

Abstract
Post-operative nausea and vomiting (PONV) is an event of multifactorial origin with an incidence of 30% in the general population. Opioids such as fentanyl are being used as adjuvant to local anesthetic for its antiemetic effect. In this context, with this study we aimed to evaluate the impact of spinal fentanyl as an adjuvant on the incidence of PONV compared with a placebo, and shivering. A systematic search of randomized controlled trials that evaluated the use of spinal fentanyl in the prevention of PONV and shivering was conducted in different databases, of which 32 studies met the inclusion criteria. A total of 2116 patients scheduled for various surgeries, including cesarean section, orthopedic surgery in the lower limb, hysterectomy, and transurethral resection of the prostate, were included in the final analysis. The meta-analysis estimated the relative risk of incidence of PONV in the first 24 hours after surgery and secondary outcomes included the shivering symptom. The use of intrathecal fentanyl was associated with lower incidence of PONV, but not statistically significant when compared to the placebo (RR: 0.74 CI95%: 0.55-1.01 P = 0.06). Subgroup analysis showed a statistically significant reduction in PONV incidences with lower doses between 10 and 15 μg (RR: 0.44 CI95%: 0.35–0.55 P < 0.00001, I2 = 0%) but not with higher doses 20–25 μg. Secondary outcomes showed a decrease in incidence with the use of fentanyl vs the placebo (RR: 0.49, CI95% 0.33-0.72 P = 0.0003). Current evidence shows that the use of spinal fentanyl decreases the incidence of PONV, an effect favored using low doses.
Keywords: Fentanyl, nausea, shivering, vomiting
Introduction
Post-operative nausea and vomiting (PONV) are a perioperative event of multifactorial origin that can occur both in ambulatory and daycare surgeries, with an incidence that varies from 80% in high-risk patients to 30% in the general population.[1,2] In high-risk patients it frequently triggers morbidity beyond patient discomfort and dissatisfaction, including dehydration, bleeding, compromised airway, among others, which interferes with the surgical outcome and quality of life.[3-6] This has led to the attempt to develop multiple strategies to reduce this problem; however, given its multifactorial origin, it continues to be a challenge for the anesthesiologist.
Traditional teaching that the use of opioids favors the generation of nausea and vomiting has been challenged recently as some lipophilic opioids such as fentanyl, frequently used as an adjuvant to local anesthetic in spinal anesthesia, have been shown to have an antiemetic effect.[7] According to Shiraishi-Zapata et al.,[8] there are few Latin-American studies that report PONV in patients operated under general anesthesia. The incidence rate for hospitals in Colombia is 10.9%.[9] The physio-pathological mechanisms that can cause this clinical scenario can be multiple,[10] however intervening in some of them and managing to reduce the incidence of these adverse effects could improve the quality of life in the patient and prevent possible secondary complications of PONV. In the current literature there are no meta-analyses that review this research problem in the general population subjected to spinal anesthesia to unify an intervention, therefore it is important to perform a meta-analysis plus a meta-regression of published, controlled, clinical trials. In the case of finding potentially favourable results for the intervention of spinal fentanyl as prevention of PONV in spinal anesthesia, it would contribute to reduce this condition that leads to greater morbidity in surgical patients.
This meta-analysis sought to evaluate the impact of spinal fentanyl on the incidence of PONV compared to a placebo in patients undergoing a neuraxial anesthetic technique with bupivacaine for various surgeries, including cesarean section, orthopedic surgery in the lower limb, hysterectomy and transurethral resection of the prostate. Moreover, it sought to establish the optimal dose of spinal fentanyl related to the prevention of nausea and vomiting in the postoperative period. It is expected that fentanyl administered intrathecally has a preventive impact on the incidence of PONV.
Material and Methods
This systematic review and meta-analysis were developed using the recommendations made by the Cochrane collaboration,[11] and following the PRISMA statement.[12] This study was not revised by an ethics committee, but the protocol is registered in PROSPERO with ID CRD42020151869.
Inclusion criteria
The following inclusion criteria were used: 1) study design: randomized controlled clinical trials where intervention with intrathecal fentanyl was used as an adjuvant for spinal anesthesia; 2) type of participants: adults older than 18 years undergoing any surgery with spinal anesthesia; 3) type of intervention: all interventions with spinal fentanyl related to nausea and vomiting, compared with placebo; 4) type of primary outcome: Incidence of PONV; 5) type of secondary outcome: Reduction of postoperative shivering.
Exclusion criteria
We excluded quasi-randomized trials and studies conducted in patients under 18 years of age. Also, clinical trials in which spinal anesthesia was performed with local anesthetics other than bupivacaine or used other adjuvants (midazolam, clonidine, morphine) with or without fentanyl. Finally, clinical trials that used different doses of bupivacaine between the control and study groups were excluded.
Research strategy
A literature search was conducted in the main databases from 1975 to December 2018, such as MEDLINE, Google Scholar, and EMBASE. In addition, to reduce publication bias, the search was carried out on the individual citations of the articles found. No language or date restrictions were applied from the 1975 until December 2018 for articles that met the inclusion criteria. A combination of the terms fentanyl, ondansetron, nausea and vomiting, postoperative, spinal anesthesia, was used for the search in all the databases as follows: 1) fentanyl (Mesh) AND placebos (Mesh) AND nausea and vomiting, postoperative (Mesh) AND spinal anesthesia (Mesh); 2) fentanyl AND placebos AND nausea, postoperative; 3) “spinal fentanyl” AND “placebos” AND nausea AND vomiting.
Study selection
Two authors independently assessed the inclusion criteria in all selected studies by title and abstract. Disagreements were resolved with a third author or through dialogue. A table was designed in Excel to extract data. Two authors extracted the data from the studies chosen with full text, and in the case of disagreements, the issue was resolved with a third author. The data was entered into the Stata software to assess its accuracy.
Statistical analysis
The methodological quality of the studies was analysed using the Cochrane risk of bias assessment tool [Figure 1]. In addition, an initial exploratory analysis was performed with the data extracted from each article, the main variables were tabulated and then the incidences of the primary outcome were expressed as percentages for each group, both intervention and placebo. A meta-analysis was performed for each outcome using the Review Manager program version 5.3 (Cochrane).
Figure 1.

Risk of bias assessment. Source: Original
Results
Research results
The articles obtained in the literature search were independently reviewed by two of the authors. A total of 2187 articles were identified in different databases. After first eliminating duplicate studies and selecting articles based on inclusion criteria, 40 articles were found and full texts were reviewed. Thirteen articles were subsequently eliminated based on inclusion criteria and exclusion criteria, and five additional articles were identified and included for a total of 32 studies [Figure 2]. One of the studies, by Seewal et al.,[13] was analysed as two different datasets for the meta-analysis.
Figure 2.
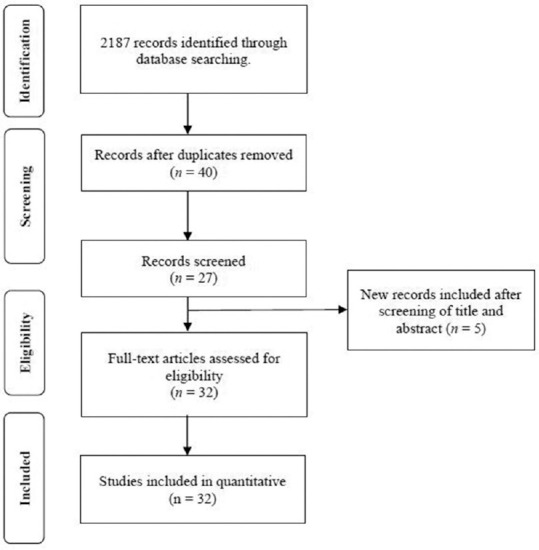
PRISMA flow chart for the selection of studies. Source: Original
Study characteristics
A total of 2116 patients scheduled for various surgeries, including cesarean section, orthopedic surgery in the lower limb, hysterectomy, and transurethral resection of the prostate, were included in the final analysis. All patients underwent spinal anesthesia with 0.5% or 0.75% hyperbaric bupivacaine (HB) with doses between 10 and 15 mg. Fentanyl was added to the intervention group at doses between 10 and 25 μg, while the control group was treated with HB with or without the addition of normal saline solution [Table 1].
Table 1.
Characteristics of the studies included in the systematic review. Source: Original
| Study | Surgery | n (total) | Dose - intervention group (HB mg+F µg) | Dose - placebo group (HB mg or HB mg+SS mL) | Nausea/vomiting - Intervention | Nausea/vomiting - placebo |
|---|---|---|---|---|---|---|
| Ahmed et al. 2017[32] | Hysterectomy | 164 | 15 mg+25 µg | 15 mg+0.5 mL | 0 | 2 |
| Akanmu et al. 2013[25] | Orthopedic in lower extremity | 60 | 10 mg+25 µg | 10 mg+0.5 mL | 4 | 6 |
| Belzarena et al. 1992[33] | Cesarean section | 60 | 15 mg+25 µg | 15 mg+0.5 mL | 4 | 3 |
| Bharti et al. 2015[34] | Transurethral resection of the prostate | 40 | 10 mg+25 µg | 10 mg | 4 | 3 |
| Bhattacharje et al. 2015[22] | Cesarean section | 60 | 10 mg+25 µg | 10 mg+0.5 mL | 13 | 2 |
| Bhure et al. 2012[35] | Cesarean section | 60 | 11 mg+25 µg | 11 mg+0.5 mL | 2 | 3 |
| Biswas et al. 2002[36] | Cesarean section | 80 | 10 mg+12.5 µg | 10 mg+0.25 mL | 1 | 8 |
| Charan et al. 2018[27] | Orthopedics in the lower extremity | 50 | 15 mg+20 µg | 15 mg | 1 | 5 |
| Farzi et al. 2017[20] | Cesarean section | 66 | 12.5 mg+25 µg | 12.5 mg+0.5 mL | 2 | 5 |
| Hassani et al. 2014[19] | Orthopedics in the lower extremity | 60 | 15 mg+25-30 µg | 15 mg+0.5-0.6 mL | 7 | 1 |
| Indurkar et al. 2015[26] | Cirugía abdomen inferior y miembro inferior | 60 | 13 mg+12.5 µg | 13 mg | 1 | 4 |
| Kazemnejad et al. 2018[27] | Orthopedics in the lower extremity | 50 | 15 mg+25 µg | 15 mg+0.5 mL | 14 | 8 |
| Khan et al. 2006[37] | Transurethral resection of the prostate | 40 | 15 mg+10 µg | 15 mg | 3 | 1 |
| Khezri et al. 2014[38] | Cesarean section | 60 | 10 mg+25 µg | 10 mg+0.5 mL | 7 | 4 |
| Kumar et al. 2016[39] | Cesarean section | 100 | 10 mg+12.5 µg | 10 mg+0.5 mL | 19 | 37 |
| Li et al. 2014[40] | Cesarean section | 42 | 10 mg+15 µg | 10 mg+2 mL | 4 | 4 |
| Lim et al. 2006[41] | Orthopedics in the lower extremity | 36 | 4 mg+15 µg | 4 mg | 0 | 0 |
| Meshram et al. 2016[42] | Cesarean section | 100 | 10 mg+25 µg | 10 mg+0.5 mL | 8 | 29 |
| Motiani et al. 2010[43] | Orthopedics in the lower extremity | 70 | 15 mg+25 µg | 15 mg+0.5 mL | 4 | 3 |
| Pallavi et al. 2017[44] | Lower abdomen | 80 | 15 mg+25 µg | 15 mg+0.5 mL | 10 | 15 |
| Paulraj et al. 2018[45] | Cesarean section | 60 | 8.5 mg+25 µg | 8.5 mg+0.5 mL | 0 | 3 |
| Rahimzadeh et al. 2018[46] | Orthopedics in the lower extremity | 60 | 12.5 mg+25 µg | 12.5 mg+0.5 mL | 1 | 4 |
| Randalls et al. 1991[47] | Cesarean section | 24 | 12.5 mg+10 µg | 12.5 mg+0.5 mL | 0 | 3 |
| Rudra et al. 2004[48] | Cesarean section | 80 | 10 mg+12.5 µg | 10 mg+0.5 mL | 10 | 30 |
| Sadegh et al. 2012[49] | Cesarean section | 80 | 12.5 mg+25 µg | 12.5 mg+0.5 mL | 11 | 27 |
| Safari et al. 2016[50] | Orthopedic in the lower extremity or lower abdomen | 56 | 12.5 mg+25 µg | 12.5 mg | 11 | 6 |
| Safavi et al. 2014[51] | Orthopedics in the lower extremity | 60 | 15 mg+20 µg | 15 mg+0.5 mL | 2 | 2 |
| Seewal et al. 2007[13] | Lower abdomen | 24 | 11 mg+10 µg | 11 mg+0.8 mL | 1 | 2 |
| Seewal et al. 2007 (B)[13] | Lower abdomen | 24 | 11 mg+20 µg | 11 mg+0.8 mL | 1 | 2 |
| Shaikh et al. 2015[52] | Cesarean section | 60 | 10 mg+12.5 µg | 10 mg+0.5 mL | 8 | 24 |
| Shashikala et al. 2014[53] | Cesarean section | 90 | 10 mg+12.5 µg | 10 mg+0.5 mL a) LCR | 6 | 8 |
| Shim et al. 2018[54] | Anorectal | 80 | 5 mg+15 µg | 5 mg+0.3 mL | 0 | 1 |
| Uike S et al. 2015[23] | Cesarean section | 80 | 10 mg+12.5 µg | 10 mg | 3 | 10 |
F: Fentanyl, HB: hyperbaric bupivacaine, HB+SS: hyperbaric bupivacaine with saline solution
Primary outcome
In the intervention group there was a decrease in nausea and vomiting when compared with the control group [171 vs 253 events (RR: 0.74 95% CI 0.55-1.01 P = 0.06)]. It is important to mention that these data are marked as heterogeneous I2 = 56 = 56%, so it was decided to perform a subgroup analysis based on the dose of fentanyl that was used (Subgroup 1: 10-15 μg vs Subgroup 2: 20-25 μg). Only in the subgroup of low doses, the decrease of nausea and vomiting persisted in the intervention group compared to the control group (RR: 0.44 95% CI 0.35-0.55 P < 0.00001, I2 = 0%). This is suggestive of a significant antiemetic effect with spinal fentanyl at low doses [Figure 3].
Figure 3.

Forest plot comparing fentanyl versus placebo for the outcome Nausea and postoperative vomiting. Source: Original
Secondary outcomes
In the secondary outcome, shivering was reduced in the group that used spinal fentanyl compared to the placebo group [Figure 4]. In the intervention group with low doses of fentanyl shivering, we observed a decrease when compared the control group [14 vs 35 events (RR: 0.35 95% CI 0.16-0.77 P = 0.009)]. The same occurred in the dose group between 20 and 25 μg, where 22 vs 41 events were presented in the intervention group and in the control group respectively (RR: 0.58 95% CI 0.36–0.93 P = 0.94). When estimating for both groups, a protection trend against shivering was maintained in the fentanyl group vs. placebo (RR: 0.49, 95% CI 0.33–0.72 P = 0.0003).
Figure 4.

Forest plot comparing fentanyl versus placebo for the outcome shivering. Source: Original
Discussion
Our meta-analysis estimated the relative risk of incidence of PONV in the first 24 hours after surgery and secondary outcomes included shivering symptom, also the use of intrathecal fentanyl was associated with lower incidence of PONV, but without statistical significance, when compared to the placebo. According to our results, the use of spinal fentanyl decreases the incidence of PONV, an effect favored with the use of low doses.
One of the most common and distressing symptoms that follow general and neuraxial anesthesia and surgery is PONV.[14] The causes of PONV are multifactorial, including hypotension due to sympathetic block/dehydration, hypoxemia in the center of vomiting, traction of the local peritoneum and the patient’s own risk factors.[15] When assessing the risk of PONV for a particular patient, it is important to know which factors are independent predictors and which are not relevant, in order to predict a possible PONV.[16] If anesthesia is not administered properly, one-third of patients who undergo surgery will have postoperative nausea and vomiting. According to our systematic review, of the 32 articles included in the meta-analysis, n = 2116 patients, 427 of these (21%) manifested nausea and/or vomiting. There are very varied estimates of the incidence of PONV, the probable result of the diverse set of patients, surgical procedures and chemical products used during anesthesia, giving an estimated incidence of PONV of approximately 30%.[17]
Many trials have been published, but the relative benefits/advantages of prophylactic antiemetic interventions remain unclear. Experimental studies on the relationship of opioids and their antiemetic effect have been described based on multiple reasons: 1) dose-dependent effect, 2) selectivity of opioids for different opioid receptors and their location, and 3) genetic polymorphisms.[17] Fentanyl, being more lipid soluble, is more potent and binds to μ receptors with high affinity; These μ receptors are located in different parts of the central nervous system (CNS), such as in the nucleus of the solitary tract, which when stimulated, have an antiemetic effect. Therefore, the potential antiemetic effect of fentanyl has been established from this explanation.[17,18] In addition to this, the μ receptors have different μ1 and μ2 subunits which mediate emetic and antiemetic effects respectively.
Due to the fact that PONV has become a problem after surgery due to patient satisfaction, discharge and financial impacts, a large number of investigations have focused on the efficacy of individual drugs and antiemetic drug combinations.[19,20] According to our meta-analysis, we observed that there were significant differences in the reduction of nausea and vomiting events in those patients who had been anesthetized with a combination of fentanyl plus HB. It should be noted that low doses of fentanyl (10 to 15 μg), with an average of 12.5 μg, showed a greater antiemetic effect compared with doses of 20 to 25 μg. This same pattern could be observed in the secondary event “ shivering “, where low doses of fentanyl had a higher protective effect over this adverse event [Figures 3 and 4]. These results can be attributed to the low dose used, the fentanyl itself, or both factors combined, have an influence on the low incidence of PONV and shivering. However, as with this study, we cannot know for certain which hypothesis is most accurate, it is appropriate to continue investigations regarding this matter.
Based on the results of the studies included in this systematic review and meta-analysis, it was observed that most of the research on PONV has been performed in patients undergoing cesarean sections; 50% of the articles evaluated were focused on the improvement of vomiting and nausea in the parturient. Of the 1062 patients who were included in these studies, 28% (n = 298) reported vomiting. The percentage of patients with PONV coincides with that reported in the literature.[17] It should be noted that, in the 16 studies on cesarean sections included in our analysis, the group of women who were anesthetized with the combination of HB plus fentanyl, showed a 67% reduction in PONV during spinal anesthesia in comparison to those that were only anesthetized with HB and saline solution.
On the basis of different comparative clinical studies, it has been shown that the addition of 12.5 mg of fentanyl and 0.5% isobaric bupivacaine for spinal anesthesia produces minimal intraoperative and postoperative side effects,[21,22] and that fentanyl is a good option for the prevention of perioperative nausea and vomiting in the parturient undergoing cesarean section compared to other anesthetics.[23] It is known that fentanyl, a short-acting, lipophilic synthetic opioid, improves the quality of spinal anesthesia and has been used both widely and successfully. The effect of adding a small dose of fentanyl to the local anesthetic solution is profound and decreases the possible side effects of neuraxial anesthesia.[24]
Orthopedic surgeries in the lower limb were the second most common group of surgeries included in our review (n = 7). We found that in those seven articles only 17% of patients presented postoperative vomiting; furthermore, when studying the number of patients with PONV treated with the different combinations of medications, it was found that the group of patients treated with the placebo (HB + saline), presented a decrease in vomiting when compared with the intervention group. Although in our meta-analysis a significant antiemetic effect was found when using spinal fentanyl at low doses in the intervention group [Figure 3], the results of subgroup analysis with this type of surgery show one of the limitations of our study, since in this meta-analysis we did not consider the influence of each particular type of surgery. It has been shown that the addition of 25 μg of fentanyl to 10 mg of 0.5% HB significantly prolonged the duration of complete analgesia, as well as effective analgesia, thus reducing the need for an early use of postoperative analgesics without an increase in adverse effects due to administration of fentanyl in spinal anesthesia during these type of surgeries.[25,26]
Several studies have shown the synergism and efficacy of opioid and local anesthetics when used in combination, for the control of PONV. Although in some cases, medication alone appears to be similar in efficacy when used as individual agents; [23,26,27]the addition of opioids such as fentanyl to HB in spinal anesthesia reduces latency, significantly prolongs duration and improves the efficacy of analgesia, when compared to bupivacaine alone.[28] Being an opioid, Fentanyl exerts its effects when combined with opioid receptors in the dorsal horn of the spinal cord and may have supraspinal action and propagation. The addition of 12.5 mg of fentanyl to 13 mg of 0.5% HB for spinal anesthesia in cesarean section provides good intraoperative treatment and significantly reduces the demand for analgesics, producing minimal intraoperative and postoperative side effects.[23] Other systematic reviews have been published in regards to the use of fentanyl in different surgeries,[29-31] but we focused not only on cesarean section, but also on other surgeries such as orthopedic surgery in the lower limb, hysterectomy, and transurethral resection of the prostate, to evaluate the effect of spinal fentanyl as an adjuvant on the incidence of PONV and shivering.
Conclusions
The combination of HB and spinal fentanyl at doses of 10 to 15 μg significantly decreased PONV in patients who received spinal anesthesia. Therefore, spinal fentanyl helps in decreasing the incidence of postoperative nausea and vomiting. Moreover, our results suggest a significant antiemetic effect with spinal fentanyl at low doses. The criteria for spinal anesthesia should be defined in future research, considering the type of surgery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Stoops S, Kovac A. New insights into the pathophysiology and risk factors for PONV. Best Pract Res Clin Anaesthesiol. Published online 2020. doi: 10.1016/j.bpa.2020.06.001. doi: https://doi.org/10.1016/j.bpa.20200.06.001. [DOI] [PubMed] [Google Scholar]
- 2.Suleiman Obsa M, Chemeda Edosa D, Muluken Desalegn Z, Desalegn Fanta N, Mulugeta Tamiru S, Tesfaye Mokenin G. Incidence of post-operative nausea and vomiting and it's predictors among adult elective surgical patients at Jimma Medical Center, South West Ethiopia. Res Sq. Published online 2020. doi:10.21203/rs. 3.rs-19271/v1. [Google Scholar]
- 3.Atallah F, Riu B, Nguyen L, Seguin P, Fourcade O. Boerhaave's syndrome after postoperative vomiting. Anesth Analg. 2004;98:1164–6. doi: 10.1213/01.ANE.0000101981.85523.82. [DOI] [PubMed] [Google Scholar]
- 4.Gan TJ. Risk Factors for postoperative nausea and vomiting. Anesth Analg. 2006;102:1884–98. doi: 10.1213/01.ANE.0000219597.16143.4D. [DOI] [PubMed] [Google Scholar]
- 5.Le TP, Gan TJ. Update on the management of postoperative nausea and vomiting and postdischarge nausea and vomiting in ambulatory surgery. Anesthesiol Clin. 2010;28:225–49. doi: 10.1016/j.anclin.2010.02.003. [DOI] [PubMed] [Google Scholar]
- 6.Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid?The perspective of patients. Anesth Analg. 1999;89:652–8. doi: 10.1097/00000539-199909000-00022. [DOI] [PubMed] [Google Scholar]
- 7.Swain A, Nag DS, Sahu S, Samaddar DP. Adjuvants to local anesthetics:Current understanding and future trends. World J Clin Cases. 2017;5:307. doi: 10.12998/wjcc.v5.i8.307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shiraishi-Zapata CJ, Arellano-Adrianzén SJ, Rodríguez-Velarde GJ. Cumulative incidence and risks factors for postoperative nausea and vomiting in adult patients undergoing cholecystectomy under balanced general anesthesia:A prospective cohort study. Rev Colomb Anestesiol. 2020;48:3–11. [Google Scholar]
- 9.Gempeler Rueda F, Miranda Pineda N, Garrido Hartmann A, Echeverry Lombana M, Tobos González L, Acosta Fernández C. Incidencia de náusea y vómito postoperatorio y factores asociados en el Hospital Universitario de San Ignacio. Univ Médica. 2016;57:11–21. [Google Scholar]
- 10.Borgeat A, Ekatodramis G, Schenker CA. Postoperative nausea and vomiting in regional anesthesia. A review. Anesthesiol J Am Soc Anesthesiol. 2003;98:530–47. doi: 10.1097/00000542-200302000-00036. [DOI] [PubMed] [Google Scholar]
- 11.Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. Chichester: John Wiley &Sons; 2019. [Google Scholar]
- 12.Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015:Elaboration and explanation. BMJ Br Med J. 2015;349:g7647. doi: 10.1136/bmj.g7647. [DOI] [PubMed] [Google Scholar]
- 13.Seewal R, Shende D, Kashyap L, Mohan V. Effect of addition of various doses of fentanyl intrathecally to 0.5% hyperbaric bupivacaine on perioperative analgesia and subarachnoid-block characteristics in lower abdominal surgery:A dose-response study. Reg Anesth Pain Med. 2007;32:20–6. doi: 10.1016/j.rapm.2006.09.007. [DOI] [PubMed] [Google Scholar]
- 14.Shaikh SI, Govindaraju C, Hegade G. Comparison of intrathecal fentanyl and midazolam for prevention of nausea-vomiting during cesarean section under spinal anesthesia. Anaesth Pain Intensive Care. 2015;19:124–9. [Google Scholar]
- 15.Shaikh S, Nagarekha D, Hegade G, Marutheesh M. Postoperative nausea and vomiting:A simple yet complex problem. Anesth Essays Res. 2016;10:388–96. doi: 10.4103/0259-1162.179310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Apfel CC. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med. 2004;351:1493–501. doi: 10.1056/NEJMoa032196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Horn CC, Wallisch WJ, Homanics GE, Williams JP. Pathophysiological and neurochemical mechanisms of postoperative nausea and vomiting. Eur J Pharmacol. 2014;722:55–66. doi: 10.1016/j.ejphar.2013.10.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Johnston K. The potential for m -opioid receptor agonists to be anti-emetic in humans:A review of clinical data. Acta Anaesthesiol Scand. 2010;54:132–40. doi: 10.1111/j.1399-6576.2009.02115.x. [DOI] [PubMed] [Google Scholar]
- 19.Hassani V, Movassaghi G, Safaian R, Safari S, Zamani MM, Hajiashrafi M, et al. Bupivacaine-sufentanil versus bupivacaine-fentanyl in spinal anesthesia of patients undergoing lower extremity surgery. Anesthesiol Pain Med. 2014;4:1–6. doi: 10.5812/aapm.12091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Farzi F, Mirmansouri A, Naderi Nabi B, Atrkar Roushan Z, Ghazanfar Tehran S, Nematollahi Sani M, et al. Comparing the Effect of Adding Fentanyl, Sufentanil, and Placebo with Intrathecal Bupivacaine on Duration of Analgesia and Complications of Spinal Anesthesia in Patients Undergoing Cesarean Section. Anesth Pain Med. 2017;7:e12738. doi: 10.5812/aapm.12738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jain P, Jigar J, Raval B. Comparision of intrathecal fentanyl and intravenous ondansetron for prevention of perioperative nausea and vomiting during cesarean delivery under spinal anesthesia. Int J Curr Pharm Clin Res. 2015;5:109–13. [Google Scholar]
- 22.Bhattacharjee A, Singh NR, Singh SS, Debbrama B, Debbarma P, Singh TH. A comparative study of intrathecal clonidine and fentanyl along with bupivacaine in spinal anesthesia for cesarean section. J Med Soc. 2015;29:145–9. [Google Scholar]
- 23.Uike S, Choudhary S, Jain A. Comparative study of analgesic effect of intrathecal bupivacaine and bupivacaine with fentanyl during and after cesarean delivery. Int J Med Res Rev. 2015;3:256–62. [Google Scholar]
- 24.Akhtar N, Quadir A, Athar M, Singh N. Recovery profile of intrathecal ropivacaine with or without fentanyl:A randomized double-blind controlled trial in equivalent doses. Int J Heal Allied Sci. 2016;5:158–63. [Google Scholar]
- 25.Akanmu ON, Soyannwo OA, Sotunmbi PT, Lawani-osunde AS, Desalu I. Analgesic effects of intrathecally administered fentanyl in spinal anesthesia for lower limb surgery. Maced J Med Sci. 2013;6:255–60. [Google Scholar]
- 26.Indurkar PS, Saibaba S. A comparative study of hyperbaric bupivacaine versus hyperbaric bupivacaine and fentanyl (12.5 mcg) in subarachnoid anesthesia for lower abdominal and lower extremity surgeries. Int J Res Med Sci. 2015;3:3147–55. [Google Scholar]
- 27.Charan P, Nanda S, Kumar Gouni U. International journal of scientific research comparative study of the effect of intrathecal fentanyl on the quality of hyperbaric bupivacaine induced subarachnoid block in Anesthesiology Dr. Uday Kumar Gouni. Int J Sci Res. 2018;7:11–2. [Google Scholar]
- 28.Piñeiro Casado E, Domínguez González E, Muguercia Sarracen K, de Arma U. Anestesia espinal con bupivacaína más fentanyl en pacientes con fractura de cadera. MEDISAN. 2017;21:250–7. [Google Scholar]
- 29.Pöpping DM, Elia N, Marret E, Wenk M, Tramr MR. Opioids added to local anesthetics for single-shot intrathecal anesthesia in patients undergoing minor surgery:A meta-analysis of randomized trials. Pain. 2012;153:784–93. doi: 10.1016/j.pain.2011.11.028. [DOI] [PubMed] [Google Scholar]
- 30.Uppal V, Retter S, Casey M, Sancheti S, Matheson K, McKeen DM. Efficacy of intrathecal fentanyl for cesarean delivery:A systematic review and meta-analysis of randomized controlled trials with trial sequential analysis. Anesth Analg. 2020;130:111–25. doi: 10.1213/ANE.0000000000003975. [DOI] [PubMed] [Google Scholar]
- 31.Sun SJ, Wang JM, Bao NR, Chen Y, Wang J. Comparison of dexmedetomidine and fentanyl as local anesthetic adjuvants in spinal anesthesia:A systematic review and meta-analysis of randomized controlled trials. Drug Des Devel Ther. 2017;11:3413–24. doi: 10.2147/DDDT.S146092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ahmed F, Khandelwal M, Sharma A. A comparative study of the effect of clonidine, fentanyl, and the combination of both as adjuvant to intrathecal bupivacaine for postoperative analgesia in total abdominal hysterectomy. J Anaesthesiol Clin Pharmacol. 2017;33:102–6. doi: 10.4103/0970-9185.202194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Belzarena SD. Clinical effects of intrathecally administered fentanyl in patients undergoing cesarean section. Anesth Analg. 1992;74:653–7. doi: 10.1213/00000539-199205000-00006. [DOI] [PubMed] [Google Scholar]
- 34.Bharti N, Batra Y, Negi S. Efficacy of intrathecal midazolam versus fentanyl for endoscopic urology surgery. South African J Anaesth Analg. 2015;21:13–6. [Google Scholar]
- 35.Bhure A, Kalita N, Ingley P, Gadkari CP. Comparative study of intrathecal hyperbaric Bupivacaine with Clonidine, Fentanyl and Midazolam for quality of anesthesia and duration of post opera- tive pain relief in patients undergoing elective cesarean section. Peoples J Sci Res. 2012;5:19–23. [Google Scholar]
- 36.Biswas B, Rudra A, Bose B, Nath S, Chakrabarty S, Bhattacharjee S. Intrathecal fentanyl with hyperbaric bupivacaine improves analgesia during cesarean delivery and in early post- operative period. Indian J Anaesth. 2002;46:469–72. [Google Scholar]
- 37.Khan F, Hamdani G. Comparison of intrathecal fentanyl and buprenorphine in urological surgery. J Pak Med Assoc. 2006;56:277–81. [PubMed] [Google Scholar]
- 38.Khezri MB, Tahaei E, Atlasbaf AH. Comparison of postoperative analgesic effect of intrathecal Ketamine and fentanyl added to bupivacaine in patients undergoing cesarean section:A prospective randomized double-blind study. Middle East J Anesthesiol. 2014;23:427–36. [PubMed] [Google Scholar]
- 39.Kumar K, Somani S, Babu K. Comparative study to evaluate antiemetic efficacy of intrathecal fentanyl and midazolam for lower segment cesarean section in subarchnoid block. IOSR J Dent Med Sci. 2016;15:49–53. [Google Scholar]
- 40.Li Z, Tian M, Zhang CY, Li AZ, Huang AJ, Shi CX, et al. A randomised controlled trial to evaluate the effectiveness of intrathecal bupivacaine combined with different adjuvants (fentanyl, clonidine and dexmedetomidine) in cesarean section. Drug Res (Stuttg) 2015;65:581–6. doi: 10.1055/s-0034-1395614. [DOI] [PubMed] [Google Scholar]
- 41.Lim Y, Jung J, Lim K, So K. Effect of intrathecal fentanyl with hyperbaric bupivacaine on unilateral spinal anesthesia for knee arthroscopy. Korean J Anesth. 2006;50:530–5. [Google Scholar]
- 42.Meshram S. Comparison of intrathecal fentanyl and midazolam as an adjuvant to bupivacaine for enhancing the quality of subarachnoid block and thereby preventing nausea and vomiting in cesarean delivery. J Evid Based Med Healthc. 2016;3:5393–9. [Google Scholar]
- 43.Motiani P, Chaudhary S, Bahl N, Sethi AK. Intrathecal sufentanil versus fentanyl for lower limb surgeries -A randomized controlled trial. J Anaesthesiol Clin Pharmacol. 2010;26:507–13. [PMC free article] [PubMed] [Google Scholar]
- 44.Pallavi P, Choubey S, Sarkar A. Comparison between Fentanyl as an adjuvant to Bupivacaine versus Bupivacaine alone among patients undergoing lower abdominal surgeries under sub arachnoid block. Central Journal of ISA. 2017;1:64–71. [Google Scholar]
- 45.Paulraj S, Kumaran C. Evaluation of the efect of intrathecal fentanyl citrate as an adjuvant with hyperbaric bupivacaine for cesarean. Indian J Appl Res. 2018;8:16–8. [Google Scholar]
- 46.Rahimzadeh P, Faiz SHR, Imani F, Derakhshan P, Amniati S. Comparative addition of dexmedetomidine and fentanyl to intrathecal bupivacaine in orthopedic procedure in lower limbs. BMC Anesthesiol. 2018;18:1–7. doi: 10.1186/s12871-018-0531-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Randalls B, Broadway JW, Browne DA, Morgan BM. Comparison of four subarachnoid solutions in a needle-through-needle technique for elective cesarean section. Br J Anaesth. 1991;66:314–8. doi: 10.1093/bja/66.3.314. [DOI] [PubMed] [Google Scholar]
- 48.Rudra P, Rudra A. Comparison of intrathecal fentanyl and midazolam for prevention of nausea-vomiting during cesarean delivery under spinal anesthesia. Indian J Anaesth. 2004;48:461–4. [Google Scholar]
- 49.Sadegh A, Tazeh-kand NF, Eslami B. Intrathecal fentanyl for prevention of shivering in spinal anesthesia in cesarean section. Med J Islam Repub Iran. 2012;26:85–9. [PMC free article] [PubMed] [Google Scholar]
- 50.Safari F, Aminnejad R, Mohajerani SA, Farivar F, Mottaghi K, Safdari H. Intrathecal dexmedetomidine and fentanyl as adjuvant to bupivacaine on duration of spinal block in addicted patients. Anesthesiol Pain Med. 2016;6:1–7. doi: 10.5812/aapm.26714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Safavi M, Honarmand A, Rahmanikhah E, Badiei S, Attari M. Intrathecal Meperidine versus intrathecal Fentanyl for prevention of shivering in lower limb orthopedic surgeries under spinal anesthesia:A randomized double-blind placebo-controlled trial. J Res Pharm Pract. 2014;3:137–41. doi: 10.4103/2279-042X.145390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Shaikh S, Govindaraju C, Hegade G. Comparison of intrathecal fentanyl and midazolam for prevention of nausea-vomiting during cesarean section under spinal anesthesia. Anaesth Pain Intensive Care. 2015;19:124–9. [Google Scholar]
- 53.Shashikala T, Srinivas V. A clinical study of effect of spinal fentanyl on subarchnoid block in parturients. J Evol Med Dent Sci. 2014;3:8980–90. [Google Scholar]
- 54.Shim S, Park J, Hyun D, Jeong E, Kim S, Lee H. The effects of adjuvant intrathecal fentanyl on postoperative pain and rebound pain for anorectal surgery under saddle anesthesia. Korean J Anesthesiol. 2018;71:213–9. doi: 10.4097/kja.d.18.27097. [DOI] [PMC free article] [PubMed] [Google Scholar]