

Abstract
Background
Preliminary evidence suggests that psychological trauma, especially childhood trauma, is a risk factor for the onset of fibromyalgia (FM).
Objective
The main objective of this study consisted of evaluating the prevalence and detailed characteristics of psychological trauma in a sample of patients with FM, the chronology of trauma across the lifespan, and its clinical symptoms. We also calculated whether childhood trauma could predict the relationship with different clinical variables.
Method
Eighty-eight females underwent an interview to assess sociodemographic data, psychiatric comorbidities, level of pain, FM impact, clinical symptoms of anxiety, depression, insomnia, quality of life, and psychological trauma.
Results
The majority of participants (71.5%) met the diagnostic criteria for current post-traumatic stress disorder (PTSD). Participants reported having suffered traumatic events throughout their lifespan, especially in childhood and early adolescence, in the form of emotional abuse, emotional neglect, sexual abuse, and physical abuse. Traumatic events predict both poor quality of life and a level of pain in adulthood. All patients showed clinically relevant levels of anxiety, depression, insomnia, suicidal thoughts, and pain, as well as somatic comorbidities and poor quality of life. Pain levels predicted anxiety, depression, dissociation, and insomnia symptoms. 84% of the sample suffered one or more traumatic events prior to the onset of pain.
Conclusions
Our data highlight the clinical complexity of patients with FM and the role of childhood trauma in the onset and maintenance of FM, as well as the high comorbidity between anxiety, depression, somatic symptoms, and FM. Our data also supports FM patients experiencing further retraumatization as they age, with an extremely high prevalence of current PTSD in our sample. These findings underscore the need for multidisciplinary programs for FM patients to address their physical pain and their psychiatric and somatic conditions, pay special attention to the assessment of psychological trauma, and provide trauma-focused interventions. Trial registration: ClinicalTrials.gov NCT04476316. Registered on July 20th, 2020.
1. Introduction
Fibromyalgia (FM) is considered the second most common rheumatic disorder [1] and affects between 2% and 4% of the population worldwide, in the majority of cases females [2]. In addition, FM is often diagnosed alongside chronic fatigue syndrome (CFS), due to the overlap between their symptoms and their underlying biological mechanisms [3]. Although the etiology of FM remains unknown [4], several explanations have been proposed for the onset of FM, including genetic factors [5, 6], hormonal and immunological alterations [7], nutritional aspects [4], and abnormalities in central pain processing [4, 8] linked to the sensitization of the central nervous system (CNS) [4, 5, 9]. In fact, the sensitization of the CNS has been suggested as one of the main pathophysiological changes involved in FM, involving neurotransmitter imbalances, altered functional connectivity, and changes in the hypothalamic-pituitary-adrenal (HPA) axis, which influence the autonomic nervous system [5, 10, 11]. Interestingly, exposure to different chronic or acute stressors, including psychological trauma, has a significant impact on the dysregulation of the HPA axis [12]. Psychological trauma is defined as a stressful life event that causes distress and exceeds an individual's ability to integrate the emotions and cognitions involved in the experience [13]. These events happen in an unexpected and uncontrollable manner, putting the individual's physical and psychological integrity at risk, exceeding their coping resources and leading to responses of helplessness and fear [14]. In some cases, exposure to one or more traumatic events can result in a diagnosis of PTSD [15, 16] or the presence of traumatic symptoms that cause discomfort without meeting the necessary criteria for a PTSD diagnosis [17]. Trauma exposure can happen throughout the entire lifespan of a person, but if it occurs during childhood, its psychopathological and somatic consequences are severe due to the vulnerability of the CNS during infancy and adolescence [18,19]. In this sense, childhood trauma or adverse childhood experiences (ACEs) encompasses various forms of physical and emotional abuse or neglect, sexual abuse, bullying, or household dysfunction experienced in childhood. Along these lines, several studies have investigated the relationship between childhood trauma and FM [5, 20–22], and have found a strong association. More specifically, these studies have shown that women diagnosed with FM score higher on the childhood trauma questionnaire (CTQ) as compared to controls [23, 24] or other medical conditions such as migraine, rheumatoid arthritis, and myofascial pain syndrome [23, 25–27]. Further studies showed a higher prevalence of emotional abuse [24, 25] and physical neglect [23] in patients with FM compared with controls, and higher scores in emotional abuse [25, 27], emotional neglect [27], physical neglect [27], and physical abuse [26], in comparison with patients affected by rheumatoid arthritis and migraine. All this data seems to indicate that childhood trauma can be considered a risk factor for the development of unexplained physical pain [28, 29], especially for FM.
Despite all the studies that highlight the relationship between childhood trauma and FM, few studies have collected in detail the chronology of the traumatic events to which these patients are exposed throughout their lifespan, from infancy to adulthood, as well as information on whether these events occurred mainly before or after the onset of pain. Likewise, many studies have focused on studying the correlation between trauma and pain. However, there is a lack of studies on possible predictor variables that explain the relationship between childhood trauma, pain, and the presence of psychiatric comorbidities, which are highly prevalent in this population and significantly affect the functionality and quality of life of the patients.
Our study aimed to analyze the prevalence and clinical characterization of traumatic events present in women with a principal diagnosis of FM and to what extent these events can predict pain levels, the presence and intensity of affective symptoms, psychiatric comorbidity, insomnia, and quality of life.
2. Materials and Methods
2.1. Participants of the Study
The study sample consisted of 90 female participants diagnosed with FM, who were consecutively derived from the rheumatology service (n = 42) and from the adult mental health services (n = 30) of the Parc de Salut Mar in Barcelona, Spain. Further participants (n = 18) from the catchment area learnt about the study through word of mouth or from local FM associations and contacted researchers to voluntarily enroll. The study was conducted between January 2020 and January 2021. All women were evaluated through an individual clinical interview that lasted approximately 1.5 hours and was conducted by two psychologists from the forum center research unit. In some cases, the assessments were carried out in person, but when participants were not able to attend the interviews because of COVID-19-related restrictions, clinical evaluations were carried out online.
Participants had to fulfill the following inclusion criteria: (1) women with an FM diagnosis based on a clinical interview aligned with the American college of rheumatology criteria [30], and (2) aged between 18 and 70 years. The exclusion criteria are as follows: (1) comorbid chronic inflammatory or autoimmune disorders; (2) neurodegenerative disorders, which can interfere in the development of the clinical interviews; (3) severe mental disorders, namely bipolar disorder, schizoaffective disorder, or schizophrenia. Of note, major depressive disorder and anxiety disorders were not excluded as exclusion criteria due to the high prevalence of these disorders in patients with FM; (4) present active suicidal ideation; and (5) dependence or substance abuse (except nicotine) in the previous month before the study enrolment. Taking into account these criteria of the 90 participants, two women were excluded because of the diagnosis of an inflammatory or autoimmune disorder; therefore, the final sample consisted of 88 women.
The investigation was developed in accordance with the latest version of the Helsinki Declaration and was approved by the ethics committee “Comité Ético de Investigación Clínica del Parc de Salut Mar” (reference number: 2020/9158). All participants gave written informed consent following a full explanation of the study before enrolling.
2.2. Clinical Outcomes and Assessment
In the clinical interview, the evaluators gathered the data following a previously designed case report form (CRF) for the study. The CRF collected sociodemographic variables such as age, race, educational level, marital status, employment status, psychiatric and somatic comorbidities, and pharmacological treatment. A series of validated scales were also administered for the evaluation of pain and FM impact, psychological trauma and associated symptoms, comorbid psychiatric disorders, clinical symptoms of depression and anxiety, insomnia, and quality of life. The scales are detailed as follows:
2.2.1. Pain and FM Impact
Visual analog scale (VAS) for pain [31]: This scale consists of a straight horizontal line, ranging from 0 (no pain) to 10 (maximum pain), which assesses the pain severity at the moment of the clinical interview. Scores are interpreted as “no pain” (0–2), “mild pain” (2–4), “moderate pain” (4–6), “severe pain” (6–8), and “maximum pain” (8–10).
Pain disability index (PDI) [32]: This scale comprises 7 items referring to different aspects of life that can be affected by chronic pain: home and family responsibilities, recreation, social activities, occupation, sexual activity, and life support activities. Each item can be rated from 0 (no disability) to 10 (total disability), and the total score is obtained by summing all the answers. Since there is currently no validated Spanish version, this scale was translated from the English version by a bilingual researcher.
Fibromyalgia impact questionnaire [33], Spanish validation (S-FIQ) [34]: This 10-item scale assesses the impact of FM over the previous 7 days. The first item contains 11 questions, which are related to physical functioning; items 2 and 3 ask the person to answer the number of days they have been unable to work because of FM; and items from 4 to 10 are scaled items (0–10), in which the person rates work difficulty, pain, fatigue, morning tiredness, rigidity, anxiety, and depression. Higher scores signify lower levels of functioning.
2.2.2. Psychological Trauma and Associated Symptoms
Chronology of traumatic events: This tool consists of a table, which gathers all the traumatic events reported by the participants over their lifespan according to their age when each occurred. The table is divided into five-year segments spanning from 0–5 up to 65–70 years. For each segment, participants are asked, “Do you remember having any traumatic or stressful experiences when you were in this age group?”. Answers are then coded using thematic analysis. Traumatic events were then subsequently categorized as one of the following: emotional abuse; physical abuse; sexual abuse; emotional neglect; physical neglect; parental violence; drug abuse by a family member; parental mental disorder; parental mental disorder; accident; physical violence in adulthood; rape, abuse or sexual attack; harassment or psychological maltreatment in adulthood; death of a loved one; abortion; surgery; imprisonment, detention, or kidnapping; illness of a first-degree relative; personal illness; pregnancy itself or pregnancy complications; personal separation or divorce; mobbing; economic problems; familiar conflicts; others (such as bullying, natural disasters, eviction, or migration processes), or no traumatic event.
Global assessment of post-traumatic stress questionnaire (EGEP-5) [35]: This 55-item scale assess PTSD according to DSM-V criteria over the month prior to the evaluation, based on the event from the chronology currently causing the greatest level of distress. It evaluates symptoms of intrusion, avoidance, alterations in cognition, mood, arousal, and reactivity, as well as duration and impact on functioning, and determines the presence or absence of PTSD, as well as specifying if depersonalization, derealization, and/or delayed expression are present.
Subjective unit of distress (SUD) [36]: this scale, ranging from 0 (no distress) to 10 (maximum distress), evaluates the level of subjective perturbation a person experiences when they bring to mind the traumatic event chosen in the EGEP-5 scale.
Holmes and Rahe social readjustment scale [37], Spanish validation [38]: This scale lists 43 possible stressful events, and participants must mark the events that have happened to them in the previous 12 months. Each event has a different score, and the global score is reached by summing all the scores of the events selected. Scores under 150 indicate low levels of stress, scores between 150 and 299 are suggestive of a 50% risk of stress-related disorders, and scores above 300 mean an 80% risk of suffering stress-related disorders.
Childhood trauma questionnaire (CTQ) [39], Spanish validation [40]: This self-applied scale evaluates the presence of childhood trauma with 30 items (CTQ-T), which can be answered on a 5-point Likert scale. The CTQ measures 5 types of childhood maltreatment: emotional (CTQ-EA), physical (CTQ-PA), sexual abuse (CTQ-SA), emotional (CTQ-EN), and physical neglect (CTQ-PN). The numerical answers correspond with responses ranging from “never true” to “very often true”, and the final score of each factor indicates severity in terms of “none to minimal”, “low to moderate”, “moderate to severe” and “severe to extreme”.
Dissociative experiences scale (DES) [41], Spanish validation [42]: This 28-item scale assesses the frequency of the presence of different dissociative experiences, excluding acute intoxication by substances. Items are rated from 0% to 100%. The total score is obtained by summing all item answers and dividing this result by 28. There are three different subscales, such as amnesia (DES-A), depersonalization/derealization (DES-DP), and dissociation (DES-D). A total score (DES-T) equal to or higher than 30 is interpreted as a dissociative disorder.
Somatoform dissociation scale-20 (SDQ-20) [43], Spanish validation [44]: This questionnaire evaluates the presence and intensity of 20 somatoform symptoms or experiences that happened during the last year. Participants are asked to rate the intensity of each experience on a 5-point Likert scale and whether there is a medical explanation for it. The total score is reached by summing the scores for each item, while the symptoms with no known cause are summed to reach the total of symptoms with no known cause.
2.2.3. Diagnosis
FM diagnosis: FM diagnosis based on a clinical interview aligned with the American college of rheumatology criteria [30], which was carried out in all participants.
Psychiatric comorbidities: MINI neuropsychiatric international interview [45], Spanish validation [46]: The MINI structured interview evaluates the presence of psychiatric comorbidity according to DSM-IV criteria. In the present research project, only the following parts of the scale have been used for the assessment: major depressive episode, dysthymic episode, manic/hypomanic episode, panic disorder, agoraphobia, social phobia, obsessive-compulsive disorder, and generalized anxiety disorder. The remaining MINI components were not used because the data were covered by the inclusion and exclusion criteria (substance dependence, substance abuse, psychotic disorders, anorexia nervosa, and bulimia nervosa), were collected during the clinical interview (suicidality), or were assessed more exhaustively by other specific psychometric scales (PTSD).
2.2.4. Clinical Symptoms, Insomnia, and Quality of Life Evaluation
Hospital anxiety and depression scale (HADS) [47], Spanish validation [48]: This self-administered scale measures the presence and intensity of anxious and depressive symptoms in the previous 7 days. It contains 14 items, seven for each of the subscales (HADS-A for anxiety and HADS-D for depression), which can be rated from 0 to 3. The sum total of the scores gives the overall score. Scores equal to or over 8 for each subscale can represent the presence of an anxiety or depressive disorder.
Athens insomnia scale (AIS) [49], Spanish validation [50]: This scale evaluates the presence of insomnia according to ICD-10 criteria. It evaluates disturbances in sleep over the previous week and consists of 8 items. The first five assess sleep induction, awakenings at night, final awakening, total sleep duration, and sleep quality, and the last three items refer to well-being, functioning capacity, and sleepiness during the day. All items can be rated from 0 to 3, providing a total score when summed between 0 and 24.
Satisfaction with life scale (SWLS) [51], Spanish validation [52]: This self-applied scale consists of 5 items evaluating the self-perception of satisfaction with one's life. Each item can be rated from 1 (totally disagree) to 5 (totally agree). Higher scores represent higher levels of satisfaction.
3. Data Analysis
3.1. Sample Size Calculation
Given that the main objective of this study was to investigate the relationship between childhood trauma (CTQ) and FM pain (VAS pain), we calculated the sample size needed to conduct a regression analysis between CTQ and VAS pain. According to the standard formula, the sample size required to detect small correlations (R = 0.30) with 80% statistical power is 84. However, researchers decided to include all candidates who were recruited between January 2020 and January 2021 who signed the informed consent and met inclusion criteria, even if the calculated number was exceeded.
3.2. Statistical Analysis
All analyses were performed using STATA statistics/data analysis, version 16.1 (StataCorp LLC, Texas, USA). Fitness to parametric assumptions was checked for all variables. To assess the normality of data distribution, the Shapiro–Wilk test was used.
First, regarding the descriptive analysis of the sociodemographic, medical, and clinical data (Tables 1 and 2), the arithmetic mean was used for quantitative variables and the proportion for categorical variables. In both cases, the standard error and confidence interval (95%) were calculated.
Table 1.
Sociodemographic characteristics of the sample. Data are presented as the mean (SD) or number (%).
| Variable | Obs/Freq | Mean/Percentage∗ | Std. Err. | (95% Conf. Interval) | ||
|---|---|---|---|---|---|---|
| Age | 88 | 51.40 | 0.97 | 49.47 | 53.34 | |
| Education (years of studies) | 88 | 14.05 | 0.41 | 13.23 | 14.87 | |
|
| ||||||
| Race | Caucasian | 74 | 84% | 0.03 | 0.74 | 0.90 |
| Latin | 12 | 13.6% | 0.03 | 0.07 | 0.22 | |
| Other | 2 | 2.2% | 0.01 | 0.005 | 0.08 | |
|
| ||||||
| Relationship status | Single | 16 | 18.1% | 0.04 | 0.11 | 0.27 |
| Married/in a couple | 69 | 78.4% | 0.04 | 0.68 | 0.85 | |
| Widowed | 3 | 3.4% | 0.01 | 0.01 | 0.10 | |
|
| ||||||
| Employment status | Full-time employment | 12 | 13.6% | 0.03 | 0.07 | 0.22 |
| Part-time employment | 5 | 5.6% | 0.02 | 0.02 | 0.13 | |
| Sick leave | 31 | 35.2% | 0.05 | 0.25 | 0.45 | |
| Unable to work due to mental health problems | 6 | 6.8% | 0.02 | 0.03 | 0.14 | |
| Unable to work due to other reasons | 17 | 19.3% | 0.04 | 0.12 | 0.29 | |
| Unemployed | 31 | 14.7% | 0.03 | 0.08 | 0.23 | |
| Others | 3 | 3.4% | 0.01 | 0.01 | 0.10 | |
| Student | 1 | 1.1% | 0.01 | 0.001 | 0.07 | |
Obs/Freq, Number of cases observed/Frequency; Std. Error, Standard Error; Conf, Confidence ∗Age and education data are presented as means. The rest of the variables are presented as percentages.
Table 2.
Clinical characteristics of the sample. Data are presented as the mean (SD) and/or number (%).
| Variable | Obs/Freq | Mean/Percentage∗ | Std. Err. | [95% Conf. Interval] | ||
|---|---|---|---|---|---|---|
| MINI | GAD | 77 | 87.5% | 0.03 | 0.78 | 0.92 |
| MDD | 67 | 76.13% | 0.04 | 0.65 | 0.83 | |
| Panic disorder | 56 | 63.6% | 0.05 | 0.52 | 0.73 | |
| Social phobia/Agoraphobia | 26 | 29.5% | 0.04 | 0.20 | 0.40 | |
| Dysthymia | 10 | 11.3% | 0.03 | 0.06 | 0.19 | |
| OCD | 3 | 3.4% | 0.01 | 0.01 | 0.10 | |
|
| ||||||
| HADS | HADS-D | 88 | 12.04 | 0.46 | 11.12 | 12.96 |
| HADS-A | 88 | 14.34 | 0.39 | 13.55 | 15.12 | |
| AIS | 88 | 14.13 | 0.52 | 13.10 | 15.17 | |
| SWLS | 87 | 11.78 | 0.49 | 10.79 | 12.76 | |
| VAS pain | 88 | 6.57 | 0.23 | 6.11 | 7.03 | |
| PDI | 88 | 46.12 | 1.21 | 43.71 | 48.53 | |
| Onset of pain | 86 | 35.44 | 1.29 | 32.87 | 38.02 | |
| Diagnosis of fibromyalgia | 87 | 44.55 | 0.92 | 42.73 | 46.37 | |
| S-FIQ | 87 | 55.58 | 1.06 | 53.47 | 57.69 | |
| Suicidal thinking | 73 | 82.9% | 0.04 | 0.73 | 0.89 | |
|
| ||||||
| Suicide attempt | 28 | 32.9% | 0.05 | 0.23 | 0.43 | |
| Violent | 4 | 4.5% | 0.02 | 0.01 | 0.11 | |
| No violent | 24 | 27.2% | 0.04 | 0.18 | 0.37 | |
| Severe | 12 | 13.6% | 0.03 | 0.078 | 0.22 | |
| Not severe | 16 | 18.1% | 0.04 | 0.11 | 0.27 | |
|
| ||||||
| Diagnostics axis III | CFS | 53 | 60.2% | 0.05 | 0.49 | 0.70 |
| Osteoarthritis | 27 | 30.6% | 0.04 | 0.21 | 0.41 | |
| Spinal disc herniation | 10 | 11.3% | 0.03 | 0.06 | 0.19 | |
| Chronic migraine | 9 | 10.2% | 0.03 | 0.05 | 0.18 | |
| Low back pain | 9 | 10.2% | 0.03 | 0.05 | 0.18 | |
| Thyroid diseases | 8 | 9% | 0.03 | 0.04 | 0.17 | |
| Rheumatoid arthritis | 6 | 6.8% | 0.02 | 0.03 | 0.14 | |
| Restless legs syndrome | 5 | 5.6% | 0.02 | 0.02 | 0.13 | |
| Chemical sensitivity syndrome | 4 | 4.5% | 0.02 | 0.01 | 0.11 | |
|
| ||||||
| Pharmacological treatment | Anxiolytics/Hypnotics | 53 | 60.9% | 0.05 | 0.50 | 0.70 |
| SNRI | 43 | 49.4% | 0.05 | 0.38 | 0.59 | |
| SSRI | 18 | 20.6% | 0.04 | 0.13 | 0.30 | |
| Other antidepressants | 33 | 37.9% | 0.05 | 0.28 | 0.48 | |
| Opioids+ Tramadol Codeine Morphine Fentanyl Oxycodone Buprenorphine Tapentadol | 32 20 1 1 1 2 1 8 |
36.7% 22.7% 1.1% 1.1% 1.1% 2.3% 1.1% 9.1% |
0.05 0.04 0.01 0.01 0.01 0.01 0.01 0.03 |
0.27 0.14 −0.01 −0.01 −0.01 −0.01 −0.01 0.03 |
0.47 0.32 0.03 0.03 0.03 0.06 0.03 0.16 |
|
| Paracetamol | 32 | 36.7% | 0.05 | 0.27 | 0.47 | |
| Anti-inflammatory drugs | 31 | 35.6% | 0.05 | 0.26 | 0.46 | |
| Anticonvulsants | 18 | 20.6% | 0.04 | 0.13 | 0.30 | |
| Antipsychotics | 8 | 9.1% | 0.03 | 0.04 | 0.17 | |
Obs/Freq : Number of cases observed/Frequency; Std. Error, Standard Error; Conf., Confidence; MINI : MINI Neuropsychiatric International Interview; MDD : Major Depressive Disorder; GAD : Generalized Anxiety Disorder; OCD : Obsessive-Compulsive Disorder; HADS : Hospital Anxiety and Depression Scale; HADS-D : Hospital Anxiety and Depression Scale-Depression; HADS-A : Hospital Anxiety and Depression Scale-Anxiety; AIS : Athens Insomnia Scale; SWLQ : Satisfaction With Life Questionnaire; VAS pain, Visual Analogue Scale for pain; PDI : Pain Disability Index; S-FIQ : Fibromyalgia Impact Questionnaire-Spanish validation; CFS : Chronic Fatigue Syndrome; SSRI : Selective Serotonin Reuptake Inhibitor; SNRI : Serotonin-Norepinephrine Reuptake Inhibitor. ∗Scales data are presented as means. The rest of the variables are presented as percentages. + also in combination.
Second, simple linear regression has been used to analyze whether different types of child maltreatment (CTQ measures) could predict different clinical variables, namely anxiety and depression.
Third, we also used the simple linear regression model to analyze whether the scores obtained on the fibromyalgia pain and impact scales (VAS, PDI, and S-FIQ) could predict the clinical variables discussed above (HADS and AIS) and the patients' quality of life (SWLQ).
4. Results
4.1. Sample Characteristics
The mean age of the 88 participants in the sample was 51.41 years, with the majority being married or in a couple, and Caucasian. According to their employment status, a high number of them were on sick leave (n = 31, 35.2%), unemployed (n = 31, 15%), or unable to work due to mental health problems or other problems (n = 23, 26%) (see Table 1).
Regarding the medical data of the sample, other comorbid axis III diagnoses were common, with the most prevalent being chronic fatigue syndrome (60.2%), followed by osteoarthritis (30.6%). Participants were prescribed various pharmacological drugs, with the most frequent being anxiolytics/hypnotics (60.9%); then, serotonin-norepinephrine reuptake inhibitors (SNRIs) (49.4%), paracetamol (36.7%), opioids (mainly tramadol and tapentadol, 22.7% and 9.1%, respectively) and anti-inflammatory drugs (35.2%) (see Table 2).
According to the MINI, anxiety disorders (87.5% for generalized anxiety disorder, 63.6% for panic disorder, and 29.5% for social phobia/agoraphobia) and mood disorders (76.1% for major depressive disorder and 11.3% for dysthymia) were the most frequent psychiatric comorbidities. These results were confirmed by higher current scores in the HADS (anxiety MD = 14.34; SD = 0.39 versus depression MD = 12.04; SD = 0.46). Participants showed marked scores in the AIS (MD = 14.14; SD = 0.52) suggestive of sleep disturbances and an important degree of dissatisfaction with their lives according to the SWLS scores (MD = 11.78; SD = 0.49). In terms of suicidal behavior, 82.9% of the participants reported having had thoughts of suicide at some point in their lives, and 32.9% had carried out at least one suicide attempt in their lifetime, of which 4.5% used violent methods (e.g. physical self-harming) and 27.2% nonviolent methods (e.g. drug over-ingest), 13.6% suffered severe consequences (e.g. hospitalization or physical lesions), and 18.18% nonsevere consequences (resolved without the need to go to health services) (see Table 2).
As expected, subjective pain perception, measured with the VAS, revealed high levels of pain (MD = 6.57; SD = 0.23). Furthermore, we also found a marked degree of disability (PDI MD = 46.12; SD = 1.21) with a generally large negative impact of FM on daily functioning and quality of life (S-FIQ MD = 55.58; SD = 1.06). The average number of years between the onset of pain and the diagnosis of FM in the sample was 9.10 (onset of pain: M = 35.44, SD = 11.93; FM diagnosis: M = 44.55, SD = 8.50) (see Table 2).
The EGEP-5 scores revealed that 71.5% of the participants met the criteria for PTSD in the last month. In relation to the event chosen by each participant for the administration of this scale, 34 women selected an event that occurred in their childhood, 47 an event that occurred in adulthood, and this data was missing for 7 participants. The average score of subjective distress, measured via SUD, was 8.23 (from 0 to 10, SD = 0.26), indicating great psychological distress in relation to that event (see Table 3). Total DES scores revealed low-to-moderate levels of dissociative symptoms in our sample (MD = 24.72; SD = 1.34); however, the dissociation subscale of dissociative experiences obtained scores above the cut-off point (MD = 36.26; SD = 1.86). Somatoform dissociative symptoms, measured by the SDQ-20, confirmed the presence of a strong somatization tendency in the sample (SD = 39.45; SD = 1.11), having an average of 4.76 symptoms with no known cause (SD = 0.3) (see Table 3).
Table 3.
Clinical variables of psychological trauma. Data are presented as the mean (SD).
| Variable | Obs/Freq | Mean/Proportion | Std. Err. | (95% Conf. Interval) | ||
|---|---|---|---|---|---|---|
| CTQ | Total | 88 | 49.97 | 2.11 | 45.78 | 54.17 |
| Emotional A | 88 | 12.10 | 0.64 | 10.81 | 13.39 | |
| Physical A | 88 | 8.19 | 0.54 | 7.11 | 9.27 | |
| Sexual A | 88 | 8.76 | 0.60 | 7.55 | 9.96 | |
| Emotional N | 88 | 12.72 | 0.63 | 11.47 | 13.97 | |
| Physical N | 88 | 7.51 | 0.30 | 6.89 | 8.12 | |
|
| ||||||
| EGEP-5 | PTSD | 63 | 0.71 | 0.04 | 0.61 | 0.80 |
| No PTSD | 24 | 0.27 | 0.04 | 0.18 | 0.37 | |
| NA | 1 | 0.01 | 0.01 | 0.001 | 0.07 | |
| SUD | 87 | 8.23 | 0.26 | 7.71 | 8.75 | |
|
| ||||||
| DES | Total | 86 | 24.72 | 1.34 | 22.05 | 27.39 |
| Amnesia | 86 | 11 | 1.20 | 8.61 | 13.38 | |
| Depersonalization Derealization |
86 | 19.47 | 1.63 | 16.22 | 22.72 | |
| Dissociation | 86 | 36.26 | 1.86 | 32.55 | 39.97 | |
|
| ||||||
| SDQ-20 | Number of symptoms | 86 | 4.76 | 0.30 | 4.16 | 5.37 |
| Total score | 86 | 39.45 | 1.11 | 37.22 | 41.67 | |
|
| ||||||
| Holmes and Rahe | Number of events | 88 | 7.64 | 0.42 | 6.80 | 8.49 |
| Total scores | 88 | 224.52 | 13.16 | 198.34 | 250.69 | |
Obs/Freq : Number of cases observed/Frequency; Std. Error, Standard Error; Conf., Confidence; CTQ : Childhood Trauma Questionnaire; Emotional A : Emotional Abuse; Physical A : Physical Abuse; Sexual A : Sexual Abuse; Emotional N : Emotional Neglect; Physical N : Physical Neglect; EGEP-5 : Global Assessment of Post-traumatic Stress Questionnaire-5; PTSD : Post-traumatic Stress Disorder; NA : Not Applicable; SUD : Subjective Unit of Disturbance; DES : Dissociative Experiences Scale; SDQ-20 : Somatoform Dissociation Questinnaire-20; Number of symptoms: Number of symptoms with unknown cause; Holmes and Rahe : Holmes and Rahe Social Readjustment Scale.
Our FM sample experienced low-to-moderate levels of all types of child maltreatment in the CTQ, with both emotional abuse (63.6%) and emotional neglect (62.5%) being the most frequent maltreatment, followed by sexual abuse (48.8%), physical neglect (40.9%), and physical abuse (31.8%). Of note, minimization and denial in the CTQ were controlled for. Furthermore, patients showed an average of 7.64 (SD = 0.42) stressful events that happened during the last year and a high total score on the Holmes and Rahe scale (MD = 224.52; SD = 13.16), which is suggestive of a 50% risk of developing stress-related disorders (see Table 3).
Regarding the chronology of traumatic events, the highest number of these events occurred in the stages of second childhood and early adolescence. However, a high number of traumatic events were also reported during the first year of life (see Figure 1(a)). From Figure, it can also be gathered that traumatic events in this population begin to occur at very early ages and continue throughout all lifespans, well into late adulthood or older age, changing the typology of the exposed traumatic event (see Figure 1(b)). The most prevalent traumatic events to occur between 0 and 15 years were physical abuse (n = 39), sexual abuse (n = 32), and emotional abuse (n = 29) (see Figure 2(a)), while the most prevalent type of traumatic event in the sample after childhood and adolescence was the death of a loved one (n = 71), followed by harassment or psychological abuse in adulthood (n = 57), and other experiences grouped in the category “other traumatic events” (n = 39) (see Figure 2(b)). Interestingly, 84% of the sample suffered from one or more types of traumatic events prior to the onset of pain.
Figure 1.
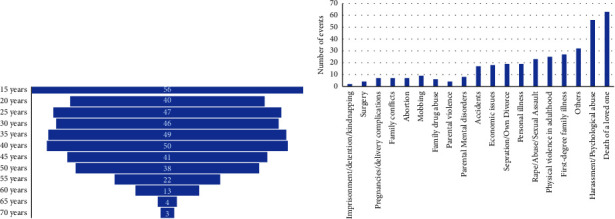
(a) Number of traumatic events per age (n = 77), and (b) typology of traumatic events throughout lifespans (n = 77).
Figure 2.
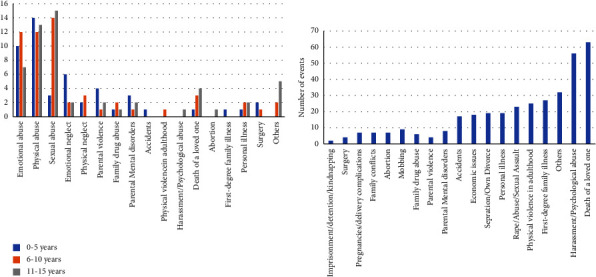
Number and typology of traumatic events (a) between 0 and 15 years (n = 77), and (b) between 16 and 70 years (n = 77).
4.2. Simple Linear Regression
All linear regression results can be gathered from Table 4. Hereby, 3 types of child maltreatment (emotional abuse (CTQ-EA : F (1, 85) = 6.30; p = 0.0140), emotional neglect (CTQ-EN : F (1, 86) = 12.94; p = 0.0005), and physical neglect (CTQ-PN : F (1, 85) = 6.10; p = 0.0155) predicted low quality of life (high scores on the SWLS) in our sample. The same was true for the total score obtained on the CTQ (CTQ-T; F (1, 85) = 8.27; p = 0.0051) and two measures of pain, the PDI and S-FIQ (F (1, 85) = 8.69; p = 0.0041 and F (1, 85) = 8.08; p = 0.0056), respectively.
Table 4.
Linear regression results.
| Variables∗ | Obs | F and prob > F | R-squared and Adj R-squared | Linear regression equation | t and P > (t) | (95% Conf. Interval) | |
|---|---|---|---|---|---|---|---|
| SWLS (Y) CTQ-T (X) |
87 | F (1, 85) = 8.27; p=0.0051 |
R
2 = 0.0887 Adj R2 = 0.0780 |
^Y = −0.069 × 15.25 | t = −2.88; p=0.005 | −0.117 | −0.021 |
| SWLS (Y) CTQ-EA (X) |
87 | F (1, 85) = 6.30; p=0.0140 |
R
2 = 0.0690 Adj R2 = 0.0580 |
^Y = −0.198 × 14.18 | t = −2.51; p=0.014 | −0.355 | −0.411 |
| SWLS (Y) CTQ-EN (X) |
87 | F (1, 86) = 12.94; p=0.0005 |
R
2 = 0.1321 Adj R2 = 0.1219 |
^Y = −0.283 × 15.40 | t = −3.60; p=0.014 | −0.440 | −0.126 |
| SWLS (Y) CTQ-PN (X) |
87 | F (1, 85) = 6.10; p=0.0155 |
R
2 = 0.0669 Adj R2 = 0.0560 |
^Y = −0.410 × 14.87 | t = −2.47; p=0.016 | −0.741 | −0.080 |
| HAD-D (Y) VAS (X) |
88 | F (1, 86) = 3.99; p=0.0489 |
R
2 = 0.0443 Adj R2 = 0.0332 |
^Y = 0.419 × 9.28 | t = 2.00; p=0.049 | 0.001 | 0.837 |
| HAD-A (Y) AS (X) |
88 | F (1, 86) = 10.08; p=0.0021 |
R
2 = 0.1049 Adj R2 = 0.0945 |
^Y = 0.547 × 10.74 | t = 3.18; p=0.002 | 0.204 | 0.889 |
| AIS (Y) VAS (X) |
88 | F (1, 86) = 19.18; p=0.000 |
R
2 = 0.1823 Adj R2 = 0.1728 |
^Y = 0.952 × 7.87 | t = 4.38; p=0.000 | 0.520 | 1.385 |
| DES-T (Y) VAS (X) |
86 | F (1, 86) = 4.31; p = 0.0410 |
R
2 = 0.0488 Adj R2 = 0.0375 |
^Y = 1.262 × 16.46 | t = 2.08; p=0.041 | 0.053 | 2.47 |
| DES-D (Y) VAS (X) |
86 | F (1, 84) = 4.30; p=0.0412 |
R
2 = 0.0487 Adj R2 = 0.0374 |
^Y = 1.750 × 24.81 | t = 2.07; p=0.041 | 0.071 | 3.43 |
| HAD-D (Y) PDI (X) |
88 | F (1, 86) = 31.14; p=0.0000 |
R
2 = 0.2658 Adj R2 = 0.2573 |
^Y = 0.197 × 2.94 | t = 5.58; p=0.000 | 0.127 | 0.267 |
| HAD-A (Y) PDI (X) |
88 | F (1, 86) = 22.58; p=0.0000 |
R
2 = 0.2079 Adj R2 = 0.1987 |
^Y = 0.147 × 7.52 | t = 4.75; p=0.000 | 0.086 | 0.209 |
| AIS (Y) PDI (X) |
88 | F (1, 86) = 8.94; p=0.0036 |
R
2 = 0.0941 Adj R2 = 0.0836 |
^Y = 0,131 × 8,07 | t = 2.99; p=0.004 | 0.044 | 0.218 |
| SWLS (Y) PDI (X) |
87 | F (1, 85) = 8.69; p=0.0041 |
R
2 = 0.0927 Adj R2 = 0.0821 |
^Y = -0.122 × 17.44 | t = −2.95; p=0.004 | −0.205 | −0.039 |
| DES-T (Y) PDI (X) |
86 | F (1, 84) = 10.50; p=0.0017 |
R
2 = 0.1111 Adj R2 = 0.1005 |
^Y = 0.361 × 8.10 | t = 3.24; p=0.002 | 0.139 | 0.582 |
| DES-A (Y) PDI (X) |
86 | F (1, 85) = 6.27; p=0.0142 |
R
2 = 0.0695 Adj R2 = 0.0584 |
^Y = 0.2551 × -0.74 | t = 2.50; p=0.014 | 0.052 | 0.457 |
| DES-DP (Y) PDI (X) |
86 | F (1, 85) = 6.29; p=0.0140 |
R
2 = 0.0697 Adj R2 = 0.0586 |
^Y = 0.3481 × 3.45 | t = 2.501 p=0.014 | 0.072 | 0.624 |
| DES-D (Y) PDI (X) |
86 | F (1, 85) = 7.56; p=0.0073 |
R
2 = 0.0826 Adj R2 = 0.0716 |
^Y = 0.4331 × 16.37 | t = 2.75 p=0.007 | 0.119 | 0.744 |
| HAD-D (Y) S-FIQ (X) |
87 | F (1, 85) = 12.39; p=0.0007 |
R
2 = 0.1272 Adj R2 = 0.1170 |
^Y = 0.1531 × 3.60 | t = 3.52 p=0.001 | 0.066 | 0.240 |
| HAD-A (Y) S-FIQ (X) |
87 | F (1, 85) = 27.16; p=0.0000 |
R
2 = 0.2422 Adj R2 = 0.2333 |
^Y = 0.1741 × 4.79 | t = 5.21 p=0.000 | 0.107 | 0.240 |
| AIS (Y) S-FIQ (X) |
87 | F (1, 85) = 7.69; p=0.0068 |
R
2 = 0.0830 Adj R2 = 0.722 |
^Y = 0.137 × 6.64 | t = 2.77 p=0.007 | 0.038 | 0.235 |
| SWLS (Y) S-FIQ (X) |
86 | F (1, 85) = 8.08; p=0.0056 |
R
2 = 0.0877 Adj R2 = 0.769 |
^Y = −0.136 × 19.24 | t = −2.84 p=0.006 | −0.231 | −0.040 |
| DES-T (Y) S-FIQ (X) |
85 | F (1, 83) = 11.83; p=0.0000 |
R
2 = 0.1247 Adj R2 = 0.114 |
^Y = 0.440 × 0.488 | t = −3.44 p=0.001 | 0.185 | 0.695 |
| DES-A (Y) S-FIQ (X) |
85 | F (1, 83) = 8.61; p=0.0043 |
R
2 = 0.0940 Adj R2 = 0.831 |
^Y = 0.342 × −7.860 |
t = 2.93 p=0.004 |
0.110 | 0.574 |
| DES-D (Y) S-FIQ (X) |
85 | F (1, 83) = 5.08; p=0.0268 |
R
2 = 0.0577 Adj R2 = 0.046 |
^Y = 0.367 × −0.792 |
t = 2.25 p=0.027 |
0.043 | 0.691 |
| DES-D (Y) S-FIQ (X) |
85 | F (1, 83) = 10.25; p=0.0019 |
R
2 = 0.1099 Adj R2 = 0.099 |
^Y = 0.575 × 4.56 |
t = 3.20 p=0.002 |
0.217 | 0.933 |
| VAS (Y) CTQ-PN (X) |
88 | F (1, 86) = 4.12; p=0.0455 |
R
2 = 0.0457 Adj R2 = 0.0346 |
^Y = −0.161 × 7.78 |
t = -2.03 p=0.046 |
−0.003 | 9.058 |
∗ Linear regression equation for predicting Y from X in two ways. CTQ-EA : CTQ Emotional Abuse; CTQ-EN : CTQ Emotional Neglect; CTQ-Physical Neglect; DES-T : DES Total; DES-D : DES Dissociation; DES-A : DES Amnesia; DES-D : DES Depersonalization; HADS-DP : Hospital Anxiety and Depression Scale-Depression; HADS-A : Hospital Anxiety and Depression Scale-Anxiety; VAS : Visual Analogue Scale for pain; AIS : Athens Insomnia Scale; PDI : Pain Disability Index; S-FIQ : Fibromyalgia Impact Questionnaire-Spanish validation; SWLS : Satisfaction With Life Scale.
In addition, linear regression analysis also showed that higher scores in physical neglect significantly predicted higher levels of pain in the VAS (CTQ-PN: F (1, 86) = 4.12; p = 0.0455).
On the other hand, linear regression showed that higher scores in the pain measures and FM impact on quality of life (VAS, PDI, and S-FIQ) significantly predicted the presence and intensity of depressive and anxious symptomatology. More specifically, the VAS significantly predicted both depressive (HADS-D: F (1, 86) = 3.99; p = 0.0489) and anxious (HADS-A: F (1, 86) = 10.08; p = 0.0021) symptomatology, which was also true for the PDI (HADS-D: F (1, 86) = 31.14; p = 0.0000); HADS-A: F (1, 86) = 22.58; p = 0.0000) and S-FIQ scales (HADS-D: F (1, 85) = 12.39; p = 0.0007); HADS-A: F (1, 85) = 27.16; p = 0.0000).
Likewise, the scores in the pain and in the FM impact (VAS, PDI, and S-FIQ) also significantly predicted the degree of dissociative experiences (DES). VAS significantly predicted both the total score (DES-T: F (1, 86) = 4.31; p = 0,0410) and the scores obtained in dissociation (DES-D: F (1, 84) = 4.30; p = 0.0412). The PDI significantly predicted the total score (DES-T: F (1, 84) = 10.50; p = 0.0017) and the scores obtained in amnesia (DES-A: F (1, 85) = 6.27; p = 0.0142), depersonalization (DES-DP: F (1, 85) = 6.29; p = 0.0140), and dissociation (DES-D: F (1, 85) = 7.56; p = 0.0073) subscales. The same was true for the S-FIQ (DES-T: F (1, 83) = 11.83; p = 0.0000), DES-A: F (1, 83) = 8.61; p = 0.0043), DES-DP: F (1, 83) = 5.08; p = 0.0268), DES-D: F (1, 83) = 10.25; p = 0.0019).
Furthermore, linear regression analysis was also suggestive that patient scores on pain and FM impact (VAS, PDI, and S-FIQ) also significantly predicted sleep disturbance (AIS: F (1, 86) = 19.18; p = 0.0000; F (1, 86) = 8.94; p = 0.0036; and F (1, 85) = 7.69; p = 0.0068, respectively).
5. Discussion
The present study evaluated 88 patients with FM in detail with regard to their sociodemographic and clinical data and biographical history, focusing on the prevalence and characterization of psychological trauma across their lifespan and how it can predict the relationship with different clinical variables.
To the best of our knowledge, this is one of the few studies that has assessed the characteristics of the traumatic events suffered by a sample of women with FM in a systematic and chronological way. The results have shown that the most prevalent traumatic events categorized by age occurred during childhood and adolescence, especially in the form of physical abuse, sexual abuse, and emotional abuse, but have continued into adulthood, modifying their typology and presenting themselves mainly in the form of deaths of loved ones, harassment and physical abuse, rape, abuse, or sexual assault. These data are clinically relevant as they suggest that female FM patients are chronically and recurrently exposed to different types of stressful or vital events throughout their lives, favoring the appearance of a process of continuous retraumatization that would explain the very high percentage of PTSD diagnoses in our sample. In fact, 100% of the participants reported having suffered at least one major traumatic event at some point in their lives, and 84% had suffered one or more types of these traumatic events prior to the onset of pain. Likewise, 71.5% of the whole sample met the criteria for current PTSD, adding a further comorbidity in this complex population. These data are far higher than the prevalence data found in the general population, which range from 0.2% to 3.8% [53], and also higher than in mental disorders such as depression (48–49%) [54], bipolar disorder (4% to 40%) [55], or substance use disorder (20.67%) [56]. It is important to note that almost half of the sample (n = 34) was selected for the administration of the EGEP-5, an event that occurred in childhood that was the most significant traumatic event in their lives. These data, therefore, once again highlight the strong and enduring impact that childhood trauma can have on health in adulthood. Our data not only reaffirm the existence of high comorbidity between PTSD and FM but also confirm that individuals with comorbid pain and PTSD report greater pain, PTSD symptoms, depression, anxiety, disability, and opioid use than people who only have one of these conditions [57].
Regarding the results of the CTQ, our participants presented low to moderate levels of all types of childhood maltreatment, especially emotional abuse and emotional neglect, followed by sexual abuse, physical neglect, and physical abuse. These results are in line with other studies which compared FM patients to controls or patients with other pain conditions, where they found higher CTQ scores in the FM group, with emotional abuse and neglect representing the most frequent subtypes [24–27, 29, 58–60]. Other studies reported physical abuse and physical neglect as being the first [23] or the second most prevalent types of maltreatment in patients with FM [24, 25, 27, 58]. These were less frequent in our sample's CTQ scores. Interestingly, despite this, physical abuse and neglect were the most frequently reported types of maltreatment in the chronological evaluation of traumatic events in our participants. One possible explanation for this phenomenon is that, although physical maltreatment has been more present in the lives of these women, emotional abuse and neglect have had a greater impact from a psychological point of view. This hypothesis would corroborate previous research that has found not only that a lack of emotional warmth from primary caregivers is one of the greatest risk factors for the development of both physical and mental disorders in both adolescence and adulthood [61, 62], but that parental support is the most significant predictor of individual resilience [63], quality of life in adulthood [64], and mental health stability in any stage of life [65]. In fact, our results show how the presence of child abuse, in particular emotional abuse and emotional and physical neglect, predicts a poorer quality of life in the women of our sample. In addition, our results also emphasize that childhood trauma is associated with greater severity of anxious and depressive symptoms and sleep disturbances in adulthood. Therefore, regardless of the order in which the different types of maltreatment occurred, all these results underline the high prevalence of childhood maltreatment in patients affected by FM, supporting previous research that found childhood trauma is not only a risk factor for developing several mental disorders in adulthood, such as depression [66], but also for the onset and maintenance of several chronic pain conditions [61, 67]. Our data also showed that only physical neglect could explain the pain reported by patients. A possible explanation for these results could be that early exposure to traumatic events may have long-term effects on the developing nociceptive system. More specifically, physical and emotional stress could provoke alterations not only in the proper functioning of the HPA axis, favoring a hyperactivation of it, but also in the pain processing system, favoring a lack of inhibition of nociceptive stimuli by descending pain control mechanisms [68].
According to the Holmes and Rahe social readjustment scale, we found a high prevalence of major stressors that happened over the last year, compounding the prior presence of trauma-related stress and increasing its negative impact on participants' well-being. In fact, people with FM suffer from more major life stressors than patients with migraine [26], rheumatoid arthritis, and healthy controls [69], which can be explained by the increased sensitivity to stressful conditions and the high risk of retraumatization they are exposed to. A recent study has found that cumulative trauma and somatoform disorders increase the impact of FM [70], which is in line with our work. Taking into account the devastating effects of chronic stress on physical, cognitive, and mental health [71], continued exposure to trauma would increase the vulnerability of these women to the development of different pathologies, including the appearance of pain and, consequently, psychological/psychiatric comorbidities.
Although our results showed that scores on pain scales predicted the occurrence of dissociation, participants showed generally low dissociation scores on the DES scale, with the exception of the dissociation subscale, where our patients scored highly. The general low scores in dissociation are surprising, taking into account the aforementioned trauma load and high prevalence of PTSD in our sample, and also considering that dissociation is a very common phenomenon in people suffering from PTSD. A possible explanation for this could be that psychotropic medication improves dissociative symptoms by exerting an inhibitory effect on the central nervous system. However, this hypothesis needs further data because pharmacological studies available in this field are scarce and inconclusive [72]. Another explanation could be that patients with FM tend to express physically traumatic memories. The appearance of medically unexplained symptoms could occur due to the disconnection between mind and body because of the impact of traumatic experiences, followed by an amplification of subthreshold body sensations [70]. Hereby, it is interesting that our FM patients scored high on the SDQ-20, which represents somatoform dissociative disorders. Other studies has demonstrated that FM is associated with high levels of somatoform dissociation [58], in comparison with controls [70] and other functional somatic syndromes (FSSs) [73]. Furthermore, previous results suggested a direct association between childhood trauma and somatoform disorders [58, 70, 73, 74], showing childhood trauma can predict the impact and the severity of FM.
Additionally, we detected a very high prevalence of psychiatric comorbidities such as generalized anxiety disorder (87.5%), major depressive disorder (76.13%), and panic disorder (63.6%), and a lower but still important prevalence of social phobia/agoraphobia (29.5%), followed by dysthymia (11.3%), and finally obsessive-compulsive disorder (3.4%). This underlines the complexity and multidiagnostic nature of FM patients and is in line with previous literature, which reports that psychiatric comorbidity among FM, anxiety, and mood disorders is common and is a factor that can complicate medical prognosis [23,75]. Of note here, we excluded bipolar disorder, schizoaffective disorder, and schizophrenia, whereas we cannot provide prevalence data accordingly. Furthermore, we observed that FM patients received a number of psychotropic drugs, most frequently anxiolytics/hypnotics (60.9%), antidepressants (SNRI: 49.4%; SSRI: 20.6%; others: 37.9%), followed by various analgesics (paracetamol: 36.7%; anti-inflammatories: 35.6%), opioids (mainly tramadol and tapentadol, 22.7% and 9.1%, respectively) and antipsychotic medication (9.1%), indicating again the high comorbidity between FM and mental suffering. Some of the medications used, such as duloxetine, have the official indication to be prescribed for FM patients.
Our results not only confirm the high anxiety and depression scores in our sample but also that the scores obtained by the participants in the pain and fibromyalgia scales (VAS, PDI, and S-FIQ) significantly predict the presence and intensity of depressive and anxious symptomatology. This bidirectionality has been reported in previous literature showing that mental disorders, such as depression or anxiety, can be a consequence of living with chronic pain [76], as well as a history of a mental disorder being considered a risk factor for developing chronic pain [77].
Of note, 82.9% of the participants in the present study reported suicidal ideation in their history, while 32.9% reported suicide attempts. These data confirm the high prevalence of suicidal behaviors in patients suffering from chronic pain compared to the general population [9]. According to previous literature, there is a whole set of risk factors that could favor suicidal behaviors, such as psychological stress, sleep disturbances, the experience of fatigue, dizziness, and weakness, depression, female gender, and physical comorbidities like headaches and gastric diseases [9, 78–81]. Therefore, as suicidal behavior is highly prevalent due to clinical manifestations of FM and its psychiatric comorbidities, it needs to be assessed routinely in patients with FM. The same is true for sleep alteration in FM patients. Our results are in agreement with other studies, which have shown a high prevalence of sleep disturbances [6, 23, 82], which can be explained not only by pain and the direct impact of FM, but also by the presence of other axis III diagnoses, and mood and anxiety comorbidities [83, 84]. Our data revealed that 93.2% of our sample suffered from sleep alterations, which is higher than in previous studies, estimating that almost 80% of patients with FM present poor sleep [85]. Interestingly, poor sleep is strongly and dose-dependently associated with pain symptom severity in FM patients [86], at the same time as interfering with the ability to cope with pain [87], resulting in tiredness and poor quality of life [82, 88].
Finally, our sociodemographic characteristics provide insight into the high co-occurrence of various axis III diagnoses, including CFS (60.2%), confirming the overlap between both diagnoses [3,89], osteoarthritis (30.6%), spinal disc herniation (11.3%), low back pain (10.2%), and chronic migraine (10.2%). In addition, we also detected thyroid diseases (9%) and restless leg syndrome, rheumatoid arthritis, and chemical sensitivity syndrome (all of them between 5% and 6%) as somatic comorbidity. This confirms the high prevalence of physical comorbidity in FM patients and the challenges of finding adequate treatment for two or more somatic disorders [75]. Similar to previous studies, participants reported severe levels of both pain and disability [24, 27, 90, 91], which was entirely expected given that FM is characterized by severe widespread musculoskeletal pain throughout the body that ends up having repercussions in different areas of the person's life and, consequently, affects their quality of life. Moreover, the delay between the onset of pain and the clinical diagnosis of FM of the participants was, on average, almost 10 years, which may have affected their functioning and recovery processes. In fact, FM patients consider the lack of a clear explanation of the etiology and their doubts about the authenticity of the illness to be key factors in the delay in receiving a diagnosis. Both aspects are related to the lack of understanding and support from family and friends due to a lack of understanding of the nature of the illness and stigma [9], something that frequently occurs in mental disorders [92].
Several limitations have to be considered when translating our results into clinical reality. The first limitation is that we did not include a matched control group to compare our results with those of the FM group, which needs to be taken into account when interpreting and generalizing our results. Second, we did not control for possible psychiatric drug effects that could be interfering with the clinical manifestations reported by the participants. Third, the sample comprised solely female participants, so we do not know whether these results can be extrapolated to the male population. However, previous data shows that mainly female patients are affected by FM [30]. Fourth, the participants were recruited mainly from two services of our hospital, with the constraints that this entails: we might have missed FM patients who are attended by their general practitioner with lower levels of pain, clinical severity, and disability. Fifth, the method for assessing trauma varied between trauma-specific scales and an individual's chronological interview by self-report, meaning it can be affected by recall bias and an individual's subjective interpretation [93]. However, a prior study emphasizes the importance and clinical relevance of subjective memories in a recent natural human behaviour publication [94]. The authors compared in a cohort of 1196 children both objective, court-documented evidence of maltreatment and subjective reports of their childhood maltreatment histories, and found psychopathology in adulthood to be associated with subjective rather than objective measures of experience of childhood maltreatment. Furthermore, amnestic dissociation might alter the recall process; interestingly, we detected very low scores in amnestic dissociation, which further underlines the consistency of subjective recalls. Finally, we did not evaluate nonpharmacological interventions in FM, such as physical exercise or others, which can exert a positive effect on anxiety and depression.
The strengths of our work included the exhaustive evaluation of psychosocial and clinical data; a detailed evaluation of psychological trauma and its impact on participants by using validated psychometric tools; and a detailed knowledge of the chronology of traumatic events, allowing us to sequence the appearance of pain in their lives. Furthermore, the homogeneity between raters has helped to obtain data, reducing observational bias.
6. Conclusions
Our data highlight the complex comorbidity of FM patients with somatic disorders, psychiatric disorders, such as anxiety, depression and PTSD, highly prevalent suicidal behavior, and sleep alterations. Patients with FM, who are usually treated by rheumatologists, receive multiple psychotropic and analgesic medications, with often unsatisfactory results [95]. Our data specifically emphasize the importance of psychological trauma, especially childhood trauma, in the onset and maintenance of pain. However, close monitoring and treatment of psychological trauma are also indicated across the lifespan of FM patients. This should encourage clinicians to assess psychological trauma routinely and to include trauma-focused therapies within established multidisciplinary health care professionals, following existing FM guidelines [96]. Future research lines should test the trauma-focused intervention in FM and could also clarify the trauma-based etiology of FM in comparison to other FSSs, medically unexplained symptoms, somatic symptoms, and related disorders following the DSM-5.
Acknowledgments
Ana Moreno-Alcázar wants to thank to the “Ministry of Universities and Research of the Department of Economics and Knowledge (2017 SGR 46 to “Centre Forum Research Unit”), Government of Catalonia” for its recognition as an emerging research group. B. Hogg is supported by the Institute of Health Carlos III with a PFIS grant (FI10/00017). A. Valiente-Gómez is supported by the Institute of Health Carlos III with a Juan Rodés grant (JR19/00001). B. L. Amann received a project grant (PI18/00009) and a mobility grant (BA21/00002) from the Institute of Health Carlos III ‐ General Sub-Directorate for Research Evaluation and Promotion ‐ National Plan 2008-2011 and 2013-2016.
Data Availability
Data are available on request due to privacy/ethical restrictions.
Disclosure
The Instituto de Salud Carlos III had no further role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Conflicts of Interest
All authors declare that they have no conflicts of interest.
Authors' Contributions
Benedikt L. Amann and Ana Moreno-Alcázzar share the last authorship.
References
- 1.Clauw D. J. Fibromyalgia: a clinical review. JAMA, the Journal of the American Medical Association . 2014;311(15):1547–1555. doi: 10.1001/jama.2014.3266. [DOI] [PubMed] [Google Scholar]
- 2.Jones G. T., Atzeni F., Beasley M., Flüß E., Sarzi-Puttini P., Macfarlane G. J. The prevalence of fibromyalgia in the general population: a comparison of the American College of Rheumatology 1990, 2010, and modified 2010 classification criteria. Arthritis & Rheumatology . 2015;67(2):568–575. doi: 10.1002/art.38905. [DOI] [PubMed] [Google Scholar]
- 3.Teodoro T., Edwards M. J., Isaacs J. D. A unifying theory for cognitive abnormalities in functional neurological disorders, fibromyalgia and chronic fatigue syndrome: systematic review. Journal of Neurology, Neurosurgery & Psychiatry . 2018;89(12):1308–1319. doi: 10.1136/jnnp-2017-317823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chinn S., Caldwell W., Gritsenko K. Fibromyalgia pathogenesis and treatment options update. Current Pain and Headache Reports . 2016;20(4):25–10. doi: 10.1007/s11916-016-0556-x. [DOI] [PubMed] [Google Scholar]
- 5.Häuser W., Ablin J., Fitzcharles M. A., et al. Fibromyalgia. Nature Reviews Disease Primers . 2015;1(1):15022–15116. doi: 10.1038/nrdp.2015.22. [DOI] [PubMed] [Google Scholar]
- 6.Sarzi-Puttini P., Giorgi V., Marotto D., Atzeni F. Fibromyalgia: an update on clinical characteristics, aetiopathogenesis and treatment. Nature Reviews Rheumatology . 2020;16(11):645–660. doi: 10.1038/s41584-020-00506-w. [DOI] [PubMed] [Google Scholar]
- 7.Lowe J. C., Yellin J. Inadequate thyroid hormone regulation as the main mechanism of fibromyalgia: a review of the evidence. Thyroid Science . 2008;3(6):1–14. [Google Scholar]
- 8.O’Brien A. T., Deitos A., Triñanes Pego Y., Fregni F., Carrillo-de-la-Peña M. T. Defective endogenous pain modulation in fibromyalgia: a meta-analysis of temporal summation and conditioned pain modulation paradigms. The Journal of Pain . 2018;19(8):819–836. doi: 10.1016/j.jpain.2018.01.010. [DOI] [PubMed] [Google Scholar]
- 9.Galvez-Sánchez C. M., Duschek S., Reyes del Paso G. A. <p>Psychological impact of fibromyalgia: current perspectives</p>. Psychology Research and Behavior Management . 2019;12:117–127. doi: 10.2147/PRBM.S178240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gold A. R. Functional somatic syndromes, anxiety disorders and the upper airway: a matter of paradigms. Sleep Medicine Reviews . 2011;15(6):389–401. doi: 10.1016/j.smrv.2010.11.004. [DOI] [PubMed] [Google Scholar]
- 11.Low L. A., Schweinhardt P. Early Life Adversity as a Risk Factor for Fibromyalgia in Later Life. Pain Research and Treatment . 2012;2012 doi: 10.1155/2012/140832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.M Nater U., Fischer S., Ehlert U. Stress as a pathophysiological factor in functional somatic syndromes. Current Psychiatry Reviews . 2011;7(2):152–169. [Google Scholar]
- 13.Kolk B. A., Brown P., Hart O. Pierre Janet on post-traumatic stress. Journal of Traumatic Stress . 1989;2(4):365–378. [Google Scholar]
- 14.Martínez Ibáñez J. J. Repensando el concepto de trauma. Una redefinición desde los aportes del psicoanálisis relacional. Clínica e Investigación Relacional . 2010;4(3):1–20. [Google Scholar]
- 15.Sin J., Furuta M., Murrells T., Norman I. Psychological interventions for post-traumatic stress disorder (PTSD) in people with severe mental illness (Review) The Cochrane Library . 2017;1:1–103. doi: 10.1002/14651858.CD011464.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Teicher M. H., Samson J. A. Childhood maltreatment and psychopathology: a case for ecophenotypic variants as clinically and neurobiologically distinct subtypes. American Journal of Psychiatry . 2013;170(10):1114–1133. doi: 10.1176/appi.ajp.2013.12070957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nievergelt C. M., Maihofer A. X., Klengel T., et al. International meta-analysis of PTSD genome-wide association studies identifies sex- and ancestry-specific genetic risk loci. Nature Communications . 2019;10(1):4558–4616. doi: 10.1038/s41467-019-12576-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Felitti V. J., Anda R. F., Nordenberg D., et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. American Journal of Preventive Medicine . 1998;14(4):245–258. doi: 10.1016/s0749-3797(98)00017-8. [DOI] [PubMed] [Google Scholar]
- 19.Teicher M. H., Gordon J. B., Nemeroff C. B. Recognizing the importance of childhood maltreatment as a critical factor in psychiatric diagnoses, treatment, research, prevention, and education. Molecular Psychiatry . 2021;27(3):1331–1338. doi: 10.1038/s41380-021-01367-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kaleycheva N., Cullen A. E., Evans R., Harris T., Nicholson T., Chalder T. The role of lifetime stressors in adult fibromyalgia: systematic review and meta-analysis of case-control studies. Psychological Medicine . 2021;51(2):177–193. doi: 10.1017/S0033291720004547. [DOI] [PubMed] [Google Scholar]
- 21.White K. P., Carette S., Harth M., Teasell R. W. Trauma and fibromyalgia: is there an association and what does it mean? Seminars in Arthritis and Rheumatism . 2000;29(4):200–216. doi: 10.1016/s0049-0172(00)80009-8. [DOI] [PubMed] [Google Scholar]
- 22.Yavne Y., Amital D., Watad A., Tiosano S., Amital H. A systematic review of precipitating physical and psychological traumatic events in the development of fibromyalgia. Seminars in Arthritis and Rheumatism . 2018;48(1):121–133. doi: 10.1016/j.semarthrit.2017.12.011. [DOI] [PubMed] [Google Scholar]
- 23.Gündüz N., Polat A., Erzincan E., Turan H., Sade I., Tural Ü. Psychiatric comorbidity and childhood trauma in fibromyalgia syndrome. Turkish Journal of Physical Medicine and Rehabilitation . 2018;64(2):91–99. doi: 10.5606/tftrd.2018.1470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Karagüzel E. Ö., Karkucak M., Saglam D. A., Tiryaki A., Karahan A., Capkin E. Sexual dysfunction and childhood trauma in female patients with fibromyalgia. Israel Journal of Psychiatry . 2018;55(2):10–14. [PubMed] [Google Scholar]
- 25.Bayram K., Erol A. Childhood traumatic experiences, anxiety, and depression levels in fibromyalgia and rheumatoid arthritis. Noro Psikiyatri Arsivi . 2014;51(4):344–349. doi: 10.5152/npa.2014.6958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.De Roa P., Paris P., Poindessous J. L., Maillet O., Héron A. Subjective experiences and sensitivities in women with fibromyalgia: a quantitative and comparative study. Pain Research and Management . 2018;2018(8269564):1–8. doi: 10.1155/2018/8269564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hellou R., Häuser W., Brenner I., et al. Self-reported Childhood Maltreatment and Traumatic Events Among Israeli Patients Suffering from Fibromyalgia and Rheumatoid Arthritis. Pain Research and Management . 2017;2017 doi: 10.1155/2017/3865249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Borsini A., Hepgul N., Mondelli V., Chalder T., Pariante C. M. Childhood stressors in the development of fatigue syndromes: a review of the past 20 years of research. Psychological Medicine . 2014;44(9):1809–1823. doi: 10.1017/S0033291713002468. [DOI] [PubMed] [Google Scholar]
- 29.Walker E. A., Keegan D., Gardner G., Sullivan M., Bernstein D., Katon W. J. Psychosocial factors in fibromyalgia compared with rheumatoid arthritis: II. Sexual, physical, and emotional abuse and neglect. Psychosomatic Medicine . 1997;59(6):572–577. doi: 10.1097/00006842-199711000-00003. [DOI] [PubMed] [Google Scholar]
- 30.Wolfe F., Clauw D. J., Fitzcharles M. A., et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care & Research . 2010;62(5):600–610. doi: 10.1002/acr.20140. [DOI] [PubMed] [Google Scholar]
- 31.Price D. D., McGrath P. A., Rafii A., Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain . 1983;17(1):45–56. doi: 10.1016/0304-3959(83)90126-4. [DOI] [PubMed] [Google Scholar]
- 32.Tait R. C., Chibnall J. T., Krause S. The pain disability Index: psychometric properties. Pain . 1990;40(2):171–182. doi: 10.1016/0304-3959(90)90068-O. [DOI] [PubMed] [Google Scholar]
- 33.Burckhardt C. S., Clark S. R., Bennett R. M. The fibromyalgia impact questionnaire: development and validation. Journal of Rheumatology . 1991;18(5):728–733. [PubMed] [Google Scholar]
- 34.Monterde S. Validación de la versión española del Fibromyalgia Impact Questionnaire. Revista Española de Reumatología: Órgano Oficial de La Sociedad Española de Reumatología . 2004;31(9):p. 507. [Google Scholar]
- 35.Crespo M., Gómez M. del M., Soberón C. TEA Ediciones . Madrid, Spain: TEA Ediciones; 2017. EGEP-5 evaluacuón global de Estrés postraumático. [Google Scholar]
- 36.Kiyimba N., O’Reilly M. The clinical use of Subjective Units of Distress scales (SUDs) in child mental health assessments: a thematic evaluation. Journal of Mental Health . 2020;29(4):418–423. doi: 10.1080/09638237.2017.1340616. [DOI] [PubMed] [Google Scholar]
- 37.Holmes T. H., Rahe R. H. The social readjustment rating scale. Journal of Psychosomatic Research . 1967;11(2):213–218. doi: 10.1016/0022-3999(67)90010-4. [DOI] [PubMed] [Google Scholar]
- 38.González de Rivera y Revuelta J. L., Morera Fumero A. La valoración de sucesos vitales: adaptación española de la escala de Holmes y Rahe. Psiquis . 1983;4(1):7–1. [Google Scholar]
- 39.Bernstein D. P., Fink L., Handelsman L., et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. American Journal of Psychiatry . 1994;151(8):1132–1136. doi: 10.1176/ajp.151.8.1132. [DOI] [PubMed] [Google Scholar]
- 40.Hernandez A., Gallardo-Pujol D., Pereda N., et al. Initial validation of the Spanish childhood trauma questionnaire-short form: factor structure, reliability and association with parenting. Journal of Interpersonal Violence . 2013;28(7):1498–1518. doi: 10.1177/0886260512468240. [DOI] [PubMed] [Google Scholar]
- 41.Dubester K. A., Braun B. G. Psychometric properties of the dissociative experiences scale. The Journal of Nervous and Mental Disease . 1995;183(4):231–235. doi: 10.1097/00005053-199504000-00008. [DOI] [PubMed] [Google Scholar]
- 42.Icaran E., Colom R., Orengo Garcia F. Experiencias disociativas: una escala de medida. Anuario de Psicología . 1996;70:69–84. [Google Scholar]
- 43.Nijenhuis E. R. S., Spinhoven P., Van Dyck R., Der Hart O. V., Vanderlinden J. The development and psychometric characteristics of the Somatoform Dissociation Questionnaire (SDQ-20) The Journal of Nervous and Mental Disease . 1996;184(11):688–694. doi: 10.1097/00005053-199611000-00006. [DOI] [PubMed] [Google Scholar]
- 44.González-Vázquez A. I., Del Río-Casanova L., Santed-German M. A, et al. Validity and reliability of the Spanish version of the somatoform dissociation questionnaire (SDQ-20) Psicothema . 2017;29(2):275–280. doi: 10.7334/psicothema2016.346. [DOI] [PubMed] [Google Scholar]
- 45.Sheehan D. V., Lecrubier Y., Sheehan K. H., et al. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry . 1998;59(Suppl 20):p. 22. [PubMed] [Google Scholar]
- 46.Ferrando L., Soto M., Bobes J., Soto O., Franco L., Gubert J. M.I.N.I. Mini international neuropsychiatric interview. Versión en español 5.0.0. DSM-IV. Intituto IAP. The Journal of clinical psychiatry . 1998;59 [Google Scholar]
- 47.Stern A. F., Snaith R. P. The hospital anxiety and depression scale. Occupational Medicine . 2014;64(5):393–394. doi: 10.1093/occmed/kqu024. [DOI] [PubMed] [Google Scholar]
- 48.De Las Cuevas Castresana C., Garcia-Estrada Perez A., Gonzalez de Rivera J. L. Hospital anxiety and depression scale Y psicopatologia afectiva. Anales de Psiquiatría . 1995;11(4):126–130. [Google Scholar]
- 49.Soldatos C. R., Dikeos D. G., Paparrigopoulos T. J. Athens insomnia scale: validation of an instrument based on ICD-10 criteria. Journal of Psychosomatic Research . 2000;48(6):555–560. doi: 10.1016/s0022-3999(00)00095-7. [DOI] [PubMed] [Google Scholar]
- 50.Portocarrero A. N., Jiménez-Genchi A. Estudio de validación de la traducción al Español de la Escala Atenas de Insomnio. Salud Mental . 2005;28(5):34–39. [Google Scholar]
- 51.Diener E., Emmons R. A., Larsen R. J., Griffin S. The satisfaction with life scale. Journal of Personality Assessment . 1985;49(1):71–75. doi: 10.1207/s15327752jpa4901_13. [DOI] [PubMed] [Google Scholar]
- 52.Atienza F. L., Pons D., Balaguer I., García-Merita M. Propiedades Psicométricas de la Escala de Satisfacción con la Vida en Adolescentes. Psicothema . 2000;12(2):314–319. [Google Scholar]
- 53.Shalev A., Liberzon I., Marmar C. Post-traumatic stress disorder. New England Journal of Medicine . 2017;376(25):2459–2469. doi: 10.1056/NEJMra1612499. [DOI] [PubMed] [Google Scholar]
- 54.Brady K. T., Killeen T. K., Brewerton T., Lucerini S. Comorbidity of psychiatric disorders and posttraumatic stress disorder. Journal of Clinical Psychiatry . 2000;61(Suppl 7):22–32. [PubMed] [Google Scholar]
- 55.Hernandez J. M., Cordova M. J., Ruzek J., et al. Presentation and prevalence of PTSD in a bipolar disorder population: a STEP-BD examination. Journal of Affective Disorders . 2013b;150(2):450–455. doi: 10.1016/j.jad.2013.04.038. [DOI] [PubMed] [Google Scholar]
- 56.Blanco L., Sió A., Hogg B., et al. Traumatic events in dual disorders: prevalence and clinical characteristics. Journal of Clinical Medicine . 2020;9(8):p. 2553. doi: 10.3390/jcm9082553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Kind S., Otis J. D. The interaction between chronic pain and PTSD. Current Pain and Headache Reports . 2019;23(12):p. 91. doi: 10.1007/s11916-019-0828-3. [DOI] [PubMed] [Google Scholar]
- 58.Bohn D., Bernardy K., Wolfe F., Häuser W. The association among childhood maltreatment, somatic symptom intensity, depression, and somatoform dissociative symptoms in patients with fibromyalgia syndrome: a single-center cohort study. Journal of Trauma & Dissociation . 2013;14(3):342–358. doi: 10.1080/15299732.2012.736930. [DOI] [PubMed] [Google Scholar]
- 59.Filippon A. P. M., Bassani D. G., Aguiar R. W. de, Ceitlin L. H. F. Association between childhood trauma and loss of functionality in adult women with fibromyalgia. Trends in Psychiatry and Psychotherapy . 2013;35(1):46–54. doi: 10.1590/s2237-60892013000100006. [DOI] [PubMed] [Google Scholar]
- 60.Häuser W., Kosseva M., Üceyler N., Klose P., Sommer C. Emotional, physical, and sexual abuse in fibromyalgia syndrome: a systematic review with Meta-Analysis. Arthritis Care & Research . 2011;63(6):808–820. doi: 10.1002/acr.20328. [DOI] [PubMed] [Google Scholar]
- 61.Huffhines L., Jackson Y. Child maltreatment, chronic pain, and other chronic health conditions in youth in foster care. Journal of Child & Adolescent Trauma . 2019;12(4):437–445. doi: 10.1007/s40653-019-0248-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Norman R. E., Byambaa M., De R., Butchart A., Scott J., Vos T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine . 2012;9(11):p. e1001349. doi: 10.1371/journal.pmed.1001349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Collishaw S., Pickles A., Messer J., Rutter M., Shearer C., Maughan B. Resilience to Adult Psychopathology Following Childhood Maltreatment: Evidence from a Community Sample. Child Abuse & Neglect . 2007;31 doi: 10.1016/j.chiabu.2007.02.004. [DOI] [PubMed] [Google Scholar]
- 64.Rikhye K., Tyrka A. R., Kelly M. M., et al. Interplay between childhood maltreatment, parental bonding, and gender effects: impact on quality of life. Child Abuse & Neglect . 2008;32(1):19–34. doi: 10.1016/j.chiabu.2007.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Cheung K., Taillieu T., Turner S., et al. Relationship and community factors related to better mental health following child maltreatment among adolescents. Child Abuse & Neglect . 2017;70(July):377–387. doi: 10.1016/j.chiabu.2017.06.026. [DOI] [PubMed] [Google Scholar]
- 66.Nanni V., Uher R., Danese A. Childhood maltreatment predicts unfavorable course of illness and treatment outcome in depression: a meta-analysis. American Journal of Psychiatry . 2012;169(2):141–151. doi: 10.1176/appi.ajp.2011.11020335. [DOI] [PubMed] [Google Scholar]
- 67.Burke N. N., Finn D. P., McGuire B. E., Roche M. Psychological stress in early life as a predisposing factor for the development of chronic pain: clinical and preclinical evidence and neurobiological mechanisms. Journal of Neuroscience Research . 2017;95(6):1257–1270. doi: 10.1002/jnr.23802. [DOI] [PubMed] [Google Scholar]
- 68.Van Houdenhove B., Egle U. T. Fibromyalgia: a stress disorder? Piecing the biopsychosocial puzzle together. Psychotherapy and Psychosomatics . 2004;73(5):267–275. doi: 10.1159/000078843. [DOI] [PubMed] [Google Scholar]
- 69.Ahles T. A., Yunus M. B., Riley S. D., Bradley J. M., Masi A. T. Psychological factors associated with primary fibromyalgia syndrome. Arthritis & Rheumatism . 1984;27(10):1101–1106. doi: 10.1002/art.1780271004. [DOI] [PubMed] [Google Scholar]
- 70.Romeo A., Tesio V., Ghiggia A., et al. Traumatic experiences and somatoform dissociation in women with fibromyalgia . Psychological Trauma: Theory, Research, Practice, and Policy; 2021. [DOI] [PubMed] [Google Scholar]
- 71.Marin M.-F., Lord C., Andrews J., et al. Chronic stress, cognitive functioning and mental health. Neurobiology of Learning and Memory . 2011;96(4):583–595. doi: 10.1016/j.nlm.2011.02.016. [DOI] [PubMed] [Google Scholar]
- 72.Sutar R., Sahu S. Pharmacotherapy for dissociative disorders: a systematic review. Psychiatry Research . 2019;281(August):p. 112529. doi: 10.1016/j.psychres.2019.112529. [DOI] [PubMed] [Google Scholar]
- 73.Näring G. W. B., Van Lankveld W., Geenen R. Somatoform dissociation and traumatic experiences in patients with rheumatoid arthritis and fibromyalgia. Clinical & Experimental Rheumatology . 2007;25(6):872–877. [PubMed] [Google Scholar]
- 74.Kilic O., Sar V., Taycan O., et al. Dissociative depression among women with fibromyalgia or rheumatoid arthritis. Journal of Trauma & Dissociation . 2014;15(3):285–302. doi: 10.1080/15299732.2013.844218. [DOI] [PubMed] [Google Scholar]
- 75.Lichtenstein A., Tiosano S., Amital H. The complexities of fibromyalgia and its comorbidities. Current Opinion in Rheumatology . 2018;30(1):94–100. doi: 10.1097/BOR.0000000000000464. [DOI] [PubMed] [Google Scholar]
- 76.Gureje O., Simon G. E., Von Korff M. A cross-national study of the course of persistent pain in primary care. Pain . 2001;92(1):195–200. doi: 10.1016/s0304-3959(00)00483-8. [DOI] [PubMed] [Google Scholar]
- 77.Magni G., Moreschi C., Rigatti-Luchini S., Merskey H. Prospective study on the relationship between depressive symptoms and chronic musculoskeletal pain. Pain . 1994;56(3):289–297. doi: 10.1016/0304-3959(94)90167-8. [DOI] [PubMed] [Google Scholar]
- 78.Asbring P. Chronic illness – a disruption in life: identity-transformation among women with chronic fatigue syndrome and fibromyalgia. Journal of Advanced Nursing . 2001;34(3):312–319. doi: 10.1046/j.1365-2648.2001.01767.x. [DOI] [PubMed] [Google Scholar]
- 79.Ehrlich G. E. Pain is real; fibromyalgia isn’t. Journal of Rheumatology . 2003;30:1665–1667. [PubMed] [Google Scholar]
- 80.Levine D., Horesh D. Suicidality in fibromyalgia: a systematic review of the literature. Frontiers in Psychiatry . 2020;11(September):p. 535368. doi: 10.3389/fpsyt.2020.535368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.McKernan L. C., Lenert M. C., Crofford L. J., Walsh C. G. Outpatient engagement and predicted risk of suicide attempts in fibromyalgia. Arthritis Care & Research . 2019;71(9):1255–1263. doi: 10.1002/acr.23748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Theadom A., Cropley M., Humphrey K. L. Exploring the role of sleep and coping in quality of life in fibromyalgia. Journal of Psychosomatic Research . 2007;62(2):145–151. doi: 10.1016/j.jpsychores.2006.09.013. [DOI] [PubMed] [Google Scholar]
- 83.Griffith J. P., Zarrouf F. A. A systematic review of chronic fatigue syndrome: don’t assume it’s depression. Primary Care Companion to the Journal of Clinical Psychiatry . 2008;10(2):120–128. doi: 10.4088/pcc.v10n0206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Neki N., van der Meer J. W. M., Bleijenberg G. Chronic fatigue syndrome – Revisited. Bangladesh Journal of Medical Science . 2016;15(3):326–328. [Google Scholar]
- 85.Wu Y. L., Chang L. Y., Lee H. C., Fang S. C., Tsai P. S. Sleep disturbances in fibromyalgia: a meta-analysis of case-control studies. Journal of Psychosomatic Research . 2017;96:89–97. doi: 10.1016/j.jpsychores.2017.03.011. [DOI] [PubMed] [Google Scholar]
- 86.Cherry B., Ruiz M., Langmesser P., et al. Poor sleep negatively impacts pain, mood and quality of life in adults with fibromyalgia. Innovation in Aging . 2017;1(suppl_1):147–148. [Google Scholar]
- 87.Smith M. T., Perlis M. L., Smith M. S., Giles D. E., Carmody T. P. Sleep quality and presleep arousal in chronic pain. Journal of Behavioral Medicine . 2000;23(1):1–13. doi: 10.1023/a:1005444719169. [DOI] [PubMed] [Google Scholar]
- 88.Cunningham T., Hoy K., Shannon C. Does childhood bullying lead to the development of psychotic symptoms? A meta-analysis and review of prospective studies. Psychosis . 2016;8(1):48–59. [Google Scholar]
- 89.Bourke J. H., Langford R. M., White P. D. The common link between functional somatic syndromes may be central sensitisation. Journal of Psychosomatic Research . 2015;78(3):228–236. doi: 10.1016/j.jpsychores.2015.01.003. [DOI] [PubMed] [Google Scholar]
- 90.Multanen J., Häkkinen A., Heikkinen P., Kautiainen H., Mustalampi S., Ylinen J. Pulsed electromagnetic field therapy in the treatment of pain and other symptoms in fibromyalgia: a randomized controlled study. Bioelectromagnetics . 2018;39(5):405–413. doi: 10.1002/bem.22127. [DOI] [PubMed] [Google Scholar]
- 91.Udina-Cortés C., Fernández-Carnero J., Romano A. A., et al. Effects of neuro-adaptive electrostimulation therapy on pain and disability in fibromyalgia: a prospective, randomized, double-blind study. Medicine . 2020;99(51) doi: 10.1097/MD.0000000000023785.e23785 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Freidl M., Spitzl S. P., Prause W., et al. The stigma of mental illness: anticipation and attitudes among patients with epileptic, dissociative or somatoform pain disorder. International Review of Psychiatry . 2007;19(2):123–129. doi: 10.1080/09540260701278879. [DOI] [PubMed] [Google Scholar]
- 93.Frissa S., Hatch S. L., Fear N. T., Dorrington S., Goodwin L., Hotopf M. Challenges in the retrospective assessment of trauma: comparing a checklist approach to a single item trauma experience screening question. BMC Psychiatry . 2016;16(1):20–29. doi: 10.1186/s12888-016-0720-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Danese A., Widom C. S. Objective and subjective experiences of child maltreatment and their relationships with psychopathology. Nature Human Behaviour . 2020;4(8):811–818. doi: 10.1038/s41562-020-0880-3. [DOI] [PubMed] [Google Scholar]
- 95.Thorpe J., Shum B., Moore R. A., Wiffen P. J., Gilron I. Combination pharmacotherapy for the treatment of fibromyalgia in adults. Cochrane Database of Systematic Reviews . 2018;2(2) doi: 10.1002/14651858.CD010585.pub2.CD010585 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Häuser W., Jones G. Psychological therapies for chronic widespread pain and fibromyalgia syndrome. Best Practice & Research Clinical Rheumatology . 2019;33(3) doi: 10.1016/j.berh.2019.05.001.101416 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data are available on request due to privacy/ethical restrictions.