

A 47-year-old man who had undergone subtotal stomach-preserving pancreatoduodenectomy presented with recurrent cholangitis, possibly due to a hepaticojejunostomy anastomosis (HJA) stricture ( Fig. 1 ). Endoscopic retrograde cholangiopancreatography using short-type single-balloon endoscopy was planned. However, as the HJA was completely occluded by a fibrous membrane, we could not insert the cannula into the bile duct. Therefore, we performed endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS).
Fig. 1.
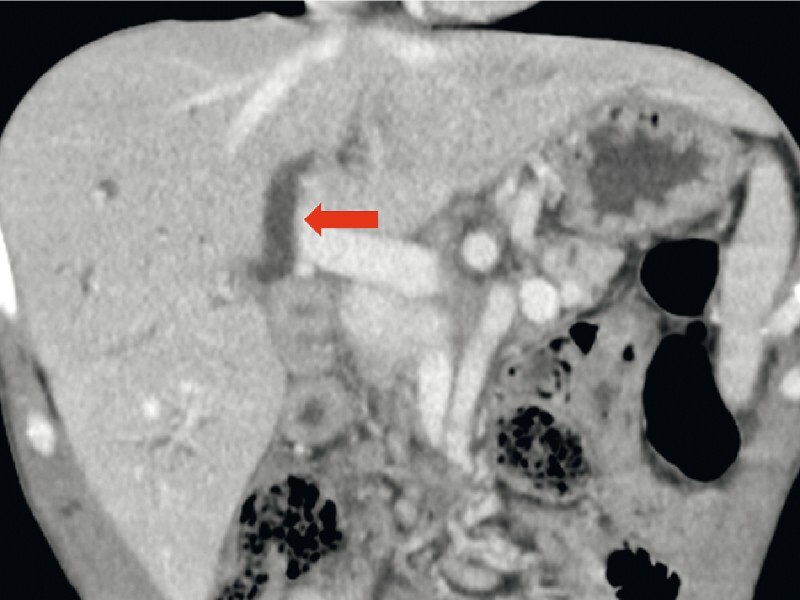
Computed tomography image showing the dilated intrahepatic bile duct (arrow).
The dilated intrahepatic bile duct (B3) was punctured with a 19-gauge needle (EZ shot 3 plus: Olympus Co., Tokyo, Japan). However, no contrast medium flowed from the dilated bile duct to the jejunum, and a 0.025-inch guidewire could not be inserted across the anastomosis ( Fig. 2 ).
Fig. 2.
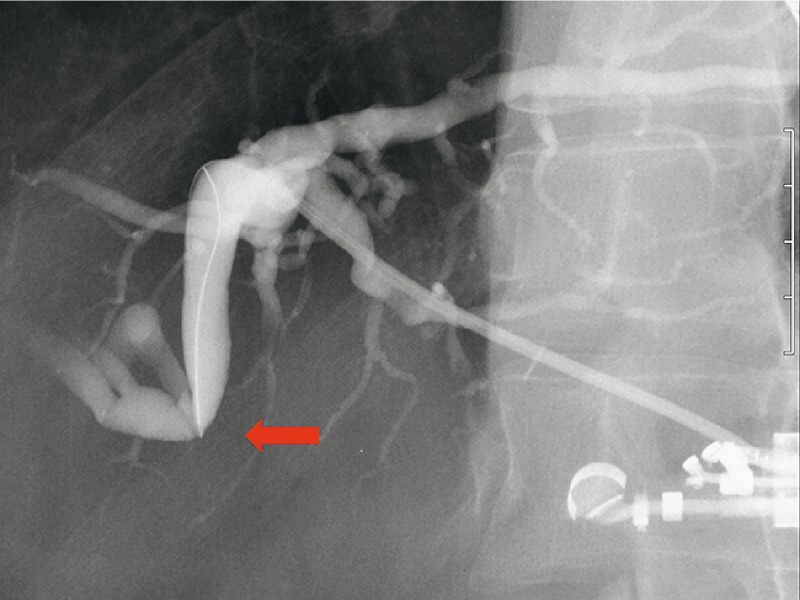
During fluoroscopy, no contrast medium flowed out of the dilated bile duct (arrow).
One month after EUS-HGS, a 7-Fr plastic stent was exchanged for a 6-mm, fully covered, self-expandable metal stent (HANAROSTENT Biliary; M.I. Tech, Gyeonggi-do, Korea) across the EUS-HGS route ( Fig. 3 ). A SpyGlass DS system (Boston Scientific Corp., Marlborough, Massachusetts, USA) was used to perform cholangioscopy to visualize the anastomosis from the inside of the bile duct ( Video 1 ). We found that the duct was completely obstructed at the anastomotic site and covered with a fibrous membrane ( Fig. 4 a ). It was difficult to break through this obstruction even with cholangioscopy guidance. Repeated poking with a stiff edge of a guidewire partially broke the fibrous membrane, and a guidewire could finally be passed thorough the anastomosis; however, a 4-Fr catheter could not be passed through the anastomosis. We dilated the anastomosis stricture by gradually removing the fibrotic tissue using biopsy forceps (SpyBite MAX; Boston Scientific Corp.) under direct cholangioscopic observation ( Fig. 4 b ). After dilation of the anastomosis using a 7-Fr catheter and a 6-mm balloon catheter, antegrade transanastomotic placement of a 7-Fr plastic stent across the EUS-HGS route was performed. No procedure-related adverse events were observed, and cholangitis improved after treatment.
Fig. 3.

A 6-mm, fully covered, self-expandable metal stent was inserted across the endoscopic ultrasound-guided hepaticogastrostomy route.
Fig. 4.

Cholangioscopy and fluoroscopy images. a Cholangioscopic image showing the completely obstructed bile duct at the anastomotic site covered with fibrous membrane (arrowheads). b Biopsy forceps were used to remove the fibrotic tissue before dilation of the anastomosis under direct cholangioscopic observation.
Video 1 Endoscopic ultrasound (EUS)-guided antegrade intervention for complete obstruction of a hepaticojejunostomy anastomosis under peroral cholangioscopy via an EUS-guided hepaticogastrostomy route.
Although EUS-guided drainage for stenosis of the HJA has been reported 1 , complete obstruction makes it difficult to recanalize the anastomosis using endoscopic procedures. Recently, the usefulness of cholangioscopy through a percutaneous transhepatic or transpapillary route for postoperative biliary strictures or obstructions has been described 2 3 . EUS-guided antegrade intervention under cholangioscopy via an EUS-HGS route is an alternative treatment.
Endoscopy_UCTN_Code_TTT_1AR_2AG
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.James T W, Fan Y C, Baron T H. EUS-guided hepaticoenterostomy as a portal to allow definitive antegrade treatment of benign biliary disease in patients with surgically altered anatomy. Gastrointest Endosc. 2018;88:547–554. doi: 10.1016/j.gie.2018.04.2353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fujii Y, Koshita S, Ito K. Percutaneous transhepatic cholangioscopy using SpyGlass DS for an anastomotic stenosis after choledochojejunostomy. Dig Endosc. 2018;30:806–807. doi: 10.1111/den.13252. [DOI] [PubMed] [Google Scholar]
- 3.Yane K, Ihara H, Sumiyoshi T et al. Successful recanalization of complete bile duct obstruction using piercing technique under cholangioscopic guidance. Endoscopy. 2021 doi: 10.1055/a-1540-6735. [DOI] [PubMed] [Google Scholar]