

Abstract
Torsion of the fallopian tube during early pregnancy is a very rare phenomenon. Most of them present with acute abdominal pain and are often misdiagnosed with a twisted ovarian cyst, ectopic pregnancy, appendicitis, etc. A 19-year-old female was referred to the medical department for pain abdomen, nausea, and vomiting. Her last menstrual period was 28 days back. The urine pregnancy test was negative. Ultrasonogram (USG) was suggestive of encapsulated exophytic hemorrhagic cyst in the right adnexa arising from the right ovary. A huge right-twisted fimbrial cyst with hemorrhagic contents (14 cm × 12 cm) along with a gangrenous right ovary was evident in emergency laparotomy. Right salpingo-oophorectomy was performed. She was discharged with an uneventful postoperative recovery. She presented again after 2 months with postoperative amenorrhea, nausea, and vomiting. USG suggested 12 weeks of pregnancy, which continued until term. Eventually, a lower segment cesarean section was done for fetal distress. A twisted fallopian tube during pregnancy is a rare phenomenon. A high index of suspicion necessitates prompt diagnosis and prevention of future fertility and obstetric morbidity.
Keywords: Fimbrial cyst, gangrenous ovary, hemorrhagic, laparotomy, ovarian cyst, salpingo-oophorectomy, torsion of fallopian tube
Introduction
Torsion of the fallopian tube is a rare phenomenon and uncommon cause of acute abdominal pain.[1,2] Most frequently it occurs in the reproductive age group. The entity was first described by Bland-Sutton and has a prevalence of one in 1.5 million women.[3] It usually presents as acute abdominal pain, nausea, and vomiting.[4,5] Presentation and clinical findings mimic those of appendicitis, ovarian torsion, or renal colic. The torsion of the fallopian tube and a para-ovarian cyst is an unusual event. It is also rare in pregnancy. Laboratory parameters are nonspecific and often difficult to diagnose radiographically. This causes a delay in diagnosis resulting in advanced necrosis where the tube cannot be salvaged. The final diagnosis and the treatment approach in most cases are determined only during the surgical intervention. Hence laparotomy should not be delayed. Here, we present a case of fallopian tube torsion with hypertrophic gangrenous ovary and ongoing pregnancy.
Case Report
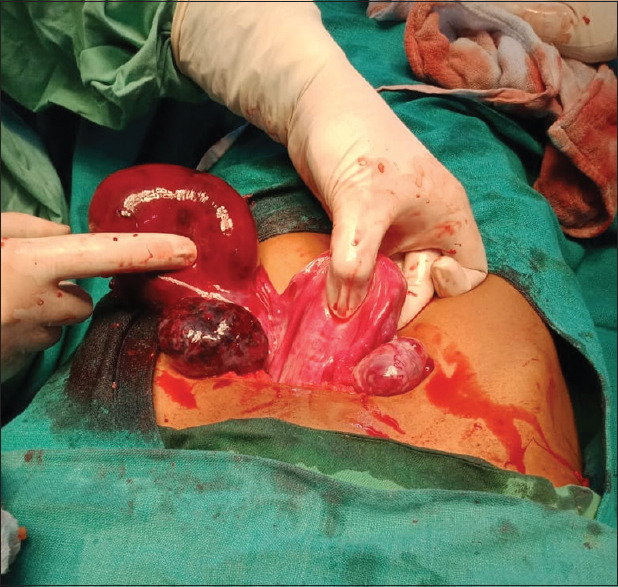
A 19-year-old female was referred to the medical department of our hospital with acute abdominal pain, nausea, and vomiting. The patient was married for one year with no living issues and regular menstrual cycles. Her last menstrual period was 28 days back. On examination her vitals were stable. Per abdominal examination revealed tenderness in the right iliac fossa with guarding and rigidity. Per vaginal examination revealed a mass present in the right fornix with severe tenderness. The urine pregnancy test was negative. Hb was 10 gm%. The blood group was A positive. The liver function test and kidney function test were within normal limits. Ultrasonogram (USG) suggested a well-encapsulated exophytic hemorrhagic cyst in the right adnexa arising from the right ovary with minimum free fluid in the pouch of Douglas [Figure 1]. She underwent an emergency laparotomy. Intraoperative, there was a huge fimbrial cyst of size (14 × 12 cm) with a gangrenous ovary on the right side [Figures 2 and 3]. The left side mesosalpinx was unusually longer than normal. Salpingo-oophorectomy was done and postoperative was uneventful. The histopathological report showed hemorrhagic fimbrial cystic structure and necrosed ovarian cortical tissue. Two months later she again presented with postoperative amenorrhea, nausea, and excessive vomiting. USG suggested 12 weeks of viable pregnancy which continued till term. She was delivered by lower segment cesarean section for fetal distress with abruptio placentae.
Figure 1.
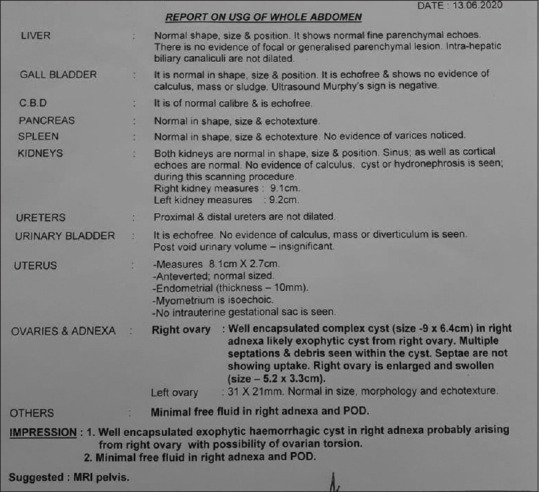
Ultrasound report
Figure 2.

Right-side twisted fimbrial cyst with gangrenous ovary
Figure 3.
Fimbrial cyst after derotation
Discussion
Fimbrial cyst torsion is rare, therefore diagnosis may be delayed. More so because of nonspecific presentation and misdiagnosis by abdominal ultrasound. It presents as acute abdomen with pain, nausea, and vomiting, thus more common diseases like acute appendicitis, ectopic pregnancy, pelvic inflammatory disease, twisted ovarian cyst, and degenerative leiomyoma are considered in the differential diagnosis. Sonography may not show accurately the origin of this lesion and most are diagnosed as ovarian cysts or other types of cystic pelvic masses. We also initially made the diagnosis of a twisted ovarian cyst based on ultrasound and clinical findings. Only when she underwent laparotomy, she was finally diagnosed with a twisted fimbrial cyst involving the ovary which was gangrenous.
The fallopian tube fimbrial cyst torsion is very rare.[6] The exact etiology of fallopian tube torsion is unknown. However, postulated causes could be intrinsic or extrinsic.[1] Intrinsic factors are hydrosalpinx, hematosalpinx, long mesosalpinx tubal neoplasm, and tubal ligation. Extrinsic factors are adnexal venous congestion, adjacent ovarian and para-ovarian masses, gravid uterus, and trauma.[7] In our case torsion occurred probably due to right-side hematosalpinx as the hemorrhagic fimbrial cyst was reported in histopathological examination. The left-side tube was very long and the ovary was normal. Clinical signs and symptoms are nonspecific and it is very difficult to diagnose preoperatively.[8,9,10] The available laboratory investigations and imaging studies cannot confirm fallopian tube torsion but can differentiate it from other etiologies.[11] A high index of suspicion is required to diagnose this uncommon condition which can be confirmed and managed only after laparotomy.[12]
Conclusion
Torsion of the fallopian tube (fimbrial cyst) with early pregnancy is rare. Such a patient presents with an acute abdomen without any specific signs and symptoms similar to ectopic pregnancy. It is very essential to differentiate it from ectopic pregnancy. Ultrasound helps in detecting adnexal mass with torsion or hemorrhage but the final diagnosis is established only after the operation and histopathological report. Early surgical intervention is essential to salvage tube, ovary, future fertility, and prevent obstetric morbidity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Gross M, Blumstein SL, Chow LC. Isolated fallopian tube torsion:A rare twist on a common theme. AJR Am J Roentgenol. 2005;185:1590–2. doi: 10.2214/AJR.04.1646. [DOI] [PubMed] [Google Scholar]
- 2.Cengiz H, Ekin M, Kaya C. Isolated fallopian tube torsion:A rare case. Cumhur Medical J. 2013;35((4/Supplement)):27–30. [Google Scholar]
- 3.Ferrera PC, Kass LE, Verdile VP. Torsion of the fallopian tube. Am J Emerg Med. 1995;13:312–4. doi: 10.1016/0735-6757(95)90208-2. [DOI] [PubMed] [Google Scholar]
- 4.Origoni M, Cavoretto P, Conti E, Ferrari A. Isolated tubal torsion in pregnancy. Eur J Obstet Gynecol Reprod Biol. 2009;146:116–20. doi: 10.1016/j.ejogrb.2009.05.002. [DOI] [PubMed] [Google Scholar]
- 5.Sasaki KJ, Miller CE. Adnexal torsion:Review of the literature. J Minim Invasive Gynecol. 2014;21:196–202. doi: 10.1016/j.jmig.2013.09.010. [DOI] [PubMed] [Google Scholar]
- 6.Bland Sutton J. Remarks on salpingitis and some of its effects. Lancet. 1890;136:1146–8. [Google Scholar]
- 7.Yalcin OT, Hassa H, Zeytinoglu S, Isiksoy S. Isolated torsion of fallopian tube during pregnancy;report of two cases. Eur J Obstet Gynecol Reprod Biol. 1997;74:179–82. doi: 10.1016/s0301-2115(97)00117-6. [DOI] [PubMed] [Google Scholar]
- 8.Kardakis S, Barranca A, Vitelli A, Amore I, Trento F, Caccia G. Isolated fallopian tube torsion. Case Rep Obstet Gynecol. 2013;2013 doi: 10.1155/2013/479698. Article ID 479698, 3 pages. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Comerci G, Colombo FM, Stefanetti M, Grazia G. Isolated fallopian tube torsion:A rare but important event for women of reproductive age. Fertil Steril. 2008;90:1198.e23–5. doi: 10.1016/j.fertnstert.2007.08.057. [DOI] [PubMed] [Google Scholar]
- 10.Hosni W, Schmidt C-M. Isolated fallopian tube torsion:A rare cause of acute abdominal pain. Obstet Gynecol Cases Rev. 2019;6:151. doi.org/10.23937/2377-9004/1410151. [Google Scholar]
- 11.Baracy MG, Jr, Hu J, Ouillette H, Aslam MF. Diagnostic dilemma of isolated fallopian tube torsion. BMJ Case Rep. 2021;14:e242682. doi: 10.1136/bcr-2021-242682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Qian L, Wang X, Li D, Li S, Ding J. Isolated fallopian tube torsion with paraovarian cysts:A case report and literature review. BMC Womens Health. 2021;21:345. doi: 10.1186/s12905-021-01483-2. [DOI] [PMC free article] [PubMed] [Google Scholar]