

To the Editor:
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Fukuhara and colleagues1 reported, in a recent and interesting article, their clinical retrospective series on the use of laser septal fenestration as an adjunct to accurately and efficiently optimize the distal landing zone during thoracic endovascular aortic repair (TEVAR) procedure in chronic type B aortic dissections (cTBAD).
Despite significant progress, TEVAR is hindered by persistent perfusion of the false lumen (FL) and aneurysm growth. Various techniques to address FL perfusion exist. As the authors stated, 2 approaches are possible; the first, through the obliteration of the FL, and the second through the creation of a common aortic lumen as the optimized distal landing zone. Both methods have pros and cons: the use of over instructions for use devices, costs, and the accidental occlusion of branch vessels in the first method, and the rare possibility of aortic rupture in the other.
In this experience, the authors perform a laser fenestration approximately 6 to 10 cm proximal to the intended distal TEVAR landing zone, cannulating a single lumen (true lumen or FL), and subsequently release the stent graft in the true lumen with possible postdilation in case of incomplete expansion. The results are excellent, with elimination of retrograde FL flow and, although the follow-up is short (median 8.2 months), with positive aortic remodeling with complete exclusion of the FL in 90% of cases.
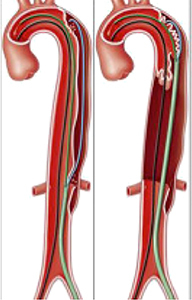
In our experience in the treatment of cTBAD, we have recently (in the last 3 years) preferred to use a scissor-technique (Figure 1)2 after creating a re-entry tear by laser (3 cases) or needle (5 cases) fenestration and subsequent release of the stent graft with 5% to 10% oversizing of the total aortic diameter. We observed technical success of FL exclusion in 100% of cases with complete remodeling in 87.5% of cases in a mean follow-up of 13 months.3, 4, 5, 6
Figure 1.
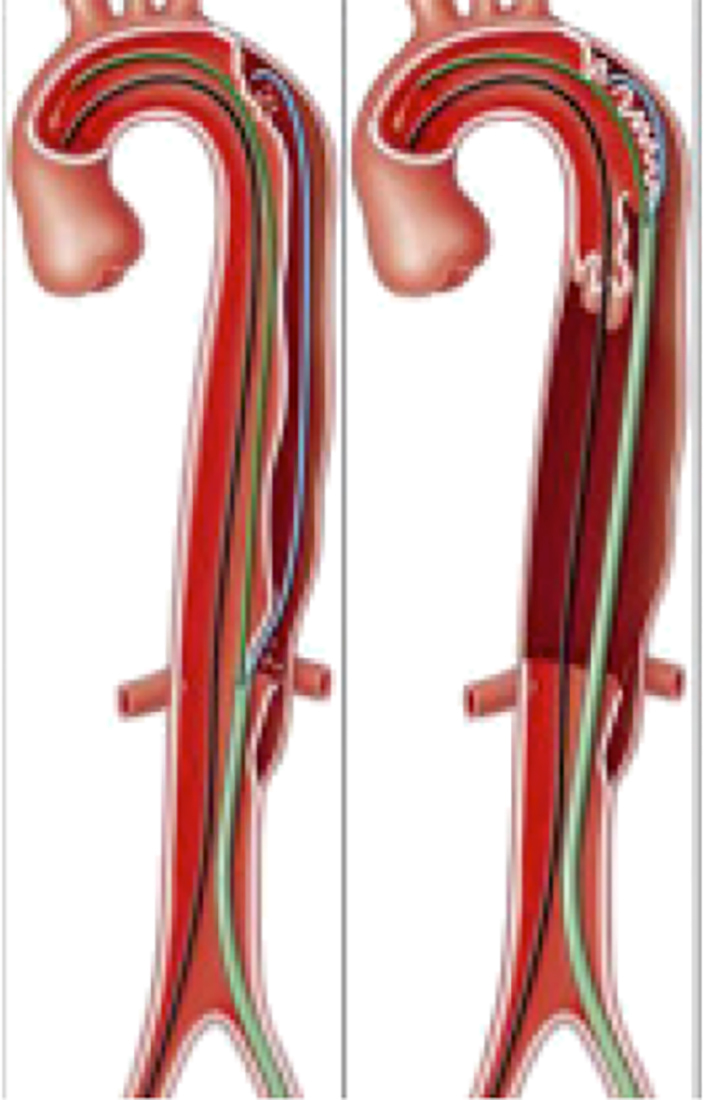
Aortic septotomy with scissor-technique.
We agree with the authors' statement to choose the distal landing zone at most proximal aortic segment with a normal caliber of its total aortic diameter. Differently, we prefer to have the simultaneous control of the 2 lumens in case of fenestration through the FL and create the new entry tear distal to the TEVAR landing zone.
In conclusion, we believe that the described procedure provides a safe and reliable tool and improves the current armamentarium in the endovascular treatment of cTBAD, and that laser fenestration is increasingly widespread in endovascular procedures.
References
- 1.Fukuhara S., Tchouta L., Pampati R., Liesman D.R., Khaja M.S. Laser aortic septotomy during thoracic endovascular aortic repair for chronic type B aortic dissection. J Thorac Cardiovasc Surg. 2022;164:450–459. doi: 10.1016/j.jtcvs.2020.08.084. [DOI] [PubMed] [Google Scholar]
- 2.Alomran F., Alsac J.M. Distal Endovascular Fenestration INsIde Thoracic Exclusion: the DEFINITE technique for complicated acute type B aortic dissections. Eur J Vasc Endovasc Surg. 2017;53:103. doi: 10.1016/j.ejvs.2016.11.005. [DOI] [PubMed] [Google Scholar]
- 3.Odero A., Bozzani A., Pirrelli S. Endovascular treatment of acute type B dissection and Kommerell's diverticulum. Ann Thorac Surg. 2007;84:1736–1738. doi: 10.1016/j.athoracsur.2007.05.077. [DOI] [PubMed] [Google Scholar]
- 4.Arici V., Bozzani A., Odero A. Successful endovascular treatment of a bronchial artery aneurysm refractory to transcatheter embolization. Ann Vasc Surg. 2013;27:802.e13–802.e15. doi: 10.1016/j.avsg.2012.07.029. [DOI] [PubMed] [Google Scholar]
- 5.Bozzani A., Arici V., Bonalumi G., Argenteri A. Descending thoracic aorta remodeling after multilayer stent release. Ann Vasc Surg. 2015;29:1018.e9–1018.e11. doi: 10.1016/j.avsg.2015.01.016. [DOI] [PubMed] [Google Scholar]
- 6.Pirrelli S., Bozzani A., Arici V., Odero A. Complete aortic arch remodeling after stent graft of acute type B dissection and Kommerell's diverticulum. Ann Thorac Surg. 2012;93:673. doi: 10.1016/j.athoracsur.2011.06.065. [DOI] [PubMed] [Google Scholar]