

Abstract
Background/Aims
Cold snare polypectomy (CSP) is commonly used for the resection of colorectal polyps ≤10 mm. Data regarding the influence of snare type on CSP effectiveness are conflicting. Hence, this meta-analysis aimed to compare the outcomes and safety of thin- and thick-wire snares for CSP.
Methods
A comprehensive search of the literature published between 2000 and 2021 was performed of various databases for comparative studies evaluating the outcomes of thin- versus thick-wire snares for CSP.
Results
Five studies with data on 1,425 polyps were included in the analysis. The thick-wire snare was comparable to the thin-wire snare with respect to complete histological resection (risk ratio [RR], 1.03; 95% confidence interval [CI], 0.97–1.09), overall bleeding (RR, 0.98; 95% CI, 0.40–2.40), polyp retrieval (RR, 1.01; 95% CI, 0.97–1.04), and involvement of submucosa in the resection specimen (RR, 1.28; 95% CI, 0.72–2.28). There was no publication bias and a small study effect, and the relative effects remained the same in the sensitivity analysis.
Conclusions
CSP using a thin-wire snare has no additional benefit over thick-wire snares in small colorectal polyps. Factors other than snare design may play a role in improving CSP outcomes.
Keywords: Cold snare polypectomy, Colorectal polyp, Dedicated snare, Histological resection, Meta-analysis
INTRODUCTION
The risk of colorectal cancer development and its associated mortality can be reduced by the endoscopic resection of colorectal polyps.1 The majority of these procedures are performed of diminutive (≤5 mm) or small (6–9 mm) lesions.2,3 Traditional hot snare polypectomy (HSP) is useful for removing these lesions.1 However, HSP is associated with a small but significant risk of serious adverse events, including post-polypectomy bleeding (PPB) and perforation.4 The American Society for Gastrointestinal Endoscopy and the European Society of Gastrointestinal Endoscopy recommend cold snare polypectomy (CSP) for colorectal lesions <10 mm in diameter.5,6 In a recent large-scale propensity score–matched study of polypectomy outcomes for colorectal lesions <10 mm, CSP had a significantly lower risk of PPB than HSP.7 Endoscopic lesion resection is the second factor that determines polypectomy efficacy, as residual lesions can be associated with post-colonoscopic interval cancer.8 The presence of residual or recurrent tissue following snare polypectomy is reportedly 3% to 14%.9,10 A recent randomized controlled trial by the POLIPEC HOT-COLD study group showed no differences in complete resection rates (CRRs) between HSP and CSP, with reduced intensity and duration of post-colonoscopy abdominal pain.11 Hence, polypectomy aims to ensure complete resection in an en bloc manner while minimizing complications.
Cold snaring requires en bloc capture of polyps with mechanical tissue transection. A snare wire is the major determinant of effective tissue transection. Considerable variations are seen in the resection techniques for these subcentimetric lesions owing to the availability of a large selection of snares. Traditional snares have thicker braided current-carrying wires and oval-shaped snare loops, while newer dedicated cold snares have thinner monofilament wires and diamond-shaped snare loops. There is no consensus regarding the best snare type for CSP. Hence, the present systematic review and meta-analysis (SRMA) was conducted to compare the efficacy and safety of thin and thick wires for cold snare polypectomies.
METHODS
SRMA was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and registered with PROSPERO (CRD42022306231).
Information sources and search strategy
We searched Medline and ScienceDirect for all relevant studies published between 2000 and October 2021. The following keywords were used for the search: (Cold snare OR CSP OR Cold polypectomy) AND (Wire OR Snare OR Technique) AND (Colon OR Colorectal). We also manually searched the reference lists of all identified trials, guidelines, and reviews on the topic for relevant trials.
Study selection
Two independent reviewers searched the titles and abstracts of the retrieved search records against the inclusion and exclusion criteria. The same two reviewers examined the full texts of potentially eligible citations. Disagreements were resolved by a third reviewer. Studies included in this SRMA were comparative and fulfilled the following PICO criteria: (1) Patients: colorectal polyp measuring ≤10 mm without endoscopic evidence of suspected submucosal invasive cancer; (2) Intervention: use of a thin-wire/dedicated snare (0.3 mm) for CSP; (3) Comparison: use of thick-wire/traditional snare (0.47 mm) for CSP; and (4) Outcomes: complete resection and adverse events. We included both original articles and conference abstracts because of the low number of retrieved studies. There was no restriction on language as long as the study outcomes were mentioned in the text. Non-comparative studies, case series, and studies involving persons aged <18 years were excluded from the analysis. Rayyan (http://rayyan.qcri.org), a free web application, was used to screen the abstracts and titles.12
Data extraction
The data extraction was independently performed by two investigators. Disagreements were resolved by a third reviewer. Data collection was performed under the following headings: study author and year, number of patients, sex distribution, intervention used and comparator arm, follow-up duration, outcomes, and adverse events.
Definition of outcomes
The primary outcome of the analysis was the rate of complete polyp resection, which was assessed by pathological examination. Overall bleeding included both intraprocedural and PPB within 2 weeks of the index procedure. Excision depth of the resected specimens was assessed by the presence of the submucosa on pathological examination.
Risk of bias in individual studies and confidence in cumulative evidence
The risk of bias was assessed by two reviewers using the Cochrane Risk of Bias tool for randomized trials13 and Cochrane Collaboration’s risk of bias in non-randomized studies of interventions tool for non-randomized studies.14 The quality of evidence was analyzed according to the Grading of Recommendations Assessment, Development, and Evaluation Working Group approach.15
Statistical analysis
Dichotomous variables were analyzed using the risk ratio (RR) and Mantel-Haenszel test. The random-effects model was used irrespective of the presence of heterogeneity. The Q and I2 statistics were used to assess heterogeneity among the studies. A p-value on the Q test <0.1 or an I2 value >50% was considered significant. Publication bias was assessed using funnel plots and Egger’s test. The sensitivity analysis was performed by conducting a leave-one-out meta-analysis, which excluded one study from each analysis to investigate the influence of each on the overall effect size estimate and identify influential studies. All statistical analyses were performed using RevMan software (ver. 5.4.1; Cochrane Collaboration) and STATA software (ver. 17; StataCorp., College Station, TX, USA).
RESULTS
Figure 1 shows the PRISMA flowchart for the article selection process, which was conducted according to updated guidelines.16 A total of 220 citations were retrieved from Medline and 83 from ScienceDirect; after the removal of duplicates, 269 were screened. Finally, five studies were included in the analysis,17-21 among which four were full-text articles and one was a conference abstract. Table 1 summarizes the characteristics of the study population and polyps. The snare used in all studies were the Exacto (Exacto snare; Steris Medical, Dublin, Ireland) cold snare, with a wire diameter of 0.3 mm (thin-wire), and the SnareMaster snare (Olympus Ltd., Tokyo, Japan), with a wire diameter of 0.47 mm (thick-wire). The abstract by Jung et al.20 did not mention snare names.
Fig. 1.
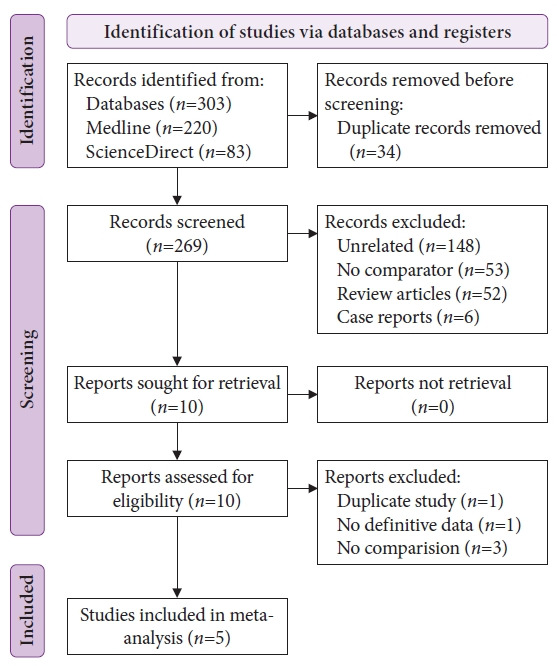
Flow diagram of the study retrieval and identification process for the meta‐analysis as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement.
Table 1.
Study characteristics
| Study | Country | Study design | Polyp criteria (mm) | No. of patients | M/F | Intervention | No. of polyps/no. of patients | Patients on anti-thrombotics, n (%) | Location of polyps (P/L) | Histology(AD/SSL/HYP/O) |
|---|---|---|---|---|---|---|---|---|---|---|
| Horiuchi et al. (2015)18 | Japan | RCT | ≤10 | 76 | 51/25 | Thin-wire | 98 (37) | 4 (11) | 58/40 | 84/5/9/0 |
| Thick-wire | 112 (39) | 4 (10) | 63/49 | 94/6/11/1 | ||||||
| Din et al. (2015)17 | UK | Prospective | 3–7 | 112 | 74/28 | Thin-wire | 89 (56) | - | 38/51 | 55/2/19/13 |
| Thick-wire | 72 (56) | - | 23/49 | 39/0/22/11 | ||||||
| Dwyer et al. (2017)19 | Australia | Prospective | ≤10 | 181 | 115/66 | Thin-wire | 126 (88) | 6 (7) | 90/36 | 73/21/22/0 |
| Thick-wire | 173 (93) | 21 (23) | 98/75 | 135/15/23/0 | ||||||
| Jung et al. (2018)20 | South Korea | RCT | 5–8 | - | - | Thin-wire | 48 (-) | - | - | - |
| Thick-wire | 47 (-) | - | - | - | ||||||
| Sidhu et al. (2022)21 | Multicentric | RCT | ≤10 | 660 | 379/281 | Thin-wire | 339 (339) | 36 (10.6) | 240/99 | 217/35/41/46 |
| Thick-wire | 321 (321) | 35 (10.9) | 223/98 | 187/33/45/55 |
M, male; F, female; P, proximal; L, left; AD, adenoma; SSL, sessile serrated lesion; HYP, hyperplastic; O, other; RCT, randomized controlled trial; -, no data available.
Outcomes
1) Complete histological resection
All five studies17-21 reported the primary outcome of histological resection. The rate of complete histological resection was comparable between thin-wire and thick-wire CSP (RR, 1.03; 95% confidence interval [CI], 0.97–1.09; I2=69%; p=0.01), with significant interstudy heterogeneity (Fig. 2).
Fig. 2.
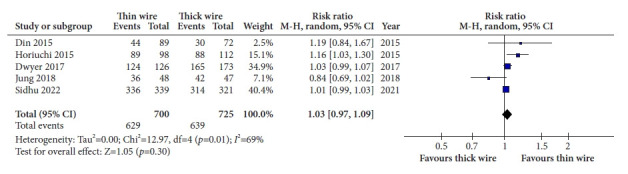
Forest plot comparing histological resection rates of thin versus thick snares. M-H, Mantel-Haenszel; CI, confidence interval.
2) Overall bleeding and perforation rates
The incidence of bleeding (immediate and delayed) was reported by all five studies.17-21 Most episodes of bleeding were immediate, and only Horiuchi et al.18 reported delayed bleeding. The rates of overall bleeding (RR, 0.98; 95% CI, 0.40–2.40; I2=38%; p=0.19) (Fig. 3) and immediate bleeding (RR, 1.02; 95% CI, 0.41–2.56; I2=35%; p=0.20) were comparable between thin-wire and thick-wire CSP without any significant interstudy heterogeneity. None of the studies reported any perforation associated with the use of either snare for CSP.
Fig. 3.
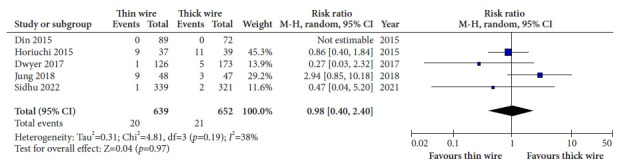
Forest plot comparing overall bleeding rates of thin versus thick snares. M-H, Mantel-Haenszel; CI, confidence interval.
3) Polyp retrieval rate
The polyp retrieval rate was reported by three studies.17,20,21 The rates of polyp retrieval were comparable between thin-wire and thick-wire CSP (RR, 1.01; 95% CI, 0.97–1.04; I2=55%; p=0.11) with significant interstudy heterogeneity (Fig. 4).
Fig. 4.
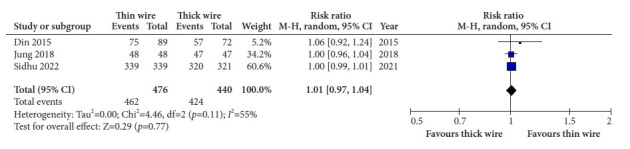
Forest plot comparing polyp retrieval rates of thin versus thick snares. M-H, Mantel-Haenszel; CI, confidence interval.
4) Presence of submucosal tissue in resection specimen
The presence of submucosal tissue in the resected specimen was reported by three studies18,20,21 and comparable between thin-wire and thick-wire CSP (RR, 1.28; 95% CI, 0.72–2.28; I2=48%; p=0.14) without any significant interstudy heterogeneity (Fig. 5).
Fig. 5.
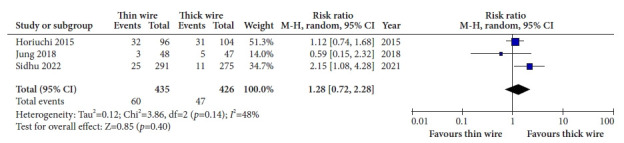
Forest plot comparing the presence of submucosa in resection specimens retrieved using thin versus thick snares. M-H, Mantel-Haenszel; CI, confidence interval.
Risk of bias assessment
Among the randomized controlled trials, two studies had a low risk of bias18,21 and one study had some concern regarding the risk of bias.20 Both non-randomized studies had a moderate risk of bias.17,19 Traffic light plots for the risk of bias are shown in Figure 6.
Fig. 6.
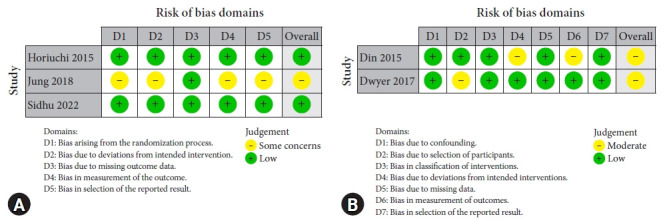
Risk of bias assessment for (A) randomized controlled studies and (B) non-randomized studies.
Publication bias, sensitivity analysis, and grade of evidence
Assessment of funnel plots for all outcomes showed no evidence of publication bias (Supplementary Fig. 1). Egger’s test for all outcomes showed no evidence of a small study effect (Supplementary Table 1). A leave-one-out meta-analysis conducted for the sensitivity analysis showed no significant change in the risk of outcomes (Supplementary Fig. 2). Table 2 summarizes the study findings and level of evidence.
Table 2.
Summary of study findings and grade of evidence
| Outcomesa) | Anticipated absolute effects (95% CI) |
Relative effect(95% CI) | No. of polyps/no. of studies | Certainty assessment |
Overall certainty of evidence | ||||
|---|---|---|---|---|---|---|---|---|---|
| Risk with thick snare | Risk with thin snare | Risk of bias | Inconsistency | Indirectness | Imprecision | ||||
| Histological resection | 881 per 1,000 | 907 per 1,000 (854–960) | RR, 1.03 (0.97–1.09) | 1,425/5 | + | + | – | – | Low |
| ●●○○ | |||||||||
| Overall bleeding | 32 per 1,000 | 31 per 1,000 (13–77) | RR, 0.98 (0.40–2.40) | 1,291/5 | + | – | – | + | Low |
| ●●○○ | |||||||||
| Polyp retrieval | 964 per 1,000 | 974 per 1,000 (935–1,002) | RR, 1.01 (0.97–1.04) | 916/3 | + | + | – | – | Low |
| ●●○○ | |||||||||
| Presence of submucosa in resection specimen | 110 per 1,000 | 141 per 1,000 (79–251) | RR, 1.28 (0.72–2.28) | 861/3 | + | – | – | + | Low |
| ●●○○ | |||||||||
PICO criteria: Population, colorectal polyps ≤10 mm; Intervention, cold snare polypectomy using thick-wire/traditional snare; Comparison, cold snare polypectomy using thin-wire/dedicated snare;
Outcomes.
CI, confidence interval; RR, risk ratio.
DISCUSSION
Apart from wire thickness, snare shape could be related to the efficacy of cold snaring of a polyp. The dedicated thin snare had a shield shape, whereas the traditional thick snare had an oval shape. Din et al.17 proposed that the shield shape might make snare positioning around tiny lesions easier than that with the oval shape. In addition, a thinner wire results in more cutting than shearing through the mucosa, thus increasing cutting ease and precision. However, the current meta-analysis showed no difference between snare types in terms of complete histological resection, polyp retrieval rate, and complications. The onus is more on operator technique than snare type for ensuring en bloc removal of small polyps without any attendant complications.
With respect to polyp size, Horiuchi et al.18 showed a significantly higher CRR in the thin versus thick-wire group for 8–10-mm lesions (83% vs. 45%, p=0.014). In contrast, the most recent study by Sidhu et al.21 demonstrated that all polyps 9 to 10 mm in size could be resected entirely using either snare. The present meta-analysis also showed no difference in CRR irrespective of size.
In an analysis of predictors of incomplete resection, Dwyer et al.19 reported that polyps with serrated or hyperplastic histology have a higher rate of incomplete resection than adenomatous polyps (7% vs. 2%, p=0.03). Other studies reported that sessile serrated lesions and a proximal polyps location are risk factors for incomplete resection.22-24 Regarding snare type, Horiuchi et al.18 reported a higher rate of complete resection with a dedicated snare in cases of adenomatous polyps. Since hyperplastic or serrated polyps tend to appear similar to the neighboring colonic mucosa without significant contrast, there is a possibility of higher CRR.25 In addition, the proximal location may require significant manipulation of the endoscope to position the polyp, which may affect the rates of complete resection.
Incomplete resection may be associated with polyp recurrence rate and increase colorectal cancer risk.26 In the study by Jung et al.,20 endoscopist experience was associated with CRR in univariate analysis (odds ratio [OR], 4.037; p=0.012). However, on multiple logistic regression analyses, there was no association between snare type, endoscopist experience, polyp size, polyp shape, polyp location, and pathologic findings and CRR. CSP was performed by ten senior consultants and seven advanced endoscopy fellows in the study by Sidhu et al.21 There was no significant difference in the incomplete resection rate between the individual endoscopists in both the groups. Dwyer et al.19 also reported no difference in CRR with respect to endoscopist experience.
The difference in histological resection reported between the two CSP methods could be a result of differences in the definition of outcomes for each study. Sidhu et al.21 and Dwyer et al.19 defined complete histological resection based on examination of both resection specimens and biopsies from the resection margin. Din et al.17 obtained biopsies from areas of residual tissue, margins, and bases only when excision was judged as incomplete or uncertain based on chromoendoscopy. In contrast, Horiuchi et al.18 defined complete histological resection based on a pathological examination of the resected specimen.
In the management of diminutive polyps, complete resection is more important than tissue retrieval. In a meta-analysis, it was reported that narrow-band imaging can allow post-polypectomy surveillance intervals to be determined in a “resect and discard” strategy in patients with small/diminutive polyps independent of histopathology.27 Thus, even in cases of tissue retrieval failure, optical diagnosis using chromoendoscopy or image-enhanced endoscopy may determine the appropriate surveillance intervals. Our meta-analysis further supports the notion that snare type does not affect the CRR of small polyps undergoing CSP.
Resection depth can be assessed based on the presence of submucosal tissue in the resected specimen. Although Sidhu et al.21 showed a significantly higher proportion of submucosal tissue in resection specimens with a thin-wire snare, the present meta-analysis showed no intergroup difference. This is important because the risk of PPB is significantly increased as resection depth increases due to the exposed deep submucosal arteries.28 Thus, the bleeding risk remained the same for both snare types.
Jung et al.29 conducted a network meta-analysis to compare the efficacy of cold polypectomy techniques for diminutive colorectal polyps. With respect to complete histological eradication, dedicated and traditional CSP were superior to cold forceps polypectomy, with dedicated CSP being superior to traditional CSP (OR, 1.76; 95% CI, 1.07–2.89). There was no difference between dedicated and traditional CSP regarding tissue retrieval rate (OR, 1.03; 95% CI, 0.44–2.38). However, the previous analysis included only two studies comparing thick and thick snares17,18; hence, the confidence of the level of evidence was very low.
The present meta-analysis had the highest number of studies comparing the outcomes of traditional (thick-wire) and dedicated (thin-wire) snares for CSP. The results of the current meta-analysis are relevant for several reasons. First, the dedicated thin-wire snare cannot be used for HSP, as it was not designed with electrocautery attachments.18 On the other hand, traditional snares can be used for both CSP and HSP in cases of multiple polyps of different sizes in the same patient, thus reducing the need for multiple snares. There are no data on the perception of ease of use of different snares among endoscopists.
The present meta-analysis has several limitations. First, it included a small number of studies and non-randomized studies. Second, it could not assess whether there was a difference in outcomes with respect to polyp size (<5 mm vs. 5–10 mm). In addition, we could not analyze the predictors of incomplete resection because the incomplete resection rate was low owing to the small size of the polyps.
Despite these limitations, the present meta-analysis provides better insight into the efficacy of various CSP techniques for diminutive polyps. Compared to the traditional belief that thin-snare CSP is superior, the current analysis showed comparable efficacy and safety of thin- and thick-wire snares for CSP. Other factors, such as polyp morphology, polyp location, operator experience, and use of standardized techniques, may have impacted the CSP outcomes; therefore, further studies are required to validate our findings.
Footnotes
Ethical Statements
Not applicable.
Conflicts of Interest
The authors have no potential conflicts of interest.
Funding
None.
Author Contributions
Conceptualization: SG, SS; Methodology: SG, VJ, HD, SS; Formal analysis: SG, VJ, HD; Project administration: SG, SS; Visualization: SG, VJ, HD; Software: SG; Validation: SG, HD, SS; Writing–original draft: SG, VJ, HD, SS; Writing–review and editing: SG, VJ, HD, SS.
Supplementary Material
Supplementary Fig. 1. Funnel plot for assessment of publication bias.
Supplementary Fig. 2. Leave-one-out meta-analysis for sensitivity analysis of all outcomes.
Supplementary Table 1. Egger’s test for assessment of small study effect.
Supplementary Table 2. PRISMA checklist for systematic review and meta-analysis.
Supplementary materials related to this article can be found online at https://doi.org/10.5946/ce.2022.141.
REFERENCES
- 1.Zauber AG, Winawer SJ, O’Brien MJ, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med. 2012;366:687–696. doi: 10.1056/NEJMoa1100370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lowenfels AB, Williams JL, Holub JL, et al. Determinants of polyp size in patients undergoing screening colonoscopy. BMC Gastroenterol. 2011;11:101. doi: 10.1186/1471-230X-11-101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lieberman DA, Holub JL, Moravec MD, et al. Prevalence of colon polyps detected by colonoscopy screening in asymptomatic black and white patients. JAMA. 2008;300:1417–1422. doi: 10.1001/jama.300.12.1417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Burgess NG, Metz AJ, Williams SJ, et al. Risk factors for intraprocedural and clinically significant delayed bleeding after wide-field endoscopic mucosal resection of large colonic lesions. Clin Gastroenterol Hepatol. 2014;12:651–661. doi: 10.1016/j.cgh.2013.09.049. [DOI] [PubMed] [Google Scholar]
- 5.Kaltenbach T, Anderson JC, Burke CA, et al. Endoscopic removal of colorectal lesions-recommendations by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2020;91:486–519. doi: 10.1016/j.gie.2020.01.029. [DOI] [PubMed] [Google Scholar]
- 6.Ferlitsch M, Moss A, Hassan C, et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2017;49:270–297. doi: 10.1055/s-0043-102569. [DOI] [PubMed] [Google Scholar]
- 7.Takamaru H, Saito Y, Hammoud GM, et al. Comparison of postpolypectomy bleeding events between cold snare polypectomy and hot snare polypectomy for small colorectal lesions: a large-scale propensity score-matched analysis. Gastrointest Endosc. 2022;95:982–989. doi: 10.1016/j.gie.2021.12.017. [DOI] [PubMed] [Google Scholar]
- 8.Brenner H, Chang-Claude J, Jansen L, et al. Colorectal cancers occurring after colonoscopy with polyp detection: sites of polyps and sites of cancers. Int J Cancer. 2013;133:1672–1679. doi: 10.1002/ijc.28166. [DOI] [PubMed] [Google Scholar]
- 9.Humphris JL, Tippett J, Kwok A, et al. Cold snare polypectomy for diminutive polyps: an assessment of the risk of incomplete removal of small adenomas. Gastrointest Endosc. 2009;69:AB207. [Google Scholar]
- 10.Gonzalez I, Riley DE, Ho SB, et al. Quality colonoscopy: midterm results of a qualitative comparison of cold snare versus cold biopsy forceps for the resection of colonic polyps. Gastrointest Endosc. 2010;71:AB244. [Google Scholar]
- 11.de Benito Sanz M, Hernández L, Garcia Martinez MI, et al. Efficacy and safety of cold versus hot snare polypectomy for small (5-9 mm) colorectal polyps: a multicenter randomized controlled trial. Endoscopy. 2022;54:35–44. doi: 10.1055/a-1327-8357. [DOI] [PubMed] [Google Scholar]
- 12.Ouzzani M, Hammady H, Fedorowicz Z, et al. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5:210. doi: 10.1186/s13643-016-0384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi: 10.1136/bmj.i4919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Puhan MA, Schünemann HJ, Murad MH, et al. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630. doi: 10.1136/bmj.g5630. [DOI] [PubMed] [Google Scholar]
- 16.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Din S, Ball AJ, Riley SA, et al. Cold snare polypectomy: does snare type influence outcomes? Dig Endosc. 2015;27:603–608. doi: 10.1111/den.12431. [DOI] [PubMed] [Google Scholar]
- 18.Horiuchi A, Hosoi K, Kajiyama M, et al. Prospective, randomized comparison of 2 methods of cold snare polypectomy for small colorectal polyps. Gastrointest Endosc. 2015;82:686–692. doi: 10.1016/j.gie.2015.02.012. [DOI] [PubMed] [Google Scholar]
- 19.Dwyer JP, Tan JY, Urquhart P, et al. A prospective comparison of cold snare polypectomy using traditional or dedicated cold snares for the resection of small sessile colorectal polyps. Endosc Int Open. 2017;5:E1062–E1068. doi: 10.1055/s-0043-113564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jung Y, Chun AR, Han SJ, et al. Comparison of the clinical efficacy of the cold snare polypectomy using a thin wire mini-snare and thick wire mini-snare for small sized colorectal polyps. Gastrointest Endosc. 2018;87:AB366. [Google Scholar]
- 21.Sidhu M, Forbes N, Tate DJ, et al. A randomized controlled trial of cold snare polypectomy technique: technique matters more than snare wire diameter. Am J Gastroenterol. 2022;117:100. doi: 10.14309/ajg.0000000000001554. [DOI] [PubMed] [Google Scholar]
- 22.Pohl H, Srivastava A, Bensen SP, et al. Incomplete polyp resection during colonoscopy-results of the complete adenoma resection (CARE) study. Gastroenterology. 2013;144:74–80. doi: 10.1053/j.gastro.2012.09.043. [DOI] [PubMed] [Google Scholar]
- 23.Lee SP, Sung IK, Kim JH, et al. Risk factors for incomplete polyp resection during colonoscopic polypectomy. Gut Liver. 2015;9:66–72. doi: 10.5009/gnl13330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pedersen IB, Bretthauer M, Kalager M, et al. Incomplete endoscopic resection of colorectal polyps: a prospective quality assurance study. Endoscopy. 2021;53:383–391. doi: 10.1055/a-1243-0379. [DOI] [PubMed] [Google Scholar]
- 25.Saito S, Tajiri H, Ikegami M. Serrated polyps of the colon and rectum: endoscopic features including image enhanced endoscopy. World J Gastrointest Endosc. 2015;7:860–871. doi: 10.4253/wjge.v7.i9.860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Pohl H, Anderson JC, Aguilera-Fish A, et al. Recurrence of colorectal neoplastic polyps after incomplete resection. Ann Intern Med. 2021;174:1377–1384. doi: 10.7326/M20-6689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.ASGE Technology Committee. Abu Dayyeh BK, Thosani N, et al. ASGE Technology Committee systematic review and meta-analysis assessing the ASGE PIVI thresholds for adopting real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc. 2015;81:502. doi: 10.1016/j.gie.2014.12.022. [DOI] [PubMed] [Google Scholar]
- 28.Bendall O, James J, Pawlak KM, et al. Delayed bleeding after endoscopic resection of colorectal polyps: identifying high-risk patients. Clin Exp Gastroenterol. 2021;14:477–492. doi: 10.2147/CEG.S282699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Jung YS, Park CH, Nam E, et al. Comparative efficacy of cold polypectomy techniques for diminutive colorectal polyps: a systematic review and network meta-analysis. Surg Endosc. 2018;32:1149–1159. doi: 10.1007/s00464-017-5786-4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Fig. 1. Funnel plot for assessment of publication bias.
Supplementary Fig. 2. Leave-one-out meta-analysis for sensitivity analysis of all outcomes.
Supplementary Table 1. Egger’s test for assessment of small study effect.
Supplementary Table 2. PRISMA checklist for systematic review and meta-analysis.