

Abstract
Context:
Thirty-day readmissions are used to gauge health care accountability, which occurs as part of the natural course of the illness or due to avoidable fallacies during the index admission. The utility of this metric is unknown in older adults from developing countries.
Aim:
To ascertain the unplanned 30-day readmission rate and enumerate predictors of avoidable hospital readmission among early (0–7 days) and late (8–30 days) readmissions.
Settings and Design:
A retrospective chart audit of 140 older adults who were readmitted to a premier tertiary care teaching hospital under Geriatrics from the neighboring states of Tamil Nadu, Andhra Pradesh, and Kerala were undertaken.
Methods and Materials:
Data from health records were collected from the hospital electronic database from May 2015 to May 2020. The data was reviewed to determine the 30-day readmission rate and to ascertain the predictors of avoidable readmissions among both early and late readmissions.
Results:
Out of 2698 older adults admitted to the geriatric wards from the catchment areas, the calculated 30-day hospital readmission rate was 5.18%, and 41.4% of these readmissions were potentially avoidable. The median duration from discharge to the first readmission was ten days (Interquartile range: 5–18 days). Patients had to spend INR 44,000 (approximately 602 USD) towards avoidable readmission. The most common causes for readmission included an exacerbation, reactivation, or progression of a previously existing disease (55.7%), followed by the emergence of a new disease unrelated to index admission (43.2%). Fifty-eight patients (41.4%) were readmitted within seven days following discharge. Early readmissions were seen in patients with malignancies [8 (13.5%) vs. 4 (4.8%); P = 0.017], on insulin (P = 0.04) or on antidepressants (P = 0.01). Advanced age was found to be an independent predictor of avoidable early readmission (OR 2.99 95%CI 1.34–6.62, P = 0.007), and admission to a general ward (as compared to those admitted in a private ward) was an independent predictor of early readmissions (OR 2.99 95%CI 1.34–6.62, P = 0.007).
Conclusion:
The 30-day readmission rate in a geriatric unit in a tertiary care hospital was 5.2%. Advanced age was considered to be an independent predictor of avoidable early readmission. Future prospective research on avoidable readmissions should be undertaken to delineate factors affecting 30-day avoidable hospital readmissions in developing nations.
Keywords: Avoidability, elderly, geriatrics, older adults, preventability, readmission
Introduction
Readmission shortly after discharge burdens a patient both economically and psychologically.[1] It serves as an indicator of healthcare quality and a guide for resource allocation.[2,3] To prevent deleterious health outcomes, primary care, and family physicians must improve post-discharge care.[4] Factors associated with readmission include improper discharge planning; failure to send the discharge plan to the primary care physician; poor follow-up practices, especially with primary care physicians; lack of social and community support; unclear instructions to patients on discharge; incomplete diagnosis; inadequately treated medical conditions; sub-optimal patient care; errors in medication reconciliation; drug interactions and side effects; frailty; malnutrition; severe chronic conditions; the persistence of underlying chronic conditions; lapses in communication between treating team members and the patient; poor management of self-care activities at home following discharge; inability in accessing health care and keeping appointments; incomplete patient education resulting in lack of awareness of whom to contact; where to go and how to manage symptoms at home; nosocomial infections; and poor adherence to medications due to cost or inaccessibility.[5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21] Contributory intrinsic factors include old age, high comorbidity burden, low literacy rate, low socio-economic status, and lack of social networks.[9,10,22,23,24] Patients discharged against medical advice are at a higher risk for early readmissions, usually within the first day following discharge (bounce-back readmissions).[25] Most research done on 30-day readmissions focus on the community model-a flow of patients between the community and the hospital. Only a segment of the population is considered in this model, and it fails to look at frail older adults in home-care settings and residential long-term care facilities whose care poses challenges to the health care system.[2] As liaisons between the various healthcare practitioners involved in patient care, primary care physicians can play a vital role in post-discharge care and reduce hospital readmissions by providing continuing care.[26,27]
According to the Hospital Readmission Reduction Program (HRRP) of the Patient Protection and Affordable Act (2010, US), readmission is defined as “admission to an acute care hospital within 30 days of discharge from the same or another acute care hospital”. HRRP excluded confounding factors like discharge against medical advice and admission for primary psychiatric diagnosis, rehabilitation, or chemotherapy. Readmission may not necessarily be linked to the cause for index hospitalization. Thirty-day readmission reflects the quality of care rendered by the health care system as it takes into account the discharge planning process and immediate follow-up care. Beyond this 30-day period, readmissions are often linked to out-patient care and individual health care choices like lifestyle measures, compliance to medications, habits, and psychosocial factors.[1]
Our study was designed to estimate the proportion of readmissions occurring in a tertiary care centre in South India and to delineate predictors of avoidable readmissions in older adults.
Materials and Methods
Study design, setting, period and population
We undertook a retrospective electronic chart audit of 5239 patients admitted to a premier tertiary care teaching hospital under Geriatrics from May 2015 to May 2020. Although this hospital caters to patients from all over India, we chose patients from Tamil Nadu and the neighbouring states of Andhra Pradesh and Kerala. The number of admissions in geriatric wards from these states (2698) was considered as a denominator for calculating the readmission rate [Figure 1]. Inpatients who were unplanned readmissions to the geriatric wards within the 30-day duration were analyzed to highlight the factors predicting avoidable readmissions in older patients, and to characterize the factors determining early and late readmissions.
Figure 1.
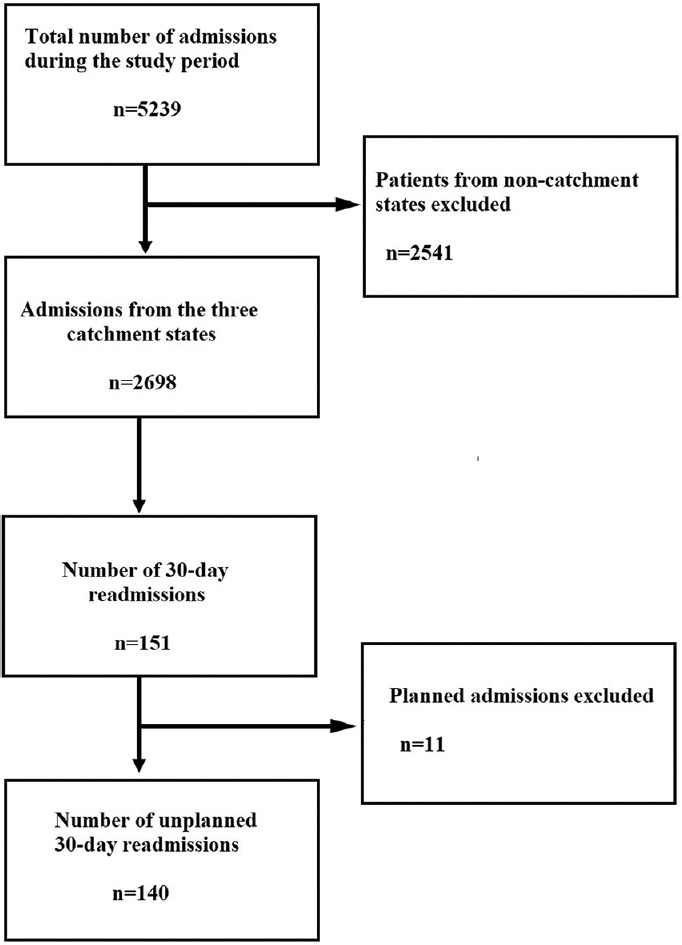
Flow diagram
Older adults of the age sixty years and above from Tamil Nadu, Andhra Pradesh, and Kerala, who had unplanned readmission to the geriatric wards within 30-days from discharge were included. Patients below sixty years of age, admitted from outside the catchment states, those who had planned readmissions, patients who got readmitted after 30 days, patients with an end-stage renal disease requiring dialysis, and those who required elective surgeries planned during the index admission were not included into the study.
The data was extracted from the electronic database of the hospital and reviewed to determine the primary reason for the 30-day readmission, based on a model used by Graham and colleagues[28]-an algorithm based on causality and preventability of readmissions. The charts of 140 patients were audited in detail by two blinded consultant geriatricians, and discrepancies among these two assessments were resolved by a final assessment by a third geriatrician. These consultants were not privy to the identity of these patients. Causality and preventability (avoidability) were measured on a 1–6 Likert scale, and ³4/6 on both scales were classified as avoidable readmissions. Diseases were classified based on the International Classification of Diseases-10 (ICD-10), and comorbidity burden was assessed using the Modified Charlson Comorbidity Index (CCI). Adverse drug reactions (ADRs), underuse of evidence-based treatment, and avoidable readmissions were measured using the Naranjo score, the Hallas criteria and clinical judgment by the two geriatricians. Completeness of discharge summary instructions was assessed based on documentation of date for review, health care contact after discharge, investigations that need to be followed up on review, and management of self-care activities at home. Patients readmitted once were those who got readmitted within 30-days from discharge following index admission; those readmitted twice were patients who got readmitted after their first discharge; and those who were readmitted thrice were patients who got readmitted following the second discharge. All these readmissions fell within 30 days of the index readmission. We defined early 30-day readmissions as readmissions occurring within seven days and late 30-day readmission as after seven days from the time of discharge from the index hospitalization.
The primary outcome was the readmission rate. Secondary outcomes included avoidable readmissions among early and late readmissions and predictors of early readmissions. Data collected from index hospitalization and readmissions were demographic variables and medical details.
Ethics approval was obtained from the Research and Ethics committee of the Institutional Review Board (Reference number: IRB Min no. 13214, 2020).
Analysis
In previous studies, readmission rates varied from 0.1% to 11.3%.[29] Assuming an anticipated Odds Ratio (OR) of about 2-times, with 90% power and 5% level of significance with 7.1% being the proportion of 30-day readmission, to show a readmission risk among older adults, the sample size was calculated to be 140.[29] EpiData 2.0 software was used to enter the raw data, and the statistical analysis was compiled by the STATA 16.0 software. A P value < 0.05 was considered statistically significant. Descriptive data were expressed as mean with standard deviation (SD) or median with interquartile range (IQR) for continuous variables and number (%) for categorical variables. Comparison of continuous variables was examined by independent student’s t-test and Mann-Whitney U test. Statistical analysis of categorical variables was performed using the Pearson Chi-square test and Fischer’s exact test. Logistic regression analysis was used to estimate the Odds Ratio with a 95% confidence interval (CI) to evaluate the association between risk factors and 30-day readmission adjusted for sex, age, and comorbidities.
Results
Of the 2698 patients admitted during the study period from the three catchment states, 140 patients (5.18%) had an unplanned readmission, 58 (41.4%) of which were potentially avoidable. Of the 140 patients readmitted, 13 patients (9.3%) were readmitted for the second time, and four patients (2.8%) got readmitted for the third time after discharge. The mean (SD) age was 75.9 years (8.2 years), and the majority were males (60.7%). Most patients (n = 96, 68.6%) were from Tamil Nadu. The comorbidity burden in the study population measured using Charlson Comorbidity Index was high (median: 6, IQR 5–8). The most common comorbidity was Coronary Artery Disease (37.1%), followed by Congestive Cardiac Failure (30.5%). Auditing the discharge medications of the index admission, we found most of the patients were on anti-platelets (64.7%). The most common presenting complaint during the first readmission was shortness of breath (37.2%). Completeness of index admission discharge summary was present only in 46% of the patients. Eighty-two patients (58.5%) were readmitted between 7–30 days. On the univariate analysis of early versus late readmissions, patients with a malignancy were readmitted within seven days of their discharge; [8 (13.5%) vs. 4 (4.8%); P = 0.017]. Early readmissions were also associated with the use of insulin (P = 0.04) and antidepressant medications (P = 0.01) [Table 1].
Table 1.
Baseline characteristics of the study population
| Variables | n (%) n=140 | Early readmission (0-7 days) n=58 | Late readmission (8-30 days) n=82 | P |
|---|---|---|---|---|
| Number of readmissions | ||||
| Readmitted once | 123 (87.9) | 53 (91.4) | 70 (85.4) | 0.63 |
| Readmitted twice | 13 (9.3) | 4 (6.9) | 9 (10.9) | |
| Readmitted thrice | 4 (2.8) | 1 (1.7) | 3 (3.7) | |
| Male | 85 (60.7) | 38 (65.5) | 47 (57.3) | 0.33 |
| Age (years)a | 75.9±8.2 | 74.7±8.3 | 76.7±8.14 | 0.14 |
| Catchment states | ||||
| Tamil Nadu | 96 (68.6) | 36 (62.1) | 60 (73.1) | 0.23 |
| Andhra Pradesh | 13 (9.3) | 5 (8.6) | 8 (9.76) | |
| Kerala | 31 (22.1) | 17 (29.3) | 14 (17) | |
| Charlson comorbidity indexb | 6 (5-8) | 6 (4-7) | 6 (5-8) | 0.27 |
| Co-morbidities | ||||
| CAD | 52 (37.1) | 21 (36.3) | 31 (37.8) | 0.85 |
| CCF | 43 (30.5) | 13 (22.4) | 30 (36.6) | 0.07 |
| CVA | 26 (18.4) | 8 (13.5) | 18 (22) | 0.22 |
| COPD | 42 (29.8) | 16 (27.1) | 26 (31.7) | 0.60 |
| Dementia | 23 (16.3) | 7 (11.8) | 16 (19.5) | 0.24 |
| Diabetes mellitus | 91 (65.0) | 40 (67.7) | 52 (63.4) | 0.27 |
| CLD | 11 (7.9) | 12 (20.6) | 11 (13.4) | 0.25 |
| CKD | 14 (10.0) | 6 (10.1) | 8 (57.) | 0.93 |
| Malignancy† | 12 (8.5) | 8 (13.5) | 4 (4.8) | 0.017 |
| Discharge drugs at index admission | ||||
| Beta blockers | 69 (49.3) | 27 (46.5) | 41 (50.6) | 0.6 |
| Alpha blocker | 37 (26.6) | 20 (34.4) | 17 (20.9) | 0.07 |
| CCB | 43 (30.7) | 20 (34.4) | 22 (27.1) | 0.51 |
| ACEi/ARBs | 54 (38.8) | 24 (41.3) | 30 (37.0) | 0.6 |
| Diuretics | 46 (33) | 22 (37.9) | 24 (29.6) | 0.3 |
| Beta agonists | 39 (28.2) | 20 (34.4) | 19 (23.7) | 0.16 |
| Antimicrobial agents | 50 (35.9) | 21 (36.2) | 29 (35.8) | 0.9 |
| Antiplatelet therapy | 90 (64.7) | 39 (67.2) | 51 (62.9) | 0.27 |
| Oral ant diabetic agents | 53 (37.9) | 23 (39.6) | 29 (35.8) | 0.21 |
| Insulin therapy | 21 (15.1) | 13 (22.4) | 8 (9.8) | 0.04 |
| Antidepressant agents | 12 (8.7) | 9 (15.5) | 3 (3.7) | 0.01 |
| Chief complaint at readmission | ||||
| Dyspnea (NYHA II-IV) | 51 (37.2) | 23 (41.8) | 28 (34.1) | 0.36 |
| Cough | 44 (31.2) | 15 (25.4) | 29 (35.3) | 0.20 |
| Fever | 40 (28.6) | 17 (28.8) | 24 (29.3) | 0.95 |
| Altered sensorium | 21 (14.8) | 5 (8.5) | 16 (19.5) | 0.06 |
| Others | 91 (64.3) | 39 (66.1) | 82 (63.4) | - |
| Completeness of discharge summary | 64 (46.0) | 25 (43.1) | 39 (48.1) | 0.5 |
aMean (Standard deviation), bMedian (Interquartile range), CAD - Coronary artery disease, CCF - Congestive cardiac failure, CVA - Cerebrovascular accident, COPD - Chronic Obstructive Pulmonary Disease, CLD - Chronic liver disease, CKD - Chronic Kidney Disease, CCB - calcium channel blockers ACE/ARBs - angiotensin-converting enzyme inhibitor or Angiotensin receptor blockers, NYHA class - New York Heart Association class for Dyspnea. †Malignancy including hematological
The reason for readmission in more than half of the study population was due to exacerbation, reactivation, or progression of previously existing disease (total readmissions: 55.7%, avoidable readmission: 63.8%), followed by an emergence of a new disease unrelated to the index admission (total readmissions: 43.2%, avoidable readmissions- 24.3%). The median length of stay for both index hospitalization and first readmission was eight-days, and the median duration between hospital admission and first readmission was ten-days. The median cost of care for an avoidable readmission was 44,000 INR (IQR: 22,000–73,000 INR) [Table 2].
Table 2.
Proportion and predictors of avoidable readmissions among early and late readmissions, and univariable analysis
| Total readmissions n (%) | Avoidable readmission | ||||
|---|---|---|---|---|---|
|
| |||||
| n (%) n=58 | Early readmission (0-7 days) n=17 | Late readmission (8-30 days) n=41 | P | ||
| Dead, n (%) | 9 (15.5) | 4 (25.5) | 5 (12.2) | 0.43 | |
| Reason for re-admission | |||||
| Reason for readmission as a result of adverse reaction to patient’s ongoing medications | 5 (3.5) | 3 (5.2) | 1 (5.8) | 2 (4.9) | 0.66 |
| Reason for readmission as a result of an adverse effect of a new drug introduced during the index admission | 17 (12) | 8 (13.8) | 1 (5.9) | 7 (17.1) | 0.249 |
| Exacerbation or reactivation or progression of previously existing condition as one of reasons for readmission | 78 (55.3) | 37 (63.8) | 11 (64.7) | 26 (63.4) | 0.59 |
| New disease as the reason for readmission | 60 (43.2) | 22 (37.9) | 8 (47.1) | 14 (34.2) | 0.26 |
| Length of hospital stay, the duration between hospital admissions, and cost of hospital readmissions | |||||
| Length of stay admission during the index admissionb | 8 (6-12) | 10 (6-13) | 8 (5-12) | 10 (7-14) | 0.16* |
| Duration of days between discharge date of primary admission and readmissionb | 10 (5-18) | 13 (6-21) | 4 (3-6) | 16 (12-22) | <0.01* |
| Length of stay during readmissionb | 8 (5-13) | 7 (5-11) | 6 (5-9) | 8 (6-12) | 0.39* |
| Cost of care during readmission (×104 in Rupees)b | 5 (2.5-11.1) | 4.4 (2.2-7.3) | 4.9 (3.4-6.6) | 4.4 (2.1-9.8) | 0.73* |
| Completeness of discharge summary | 65 (46.43) | 23 (37.29) | 11 (39.29) | 11 (35.48) | 0.763 |
*Two-sample Wilcoxon rank-sum (Mann-Whitney) test for comparison of variables among avoidable and non-avoidable readmission. aMean (Standard deviation), bMedian (Interquartile range)
On multivariable analysis, advanced age was found to be independent predictors of avoidable early readmission (OR 1.11 95% CI 1.02–1.22, P = 0.017) [Table 3] and admission to the general ward was associated with early readmissions (OR 2.99 95% CI 1.34–6.62, P = 0.007) [Table 4].
Table 3.
Multivariable model of predictors of potentially avoidable readmissions of early and late readmissions
| Variable | Early readmission | Late readmission | ||
|---|---|---|---|---|
|
|
|
|||
| Odds ratio (95% CI) | P | Odds ratio (95% CI) | P | |
| Age | 1.11 (1.02-1.22) | 0.017 | 1.06 (0.99-1.14) | 0.072 |
| GW patients | 1.16 (0.26-5.15) | 0.841 | 0.63 (0.22-1.82) | 0.389 |
| Delirium | 0.42 (0.06-8.52) | 0.465 | 0.99 (0.29-3.33) | 0.998 |
| CCF | 3.39 (0.67-17.04) | 0.139 | 2.48 (0.91-6.78) | 0.077 |
| Alpha-blockers | 6.28 (0.87-45.22) | 0.068 | 0.65 (0.20-2.11) | 0.476 |
| Beta agonist | 1.88 (0.35-10.23) | 0.464 | 1.16 (0.37-3.64) | 0.797 |
| Antidepressants | 0.45 (0.05-4.02) | 0.472 | 1.55 (0.27-9.05) | 0.624 |
| Insulin use | 2.14 (0.29-15.39) | 0.448 | 1.45 (0.32-6.59) | 0.626 |
CI – Confidence interval, GW – General ward, CCF – Congestive cardiac failure, GW – General ward, Anti-PD – Anti-Parkinson’s disease drugs
Table 4.
Multivariable analysis of predictors of early readmission
| Variable | Early readmission | |
|---|---|---|
|
| ||
| Odds ratio (95% CI) | P | |
| Age | 0.96 (0.91-1.01) | 0.167 |
| GW patients | 2.99 (1.34-6.62) | 0.007 |
| CCF | 0.51 (0.22-1.18) | 0.119 |
| Delirium | 2.53 (0.78-8.21) | 0.121 |
| Alpha-blockers | 1.10 (0.44-2.70) | 0.835 |
| Antidepressants | 0.97 (0.26-3.58) | 0.967 |
| Anti-PD drugs | 1.48 (0.25-8.73) | 0.660 |
| AChEi | 0.61 (0.68-54.5) | 0.105 |
| Insulin use | 0.53 (0.18-1.50) | 0.234 |
CI – confidence interval, GW – general ward, CCF – Congestive cardiac failure, Anti-PD drugs – Parkinson’s disease drugs, AChEi – Acetyl cholinesterase inhibitor
The reason for readmission for the second time (10.8%) included aspiration pneumonia, candidemia, chronic obstructive pulmonary disease exacerbation, septicemia, Non-ST elevation myocardial infarction and heart failure, thalamic stroke, H1N1 pneumonia, and hepatic encephalopathy.
Discussion
Unplanned hospital readmissions often weigh down health care resources and cause unanticipated health care expenses for patients and their families. It serves as an indicator of health care quality and integrity of transitional care.[16,30] We reviewed 2698 charts and found that the unplanned 30-day readmission rate was 5.18% with a mean (SD) age of 75.9 years (8.2 years). In a Swedish study conducted among adults aged over 65 years admitted in medical and surgical specialties, readmission rate was 18%. The mean 30-day readmission rate was 12.9% in a retrospective study done in Texas among patients visiting primary health care physicians.[10,31] Another study found the odds of readmission reduced by 56% when discharge plans were sent to primary care physicians.[18] Therefore, primary care and family physicians play a vital role in improving transition care resulting in reduced hospital readmissions,[26,32] and their turnover can affect readmission rates.[33] We conducted the first study analyzing avoidable readmissions among older adults in India.
It is difficult to ascertain whether a higher readmission rate could be attributed to easy accessibility to a health care facility, variations in the care provided, or multiple comorbid conditions of patients.[10]
Older adults from rural areas of India have poor access to quality health care services and rely on prevalent unproven home remedies or native medications.[34] Although females have higher life expectancy,[35] we found a lower readmission rate among them as 60.9% who got readmitted were males. Older adults, especially females, are often limited to home care even for life-threatening conditions due to financial constraints.[36,37,38,39]
As observed in previous studies, 30-day readmissions had a higher comorbidity burden (mean Charlson comorbidity index 6, IQR 5–8), possibly due to the pathological changes and physiological processes associated with aging, such as declining functional reserves.[10,40,41] Although malignancy (metastatic malignancies, lymphoma, leukemia) was associated with early readmissions [8 (13.5%) vs. 4 (4.8%), P = 0.017], data from previously published studies show that early readmission rates were low (2%) compared to late readmissions in patients admitted for cancer treatment.[42] Since data on early and late readmissions in oncology and hematology are limited, especially among older adults, research in this area is imperative.
Previous studies show that medications like corticosteroids, antimicrobial agents, and anti-diabetic agents (mainly insulin) along with polypharmacy are associated with 30-day readmission.[43,44,45] In one of the few studies done on patients taking anti-depressants, readmission rate was found to be lower.[46] In our study, early readmissions were associated with the use of anti-depressant medications [9 (15.5%) vs. 3 (3.7%), P = 0.01] and insulin therapy [13 (22.4%) vs. 8 (9.8%), P = 0.04].
Of the 140 readmissions, 58 (41.4%) were labelled as avoidable readmissions by two blinded geriatricians auditing the electronic charts. Any discrepancy was resolved by a third geriatrician, and the decision was considered final. A systematic review found that the median proportion of readmissions termed “avoidable” based on a single reviewer was 27.1%, with a wide confidence interval (5 to 79%). Another survey calculated the avoidable readmission rate to be 26.9% based on two-physician reviews. Data on the avoidable 30-day readmission rate in older adults in India is lacking, and the true proportion of avoidable readmissions is inconclusive due to the complex factors interlinked with readmissions, such as post-discharge care, caregiver burden, and socio-economic factors. Indicators of potentially avoidable readmissions include decision-making in the emergency department, failure to convey vital information to the out-patient healthcare professional, premature discharge, and failure to establish care goals in patients with serious illnesses.[3,28]
According to a retrospective study, the rate of preventable early readmission was higher than late readmission, with different risk factors associated with each. Early readmissions were related to an acute illness burden, duration of index hospitalization, and assessment by a rapid response team during the index admission. Late readmissions were associated with chronic illness burden, social determinants of health, and health education.[47]
In an observational study, two chronic diagnoses (heart failure, chronic obstructive pulmonary disease), and three acute diagnoses (acute coronary syndrome, community-acquired lower respiratory tract infection, gastrointestinal bleed) were associated with a drop of readmission rate from 16.5% to 13.8% with a decrease in the length of stay from 5.44 days to 3.98 days (2% annually).[48] In our study, the median duration of hospital stay during the index admission was eight days (IQR 6–12 days), and the median duration between discharge from the index admission and first readmission was ten days (IQR 5–18 days). Late readmissions constituted 58.5% of total readmissions, consistent with the trend reported in India.[29] The financial impact of readmission was gigantic. The median amount patients spent was 44,000 Indian Rupees (IQR 22,000–73,000 INR), equivalent to approximately 602 US Dollars (1 USD = 73.01 INR, as of 1 September, 2021), for medical care during avoidable readmission. This is the first study in India showing the economic burden associated with avoidable hospital readmission.
The most common cause for readmission was exacerbation, reactivation, or progression of a previously existing disease (55.3%), followed by an emergence of a new disease unrelated to the index admission (43.5%). In India, ‘admission per the decision of the treating doctor’ was the most common reason given for 30-day readmission in general medicine (16.8%).[29] In this retrospective study, data on social care, family environment, treatment adherence, and documentation of care plans were not uniformly available for analysis. Discharge summaries of index admissions showed that only 46% had clear instructions for review, patient care at home, and follow-up investigations and out-patient visits. This figure was higher than that reported in Medicare claims, indicating that only half of the patients discharged had an appointment for the first follow-up out-patient visit.[40]
As compared to a previous study, we found that advanced age was an independent predictor of early potentially avoidable 30-day readmission (OR 1.11, 95% CI 1.02–1.22, P = 0.017).[23] This may be due to bed availability, health insurance coverage, or affordability [Table 3].
In a meta-analysis, increasing the number of team-based healthcare delivery and encouraging self-care were found to be more effective than other strategies in reducing the 30-day readmission rate. Other discharge interventions included proper discharge planning, case management, follow-up via telephone, telemonitoring, health education, medication reconciliation, home visits, scheduled out-patient follow-ups, patient-tailored discharge instructions, rehabilitative interventions aimed at improving functional status, streamlining of services provided, caregiver education, and peer mentoring.[49] A recent meta-analysis in older adults with comorbidities showed that short-term (less than three months) readmissions can be reduced by continuity of care. A recent retrospective study showed that the Hospital Elder Life Program (HELP) used to reduce in-patient delirium can reduce the length of stay during readmission and economic burden among older adults above seventy years of age. Implementing Sub-Acute care for Frail Elderly (SAFE) units following discharge from acute care was not associated with a reduction in the 30-day readmission rate, but the duration of hospital stay was reduced to less than one day in 75% patients.[27] A more recent meta-analysis of 19 trials from seven countries showed that communicating about the disease with the patient and counselling on medications reduced 30-day readmissions.[5]
This study was done in a tertiary care center that caters to the middle- and affluent classes of society. Most patients (31.3%) came from far-flung places, were not well represented in the readmission analysis, and could have received medical attention from primary care or family physicians upon return to their own homes.
Conclusion
The 30-day readmission rate in a geriatric unit at a tertiary care center was 5.18%. Advanced age was an independent predictor of early potentially avoidable 30-day readmission, and admission to the general ward was an independent predictor of early readmission.
Key points
The 30-day readmission rate in a geriatric unit at a tertiary care hospital was 5.18%.
Advanced age was an independent predictor of early potentially avoidable 30-day readmission among older adults.
The odds of early readmission were higher among patients admitted to general wards compared to patients admitted in private wards.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We thank the nursing staff and other hospital workers who contributed to patient care during the course of the patients’ stay.
References
- 1.Allaudeen N, Vidyarthi A, Maselli J, Auerbach A. Redefining readmission risk factors for general medicine patients. J Hosp Med. 2011;6:54–60. doi: 10.1002/jhm.805. [DOI] [PubMed] [Google Scholar]
- 2.Gruneir A, Fung K, Fischer HD, Bronskill SE, Panjwani D, Bell CM, et al. Care setting and 30-day hospital readmissions among older adults: A population-based cohort study. CMAJ. 2018;190:E1124–33. doi: 10.1503/cmaj.180290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: A systematic review. CMAJ. 2011;183:E391–402. doi: 10.1503/cmaj.101860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Saluja S, Hochman M, Bourgoin A, Maxwell J. Primary care: The new frontier for reducing readmissions. J Gen Intern Med. 2019;34:2894–7. doi: 10.1007/s11606-019-05428-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Becker C, Zumbrunn S, Beck K, Vincent A, Loretz N, Müller J, et al. Interventions to improve communication at hospital discharge and rates of readmission: A systematic review and meta-analysis. JAMA Netw Open. 2021;4:e2119346. doi: 10.1001/jamanetworkopen.2021.19346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ghosh A, Sharma N, Noble D, Basu D, Mattoo SK, Bn S, Pillai RR. Predictors of five-year readmission to an inpatient service among patients with alcohol use disorders: Report from a low-middle income country. Subst Use Misuse. 2022;57:123–33. doi: 10.1080/10826084.2021.1990341. [DOI] [PubMed] [Google Scholar]
- 7.Cheon O, Baek J, Kash BA, Jones SL. An exploration of community partnerships, safety-net hospitals, and readmission rates. Health Serv Res. 2020;55:531–40. doi: 10.1111/1475-6773.13287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Coppa K, Kim EJ, Oppenheim MI, Bock KR, Conigliaro J, Hirsch JS. Examination of post-discharge follow-up appointment status and 30-day readmission. J Gen Intern Med. 2021;36:1214–21. doi: 10.1007/s11606-020-06569-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fatima S, Shamim S, Riffat S, Tariq M. Hospital readmissions in internal medicine specialty: Frequency, associated factors and outcomes. Pak J Med Sci. 2021;37:2008–13. doi: 10.12669/pjms.37.7.3575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Glans M, Kragh Ekstam A, Jakobsson U, Bondesson Å, Midlöv P. Risk factors for hospital readmission in older adults within 30 days of discharge –A comparative retrospective study. BMC Geriatr. 2020;20:467. doi: 10.1186/s12877-020-01867-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Herledan C, Baudouin A, Larbre V, Gahbiche A, Dufay E, Alquier I, et al. Clinical and economic impact of medication reconciliation in cancer patients: A systematic review. Support Care Cancer. 2020;28:3557–69. doi: 10.1007/s00520-020-05400-5. [DOI] [PubMed] [Google Scholar]
- 12.Huang H-H, Chang JC-Y, Tseng C-C, Yang YJ, Fan JS, Chen YC, et al. Comprehensive geriatric assessment in the emergency department for the prediction of readmission among older patients: A 3-month follow-up study. Arch Gerontol Geriatr. 2021;92:104255. doi: 10.1016/j.archger.2020.104255. doi: 10.1016/j.archger.2020.104255. [DOI] [PubMed] [Google Scholar]
- 13.Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: Implications for patient safety and continuity of care. JAMA. 2007;297:831–41. doi: 10.1001/jama.297.8.831. [DOI] [PubMed] [Google Scholar]
- 14.Lewis P, Braddock K, Tolaymat L, Haga C, Gillis M, Yin M, et al. Discharge summary completion timeliness and the association of 30-day readmission. South Med J. 2021;114:319–21. doi: 10.14423/SMJ.0000000000001243. [DOI] [PubMed] [Google Scholar]
- 15.Morkisch N, Upegui-Arango LD, Cardona MI, van den Heuvel D, Rimmele M, Sieber CC. Components of the transitional care model (TCM) to reduce readmission in geriatric patients: A systematic review. BMC Geriatr. 2020;20:345. doi: 10.1186/s12877-020-01747-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pereira F, Verloo H, Zhivko T, Di Giovanni S, Meyer-Massetti C, von Gunten A, et al. Risk of 30-day hospital readmission associated with medical conditions and drug regimens of polymedicated, older inpatients discharged home: A registry-based cohort study. BMJ Open. 2021;11:e052755. doi: 10.1136/bmjopen-2021-052755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wang A, Pridham KF, Nisenbaum R, Pedersen C, Brown R, Hwang SW. Factors associated with readmission among general internal medicine patients experiencing homelessness. J Gen Intern Med. 2021;36:1944–50. doi: 10.1007/s11606-020-06483-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mansukhani RP, Bridgeman MB, Candelario D, Eckert LJ. Exploring Transitional Care: Evidence-Based Strategies for Improving Provider Communication and Reducing Readmissions. Pharm Ther. 2015;40:690–4. [PMC free article] [PubMed] [Google Scholar]
- 19.Matthews C, Shankar B, Marshall S, Pearcy J, Somani A, Agarwal E. Prevalence of malnutrition and poor food intake and their association with health-related outcomes in older adults in Indian hospitals. Nutr Diet. 2021;78:135–44. doi: 10.1111/1747-0080.12641. [DOI] [PubMed] [Google Scholar]
- 20.Bailey SC, Fang G, Annis IE, O'Conor R, Paasche-Orlow MK, Wolf MS. Health literacy and 30-day hospital readmission after acute myocardial infarction. BMJ Open. 2015;5:e006975. doi: 10.1136/bmjopen-2014-006975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Baker DW, Gazmararian JA, Williams MV, Scott T, Parker RM, Green D, et al. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am J Public Health. 2002;92:1278–83. doi: 10.2105/ajph.92.8.1278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hoyer EH, Golden B, Dougherty G, Richardson M, Lepley D, Leung C, et al. The paradox of readmission prevention interventions: Missing those most in need. Am J Med. 2021;134:1142–7. doi: 10.1016/j.amjmed.2021.04.006. [DOI] [PubMed] [Google Scholar]
- 23.Sterling MR, Ringel JB, Pinheiro LC, Safford MM, Levitan EB, Phillips E, et al. Social determinants of health and 90-day mortality after hospitalization for heart failure in the REGARDS study. J Am Heart Assoc. 2020;9:e014836. doi: 10.1161/JAHA.119.014836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dorajoo SR, See V, Chan CT, Tan JZ, Tan DS, Abdul Razak SM, et al. Identifying potentially avoidable readmissions: A medication-based 15-day readmission risk stratification algorithm. Pharmacotherapy. 2017;37:268–77. doi: 10.1002/phar.1896. [DOI] [PubMed] [Google Scholar]
- 25.Nall RW, Herndon BB, Mramba LK, Vogel-Anderson K, Hagen MG. An interprofessional primary care-based transition of care clinic to reduce hospital readmission. Am J Med. 2020;133:e260–8. doi: 10.1016/j.amjmed.2019.10.040. [DOI] [PubMed] [Google Scholar]
- 26.Robert B, Sun AH, Sinden D, Spruin S, Hsu AT. A case-control study of the sub-acute care for frail elderly (SAFE) unit on hospital readmission, emergency department visits and continuity of post-discharge care. J Am Med Dir Assoc. 2021;22:544–50.e2. doi: 10.1016/j.jamda.2020.07.020. [DOI] [PubMed] [Google Scholar]
- 27.Auerbach AD, Kripalani S, Vasilevskis EE, Sehgal N, Lindenauer PK, Metlay JP, et al. Preventability and causes of readmissions in a national cohort of general medicine patients. JAMA Intern Med. 2016;176:484–93. doi: 10.1001/jamainternmed.2015.7863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Thomas JW, Holloway JJ. Investigating early readmission as an indicator for quality of care studies. Med Care. 1991;29:377–94. doi: 10.1097/00005650-199104000-00006. [DOI] [PubMed] [Google Scholar]
- 29.Singh S, Goodwin JS, Zhou J, Kuo YF, Nattinger AB. Variation among primary care physicians in 30-day readmissions. Ann Intern Med. 2019;170:749–55. doi: 10.7326/M18-2526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Arsenault-Lapierre G, Kremer B, Sourial N, Gagnon J, Ladores M, Vedel I. Impact of a family medicine-based transitional care intervention on readmission and length of stay: A pilot study. McGill J Med. 2020;18 doi: 10.26443/mjm.v18i1.147. [Google Scholar]
- 31.Tang N, Maselli JH, Gonzales R. Variations in 30-day hospital readmission rates across primary care clinics within a tertiary referral center. J Hosp Med. 2014;9:688–94. doi: 10.1002/jhm.2243. [DOI] [PubMed] [Google Scholar]
- 32.Sharma E, Dubey A, Malhotra S, Manocha S, Handu S. Use of complementary and alternative medicines in Indian elderly patients. Natl J Physiol Pharm Pharmacol. 2017;7:929–34. [Google Scholar]
- 33.Life expectancy at birth, total (years)-India. Data. [Last accessed on 2021 Jul 01]. Available from: https://data.worldbank.org/indicator/SP. DYN. LE00. IN?locations=IN .
- 34.Kalavar JM, Jamuna D. Aging of Indian women in India: The experience of older women in formal care homes. J Women Aging. 2011;23:203–15. doi: 10.1080/08952841.2011.587730. [DOI] [PubMed] [Google Scholar]
- 35.Kulcsár LJ, Curtis KJ. Why Does Rural Demography Still Matter? In: Kulcsár LJ, Curtis KJ, editors. Int Handb Rural Demogr [Internet] Dordrecht: Springer Netherlands; 2012. [Last accessed on 2022 Apr 07]. pp. 1–6. Available from: https://doi.org/10.1007/978-94-007-1842-5_1. [Google Scholar]
- 36.Kasthuri A. Challenges to healthcare in India-The five A's. Indian J Community Med. 2018;43:141–3. doi: 10.4103/ijcm.IJCM_194_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Mudge AM, Kasper K, Clair A, Redfern H, Bell JJ, Barras MA, et al. Recurrent readmissions in medical patients: a prospective study. J Hosp Med. 2011;6:61–7. doi: 10.1002/jhm.811. [DOI] [PubMed] [Google Scholar]
- 38.Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the medicare fee-for-service program. N Engl J Med. 2009;360:1418–28. doi: 10.1056/NEJMsa0803563. [DOI] [PubMed] [Google Scholar]
- 39.Pedersen MK, Meyer G, Uhrenfeldt L. Risk factors for acute care hospital readmission in older persons in Western countries: A systematic review. JBI Database Syst Rev Implement Rep. 2017;15:454–85. doi: 10.11124/JBISRIR-2016-003267. [DOI] [PubMed] [Google Scholar]
- 40.Brown EG, Burgess D, Li C-S, Canter RJ, Bold RJ. Hospital readmissions: Necessary evil or preventable target for quality improvement. Ann Surg. 2014;260:583–91. doi: 10.1097/SLA.0000000000000923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. Adverse drug events occurring following hospital discharge. J Gen Intern Med. 2005;20:317–23. doi: 10.1111/j.1525-1497.2005.30390.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Budnitz DS, Shehab N, Kegler SR, Richards CL. Medication use leading to emergency department visits for adverse drug events in older adults. Ann Intern Med. 2007;147:755–65. doi: 10.7326/0003-4819-147-11-200712040-00006. [DOI] [PubMed] [Google Scholar]
- 43.Allaudeen N, Vidyarthi A, Maselli J, Auerbach A. Redefining readmission risk factors for general medicine patients. J Hosp Med. 2011;6:54–60. doi: 10.1002/jhm.805. [DOI] [PubMed] [Google Scholar]
- 44.Warnke I, Nordt C, Moock J, Kawohl W, Rössler W. Antidepressants: Relationship to the time to psychiatric readmission and probability of being in hospital in depressive patients. Front Public Health. 2014;2:40. doi: 10.3389/fpubh.2014.00040. doi: 10.3389/fpubh.2014.00040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Graham KL, Dike O, Doctoroff L, Jupiter M, Vanka A, Davis RB, et al. Preventability of early vs. late readmissions in an academic medical center. PLoS One. 2017;12:e0178718. doi: 10.1371/journal.pone.0178718. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5473551/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Kaboli PJ, Go JT, Hockenberry J, Glasgow JM, Johnson SR, Rosenthal GE, et al. Associations between reduced hospital length of stay and 30-day readmission rate and mortality: 14-year experience in 129 Veterans Affairs hospitals. Ann Intern Med. 2012;157:837–45. doi: 10.7326/0003-4819-157-12-201212180-00003. [DOI] [PubMed] [Google Scholar]
- 47.Leppin AL, Gionfriddo MR, Kessler M, Brito JP, Mair FS, Gallacher K, et al. Preventing 30-day hospital readmissions: A systematic review and meta-analysis of randomized trials. JAMA Intern Med. 2014;174:1095–107. doi: 10.1001/jamainternmed.2014.1608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Facchinetti G, D'Angelo D, Piredda M, Petitti T, Matarese M, Oliveti A, et al. Continuity of care interventions for preventing hospital readmission of older people with chronic diseases: A meta-analysis. Int J Nurs Stud. 2020;101:103396. doi: 10.1016/j.ijnurstu.2019.103396. doi: 10.1016/j.ijnurstu.2019.103396. [DOI] [PubMed] [Google Scholar]
- 49.Zachary W, Kirupananthan A, Cotter S, Barbara GH, Cooke RC, 3rd, Sipho M. The impact of hospital elder life program interventions, on 30-day readmission rates of older hospitalized patients. Arch Gerontol Geriatr. 2020;86:103963. doi: 10.1016/j.archger.2019.103963. doi: 10.1016/j.archger.2019.103963. [DOI] [PubMed] [Google Scholar]