

Abstract
Oxytocin is a neurohormone that is routinely administered to patients during dilation and evacuation procedures (D&E) to control bleeding despite minimal evidence in support of this common practice. In this study, the authors sought to evaluate patients with hypotension after receiving oxytocin during D&E procedures. The secondary data from a double-blind, randomized, placebo-controlled trial involving 112 patients who underwent a D&E at 18-24 weeks gestation and prophylactically received an intravenous bolus of either 30 units of oxytocin in 500 mL of normal saline or 500 mL of saline alone at the start of the procedure were analyzed. Anesthesia providers measured blood pressure before, at the time of, and after study medication administration in 5-minute increments until the end of the procedure. No differences in demographic characteristics or mean blood pressure between the 2 groups were observed. The proportion of hypotensive patients was not statistically different at 5 minutes following fluid bolus (oxytocin 25% versus placebo 13%, P=.09). The proportion of hypotensive patients was similar by 10 minutes (oxytocin 20% versus placebo 16%, P=.62). A sample size of 112 provided the ability to detect a 23% difference in the proportion of patients who experienced hypotension (2-sided 95% CI, power of 80%). These findings suggest that oxytocin may have a transient hypotensive effect.
Keywords: oxytocin, blood pressure, hypotensive
Introduction
Approximately 120 000 second-trimester abortions are performed annually in the US and 95% are done surgically via dilation and evacuation (D&E).1,2 Hemorrhage, defined as a blood loss of 500 mL or more, occurs in 0.9-10 per 1000 D&E cases, but accounts for 40% of all D&E-related deaths.3 In a randomized, double-blind, placebo-controlled trial, the current authors demonstrated that 30 units of oxytocin in 500 mL of normal saline administered as a fluid bolus upon speculum insertion for D&E resulted in a significant reduction in rates of hemorrhage.4 Findings from this study resulted in an increase in the routine use of oxytocin at the time of D&E.
Oxytocin acts as both a hormone released into circulation from the neurohypophysis and a neurotransmitter released from parvocellular neurons within the hypothalamus to many areas of the central nervous system (CNS).5 As such, oxytocin is theorized to impact blood pressure through its effects on both the CNS and other organs such as the heart and blood vessels.5 Specifically, oxytocin has been shown to reduce heart rate and contractility as well as vascular resistance of peripheral blood vessels ultimately leading to a decrease in arterial blood pressure.6 A few clinical studies describe the effect of oxytocin on blood pressure when administered intravenously during pregnancy terminations, but only during first trimester surgical abortion and findings are inconsistent.7,8 In a study of women undergoing first trimester surgical abortion under general anesthesia, investigators used digital photoplethysmography pulse wave analysis to evaluate the effects of 5 units of oxytocin administered intravenously on cardiac function and vascular tone in large and small arteries.7 Results suggest that oxytocin had a vasodilatory effect on small and peripheral arteries, which led to significant declines in blood pressure, heart rate, and vascular tone in small and peripheral arteries.7 However, the authors noted that the anesthesia may have augmented the vasodilatory effects of oxytocin.7 In contrast, other studies have failed to find significant differences in blood pressure, including a study that found no difference when comparing blood pressure following intravenous injections of 10 mg of oxytocin and normal saline in first trimester abortion.8 No studies that evaluated the effects of oxytocin on blood pressure during D&E in the second trimester were identified to date.
Oxytocin reaches its peak serum level within the first minutes of administration and has a short half-life of 3 minutes.9 A better understanding of the effect of an intravenous infusion of oxytocin on blood pressure at the time of D&E is critically important as significant hypotension can have implications for systemic perfusion intraoperatively. For example, oxytocin-induced hypotension may raise providers’ concerns for intraoperative hemorrhage in a previously normotensive patient.10 This could ultimately lead to unnecessary interventions like volume resuscitation with intravenous crystalloid fluids and blood products or even additional surgical procedures in an attempt to control bleeding.11 Furthermore, in the setting of a hemorrhage, the administration of oxytocin could significantly reduce systemic perfusion and worsen the patient’s condition. In addition to hemorrhage, other abortion-related complications include uterine perforation, injury to surrounding structures like the bladder or bowel, cervical laceration, failed or septic abortion, and disseminated intravascular coagulation.11 Given that the estimated complication rate of second trimester surgical abortions is slightly greater than that of first trimester aspiration abortions (1.5% versus 1.3%), it is important for clinicians to monitor hemodynamic status for early identification of complications during D&E.11 The authors sought to evaluate the effect of an IV bolus of 30 units of oxytocin in a 500 mL bolus of normal saline on the proportion of patients experiencing hypotension at the time of D&E.
Materials and Methods
The current study is a secondary analysis of a randomized, placebo controlled, double-blind study approved by The Queen’s Medical Center Institutional Review Board (Clinical Trial # NCT02083809) conducted with participant consent between November 2014 and February 2018 among participants aged 14 – 50 years to explore the effect of oxytocin on the rate of provider interventions to control excess blood loss at the time of D&E at 18 to 24 weeks of gestation. The original study included a total of 160 patients: 112 in Honolulu, Hawai‘i and 48 in Seattle, Washington; the secondary analysis presented here includes only the 112 Hawai‘i patients. Participants were excluded if they had multiple gestation, anticoagulant use 5 days prior to the procedure, history of coagulopathy, known uterine anomalies, chorioamnionitis or sepsis, suspected placenta accreta, or cervical preparation with misoprostol.
The procedures in Hawai‘i were performed in an operating room with either general anesthesia or deep sedation. Anesthesia providers measured and recorded blood pressure in 5-minute increments intraoperatively until the end of the procedure according to the institution’s protocol. This standardization of blood pressure measurement allowed for a comparison of blood pressure between the placebo and oxytocin groups. The number of blood pressure measurements recorded depended on the duration of the procedure. Patients received 500 mL of normal saline or 500 mL of normal saline with 30 units of an oxytocin analog (Pitocin ®) as an intravenous bolus at the time of speculum placement. All patients received a paracervical block with 5 units of vasopressin and 10 mL of 1% lidocaine. Anesthesia providers measured blood pressure with an automated oscillatory cuff. Blood pressure was manually recorded on the anesthesia record at the start of the D&E, at the time of medication provision, and again every 5 minutes until the procedure was complete. Anesthesia providers were free to administer anesthetic agents of their choosing. Complications and measured blood loss were documented in the earlier study.4 Unless there were contraindications, participants received 15 mg of intravenous ketorolac at the conclusion of the procedure.
The primary analysis was to assess the proportion of patients with hypotension (defined as systolic blood pressure <90 mmHg or diastolic blood pressure <60 mmHg) after receiving oxytocin during D&E. With a sample size of 112, the study had the ability to detect a 23% difference in the proportion of patients who experienced hypotension (2-sided 95% CI, power of 80%). The proportion of patients who experienced hypotension was compared using chi-square tests for categorical variables. The secondary analysis compared mean blood pressure between the placebo and oxytocin groups at 5-minute increments. Mean blood pressure was compared using a Student’s t-test. Continuous and categorical demographic variables were compared using Student’s t-tests and chi-square tests, respectively. Data were analyzed using SPSS Version 25.0 (IBM Corp., Armonk, NY).
Results
A total of 112 women were included in this analysis, 56 were randomized to the placebo group and 56 to the oxytocin group. There were no statistical differences in demographic characteristics between the groups (Table 1). Mean gestational age was similar among the oxytocin and placebo groups, at 19.8 (SD 1.2) and 20.1 (SD 1.3) weeks, respectively (P=.25). A difference in medication use was observed only with acetaminophen use (oxytocin 5% versus placebo 21%, P=.02) (Table 2).
Table 1.
Characteristics of Patients Who Received Oxytocin (n=56) or Placebo (n=56) and Undergoing Dilation and Evacuation
| Characteristics | Placebo n=56 |
Oxytocin n=56 |
P-value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Gestational age (weeks) | 20.1 ± 1.3 | 19.8 ± 1.2 | .25 |
| BMI (kg/m2) | 26.7 ± 5.0 | 25.1 ± 5.5 | .1 |
| Hemoglobin | 11.5 ± 1.1 | 11.7 ± 1.5 | .44 |
| Hematocrit | 34.3 ± 2.8 | 35.1 ± 3.0 | .18 |
| Measured blood loss (mL) | 362.1 ± 317.4 | 161.1 ± 113.4 | <.001 |
| N (%) | N (%) | ||
| Current/recent smoker | 21 (38) | 21 (38) | >.99 |
| Reported recent drug use | 9 (16) | 13 (23) | .66 |
| Alcohol use | 17 (30) | 13 (23) | .39 |
Table 2.
Frequency of Administration of Medications by Anesthesia Providers during Dilation and Evacuation in Patients who Received Oxytocin or Placebo
| Medication | Number of Patients Who Received Medication N |
Placebo N (%)a |
Oxytocin N (%) |
P-value |
|---|---|---|---|---|
| Acetaminophen | 15 | 12 (80) | 3 (20) | .02 |
| Cisatracurium | 2 | 1 (50) | 1 (50) | <.99 |
| Desflurane | 5 | 3 (60) | 2 (40) | .65 |
| Dexamethasone | 54 | 27 (50) | 27 (50) | <.99 |
| Famotidine | 1 | 0 (0) | 1 (100) | .32 |
| Fentanyl | 104 | 50 (48) | 54 (52) | .14 |
| Isoflurane | 5 | 4 (80) | 1 (20) | .17 |
| Lidocaine | 25 | 13 (52) | 12 (48) | .82 |
| Metoclopramide | 11 | 3 (27) | 8 (73) | .11 |
| Midazolam | 46 | 19 (41) | 27 (59) | .18 |
| Nitrous oxide | 17 | 8 (47) | 9 (53) | .79 |
| Ondansetron | 82 | 42 (51) | 40 (49) | .67 |
| Phenylephrine | 2 | 2 (100) | 0 (0) | .15 |
| Promethazine | 1 | 1 (100) | 0 (0) | .32 |
| Propofol | 105 | 53 (50) | 52 (50) | .70 |
| Rocuronium | 18 | 7 (39) | 11 (61) | .30 |
| Sevoflurane | 91 | 43 (47) | 48 (53) | .23 |
| Succinylcholine | 54 | 27 (50) | 27 (50) | <.99 |
N represents the number of participants who received the medication in the placebo or oxytocin groups; % represents the frequency of those who received the medication by group.
There were no differences in mean blood pressure between the groups at any time point (Table 3). Among patients in the oxytocin group, 9% were hypotensive at the time of medication administration, compared with 13% in the placebo group (P=.54). Five minutes after medication administration, twice as many patients in the oxytocin group as in the placebo group were hypotensive (oxytocin 25% versus placebo 13%, P=.09) though the difference was not significant (Figure 1). Ten minutes after medication administration, a similar number of patients in both groups were hypotensive (oxytocin 20% versus placebo 16%, P=.62). No patients in either group experienced a clinically significant cardiac arrhythmia or cardiac arrest.
Table 3.
Mean Systolic and Diastolic Blood Pressure of Participants Undergoing Dilation and Evacuation Who Received Placebo (n=56) or Oxytocin (n=56) Measured at Enrollment and Throughout the Procedurea
| Time of Blood Pressure Measurement | Placebo | Oxytocin | ||
|---|---|---|---|---|
| Systolic Mean ± SD |
Diastolic Mean ± SD |
Systolic Mean ± SD |
Diastolic Mean ± SD |
|
| Enrollment | 113.6 ± 13.2 | 72.6 ± 9.0 | 113.8 ± 15.2 | 73.0 ± 8.6 |
| Procedure start | 121.5 ± 13.6 | 69.0 ± 12.8 | 122.5 ± 16.2 | 69.4 ± 10.1 |
| Medication provision | 112.9 ± 18.8 | 64.9 ± 15.8 | 114.0 ± 18.0 | 63.5 ± 12.9 |
| 5 minutes | 106.3 ± 15.9 | 60.0 ± 14.3 | 105.2 ± 16.8 | 59.0 ± 11.6 |
| 10 minutes | 103.3 ± 12.8 | 58.1 ± 12.2 | 102.1 ± 13.2 | 56.1 ± 8.5 |
| 15 minutes | 102.6 ± 14.0 | 56.1 ± 11.9 | 101.7 ± 11.9 | 55.6 ± 9.8 |
| 20 minutes | 102.1 ± 11.1 | 55.9 ± 10.4 | 101.7 ± 9.9 | 55.4 ± 7.9 |
| 25 minutes | 101.0 ± 10.0 | 54.5 ± 10.3 | 103.6 ± 8.6 | 56.7 ± 8.7 |
| 30 minutes | 102.7 ± 12.1 | 55.1 ± 13.6 | 105.6 ± 9.0 | 58.6 ± 7.4 |
| 35 minutes | 104.9 ± 12.6 | 56.9 ± 12.5 | 104.3 ± 9.3 | 58.7 ± 7.3 |
Procedure duration varied so some patients did not have blood pressure measurements at all time points after 15 minutes (at 15 minutes: placebo (n=53) and oxytocin (n=53), at 20 minutes: placebo (n=44) and oxytocin (n=46), at 25 minutes placebo (n=33) and oxytocin (n=36), at 30 minutes: placebo (n=28) and oxytocin (n=25), at 35 minutes placebo (n=18) and oxytocin (n=15).
Figure 1.
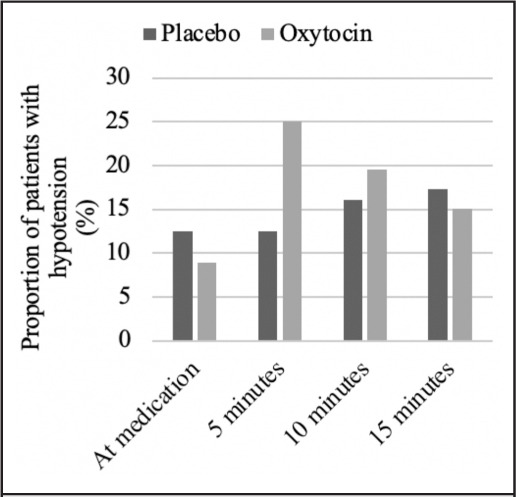
Proportion of Patients Who Received Oxytocin (n=56) or Placebo (n=56) with Recorded Hypotensiona after Bolus of 30 Units of Oxytocin in 500 mL Fluid During Dilation and Evacuationw
Discussion
Among patients who received general anesthesia or deep sedation during D&E at 18 to 24 weeks of gestation, a higher proportion of patients who received 30 units of oxytocin in 500 mL of normal saline fluid bolus experienced hypotension compared to those who received normal saline alone. The study was not powered to detect a difference in this outcome and the results were not statistically different. If oxytocin has an effect, it is transient, occurring within the first 5 minutes of administration.
Many anesthetic medications affect blood pressure, and, in this study, the intraoperative anesthetics patients received were not standardized. Rabow et al stated a similar challenge regarding their investigation of oxytocin’s effect on blood pressure during first trimester surgical abortion.7 As anesthetic depth and sympathetic activity could not be controlled in the study, it is possible that the effect of oxytocin on vascular tone was enhanced by the vasodilatory effects of anesthesia.7 In the same way, it is possible that the anesthesia medications provided in the current study affected blood pressure. However, patients were randomized to study groups and use of all medications did not differ between groups with the exception of acetaminophen. Another potential limitation of the current study is the variation in D&E procedure length, as some were as short as 10 minutes and others as long as 35 minutes. It is possible that the shorter procedures did not provide enough time to gather meaningful blood pressure data that accurately reflected the effect of oxytocin.
Despite the limitations, the results suggest that oxytocin may cause patients to experience transient hypotension shortly after administration. Since blood pressure is considered a marker of hemodynamic stability, monitoring blood pressure in D&E procedures is critically important as evidence of hypotension could indicate an underlying surgical complication like hemorrhage. Abortion and anesthesia providers should be aware of the potential transient hypotensive effects of oxytocin on blood pressure during D&E to limit rates of interventions to control blood pressure. This knowledge could save patients from receiving volume resuscitation with intravenous fluids, vasopressors, and blood products or even from undergoing additional surgical procedures unnecessarily. Possible avenues for future studies include monitoring blood pressure measurements frequently or standardizing anesthetic medications during D&E to further elucidate when the hypotensive effects of oxytocin are most significant and when they dissipate.
Acknowledgements
We are grateful to the Society of Family Planning for supporting the original study.
Abbreviations and Acronyms
- CNS
central nervous system
- D&E
dilation and evacuation
- mL
milliliters
- SD
standard deviation
Conflict of Interest
None of the authors identify a conflict of interest.
Disclosure Statement
This study was funded by a grant from the Society of Family Planning
References
- 1.Rosenstein MG, Turk JK, Caughey AB, Steinauer JE, Kerns JL. Dilation and evacuation training in maternal-fetal medicine fellowships. Am J Obstet Gynecol. 2014;210((6)):569.e1–569.e5695. doi: 10.1016/j.ajog.2014.01.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lohr P. Surgical abortion in the second trimester. Reprod Health Matters. 2008;16((31 Supplement)):151–161. doi: 10.1016/S0968-8080(08)31388-3. [DOI] [PubMed] [Google Scholar]
- 3.Kerns J, Steinauer J. Management of postabortion hemorrhage: release date November 2012 SFP Guideline #20131. Contraception. 2013;87((3)):331–342. doi: 10.1016/j.contraception.2012.10.024. [DOI] [PubMed] [Google Scholar]
- 4.Whitehouse K, Tschann M, Soon R, et al. Effects of prophylactic oxytocin on bleeding outcomes in women undergoing dilation and evacuation: A randomized controlled trial [published correction appears in Obstet Gynecol. 2019 Jun;133(6):1287-1288] Obstet Gynecol. 2019;133((3)):484–49. doi: 10.1097/AOG.0000000000003104. [DOI] [PubMed] [Google Scholar]
- 5.Petersson M. Cardiovascular effects of oxytocin. Prog Brain Res. 2002;139:281–288. doi: 10.1016/s0079-6123(02)39024-1. [DOI] [PubMed] [Google Scholar]
- 6.Janowski M, Broderick T, Gutkowska J. The role of oxytocin in cardiovascular protection. Front Psychol. 2020;11:2139. doi: 10.3389/fpsyg.2020.02139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rabow S, Hjorth U, Schönbeck S, Olofsson P. Effects of oxytocin and anaesthesia on vascular tone in pregnant women: a randomised double-blind placebo-controlled study using non-invasive pulse wave analysis. BMC Pregnancy Childbirth. 2018;18((1)):453. doi: 10.1186/s12884-018-2029-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Beeby D, Morgan Hughes JO. Oxytocic drugs and anaesthesia. A controlled clinical trial of ergometrine, syntocinon and normal saline during evacuation of the uterus after spontaneous abortion. Anaesthesia. 1984;39((8)):764–767. doi: 10.1111/j.1365-2044.1984.tb06519.x. [DOI] [PubMed] [Google Scholar]
- 9.Chang F-W, Yu M-H, Ku C-H, Chen C-H, Wu G-J, Liu J-Y. Effect of uterotonics on intra-operative blood loss during laparoscopy- assisted vaginal hysterectomy: a randomised controlled trial. BJOG. 2006;113:47–52. doi: 10.1111/j.1471-0528.2005.00804.x. [DOI] [PubMed] [Google Scholar]
- 10.Nathan HL, Duhig K, Hezelgrave ML, Chappell LC, Shennan AH. Blood pressure measurement in pregnancy. TObstet Gynaecol. 2015;17:91–98. doi: 10.1111/tog.12173. [DOI] [Google Scholar]
- 11.Sajadi-Ernazarova KR, Martinez CL. Abortion Complications. [Updated 2021 May 24] In: StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430793/