

The in situ left ITA was the sole blood source for the LAD graft and the right ITA graft.
Central Message.
In CABG for HD patients, an in situ ITA graft ipsilateral to the upper-extremity AVF as a sole graft inflow should be avoided to prevent aggravation of hemodynamics induced by coronary steal.
In coronary artery bypass grafting for patients requiring chronic hemodialysis, there is the possibility of coronary steal associated with using an in situ internal thoracic artery (ITA) graft ipsilateral to an upper-extremity arteriovenous fistula (AVF). Here, we present a case of in situ left ITA graft ipsilateral to the AVF as the sole bypass graft inflow. Immediately after surgery, the patient experienced shock requiring cardiopulmonary resuscitation.
The data for this report were collected with the approval of the patient and Regional Ethics Committee of Asahikawa Medical University (approval date, April 22, 2020; reference no. 20108). The patient of this case report was provided informed consent appropriately. We also note that the identity of the patient has been protected.
Case Presentation
A 59-year-old woman presented to our institution with unstable angina via referral. The patient had end-stage renal disease and had been undergoing dialysis for 11 years. Blood access for dialysis was ensured through a left radiocephalic AVF. Coronary angiography showed a 90% in-stent restenosis in the right coronary artery, 90% stenosis in the left anterior descending artery (LAD), and chronic total occlusion of the left circumflex branch.
We performed on-pump coronary artery bypass grafting using the bilateral ITA for the composite T-graft technique. The in situ left ITA was anastomosed to the LAD, and the right ITA was implanted into the left ITA as a T-graft and was revascularized to the obtuse marginal branches and vessels of the right coronary artery. Therefore, the in situ left ITA was the sole blood source for the LAD and right ITA grafts. No additional vein graft was used because the left lower limb had already undergone an above-the-knee amputation, and the right saphenous vein graft was preserved for lower-extremity bypass due to chronic limb-threatening ischemia. The right gastroepiploic artery was unfeasible due to arteriosclerotic change, and radial arteries were unavailable for AVF. Although the intraoperative flow measurements of the left and right ITAs were both sufficient after weaning from cardiopulmonary bypass, hemodynamics temporarily failed in the patient, and internal cardiac massage was required. Subsequently, hemodynamic stability was obtained without any circulatory assist devices.
However, 1 hour after entering the intensive care unit, the patient experienced shock and was unresponsive to cardiopulmonary resuscitation. Subsequently, internal cardiac massage was successfully performed, and under central extracorporeal membrane oxygenation and intra-aortic balloon pumping, the hemodynamic status was stabilized. On postoperative day 1, central extracorporeal membrane oxygenation decannulation and AVF ligation were performed simultaneously. On postoperative day 5, intra-aortic balloon pumping was decannulated.
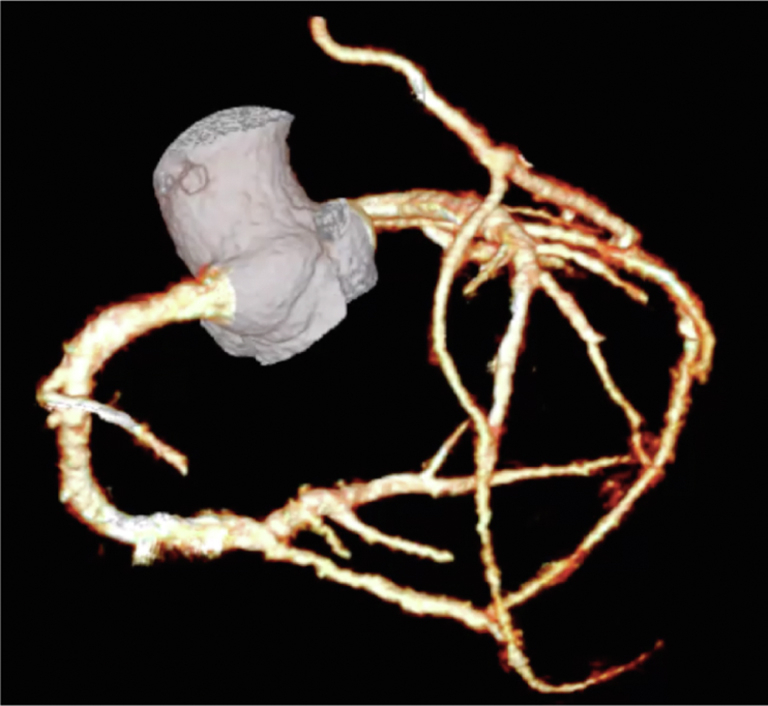
The patient had a stable postoperative course without the occurrence of cardiovascular events. Superficialization of the left brachial artery was performed, and hemodialysis was conducted uneventfully. Postoperative contrast-enhanced multislice computed tomography demonstrated patency of both in situ left ITA and right ITA grafts (Figure 1). The patient was discharged ambulatory and remained symptom-free for 2 years postoperatively.
Figure 1.

A and B, Postoperative contrast-enhanced multislice computed tomography demonstrated patency of both in situ left ITA graft to the left anterior descending artery and the right ITA implanted into the left ITA as a T-graft to the obtuse marginal branches and vessels of the right coronary artery.
Discussion
Whether in situ ITA graft ipsilateral to the upper-extremity AVF causes coronary steal remains debatable. Previous studies reported that the risk of cardiac events was more significant in the group with ipsilateral ITA grafts and AVFs than in the group with contralateral ones.1,2 In contrast, Hachiro and colleagues3 reported that in situ ITA grafts ipsilateral to the AVF were not associated with worse postoperative outcomes. However, in their study, the ipsilateral in situ ITA graft group contained bilateral ITA used as a separate graft and gastroepiploic artery and/or saphenous vein graft used as individual grafts. Securing the blood supply from multiple conduits may contribute to the hydrodynamic stability. In this respect, in our case, the in situ left ITA served as the sole blood inflow; therefore, even a slight flow reduction may affect all revascularized branches, leading to acute hemodynamic compromise. Meanwhile, in our case, to resolve coronary steal, AVF ligation was performed. However, it is worth noting that anastomosing the proximal left ITA on the ascending aorta may resolve the problem to secure blood supply which was unaffected by the AVF location.
Several procedures can be performed to prevent coronary steal. Hachiro and colleagues3 reported that for preoperative differences of ≥20 mm Hg between the blood pressure of both upper arms preoperatively, the lower value side of the ITA was avoided because subclavian artery stenosis was suspected. Minami and colleagues4 pointed out the usefulness of intraoperative transit-time flow measurements of the ITA graft.
Considering that a low left ventricular ejection fraction was indicated as a risk factor for a coronary steal,5 for patients requiring chronic hemodialysis with decreased cardiac reserve, use of in situ ITA ipsilateral to the AVF, especially in composite grafts, should be avoided to prevent aggravation of hemodynamics induced by coronary steal.
Footnotes
Disclosures: The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
References
- 1.Feldman L., Tkacheva I., Efrati S., Rabin I., Beberashvili I., Gorelik O., et al. Effect of arteriovenous hemodialysis shunt location on cardiac events in patients having coronary artery bypass graft using an internal thoracic artery. Ther Apher Dial. 2014;18:450–454. doi: 10.1111/1744-9987.12158. [DOI] [PubMed] [Google Scholar]
- 2.Shim H., Jeong D.S., Kim W.S., Park P.W., Sung K., Jeon C.S., et al. Impact of arteriovenous fistula for hemodialysis on clinical outcomes of coronary artery bypass. Ann Thorac Surg. 2018;106:1820–1826. doi: 10.1016/j.athoracsur.2018.06.071. [DOI] [PubMed] [Google Scholar]
- 3.Hachiro K., Kinoshita T., Suzuki T., Asai T. Internal thoracic artery graft ipsilateral to the arteriovenous fistula in haemodialysis patients. Interact Cardiovasc Thorac Surg. 2021;32:864–872. doi: 10.1093/icvts/ivab022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Minami T., Uranaka Y., Tanaka M., Negishi K., Uchida K., Masuda M. Coronary subclavian steal syndrome detected during coronary bypass surgery in a hemodialysis patient. J Card Surg. 2015;30:154–156. doi: 10.1111/jocs.12444. [DOI] [PubMed] [Google Scholar]
- 5.Ahn S., Han A., Kim S.Y., Choi C., Min S.I., Ha J., et al. The incidence and risk factors of coronary steal after ipsilateral AVF in patients with a coronary artery bypass graft. J Vasc Access. 2017;18:290–294. doi: 10.5301/jva.5000690. [DOI] [PubMed] [Google Scholar]