Debate continues as to whether the disease first appeared in Europe or was brought into Europe from The Americas with the return of Christopher Columbus and his crews.
Yellow fever, originating in Africa, was transmitted to the Western Hemisphere via the slave trade with notable outbreaks occurring in the Yucatan (1648), Hispaniola (17931804), Philadelphia (1793) and Swansea in South Wales (1865). The Swansea outbreak was brought from Cuba on the barque Helca. A total of 28 passengers contracted the disease and 16 died. Several crew members were taken ill and died, and at least 27 inhabitants of Swansea contracted the infection and 15 of them died.6
Smallpox occurred in The Americas, Iceland, The Balkans and 18th and 19th century Europe, during which some half a million people died.
Carrion’s disease occurs in Peru and was studied by Daniel Carrion (Fig 2) who was appalled by the death rate (over 10,000 deaths between 1870 and 1871). He observed that verruga peruana and Oroya fever were transmitted by a sandfly vector and, by injecting himself with verruca material, subsequently died of Oroya fever demonstrating they were different manifestations of the same disease.
Fig 2.
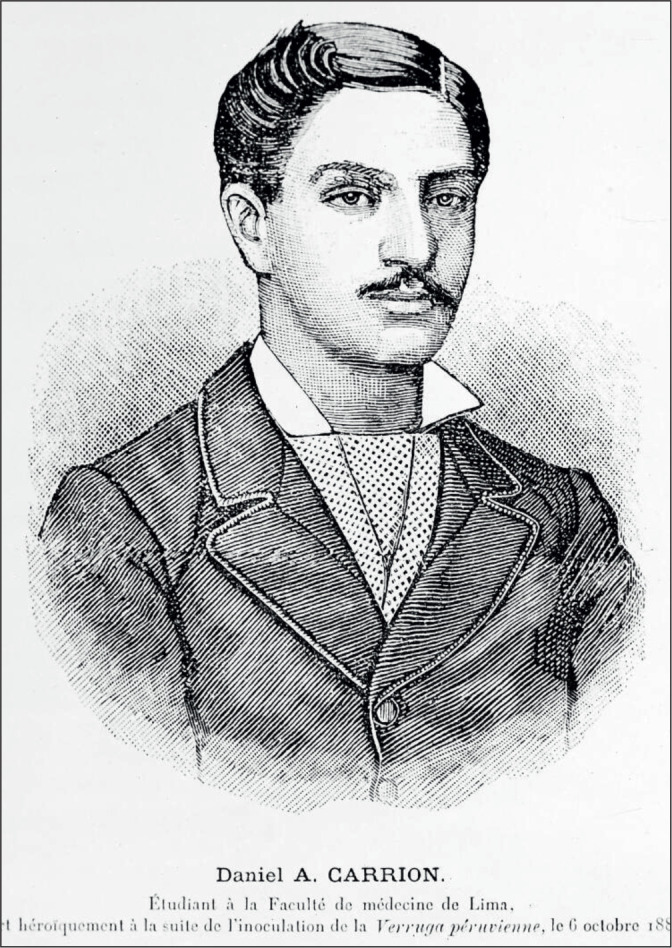
Daniel Carrion
Demonstrated that verrugua peruana and Oroya Fever were manifestations of the same diseases. Wellcome Images
Contemporary 20th century disease epidemics have consisted of poliomyelitis, malaria, tuberculosis, Eastern Equine Encephalitis, Dengue fever, Chikungunya fever, Zika virus and the human immunodeficiency virus causing AIDS, all leading to significant morbidity and mortality.
For those diseases that are mosquito-borne the vector is often an invasive species of mosquito that is spread by international trade and whose common breeding ground is stagnant water, including in old stored tyres. Affected countries include those in Europe, the United States, Latin America and South Africa.
Twenty million cases of tuberculosis with 1.5 to two million deaths each year and approximately 10,000 deaths occurred each year from poliomyelitis between 1945 and 1955 before vaccination was introduced.
PANDEMICS: PREPAREDNESS AND PREVENTION
It is now generally accepted that there is a significant chance of future pandemics and of possible health system collapse, especially in poorer countries.7 It has been estimated that any pandemic arising from natural or animal causes could lead to significant mortality worldwide.
HISTORICAL CAUSES OF EPIDEMICS
Throughout history the causes of epidemics have been attributed to a number factors. The anger of a vengeful or unforgiving God is typified in the lliad where Homer describes Apollo raining down plague on the Greek army. Similarly, The Holy Bible describes the “ten plagues” of Egypt as reflecting the wrath of God punishing the Egyptian people in the book of Exodus.
Astrological movements have been assumed to be the source of pandemics. For example, on 20th February 1345 the alignment of Saturn, Jupiter and Mars in the constellation of Aquarius was blamed for the outbreak of The Black Death. Expectation of such astrological events could help to place prevention steps in place.
The presence of bad or poisoned air, known as Miasma, was to be avoided8 such as associated with marshes (for example in ancient Rome) and human waste dumps. Overcrowded or slum areas were also included in areas to be avoided. In 1518 King Henry VIII ordered slaughter houses to be placed outside of city walls, banned kissing and introduced social distancing9 in plague orders issued by decree (Fig 3).
Fig 3.
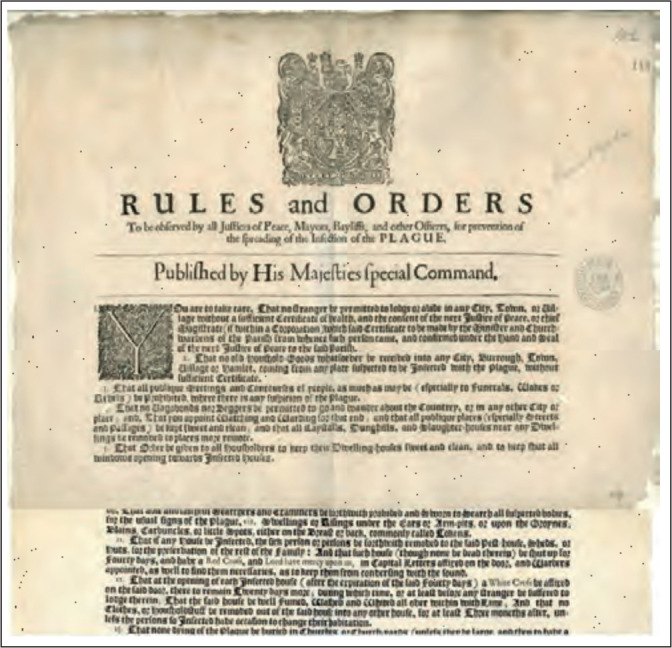
Henry VIII Plague rules and orders. National Archives
Religion has played a part in apportioning blame to the rise of epidemics. Accusing Jewish people of poisoning wells was commonplace in the Middle Ages. On 14th February 1349, 2000 Jews were burned to death in Strasbourg.
In the early modern era vermin were apportioned the blame for disease such that in 1647 Aberdeen council ordered the poisoning of rats and mice to prevent the spread of diseases.
In the modern era particularly, changes in land use have led to deforestation and the change of the use of land to farming, mining and oil extraction. Such changes have resulted in closer contact between humans and wild animal and rodent reservoirs – so-called “spill over events”.
HISTORY OF PREVENTION
To the end of the 17th century diseases were assumed to be the sign of a poor moral and spiritual condition. The public effort to control disease included isolation of the sick and the quarantine of travellers. In 1665, houses in London were placed under quarantine in an attempt to stop the plague.
In the 18th century isolation and quarantine became more common across Europe especially in sea ports around the Mediterranean. Lady Mary Montagu, (Fig 4), having recovered from smallpox in 1715, reported on the use of “variolation” against smallpox on her visit to the Ottoman Empire in 1717. Her six-year-old son was variolated in 1718 and her two-year-old daughter in 1721. Lady Mary Wortley Montagu was, it is thought, responsible for importing variolation into England in 1721.10
Fig 4.

Lady Mary Wortley Montagu.
Thought to have imported variolation into England in 1721.
Benjamin Jesty, a Dorset farmer, used cowpox to “vaccinate” his family against smallpox in 1774, noticing that milkmaids with cowpox lesions on their hands were “resistant” to suffering from smallpox. Edward Jenner improved the outcome and safety of patients by using smallpox vaccine in 1796.
The 19th Century
In 1853 vaccination against smallpox was made compulsory. Louis Pasteur and Robert Koch developed the Germ Theory of disease and suggested that disease is caused by bacteria and “unfilterable agents”. Koch, together with Freidrich Loeffler, formulated Koch’s postulates in 1884 as a result. Identification of filth as a cause and vehicle of transmission is termed “The Great Sanitary Awakening” and changed perceptions about health.
Disease was recognised as an indication of poor social and environmental conditions, and increasing urbanisation led to an increase in the number of diseased individuals, with London experiencing unprecedented numbers of cholera, typhoid and tuberculosis (consumption). As a result isolation and quarantine became difficult to establish.
The 20th Century
Sir Arthur Newsholme,11 (Fig 5) a Local Government Board physician, advised people to stay at home if they were sick and to avoid large gatherings during the 1917-1918 influenza pandemic. Unfortunately, his advice was not published by the Government of the day. He argued that many lives could have been saved if his suggestions were followed. There were no imposed lockdowns until it was too late and the attempt to limit crowds at large sporting events was delayed. Vaccination against influenza was introduced in the 1930s with large-scale availability in the 1940s. Development of vaccines then became a priority for many countries.
Fig 5.
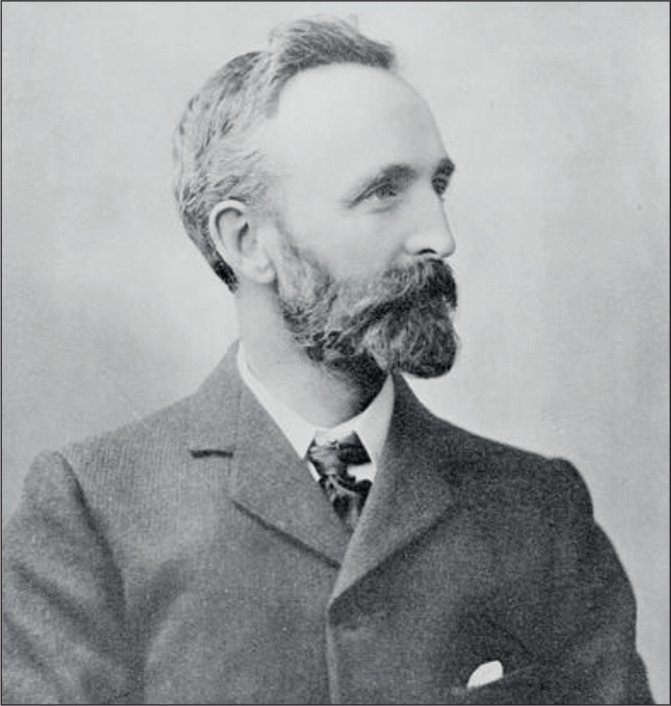
Sir Arthur Newsholme.
Local Government Board Physician during the 1917-1918 Influenza pandemic
Epidemics and pandemics of infectious diseases have devastated civilisations and over the centuries mankind has developed effective tools to deal with such outbreaks. A clearer understanding of quarantine and hygiene together with improved science has led to better hygiene and infection control together with the development of antibiotics, antiviral agents, vaccines, diagnostics and better reporting and surveillance.
WHAT HAVE WE LEARNED?12
Early warning detection, preparedness and laboratory facility
It has been demonstrated that international collaboration is essential for dealing with pandemics.
The need for early warning has led to improved local, national and international epidemiological surveillance. This has resulted in the development of a network of bodies that monitor, report and give advice. Organisations such as Public Health England (PHE), the US Centers for Disease Control and Prevention (CDC), the European Centre for Disease Prevention and the World Health Organization Global Outbreak Alert and Response Network. History has shown that lack of training, poor engagement of clinical staff, politicians and the general population, together with poor surveillance, isolation and the response capacity leads to poor control of outbreaks.
It has also been recognised that a resilient network of special and routine laboratory services has become essential for the detection and diagnosis of infectious diseases, especially when the disease is novel.
Development of novel diagnostics and effective vaccines
It has been demonstrated that international collaboration is essential for the dissemination of information necessary for the identification, detection and epidemiological typing of outbreak and pandemic strains to enable a clearer understanding of their epidemiology.
Development of vaccines, antimicrobial agents and vector control greatly impacts on the progress of an epidemic as demonstrated by earlier epidemics and pandemics.
WORLDWIDE PANDEMICS: COMPARISON OF EFFECTS
Between 1347 and 2019 there have been 16 pandemics causing at least 147 million deaths.
Table 2 lists these pandemic events with their estimated global death tolls.
Table 2.
Pandemic events from 14th to 21st centuries.
| Pandemic | Estimated death toll |
|---|---|
| The Black Death 1347-1352 | 75 million |
| The Great Plague of Seville 1647-1652 | 2 million |
| The Russian Cholera Pandemic 1852-1860 | 1 million |
| Global Influenza Pandemic 1889-1890 | 1 million |
| “Spanish Flu” Influenza Pandemic 1918-1920 | 50 million |
| “Asian Flu” Influenza Pandemic 1957-1958 | 2 million |
| “Hong Kong Flu” Influenza Pandemic 1968-1969 | 1 million |
| SARS-CoV-2 2019-???? | 15 million (WHO estimate) |
Effects on healthcare systems
In Mediaeval Europe science, technology and medical practice lagged behind the Islamic world. A combination of local knowledge of healing herbs and the use of town-based practitioners such as apothecaries and barber surgeons and university trained physicians were consulted but these groups did not share helpful information. Early hospitals in Europe, established mainly in response to the injured from the Crusades, were primitive. Sanitation and hygiene were poor and disease transmission poorly understood. Earliest attempts at disease control is believed to have occurred in Venice with other major ports adopting a detention period of 40 days (quarantine).
The influenza pandemic beginning in 1918, thought to be caused by the bacterium Haemophilus influenzae (no laboratory methods were available to detect viruses), had no treatment and the only protection in use at the time were face masks (Fig 6). The healthcare systems were seriously understaffed owing to losses caused by the First World War together with the high death rates from influenza. Medical school graduates, retired medical personnel, student nurses and dentists were drafted to make up for the losses. Healthcare was fragmented, social distancing measures were introduced but often too late.13
Fig 6.

Page appearing in Time magazine encouraging the wearing of masks during the influenza pandemic.
The introduction of socialised medicine in the late 1920s began to provide healthcare free at the point of access, first introduced in Russia followed by Germany, France and the United Kingdom.
The opening, in Vienna, of an international bureau for fighting epidemics was established in 1919 and was recognised as the forerunner of the World Health Organization.14
Economic effects
The Black Death ended population growth with one-third to a half of the population of Europe dying. The relationship between land-owning lords and the peasants working their land deteriorated significantly. Workforce reduction occurred owing to high levels of mortality resulting in demands for higher wages and greater competitive marketing particularly trading in wool, textiles and silk resulting, paradoxically, in increased economic welfare of the surviving population. Little coordination of sanitary efforts occurred, medical efforts failed since the profession was unprepared for such large-scale outbreaks resulting in many doctors and priests either dying or fleeing.
The influenza pandemic of 1918-1920 had short-lived negative effects with recovery of per capita income and economic recovery before the downturn experienced in the 1930s.
The retail grocery sector declined and an increased demand for beds, mattresses and bedpans occurred owing to massive increases in patient numbers. Labour supply temporarily declined owing to losses of men resulting from the First World War.
ANIMALPLAGUES, PESTILENCE AND PANDEMICS
As with humans many diseases have had a devastating impact on wild and economically important animals. Deliberate or accidental introduction of animals such as cats, mice, rabbits and rats into new habitats has led them to become plagues in their own right; as predators or sources of disease. The use of animals for biological control has also produced important unforeseen effects. Important animal epidemics are listed below.
African swine fever became endemic to sub-Saharan Africa in wild pigs and warthogs and has now spread worldwide leading to two massive losses of farmed pigs. In 1957 it became established on the Iberian Peninsula with concomitant outbreaks in France and Belgium which led to spread among wild boar across the Caucasus, Eastern Europe, Greece, Russia, Iran and Azerbaijan. The disease reached China in August of 2018 and India in 2020 and continues to spread.15
Bat White Nose Syndrome was first detected in New York and subsequently spread across North America in 2006 killing nearly six million bats with some species declining by 99% Caused by Pseudogymnoascus destructans, bat hibernation is disrupted leading to depletion of fat reserves and subsequent starvation. Paradoxically, it is not yet been found in Europe.16
Chlamydia infection in Koala bears is sexually transmitted, caused by Chlamydia pecorum, and leads to infertility, urinary and respiratory infections, blindness and death. Combined with drought and concurrent retrovirus infection, it has massively reduced Koala populations.17
Chytridiomycosis, an infection by the chytrid fungi Batrachochytrium dentrobatis and B. salamandivorans, has been linked to dramatic population decline and extinctions of amphibians in the Americas, Australia, East Africa and the Caribbean. Over 200 species have been affected and in Panama 30 species have been lost. American bullfrogs and African clawed toads seem to be resistant to infection and trade in these two species is blamed for the spread of the disease18.
B. dendrobatids was first reported in Europe in the early 2000s and in the UK in 2005. As in the rest of the world, infection with this fungus is having a devastating effect on native amphibians. As an example, it has been associated with mass die-off of wild European fire salamanders, leading to a 99% decline in the national population of this species in the Netherlands.
Ebola infection in Great Apes has become a recent and serious problem. It is known that infection with Ebola virus will kill 95% of Great Apes. The chimpanzee population in Cote d’Ivoire was decimated in the early 1990s and repeated outbreaks in the Democratic Republic of Congo have taken a heavy toll on the Gorilla population. Approximately 5000 Western Gorillas died in the period 2002-2003.19
Foot and Mouth disease is a debilitating and sometimes fatal viral infection of cloven-hoofed animals, including domestic and wild bovids, sheep, goats and wild animals including elephants and hedgehogs. Highly contagious, it has severe implications for the farming industry as control is achieved by the culling of affected herds and requires scrupulous decontamination of equipment, vehicles, clothing and feed. Table 3 outlines the major outbreaks of Foot and Mouth disease since the 1870s
Table 3.
Major outbreaks of Foot and Mouth disease.
| Outbreak | Detail |
|---|---|
| United States of America | Two detailed major outbreaks. |
| Nine major outbreaks between 1870 and 1929 | 1914-1929; resulting in slaughter of cattle, sheep, swine and deer. 1929; outbreak originating in hogs that had eaten infected Argentinian meat from a tourist ship. |
| United Kingdom | 1967; Infected lambs from Argentina and Chile led to the slaughter of 442,000 animals at an estimated cost of £370 million. 2001; 2000 cases identified; six million animals culled. 2007; Outbreak in Surrey caused by the 01 BFS67 strain (a vaccine-like strain) which was used at the Institute of Animal Health four Km from the outbreak. Outbreaks occurred in nearby farms, all at-risk animals culled. Windsor Great Park closed to protect the deer population. |
| China, Taiwan, Japan and Korea | Experienced major outbreaks |
Rinderpest is a viral disease of cattle and even-toed ungulates and has a mortality approaching 100% in immunologically naive populations. After a global eradication programme (Fig 7) the last case was recorded in 2001.20 It is thought that measles and canine distemper, similarly causing devastating disease in naive populations, possibly emerged from rinderpest around 600 BCE.
Fig 7.

Rinderpest campaign stamp.
Only the second global viral disease to have been eradicated.
West Nile Encephalitis was originally found causing disease in birds. This mosquito-transmitted virus was isolated in 1999 from patients with encephalitis in New York. At the same time several crows in the city and birds at the Bronx zoo were found to have died of this infection. Millions of birds in the United States of America have died of this disease and the virus has been detected in 48 species of mosquito and in 250 bird species and in horses.21
Sarcoptic mange (caused by Sarcoptes scabei) affects over 100 animal species as well as humans. It infests wombats, red foxes, lynx, wolves and domestic dogs and is thought to have rendered foxes on Bornholm extinct.22
Sylvatic plague arrived in North America around 1900 on ships from Europe carrying rats. Entire colonies of prairie dogs have been destroyed and 90% of black-footed ferrets, predators of prairie dogs, have subsequently been lost. Transmission to humans occasionally occurs, particularly among hunters.23
MAN-MADE THREATS AND DISASTERS
Human intent or negligence has led to great damage to human life, habitat and property. These have resulted in ill health and loss of life due to the release of microbiological agents, toxic chemicals or radiation into the environment.
Laboratory accidents
Accidents in the laboratory have led to exposure to chemical toxicity, radiation and biological agents.
Table 4 lists the most important events that have led to death, potential serious harm or injury.
Table 4.
Laboratory accidents leading to death or potential serious injury.
| Year | Site | Event |
|---|---|---|
| 1958 | Los Alamos National Laboratory, United States of America | Accidental exposure of scientist to a fatal dose of radiation |
| 1967 | Marburg Laboratory, Germany | Seven fatalities following work with monkeys infected with Marburg virus |
| 1978 | Birmingham, United Kingdom | Medical photographer fatally exposed to smallpox virus via unfiltered air duct24 |
| 1997 | United States | Chemistry Professor, death due to skin absorption of dimethyl mercury25 |
| 2007 | Pirbright Institute, Surrey, UK | Culpable in Foot and Mouth disease via drainage leak. |
| 2009 | CDC, Atlanta, USA | Viable anthrax spores sent via postal system. |
| 2011 | Yale University, USA | Student dies via hair entrapment in lathe while working alone out of hours. |
| 2012 | Animal Health and Veterinary Laboratory, Surrey, UK | Viable anthrax spores sent other laboratories |
| 2015 | Tsinghua University, China | Researcher dies in explosion and fire26 |
| 2016 | University of Hawaii, Honolulu, USA | Researcher lost arm as a result of hydrogen/oxygen explosion. |
| 2018 | Science Institute, Bengaluru, India | Cylinder gas explosion. One death and three seriously injured |
Biological and chemical warfare
The use of biological agents, chemical toxins and radiological agents has occurred as a deterrent or for offensive purposes.27-29 Possibly most infamously was the use of chlorine and mustard gas in the First World War in 1917 resulting in 6000 fatalities and 185,000 injuries. Preparation of sugar lumps containing tiny vials of anthrax spores 30 and the preparation of glanders and cholera as weapons was also documented. Experimental use of anthrax and plague on Japanese prisoners of war was recorded and subsequent preparation of biological weapons was developed by Israel, Iraq, Soviet Union, Libya, the USA and the UK. In 1972 The Biological Weapons Convention introduced regulations to control development and stockpiling of such weapons. However, in 1979 the accidental release of anthrax from a military unit near Moscow resulted in 64 deaths. Anthrax, used as a bioterror weapon sent through the national post in the USA resulted in five deaths. Chemical poisoning using a polonium-210 isotope poisoned Alexander Litvinenko, and Novochock nerve agent has been responsible for the poisoning of three people in England and the political activist Alexei Navalny.
Chemical accidents
In 1952 groundwater, soil and nearby water wells were contaminated by hexavalent chromium produced by a cooling tower leakage from a compressor station in Hinkley, California, USA. It was responsible for a number of cancer cases including of the lung and nasal sinuses. In the same year the great “smog” of London, smoke containing pollutants, resulted in at least 6000 people dying from respiratory complications with many more suffering prematurely from long-term respiratory disease.31
In Japan, in 1956 (Minamata)32, 33 and 1960 (Yokkaichi), two serious chemical releases occurred involving toxic methylmercury discharged into Minamata bay which accumulated in the local fish and was subsequently eaten by the local population. Over 2265 victims were documented many suffering coma and death. Airborne sulphur dioxide released from the petrochemical refinery in Yokkaichi gave rise to severe respiratory symptoms in the population leading to a 10- to 20-fold higher mortality rate above the national average.
Perhaps the most well-known chemical accident occurred in Bhopal, India where at least 40 tons of highly toxic methyl isocyanate gas leaked from the Union Carbide pesticide company owing to equipment failures including safety devices.34 At least 3800 died immediately with an estimated 20,000 premature deaths over the next two decades from associated complications.
Radiation
The Three Mile Island nuclear power plant in Pennsylvania, USA suffered a partial reactor meltdown in 1979 due to mechanical and human error involving the cooling system. Radioactive gases were released including iodine-131 leading to the mass evacuation of 200,000 people. Similarly, in 1986 in Chernobyl, Ukraine a powerful explosion in the nuclear reactor occurred followed by a core fire and second explosion resulted in the release of around 70 tons of nuclear fuel containing iodine-131 and caesium-137 during a nine-day period (Fig 8).35 The radioactive cloud spread across Europe as far as the United Kingdom. Over 200,000 people were evacuated from the nearby surroundings. Two reactor staff died, 237 staff and fire fighters suffered acute radiation sickness and approximately 4000-5000 other cancer types were recorded.
Fig 8.

The destroyed reactor at the Chernobyl nuclear plant.
In 2011 a large earthquake followed by a large tsunami resulted in three nuclear core meltdowns with three hydrogen air explosions and flooding of the lower reactors in the nuclear plant at Fukushima in Japan resulting in the evacuation of 154,000 people.
Footnotes
UMJ is an open access publication of the Ulster Medical Society (http://www.ums.ac.uk).
REFERENCES
- 1.Torrey EF, Yolken RH. Beasts of the earth: animals, humans and disease. New Brunswick, NJ: Rutgers: University Press; 2014. [Google Scholar]
- 2.Baker RE, Mahmud AS, Miller IF, Rajeev M, Rasambainarivo F, Rice BL, et al. Infectious disease in an era of global change. Nat Rev Microbiol. 2022;20(4):193–205. doi: 10.1038/s41579-021-00639-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Judson SD, Rabinowitz PM. Zoonoses and global epidemics. Curr Opin.Infect Dis. 2021;34(5):385–92. doi: 10.1097/QCO.0000000000000749. [DOI] [PubMed] [Google Scholar]
- 4.Wolfe N, Dunavan PC, Diamond J. Origins of major human infectious diseases. Nature. 2007;447(7142):279–83. doi: 10.1038/nature05775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yue RP, Lee HF, Wu CY. Trade routes and plague transmission in pre-industrial Europe. Sci Rep. 2017;7(1):12973. doi: 10.1038/s41598-017-13481-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Smith CE, Gibson ME. Yellow fever in South Wales, 1865. Med Hist. 1986;30(3):322–40. doi: 10.1017/s0025727300045737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gates B. The next epidemic - lessons from Ebola. N Engl J Med. 2015;372(15):1381–4. doi: 10.1056/NEJMp1502918. [DOI] [PubMed] [Google Scholar]
- 8.Cipolla CC. In: Miasma and disease: public health and environment in the pre-industrial age. Potter Elizabeth., translator. London: Yale University Press; 1992. [Google Scholar]
- 9.Roger EC. “To Be Shut Up”: new evidence for the development of quarantine regulations in early-Tudor England. Soc Hist Med. 2020;33(4):1077–96. [Google Scholar]
- 10.Willet J. The pioneering life of Mary Wortley Montagu: scientist and feminist. Barnsley, UK: Pen & Sword; 2021. [Google Scholar]
- 11.Eyler JM. Sir Arthur Newsholme and State Medicine, 1885-1935. Cambridge, UK: Cambridge University Press; 1997. [Google Scholar]
- 12.Gates B. Innovation for pandemics. N Engl J Med. 2018;378(22):2057–60. doi: 10.1056/NEJMp1806283. [DOI] [PubMed] [Google Scholar]
- 13.Spinney L. How the 1918 flu pandemic revolutionized public health. [Internet] Smithsonian Magazine. 2017. Sep 27, (cited 2021 Feb 2) Available from: https://www.smithsonianmag.com/history/how-1918-flu-pandemic-revolutionized-public-health-180965025/
- 14.Schoch-Spana M. Implications of pandemic influenza for bioterrorism response. Clin Infect Dis. 2000;31(6):1409–13. doi: 10.1086/317493. [DOI] [PubMed] [Google Scholar]
- 15.Dixon LK, Sun H, Roberts H. African swine fever. Antiviral Res. 2019;165(5):34–41. doi: 10.1016/j.antiviral.2019.02.018. [DOI] [PubMed] [Google Scholar]
- 16.Blehert DS, Hick SC, Behr M, Meteyer CU, Berlowski-Zier BM, Buckles EL, et al. Bat white-nose syndrome: an emerging fungal pathogen? Science. 2008;323(5911):227. doi: 10.1126/science.1163874.. [DOI] [PubMed] [Google Scholar]
- 17.Westcott B. Koalas are dying from Chlamydia, and climate change is making it worse. [Internet] CNN Australia. 2021. Nov 8, (cited 2021 Feb 2) Available from: https://edition.cnn.com/2021/11/06/australia/australia-koala-chlamydia-intl-dst-hnk/index.html.
- 18.Chytridiomycosis. [Internet] Wikipedia. 2021. (cited 2022 Feb 2) Available from: https://en.wikipedia.org/wiki/Chytridiomycosis.
- 19.Ying Zaao. Epidemics and wildlife: How Ebola affects gorillas and chimpanzees. [Internet] China Global Television Network, Animal. 2020;20:53. (cited 2022 Feb 2) Available from: https://news.cgtn.com/news/2020-02-09/How-Ebola-affects-gorillas-and-chimpanzees-NW4XUMFBJe/index.html. [Google Scholar]
- 20.Rinderpest. [Internet] Wikipedia. 2021. (cited 2022 Feb 2) Available from: https://en.wikipedia.org/wiki/Rinderpest.
- 21.Petersen LR. Epidemiology of West Nile virus in the United States: Implications for arbovirology and public health. J Med Entomol. 2019;56(6):1456–62. doi: 10.1093/jme/tjz085. [DOI] [PubMed] [Google Scholar]
- 22.Forchhammer MC, Asferg T. Invading parasites cause a structural shift in red fox dynamics. Proc Biol Sci. 2000;267(1445):779–86. doi: 10.1098/rspb.2000.1071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Antolin MF, Gober P, Luce B, Biggins DE, Van Pelt WE. Lincoln: Digital Commons, University of Nebraska, US Fish and Wildlife Publications; [Internet]. The Influence of Sylvatic Plagueon North American Wild life at the landscape level, with special emphasis on Black-Footed Ferret and Prairie Dog Conservation. (cited 2022 Feb 2) Available from: https://digitalcommons.unl.edu/usfwspubs/57. [Google Scholar]
- 24.Weiss MM, Weiss PD, Mathisen G, Guze P. Rethinking smallpox. Clin Infect Dis. 2004;39(11):1668–73. doi: 10.1086/425745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nierenberg DW, Nordgren RE, Chang MB, Siegler RW, Blayney MB, Hochberg F, et al. Delayed cerebellar disease and death after accidental exposure to dimethylmercury. N Engl J Med. 1998;338(23):1672–76. doi: 10.1056/NEJM199806043382305. [DOI] [PubMed] [Google Scholar]
- 26.Cyranoski D. Postdoc dies in lab fire at Tsinghua University. Nature. 2015 doi: 10.1038/nature.2015.19066. [DOI] [Google Scholar]
- 27.Pitchman V. Overall view of chemical and biochemical weapons. Toxins(Basel) 2014;6(6):1761–84. doi: 10.3390/toxins6061761.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Clark DP, Pazdernik NJ. Biological warfare: infectious disease and bioterrorism. In: Clark DP, Pazdernik NJ, editors. Biotechnology. 2nd edn. Berkeley, CA: Elsevier; 2016. pp. 687–719. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7150198/ [Google Scholar]
- 29.Oliveira M, Mason-Buck G, Ballard D, Branicki W, Amorim A. Biowarfare, bioterrorism and biocrime: A historical overview onmicrobial harmful applications. Forensic Sci Int. 2020;314:110366. doi: 10.1016/j.forsciint.2020.110366.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Redmond C, Pearce MJ, Manatee RJ, Bernal BP. Deadly relic of the Great War. Nature. 1998;393(6687):747–8. doi: 10.1038/31612. [DOI] [PubMed] [Google Scholar]
- 31.Hunt A, Abraham JL, Judson B, Berry CL. Toxicologic and epidemiologic cluesfrom the characterization of the 1952 London smog fine particulate matter in archival lung tissues. Environ Health Prospect. 2003;111(9):1209–14. doi: 10.1289/ehp.6114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hong YS, Kim YM, Lee KE. Methylmercury exposure and health effects. J Prev Med Public Health. 2012;45(6):353–63. doi: 10.3961/jpmph.2012.45.6.353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Watanabe C, Satoh H. Evolution of our understanding of methyl mercuryas a health threat. Environ Health Perspect. 1996;104(Suppl 2):367–79. doi: 10.1289/ehp.96104s2367.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Dhara VR, Dhara R. The Union Carbide disaster in Bhopal: a review of health effects. Arch Environ Health. 2002;57(5):391–404. doi: 10.1080/00039890209601427. [DOI] [PubMed] [Google Scholar]
- 35.Jaworowski Z. Observations on the Chernobyl disaster and LNT. Dose Response. 2010;8(2):148–71. doi: 10.2203/dose-response.09-029.Jaworowski. [DOI] [PMC free article] [PubMed] [Google Scholar]