

Abstract
Background:
Frontline health care workers (FLHCW) like doctors and nurses are bound to treat COVID patients being themselves not immune to disease are at a greater risk of COVID infection than the general population. The study was started with objectives to find out the vaccine hesitancy towards the COVID vaccine and to find out the factors associated with vaccine hesitancy among FLHCW working in a designated COVID care center.
Materials and Methods:
The present study was a cross-sectional study carried out for a period of 6 months from Jan 2021 to June 2021 at a designated COVID care center. FLHCWs who were part of treating COVID patients were our study participants. Among them, FLHCWs who had not received even one dose of COVID vaccine (Covishield) were included in the study. FLHCWs who had been part of the COVID vaccine trial were excluded from the study. The sample size calculated based on a previous study found to be 240. The data collected were entered into a Microsoft office excel sheet, analyzed using SPSS v 22(IBM Corp). Descriptive statistics were applied, and parametric tests were used to compare among the groups with statistically significant P value lesser than 0.05
Results:
A total of 121 (52.6%) of FLHCWs were aged more than 30 years, 118 (51.5%) were male participants, 100 (43.5%) were paramedics by occupation, 51 (22.1%) had contracted COVID infection, 202 (87.8%) had received information, education, and communication (IEC) regarding COVID vaccine. FLHCWs more than 30 years, male participants, currently not working in COVIDward, FLHCWs who had not received IEC about COVIDvaccination and paramedics had higher scores of Vaccine hesitancy, and the difference was statistically significant indicating vaccine hesitancy.
Conclusion:
Vaccine hesitancy remains a persistent global threat. Awareness campaigns can be tailored to specific locales to address identified concerns regarding vaccines.
Keywords: COVID vaccine, frontline health care workers, vaccine hesitancy
Introduction
The world witnessed the COVID pandemic which started in 2019 and has shown little signs of weaning since then. Health care workers are tirelessly working since the start of the pandemic risking their life and family. Factors like inadequate protective gears at the initial phase of pandemic, overstrained infrastructure due to the huge number of COVID infections, under-exposure, and lesser experience to epidemics have psychologically affected the frontline health care (FLHCW) workers immensely.[1] Even though FLHCW() like doctors and nurses are bound to treat COVID patients, they themselves are not immune to disease and have contracted the infection showing that frontline workers are at a greater risk than the general population.[2,3] This tricky situation has put the FLHCW into various mental health issues like increased anxiety, stress, disturbed sleep before getting infected and after being diagnosed with COVID have faced social isolation, stigma, depression, and sometimes death.[4,5,6] With time, the pathology of COVID was more understood and so the communication of disease and prevention of its spread. Ongoing in vitro trials started showing vaccination could be effective.[7,8]
The world started witnessing the downfall of cases along with the initiation of a vaccination drive. Though there were many vaccines under trial, India started the largest vaccination drive with FLHCW given the first preference.[9] One of the main reasons for vaccinating FLHCWs for vaccination was that they can be the potential ambassadors of COVID-19 vaccine acceptance, helping to ensure that sufficient members of a hesitant public accept COVID-19 vaccines to achieve population immunity and suppress this pandemic by having adequate herd immunity.[10] However, there was vaccine hesitancy for COVID-19 in various parts of the world. “Vaccine hesitancy” is the term used to describe the delay in acceptance or refusal of vaccination despite the availability of vaccination services.[11,12] So, with this background, the study was started with objectives to find out the vaccine hesitancy towards COVID vaccine and to find out the factors associated with vaccine hesitancy among frontline health care workers working in a designated COVID care center.
Materials and Methods
The present study was a cross-sectional study carried out for a period of 6 months from January 2021 to June 2021 carried out at R.L. Jalappa Hospital and Research center, Tamaka, Kolar which is a designated COVID carecenter. FLHCWs aged less than 60 years and more than 18 years who were part of treating COVID patients were our study participants. Among them, FLHCWs who had not received even one dose of COVID vaccine (Covishield) were included in the study. FLHCWs who had contracted COVID infection for which they could not take vaccination and FLHCWs who have been part of the COVID vaccine trial were excluded from the study. Sample size calculated based on a previous study where vaccine hesitancy for COVID was found to be 31.4%(p) among health care professionals with an error of 6%, 95% confidence interval sample size calculated was 240.[13] The sample size was calculated using the online tool Open Epi software version 3.01 selection of frontline health care workers have been depicted in [Flowchart 1]. To assess the socio-demographic details, pretested semi-structured questionnaire was used. To assess the attitude towards a vaccine, the Vaccination Attitudes Examination (VAX) scale was used. The VAX scale contains 12 questions assessing the attitudes that may underlie vaccine hesitancy. Questions tap into mistrust of vaccine benefit, worries about unforeseen future effects, concerns about commercial profiteering, and preference for natural immunity. Items were scored on a five-point scale (1 = “strongly disagree” to 5 = “strongly agree”), and higher scores represent more negative views towards vaccination.[14] All data collected by Interview technique lasting not more than 15 min. The data collected were entered into a Microsoft office excel sheet, analyzed using SPSS v 22(IBM Corp). Descriptive statistics were applied. After checking the normality of data, a parametric test wasapplied. To compare the difference between two groups, a t-test was applied and for three groups, ANOVA was applied with post hoc test and Bonferoni corrections. Level of significance was defined as P- value less than 0.05. The study was started after obtaining Ethical committee clearance from the Institutional Ethical Committee of the University (SDUMC/KLR/IEC/136/2021-22) Informed written consent was taken from the study participants by informing them about the benefits and risks involved in the study. Participation by the study participant was voluntary. Confidentiality of the participants’ was maintained.
Flowchart 1.
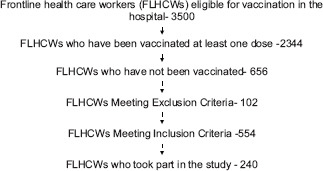
Selection of FLHCWs for study
Results
A total of 126 (52.5%) of FLHCWs were aged more than 30 years, 123 (51.2%) were male participants, 106 (44.2%) were paramedics by occupation, 61 (25.4%) had contracted COVID infection, 202 (84.1%) had received information, education, and communication (IEC) regarding COVID vaccine [Table 1].
Table 1.
Distribution of FLHCWs according to socio-demographic profile
| Socio-demographic features | Frequency | Percent |
|---|---|---|
| Age in years | ||
| <30 | 114 | 47.5 |
| >30 | 126 | 52.5 |
| Gender | ||
| Male | 123 | 51.2 |
| Female | 117 | 48.8 |
| Currently Working in COVID Wards/OPD/ICU | ||
| Yes | 114 | 47.5 |
| No | 126 | 52.5 |
| Occupation | ||
| Doctors | 54 | 22.5 |
| Nurses | 80 | 33.3 |
| Para Medics | 106 | 44.2 |
| Contracted COVID infection | ||
| Yes | 61 | 25.4 |
| No | 179 | 74.6 |
| Received IEC on COVID vaccine | ||
| Yes | 202 | 84.1 |
| No | 38 | 15.9 |
FLHCWs more than 30 years compared to FLHCWs less than 30 years, male participants compared with female participants, FLHCWs currently not working in COVID ward compared with those working in COVID ward/ICU/OPD, FLHCWs who had not received IEC about COVID vaccination compared with those who had received IEC, and paramedics compared with doctors and nurses had higher scores, and the difference was statistically significant [Table 2].
Table 2.
Comparison of Vax Scores between various groups
| Socio-demographic variables | Mean±SD | P |
|---|---|---|
| Age in years | ||
| <30 | 47.5±9.2 | 0.02* |
| >30 | 50.2±6.8 | |
| Gender | ||
| Male | 50.4±8.1 | 0.05* |
| Female | 47.3±7.4 | |
| Currently Working in COVID Wards/OPD/ICU | ||
| Yes | 45.7±9.7 | 0.001* |
| No | 50.2±6.5 | |
| Contracted COVID infection | ||
| Yes | 46.8±9.0 | 0.13 |
| No | 49.3±7.6 | |
| Received IEC on COVID vaccine | ||
| Yes | 48.5±7.8 | 0.02* |
| No | 54.2±7.6 | |
| Occupation | ||
| Doctors | 44.5±9.1 | 0.01** |
| Nurses | 48.1±9.3 | |
| Paramedics | 51.8±4.9 |
P<0.05. *Statistically significant, Independent t-test. P<0.05** statistically significant, One way ANOVA test
FLHCWs aged more than 30 years had higher scores in sub-domains Worrisome future and Commercial profiteering compared to those less than 30 years, and this difference was statistically significant. FLHCWs currently not working in COVID ICU/ward/OPD had higher scores in Worrisome future and Commercial profiteering compared to those working in COVID wards/ICU/OPD, and this difference was statistically significant. Paramedics had a higher score in the commercial profiteering subdomain compared with doctors and nurses, and this difference was statistically significant [Table 3].
Table 3.
Comparison between groups according to various sub domains
| Socio-demographic variables | Mean±SD | |||
|---|---|---|---|---|
|
| ||||
| Mistrust | Worrisome future | Commercial profiteering | Natural immunity | |
| Age in years | ||||
| <30 | 11.5±3.2 | 13.0±2.8 | 10.6±3.5 | 11.8±3.4 |
| >30 | 12.0±2.4 | 13.4±2.5 | 12.5±3.8 | 12.1±2.2 |
| P | 0.15 | 0.01* | 0.02* | 0.54 |
| Gender | ||||
| Male | 12.0±2.7 | 13.6±2.7 | 12.0±4.2 | 12.3±2.5 |
| Female | 11.6±2.8 | 12.8±2.6 | 11.2±3.3 | 11.5±3.0 |
| P | 0.25 | 0.12 | 0.1 | 0.49 |
| Currently Working in COVID Wards/OPD/ICU | ||||
| Yes | 12.1±4.0 | 12.3±3.4 | 9.6±4.4 | 11.6±3.6 |
| No | 11.6±2.1 | 13.6±2.1 | 12.5±3.2 | 12±2.8 |
| P | 0.28 | 0.01* | 0.01* | 0.21 |
| Contracted COVID infection | ||||
| Yes | 11.8±3.0 | 12.7±2.1 | 10.5±3.6 | 11.7±2.8 |
| No | 11.8±2.7 | 13.4±2.6 | 11.9±3.8 | 12±2.8 |
| P | 0.9 | 0.1 | 0.5 | 0.6 |
| Received IEC on COVID vaccine | ||||
| Yes | 11.8±2.9 | 13.1±2.7 | 11.5±3.8 | 11.9±2.8 |
| No | 11.5±1.5 | 14.6±1.5 | 12.8±3.1 | 13.2±2.3 |
| P | 0.5 | 0.08 | 0.19 | 0.07 |
| Occupation | ||||
| Doctors | 12.5±4.3 | 12.5±4.3 | 8.4±4.1 | 11.6±3.8 |
| Nurses | 11.5±2.7 | 11.5±2.7 | 10.8±3.3 | 11.8±3.1 |
| Paramedics | 11.7±1.8 | 11.7±1.8 | 13.8±2.5 | 12.2±1.8 |
| P | 0.1 | 0.18 | 0.02** | 0.5 |
Independent sample t-test P<0.05*. One way ANOVA test P<0.05**
Discussion
The present study was a cross-sectional study carried out for a period of 6 months from Jan 2021 to June 2021 carried out at R.L.Jalappa Hospital and Research center, Tamaka, Kolar which is a designated COVID care center. FLHCWs vaccine hesitancy towards COVID vaccine was assessed using the VAX scale which showed that FLHCWs more than 30 years, male participants, currently not working in COVID ward, FLHCWs who had not received IEC about COVVID vaccination, and paramedics had higher scores, and the difference was statistically significant indicating vaccine hesitancy.
COVID-19 vaccine acceptance had been low in the initial days of the drive in many parts of the world. A study done in Palestine among FLHCWs have shown lower acceptance for COVID-19 vaccine with male, those not having COVID19 information had more COVIDvaccine nonacceptance similar to our study with a main reason for poor acceptance being preferring the natural immunity and citing vaccine-induced immunity may not last long.[15] A study done by Harapan et al. showed that HCWs had higher acceptance of COVID vaccine irrespective of their efficacy rate or side effects.[16] A study done by Gadoth et al.[17] showed that doctors had better acceptance for COVID vaccine compared to nurses which is similar to our study where doctors had lesser scores of vaccine hesitancy compared to nurses and paramedics. COVID-19 infection being naive for the world, the fear of COVID infection has not settled, and people still have a lot of apprehension for infection.[18] Poor acceptance for COVID vaccine could be because of inadequate knowledge of the COVID-19 vaccine as few of COVID vaccines were introduced even before publishing the interim results of trials, long-term and severe side-effects concerns which were not adequately addressed with the added fear of the vaccine causing the disease and confusion about efficacy.[19,20] As COVID pandemic has shown to affect the community in waves, to control morbidity and mortality, there is a need for accelerated vaccination coverage. It is very crucial to build confidence in COVID-19 Vaccination. Governments and health authorities should improve communication and increase trust.[21]
A study done by Kwok et al.[22] among nurses showed that 37% were not willing for COVID vaccine even before the introduction of COVID vaccine and reasons were potential effectiveness, dreadful side effects and effective duration of the protectiveness of COVID-19 vaccine. Various studies done at different parts of the world among the general public before the introduction of the vaccine have shown poor acceptance and a few important reasons which needs to be addressed at early would be lack of confidence in vaccines due to quicker pace of development. It is very important to know that no single intervention is likely to be able to address vaccine hesitancy.[23,24,25,26,27]
As this pandemic has exposed vulnerability in all sectors of life, adult vaccination has also been a huge setback. Lower middle-income countries have very few or no adult vaccination in their national schedules. The success of adult vaccination depends on proper availability of vaccine stock, addressing the potential barriers of the vaccination campaign, proper national guidelines, and more of IECactivities to bring out the behavioral change, so that there is more acceptance of the vaccine.[28,29,30] The FLHCWs were chosen for COVID vaccination drive so that they can be the catalyst and bring out the behavioral modification to avoid vaccine hesitancy. Paradoxically, FLHCWs were found to have vaccine hesitancy. This needs to be addressed early as vaccinating the entire community will be the next biggest challenge, and FLHCWs need to be the role models for the successful vaccination campaign and break the chain of transmission. The general notion of the COVID vaccine is that FLHCWs will accept the vaccine better and can be role models in delivering the message of vaccination compliance. FLHCWs can influence the general public’s attitude to create interventions to alleviate the fear and misunderstandings about the COVID vaccines among health professionals. If there is poor uptake of COVID-19 vaccination campaign by FLHCWs, fighting this deadly global pandemic is expected to be more prolonged than usual. Vaccine hesitancy remains a persistent global threat. Awareness campaigns can be tailored to specific locales to address identified concerns regarding vaccines.[31,32] The uniqueness of the present study is that in spite of FLHCWs working in COVID care center are being in the close coalition against the fight of COVID pandemic, vaccine hesitancy against coronavirus disease among them was not uncommon. Having an excellent opportunity to get vaccinated against the COVID virus, many FLHCWs did not volunteer to take the vaccine, and the present study shows a few possible reasons how vaccine hesitancy could be a major factor for not getting COVID vaccination. The strengths of the study were a validated tool was used to assess vaccine hesitancy. There are very few studies showing vaccine hesitancy after the introduction of vaccines in the country’s vaccination drive. Theimitations of the study being relatively small sample size covered in only one COVID care center makes it a study of poor external validity.
Key points
FLHCWs more than 30 years, male participants, FLHCWs currently not working in COVID ward, FLHCWs who had not received IEC about COVID vaccination, and paramedics had higher scores for vaccine hesitancy. Mistrust, worrisome future, commercial profiteering, and natural immunity were few sub-domains tested where aged more than 30 years, FLHCWs not working in COVID wards/ICU/OPD and paramedics had higher scores of vaccine hesitancy.
Conclusions
As FLHCWs are the first recipients of coronavirus vaccines, their buy-in and participation in vaccination are critical in promoting uptake to a broader population. Primary health care physicians being the part of COVID vaccination drive, their participation by volunteering to get inoculated will reduce the barrier and avoid the COVID vaccine hesitancy as vaccination is the only tool that can bring down this pandemic.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Jacob J, Vijay VR, Issac A, Stephen S, Dhandapani M, Rakesh VR, et al. Factors associated with psychological outcomes among frontline healthcare providers of India during COVID-19 pandemic. Asian J Psychiatr. 2021;55:102531. doi: 10.1016/j.ajp.2020.102531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chatterjee SS, Chakrabarty M, Banerjee D, Grover S, Chatterjee SS, Dan U. Stress, sleep and psychological impact in healthcare workers during the early phase of COVID-19 in India: A factor analysis. Front Psychol. 2021;12:611314. doi: 10.3389/fpsyg.2021.611314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Misra A. Doctors and healthcare workers at frontline of COVID 19 epidemic: Admiration, a pat on the back, and need for extreme caution. Diab Metab Syndr. 2020;14:255–6. doi: 10.1016/j.dsx.2020.03.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gupta S, Sahoo S. Pandemic and mental health of the front-line healthcare workers: A review and implications in the Indian context amidst COVID-19. Gen Psychiatr. 2020;33:e100284. doi: 10.1136/gpsych-2020-100284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cabarkapa S, Nadjidai SE, Murgier J, Ng CH. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain Behav Immun Health. 2020;8:100144. doi: 10.1016/j.bbih.2020.100144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Uvais NA, Rasmina V. Physician deaths in India during COVID-19 pandemic. Occup Med. 2020;70:612–4. doi: 10.1093/occmed/kqaa159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.DeRoo SS, Pudalov NJ, Fu LY. Planning for a COVID-19 vaccination program. JAMA. 2020;323:2458–9. doi: 10.1001/jama.2020.8711. [DOI] [PubMed] [Google Scholar]
- 8.Dalvie NC, Rodriguez-Aponte SA, Hartwell BL, Tostanoski LH, Biedermann AM, Crowell LE, et al. Engineered SARS-CoV-2 receptor binding domain improves immunogenicity in mice and elicits protective immunity in hamsters. bioRxiv. 2021 doi: 10.1073/pnas.2106845118. 2021.03.03.433558. doi: 10.1101/2021.03.03.433558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bagcchi S. The world's largest COVID-19 vaccination campaign. Lancet Infect Dis. 2021;21:323. doi: 10.1016/S1473-3099(21)00081-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kumar VM, Pandi-Perumal SR, Trakht I, Thyagarajan SP. Strategy for COVID-19 vaccination in India: The country with the second highest population and number of cases. NPJ Vaccines. 2021;6:60. doi: 10.1038/s41541-021-00327-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.MacDonald NE. Sage Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine. 2015;33:4161–4. doi: 10.1016/j.vaccine.2015.04.036. [DOI] [PubMed] [Google Scholar]
- 12.Paul E, Steptoe A, Fancourt D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg Health Eur. 2021;1:100012. doi: 10.1016/j.lanepe.2020.100012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kose S, Mandiracioglu A, Sahin S, Kaynar T, Karbus O, Ozbel Y. Vaccine hesitancy of the COVID-19 by health care personnel. Int J Clin Pract. 2020:e13917. [Google Scholar]
- 14.Martin LR, Petrie KJ. Understanding the dimensions of anti-vaccination attitudes: The vaccination attitudes examination (VAX) scale. Ann Behav Med. 2017;51:652–60. doi: 10.1007/s12160-017-9888-y. [DOI] [PubMed] [Google Scholar]
- 15.Maraqa B, Nazzal Z, Rabi R, Sarhan N, Al-Shakhrah K, Al-Keile M. COVID-19 vaccine hesitancy among health care workers in Palestine: A call for action. Prev Med. 2021;149:106618. doi: 10.1016/j.ypmed.2021.106618. doi: 10.1016/j.ypmed.2021.106618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Harapan H, Wagner AL, Yufika A, Winardi W, Anwar S, Gan AK, et al. Acceptance of a COVID-19 vaccine in southeast Asia: A cross-sectional study in Indonesia. Front Public Health. 2020;8:381. doi: 10.3389/fpubh.2020.00381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gadoth A, Halbrook M, Martin-Blais R, Gray A, Tobin NH, Ferbas KG, et al. Cross-sectional assessment of COVID-19 vaccine acceptance among health care workers in Los Angeles. Ann Intern Med. 2021;174:882–5. doi: 10.7326/M20-7580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Doshi D, Karunakar P, Sukhabogi JR, Prasanna JS, Mahajan SV. Assessing coronavirus fear in Indian population using the fear of COVID-19 scale. Int J Ment Health Addict. 2020:1–9. doi: 10.1007/s11469-020-00332-x. doi: 10.1007/s11469-020-00332-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Edwards KM, Orenstein MA. Coronavirus disease 2019 (COVID-19): Vaccines to prevent SARS-CoV-2 infection. Waltham (MA): UpToDate. 2021;27 [Google Scholar]
- 20.Vasilevska M, Ku J, Fisman DN. Factors associated with healthcare worker acceptance of vaccination: A systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2014;35:699–708. doi: 10.1086/676427. [DOI] [PubMed] [Google Scholar]
- 21.Soares P, Rocha JV, Moniz M, Gama A, Laires PA, Pedro AR, et al. Factors associated with COVID-19 vaccine hesitancy. Vaccines. 2021;9:300. doi: 10.3390/vaccines9030300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kwok KO, Li KK, Wei WI, Tang A, Wong SY, Lee SS. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int J Nurs Stud. 2021;114:103854. doi: 10.1016/j.ijnurstu.2020.103854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Barello S, Nania T, Dellafiore F, Graffigna G, Caruso R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur J Epidemiol. 2020;35:781–3. doi: 10.1007/s10654-020-00670-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Fisher KA, Bloomstone SJ, Walder J, Crawford S, Fouayzi H, Mazor KM. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of US adults. Ann Intern Med. 2020;173:964–73. doi: 10.7326/M20-3569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wang K, Wong EL, Ho KF, Cheung AW, Chan EY, Yeoh EK, et al. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine. 2020;38:7049–56. doi: 10.1016/j.vaccine.2020.09.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Pogue K, Jensen JL, Stancil CK, Ferguson DG, Hughes SJ, Mello EJ, et al. Influences on attitudes regarding potential COVID-19 vaccination in the United States. Vaccines. 2020;8:582. doi: 10.3390/vaccines8040582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Detoc M, Bruel S, Frappe P, Tardy B, Botelho-Nevers E, Gagneux-Brunon A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine. 2020;38:7002–6. doi: 10.1016/j.vaccine.2020.09.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bhopal S, Nielsen M. Vaccine hesitancy in low-and middle-income countries: Potential implications for the COVID-19 response. Arch Dis Childhood. 2021;106:113–4. doi: 10.1136/archdischild-2020-318988. [DOI] [PubMed] [Google Scholar]
- 29.Neufeind J, Betsch C, Habersaat KB, Eckardt M, Schmid P, Wichmann O. Barriers and drivers to adult vaccination among family physicians–Insights for tailoring the immunization program in Germany. Vaccine. 2020;38:4252–62. doi: 10.1016/j.vaccine.2020.04.052. [DOI] [PubMed] [Google Scholar]
- 30.Dash R, Agrawal A, Nagvekar V, Lele J, Di Pasquale A, Kolhapure S, et al. Towards adult vaccination in India: A narrative literature review. Hum Vaccin Immunother. 2020;16:991–1001. doi: 10.1080/21645515.2019.1682842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Capulong HG. Mindfulness as key in easing COVID-19 vaccine hesitancy. J Public Health. 2021;43:e338–9. doi: 10.1093/pubmed/fdab050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.McAteer J, Yildirim I, Chahroudi A. The VACCINES Act: Deciphering vaccine hesitancy in the time of COVID-19. Clin Infect Dis. 2020;71:703–5. doi: 10.1093/cid/ciaa433. [DOI] [PMC free article] [PubMed] [Google Scholar]