

Abstract
Background
There exists a vast number of surgical treatment options for acromioclavicular (AC) joint injuries, and the current literature has yet to determine an equivocally superior treatment. AC joint repair has a long history and dates back to the beginning of the twentieth century.
Main body
Since then, over 150 different techniques have been described, covering open and closed techniques. Low grade injuries such as Type I-II according to the modified Rockwood classification should be treated conservatively, while high-grade injuries (types IV-VI) may be indicated for operative treatment. However, controversy exists if operative treatment is superior to nonoperative treatment, especially in grade III injuries, as functional impairment due to scapular dyskinesia or chronic pain remains concerning following non-operative treatment. Patients with a stable AC joint without overriding of the clavicle and without significant scapular dysfunction (Type IIIA) may benefit from non-interventional approaches, in contrast to patients with overriding of the clavicle and therapy-resistant scapular dysfunction (Type IIIB). If these patients are considered non-responders to a conservative approach, an anatomic AC joint reconstruction using a hybrid technique should be considered. In chronic AC joint injuries, surgery is indicated after failed nonoperative treatment of 3 to 6 months. Anatomic AC joint reconstruction techniques along with biologic augmentation (e.g. Hybrid techniques, suture fixation) should be considered for chronic high-grade instabilities, accounting for the lack of intrinsic healing and scar-forming potential of the ligamentous tissue in the chronic setting. However, complication and clinical failure rates remain high, which may be a result of technical failures or persistent horizontal and rotational instability.
Conclusion
Future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint.
Keywords: Acromioclavicular joint, Acromioclavicular joint reconstruction, AC joint, Horizontal instability, Vertical instability, Anatomic acromioclavicular joint reconstruction
Background
Current literature covers a vast number of surgical treatments for acromioclavicular (AC) joint injuries, emphasizing the incertitude regarding the best treatment. Historically, a few of these techniques have been abandoned or re-invented secondary to high complication and clinical failure rates. Classically, the Rockwood Classification attempts to characterize these injuries based upon the associated ligamentous injury and degree of displacement. This is highlighted in the Table 1. Current concepts reviews, systematic reviews and meta-analyses have attempted to reveal the evidence for the optimal treatment of AC joint injuries [1–6].
Table 1.
Rockwood Classification of Acromioclavicular Joint Injury
| Type | Definition | Physical Examination | Radiographic features |
|---|---|---|---|
| I |
• AC ligament sprain with ligaments intact • No displacement or instability |
• Tenderness at ACJ • Provocative tests positive (cross body adduction, etc) |
• No obvious radiographic abnormality |
| II |
• Ac ligaments torn • CC ligaments sprained but intact |
• ACJ subluxation/displacement with provocative stress | • Can show subtle distal clavicle elevation, but no obvious separation |
| III |
• Disruption of AC and CC ligaments • A/P and superior/inferior instability |
• Superior displacement of the distal clavicle • Acromion and shoulder girdle inferior to distal clavicle |
• Radiographs may show up to 100% or greater increase in CC distance |
| IV |
• Disruption of AC and CC ligaments • Posterior displacement of distal clavicle through trapezius |
• Palpable distal clavicle posteriorly through trapezial fascia • Also associated with anterior SC joint injury/dislocation |
• Subtle findings on AP/Zanca view • Critical to evaluate for posterior distal clavicle displacament on axillary view |
| V |
• Disruption of AC and CC ligaments • Significant displacement of acromion/scapula due to weight of the extremity |
• Gross superior displacement of distal clavicle and inferior translation of acromion/scapular complex • Can protrude through trapezial/deltoid fascia and tent skin |
• CC distance grossly increased, greater than 100% |
| VI |
• Inferior displacement/dislocation of distal clavicle • Can be displaced subacromial or subcorocoid |
• Can palpable defect and displaced distal clavicle • Neurovascular exam critical to rule out associated neurovascular compromise |
• Detect distal clavicle in subcorocoid/subacromial position |
Operative treatment may be reserved for heavy physical laborers, younger patients, overhead athletes, and frequent overhead users [7–10]. However, little evidence supports the claim that these patients would significantly benefit from operative treatment when compared to nonoperative treatment [11]. Especially, long-term data comparing operative versus nonoperative treatment is limited [4–6, 12].
AC joint repair has a long history and dates back to 1917, when Cadenet first introduced his technique for AC joint instabilities [13]. Since then, over 150 different techniques have been described [14], covering open and closed techniques including metallic wires, pins, hook plates, auto- or allografts, suspension devices, synthetic ligaments, ligament or tendon transfers, clavicle osteotomy or excision. Complication rates have been reported to vary widely between 5 and 30% of cases, mostly depending on the type of repair [15].
Currently proposed surgical methods vary widely. These include anatomic coracoclavicular ligament reconstruction, coracoacromial ligament transfer, reconstruction with internal fixation, and reconstruction with implantable suture fixation devices. This review of current concepts aims to give an overview of the relevant biomechanics and pathoanatomy, review the current available treatment modalities, and highlights current challenges while pointing out the authors’ preferred treatment algorithm.
Main text
Epidemiology and Pathoanatomy
The highest prevalence of AC joint injuries have been reported in 20- to 30- year old male patients participating in high contact sports, with AC joint injuries generally accounting for 12% of all shoulder injuries in the overall population [16]. The mechanism of most AC joint injuries is a direct fall on the superolateral aspect of the shoulder with the arm in an adducted position. In contrast, indirect injury occurs by falling on the outstretched arm, causing the humeral head to translocate superiorly and drive the humeral head into the acromion.
Acromioclavicular anatomy and biomechanics
The acromioclavicular joint is formed from the diarthrodial articulation between the distal end of the clavicle and the acromion process of the scapula, and is stabilized by various static and dynamic constraints. The acromioclavicular (AC) ligament complex is comprised of anterior,posterior, superior, and inferior ligaments. The corococlavicular (CC) ligaments are composed of the trapezoid and conoid ligaments. These AC and CC ligamentous complexes are the static stabilizing structures of the AC joint. The dynamic stabilizers include the trapezius and deltoid musculofascial attachments [1, 17–19].
The AC ligament complex, in particular the superior and posterior AC ligaments contribute to anterior/posterior stability of the AC joint, while the CC ligament complex (conoid and trapezoid) conveys superior/inferior stability. However, when the AC ligaments are ruptured, the conoid and trapezoid ligaments function to resist anterior and posterior forces, respectively. This highlights the importance of the CC ligament complex with regards to AC joint biomechanics and preventing instability not just vertically, but in the horizontal plane as well [19].
The trapezoid ligament attaches anterolaterally onto the distal clavicle, with the broader, robust conoid ligament attaching in a more posteromedial position. Biomechanical analysis has demonstrated the conoid and trapezoid tuberosities as distinct bony landmarks demarcating the anatomic relationship between the distal clavicle and coracoclavicular ligaments [18]. Rios et al. demonstrated that the distance from the distal edge of the clavicle to the medial aspect of the conoid tuberosity in male and female specimens was 47.2 ± 4.6 mm and 42.8 ± 5.6 mm, respectively. The distance to the trapezoid tuberosity was 25.4 ± 3.7 mm in males, and 22.9 ± 3.7 mm in females [18]. The distinct attachment sites of the conoid and trapezoid ligaments provide their inherent stability, and anatomical reconstruction techniques aim to re-establish this native anatomical relationship [1, 17–19].
Patient selection
Low grade injuries such as type I-II according to Rockwood should be treated non-operatively [7], as current conservative management strategies show favourable outcomes, higher return to activity and less complications rates [1, 2]. In contrast, in high-grade injuries such as types IV-VI according to Rockwood surgery should be recommended [1, 2, 20]. However, to date, controversy arises if operative treatment is superior to conservative treatment, especially in the challenging grade III injury population. To date, clinical studies failed to show significant advantage for surgical interventions [11]. Functional impairment due to scapular dyskinesia or chronic pain remains has been showed to be highly concerning following non-operative treatment. Some studies indicate that operative treatment may result in less pain and better endurance, especially during overhead work [21, 22], as well as improved patient satisfaction in both short- and long-term follow-up studies [12, 23].
However, according to a meta-analysis, no differences between operative and nonoperative treatment have been observed in terms of shoulder strength, pain relief, throwing ability, or development of osteoarthritis (OA) [12]. In contrast, longer sick leave and better cosmesis may occur with operative treatment [12]. While operative treatment can address clavicular displacement and restore the radiographic alignment in grade III injuries, it has also been shown to improve subjective and objective outcome measures [24]. A survey from McFarland and colleagues conducted in professional throwing athletes showed that complete pain relief and return to ‘normal’ was achieved more predictably with operative treatment compared to nonoperative treatment (92% vs. 80%) [25]. Additionally, Cardone and Brown reported more satisfactory outcomes and a trend toward earlier return to Australian football following operative treatment [26].
Finally, the highly variable severity of type III injuries recently led to a consensus statement published by the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) to further subdivide type III injuries, in order to more accurately identify patients who may benefit from surgery [2]: type IIIA injuries are considered stable without overriding of the clavicle on the cross-body adduction view and without significant scapular dysfunction, whereas type IIIB injuries present with horizontal instability and therapy-resistant scapular dysfunction. Accordingly, persistent scapular dysfunction remains a major concern following AC joint injuries. The AC and CC ligaments have been noted to ensure a physiological motion of the scapula [27, 28], with injuries to those ligaments may result in a more protracted and internally rotated position of the scapula, consequently leading to motion deficits and shoulder pain [29]. Interestingly, Gumina and colleagues demonstrated that in patients with chronic type III injuries, scapular dyskinesis is present in 70.6% of cases, of whom 58.3% demonstrated a SICK scapula syndrome (scapular malposition, inferior medial scapular winging, coracoid tenderness, and scapular dyskinesis), which is associated with inferior shoulder function [30]. Unfortunately, 20% of these patients still present with scapular dysfunction, even after successful completion of conservative treatment [31]. Thus, delayed surgical intervention should be indicated in patients present with persistent pain, recurrent instability or severe scapulothoracic dyskinesia after failing a trail of conservative treatment for at least 3 to 6 weeks [2].
.
History, physical examination, and diagnostic imaging
A detailed physical examination and accurate radiographic imaging are key for correct classification of the injury [2], including examination of glenohumeral joint, sternoclavicular joint, cervical spine and ipsilateral upper extremity along with a complete neurovascular exam to rule out concomitant injuries. Intraarticular comorbidities such as lesions of the long head of the biceps tendon or SLAP lesions (superior labral anterior posterior lesions) have been reported to occur in up to 18% of high grade AC joint dislocations [32], making these injuries a possible intra-articular pain source. Depending on the severity of the injury, ecchymosis and AC joint deformity may occur. In the absence of obvious AC joint deformity, tenderness to direct palpation over the AC joint and a painful cross body adduction test may indicate an injury of the AC joint. If needed, relief of symptoms by injection of local anaesthetic into the AC joint may be performed, however, this approach should be considered as an indirect and less common way of confirming the diagnosis.
Once AC joint injury has been confirmed, surgeons should focus on testing vertical displacement, horizontal and rotational instability. Horizontal stability of the AC joint is assessed by moving the clavicle in an anterior to posterior direction while stabilizing the acromion. Even though slight horizontal instability may not significantly influence clinical outcomes, physical examination should detect if present (chronic) horizontal or rotational instability may result in scapula dysfunction [33], or more importantly, in pain. Assessment of scapulothoracic motion is essential, as proper function of the AC joint is critical for correct scapulothoracic rhythm. Thus, in chronic AC joint injuries, the scapula may lack anterior strut resulting in excessive scapular internal rotation with anterior tilt [2], which may lead to persisting rotational and horizontal instability resulting in chronic pain. At this point, a detailed radiological evaluation using feasible and precise methods is required. However, a huge range of radiographic techniques without a clear standardized radiographic protocol have been described in current literature [34]. These radiographic techniques include: Bilateral Zanca view, bilateral panoramic view, (dynamic) axillary view and stress imaging.
Radiographic assessment of vertical instability
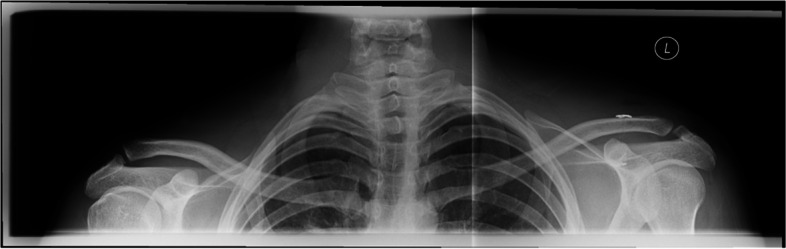
Vertical instability can be diagnosed with high inter- and intra-observer reliability in a bilateral panoramic view by measuring the coracoclavicular (CC) distance]. Bilateral views allow direct correlation of the CC-distance to the uninjured contralateral AC joint (Figs. 1 and 2) [35, 36].
Fig. 1.
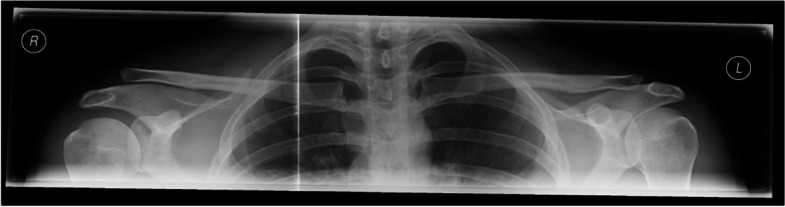
Preoperative bilateral panoramic view allowing for direct correlation of the CC-distance to the uninjured contralateral AC joint
Fig. 2.
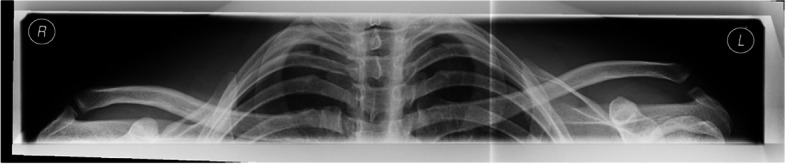
Preoperative bilateral panoramic view of a patient with Rockwood IIIB instability (Left side)
Assessment of horizontal and rotational instability
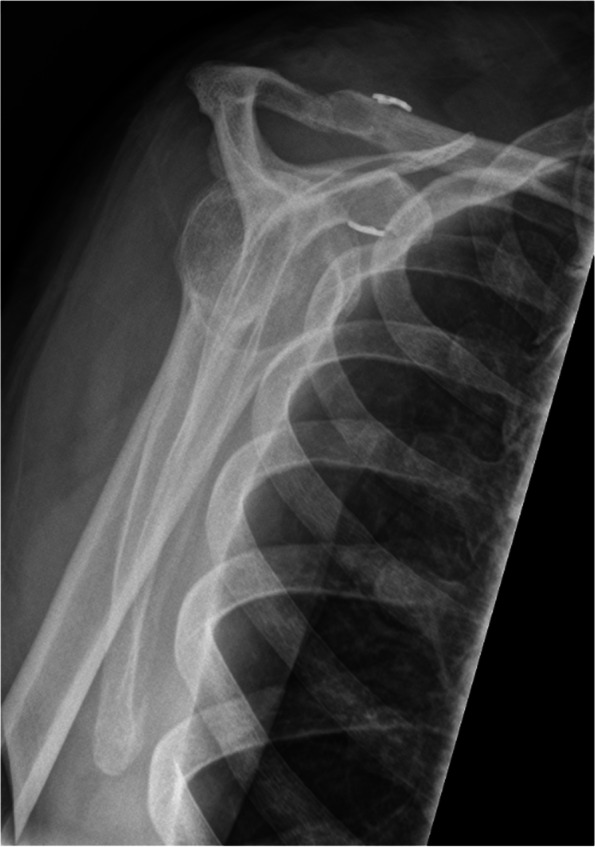
Accurate assessment of horizontal instability has been shown to be one of the most important steps in AC joint treatment recommendations [1]. However, correct and reliable diagnosis is often difficult with heterogeneous inter- and intra-observer reliability being reported [34]. Literature suggests bilateral Alexander (modified y-view; Figs. 3 and 4) views [37] for quantifying dynamic horizontal instability, especially in patients with grade IIIB instability [38], however, there remains a lack of evidence in the advantage of this radiographic view [34]. In contrast, static horizontal instability (Rockwood type IV) may be best seen on axillary views Additionally, Karagyris et al. recently proposed the acromial center line to dorsal clavicle (AC-DC) distance to define watershed cases (i.e. IIIA/IIIB/IV) [39], while Zumstein et al. recommended the glenoid centre line to posterior clavicle (GC-PC) for assessing horizontal instability [40].
Fig. 3.
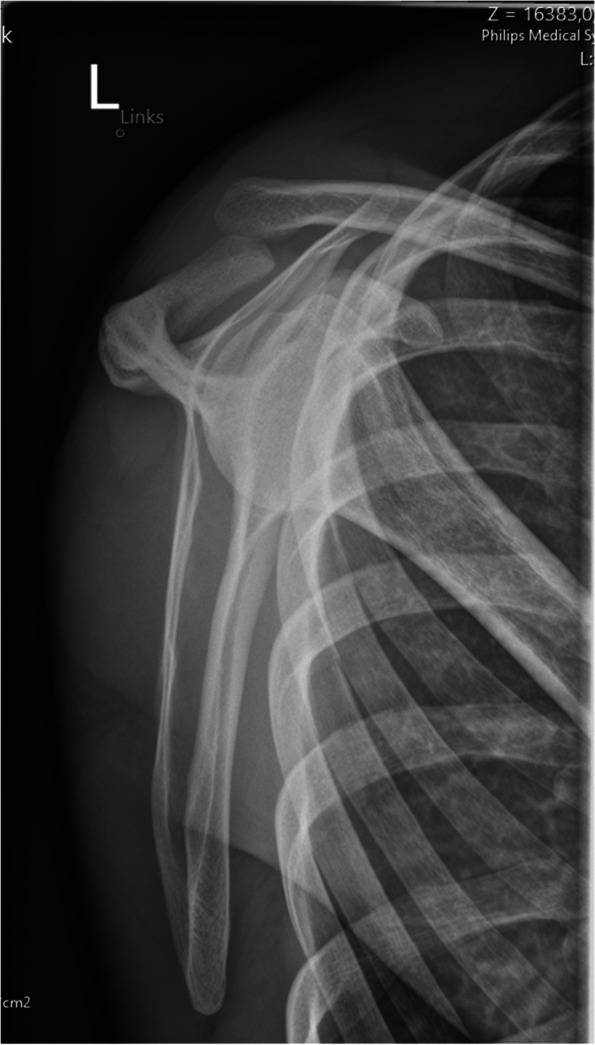
Preoperative modified y-view (Alexander view) allowing for visualization of dynamic horizontal instability (overriding of the lateral clavicle)
Fig. 4.
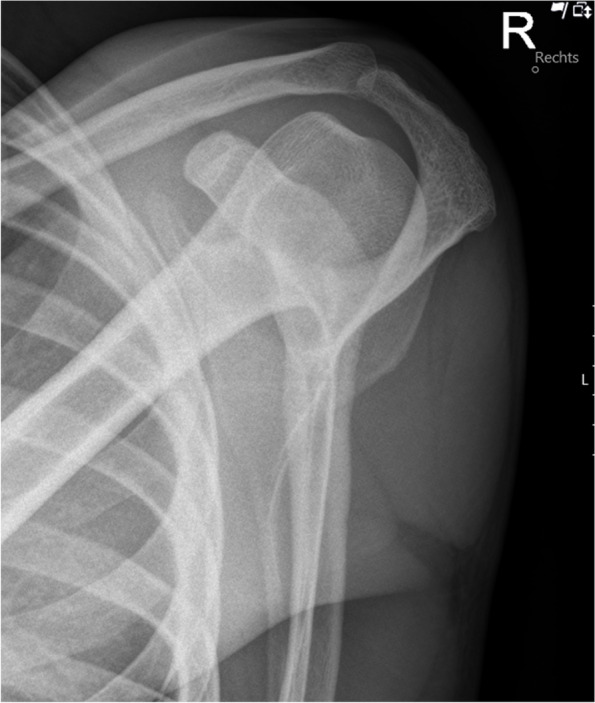
Preoperative modified y-view (Alexander view) of an intact AC joint without overriding of the lateral clavicle
Magnetic resonance imaging (MRI) and computed tomography (CT)
In order to complete an exact examination, MRI scans may be useful for detecting concomitant injuries of the glenohumeral joint, including SLAP lesions or rotator cuff tears as they occur in up to 20% of the cases [32, 41]. In chronic cases, CT scans may be helpful for a detailed visualization of osseous structures. In case of revision surgery, CT diagnosis is essential to detect insufficient fixation, technical failures (tunnel widening, tunnel position; Figs. 5 and 6) or clavicular and/or coracoid fractures.
Fig. 5.
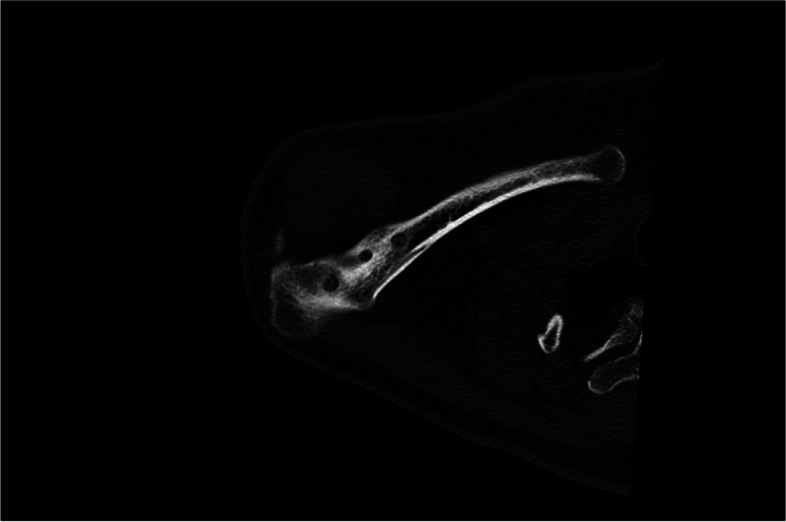
Computed tomography allowing for adequate visualization of bony imparities such as clavicular bone tunnel position, tunnel width or fractures
Fig. 6.
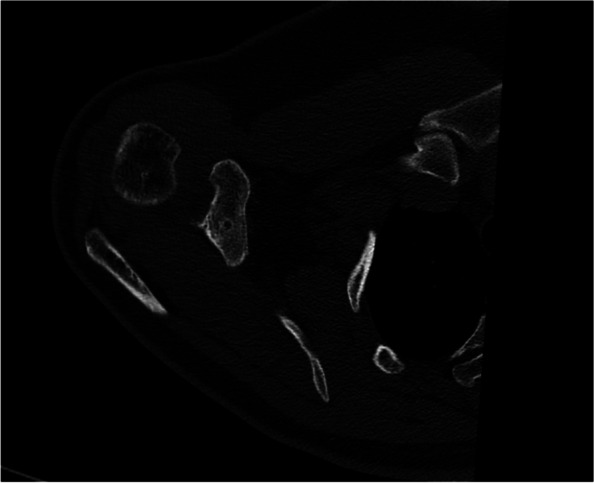
Computed tomography allowing for adequate visualization of bony imparities such as coracoid bone tunnel position, tunnel width or fractures
Choosing the optimal surgical technique
Open procedures
Anatomic Coracoclavicular ligament reconstruction (ACCR)
Historically, an anatomic and biologic solution for CC ligament reconstruction was eloquently described in 1928 by Bunnell, who incorporated a fascial graft weave that offered stability between the clavicle and the scapula at both sites [42]. Since then, anatomic and biologic approaches for AC joint reconstruction have gained popularity [43], as reliable restoration of function and comfort is seen as dependent on the durable restoration of anatomic parameters, including the congruency and stability of the AC joint. A first clinical trial has been described by Jones and colleagues [44], followed by several biomechanical investigations demonstrating that anatomic coracoclavicular ligament reconstruction (ACCR) using autograft or allograft tendon to replicate the CC ligaments at their anatomic location are more effective in mimicking the properties of the native CC ligaments compared to ligament transfers [45–48].
Biomechanical investigations
When compared to thee (modified) Weaver-Dunn procedure, nonanatomic allograft, anatomic suture, and graft-rope techniques, ACCR demonstrates superior load-to-failure characteristics [45, 46, 49]. In addition, anatomic reconstruction of the CC ligaments best restores the biomechanical properties of the native CC ligaments [45, 46], reproducing peak loads equivalent to that of the native CC ligaments, however, with lower stiffness [50, 51]. Further, Costic showed that anatomic reconstruction with a semitendinosus tendon failed to demonstrate significant graft elongation during cyclic loading [47].
Optimal tunnel placement in the clavicle is of high importance to achieve optimal strength and reduce potential risk of failures [43]. Geaney et al. showed that tunnel placement in the clavicle corresponding to the attachment of the CC ligaments has the highest bone marrow density (BMD), and correlates to higher loads to failure experimentally [52]. To reduce persistent horizontal and rotational instability of the AC joint following reconstruction [14, 53], the AC capsule should be reconstructed [14, 51, 54]. Voss and colleagues showed, that the posterior-medial acromion closest to the AC joint reveals the highest BMD with increasing density from lateral to medial; thus, fixation at this location might be favorable [55], with tunnels placed at the acromion within the “safe zone” (i.e., within the anterior half of the acromion) to not affect the load-to-failure at the acromion [56]. However, as persistent rotational instability remains a concern and may play a significant role in AC joint reconstruction failure [57, 58], future research is warranted in this area.
Surgical outcomes and complications
Open anatomic techniques generally yield in good and satisfactory outcomes [43, 59]. Muench et al. reported on 43 patients undergoing ACCR for acute and chronic type III and V AC joint injuries with 81% of patients reaching the substantial clinical benefit (SCB) after surgical reconstruction [20]. Similar, good outcomes can be expected in revision cases using the ACCR technique [60].
Coracoacromial ligament and tendon transfer
Coracoacromial ligament (CAL) transfer as an operative approach for AC joint injuries has a long history and dates back to 1917 [43], when Cadenet treated dislocations and fractures of “the outer end of the clavicle” using his technique [13]. In the early 1950s, Neviaser advocated [61] and Weaver and Dunn (WD) finally modified the technique and used it for both acute and chronic type III injuries [62]. Since then, a diversity of modifications has been proposed, all using the CAL transfer or WD technique in the same or a similar manner [63–69]. Accordingly, the CAL is transferred to the clavicle with or without an accompanying fragment of bone and may be enhanced by supplementary fixation. In 1965, Dewar et al. first described tendon transfers as a treatment for AC joint injuries [70], by performing an osteotomy of the tip of the coracoid process, including the coracobrachialis and the short head of the biceps tendon and attaching it to the clavicle [71–73].
Biomechanical investigations
When compared to intact CC ligaments, the CAL transposition as used in the Weaver-Dunn reconstruction is biomechanically significantly weaker and lax [48, 74–76]. Mazzocca and colleagues showed, that the (modified) Weaver-Dunn procedure failed to reproduce the load-to-failure durability of the intact AC and CC ligament complex [43, 46]. In contrast, LaPrade et al. demonstrated that motion at the AC joint may be restored to near-normal values,when the Weaver-Dunn reconstruction is combined with coracoid transclavicular cerclage [77]. Similar, Lee et al. concluded that for sufficient resistance to AC joint motion, surgeon’s should consider using a biological graft to further enhance the Weaver-Dunn reconstruction [78]. However, when comparing the Weaver-Dunn reconstruction to more “anatomic” reconstructions, (modified) Weaver-Dunn reconstructions are considered biomechanically inferior [49, 79, 80].
Tendon transfers have also been investigated biomechanically. Sloan and colleagues recognized, that the strength of the lateral half of the conjoined tendon (265 N) was inferior to the intact ligaments, but similar to that of the CAL (246 N) [81]. Of interest, Wellmann et al. advocated the use of the pectoralis minor tendon to prevent the complications that may arise from the CAL transfer, as the pectoralis major showed similar biomechanical properties compared to the CAL [82].
Surgical outcomes and complications
Using the CAL transfer or modified Weaver-Dunn technique may yield in satisfactory results [62, 66, 68, 83], however, to date there is only low-level evidence to support the clinical use of CAL transfer [84]. Similarly, mixed results have been reported for the treatment of type III injuries with transposition of the tip of the coracoid process [71, 85, 86], thus, this procedure may not be indicated in this patient cohort [43, 85].
AC joint reconstruction with hook plates
In 1976, Balser advocated the use of a hook plate in the treatment of AC joint dislocations for the first time [87]. In the past decade, different hook plate designs have been presented, all based on the same principles: open reduction and internal fixation (ORIF) with a precontoured hooked plate affording rigid internal fixation and sparing the articular surfaces of the joint [43, 88–90]. Advantages of hook plates comprise the simultaneous stabilization of CC and AC ligaments, which is mostly afforded by scar tissue. Several modifications have been described to further enhance the construct, including direct CC ligament repair, suturing the capsuloligamentous complex, additional screw fixation, biological or artificial augmentation or ligament/tendon transfers [89, 91, 92]. However, implant removal may be needed between 4 and 24 weeks postoperatively [93], whereas some authors do not routinely remove the device [94].
Biomechanical investigations
Patients undergoing hook plate fixation may demonstrate reduced internal rotation along with increased anterior translation (2 mm) of the clavicle with respect to the medial acromion, when compared to the native AC joint [43, 95]. Compared to TightRope and bone anchor systems, Nüchtern and colleagues demonstrated higher axial stiffness for the hook plate [96].
Surgical outcomes and complications
The use of hook plates has become extensively widespread especially in Europe, with consistent high clinical outcomes being reported [43, 88, 90, 93, 94, 97, 98], along with poor correlations between clinical and radiographic results being observed [90, 92, 94]. In case of persistent anterior-posterior instability, clinical scores have been shown to be lower [90, 99], however, early return to work and sports remains common [97–99]. When comparing acute or delayed treatment, Ejam et al. found no significant differences in clinical outcomes [93]. Additionally, Gstettner et al. showed better radiographic and clinical outcomes in patients treated with the hook plate compared to nonoperative treatment [89]. Interestingly, Di Francesco and colleagues observed scarring/healing of the CC ligaments in 88% of patients on MRI [98]. Subsequent plate removal has been demonstrated to not lead to loss of reduction or poorer clinical outcomes [100].
However, Mah et al. questioned the efficacy of hook plate stabilization in the setting of acute, high-grade AC joint instability, as they found no difference in general health status between nonoperative and operative treatment [101].
Arthroscopic assisted techniques
Suture augmentation and synthetic devices
Multiple kinds of suture augmentation and synthetic ligaments have been used for AC joint stabilization [43, 102–104], and can be passed extraosseous, intraosseous, and transosseous using drill holes in the clavicle, the coracoid, or in both. Advantages include less risk of neurovascular damage, less blood loss, shorter operative time, or no need for potential hardware removal [14, 105]. By passing nonabsorbable sutures through anatomic tunnels at the location of the conoid and trapezoid ligament footprints [106], optimal construct strength may be achieved. Additionally, CC ligament repair may be performed [105, 107].
Additionally, newer constructs such as high-tensile sutures with endobutton fixation have been advocated over the past years [14, 38, 90, 108–110], (Figs. 7 and 8) with the first arthroscopic-assisted AC joint reconstruction dating back to 2002 [111, 112]. Especially in chronic or revision cases, biological augmentation may be required to support healing of the torn structures and preserve stability of the reconstruction [113]. The use for biologic grafts may not be dependent on the strength of the reconstruction, which can be comparably achieved with nonbiologic materials, but rather on the necessity of a biologic substrate [114].
Fig. 7.
Postoperative bilateral panoramic view after stabilization of chronic Rockwood type IIIB AC joint instability using the arthroscopic-assisted hybrid technique
Fig. 8.
Postoperative y-view after stabilization of chronic Rockwood type IIIB AC joint instability using the arthroscopic-assisted hybrid technique
Biomechanical investigations
Biomechanically, suture augmentation may act as a temporary internal brace, maintaining reduction of the AC joint until ligamentous healing is complete [14, 43, 115, 116]. Synthetic suture devices have failure loads comparable to the intact CC ligament (725 N) when passed around or through the clavicle [115]. Contrary, Martetschläger et al. demonstrated inferior biomechanical properties of braided polyethylene suture (PDS) sutures used to reconstruct the AC and CC ligaments [117]. Thus, PDS may be too weak to achieve vertical stability [117], however, it is considered biomechanically superior compared to direct coracoid suture anchor repair [114].
As adequate tunnel placement if of great importance for recreating native anatomy, various methods to pass synthetic sutures through the clavicle and/or coracoid, with or without biologic augmentation, and methods to secure sutures and/or grafts have been described. Especially in chronic or revision cases, biological augmentation may be required to support healing of the torn structures and preserve stability of the reconstruction [113]. Native-like biomechanical properties of double graft tendons using hybrid techniques, such as the combination of Tight Ropes and Fibertapes with tendon grafts, may be achieved [46, 47]. Similar biomechanical properties may be expected when comparing coracoid-side flip-button tendon graft with tendon looping around the coracoid and synthetic suture augmentation [118]. Passage via double tunnels in both the clavicle and the coracoid may result in a reconstruction close to the native state compared with a single tunnel in the coracoid [119], especially when using a transosseous TightRope (Arthrex Inc., Naples, FL, USA) method [120]. This observation contradicts findings from Beitzel et al., who showed no difference between one and two tunnels in the clavicle [79, 80]. Ferreira and colleagues demonstrated higher load-to-failure of the repair construct when placing the coracoid bone tunnel center-and-center or medial-and-center, respectively [121]. However, Coale et al. found significant risks when attempting restoration of the anatomic footprint of the conoid and trapezoid ligaments [122]. Recreating both anatomic ligament footprints may enhance significant risk of cortical breach and fracture [122, 123]. Further, tunnel size, especially in the clavicle, is of great importance, as larger bone tunnels may increase fracture risk [124, 125]. Placing a hamstring tendon graft through 6 mm tunnels significantly weakens the clavicle compared to a cortical button and suture placed through 2.4 mm tunnels [124].
Finally, repair of the AC capsule may result in improved horizontal and rotational stability [54, 126], as almost 80% of the horizontal stability is provided by an intact superior-posterior capsuloligamentous complex. 28, 29, 50, 67, 7 Thus, these structures should be addressed in chronic cases, as persisting horizontal instability may lead to chronic pain and limited shoulder function [17, 57, 58, 127, 128]. When using different types of synthetic material for horizontal AC joint stabilization, no differences in outcomes may be expected. However, biomechanically, a box-shaped configuration for AC joint capsule repair may be best suited for optimal repair and may be superior to a Figure of eight configuration [58].
Surgical outcomes and complications
Generally, when reconstructing the AC joint using synthetic devices and ligaments, favorable clinical outcomes and return to preinjury activity levels may be expected [43, 92, 105, 106]. At 2 years, a 83% survivorship using these techniques has been identified [15].
When using transclavicular nonabsorbable sutures secured to the coracoid with suture anchors, satisfactory clinical outcome scores may also be expected [129]. Additionally, transosseous sutures spanning the CC interval secured through endobutton fixation on the lateral clavicle lead to early clinical success rates of nearly 90% along with radiographic stability restoration [99, 109, 130]. Rosslenbroich et al. demonstrated that younger patients achieve higher outcome values [131]. When assessing AC joint capsule repair, Tauber et al. found that combined AC and CC Ligament reconstruction better restored horizonal stability and that patients undergoing combined reconstruction showed improved patient reported and radiographic outcomes [132]. An increased risk for osteoarthritis around the AC joint has not been described so far.
Although the efficacy of Ligastic, Ligament Augmentation and Reconstruction System (LARS) or double braided polyester devices has been confirmed [133], structural failures of this device leading to inferior clinical outcomes may occur.
Discussion and therapeutic decision making
Based on the available evidence, firm conclusions are challenging regarding operative versus nonoperative treatment, the timing of surgery, open versus arthroscopic surgery, and choice of surgical procedure. Several studies demonstrated the lack of correlation between clinical outcomes and abnormal radiologic findings [3, 4, 6, 14]. As there is currently limited level I evidence, treatment considerations are mostly based on surgeon-specific factors such as experience and patient-specific factors such as age or functional demands,
In the majority of cases, nonoperative treatment of acute low-grade injuries is seen as appropriate, despite the risk of continuous pain and future development of chronic AC joint instability. High-grade injuries are typically managed operatively due to the loss of stability of the shoulder girdle and subsequent scapulothoracic imbalance [1–4, 6, 11, 14, 23, 24, 134].
The treatment algorithm (Fig. 9) proposed in this review is focused on specific and clinically relevant considerations based on the available literature. The authors of this paper developed a therapeutic decision making based on information’s obtained from recent clinical and biomechanical studies. Interestingly, within the past decade, an exponential increase in arthroscopically assisted techniques has been published, which demonstrates the raised importance of combined procedures. In addition, arthroscopic approaches may decrease the risk of serious soft tissue infection [135].
Fig. 9.

Non-operative or operative treatment based on the author’s therapeutic decision making
As the AC joint ligaments lose their potential to heal after 3 weeks following injury [68, 136], less than 3 weeks has been established as a cut-off for acute injuries [2, 137]. Thus, patients presenting with acute high-grade AC joint injuries (e.g. types IV, V, VI) should be indicated for operative treatment [2]. However, when an acute AC joint dislocation is graded as type III, an initial trial of conservative treatment may be indicated, thus making the definition “acute” challenging. Patients with a stable AC joint without overriding of the clavicle and without significant scapular dysfunction (Type IIIA) may benefit from a more conservative, nonoperative approach in contrast to patients with overriding of the clavicle and therapy-resistant scapular dysfunction (Type IIIB). If these patients fail to respond to conservative measures, an anatomic AC joint reconstruction using a hybrid technique should be considered. Besides, acute superior acromioclavicular ligament complex injuries were shown to follow distinct tear patterns, including clavicular-sided tears, oblique tears, midportion tears and acromial-sided tears. It has been shown that type-specific operative repair of acute acromioclavicular ligament complex tears might promote biological healing, consequently, lower rates of horizontal AC joint instability may occur [18], .as the integrity of the CC and AC ligaments has an impact on clinical and radiographic parameters [19].
In chronic AC joint injuries, surgery is indicated after failed nonoperative treatment of 3 to 6 months. Anatomic AC joint reconstruction techniques along with biologic augmentation (e.g. Hybrid techniques, combining Tight Rope) should be considered for chronic high-grade instabilities, accounting for the lack of intrinsic healing and scar-forming potential of the ligamentous tissue in the chronic setting. This approach has been demonstrated to provide better results regarding anterior and superior translation of the clavicle.412 Additionally, recent studies demonstrated native-like biomechanical properties of double graft tendons using hybrid techniques, such as the combination of Tight Ropes and Fibertapes with tendon grafts. However, as complication rates have been reported to be as high as 30% of cases, focus is placed more on reducing the size and number of bone tunnels during arthroscopically assisted stabilization techniques [15, 138]. Recent studies have shown the risk of postoperative fractures (clavicular and/or coracoid) to be related to the number and size of bone tunnels [56, 139, 140]. Therefore, reducing both variables may be of benefit in the setting of chronic ACJ stabilization. Focus should also be placed on restoring physiological horizontal and vertical ACJ stability. As the AC capsule and deltotrapezoidal fascia are significantly contributing to horizontal sand rotational stability, augmentation of the AC capsule is required.
Limitations
The concepts and careful conclusions presented in this review are largely limited to the lack of high-level studies found in the literature. The large heterogeneity of studies made direct comparisons as well as drawing of definite conclusions regarding treatments difficult. However, the authors aimed to customize the suggested algorithm to the available clinical and biomechanical evidence.
Future perspectives
The simple fact that over 150 different operative treatment strategies for AC joint injuries have been developed since 1917 emphasizes that the vast majority of the current techniques does not allow for complete restoration of native physiological and biomechanical AC joint properties. In the past decade, some authors advocated the importance of recreating the AC ligaments and capsule, as chronic horizontal and rotational instability may lead to chronic pain, and clinical failures [57, 58, 128]. Future clinical and biomechanical investigations should focus on addressing horizontal and rotational instability, as it remains a common challenge for shoulder surgeons. In addition, surgical techniques should only be classified as “anatomic”, if they “anatomically” reproduce the conoid and trapezoid ligaments.
Of interest, future studies may investigate on clinical and biomechanical outcomes on the newest arthroscopic-assisted technique, the knotless Tight Rope technique (2nd generation). By using this technique, less abrasive wear or shield stress (especially in bone tunnels) may be expected due to the knotless technique, which may reduce subsequent clinical failures. However, as for every new technique released, its advantages and superiority as well as its biomechanical properties still have to be demonstrated.
To this, despite advances in surgical techniques with additionally addressing the AC joint capsule using cerclages or the excess graft in order to improve horizontal stability, these approaches may not be able to adequately ensure rotational stability, which may subsequently lead to the observed postoperative failures [57, 58, 128]. Finally, a consent on optimal timing of surgery including the definition of “acute” and “chronic” has to be taken in future trials.
Conclusion
Finding the right patient, establishing the correct diagnosis, and implementing the appropriate surgical technique remains a major challenge for shoulder surgeons. In the past decade, a trend towards arthroscopic assisted techniques has been noted. However, complication and clinical failure rates remain high, which may be a result of technical failures or persistent horizontal and rotational instability. Thus, future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint.
Acknowledgements
None
Abbreviations
- AC
Acromioclavicular
- CC
Corococlavicular
- ACJ
Acromioclavicular joint
- SICK scapula syndrome
Scapular malposition, inferior medial scapular winging, coracoid tenderness, and scapular dyskinesis
- SLAP lesions
Superior labral anterior posterior lesions
- MRI
Magnetic Resonance Imaging
- CT
Computed Tomography
- ACCR
Anatomic Coracoclavicular Ligament Reconstruction
- BMD
Bone marrow density
- SCB
Substantial clinical benefit
- CAL
Coracoacromial ligament
- WD
Weaver and Dunn
- N
Newton
- ORIF
Open reduction and internal fixation
- LARS
Ligastic, Ligament Augmentation and Reconstruction System
Authors’ contributions
DPB, LNM and PG wrote the manuscript. FD, AV helped creating the Figures and Tables. ADM, ABI, SS, BS and KB helped with the final revisions and provided intellectual content. All authors have read and approved the manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Availability of data and materials
All authors had unrestricted access to all the data of this study. Raw data can be requested from the corresponding author.
Declarations
Ethics approval and consent to participate
The study was reported via Human Research Determination Form to the institutional review board (IRB) of the University of Connecticut and it was documented, that no IRB approval was required.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Beitzel K, Cote MP, Apostolakos J, Solovyova O, Judson CH, Ziegler CG, Edgar CM, Imhoff AB, Arciero RA, Mazzocca AD. Current concepts in the treatment of acromioclavicular joint dislocations. Arthroscopy. 2013;29(2):387–397. doi: 10.1016/j.arthro.2012.11.023. [DOI] [PubMed] [Google Scholar]
- 2.Beitzel K, Mazzocca AD, Bak K, Itoi E, Kibler WB, Mirzayan R, Imhoff AB, Calvo E, Arce G, Shea K. ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy. 2014;30(2):271–278. doi: 10.1016/j.arthro.2013.11.005. [DOI] [PubMed] [Google Scholar]
- 3.Gowd AK, Liu JN, Cabarcas BC, Cvetanovich GL, Garcia GH, Manderle BJ, Verma NN. Current concepts in the operative Management of Acromioclavicular Dislocations: a systematic review and Meta-analysis of operative techniques. Am J Sports Med. 2019;47(11):2745–2758. doi: 10.1177/0363546518795147. [DOI] [PubMed] [Google Scholar]
- 4.Aliberti GM, Kraeutler MJ, Trojan JD, Mulcahey MK. Horizontal instability of the acromioclavicular joint: a systematic review. Am J Sports Med. 2019;363546519831013. [DOI] [PubMed]
- 5.Moatshe G, Kruckeberg BM, Chahla J, Godin JA, Cinque ME, Provencher MT, LaPrade RF. Acromioclavicular and Coracoclavicular ligament reconstruction for acromioclavicular joint instability: a systematic review of clinical and radiographic outcomes. Arthroscopy. 2018;34(6):1979–1995 e1978. doi: 10.1016/j.arthro.2018.01.016. [DOI] [PubMed] [Google Scholar]
- 6.Borbas P, Churchill J, Ek ET. Surgical management of chronic high-grade acromioclavicular joint dislocations: a systematic review. J Shoulder Elb Surg. 2019;28(10):2031–2038. doi: 10.1016/j.jse.2019.03.005. [DOI] [PubMed] [Google Scholar]
- 7.Rockwood C. Disorders of the acromioclavicular joint. In: Rockwood CA, Matsen FA, editors. The shoulder Vol. 1. Pennsylvania: WB Saunders Company; 1998. [Google Scholar]
- 8.Trainer G, Arciero RA, Mazzocca AD. Practical management of grade III acromioclavicular separations. Clin J Sport Med. 2008;18(2):162–166. doi: 10.1097/JSM.0b013e318169f4c1. [DOI] [PubMed] [Google Scholar]
- 9.Larsen E, Bjerg-Nielsen A, Christensen P. Conservative or surgical treatment of acromioclavicular dislocation. A prospective, controlled, randomized study. J Bone J Surg Am. 1986;68(4):552–555. doi: 10.2106/00004623-198668040-00011. [DOI] [PubMed] [Google Scholar]
- 10.Larsen E, Hede A. Treatment of acute acromioclavicular dislocation. Three different methods of treatment prospectively studied. Acta Orthop Belg. 1987;53(4):480–484. [PubMed] [Google Scholar]
- 11.Spencer EE., Jr Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007;455:38–44. doi: 10.1097/BLO.0b013e318030df83. [DOI] [PubMed] [Google Scholar]
- 12.Smith TO, Chester R, Pearse EO, Hing CB. Operative versus non-operative management following Rockwood grade III acromioclavicular separation: a meta-analysis of the current evidence base. J Orthop Traumatol. 2011;12(1):19–27. doi: 10.1007/s10195-011-0127-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cadenet FM. The treatment of dislocations and fractures of the outer end of the clavicle. Clin Orthop. 1917;1:145–169. [Google Scholar]
- 14.Dyrna F, Berthold DP, Feucht MJ, Muench LN, Martetschläger F, Imhoff AB, Mazzocca AD, Beitzel K. The importance of biomechanical properties in revision acromioclavicular joint stabilization: a scoping review. Knee Surg Sports Traumatol Arthrosc. 2019;27(12):3844–3855. doi: 10.1007/s00167-019-05742-6. [DOI] [PubMed] [Google Scholar]
- 15.Martetschläger F, Horan MP, Warth RJ, Millett PJ. Complications after anatomic fixation and reconstruction of the coracoclavicular ligaments. Am J Sports Med. 2013;41(12):2896–2903. doi: 10.1177/0363546513502459. [DOI] [PubMed] [Google Scholar]
- 16.Fraser-Moodie J, Shortt N, Robinson C. Injuries to the acromioclavicular joint. J Bone Joint Surg (Br) 2008;90(6):697–707. doi: 10.1302/0301-620X.90B6.20704. [DOI] [PubMed] [Google Scholar]
- 17.Martetschläger F, Kraus N, Scheibel M, Streich J, Venjakob A, Maier D. The diagnosis and treatment of acute dislocation of the acromioclavicular joint. Deutsches Aerzteblatt International. 2019;116(6). [DOI] [PMC free article] [PubMed]
- 18.Maier D, Jaeger M, Reising K, Feucht MJ, Südkamp NP, Izadpanah K. Injury patterns of the acromioclavicular ligament complex in acute acromioclavicular joint dislocations: a cross-sectional, fundamental study. BMC Musculoskelet Disord. 2016;17(1):385. doi: 10.1186/s12891-016-1240-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Minkus M, Wieners G, Maziak N, Plachel F, Scheibel M, Kraus N. The ligamentous injury pattern in acute acromioclavicular dislocations and its impact on clinical and radiographic parameters. J Shoulder Elb Surg. 2021;30(4):795–805. doi: 10.1016/j.jse.2020.10.026. [DOI] [PubMed] [Google Scholar]
- 20.Muench LN, Kia C, Jerliu A, Murphy M, Berthold DP, Cote MP, Arciero RA, Mazzocca AD. Functional and radiographic outcomes after anatomic Coracoclavicular ligament reconstruction for type III/V acromioclavicular joint injuries. Orthopaedic journal of sports medicine. 2019;7(11):2325967119884539. doi: 10.1177/2325967119884539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Park JP, Arnold JA, Coker TP, Harris WD, Becker DA. Treatment of acromioclavicular separations. A retrospective study. Am J Sports Med. 1980;8(4):251–256. doi: 10.1177/036354658000800407. [DOI] [PubMed] [Google Scholar]
- 22.Lynch TS, Saltzman MD, Ghodasra JH, Bilimoria KY, Bowen MK, Nuber GW. Acromioclavicular joint injuries in the National Football League: epidemiology and management. Am J Sports Med. 2013;41(12):2904–2908. doi: 10.1177/0363546513504284. [DOI] [PubMed] [Google Scholar]
- 23.Phillips AM, Smart C, Groom AF. Acromioclavicular dislocation. Conservative or surgical therapy. Clin Orthop Relat Res. 1998;353:10–17. doi: 10.1097/00003086-199808000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Korsten K, Gunning AC, Leenen LP. Operative or conservative treatment in patients with Rockwood type III acromioclavicular dislocation: a systematic review and update of current literature. Int Orthop. 2014;38(4):831–838. doi: 10.1007/s00264-013-2143-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McFarland EG, Blivin S, Doehring C, Curl L, Silberstein C. Treatment of grade III acromioclavicular separations in professional throwing athletes: results of a survey. Am J Orthop (Belle Mead NJ) 1997;26(11):771–774. [PubMed] [Google Scholar]
- 26.Cardone D, Brown JN, Roberts SN, Saies AD, Hayes MG. Grade III acromioclavicular joint injury in Australian rules football. J Sci Med Sport. 2002;5(2):143–148. doi: 10.1016/S1440-2440(02)80035-4. [DOI] [PubMed] [Google Scholar]
- 27.Seo Y-J, Yoo Y-S, Noh K-C, Song S-Y, Lee Y-B, Kim H-J, Kim HY. Dynamic function of coracoclavicular ligament at different shoulder abduction angles: a study using a 3-dimensional finite element model. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2012;28(6):778–787. doi: 10.1016/j.arthro.2012.04.001. [DOI] [PubMed] [Google Scholar]
- 28.Izadpanah K, Weitzel E, Honal M, Winterer J, Vicari M, Maier D, Jaeger M, Kotter E, Hennig J, Weigel M. In vivo analysis of coracoclavicular ligament kinematics during shoulder abduction. Am J Sports Med. 2012;40(1):185–192. doi: 10.1177/0363546511423015. [DOI] [PubMed] [Google Scholar]
- 29.Kibler WB, Sciascia A. Current concepts: scapular dyskinesis. Br J Sports Med. 2010;44(5):300–305. doi: 10.1136/bjsm.2009.058834. [DOI] [PubMed] [Google Scholar]
- 30.Gumina S, Carbone S, Postacchini F. Scapular dyskinesis and SICK scapula syndrome in patients with chronic type III acromioclavicular dislocation. Arthroscopy. 2009;25(1):40–45. doi: 10.1016/j.arthro.2008.08.019. [DOI] [PubMed] [Google Scholar]
- 31.Carbone S, Postacchini R, Gumina S. Scapular dyskinesis and SICK syndrome in patients with a chronic type III acromioclavicular dislocation. Results of rehabilitation. Knee Surg Sports Traumatol Arthrosc. 2015;23(5):1473–1480. doi: 10.1007/s00167-014-2844-5. [DOI] [PubMed] [Google Scholar]
- 32.Tischer T, Salzmann GM, El-Azab H, Vogt S, Imhoff AB. Incidence of associated injuries with acute acromioclavicular joint dislocations types III through V. Am J Sports Med. 2009;37(1):136–139. doi: 10.1177/0363546508322891. [DOI] [PubMed] [Google Scholar]
- 33.Scheibel M, Dröschel S, Gerhardt C, Kraus N. Arthroscopically assisted stabilization of acute high-grade acromioclavicular joint separations. Am J Sports Med. 2011;39(7):1507–1516. doi: 10.1177/0363546511399379. [DOI] [PubMed] [Google Scholar]
- 34.Pogorzelski J, Beitzel K, Ranuccio F, Wörtler K, Imhoff AB, Millett PJ, Braun S. The acutely injured acromioclavicular joint–which imaging modalities should be used for accurate diagnosis? A systematic review. BMC Musculoskelet Disord. 2017;18(1):515. doi: 10.1186/s12891-017-1864-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Schneider MM, Balke M, Koenen P, Frohlich M, Wafaisade A, Bouillon B, Banerjee M. Inter- and intraobserver reliability of the Rockwood classification in acute acromioclavicular joint dislocations. Knee Surg Sports Traumatol Arthrosc. 2016;24(7):2192–2196. doi: 10.1007/s00167-014-3436-0. [DOI] [PubMed] [Google Scholar]
- 36.Gastaud O, Raynier JL, Duparc F, Baverel L, Andrieu K, Tarissi N, Barth J. Reliability of radiographic measurements for acromioclavicular joint separations. Orthop Traumatol Surg Res. 2015;101(8 Suppl):S291–S295. doi: 10.1016/j.otsr.2015.09.010. [DOI] [PubMed] [Google Scholar]
- 37.Alexander OM. Dislocation of the acromioclavicular joint. Radiography. 1949;15(179):260. [PubMed] [Google Scholar]
- 38.Berthold D, Dyrna F, Imhoff A, Martetschlaeger F. Innovations for treatment of acromioclavicular joint instability. Arthroskopie. 2019;32(1):11–14. doi: 10.1007/s00142-018-0245-3. [DOI] [Google Scholar]
- 39.Karargyris O, Murphy RJ, Arenas A, Bolliger L, Zumstein MA. Improved identification of unstable acromioclavicular joint injuries in a clinical population using the acromial center line to dorsal clavicle radiographic measurement. J Shoulder Elb Surg. 2020;29(8):1599–1605. doi: 10.1016/j.jse.2019.12.014. [DOI] [PubMed] [Google Scholar]
- 40.Zumstein MA, Schiessl P, Ambuehl B, Bolliger L, Weihs J, Maurer MH, Moor BK, Schaer M, Raniga S. New quantitative radiographic parameters for vertical and horizontal instability in acromioclavicular joint dislocations. Knee Surg Sports Traumatol Arthrosc. 2018;26(1):125–135. doi: 10.1007/s00167-017-4579-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ruiz Ibán MA, Moreno Romero MS, Diaz Heredia J, Ruiz Díaz R, Muriel A, López-Alcalde J. The prevalence of intraarticular associated lesions after acute acromioclavicular joint injuries is 20%. A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2020;29(7):2024–2038. doi: 10.1007/s00167-020-05917-6. [DOI] [PubMed] [Google Scholar]
- 42.Bunnell S. Fascial graft for dislocation of the acromioclavicular joint. Surg Gynecol Obstet. 1928;46:563–564. [Google Scholar]
- 43.Matsen FA, Cordasco FA, Sperling JW, Lippitt SB. Rockwood and Matsen’s the shoulder. Elsevier Health Sciences; 2021. [Google Scholar]
- 44.Jones HP, Lemos MJ, Schepsis AA. Salvage of failed acromioclavicular joint reconstruction using autogenous semitendinosus tendon from the knee: surgical technique and case report. Am J Sports Med. 2001;29(2):234–237. doi: 10.1177/03635465010290022001. [DOI] [PubMed] [Google Scholar]
- 45.Mazzocca AD, Conway JE, Johnson S, Rios CG, Dumonski ML, Santangelo SA, Arciero RA. The anatomic coracoclavicular ligament reconstruction. Oper Tech Sports Med. 2004;12(1):56–61. doi: 10.1053/j.otsm.2004.04.001. [DOI] [Google Scholar]
- 46.Mazzocca AD, Santangelo SA, Johnson ST, Rios CG, Dumonski ML, Arciero RA. A biomechanical evaluation of an anatomical coracoclavicular ligament reconstruction. Am J Sports Med. 2006;34(2):236–246. doi: 10.1177/0363546505281795. [DOI] [PubMed] [Google Scholar]
- 47.Costic RS, Labriola JE, Rodosky MW, Debski RE. Biomechanical rationale for development of anatomical reconstructions of coracoclavicular ligaments after complete acromioclavicular joint dislocations. Am J Sports Med. 2004;32(8):1929–1936. doi: 10.1177/0363546504264637. [DOI] [PubMed] [Google Scholar]
- 48.Lee SJ, Nicholas SJ, Akizuki KH, McHugh MP, Kremenic IJ, Ben-Avi S. Reconstruction of the coracoclavicular ligaments with tendon grafts. Am J Sports Med. 2003;31(5):648–654. doi: 10.1177/03635465030310050301. [DOI] [PubMed] [Google Scholar]
- 49.Thomas K, Litsky A, Jones G, Bishop JY. Biomechanical comparison of coracoclavicular reconstructive techniques. Am J Sports Med. 2011;39(4):804–810. doi: 10.1177/0363546510390482. [DOI] [PubMed] [Google Scholar]
- 50.Staron JS, Esquivel AO, Pandhi NG, Hanna JD, Lemos SE. Biomechanical evaluation of anatomical double-bundle coracoclavicular ligament reconstruction secured with knot fixation versus screw fixation. Orthopedics. 2013;36(8):e1047–e1052. doi: 10.3928/01477447-20130724-22. [DOI] [PubMed] [Google Scholar]
- 51.Grantham C, Heckmann N, Wang L, Tibone JE, Struhl S, Lee TQ. A biomechanical assessment of a novel double endobutton technique versus a coracoid cerclage sling for acromioclavicular and coracoclavicular injuries. Knee Surg Sports Traumatol Arthrosc. 2016;24(6):1918–1924. doi: 10.1007/s00167-014-3198-8. [DOI] [PubMed] [Google Scholar]
- 52.Geaney LE, Beitzel K, Chowaniec DM, Cote MP, Apostolakos J, Arciero RA, Mazzocca AD. Graft fixation is highest with anatomic tunnel positioning in acromioclavicular reconstruction. Arthroscopy. 2013;29(3):434–439. doi: 10.1016/j.arthro.2012.10.010. [DOI] [PubMed] [Google Scholar]
- 53.Saier T, Venjakob AJ, Minzlaff P, Föhr P, Lindell F, Imhoff AB, Vogt S, Braun S. Value of additional acromioclavicular cerclage for horizontal stability in complete acromioclavicular separation: a biomechanical study. Knee Surg Sports Traumatol Arthrosc. 2015;23(5):1498–1505. doi: 10.1007/s00167-014-2895-7. [DOI] [PubMed] [Google Scholar]
- 54.Beitzel K, Obopilwe E, Apostolakos J, Cote MP, Russell RP, Charette R, Singh H, Arciero RA, Imhoff AB, Mazzocca AD. Rotational and translational stability of different methods for direct acromioclavicular ligament repair in anatomic acromioclavicular joint reconstruction. Am J Sports Med. 2014;42(9):2141–2148. doi: 10.1177/0363546514538947. [DOI] [PubMed] [Google Scholar]
- 55.Voss A, Dyrna F, Achtnich A, Hoberman A, Obopilwe E, Imhoff AB, Mazzocca AD, Beitzel K. Acromion morphology and bone mineral density distribution suggest favorable fixation points for anatomic acromioclavicular reconstruction. Knee Surg Sports Traumatol Arthrosc. 2017;25(7):2004–2012. doi: 10.1007/s00167-017-4539-1. [DOI] [PubMed] [Google Scholar]
- 56.Dyrna F, de Oliveira CCT, Nowak M, Voss A, Obopilwe E, Braun S, Pauzenberger L, Imhoff AB, Mazzocca AD, Beitzel K. Risk of fracture of the acromion depends on size and orientation of acromial bone tunnels when performing acromioclavicular reconstruction. Knee Surg Sports Traumatol Arthrosc. 2018;26(1):275–284. doi: 10.1007/s00167-017-4728-y. [DOI] [PubMed] [Google Scholar]
- 57.Dyrna FGE, Imhoff FB, Voss A, Braun S, Obopilwe E, Apostolakos JM, Morikawa D, Comer B, Imhoff AB, Mazzocca AD, et al. The integrity of the acromioclavicular capsule ensures physiological centering of the acromioclavicular joint under rotational loading. Am J Sports Med. 2018;46(6):1432–1440. doi: 10.1177/0363546518758287. [DOI] [PubMed] [Google Scholar]
- 58.Dyrna F, Imhoff FB, Haller B, Braun S, Obopilwe E, Apostolakos JM, Morikawa D, Imhoff AB, Mazzocca AD, Beitzel K. Primary stability of an acromioclavicular joint repair is affected by the type of additional reconstruction of the acromioclavicular capsule. Am J Sports Med. 2018;46(14):3471–3479. doi: 10.1177/0363546518807908. [DOI] [PubMed] [Google Scholar]
- 59.Millett PJ, Horan MP, Warth RJ. Two-year outcomes after primary anatomic Coracoclavicular ligament reconstruction. Arthroscopy. 2015;31(10):1962–1973. doi: 10.1016/j.arthro.2015.03.034. [DOI] [PubMed] [Google Scholar]
- 60.Berthold DP, Muench LN, Beitzel K, Archambault S, Jerliu A, Cote MP, Scheiderer B, Imhoff AB, Arciero RA, Mazzocca AD. Minimum 10-year outcomes after revision anatomic Coracoclavicular ligament reconstruction for acromioclavicular joint instability. Orthopaedic journal of sports medicine. 2020;8(9):2325967120947033. doi: 10.1177/2325967120947033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Neviaser JS. Acromioclavicular dislocation treated by transference of the coracoacromial ligament. AMA Arch Surg. 1952;64(3):292–297. doi: 10.1001/archsurg.1952.01260010306004. [DOI] [PubMed] [Google Scholar]
- 62.Weaver JK, Dunn HK. Treatment of acromioclavicular injuries, especially complete acromioclavicular separation. J Bone Joint Surg Am. 1972;54(6):1187–1194. doi: 10.2106/00004623-197254060-00005. [DOI] [PubMed] [Google Scholar]
- 63.Dumontier C, Sautet A, Man M, Apoil A. Acromioclavicular dislocations: treatment by coracoacromial ligamentoplasty. J Shoulder Elb Surg. 1995;4(2):130–134. doi: 10.1016/S1058-2746(05)80067-9. [DOI] [PubMed] [Google Scholar]
- 64.Shoji H, Roth C, Chuinard R. Bone block transfer of coracoacromial ligament in acromioclavicular injury. Clin Orthop Relat Res. 1986;208:272–277. doi: 10.1097/00003086-198607000-00047. [DOI] [PubMed] [Google Scholar]
- 65.Kawabe N, Watanabe R, Sato M. Treatment of complete acromioclavicular separation by coracoacromial ligament transfer. Clin Orthop Relat Res. 1984;185:222–227. doi: 10.1097/00003086-198405000-00036. [DOI] [PubMed] [Google Scholar]
- 66.Lemos MJ. The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med. 1998;26(1):137–144. doi: 10.1177/03635465980260010801. [DOI] [PubMed] [Google Scholar]
- 67.Ponce BA, Millett PJ, Warner JJ. Acromioclavicular joint instability—reconstruction indications and techniques. Oper Tech Sports Med. 2004;12(1):35–42. doi: 10.1053/j.otsm.2004.04.004. [DOI] [Google Scholar]
- 68.Weinstein DM, McCann PD, Mcllveen SJ, Flatow EL, Bigliani LU. Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med. 1995;23(3):324–331. doi: 10.1177/036354659502300313. [DOI] [PubMed] [Google Scholar]
- 69.Tienen TG, Oyen JF, Eggen PJ. A modified technique of reconstruction for complete acromioclavicular dislocation: a prospective study. Am J Sports Med. 2003;31(5):655–659. doi: 10.1177/03635465030310050401. [DOI] [PubMed] [Google Scholar]
- 70.Dewar FP, Barrington TW. The treamtnet of chronic acromio-clavicular dislocation. J Bone Joint Surg (Br) 1965;47:32–35. doi: 10.1302/0301-620X.47B1.32. [DOI] [PubMed] [Google Scholar]
- 71.Bailey R, O’Connor G, Titus P, Baril J. Dynamic repair for acute and chronic injuries of acromioclavicular area. J Bone Joint Surg Am. 1972;54(8):1802–1835. [Google Scholar]
- 72.Brunelli G, Brunelli F. The treatment of acromio-clavicular dislocation by transfer of the short head of biceps. Int Orthop. 1988;12(2):105–108. doi: 10.1007/BF00266973. [DOI] [PubMed] [Google Scholar]
- 73.Vargas L, De Janeiro R. Repair of complete acromioclavicular dislocation, utilizing the short head of the biceps. JBJS. 1942;24(4):772–773. [Google Scholar]
- 74.Deshmukh AV, Wilson DR, Zilberfarb JL, Perlmutter GS. Stability of acromioclavicular joint reconstruction: biomechanical testing of various surgical techniques in a cadaveric model. Am J Sports Med. 2004;32(6):1492–1498. doi: 10.1177/0363546504263699. [DOI] [PubMed] [Google Scholar]
- 75.Motamedi AR, Blevins FT, Willis MC, McNally TP, Shahinpoor M. Biomechanics of the coracoclavicular ligament complex and augmentations used in its repair and reconstruction. Am J Sports Med. 2000;28(3):380–384. doi: 10.1177/03635465000280031701. [DOI] [PubMed] [Google Scholar]
- 76.Harris RI, Wallace AL, Harper GD, Goldberg JA, Sonnabend DH, Walsh WR. Structural properties of the intact and the reconstructed coracoclavicular ligament complex. Am J Sports Med. 2000;28(1):103–108. doi: 10.1177/03635465000280010201. [DOI] [PubMed] [Google Scholar]
- 77.LaPrade RF, Wickum DJ, Griffith CJ, Ludewig PM. Kinematic evaluation of the modified Weaver-Dunn acromioclavicular joint reconstruction. Am J Sports Med. 2008;36(11):2216–2221. doi: 10.1177/0363546508319048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Lee SJ, Keefer EP, McHugh MP, Kremenic IJ, Orishimo KF, Ben-Avi S, Nicholas SJ. Cyclical loading of coracoclavicular ligament reconstructions: a comparative biomechanical study. Am J Sports Med. 2008;36(10):1990–1997. doi: 10.1177/0363546508324284. [DOI] [PubMed] [Google Scholar]
- 79.Beitzel K, Obopilwe E, Chowaniec DM, Nowak MD, Hanypsiak BT, Guerra JJ, Arciero RA, Mazzocca AD. Biomechanical properties of repairs for dislocated AC joints using suture button systems with integrated tendon augmentation. Knee Surg Sports Traumatol Arthrosc. 2012;20(10):1931–1938. doi: 10.1007/s00167-011-1828-y. [DOI] [PubMed] [Google Scholar]
- 80.Beitzel K, Obopilwe E, Chowaniec DM, Niver GE, Nowak MD, Hanypsiak BT, Guerra JJ, Arciero RA, Mazzocca AD. Biomechanical comparison of arthroscopic repairs for acromioclavicular joint instability: suture button systems without biological augmentation. Am J Sports Med. 2011;39(10):2218–2225. doi: 10.1177/0363546511416784. [DOI] [PubMed] [Google Scholar]
- 81.Sloan SM, Budoff JE, Hipp JA, Nguyen L. Coracoclavicular ligament reconstruction using the lateral half of the conjoined tendon. J Shoulder Elb Surg. 2004;13(2):186–190. doi: 10.1016/j.jse.2003.12.002. [DOI] [PubMed] [Google Scholar]
- 82.Wellmann M, Wiebringhaus P, Lodde I, Waizy H, Becher C, Raschke MJ, Petersen W. Biomechanical evaluation of a single-row versus double-row repair for complete subscapularis tears. Knee Surg Sports Traumatol Arthrosc. 2009;17(12):1477–1484. doi: 10.1007/s00167-009-0890-1. [DOI] [PubMed] [Google Scholar]
- 83.Cerciello S, Edwards TB, Morris BJ, Cerciello G, Walch G. The treatment of type III acromioclavicular dislocations with a modified Cadenat procedure: surgical technique and mid-term results. Arch Orthop Trauma Surg. 2014;134(11):1501–1506. doi: 10.1007/s00402-014-2085-6. [DOI] [PubMed] [Google Scholar]
- 84.Sood A, Wallwork N, Bain GI. Clinical results of coracoacromial ligament transfer in acromioclavicular dislocations: a review of published literature. Int J Shoulder Surg. 2008;2(1):13. doi: 10.4103/0973-6042.39582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Skjeldal S, Lundblad R, Dullerud R. Coracoid process transfer for acromioclavicular dislocation. Acta Orthop Scand. 1988;59(2):180–182. doi: 10.3109/17453678809169704. [DOI] [PubMed] [Google Scholar]
- 86.Jiang C, Wang M, Rong G. Proximally based conjoined tendon transfer for coracoclavicular reconstruction in the treatment of acromioclavicular dislocation. J Bone J Surg Am. 2007;89(11):2408–2412. doi: 10.2106/00004623-200711000-00010. [DOI] [PubMed] [Google Scholar]
- 87.Balser D. Eine neue Methode zur operativen Behandlung der akromioklavikulären Luxation. Chir Prax. 1976;24:275. [Google Scholar]
- 88.Göhring U, Matusewicz A, Friedl W, Ruf W. Results of treatment after different surgical procedures for management of acromioclavicular joint dislocation. Chirurg. 1993;64(7):565–571. [PubMed] [Google Scholar]
- 89.Gstettner C, Tauber M, Hitzl W, Resch H. Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elb Surg. 2008;17(2):220–225. doi: 10.1016/j.jse.2007.07.017. [DOI] [PubMed] [Google Scholar]
- 90.Jensen G, Katthagen JC, Alvarado LE, Lill H, Voigt C. Has the arthroscopically assisted reduction of acute AC joint separations with the double tight-rope technique advantages over the clavicular hook plate fixation? Knee Surg Sports Traumatol Arthrosc. 2014;22(2):422–430. doi: 10.1007/s00167-012-2270-5. [DOI] [PubMed] [Google Scholar]
- 91.Lin H-Y, Wong P-K, Ho W-P, Chuang T-Y, Liao Y-S, Wong C-C. Clavicular hook plate may induce subacromial shoulder impingement and rotator cuff lesion-dynamic sonographic evaluation. J Orthop Surg Res. 2014;9(1):6. doi: 10.1186/1749-799X-9-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Yoon JP, Lee B-J, Nam SJ, Chung SW, Jeong W-J, Min W-K, Oh JH. Comparison of results between hook plate fixation and ligament reconstruction for acute unstable acromioclavicular joint dislocation. Clin Orthop Surg. 2015;7(1):97–103. doi: 10.4055/cios.2015.7.1.97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Ejam S, Lind T, Falkenberg B. Surgical treatment of acute and chronic acromioclavicular dislocation Tossy type III and V using the hook plate. Acta Orthop Belg. 2008;74(4):441–445. [PubMed] [Google Scholar]
- 94.De Baets T, Truijen J, Driesen R, Pittevils T. The treatment of acromioclavicular joint dislocation Tossy grade III with a clavicle hook plate. Acta Orthop Belg. 2004;70(6):515–519. [PubMed] [Google Scholar]
- 95.Kim YS, Yoo Y-S, Jang SW, Nair AV, Jin H, Song H-S. In vivo analysis of acromioclavicular joint motion after hook plate fixation using three-dimensional computed tomography. J Shoulder Elb Surg. 2015;24(7):1106–1111. doi: 10.1016/j.jse.2014.12.012. [DOI] [PubMed] [Google Scholar]
- 96.Nüchtern JV, Sellenschloh K, Bishop N, Jauch S, Briem D, Hoffmann M, Lehmann W, Pueschel K, Morlock MM, Rueger JM. Biomechanical evaluation of 3 stabilization methods on acromioclavicular joint dislocations. Am J Sports Med. 2013;41(6):1387–1394. doi: 10.1177/0363546513484892. [DOI] [PubMed] [Google Scholar]
- 97.Pereira-Graterol E, Alvarez-Diaz P, Seijas R, Ares O, Cusco X, Cugat R. Treatment and evolution of grade III acromioclavicular dislocations in soccer players. Knee Surg Sports Traumatol Arthrosc. 2013;21(7):1633–1635. doi: 10.1007/s00167-012-2186-0. [DOI] [PubMed] [Google Scholar]
- 98.Di Francesco A, Zoccali C, Colafarina O, Pizzoferrato R, Flamini S. The use of hook plate in type III and V acromio-clavicular Rockwood dislocations: clinical and radiological midterm results and MRI evaluation in 42 patients. Injury. 2012;43(2):147–152. doi: 10.1016/j.injury.2011.04.002. [DOI] [PubMed] [Google Scholar]
- 99.Metzlaff S, Rosslenbroich S, Forkel P, Schliemann B, Arshad H, Raschke M, Petersen W. Surgical treatment of acute acromioclavicular joint dislocations: hook plate versus minimally invasive reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016;24(6):1972–1978. doi: 10.1007/s00167-014-3294-9. [DOI] [PubMed] [Google Scholar]
- 100.Wei C, Zhagn Q, YL SU, Zhang ZK, Hou ZY, Pan JS, Zhang XL, Zhang YZ. Axial and tangential views of the acromioclavicular joint: the introduction of new projections. Chin Med J. 2012;125(14):2493–2498. [PubMed] [Google Scholar]
- 101.Mah JM. General health status after nonoperative versus operative treatment for acute, complete acromioclavicular joint dislocation: results of a multicenter randomized clinical trial. J Orthop Trauma. 2017;31(9):485–490. doi: 10.1097/BOT.0000000000000881. [DOI] [PubMed] [Google Scholar]
- 102.Kany J, Amaravathi RS, Guinand R, Valenti P. Arthroscopic acromioclavicular joint reconstruction using a synthetic ligament device. Eur J Orthop Surg Traumatol. 2012;22(5):357–364. doi: 10.1007/s00590-011-0856-0. [DOI] [Google Scholar]
- 103.Mares O, Luneau S, Staquet V, Beltrand E, Bousquet P-J, Maynou C. Acute grade III and IV acromioclavicular dislocations: outcomes and pitfalls of reconstruction procedures using a synthetic ligament. Orthop Traumatol Surg Res. 2010;96(7):721–726. doi: 10.1016/j.otsr.2010.06.004. [DOI] [PubMed] [Google Scholar]
- 104.Giannotti S, Dell’Osso G, Bugelli G, Cazzella N, Guido G. Surgical treatment of acromioclavicular dislocation with LARS artificial ligament. Eur J Orthop Surg Traumatol. 2013;23(8):873–876. doi: 10.1007/s00590-012-1113-x. [DOI] [PubMed] [Google Scholar]
- 105.Choi SW, Lee TJ, Moon KH, Cho KJ, Lee SY. Minimally invasive coracoclavicular stabilization with suture anchors for acute acromioclavicular dislocation. Am J Sports Med. 2008;36(5):961–965. doi: 10.1177/0363546507312643. [DOI] [PubMed] [Google Scholar]
- 106.Huang T-W, Hsieh P-H, Huang K-C, Huang K-C. Suspension suture augmentation for repair of coracoclavicular ligament disruptions. Clin Orthop Relat Res. 2009;467(8):2142–2148. doi: 10.1007/s11999-008-0684-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Lu N, Zhu L, Ye T, Chen A, Jiang X, Zhang Z, Zhu Q, Guo Q, Yang D. Evaluation of the coracoclavicular reconstruction using LARS artificial ligament in acute acromioclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2014;22(9):2223–2227. doi: 10.1007/s00167-013-2582-0. [DOI] [PubMed] [Google Scholar]
- 108.Horst K, Dienstknecht T, Pishnamaz M, Sellei RM, Kobbe P, Pape H-C. Operative treatment of acute acromioclavicular joint injuries graded Rockwood III and IV: risks and benefits in tight rope technique vs. k-wire fixation. Patient Saf Surg. 2013;7(1):18. doi: 10.1186/1754-9493-7-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Glanzmann MC, Buchmann S, Audige L, Kolling C, Flury M. Clinical and radiographical results after double flip button stabilization of acute grade III and IV acromioclavicular joint separations. Arch Orthop Trauma Surg. 2013;133(12):1699–1707. doi: 10.1007/s00402-013-1858-7. [DOI] [PubMed] [Google Scholar]
- 110.Martetschläger F, Tauber M, Habermeyer P, Hawi N. Arthroscopically assisted acromioclavicular and coracoclavicular ligament reconstruction for chronic acromioclavicular joint instability. Arthroscopy techniques. 2016;5(6):e1239–e1246. doi: 10.1016/j.eats.2016.07.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Chernchujit B, Tischer T, Imhoff AB. Arthroscopic reconstruction of the acromioclavicular joint disruption: surgical technique and preliminary results. Arch Orthop Trauma Surg. 2006;126(9):575–581. doi: 10.1007/s00402-005-0073-6. [DOI] [PubMed] [Google Scholar]
- 112.Elser F, Chernchujit B, Ansah P, Imhoff AB. A new minimally invasive arthroscopic technique for reconstruction of the acromioclavicular joint. Unfallchirurg. 2005;108(8):645–649. doi: 10.1007/s00113-005-0933-0. [DOI] [PubMed] [Google Scholar]
- 113.Rolf O, von Weyhern AH, Ewers A, Boehm TD, Gohlke F. Acromioclavicular dislocation Rockwood III–V: results of early versus delayed surgical treatment. Arch Orthop Trauma Surg. 2008;128(10):1153–1157. doi: 10.1007/s00402-007-0524-3. [DOI] [PubMed] [Google Scholar]
- 114.Wellmann M, Kempka JP, Schanz S, Zantop T, Waizy H, Raschke MJ, Petersen W. Coracoclavicular ligament reconstruction: biomechanical comparison of tendon graft repairs to a synthetic double bundle augmentation. Knee Surg Sports Traumatol Arthrosc. 2009;17(5):521–528. doi: 10.1007/s00167-009-0737-9. [DOI] [PubMed] [Google Scholar]
- 115.Wickham M, Wyland D, Glisson R, Speer K. A biomechanical comparison of suture constructs used for coracoclavicular fixation. J South Orthop Assoc. 2003;12(3):143–148. [PubMed] [Google Scholar]
- 116.Dawson PA, Adamson GJ, Pink MM, Kornswiet M, Lin S, Shankwiler JA, Lee TQ. Relative contribution of acromioclavicular joint capsule and coracoclavicular ligaments to acromioclavicular stability. J Shoulder Elb Surg. 2009;18(2):237–244. doi: 10.1016/j.jse.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 117.Martetschläger F, Buchholz A, Sandmann G, Siebenlist S, Döbele S, Hapfelmeier A, Stöckle U, Millett PJ, Elser F, Lenich A. Acromioclavicular and coracoclavicular PDS augmentation for complete AC joint dislocation showed insufficient properties in a cadaver model. Knee Surg Sports Traumatol Arthrosc. 2013;21(2):438–444. doi: 10.1007/s00167-012-2067-6. [DOI] [PubMed] [Google Scholar]
- 118.Schliemann B, Lenschow S, Schürmann P, Schroeglmann M, Herbort M, Kösters C, Raschke MJ. Biomechanics of a new technique for minimal-invasive coracoclavicular ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2013;21(5):1176–1182. doi: 10.1007/s00167-012-2041-3. [DOI] [PubMed] [Google Scholar]
- 119.Abat F, Sarasquete J, Natera LG, Calvo A, Pérez-Espana M, Zurita N, Ferrer J, Del Real JC, Paz-Jimenez E, Forriol F. Biomechanical analysis of acromioclavicular joint dislocation repair using coracoclavicular suspension devices in two different configurations. J Orthop Traumatol. 2015;16(3):215–219. doi: 10.1007/s10195-015-0346-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Walz L, Salzmann GM, Fabbro T, Eichhorn S, Imhoff AB. The anatomic reconstruction of acromioclavicular joint dislocations using 2 TightRope devices: a biomechanical study. Am J Sports Med. 2008;36(12):2398–2406. doi: 10.1177/0363546508322524. [DOI] [PubMed] [Google Scholar]
- 121.Ferreira JV, Chowaniec D, Obopilwe E, Nowak MD, Arciero RA, Mazzocca AD. Biomechanical evaluation of effect of coracoid tunnel placement on load to failure of fixation during repair of acromioclavicular joint dislocations. Arthroscopy. 2012;28(9):1230–1236. doi: 10.1016/j.arthro.2012.02.004. [DOI] [PubMed] [Google Scholar]
- 122.Coale RM, Hollister SJ, Dines JS, Allen AA, Bedi A. Anatomic considerations of transclavicular-transcoracoid drilling for coracoclavicular ligament reconstruction. J Shoulder Elb Surg. 2013;22(1):137–144. doi: 10.1016/j.jse.2011.12.008. [DOI] [PubMed] [Google Scholar]
- 123.Xue C, Zhang M, Zheng T-S, Zhang G-Y, Fu P, Fang J-H, Li X. Clavicle and coracoid process drilling technique for truly anatomic coracoclavicular ligament reconstruction. Injury. 2013;44(10):1314–1320. doi: 10.1016/j.injury.2013.06.022. [DOI] [PubMed] [Google Scholar]
- 124.Spiegl UJ, Smith SD, Euler SA, Dornan GJ, Millett PJ, Wijdicks CA. Biomechanical consequences of Coracoclavicular reconstruction techniques on clavicle strength. Am J Sports Med. 2014;42(7):1724–1730. doi: 10.1177/0363546514524159. [DOI] [PubMed] [Google Scholar]
- 125.Rylander LS, Baldini T, Mitchell JJ, Messina M, Ellis IAJ, McCarty EC. Coracoclavicular ligament reconstruction: coracoid tunnel diameter correlates with failure risk. Orthopedics. 2014;37(6):e531–e535. doi: 10.3928/01477447-20140528-52. [DOI] [PubMed] [Google Scholar]
- 126.Barth J, Duparc F, Andrieu K, Duport M, Toussaint B, Bertiaux S, Clavert P, Gastaud O, Brassart N, Beaudouin E. Is coracoclavicular stabilisation alone sufficient for the endoscopic treatment of severe acromioclavicular joint dislocation (Rockwood types III, IV, and V)? Orthop Traumatol Surg Res. 2015;101(8):S297–S303. doi: 10.1016/j.otsr.2015.09.003. [DOI] [PubMed] [Google Scholar]
- 127.Klimkiewicz JJ, Williams GR, Sher JS, Karduna A, Des Jardins JD, Iannotti JP. The acromioclavicular capsule as a restraint to posterior translation of the clavicle: a biomechanical analysis. J Shoulder Elb Surg. 1999;8(2):119–124. doi: 10.1016/S1058-2746(99)90003-4. [DOI] [PubMed] [Google Scholar]
- 128.Morikawa D, Dyrna F, Cote MP, Johnson JD, Obopilwe E, Imhoff FB, Beitzel K, Mazzocca AD, Scheiderer B. Repair of the entire superior acromioclavicular ligament complex best restores posterior translation and rotational stability. Knee Surg Sports Traumatol Arthrosc. 2019;27(12):3764–3770. doi: 10.1007/s00167-018-5205-y. [DOI] [PubMed] [Google Scholar]
- 129.Breslow MJ, Jazrawi LM, Bernstein AD, Kummer FJ, Rokito AS. Treatment of acromioclavicular joint separation: suture or suture anchors? J Shoulder Elb Surg. 2002;11(3):225–229. doi: 10.1067/mse.2002.123904. [DOI] [PubMed] [Google Scholar]
- 130.Yi Y, Kim JW. Coronal plane radiographic evaluation of the single TightRope technique in the treatment of acute acromioclavicular joint injury. J Shoulder Elb Surg. 2015;24(10):1582–1587. doi: 10.1016/j.jse.2015.02.022. [DOI] [PubMed] [Google Scholar]
- 131.Rosslenbroich SB, Schliemann B, Schneider KN, Metzlaff SL, Koesters CA, Weimann A, Petersen W, Raschke MJ. Minimally invasive coracoclavicular ligament reconstruction with a Flip-button technique (MINAR) clinical and radiological midterm results. Am J Sports Med. 2015;43(7):1751–1757. doi: 10.1177/0363546515579179. [DOI] [PubMed] [Google Scholar]
- 132.Tauber M, Valler D, Lichtenberg S, Magosch P, Moroder P, Habermeyer P. Arthroscopic stabilization of chronic acromioclavicular joint dislocations: triple-versus single-bundle reconstruction. Am J Sports Med. 2016;44(2):482–489. doi: 10.1177/0363546515615583. [DOI] [PubMed] [Google Scholar]
- 133.Tiefenboeck T, Boesmueller S, Popp D, Payr S, Joestl J, Binder H, Schurz M, Komjati M, Fialka C, Ostermann R. The use of the LARS system in the treatment of AC joint instability–long-term results after a mean of 7.4 years. Orthop Traumatol Surg Res. 2018;104(6):749–754. doi: 10.1016/j.otsr.2018.02.010. [DOI] [PubMed] [Google Scholar]
- 134.Rabalais RD, McCarty E. Surgical treatment of symptomatic acromioclavicular joint problems: a systematic review. Clin Orthop Relat Res. 2007;455:30–37. doi: 10.1097/BLO.0b013e31802f5450. [DOI] [PubMed] [Google Scholar]
- 135.Woodmass JM, Esposito JG, Ono Y, Nelson AA, Boorman RS, Thornton GM, Lo IK. Complications following arthroscopic fixation of acromioclavicular separations: a systematic review of the literature. Open access journal of sports medicine. 2015;6:97. doi: 10.2147/OAJSM.S73211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Maier D, Tuecking L-R, Bernstein A, Lang G, Wagner FC, Jaeger M, Ogon P, Südkamp NP, Izadpanah K. The acromioclavicular ligament shows an early and dynamic healing response following acute traumatic rupture. BMC Musculoskelet Disord. 2020;21(1):1–11. doi: 10.1186/s12891-020-03614-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Flint JH, Wade AM, Giuliani J, Rue JP. Defining the terms acute and chronic in orthopaedic sports injuries: a systematic review. Am J Sports Med. 2014;42(1):235–241. doi: 10.1177/0363546513490656. [DOI] [PubMed] [Google Scholar]
- 138.Braun S, Martetschlager F, Imhoff AB. Arthroscopically assisted reconstruction of acute and chronic AC joint separations. Oper Orthop Traumatol. 2014;26(3):228–236. doi: 10.1007/s00064-013-0276-x. [DOI] [PubMed] [Google Scholar]
- 139.Voss A, Beitzel K, Alaee F, Dukas A, Herbst E, Obopilwe E, Apostolakos J, DiVenere J, Singh H, Cote MP. A biomechanical analysis of different clavicular tunnel diameters in anatomic acromioclavicular ligament reconstruction. Arthroscopy. 2016;32(8):1551–1557. doi: 10.1016/j.arthro.2016.01.050. [DOI] [PubMed] [Google Scholar]
- 140.Thangaraju S, Tauber M, Habermeyer P, Martetschlager F. Clavicle and coracoid process periprosthetic fractures as late post-operative complications in arthroscopically assisted acromioclavicular joint stabilization. Knee Surg Sports Traumatol Arthrosc. 2019;27(12):3797–3802. doi: 10.1007/s00167-019-05482-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All authors had unrestricted access to all the data of this study. Raw data can be requested from the corresponding author.