

Abstract
Objective:
Binge-eating disorder (BED), the most prevalent eating disorder, is a serious public health problem associated with obesity, psychiatric/medical comorbidities, and functional impairments. BED remains underrecognized, infrequently treated, and few evidence-based treatments exist. We tested effectiveness of naltrexone/bupropion and behavioral weight-loss therapy (BWL), alone and combined, for BED comorbid with obesity.
Methods:
Randomized double-blind placebo-controlled single-site trial, conducted February 2017 to February 2021, tested naltrexone/bupropion and BWL using 2×2 balanced factorial design. 136 patients with BED (81.6% women, mean age 46.5, mean BMI 37.1 kg/m2) were randomized to one of four 16-week treatments: placebo (N=34), naltrexone/bupropion (N=32), BWL+placebo (N=35), or BWL+naltrexone/bupropion (N=35); 81.7% completed independent posttreatment assessments.
Results:
Intention-to-treat binge-eating remission rates were 17.7% (placebo), 31.3% (naltrexone/bupropion), 37.1% (BWL+placebo), and 57.1% (BWL+naltrexone/bupropion). Logistic regression of binge-eating remission revealed that BWL was significantly superior to no-BWL, and that naltrexone/bupropion was significantly superior to placebo, but there was no significant interaction between BWL and medication. Mixed models of complementary measures of binge-eating frequency also indicated that BWL was significantly superior to no-BWL. Rates attaining 5% weight-loss were 11.8% (placebo), 18.8% (naltrexone/bupropion), 31.4% (BWL+placebo), and 38.2% (BWL+ naltrexone/bupropion). Logistic regression of 5% weight loss and mixed models of percent weight loss both revealed that BWL was significantly superior to no-BWL. Mixed models revealed significantly greater improvements for BWL than no-BWL for secondary measures (eating-disorder psychopathology, depression, eating behaviors, cholesterol, Hb1Ac).
Conclusions:
BWL and naltrexone/bupropion were associated with significant improvements in BED, with a consistent pattern of BWL being superior to no-BWL.
Keywords: obesity, eating disorders, behavior therapy, pharmacotherapy, binge eating, weight loss
Binge-eating disorder (BED), a new official diagnosis in the DSM-5 (1), is a serious public health problem (2) with substantial social and economic costs (3). BED is defined by recurrent binge eating (eating unusually large amounts of food while experiencing loss-of-control) and marked distress without inappropriate weight-compensatory behaviors (1). BED is prevalent, associated with elevated rates of psychiatric/medical disorders, with psychosocial impairments (2,4,5), and is predictive of future medical conditions (2,6). While BED is associated strongly with obesity (2,4), this psychiatric disorder has distinct behavioral, psychopathological, and neurobiological features from the medical diagnosis of obesity (7). Despite high levels of morbidity, BED remains underrecognized and most people with BED go untreated (2,8).
Controlled treatment research has identified certain psychological and pharmacological treatments with efficacy for BED (9,10). Cognitive-behavioral therapy (CBT) and interpersonal psychotherapy (IPT) have empirical support for BED, generally resulting in 50% remission rates and durable therapeutic benefits through 24-month follow-ups (11). These “specialist” treatments, however, are neither frequently sought nor widely available (8) and they fail to produce weight loss (11,12). Growing evidence suggests that behavioral weight loss (BWL), a “generalist” and disseminable behavioral treatment (11), produces binge-eating outcomes in BED that are comparable to CBT and IPT but with the advantage of significant weight losses (11,12,13). BWL trials have reported binge-eating remission rates ranging 38%–74% and percent weight loss ranging 2.6%–5.1% (11,12,13).
The sole pharmacological treatment for BED approved by the US Food and Drug Administration (FDA) is lisdexamfetamine, which results in binge-eating abstinence rates of 32–40% (14,15). Lisdexamfetamine, however, is contraindicated for individuals with histories of substance misuse and has a “limitation of use” that it is not recommended for obesity. Several other medications have yielded statistically significant reductions in binge eating (10) but only topiramate has reliably reduced both binge eating and weight (16) and when combined with psychological treatments (17,18). Unfortunately, topiramate has limited tolerability and high discontinuation rates (10).
Many patients do not benefit sufficiently even when they receive best-available treatments for BED (9,10). The strong association between BED and obesity plus patients’ treatment goals suggest that focusing solely on either binge eating or on weight is a false dichotomy that fails to meet patients’ preferences and medical needs (19). To date, achieving weight loss in patients with BED and obesity has been difficult and BWL is the sole psychological approach that has reliably produced weight loss alongside reduced binge eating (13). Weight losses with existing treatments for BED are often insufficient (18) and frequently less than those reported with treatments for obesity without BED (20). Thus, identifying effective pharmacological and combination approaches for reducing both binge eating and weight in BED remains a pressing need (18).
Although there exist several FDA-approved weight-loss medications, no centrally-acting agents have been tested alone and combined with psychological treatments for BED (18). Orlistat, a lipase inhibitor, significantly enhanced weight-loss albeit only modestly and effects on binge eating were non-significant (21). One current FDA-approved obesity agent, naltrexone/bupropion combination (22), is logical to consider for BED because its putative mechanisms are relevant for both binge eating and obesity. Naltrexone/bupropion has hypothesized effects in regulating food intake and weight based on leptin’s mechanisms of action (23). Leptin’s excitatory effects on pro-opiomelanocortin (POMC) neurons in the hypothalamus melanocortin system produce anorectic effects (24). Stimulated POMC signaling decreases food intake and increases energy expenditure but is inhibited by endogenous feedback (24). The rationale for this medicine combination is to stimulate POMC neurons (bupropion) plus to block endogenous feedback that inhibits POMC activity (naltrexone) (23,25). Trials found naltrexone/bupropion effective for obesity (25,26) leading to FDA-approval (22) and one trial found it significantly enhanced BWL outcomes for obesity (27). A pilot study reported that naltrexone/bupropion was well tolerated in patients with BED and a greater proportion attained weight loss relative to placebo (28). This study is a randomized double-blind placebo-controlled trial (RCT) designed to test the effectiveness of BWL and naltrexone/bupropion, alone and in combination, for BED with comorbid obesity.
METHODS
This single-site RCT protocol was approved by the Yale institutional review board and followed a data safety and monitoring plan with a physician safety officier. Participants provided written informed consent.
Participants
Participants (N=136), recruited via advertisements, were eligible if they met DSM-5 (1) criteria for BED, were 18–70 years old, and had a body mass index (BMI) ≥30.0 and ≤50.0 (or ≥27.0 with obesity-related comorbidity). Minimal exclusion criteria were used, comprising clinical issues that, regardless of setting, would dictate need for alternative treatment or represent contraindications to naltrexone/bupropion. Exclusionary criteria included: concurrent treatment for eating/weight disorders, taking contraindicated medications (e.g., opiates), uncontrolled medical conditions or contraindications to naltrexone/bupropion (e.g., seizure history, bulimia nervosa or anorexia nervosa history, cardiovascular disease, psychosis/bipolar disorder, systolic blood pressure>160mmHg, diastolic blood pressure>100mmHg, or heart rate>100 beats/minute), and pregnancy/breastfeeding.
The 136 participants had mean age of 46.5 (SD=12.2) years and mean BMI of 37.1 (SD=4.9); 81.6% (N=111) were female, 84.6% (N=115) attended/finished college, and 77.9% (N=106) were White. Table 1 summarizes the participants’ sociodemographic characteristics and Table 2 summarizes their clinical characteristics.
TABLE 1.
Demographic characteristics overall and across treatment conditions.
| Overall | Placebo | NB | BWL+Placebo | BWL+NB | Test statistic | p value | Effect size | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N=136 | n=34 | n=32 | n=35 | n=35 | |||||||||
|
| |||||||||||||
| Age, M (SD) | 46.50 | (12.23) | 46.94 | (12.57) | 46.03 | (11.95) | 46.00 | (11.87) | 46.99 | (12.98) | 0.07 | 0.98 | 0.002 |
| Sex (n, %) | 3.77 | 0.71 | 0.166 | ||||||||||
| Male | 22 | 16.2% | 6 | 17.6% | 5 | 15.6% | 5 | 14.3% | 6 | 17.1% | |||
| Female | 111 | 81.6% | 28 | 82.4% | 26 | 81.3% | 28 | 80.0% | 29 | 82.9% | |||
| Other | 3 | 2.2% | 0 | 0.0% | 1 | 3.1% | 2 | 5.7% | 0 | 0.0% | |||
| Race (n, %) | 9.26 | 0.41 | 0.261 | ||||||||||
| White | 106 | 77.9% | 26 | 76.5% | 25 | 78.1% | 26 | 74.3% | 29 | 82.9% | |||
| Black | 18 | 13.2% | 3 | 8.8% | 3 | 9.4% | 8 | 22.9% | 4 | 11.4% | |||
| Asian | 5 | 3.7% | 3 | 8.8% | 1 | 3.1% | 0 | 0.0% | 1 | 2.9% | |||
| Multiracial | 7 | 5.1% | 2 | 5.9% | 3 | 9.4% | 1 | 2.9% | 1 | 2.9% | |||
| Ethnicity (n, %) | 1.85 | 0.60 | 0.117 | ||||||||||
| Hispanic or Latinx | 20 | 14.7% | 4 | 11.8% | 7 | 21.9% | 5 | 14.3% | 4 | 11.4% | |||
| Not Hispanic or Latinx | 116 | 85.3% | 30 | 88.2% | 25 | 78.1% | 30 | 85.7% | 31 | 88.6% | |||
| Sexual Orientation (n, %) | 5.31 | 0.81 | 0.198 | ||||||||||
| Heterosexual | 125 | 91.9% | 30 | 88.2% | 29 | 90.6% | 33 | 94.3% | 33 | 94.3% | |||
| Gay or Lesbian | 4 | 2.9% | 2 | 5.9% | 0 | 0.0% | 1 | 2.9% | 1 | 2.9% | |||
| Bisexual | 4 | 2.9% | 1 | 2.9% | 2 | 6.3% | 0 | 0.0% | 1 | 2.9% | |||
| Other | 3 | 2.2% | 1 | 2.9% | 1 | 3.1% | 1 | 2.9% | 0 | 0.0% | |||
| Education (n, %) | 8.54 | 0.48 | 0.251 | ||||||||||
| High School | 21 | 15.4% | 7 | 20.6% | 5 | 15.6% | 4 | 11.4% | 5 | 14.3% | |||
| Some college | 40 | 29.4% | 9 | 26.5% | 6 | 18.8% | 14 | 40.0% | 11 | 31.4% | |||
| College | 32 | 23.5% | 10 | 29.4% | 7 | 21.9% | 5 | 14.3% | 10 | 28.6% | |||
| More than college | 43 | 31.7% | 8 | 23.5% | 14 | 43.8% | 12 | 34.3% | 9 | 25.7% | |||
| Age onset BED, mean (SD) | 28.32 | (13.40) | 25.45 | (13.53) | 29.94 | (13.41) | 28.29 | (13.48) | 29.70 | (13.31) | 0.77 | 0.52 | 0.018 |
Note: Test statistic = chi-square for categorical variables and ANOVAs for dimensional variables. P values are for two-tailed tests. Effect size = phi for categorical variables and eta squared for dimensional variables. BWL = behavioral weight loss. NB = naltrexone/bupropion. M = mean. SD = standard deviation. N = number. BED = binge-eating disorder.
TABLE 2.
Clinical measures across treatment conditions.
| Placebo | NB | BWL+Placebo | BWL+NB | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n=34 | n=32 | n=35 | n=35 | |||||||||
| n | M | SD | n | M | SD | n | M | SD | n | M | SD | |
|
| ||||||||||||
| EDE Binge Eating | ||||||||||||
| Pre-Treatment | 34 | 19.85 | 22.10 | 32 | 15.25 | 11.17 | 35 | 22.86 | 16.12 | 35 | 18.66 | 13.14 |
| Post-Treatment | 29 | 9.90 | 20.31 | 27 | 7.63 | 9.77 | 27 | 3.30 | 5.28 | 29 | 1.97 | 4.87 |
| Change | 29 | −6.83 | 9.41 | 27 | −7.63 | 15.73 | 27 | −18.89 | 16.24 | 29 | −16.34 | 14.96 |
| EDE-Q Binge Eating | ||||||||||||
| Pre-Treatment | 34 | 13.88 | 8.96 | 32 | 13.50 | 7.17 | 35 | 17.14 | 9.59 | 35 | 15.89 | 9.74 |
| Post-treatment | 29 | 8.11 | 12.39 | 27 | 6.59 | 7.37 | 27 | 3.96 | 6.25 | 29 | 1.96 | 3.64 |
| Change | 29 | −3.74 | 11.32 | 27 | −5.44 | 7.89 | 27 | −10.92 | 11.51 | 29 | −12.79 | 8.24 |
| Weight | ||||||||||||
| Pre-Treatment | 34 | 226.36 | 35.86 | 32 | 227.18 | 32.01 | 35 | 232.29 | 45.79 | 35 | 228.56 | 44.14 |
| Post-Treatment | 29 | 228.09 | 38.80 | 26 | 224.69 | 32.15 | 26 | 223.05 | 51.85 | 29 | 213.59 | 44.85 |
| Change | 29 | 2.58 | 10.07 | 26 | −5.28 | 12.96 | 26 | −9.48 | 12.52 | 29 | −13.11 | 13.77 |
| % Change | 29 | 1.05 | 4.26 | 26 | −2.11 | 5.41 | 26 | −4.42 | 5.70 | 29 | −5.71 | 5.85 |
| EDE Global Score | ||||||||||||
| Pre-Treatment | 34 | 2.59 | 1.01 | 32 | 2.5 | 0.68 | 35 | 2.66 | 0.92 | 35 | 2.71 | 0.89 |
| Post-Treatment | 28 | 1.92 | 0.88 | 27 | 2.18 | 0.87 | 27 | 2.03 | 0.99 | 29 | 1.48 | 0.85 |
| Change | 28 | −0.61 | 0.65 | 27 | −0.2301 | 0.74 | 27 | −0.73 | 0.72 | 29 | −1.23 | 0.95 |
| BDI-II Depression Score | ||||||||||||
| Pre-Treatment | 34 | 13.85 | 8.63 | 32 | 13.88 | 9.69 | 35 | 13.66 | 9.94 | 35 | 15.80 | 9.24 |
| Post-Treatment | 27 | 10.04 | 10.57 | 27 | 10.11 | 8.60 | 25 | 7.28 | 6.50 | 29 | 5.00 | 6.34 |
| Change | 27 | −4.44 | 9.09 | 27 | −4.04 | 5.65 | 25 | −7.12 | 10.95 | 29 | −11.59 | 7.66 |
| TFEQ Restraint Score | ||||||||||||
| Pre-Treatment | 34 | 8.53 | 4.23 | 32 | 9.84 | 4.57 | 35 | 7.63 | 4.39 | 35 | 8.83 | 4.35 |
| Post-Treatment | 27 | 9.11 | 4.89 | 27 | 9.19 | 4.36 | 25 | 13.68 | 3.45 | 29 | 14.28 | 4.70 |
| Change | 27 | 0.04 | 3.50 | 27 | −0.04 | 4.03 | 25 | 5.44 | 4.59 | 29 | 5.00 | 5.18 |
| TFEQ Disinhibition Score | ||||||||||||
| Pre-Treatment | 34 | 12.74 | 2.26 | 32 | 13.19 | 1.89 | 35 | 13.49 | 1.92 | 35 | 12.91 | 2.01 |
| Post-Treatment | 27 | 11.96 | 3.04 | 27 | 10.59 | 3.21 | 25 | 8.32 | 3.73 | 29 | 8.31 | 3.72 |
| Change | 27 | −0.78 | 2.42 | 27 | −2.19 | 2.76 | 25 | −5.32 | 3.60 | 29 | −4.66 | 3.27 |
| TFEQ Hunger Score | ||||||||||||
| Pre-Treatment | 34 | 9.18 | 4.01 | 32 | 10.38 | 3.07 | 35 | 10.26 | 3.22 | 35 | 9.69 | 3.11 |
| Post-Treatment | 27 | 7.93 | 3.76 | 27 | 7.70 | 4.20 | 25 | 5.44 | 4.02 | 29 | 5.31 | 3.68 |
| Change | 27 | −0.78 | 2.89 | 27 | −2.96 | 3.41 | 25 | −4.88 | 4.24 | 29 | −4.07 | 3.49 |
| FCI Score | ||||||||||||
| Pre-Treatment | 34 | 1.69 | 0.78 | 32 | 1.80 | 0.64 | 35 | 1.72 | 0.65 | 35 | 1.75 | 0.58 |
| Post-Treatment | 27 | 1.25 | 0.56 | 27 | 1.22 | 0.48 | 25 | 0.91 | 0.56 | 29 | 0.96 | 0.69 |
| Change | 27 | −0.26 | 0.43 | 27 | −0.54 | 0.52 | 25 | −0.85 | 0.73 | 29 | −0.76 | 0.67 |
| PFS Score | ||||||||||||
| Pre-Treatment | 34 | 56.09 | 12.03 | 32 | 55.44 | 12.29 | 35 | 59.11 | 13.65 | 35 | 57.60 | 10.77 |
| Post-Treatment | 27 | 48.89 | 13.54 | 27 | 45.59 | 13.26 | 25 | 38.04 | 12.79 | 29 | 37.55 | 14.14 |
| Change | 27 | −5.67 | 9.73 | 27 | −8.93 | 11.86 | 25 | −21.48 | 10.19 | 29 | −19.66 | 14.67 |
| Cholesterol Total | ||||||||||||
| Pre-Treatment | 34 | 194.65 | 36.88 | 32 | 199.69 | 43.11 | 34 | 203.88 | 50.95 | 33 | 195.79 | 36.27 |
| Post-Treatment | 28 | 201.21 | 32.97 | 26 | 196.15 | 31.54 | 26 | 199.08 | 38.97 | 29 | 188.72 | 28.64 |
| Change | 28 | 0.89 | 23.96 | 26 | 1.77 | 19.53 | 26 | −5.65 | 33.61 | 27 | −14.81 | 23.80 |
| HDL | ||||||||||||
| Pre-Treatment | 34 | 54.24 | 15.11 | 32 | 55.50 | 12.08 | 34 | 52.26 | 13.56 | 33 | 55.27 | 12.83 |
| Post-Treatment | 28 | 53.18 | 16.53 | 26 | 54.38 | 10.90 | 26 | 49.54 | 9.25 | 29 | 53.93 | 13.20 |
| Change | 28 | −1.75 | 7.59 | 26 | 0.04 | 5.77 | 26 | −2.42 | 8.97 | 27 | −4.22 | 8.01 |
| LDL | ||||||||||||
| Pre-Treatment | 34 | 116.71 | 31.96 | 32 | 122.47 | 32.81 | 33 | 126.21 | 38.41 | 33 | 118.27 | 26.99 |
| Post-Treatment | 28 | 123.61 | 26.71 | 26 | 119.00 | 25.79 | 25 | 126.92 | 32.44 | 29 | 114.28 | 24.25 |
| Change | 28 | 1.96 | 18.46 | 26 | 0.12 | 16.69 | 25 | 1.36 | 23.49 | 27 | −9.44 | 16.92 |
| HbA1c | ||||||||||||
| Pre-Treatment | 34 | 5.47 | 0.51 | 32 | 5.40 | 0.39 | 34 | 5.47 | 0.39 | 34 | 5.46 | 0.50 |
| Post-Treatment | 28 | 5.41 | 0.36 | 26 | 5.35 | 0.41 | 25 | 5.37 | 0.40 | 29 | 5.30 | 0.23 |
| Change | 28 | 0.01 | 0.17 | 26 | −0.06 | 0.21 | 25 | −0.12 | 0.22 | 28 | −0.16 | 0.30 |
Note: EDE = Eating Disorder Examination Interview; EDE-Q = Eating Disorder Examination – Questionnaire; BDI-II = Beck Depression Inventory-II; TFEQ = Three Factor Eating Questionnaire; FCI = Food Craving Inventory; PFS = Power of Food Scale; HbA1c = glycated hemoglobin A1c (%); BWL = behavioral weight loss; NB = naltrexone/bupropion; N = number; M = mean; SD = standard deviation.
Assessments
Assessment procedures were performed by doctoral-level research-clinicians who were monitored throughout the study. Primary outcomes (binge-eating, measured weight) and secondary outcomes were assessed using a battery of established interviews, self-reports, and laboratory-tests selected to assess specific eating/weight disorder constructs and associated psychological and metabolic variables.
The Eating Disorder Examination-Interview (EDE; 16th-edition; 29) was administered to diagnose BED and assess binge-eating frequency and eating-disorder psychopathology at baseline and post-treatment. This interview, often used as a primary measure in eating-disorder RCTs (9), has good inter-rater/test-retest reliability in BED (30); the global score (alpha =0.81) reflects eating-disorder psychopathology. In this study, inter-rater (N=50) reliability of EDE was excellent; intra-class correlation coefficients (ICC) were 0.91 (95% CI 0.844–0.950) for binge-eating frequency and 0.98 (95% CI 0.969–0.990) for the global score.
Weight and height were measured at baseline and weight was measured monthly and at post-treatment. Fasting cholesterol (total, HDL, and LDL) and glycated hemoglobin A1c (HbA1c; average glucose control previous 3 months) were obtained at baseline and post-treatment.
A battery of self-report measures was completed at baseline, monthly, and posttreatment. The Eating Disorder Examination-Questionnaire, which has good test-retest reliability (32), obtained binge-eating frequency data during the past 28 days. The Beck Depression Inventory-II (alpha=0.91) is a well-established measure of depression symptoms/levels (33). The Three-Factor Eating Questionnaire (alpha=0.72) measures eating behaviors (cognitive restraint, disinhibition, and hunger); it is validated and shows differential responses across treatments consistent with putative mechanisms (34). The Food Craving Inventory (alpha=0.90) is a measure of cravings for specific foods and is validated in BED (35). The Power of Food Scale (alpha=0.93) assesses psychological drive to consume palatable foods; it measures appetite (not consumption) for palatable foods and is validated (36).
Randomization
Participants were randomized to one of four treatments (balanced 2-by-2 factorial design) for 16 weeks: placebo, naltrexone/bupropion, BWL+placebo, or BWL+naltrexone/bupropion. Randomization, without stratification, assigned participants to the four treatments in blocks of eight (to obviate secular trends and ensure approximately equal proportions). A biostatistician developed the randomization schedule, which was concealed prior to each randomization. Medication was double-blind; naltrexone/bupropion and placebo were prepared in capsules and matched in frequency and appearance by Yale Investigational Drug Service. Randomization assignment to BWL conditions was kept blinded from participants until treatment started. Assessors of posttreatment outcomes were blinded to whether participants received BWL in addition to the (double-blind) medication. Participants were reminded before each assessment not to disclose any details about treatments during meetings with assessors.
Treatments
Behavioral Weight Loss Therapy (BWL).
BWL followed the protocol developed/refined originally for obesity trials (37) and since adapted for BED (12,13). BWL was delivered in individual 45-minute sessions following the manualized protocol. Participants were given patient-version manuals covering all the BWL information and components. Weekly homework assignments were keyed to specific material to reinforce learning and using behavioral techniques. BWL focuses on gradual behavioral lifestyle changes, including moderate caloric decreases (approximate goals of 1500kcal/day), improved nutrition quality (<30% fat), and moderate physical activity (30 minutes/five times weekly). Behavioral techniques include goal setting, monitoring food intake and physical activity, stimulus control to achieve/maintain the lifestyle changes, and problem-solving skills to overcome challenges.
BWL was delivered by 11 research-clinicians with programmatic interests in eating disorders and obesity; six were clinical psychology graduate students (M=4.3 (SD=1.4) years graduate education) and five were postdoctoral psychologists (M=8.0 (SD=0.7) years graduate education). Clinicians received intensive training in the manualized protocols and were supervised weekly (including reviews of recorded sessions) by the investigators to monitor quality and adherence. Supervision included review of the structure, process, and content of sessions to ensure fidelity and to prevent drift, per previous trials (12,13).
Medication (Naltrexone/Bupropion or Placebo)).
Naltrexone/bupropion comprised naltrexone-sustained-release (32 mg/day) combined with bupropion-sustained-release (360 mg/day); two tablets taken twice daily, each containing 8mg naltrexone and 90mg bupropion. Placebo was given in capsules matched in appearance and frequency. Naltrexone/bupropion dosing began with a quarter of full-dose and was increased weekly until achieving the full-dose by the fourth week (26,27). If patients developed intolerable side-effects, the study physician reduced dosing to achieve tolerability; if patients experienced adverse events and/or could not tolerate the medication, they were withdrawn from medication.
Two faculty-level study physicians delivered the pharmacotherapy focused on medication management (addressing compliance, safety, and side-effects). Additional psychotherapeutic interventions were proscribed. Medication adherence and detailed side-effect and safety checklists were performed monthly. Monthly medication refills were accompanied by re-review of medication compliance and dosing schedules and pill bottles were returned for pill counts at post-treatment.
Statistical Analysis
Sample size was based on power calculations using data from RCTs testing BWL for BED (11,12), placebo for BED (14,15) and naltrexone/bupropion for weight-loss (25,26). Although some reported effects sizes were in the medium-to-large ranges, we conservatively powered this RCT to detect medium effects after considering clinically meaningful effect sizes and performing sensitivity analyses for different outcomes. A sample of N=140, allocated to four treatment conditions, yielded greater than 80% power for medium effect sizes (f=0.25) for main effects for BWL and naltrexone/bupropion treatments and for interaction effects between BWL and naltrexone/bupropion at two-sided alpha level of 0.05., even after assuming 20% attrition.
Analyses to compare treatments were all intention-to-treat and were performed for all randomized patients who attended the first treatment session. The two co-primary outcome variables were binge eating and weight loss, both analyzed using complementary approaches. Binge eating was analyzed as continuous and categorical outcomes (i.e., monthly frequency and remission, respectively). “Remission” from binge eating was defined as zero episodes during the previous 28 days (on the Eating Disorder Examination-Interview) with any missing data imputed as failure (i.e., non-remission). Weight-loss (measured) was analyzed as continuous and categorical outcomes (i.e., percent weight-loss and attaining 5% weight loss, respectively). 5% weight loss category was based on measured weight loss from baseline with missing data imputed as failure; this is a common outcome in obesity trials (26,27,37) because it is associated with clinical benefits (38). Secondary treatment outcomes were eating-disorder psychopathology (Eating Disorder Examination Global), depression (Beck Depression Inventory-II), eating behaviors (Three Factor Eating Questionnaire, Food Craving Inventory, Power of Food Scale), and cardiometabolic/endocrine variables (cholesterol, Hb1Ac).
For analyses of continuous measures, intention-to-treat analyses used all available data in mixed models without imputation. Variables not conforming to normality were log-transformed prior to analysis. Mixed effects models (39) were fitted with fixed factors including BWL treatment (yes vs. no), medication (naltrexone/bupropion vs. placebo), time (all relevant time points of baseline, month 1, month 2, month 3, post-treatment), and all possible interactions. In each model, we considered different error structures and selected the best-fitting structure using the Schwartz’ Bayesian Criterion. Focused comparisons of least square means (effect slices) were used to explain significant effects in the models. Statistical testing was performed at 0.05 significance level.
For categorical outcomes (e.g., binge-eating remission, 5% weight loss), logistic regression tested the outcomes assessed at post-treatment. The independent variables were the two treatments (BWL and medication, each at two levels) and their interaction. Odds ratios and 95% confidence intervals were used to explain significant effects in the models.
We explored whether time of measurement (before or during the COVID pandemic; in-person versus remote visit) affected the results by including an indicator for timing of measurement as a covariate. The results did not change substantively and therefore the final models are not adjusted for COVID.
RESULTS
Randomization and Participant Characteristics
Figure 1 (CONSORT) summarizes participant flow throughout the study. Of the 2648 respondents screened, 289 consented and were evaluated for eligibility, and 136 were randomized and attended baseline. Of the 136 participants, N=34 received placebo, N=32 received naltrexone/bupropion, N=35 received BWL+placebo, and N=35 received BWL+naltrexone/bupropion. Post-treatment assessments were obtained for 82.4% of participants; rates did not differ significantly across treatments.
Figure 1. Participant flow throughout the study.
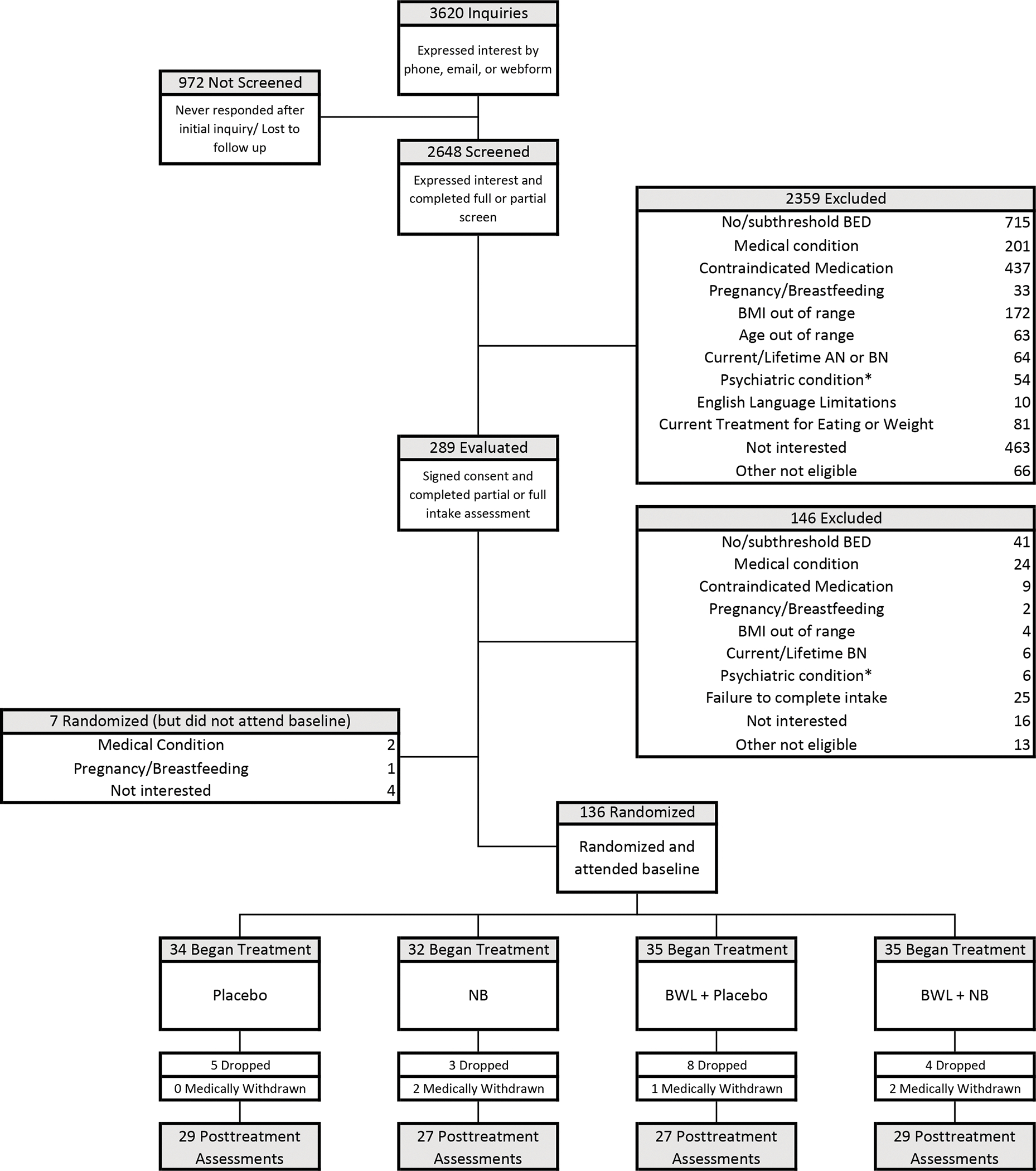
AN = anorexia nervosa; BN = bulimia nervosa; BED = binge-eating disorder; NB=naltrexone/bupropion; BWL=behavioral weight loss; BMI = body mass index.
*Psychiatric condition: participants reporting serious mental illness such as psychosis, bipolar disorder, and current substance use disorder were excluded.
Primary Outcomes
Table 2 shows descriptive statistics for co-primary outcomes (binge-eating and weight-loss) and Figures 2–3 summarize analyses for continuous and categorical variables; Supplemental Table 1 shows the test statistics and p-values for all the main and interaction effects in the mixed models for the co-primary continuous outcomes.
Figure 2. Binge-eating outcomes across treatment conditions.
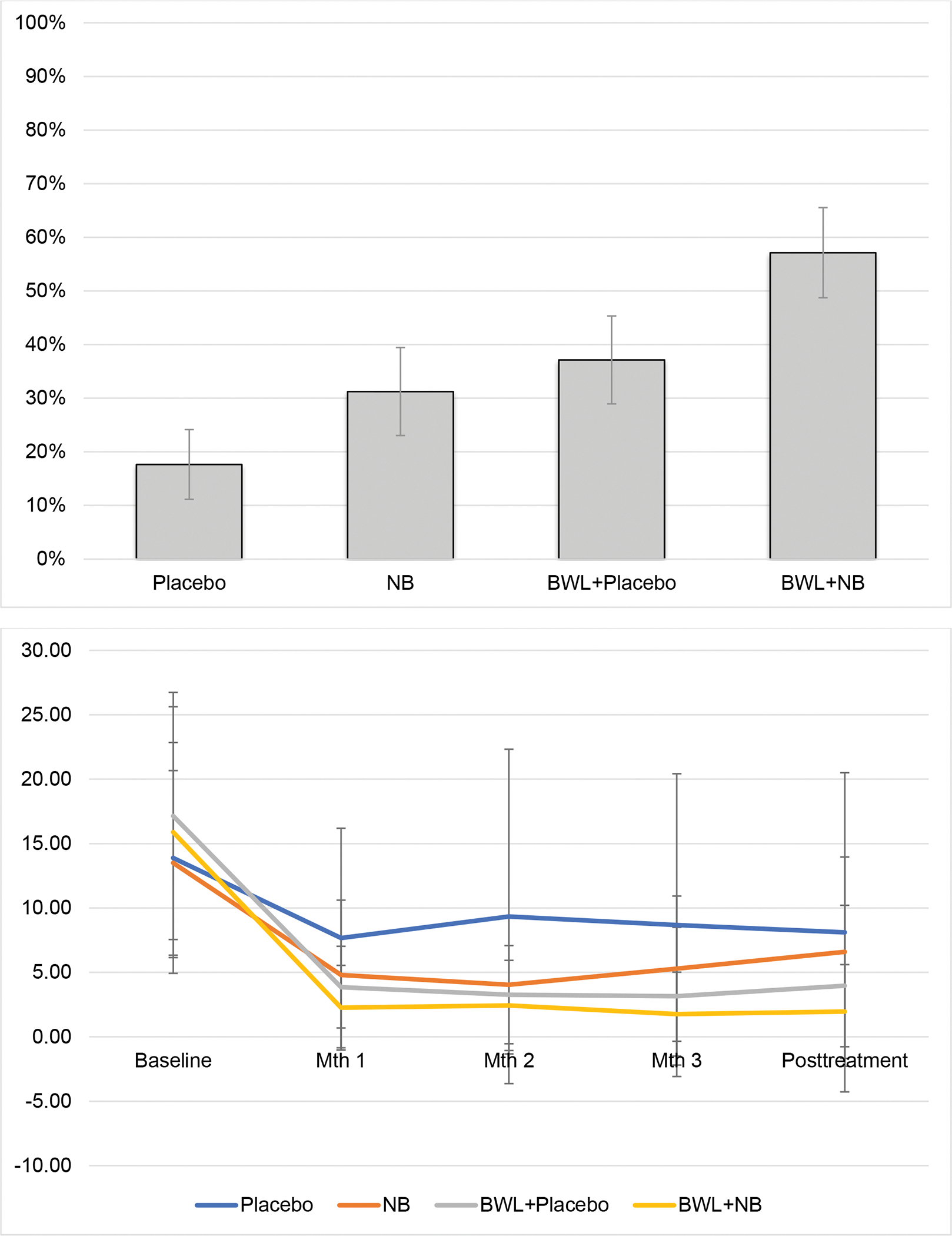
Figure 2-A (top panel).
Binge-eating remission rates at posttreatment across treatment conditions. Remission rates are defined as zero episodes of binge eating during the last 28 days assessed using the Eating Disorder Examination-Interview. The rates are based on the intention-to-treat sample (N=136) with any missing data imputed as failure to remit. BWL was associated with significantly higher remission rates than no-BWL (p=0.006; Odds Ratio=2.84, 95% Confidence Interval 1.34–6.03). Naltrexone/bupropion was associated with significantly higher remission rates than placebo (p=0.04; Odds Ratio=2.19, 95% Confidence Interval 1.03–4.63). NB = naltrexone/bupropion; BWL = behavioral weight loss
Figure 2-B (bottom panel).
Frequency of binge eating during the last 28 days assessed monthly using the Eating Disorder Examination-Questionnaire. BWL was associated with significantly lower binge-eating frequency at all post-baseline timepoints compared to no-BWL (all ps<0.02). Naltrexone/bupropion was associated with significantly lower binge-eating frequency than placebo only at months 1 and 2 (ps<0.02) but not at month 3 or at posttreatment (ps>0.16). Mth = Month; NB = naltrexone/bupropion; BWL = behavioral weight loss
Figure 3. Percent weight loss across the treatments.
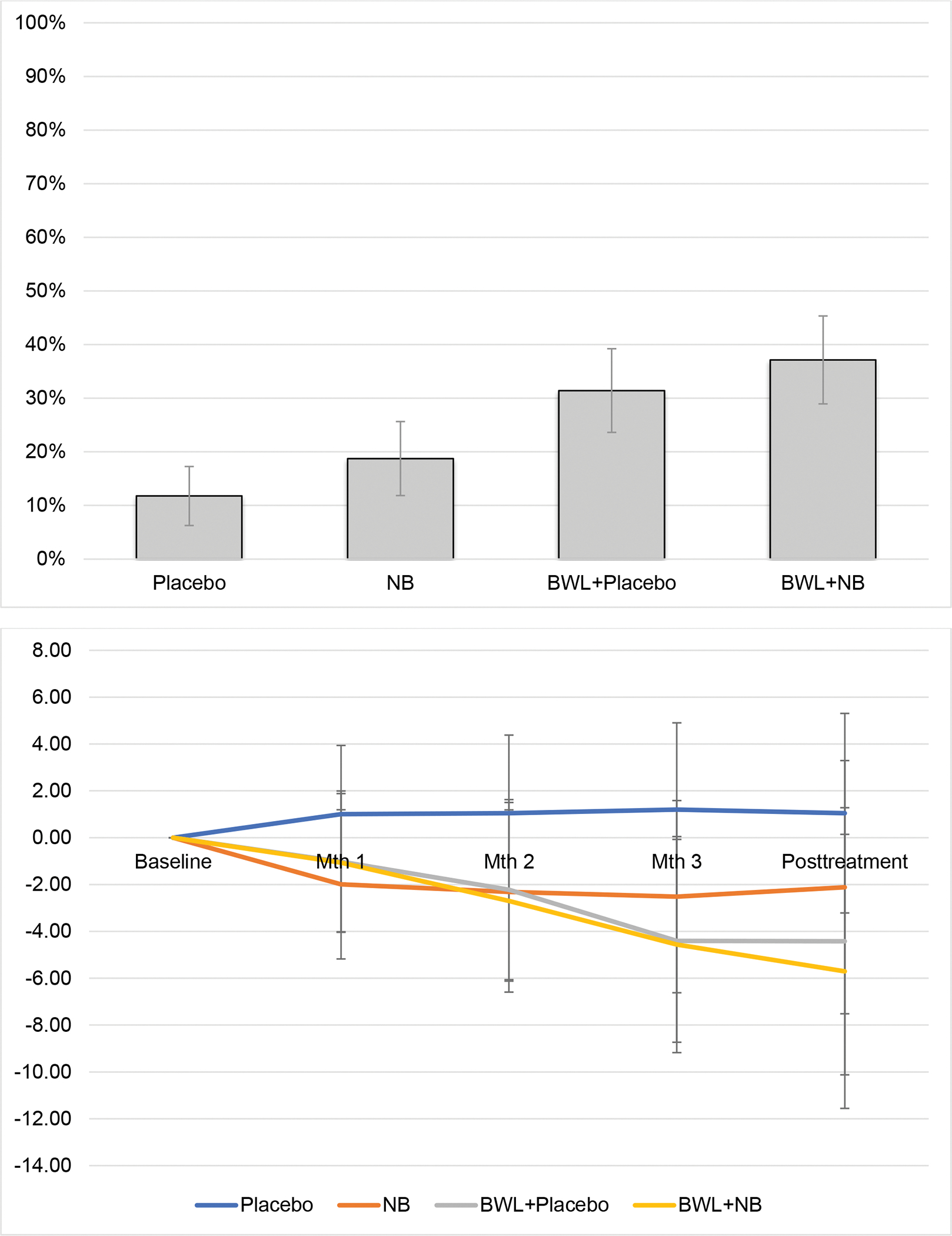
Figure 3-A (top panel).
Proportion of patients attaining 5% weight loss or greater (from baseline) calculated using measured values at post-treatment. The frequencies are based on the intention-to-treat sample (N=136) with any missing data imputed as failure to attain 5% weight loss. BWL was associated with significantly higher proportion of patients with 5% weight loss than no-BWL (p=0.01; Odds Ratio=2.97, 95% Confidence Interval 1.27–6.91). Naltrexone/bupropion was not associated with significantly higher remission rates than placebo (p=0.35). NB = naltrexone/bupropion; BWL = behavioral weight loss
Figure 3-B (bottom panel).
Percent weight loss (from baseline) calculated using measured values at baseline, measured monthly during treatment, and measured at post-treatment. BWL was associated with greater percent weight loss than no-BWL at month 2, month 3, and at post-treatment (all ps <0.01). Naltrexone/bupropion was not associated with significantly greater percent weight loss than placebo (p=0.32). Mth = Month; NB = naltrexone/bupropion; BWL = behavioral weight loss
Figure 2-A illustrates intention-to-treat binge-eating remission rates at post-treatment by treatment condition. Remission rates were: 17.7% for placebo, 31.3% for naltrexone/bupropion, 37.1% for BWL+placebo, and 57.1% for BWL+naltrexone/bupropion. Logistic regression revealed significant main effects of BWL (Chi-sq(1)=7.45, p=0.006) and of medication (Chi-sq(1)=4.18, p=0.04) but no significant BWL-by-medication interaction (Chi-sq(1)=0.007, p=0.94). BWL (compared to no-BWL) was associated with nearly three times higher odds of remission (OR=2.84, 95% CI: 1.34, 6.03) whereas naltrexone/bupropion (compared to placebo) was associated with roughly two times higher odds of remission (OR=2.19, 95% CI: 1.03, 4.63).
Mixed models analyses of binge-eating frequency (episodes during the past month) at post-treatment (Eating Disorder Examination-Interview) revealed a significant interaction between BWL and time (F(1,111)=24.34, p<0.0001) and a significant main effect of time (F(1,111)=239.39, p<0.0001). Medication effects were not statistically significant (see Supplemental Table for full results). Binge-eating frequency decreased significantly from baseline to post-treatment for BWL (F(1,110)=16.01, p<0.0001) but not for no-BWL (F(1,132)=3.30, p=0.07).
Figure 2-B summarizes frequency of binge-eating (during the past month) assessed monthly throughout the course of treatment. Mixed models revealed significant interactions between BWL and time (F(4,407)=5.99, p<0.0001) and between medication and time (F(4,407)=2.57, p=0.04) but the three-way interaction was not significant (p=0.37). The main effect of time was also significant (F(4,407)=92.84, p<0.0001). BWL was associated with significantly lower frequency at all post-baseline timepoints compared to no-BWL (ps<0.02), whereas naltrexone/bupropion was associated with significantly lower frequency at months 1 and 2 (ps<0.02) but not at month 3 or post-treatment (ps>0.16) compared to placebo.
Figure 3-A shows intention-to-treat rates of participants attaining 5% or greater weight loss at post-treatment by treatment condition. Rates attaining 5% weight loss were: 11.8% for placebo, 18.8% for naltrexone/bupropion, 31.4% for BWL+placebo, and 37.1% for BWL+ naltrexone/bupropion. Logistic regression revealed a significant main effect of BWL (Chi-sq(1)=6.36, p=0.01) but no significant main effect of medication (Chi-sq(1)=0.87, p=0.35) nor significant BWL-by-medication interaction (Chi-sq(1)=0.12, p=0.73). BWL had three times higher odds than no-BWL of attaining 5% weight loss (OR=2.97, 95% CI: 1.27, 6.91).
Figure 3-B summarizes percent weight loss throughout the course of the treatments and Table 2 shows weight values at baseline and post-treatment and changes. Mixed models of percent weight loss revealed a significant interaction between BWL and time (F(3,111)=10.70, p<0.0001) and a significant main effect of time (F(3,111)=12.56, p<0.0001) but no significant interaction between medication and time (F(3,11)=0.58, p=0.63) and no significant three-way interaction (p=0.32). Comparisons between BWL and no-BWL (p-values<0.01) were significant at posttreatment and at all monthly time-points except month one.
Secondary Outcomes
Table 2 shows descriptive statistics for secondary outcomes of eating-disorder psychopathology, depression, eating behaviors, and metabolic variables across treatments.
For eating-disorder psychopathology, mixed models of Eating Disorder Examination global scores revealed a significant three-way interaction between BWL, medication, and time (F(4,114)=9.98, p=0.002), a significant interaction between BWL and time (F(1,114)=12.59, p=0.0006), and a significant main effect of time (F(1,114)=94.61, p<0.0001). Significantly greater decreases in eating-disorder psychopathology occurred in BWL than no-BWL (p=0.02).
Mixed models of depression scores revealed a significant interaction between BWL and time (F(4,405)=3.35, p=0.01) and a significant main effect of time (F(4,405)=24.53, p<0.0001). Depression scores decreased significantly more in BWL than no-BWL, with the difference statistically significant at later monthly time-points and post-treatment (ps< 0.04).
Mixed models of eating behaviors measured by the Three Factor Eating Questionnaire (restraint, disinhibition, and hunger scales) revealed consistent patterns of significantly greater improvements with BWL than no-BWL. For each of the three scales, there were significant interactions between BWL and time (F(2,225)=23.87, p<0.0001; F(2,234)=17.66, p<0.0001; and F(2,226)=9.02, p=0.0002, respectively) and significant main effects of time (F(2,225)=22.45, p<0.0001; F(2,234)=64.52, p<0.0001; and F(2,226)=53.00, p<0.0001, respectively), but non-significant medication effects. Mixed models of other eating behaviors (craving [Food Craving Inventory] and drive to consume palatable foods [Power of Food Scale]) also revealed consistent patterns of significantly greater improvements with BWL than no-BWL. There were significant interactions between BWL and time (F(2,219)=5.12, p=0.007 and F(2,225)=18.61, p<0.0001, respectively, for the craving and drive to consume foods) and significant main effects of time (F(2,219)=72.31, p<0.0001; F(2,225)=97.29, p<0.0001), but non-significant medication effects.
Mixed models of total cholesterol revealed a significant interaction between BWL and time (F(1,107)=4.66, p=0.03) but not for medication by time; mixed models for cholesterol components of HDL and LDL, however, did not reveal significant effects. Mixed models of HbA1c revealed a significant interaction between BWL and time (F(1,106)=5.85, p=0.02) and a significant main effect of time (F(1,106)=15.51, p=0.0001), but there were no significant medication effects.
DISCUSSION
In this study of adults with BED and obesity, BWL and naltrexone/bupropion were associated with significant improvements, with a consistent pattern of BWL being superior to no-BWL. Co-primary outcomes were binge eating (i.e., attaining remission and frequency) and weight loss (i.e., attaining 5% weight loss and % loss). For binge-eating remission, BWL was significantly superior to no-BWL, naltrexone/bupropion was significantly superior to placebo, but there was no significant interaction between BWL and medication. For binge-eating frequency, analyses using complementary measures revealed BWL was significantly superior to no-BWL, but that naltrexone/bupropion was not significantly superior to placebo nor was the interaction between BWL and medication significant. For weight loss, analyses of rates attaining 5% weight loss and of percent weight-loss both converged revealing that BWL was significantly superior to no-BWL, but that naltrexone/bupropion was not superior to placebo nor was there a significant interaction between BWL and medication. Analyses of secondary measures converged indicating BWL, but not naltrexone/bupropion, was associated with significant improvements across broad outcomes (eating-disorder psychopathology, depression, eating behaviors, cholesterol, and Hb1Ac).
Findings provide further support for the effectiveness of BWL for BED, extending previous studies of BWL (11,12,13) in important ways. First, the superiority of BWL in this study supports the “specificity” of the effectiveness of BWL (i.e., statistical superiority over a credible pharmacologic treatment) (9). Second, the effectiveness of BWL for BED was observed across broad outcomes reflecting eating, psychological, and metabolic clinical domains. Finally, the significant weight-loss findings (means of −5.7% for both BWL+placebo and for BWL+naltrexone/bupropion, with 31.4% and 37.1% of patients attaining 5% or greater weight loss) approximate closely the findings reported for BWL (without pharmacotherapy) for BED in recent trials (11,12,13). These findings are encouraging given the well-known difficulty in producing weight loss in patients with BED and comorbid obesity (9,18,20). In comparing our 16-week findings to those of a similar, albeit substantially longer (56-week), trial for obesity without BED (27), the 5.7% weight loss for BWL+placebo approximates their 4.9% weight loss whereas the 5.7% for BWL+naltrexone/bupropion was less than their 7.8% weight loss (27).
Findings provide support for the potential effectiveness of naltrexone/bupropion for BED. Binge-eating remission rates (31.3%) with naltrexone/bupropion, which had roughly two times higher odds of remission than placebo, approximated the 36%–40% rates reported for lisdexamfetamine (15), the sole FDA-approved medicine for BED. Unlike lisdexamfetamine, which is not indicated for obesity, naltrexone/bupropion is FDA-approved for obesity, and this study employed fewer exclusionary criteria than lisdexamfetamine trials (14,15). In terms of weight-loss, however, naltrexone/bupropion did not differ significantly from placebo and the observed 2.1% weight-loss was lower than the 6.1% reported for obesity without BED (26).
Analyses revealed non-significant interaction effects between BWL and naltrexone/bupropion, which converges with prior BED studies testing other medications combined with various psychotherapies (18), except topiramate (17). Future research should perform comparative tests of different medications, and of psychological versus pharmacological approaches, designed with a priori tests of moderators of outcomes.
Study strengths include manualized behavior therapy and pharmacotherapy delivered by trained/monitored psychologists/physicians, independent assessments using well-validated measures, minimal exclusionary criteria to enhance generalizability, and good retention. Several study limitations are noteworthy. Generalizability of findings to different settings or persons with different sociodemographic/clinical characteristics is uncertain. The sample size had limited power to detect smaller magnitude main or interaction effects of treatments. We did not include a BWL-only condition (without placebo). Longer-term outcomes of these acute findings are unknown. Whether variations in clinicians’ adherence or patients’ compliance with the behavioral/pharmacologic interventions moderate outcomes is unknown. With these strengths and limitations as context, we conclude BWL and naltrexone/bupropion were associated with significant improvements in patients with BED and obesity, with BWL demonstrating superior improvements.
Supplementary Material
Funding:
National Institutes of Health grant R01 DK49587 (Grilo), K23 DK115893 (Lydecker) and UL1 TR001863. The investigators sought funding from the NIDDK for this study because of that NIH institute’s interest in both binge-eating disorder (a psychiatric and behavioral mental health concern) and obesity (a metabolic and medical concern). The funding agency (National Institutes of Health and the Public Health Service) played no role in the content of this paper.
Footnotes
Potential Conflicts of interest: The authors declare no conflicts of interest. Dr. Grilo reports broader interests, which did not influence this research, including Honoraria for lectures, and Royalties from Guilford Press and Taylor & Francis Publishers for academic books.
Clinicaltrials.gov registration: NCT03045341
(Behavioral and Pharmacologic Treatment of Binge Eating and Obesity: Acute Treatment)
Contributor Information
Carlos M. Grilo, Department of Psychiatry, Yale University School of Medicine, New Haven
Janet A. Lydecker, Department of Psychiatry, Yale University School of Medicine, New Haven
Sarah K. Fineberg, Department of Psychiatry, Yale University School of Medicine, New Haven
Jorge O. Moreno, Department of Internal Medicine, Yale University School of Medicine, New Haven
Valentina Ivezaj, Department of Psychiatry, Yale University School of Medicine, New Haven
Ralitza Gueorguieva, Department of Biostatistics, Yale School of Public Health, New Haven
Data Sharing:
De-identified data will be provided in response to reasonable written request to achieve goals in an approved written proposal.
REFERENCES
- 1.American Psychiatric Association: Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association, 2013 [Google Scholar]
- 2.Kessler RC, Berglund PA, Chiu WT, et al. : The prevalence and correlates of binge eating disorder in the World Health Organization World Mental Health Surveys. Biol Psychiatry 2013;73:904–914 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Streatfeild J, Hickson J, Austin SB, et al. : Social and economic cost of eating disorders in the United States: evidence to inform policy. Int J Eat Disord 2021;54:851–868 [DOI] [PubMed] [Google Scholar]
- 4.Udo T, Grilo CM: Prevalence and correlates of DSM-5-defined eating disorders in a nationally representative sample of US adults. Biol Psychiatry 2018;84:345–354 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Udo T, Grilo CM: Psychiatric and medical correlates of DSM-5 eating disorders in a nationally representative sample of adults in the United States. Int J Eat Disord 2019;52:42–50 [DOI] [PubMed] [Google Scholar]
- 6.Hudson JI, Lalondie JK, Coit CE, et al. : Longitudinal study of the diagnosis of components of the metabolic syndrome in individuals with binge-eating disorder. Am J Clin Nutr 2010:91:1568–1573 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Balodis IM, Grilo CM, Potenza MN: Neurobiological features of binge eating disorder. CNS Spectr 2015:20:557–565 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Coffino JA, Udo T, Grilo CM: Rates of help-seeking in U.S. adults with lifetime DSM-5 eating disorders: Prevalence across diagnoses and sex and ethnic/racial differences. Mayo Clin Proc 2019;94:1415–1426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hilbert A, Petroff D, Herpertz S, et al. : Meta-analysis of the efficacy of psychological and medical treatments for binge-eating disorder. J Consult Clin Psychol 2019;87:91–105 [DOI] [PubMed] [Google Scholar]
- 10.McElroy SL: Pharmacologic treatments for binge-eating disorder. J Clin Psychiatry 2017;78S1:14–19 [DOI] [PubMed] [Google Scholar]
- 11.Wilson GT, Wilfley DE, Agras WS, et al. : Psychological treatments of binge eating disorder. Arch Gen Psychiatry 2010;67:94–101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Grilo CM, Masheb RM, Wilson GT, et al. : Cognitive-behavioral therapy, behavioral weight loss, and sequential treatment for obese patients with binge-eating disorder: a randomized controlled trial. J Consult Clin Psychol 2011;79:675–685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Grilo CM, White MA, Masheb RM, et al. : Randomized controlled trial testing the effectiveness of adaptive “SMART” stepped-care treatment for adults with binge-eating disorder comorbid with obesity. Am Psychologist 2020;75:204–218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McElroy SL, Hudson JI, Mitchell JE, et al. : Efficacy and safety of lisdexamfetamine dimesylate for treatment of adults with moderate to severe binge-eating disorder: a randomized clinical trial. JAMA Psychiatry 2015;72:235–46 [DOI] [PubMed] [Google Scholar]
- 15.McElroy SL, Hudson J, Ferreira-Cornwell M, et al. : Lisdexamfetamine dimesylate for adults with moderate to severe binge-eating disorder: Results of two pivotal phase 3 randomized controlled trials. Neuropsychopharm 2016;41:1251–60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.McElroy SL, Arnold LM, Shapira NA, et al. : Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2007;160:255–61 [DOI] [PubMed] [Google Scholar]
- 17.Claudino AM, de Oliveira IR, Appolinario JC, et al. : Double-blind, randomized, placebo-controlled trial of topiramate plus cognitive-behavior therapy in binge-eating disorder. J Clin Psychiatry 2007;68:1324–32 [DOI] [PubMed] [Google Scholar]
- 18.Reas DL, Grilo CM: Psychotherapy and medications for eating disorders: better together? Clin Ther 2021;43:19–39 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cardel MI, Newsome FA, Pearl RL, et al. : Patient centered care for obesity: how health care providers can treat obesityy while actively addressing weight stigma and eating disorder risk. J Acad Nutr Diet 2022; Jan 13:S2212–2672(22)00007–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Blaine B, Rodman J: Responses to weight loss treatment among obese individuals with and without BED: matched-study meta-analysis. Eat Weight Disord 2007;12:54–60 [DOI] [PubMed] [Google Scholar]
- 21.Grilo CM, Masheb RM, Salant SL: Cognitive behavioral therapy guided self-help and orlistat for the treatment of binge eating disorder: a randomized, double-blind, placebo-controlled trial. Biol Psychiatry, 2005;57:1193–1201 [DOI] [PubMed] [Google Scholar]
- 22.Yanovski SZ, Yanovski JA: Naltrexone extended-release plus bupropion extended-release for treatment of obesity. JAMA, 2015;313:1213–1214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Billes SK, Greenway FL: Combination therapy with naltrexone and bupropion for besity. Expert Opin Pharmacother 2011;12:1813–26 [DOI] [PubMed] [Google Scholar]
- 24.Cowley MA, Smart JL, Rubinstein M, et al. : Leptin activates anorexigenic POMC neurons through neural network in the arcuate nucleus. Nature 2001;411(6836):480–484 [DOI] [PubMed] [Google Scholar]
- 25.Greenway FL, Dunayevich E, Tollefson G, et al. : Comparison of combined bupropion and naltrexone therapy for obesity with monotherapy and placebo. J Clin Endocrinol Metabol 2009;94:4898–906 [DOI] [PubMed] [Google Scholar]
- 26.Greenway FL, Fujioka K, Plodkowski RA, et al. : Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multi-centre randomized double-blind placebo-controlled phase 3 trial. Lancet 2010;376:595–605 [DOI] [PubMed] [Google Scholar]
- 27.Wadden TA, Foreyt JP, Foster GD, et al. : Weight loss with naltrexone SR/bupropion SR combination therapy as an adjunct to behavior modification: the COR-BMOD trial. Obesity 2011;19:110–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Grilo CM, Lydecker JA, Morgan PT, et al. : Naltrexone + bupropion combination for the treatment of binge-eating disorder with obesity: a randomized controlled pilot study. Clin Ther 2021;43:112–122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Fairburn CG, Cooper Z, O’Connor M: Eating Disorder Examination (16.0D). In Fairburn CG. Cognitive Behavior Therapy and Eating Disorders. NY: Guilford Press, 2008 [Google Scholar]
- 30.Grilo CM, Masheb RM, Lozano-Blanco C, et al. : Reliability of the Eating Disorder Examination in patients with binge eating disorder. Int J Eat Disord 2004;35:80–85 [DOI] [PubMed] [Google Scholar]
- 31.Grilo CM, Masheb RM, Wilson GT: A comparison of different methods for assessing the features of eating disorders in patients with binge eating disorder. J Consult Clin Psychol 2001;69:317–322 [DOI] [PubMed] [Google Scholar]
- 32.Reas DL, Grilo CM, Masheb RM: Reliability of the eating disorder examination-questionnnaire in patients with binge eating disorder. Behav Res Ther 2006;44:43–51 [DOI] [PubMed] [Google Scholar]
- 33.Beck AT, Steer R, Garbin M: Psychometric properties of the Beck Depression Inventory: 25 years of evaluation. Clin Psychol Rev 1998;8:77–100 [Google Scholar]
- 34.Stunkard AJ, Messick S: The three-factor eating questionnaire to measure dietary restraint, disinhibition, and hunger. J Psychosom Res 1985;29:71–83 [DOI] [PubMed] [Google Scholar]
- 35.White MA, Grilo CM: Psychometric properties of the Food Craving Inventory among obese patients with binge eating disorder. Eat Behav 2005;6:239–245 [DOI] [PubMed] [Google Scholar]
- 36.Cappelleri JC, Bushmakin AG, Gerber RA, et al. : Evaluating the Power of Food Scale in obese subjects and a general sample of individuals: development and measurement properties. Int J Obesity 2009;33:913–22 [DOI] [PubMed] [Google Scholar]
- 37.Wadden TA, Berkowitz RI, Womble LG, et al. : Randomized trial of lifestyle modification and pharmacotherapy for obesity. New Engl J Med 2005;353:2111–2120 [DOI] [PubMed] [Google Scholar]
- 38.Brown JD, Buscemi J, Milsom V, et al. : Effects on cardiovascular risk factors of weight losses limited to 5–10%. Trans Behav Med 2016;6:339–346 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Gueorguieva RV, Krystal J: Move over ANOVA: Progress in analyzing repeated measures data and its reflection in papers published in the Archives of General Psychiatry. Arch Gen Psychiatry 2004;61:310–317 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
De-identified data will be provided in response to reasonable written request to achieve goals in an approved written proposal.