

Abstract
Purpose –
Total Worker Health® (TWH) programs, which represent a holistic approach for advancing worker safety, health and well-being, require an employer to adapt programmatic coordination and employee involvement in program design and delivery. Organizational readiness for such measures requires competencies in leadership, communication, subject expertise and worker participation. In the absence of documented methods for TWH readiness assessment, the authors developed a process to prospectively identify implementation facilitators and barriers that may be used to strengthen organizational competencies and optimize the organizational “fit” in advance.
Design/methodology/approach –
The mixed-method baseline assessment instruments comprised an online organizational readiness survey and a key leader interview; these were administered with key organizational and labor leaders in five US healthcare facilities. Findings about organizational resources, skills available and potential implementation barriers were summarized in a stakeholder feedback report and used to strengthen readiness and tailor implementation to the organizational context.
Findings –
The research team was able to leverage organizational strengths such as leaders’ commitment and willingness to address nontraditional safety topics to establish new worker-led design teams. Information about program barriers (staff time and communication) enabled the research team to respond with proactive tailoring strategies such as training on participant roles, extending team recruitment time and providing program communication tools and coaching.
Originality/value –
A new method has been developed for prospective organizational readiness assessment to implement a participatory TWH program. The authors illustrate its ability to identify relevant organizational features to guide institutional preparation and tailor program implementation.
Keywords: Total Worker Health, Organizational readiness, Organizational interventions, Tailoring implementation, Worker participation, Occupational health
Background
Occupational health and safety practice in the United States has been undergoing a paradigm shift to meet the challenges of rapidly evolving changes in the nature of working conditions for contingent workers, workers in an expanded services sector, an increasing number of older workers, low-wage workers and workers with chronic conditions (Peckham et al., 2017). These trends have necessitated expanding the traditional occupational safety and health focus to include more attention to workplace psychosocial stressors and to consider the impact of the organization of work on health conditions such as cardiovascular disease, anxiety and depression, and obesity that previously were thought to be unrelated to working conditions (Punnett et al., 2020a).
To respond to these challenges, the National Institute for Occupational Safety and Health (NIOSH) promotes a comprehensive, interdisciplinary approach known as Total Worker Health® (TWH) (Schill et al., 2019; Schill and Chosewood 2013). TWH promotes the integration of policies, programs and practices of occupational safety and health (OSH) with other efforts to advance worker well-being (Schill and Chosewood, 2016). This calls for multilevel worker engagement and systematic linkages among multiple organizational units (Punnett et al., 2020a). The comprehensive nature of TWH programs necessarily requires their development and implementation to be an organizational effort, requiring multiple actors from different work units and different levels of the organizational hierarchy to communicate effectively, coordinate planning efforts, make decisions and provide support for meaningful front-line worker involvement. Taken together, TWH workplace programs require a range of competencies in leadership, vertical and horizontal communication, technical OSH expertise and worker participation. Therefore, screening for these competencies aids in identifying gaps that can be addressed to support program implementation success.
Implementation science highlights the importance of assessing the fit of an intervention to the local context and needs, and to the skills, competencies and mental models of the target audience (Nielsen, 2013). Contextual fit is especially relevant for organization-level interventions that require involvement of multiple actors and new organizational processes and procedures to support front-line worker engagement. Conducting a baseline assessment of the organizational context and implementation stakeholders’ attitudes would inform the implementation process by leveraging conditions that are conducive to overcoming barriers (Schwatka et al., 2018 and Nielsen and Abildgaard, 2013). Tailoring an intervention represents a plan to adapt the intervention to a specific situation or setting and can take place at multiple stages in the research spectrum (Hoffmann et al., 2014). Research teams or organizations can also use tailoring to fit the implementation of an intervention to the organizational context. A good intervention fit promotes intervention adoption, targets priority issues perceived by organizational members and fosters a feeling of ownership among the intended participants (Nielsen et al., 2014 and Peters et al., 2020).
Given the resources required to conduct an organizational intervention study, it is obviously desirable to determine in advance whether uptake and implementation will be likely. To the best of our knowledge, there has been little attention in the literature to assessing program fit or potential implementation facilitators and barriers prior to the start of participatory TWH programs; we identify only one such study in the food service industry (Peters et al., 2020). TWH intervention research has retrospectively identified facilitators to program implementation such as perceived program feasibility (Farewell et al., 2020), employee engagement and building dedicated roles such as on-site champions (Zhang et al., 2016). Similarly, retrospective evaluations reported barriers to participatory TWH interventions, including staffing issues (Farewell et al., 2020), difficulty to secure time for intervention activities, lack of communication, hierarchical decision-making structures (Zhang et al., 2016) and the ongoing challenge of sustaining program support in the face of leadership changes and normal turnover (Kotejoshyer et al., 2019; Strickland et al., 2019). While there could also be obstacles on the part of employees, these obstacles primarily point to management practices and reluctance to commit to recruitment, uptake and implementation. It remains unclear how readily such obstacles could be assessed in an organization prior to initiating a full-scale TWH program.
TWH programs that emphasize an employee participatory approach show promising benefits (Punnett et al., 2013); however, implementation guidance and planning tools are very limited. The Center for the Promotion of Health in the New England Workplace (CPH–NEW) has developed the Healthy Workplace Participatory Program (HWPP) Toolkit, providing a comprehensive set of tools and instructions necessary to guide employers and occupational health professionals interested in implementing a participatory TWH program (Nobrega et al., 2017). Case studies in multiple work settings have demonstrated the usefulness of the program for generating integrated TWH interventions, engaging front-line employees in intervention design efforts, and enhancing management-worker mutual understanding and communication (Nobrega et al., 2017; Robertson et al., 2015).
The goal of this paper is to present a method for tailoring a HWPP program in accordance with facilitators and barriers identified prior to implementation. The advance assessment of organizational features known to support participatory programs (van Eerd et al., 2010) can provide useful diagnostic information to capitalize on organizational strengths and address weaknesses before and during program implementation. This study addresses the following research questions:
What organizational strengths, barriers and facilitators can be identified in advance of implementing a participatory TWH program?
In what ways can researchers assist key organizational stakeholders to respond to barriers and to leverage facilitators for implementing a participatory TWH program?
Methods
Program implementation context
The “Safety and Health through Integrated Facilitated Teams” (SHIFT) study (Punnett et al., 2020b) utilizes the HWPP to engage front-line employees in the design of local TWH interventions, offering a structured engagement process to select and analyze problems and generate and evaluate potential solutions (Robertson et al., 2013, 2015). A Design Team (DT) is composed of roughly equal numbers of front-line employees and mid-level managers; a Steering Committee (SC) is the facility’s senior management team. Two co-facilitators are trained to lead the DT, one front-line and one managerial, and a champion is identified within the SC to oversee and support the HWPP implementation.
The SHIFT study involved five public healthcare facilities in the New England region of the United States. Two facilities provide in-patient behavioral health care to civilian patients; two provide long-term and assistive living services to veterans and one provides long-term and in- and outpatient medical care to veterans. The facilities ranged in size from small to large in workforce and patient capacity (Table 1). The majority of the workforce at each one comprises direct patient caregivers, either nursing assistants at the veteran care facilities or mental health workers at the behavioral healthcare facilities.
Table I.
Characteristics of facilities included in the studya
| Facility 1 | Facility 2 | Facility 3 | Facility 4 | Facility 5 | |
|---|---|---|---|---|---|
| Size of workforceb | Small | Large | Mid-size | Mid-size | Large |
| Number of hospital beds | 45 | 320 | 0 | 0 | 67 |
| Number of assisted living beds | 0 | 0 | 305 | 30 | 0 |
| Number of long-term care beds | 0 | 0 | 150 | 269 | 100 |
| Services offered | Mental health and substance use rehabilitation support for civilian and (Facility 2 only) forensic patients | Skilled nursing care and long- term care | In-patient and outpatient services and long-term care | ||
| Primary direct care staff | Mental Health Workers | Nursing Assistants | |||
Data obtained from facility representatives and the facility websites.
Small: 101–250 employees; mid-size: 251–750 employees; large: 751 or more employees.
Study population
The participants in this study were 92 key stakeholders among the five participating facilities who were likely to be involved in leading or supporting the implementation of the program. The research team approached each facility with a list of job titles to request initial baseline data collection (survey and interview) that included the facility administrator, the director of nursing, safety, environment of care, facilities, human resources, and the presidents of all bargaining units. These participants were selected for the baseline assessment activities as described below. Some of these participants would later be asked to serve as members of the SC or DT for their respective facilities.
Instrument development
Survey of organizational readiness.
The Organizational Readiness Tool (ORT) (Robertson et al., 2018, 2021) developed by the authors is a survey that includes 51 questions in eight domains (see examples of question items in Table 2). The ORT was designed to assess opinions about the organization’s resources and approach for safety and health, communication related to safety and health, prior history with change initiatives, use of teams, climate for employee participation and ability to commit the time necessary for a HWPP. The first domain includes programmatic questions, and the remaining seven domains have items with a four-point Likert scale ranging from strongly disagree to strongly agree. The ORT could be completed in approximately 10–15 min.
Table II.
Domains and sample items in the Organizational Readiness Tool (ORT)
| Survey domains and sample items | Number of items per domain |
|---|---|
| 3 | |
| Sample item: “Which
statement is a better description of your
organization?” - Safety activities occur separately from health and wellbeing activities - Safety activities occur together with health and wellbeing activities - Not sure | |
| 6 | |
| Sample item: “This organization improves working conditions that may affect health or safety, such as shift work, scheduling, work pace, or over-time.” | |
| 4 | |
| Sample item: “In this organization there are knowledgeable employees available to assess the effectiveness of a new health and safety program.” | |
| 11 | |
| Sample item: “Management provides sufficient budget to train staff on changes to health and safety programs.” | |
| 6 | |
| Sample item: “In this organization it would be easy for a team of employees, supervisors, and managers to be brought together to meet every other week.” | |
| 8 | |
| Sample item: “My immediate supervisor takes time to listen carefully and discuss people’s concerns.” | |
| 6 | |
| Sample item: “Suggestions from employees are considered equally with suggestions of supervisors.” | |
| 7 | |
| Sample item: “Supervisors and managers communicate regularly about safety, health, and well-being issues with employees.” |
Domain 1: Response options as shown
Domains 2–8: Each item scored on a 4-point Likert scale (range: 1=strongly disagree to 4=strongly agree)
Key leader interviews.
A semi-structured interview protocol was developed to explain the planned participatory TWH intervention and to collect participants’ perceptions about priority employee safety and health issues; the performance, strengths and challenges of the existing safety and health or environment of care committee; and their expectations of the HWPP including anticipated outcomes, potential implementation barriers and alignment between program goals and their facility’s mission. The questions were designed with the goals of engaging leaders in the intervention, gaining their commitment for resources needed, understanding their perspectives on employee well-being and identifying potential obstacles that would need to be addressed before or during program implementation. Learning and responding to leader concerns is especially important for a participatory program because managers play a crucial role in supporting front-line worker involvement and they may be reluctant to share decision-making power during the design of interventions.
Data collection
Invitations were sent by email to each key stakeholder for the ORT survey and the interview separately. Participants were given a link to complete the ORT survey in Qualtrics (2020) approximately one week prior to their interview. The research team reviewed the survey results when preparing for individual interviews to identify particular domains with low scores that should be explored in depth. Qualitative data were collected from in-person interviews with the same key facility personnel who were surveyed with the ORT, to the extent possible. Interviews were recorded with the consent of the participant, and a research assistant collected detailed notes. Interviews were completed in 30–45 min. Following each interview, the interview notes were merged with details from the audio recording, and this document served as the transcript to be coded.
Compilation of findings for stakeholder feedback and intervention tailoring
ORT survey analysis.
Descriptive statistics (mean, standard deviation and range) were generated for data collected using the ORT survey. For each facility, mean scores for each domain were computed by averaging the scores of all items within the domain. All analyses were executed using SPSS version 25.0 (IBM Corp, 2017). The research team inspected the results to identify high-scoring (facilitator) and low-scoring (barrier) domains along with specific individual items that were observed to be especially high or low.
Interview data analysis.
Interview transcripts were imported into NVivo version 12 for analysis (QSR International Pty Ltd, 2018). Structured themes defined in the interview served as the primary nodes in the node structure. Secondary nodes representing specific subthemes of the primary nodes were established after reading interview notes. Qualitative data were coded by two research team members independently. Once the independent coding process was complete, coders met to review the coding consistency and reconcile discrepancies. A third member of the research team helped to resolve discrepancies when the two team members could not reach an agreement. After reconciling discrepancies, the kappa statistic for inter-rater reliability was 0.790, satisfying the threshold standard of 0.75 (QSR International Pty Ltd, 2020). Qualitative data in each node were then summarized by facility based on frequency and relevance. Themes were coded as positive (enabling implementation) or negative (impeding implementation).
Stakeholder feedback report.
Facilitators and barriers to the implementation of this study were identified from the organizational readiness surveys and the thematic content analysis of the interviews. For each facility, the ORT survey results were compiled into a customized report to be shared with the key stakeholders in that facility. The report displayed an overall score for each domain and bar charts for all items within a domain expressed in a dichotomous format; that is, the percentage of respondents who agree or strongly agree, and the percentage of respondents who disagree or strongly disagree. The report also provided an explanation for each domain related to what it measured, why it was important, and how to interpret high and low scores. For example, the interpretive message for low scores in the readiness for change initiatives domain was, “Your organization needs to prepare more before implementing a participatory Total Worker Health program. A careful planning process includes communication at all levels to explain reasons, roles, and timeline for program implementation, a means to identify and address concerns, and training for all employees involved.”
The themes from qualitative analysis of the leader interviews were summarized according the four main interview topic areas: priority health and safety concerns, strengths and weaknesses of the current safety program, degree of alignment between the HWPP and the organizational mission and goals, and outcome expectancies of the study. A customized one-page summary of these findings was prepared for stakeholders in each facility and incorporated into the facility report.
The research team arranged an in-person meeting with key leaders at each facility to present and discuss the findings in their customized report. In these meetings, the research team engaged stakeholders in discussing the overall strengths and the resource or skill areas that needed to be strengthened early in the implementation phase. The goal was to build motivation and confidence among the leaders regarding authentic employee participation, align organizational and project goals and secure commitment for establishing sufficient resources. In addition, the research team offered an initial set of recommendations for tailoring the implementation process, including how to leverage facilitators as well as overcome barriers to program implementation. The feedback meetings concluded with summarizing needs and action steps for strengthening readiness in preparation for implementing the intervention. Figure 1 depicts the HWPP implementation timeline showing when baseline data were collected and implementation tailoring efforts began.
Figure 1.
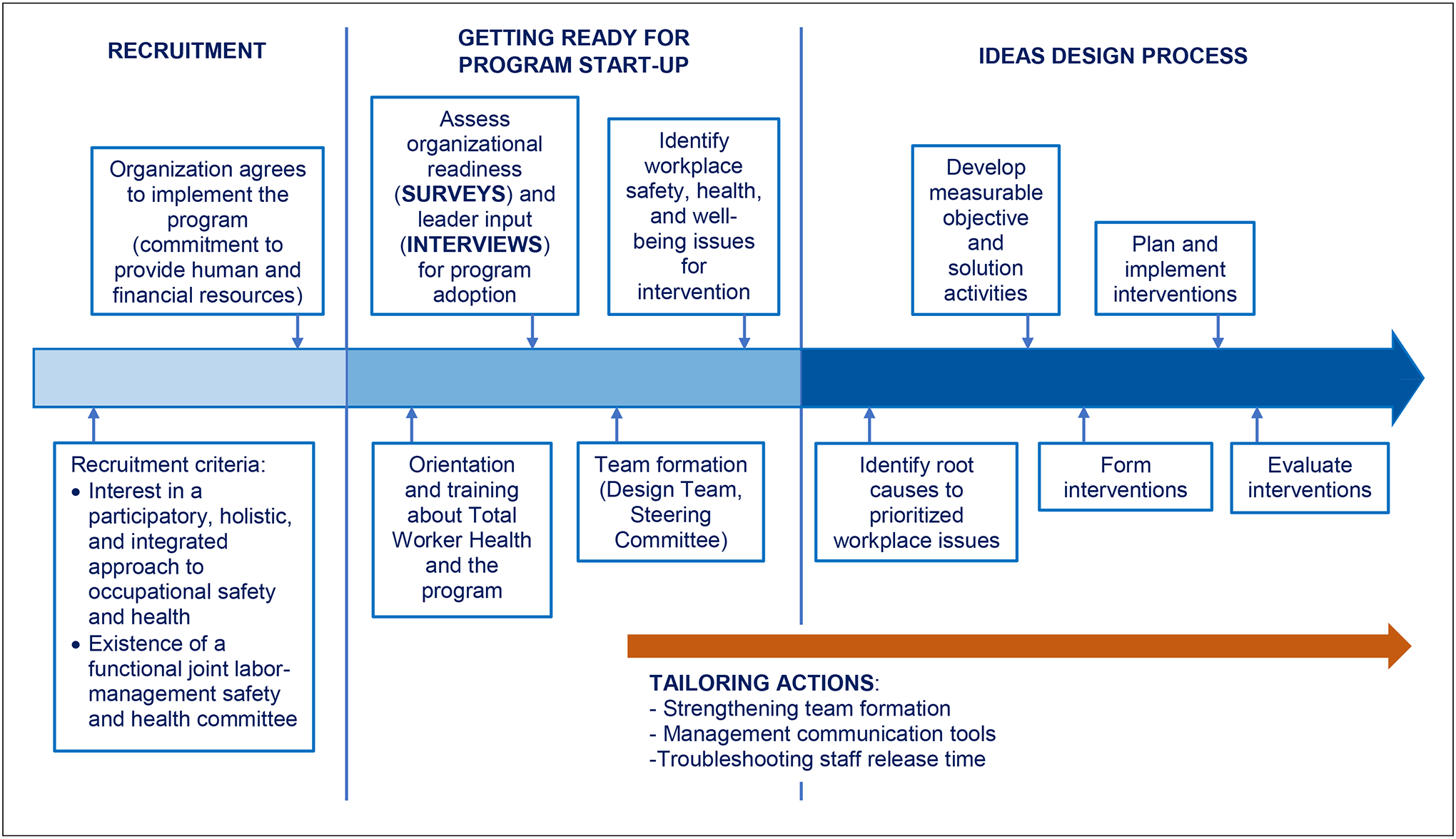
Implementation timeline of the Healthy Workplace Participatory Program
Results
Characteristics of study participants
A total of 78 participants completed a leadership interview (n = 59) and/or the ORT survey (n = 56) between September 2017 and August 2018. From the 78 participants, 37 completed both leadership interview and the ORT survey, 22 completed only the leadership interview, and 19 only the ORT survey. The demographics of participants were observed to be similar across both instruments (Table 3). Study participants mostly were White (89.9%), non-Hispanic/Latino (95.6%), working as supervisors or higher rank (68.5%), providing clinical services (46.6%) and with an average tenure of 9.7 years (SD: 9.3). One-quarter of participants held a union leadership role.
Table III.
Demographic characteristics of study participants (n=78)a
| Variable | Leadership interviews (n=59) | Organizational readiness survey (n=56) | All combined (n=78) |
|---|---|---|---|
| n (%) or mean(SD) | n (%) or mean(SD) | n (%) or mean(SD) | |
| Gender | |||
| Female | 30 (50.8%) | 28 (50.0%) | 39 (50.0%) |
| Male | 29 (49.2%) | 28 (50.0%) | 39 (50.0%) |
| Race | |||
| White | 53 (89.8%) | 42 (89.4%) | 62 (89.9%) |
| African American | 3 (5.1%) | 1 (2.1%) | 3 (4.3%) |
| Two or more races | 3 (5.1%) | 4 (8.5%) | 4 (5.8%) |
| Ethnicity | |||
| Hispanic/Latino | 2 (5.7%) | 2 (5.7%) | 2 (4.4%) |
| Not Hispanic/Latino | 33 (94.3%) | 33 (94.3%) | 43 (95.6%) |
| Organizational position | |||
| Director/Executive | 25 (42.4%) | 20 (39.2%) | 28 (38.4%) |
| Supervisor/Manager | 21 (35.6%) | 15 (29.4%) | 22 (30.1%) |
| Front-line staff | 13 (22.0%) | 16 (31.4%) | 23 (31.5%) |
| Function | |||
| Clinical services | 27 (45.8%) | 23 (45.1%) | 34 (46.6%) |
| Administrative services | 19 (32.2%) | 12 (23.5%) | 20 (27.4%) |
| Non-clinical services | 8 (13.6%) | 11 (21.6%) | 11 (15.1%) |
| Safety and health services | 5 (8.5%) | 5 (9.8%) | 8 (11.0%) |
| Union Membership | |||
| Yes | 19 (32.2%) | 14 (25.0%) | 20 (25.6%) |
| No | 40 (67.8%) | 42 (75.0%) | 58 (74.4%) |
| Tenure | 9.5 (9.8) | 9.7 (9.1) | 9.7 (9.3) |
Numbers may not add to 78 due to missing data
Organizational readiness tool scores
The ORT survey response rate in four of the five facilities ranged from 63% to 76% of invitees; in Facility 5, the response rate was 26%.
Across all facilities there was very low reporting of OSH and workforce health and well-being activities occurring together, indicating lack of program integration in TWH (Table 4).
Table IV.
Organizational programs to employee safety, health, and well-being by facility
| Variable | Facility | |||||
|---|---|---|---|---|---|---|
| No (%) | No (%) | No (%) | No (%) | No (%) | No (%) | |
| There are safety activities for employees | 11 (84.6%) | 18 (94.7%) | 5 (55.6%) | 9 (90.0%) | 5 (100.0%) | 48 (85.7%) |
| There are health and well-being activities for employees | 0 (0.0%) | 1 (5.3%) | 1 (11.1%) | 3 (30.0%) | 4 (80.0%) | 9 (16.1%) |
| Safety activities occur together with health and well-being activities | 2 (15.4%) | 0 (0.0%) | 0 (0.0%) | 1 (10.0%) | 0 (0.0%) | 3 (5.4%) |
Across all five facilities, the highest rated domains were teamwork in your work group (mean: 3.1; SD: 0.5) and resources available for safety, health and well-being (mean: 2.9; SD: 0.6), while the lowest rated domain was management communication about safety, health and well-being (mean: 2.2; SD: 0.7). The research team identified this latter domain as a resource need (e.g., training and tools) for all facilities as we engaged them in preparing for the intervention (Table 5).
Table V.
Averaged organizational readiness scores in each survey domain by facility (n=56)a
| Organizational readiness domain | ||||||
|---|---|---|---|---|---|---|
| mean(SD) | mean(SD) | mean(SD) | mean(SD) | mean(SD) | mean(SD) | |
| Current approaches to safety, health, and wellbeing in this organization | 2.7 (0.6) | 2.4 (0.5) | 2.6 (0.3) | 2.7 (0.4) | 2.8 (1.0) | 2.6 (0.6) |
| Resources available for safety, health, and well-being | 3.0 (0.6) | 2.6 (0.7) | 2.9 (0.5) | 3.1 (0.5) | 3.0 (0.8) | 2.9 (0.6) |
| Resources and readiness for change initiatives to improve safety, health, and well-being | 2.6 (0.6) | 2.4 (0.3) | 2.5 (0.3) | 2.5 (0.1) | 2.5 (0.5) | 2.5 (0.4) |
| Resources and readiness for use of teams | 2.5 (0.7) | 2.5 (0.6) | 2.6 (0.7) | 2.9 (0.6) | 2.1 (0.6) | 2.5 (0.6) |
| Teamwork in your work group | 3.1 (0.5) | 3.3 (0.5) | 2.9 (0.3) | 2.9 (0.2) | 3.4 (1.0) | 3.1 (0.5) |
| Resources and readiness for employee participation | 2.8 (0.6) | 2.1 (0.8) | 2.5 (0.8) | 2.8 (0.6) | 2.6 (1.4) | 2.5 (0.8) |
| Management communication about safety, health, and well-being | 2.7 (0.4) | 1.9 (0.5) | 2.1 (0.7) | 2.2 (1.0) | 1.9 (0.7) | 2.2 (0.7) |
Lowest score: 1=strongly disagree, highest score: 4=strongly agree
Leadership interviews
Openness to Total Worker Health constructs.
Leaders from all facilities identified concerns beyond the traditional scope of physical occupational safety hazards. In particular, while respondents at each facility noted one or more known safety hazards in the healthcare environment, they also consistently reported employees’ workload and its impact on burnout and stress as a priority issue (Table 6). A majority of interviewees across facilities perceived alignment between the stated goals of the new TWH program and their facility’s mission; they also perceived the planned employee assessment activities would be valuable for prioritizing topics for improvement. These points were all noted as shared goals between facility leaders and the researchers, and they were referred to in later conversations and reports to continue reinforcing leadership motivation to support the project.
Table VI.
Leader perspectives about potential implementation facilitators
| Themes/ subthemes | Facility 1 (n=11) | Facility 2 (n=11) | Facility 3 (n=10) | Facility 4 (n=16) | Facility 5 (n=11) | |
|---|---|---|---|---|---|---|
| Priority safety, health, and well-being issues | Workload – burnout, stress | X | X | X | X | X |
| Patient violence | X | X | X | |||
| Security – visitors, physical building | X | X | X | |||
| Patient handling (back injuries) | X | X | X | |||
| Slips, trips, and falls | X | X | ||||
| Strengths of the facility’s safety and health or Environment of Care committee | Leaders are engaged/committed | X | X | X | X | |
| Leaders are knowledgeable | X | X | X | |||
| Multidisciplinary team | X | X | ||||
| Good collaboration and support | X | X | ||||
| Continuous meetings and inspections | X | X | ||||
| Timely reporting of industrial accidents | X | |||||
| Alignment between the study goals and facility’s mission | Agreement among most interviewees | X | X | X | X | X |
| Desired study outcomes for the organization | Identify areas in need of improvement | X | X | X | X | X |
| Improve communication | X | X | X | X | ||
| Implement effective/practical solutions | X | X | X | |||
| Engage front-line workers in safety | X | X | X | |||
Identification of potential implementation barriers.
Across most facilities, interview participants reported that the main anticipated challenges to implementing a HWPP were the limited resources that the facility could offer including time available for meetings, having sufficient staff to participate in the study and funding to implement changes (Table 7). In three of the facilities, most leaders reported prior difficulties in reaching agreement on which safety and health priorities should be the primary focus of their safety program. In one facility, researchers learned from the interviewees there was no functional safety and health committee. The reasons for its committee not meeting provided important insights into labor-management challenges that the program later sought to address. Examples of implementation tailoring strategies to address these challenges follow in the remainder of the results section.
Table VII.
Leader perspectives about potential implementation barriers by facility
| Themes/ subthemes | Facility 1 (n=11) | Facility 2 (n=11) | Facility 3 (n=10) | Facility 4 (n=16) | Facility 5 (n=11) | |
|---|---|---|---|---|---|---|
| Obstacles to the study | Limited resources – time, staff, funding | X | X | X | X | |
| Lack of participation and engagement of front- line workers | X | X | ||||
| Large facility – difficulty in monitoring and communicating with all staff | X | X | ||||
| Challenges of the facility’s safety committee | Difficulty developing consensus on priorities because of competing demands | X | X | X | ||
Tailoring program implementation based on baseline stakeholder assessment
The research team, in partnership with stakeholders at each facility, initiated a set of actions to overcome identified barriers to the HWPP as well as to leverage facilitators.
Reinforcing leaders’ support for a TWH approach.
Leaders’ willingness to address an expanded set of concerns in their safety program (Table 6) was interpreted as a program implementation facilitator because it would give the DT freedom to select from a broad range of concerns as they designed local TWH interventions. The research team reinforced the leaders’ willingness to adopt TWH during the in-person meetings with facility leaders to report baseline results and when coaching DTs to design TWH initiatives that address the specific facility context.
Leveraging leaders’ health and safety knowledge and commitment.
The research team used leaders’ knowledge about strengths and gaps in safety leadership when recruiting program participants to serve on their facility’s DT. For instance, in facilities where leaders reported highly favorable commitment and expertise among the safety committee leadership (Table 6), safety specialists and managers were equal partners in recruiting appropriate personnel. In the facility with no functioning safety committee, the research team learned of historic difficulties in labor-management relations that had contributed to a lack of a functioning safety program. The research team identified this capacity gap as a serious barrier to the HWPP that needed attention to properly recruit employees willing to participate in the DT and the SC. Therefore, researchers met multiple times with representatives from each of the staff unions to discuss with them the relevance of their involvement for creating worker-driven interventions.
Resource limitations of funds, time and staffing were frequently identified as potential barriers to the implementation of the HWPP (Table 7). These issues were prioritized for immediate discussion with the HWPP champion to secure the resources needed to implement the program. Similarly, the research team initiated discussions with the champion and other SC leaders early in the team formation phase to plan feasible strategies to provide staff release time and also to select DT members and co-facilitators who could fulfill those roles. In some cases, it took time to arrive at a release time strategy that would be workable. In one facility, meeting length and frequency were adjusted three times before finding a workable solution.
Defining roles and building confidence for employee participation.
In some facilities, leaders expressed previous difficulties with gaining consensus on priority safety issues; they were also skeptical about whether workers would engage in the participatory program (Table 7). The tailoring approach to address these concerns included providing detailed training to the champion, SC members and DT members about their roles and clarifying the procedures for issue identification and selection. For example, in the HWPP, DT members prioritize issues and later collaborate with SC and key leaders for approval of proposed interventions. This training provided opportunities for participants to discuss how decisions would be made and to acknowledge uncertainty regarding the specific forms of worker participation. In those training discussions, SC members expressed their support for goals of the HWPP and committed to facilitating the DT formation process.
Concerns about a lack of participatory culture were expressed by leaders in some facilities during the interviews (Table 7) and through specific items (7a, 7d, 7e, not shown) of the ORT survey domain 7. The research team interpreted low participatory culture at baseline as a potential barrier to successful HWPP implementation because it indicated that both front-line and managerial personnel were not used to interacting and communicating together about safety and health topics. In response, the research team worked with all program participants to help them better understand their roles in the HWPP and the importance of positive communication methods and trust-building in the participatory process. The research team and co-facilitators demonstrated program reliability and commitment to the intervention design process over time by consistently following through on tasks; adhering to strict privacy protocols and promoting decision-making within team meetings; and senior managers on the SC allowed the DT to select issues they would target for interventions.
Building trust for DT initiated workplace changes.
The ORT survey measures for participants’ “felt need for change” (ORT item 4 g, not shown) was consistently high across all facilities as was leaders’ hope that the HWPP would identify areas in need of improvement (Table 6). These results suggested a general readiness to learn more about managing change initiatives. To this end, the research team explained to leaders how the program components would accomplish some of their desired outcomes (e.g. needs identified, improved communication, worker engagement and new solutions). This messaging was incorporated in program start-up meetings and also in meetings with leaders and DT members during the implementation phase. We undertook this strategy to inform as well as to promote enthusiasm, motivation and assurance of the top-down commitment for staff time and other resources needed by the DT to design and help implement integrated TWH interventions.
Expanding communication tools and resources.
ORT survey scores in the domain of management communication about safety, health and well-being were consistently low across most facilities (Table 5). Leaders from most facilities also reported a desire for the HWPP to improve organizational communication (Table 6). When low communication scores were discussed in the feedback reporting meetings, leaders acknowledged the need for improved communication and, in some cases, they expressed a desire to take action to strengthen capacity in this area. Therefore, the research team prioritized communication as an important potential barrier to address with facilities during the HWPP implementation.
To support the facilities’ communication efforts during the HWPP implementation, the research team developed and distributed sample program communication tools to help DT and SC members communicate with the workforce about the program. Their intent was to raise employee awareness about the HWPP so that a broad range of workers would engage with and respond to the DT throughout the intervention design process. Examples of communications tools included sample HWPP program announcements and updates, and a template for constructing a poster board display to capture feedback from employees who were not members of the DT. The research team also initiated a monthly project newsletter for facility team members, including co-facilitators, SC and DT members. The newsletter provided resource material on topics related to their intervention foci and personal stories from research team members to build relationships. Early metrics of newsletter open rate indicate greater engagement by front-line employees compared to managers. DT members in three facilities took it upon themselves to print out the electronic newsletter and post in on a bulletin board for employees without email accounts.
The research team liaison continued to provide communication coaching during the interactions between the DT and SC to model positive communication behavior between front-line workers and mid-level and senior leadership. Communication process evaluation is part of the SHIFT study data collection protocol to monitor the quality and frequency of organizational communication throughout the different phases of HWPP implementation.
Discussion
This study employed a mixed-method approach to prospectively assess potential facilitators and barriers to a participatory TWH program in five public healthcare facilities. Our evaluation approach was grounded in the literature regarding participatory, organization-level interventions that promote worker health and well-being (Abildgaard et al., 2018, Ipsen et al., 2015 and Karanika-Murray and Weyman, 2013). We have attempted to address a gap in the literature related to the assessment of potential facilitators and barriers prior to the implementation of participatory program interventions to address workforce health. Prospective assessment of facilitators and barriers enabled the research team, in collaboration with internal program implementers, to respond proactively by identifying areas of concern and making relevant recommendation to strengthen the organizational context to support the intervention implementation process. This method may be useful for organizational leaders, intervention researchers and consultants when implementing participatory TWH interventions in any industry sector.
The literature in organizational intervention research has documented the relevance of analyzing the organizational context to facilitate fitting the intervention to the organization (Hasle et al., 2012) given the complex and dynamic social systems where organizational interventions take place. Given the essential role of leadership support in the success of workplace health interventions (Ipsen et al., 2018 and Mellor and Webster, 2013), organizational interventions should be responsive to the setting and the personal characteristics of key implementation agents, such as managers and supervisors (Justesen et al., 2017, Karanika-Murray et al., 2018 and Pedersen et al., 2012). This is even more important for a program with a high degree of worker participation as managers may be reluctant to cede decision-making authority, and thus, it is critical to engage with them about their concerns in advance.
The ORT results indicated a consistent gap in health and safety communication systems at all facilities in the study. Organizational communication issues have been reported as a barrier in previous participatory TWH interventions (Zhang et al., 2015, 2016). In the HWPP, effective communication systems are needed to facilitate the flow of information between the DT and the SC, between the DT and co-workers to receive input on their work (bottom up), and between organizational leaders and the workforce (top-down). In addition, employees need to be aware of those mechanisms to disseminate information and believe that using them will be effective. Our experience with these facilities showed the complexity of addressing organizational communication issues and the limited influence that the research team can have on improving systems of communications within an organization. Improving communication (especially bidirectional) may be more challenging in large facilities with multiple buildings. We anticipate that workplace communication can be improved if the recommended program communication protocols involving DT, SC and workforce are successfully implemented. We also expect that the participatory activities of the HWPP facilitate team building and organizational communication between front-line workers and leadership. Evaluation of this and other tailoring responses is ongoing in the SHIFT study.
The HWPP implementation requires management commitment to secure resources, including staff time and a physical space for the DT meetings and access to subject matter experts who can manage and evaluate proposed DT initiatives. Our assessment identified funding and personnel time as potential threats to implementation of the HWPP. Previous TWH studies have also reported the limited availability of staff time to attend meetings and project activities as barriers to program implementation (Farewell et al., 2020; Strickland et al., 2019; Sedani et al., 2019; Peters et al., 2018). We addressed these issues by negotiating a commitment of personnel resources that management deemed feasible before commencing with participant recruitment and then engaging management in troubleshooting as needed as the implementation proceeded. Beyond that, the HWPP intervention design protocol specifically addresses resource allocation for interventions generated by the DT. Each intervention proposed has an associated business case, which is reviewed by managers to make funding decisions and to create action plans for securing resources.
The strength of this study is the use of mixed methods to prospectively identify potential facilitators and barriers to program implementation (Green et al., 2015). We used a quantitative theory-based ORT to assess attitudes about organizational characteristics that are relevant to supporting a participatory TWH change effort. The qualitative data from interviews complemented ORT survey results by providing specific context and depth to the quantitative data (e.g., the size of the facility influencing communication challenges). Our results showed that using these two assessment methods at baseline yielded complementary, practical information that could be used for developing action plans to promote HWPP implementation. For example, the ORT survey identified a shared perception that organizational communication was a readiness gap, whereas this issue was not highlighted during interviews.
A limitation was the reliance on self-reported data from a sample of leaders in each facility. We did not analyze objective data (such as meeting documents and communications materials) to validate the participants’ responses from the baseline assessment. It is also possible that we would have learned of additional barriers and facilitators if we were able to speak with more people, and especially more representatives of middle managers and front-line employees. Nonetheless, the report-back meetings with key facility leaders provided ample opportunity to identify gaps and inaccuracies in our interpretation of the data. No new issues were identified in the stakeholder meetings, suggesting there were no major gaps in our assessment. However, it is still possible that a larger sample of employees in non-managerial positions might have yielded different perspectives and experiences (Zhang et al., 2011).
We cannot rule out the effects of social desirability bias in these subjective data. Some leaders may have been more vocal when reporting strengths than challenges about the facility safety program. They may have been concerned with presenting a positive, competent image; they may have wanted to appear “ready” to engage in the project in order to obtain technical OSH support and/or they might genuinely perceive fewer challenges than do the staff at lower levels within the organization.
Our intent for prioritizing organizational leaders in the assessment was to gain their support for a process featuring a high degree of worker participation and to identify any concerns so that these could be addressed during the implementation. Some upper manager study participants had a strategic importance as prospective HWPP SC members, but they had limited direct knowledge of the ongoing activities in the facility’s safety and health committee. It is possible that if a greater proportion of respondents were front-line staff, we might have learned of additional barriers to implementation or we might have observed less favorable scores reported in the organizational readiness surveys. Involving at least equal numbers of front-line and managerial personnel in baseline assessment would be advisable in future projects.
Looking to the future, the SHIFT study data collection protocol going forward includes robust and comprehensive process evaluation methods to monitor the impact of the tailored strategies reported in this manuscript and to make timely adjustments in how the program is being implemented. Plans are in place to further refine the ORT through additional psychometric testing across populations and settings. In addition, the ORT survey and key leader interviews will be re-administered at facilities in the SHIFT study to assess the predictive value of the readiness domains and to support continuous learning about new barriers and facilitators that may arise over the course of the SHIFT study period. Future research would be useful to test the effectiveness of these instruments and methods for implementing a participatory TWH program in other industry sectors or in other regions or countries.
Conclusions
In this study, we report on a prospective assessment method to identify facilitators and barriers prior to implementing a participatory TWH program in public healthcare facilities. Prospective assessment provided useful diagnostic information that enabled the research team, in collaboration with internal program implementers, to respond in a proactive manner by tailoring specific program implementation processes. Examples included planning for greater staff participation in program meetings, providing tools and training on essential skills in gap areas, setting aside more time for relationship building during team formation and creating targeted messaging that team members could use to address areas of program uncertainty.
A mixed-method prospective assessment approach is a feasible and useful mechanism to identify program implementation facilitators and barriers in the early stages of implementing a participatory TWH program. These early data can be used to tailor the implementation process by building on organizational and personnel strengths and applying resources to build skills and fill gaps in resources needed for successful program implementation. Future project evaluations will seek to determine whether or not the baseline assessments presaged later program developments, the relative strength of each readiness element in predicting program outcomes and the extent to which facilities committed the supports needed for adopting and sustaining program implementation.
Funding:
The study is supported by Grant Number 1 U19 OH008857 from the U.S. National Institute for Occupational Safety and Health. This content is solely the responsibility of the authors and does not necessarily represent the official views of NIOSH.
The authors thank members of the SHIFT Research Team, including Merve Armagan, MS for her assistance with coding interview data; Winnie Chin, ScD, Yuan Zhang, PhD, and Jessica Espinoza for conducting interviews; and Diana Tubbs, PhD, for her contributions to the design and production of the employer ORT customized reports for each facility. Winnie Chin, ScD, was instrumental in the implementation of the HWPP in the facilities in the study and assisted in developing and communicating the tailored recommendations to facility personnel using results from the baseline assessment. We are also grateful for the support from key facility personnel in the facilities where these data were collected.
Contributor Information
Suzanne Nobrega, Department of Biomedical Engineering, University of Massachusetts Lowell, Lowell, Massachusetts, USA.
Cesar Morocho, Department of Biomedical Engineering, University of Massachusetts Lowell, Lowell, Massachusetts, USA.
Michelle M. Robertson, Department of Psychological Sciences, University of Connecticut, Storrs, Connecticut, USA Management and Organizational Development, Northeastern University, Boston, Massachusetts, USA.
Alicia Kurowski, Department of Biomedical Engineering, University of Massachusetts Lowell, Lowell, Massachusetts, USA.
Serena Rice, Department of Biomedical Engineering, University of Massachusetts Lowell, Lowell, Massachusetts, USA.
Robert A. Henning, Department of Psychological Sciences, University of Connecticut, Storrs, Connecticut, USA
Laura Punnett, Department of Biomedical Engineering, University of Massachusetts Lowell, Lowell, Massachusetts, USA.
References
- Abildgaard JS, Hasson H, von Thiele Schwarz U, Løvseth LT, Ala-Laurinaho A and Nielsen K (2018), “Forms of participation: the development and application of a conceptual model of participation in work environment interventions”, Economic and Industrial Democracy, Vol. 41 No. 3, pp. 746–769, doi: 10.1177/0143831X17743576. [DOI] [Google Scholar]
- Farewell CV, Powers J and Puma J (2020), “Safety and health innovation in preschools: a Total Worker Health pilot project”, Journal of Occupational and Environmental Medicine, Vol. 62 No. 5, pp. e192–e199, doi: 10.1097/JOM.0000000000001848. [DOI] [PubMed] [Google Scholar]
- Green CA, Duan N, Gibbons RD, Hoagwood KE, Palinkas LA and Wisdom JP (2015), “Approaches to mixed methods dissemination and implementation research: methods, strengths, caveats, and opportunities”, Administration and Policy in Mental Health and Mental Health Services Research, Vol. 42 No. 5, pp. 508–523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasle P, Kvorning LV, Rasmussen CDN, Smith LH and Flyvholm M-A (2012), “A model for design of tailored working environment intervention programmes for small enterprises ”, Safety and Health at Work, Vol. 3 No. 3, pp. 181–191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, Altman DG, Barbour V, Macdonald H, Johnston M, Lamb SE, Dixon-Woods M, McCulloch P, Wyatt JC, Chan AW and Michie S (2014), “Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide”, BMJ, Vol. 348 No. g1687, doi: 10.1136/bmj.g1687. [DOI] [PubMed] [Google Scholar]
- IBM Corp (2017), IBM SPSS Statistics for Windows, Version 25.0, IBM, Armonk, NY. [Google Scholar]
- Ipsen C, Gish L and Poulsen S (2015), “Organizational-level interventions in small and medium-sized enterprises: enabling and inhibiting factors in the PoWRS program”, Safety Science, Vol. 71, pp. 264–274, doi: 10.1016/j.ssci.2014.07.017. [DOI] [Google Scholar]
- Ipsen C, Karanika-Murray M and Hasson H (2018), “Intervention leadership: a dynamic role that evolves in tandem with the intervention”, International Journal of Workplace Health Management, Vol. 11 No. 4, pp. 190–192, doi: 10.1108/IJWHM-08-2018-114. [DOI] [Google Scholar]
- Justesen JB, Eskerod P, Christensen JR and Sjøgaard G (2017), “Implementing workplace health promotion – role of middle managers”, International Journal of Workplace Health Management, Vol. 10 No. 2, pp. 164–178, doi: 10.1108/IJWHM-04-2016-0030. [DOI] [Google Scholar]
- Karanika-Murray M and Weyman AK (2013), “Optimising workplace interventions for health and well-being: a commentary on the limitations of the public health perspective within the workplace health arena”, International Journal of Workplace Health Management, Vol. 6 No. 2, pp. 104–117, doi: 10.1108/IJWHM-11-2011-0024. [DOI] [Google Scholar]
- Karanika-Murray M, Gkiontsi D and Baguley T (2018), “Engaging leaders at two hierarchical levels in organizational health interventions”, International Journal of Workplace Health Management, Vol. 11 No. 4, pp. 210–227, doi: 10.1108/IJWHM-07-2018-0086. [DOI] [Google Scholar]
- Kotejoshyer R, Zhang Y, Flum M, Fleishman J and Punnett L (2019), “Prospective evaluation of fidelity, impact and sustainability of participatory workplace health teams in skilled nursing facilities”, International Journal of Environmental Research and Public Health, Vol. 16 No. 9, doi: 10.3390/ijerph16091494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mellor N and Webster J (2013), “Enablers and challenges in implementing a comprehensive workplace health and well-being approach”, International Journal of Workplace Health Management, Vol. 6 No. 2, pp. 129–142, doi: 10.1108/IJWHM-08-2011-0018. [DOI] [Google Scholar]
- Nielsen K and Abildgaard JS (2013), “Organizational interventions: a research-based framework for the evaluation of both process and effects”, Work and Stress, Vol. 27 No. 3, pp. 278–297, doi: 10.1080/02678373.2013.812358. [DOI] [Google Scholar]
- Nielsen K, Abildgaard JS and Daniels K (2014), “Putting context into organizational intervention design: using tailored questionnaires to measure initiatives for worker well-being”, Human Relations, Vol. 67 No. 12, pp. 1537–1560, doi: 10.1177/0018726714525974. [DOI] [Google Scholar]
- Nielsen K (2013), “Review article: how can we make organizational interventions work? employees and line managers as actively crafting interventions”, Human Relations, Vol. 66 No. 8, pp. 1029–1050, doi: 10.1177/0018726713477164. [DOI] [Google Scholar]
- Nobrega S, Kernan L, Plaku-Alakbarova B, Robertson M, Warren N and Henning R (2017), “Field tests of a participatory ergonomics toolkit for Total Worker Health”, Applied Ergonomics, Vol. 60, pp. 366–379, doi: 10.1016/j.apergo.2016.12.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peckham TK, Baker MG, Camp JE, Kaufman JD and Seixas NS (2017), “Creating a future for occupational health”, Annals of Work Exposures and Health, Vol. 61 No. 1, pp. 3–15, doi: 10.1093/annweh/wxw011. [DOI] [PubMed] [Google Scholar]
- Pedersen LM, Nielsen KJ and Kines P (2012), “Realistic evaluation as a new way to design and evaluate occupational safety interventions”, Safety Science, Vol. 50 No. 1, pp. 48–54, doi: 10.1016/j.ssci.2011.06.010. [DOI] [Google Scholar]
- Peters SE, Grant MP, Rodgers J, Manjourides J, Okechukwu CA and Dennerlein JT (2018), “A cluster randomized controlled trial of a Total Worker Health intervention on commercial construction sites”, International Journal of Environmental Research and Public Health, Vol. 15 No. 11, doi: 10.3390/ijerph15112354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters SE, Nielsen KM, Nagler EM, Revette AC, Madden J and Sorensen G (2020), “Ensuring organization-intervention fit for a participatory organizational intervention to improve food service workers’ health and wellbeing: workplace organizational health study”, Journal of Occupational and Environmental Medicine, Vol. 62 No. 2, pp. e33–e45, doi: 10.1097/jom.0000000000001792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Punnett L, Warren N, Henning R, Nobrega S and Cherniack M (2013), “Participatory ergonomics as a model for integrated programs to prevent chronic disease”, Journal of Occupational and Environmental Medicine, Vol. 55 No. 12, pp. 19–24, doi: 10.1097/JOM.0000000000000040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Punnett L, Cavallari JM, Henning RA, Nobrega S, Dugan AG and Cherniack MG (2020a), “Defining ‘integration’ for Total Worker Health: a new proposal”, Annals of Work Exposures and Health, Vol. 64 No. 3, pp. 223–235, doi: 10.1093/annweh/wxaa003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Punnett L, Nobrega S, Zhang Y, Rice S, Gore R and Kurowski A and SHIFT Project Research Team (2020b), “Safety and health through integrated, facilitated teams (SHIFT): stepped-wedge protocol for prospective, mixed-methods evaluation of the healthy workplace participatory program”, BMC Public Health, Vol. 20, p. 1463, doi: 10.1186/s12889-020-09551-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- QSR International Pty Ltd (2018), NVivo Qualitative Data Analysis Software, Version 12, QSR International, Chadstone, Victoria. [Google Scholar]
- QSR International Pty Ltd (2020), “Coding comparison query”, available at: https://help-nv.qsrinternational.com/12/win/v12.1.90-d3ea61/Content/queries/coding-comparison-query.htm (accessed 26 September 2020).
- Qualtrics (2020), Qualtrics, Qualtrics, Utah, Provo. [Google Scholar]
- Robertson M, Henning R, Warren N, Nobrega S, Dove-Steinkamp M, Tibirica L and Bizarro A (2013), “The intervention design and analysis scorecard: a planning tool for participatory design of integrated health and safety interventions in the workplace”, Journal of Occupational and Environmental Medicine, Vol. 55 No. 12, pp. S86–S88, doi: 10.1097/JOM.0000000000000036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robertson MM, Henning RA, Warren N, Nobrega S, Dove-Steinkamp M, Tibirica L and Bizarro A (2015), “Participatory design of integrated safety and health interventions in the workplace: a case study using the intervention design and analysis scorecard (IDEAS) tool”, International Journal of Human Factors and Ergonomics, Vol. 3 No. 3, pp. 303–326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robertson MM, Tubbs D, Henning RA, Nobrega S, Calvo A and Murphy L (2018), “Designing an organizational readiness survey for Total Worker Health® workplace initiatives”, in Bagnara S, Tartaglia R, Albolino S, Alexander T and Fujita Y (Eds), 20th Congress of the International Ergonomics Association, Vol. 821, pp. 437–445, doi: 10.1007/978-3-319-96080-7_52. [DOI] [Google Scholar]
- Robertson MM, Tubbs D, Henning R, Nobrega S and Calvo A (2021), “Assessment of organizational readiness for participatory occupational safety, health and well-being programs”, Working paper, Department of Psychology, Center for Promotion of Health in the New England Workplace, University of Connecticut, Storrs, Connecticut. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schill AL and Chosewood LC (2016), “Total Worker Health®: more implications for the occupational health nurse”, Workplace Health and Safety, Vol. 64 No. 1, pp. 4–5, doi: 10.1177/2165079915612790. [DOI] [PubMed] [Google Scholar]
- Schill AL, Chosewood LC and Howard J (2019), “The NIOSH Total Worker Health vision”, in Hudson HL, Nigam JAS, Sauter SL, Chosewood LC, Schill AL and Howard J (Eds), Total Worker Health, American Psychological Association, Washington, DC, pp. 29–45. [Google Scholar]
- Schill AL and Chosewood LC (2013), “The NIOSH Total Worker Health™ program: an overview”, Journal of Occupational and Environmental Medicine, Vol. 55, pp. S8–S11, doi: 10.1097/JOM.0000000000000037. [DOI] [PubMed] [Google Scholar]
- Schwatka NV, Tenney L, Dally MJ, Scott J, Brown CE, Weitzenkamp D, Shore E and Newman LS (2018), “Small business Total Worker Health: a conceptual and methodological approach to facilitating organizational change”, Occupational Health Science, Vol. 2 No. 1, pp. 25–41, doi: 10.1007/s41542-018-0013-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sedani A, Stover D, Coyle B and Wani RJ (2019), “Assessing workplace health and safety strategies, trends, and barriers through a statewide worksite survey”, International Journal of Environmental Research and Public Health, Vol. 16 No. 14, p. 2475, doi: 10.3390/ijerph16142475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strickland JR, Kinghorn AM, Evanoff BA and Dale AM (2019), “Implementation of the healthy workplace participatory program in a retail setting: a feasibility study and framework for evaluation”, International Journal of Environmental Research and Public Health, Vol. 16 No. 4, doi: 10.3390/ijerph16040590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Eerd D, Cole D, Irvin E, Mahood Q, Keown K, Theberge N, Village J, St Vincent M and Cullen K (2010), “Process and implementation of participatory ergonomic interventions: a systematic review”, Ergonomics, Vol. 53 No. 10, pp. 1153–1166, doi: 10.1080/00140139.2010.513452. [DOI] [PubMed] [Google Scholar]
- Zhang Y, Flum M, Nobrega S, Blais L, Oamili S and Punnett L (2011), “Work organization and health issues in long-term care centers: comparison of perceptions between caregivers and management”, Journal of Gerontological Nursing, Vol. 37 No. 5, pp. 32–40, doi: 10.3928/00989134-20110106-01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Y, Flum M, West C and Punnett L (2015), “Assessing organizational readiness for a participatory occupational health/health promotion intervention in skilled nursing facilities”, Health Promotion Practice, Vol. 16 No. 5, pp. 724–732, doi: 10.1177/1524839915573945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Y, Flum M, Kotejoshyer R, Fleishman J, Henning R and Punnett L (2016), “Workplace participatory occupational health/health promotion program: facilitators and barriers observed in three nursing homes”, Journal of Gerontological Nursing, Vol. 42 No. 6, pp. 34–42, doi: 10.3928/00989134-20160308-03. [DOI] [PMC free article] [PubMed] [Google Scholar]